osteoporosis review · · 2017-03-14osteoporosis review ... (arh) are up to four times more...
TRANSCRIPT

OsteoporosisReview
www.nos.org.uk
IN THIS ISSUE...
Autumn 2016 • Volume 24 • Number 2
Editor: Elaine Dennison, MB BChir MA MSc PhD FRCP, Professor of Musculoskeletal Epidemiology and Honorary Consultant in Rheumatology MRC Lifecourse Epidemiology Unit, University of Southampton
Editorial Board: Terence O’Neill MD FFPH FRCP Professor, University of Manchester, Judith Adams MB BS MRCS(Eng) DMRD FRCR FRCP Professor of Clinical Radiology, University of Manchester. Jonathan Bayly BA MB BS MRCGP Associate Lecturer, University of Derby. Pam Brown MB ChB DFFP MBA GP, Swansea. Nicholas Harvey MA, MB, BChir, PhD, FRCP, Professor of Rheumatology and Clinical Epidemiology, MRC Lifecourse Epidemiology Unit, University of Southampton. Geeta Hampson MB ChB MSc MD FRCPath, Consultant chemical pathologist, St Thomas’ and Guy’s Hospitals. Susan Lanham-New BA MSc PhD RPHNutr Head of Nutritional Sciences, University of Surrey, Guildford. Rachel Lewis MCSP SRP HT Superintendent Physiotherapist, Southmead Hospital, North Bristol NHS Trust. David Reid MBChB FRCPEdin MD Professor of Rheumatology, University of Aberdeen. Opinder Sahota MBChB MRCP Consultant Physician, University Hospital, Nottingham. Stephen Tuck Consultant Rheumatologist James Cook University Hospital, Middlesbrough and Honorary Senior Lecturer, Newcastle University. Nicola Peel DM, FRCP Consultant in Metabolic Bone Medicine, Sheffield Teaching Hospitals NHS Foundation Trust.
Journal of the National Osteoporosis Society
Are we doing enough to prevent fractures in those who abuse alcohol?Elinor Archer, Queen Elizabeth Hospital, Gateshead; Killian Turbitt, Final Year Medical Student, University of Newcastle upon Tyne; Laura Moyles, Final Year Medical Student, University of Newcastle upon Tyne; Clive Kelly MBBS, Queen Elizabeth Hospital, Gateshead.
This paper addresses the increased incidence of fracture occurring in those who consume excessive amounts of alcohol. It examines the limited evidence base for its prevention and treatment.
Why is this important?
In recent years alcohol abuse has become an ever increasing problem with 10.8 million adults drinking to a degree that poses harm to their health, and 1.6 million with some level of alcohol dependence in the UK alone1. Alcohol abuse contributes significantly to hospital admissions. In England and Wales alcohol accounts for a third of a million admissions annually1.
There are many adverse consequences of long-term alcohol abuse, and while some are well recognised such as
its effects on the brain and liver, the effects on bone have received far less attention. Patients with alcohol related harm (ARH) are up to four times more likely to have fractures compared to age-matched controls2. Such individuals are already at a higher risk of morbidity and mortality as a result of liver disease, and this risk increases in patients with concurrent fractures due to prolonged bleeding times2.
Fractures themselves carry a significant mortality. Hip fractures have a mortality of 10% within one month and 30% within a year3. Vertebral fractures also carry increased mortality in addition to causing severe pain and immobility. Complicating this is the effect chronic alcohol abuse has on bone healing, with delayed or non – union well described4.
1 Alcohol & FracturesElinor Archer, Killian Turbitt,Laura Moyles, Clive Kelly
7 Peer ReviewJill Griffin
12 National Osteoporosis Society update
14 EUGMSRachel Cowan, Tahir Masud
17 Bone health in peopleliving with HIV Karen Walker-Bone
23 Arthritis and osteoporosisAlice Mason, Anna Litwic

Osteoporosis Review 2016; Vol 24 No22
Direct effect of bone cells–induction of osteocyte
apoptosis
Stimulation of Parathormone leading to increased
osteoclast activity
Pancreatic dysfunction leading malabsorption and
reduced Vitamin D levels
Imbalance of cytokine expression
Sex hormone deficiency leading to reduced osteoblast
activity
Liver disease–reduction in Insulin growth factor 1
(IGF-1) leading to reduction in osteoblast activity
Pharmacological intervention for other morbidities e.g loop
diuretics, proton pump inhibitors and glucocorticoids
Alcohol & Fractures
Effect of alcohol on bone
A moderate amount of alcohol consumption may increase bone mineral density (BMD) in women5, possibly mediated via an effect of alcohol on oestrogen levels6. In heavy drinkers with ARH, alcohol causes bony demineralisation7, with a resulting decrease in BMD8 and an increased fracture rate9. The increased risk of falls contributes to the high fracture risk in ARH. Other risk factors for osteoporosis often co-exist in these patients and include low body mass index (BMI), smoking and reduced physical activity10. The factors relating to bone loss and increased fracture rate in patients with ARH are summarised in Figure 1. BMD is reduced more markedly at the spine than at the hip in patients with ARH, and alcohol excess is the commonest cause of vertebral osteoporosis in younger patients. The consequences of fractures among patients with ARH may also be more significant. Increased social isolation, low employment rates and poor diet may all contribute to an increased risk both of complications and of further fractures.
Alcohol excess and fracture site
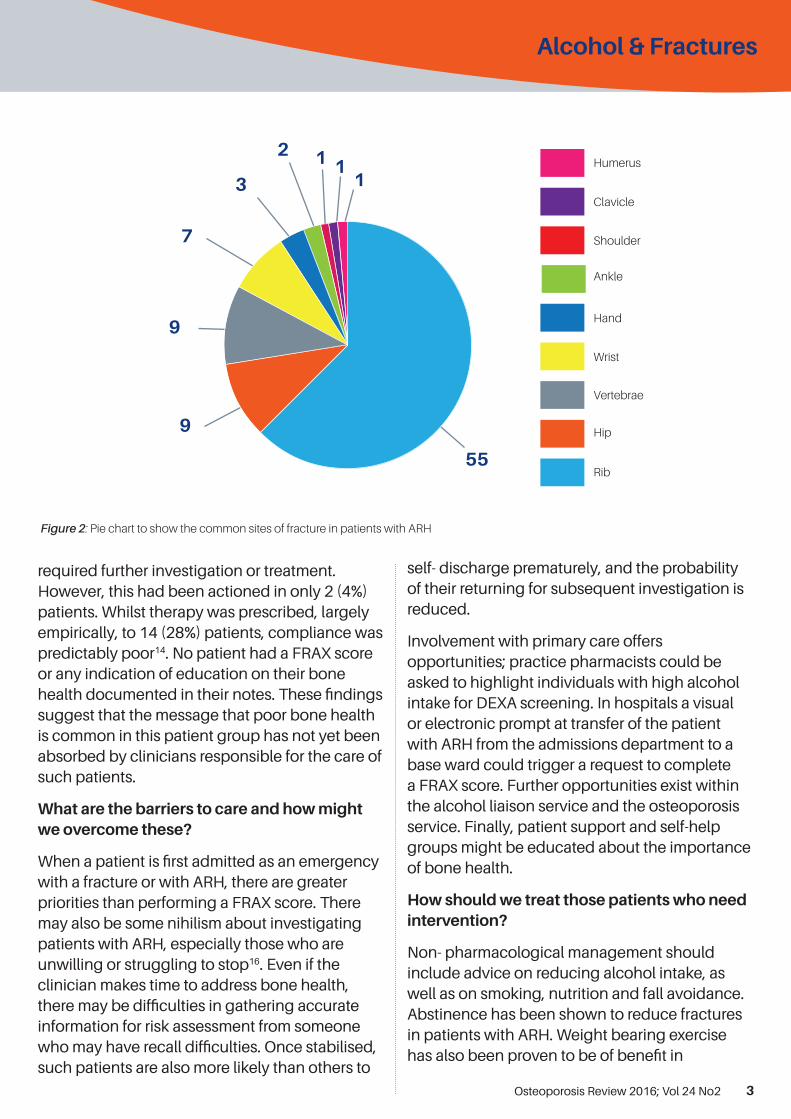
A number of sites are prone to fracture in those with ARH including ribs, vertebrae, hips and wrist8 -11. Figure 2 summarises the commonest fracture sites in patients admitted to hospital with a background of alcoholic liver disease8, 9 or with ethanol consumption over 100g/day11. The Fracture Risk Assessment (FRAX) score is a tool used to assess the 10-year risk of fragility fracture. It is recommended for use by the World Health Organisation (WHO) and assesses several clinical risk factors including alcohol consumption and, where indicated, BMD at the femoral neck12. This provides an individual assessment of osteoporotic fracture risk over the next decade13.
Are we investigating our ARH patients?
We have previously recommended a strategy for investigating bone health in patients admitted to hospital with ARH2. Recently we assessed compliance with these recommendations. FRAX scores in 50 patients with a median age of 58 years admitted with ARH indicated that 29 (58%)
Mechanisms of bone loss in Alcoholic Liver Disease
Figure 1: Diagram showing the methods of bone loss in ALD2
Osteoporosis Review 2016; Vol 24 No2 3
Alcohol & Fractures
required further investigation or treatment. However, this had been actioned in only 2 (4%) patients. Whilst therapy was prescribed, largely empirically, to 14 (28%) patients, compliance was predictably poor14. No patient had a FRAX score or any indication of education on their bone health documented in their notes. These findings suggest that the message that poor bone health is common in this patient group has not yet been absorbed by clinicians responsible for the care of such patients.
What are the barriers to care and how might we overcome these?
When a patient is first admitted as an emergency with a fracture or with ARH, there are greater priorities than performing a FRAX score. There may also be some nihilism about investigating patients with ARH, especially those who are unwilling or struggling to stop16. Even if the clinician makes time to address bone health, there may be difficulties in gathering accurate information for risk assessment from someone who may have recall difficulties. Once stabilised, such patients are also more likely than others to
self- discharge prematurely, and the probability of their returning for subsequent investigation is reduced.
Involvement with primary care offers opportunities; practice pharmacists could be asked to highlight individuals with high alcohol intake for DEXA screening. In hospitals a visual or electronic prompt at transfer of the patient with ARH from the admissions department to a base ward could trigger a request to complete a FRAX score. Further opportunities exist within the alcohol liaison service and the osteoporosis service. Finally, patient support and self-help groups might be educated about the importance of bone health.
How should we treat those patients who need intervention?
Non- pharmacological management should include advice on reducing alcohol intake, as well as on smoking, nutrition and fall avoidance. Abstinence has been shown to reduce fractures in patients with ARH. Weight bearing exercise has also been proven to be of benefit in
Humerus
Clavicle
Shoulder
Ankle
Hand
Wrist
Vertebrae
Hip
Rib
9
9
7
3
2 1 11
55
Figure 2: Pie chart to show the common sites of fracture in patients with ARH

