overview of guidelines in the management of hypertension
TRANSCRIPT

An Overview of Guidelines in the Management of Hypertension
Dr. Jayaprakash S. AppajigolConsultant Physician, KLE’s Dr. Prabhakar Kore Hospital and
MRC.Associate professor of Medicine,
JNMC, Belgaum

Objectives
•Understand and critic JNC 8 guidelines
•Use clinical scenarios to discuss and understand some of these recommendations
•Compare JNC-8 with other hypertension guidelines
• SPRINT trial

JNC-7 Classification of HTN
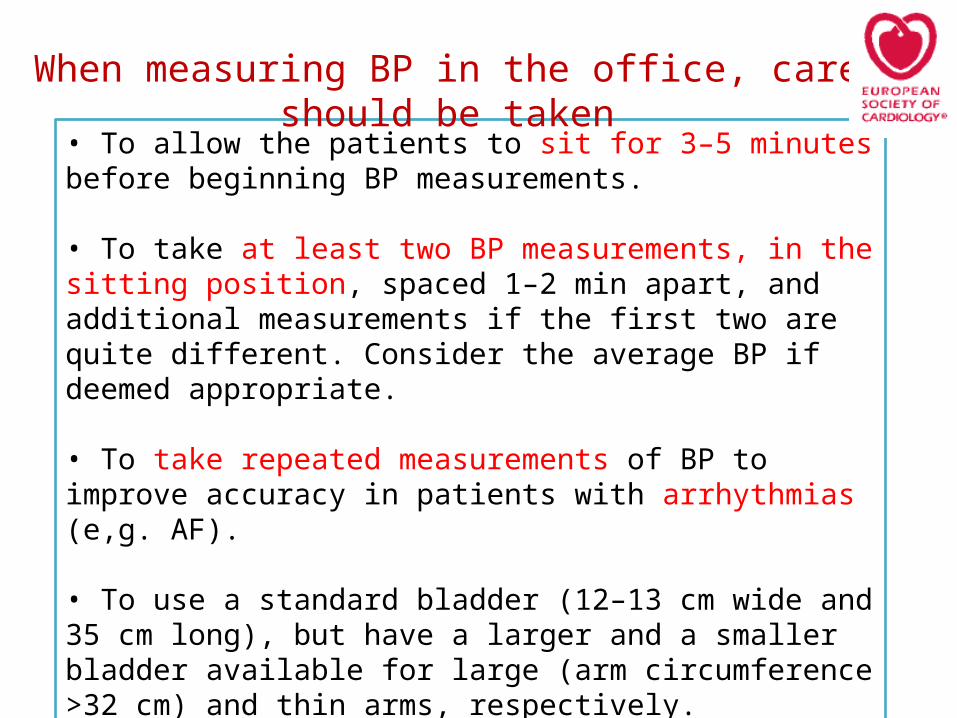
• To allow the patients to sit for 3–5 minutes before beginning BP measurements.
• To take at least two BP measurements, in the sitting position, spaced 1–2 min apart, and additional measurements if the first two are quite different. Consider the average BP if deemed appropriate.
• To take repeated measurements of BP to improve accuracy in patients with arrhythmias (e,g. AF).
• To use a standard bladder (12–13 cm wide and 35 cm long), but have a larger and a smaller bladder available for large (arm circumference >32 cm) and thin arms, respectively.
• To have the cuff at the heart level, whatever the position of the patient.
When measuring BP in the office, care should be taken

• When adopting the auscultatory method, use phase I and V (disappearance) Korotkoff sounds to identify systolic and diastolic BP, respectively.
• To measure BP in both arms at first visit to detect possible differences. In this instance, take the arm with higher value as the reference.
• To measure at the first visit, BP 1 and 3 min after assumption of the standing position in elderly subjects, diabetic patients, and in other conditions in which orthostatic hypotension may be frequent or suspected.
When measuring BP in the office, care should be taken

2003 2014
JNC-7 JNC-8
2005 2007 2009 2011
REIN-2
ESH/ESC
AHA
ACCOMPLISH
ONTARGET
HYVET ACCORD-BP
NICE
ACCF/AHA
ESH/ESC
ASH/ISH
CAMELOT
ALTITUDE
Growing Evidence
SPRINT study2015

The panel members appointed to JNC 8 were selected from more than 400 nominees based on expertise in hypertension (n = 14), primary care (n = 6), including geriatrics (n = 2), cardiology (n = 2), nephrology (n = 3), nursing (n = 1), pharmacology (n = 2), clinical trials (n = 6), evidence-based medicine (n = 3), epidemiology (n = 1), informatics (n = 4), and the development and implementation of clinical guidelines in systems of care (n = 4).
Who is the JNC-8

2014 JAMA HTN GuidelinesClinical Questions (JNC-8)


Case Scenario-1
A 67 year male is on regular treatment for HTN.
He does not have any complaints.
His average blood pressure in the last week is 136/88 mmHg ( Verified by repeated check ups).
What to do for him?

