p 2 s -e c w p o -e -r b m - world...
TRANSCRIPT

CAPACITY BUILDING IN METAP COUNTRIES FOR
THE COST OF ENVIRONMENTAL DEGRADATION
POLICY PAPER 2
SOCIO-ECONOMIC COST OF WATER POLLUTION
AT THE OUM-ER-RBIA BASIN, MOROCCO
Submitted to
The World Bank
Sponsored by
September 2008

i
ACKNOWLEDGEMENT This paper is based on the data and methodologies presented in the study conducted by IRAM
développement (Institut de Recherches et d’Applications des Méthodes de Développements) and
sponsored by the World Bank, on the sanitary and economic impact of pollution reduction in ground
and surface water resources in the Oum Er Rbia basin in Morocco, in June 2007. The study and
associated data were made available by the World Bank.
Special thanks are extended to Dr. Dahlia Lotayef, Senior Environmental Specialist at the World Bank
and METAP Coordinator for the Middle East and North Africa Region, and Ms. Saliha Dobardzic,
METAP Operations Officer at The World Bank, as well as Mr. Fadi Doumani, Consultant at the World
Bank for their support and assistance during the implementation of this project.

ii
CONTENTS
ACKNOWLEDGEMENT ..................................................................................................................i
CONTENTS ..................................................................................................................................ii
TABLES ....................................................................................................................................... iii
FIGURES ..................................................................................................................................... iii
ACRONYMS ................................................................................................................................ iii
EXECUTIVE SUMMARY ............................................................................................................... iv
1 BACKGROUND......................................................................................................................... 1
2 STUDY AREA CHARACTERIZATION ........................................................................................... 3
3 METHODOLOGY ...................................................................................................................... 7
4 RESULTS .................................................................................................................................. 8
4.1 Damage Assessment.......................................................................................................... 8
4.2 Premature Mortality.........................................................................................................10
4.2.1 Human Capital Approach ......................................................................................11
4.2.2 Willingness to pay approach .................................................................................11
4.3 Morbidity .........................................................................................................................11
4.3.1 Cost of illness approach ........................................................................................11
4.3.2 Cost of pain and suffering (DALY) ..........................................................................15
4.4 Benefits ............................................................................................................................15
5 PRIORITIZATION OF INVESTMENT OPTIONS ...........................................................................15
6 CONCLUSION AND LIMITATIONS ............................................................................................17
BIBLIOGRAPHY ..........................................................................................................................17 ANNEX A- Location of Planned Sanitation Investments in the Oum Er Rbia Basin ......................19

