paediatric and child health_self assessment_all_2009
TRANSCRIPT

Egyptian_Pediatric yahoo group
http://health.groups.yahoo.com/group/egyptian_pediatric/
Egyptian_Pediatric yahoo group
http://health.groups.yahoo.com/group/egyptian_pediatric/
self-assessment
Paediatrics and child health 19:1 50 © 2008 elsevier ltd. all rights reserved.
Questions
Question 1A 3-year-old boy presents with septic shock secondary to meningococcal septicaemia, and is treated in the regional pae-diatric intensive care unit (PICU). He is treated with 7 days of intravenous (i.v.) ceftriaxone 50 mg/kg daily. He required 180 ml/kg of fluid in the first 24 hours, received adrenaline and milrinone infusions until day 3, but was successfully extu-bated on day 4, and returned to the ward on day 5. He has not had a lumbar puncture.
It is now day 7, and his antibiotics are due to be discontinued.
His mother reports he is less well in the past 24 hours – he is miserable and does not want to get out of bed. He says his leg is sore. The discharge summary from PICU shows that he had been afebrile since day 2. He had his urinary catheter and central venous line removed on the day of discharge form PICU.
On examination he has a temperature of 38.8 °C. He has a few maculopapular spots on his trunk and upper arms, and two of them appear blistered. There are no petechiae. The rash is new. His chest is clear, his abdomen soft and his heart sounds normal. He has no neck stiffness. He has a slightly swollen right knee, with slight restriction of flexion due to pain.
His blood results from this morning are as follows:
hb 12 g/dl na 139 mmol/l
WBc 22 × 109/l K 3.2 mmol/l
neutrophils 17 × 109/l Urea 5.3 mmol/l
lymphocytes 4 × 109/l creatinine 29 μmol/l
Platelets 432 × 109/l
crP 89 mg/l (31 previous
day)
(a) What is the most likely diagnosis? Chose ONE of the following:Drug reactionRecurrent meningococcal septicaemiaSeptic arthritisPost-meningococcal immune complex mediated diseaseIncompletely treated meningitis
Question 2A 1-year-old boy weighing 11 kg has been transferred to PICU after presenting to his local hospital with a 48-hour history of lethargy, poor feeding and fever, culminating in a prolonged tonic seizure. He needed to be intubated and ventilated during the seizure after being treated with lorazepam, phenytoin and
Allan Wardhaugh MB ChB MRCPCH MRCGP DRCOG is a Consultant in
Paediatric Intensive Care at University Hospital of Wales Cardiff, UK.
self-assessment
paraldehyde. The seizure stopped as he was given thiopentone to induce anaesthesia. The total duration of seizure time was 55 minutes.
He is ventilated with pressures of 22/6cm H2O at 25 per minute and 40% oxygen giving a tidal volume of 90 ml, oxy-gen saturations of 100%. He has an area of right upper zone consolidation on his chest x-ray.
His heart rate is 125/min, blood pressure 90/45mm Hg, mean 60mm Hg, with a capillary refill time of 2 seconds. He has required three 20 ml/kg boluses of 0.9% saline in the past 4 hours and has not been started on inotropes. His i.v. mainte-nance fluid is running at 100% of normal requirements.
He had a computed tomography (CT) of his head with con-trast, which showed a degree of meningeal enhancement, but is otherwise normal.
He is sedated with morphine and midazolam infusions. He has been treated with aciclovir and ceftriaxone.
Blood results are shown:
hb 11.1 g/dl na 139 mmol/l
WBc 16.4 × 109/l K 3.7 mmol/l
neutrophils 11.9 × 109/l Urea 2.6 mmol/l
lymphocytes 3.1 × 109/l creatinine 22 μmol/l
Platelets 194 × 109/l
arterial gas
crP 142 mg/l ph 7.26
pcO2 6.9 kPa
pO2 18.4 kPa
hcO3 21 mmol/l
Base excess −8.1 mmol/l
chloride 112 mmol/l
lactate 5.3 mmol/l
(a) Which of the following statements is true? Choose ONE of the following:Lumbar puncture should be performed nowHis ventilator settings should be changedInotropes should be startedHis i.v. fluid requirements should be restrictedHe should have a bolus of 20 ml/kg 4% human albumin
He remains relatively stable for the next 48 hours. Blood culture results have been telephoned through from his original hospital, and show Streptococcus pneumoniae. His observa-tion chart shows stable heart rate 120–130/min, blood pres-sure mean of 60 mmHg, stable and normal blood gases, urine output of 0.7 ml/kg/hour. His routine bloods for the day come back:
hb 7.6 g/dl na 129 mmol/l
WBc 12.4 × 109/l K 4.3 mmol/l
neutrophils 8.5 × 109/l Urea 14.5 mmol/l
lymphocytes 2.9 × 109/l creatinine 147 μmol/l
Platelets 44 × 109/l Phosphate 2.9 mmol/l
calcium (ionised) 1.03 mmol/l
crP 98 mg/l magnesium 0.81 mmol/l
self-assessment
Paediatrics and child health 19:1 51 © 2008 elsevier ltd. all rights reserved.
Pt 12 s
aPtt 31 s
fibrinogen 2.1 g/l
(b) What investigation should you do now? Choose ONE of the following:Stool cultureFerritinCoombs testBlood filmRenal ultrasound
(c) A provisional blood culture result is phoned through the following day and reports Gram-positive diplococci. What is the likely diagnosis? Choose ONE of the following:Haemolytic uraemic syndrome – pneumococcalDisseminated intravascular coagulationHaemolytic uraemic syndrome – Escherichia coli H7:0157Idiopathic thrombocytopeniaPrimary bone marrow failure
Question 3An 11-year-old boy presents with a swollen left ankle. He had presented to Accident and Emergency 3 days ago after having hurt his ankle playing football. An x-ray at that time showed no fracture, and he was sent home. Since then his ankle has remained swollen and red, but his parents think it is no worse than at onset. The previous day he developed diarrhoea. He has also complained of aching arms and legs. A repeat x-ray does not demonstrate any fracture, and shows only soft tissue swelling. You have been asked to give a paediatric opinion.
His past medical history is unremarkable, and there is no family history of note.
On examination his temperature is 39.1 °C, and he appears flushed. His heart rate is 120/minute, his capillary refill time is 2 seconds and his blood pressure is 84/38mm Hg. His respiratory rate is 24/minute. There is a 2 cm abrasion just above his medial malleolus, and his ankle is a little swollen and warm. It is painful to move, but he does have a full range of movement in the joint.
You suspect he has cellulitis, and admit him to the ward for intravenous penicillin and flucloxacillin after taking blood for culture, full blood count, urea and electrolytes, and C-reactive protein (CRP).
Over the next 12 hours he becomes more unwell. Nursing staff report him as being intermittently confused. His heart rate remains 120 per minute, and his systolic blood pressure is between 70 and 80 mmHg. He has developed a widespread erythematous rash which looks like sunburn, and has a bilat-eral conjunctivitis. His urine output is 0.3 ml/kg/hour.
His laboratory results from admission are below:
hb 9.8 g/dl na 131 mmol/l
WBc 4.8 × 109/l K 4.2 mmol/l
neutrophils 1.0 × 109/l Urea 10.2 mmol/l
lymphocytes 3.2 × 109/l creatinine 182 μmol/l
Platelets 44 × 109/l
crP 256 mg/l
(a) Which of the following diagnoses is most likely? Choose ONE of the following:Septic arthritisKawasaki diseaseStevens–Johnson syndromeNecrotising fasciitisToxic shock syndrome
(b) In addition, discussing him with an intensivist, and giving him a 20 ml/kg bolus of fluid, which one of the following would you do? Choose ONE of the following:Treat with intravenous clindamycinTreat with intravenous immunoglobulinStart high dose corticosteroidsObtain an ultrasound of his ankleObtain a paediatric nephrology opinion to arrange early dialysis
Answers
Question 1(a) Post-meningococcal immune complex mediated diseaseIn meningococcal disease, type 3 hypersensitivity reaction, or immune complex associated complications (IAC), can present as arthritis, vasculitis, episcleritis, or pericarditis. Nephritis is very rare. It usually takes 4–10 days after the onset of disease for the first symptoms and signs of IAC to develop.1
The diagnostic features are:
arthritis arthralgia, joint swelling and redness, limitation of
movement synovial fluid shows no bacteria, cultures
remain negative
Vasculitis Pustular, bullous, nodular lesions or rash
Pericarditis retrosternal pain, pericardial friction rub, ecG
abnormalities, cardiac enlargement on x-ray/ultrasound
Pleuritis Pleural effusion on x-ray. Pain on inspiration. impaired
percussion. Pleural rub
Up to 15% of children may show one or more of these fea-tures after severe meningococcal disease. There is typically a secondary fever (i.e. a fever occurs after the patient has been afebrile for some time), a raised CRP and a leucocytosis.
Although it is a diagnosis of exclusion, knowledge of its common incidence may prevent over-investigation of patients. Anti-inflammatory medication will relieve symptoms, and the course is benign and self-limiting in general. A pericardial effu-sion has the potential to cause more serious effects secondary to tamponade, but these features would be clinically manifest if significant.
Drug allergy (particularly penicillin) can cause this type of rash, but is often associated with an eosinophilia. It is much less common then IAC.
Partially treated meningitis, or recurrent meningococcal dis-ease are unlikely as the patient has had appropriate antibiotic therapy. Patients can have meningococcal disease more than once in their life, as there are different serotypes, but it would
self-assessment
Paediatrics and child health 19:1 52 © 2008 elsevier ltd. all rights reserved.
also prompt a search for defects in complement production or opsonisation, which are associated with recurrent meningo-coccal and pneumococcal infections.
Question 2(a) His ventilator settings should be changedCerebral blood flow is very closely associated with arterial partial pressure of carbon dioxide (pCO2). Increased pCO2 causes cerebral vasodilatation, and the increased cerebral blood flow can cause an increase in intracranial pressure if there is a lack of intracranial space to accommodate it, or a failure of normal cerebral circulatory autoregulation. In ven-tilated patients who are at risk of raised intracranial pressure, such as those with suspected meningitis, the target pCO2 is 4.5–5.0 kPa. This patient should have a change to ventilator parameters that reduce his minute ventilation, and his pCO2 re-checked 30 minutes after the change.
This presenting feature makes meningitis a possibility as an underlying diagnosis, especially given the appearances of meningeal enhancement. However, this patient was drowsy, and there is a possibility of raised intracranial pressure, which is a contraindication to lumbar puncture. Raised intracranial pressure may be present even if not demonstrated on a CT of the head.2 It would be safer to treat for meningo-encephalitis and perform a lumbar puncture once the child’s conscious level is shown to have improved – the biochemical and cel-lular changes within cerebrospinal fluid (CSF) will persist for 2–3 days after antibiotic treatment has started.3
His lactic acid levels are raised, but this is very common after a prolonged tonic clonic seizure, and his normal heart rate, perfusion and mean blood pressure would re-assure you that he does not have shock, and does not require inotropes. Likewise, there is no indication for a fluid bolus.
A popular misconception is that routine fluid restriction should be used in meningitis. This is not supported by pub-lished evidence – this patient will be started on routine fluid requirements, subsequently adjusted on the basis of clinical and laboratory information.
(b) Blood filmThe striking feature of this set of blood results is renal failure and an acute drop in haemoglobin and platelet count. The latter two often occur in sepsis secondary to a dilutional effect from fluid resuscitation, and disseminated intravascular coag-ulation. However, his coagulation profile is not supportive of disseminated intravascular coagulation. Haemolytic-uraemic syndrome (HUS) has to be a strong possibility, and a blood film will demonstrate the red cell fragmentation typical of this microangiopathic haemolytic anaemia.
(c) Haemolytic uraemic syndrome – pneumococcalAlthough E. coli H7:0157 is the most common cause of HUS in children, other bacteria such as Shigella dysenteriae produce the verocytotoxin (or shiga-like toxin) to produce HUS. The toxin acts on vascular endothelial cells to produce a multi-system vasculitis.
Streptococcus pneumoniae produces the enzyme neuramini-dase. This cleaves N-acetylneuraminic acid from cell mem-brane surfaces exposing a cryptantigen, Thomsen–Freidenreich antigen (T-antigen), on red blood cells, platelets and glomeru-lar capillaries. Most people possess a naturally occurring anti-body to this antigen, and the cells are attacked and destroyed. Some hospital laboratories will perform a confirmatory test demonstrating the presence of T-antigen.4 Pneumococcal HUS almost always occurs in children less than 2 years of age. The clinical course is more severe than non-pneumococ-cal, and the patients are more likely to require dialysis.5
Question 3(a) Toxic shock syndromeToxic shock syndrome (TSS) is caused by toxin-producing strains of Staphylococcus aureus or Streptococcus pyogenes (Group A streptococcus). Toxic shock syndrome toxin-1 (TSST-1) is best known in S. aureus infections, but other toxins are also produced and believed to function as ‘supe-rantigens’, causing a powerful stimulatory effect on T-cell proliferation, and increased production of inflammatory cytokines like tumour necrosis factor and interleukin-1 (IL-1).6
Clinical criteria have been defined for the diagnosis. For staphylococcal TSS these are:
Negative blood throat and CSF cultures (if taken); blood culture may be positive for S. aureus.
Negative serology for measles, leptospirosis or Rocky Mountain spotted fever.Major (all four must be met):
• Fever more than 38.9 °C
• Rash – diffuse macular erythroderma
• Hypotension – systolic nlood pressure less than 5th centile for age
• Desquamation –1 or 2 weeks after the acute illnessMulti-system involvement (three must be met)
• Gastrointestinal: vomiting or diarrhoea at onset
• Muscular: severe myalgia or creatine kinase level greater than twice upper limit of normal
• Mucous membranes: vaginal, oropharyngeal, or conjunctival hyperaemia
• Renal: urea or creatinine more than twice the upper limit of normal
• Hepatic: bilirubin, ALT or AST upper limit of normal
• Platelets less than 100 × 109/l
• Altered consciousness when fever and hypotension not present
The definition of staphylococcal TSS does not require the isolation of S. aureus, but that for streptococcal TSS requires isolation of Group A streptococcus from a normally sterile site (e.g. blood, CSF) to make a definite diagnosis, or isolation from a non-sterile site (e.g. throat, skin) to make a diagnosis of a probable case.
Clearly, because of the requirement for desquamation, the definitive diagnosis cannot be made while treatment is being initiated, so management is based on clinical suspicion.

self-assessment
Paediatrics and child health 19:1 53 © 2008 elsevier ltd. all rights reserved.
Although this patient had a suspected entry wound for infec-tion, a positive site for primary infection is less common in staphylococcal TSS than it is in streptococcal.
This patient grew S. aureus from blood culture and had a desquamating rash shortly before discharge from the PICU where he was admitted.
Kawasaki disease is also believed to be a superantigen-mediated disease, so clinical features are similar. However, it is most common in children less than 1 year old and very rare over the age of 5 years.
Septic arthritis is usually associated with restricted joint movement. Necrotising fasciitis is characterised by severe pain around the infection site, and a rapidly spreading cellulitis – the degree of pain in the early stages is often disproportionate to the clinical appearances. Stevens–Johnson syndrome produces a characteristic rash with target lesions and mucosal ulceration.
(b) Treat with intravenous clindamycinThe general principles of caring for critically ill patients apply, suing fluid boluses and inotropes are necessary to maintain organ perfusion and oxygenation. Many patients will require to be treated in an intensive care unit.
At this stage in treatment, the likely diagnosis is TSS, although whether it is streptococcal or staphylococcal is not certain. Clindamycin is known to suppress toxin production in both types, and so is added in to the antibiotic regimen. Antibiotic treatment is continued for a minimum of 10 days, but may be longer if the source of primary infection requires it (e.g. osteomyelitis).
Intravenous immunoglobulin may have a role, but evi-dence is not compelling. It is currently recommended for cases of TSS that are not responding to conventional treatment.
There is no place for high dose steroids in this condition. Steroids may be used if there is inotrope resistant hypoten-sion, but in physiological replacement doses in the manner recommended for treating septic shock.
The issue of whether this patient has a septic arthritis should be resolved, but it is not his most urgent problem, and will not change immediate management. Given the lack of impairment of joint mobility it is very unlikely. ◆
RefeRences
1 Goedvolk ca, ia von rosenstiel, Bos aP. immune complex
associated complications in the subacute phase of
meningococcal disease: incidence and literature review. Arch Dis
Child 2003; 88: 927–930.
2 rennick G, shann f, de campo J. cerebral herniation during
bacterial meningitis in children. BmJ 1993; 306: 953–955.
3 riordan fai, cant aJ. When to do a lumbar puncture. Arch Dis
Child 2002; 87: 235–7.
4 cabrera Gr, fortenberry Jd, Warshaw Bl, et al. hemolytic uremic
syndrome associated with invasive streptococcus pneumoniae
infection. Pediatrics 1998; 101: 699–703.
5 Brandt J, Wong c, mihm s, et al. invasive pneumococcal disease
and hemolytic uremic syndrome. Pediatrics 2002; 110: 371–376.
6 american academy of Pediatrics. toxic shock syndrome. in:
Pickering lK, ed. report of the committee on infectious diseases.
27th edn. elk Grove Village, il: red Book; 2006. american academy
of Pediatrics.