HTN in the Elderly
• Comparison of different guidelines
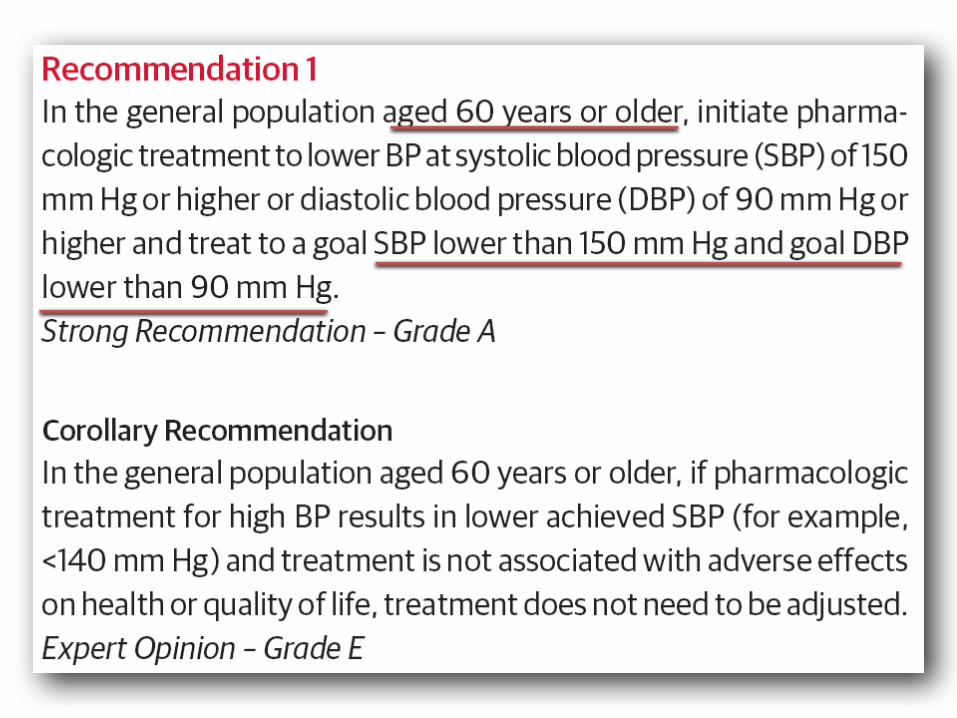
– 2014 JAMA: > 60 y/o = < 150/90
– ESH/ESC: >80 y/o or elderly < 80 y/o = < 150/90
– CHEP: >80 y/o = < 150/90
– NICE: > 80 y/o = < 150/90
– ASH/ISH: > 80 y/o = < 150/90

Case Scenario-1
A 67 year male is on regular treatment for HTN.
He does not have any complaints.
His average blood pressure in the last week is 136/88 mmHg ( Verified by repeated check ups).
What to do for him?
Continue the same medications
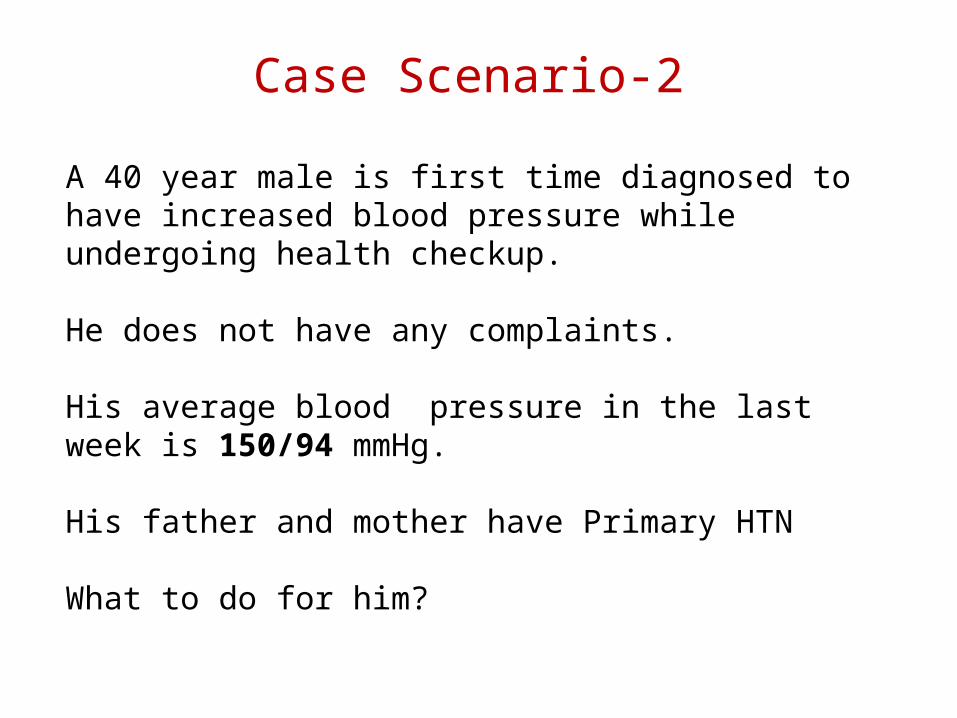
Case Scenario-2
A 40 year male is first time diagnosed to have increased blood pressure while undergoing health checkup.
He does not have any complaints.
His average blood pressure in the last week is 150/94 mmHg.
His father and mother have Primary HTN
What to do for him?


