otoscopy
DESCRIPTION
JjTRANSCRIPT

OTOSCOPY
1. Greet the patient, Introduce yourself, Check her/his identity
2. Explain the procedure/ purpose of visit: “I am here to examine the inside of your ear with a
special instrument called otoscope. During the examination I will be coming very close to you.
If you are uncomfortable any time, tell me. I will perform a special test with another instrument
called tuning fork.”
3. Exposure / position: “You can sit with head and neck slightly tilted to the other side.”
4. Privacy and Chaperone
5. Take a verbal consent
6. Check instruments:
a. Otoscope in working position
b. Tuning fork- 512 Hz or 256 Hz
7. Inspection: First inspect both ears and then say: “On inspection, there is no swelling, no
redness, no signs of trauma, external discharge wax.
8. Palpation:
a. Temperature: Warm your hands and compare each ear with lateral of neck.
“There is no local rise of temperature.”
b. Tenderness: you are at the right side of the patient; examine the ears on by one by
looking at his face for tenderness.
i. pre-auricular – pulp of finger
ii. auricular – thumb and index finger
iii. post auricular – pulp of finger
9. Rule out the contraindications with Tragus test:
“Tragus test is negative on the right side. I will precede Otoscopy.”
10. Tuning fork test:
a. Rinne’s test: “this is a buzzing instrument. I will be placing at two
point – show the patient while saying- tell me where you hear
that?” place it on the mastoid bone and in front of hearing canal.
AC>BC = normal or sensorineural … AC< BC conductive
CSSO (Conductive Same Sensorineural Opposite)
b. Weber’s test: “this time, I will be placing it on your forehead,
please tell me in which ear you hear better?”
(No lateralisation= normal Weber’s test)
11. Otoscopy:
a. Change the speculum.
b. Make sure it is working
c. Hold it like a pen in your right hand.
d. Hold the ear backward, upward with left thumb and index fingers.
