osteoporosis - danielle conlon filediagnosis of osteoporosis looks at: o bone mineral content (bmc):...
TRANSCRIPT

Osteoporosis
Outline I. Bone Structure (Jen)
I. Types of bone tissue
II. Bone modeling/remodeling
II. Pathophysiology/etiology (Jen)
III. Diagnosis (Danielle)
IV. Types (Krista)
V. Risk Factors (Krista)
VI. Prevention (Krista)
VII. Treatments (Heather)
VIII. Cochrane Review (Heather)
IX. Case study (Danielle)

Incidence and Prevalence • 24 million in USA (200 million worldwide)
• 80% are women
• 40% fracture
• 20% are men
• 15-30% fracture

Composition of Bone • Osteoid
• Organic protein structure
• Collagen fibers
• Calcium phosphate + calcium carbonate = crystals of hydroxyapatite
• Flexibility and Strength

Bone Structure • Types of Bone Tissue
• Cortical Bone (Compact)
• 80% of skeleton
• Shafts of the long bone
• Trabecular Bone (Cancellous)
• 20% of skeleton
• Knobby ends of long bones, iliac crest of pelvis, wrists, scapulae, vertebrae, and the regions of the bone that line the marrow
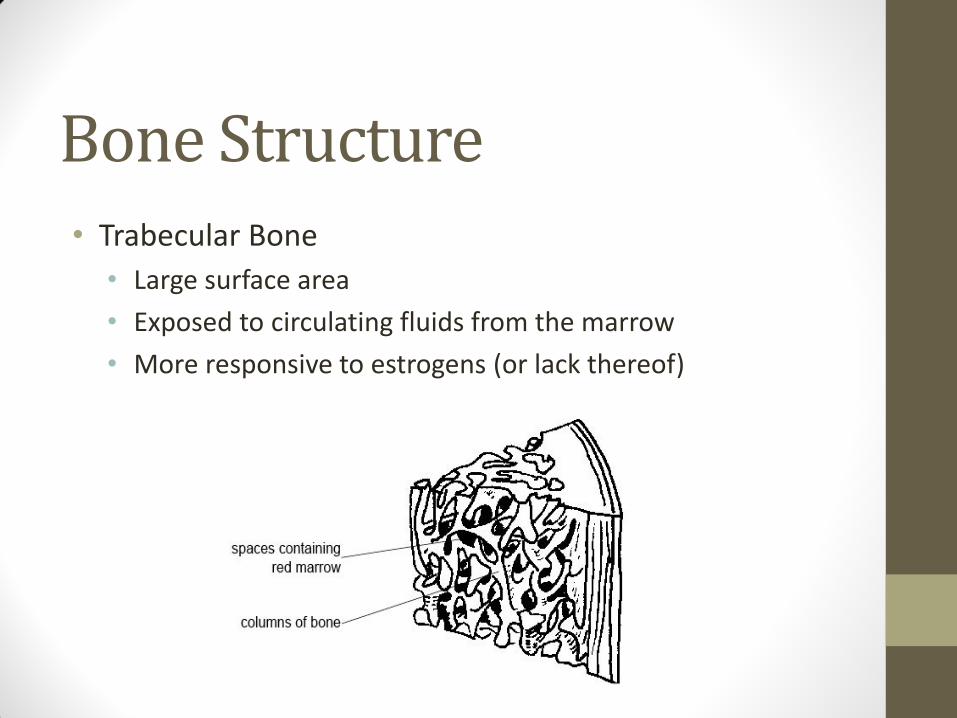
Bone Structure • Trabecular Bone
• Large surface area
• Exposed to circulating fluids from the marrow
• More responsive to estrogens (or lack thereof)

Bone Modeling • Growth of the skeleton until mature height is achieved
• Formation > Breakdown
• Typically completed:
• Girls by ages 16 to 18
• Boys by ages 18 to 20

Bone Remodeling • After skeletal growth is complete
• Bone is continuously resorbed and reformed (dynamic)
• Osteoblasts
• Osteoclasts
• Triggers
• Strains on skeleton
• Changes in lifestyle factors/dietary intakes
• Changes in calcium plasma concentrations
• Microscopic fractures over time

Bone Remodeling • Activation
• Interleukin-1 (IL-1) and other cytokines
• Preosteoclastic cells
• Migrate and mature
• Resorption
• Osteoclasts
• Acids and photolytic enzymes
• Formation
• Osteoblasts
• Collagen and other matric proteins
• Hydroxyapatite crystals

Bone Remodeling

Peak Bone Mass (PBM) • The greatest amount (mass) of bone
accumulated at any age
• 30 years of age
• Greater in men
• 60% genetic, 40% environmental
• PBM is related to:
• Dietary calcium intake
• Weight-bearing physical activity

Peak Bone Mass (PBM)

Peak Bone Mass (PBM) • Dietary calcium intake

Peak Bone Mass (PBM) • Weight-bearing physical activity
Bone Loss • Bone begins to decline at about age 20
• Increases greatly in women after age 50 (menopause)
• Trabecular vs. Cortical
• Decline of osteoblastic function