Case Scenario-2
A 40 year male is first time diagnosed to have increased blood pressure while undergoing health checkup.
He does not have any complaints.
His average blood pressure in the last week is 150/94 mmHg.
His father and mother have Primary HTN
What to do for him?
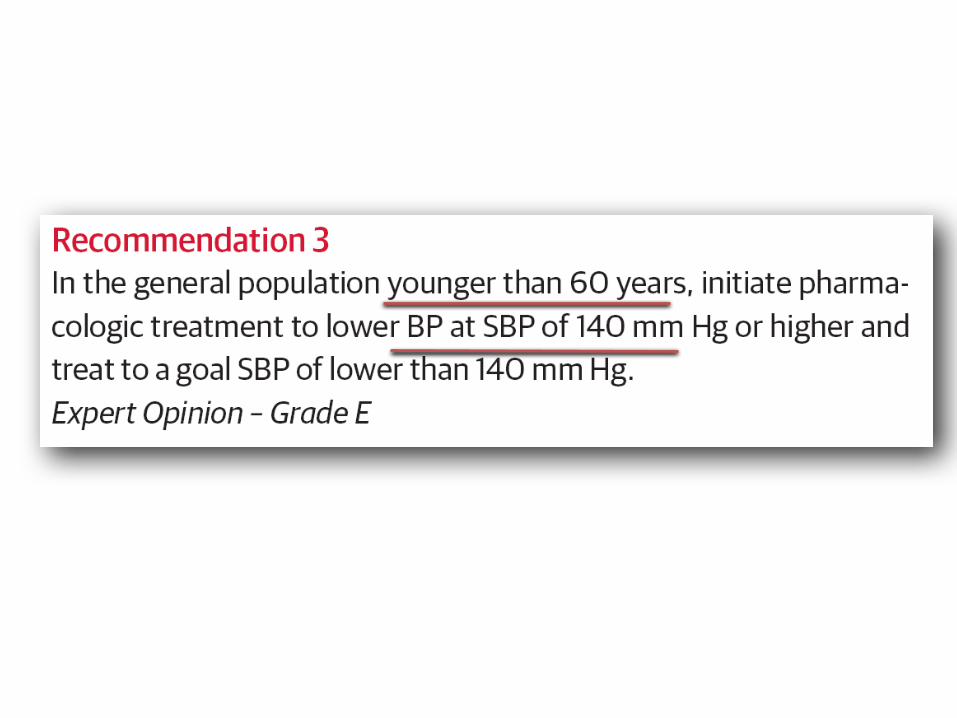
His DBP should be brought to <90 mm HgSBP should be brought <140 mm Hg

A 43 y/o woman with HTN returns for a follow up visit of her BP. On exam today, her BP is 138/88 (and verified on repeat). Her serum creatinine is 1.6 mg/dL, and her RUA reveals > 500 mg/dL of proteinuria. She is on Losartan 100 mg/day.
A. Change to ACE inhibitor like Ramipril
B. Add thiazide diuretic
C. Increase her ARB dose
D. Continue Same
Case Scenario-3