self-assessment
Questions
Case 1A 3-year-old boy presents to A&E with fever of 39°C, HR of 140/min, capillary refill time of 3–4 s and slightly drowsy. On further questioning, it is revealed that he had returned 2 weeks previously from an East African safari, and had taken the recommended malaria prophylaxis.
1. What are the two most likely diagnoses? Choose TWO answers from the following options:A. Plasmodium falciparum malariaB. Plasmodium vivax malariaC. Bacterial sepsisD. InfluenzaE. Dengue fever
2. Which of the following investigations should have priority? Chose ONE answer from the following options:A. Malarial blood filmB. Blood glucoseC. Arterial blood gasD. FBC
3. What should be the immediate management of this child? Chose ONE answer from the following options:A. Intravenous infusion of quinine sulphateB. Exchange transfusionC. Fluid restriction to 80% maintenance and intravenous
quinineD. Bolus of 20 ml/kg colloid or 0.9% saline.
4. With what definitive antimalarial treatment should this child be treated? Chose ONE answer from the following options:A. Parenteral quinine for 7 daysB. 3-day course of chloroquineC. Parenteral artesunateD. Intravenous quinine followed by a full course of oral
medication with either mefloquine, proguanil with atovaquone, or artemeter with lumefantrine
Case 2A 65-year-old woman visiting her family from India is admit-ted with a febrile illness and cough. She has a caseating lesion in the left upper lobe on chest X-ray and a sputum smear is positive for acid-fast bacilli. She had been staying with her daughter and grandchildren, who are 3 weeks, 18 months and 4 years old, respectively.
Jennifer Evans MD MRCPCH is a Consultant Paediatrician, University
Hospital of Wales, Cardiff, Wales, UK.
self-assessment
1. The 3-week-old baby is well and thriving. Which management plan should be followed? Chose ONE answer from the following options:A. Give BCG and keep under regular outpatient follow-upB. Perform a Mantoux test and if positive, treat with full
antituberculous treatment with isoniazid, rifampicin and pyrazinamide
C. Start on isoniazid 5 mg/kg and then perform a Mantoux test after 3 months’ treatment
D. See in regular outpatients until he is 6 months old and then perform a Mantoux test
2. The 18 month old, who had a BCG when she was 1 week old, is well when first seen. Which management plan should be followed for her? Chose ONE answer from the following options:A. Keep under regular outpatient follow-upB. Perform a Mantoux testC. Start on isoniazid 5 mg/kg and then perform a Mantoux
test after 3 months’ treatment
The Mantoux test is positive at 17 mm. The child is well with height and weight on the 75th centile and she has no fevers or night sweats. A chest X-ray shows prominent right hilum and partial collapse consolidation of the right upper lobe.
3. What course of management should be followed? Chose ONE answer from the following options:A. The child is well and should be treated for latent TB
with isoniazid and rifampicin for 3 monthsB. The X-ray changes are probably due to intercurrent
infection and should be treated with a course of oral co-amoxyclav with a follow-up X-ray
C. The chest X-ray shows evidence of clinical disease and the child should be treated with 6 months’ antituberculous treatment
4. The 4-year-old had a BCG as a baby and has a visible scar on his upper arm. He is well. Which management plan should be followed for him? Chose ONE answer from the following options:A. Perform a Mantoux testB. No further action required as he has had a BCGC. The child is well and should be treated for latent TB
with isoniazid and rifampicin for 3 months
The child is reviewed with the results of the Mantoux test, which is 16 mm. He goes on to have a gamma-interferon test which is negative.
5. What should happen now? Chose ONE answer from the following options:A. Perform a chest X-ray and treat for active TB
Paediatrics and child health 19:2 93 © 2008 Published by elsevier ltd.
self-assessment
B. Inform and advise his parents, and discharge him from the clinic
C. Treat for latent TB and X-ray again in 6 monthsD. Perform a further BCG
Case 3A 3-year-old boy is brought to A&E. He is with his grandmother who reports that he fell off his bike earlier in the day, but she did not think it was serious. He is now lethargic and complain-ing of left leg pain. On examination he is febrile at 38°C, HR of 160/min and is complaining of leg pain, but there is a full range of movement. He has two small bruises on his legs and two non-blanching petechiae on his abdomen.
1. What is the immediate management? Chose ONE answer from the following options:A. Prescribe paracetamol for the pain and discharge homeB. Place his leg in a cast, give paracetamol and await a
trauma opinion in the morningC. Assess his airway patency and breathing, consider
giving high flow oxygen, further assess for signs of shock, obtain IV access and give a bolus of 20 ml/kg fluid
D. Take a blood culture and start IV antibiotics with flucloxacillin
The rash extends and several purpura appear on his legs. The child however is much more alert and is talking normally to his grandmother. His HR remains 160–170/min and capillary refill time centrally is 4 s.
2. What is the optimal further management? Chose ONE answer from the following options:A. Urgent MRI of his leg to exclude osteomyelitisB. A diagnosis of meningococcal disease is likely so he
should be given IV penicillin, corticosteroids and a lumbar puncture
C. Place on IV antibiotics and fluids and assess 2 hourly for signs of shock
D. Give a further bolus of 20 ml/kg of colloid, IV ceftriaxone and make contact with a PICU and anaesthetics
3. Which two of the following blood tests will be most useful:A. Arterial blood gasB. Clotting screenC. Liver function testsD. CRPE. CSF culture
4. He has two brothers, aged 5 and 7, and his mother is pregnant. How should they be managed? Chose ONE answer from the following options:A. Children should receive rifampicin 10 mg/kg and the
mother rifampicin 600 mgB. Children should receive rifampicin 10 mg/kg and the
mother 500 mg ciprofloxacin as she is pregnant
C. Children should receive rifampicin 10 mg/kg and the mother ceftriaxone 250 mg in a single IM dose
Answers
Case 1
1. A and C
The most likely diagnoses are Plasmodium falciparum malaria or bacterial sepsis, which clinically can appear to be very similar, both presenting with shock. The presence of shock makes influenza less likely. That the boy has taken malaria chemoprophylaxis is no reassurance, as this cannot pre-vent all cases of malaria. Plasmodium vivax is prevalent on the Indian subcontinent and in Central America but is only rarely seen in Africa as it preferentially invades erythrocytes bearing the Duffy blood group antigen, rarely found in the African population. Worldwide Plasmodium falciparum is responsible for cases of severe and complicated malaria, which untreated has a significant mortality. Dengue fever is also associated with fever and shock but is much more com-mon in the tropical areas of Asia and America and is unusual in East Africa.
2. B
Although all four of these investigations are necessary, a blood glucose is urgent in severe malaria where hypoglycaemia can occur, causing reduced conscious level and convulsions.
3. D
This child has several features indicating he is at high risk and in need of urgent supportive management. These include a depressed conscious level and evidence of shock with tachycardia and a prolonged capillary refill time. The emergency assessment and management of the child should follow the structured approach advocated in the APLS guide-lines. Emergency management must not be delayed while the diagnosis of malaria is confirmed. The initial management of shock should include a bolus of 20 ml/kg of colloid or normal saline. There is no evidence that exchange transfu-sion has a role in the initial management of children with suspected malaria and it may distract from simpler resuscita-tion measures.
4. D
Parenteral quinine remains the antimalarial treatment of choice for patients with severe falciparum malaria and should be prescribed for 7 days. However, children often recover clinically before then and the course may be shortened by switching to a full oral course of an appropriate non-quinine medication. Oral quinine has a bitter taste and is associated with poor compliance; therefore, other oral medications are
Paediatrics and child health 19:2 94 © 2008 Published by elsevier ltd.

self-assessment
recommended. Parenteral artesunate has been shown to be superior to quinine in the treatment of severe malaria in adults in South-East Asia. These results cannot however be extrapolated to children and a multicentre study in children is currently ongoing. Chloroquine resistance is now wide-spread and is no longer the first-line treatment for falciparum malaria.
Further reAding
maitland K, nadel s, Pollard aJ, Williams tn, newton crJc, levin m.
management of severe malaria in children: proposed guidelines
for the United Kingdom. BMJ 2005; 331: 337–343.
Case 21. C2. B3. C4. A5. B
The management of close contacts of individuals with active tuberculosis have to be contacted and screened and are man-aged according to the NICE guidelines.1 The management is determined by the age of the child and whether they have received a BCG.
The 3 week old baby: Neonates who have been in close contact with people with sputum smear-positive TB who have not received at least two weeks’ anti-tuberculosis drug treatment should be treated as follows:
• The baby should be started on isoniazid 5 mg/kg and then a Mantoux test performed after three months’ treatment.
• If the Mantoux test is positive (6 mm or greater) the baby should be assessed for active TB with clinical assessment and chest X ray. If this assessment is negative, then isoniazid should be continued for a total of six months.
• If the test is negative (less than 6 mm), then isoniazid should be stopped and a BCG vaccination performed.
The 18 month old child:BCG-vaccinated children aged older than four weeks but
younger than two years, in close contact with people with sputum smear-positive respiratory TB, should have a Man-toux test. This is considered to be positive if measures 15 mm or more and the child should then be assessed for active TB. An abnormal chest X-ray in an asymptomatic child is a sign of active disease requiring six months treatment with at least three drugs for the initial two months.
The seven year old child had had prior BCG but the man-toux measured more than 15 mm so is considered to be posi-tive. The use of the interferon-gamma blood test helps to distinguish between mantous reactivity due to prior BCG or to actual infection with Mycobacterium tuberculosis.2 A nega-tive test in this child indicated the mantoux test was probably due to the prior BCG and not to either active or latent tuberculosis.
Further reAding
1 national collaborating centre for chronic conditions.
tuberculosis: clinical diagnosis and management of
tuberculosis, and measures for its prevention and control.
london: royal college of Physicians, 2006.
2 taylor re, cant aJ, clark Je. Potential effect of nice tuberculosis
guidelines on paediatric tuberculosis screening. Arch Dis Child
2008; 93: 200–203.
Case 31. C2. D3. A and B4. C
Meningococcal disease remains an important cause of mor-tality in children in the UK. Studies have shown that an increased risk of death is associated with the failure to rec-ognize complications, such as shock or raised intracranial pressure, and how ill children are; being managed by unsu-pervised junior doctors and by non-paediatric trained staff; and management that is often not sufficiently aggressive, as indicated by a failure to use enough inotropes in septicaemic patients.1
A key feature in this patient is the severe limb pain in the absence of any other physical signs in the limb, which is a well-established phenomenon in meningococcal disease and must not be attributed to a possible accident, especially in the presence of other clues such as fever. The pain can be very severe and children have been mistakenly put into plaster to treat presumed fractures.
Underlying disease may be very advanced by the time a rash appears. The rapidly evolving haemorrhagic rash may be a very late sign. The appearance of purpura in this boy (haemorrhagic lesions of >2 mm) is a further sign of advanc-ing disease. Shock is a clinical diagnosis and is clearly present in this patient. The signs are a result of circulatory failure but, as here, in early shock the child may still be alert and have a normal blood pressure.
The early signs of shock include tachycardia and a prolonged capillary refill time. If the clinical response to a bolus of 20 ml/kg of fluid is short-lived or absent, and shock does not improve or progresses, large volumes may be required (over 60 ml/kg in the first hour). In this case, there is a significant risk of pulmonary oedema, so elective tracheal intubation and mechanical ventilation should be initiated, even if there are no signs of respiratory failure, to optimize oxygenation, reduce the work of breathing and improve cardiac function. Therefore, it is important to alert senior staff early. The presence of a metabolic acidosis with a base deficit of less than −5 will give a guide to the sever-ity of illness and the need for further fluid and bicarbonate. Coagulopathy is also a marker of severity of disease and if deranged indicates the need for fresh frozen plasma. Hypoglycaemia (< 3.3 mmol/L) is common and should be corrected.2,3
Paediatrics and child health 19:2 95 © 2008 Published by elsevier ltd.
self-assessment
All cases of meningococcal disease should be reported to public health and close contacts given prophylaxis to prevent secondary cases.
Further reAding
1 ninis n, Phillips c, Bailey l, et al. the role of healthcare delivery
in the outcome of meningococcal disease in children: case
control study of fatal and non-fatal cases. BMJ 2005;
330: 1475.
2 Pollard aJ, nadel s, ninis n, faust sn, levin m. emergency
management of meningococcal disease: eight years on. Arch Dis
Child 2007; 92: 283–286.
3 ninis n, nadel s, Glennie l. clinician’s Guide to recognition
and early management of meningococcal disease in children.
an e learning tool accessible from the meningitis research
foundation’s website www.meningitis.org.
Paediatrics and child health 19:2 96 © 2008 Published by elsevier ltd.

self-assessment
Paediatrics and child health 19:3 145 © 2009 elsevier ltd. all rights reserved.
Case 1A previously well, 11-year-old boy presented to the emer-
gency department with a 4-day history of being unwell. His symptoms started with a headache and redness of the left eye. After 1 day he developed a fever of 40 °C together with an erythematous skin rash, a sore throat and generalized abdomi-nal pain.
He was seen by his GP 3 days prior to admission, was diag-nosed with tonsillitis and sinusitis, and was commenced on oral penicillin. He came to the emergency department today as his temperature was increasing, his rash had become more florid, and he had developed painful swallowing. He was drinking less, passing minimal amounts of urine and had three loose stools.
His initial observations are as follows: weight 48 kg, tem-perature 37.7 °C, heart rate 130 beats/min, blood pressure 87/33 mmHg, respiratory rate 40 breaths/min, capillary refill time less than 2 s, saturations 99% in air.
On examination he looks unwell, with bilateral red itchy eyes and red lips, and his tongue is very dry and cracked. He has bilateral tender cervical lymphadenopathy. His rash is erythematous, warm and blanching. He has bilateral enlarged tonsils with pus in the pharynx (Figure 1).
Mehrengise Cooper FRCPCH is a Consultant Paediatric Intensivist,
Paediatric Intensive Care Unit, St Mary’s Hospital, Paddington,
London W2 1NY, UK.
Shermina Sayani MBBS BSc MRCPCH is a Fellow in Medical Education,
Imperial College Healthcare NHS Trust, Praed Street, London W2
1NY, UK.
self-assessment
Initial investigations showed:
Haemoglobin 11.8 g/dl (9.6–14.8)White blood cell count 6.6 × 109/L (5.0–14.0)Neutrophil count 5.79 × 109/L (1.5–8.0)Platelet count 116 × 109/L (200–420)Sodium 125 mmol/L (135–145)Potassium 3.2 mmol/L (3.5–5.0)Urea 17.0 mmol/L (2.9–7.5)Creatinine 113 mmol/L (44–108)C-reactive protein 325 mg/L (0–5)
1. What is the most likely diagnosis? Choose ONE answer ONLY from the following:A. Kawasaki’s diseaseB. Tonsillitis and penicillin allergyC. Toxic shock syndromeD. MeaslesE. Scarlet fever
2. What is the most important initial management? Choose ONE answer ONLY from the following:A. Intravenous immunoglobulin (IVIG)B. CorticosteroidsC. ChlorpheniramineD. Intravenous benzylpenicillinE. Intravenous 0.9% saline fluid boluses
His condition remains resistant to the intervention above and he requires intubation and commencement of mechanical ven-tilation and transfer to the paediatric intensive care unit. His current observations include a heart rate of 150 beats/min and a mean blood pressure of 50 mmHg.
3. Which of the following management options should be used next? Choose ONE answer ONLY from the following:A. FurosemideB. AspirinC. Inotropic supportD. CorticosteroidsE. Intravenous immunoglobulin (IVIG)
Case 2A previously fit and well, 12-year-old girl is admitted to the paediatric ward. She has been unwell for 1 day with vomiting and abdominal pain. In the emergency department, she was seen by the SHO who referred her to the surgeons.
She is assessed on the paediatric ward and is dehydrated with dry mucous membranes and sunken eyes, and has gen-eralized abdominal tenderness. The surgical team has sug-gested ordering an abdominal ultrasound. Unfortunately, it was not possible to obtain intravenous access in the Emer-gency department, but this is undertaken successfully on the ward.
Figure 1 rash found on examination.