iii
TABLES Table
1. Reduction in diarrheal disease morbidity by type of intervention based on meta-analysis
(Fewtrell et al., 2005) .....................................................................................................................2
2. Levels of Fecal Coliform (CFU/100 ml) in the Oum Er Rbia River water measured during 1999
and 2002 (adapted from IRAM développement, 2007) ..................................................................5
3. Pollutant levels in water samples from selected wells in 2004.......................................................6
4. Economic data .................................................................................................................................8
5. Incidence of water-related diseases in 2005 in the provinces of Settat, Safi, Al Jadida,
Khounifra, and Khourbiga ................................................................................................................8
6. Incidence of water-related diseases in 2005 in the Beni Mellal Province in the Oum Er Rbia basin ..........................................................................................................................9
7. Main inputs for the COI estimation by province ...........................................................................10
8. Calculation of DALYs due to child mortality in the Oum Er Rbia basin..........................................11
9. Cost of outpatient treatment and hospitalization in the provinces of Settat, Safi, Al Jadida,
Khounifra, and Khourbiga ..............................................................................................................12
10. Cost of Illness for non-hospitalized cases in 2005 in USD .............................................................13
11. Cost of hospitalization due to water-related diseases in the Beni-Mellal Province in USD ..........14
12. Cost of lost work days due to water-related diseases in the Oum Er Rbia Basin..........................14
13 Summary of estimated damage cost from morbidity associated with inadequate water and
wastewater management..............................................................................................................15
FIGURES
Figure
1. Population density distribution in the Oum Er Rbia basin (IRAM développement, 2007)..............4
2. Prioritization of investments based on reduction in the burden of disease .................................16
3. Prioritization of investments based on reduction in socio-economic costs..................................16
ACRONYMS
DALY = Disability Adjusted Life Years
GDP = Gross Domestic Product
HCA = Human Capital Approach
IRAM = Institut de Recherches et d’Applications des Méthodes de Développements
USD = United States Dollars
USEPA = United States Environmental Protection Agency WHO = World Health Organization
WTP = Willingness To Pay
iv
EXECUTIVE SUMMARY Domestic water supplies and environmental sanitation contribute to livelihoods in a wide range of
ways. They have important roles in promoting food security, health and household maintenance,
and water-based livelihoods. Poor water quality coupled with inadequate water and sanitation
services and hygiene practices has long been associated with higher water-borne diseases resulting
in a serious cost to society in the form of cost of illness and forgone earnings directly related to
increased morbidity and premature mortality, as well as cost of protective measures. In the Oum Er
Rbia basin, the uncontrolled discharge of untreated domestic and industrial wastewater along the
river and its tributaries, as well as agricultural runoff has caused significant degradation of surface
and ground water quality in the area. This has been associated with adverse health impacts on the
population in the basin, which manifested itself in terms of high incidence of waterborne diseases and infant mortality due to diarrheal diseases. Accordingly, this report assesses the socio-economic
costs of water pollution in the Oum Er Rbia river basin, based to a great extent on the outcome of
the study conducted in 2007 by IRAM développement and sponsored by the World Bank.
Methodology
As a first step, data collected from seven provinces by IRAM développement via field surveys and
secondary sources were analyzed. The surveys were conducted to estimate the number of water-
related morbidity cases, namely diarrhea, acute gastroenteritis, typhoid hepatitis, and dysentery,
recorded at medical facilities within the study area for one complete year (2005) as well as the
associated treatment costs. Mortality cases were not available so they were estimated indirectly. This was followed by the application of 1) the human capital and the willingness to pay approaches
for mortality valuation and 2) the cost of illness, pain and suffering approach for morbidity valuation.
The choice of valuation methods adopted was largely based on the availability of data concerning
each impact.
Findings
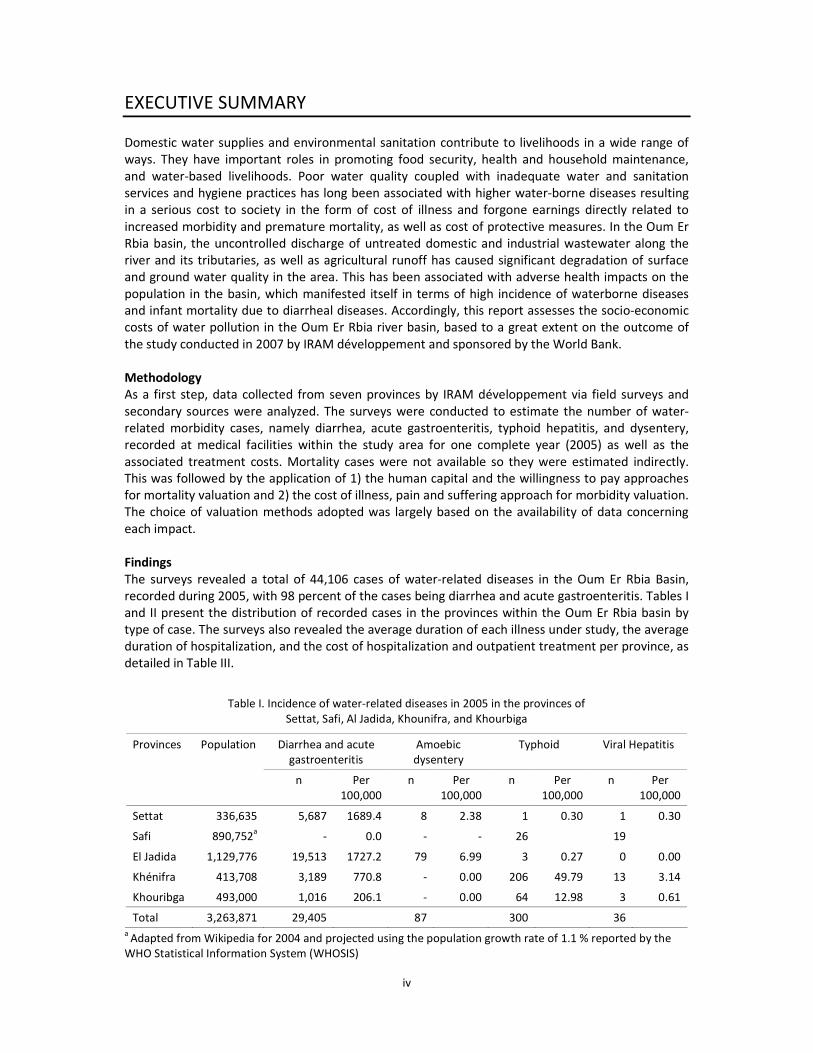
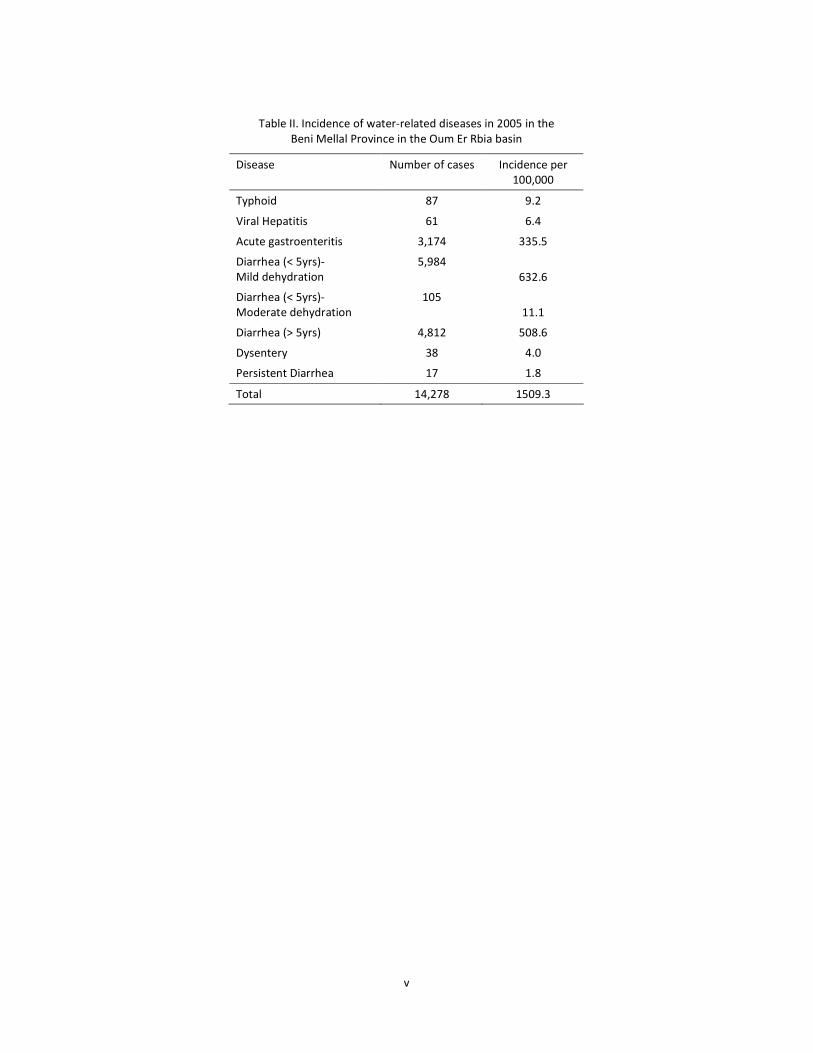
The surveys revealed a total of 44,106 cases of water-related diseases in the Oum Er Rbia Basin,
recorded during 2005, with 98 percent of the cases being diarrhea and acute gastroenteritis. Tables I
and II present the distribution of recorded cases in the provinces within the Oum Er Rbia basin by
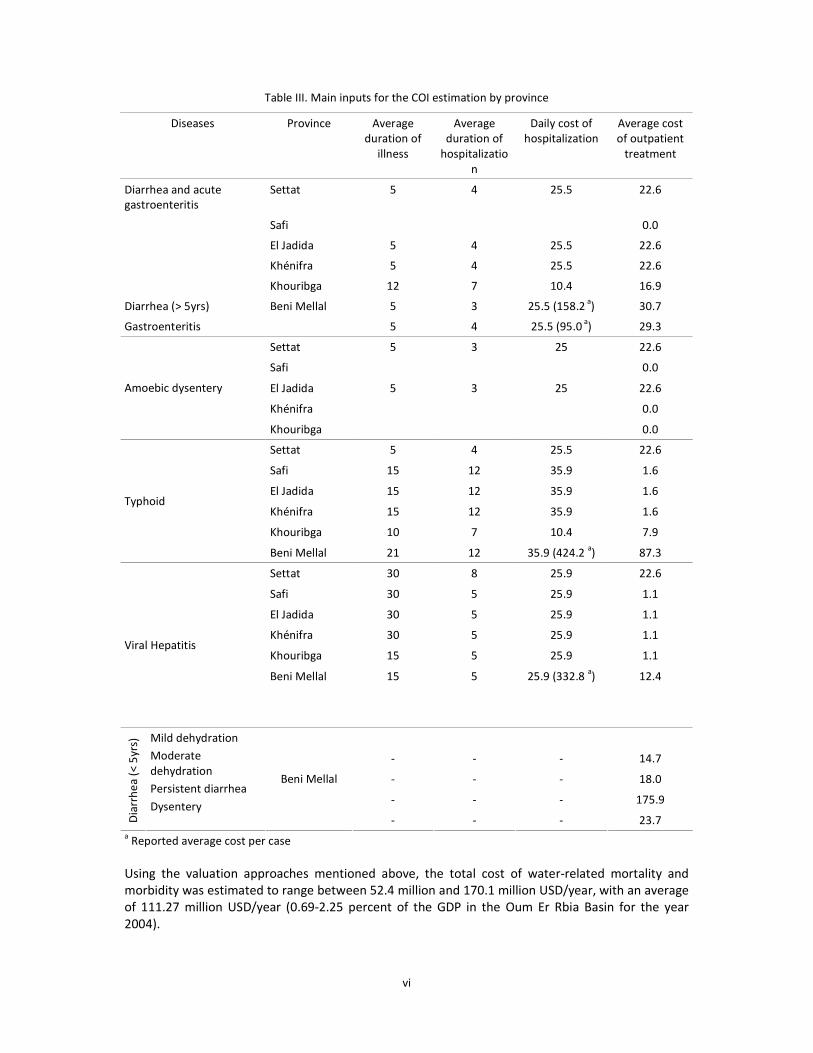
type of case. The surveys also revealed the average duration of each illness under study, the average
duration of hospitalization, and the cost of hospitalization and outpatient treatment per province, as
detailed in Table III.
Table I. Incidence of water-related diseases in 2005 in the provinces of
Settat, Safi, Al Jadida, Khounifra, and Khourbiga
Diarrhea and acute
gastroenteritis
Amoebic
dysentery
Typhoid Viral Hepatitis Provinces Population
n Per
100,000
n Per
100,000
n Per
100,000
n Per
100,000
Settat 336,635 5,687 1689.4 8 2.38 1 0.30 1 0.30
Safi 890,752a - 0.0 - - 26 19
El Jadida 1,129,776 19,513 1727.2 79 6.99 3 0.27 0 0.00
Khénifra 413,708 3,189 770.8 - 0.00 206 49.79 13 3.14
Khouribga 493,000 1,016 206.1 - 0.00 64 12.98 3 0.61
Total 3,263,871 29,405 87 300 36 a
Adapted from Wikipedia for 2004 and projected using the population growth rate of 1.1 % reported by the
WHO Statistical Information System (WHOSIS)
v
Table II. Incidence of water-related diseases in 2005 in the
Beni Mellal Province in the Oum Er Rbia basin
Disease Number of cases Incidence per
100,000
Typhoid 87 9.2
Viral Hepatitis 61 6.4
Acute gastroenteritis 3,174 335.5
Diarrhea (< 5yrs)-
Mild dehydration
5,984
632.6
Diarrhea (< 5yrs)-
Moderate dehydration
105
11.1
Diarrhea (> 5yrs) 4,812 508.6
Dysentery 38 4.0
Persistent Diarrhea 17 1.8
Total 14,278 1509.3
vi
Table III. Main inputs for the COI estimation by province
Diseases Province Average
duration of
illness
Average
duration of
hospitalizatio
n
Daily cost of
hospitalization
Average cost
of outpatient
treatment
Diarrhea and acute gastroenteritis
Settat 5 4 25.5 22.6
Safi 0.0
El Jadida 5 4 25.5 22.6
Khénifra 5 4 25.5 22.6
Khouribga 12 7 10.4 16.9
Diarrhea (> 5yrs) 5 3 25.5 (158.2 a) 30.7
Gastroenteritis
Beni Mellal
5 4 25.5 (95.0 a
) 29.3
Settat 5 3 25 22.6
Safi 0.0
El Jadida 5 3 25 22.6
Khénifra 0.0
Amoebic dysentery
Khouribga 0.0
Settat 5 4 25.5 22.6
Safi 15 12 35.9 1.6
El Jadida 15 12 35.9 1.6
Khénifra 15 12 35.9 1.6
Khouribga 10 7 10.4 7.9
Typhoid
Beni Mellal 21 12 35.9 (424.2 a) 87.3
Settat 30 8 25.9 22.6
Safi 30 5 25.9 1.1
El Jadida 30 5 25.9 1.1
Khénifra 30 5 25.9 1.1
Khouribga 15 5 25.9 1.1
Beni Mellal 15 5 25.9 (332.8 a) 12.4
Viral Hepatitis
- - - 14.7
- - - 18.0
- - - 175.9
Dia
rrh
ea
(< 5
yrs)
Mild dehydration
Moderate
dehydration
Persistent diarrhea
Dysentery
Beni Mellal
- - - 23.7 a Reported average cost per case
Using the valuation approaches mentioned above, the total cost of water-related mortality and
morbidity was estimated to range between 52.4 million and 170.1 million USD/year, with an average
of 111.27 million USD/year (0.69-2.25 percent of the GDP in the Oum Er Rbia Basin for the year
2004).

vii
Table IV. Estimated incurred damage costs associated with water pollution and uncontrolled
wastewater discharge in the Oum Er Rbia basin
Impact Methodology Total damage cost in
million USD
Total damage cost in percent of
GDP1(%)
Mortality HCA 46.2
WTP 163.9
Subtotal 46.2-163.9 0.6-2.2
Morbidity COI 6.17
DALY 0.047
Subtotal 6.22 0.09
Total 52.4-170.1 0.69-2.29
Finally, the annual benefits accrued from improved water supply and sanitation in the Oum Er Rbia
basin are estimated to range between 31.4 and 102.1 million USD per year, constituting 0.42 to 1.35
percent of the GDP in the Oum Er Rbia Basin for the year 2004. Using a social discount rate of 4%,
the present value of the flow of damage costs associated with pollution over a time span of 16 years
(till 2020) ranges between 366 million USD and 1,190 million USD with an average of 778 million
USD, which exceeds significantly the estimated cost of investment in water supply and sanitation in
the basin, amounting to 300 million USD.