e. Before going inside, check external for any bleeding or foreign body.
“I cannot appreciate any bleeding, any foreign body.”
f. Don’t talk while doing Otoscopy.
g. While taking out otoscope, check for any bleeding or discharge. “I’ll check speculum for
any bleeding or discharge. And discard it. I’ll thank the patient.”
h. I can appreciate… my most probably diagnosis is …
i. Comment on:
a. Cone of light
b. Handle of malleus
c. Umbo
d. Annulus
e. Pars flaccida/ pars tensa
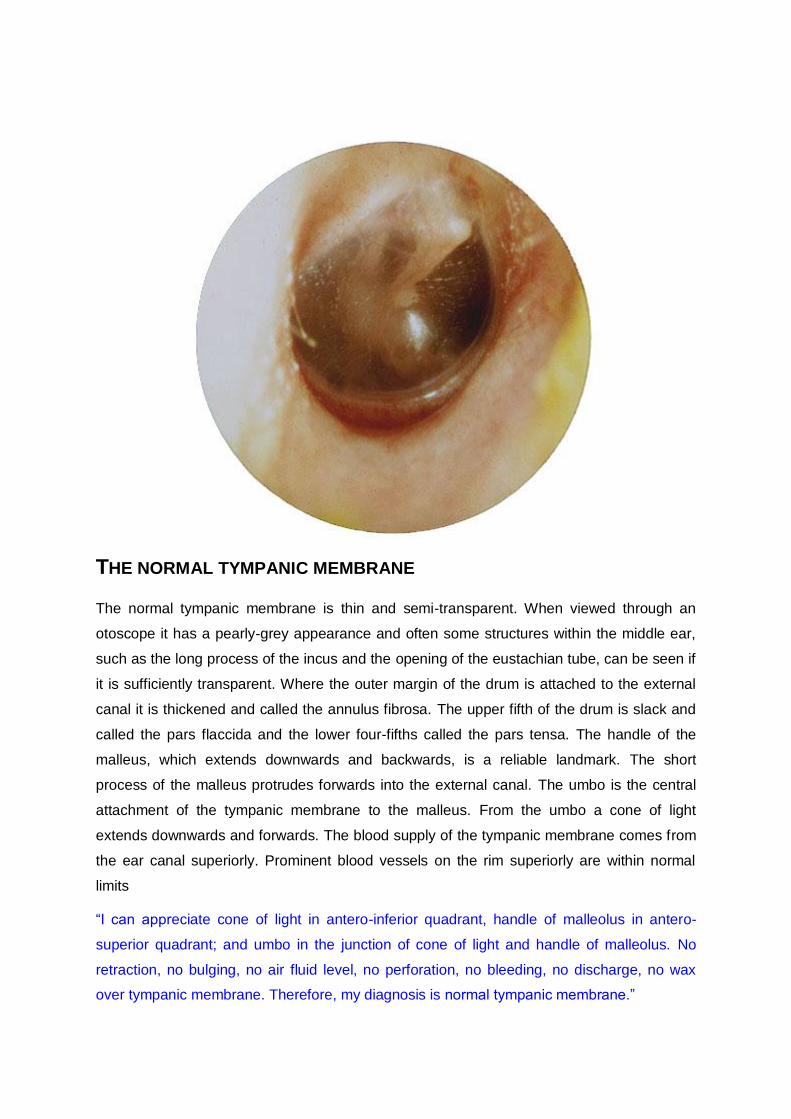
THE NORMAL TYMPANIC MEMBRANE
The normal tympanic membrane is thin and semi-transparent. When viewed through an
otoscope it has a pearly-grey appearance and often some structures within the middle ear,
such as the long process of the incus and the opening of the eustachian tube, can be seen if
it is sufficiently transparent. Where the outer margin of the drum is attached to the external
canal it is thickened and called the annulus fibrosa. The upper fifth of the drum is slack and
called the pars flaccida and the lower four-fifths called the pars tensa. The handle of the
malleus, which extends downwards and backwards, is a reliable landmark. The short
process of the malleus protrudes forwards into the external canal. The umbo is the central
attachment of the tympanic membrane to the malleus. From the umbo a cone of light
extends downwards and forwards. The blood supply of the tympanic membrane comes from
the ear canal superiorly. Prominent blood vessels on the rim superiorly are within normal
limits
“I can appreciate cone of light in antero-inferior quadrant, handle of malleolus in antero-
superior quadrant; and umbo in the junction of cone of light and handle of malleolus. No
retraction, no bulging, no air fluid level, no perforation, no bleeding, no discharge, no wax
over tympanic membrane. Therefore, my diagnosis is normal tympanic membrane.”