31 YOM
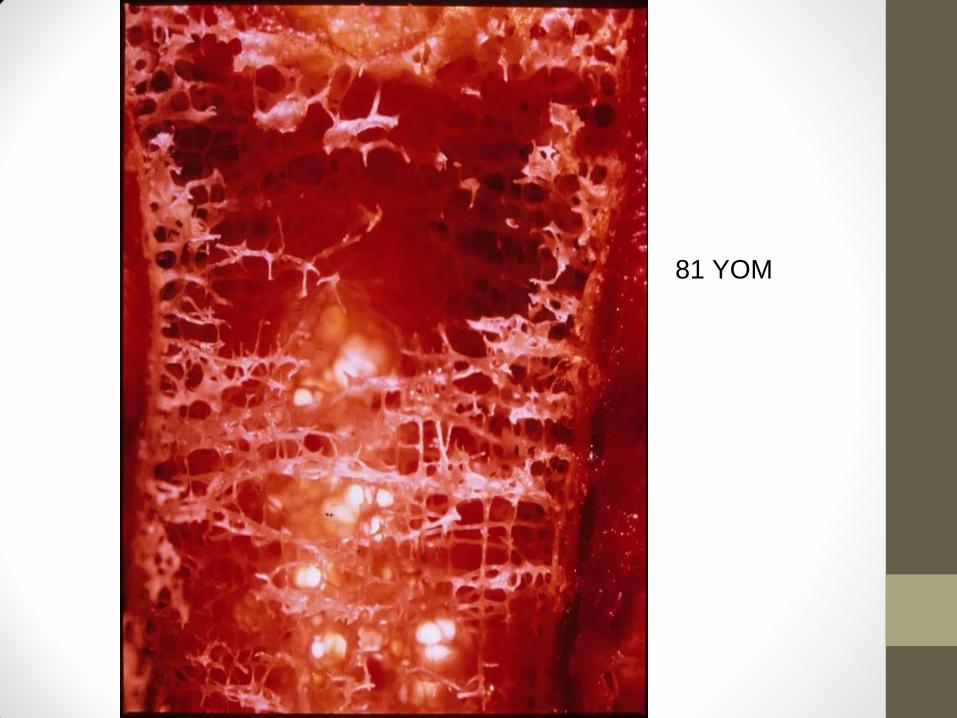
81 YOM


Diagnosis • Diagnosis of Osteoporosis looks at:
o Bone Mineral Content (BMC): the amount of minerals in bones
o Measured in grams.
o Bone Area (BA): The area of the bone
o Measured in cm2
o Bone Mineral Density (BMD):
o Average mineral concentration bone
o Measured in g/cm2

Diagnosis of Osteoporosis Steps to Diagnosing Osteoporosis
• Medical History
• Physical exam
• Bone Density Tests
o DXA (gold standard)
o X-rays and Bone Scans
o Lab Tests
o FRAX

Sites of Diagnosis • Hip
• Spine

DXA • Dual X-ray Absorptiometry
• Z-Score
o comparison of bone density with a healthy 30 year old of the same sex
Z-scores aren’t used to formally diagnose osteoporosis
• T-Score
o Comparison of bone density with an average person of the same age and sex
o Diagnose
osteoporosis
formally
If Your T-Score Is... Then You Have...
+1 to -1 Healthy Bones
-1 to -2.5 Low Bone Density or Osteopenia
-2.5 or lower Osteoporosis

DXA

X-rays • Ultrasound
o Looks at bone structure and strength
Calcaneus
• CT Scan
o Creates a 3D picture of the area being scanned
o Useful after compression fractures in the spine
X-rays cont. • MRI
o Doesn’t diagnose osteoporosis but can identify fractures and diagnose a comorbidity
• X-ray
o Identifies fractures
• Bone Scan
o Uses radioactive material to see fractures that may have been missed by other means

Lab Tests
• Bone Calcium Levels
• Urine Calcium Test
• Thyroid function tests
• 25-hydroxyvitamin D test
• NTx and CTx
o Bone turnover tests
o Measure type-1 collagen levels in the bones
This is an indicator of BMD and fracture risk