1
1 BACKGROUND
Domestic water supplies and environmental sanitation contribute to livelihoods in a wide range of
ways. They have important roles in promoting food security, health and household maintenance,
and water-based livelihoods. In addition, the management of water supply and sanitation systems
has important effects on ecosystems that support livelihoods (Butterworth and Soussan, 2001). In
fact, polluted water, water shortages, and unsanitary living conditions, which are commonly
associated with increased waterborne illnesses and premature mortality, are one of the most
important global risk factors (WHO, 2004a; Esrey et al., 1991), whereby the burden created by this
risk factor has been reported to exceed many major diseases such as malaria or tuberculosis (Pruss
et al., 2002). With nearly 3 billion people lacking safe drinking water and adequate sanitation facilities (IRC 2007), water-related diseases have become a human tragedy, resulting in millions of
deaths each year, preventing millions more from leading healthy lives, and undermining global
development efforts. In 2004, an estimated 1.8 million deaths were attributed to unsafe water and
sanitation, including lack of hygiene, whereby 90 percent of this burden falls on children under five,
mostly in developing countries (WHO, 2004). Other vulnerable groups include the elderly and
pregnant women. In most countries the main risks to human health associated with the
consumption of polluted water are microbiological in nature. Waterborne and other water-related
diseases consist mainly of infectious diarrhea, typhoid and paratyphoid, cholera, salmonellosis,
shigellosis, amoebiasis, and other protozoan and viral intestinal infections. Some pathogens causing
these diseases are transmitted by water, but other forms of transmission do occur such as person-to-person contact, animal-to-human contact, and food and aerosols (Hunter, 1998). In addition to
water pollution by biological agents, chemical contamination should not be underestimated.
Chemicals such as nitrates, fluoride or arsenic in water can have long-term toxic effects.
There is significant evidence that the provision of improved water and sanitation to communities
lacking basic sanitation and using vulnerable and contaminated water can lead to a considerable
reduction in mortality and morbidity from water-related infectious disease. Fewtrell et al. (2005)
conducted a systematic review and meta-analysis to compare the effectiveness of these and similar
interventions. The examined interventions were reported to reduce the risks of diarrheal illness
significantly. Most interventions had a similar degree of impact on diarrhea illness, with the relative
risk estimates from the overall meta-analyses ranging between 0·63 and 0·75. Furthermore, multiple
interventions (consisting of combined water, sanitation, and hygiene measures) were not more
effective than interventions with a single focus (Table 1).

2
Table 1. Reduction in diarrheal disease morbidity by type of intervention
based on meta-analysis (Fewtrell et al., 2005)
Intervention Number of studies Relative risk
(95% Cl)
Hygiene 11 0·63 (0·52–0·77)
Excluding poor quality studies 8 0·55 (0·40–0·75)
Handwashing 5 0·56 (0·33–0·93)
Education 6 0·72 (0·63–0·83)
Sanitation 2 0·68 (0·53–0·87)
Water supply 6 0·75 (0·62–0·91)
Diarrhoea only 4 1·03 (0·73–1·46)
Household connection 2 0·90 (0·43–1·93)
Standpipe or community connection 3 0·94 (0·65–1·35)
Water quality 15 0·69 (0·53–0·89)
Source treatment only 3 0·89 (0·42–1·90)
Household treatment only 12 0·65 (0·48–0·88)
Household treatment
• excluding poor quality studies 8 0·61 (0·46–0·81)
• rural location 6 0·61 (0·39–0·94)
• urban/periurban 4 0·74 (0·65–0·85)
Multiple 5 0·67 (0·59–0·76)
Valuing the socio-economic benefits of such interventions requires a valuation of the cost of water
pollution and inadequate sanitation and hygiene, in the form of cost of illness and forgone earnings
associated with increased morbidity and premature mortality or cost of protective measures
referred to as averting expenditures such as purchasing bottled water or the incremental cost paid
to transport cleaner water from other sources (Esrey et al., 1991; Muller and Morera, 1994; WHO,
1996; 1998). Valuing the health impacts of water pollution faces many difficulties, including the
actual identification and measurement of health impacts and the estimation of monetary values for
associated mortality and morbidity. Generally, the economic valuation of health impacts proceeds by
conducting epidemiological studies in order to establish dose-response relationships (DRRs) linking environmental variables with observable health effects. However, in the case of water pollution,
establishing dose-response functions (DRFs) is complicated and less advanced than is the case of
evaluating health impacts from air pollution, for instance. Lately, efforts have concentrated on
quantifying this cost through the environmental burden of disease approach (Fewtrell et al., 2007;
Pruss et al., 2002), which adopted the Disability Adjusted Life Years (DALYs) as a unit measurement.
Pruss et al. (2002) calculated the burden of disease associated with water sanitation and hygiene
and estimated that globally these factors are responsible for 4 percent (2,213,000 cases) of all
deaths and 5.7% of disease burden. The authors also reported that the disease burden can be up to
240 times higher in developing regions when compared with a developed region. Yet, it should be
noted that the quantification of the disease burden due to water, sanitation, and hygiene is a complex task because of a) the numerous interrelated causes leading to transmission of water-
related diseases (source factors, pathway factors, behavioral factors); b) the complex exposure
patterns at the household and community level; and c) the scarce information on the risk factor–
disease relationship (Pruss et al. 2002).
Using various economic valuation approaches, this study examines the damage cost of water
pollution in the Oum Er Rbia Basin in Morocco where surface and groundwater water pollution

3
coupled with the lack of proper environmental service provisions are suspected to contribute to
significant health and other socio-economic impacts. An analysis is then conducted to prioritize
planned infrastructure interventions in the area, based on the results of the socio-economic
assessment. This paper is based on the study conducted by IRAM développement (2007) in the basin
of Oum Er Rbia. The data on the incidence of water-related morbidity and mortality and on the costs of treatment reported in the IRAM study were used without field ascertainment. The methodologies
adopted and calculations reported by IRAM développement were followed closely, and revised
when necessary. Mortality valuation methodologies were added to complement the existing
calculations. Not all data and valuation results were adopted, particularly when the methodology
followed in IRAM développement (2007) was not clear.
It is important to highlight the weaknesses of the data used in this assessment. First, no data on
mortality was available, and therefore, as reasonable as possible, assumptions were made to fill in
this gap. Second, the morbidity data collected were not clear with respect to the age distribution of
the cases and the percentage of the cases that were hospitalized. Third, there was no clear distinction between the characteristics of hospitalized and non-hospitalized cases. Fourth, the type
of data collected was not uniform across the various provinces in the Oum Er Rbia basin. As a result,
uncertainties in the calculations of the cost of illness are expected. In addition, the methodology for
the prioritization of the investment options was not explained in the study documents. Evidently, the
case provides guidelines and lessons about the need to clearly define data inputs at the onset of a
socio-economic assessment study to ensure that uniform data are collected all throughout and
minimize the assumptions that have to be made to bring the assessment to completion. Despite
these limitations which were addressed through relatively conservative assumption, it is clear that
the socio-economic cost of water pollution and inadequate sanitation in the Oum Er Rbia basin is
significant and that the planned investments are likely to be economically justified.
2 STUDY AREA CHARACTERIZATION
The Oum Er Rbia River is a main river in central Morocco and the longest in the country. The 550-km
long river has an average water debit of about 105 m3/s. It originates from the Middle Atlas at an
altitude of 1,800 m ASL, passes through the city of Khénifra in the Tadla plain and ends in the
Atlantic Ocean in Azemmour, 16 kms from the city of El Jadida. Oum Er-Rbia River has six dams, the
most important of which is Almassira Dam. Its main tributaries are El-Abid River, Tessaoute River,
and Lakhdar River (INECO Morocco, 2008; Wikipedia, 2008).
The Oum Er Rbia Basin has a population of around 4.5 million (19% of the total population) spread
over eight provinces, namely Beni Mellal, Khouribga, Settat, Khenifra, Azilal, El Kalaa of Sraghna, El
Jadida and Safi (Figure 1). Around 65 percent of the population in the basin lives in rural areas. The
economic activity in the basin is quite varied, including irrigated and rain-fed agriculture, agro-food
industries, mining industries, and numerous large transformation industries. In fact, the Oum Er Rbia
basin encompasses half of Morocco’s large scale irrigated areas and it produces 60 percent of the
country’s sugar beet, 40 percent of olives and 40 percent of the milk production.

