ovarian tumor in children and adolscent
TRANSCRIPT
Dr.Yassin AlsalehCase presentation


Case scenario• Lyan is 4 year old girl previously healthy presented with :• progressive breast enlargement and pubic hair growth for 5
months. • One day prior to admission patient developed vaginal bleeding• On examination :• her weight : 16.1 kg (75th) percentile. • The height 104 cm (75th) ,• Breast tanner stage IV , pubic hair tanner III . • No palpable mass in abdominal exam ,local genital exam within
normal limit.• No café-au-lait spots, or bony deformity .• CVS.CHEST and CNS examination was within normal limits.
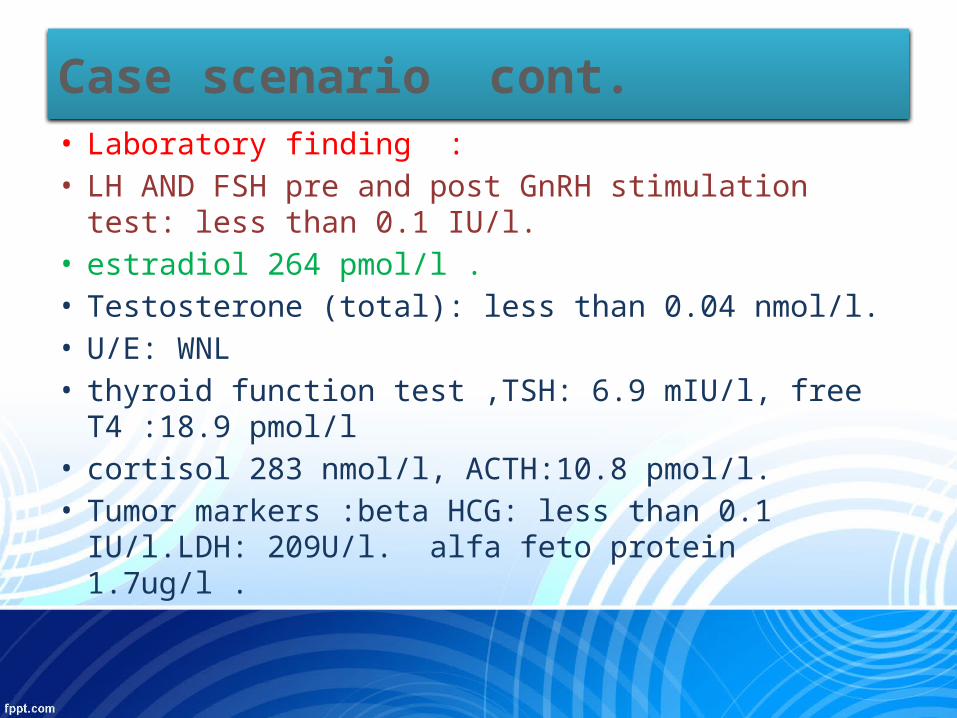
• Laboratory finding :• LH AND FSH pre and post GnRH stimulation test: less
than 0.1 IU/l. • estradiol 264 pmol/l .• Testosterone (total): less than 0.04 nmol/l. • U/E: WNL • thyroid function test ,TSH: 6.9 mIU/l, free T4 :18.9
pmol/l • cortisol 283 nmol/l, ACTH:10.8 pmol/l. • Tumor markers :beta HCG: less than 0.1 IU/l.LDH:
209U/l. alfa feto protein 1.7ug/l .
Case scenario cont.

• Bone age: was advanced .• Ultrasonography of pelvis showed: predominaently solid mass
lesion in the right adnexal region most likely arising from the right ovary measuring 5.6 x 3.8 x 6.0 cm volume approximately 66 ml. Uterus enlarged for the age of the patient with endometrial thickening.
• CT abdomen and pelvis with contrast showed: smoothly marginated solid soft tissue mass involving the right ovary ,shows contrast enhancement and tumor vessels. mass is displacing the surrounding bowel loops, abutting the urinary bladder, anterior abdominal wall and the psoas muscle. There was no evidence of free fluid or lymphadenopathy in abdomen or pelvis.
Case scenario cont.