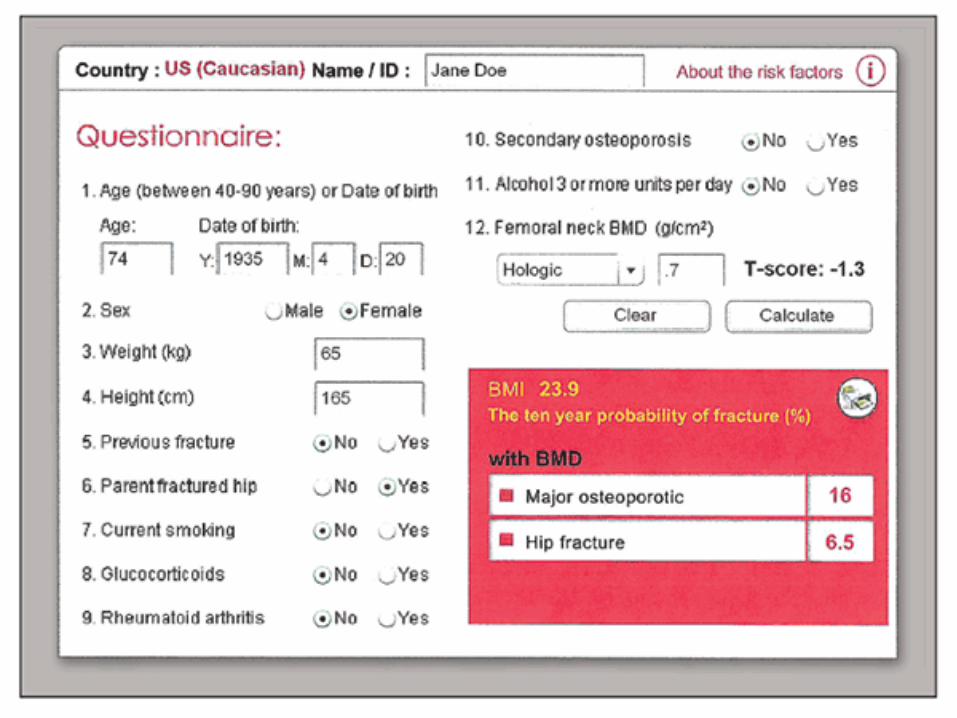
FRAX • Fracture Risk Assessment Tool
o Algorithm that assesses your risk for fractures within the next 10 years.
Age
Height and Weight
Smoking and alcohol history
Other medical conditions
Corticosteroid use
Family history of fractures
Personal history of fractures
FRAX

Who Should be Tested?
• Women: >65 years old
• Men: >70 years old
• Adults who have had a fracture after age 50
• Adults taking a medication that causes bone loss
o Prednisone
• Postmenopausal women who are discontinuing estrogen treatment

MNT once osteoporosis is diagnosed
● Goal is to prevent fractures
● Balanced Diet
○ Calories
○ Food groups
○ Specific Nutrients
■ Vitamin K
■ Calcium
● 1000 mg/day
■ Vitamin D
● 800-1000 IU/ day

Other Nutrients ● Phosphorus
○ goes hand in hand with Ca
○ Part of the bones
● Protein
○ loss of Ca through the kidneys (esp. excessive animal protein)
● Sodium
○ decreases body’s ability to retain Ca

Types of Osteoporosis ● Osteomalacia: a condition of impaired mineralization
caused by vit D and Calcium deficiency
● Osteopenia: a condition that occurs when BMD drops below healthy levels (1 SD)
● Osteoporosis: >2.5 SDs below healthy levels, when skeletons cannot sustain normal strains
Types of Osteoporosis ● Secondary osteoporosis: when bone tissue is lost
due to drugs or other diseases
● Age related osteoporosis: age 70+
● Estrogen-androgen deficient osteoporosis: After menopause
○ Loss of trabecular bone tissue
○ No ovarian production of estrogens
Rickets ● Vitamin deficiency in young children
● Supplement 400 IU of Vit D
○ Exclusively breastfed infants
● Supplement 400 IU of Vit D until taking 1 L of formula a day
○ Breastfed/formula fed
● Supplement for 1 year until taking Vit D fortified milk

Risk Factors ● Older age
● 80% female
● Genetics
● LBW
● Caucasians/Asian/Latino Race
● Broken bone history
● Low estrogen levels
○ Estrogen protects bone
Controllable Risk Factors ● Cigarette smoking
● Excessive alcohol
● Caffeine
● Soft drinks
● Not exercising

Conditions that can lead to Osteoporosis
● Hyperparathyroidism
● Hyperthyroidism
● Multiple Myeloma
● Inflammatory Bowel Disease (IBD)
● Celiac Disease
● Organ Transplants
● Wt loss
● Ht loss
● Others
Prevention ● Adequacy of Calcium and Vitamin D intake
● Exercise
● Avoidance of tobacco
● None to moderate intake of alcohol
● Avoidance of falls/accidents
● Live a healthy lifestyle

Calcium and Vitamin D Recommendations
Children and Adolescents Calcium (Daily) Vitamin D (Daily)
1-3 years 500 mg 200 IU**
4-8 years 800 mg 200 IU**
9-18 years 1,300 mg 200 IU**
Adult Women and Men Calcium (Daily) Vitamin D3 (Daily)*
19-49 years 1,000 mg 400-800 IU
50 years and over 1,200 mg 800-1,000 IU
Pregnant and Breastfeeding Women
Calcium (Daily) Vitamin D3 (Daily)*
18 years and over 1,300 mg 400-800 IU
19 years and over 1,000 mg 400-800 IU

NOF’s Calcium and Vitamin D Recommendations
Men
Age 70 & younger 1,000 mg/d
Age 71 & older 1,200 mg/d
Women
Age 50 & younger 1,000 mg/d
Age 51 & older 1,200 mg/d
Men and Women
Under age 50 400-800 IU/d
Age 50 and older 800-1,000 IU/d
Calcium
Vitamin D

Exercise ● Weight-bearing/Impact
● Resistance/Strength
● Balance
● Posture
● Functional

