outline epidemiology presentation investigations optimal management
TRANSCRIPT

Outline
• Epidemiology
• Presentation
• Investigations
• Optimal management

Tuberculosis notifications by site of disease (pulmonary/non-pulmonary), England and Wales, 1982-
2009
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
TB - Epidemiology
• Rising prevalence nationally and locally
• Traditionally mostly pulmonary TB– 60%– 40% extra-pulmonary TB
• Increasing proportion of EPTB (50%)
• 10% of EPTB are joint TB

Joint TB - presentation
• Presentation is often insidious and atypical
• Can be sub-acute and therefore there can be a delay in diagnosis
• Painful joints may precede systemic symptoms by several weeks
• Sometimes is the tip of the iceberg of a multi-focal TB
Joint TB - presentation
• Early– Usually a single joint– Painful– No swelling or deformity
• Later joints may become warm and swollen• Sometimes they have a fever• Look for other symptoms eg cough
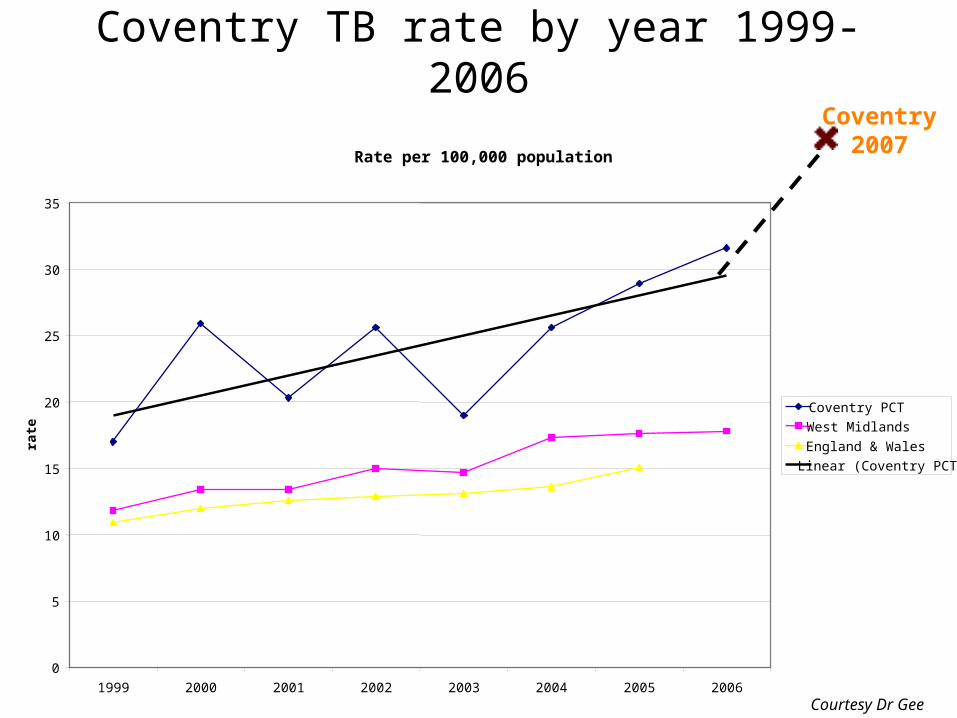
Coventry TB rate by year 1999-2006
Rate per 100,000 population
0
5
10
15
20
25
30
35
1999 2000 2001 2002 2003 2004 2005 2006
rate
Coventry PCT
West Midlands
England & Wales
Linear (Coventry PCT)
Coventry 2007
Courtesy Dr Gee
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Figure 4. Tuberculosis case reports and rates by age group and place of birth, UK, 2008
Tuberculosis case reports and rates by place of birth and ethnic group, UK, 2008
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
World health organisation

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Three-year average tuberculosis case rates by primary care organisation, UK, 2006-2008

Joint TB -presentation
• Ask about previous TB/contact history– But absence does not rule out TB or make it
unlikely
• Ethnicity is important• Think osteo-articular TB …• Have a high index of suspicion..
– In a young patient with a single chronic painful joint and from an area of high background incidence of TB
TB
• Beware of the young patient (from an area of high incidence) with backache that doesn’t go away
• Must also consider the diagnosis in pregnant ladies

Joint TB - Investigations
• Plain x-rays often normal• MRI can be helpful in diagnosis1
– But there needs to be a high index of suspicion to request this
• Aspiration of synovial fluid for TB culture • Synovial biopsy
– ie tissue for TB culture should sent in saline or water
– Higher yield2
1. Desai.J Bone Joint surg Br.19942. osteoarticular TB in a general hospital in the last decade.ruiz.clin microbiol
infect.2003

Joint TB - Management
• Standard quadruple therapy*• Rifampicin• Isoniazid• Pyrazinamide• Ethambutol
*short course chemotherapy for spinal Tb.parthasarathy.journal of bone and joint surgery.1999
How long for?

Joint TB - management
• Usually 6 months is standard
• No controlled trials for peripheral joint TB
• 6 months?
• 12 months?
• Do they require surgery?

Joint TB - management
• 1A multicentre MRC study of spinal tuberculosis suggests good results can be achieved with 6-9 months of treatment and this is currently the recommendation of The British Thoracic Society Guidelines/NICE
1.Fourteenth report of the Medical Research Council Working Party on Tuberculosis of the Spine.
Int Orthop. 1999; 23(2): 73-81

Outcome at 5 yearsOutcome Hong Kong
Surgery+6HRsNo %
Hong KongSurgery+9HRsNo %
MadrasSurgery+6HRNo %
Madras6HRNo %
Madras9HRNo %
Favourable 23 96 25 96 72 88 75 91 84 98
Unfavourable 1 4
1 4 10 9 7 8 2 2
Total 24 26 82 82 86
Joint TB - management
• Even quite extensive joint disease with severe radiographic changes can resolve with medical treatment alone

Joint TB - management
• However, if treatment is delayed, there can be considerable loss of function and a requirement for extensive surgical intervention.

Key messages
• Peripheral joint tuberculosis should be considered in any patient with chronic joint pain
• and particularly if there is swelling present • and especially if the patient is from an ethnic
group with a high background incidence of tuberculosis.
• Biopsy and culture is important to identify MDR-TB
• Chemotherapy is sufficient in many cases and surgery is helpful in selected cases

Supplementary slides
Short course chemotherapy
• MRC working party on TB of spine
• 3 countries: Hong Kong, India and Korea
• 3 randomised trials
• 5 year assessment
International Orthopaedics 1999 23 : 73-81
International Orthopaedics 1999 23 : 73-81
Short course chemotherapy
• Comparison of ….– Hong Kong radical resection +6HRS– Ambulant therapy 6HR (medical)– Ambulant therapy 9HR (medical)
International Orthopaedics 1999 23 : 73-81
Short course chemotherapy
• Outcomes– Unfavourable outcome– Favourable outcome
• (full functional activity, radiologically quiescent, no myelopathy with functional impairment, modification of therapy)
Therapy
• Medical therapy usually sufficient
• Surgery in selected cases (cord compression, progressive neurology, marked kyphosis)
• 6(-9) months therapy – 2HRZE+ 4HR

Indications for surgery
• patients aged less than 15 years, in whom the initial angle of kyphosis is more than 30º
• patients started on ambulant chemotherapy who develop progressive kyphosis

Indications for surgery
• children aged less than ten years with destruction of vertebral bodies who have partial or no fusion even during programme
• patients with compression of the spinal cord in whom the neurological status deteriorates in spite of chemotherapy