Osteoporosis Review 2016; Vol 24 No24
Alcohol & Fractures
osteoporosis (in other groups)16. A decision to initiate treatment for osteoporosis can be made without a DEXA result in those at high risk of fracture on FRAX. In patients with intermediate risk, a DEXA scan is indicated and the need for treatment is guided by the result. It is important to ensure adequate intake of vitamin D and calcium in patients with alcohol excess who may have poor diets and spend little time outside.
Although the first line pharmacological treatment is usually an oral bisphosphonate based on cost and efficacy, concordance rates of only 35- 45% at one year are reported in the general population17. We know overall compliance with medication in patients with ARH is worse than in the general population18. In addition, the risks of treatment with oral bisphosphonates may be greater in patients with ARH because of their prolonged clotting and the high risk of varices where bleeding may be triggered by the development of oesophagitis.
Hence parenteral therapies may be particularly appropriate in these patients, as they reduce the risk of unwanted side effects and improve compliance. This is especially true if therapy is commenced in hospital, ideally during their admission. Such second line treatment options include Denosumab, a monoclonal antibody that reduces osteoclast activity. This is administered subcutaneously every six months and has been shown to be effective and well tolerated19. Another treatment option is the potent intravenous bisphosphonate Zoledronic acid, administered annually. Both these agents reduce bone turnover, and may be given for up to five years. A third option is the anabolic agent Teriparatide, an expensive parathyroid hormone peptide given as a daily subcutaneous injection for a maximum of two years. However, the criteria for using this agent are rarely achieved by ARH patients.
Very little published work has been done on the role of any of these agents in patients with
ARH, so there is very limited evidence base to guide therapy. In the general population, Zoledronic acid administered annually reduced the frequency of further fractures by 35% in those with a previous hip fracture20. Furthermore there was a decrease in death from any cause of 28% compared to those treated with placebo. It is essential that both calcium and vitamin D levels are adequate prior to therapy to reduce the risk of hypocalcaemia, and that eGFR is at least 25 ml/hour. Both improvement in BMD and decrease in risk of vertebral fracture are similar with Zoledonic acid and Denosumab, though studies comparing the two are limited. Both agents appear to be of similar efficacy and carry comparable risks and benefits. It may matter less which one is used in patients with ARH at high fracture risk, than that the decision to commence therapy is made early while the patient is still in hospital.
Key Points:
• Alcohol related bone fractures arecommon and frequently affect youngerpatients
• Low bone density at the spine is oftenassociated with alcohol excess in bothmen and women. Careful enquiry aboutalcohol consumption is important insuch patients.
• Mechanisms for bone loss as a result ofalcohol are complex with new pathwaysrecently reported, some of which offernew therapeutic opportunities
• Apart from abstinence, no formalstudies of therapeutic intervention havebeen performed in patients with alcoholrelated bone disease
• The role of both IV Zoledronic acid and SC Denosumab in treating patients with alcohol related fractures is deserving of further consideration.
Osteoporosis Review 2016; Vol 24 No2 5
Alcohol & Fractures
References
1. https://www.gov.uk/government/publications/health-matters-harmful-drinking-and-alcohol-dependence/health-matters-harmful-drinking-and-alcohol-dependence?utm_source=Blog&utm_medium=ToolsBlogAlc&utm_campaign=HealthMatters#contents
2. Kieran Kelly, Clive Kelly. The pattern and causeof fractures in patients who abuse alcohol -What should we do about it? PostGrad MedJ 2013 doi131990 23 July. Available: http://pmj.bmj.com/content/early/2013/07/26/postgradmedj-2013-131990.full.pd
3. National Clinical Guidelines. The managementof hip fractures in adults, 2011. http://guidance.nice.org.uk/CG124.
4. Chakkalakal, DA. Alcohol-induced bone lossand deficient bone repair. Alcohol Clin Exp Res2005; 29: 2077–2090
5. Williams FMK, Cherkas LF, Spector TD,MacGregor AJ. The effect of moderate alcoholconsumption on bone mineral density: a studyof female twins. Ann Rheum Dis 2005; 64: 309–310.
6. Berg KM, Kunins HV, Jackson JL, et al.Association between alcohol consumption andboth osteoporotic fracture and bone density.The American Journal of Medicine 2008; 121(5):406-418
7. Díez-Ruiz A, García-Saura PL, García-Ruiz P etal. Bone mineral density, bone turnover markersand cytokines in alcohol-induced cirrhosis.Alcohol and Alcoholism 2010; 45(5): 427–430
8. Kelly C, Bartholomew P, Reddy A. Seriouseffects of alcohol on Bone density and fractureincidence. Ann Rheum Dis 2012 (EULARabstracts) Number 1013
9. Chang Seok Bang. Osteoporosis and bonefractures in alcoholic liver disease: A meta-analysis. World J Gastroenterology 2015;21(13): 4038-4047
10. Kanis JA, Johnell O, Oden A, Johansson H,McCloskey E. FRAX and the assessment offracture probability in men and women from theUK. Osteoporos Int 2008; 19: 385-397
11. González-Reimers E, Alvisa-Negrín J, Santolaria-Fernández F et al. - Vitamin D and nutritionalstatus are related to bone fractures in alcoholics.Alcohol and Alcoholism2011;46(2): 148-55
12. WHO Fracture Risk Assessment Tool (FRAX).Available from: URL: http://www.shef.ac.uk/FRAX
13. WHO National Osteoporosis Guideline Grouprecommendations. Available from URL: http://www.shef.ac.uk/NOGG
14. Moyles L, Archer E and Kelly C. How well dowe identify and treat bone disease in patientsadmitted with alcohol. Foundation JournalAugust 2016 In press.
15 Miller NS, Sheppard LM, Colenda CC, Magen J. Why Physicians Are Unprepared to Treat Patients Who Have Alcohol‐ and Drug‐related Disorders. Academic Medicine 2001; 76(5): 410- 418.
16. Howe TE, Shea B, Dawson L et al. Exercisefor preventing and treating osteoporosisin postmenopausal women. CochraneDatabase Systemic Review 2011; Jul 6;(7):DOI:0.1002/14651858.CD000333.pub2
17. Silverman SL, Schousboe JT, Gold DT. Oralbisphosphonate compliance and persistence:a matter of choice? Osteoporosis International2011; 22(1): 21–26.
18. Silverman SL, Gold DT. Compliance andpersistence with osteoporosis medications:A critical review of the literature. Rev EndocrMetab Disord. 2010; 11(4): 275–280.
19. Adler RA, Gill RS. Clinical utility of denosumabfor treatment of bone loss in men and women.Clin Interv Aging. 2011; 6: 119–124.
20. Lyles KW. Zoledronic Acid in Reducing ClinicalFracture and Mortality after Hip Fracture. NewEngland Journal of Medicine 2007; 357: 1799-1809

Fracture Liaison Service Champions’ Summit 2017
The Summit will include:
• Updates on FLS implementation acrossthe UK
• Latest developments on the FLS-DB
• Opportunities to question some of themost influential speakers in the field
• Bespoke workshops on FLS andsecondary fracture prevention.
Friday March 3rd 201710.30 - 16.30
Register for this FREE event
Cavendish Conference Centre, 22 Duchess Mews, London, W1G 9DT
To register your place call: 01761 473 263 or email: [email protected] for a registration form
5 CPD CreditsJoin the network at: www.nos.org.uk/champions
Support the development of FLS across the UK through a collective network of knowledge and expertise, sharing best practice in FLS and secondary fracture prevention
2017 Summit A4 ad.indd 1 01/09/2016 13:53:34