self-assessment
Paediatrics and child health 19:3 146 © 2009 elsevier ltd. all rights reserved.
Her initial observations are as follows: temperature 37.9°C, heart rate 120 beats/min with normal pulses, blood pressure 90/50 mmHg, respiratory rate 40 breaths/min, capillary refill time 3–4 s, saturations 95% in room air.
A venous blood gas taken when intravenous access was gained shows:
pH 7.18 (7.35–7.45)pCO2 2.5 kPa (4.7–6.0)pO2 5.3 kPa (8.0–10.0)HCO3 9 mmol/L (22.0–26.0)Base excess −18 (−2.0 to + 2.0)Sodium 134 mmol/L (135–145)Potassium 4.5 mmol/L (3.5–5.0)Glucose ***
1. Which of the following investigations will help to confirm the diagnosis? Choose ONE answer ONLY from the following:A. Ultrasound abdomenB. Full blood countC. Urine microscopy and cultureD. Stool cultureE. Urine dipstick
2. What is the most appropriate initial fluid prescription? Choose ONE answer ONLY from the following:A. IV 0.45% saline and 5% dextrose maintenance +
deficit over 24 hB. IV 0.45% saline and 5% dextrose with potassium as
maintenance over 24 hC. Trial of NG DioralyteD. 10 ml/kg normal saline bolus, followed by normal saline
with potassium as maintenance + 10% deficit over 48 hE. 10 ml/kg normal saline bolus followed by 0.45% saline
and 5% dextrose maintenance + deficit over 48 h
Note deficit = % dehydration × body weight (kg)Later that night you review the patient as she has been com-
plaining of a headache. She has been given some paracetamol and by the time you arrive she has become drowsy. Her obser-vations show the following: heart rate 70 beats/min, blood pressure 150/80 mmHg, capillary refill time less than 2 s and BM 10 mmol/L. You assess her Glasgow coma score (GCS) and it is 12/15.
3. What should you do next? Choose ONE answer ONLY from the following:A. Return to review her again in a couple of hoursB. A full neurological exam in the morning when she is
more awakeC. CT head scanD. Repeat blood gasE. Treat raised intracranial pressure with mannitol or 3%
saline
Case 3A 9-month-old boy is brought to the Emergency department by his mother. He has a 2-day history of poor feeding and coryza.
Yesterday he only took three of his normal feeds. He was born at term with no complications.
On examination his heart rate is 140 beats/min, with a respiratory rate of 70 breaths/min and saturations of 92% in room air. He has moderate intercostal recession and, on auscultation, crepitations and wheeze throughout both lung fields. His temperature is 37.5 °C. He is pink, active and inter-acting with his mother.
1. What is the most appropriate next step? Choose ONE answer ONLY from the following:A. Capillary blood gasB. Chest X-rayC. Blood cultureD. Admit and start supportive treatmentE. Salbutamol nebulizer
You are called to review him later that evening as he has dete-riorated, becoming more tachypnoeic with an increasing oxy-gen requirement. You take a capillary blood gas and organise a chest X-ray (Figure 2). A nasopharyngeal aspirate (NPA) is positive for respiratory syncytial virus (RSV).
His venous blood gas shows:
pH 7.30 (7.35–7.45)PCO2 6.8 kPa (4.7–6.0)Bicarbonate 25 mmol/L (22.0–26.0)Base excess 3 (−2.0 to + 2.0)
2. Which of the following is the appropriate next step? Choose ONE answer ONLY from the following:A. Atrovent nebulizerB. CorticosteroidsC. Adrenaline nebulizer
Figure 2 chest X-ray of patient.
self-assessment
Paediatrics and child health 19:3 147 © 2009 elsevier ltd. all rights reserved.
D. Stop feeds and commence intravenous fluidsE. Salbutamol nebulizer
His nurse tells you that over the previous 3 h he has had three episodes of desaturation to 70% for 30 s, and required stimulation and increased oxygen to return to more than 95% in nasal cannulae oxygen.
3. Which other therapeutic option will be beneficial to this patient? Choose ONE answer ONLY from the following:A. Intravenous antibioticsB. Start nasal CPAPC. DiureticsD. Review in 1 h with repeat capillary blood gasE. Arrange for intubation and ventilation
Case 4A 7-year-old boy presents to the Emergency department with a 10-day history of fever, vomiting, mainly in the mornings, a headache which is not improving with regular ibuprofen, and he is more sleepy than normal. He has had no history of loss of consciousness. He has been feeling weak, has not been walking for 1 day and has started behaving strangely.
His initial observations are: temperature 36 °C, pulse 92 beats/min, mean blood pressure 80 mmHg, respiratory rate 30/min, saturations 99% in air, capillary refill time less than 2 s. His BM is 6.2 mmol/L and his urine dipstick is NAD.
He is alert, but moaning in pain with a GCS of 15/15. He has neck stiffness with a negative Kernig’s sign. His cranial nerve examination is normal. Of note, on examining his reflexes, he has downgoing plantars. He has cervical lymphadenopathy and his tonsils are enlarged with an exudate present.
His initial venous blood gas is:
pH 7.52 (7.35–7.45)pCO2 3.7 kPa (4.7–6.0)HCO3 22.9 mmol/L (22.0–26.0)BE 1.1 (−2.0 to + 2.0)
Initial investigations showed the following:
Hb 12.2 g/dl (9.6–14.8)White blood cell count 23.7 × 109/L (5.0–14.0)Neutrophils 16 × 109/L (1.5–8.0)Platelet count 555 × 109 g/dl (200–420)Sodium 130 mmol/L (135–145)Potassium 3.4 mmol/L (3.5–5.0)Urea 2.2 mmol/L (2.9–7.5)Creatinine 61 mmol/L (44–108)C-reactive protein 6.5 mg/L (0–5.0)
1. What is your management plan at this point? Choose ONE answer ONLY from the following:A. Explain this is probably a viral infection, reassure and
discharge homeB. CT head scan and lumbar puncture
C. Discharge home with penicillin V for the tonsillitisD. Ask to return in 2 days if there is no improvementE. Admit to the ward for observation
While you are writing in your notes, before you have carried out your management plan, the nurse calls you over to review him. His vital signs are the following: temperature 37 °C, heart rate 68 beats/min, mean blood pressure 110 mmHg, respiratory rate 30–40 breaths/min with an irregular pattern, capillary refill time less than 2 s and saturations 92% in air. His GCS is 9.
2. What would you do next? Choose ONE answer ONLY from the following:A. CT head scan and lumbar punctureB. Give intravenous mannitol at a dose of 0.25–0.5 g/kgC. Intubate and commence mechanical ventilationD. Commence neurological observations every 15 min
and review after 1 hE. Fluid restriction
After an initial improvement, he has a further deterioration, is now making sterterous sounds and has developed focal seizures affecting his left leg. He is intubated and commenced on mechanical ventilation. His bloods are repeated and his serum sodium is 128 mmol/L.
3. What therapeutic manoeuvre will you institute next? Choose ONE answer ONLY from the following:A. Give intravenous mannitol at a dose of 0.25–0.5 g/kgB. Fluid restriction to 60% maintenanceC. Dose of intravenous 3% saline at a dose of 3 ml/kgD. Dose of intravenous lorazepam at 100 μg/kgE. Referral to neurosurgeon for placement of ICP bolt
Case 5A 7-day-old baby presents to the emergency department with a 24-h history of poor feeding, and episodes of cyanosis. She was born at full-term by spontaneous vaginal delivery fol-lowing an uncomplicated pregnancy with a birth weight of 3.2 kg. Her parents are non-consanguinous and she has a 2- year-old sibling who is well. She was discharged home on the second day of life, and has been breast feeding well.
On examination she is pale, and lethargic. Her weight is 3.5 kg, and she is tachypnoeic with a respiratory rate of 80 breaths/min. Her heart rate is 180 beats/min and her capil-lary refill time is 5 s. She has a liver palpable to 4 cm below the costal angle. It has been difficult to feel her femoral pulses and obtain a blood pressure in her lower limbs.
Intravenous access is gained and an initial venous blood gas shows:
pH 7.07 (7.35–7.45)pCO2 3.7 kPa (4.7–6.0)pO2 2.8 kPaHCO3 10 mmol/L (22.0–26.0)Base excess −20 (−2.0 to + 2.0)Lactate 12 mmol/L (0–2.0)

self-assessment
Paediatrics and child health 19:3 148 © 2009 elsevier ltd. all rights reserved.
1. Which of the following best describes this blood gas? Choose ONE answer ONLY from the following:A. Respiratory acidosisB. Respiratory alkalosisC. Metabolic alkalosis with respiratory compensationD. Metabolic acidosis with respiratory compensationE. Respiratory acidosis with metabolic compensation
2. What is the likely diagnosis? Choose ONE answer ONLY from the following:A. BronchiolitisB. Neonatal sepsisC. Transposition of the great arteriesD. Coarctation of the aortaE. Metabolic disorder
The baby deteriorates developing marked increased work of breathing followed by a prolonged apnoea and is fully resus-citated, with intravenous fluids and is intubated and com-menced on mechanical ventilation.
3. What therapy would be most valuable next? Choose ONE answer ONLY from the following:A. Infusion of prostaglandinB. Inhaled nitric oxideC. Intravenous antibioticsD. Inotropic supportE. Balloon atrial septostomy
Answers
Case 11. CToxic shock syndrome (TSS) is an acute, toxin-mediated febrile illness that rapidly leads to multiorgan failure, with serious morbidity and mortality. This patient meets the clini-cal criteria for diagnosis of TSS, i.e. a fever of at least 38.9 °C, a diffuse macular erythematous rash and hypotension. For diagnostic completion, toxin action on at least three sys-tems must be demonstrated with either diarrhoea or vomit-ing, myalgia or raised creatinine kinase, mucous membrane hyperaemia, elevated concentrations of blood creatinine or urea, elevated transaminases, thrombocytopenia and confu-sion or drowsiness.
TSS is classically associated with the use of tampons, but it is well described in other circumstances. TSS is caused by Staphylococcus aureus and Group A β-haemolytic streptococ-cus. The bacterial toxins are known as ‘superantigens’ due to their ability to bypass the usual steps seen in the anti-gen-mediated immune response and directly to activate the immune system.
2. EThis child is shocked, which is apparent from his tachycar-dia, tachypnoea, hypotension (note the low diastolic pres-sure) and low urine output. Typically this is described as distributive shock and occurs when blood is redistributed
among organs. He is at risk of developing decompensated shock and requires urgent fluid resuscitation. The first-line fluid should be 0.9% saline and should be given as a fluid bolus of 20 ml/kg, maintaining close observations throughout.
3. CThis child requires inotropic support; the low diastolic blood pressure indicates peripheral vasodilation and an inotrope must be commenced.
IVIG (intravenous immunoglobulin) may be used for TSS and there is some evidence to suggest immunoglobulins directed against the toxins are an effective additional therapy, and useful when conventional therapies do not control the symptoms. It is thought that IVIG probably provides the anti-bodies to neutralize the antitoxin.
The use of corticosteroids in shock is controversial and should be discussed with a paediatric intensive care unit. As a therapy for TSS, they are not effective.
Further reAding
Barry W, hudgins l, donta st, Pesanti el. intravenous
immunoglobulin therapy for toxic shock syndrome. JAMA
1992;267:3315–3316.
Buchdahl r, levin m, Wilkins B, et al. toxic shock syndrome. Arch
Dis Child 1985;60:563–567.
dellinger rP, levy mm, carlet Jm, et al. surviving sepsis campaign:
international guidelines for the management of severe sepsis
and septic shock 2008. Crit Care Med 2008;36:297–327.
Williams Gr. the toxic shock syndrome. BMJ 1990;300:960.
Case 21. EThis child is dehydrated with abdominal pain and vomiting. In addition, she is tachypnoeic, has a metabolic acidosis and her glucose has not been recorded. Urine dipstick would con-firm glycosuria and ketonuria, giving a diagnosis of diabetic ketoacidosis (DKA). A laboratory glucose will confirm this but it was not possible in the case described. DKA can some-times present with features consistent with an acute abdo-men. It is therefore important to dipstick the urine of any child who has abdominal pain or is vomiting.
2. DShe is 10% dehydrated, vomiting and acidotic, and requires IV fluids. In the management of DKA an initial fluid bolus may be given slowly if required followed by maintenance fluids. In order to correct the percentage of dehydration, the deficit of 10% is added to the fluid requirement and this should run over 48 h so as to not lead to any large fluid shifts and electrolyte changes. Maintenance fluids are always given initially as normal saline. Potassium may be required after initial resuscitation as insulin drives potas-sium uptake into cells; thus, serum electrolytes must be monitored regularly.