4
Figure 1. Population density distribution in the Oum Er Rbia basin (IRAM développement, 2007)
Surface and ground water resources in the Oum Er Rbia basin are subject to significant pollution
from source and non-point sources. Given the intensive agricultural activity in the basin, agricultural
runoff laden with chemical fertilizers, pesticides, and herbicides is considered a major non-point
source of pollution, particularly nitrogen and phosphate. Another source of pollution in the basin is
domestic wastewater, which is discharged in an uncontrolled manner and without prior treatment
into the River. The daily discharge of raw wastewater into the river is estimated at 65,000 m3/d
(adapted from UNEP, 1995). Pollution from domestic wastewater discharge is more pronounced
during the dry season in downstream areas, particularly in Khenifra, Kasba Tadla, Beni Mellal, and
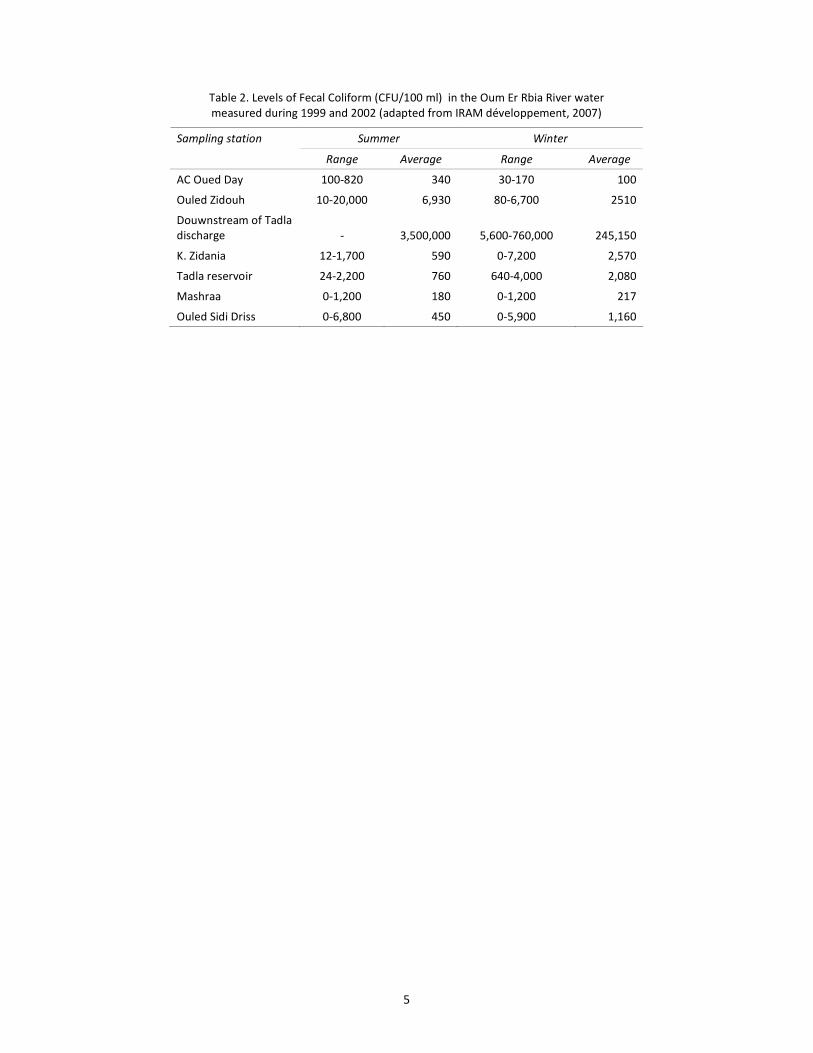
Azemmour. Polluted water from the River is often used for irrigation, which poses a risk to public
health. Table 2 shows fecal coliform levels in water samples from six stations along the Oum Er Rbia
River at various times of the year for the period 1999 to 2001. The reported concentrations ascertain the presence of significant microbiological pollution in the river water and thus the urgent need for
intervention. Groundwater aquifers were found to be equally vulnerable to domestic wastewater
pollution, whereby most local wells tested in 1995 showed bacteriological contamination, in addition
to elevated nitrate levels (Table 3). A third major source of water pollution in the Oum Er Rbia basin
is industrial in nature. Sugar refineries in Beni Mellal, Soul Sebti, and Oulad Ayyad, tanneries in
Khenifra and Beni Mellal, and olive presses in Afourer, Boujaad, and Fquih Ben Saleh, discharge their
industrial effluent into the environment without prior treatment. Levels of cadmium and arsenic,
slightly exceeding international water quality standards were detected in groundwater wells (Table
3). Finally, while the available data on water quality in the Oum Er Rbia basin are relatively old,
sporadic and incomplete, they are still indicative of the level of pollution in the basin with potential adverse impact on public health in the area.
5
Table 2. Levels of Fecal Coliform (CFU/100 ml) in the Oum Er Rbia River water
measured during 1999 and 2002 (adapted from IRAM développement, 2007)
Summer Winter Sampling station
Range Average Range Average
AC Oued Day 100-820 340 30-170 100
Ouled Zidouh 10-20,000 6,930 80-6,700 2510
Douwnstream of Tadla
discharge - 3,500,000 5,600-760,000 245,150
K. Zidania 12-1,700 590 0-7,200 2,570
Tadla reservoir 24-2,200 760 640-4,000 2,080
Mashraa 0-1,200 180 0-1,200 217
Ouled Sidi Driss 0-6,800 450 0-5,900 1,160

6
Table 3. Pollutant levels in water samples from selected wells in 2004
Province Parameter Arsenic (As)
(mg/l)
Cadmium (Cd)
(mg/l)
Chromium (Cr)
(mg/l)
Lead (Pb)
(mg/l)
Selenium (Se)
(mg/l)
Ammonium (NH4+)
(mg/l)
Nitrates (NO3-)
(mg/l)
Floride (F-)
(mg/l)
FC
(CFU/100 ml)
TC
(CFU/100 ml)
SC
(CFU/100 ml)
Min - - - - - 0.002 35.7 - 196 - -
Max - - - - - 0.89 35.7 - 4,716 - - Beni Mellal
Avg - - - - - 0.2900429 35.7 - 1931 - -
Min 0 0 0 0 0 0 0.626 0.12 0 0 0
Max 0.012 0.003 0.001 0.009 0.029 0.000 8,655 0.21 114 249 124 Khenifra
Avg 0.003 0.000 0.000 0.002 0.008 0.000 964.9 0.16 10 25 12
Min 0 0 0 0 0 0.0005 0.3 0.22 - - -
Max 0.005 0 0.002 0.002 0.001 0.060 65.9 1.20 - - - Azilal
Avg 0.003 0 0.002 0.002 0.001 0.032 26.6 0.50 - - -
Min 0.00225 0.00083 0.0037 0.004 0.002 0.00025 3.4 0.19 - - -
Max 0.004 0.001 0.014 0.036 0.007 0.220 2,758 1.32 - - - Khouribga
Avg 0.003 0.001 0.006 0.008 0.003 0.038 148.4 0.48 - - -
USEPA MAL 0.05 0.005 0.1 0.015 NA NA 10 4 0 0 NA Drinking water
Standards WHO GV 0.01 0.003 0.05 0.01 NA NA NA NA 0 0 NA

7
3 METHODOLOGY
In order to assess the impact of water pollution on health in the Oum Er Rbia basin, a field survey
was conducted to collect data from 13 centers in the province of Beni Mellal where investment
projects in water and sanitation are proposed. Accordingly concerned districts and municipalities
were visited. Data were collected on four waterborne diseases, namely typhoid, viral hepatitis, acute
gastroenteritis, and diarrhea. The data included the existing conditions of drinking water supply and
sanitation provision, incidence of diseases, the total population and the population under five. In addition, data on the costs of diseases, including out-patient consultation, hospitalization, and
treatment outside the hospital were provided by the Regional Hospital Center of Beni Mellal, the
Sanitary Division of Beni Mellal, and the French Agency for Development (through a study performed
on the profitability of the Wastewater Treatment Plant in Fez). Similar data were collected from
secondary sources for the provinces of Settat, Safi, Al Jadida, Khounifra, and Khourbiga. The data
were compiled and analyzed and then used to calculate the incidence of water-related diseases in
the basin and to estimate the cost of illness incurred by the society.
The next step was to estimate the damage cost of waterborne illnesses whereby health outcomes
were grouped into premature mortality and morbidity. While morbidity data were available through the health survey, mortality data were estimated based on statistics published by the World Bank
and the World Health Organization (WHO). Health outcomes during the year 2005 were considered
in the calculations, since they were the most complete. Mortality was expressed in terms of DALYs, a
methodology developed and applied by WHO and the World Bank in collaboration with international
experts to provide a common measure of the burden of disease for various illnesses and premature
mortality (World Bank, 2004). The DALY is defined as a health gap measure that extends the concept
of potential years of life lost due to premature death to include equivalent years of ‘healthy’ life lost
by virtue of being in states of poor health or disability (Murray and Lopez, 1996). It thus combines in
one measure the time lived with disability and the time lost due to premature mortality. To estimate
the DALY for a particular cause during a particular time period, the number of incident cases in that period is multiplied by the average duration of the disease and a weight factor that reflects the
severity of the disease on a scale from 0 (being in perfect health) to 1 (representing death). A year
lost to premature mortality represents one DALY, and future years lost are discounted at a fixed rate
of 3 percent to account for a social preference for a healthy year now, rather than in the future
(Pruss et al., 2003). Note that age weighting was not applied in the calculations.
In the valuation of mortality, the human capital approach was used to reflect the lower bound of the
estimation. This approach is based on foregone earnings and estimates the production lost from
premature death, accordingly the loss of one statistical year is valued at the level of Gross Domestic
Product (GDP) per capita. The upper bound is given by the willingness to pay approach (WTP), where
one DALY is assessed at the WTP for mortality risk reduction. The WTP approach uses statistical
techniques to record human behavior in trading off risk of dying with a certain amount of money.
Willingness to pay measures reflect the whole range of costs associated with premature death,
including loss of production (as in the human capital approach), suffering, losses imposed on other
family members and society, and other complex attributes associated with a human life.
To assign a monetary value for morbidity, the cost of illness approach (COI) was used to estimate
treatment costs, including medical consultation fees, medications and hospitalizations, as well as the
opportunity cost of the time spent being sick or lost work days. This was complemented by a valuation of DALYs lost to morbidity in relation to GDP per capita to account for the cost of pain and
suffering from illness.