Osteoporosis Review 2016; Vol 24 No2 7
Peer Review
Peer Review of Osteoporosis and Metabolic Bone Services -24 hours as a reviewer.Jill Griffin DCR (R)
When one thinks of peer review and hospital review teams, jobbing radiographers don’t automatically spring to mind. Service reviewers must be high achieving, well-known-in-the-field medics, managers and senior specialists, right?
Actually, in practice reviewers should be from a cross section of clinical backgrounds working together. The only qualification is that a reviewer should have first-hand and current experience in the type of practice to be reviewed.
Peer review means just that: professionals on the ground providing services and seeing patients, taking a look with fresh eyes at other services. Because we know and understand the challenges, and the ‘nitty gritty’, of day to day delivery of these services, each of us ‘in the business’ are qualified. If you work clinically in any aspect of delivering osteoporosis or bone health services then peer review is a great opportunity to develop your skills, build relationships. It’s also a great addition to your CV.
Peer review is an invitation to share good practice, identify black spots in service delivery, guide direction where change might be beneficial and make contact with peers in the field. In short, peer review is good for all levels of a clinical team and learning from each other has to be a positive way of developing good standards in service delivery.
Down to business–
24 hours in the life of a reviewer.
Although we’re looking at 24 hours in the life of a reviewer for the purpose of this article, the groundwork and preparation for a peer review will start a long time before the actual day.
3-6 months before a review:
I see a call for reviewers via a National Osteoporosis Society (Charity) publication to travel to a District General Hospital in a fairly rural location arranged for a date later in the year. I think this will be an interesting experience and wonder whether I can add value to the review team.
After a brief email exchange with Hilary Arden, the National Osteoporosis Society’s Head of Service Delivery who manages Peer Review for the charity, I find I needn’t have worried – as a long time DXA Radiographer I’m well suited to being able to look at the bone densitometry element of the osteoporosis service that has requested a review. I’m on the team!
A couple more emails circulate to introduce the final review team to each other. I’m working with a Fracture Liaison Service (FLS) nurse, a Rheumatologist, the Charity’s Clinical and Operations Director Fizz Thompson and a member of the Charity’s Service Development team.
3-4 weeks before the review:
I make my travel arrangements with the help of the charity, who also make sure I have a room for the night in a local hotel. I book my trains so that I arrive in plenty of time the evening before the review. The Charity sends me an expense claim form so that my expenses can be reimbursed.
2-3 weeks before the review:
The team receives an email containing the final arrangements including the programme for the review and the pre-review questionnaire that has been completed by the service lead at the hospital we are reviewing.
Osteoporosis Review 2016; Vol 24 No28
I take an hour to read through this to get a good understanding of the service and how it is run. I also make a few notes in the margins with queries and questions I think of. I can’t help but compare them to the service I work in and wonder how different it will be in person. Amongst the paperwork, I have received a toolkit for reviewing the DXA aspects of the service with question prompts to ask the staff. This is linked to service standards, so I feel pretty well prepared. The document covers things like Local Radiation rules, IR(ME)R responsibilities, clinical audit, training and scan reports, as well as things like the scan room environment and information leaflets patients can access.
1 day before:
I take a look through the questionnaire again while I am on the train travelling. Check in is no problem and I have a comfortable room and time to unpack and have a cuppa before I meet the rest of the review team in the hotel bar for a meal and pre-review meeting.
Our Rheumatologist colleague is going to be chairing the review and he makes us all very welcome and listens to what we all have to say. We all appear to have the same ideas about the service and are looking forward to hearing from them in the morning about what they want to gain from the review.
Peer Review
Review day:
In the morning we arrive at the hospital with about 10 minutes to spare and the porter’s lodge calls their service lead who arrives promptly and we are shown to the meeting room we have for the day. There’s coffee, tea and biscuits so we feel very welcome and well prepared for all the talking that’s ahead of us.
9.00am - Our first interview with the osteoporosis team: there’s the lead clinician, FLS nurse lead and the Radiographer lead. Kicking off with the usual round of introductions, our chair begins the review by asking what the team would like to get from the day. The service lead also describes their service and outlines the area demographic, how the local systems work and the commissioning process, which paints a good picture for us.
10.00am - Clinician interviews: We meet with a variety of clinicians involved in the service: an ortho-geriatrician, orthopaedic surgeon, radiologist and rheumatologist. We begin to see how this service works and what some of the stake-holding clinicians feel are good and less good aspects of the service.
11.00am - Time to visit the departments: we visit outpatients, the day case unit and we chat to nurses giving the zoledronic acid infusions. We see the falls clinic and chat to the lead falls clinician. We begin to discover that this service is pretty ‘joined up’. Everyone is really welcoming and we also get a chance to ask some patients what they think about the service. We visit the hip fracture ward and are able to speak with the nurses and physiotherapists caring for the fragility fracture patients.
12.30pm - Lunch time! We have a working lunch with clinicians and managers of the services joining us. Of course, we talk ‘shop’ and compare our respective services.
Osteoporosis Review 2016; Vol 24 No2 9
Peer Review
1.15pm - We split up and I go with the rheumatologist on the team to the DXA scanning room, while the others visit the administrative offices and the FLS team.
We meet with the Radiographer of the day who has a patient who is happy to have us visit during the scan. It was really useful to see the scanner in practice and am pleased to see good quality scans being made. When the patient leaves I go through the DXA review tool kit questionnaire to make sure I don’t miss anything and the radiographer and I chat about training and staffing and how our services differ.
We look at some of their protocols and I make some suggestions about how she could formalise some clinical audit around quality. We are both quite enthused about making that happen. We exchange email addresses and promise to keep in touch.
Meanwhile our rheumatologist has been reviewing some of the scan reports which I cast my eye over from a technical point of view. Again we make some suggestions to improve the continuity across individuals reporting scans.
2.30pm - We reconvene in the meeting room to meet with some of the hospital contracting team to learn about commissioning in the area, and then with some of the service line managers, including radiology and I am able to ask some questions about reporting of vertebral fractures.
3.30pm - Tea and biscuits arrive while we have a ‘closed door’ review team meeting to discuss our findings and plan any suggestions or recommendations we have for the hospital team. We are all impressed with the welcome and openness of everyone we have met and their willingness to embrace suggested service improvement.
4.00pm - The hospital team gather in the meeting room eager to find out what we think. Our chair sums up the general flavour of our visit and we each get a chance to outline our own thoughts and suggestions. I’m thrilled to have been able to make useful suggestions and provide positive feedback to the radiographer.
4.30pm - We say our good byes and make our way to the train station.
I take the opportunity on the train journey home to write up my notes into something that will make sense when contributing to the writing of the final report. The tool kit made it easy to ask the right questions during our discussions and will help me think about my own service. I wonder if our service ‘ticks all the boxes’?
2-3 weeks after the review:
I complete my parts of the draft review report via the National Osteoporosis Society’s template. It doesn’t take me very long – just an hour or two. A few days later I receive an email with the first completed draft of the report and I make a few edits and feel I can add to some of the other areas my colleagues have drafted.
The reviewed Radiographer and I exchange a few
emails and I send her some of my clinical audit
documents for her to adapt.
I also take a look at my own service with the DXA
review toolkit and add an item or two to our team
meeting agenda to discuss with my own team.
All in all, I can only have positive thoughts about
my peer preview experience, I didn’t think I was
‘qualified’ to be a reviewer but of course I am, and
sharing and learning from each other can only benefit
those who take part. I know the Charity are keen to
widen the pool of DXA practitioners/radiographers
to help with peer review and I would heartily
recommend it.
For further information or to request to take part in a peer review, please contact Hilary Arden at the National Osteoporosis Society: [email protected]

10 Osteoporosis Review 2016; Vol 24 No1

CommentElaine Dennison
Osteoporosis Review 2016; Vol 24 No2 11
The term “secondary osteoporosis” is applied to all patients with osteoporosis in whom the identifiable causal factors are other than menopause and aging, and a large proportion of this issue focuses on three exemplar causal factors.
In this issue of Osteoporosis Review, Clive Kelly and colleagues from the University of Newcastle, discuss the importance of alcohol intake in relation to bone health. In the same article, they discuss strategies to ensure that as clinicians we consider alcohol intake when assessing patients who present with low bone mineral density or fragility fracture.
Karen Walker-Bone from the MRC Lifecourse Epidemiology Unit in Southampton, reviews HIV infection and the risk of osteoporosis; an increasingly important public health issue as the available therapies for treatment of HIV infection have improved so considerably in recent years.
Finally, Alice Mason and Anna Litwic from University Hospital Southampton, present a review of the association between rheumatoid arthritis and bone health. Rheumatoid arthritis affects about 1% of the population – about 700,000 people in the UK – so consideration of bone health in this population is critical.
Elsewhere in this issue, Tahir Masud and colleagues provide a review of the recent European Union Geriatric Medicine Society (EUGMS) statement on fracture prevention, and their recommendations for a strategy to promote best practice.
Our final piece is also centred around good practice; Jill Griffin a Consultant Practitionerat the Healthy Bones Service at Derriford Hospital, provides an in-depth account of what it is like to participate as a peer reviewer for an osteoporosis and metabolic bone service. As someone who has also contributed to a peer review panel, I would urge all our readers to consider volunteering. I came away with so many good ideas for my own practice, and the organisational skills of the National Osteoporosis Society (and the wonderful hospitality of the site that was being reviewed) made for a very positive experience.
As summer draws to a close and autumn approaches, I hope that our readers are feeling refreshed, and vitamin D replete...but more of that in the next issue!
Editorial