How to Reduce the Risk of Falls
● Maintain vit D intake
● Physical Activity
● TaiChi
● Assess & modify the safety of the home
● Individual risk assessment

Treating Osteoporosis • Most people find out they have osteoporosis AFTER
breaking a bone
• Goal of treatment is to recover from broken bones and prevent future fractures
Factors to Consider Prior to Treatment
• Gender (has the woman reached menopause?)
• Age (70+)
• Severity
• Secondary problems
• Personal preferences

Two Categories of Medication
• Antiresorptives: slow breakdown of bone
o types: bisphosphonates, calcitonin, estrogen/hormone therapy, estrogen agonists/antagonists
• Anabolics: speed up rate of bone formation
o types: parathyroid hormone
Six Classes of Medication
1. Estrogen Replacement Therapy
2. Androgen Replacement Therapy
3. Bisphosphonates
4. Selective Estrogen Receptor Modulators
5. Intermittent PTH Therapy
6. Others

Estrogen Replacement Therapy • postmenopausal women are at a greater risk
for developing osteoporosis because estrogen production slows down with age
• Estrogens regulate osteoclast apoptosis
• As estrogen production declines, osteoclasts live longer and resorb more bone
• goal of therapy is to increase serum estrogen levels

Estrogen Replacement Therapy
• can be a pill, patch, or topical treatment
• rarely used because high risk of developing breast/endometrial cancers
• phytoestrogens o plant product estrogen substitute
o bind to estrogen receptors
o example is isoflavones, commonly found in soy and red clover
o little research to suggest if effective or not

Estrogen Replacement Therapy
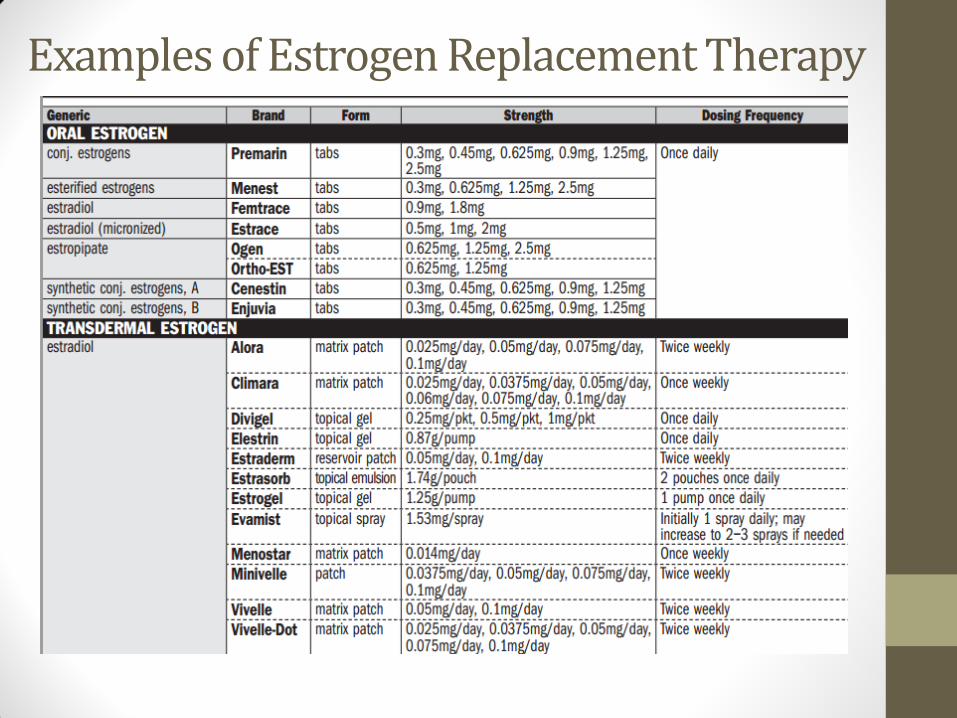
Examples of Estrogen Replacement Therapy

Androgen Replacement Therapy
• can help men maintain bone mass and limits fractures
• more commonly used in men with forms of primary hypogonadism such as pituitary insufficiency or klinefelter syndrome
• rarely used because of side effects
o increases prostate growth

Examples of Androgen Replacement Therapy • Androgel
• Axiron
• Testim
• Androderm
• Bio-T-Gel
• Delatestryl
• Depo-Testosterone
• Fortesta
• Striant