introduction
• Ovarian neoplasms account for approximately 1 % of all tumors in children and adolescents.
• Most ovarian neoplasms are benign.• However, it is important to establish an early
diagnosis to reduce the risk of ovarian torsion and to improve the prognosis for the malignant lesions.
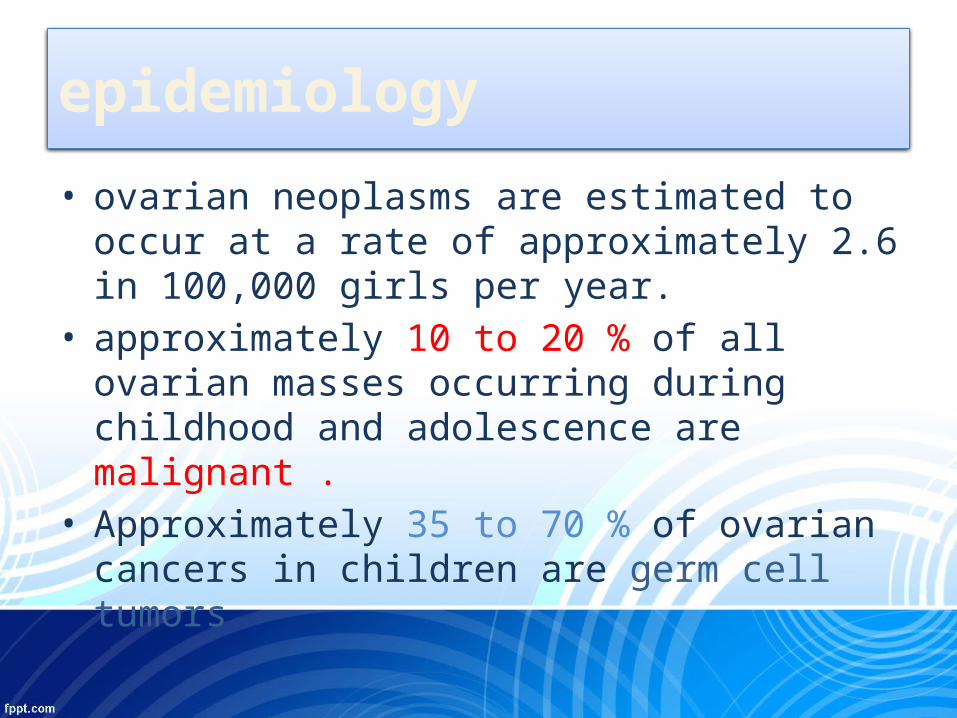
• ovarian neoplasms are estimated to occur at a rate of approximately 2.6 in 100,000 girls per year.
• approximately 10 to 20 % of all ovarian masses occurring during childhood and adolescence are malignant .
• Approximately 35 to 70 % of ovarian cancers in children are germ cell tumors
epidemiology

• In girls younger than nine years of age, approximately 80 percent of ovarian neoplasms are malignant.
• Epithelial neoplasms and sex cord-stromal tumor are rare in the prepubertal age group.
epidemiology
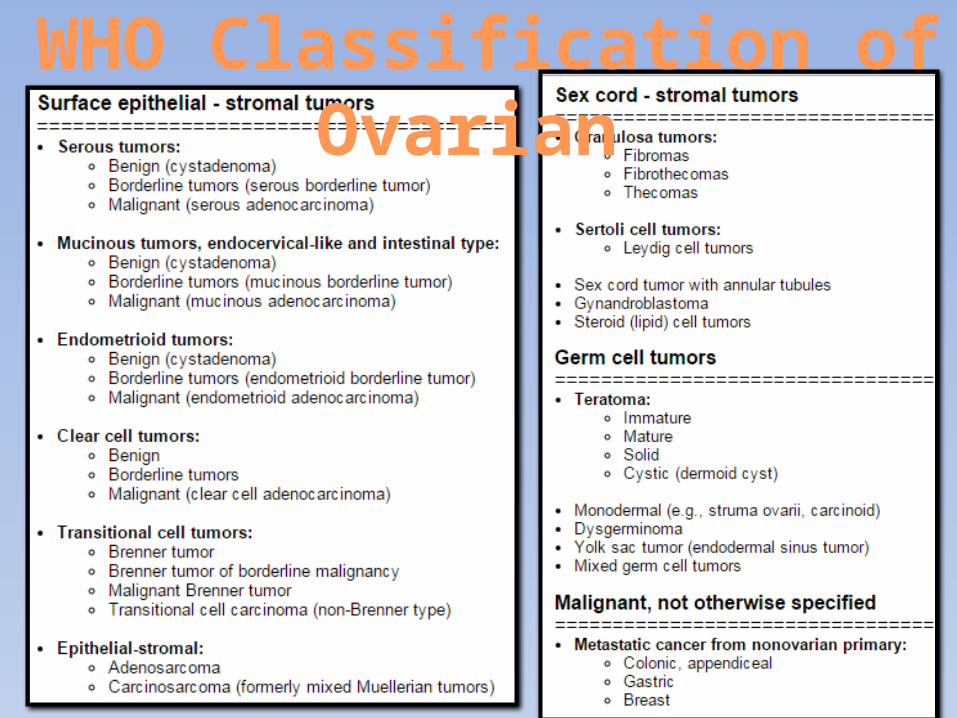
WHO Classification of Ovarian
presentation
• abdominal pain .• abdominal distension,• palpable abdominal mass.• nausea, and vomiting. • Pseudoprecocity and hirsutisim.• vaginal bleeding• difficulty in urination or defecation• or they may be asymptomatic.
• Granulosa cell and germ cell tumors of the ovary can secrete both androgens and estradiol.
• granulosa cell tumors being the most frequent ovarian tumor that induces precocious puberty.
presentation