Comparison:– ESH/ESC: no proteinuria = < 140/90 with proteinuria = < 130/90-- CHEP: < 140/90 for all-- KDIGO: no proteinuria = < 140/90 with proteinuria = < 130/80

A 43 y/o woman with HTN returns for a follow up visit of her BP. On exam today, her BP is 138/88 (and verified on repeat). Her serum creatinine is 1.6 mg/dL, and her RUA reveals > 500 mg/dL of proteinuria. She is on Losartan 100 mg/day.
A. Change to ACE inhibitor like Ramipril
B. Add thiazide diuretic
C. Increase her ARB dose
D. Continue Same
Case Scenario-3
KDIGO, ESH/ESC
JNC-8

A 43 y/o Type 2 DM and HTN, presents for follow up. His medication regimen: Metformin 500mg BID, Lis/HCT 20/25mg daily, Amlodipine 5mg, and ASA 81mg.
On exam, his BP = 138/88 mmHg.On lab review, his CBC, BMP, and RUA are normal. His A1c=8.3%.In addition to adjusting his Type 2 DM medication regimen, what additional changes would you make?
A. NoneB. Increase Amlodipine to 10mgC. Increase Lisinopril to 40mgD. Add an additional BP agent, such as a beta-blocker
Case Scenario-4

A 43 y/o Type 2 DM and HTN, presents for follow up. His medication regimen: Metformin 500mg BID, Lis/HCT 20/25mg daily, Amlodipine 5mg, and ASA 81mg.
On exam, his BP = 138/88 mmHg.On lab review, his CBC, BMP, and RUA are normal. His A1c=8.3%.In addition to adjusting his Type 2 DM medication regimen, what additional changes would you make?
A. NoneB. Increase Amlodipine to 10mgC. Increase Lisinopril to 40mgD. Add an additional BP agent, such as a beta-blocker
Case Scenario-4
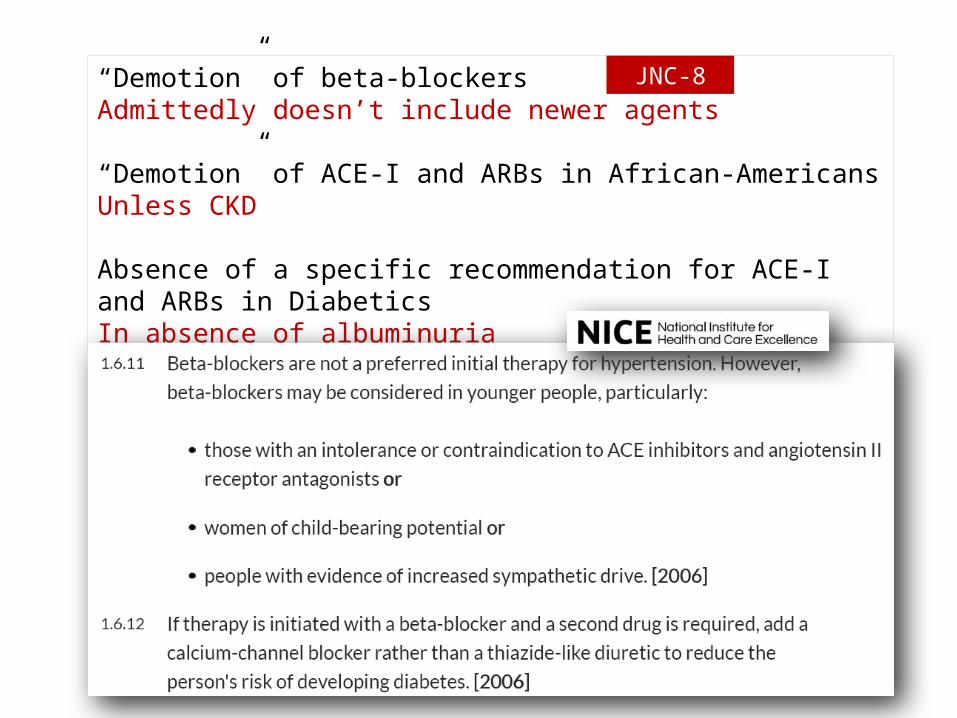
“Demotion” of beta-blockersAdmittedly doesn’t include newer agents
“Demotion” of ACE-I and ARBs in African-AmericansUnless CKD
Absence of a specific recommendation for ACE-I and ARBs in DiabeticsIn absence of albuminuria
JNC-8