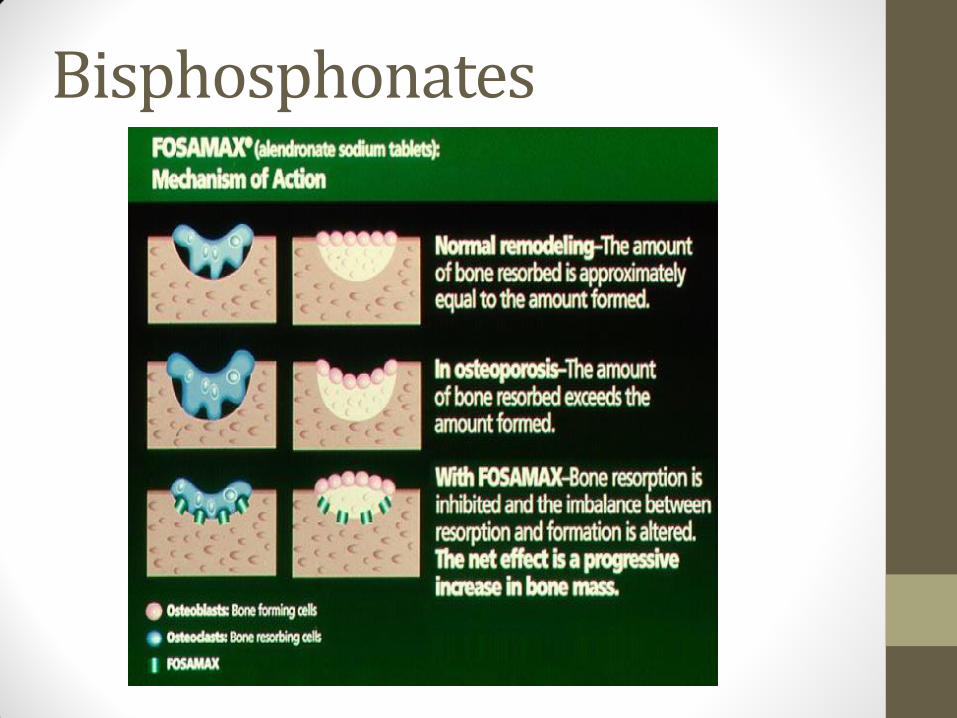
Bisphosphonates • overall goal is to inhibit
osteoclasts
• mimic pyrophosphate which is present on bone crystal surfaces

Bisphosphonates How do they work?
• Bisphosphonate attaches to calcium on bone surface
• As osteoclasts break down bone, they “ingest” the bisphosphonate and lose ability to function (apoptosis)
• Inhibit mature osteoclast function
• Decrease bone resorption rate and maintain structural properties of bone
Bisphosphonates

Bisphosphonates

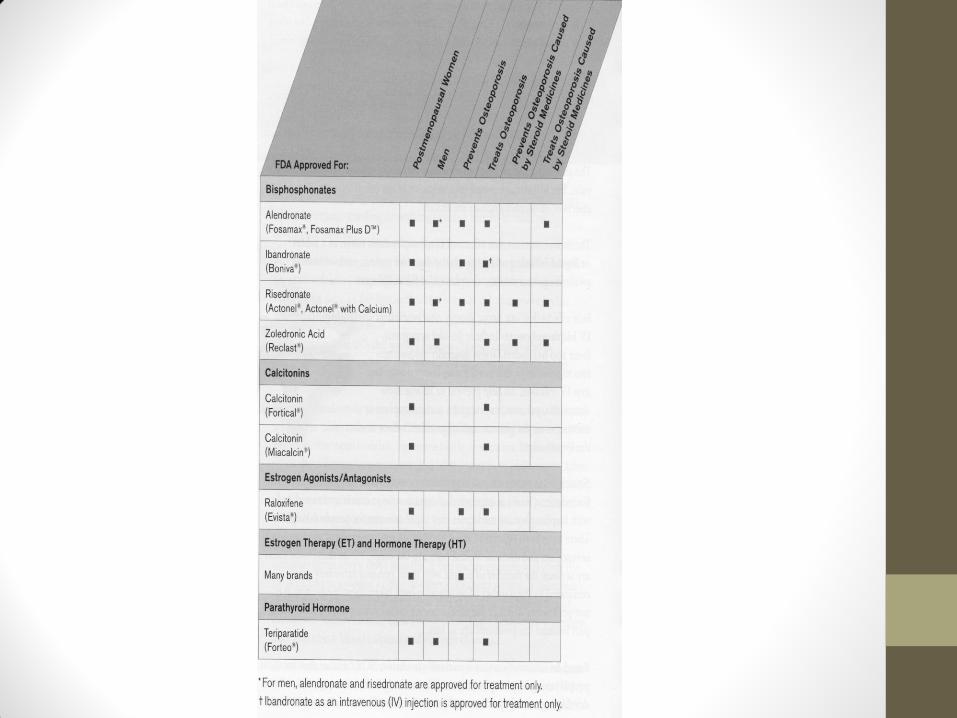
Examples of Bisphosphonates
• Taken by mouth 1-2 times a week, or once a month
• Zoledronic acid given intravenously
Brand Name Generic Name
Fosamax Alendronate
Boniva Ibandronate
Actonel, Atelvia Risedronate
Reclast Zoledronic Acid

Selective Estrogen Receptor Modulators • Stimulate estrogen receptors in the bone
tissue
• Types
o Tamoxifen: originally prescribed to prevent breast cancer, but researchers discovered by chance that it also conserved bone
o Raloxifene: proven effective to maintain bone

Examples of Selective Estrogen Receptors
• Evista (Raloxifene)
• Nolvadex (Tamoxifen)
• Fareston (Toremifene)
• Osphena (Ospemifene)
• Soltamox (Tamoxifen)

Intermittent PTH Therapy • One of the few anabolic therapies available
• increases osteoblast formation of new tissue
• administered as subcutaneous injections
• Although high serum PTH concentrations result in bone resorption, exogenous intermittent PTH therapy stimulates bone formation instead of resorption
• Example is Teriparatide (Forteo), which is a section of PTH with amino acid sequence 1 through 34

Intermittent PTH Therapy
The 1-34 molecule is fragmented. It has been FDA approved for adults with severe osteoporosis. The 1-84 molecule (which is full length) has not been approved yet.