self-assessment
Paediatrics and child health 19:3 149 © 2009 elsevier ltd. all rights reserved.
An intravenous insulin infusion should be commenced at 0.05–0.1 U/kg/h. The infusion should be titrated to aim for a fall of glucose no more than 5 mmol/L/h. This child must have hourly observations of her vital signs, including neu-rological observations. She should have ½ hourly to hourly blood glucose measurements and 4 hourly electrolytes. Regu-lar monitoring and titration of insulin and fluids is essential in order to prevent deterioration.
3. EThis child has developed some signs of raised intracranial pressure, most likely due to cerebral oedema. This is evi-dent with her headache, reduced GCS, increasing blood pressure and dropping heart rate. This must be treated as soon as possible with a hyperosmolar agent. Her blood glu-cose has dropped to 10 mmol/L. This rapid reduction in blood glucose and any accompanying fluid shifts may be associated with the development of intracranial hyperten-sion in DKA.
Further reAding
dunger dB, sperling ma, acerini cl, et al. esPe/lWPes consensus
statement on diabetic ketoacidosis in children and adolescents.
Arch Dis Child 2004;89:188–194.
Glaser n, Barnett P, mccaslin i, et al. risk factors for cerebral
edema in children with diabetic ketoacidosis. N Engl J Med
2001;344:264–269.
Wolfsdorf J, craig me, daneman d, et al: isPad clinical Practice
consensus Guidelines 2006–2007. diabetic ketoacidosis. Pediatr
Diabetes 2007;8:28–43.
Case 31. DBronchiolitis is the most common respiratory illness affecting children under the age of 2 years, with an incidence peaking in the first year of life. Its typical features start with symp-toms of an upper airway viral infection, and over the follow-ing 4–6 days, the lower respiratory tract becomes affected with cough, tachypnoea, hyperinflation, widespread crackles and wheeze. In November 2006 the Scottish Intercollegiate Guidelines Network (SIGN) published an evidence-based guideline on the management of bronchiolitis. For the hos-pital management of bronchiolitis, it recommends that all infants with oxygen saturation ≤92% require inpatient care and that infants with oxygen saturations more than 94% in room air may be considered for discharge. Blood culture and chest X-ray are not necessary. Blood gas measurement is only required in severe cases.
2. DAs this child has become more distressed, it is most appro-priate to stop gastric feeds and commence intravenous fluids. The use of nebulized agents has no scientifically defined recommendation; however, in the clinical setting,
it may be useful to administer these agents at least on a trial basis.
3. BThe use of CPAP is appropriate where there is a respiratory deterioration and apnoeas. If there is no benefit from CPAP, then intubation and mechanical ventilation are indicated.
Further reAding
meates-dennis m. Bronchiolitis. Arch Dis Child Educ Pract Ed
2005;90:ep81–86.
Case 41. BThis child has signs and symptoms consistent with a menin-goencephalitis. Initially the child is stable and at this point it is advisable to perform a CT head to rule out a space-occupy-ing lesion, e.g. a cerebral abscess, and if appropriate to pro-ceed to perform a lumbar puncture. A normal CT brain scan does not rule out raised intracranial pressure. This is safe to do as his neurological examination is normal and there are no other contraindications.
2. BHe has developed signs of raised intracranial pressure with a decreased level of consciousness, raised blood pressure and bradycardia. At this point the lumbar puncture is not indi-cated because the risk of cerebral herniation is high.
Hyperosmolar therapy is used for treating raised intracra-nial pressure in the acute setting. The agents used for hyper-osmolar therapy are mannitol and 3% saline. Mannitol acts by reducing blood viscosity and therefore blood vessel diam-eter – where there is intact cerebral autoregulation. Mannitol also acts by its osmotic effect. Although no studies on man-nitol have been carried out in children, it is used extensively. Hypertonic saline also acts to increase the hypertonicity of cells, and is becoming incorporated into the acute manage-ment of intracranial hypertension.
3. DHe has developed focal seizures that must be controlled as soon as possible. The algorithm for the management of sei-zures must be followed. The seizures may be due to intracra-nial hypertension and treatment can be instituted for this.
Further reAding
riordan fai, cant aJ. When to do a lumbar puncture. Arch Dis Child
2002;87:235–237.
the Paediatric accident and emergency research Group. rcPch
Guideline november 2005. The Management of a Child with
a Decreased Conscious Level. london: royal college of
Paediatrics and child health, 2005.

self-assessment
Paediatrics and child health 19:3 150 © 2009 elsevier ltd. all rights reserved.
Case 51. DThis baby has developed a metabolic acidosis with respira-tory compensation.
2. D
3. ACoarctation of the aorta presenting in the neonatal period usually has an acute onset of obstruction to systemic blood flow, leading to left ventricular failure and cardiovascular col-lapse. A patent ductus arteriosus (PDA) allows blood to pass from the right ventricle to the descending aorta, and when the PDA closes, this leads to acute cardiovascular collapse. This can lead to a baby presenting with severe shock, metabolic
acidosis and end-organ ischaemia. Other left-sided obstruc-tive lesions, including hypoplastic left heart syndrome, may present in a similar way. The baby must be resuscitated on presentation, and for any duct-dependent cardiac lesion this includes an infusion of Prostaglandin in order to open up the duct to allow blood to flow into the descending aorta.
These babies must be reviewed by a paediatric cardiologist as soon as possible, in order to perform an echocardiogram to confirm and review the anatomical diagnosis.
Further reAding
chang ac, hanley fl, Wernovsky G, Wessel d (eds). Pediatric
Cardiac Intensive Care 1998.
self-assessment
Questions
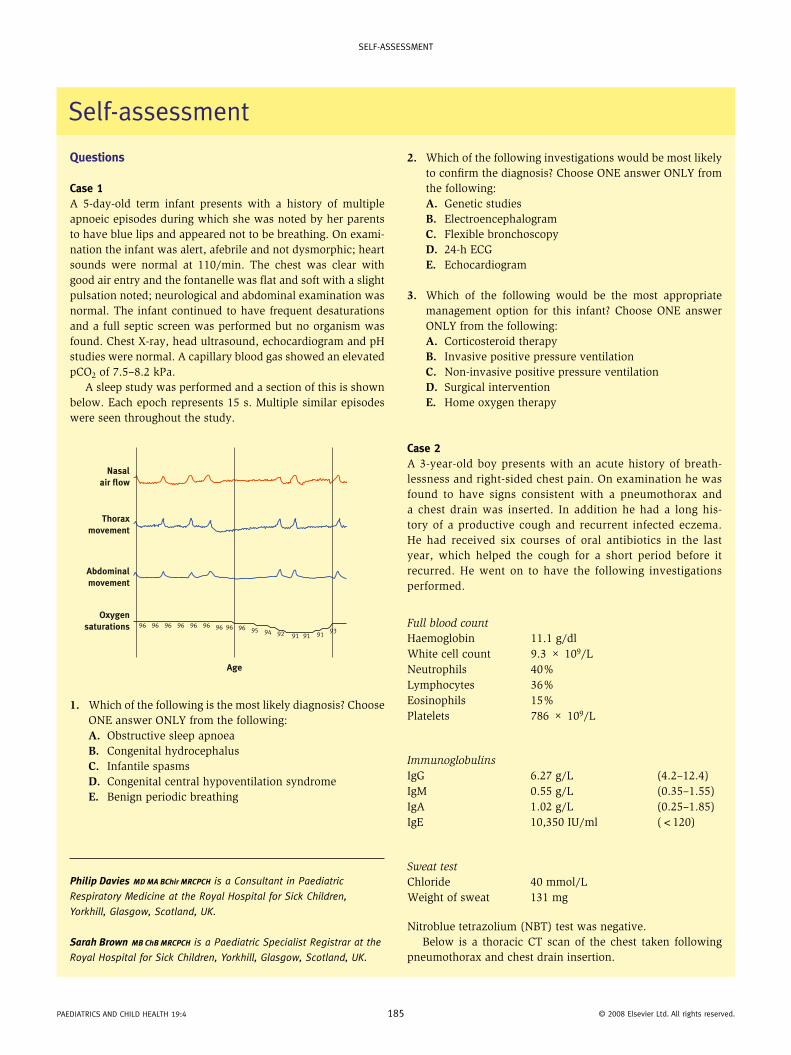
Case 1A 5-day-old term infant presents with a history of multiple apnoeic episodes during which she was noted by her parents to have blue lips and appeared not to be breathing. On exami-nation the infant was alert, afebrile and not dysmorphic; heart sounds were normal at 110/min. The chest was clear with good air entry and the fontanelle was flat and soft with a slight pulsation noted; neurological and abdominal examination was normal. The infant continued to have frequent desaturations and a full septic screen was performed but no organism was found. Chest X-ray, head ultrasound, echocardiogram and pH studies were normal. A capillary blood gas showed an elevated pCO2 of 7.5–8.2 kPa.
A sleep study was performed and a section of this is shown below. Each epoch represents 15 s. Multiple similar episodes were seen throughout the study.
Age
Nasalair flow
Thoraxmovement
Abdominalmovement
Oxygensaturations 96 96 96 96 96 96 96 96 96 95 94 92 91 91 91
93
1. Which of the following is the most likely diagnosis? Choose ONE answer ONLY from the following:A. Obstructive sleep apnoeaB. Congenital hydrocephalusC. Infantile spasmsD. Congenital central hypoventilation syndromeE. Benign periodic breathing
Philip Davies MD MA BChir MRCPCH is a Consultant in Paediatric
Respiratory Medicine at the Royal Hospital for Sick Children,
Yorkhill, Glasgow, Scotland, UK.
Sarah Brown MB ChB MRCPCH is a Paediatric Specialist Registrar at the
Royal Hospital for Sick Children, Yorkhill, Glasgow, Scotland, UK.
self-assessment
2. Which of the following investigations would be most likely to confirm the diagnosis? Choose ONE answer ONLY from the following:A. Genetic studiesB. ElectroencephalogramC. Flexible bronchoscopyD. 24-h ECGE. Echocardiogram
3. Which of the following would be the most appropriate management option for this infant? Choose ONE answer ONLY from the following:A. Corticosteroid therapyB. Invasive positive pressure ventilationC. Non-invasive positive pressure ventilationD. Surgical interventionE. Home oxygen therapy
Case 2A 3-year-old boy presents with an acute history of breath-lessness and right-sided chest pain. On examination he was found to have signs consistent with a pneumothorax and a chest drain was inserted. In addition he had a long his-tory of a productive cough and recurrent infected eczema. He had received six courses of oral antibiotics in the last year, which helped the cough for a short period before it recurred. He went on to have the following investigations performed.
Full blood countHaemoglobin 11.1 g/dlWhite cell count 9.3 × 109/LNeutrophils 40%Lymphocytes 36%Eosinophils 15%Platelets 786 × 109/L
ImmunoglobulinsIgG 6.27 g/L (4.2–12.4)IgM 0.55 g/L (0.35–1.55)IgA 1.02 g/L (0.25–1.85)IgE 10,350 IU/ml (<120)
Sweat testChloride 40 mmol/LWeight of sweat 131 mg
Nitroblue tetrazolium (NBT) test was negative.Below is a thoracic CT scan of the chest taken following
pneumothorax and chest drain insertion.
Paediatrics and child health 19:4 185 © 2008 elsevier ltd. all rights reserved.

self-assessment
1. In addition to the pneumothorax and chest drain, what anomaly is shown on the CT scan? Choose ONE answer ONLY from the following:A. PneumatocoeleB. BronchiectasisC. Pulmonary lobar emphysemaD. Congenital cystic adenomatous malformationE. Pulmonary sequestration
2. Which of the following organisms is most likely to be responsible for the lung pathology seen? Choose ONE answer ONLY from the following:A. Mycobacterium tuberculosisB. Aspergillus fumigatusC. Esherichia coliD. Pseudomonas aeruginosaE. Staphylococcus aureus
3. Which of the following options is the most likely underlying diagnosis? Choose ONE answer ONLY from the following:A. Cystic fibrosisB. Job syndromeC. Wiskott–Aldrich syndromeD. Primary ciliary dyskinesiaE. Chronic granulomatous disease
Case 3A 4-year-old boy presented to his local hospital with a 5-day history of cough, abdominal pain, pyrexia, malaise and poor oral intake. He was noted to have a respiratory rate of 35 breaths/min with intercostal recession, oxygen saturations of 91% in air and decreased air entry in the left lower region. A chest X-ray was performed which showed opacification of the left lower lobe. The patient was admitted for intravenous anti-biotics and oxygen therapy. Blood tests taken on admission gave the following results:
ElectrolytesNa+ 126 mmol/L (135–145)K+ 3.5 mmol/L (3.5–5.6)
Chloride 101 mmol/L (95–110)Bicarbonate 28 mmol/L (18–26)Urea 3.0 mmol/L (2.5–6.0)Creatinine 36 μmol/L (18–40)CRP 283 mg/L (<7)
Full blood countHaemoglobin 12.8 g/dlWhite cell count 24.3 × 109/LNeutrophils 92%Lymphocytes 6%Platelets 247 × 109/L
Over the next 4 days, the patient’s symptoms persisted and, on examination, the chest became stony dull to percussion. Repeat chest X-ray showed a ‘white out’ of the left side, with apparent scoliosis. A chest ultrasound demonstrated a locu-lated, parapneumonic effusion. The child was referred to the paediatric tertiary referral centre for further management.
1. Which of the following is the most likely cause of his hyponatraemia? Choose ONE answer ONLY from the following:A. Low sodium intakeB. Increased renal sodium excretionC. Hyponatraemic dehydrationD. Increased sodium dilutionE. High sweat sodium concentrations
2. Which of the following organisms is most likely to be responsible for his symptoms? Choose ONE answer ONLY from the following:A. Staphylococcus aureusB. Streptococcus pneumoniaeC. Klebsiella pneumoniaeD. Mycobacterium tuberculosisE. Mycoplasma pneumoniae
3. On arrival at the paediatric tertiary centre, which of the following actions is the most appropriate next step in management? Choose ONE answer ONLY from the following:A. Surgical decorticationB. Conservative management and observation for 48 hC. Small bore chest drain insertion with intrapleural
fibrinolyticsD. Large bore chest drain insertionE. Chest drain insertion (small or large bore) with
intrapleural antibiotics
Case 4A 15-year-old boy presents with a recurrent dry cough and breathlessness with activity which has become more obvi-ous over the previous 6 months. Of note in his past medical history, at age 6 he was diagnosed with stage IV neuroblas-toma and completed treatment consisting of chemotherapy,
Paediatrics and child health 19:4 186 © 2008 elsevier ltd. all rights reserved.
self-assessment
radiation and an autologous stem cell graft. Prior to this, he was well; however, he was prescribed a salbutamol inhaler to use before exercise.
On examination he was noted to have fine crepitations audible throughout both lung fields and there was good air entry bilaterally. The rest of the clinical examination was normal.
His full blood count showed the following result:
Haemoglobin 13.1 g/dlWhite cell count 5.8 × 109/LNeutrophils 45%Lymphocytes 40%Platelets 214 × 109/L
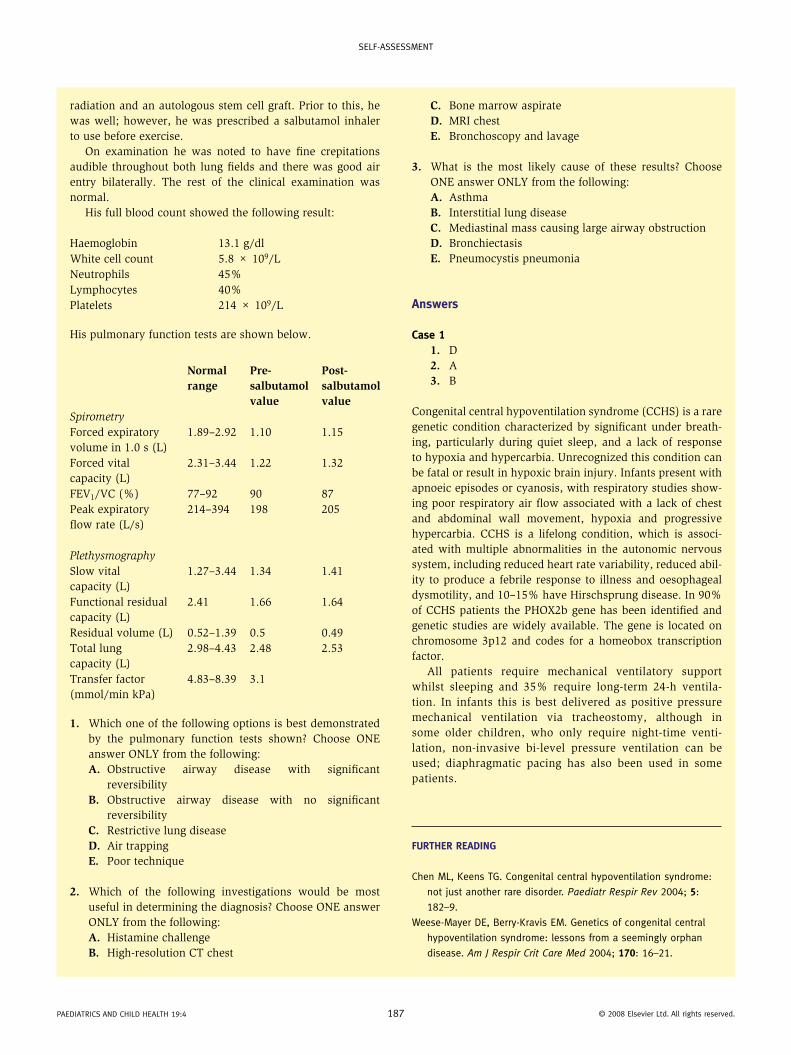
His pulmonary function tests are shown below.
Normal range
Pre- salbutamol value
Post- salbutamol value
SpirometryForced expiratory volume in 1.0 s (L)
1.89–2.92 1.10 1.15
Forced vital capacity (L)
2.31–3.44 1.22 1.32
FEV1/VC (%) 77–92 90 87Peak expiratory flow rate (L/s)
214–394 198 205
PlethysmographySlow vital capacity (L)
1.27–3.44 1.34 1.41
Functional residual capacity (L)
2.41 1.66 1.64
Residual volume (L) 0.52–1.39 0.5 0.49Total lung capacity (L)
2.98–4.43 2.48 2.53
Transfer factor (mmol/min kPa)
4.83–8.39 3.1
1. Which one of the following options is best demonstrated by the pulmonary function tests shown? Choose ONE answer ONLY from the following:A. Obstructive airway disease with significant
reversibilityB. Obstructive airway disease with no significant
reversibilityC. Restrictive lung diseaseD. Air trappingE. Poor technique
2. Which of the following investigations would be most useful in determining the diagnosis? Choose ONE answer ONLY from the following:A. Histamine challengeB. High-resolution CT chest
C. Bone marrow aspirateD. MRI chestE. Bronchoscopy and lavage
3. What is the most likely cause of these results? Choose ONE answer ONLY from the following:A. AsthmaB. Interstitial lung diseaseC. Mediastinal mass causing large airway obstructionD. BronchiectasisE. Pneumocystis pneumonia
Answers
Case 11. D2. A3. B
Congenital central hypoventilation syndrome (CCHS) is a rare genetic condition characterized by significant under breath-ing, particularly during quiet sleep, and a lack of response to hypoxia and hypercarbia. Unrecognized this condition can be fatal or result in hypoxic brain injury. Infants present with apnoeic episodes or cyanosis, with respiratory studies show-ing poor respiratory air flow associated with a lack of chest and abdominal wall movement, hypoxia and progressive hypercarbia. CCHS is a lifelong condition, which is associ-ated with multiple abnormalities in the autonomic nervous system, including reduced heart rate variability, reduced abil-ity to produce a febrile response to illness and oesophageal dysmotility, and 10–15% have Hirschsprung disease. In 90% of CCHS patients the PHOX2b gene has been identified and genetic studies are widely available. The gene is located on chromosome 3p12 and codes for a homeobox transcription factor.
All patients require mechanical ventilatory support whilst sleeping and 35% require long-term 24-h ventila-tion. In infants this is best delivered as positive pressure mechanical ventilation via tracheostomy, although in some older children, who only require night-time venti-lation, non-invasive bi-level pressure ventilation can be used; diaphragmatic pacing has also been used in some patients.
Further reAding
chen ml, Keens tG. congenital central hypoventilation syndrome:
not just another rare disorder. Paediatr Respir Rev 2004; 5:
182–9.
Weese-mayer de, Berry-Kravis em. Genetics of congenital central
hypoventilation syndrome: lessons from a seemingly orphan
disease. Am J Respir Crit Care Med 2004; 170: 16–21.
Paediatrics and child health 19:4 187 © 2008 elsevier ltd. all rights reserved.