• Sex hormones : normal or high.• Gonadotropins : normal or suppresed.
laboratory
Tumor markers
• Tumor markers can be helpful in making a diagnosis and following the clinical response to treatment .
• Alpha-fetoprotein (AFP) • It is produced by endodermal sinus tumors, mixed
germ cell tumors, and immature teratomas.• Lactate dehydrogenase (LDH) • is elevated with dysgerminomas• ●CA-125 is a marker for epithelial ovarian cancer that
is highly sensitive, but not very specific,

• Human chorionic gonadotropin (hCG) • is produced by trophoblastic cells and thus will be
elevated with choriocarcinoma, and embryonal ovarian carcinomas
• Carcinoembryonic antigen (CEA) • can be produced by epithelial or germ cell tumors• Inhibin and mullerian inhibiting substance (MIS)• are elevated in children with granulosa-theca cell
tumors
Tumor markers

IMAGING• US: • to determine the overall size of the mass.• to identify whether it is simple, complex, solid,
bilateral, or associated with free fluid. • The pattern of blood supply .
TREATMENT
• a unilateral salpingo- oophorectomy/ oophorectomy.• It is preferable to subject the patient to a second
procedure after the final pathology specimens are reviewed than to perform an unnecessary ablative procedure.
• Chemotherapy.

juvenile granulosa cell tumor
• Also called Granulosa-theca cell tumors• one of the rare sex cord stromal tumors of the ovary.
• Juvenile granulosa cell tumors makes up less than 5% of ovarian tumors in childhood and adolescence.
• There are two types: 1-adult granulosa cell tumor(95% of cases) 2-juvenile granulosa cell tumor(5% of cases)
• only 1 % of all cases of sexual precocity in prepubertal girls are due to granulosa and theca cell tumors

Pathology /pathogenesis
• tumors composed of granulosa cells, theca cells, and fibroblasts in varying degrees and combinations.
• There are a group of cells with ability to secret steroid hormones.
• The pathogenesis of ovarian GCT is still unknown• juvenile granulosa cell tumors are usually benign
with low malignant potential.

presentation• The most common presentation of these tumors in
children is peripheral precocious puberty (70-80 %). • breast development are the initial changes,• Pubic hair development.• increased linear growth.• vaginal bleeding .• Abdominal pain• Hirsutisim and clitoral enlargement.• Ascities• CPP.
imaging
• bone age usually advanced .• On CT and sonography:• they most typically appear as large, multilocular
masses• with either thin septations or thick.• solid components ,predominantly solid or large
multicystic mass• Tumors are capsulated. • Extra capsular invasion is rare.
• Tumor staging is by International Federation of Gynecology and Obstetrics (FIGO) system.
• Most tumors are unilateral and are FIGO stage 1 with sporadic origin.
Staging

Staging

treatment
• Because most of these lesions are benign, ovarian-preserving operations should be performed whenever feasible
• Ophorectomy is procedure of choice.

prognosis
• The prognosis is excellent when JGCT is limited to the ovaries.
• early diagnosis of JGCT is important, as adjuvant treatment may not be necessary if the tumor is localized in ovaries
• Most tumors at FIGO stage IA have a favorable prognosis, whereas those at higher stages have a less favorable outcome
• Five-year survival rates are 90-95% for FIGO stage I tumors and 25-50% for advanced stages.

Home messege
• Ovarian masses, although rare in children, must be included in the differential diagnosis of all girls who present with precocious puberty.
• A solid ovarian mass in childhood is always considered malignant until proven otherwise by histological examination.
references1. Merras-Salmio L, Vettenranta K, Mottonen M, Heikinheimo M. Ovarian
granulosa cell tumors in childhood. Pediatr Hematol Oncol. 2002;19(3):145–56.
2. Cass DL, Hawkins E, Brandt ML, et al. Surgery for ovarian masses in infants, children, and adolescents: 102 consecutive patients treated in a 15-year period. J Pediatr Surg. 2001; 36(5): 693-9.
3. Eun Young Ki, Seung Won Byun, Yoon Jin Choi, et al. Clinicopathologic Review of Ovarian Masses in Korean Premenarchal Girls. International Journal of Medical Sciences2013; 10(8):1061-1067.
4. Fink D, Kubik-Huch RA, Wildermuth S. Juvenile granulosa cell tumor. Abdom Imaging.2001;26(5):550–2.
5. Kdous M, Hachica R, Gamoudi A. Early isosexual precocious pseudopuberty revealing a juvenile granulosa cell tumor in a six-year-old girl. Gynecol Obstet Fertile. 2004;32(4):311–4.