8
Finally the health impact of water pollution and inadequate sanitation was calculated as an annual
value, based on 2004 mortality data and 2005 morbidity data. Other economic data used in the
calculations are summarized in Table 4.
Table 4. Economic data
Parameter Value Reference
Morocco population (2004) 29.8 million World Bank (2006)
Oum Er Rbia population (2004) 4.5 million IRAM développement (2007)
GDP (2004) 50,031 million USD World Bank (2006)
GDP per capita (2004) 1,679 USD World Bank (2006)
Parity (Average for 2004-2005) 8.867 (Dh/USD) CIA World Fact Book (2008)
4 RESULTS
4.1 Damage Assessment
The survey revealed a total of 44,106 cases of water-related diseases in the Oum Er Rbia Basin,
recorded during 2005, with 98 percent of the cases being diarrhea and acute gastroenteritis. Table 5
and Table 6 present the distribution of recorded cases in the provinces within the Oum Er Rbia basin
by type of case. Note that it was not clear whether the reported cases pertained strictly to morbidity
or whether they encompassed mortality cases as well. As such, these cases were considered only
morbidity cases and mortality cases were estimated separately.
Table 5. Incidence of water-related diseases in 2005 in the provinces of
Settat, Safi, Al Jadida, Khounifra, and Khourbiga
Diarrhea and acute
gastroenteritis
Amoebic
dysentery
Typhoid Viral Hepatitis Provinces Population
n Per
100,000
n Per
100,000
n Per
100,000
n Per
100,000
Settat 336,635 5,687 1689.4 8 2.38 1 0.30 1 0.30
Safi 890,752a - 0.0 - - 26 19
El Jadida 1,129,776 19,513 1727.2 79 6.99 3 0.27 0 0.00
Khénifra 413,708 3,189 770.8 - 0.00 206 49.79 13 3.14
Khouribga 493,000 1,016 206.1 - 0.00 64 12.98 3 0.61
Total 3,263,871 29,405 87 300 36 a
Adapted from Wikipedia for 2004 and projected using the population growth rate of 1.1 % reported by the
WHO Statistical Information System (WHOSIS)
9
Table 6. Incidence of water-related diseases in 2005 in the
Beni Mellal Province in the Oum Er Rbia basin
Disease Number of cases Incidence per
100,000
Typhoid 87 9.2
Viral Hepatitis 61 6.4
Acute gastroenteritis 3,174 335.5
Diarrhea (< 5yrs)-
Mild dehydration
5,984
632.6
Diarrhea (< 5yrs)-
Moderate dehydration
105
11.1
Diarrhea (> 5yrs) 4,812 508.6
Dysentery 38 4.0
Persistent Diarrhea 17 1.8
Total 14,278 1509.3
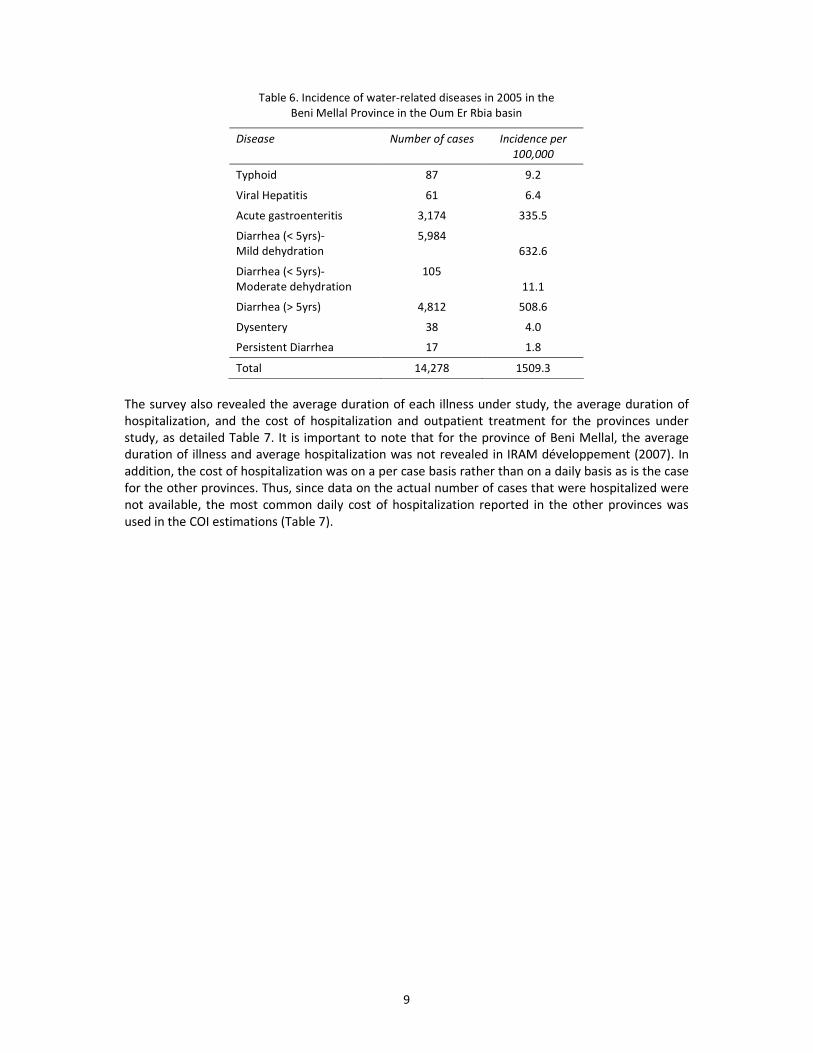
The survey also revealed the average duration of each illness under study, the average duration of
hospitalization, and the cost of hospitalization and outpatient treatment for the provinces under
study, as detailed Table 7. It is important to note that for the province of Beni Mellal, the average duration of illness and average hospitalization was not revealed in IRAM développement (2007). In
addition, the cost of hospitalization was on a per case basis rather than on a daily basis as is the case
for the other provinces. Thus, since data on the actual number of cases that were hospitalized were
not available, the most common daily cost of hospitalization reported in the other provinces was
used in the COI estimations (Table 7).

10
Table 7. Main inputs for the COI estimation by province
Diseases Province Average
duration of
illness
Average
duration of
hospitalization
Daily cost of
hospitalization
Average cost
of outpatient
treatment
Diarrhea and acute
gastroenteritis
Settat 5 4 25.5 22.6
Safi 0.0
El Jadida 5 4 25.5 22.6
Khénifra 5 4 25.5 22.6
Khouribga 12 7 10.4 16.9
Diarrhea (> 5yrs) 5 3 25.5 (158.2 a) 30.7
Gastroenteritis
Beni Mellal
5 4 25.5 (95.0 a
) 29.3
Settat 5 3 25 22.6
Safi 0.0
El Jadida 5 3 25 22.6
Khénifra 0.0
Amoebic dysentery
Khouribga 0.0
Settat 5 4 25.5 22.6
Safi 15 12 35.9 1.6
El Jadida 15 12 35.9 1.6
Khénifra 15 12 35.9 1.6
Khouribga 10 7 10.4 7.9
Typhoid
Beni Mellal 21 12 35.9 (424.2 a) 87.3
Settat 30 8 25.9 22.6
Safi 30 5 25.9 1.1
El Jadida 30 5 25.9 1.1
Khénifra 30 5 25.9 1.1
Khouribga 15 5 25.9 1.1
Beni Mellal 15 5 25.9 (332.8 a) 12.4
Viral Hepatitis
- - - 14.7
- - - 18.0
- - - 175.9
Dia
rrh
ea
(< 5
yrs)
Mild dehydration
Moderate
dehydration
Persistent diarrhea
Dysentery
Beni Mellal
- - - 23.7 a Reported average cost per case
4.2 Premature Mortality
In the absence of population-based vital registries, mortality rates in the Oum Er Rbia basin due to
diarrhea were estimated from statistical data published by the World Bank and were limited to
children under five. As depicted in Table 8, given a child mortality rate of 38 per 1,000 (World Bank,