Review Article: Intermittent Parathyroid Hormone Therapy To Increase Bone Formation
• Low doses of modified PTH (1-34)
molecule may increase bone density
• After one year of treatment, lumbar
vertebrae bone mineral density
increased by 15%
• Total body bone mineral density
increased by 5-10%

Others The following are not directly intended for osteoporosis and need further research
• Calcitonin
o inhibits osteoclasts by blocking PTH stimulation
• Osteoprotegerin (OPG)
o inactivates cytokines that regulate osteoclasts

Others • Sodium Fluoride
o increases bone mass, but the quality of the bone is not normal
o alters the size and structure of bone crystals to the point that bone is not mechanically competent

• Prolia (Denosumab)
• Treatment for women who have experienced menopause
• A subcutaneous injection administered twice a year
• Binds to and inhibits RANK (receptor activator of nuclear factor-kappa B)
• RANK promotes maturation of pre-osteoclasts into osteoclasts
• Prolia halts osteoclast development
Others

Kyphosis and Lordosis
• Kyphosis: excess outward curvature of spine
• Lordosis: excess inward curvature of spine


Types of Surgeries • kyphoplasty
• insert a balloon device into fractured vertebral area
• inflate balloon to restore height of vertebra
• fill empty space with bone cement
• improves pain and deformity of spine

Types of Surgeries The goal of most surgeries is to address hip, vertebral, or wrist fractures
• vertebroplasty
o inject bone cement into fractured vertebral area of spine
o reduces pain
o increases ability to be active

Hip Replacements WHY?
• Joint damage causes pain in everyday activity
HISTORY
• Surgeries were primarily for people over age 60
• Physical activity and overall health are important factors

Hip Replacements

Hip Replacements
Recovery
• Adequate Ca and vit D intake
• Restore strength and balance
• Medication: Reclast® (zoledronic acid)
• Reduces the risk of breaking more bones
• Extends life for those who have Osteoporosis and have broken a hip
• Rehab: Physical Therapy
• Return to exercise (slowly)
• Fall-proof the home

Hip Replacements
Recovery • usually takes 3-6 months
Complications
• Hip dislocations
• Inflammation
• Treatment: anti-inflammatory medication
• Infection
• Blood Clots
• Heterotopic bone formation

Hip Replacements
Recovery • Postoperative pain
• Opioids
• Sleep disturbances
• REM sleep cycle rebound phenomenon
• Can result in respiratory and/or cardiac complications
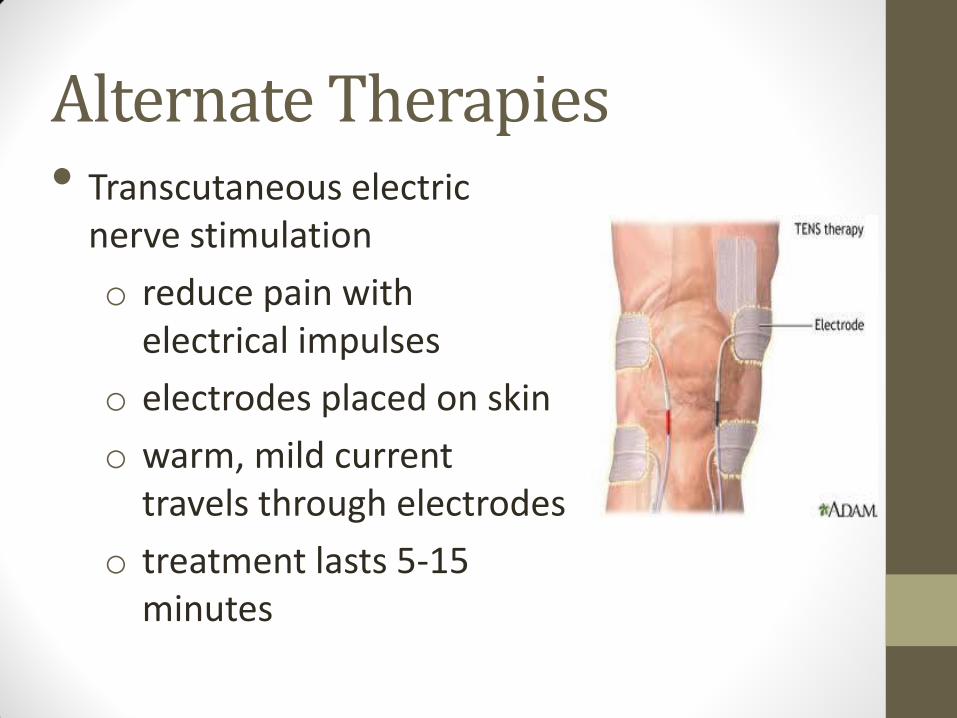
Alternate Therapies • Transcutaneous electric
nerve stimulation
o reduce pain with electrical impulses
o electrodes placed on skin
o warm, mild current travels through electrodes
o treatment lasts 5-15 minutes