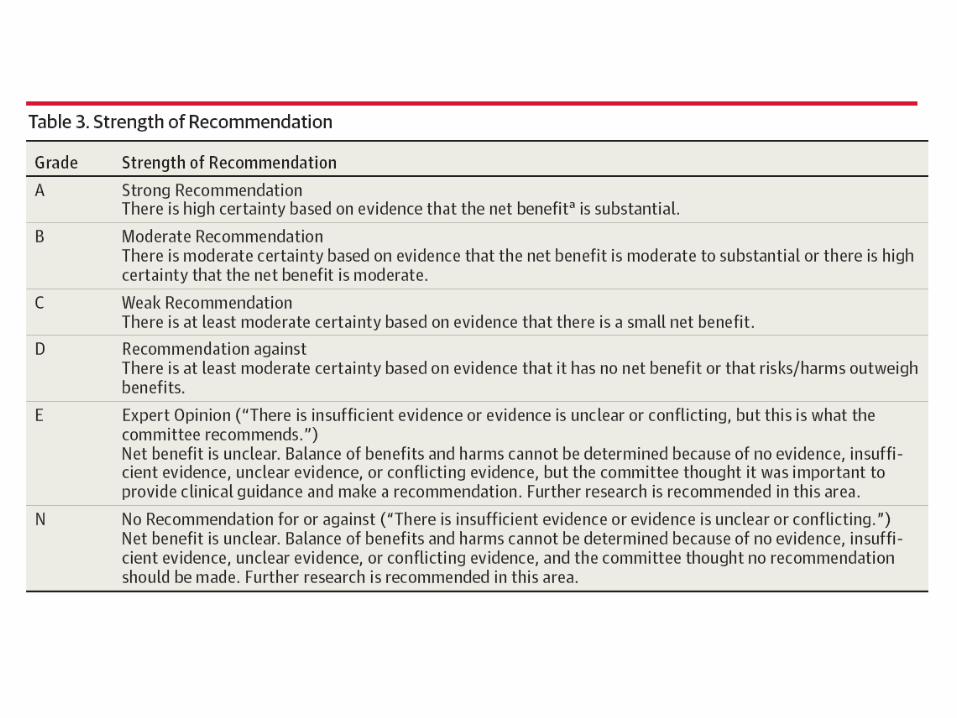
Recommendation Level of Evidence
1. General population > 60 y/o, initiate medications and treat to BP goal of 150/90 mmHg.
A
2. General population < 60 y/o, initiate medications and treat to DBP goal of 90 mmHg.
A/E
3. General population < 60 y/o, initiate medications and treat to SBP goal of 140 mmHg.
E
4. In population > 18 y/o with CKD, initiate medications and treat to BP goal of 140/90 mmHg.
E
5. In population > 18 y/o with DM, initiate medication and treat to BP goal of 140/90 mmHg.
E
2014 JAMA Hypertension Guideline Recommendations

Recommendation Level of Evidence
6. In nonblack population (including DM), initial anti-hypertensive therapy should consist of thiazide diuretic, CCB, ACE-I or ARB.
B
7. In general black population (including DM), initial anti-hypertensive therapy should include thiazide diuretic or CCB.
C
8. In population with CKD, initial (or add-on) anti-hypertensive therapy should include ACE-I or ARB.
B
9. Main objective of therapy is to attain and maintain a BP goal and can be accomplished in one of two ways if not accomplished with initial therapy: 1. Increase dose of initial agent. 2. Add a second or, eventually, third agent from above list.ACE-I and ARB should not be used in combination. Other agents may be necessary if goal BP cannot be attained or maintained from above list.
E
2014 JAMA Hypertension Guideline Recommendations

Remarks JNC-8
Five of 9 recommendations
are “E” No recommendation to decrease medicines in well-controlled elderlyOnly deals with
one risk factor—BP

9361 peopleWith Cardiovascular Risks
SBP>130 mm HgNon-DM
Systolic Blood Pressure Intervention TrialNEJM Nov 9,2015
Intensive SBP control <120 mm Hg
Standard SBP control<140 mm Hg
121.4 mm Hg 136.2 mm Hg
After one year of study
Reduced Cardiovascular Mortality and All cause mortality
Increased rates of Syncope, Hypotension, electrolyte imbalances ,AKI
Conclusions
The risk of CVD beginning at 115/75 mmHg and
doubles with each increment of 20/10 mmHg
Individuals who are normotensive at age 55 have a
90 percent lifetime risk for developing hypertension
Diagnosing and starting treatment is a challenge at community level because many of them are asymptomatic
Diagnose if >140/90Treat to <140/90

The More We Learn, the Less We Know
Thank youDiagnose if >=140/90Treat to <140/90