11
2006) of which 20 percent are attributable to diarrhea (World Bank, 2003), the annual number of
deaths due to diarrhea among children under five was estimated at 786 cases.
Table 8. Calculation of child mortality in the Oum Er Rbia basin
Parameter Value
Population in Oum Er Rbia Basin 4.5 million
Birth rate in Morocco in 2004 a 23 births per 1,000 population
Live births in Oum Er Rbia Basin in 2004 103,500
Child mortality rate 38 per 1,000 live births
Annual child deaths (all causes) 3,933 per year
Child diarrheal disease deaths b 20.0% of child mortality rate
Annual child diarrheal disease deaths 786
4.2.1 Human Capital Approach
According to the Global Burden of Disease approach (Murray and Lopez, 1996), it is estimated that the death of a child under five represents the loss of 35 DALYs. Thus, the estimated child deaths in
the Oum Er Rbia basin due to diarrhea represent an annual loss of 27,510 DALYs. Using the human
capital approach (HCA), if one year of a person’s life is lost, society loses, at the very least, the
contribution of this person to production, approximated by the GDP per capita, for income during
the ages of 20 to 65 years, at a discount rate of 3 percent. One DALY is assessed at 1,679 USD, which
is the equivalent GDP per capita (World Bank, 2006). Thus, the loss of DALYs due to children
mortality is estimated at 46.2 million USD (0.6 percent of the GDP in the Oum Er Rbia region for the
year 2004).
4.2.2 Willingness to pay approach
While WTP data for Morocco are not available, WTP estimated in Europe and North America can be applied by adjusting for GDP per capita differentials. The adjusted WTP in Morocco for mortality risk
reduction of adults is estimated at 5,957 USD (World Bank, 2003). Accordingly, the loss of DALYs due
to children mortality, based on the willingness to pay approach is estimated at 163.9 million USD. As
such, the damage cost due to infant premature mortality, taking both the HCA and WTP approaches
into account is estimated to range between 46.2 and 163.9 million USD, with an average of 98.3
million USD (0.6-2.2 percent of the GDP in the Oum Er Rbia region for the year 2004).
4.3 Morbidity
Morbidity valuations were conducted based on the available data in each province. Cases that were
considered in the provinces of Settat, Safi, Al Jadida, Khounifra, and Khourbiga pertained to diarrhea,
acute gastroenteritis, viral hepatitis, typhoid, and amoebic dysentery. In the Beni Mellal province, in
addition to the diseases mentioned above, diarrhea cases were categorized according to age and to the severity of the associated dehydration (Table 6).
4.3.1 Cost of illness approach
Based on the inputs obtained via the health survey by IRAM développement (2007) and listed in
Table 7, the cost of outpatient treatment and hospitalization in the Settat, Safi, Al Jadida, Khounifra,
and Khourbiga provinces amounted to 3.83 million USD (Table 9).

12
Table 9. Cost of outpatient treatment and hospitalization in the provinces of
Settat, Safi, Al Jadida, Khounifra, and Khourbiga
Provinces Diseases
Settat Safi El Jadida Khénifra Khouribga
Total
No. of cases 5,687 - 19,513 3,189 1,016 29,405 Diarrhea
Cost (USD) 708,069 - 2,429,497 397,052 90,978 3,625,596
No. of cases 8 - 79 - - 87 Amoebic
dysentery Cost (USD) 792 - 7,822 - - 8,615
No. of cases 1 26 3 206 64 300 Typhoid
Cost (USD) 125 11,230 1,296 88,979 88,979 190,609
No. of cases 1 19 - 13 3 36 Viral Hepatitis
Cost (USD)) 230 2,486 - 1,701 392 4,809
Total (USD) 709,216 13,716 2,438,616 487,732 180,350 3,829,629
Morbidity valuation using the COI approach for the Beni Mellal province was conducted separately
from the other provinces as different input data were available. Accordingly, the cost of outpatient
treatment was estimated separately to be around 0.33 million USD. Around 45 percent of the cost
pertains to diarrhea cases greater than 5 yrs of age and 28 percent of the cost pertains to cases of
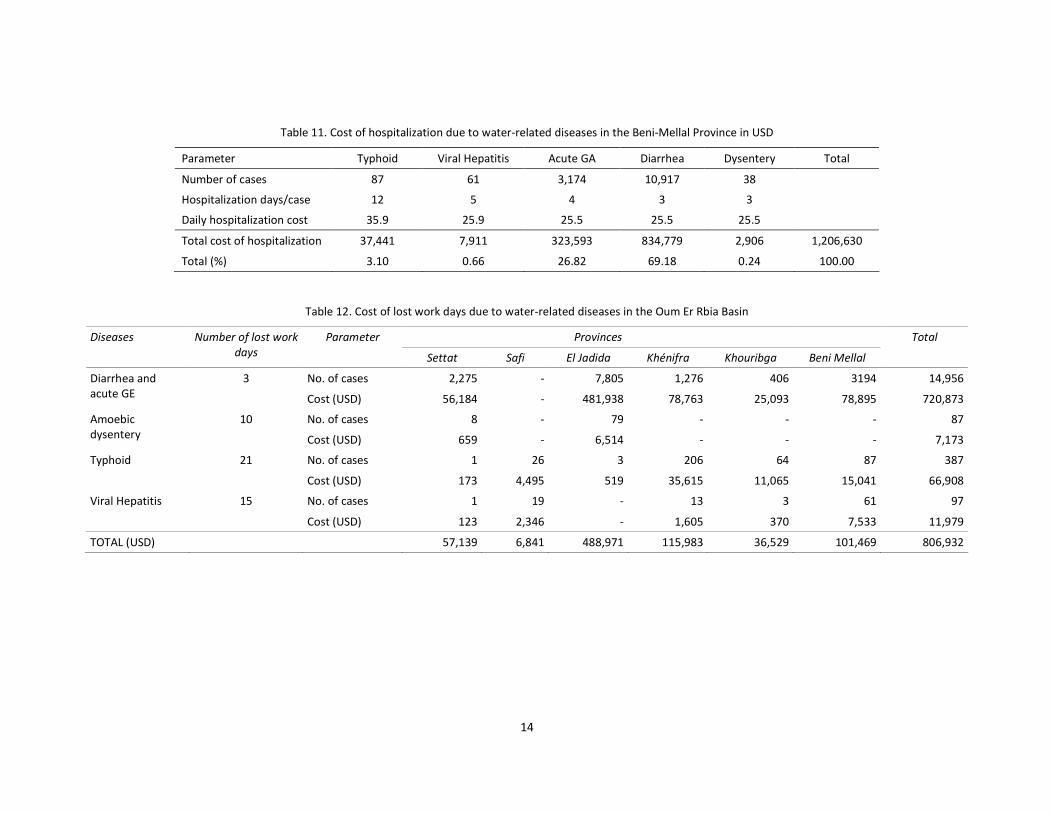
acute gastroenteritis (Table 10). As for the cost of hospitalization, and in the absence of the exact
number of cases that were hospitalized, the same methodology that was applied to the other
provinces was applied for Beni Mellal. In other words, each of the reported cases was considered to
have received hospitalized treatment. Accordingly, the cost of hospitalization due to water-related
illnesses in the Beni Mellal province amounted to 1.2 million USD (Table 11). Around 69 percent of
the cost pertains to diarrhea cases and 27 percent pertains to cases of acute gastroenteritis.
Regarding the cost of lost work days in the Oum Er Rbia basin, and in the absence of age distribution
of cases, it is assumed the 40 percent of the reported diarrhea and gastroenteritis cases are adults. For the remaining diseases, it is assumed that 100 percent of the cases pertain to adults. Based on
the average number of lost work days listed in Table 12 and an average wage rate of 8.23 USD per
day (taking urban and rural wage rates into account), the total cost of lost work days in the Oum Er
Rbia basin due to water-related diseases amounted to 0.8 million USD.