self-assessment
Case 21. A2. E3. B
Job syndrome (also called the hyper IgE-syndrome) is a rare multisystem disorder of immunity and connective tissue. Children usually have recurrent pneumonias and infected eczema, with Staphylococcus aureus being the most common pathogen, leading to the development of pneumatocoeles in the lung and skin abscesses, which are frequently ‘cold’ in nature. In addition, there are a number of skeletal symptoms, including hyperextensible joints, scoliosis, retained primary dentition and coarse facial features in older children. Labora-tory investigations demonstrate extremely elevated IgE levels (more than 2000 IU/ml) and raised eosinophil counts.
Job syndrome has been identified in all ethnic groups and is found equally in both sexes. It may be sporadic in nature and, although most pedigrees are consistent with an auto-somal dominant inheritance, this may vary. Recent studies have identified mutations in the signal transducer and acti-vator of the transcription 3 (STAT3) gene. The underlying mechanism of Job syndrome is still not clear but theories include an imbalance in the normal T helper 1 cell (Th-1)/T helper 2 cell (Th-2) cytokine response, leading to increased IgE production.
There is no specific therapy available, although aggressive treatment of active infection and antistaphylococcal prophy-laxis is important. Immune modulators such as interferon-γ, cyclosporine A and intravenous immunoglobulin infusions have been used with limited response; bone marrow trans-plantation has not been shown to be curative.
Further reAding
Grimbacher B, holland sm, Puck Jm. hyper-ige syndromes. Immunol
Rev 2005; 203: 244–50.
holland sm, deleo fr, elloumi hZ, et al. stat3 mutations in the
hyper-ige syndrome. N Engl J Med 2007; 357: 1608–19.
Case 31. D2. B3. C
The hyponatraemia was due to syndrome of inappropriate antidiuretic hormone (SIADH). ADH is usually secreted in response to rising plasma osmolality in order to increase re-absorption of water in the distal tubules and the collecting ducts of nephrons. In certain pathological situations, including lower respiratory tract infections, too much ADH is secreted, leading to excess water retention and hyponatraemia, with fluid restriction being the most appropriate treatment.
The incidence of empyema has been steadily increasing since the mid 1990s and this appears to be unrelated to any increase in cases of pneumonia. Empyema is more common
Paediatrics and child health 19:4 188
in males and the highest incidence is seen between the ages of 1 and 4 years. Seventeen per cent of cases yield a positive organism, with Streptococcus pneumoniae serotype 1 being responsible for 50% of these cases. Blood cultures, sputum cultures and pleural fluid should be sent for analysis. Identi-fication yields may be increased by using polymerase chain reaction and latex agglutination techniques.
All children with empyema or loculated parapneumonic effusion should be managed in the respiratory unit of a tertiary referral centre. Delay in diagnosis leads to increased morbid-ity and a prolonged hospital stay, due to the difficulties in treating advanced, organized empyemas. Early intervention with chest drain insertion reduces the period of illness and hospital stay.
A small bore chest drain should be inserted under ultra-sound guidance. There is no evidence that large bore drains are preferable; small bore drains allow for more patient movement and are better tolerated. Intrapleural fibrinolytics (such as urokinase) have been shown to reduce hospital stay. In some centres a mini-thoracotomy or video-assisted tho-racotomy (VATS) are used prior to chest drain insertion. If symptoms continue, a thoracic surgeon should be consulted as decortication may be required.
In contrast to adults, the long-term outcome for chil-dren with empyema is extremely good, with the majority of children being clinically back to full health by 4 weeks and with most chest radiographs returning to near normal in 3–6 months. The majority of children who develop empyema will have been in good health prior to the acute infection and will have no long-term clinical consequences; provided the chest X-rays return to normal, further follow up investigations are unnecessary.
Further reAding
Balfour-lynn im, abrahamson e, cohen G, et al. Bts guidelines for
the management of pleural infection in children. Thorax 2005;
60 (suppl 1): i1–21.
eastham Km, freeman r, Kearns am, et al. clinical features,
aetiology and outcome of empyema in children in the north
east of england. Thorax 2004; 59: 522–5.
roxburgh cs, Youngson GG, townend Ja, turner sW. trends in
pneumonia and empyema in scottish children in the past 25
years. Arch Dis Child 2008; 93: 316–8.
Case 41. C2. B3. B
Spirometry shows a proportional reduction in both forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC), with the FEV1/FVC ratio being within normal limits, excluding obstructive airways disease. Plesthsymography demonstrates a reduced total lung capacity and residual volume, which indicates a restrictive lung disease. Transfer
© 2008 elsevier ltd. all rights reserved.
self-assessment
factor is a measure of how readily carbon monoxide crosses the interstitium and is reduced if infiltrates or fibrosis are present within the lung parenchyma, as found in interstitial lung disease.
High-resolution CT is the most sensitive imaging modal-ity to confirm the diagnosis of interstitial lung disease and demonstrates the extent of parenchymal lung disease; it may also determine suitable biopsy sites should a tissue diagnosis be required.
Restrictive lung disease may be secondary to the following causes:• intrinsic lung disease (e.g. primary interstitial lung
diseases, infectious and post-infectious disorders)• extrinsic disorders (e.g. scoliosis, neuromuscular disorders
such as Duchenne muscular dystrophy, morbid obesity)• secondary to systemic disease (e.g. sarcoidosis,
histiocytosis)• drug induced (e.g. chemotherapy agents, radiation).
Paediatric interstitial lung disease is rare. The types, causes and prognosis are ill-defined, and do not follow the patterns seen in adults. In approximately half of cases, the aetiol-ogy is unknown. In this case, the restrictive defect is most probably a consequence of treatment of the stage IV neu-roblastoma. Many of the treatments used to treat childhood cancer can result in pulmonary fibrosis in subsequent years,
Paediatrics and child health 19:4 189
including alkylating agents such as bulsulphan, bleomycin and cyclophosphamide. Radiotherapy can also cause pulmo-nary fibrosis, particularly if used in combination with alkyl-ating agents. The prognosis of pulmonary fibrosis in cancer survivors is variable and symptoms may improve, remain unchanged or worsen with time. Any child at risk of develop-ing restrictive lung disease should have baseline pulmonary function tests performed at the end of therapy and repeated if clinically indicated.
The treatment of interstitial lung disease in children is dependent upon the aetiology. Steroids remain the primary therapeutic option, with other immunosuppressive agents such as azathioprine, cyclophosphamide or hydroxycholoro-quine being of benefit in some patients.
Further reAding
fan ll, deterding rr, langston c. Pediatric interstitial lung disease
revisited. Pediatr Pulmonol 2004; 38: 369–78.
mertens ac, Yasui Y, liu Y, et al. Pulmonary complications in
survivors of childhood and adolescent cancer, a report from the
childhood cancer survivor study. Cancer 2002; 95: 2431–41.
scottish collegiate Guidelines network. long term follow up of
survivors of childhood cancer. a national clinical guideline,
2004. http://www.sign.ac.uk/pdf/sign76.pdf.
© 2008 elsevier ltd. all rights reserved.
self-assessment
Questions
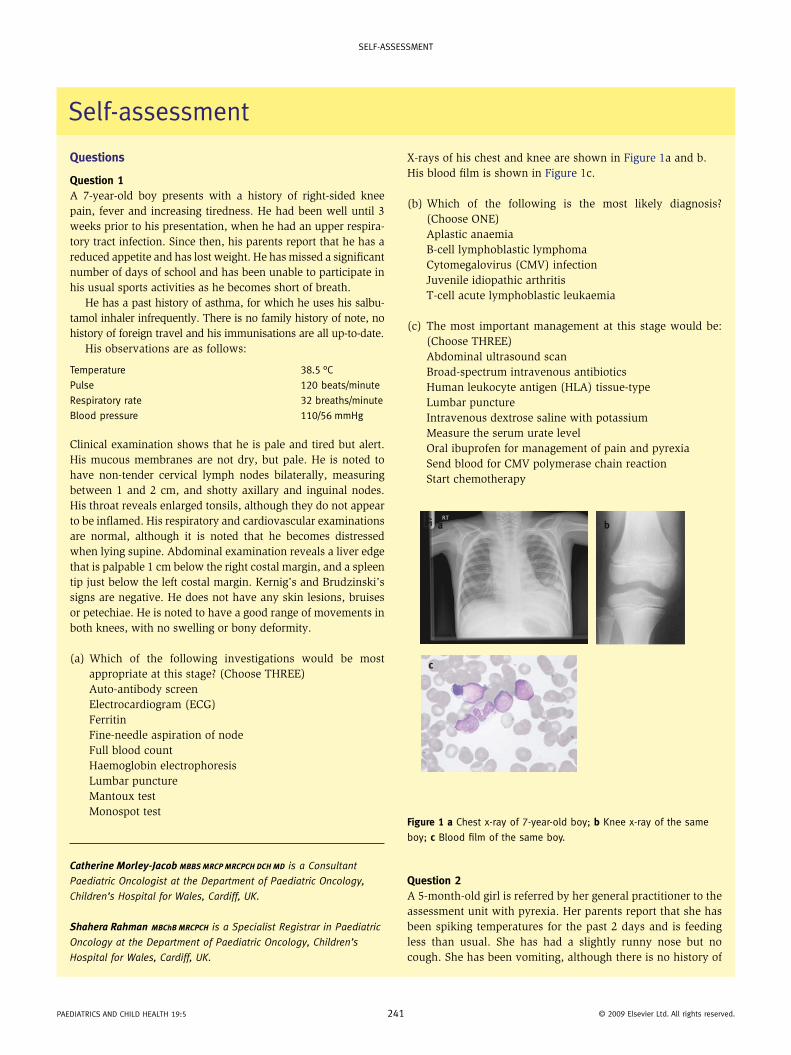
Question 1A 7-year-old boy presents with a history of right-sided knee pain, fever and increasing tiredness. He had been well until 3 weeks prior to his presentation, when he had an upper respira-tory tract infection. Since then, his parents report that he has a reduced appetite and has lost weight. He has missed a significant number of days of school and has been unable to participate in his usual sports activities as he becomes short of breath.
He has a past history of asthma, for which he uses his salbu-tamol inhaler infrequently. There is no family history of note, no history of foreign travel and his immunisations are all up-to-date.
His observations are as follows:
temperature 38.5 °cPulse 120 beats/minute
respiratory rate 32 breaths/minute
Blood pressure 110/56 mmhg
Clinical examination shows that he is pale and tired but alert. His mucous membranes are not dry, but pale. He is noted to have non-tender cervical lymph nodes bilaterally, measuring between 1 and 2 cm, and shotty axillary and inguinal nodes. His throat reveals enlarged tonsils, although they do not appear to be inflamed. His respiratory and cardiovascular examinations are normal, although it is noted that he becomes distressed when lying supine. Abdominal examination reveals a liver edge that is palpable 1 cm below the right costal margin, and a spleen tip just below the left costal margin. Kernig’s and Brudzinski’s signs are negative. He does not have any skin lesions, bruises or petechiae. He is noted to have a good range of movements in both knees, with no swelling or bony deformity.
(a) Which of the following investigations would be most appropriate at this stage? (Choose THREE)Auto-antibody screenElectrocardiogram (ECG)FerritinFine-needle aspiration of nodeFull blood countHaemoglobin electrophoresisLumbar punctureMantoux testMonospot test
Catherine Morley-Jacob MBBS MRCP MRCPCH DCH MD is a Consultant
Paediatric Oncologist at the Department of Paediatric Oncology,
Children’s Hospital for Wales, Cardiff, UK.
Shahera Rahman MBChB MRCPCH is a Specialist Registrar in Paediatric
Oncology at the Department of Paediatric Oncology, Children’s
Hospital for Wales, Cardiff, UK.
self-assessment
Paediatrics and child health 19:5 241
X-rays of his chest and knee are shown in Figure 1a and b.His blood film is shown in Figure 1c.
(b) Which of the following is the most likely diagnosis? (Choose ONE)Aplastic anaemiaB-cell lymphoblastic lymphomaCytomegalovirus (CMV) infectionJuvenile idiopathic arthritisT-cell acute lymphoblastic leukaemia
(c) The most important management at this stage would be: (Choose THREE)Abdominal ultrasound scanBroad-spectrum intravenous antibioticsHuman leukocyte antigen (HLA) tissue-typeLumbar punctureIntravenous dextrose saline with potassiumMeasure the serum urate levelOral ibuprofen for management of pain and pyrexiaSend blood for CMV polymerase chain reactionStart chemotherapy
Question 2A 5-month-old girl is referred by her general practitioner to the assessment unit with pyrexia. Her parents report that she has been spiking temperatures for the past 2 days and is feeding less than usual. She has had a slightly runny nose but no cough. She has been vomiting, although there is no history of
a b
c
Figure 1 a chest x-ray of 7-year-old boy; b Knee x-ray of the same
boy; c Blood film of the same boy.
© 2009 elsevier ltd. all rights reserved.
self-assessment
diarrhoea. There is no history of offensive-smelling urine. She has been previously been fit and well, with no past medical history of note.
On examination, she has a temperature of 38.5 °C. She is sleeping but easily rousable, although grizzly. She has a nor-mal cry and normal movements. She has a full, wet nappy. Systemic examination does not reveal any abnormalities and her observations show:
heart rate 105 beats/minute
respiratory rate 40 breaths/minute
capillary refill time <2 seconds
(a) What further tests would be most appropriate at this time: (choose TWO)Capillary blood gasChest x-rayFull blood countLumbar punctureNasopharyngeal aspirateUrine for microscopy
(b) The urine dipstick is negative for leukocyte esterase and positive for nitrites, and the urine is sent for microscopy and culture. The appropriate management at this stage would be: (Choose ONE)Await results of urine culture and if positive, start antibioticsCommence intravenous (i.v.) ceftriaxoneCommence 7–10 days of oral trimethoprimCommence 3–5 days of oral augmentinRepeat urine and then start antibiotics
(c) The urine culture shows Escherichia coli at more than 100,000 organisms/ml, with typical sensitivities. She has responded well to treatment and is apyrexial within 48 hours of commencing antibiotics. The ongoing management of this patient should include: (Choose ANY number)Dimercapto-succinic acid (DMSA) scanFollow-up in general paediatric clinicMicturating cystourethrogram (MCUG)Prophylactic trimethoprim6-week ultrasound scanUltrasound scan during acute episode
Question 3A term baby is seen in the out-patient clinic as follow-up for hypoglycaemia in the neonatal period. She is the second child of Afro-Caribbean parents. The pregnancy was unremarkable and she was born by normal vaginal delivery with Apgars of 7, 9 and 9. She weighed 2.95 kg and had no obvious dysmor-phic features at birth. She was admitted to the neonatal unit at 12 hours of age and was discharged back to her mother at 3 days of age. She is now 8 weeks old and is well and smiling but her parents are worried that she keeps sticking her tongue out. She is feeding well, is 10% below her birth centile for weight, and is alert and active. On examination she appears well, and the only abnormal findings are a liver edge,
Paediatrics and child health 19:5 24
just palpable, and macroglossia. Clinically she has features of Beckwith–Wiedemann syndrome.
(a) What other clinical features would you look for in this baby, now and throughout her childhood? (Choose TWO)AniridiaCafe-au-lait patchesCardiomyopathyCleft palateHemihypertrophyUmbilical hernia
(b) The appropriate management at this stage would be: (Choose ONE)Check her blood glucose levelRefer to clinical geneticsRequest an urgent abdominal ultrasound scanReview her 3-monthly to examine her abdomenSend urine for catecholamines
(c) Which of the following tumours is she most at risk from? (Choose TWO)Ewing’s sarcomaHepatoblastomaNeuroblastomaRhabdomyosarcomaTeratomaWilms’ tumour
Question 4A 9-month-old presents with a small, painless, purple lump just below his left clavicle. He is well and thriving. His mother describes him as a happy, lazy baby who is always smiling, who interacts socially and appropriately but who refuses to sit unaided. In the clinic he is sitting propped up on his mother’s lap playing happily with her keys. You suspect the diagnosis may be neuroblastoma. He makes no effort to bear weight when held upright.
(a) Which of these topics is important to discuss with his mother? (Choose ONE)DiarrhoeaPetechiaeRecurrent infectionsSkin flushingUrinary stream
Respiratory and cardiovascular examinations are unre-markable. His abdomen is soft, with no palpable masses or organomegaly. Examination of his legs shows bilateral flaccid paralysis with no sensation.
His chest x-ray is shown in Figure 2.
(b) The appropriate next management step is: (choose ONE)Refer urgently for removal of subcutaneous lumpRefer urgently for removal of the mass seen on x-rayRequest an urgent magnetic resonance imaging (MRI) scan
2 © 2009 elsevier ltd. all rights reserved.
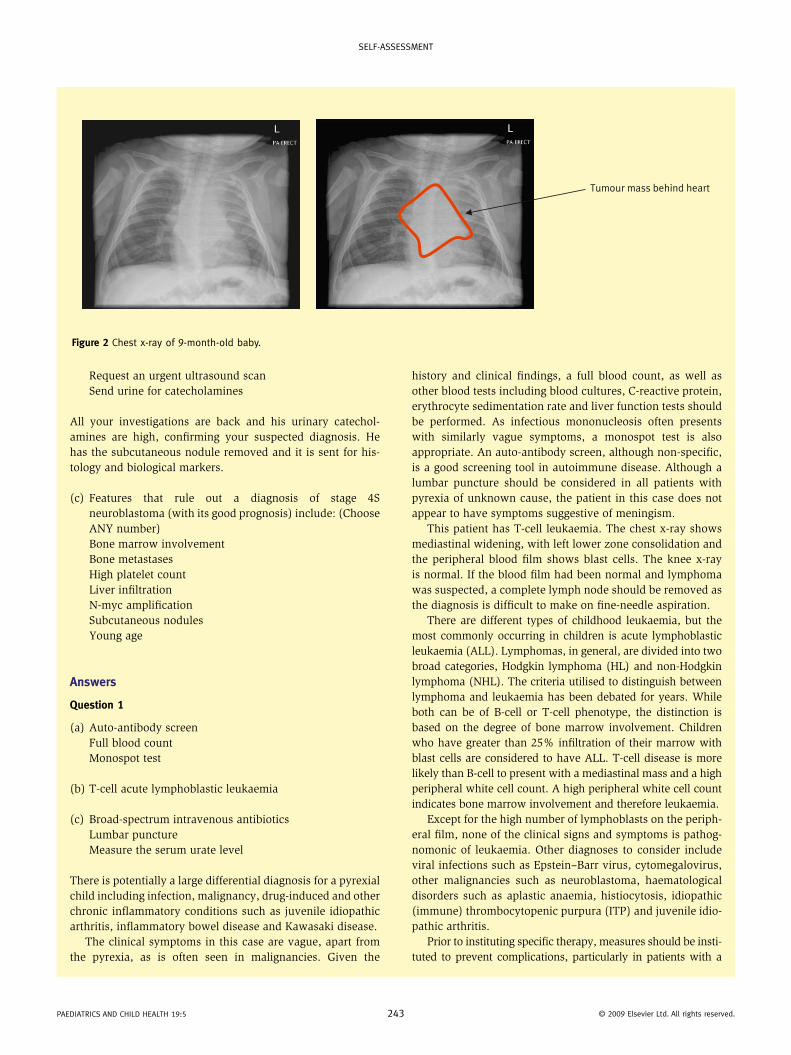
self-assessment
Tumour mass behind heart
Figure 2 chest x-ray of 9-month-old baby.
Request an urgent ultrasound scanSend urine for catecholamines
All your investigations are back and his urinary catechol-amines are high, confirming your suspected diagnosis. He has the subcutaneous nodule removed and it is sent for his-tology and biological markers.
(c) Features that rule out a diagnosis of stage 4S neuroblastoma (with its good prognosis) include: (Choose ANY number)Bone marrow involvementBone metastasesHigh platelet countLiver infiltrationN-myc amplificationSubcutaneous nodulesYoung age
Answers
Question 1
(a) Auto-antibody screenFull blood countMonospot test
(b) T-cell acute lymphoblastic leukaemia
(c) Broad-spectrum intravenous antibioticsLumbar punctureMeasure the serum urate level
There is potentially a large differential diagnosis for a pyrexial child including infection, malignancy, drug-induced and other chronic inflammatory conditions such as juvenile idiopathic arthritis, inflammatory bowel disease and Kawasaki disease.
The clinical symptoms in this case are vague, apart from the pyrexia, as is often seen in malignancies. Given the
Paediatrics and child health 19:5 243
history and clinical findings, a full blood count, as well as other blood tests including blood cultures, C-reactive protein, erythrocyte sedimentation rate and liver function tests should be performed. As infectious mononucleosis often presents with similarly vague symptoms, a monospot test is also appropriate. An auto-antibody screen, although non-specific, is a good screening tool in autoimmune disease. Although a lumbar puncture should be considered in all patients with pyrexia of unknown cause, the patient in this case does not appear to have symptoms suggestive of meningism.
This patient has T-cell leukaemia. The chest x-ray shows mediastinal widening, with left lower zone consolidation and the peripheral blood film shows blast cells. The knee x-ray is normal. If the blood film had been normal and lymphoma was suspected, a complete lymph node should be removed as the diagnosis is difficult to make on fine-needle aspiration.
There are different types of childhood leukaemia, but the most commonly occurring in children is acute lymphoblastic leukaemia (ALL). Lymphomas, in general, are divided into two broad categories, Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL). The criteria utilised to distinguish between lymphoma and leukaemia has been debated for years. While both can be of B-cell or T-cell phenotype, the distinction is based on the degree of bone marrow involvement. Children who have greater than 25% infiltration of their marrow with blast cells are considered to have ALL. T-cell disease is more likely than B-cell to present with a mediastinal mass and a high peripheral white cell count. A high peripheral white cell count indicates bone marrow involvement and therefore leukaemia.
Except for the high number of lymphoblasts on the periph-eral film, none of the clinical signs and symptoms is pathog-nomonic of leukaemia. Other diagnoses to consider include viral infections such as Epstein–Barr virus, cytomegalovirus, other malignancies such as neuroblastoma, haematological disorders such as aplastic anaemia, histiocytosis, idiopathic (immune) thrombocytopenic purpura (ITP) and juvenile idio-pathic arthritis.
Prior to instituting specific therapy, measures should be insti-tuted to prevent complications, particularly in patients with a
© 2009 elsevier ltd. all rights reserved.