WAX
Wax, or cerumen, is a normal secretion in the cerumenous glands in the outer part of the
meatus, and can obscure or partially obscure the drum. When it is first produced it is
colourless and semi-liquid in consistency, but with time it changes from pale yellow, to
golden yellow, to light brown and finally black. As the wax darkens it also hardens, and the
darker the colour the denser the consistency.
“I can appreciate tympanic membrane, obstructed with a brown material; colour of wax in
transition from pale yellow, golden yellow, golden brown, finally brown. Cone of light, handle
of malleolus and umbo cannot be appreciated. Therefore, my diagnosis is wax over
tympanic membrane.”

ACUTE OTITIS MEDIA WITH EFFUSION (A)
There is distortion of the drum, prominent blood vessels in the upper half, with dullness of
the lower half. There is also bulging of the upper half of the drum and the outline of the
malleus is obscured.
“I can see tympanic membrane which is red, inflamed, congested, oedematous, and tense. I
can appreciate an air fluid level in antero superior and postero-superior quadrants. Cone of
light, handle of malleolus and umbo cannot be appreciated. Annulus can be appreciated.
Therefore, my diagnosis is acute otitis media with effusion.”

ACUTE OTITIS MEDIA WITH EFFUSION (B)
The handle of the malleus is obscured, and fluid levels are obvious behind the drum.
“I can see tympanic membrane which is red, inflamed, congested, oedematous, and tense.
There is no air fluid level. Cone of light, handle of malleolus and umbo cannot be
appreciated. Annulus can be appreciated. Therefore, my diagnosis is acute otitis media
without effusion.”
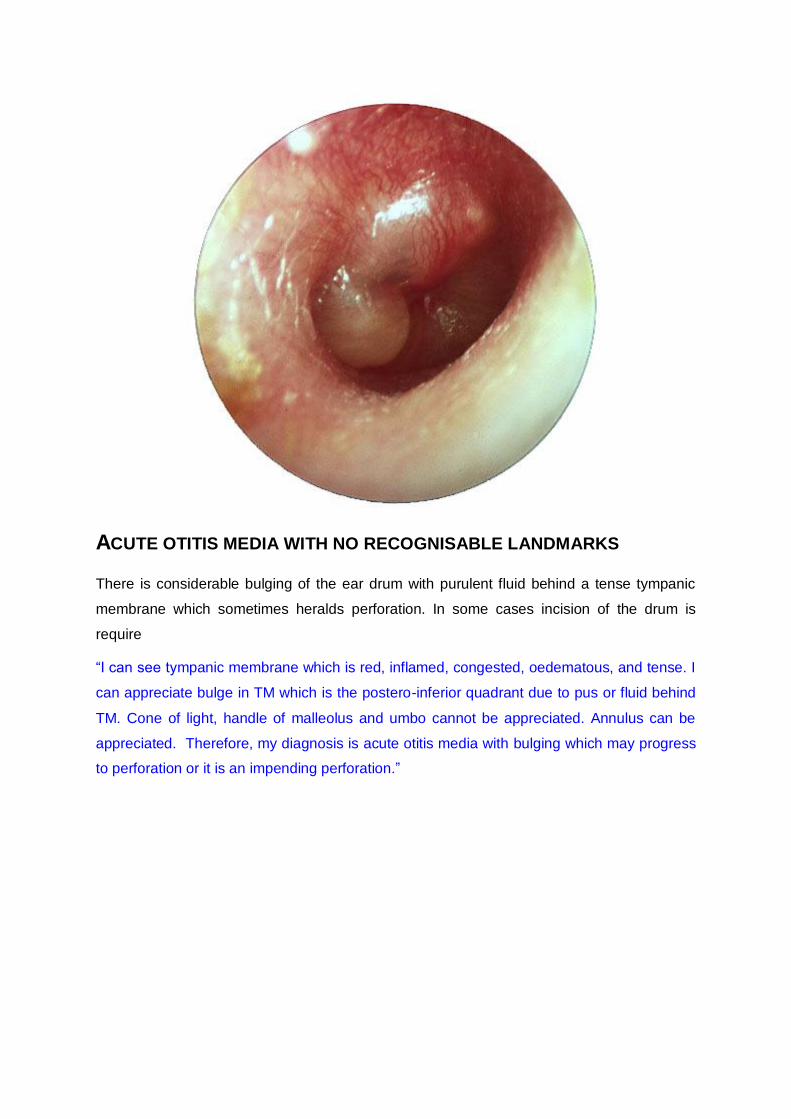
ACUTE OTITIS MEDIA WITH NO RECOGNISABLE LANDMARKS
There is considerable bulging of the ear drum with purulent fluid behind a tense tympanic
membrane which sometimes heralds perforation. In some cases incision of the drum is
require
“I can see tympanic membrane which is red, inflamed, congested, oedematous, and tense. I
can appreciate bulge in TM which is the postero-inferior quadrant due to pus or fluid behind
TM. Cone of light, handle of malleolus and umbo cannot be appreciated. Annulus can be
appreciated. Therefore, my diagnosis is acute otitis media with bulging which may progress
to perforation or it is an impending perforation.”

SEROUS (SECRETORY) OTITIS MEDIA (A)
The ear drum has lost its lustre and an effusion is visible through the ear drum with a fluid
meniscus defining the upper margin.
“I can see tympanic membrane which is red, inflamed, congested, oedematous, and tense.
There is no air fluid level or bulge. Cone of light, handle of malleolus and umbo cannot be
appreciated. Annulus can be appreciated. Therefore, my diagnosis is secretory otitis media.”

FLUID BEHIND THE EARDRUM
Seen in an asymptomatic child. Effusion is visible with a fluid level in the lower half of the ear
drum. The handle of the malleus is also difficult to visualise.