6. Shruti Dogra, Yogesh Kr Yadav, Uma Sharma, Juvenile granulosa cell tumor with an unusual immunoprofile, presenting as precocious puberty. South Asian J Cancer. 2013 Jul-Sep; 2(3): 150
7. Rokitansky CV. Über Abnormalitäten des Corpus Luteum. Wien Med Ztc. 1859;4:253–4
8-Nisha Nigil Haroon, Gaurav Agarwal, Rakesh Pandey, Preeti Dabadghao .Juvenile granulosa cell tumor presenting as isosexual precocious puberty: A case report and review of literature Indian J Endocrinol Metab. 2013 Jan-Feb; 17(1): 157–159.
9. Mitrović K, Zdravković D, Milenković T, Sedlecki K, Stanković Z.Ovarian cysts and tumors as the cause of isosexual pseudoprecocious puberty]. Srp Arh Celok Lek. 2006 Jul-Aug;134(7-8):305-9.
10. Lee CT, Tung YC, Tsai WY. Etiology and clinical features of isosexual precocious puberty in Taiwanese girls: twenty-three years' experience in National Taiwan University Hospital. J Pediatr Endocrinol Metab. 2009 Oct;22(10):947-53.
references

11. Mahin H, Mohammad H, Masoud N,Parvin M, ,Mehdi Salek. Granulosa cell tumor in a six-year-old girl presented as precocious puberty. J Res Med Sci. 2010 Jul-Aug; 15(4): 240–242.
12. Brito VN, Latronico AC, Arnhold IJ, Mendonça BB. Update on the etiology, diagnosis and therapeutic management of sexual precocity. Arq Bras Endocrinol Metabol. 2008 Feb;52(1):18-31.
13. Kalfa N, Méduri G, Philibert P, Patte C, Unusual virilization in girls with juvenile granulosa cell tumors of the ovary is related to intratumoral aromatase deficiency.Horm Res Paediatr. 2010;74(2):83-91.. Epub 2010 Apr 15 .
14. Nomelini RS, Micheletti AM, Adad SJ, Murta EF. Androgenic juvenile granulosa cell tumor of the ovary with cystic presentation: a case report. Eur J Gynaecol Oncol. 2007;28(3):236-8.
15. Plantaz D, Flamant F, Vassal G, Chappuis JP, Baranzelli MC, Bouffet E, Dyon JF, [Granulosa cell tumors of the ovary in children and adolescents. Multicenter retrospective study in 40 patients aged 7 months to 22 years]. Arch Fr Pediatr. 1992 Nov;49(9):793-8.
references

16. Valeria Calcaterra, Ghassan Nakib, Gloria Pelizzo, Barbara Rundo,Central Precocious Puberty and Granulosa Cell Ovarian Tumor in An 8-Year Old Female .Pediatr Rep. 2013 Jul 29; 5(3): e13.
17. Cartault A, Caula-Legriel S, Baunin C, Le Mandat A, Lemasson F, Galinier P, Pienkowski C. Ovarian masses in adolescent girls. Endocr Dev. 2012;22:194-207..
18. Oltmann SC, Garcia N, Barber R, Huang R, Hicks B, Fischer A. Can we preoperatively risk stratify ovarian masses for malignancy? J Pediatr Surg. 2010 Jan;45(1):130-4.
19. Spinelli C1, Pucci V, Buti I, Liserre J, Messineo A, Bianco F, Ugolini C. The role of tumor markers in the surgical approach of ovarian masses in pediatric age: a 10-year study and a literature review. Ann Surg Oncol. 2012 Jun;19(6):1766-73
references

20. Al Jama FE1, Al Ghamdi AA, Gasim T, Al Dakhiel SA, Rahman J, Rahman MS. Ovarian tumors in children and adolescents--a clinical study of 52 patients in a university hospital. J Pediatr Adolesc Gynecol. 2011 Feb;24(1):25-8.
21. Azin Ashnagar, Samin Alavi, , Yalda Nilipour, Roxana Azma, and Farahnaz Falahati .Massive Ascites as the Only Sign of Ovarian Juvenile Granulosa Cell Tumor in an Adolescent: A Case Report and a Review of the Literature. Case Rep Oncol Med. 2013; 2013: 386725.
references