self-assessment
Pa
high white cell count or bulk disease. Serum urate, renal function, serum calcium, phosphate and magnesium should be measured regularly in these patients to monitor for tumour lysis. Tumour lysis can occur spontaneously or as a result of chemotherapy lead-ing to serious metabolic complications such as hyperuricaemia, hyperkalaemia and hyperphosphataemia. This combination can ultimately lead to renal failure or cardiac arrest if left untreated. Prevention is with hyperhydration, anti-urate drugs (allopurinol or rasburicase) and maintenance of urine output. Fluid should not contain potassium, as this may exacerbate hyperkalaemia. Pyrexia in patients may be secondary to the disease process itself or due to sepsis. Given that the immune system is compromised in such patients, despite the high white cell count, they should routinely be given broad spectrum intravenous antibiotics, even with low grade pyrexia. Ibuprofen is not recommended in these patients as poor platelet function in patients with thrombocyto-penia may lead to bleeding. Airway compromise and pleural effu-sions can be an acute problem with large mediastinal masses.
The diagnosis of ALL must be established beyond any doubt and, therefore, a complete work-up is generally consid-ered as important as rapidly initiated therapy in a stable child.
ediatrics and child health 19:5 2
Bone marrow aspiration should be performed for morphology, immunophenotyping and cytogenetics and a lumbar puncture to exclude central nervous system disease. A liver ultrasound is unlikely to aid diagnosis or management, as the hepatospleno-megaly is a reflection of disease burden. A child with leukae-mia would not routinely need a bone marrow transplant and, therefore, routine HLA typing is not necessary at diagnosis.
Question 2
(a) Full blood countUrine for microscopy
(b) Commence 7–10 days of oral trimethoprim(c) 6-week ultrasound scan
According to the National Institute for Clinical Excellence (NICE) guidelines (May 2007), children with a feverish illness should be assessed for the presence or absence of symptoms and signs that can be used to predict the risk of serious ill-ness. For this purpose, a traffic light system was devised, as illustrated in Table 1.
Green-low risk amber – intermediate risk red – high risk
colour • normal colour of skin, lips and
tongue
• Pallor reported by parent/carer • Pale/mottled/ashen/blue
activity • responds normally to social
cues
• content/smiles
• stays awake or awakens
quickly
• strong normal cry/not crying
• not responding normally to social
cues
• Wakes only with prolonged
stimulation
• decreased activity
• no smile
• no response to social cues
• appears ill to a healthcare
professional
• does not wake or if roused does not
stay awake
• Weak, high-pitched or continuous cry
respiratory • nasal flaring
• tachypnoea:
rr > 50 breaths/mintues,
age 6–12 months
rr > 40 breaths/minutes,
age > 12 months
• Oxygen saturation ≤ 95% in air
• crackles
• Grunting
• tachypnoea: rr > 60 breaths/minutes
• moderate or severe chest indrawing
hydration • normal skin and eyes
• moist mucous membranes
• dry mucous membranes
• Poor feeding in infants
capillary refill time ≥ 3 seconds
• reduced urine output
• reduced skin turgor
Other • none of the amber or red
symptoms or signs
• fever for ≥ 5 days • age 0–3 months, temperature ≥ 38 °c• age 3–6 months, temperature ≥ 39 °c
• swelling of a limb or joint
• non-weight bearing/not using an
extremity
• non-blanching rash
• Bulging fontanelle
• neck stiffness
• status epilepticus
• focal neurological signs
• focal seizures
• a new lump > 2 cm • Bile-stained vomiting
Table 1 table modified from nice Guidance: feverish illness in children (assessment and initial management in children younger than 5 years –
may 2007)
44 © 2009 elsevier ltd. all rights reserved.