RESOLUTION OF MIDDLE EAR INFECTION
The handle of the malleus is still foreshortened and the horizontal. Signs in the upper half of
the ear drum suggest that fluid is still present in the middle ear.

SEROUS OTITIS MEDIA (B)
There is indrawing of a dull ear drum and the handle of the malleus is characteristically
horizontal. Eustachian tube obstruction had led to failure of replacement of air which is
normally absorbed from the middle ear resulting in vacuum formation and effusion of fluid.
“I can see tympanic membrane which is red, inflamed, congested, oedematous, and tense.
There is no air fluid level or bulge. Cone of light, handle of malleolus and umbo cannot be
appreciated. Annulus can be appreciated. Therefore, my diagnosis is secretory otitis media.”
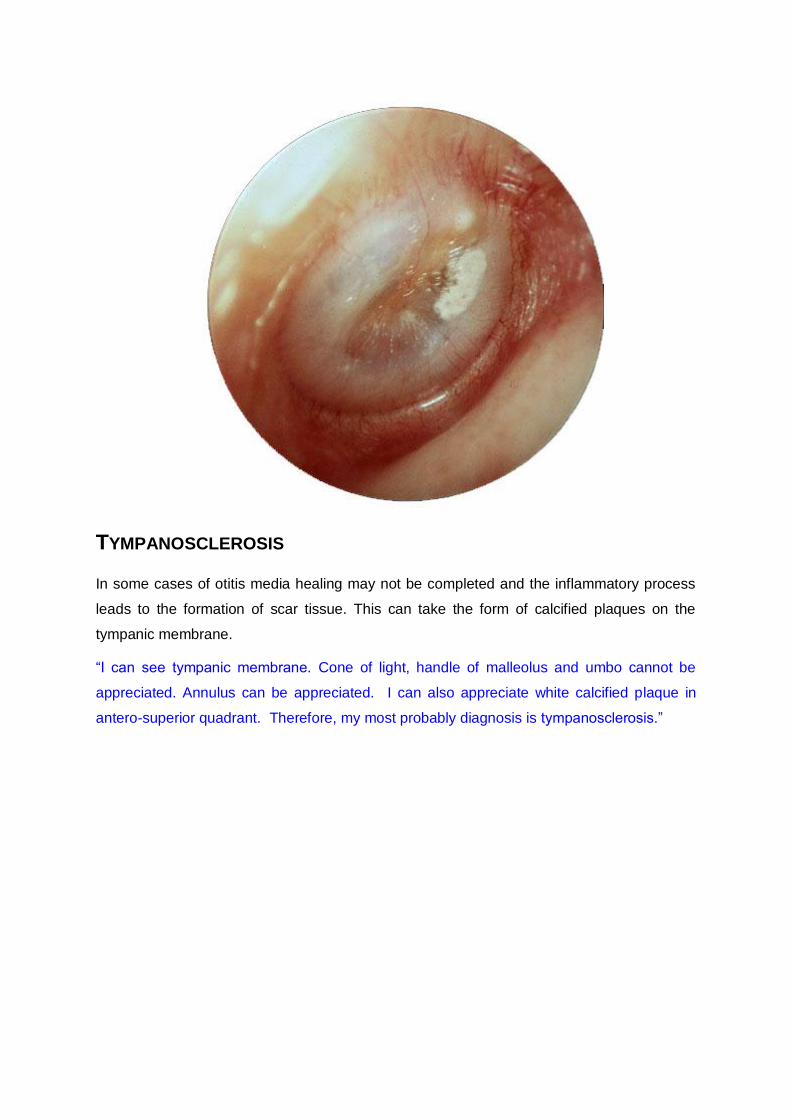
TYMPANOSCLEROSIS
In some cases of otitis media healing may not be completed and the inflammatory process
leads to the formation of scar tissue. This can take the form of calcified plaques on the
tympanic membrane.
“I can see tympanic membrane. Cone of light, handle of malleolus and umbo cannot be
appreciated. Annulus can be appreciated. I can also appreciate white calcified plaque in
antero-superior quadrant. Therefore, my most probably diagnosis is tympanosclerosis.”