Alternate Therapies • acupuncture
o insert needles in skin o alters body’s flow of energy
• biofeedback/relaxation techniques o learn techniques to better manage stress o decreases blood pressure, heart rate, and overall
body pain o includes deep breathing, progressive muscle
relaxation, guided imagery • physical activity
o body releases endorphins that can relieve pain o may improve bone mineral density

Cochrane Review: Exercise for Preventing and Treating Osteoporosis in Postmenopausal Women
• Can exercise be a treatment option?
• Examined how effective various exercise programs were in improving bone mineral density in postmenopausal women
• Most effective exercise programs were “combination” programs
• Includes a combination of aerobics, lifting weights, walking, and tai chi

Cochrane Review: Exercise for Preventing and Treating Osteoporosis in Postmenopausal Women
• Women in the exercise groups had a lower risk of fractures than women in control groups
• Bone mineral density of the spine increased from 1.90 to 4.64
• a small fraction of women experienced fractures during exercise, so doctors must prescribe exercise with
discretion
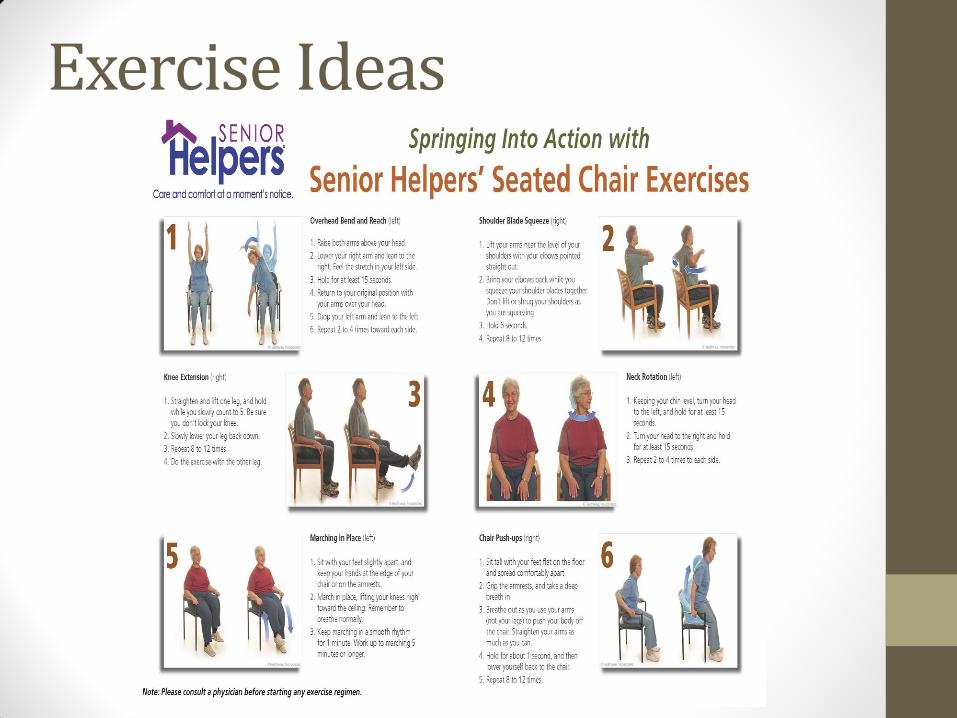
Exercise Ideas

Nutrition Assessment
• Anthropometrics: o BMI: 18.9
o IBW: 125 lbs; currently 113
o Calorie needs: 1565
Using with the EER equations

Biochemical
• Sodium: 133 (WNL)
• Potassium: 3.4 (low)
• Calcium: 9.4 (WNL)
• Albumin: 3.5 (WNL)
• HGB: 12.6 (WNL)
• HCT: 36.8% (WNL)
• BUN: 10 (WNL)
• Creat: 0.9 (WNL)
• DXA: -3.5 (osteoporosis)

Clinical • Went through menopause in early 50’s
• Curvatures in upper thoracic and lower spinal regions
• On a Vitamin D and Calcium supplement

Dietary • Doesn’t drink much milk or consume many dairy products
• Eats mostly salads and soups
o Missing calcium and Vitamin D
• Has coffee for breakfast most mornings

Nutrition Intervention ● Supplements
○ Calcium
○ Vitamin D
● Medications
○ Forteo
● Sunlight
● Diet

PES Statement Decreased bone mineral density related to decreased
calcium intake evidenced by a DXA score of -3.5 and a right hip fracture.