self-assessment
This patient would fall into the intermediate group, with her history of poor feeding and vomiting. NICE guidelines (May 2007) suggest that that urine should be collected and blood tests (full blood count, C-reactive protein and blood cultures) performed. A chest x-ray should also be considered particularly with a temperature more than 39 °C and/or a white cell count more than 20 × 109/l. A lumbar puncture should also be considered, especially in children under the age of 1 year.
According to the NICE guidelines for treating urinary tract infection (UTI) in children (August 2007), with a negative leu-kocyte esterase and a positive nitrite on dipstick, the child should be started on antibiotics. Treatment should not be delayed to collect another urine specimen. If the converse is true, with a positive leukocyte esterase and a negative nitrite, treatment for UTI should only be started if there is good clini-cal evidence of UTI, as the result may also indicate infection elsewhere.
In children with bacteriuria but no systemic symptoms, 3 days of oral antibiotics are sufficient. With systemic symptoms or in children with acute pyelonephritis or upper UTI, a 7–10 day course of oral antibiotics should be used. If oral antibiot-ics are not tolerated, i.v. antibiotics should be considered. In children who are septic or in infants under 3 months of age, i.v. antibiotics should be used.
Antibiotic prophylaxis should not routinely be used in chil-dren following their first UTI or with asymptomatic bacteri-uria, but should be considered with recurrent UTIs.
Infants and children with atypical UTIs (seriously ill child, bladder mass, raised creatinine, septicaemia, failure to respond to suitable antibiotics within 48 hours) should have an ultrasound of the urinary tract during the acute infection to identify structural abnormalities of the urinary tract, such as obstruction. In children with their first UTI that responds to treatment, an ultrasound should only be performed at 6 weeks in infants younger than 6 months, or if the UTI is atypical.
DMSA and MCUG scans are required with atypical or recur-rent UTIs or with an abnormal ultrasound scan in infants less than 6 months of age. In older children, DMSA scans (only) should be arranged in similar situations.
Infants and children who do not undergo imaging investi-gations should not routinely be followed-up.
Paediatrics and child health 19:5 24
Question 3
(a) HemihypertrophyUmbilical hernia
(b) Refer to clinical genetics(c) Hepatoblastoma
Wilms’ tumour
Beckwith–Wiedemann syndrome (BWS) is an imprinting dis-order (abnormality at 11p15). Imprinting is a process by which certain genes are switched off during early embryonic develop-ment, according to whether they are inherited from the father or the mother. A number of distinct errors involving 11p15 have been identified in BWS patients. Some patients have a rearrangement within the maternal copy of 11p15, while oth-ers have paternal uniparental disomy, where the maternal copy of this region is replaced with an extra paternal copy. Affected individuals may have abnormal DNA methylation in different areas of 11p15 or have a mutation of a single gene located within 11p15. Even after extensive molecular testing, the specific defect causing BWS remains unknown in one-third of affected individuals.
One of the genes at 11p15, IGF-2, codes for a growth fac-tor protein, explaining the features of overgrowth, including macroglossia and organomegaly. Additional features in BWS include neonatal hypoglycaemia, hemihypertrophy, abdominal wall defects and urogenital abnormalities. Aniridia (absence of the iris) is associated with Wilms’ tumour but not BWS.
Children with clinical features of BWS should be referred to a clinical geneticist for discussion of the genetic implications, to access the diagnostic molecular tests and to start surveil-lance screening.
It is well-known that BWS predisposes an individual to Wilms’ tumour but there is an increased risk of other embryonal tumours, particularly hepatoblastoma. Abdominal ultrasound scans should pick up both, but alpha-fetoprotein can also be used as a screening tool. The overall risk of devel-oping a tumour in BWS is estimated at 5–10%. The Wilms’ tumour does not necessarily occur on the side of overgrowth in hemihypertrophy.
FurTher reAding
national institute for clinical excellence. feverish illness in
children: assessment and initial management in children
younger than 5 years. clinical guideline. london: nice. may
2007.
national institute for clinical excellence. Urinary tract infection:
diagnosis, treatment and long-term management of urinary
tract infection in children. clinical guideline. london: nice.
august 2007.
FurTher reAding
the Wilms tumour surveillance Working Group. surveillance for
Wilms tumour in at-risk individuals: pragmatic recommendations
for best practice. april 2005. available at: http://www.icr.ac.uk/
research/research_sections/cancer_genetics/cancer_genetics_
teams/genetic_susceptibility/Wilms_tumour_surv_group/2145.
shtml. date accessed: 5/2/09.
choyke Pl, siegel mJ, craft aW, Green dm, deBaun mr. screening
for Wilms tumor in children with Beckwith-Wiedemann syndrome
or idiopathic hemihypertrophy. med Pediatr Oncol 1999; 32:
196–200.
5 © 2009 elsevier ltd. all rights reserved.
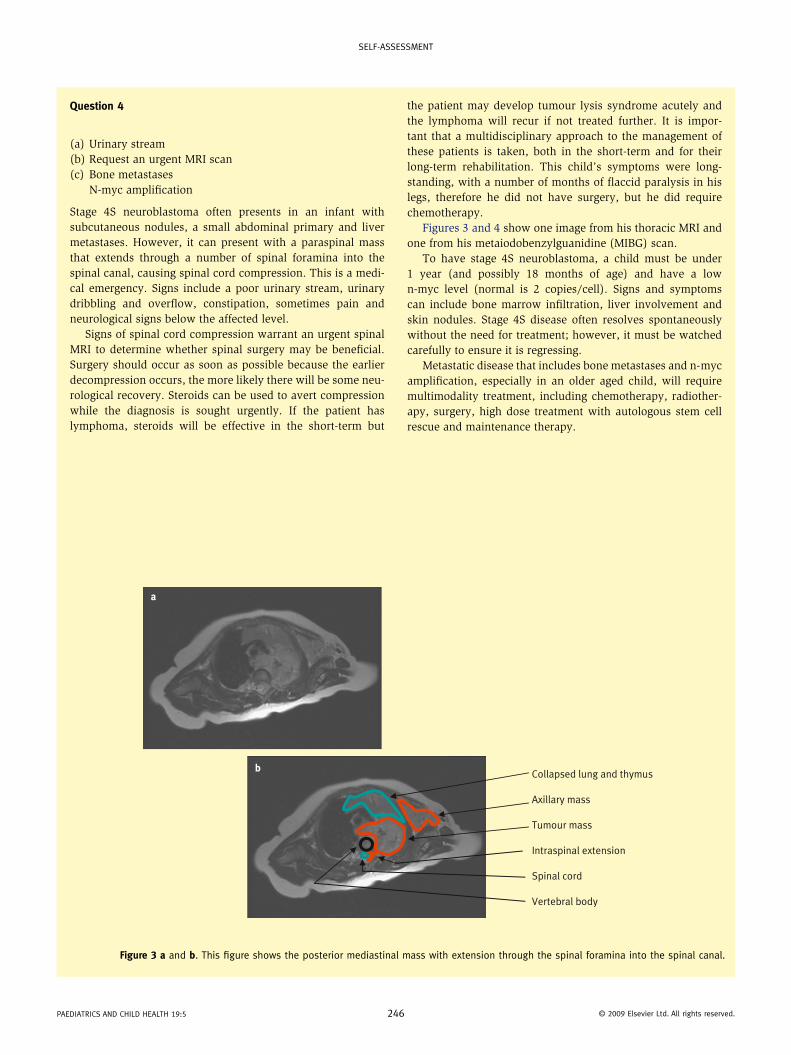
self-assessment
Question 4
(a) Urinary stream(b) Request an urgent MRI scan(c) Bone metastases
N-myc amplification
Stage 4S neuroblastoma often presents in an infant with subcutaneous nodules, a small abdominal primary and liver metastases. However, it can present with a paraspinal mass that extends through a number of spinal foramina into the spinal canal, causing spinal cord compression. This is a medi-cal emergency. Signs include a poor urinary stream, urinary dribbling and overflow, constipation, sometimes pain and neurological signs below the affected level.
Signs of spinal cord compression warrant an urgent spinal MRI to determine whether spinal surgery may be beneficial. Surgery should occur as soon as possible because the earlier decompression occurs, the more likely there will be some neu-rological recovery. Steroids can be used to avert compression while the diagnosis is sought urgently. If the patient has lymphoma, steroids will be effective in the short-term but
Paediatrics and child health 19:5 2
the patient may develop tumour lysis syndrome acutely and the lymphoma will recur if not treated further. It is impor-tant that a multidisciplinary approach to the management of these patients is taken, both in the short-term and for their long-term rehabilitation. This child’s symptoms were long- standing, with a number of months of flaccid paralysis in his legs, therefore he did not have surgery, but he did require chemotherapy.
Figures 3 and 4 show one image from his thoracic MRI and one from his metaiodobenzylguanidine (MIBG) scan.
To have stage 4S neuroblastoma, a child must be under 1 year (and possibly 18 months of age) and have a low n-myc level (normal is 2 copies/cell). Signs and symptoms can include bone marrow infiltration, liver involvement and skin nodules. Stage 4S disease often resolves spontaneously without the need for treatment; however, it must be watched carefully to ensure it is regressing.
Metastatic disease that includes bone metastases and n- myc amplification, especially in an older aged child, will require multimodality treatment, including chemotherapy, radiother-apy, surgery, high dose treatment with autologous stem cell rescue and maintenance therapy.
Collapsed lung and thymus
Axillary mass
Tumour mass
Intraspinal extension
Spinal cord
Vertebral body
a
b
Figure 3 a and b. this figure shows the posterior mediastinal mass with extension through the spinal foramina into the spinal canal.
46 © 2009 elsevier ltd. all rights reserved.
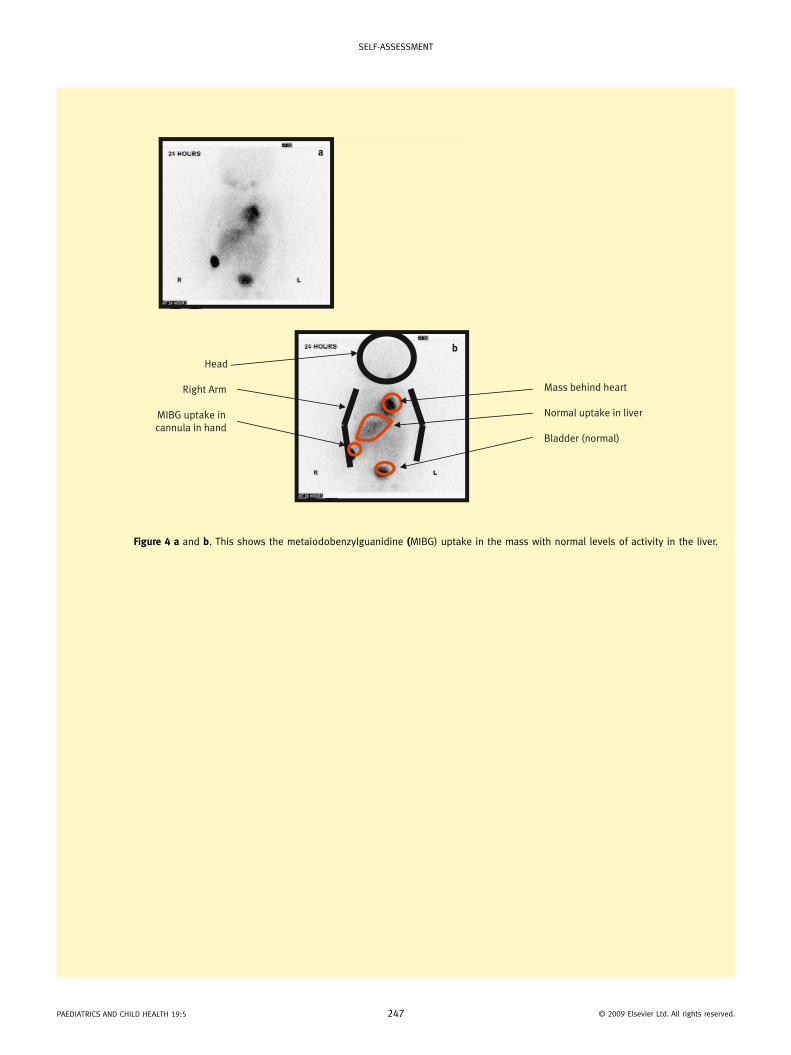
self-assessment
Paediatrics
Head
Right Arm
MIBG uptake incannula in hand
Mass behind heart
Normal uptake in liver
Bladder (normal)
a
b
Figure 4 a and b. this shows the metaiodobenzylguanidine (miBG) uptake in the mass with normal levels of activity in the liver.
and child health 19:5 247 © 2009 elsevier ltd. all rights reserved.

self-assessment
Questions
Case 1A 3-year-old girl presented to the Emergency Department with a 6-week history of a reluctance to walk, and a limp more pronounced in the morning. Prior to onset of these symptoms she had had 2 days of fever with some associated rhinorhoea and cough.
A bone scan done at another hospital a week earlier had been reported as normal. There was no recent history of night sweats, weight loss or gastrointestinal symptoms. Treatment had included non-steroidal anti-inflammatory drugs (NSAIDs), with minimal improvement. Antibiotics had not been given at any stage.
On examination she was afebrile, had an antalgic gait, and on hip examination had limited internal rotation. There was also mild swelling and a decreased range of movement of the left knee. There was no bony tenderness and no obvious swelling or limitation of movement of other joints. There was no lymphadenopathy, and the eye, cardiovascular, respiratory and abdominal examination were normal.
Investigations
• Full blood count
Value Reference range
haemoglobin 113 g/l 110–140 g/l
haematocrit 0.32 (l) 0.34–0.42 l
rcc 4.31 × 1012/l 3.9–5.3 × 1012/l
mch 26.2 pg 24–30 pg
mcV 74 l* fl 75–90 flrdW 12.7% 11–14%
Platelets 602 × 109/l (h) 150–400 × 109/l
Wcc 13.2 × 109/l 6.0–17.0 × 109/l
neut seg 6.69 × 109/l 1.5–8.5 × 109/l
lymphocytes 5.77 × 109/l 3.0–9.5 × 109/l
monocytes 0.63 × 109/l 0.1–1.0 × 109/l
eosinophils 0.05 × 109/l 0–0.8 × 10e9/l
Basophils 0.05 × 109/l 0–0.1 × 109/l
rcc, red cell count; mch, mean corpuscular haemoglobin; mcV, mean corpus-cular volume; rdW, red cell distribution width; Wcc, white cell count; l, low; h, high.
• Erythrocyte sedimentation rate (ESR) 140 mm/h (range 0–6 mm/h)
• C-reactive protein (CRP) 63 mg/l (<8 mg/l)
• Hip x-ray: normal
• Hip ultrasound: thickened synovium bilaterally, nil joint effusion
Nigel Crawford BMBS MPH FRACP (Paediatrics) is a paediatrician for the
NHMRC CCRE in Childhood & Adolescent Immunization, SAEFVIC-
Immunization Safety Surveillance Unit, Department of General
Medicine, MCRI/Royal Children’s Hospital, Melbourne, Australia.
self-assessment
(a) What is the most likely diagnosis?Irritable hip (reactive arthropathy)Juvenile idiopathic arthritisLeukaemiaMultifocal osteomyelitisTrauma
(b) What investigation would you recommend?Repeat bone scanJoint aspiration/biopsyMagnetic resonance imaging (MRI) of hips/knee joints with contrastBone-marrow aspirate
(c) What treatment would you recommend?Corticosteroid joint injectionsIntravenous methylprednisoloneIntravenous antibioticsSurgery
Case 2A 9-week-old boy was well on the day of his routine 2-month scheduled vaccinations (diphtheria/tetanus/pertussis (acellu-lar)/haemophilus influenzae type b/polio/pneumococcus). He was a little unsettled immediately post-immunization and was put down for a sleep on returning home, now 2 hours post-vaccination. When his mother went back into the bedroom 5 minutes later he was staring upwards and ‘she thought he was dead’, as he appeared very pale, unresponsive and floppy. She immediately picked him up; he was breathing, and slowly came around over the next 5–10 minutes. An ambulance was called and he was taken to hospital and monitored for 4 hours, where he remained well. Over the next 24 hours he was more sleepy than normal, but there were no further events.
Past medical history: he was born via a normal vaginal delivery. At 1 month of age he had some recurrent vomiting consistent with gastro-oesophageal reflux, and settled with thickened feeds. Developmentally he was smiling, interactive, and had normal newborn hearing screening. There is no sig-nificant family history.
Examination
• Growth: weight = 5 kg (50th centile)
• Head circumference = 41 cm (75th centile)
• Length = 58 cm (75th centile)On examination he was alert, smiling, had a number of Mon-golian blue spots on the buttocks, but no other neurocutaneous stigmata. He had normal tone, power, and reflexes. Cardiovas-cular, respiratory, and abdominal examinations were normal.(a) What is the most likely diagnosis?
Episode related to gastro-oesophageal reflux (GORD)ArrhythmiaHypotonic hyporesponsive episode (HHE)
Paediatrics and child health 19:6 294 © 2009 elsevier ltd. all rights reserved.
self-assessment
Atonic seizureAcute life-threatening episode (ALTE)
(b) What investigations would you recommend?Electrocardiogram (ECG)Electroencephalogram (EEG)pH studyNone required
(c) What would you recommend for future vaccinationsNo further vaccinationsSeparate vaccinations (i.e. one vaccine at a time)Vaccinate under supervision in clinic/hospital
(d) Vaccinate as per schedule with normal immunization provider
Case 3A 10-month-old boy presented with a 4-week history of vomit-ing, increased peripheral oedema and weight loss. Five days prior to admission he developed diarrhoea Six weeks earlier he had had an episode of bronchiolitis, but no other signifi-cant past medical history. He was exclusively breast-fed for 6 months before starting solids, and at presentation was on an extensive diet and three to four breast-feeds daily. There was no recent history of overseas travel, he was not on any medi-cations, and immunizations were up to date.
On admission
• Weight = 8.65 kg (10–25th centile)
• Blood pressure = 90/60
• Pulse rate = 80/min regular
• Capillary return less than 2 seconds
• Oedema of legs (non-pitting) to ankles and mild swelling of hands
• Chest clear, normal percussion
• Abdomen soft and non-tender, no masses, no organomegaly, no ascites
• Cardiovascular examination normal
Investigations
• Full blood count Value Reference range
haemoglobin 136 g/l (h) 105–135 g/l
haematocrit 0.40 0.33–0.41
rcc 5.56 × 1012/l (h) 3.7–5.3 × 1012/l
mch 24.5 pg 23–31 pg
mcV 72 fl 70–90 fl
rdW 16.8% (h) 11–14%
nuc rBc 0.4 × 109/l (h) 0–0
Platelets 524 × 109/l (h) 150–400 × 109/l
Wcc 40.7 × 109/l (h) 6.0–18.0 × 109/l
i/t ratio 0.04 less than 0.12
neut seg 14.98 × 109/l (h) 1.0–8.5 × 109/l
Value Reference range
lymphocytes 12.62 × 109/l (h) 4.0–10.0 × 109/l
monocytes 2.85 × 109/l (h) 0.1–1.0 × 109/l
eosinophils 2.44 × 109/l (h) 0–0.8 × 109/l
Bands 0.81 × 109/l (h) 0–0.5 × 109/l
rcc, red cell count; mch, mean corpuscular haemoglobin; mcV, mean corpus-cular volume; rdW, red cell distribution width; nuc rBc, nucleated red blood cells; Wcc, white cell count; i/t ratio, immature to total neutrophil ratio; neut seg, segmented neutrophils; h, high.
Blood film
• Left shift
• High neutrophil count and reactive lymphocytes
• Normal morphology
• Nil blastsESR: 12 mm/h (range 0–6)CRP: 18 mg/l (less than 8)
Faeces
Macroscopic
appearance:
Cream unformed
microscopy White blood cells not detected
red blood cells not detected
fat globules not detected
fatty acid crystals ++
ethyl acetate conc.
performed (Y/n)
no growth
Parasites Ova, cysts or parasites
not detected
culture Salmonella, Shigella, Campylobacter,
Aeromonas, Plesiomonas, Yersinia
not isolated
Electrolytes & liver function tests
Value Reference range
sodium 130 mmol/l (l) 135–145 mmol/l
Potassium 3.2 mmol/l (l) 3.5–5.1 mmol/l
chloride 110 mmol/l 98–110 mmol/l
Urea 3.1 mmol/l 1.3–6.6 mmol/l
creatinine 0.03 mmol/l 0.01–0.03 mmol/l
total Bili
(Bu + Bc)
1 μmol/l
Bu 1 μmol/l 0–10 μmol/l
Bc 0 μmol/l 0–5 μmol/l
alP 85 iU/l (l) 100–350 iU/l
GGt less than 5 iU/l 0–40 iU/l
Paediatrics and child health 19:6 295 © 2009 elsevier ltd. all rights reserved.