National Osteoporosis Society update
Osteoporosis Review 2016; Vol 24 No212
Update
Professor Ignac Fogelman
It is with great sadness that the National Osteoporosis Society has learnt of the death of Professor Ignac Fogelman.
Professor Fogelman was an Honorary Consultant Physician at Guy’s and St Thomas’ Hospital and headed up the osteoporosis screening and research unit at the Trust. He was involved in a wide range of research projects, including pioneering work on the development of techniques to measure bone density.
He was a National Osteoporosis Society Trustee, spoke at many of our events and conferences and acted as a press spokesman supporting our campaigns.
Professor Cyrus Cooper OBE, Director and Professor of Rheumatology at MRC Lifecourse Epidemiology Unit at the University of Oxford said:
“Ignac was a strong supporter of the NOS for the thirty years since the founding of the society. He was intimately involved in the translation of bisphosphonate therapy to patient care in metabolic bone disease, and pioneered the development of novel techniques to assess bone metabolism.
In addition to these major contributions to patient care and research, Ignac served as a member of the Board of Trustees of the NOS and thereby informed the policy developments in osteoporosis care throughout the decade leading up to the NICE guidance released in 2009.
He brought diligence, sharp focus and good humour to all these activities, and was well loved by patients and colleagues alike.”
Will you step forward and help?
We are pleased to announce that the National Osteoporosis Society’s #laceupforbones campaign is back for another year! And you have the chance to do something amazing. Buy a special pair of our newly designed, bright orange laces and take a step to help end the pain of osteoporosis. It’s really that simple.
Just head over to www.laceupforbones.co.uk where you can take one really important step and buy a pair of orange laces for £3.50 (including postage and packing). That one step could help transform the lives of those with or at risk of osteoporosis.
That’s because every pair of orange laces bought, and every step taken moves us closer to a future without pain and suffering, for millions of people across the UK. We don’t know how long the journey is, or how many steps we need to take, just that we must keep going. And with your help, we can.
Osteoporosis Review is copyright of the National Osteoporosis Society. The Society does not charge for, and grants use without permission, for:
• Original authors wanting to reproduce figures or tables from their own work to publish in not-for-profit formatsor venues, provided that full acknowledgement of thesource appears in the new work
• Students wanting to reproduce or republish their workfor educational purposes
• Students using other authors’ material for their theses
• Photocopying up to five copies for personal use
• Multiple photocopies of articles for classroomuse by non-profit educational institutions; all suchreproduction must utilise institutionally ownedequipment for this purpose.
Use of copyrighted material requires proper citation. For all other uses, email [email protected] or call the Communications Department on 01761 473148.
Products and services advertised in Osteoporosis Review are not necessarily endorsed by the National Osteoporosis Society.
National Osteoporosis Society Camerton, Bath, BA2 0PJ Tel: 0845 130 3076. Helpline: 0845 450 0230. email: [email protected] www.nos.org.uk Registered charity No. 1102712 in England and Wales and No. SC039755 in Scotland.Registered company No. 4995013
Diary Dates
Osteoporosis Review 2016; Vol 24 No2 13
Update
Consultation responses under way from National Osteoporosis Society for NICE and others
Part of the work of the National Osteoporosis Society involves offering views and expert opinions to those writing reports, standards and guidelines produced by the NHS, NICE and a wide range of health organisations. This work ensures those making decisions about health take osteoporosis into account.
Our policy team is currently busy with consultation responses for a number of different organisations.
We are feeding into NICE’s work to develop Quality Standards on menopause, falls, osteoporosis and hip fracture (due for publication in November 2016.)
We are also submitting a response to the revised guidance for dentists relating to osteonecrosis of the jaw and dental treatment. See the Scottish Dental Clinical Effectiveness Programme’s Draft guidance on Oral Health Management of Patients Prescribed Anti-resorptive or Anti-angiogenic drugs.
Finally, we’re also feeding into a consultation process launched recently by The Commissioner for Older People for Northern Ireland, Eddie Lynch, in response to draft priorities for action.
Osteoporosis Conference 2016BirminghamNovember 7–9www.nos.org.uk/conference
The Institute of Osteopathy Annual ConferenceWindsorNovember 25th–27thwww.osteopathy.org
World Congress on Osteoporosis, osteoarthritis and musculoskeletal diseasesFlorence, Italy Date: 23-26 March 2017 www.wco-iof-esceo.org
8th International Conference on Children’sBone HealthWürzburg, Germany10-13 June 2017www.iccbh.org

Osteoporosis Review 2016; Vol 24 No214
EUGMS
Three quarters of all fractures occur in adults aged 65 years and over2. It is widely acknowledged that hip fracture confers a significant risk of dying or loss of independence, yet it is important to recognise the significant morbidity and mortality associated with other major osteoporotic fractures.
The challenge and complexity of managing the health needs of our ageing population is an important public health priority. However, there is no consensus on the most efficacious strategy for fracture prevention in older people.
The European Union Geriatric Medicine Society (EUGMS) mission to develop geriatric medicine within the European Union includes the promotion of evidence-based guidelines for preventative and treatment strategies for older people. This article is a review of the recent EUGMS statement on fracture prevention, and their recommendations for a strategy to address the main points that make up this debate1.
Falls prevention
International operational definitions and diagnostic criteria for assessing the risk of falling need to be established
There is no internationally agreed best practice model for assessing the falls risk of older people. There are well described risk factors for falls in people aged 75 and over; these include a history of a fall in the previous 12 months, fear of falling, and significant gait / muscle strength / balance problems 3–9. But the overall risk of falls is dependent on other more subjective factors which lead to a relationship between balance and gait and falls risk that is not linear10.These factors are complex to identify and affect a person’s degree of exposure to a situation that would put them at risk of falling.
For example, fall rates are higher in those who are able to rise from a chair but not stand unaided, and lowest in those who can neither rise from a chair nor stand unaided.
An awareness of the need for screening of older patients for risk of falling
The majority of falls in adults occur in older people, and older people are more likely to sustain an injury as a consequence of a fall; around 10% of falls result in fracture11. Of those living in the community, a third of people aged 65 years and over fall at least once a year, and this rises to half in those aged 80 years and over3,12.
The EUGMS endorse the 2010 American Geriatric Society / British Geriatrics Society Clinical Practice Guideline, which highlights the responsibility of healthcare professionals to ensure that older people under their care are asked at least annually about falls, with further evaluation to be organised if indicated.
Evidence-based measures – particularly evidence based community exercise fall prevention programmes – should be widely available to prevent non-vertebral fractures in older people at low or moderate risk of falling
Multicomponent exercise programmes have consistently demonstrate efficacy in reducing the incidence of serious falls and non-vertebral fractures (except hip fractures) in predominantly community-dwelling older people deemed to be at low to moderate risk of falls 5,13,14. The programmes described include progressive, challenging and regular exercises designed to improve balance and muscle strength.
Single interventions when applicable are effective in the prevention of falls, but the impact on
Fracture prevention in older adults: a brief summary of the European Union Geriatric Medicine Society (EUGMS) strategy1
Rachel Cowan, Tahir Masud, Nottingham University Hospitals NHS Trust
Osteoporosis Review 2016; Vol 24 No2 15
EUGMS
fracture risk is not clear13,15,16. Interventions include treatment of cataracts, cardiac pacing for carotid sinus hypersensitivity, correction of vitamin D deficiency, and improving the safety of indoor activities and outdoor walking environment.
People at high risk of falls should be able to access individually tailored multifactorial measures based on a comprehensive geriatric assessment
Single targeted interventions seem less effective; in older nursing home residents, vitamin D supplementation is the only single intervention that has been shown to reduce falls17.
A multifactorial and multidisciplinary approach to identify and address modifiable risk factors for falls is potentially more appropriate in older people at high risk of falling10,17,18. High falls risk is often seen in the context of frailty; it has been demonstrated that the multifactorial approach in this group can improve the ability to live independently19.
Bone health
In individuals at risk of fracture (i.e. at risk of falling, predisposition to bone fragility) bone mineral density should be ascertained by dual-energy X-ray absorptiometry (DXA), ideally combined with an assessment for vertebral fractures
Osteoporosis and falls risk are the highest risk factors for non-vertebral fractures in post-menopausal women20. The prevalence of osteoporosis increases in those with frailty syndrome, for which recurrent falls is a marker; sarcopenia, low body weight and poor mobility are risk factors for both falls and osteoporosis. Therefore, the presence of osteoporosis should be ascertained both in people with conditions that predispose them to low bone mineral density and in those at risk of falls, and vice versa.
Vertebral compression fractures are common and often go unrecognised in older people. EUGMS emphasises the need for medical staff to identify the need to organise X-ray examination in patients presenting with back pain or noted to have
significant loss of height (>5cm) or kyphosis, and the opportunity for incidental vertebral fracture reporting on radiological investigations to trigger a referral to fracture liaison services.
Treatments acting on bone metabolism (TABM) should be considered after a careful risk/benefit assessment in patients at high risk of fracture
Osteoporosis is currently defined by bone densitometry, when the bone mineral density (BMD) is 2.5 standard deviations or more below that of the mean level for a young adult reference population (T score of -2.5 or less at the lumbar spine, hip or distal radius). The measurement of BMD is prone to artefactual error, however, particularly in the lumbar spine where osteoarthrosis and aortic calcification (which are radiological findings associated with advancing age) make this calculation less reliable21.
TABM – which include anti-resorptive agents (bisphosphonates, denosumab) and anabolic therapy (teriparatide) – are effective in preventing major fractures in people with a T score of -2.5 or less at the spine or hip, or after a hip fracture 22. There is continued debate as to the cost effectiveness and efficacy of pharmacological management outside of this population.
Fracture prediction tools (including the FRAX tool, the Garvan Fracture Risk calculator or the Q-fracture Risk Calculator) take into account other risk factors for bone fragility in association with BMD (including history of fracture, low body weight, parental history of hip fracture, use of glucocorticoids, excessive alcohol consumption, diseases with bone adverse effects). The indication for treatments acting on bone metabolism must be considered on an individual patient-centred basis, dependent on a combination of a diagnosis (or presumed diagnosis) of osteoporosis after fragility fracture or DXA, other risk factors for fractures and risk of falls.
TABM should not be initiated when the life expectancy is less than 6-12 months, the minimum time needed for drugs to be effective in fracture prevention