CENTRAL PERFORATION OF THE EAR DRUM
Perforations are usually single but may be multiple. Spontaneous rupture of the drum can
occur in association with acute infection when the tense drum perforates and releases pus.
The ear drum illustrated has a long standing perforation accompanied by tympanosclerosis
of the drum.
“I can see tympanic membrane. Cone of light and umbo cannot be appreciated; but can
appreciate handle of malleolus which is distorted. I can appreciate a large central perforation
in antero-inferior and postero-inferior quadrants. I can also appreciate few white calcified
plaques over tympanic membrane. Therefore, my most probably diagnosis is Central
perforation with tympanosclerosis.”
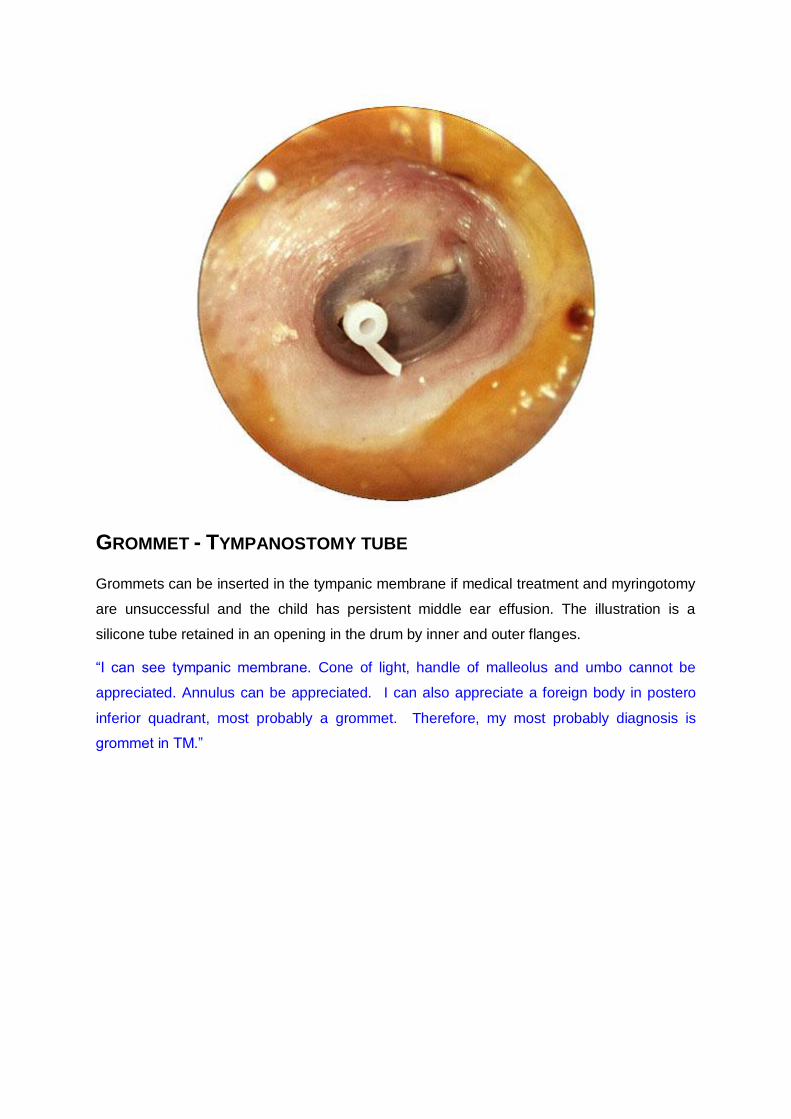
GROMMET - TYMPANOSTOMY TUBE
Grommets can be inserted in the tympanic membrane if medical treatment and myringotomy
are unsuccessful and the child has persistent middle ear effusion. The illustration is a
silicone tube retained in an opening in the drum by inner and outer flanges.
“I can see tympanic membrane. Cone of light, handle of malleolus and umbo cannot be
appreciated. Annulus can be appreciated. I can also appreciate a foreign body in postero
inferior quadrant, most probably a grommet. Therefore, my most probably diagnosis is
grommet in TM.”

TEST YOURSELF