self-assessment
Value Reference range
total protein 30 g/l (l) 50–71 g/l
albumin 14 g/l (l) 29–45 g/l
alt 54 iU/l less than 55 iU/l
Bili, bilirubin; Bu, unconjugated bilirubin; Bc, conjugated bilirubin; alP, alka-line phosphatase; GGt, γ-glutamyl transferase alt, alanine aminotransferase; l, low.
α1 antitrypsin
Value Reference range
faecal α1
antitrypsin
1615 mg/l (h) 2–324 mg/l
a1 antitrypsin
clearance
27.8 ml/day (h) 0.5–16.4 ml/day
h, high.
Urine protein/creatinine ratio
Value Reference range
Urine protein (random) 0.11 g/l
Urine creatinine: 2.21 mmol/l
Protein/creatinine ratio: 0.05 g/mmol
creatinine
(less than 0.06)
Coeliac screen
Value Reference range
iga (quantitative) 0.12 0.1–1.29
deamidated gliadin peptide ab iga 8 lU negative (less
than 20)
tissue transglutaminase ab iga 3 lU negative (less
than 20)
ab, antibody; iga, immunoglobulin a.
Serum allergy test results
RAST
egg white 0.02 kUa/l
milk 0.05 kUa/l
Wheat 0.06 kUa/l
Interpretation Of RAST scores less than 0.35 kUa/l: negative
0.35–0.70 kUa/l: low positive
0.7–3.5 kaU/l: moderate positive
3.5–17.5 kaU/l: high positive
greater than 17.5 kaU/l: very high
positive
rast, radioallergosorbent test.
Chest x-ray: normal, no evidence of pleural or pericardial effusion.
Ultrasound:• Multiple peristalsing thick-walled fluid-filled loops of
bowel seen throughout the abdomen
• No free intraperitoneal fluid
• No abnormal mass or collection
• Normal liver, spleen, kidneys
(a) What is the most likely diagnosis?
Intestinal lymphangiectasiaLeukaemiaCoeliac diseaseEosinophilic gastroenteritisInflammatory bowel disease
(b) What investigations would you recommend?
Computed tomography (CT) of abdomenBone-marrow aspirateSerum immunoglobulinsGastroscopy/colonoscopy and biopsyAll of the above
(c) What would you recommend as initial treatment whilst awaiting investigations?
Amino-acid-based formulaMedium-chain triglyceride (MCT) formula20% albumin infusionGluten-free diet
Answers
Case 1
(a) Juvenile idiopathic arthritis (JIA)
JIA comprises a group of diseases of unknown aetiology that are manifested by chronic joint inflammation. Over the past decade JIA has been treated with more intensive therapy through a multidisciplinary approach to try and minimize the morbidity from chronic arthritis. Multiple classification sys-tems are used internationally, but the key features are onset at less greater than 16 years of age, clinical arthritis, duration of greater than 6 weeks, and type defined by presentation: oligo-arthritis/pauci-articular disease, polyarthritis, or systemic-onset disease.
A thorough rheumatological examination and baseline investigations are very helpful in excluding differential diag-noses, including infection (septic arthritis, osteomyelitis) or postinfectious causes such as reactive arthropathy. The rheu-matological differential includes other conditions that can be present with arthritis, including systemic lupus erythematosus,
Paediatrics and child health 19:6 296 © 2009 elsevier ltd. all rights reserved.

self-assessment
juvenile dermatomyositis sarcoidosis and vasculitic syndrome. Arthritis can also be seen in leukaemia, although it is often deeper bone pain, and oligoarthritis can be seen with other chronic diseases such as inflammatory bowel disease.
Haematological investigations in JIA may show a raised white cell count and inflammatory markers. These investigations are often done in conjunction with radiological investigations such as skeletal x-rays, bone scans and ultrasound, especially when considering the differential diagnoses of infection or trauma. Rheumatoid factor is positive in around 7–10% of older patients with polyarticular JIA and is a indicator of poor prognosis. Other features associated with poor prognsosis include: older age at onset, the presence of rheumatoid nodules, and disease of the cervical spine or hip. JIA rarely presents as isolated arthritis of the hip, so an irritable hip or reactive arthropathy was the most likely diagnosis early in the course of the illness in the case outlined above. JIA became more likely as the symptoms continued at 6 weeks, were worse in the morning, response to NSAIDs was minimal, and other joints became involved.
(b) MRI joints with contrast
MRI is a helpful adjunct in investigating joint pathology, as it is the only radiological modality that can differentiate proliferating synovial tissue from an effusion and the other joint components (e.g. cartilage, bone, ligaments and ten-dons). Since proliferating tissue enhances, contrast (e.g. gadolinium), is required to improve the sensitivity, but as it dissipates quickly only three or four joints can be reviewed at one time. MRI of the joints may also be used to monitor disease progression and response to treatment.
(c) Corticosteroid joint injections
Treatment of JIA aims to minimize longer-term morbidity and progression into adulthood. A multidisciplinary approach includes paediatric rheumatologists, nurse specialists, physio-therapists, occupational therapists and psychologists. Regular ophthalmological review is also required to detect asymptom-atic uveitis. Standard drug therapy initially involves the use of NSAIDS and corticosteroid injections into affected joints. Oral or systemic glucocorticoids are usually reserved for overwhelming inflammatory or systemic illness (e.g. sys-temic-onset disease), their longer-term role being limited by side-effects. Methotrexate is the most commonly used sec-ond-line agent which can be given weekly either orally or subcutaneously. More intensive therapy is also now offered to refractory patients and may include disease-modifying bio-logic agents such as etanercept (a tumour necrosis factor α (TNFα) inhibitor), anakinra (an interleukin 1 (IL-1) receptor antagonist), infliximab (a TFNα inhibitor), and adalimumab (an IgG1 humanized monoclonal anti-TNFα antibody). Newer drugs are emerging with the ever-increasing understanding of the role of cytokines and cytokine genotypes in subgroups of JIA. This will allow for improved therapy based on individual host factors.
FURthER REAdIng
Gardner-medwin Jm, irwin G, Johnson K. mri in Juvenile idiopathic
arthritis and Juvenile dermatomyositis. Annn y Acad Sci 2009;
1154: 52–83.
mccann lJ, Wedderburn lr, hasson n. Juvenile idiopathic arthritis
Arch Dis Child Ed Pract 2006; 91: ep29–ep36.
miller ml, cassidy Jt. Juvenile rheumatoid arthritis. pp: 1001–
1010. in: Kliegman rm, Behrman re, Jenson hB, stanton Bf,
eds. Nelson textbook of pediatrics. 18th edn. Philadelphia:
saunders; 2007.
Case 2
(a) hypotonic hyporesponsive episode (hhE)
This reaction post-vaccination is consistent with a significant adverse event following immunization (AEFI) called a hypo-tonic hyporesponsive episode (HHE). Other terms for these events have included ‘collapse’ or ‘shock-like episodes’. They have clinical features of the child appearing acutely pale, floppy (hypotonic), and unresponsive. Usually patients do not respond to direct stimulation and slowly come around over the next 1–30 minutes. They are often more sleepy than usual over the next 24 hours. The reactions can be a frighten-ing experience for parents and physicians. It is an uncommon AEFI which occurs in approximately one in 20–40,000 vaccine doses. It is most commonly seen with the first infant vac-cines at 2 months of age, and usually occurs around 3–4 hours post-immunization, but can occur immediately or up to 24–48 hours post-vaccination. It was seen more commonly with whole-cell pertussis vaccine, but does still occur with other vaccines, including those containing acellular pertussis.
The differential includes an atonic seizure, but this is usu-ally characterized by unconsciousness rather than hypore-sponsiveness, and whilst tone is decreased there is usually no pallor or cyanosis. An acute life-threatening episode (ALTE) has similar features that overlap with an HHE, but classically ALTE has associated apnoea and/or cyanosis. In addition, an HHE, as outlined above, usually occurs within 48 hours of an immunization. In this case there was no history of previous events and no family history or examination findings to sug-gest a cardiac anomaly.
The pathophysiology of HHE remains uncertain. It appears that multiple factors are implicated, including host or vac-cinee characteristics, neurological development, immunologi-cal phenomena, and some component of the vaccine(s). The constellation of symptoms described in an HHE is the same as a vaso-vagal or fainting type of event, and this term is preferred in children over the age of 2 years who more com-monly have an immediate event post-immunization.
(b) none required
Assessment following an HHE includes a thorough history and physical/neurological examination. Investigations are
Paediatrics and child health 19:6 297 © 2009 elsevier ltd. all rights reserved.

self-assessment
often not indicated, but should be undertaken if the patient has atypical features: e.g. ECG if the cardiac exam is abnor-mal or there is a family history of arrhythmias, EEG if features or history are suggestive of a possible seizures.
(c) Vaccinate under supervision
In the past an HHE was a contraindication to further whole-cell pertussis immunization, which had an HHE rate of 1 in 3000 vaccine doses, but is not for acellular pertussis or other vac-cines. The recurrence rate in the limited number of published studies has been between 0 and 5%. As the recurrence rate is low, most vaccinologists would not recommend separating the future vaccinations required. The difficulty is that the HHE episodes can occur up to 24 hours post-vaccination, and many centres would recommend administration of future vaccina-tion under medical supervision either in a day medical unit or with overnight admission, especially if the HHE was delayed. This will often help reassure the parents and ensure the child is adequately protected from vaccine-preventable diseases. Importantly, the studies following up children who have had an HHE showed that these episodes have no long-term effect on development when compared with school age-matched peers.
FURthER REAdIng
Baraff lJ, shields Wd, Beckwith l, et al. infants and children
with convulsions and hypotonic–hyporesponsive episodes
following diphtheria–tetanus–pertussis immunization: follow-up
evaluation. Pediatrics 1988; 81: 789–94.
Buettcher m, heininger U, Braun m, et al. hypotonic-hyporesponsive
episode (hhe) as an adverse event following immunization in
early childhood: case definition and guidelines for data collection,
analysis, and presentation. Vaccine 2007; 25: 5875–81.
Goodwin h, nash m, Gold m, et al. Vaccination of children following
a previous hypotonic hyporesponsive episode. J Paediatr Child
Health 1999; 35: 549–52.
Case 3
(a) Intestinal lymphangiectasia
Children with a protein-losing enteropathy classically present with ascites, peripheral oedema, and a low serum albumin. Albumin loss from the gastrointestinal tract is usually less than 15% of the total body albumin, but may be high as 60% in an enteropathy as seen in this case. Faecal antitrypsin lev-els are elevated as this protein is negligibly broken down in the gastrointestinal tract and is therefore a good screening test for protein loss.
There is a long list when It comes to the differential diag-nosis of a protein-losing enteropathy. Diagnoses are usually classified into groups depending on the aetiology:
mucosal damage leading to increased permeability:
• Erosive: ulceration of stomach/duodenum, pseudomem-branous colitis, ulcerative colitis
• Non-erosive: connective tissue disorders, coeliac diseases, allergic (eosinophilic) gastroenteritis, parasitic infection
mechanical lymphatic obstruction:
• For example, intestinal lymphangiectasia, tuberculosis, sarcoidosis
(b) All of the above
Intestinal lympangiectasia presents with the symptoms of a pro-tein-losing enteropathy, and the obstruction of lymphatic drain-age may be due to congenital defects in lymphatic ducts or to secondary causes such as constrictive pericarditis, malrotation, lymphoma and post-cardiac surgery. Patients with congenital lympangiectasia usually present in the first decade of life, with the first signs often being peripheral oedema and diarrhoea. Fal-tering growth may be a presenting feature in younger children. Immunoglobulins are usually low due to protein loss, but oppor-tunistic infections rarely occur. A bone-marrow aspirate should be strongly considered to rule out occult malignancy, which may have supportive examination and haematological findings. Abdominal ultrasound and CT scans can help identify dilated intestinal loops, thickened folds and nodular protrusions, and can be very helpful when considering other differential diagno-ses. Chylous pleural effusions may also be seen on chest x-ray in some cases. Endoscopy and jejunal biopsy is the gold stan-dard in histologic confirmation of intestinal lymphangiectasia. Macroscopically, white nodules and xanthomatous plaques are often visualized and submucosal elevations identified. Because of the patchy nature of the disease in the small intestine, often multiple biopsies need to be taken which show dilated lacteals with distortion of mucosal and submucosal villi in the absence of an inflammatory response. Capsule endoscopy is a new tech-nique for visualizing characteristic features in the small intestine which cannot be seen with standard endoscopy.
(c) Medium-chain triglyceride (MCt) formula
Treatment of intestinal lymphangiectasia includes dietary management, minimizing long-chain fat intake by using a medium-chain triglyceride (MCT) formula. Supplementation with fat-soluble vitamins (e.g. A, D, E, and K) is important because of losses due to malabsorption. If an isolated area of bowel is involved, surgical resection may be a management option. Treatment with albumin infusions is usually reserved for haemodynamic instability, as replacement will not treat the underlying cause. Octreotide has been reported as a therapy in refractory cases. Treatment of secondary intestinal lymphangiectasia involves dietary modulation as per above, as well as management of the underlying cause.
FURthER REAdIng
sood mr. disorders of malabsorption. in: Kliegman rm, Behrman
re, Jenson hB, stanton Bf, eds. Nelson textbook of pediatrics.
18th edn. Philadelphia: saunders; 2007, pp. 1584–1593.
radhakrishnan K, rockson sG. the clinical spectrum of lymphatic
disease. Ann NY Acad Sci 2008; 1131: 155–84.
Paediatrics and child health 19:6 298 © 2009 elsevier ltd. all rights reserved.