Osteoporosis Review 2016; Vol 24 No216
EUGMS
Fracture Liaison Services
The pathway from identification of a fragility fracture to assessment of future falls and fracture risk to consideration of the risk/benefit ratio of treatment for osteoporosis is complex. The EUGMS supports the International Osteoporosis Foundation recommendation that the presentation with fracture in those aged 65 years and over should prompt a referral to a fracture liaison service23. This should be linked with geriatric medicine services to offer a combined falls risk assessment, and is a care model that has been shown to be cost effective24.
Conclusion
The EUGMS recommend a comprehensive and multidisciplinary fracture prevention strategy in individuals aged 65 and over which has three fundamental concepts. Firstly, there is a need to ensure better education (for both the general population and healthcare professionals) with respect to lifestyle measures and medical approaches to optimise bone health and prevent falls. Secondly, in both primary and secondary care, there must be a focus on screening for and optimising management of osteoporosis in those at increased risk of falls (and vice versa). Thirdly, the importance of integrating services is highlighted, with an emphasis on the strong collaboration between fracture liaison services, geriatric medicine and primary care.
References1. Blain H, Masud T, Dargent-Molina P et al. A comprehensive fracture
prevention strategy in older adults: the European Union Geriatric MedicineSociety (EUGMS) statement. Aging Clin Exp Res (2016) 28:797-803
2. Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726-1733.
3. Tinetti ME (2003) Preventing falls in elderly persons. N Engl J Med 348:42-49.
4. Stevens JA, Phelan EA (2013) Development of STEADI: a fall preventionresource for health care providers. Health Promot Pract 14:706-714.
5. El-Khoury F, Cassou B, Latouche A et al (2015) Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75–85 living in community: Ossébo randomised controlled trial. BMJ 351:h3830.
6. Wagner H, Melhus H, Gedeborg R et al (2009) Simply ask them about theirbalance—future fracture risk in a nationwide cohort study of twins. Am J Epidemiol 169:143-149.
7. Caillet P, Klemm S, Ducher M et al (2015) Hip fracture in the elderly: a re-analysis of the EPIDOS study with causal Bayesian networks. PLoS ONE 10:e0120125.
8. Furrer R, van Schoor NM, de Haan A et al (2014) Gender-specific associations between physical functioning, bone quality, and fracture risk in older people. Calcif Tissue Int 94:522-530.
9. Lundin H, Sääf M, Strender LE et al (2014) One-leg standing time and hip-fracture prediction. Osteoporos Int 25:1305-1311.
10. Lord SR, March LM, Cameron ID et al (2003) Differing risk factors for falls in nursing home and intermediate-care residents who can and cannot stand unaided. Am Geriatric Soc 51:1645-50.
11. Campbell AJ, Borrie MJ, Spears GF et al (1990) Circumstances and consequences of falls experienced by a community population 70 years and over during a prospective study. Age Ageing 19:136-141.
12. O’Laughlin JL, Robitaille Y, Boivin JF et al (1993) Incidence of and risk factors for falls and injurious falls among the community-dwelling elderly.Am J Epidemiol 137:342-354.
13. Gillespie LD, Robertson MC, Gillespie WJ et al (2012) Interventions for preventing falls in older people living in the community. Cochrane DatabaseSyst Rev 9:CD007146
14. El-Khoury F, Cassou B, Charles MA et al (2013) The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: systematic review and meta-analysis of randomised controlled trials. BMJ 347:f6234
15. Keall MD, Pierse N, Howden-Chapman P et al (2015) Home modifications toreduce injuries from falls in the home injury prevention intervention (HIPI) study: a cluster-randomised controlled trial. Lancet 385:231-238.
16. Li W, Procter-Gray E, Lipsitz LA et al (2014) Utilitarian walking, neighborhoodenvironment, and risk of outdoor falls among older adults. Am J Public Health 104:e30-e37.
17. Cameron ID, Gillespie LD, Robertson MC et al (2012) Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev 9:CD005465.
18. Stubbs B, Brefka S, Denkinger MD (2015) What works to prevent falls in community-dwelling older adults? Umbrella review of meta-analyses of randomized controlled trials. Phys Ther 95:1095-1110.
19. Beswick AD, Rees K, Dieppe P et al (2008) Complex interventions to improvephysical function and maintain independent living in elderly people: a systematic review and meta-analysis. Lancet 371:725-735.
20. Blain H, Rolland Y, Beauchet O et al (2014) Groupe de recherche et d’information sur les ostéoporoses et la Société française de gérontologie et gériatrie. Usefulness of bone density measurement in fallers. Joint Bone Spine 81:403-408.
21. Masud T, Langley S, Wiltshire P et al (1993) Effect of spinal osteophytosis on bone mineral density measurements in vertebral osteoporosis. BMJ 307:172-173.
22. Crandall CJ, Newberry SJ, Diamant A et al (2014) Comparative effectivenessof pharmacologic treatments to prevent fractures: an updated systematic review. Ann Intern Med 161:711-723.
23. Javaid MK, Kyer C, Mitchell PJ et al (2015) IOF Fracture Working Group; EXCO. Effective secondary fracture prevention: implementation of a global benchmarking of clinical quality using the IOF Capture the Fracture® Best Practice Framework tool. Osteoporos Int 26:2573-2578.
24. Yong JH, Masucci L, Hoch JS, Sujic R, Beaton D (2016) Cost-effectivenessof a fracture liaison service-a real-world evaluation after 6 years of service provision. Osteoporos Int 27:231-240.
Osteoporosis Review 2016; Vol 24 No2 17
Bone health in people living with HIV
Bone health in people living with HIVProfessor Karen Walker –Bone Professor of Occupational Rheumatology
MRC Lifecourse Epidemiology Unit, Southampton General Hospital
According to recent 2016 data, there are an estimated 36.7 million people living with HIV infection (PLWHIV) worldwide1. Since the recognition of the human immunodeficiency virus (HIV) in the 1980s, unprecedented worldwide collaboration enabled the rapid development of anti-retroviral therapy (ART) which, with good compliance, markedly reduces mortality so that life expectancy approaches that of the general population2. Importantly also, when ART effectively suppresses viral activity, it significantly attenuates the risk of transmission of the virus between individuals. There are now six classes of ART, defined by their mode of action against the virus, and >25 different drugs used in various combinations (Table 1).
However, the development of ART has brought new challenges: since the majority of the infections are in sub-Saharan Africa and other resource-poor nations, fewer than half (46%) of those infected with HIV receive ART1 and consequently 66% of the 2.1 million new infections annually occurred in this part of the world1. Secondly, in countries where resources for ART are available, there is a rapidly growing population of PLWHIV aged >50 years. It is currently estimated that over 33% of those infected in Europe are aged >50 years and it has been projected that this will increase to more than 70% by 20303. As the numbers of PLWHIV aged >50 years has grown, so has recognition of associated comorbidities in this population
causing a phenotype sometimes characterised as ‘premature ageing’ with increased risk of cardiovascular disease, diabetes mellitus, liver and renal disease, malignancies, cognitive dysfunction and osteoporosis4. The focus of this review is on bone health among PLWHIV concentrating on opportunities for prevention or treatment.
Systemic inflammation
Chronic inflammation and persistently elevated cytokines, such as tumor necrosis factor (TNFɑ) or interleukins (Il-1 and Il-6),activate proteins including receptor activator of nuclear factor kappa-B ligand (RANKL) which leads to osteoclast activation and bone resorption5. Acute HIV infection is associated with marked systemic inflammation and cytokine activation and whilst the virus remains unsuppressed, chronic systemic inflammation remains unchecked likely leading to significant widespread skeletal effects. Laboratory studies have shown that systemic inflammation, as measured by cytokine levels, remains detectable after commencement of ART and remains persistent even after effective suppression of viral replication by the ART and that this is associated with bone turnover markers5. This chronic systemic inflammation despite viral suppression is under intensive investigation as it is also implicated in the other non-AIDS comorbidities and ’premature ageing’.
The impact of ART on bone health
Soon after the advent of ART, a number of case-control studies were published showing a much increased risk of osteopenia and osteoporosis among HIV-infected cases as compared with uninfected controls. In a meta-analysis, a pooled odds ratio of 6.4 for the risk of low bone density and 3.7 for the risk of osteoporosis was estimated among PLWHIV6. Their results also implicated ART (predominantly protease inhibitors, which were in widespread use at

Osteoporosis Review 2016; Vol 24 No218
Bone health in people living with HIV
the time) suggesting that the risk of low bone mineral density was 2.5-fold higher among ART treated patients as compared with treatment naïve patients. Since then, there have been many more studies published with longitudinal data mainly available only from ART trials. The results fairly consistently demonstrate a loss of BMD at the spine and hip after initiation of ART ranging between 2-6% with stabilisation of bone loss thereafter. Moreover, the SMART sub-study, which compared continuous ART with intermittent therapy found that the only health measure which improved by intermittent, as compared with continuous, therapy was BMD7. Although the bone loss patterns are consistent, tenofovir disoproxil (TDF) regimens have been associated with higher rates of bone loss. The mechanism of this is poorly understood but TDF can cause renal complications, phosphaturia and frank Fanconi syndrome and it is postulated that this may be at least part of the mechanism8. TDF containing regimens are also prescribed for HIV pre-exposure prophylaxis (PrEP) among patients at risk of infection. In this setting, the TDF is associated with a measurable, although likely clinically insignificant bone loss.
It appears that some of the more modern therapies cause less bone loss, for example the integrase inhibitor raltegravir has been shown to cause minimal negative effects on BMD. Moreover, the recently-licensed pro-drug of tenofovir, tenofovir alefanamide (TAF) has been shown to cause less bone loss when initiated in a combination with elvitegravir, cobicistat and emtricitabine (E/C/F/TAF) as a single tablet and even to cause increases in BMD among patients switching from TDF-containing regimens to E/C/F/TAF9.
The mechanism of bone loss in early ART treatment is poorly understood (Table 1). Studies including bone turnover markers suggest uncoupling of bone resorption and formation perhaps caused by direct drug effects on bone
cells or bone-cell signalling. Efavirenz, and some protease inhibitors, affect vitamin D metabolism and may increase vitamin D deficiency. Immune reconstitution after initiation of ART leads to a rapid influx of memory T-cells that have been trapped within inflamed lymphatic tissue followed by a slow recovery of naïve T-cells after re-distribution to the periphery and new thymic production. Immune reconstitution as measured by changes in CD4 + cell recovery was recently found to be associated with markers of bone resorption10.
Risk factors
Conventional risk factors for osteoporosis in the general population remain important in the HIV positive population and are often found to be more prevalent in PLWHIV. Age, cigarette smoking, excess alcohol consumption, opioid abuse, low body mass index, reduced levels of physical activity, comorbidities (liver and renal disease), hypogonadism and vitamin D deficiency can all play a role in osteoporosis among PLWHIV. Moreover, the association of HIV with other comorbidities increases the risk of exposure to drugs associated with bone effects such as glucocorticoids and proton pump inhibitors. Additionally, co-infection with other bloodbourne viruses including hepatitis C appears to significantly increase the risk of osteoporosis11.
Fracture in HIV
To date, studies of fracture in HIV are limited to Australia, Europe and USA. They seem to show a consistent but modest increased risk of fractures in PLWHIV12. Risk factors for fracture include alcohol abuse, injectable drug use, smoking, low body mass index, older age, white race, lower nadir CD4+ count and hepatitis co-infection. Some, but not all, studies suggest ART, and possibly TDF, is an independent risk factor for fracture9.