13
Table 10. Cost of Illness for non-hospitalized cases in 2005 in USD
Diarrhea (< 5yrs)
Dehydration
Population center Typhoid Epidemic
Hepatitis
Acute
Gastroenteritis
Diarrhea (> 5yrs)
A B C
Dysentery Persistent
diarrhea
Total
Aghbala 786 0 7,653 2,151 2,170 0 0 0 0 12,760
Beni Mellal 3,928 236 16,274 51,722 27,387 1,895 0 308 2,287 104,036
Bradia 262 12 0 1,905 2,478 0 0 0 0 4,657
Dar Ould Zidouh 0 50 29 17,671 2,419 0 0 308 704 21,181
El Ksiba 524 0 0 1,567 2,097 0 0 0 0 4,188
Fquih Ben Salah 87 335 26,214 11,432 7,096 0 0 0 0 45,165
Kasba Tadla 175 99 31,404 9,220 6,246 0 0 0 0 47,143
Ouled Ayad 87 0 880 22,619 7,404 0 0 0 0 30,990
Ouled M'barek 0 0 0 3,227 1,745 0 0 0 0 4,972
Ouled Yaich 262 0 4,809 3,442 792 0 0 0 0 9,304
Sebt Ouled Nemma 175 25 176 10,787 8,020 0 0 0 0 19,182
Sidi Jaber 0 0 0 2,489 1,041 0 0 0 0 3,530
Zaouiat Echeikh 1,309 0 5,630 9,373 5,337 0 0 284 0 21,933
Total 7,594 757 93,069 147,606 74,229 1,895 0 900 2,991 329,040
Total (%) 2.31 0.23 28.28 44.86 22.56 0.58 0.00 0.27 0.91 100.00
14
Table 11. Cost of hospitalization due to water-related diseases in the Beni-Mellal Province in USD
Parameter Typhoid Viral Hepatitis Acute GA Diarrhea Dysentery Total
Number of cases 87 61 3,174 10,917 38
Hospitalization days/case 12 5 4 3 3
Daily hospitalization cost 35.9 25.9 25.5 25.5 25.5
Total cost of hospitalization 37,441 7,911 323,593 834,779 2,906 1,206,630
Total (%) 3.10 0.66 26.82 69.18 0.24 100.00
Table 12. Cost of lost work days due to water-related diseases in the Oum Er Rbia Basin
Provinces Diseases Number of lost work
days
Parameter
Settat Safi El Jadida Khénifra Khouribga Beni Mellal
Total
No. of cases 2,275 - 7,805 1,276 406 3194 14,956 Diarrhea and
acute GE
3
Cost (USD) 56,184 - 481,938 78,763 25,093 78,895 720,873
No. of cases 8 - 79 - - - 87 Amoebic
dysentery
10
Cost (USD) 659 - 6,514 - - - 7,173
No. of cases 1 26 3 206 64 87 387 Typhoid 21
Cost (USD) 173 4,495 519 35,615 11,065 15,041 66,908
No. of cases 1 19 - 13 3 61 97 Viral Hepatitis 15
Cost (USD) 123 2,346 - 1,605 370 7,533 11,979
TOTAL (USD) 57,139 6,841 488,971 115,983 36,529 101,469 806,932

15
As such the total cost of illness due to water-related diseases in the Oum Er Rbia province amounted to 6.17 million USD.
4.3.2 Cost of pain and suffering (DALY)
For a total of 30,897 reported cases of diarrhea and acute gastroenteritis in the Oum Er Rbia basin,
and based on an average duration of 3 days per diarrhea case and a severity weight of 0.11 (Murray and Lopez, 1996), the total number of DALYs lost because of pain and discomfort resulting from diarrhea is estimated at 28. For a GDP of 1,679 USD/capita (World Bank, 2006), the estimated cost of
years lost due to disability caused by diarrhea is 47,012 USD (number of DALYs × per capita GDP).
DALY calculations were limited to diarrhea and acute gastro-enteritis cases since no severity weight has been reported in the literature for the other water-related diseases. Based on the above estimations, the yearly total cost of morbidity resulting from typhoid, viral
hepatitis, diarrhea, acute gastroenteritis, and amoebic dysentery amounted to 6.22 million USD (0.09 percent of the GDP in the Oum Er Rbia region for the year 2004) (Table 13). The major part of this cost is associated with health treatment (86 %), followed by time (13 %) and discomfort (0.8 %).
Table 13. Summary of estimated damage cost from morbidity associated with inadequate
water and wastewater management
Cost (million USD) Cost (%)
Cost of treatment 5.36 86.2
Cost of lost work days 0.81 13.0
Cost of years lost due to disability 0.05 0.8
Total morbidity cost (USD) 6.22 100
4.4 Benefits
Based on the valuation presented above, the total cost of water-related mortality and morbidity was
estimated to range between 52.4 million and 170.1 million USD/year, with an average of 111.27 million USD/year (0.69-2.25 percent of the GDP in the Oum Er Rbia Basin for the year 2004). IRAM développement estimated the percentage of the cost attributed to water pollution to be 60 percent, based on Valent et al. (2002) and Spandaro (2002). Accordingly, the annual benefits accrued from improved water supply and sanitation in the Oum Er Rbia basin are estimated to range between 31.4 and 102.1 million USD per year, constituting 0.42 to 1.35 percent of the GDP in the Oum Er Rbia Basin for the year 2004. Using a social discount rate of 4%, the present value of the flow of damage
costs associated with pollution over a time span of 16 years (till 2020) ranges between 366 million USD and 1,190 million USD with an average of 778 million USD.
5 PRIORITIZATION OF INVESTMENT OPTIONS
As part of the National Water Sanitation Plan, fifty-one investments are planned for the Oum Er Rbia basin, which are expected to directly benefit about two million inhabitants, not to mention visitors,
agricultural and fisheries activities (Annex A). The total cost of the planned investments is estimated at 300 million USD for the period 2003-2020, of which 45% is allocated for water treatment.
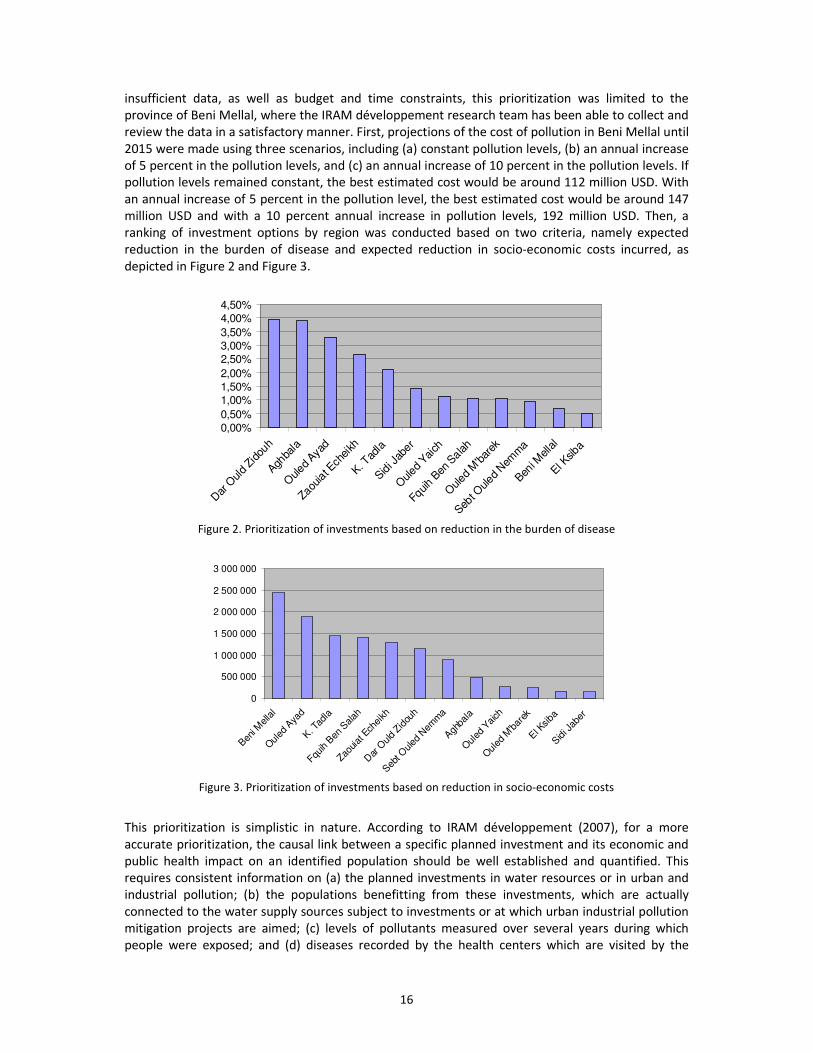
Given the results of the health valuation, IRAM développement (2007) attempted to prioritize investment options planned for the Oum Er Rbia basin. However, due to the fragmented and
16
insufficient data, as well as budget and time constraints, this prioritization was limited to the province of Beni Mellal, where the IRAM développement research team has been able to collect and review the data in a satisfactory manner. First, projections of the cost of pollution in Beni Mellal until
2015 were made using three scenarios, including (a) constant pollution levels, (b) an annual increase of 5 percent in the pollution levels, and (c) an annual increase of 10 percent in the pollution levels. If pollution levels remained constant, the best estimated cost would be around 112 million USD. With
an annual increase of 5 percent in the pollution level, the best estimated cost would be around 147 million USD and with a 10 percent annual increase in pollution levels, 192 million USD. Then, a ranking of investment options by region was conducted based on two criteria, namely expected reduction in the burden of disease and expected reduction in socio-economic costs incurred, as
depicted in Figure 2 and Figure 3.
0,00%
0,50%
1,00%
1,50%
2,00%
2,50%
3,00%
3,50%
4,00%
4,50%
Dar
Oul
d Zid
ouh
Aghba
la
Ouled
Ayad
Zaouiat E
chei
kh
K. Tad
la
Sidi J
aber
Ouled
Yai
ch
Fquih
Ben S
alah
Ouled
M'bar
ek
Sebt O
uled
Nem
ma
Beni M
ella
l
El Ksib
a
Figure 2. Prioritization of investments based on reduction in the burden of disease
0
500 000
1 000 000
1 500 000
2 000 000
2 500 000
3 000 000
Beni M
ella
l
Oul
ed A
yad
K. T
adla
Fquih B
en S
alah
Zaouiat
Ech
eikh
Dar
Ould
Zidou
h
Seb
t Ouled
Nem
ma
Agh
bala
Oul
ed Y
aich
Oul
ed M
'bar
ek
El K
siba
Sidi J
aber
Figure 3. Prioritization of investments based on reduction in socio-economic costs
This prioritization is simplistic in nature. According to IRAM développement (2007), for a more
accurate prioritization, the causal link between a specific planned investment and its economic and public health impact on an identified population should be well established and quantified. This requires consistent information on (a) the planned investments in water resources or in urban and industrial pollution; (b) the populations benefitting from these investments, which are actually
connected to the water supply sources subject to investments or at which urban industrial pollution mitigation projects are aimed; (c) levels of pollutants measured over several years during which people were exposed; and (d) diseases recorded by the health centers which are visited by the