Osteoporosis Review 2016; Vol 24 No2 19
Bone health in people living with HIV
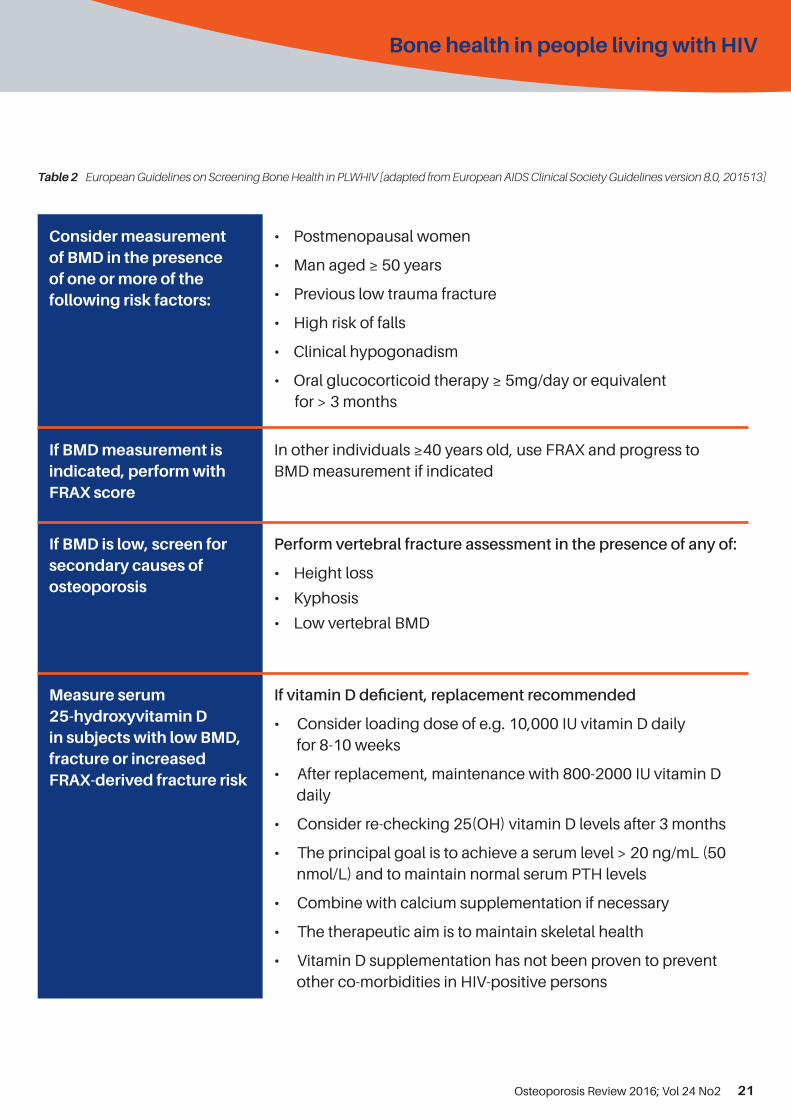
Assessment of fracture risk
The European AIDS Clinical Society (EACS) has produced guidance on screening PLWHIV for bone disease, measurement of vitamin D and management of hypovitaminosis D13 (Table 2). Although FRAX is recommended, there is evidence that FRAX under-estimates absolute fracture risk in PLWHIV and in practice, most clinicians tick the “secondary causes of osteoporosis” box in the FRAX algorithm although this has not been demonstrated to mitigate the under-estimation completely.
Treatment of HIV-associated osteoporosis
As with all patients, lifestyle advice is recommended including smoking cessation, safe alcohol consumption and the importance of diet (particularly dietary calcium intake) and physical activity levels. An assessment of falls risk is also important, particularly as both ART and the virus itself are associated with peripheral neuropathy. To date, there has been insufficient evidence to recommend ‘safer’ ART regimens for bone health unless in the clinical presentation of overt phosphate deficiency/Fanconi syndrome associated with TDF.
There are some data on treating osteoporosis in PLWHIV with calcium and vitamin D, Alendronate, testosterone and intravenous zoledronate although none of these studies used fracture as the clinical endpoint14. The bisphosphonates alendronate and intravenous zoledronate have been shown to effectively increase bone mass in PLWHIV and are recommended with calcium and vitamin D supplementation if dietary calcium intake is inadequate and/or there is evidence of vitamin D insufficiency.
In patients starting ART for the first time, there is evidence that calcium and vitamin D supplementation attenuates bone loss15. Very recently, a single-centre proof-of-concept
study showed that intravenous zoledronate 5g administered at the start of ART was also effective in prevention of the early bone loss associated with ART16. However, it is unclear whether the risk: safety benefit favours the wide recommendation of this for all patients starting ART.
Future research needs
There is accumulating evidence that people infected vertically or during their adolescent years have measureable impact on their bone health and possibly reduced peak bone mass, potentially leading to higher risk of fracture later in life. There are limited data in these patients and more research is required. Worldwide, PLWHIV are considerably more likely to be male than female. As a result, much of the research, and particularly the clinical trials, have included considerably more men than women. There are a few more studies of the effects of HIV on bone health in women emerging but more research is urgently required as post-menopausal women with HIV will be the group at greatest risk of osteoporotic fracture, particularly since HIV is thought to be associated with sub-optimal gonadal function and early menopause.
Please turn the page for tables 1 and 2.
Conflict of interest statement
The author has received consultancy and speaking fees from Gilead.

Osteoporosis Review 2016; Vol 24 No220
Bone health in people living with HIV
Table 1 Summary of current anti-retroviral therapies (ART) and what is known of their effects on bone health
ClassExamples of drugs in this class
Drug-specific bone effects where described*
Non-nucleoside reverse transcriptase inhibitors (NNRTIs)
EfavirenzMay affect vitamin D metabolism – risk of vitamin D deficiency increased
Etravirine
Nevirapine
Rilpivarine
Nucleoside reverse transcriptase inhibitors (NRTIs)
Abacavir
Didanosine
Emtricitabine
Lamivudine
Stavudine
Tenofovir disoproxil fumarate (TDF)
Implicated in higher rates of bone loss on initiation but not in fracture risk
Tenofovir alefanamide (TAF)
Bone density maintained when used in treatment-naïve patients in combination with elvitegravir /cobicistat / emtricitabine (E/C/F/TAF)
Zidovudine
Protease inhibitors (PIs)Some protease inhibitors affect vitamin D metabolism and may increase risk of vitamin D deficiency
AtazanavirDarunavirFosamprenavirIndinavirLopinavir/ritonavirNelfinavir
RitonavirIncreases bio-availability of glucocorticoids administered by any route – increased risk of steroid-induced osteoporosis
Saquinavir
Tipranavir
Fusion inhibitors Enfurvitide
Chemokine Coreceptor (CCR5) antagonists (also called entry inhibitors)
Maraviroc
Integrase strand transfer inhibitors
DolutegravirElvitegravir
Raltegravir
Pharmacokinetic enhancers Cobicistat Increases bio-availability of glucocorticoids administered by any route – increased risk of steroid-induced osteoporosis
*ART is used in combinations although increasingly they are available in a single-tablet formulation. Where longitudinal dataare available (usually in trials), most combinations are associated with loss of BMD 2-6% over the first 1-2 years after initiation and stabilisation thereafter
Osteoporosis Review 2016; Vol 24 No2 21
Bone health in people living with HIV
Table 2 European Guidelines on Screening Bone Health in PLWHIV [adapted from European AIDS Clinical Society Guidelines version 8.0, 201513]
Consider measurement of BMD in the presence of one or more of the following risk factors:
• Postmenopausal women
• Man aged ≥ 50 years
• Previous low trauma fracture
• High risk of falls
• Clinical hypogonadism
• Oral glucocorticoid therapy ≥ 5mg/day or equivalentfor > 3 months
If BMD measurement is indicated, perform with FRAX score
In other individuals ≥40 years old, use FRAX and progress to BMD measurement if indicated
If BMD is low, screen for secondary causes of osteoporosis
Perform vertebral fracture assessment in the presence of any of:
• Height loss
• Kyphosis
• Low vertebral BMD
Measure serum 25-hydroxyvitamin D in subjects with low BMD, fracture or increased FRAX-derived fracture risk
If vitamin D deficient, replacement recommended
• Consider loading dose of e.g. 10,000 IU vitamin D dailyfor 8-10 weeks
• After replacement, maintenance with 800-2000 IU vitamin Ddaily
• Consider re-checking 25(OH) vitamin D levels after 3 months
• The principal goal is to achieve a serum level > 20 ng/mL (50nmol/L) and to maintain normal serum PTH levels
• Combine with calcium supplementation if necessary
• The therapeutic aim is to maintain skeletal health
• Vitamin D supplementation has not been proven to preventother co-morbidities in HIV-positive persons

Osteoporosis Review 2016; Vol 24 No222
Bone health in people living with HIV
Key Points:
• Advances in HIV treatment have ledto a rapidly-growing population ofpeople living with HIV (PLWHIV) aged>50 years
• Several ‘ageing’ comorbidities havebeen described in PLWHIV includingosteoporosis and fracture
• Conventional risk factors play a role inadverse bone health but anti-retroviraltherapy, systemic inflammation andHIV itself have negative bone effects
• More research is needed amongpeople infected vertically or inadolescent life and post-menopausalwomen, as these are the groupslikely to have the biggest risk ofosteoporotic fracture in the future
References
1. World Health Organisation Global AIDS Update,2016. http://www.who.int/hiv/pub/arv/global-AIDS-update-2016_en.pdf?ua=1 (last accessed8.8.2016)
2. May MT, Vehreschild JJ, Trickey A, et al.Mortality According to CD4 Count at Start ofCombination Antiretroviral Therapy Among HIV-infected Patients Followed for up to 15 YearsAfter Start of Treatment: Collaborative CohortStudy. Clin Infect Dis. 2016 Mar 29. pii: ciw183.[Epub ahead of print]
3. Smit M, Brinkman K, Geerlings S et al. Futurechallenges for clinical care of an ageingpopulation infected with HIV: a modellingstudy. Lancet Infect Dis. 2015 Jul;15(7):810-8.
4. Calcagno A, Nozza S, Muss C, et al. Ageingwith HIV: a multidisciplinary review. Infection2015;43:509-22.
5. de Menezes EG, Machado AA, Barbosa F, de PaulaFJ, Navarro AM. Bone metabolism dysfunctionmediated by the increase of proinflammatorycytokines in chronic HIV infection. J Bone MinerMetab 2016. DOI 10.1007/s00774-016-0749-8[E-pub ahead of print].
6. Brown TT, Qaqish RB. Antiretroviral therapy and theprevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS. 2006; 20:2165-74.
7. Grund B, Peng G, Gibert CL, et al. Continuousantiretroviral therapy decreases bone mineraldensity. AIDS 2009; 23:1519–1529.
8. Casado JL, Santuiste C, Vazquez M, et al. Bonemineral density decline according to renal tubulardysfunction and phosphaturia in tenofovir-exposedHIV-infected patients. AIDS 2016;30:1423-31.
9. Compston J. HIV infection and bone disease. J IntMed 2016; doi:10.1111/joim.12520. [Epub ahead ofprint].
10. Ofotokun I, Titanji K, Vikulina T, et al. Role of T-cellreconstitution in HIV-1 antiretroviral therapy-induced bone loss. Nat Commun 2015;6:8282.
11. Bedimon R, Maalouf NM, Lo Re V 3rd. Hepatitis Cvirus coinfection as a risk factor for osteoporosis andfracture. Curr Opin HIV AIDS 2016;11:285-93.
12. Shiau S1, Broun EC, Arpadi SM, Yin MT. Incidentfractures in HIV-infected individuals: a systematicreview and meta-analysis. AIDS. 2013 Jul31;27(12):1949-57
13. European AIDS Clinical Society Guidelines version8.0, 2015. Available at: http://www.eacsociety.org/files/guidelines_8_0-english_web.pdf (last accessed10.8.16)
14. Negredo E, Warriner AH. Pharmacologicapproaches to the prevention and management oflow bone mineral density in HIV-infected patients.Curr Opin HIV AIDS 2016;11:351-7.
15. Overton ET, Chan ES, Brown TT, et al. High-dosevitamin D and calcium attenuates bone loss withantiretroviral therapy initiation. Ann Intern Med2015; 162:815-24.
16. Ofotokun I, Titanji K, Lahiri CD, et al. A Single-dose Zoledronic Acid Infusion PreventsAntiretroviral Therapy-induced Bone Loss inTreatment-naive HIV-infected Patients: A Phase IIbTrial. Clin Infect Dis. 2016 May 18. pii: ciw331. [Epubahead of print]
Osteoporosis Review 2016; Vol 24 No2 23
Inflammatory arthritis
Introduction
This article aims to summarise the epidemiology and aetiology of rheumatoid arthritis and osteoporosis, and to describe the reasons patients with rheumatoid arthritis are at risk of osteoporosis. We will discuss appropriate assessment of bone disease in rheumatoid arthritis patients, and go on to discuss current treatment options and potential treatment options for the future.
Background
Rheumatoid arthritis (RA) is the most common inflammatory arthritis and an important cause of morbidity and mortality. This often disabling disease has a prevalence of approximately 1% among adults in most populations (1). The aetiology of RA is complex and both genetic and environmental factors contribute to development of the disease. The presentation includes pain, stiffness, swelling and functional impairment, general malaise and profound fatigue. The main aim of management of RA is to control the symptoms and signs of disease, maintain function, address complications and associated comorbidity and evaluate the impact of the condition on the patient’s quality of life. The long-term prognosis of RA has improved significantly with the introduction of effective medications and as the result of regular adjustment of treatments aiming to achieve disease remission; however, comorbidities associated with the disease may lead to functional decline and negatively impact the life span of patients with RA (2). The causes
of some of the comorbidities associated with RA are multi-factorial and include the effects of medication (in particular, the effects of glucocorticoids), lifestyle factors and chronically active inflammation (3-5).
Osteoporosis is the main extra – articular complication of RA. It is a systemic disorder characterized by low bone mass and microarchitectural deterioration of bone tissue with a consequent increase in bone fragility and susceptibility to fracture (6). Osteoporosis has a significant impact on public health through the increased morbidity, mortality, and economic costs associated with fractures. Epidemiological studies from North America have estimated the remaining lifetime risk of fragility hip fracture to be 17.5% among white women aged 50 years and 6% for men; for clinically diagnosed vertebral fracture figures were 15.6 % and 5%, and for wrist fracture 16% and 2.5% respectively (7). These findings were consistent with data from the Clinical Practice Research Datalink from the UK (8), suggesting that almost one in two women 50 years old will have an osteoporotic fracture in their remaining lifetime; the figure for men is one in five. The risk of hip fracture, vertebral fracture and of other fractures is further increased in patients with RA (9, 10). RA has therefore been incorporated as a dichotomous predictor in the WHO FRAX algorithm for predicting the 10-year risk of hip or major osteoporotic fracture (11). The underlying reasons for the increased fracture risk in RA are complex and the remainder of this review will provide an overview of how bone health is affected in this patient group.
Osteoporosis in Patients With Rheumatoid ArthritisAlice Mason, University Hospital Southampton, Anna Litwic, MRC Lifecourse Epidemiology Unit, University of Southampton

Osteoporosis Review 2016; Vol 24 No224
Inflammatory arthritis
Causes of osteoporosis in Rheumatoid Arthritis
As discussed above, having RA has been shown to be an independent risk factor for osteoporosis. Whilst osteoporosis can result as a direct result of disease there are several other independent risk factors, such as steroid use and immobility, which can also make osteoporosis more prevalent in the RA population. When looking at the direct result of the disease process, Goldring et al. described three forms of bone disease in RA. Inflammation in RA can lead to focal bone loss affecting the immediate subchondral bone and bone at the joint margins; periarticular osteopenia adjacent to inflamed joints; and generalised osteoporosis involving the axial and appendicular skeleton (12). All these mechanisms of loss of bone density involve an imbalance between the rate of bone resorption and formation. It is thought that focal bone loss, periarticular osteopenia and generalised osteoporosis share common pathways. In RA activated t cells within the synovium express receptor activator of nuclear factor kappa B ligand (RANKL) and produce cytokines, in particular tumour necrosis factor alpha (TNF alpha), interleukin-1 (IL-1), interleukin-17 (IL-17) and prostaglandins. This leads to stimulation of osteoclast precursors which mature into fully functioning osteoclasts, thereby leading to bone resorption (13, 14). Several inflammatory diseases, Systemic Lupus Erythematosis, Chronic Obstructive Pulmonary Disease and Inflammatory Bowel Disease have been associated with osteoporosis supporting the idea of a link between chronic inflammation and generalised osteoclast activation (15).
The amount of inflammation appears to have a quantitative effect on the degree of bone loss, with disease duration and activity having both been associated with reduced bone mass (16). Interestingly RA leads to a more marked loss of the peripheral bone density whilst maintaining
relatively well preserved axial bone density which is likely due to the result of localised inflammation in the joints.
The use of glucocorticosteroids both reduces bone formation and increases bone resorption. As well as this glucocorticosteroids can reduce calcium absorption from the gut and can induce renal calcium excretion. Fracture risk increases 3-6 months after glucocorticosteoids are commenced and returns to baseline after cessation (17). Many RA patients will be on regular or have frequent courses glucocorticosteoids, usually prednisolone putting them at further increased risk of osteoporosis. Glucocorticosteroids should be given at the lowest dose possible for the shortest duration.
There are other reasons a patient with RA may have increased risk of osteoporosis; reduced mobility due to painful joints or loss of joint function, fatigue, poor nutritional status and sarcopenia all contribute to osteoporosis risk.
Assessment
It is important to consider osteoporosis early in rheumatoid arthritis. Shibuya et al. showed that bone density loss began early in the disease process and thus should be considered from the point of diagnosis onwards (18). As outlined above there is strong evidence that decrease in bone mass is associated with fragility fracture and this comes with significant morbidy and mortality. NICE guidance suggests fracture risk assessment of all patients over the age of 50 with a secondary causes of osteoporosis including RA. They recommend assessment of all patients at any age with any major risk factor including steroid use (19). It is then a clinical decision as to whether a DXA scan should be performed and the WHO FRAX tool can be used to help guide the decision process. The BSR guidelines suggest all persons 65 years or older with RA taking corticosteroids for 12 weeks or