17
exposed populations. However, the data obtained by the IRAM développement were fragmentary and insufficient to allow spatial analysis and the planned calculations.
6 CONCLUSION AND LIMITATIONS
Inadequate water supply and sanitation in the Oum Er Rbia basin is imposing significant socio-economic costs on the population in the area in terms of water-related mortality and morbidity.
These costs were estimated to range between 52.4 million and 170.1 million USD/year, with an average of about 111 million USD/year (0.69-2.25 percent of the GDP in the Oum Er Rbia Basin for the year 2004). Accordingly, improving the quality of water supply and sanitation is expected to result in considerable economic benefits, estimated to range between 31 and 102 million USD per
year, constituting 0.42 to 1.35 percent of the GDP in the Oum Er Rbia Basin for the year 2004. The present value of the flow of damage costs associated with pollution over a time span of 16 years (till 2020) ranges between 366 million USD and 1,190 million USD with an average of 778 million USD,
which exceeds by far the estimated cost of the planned investment in the Oum Er Rbia basin of 300 million USD. Hence, despite the inadequacy of the prioritization process and the fact that the true relation between the degree of improvement in water supply and sanitation and the expected reduction in disease prevalence and mortality still needs to be ascertained, the present figures are
sufficient to prompt decision-makers to continue investing in implementing the planned National Water Sanitation Plan.
Finally, the estimated figures reflecting the damage cost of sub-standard water quality, inadequate sanitation facilities and sanitary practices, and inadequate personal, food and domestic hygiene, should be regarded as indicative numbers and minimum estimates for the following reasons:
� The causes of morbidity and mortality cases in Morocco are not recorded as systematically as
required for this study. � Health impacts due to chemical pollution of water resources cannot be accounted for due to the
difficulty in linking them to exposure as they are long term in nature. � The exposure approach does not account for all routes, such as exposure to recreational water
or sewage polluted fish/ food. � Data on the number of morbidity cases is limited to the hospitalized ones. Many patients may
visit only dispensaries and may not visit medical facilities at all, especially for mild diarrhea cases. They do simply buy medicaments from pharmacies, without consulting a hospital, a dispensary or a private clinic.
� Water pollution and possible contamination of municipal water in the distribution system has also a cost to society revealed in terms of averting expenditures such as the purchase of bottled water or the incremental cost paid to transporting cleaner water from other sources. However, this issue was not investigated.
BIBLIOGRAPHY
Butterworth, J. and Soussan, J. 2001. Water Supply and Sanitation and Integrated Water Resources
Management: why seek better integration? Prepared for WHIRL project workshop on ‘Water Supply &
Sanitation and Watershed Development: positive and negative interactions’, Andhra Pradesh, India, May
2001.
CIA World Factbook, 2008. Online. Available: https://www.cia.gov/library/publications/the-world-
factbook/geos/mo.html
18
Esrey, S.A., Potash, J.B., Roberst, L., and Shiff, C., 1991. “Effects of improved water supply and sanitation on
ascariasis, diarrhea, dracunculiasis, hookworm infection, schistosomiasis and trachoma”, Bulletin of the
World Health Organization, 69, No 5, pp 609-621.
Fewtrell, L., Prüss-Üstün, A., Bos, R., Gore, F., and Bartram, J. 2007. Water, sanitation and hygiene: Quantifying
the health impact at national and local levels in countries with incomplete water supply and sanitation
coverage. Environmental Burden of Disease Series, No. 15. World Health Organization, Geneva.
Hunter, P. R. (1998). Waterborne diseases, epidemiology and ecology. Chichester, UK., Wiley & Sons Ltd.
INECO Morocco, 2008. Online. Available: http://environ.chemeng.ntua.gr/ineco/Default.aspx?t=337
IRAM développement (Institut de Recherches et d’Applications des Méthodes de Développements), 2007.
Impact sanitaire et économique de la réduction de la pollution des eaux souterraines et de surface dans le
bassin de l’Oum-Er-Rbia au Maroc. Final Report. June 2007.
IRC 2007. Sanitation for all. International Water and Sanitation Center. Thematic Overview Paper 20 by Bruijne
G., Geurts M., and Appleton B.
Muller, R. and Morera, P. (1994), Helminthoses In: Health and disease in developing countries, Lankinen, K.S.,
Berström, S., Mäkelä, P.H., and Peltomaa, M., (Eds.). London, Macmillan Press, 1994.
Murray, J., and A. Lopez. 1996. The global burden of disease: a comprehensive assessment of mortality and
disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Harvard University Press.
Prüss, A,, Kay, D., Fewtrell, L., and Bartram, J. 2002. Estimating the burden of disease from water, sanitation
and hygiene at a global level. Environmental Health Perspectives, 110 (5), 538-542.
Valent F. et al., 2004. Environmental Burden of Disease Series n°8. Burden of disease attributable to selected
environmental factors, World Health Organization.
Spadaro J., 2002. A tool for assessing the Environmental Impacts and Damage Costs to Human Health,
International Atomic Energy Agency, October 2002.
WHO (World Health Organization), 1996. The World Health Report 1996: Fighting Disease, Fostering
Development. WHO, Geneva.
WHO (World Health Organization), 1998. Division of Control of Tropical Disease homepage,
http://www.who.ch/ctd/.
WHO (World Health Organization), 2004a. Water, Sanitation and Hygiene Links to Health: Facts and Figures.
Online. Available:
http://www.who.int/water_sanitation_health/en/factsfigures04.pdf
Wikipedia, 2008. http://en.wikipedia.org/wiki/Oum_Er-Rbia_River
World Bank, 2006. Morocco: Integrated Resource Protection Project. Concept Stage. Project Information
Document. Report No.: AB2227. Middle East and North Africa Region, The World Bank.
World Bank, 2003. Cost Assessment of Environmental Degradation in the Kingdom of Morocco. Report No.
25992-MOR. Water, Environment, Social and Rural Development Department, Middle East and North
Africa Region, The World Bank.
World Bank, 2006. World Development Indicators. Online. Available:
http://devdata.worldbank.org/wdi2006/contents/Section2.htm

19
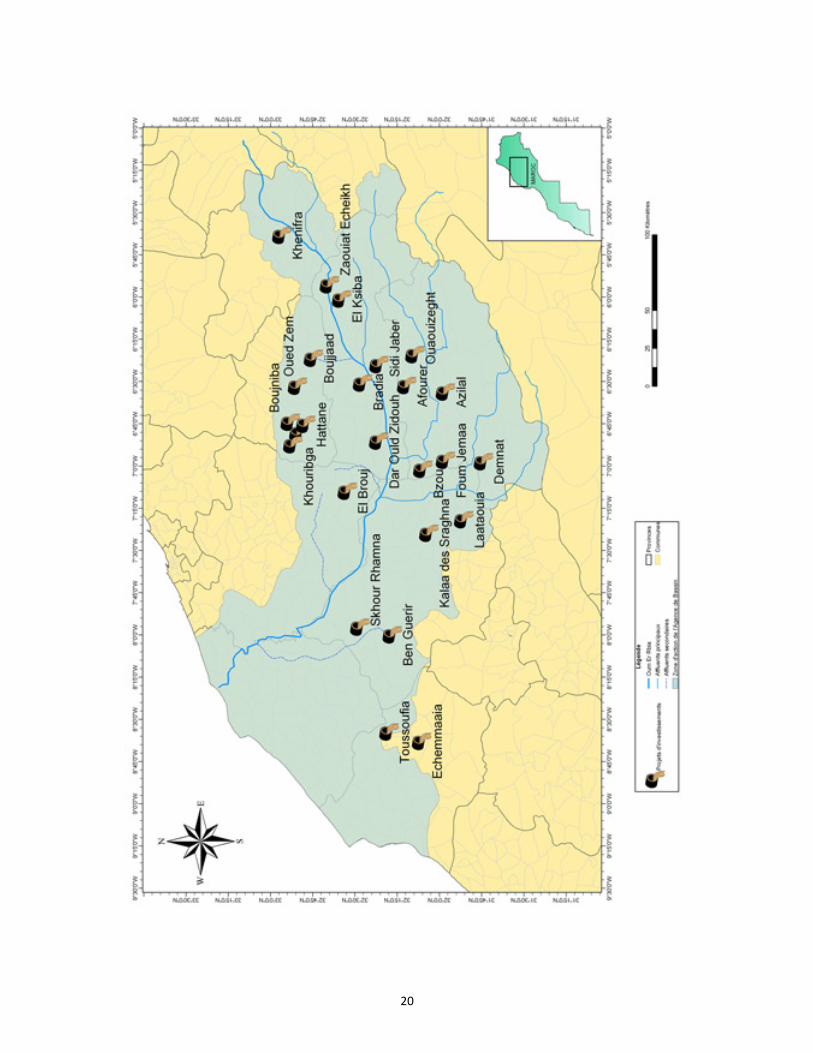
ANNEX A
Location of Planned Sanitation Investments in the Oum Er Rbia Basin
20