Osteoporosis Review 2016; Vol 24 No2 25
Inflammatory arthritis
more should be offered bone protective therapy. Persons under 65 with no previous fragility fracture should be offered DXA scanning to assess the risk of osteoporosis. If, in persons under 65 with rheumatoid arthritis, there is a previous fragility fracture or incident fracture during glucocorticoid therapy, bone protective therapy should be considered (20). There is no direct guidance on the time intervals between fracture risk assessment.
Treatment
Control of inflammation is of the upmost importance to reduce production of cytokines. Commencing and escalating RA treatments promptly are essential in achieving this. New treat to target guidance for RA may be having a beneficial impact on the bone mass of newly diagnosed patients.
Osteoporosis in RA is due to over activity of osteoclasts and therefore can be treated with antiresorptive therapy. Bisphosphates are well established as a treatment for osteoporosis in RA and denosumab is also now widely available (21). Bispohosphonates have been also been shown to be beneficial in steroid induced osteoporosis (22). In addition supplementation of calcium and vitamin D is also advised. The use of hormone replacement therapy in post-menopausal females with RA has been shown to improve bone mineral density (23). The use of teriparatide has been promising and should be considered where regional guidelines allow (24).
The observation that focal bone erosions and periarticular bone degradation can be as a result of cytokine release which stimulates recruitment and activation of osteoclasts leads to the theory that inhibiting these cytokines could be a potential treatment for osteoporosis prevention in RA. Some studies have suggested that the use of anti-TNF can slow the loss of bone mass (25). There are ongoing studies looking at anti-TNF and IL-1 receptor antagonists in RA as new
potential treatments for osteoporosis secondary to inflammation. Other newer medications such as cathepsin K inhibitors, anti sclerostin antibodies and parathyroid hormone related proteins have yet to be assessed in rheumatoid arthritis but may prove to be useful therapeutic alternatives in the future. Other studies are underway looking at 3 dimensional imaging techniques of bone, such as high resolution peripheral quantitative computed tomography to better our understanding of the bone’s macrostructure, microstructure, and strength in patients with RA and inflammatory disease.
Conclusion
Chronic inflammation has been shown to be linked to osteoporosis via osteoclast activation. In RA and other diseases of chronic inflammation clinicians should be aware of the associated risk and consider further assessment with DEXA if appropriate. Controlling inflammation is crucial in helping prevent loss of bone mass. If patients with RA have a diagnosis of osteoporosis, treatment with antiresorptive therapies has been shown to be affective and potential new treatment options are on the horizon.

Fracture Liaison Service Champions Network
The FLS Champions Network has three main aims:
• To support the development of FLS across the UK through a collective network of knowledge and expertise, sharing best practice in FLS and secondary fracture prevention.
• To ensure those working in FLS remain up-to-date with all relevant work programmes regarding FLS and secondary fracture prevention across the UK.
• To provide the opportunity to communicate directly with the National Osteoporosis Society and the relevant resources we provide.
For further information email: [email protected]
Join the network at: www.nos.org.uk/champions
Your opportunity to share and gain knowlege, expertise and best practice in FLS and secondary fracture prevention, and support the roll-out of FLS across the UK.
FLS Champions A4.indd 1 19/05/2016 14:54:14
Osteoporosis Review 2016; Vol 24 No226
Inflammatory arthritis
References
1. Gibofsky A. Overview of epidemiology, pathophysiology,and diagnosisof rheumatoid arthritis. The Americanjournal of managed care. 2012;18(13 Suppl):S295-302.
2. Dougados M, Soubrier M, Antunez A, Balint P, BalsaA, Buch MH, et al. Prevalence of comorbidities inrheumatoid arthritis and evaluation of their monitoring:results of an international, cross-sectional study(COMORA). Ann Rheum Dis. 2014;73(1):62-8.
3. Liao KP, Solomon DH. Traditional cardiovascularrisk factors, inflammation and cardiovascular risk inrheumatoid arthritis. Rheumatology (Oxford, England).2013;52(1):45-52.
4. Wotton CJ, Goldacre MJ. Risk of invasive pneumococcaldisease in people admitted to hospital with selectedimmune-mediated diseases: record linkage cohortanalyses. Journal of epidemiology and communityhealth. 2012;66(12):1177-81.
5. Solomon DH, Kremer J, Curtis JR, Hochberg MC, ReedG, Tsao P, et al. Explaining the cardiovascular riskassociated with rheumatoid arthritis: traditional riskfactors versus markers of rheumatoid arthritis severity.Ann Rheum Dis. 2010;69(11):1920-5.
6. Consensus development conference: prophylaxis andtreatment of osteoporosis. The American journal ofmedicine. 1991;90(1):107-10.
7. Office of the Surgeon G. Reports of the Surgeon General.Bone Health and Osteoporosis: A Report of the SurgeonGeneral. Rockville (MD): Office of the Surgeon General(US); 2004.
8. Curtis EM, van der Velde R, Moon RJ, van den Bergh JP,Geusens P, de Vries F, et al. Epidemiology of fractures inthe United Kingdom 1988-2012: Variation with age, sex,geography, ethnicity and socioeconomic status. Bone.2016;87:19-26.
9. van Staa TP, Geusens P, Bijlsma JW, Leufkens HG,Cooper C. Clinical assessment of the long-term risk offracture in patients with rheumatoid arthritis. ArthritisRheum. 2006;54(10):3104-12.
10. Orstavik RE, Haugeberg G, Mowinckel P, Hoiseth A, UhligT, Falch JA, et al. Vertebral deformities in rheumatoidarthritis: a comparison with population-based controls.Archives of internal medicine. 2004;164(4):420-5.
11. Kanis JA, Oden A, Johnell O, Johansson H, De Laet C,Brown J, et al. The use of clinical risk factors enhancesthe performance of BMD in the prediction of hip andosteoporotic fractures in men and women. Osteoporosisinternational : a journal established as result ofcooperation between the European Foundation forOsteoporosis and the National Osteoporosis Foundationof the USA. 2007;18(8):1033-46.
12. Goldring SR, Gravallese EM: Mechanisms of bone lossin inflammatory arthritis: diagnosis and therapeuticimplications. Arthritis Res 2000;2:33-37.
13. Gillespie MT. Impact of cytokines and T lymphocytesupon osteoclast differentiation and function. Arthritis ResTher. 2007;9:103.
14. Schett G, Teitelbaum SL. Osteoclasts and Arthritis. JBone Miner Res. 2009;24:1142-1146.
15. Mundy GR. Osteoporosis and inflammation. Nutr Rev.2007;65:147-51.
16. Gough AK, Lilley J, Eyre S, Holdin R, Emery P.Generalized bone loss in patients with rheumatoidarthritis. Lancet. 1994;344:23-27.
17. Gregório LH, Lacativa PG, Melazzi AC, Russo LA.Glucocorticoid-induced osteoporosis. Arq BrasEndocrinol Metab. 2006;50(4):793-801.
18. Shibuya K, Hagino H, Morio Y, et al. Cross-sectionaland longitudinal study of osteoporosis in patients withrheumatoid arthritis. Clin Rheumatol 2002;21:150-158.
19. National Institute for Health and Care Excellence (NICE)(2012). Osteoporosis: Assessing the Risk of FragilityFracture. Available at: https://www.nice.org.uk/guidance/cg146?unlid
20. British Society of Rheumatology (BSR). Guidelines onStandards of Care for Persons with Rheumatoid Arthritis(2005). Available at: http://www.rheumatology.org.uk/includes/documents/cm_docs/2009/s/standards_of_care_for_persons_with_rheumatoid_arthritis.pdf
21. Haugeberg G, Orstavik R, Uhlig T, et al. Bone lossin patients with rheumatoid arthritis: results from apopulation based cohort of 366 patients followed overtwo years. Arthritis Rheum 2002;46:1720-1728.
22. Gregório LH, Lacativa PG, Melazzi AC, Russo LA.Glucocorticoid-induced osteoporosis. Arq BrasEndocrinol Metab. 2006;50793-801.
23 MacDonald AG, Murphy EA, Capell HA, Bankowska UZ, Ralsoton SH. Effects of hormone replacement therapy in rheumatoid arthritis: a double blind placebo-controlled study. Ann Rheum Dis. 1994;53: 54-57.
24. Ebina K et al. Comparison of the effect of 18-month dailyteriparatide administration on patients with rheumatoidarthritis and postmenopausal osteoporosis patients.Osteoporos Int. 2014;25(12):2755-65.
25. Vis M et al. Evaluation of bone mineral density, bonemetabolism, osteoprotegerin and receptor activator ofthe NFkappaB ligand serum levels during treatmentwith infliximab in patients with rheumatoid arthritis. AnnRheum Dis. 2006;65:1495-1499.

Fracture Liaison Service Champions Network
The FLS Champions Network has three main aims:
• To support the development of FLSacross the UK through a collective network of knowledge and expertise, sharing best practice in FLS and secondary fracture prevention.
• To ensure those working in FLSremain up-to-date with all relevant work programmes regarding FLS and secondary fracture prevention across the UK.
• To provide the opportunity tocommunicate directly with the National Osteoporosis Society and the relevant resources we provide.
For further information email: [email protected]
Join the network at: www.nos.org.uk/champions
Your opportunity to share and gain knowlege, expertise and best practice in FLS and secondary fracture prevention, and support the roll-out of FLS across the UK.
FLS Champions A4.indd 1 19/05/2016 14:54:14
Osteoporosis Review 2016; Vol 24 No2 27
Register online nowwww.nos.org.uk/conference
@OsteoporosisSoc /buildingstrongerbones /national-osteoporosis-society
Osteoporosis CONFERENCE 2016 Birmingham ICC 07–09 November
• Learn from renowned experts
• Interact and network
• Exchange ideas and experiences
• Discover how to tackle complex challenges
The UK’s leading event
on osteoporosis and bone health
NOS Conference 2016 flyer A4 1pp.indd 1 07/09/2016 14:09:10