Calorie Requirements ● EER
○ PA=1 (sedentary female)
○ wt=51.4kg
○ ht=1.7 m
○ age=73 years
● 1565 kcals
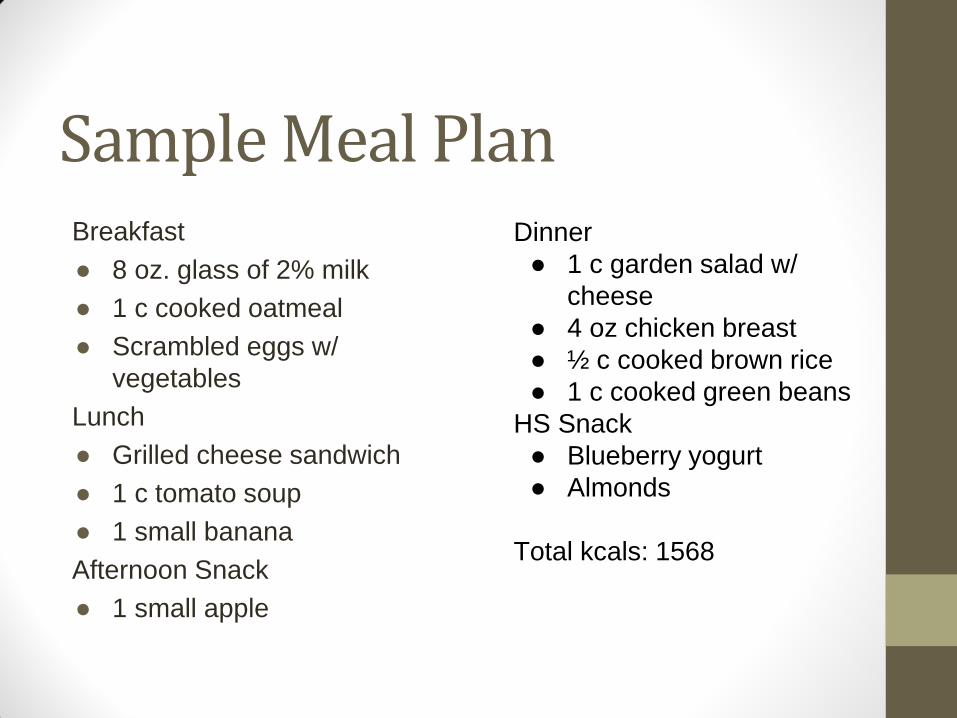
Sample Meal Plan Breakfast
● 8 oz. glass of 2% milk
● 1 c cooked oatmeal
● Scrambled eggs w/
vegetables
Lunch
● Grilled cheese sandwich
● 1 c tomato soup
● 1 small banana
Afternoon Snack
● 1 small apple
Dinner
● 1 c garden salad w/
cheese
● 4 oz chicken breast
● ½ c cooked brown rice
● 1 c cooked green beans
HS Snack
● Blueberry yogurt
● Almonds
Total kcals: 1568

Cutting cone in cortical bone
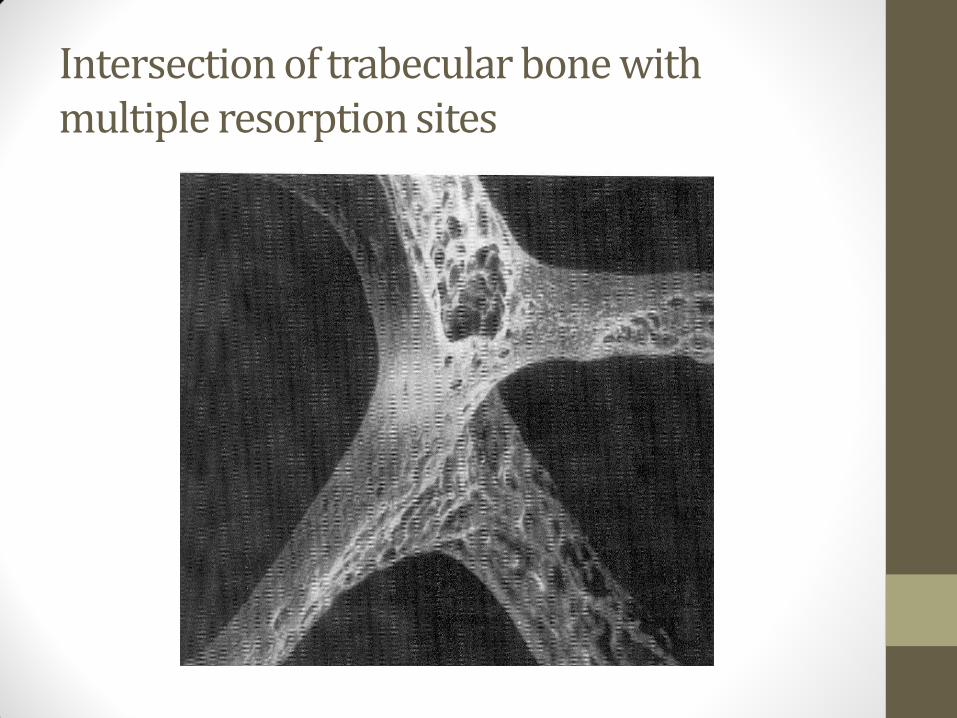
Intersection of trabecular bone with multiple resorption sites


31
YO
M

81
YOM
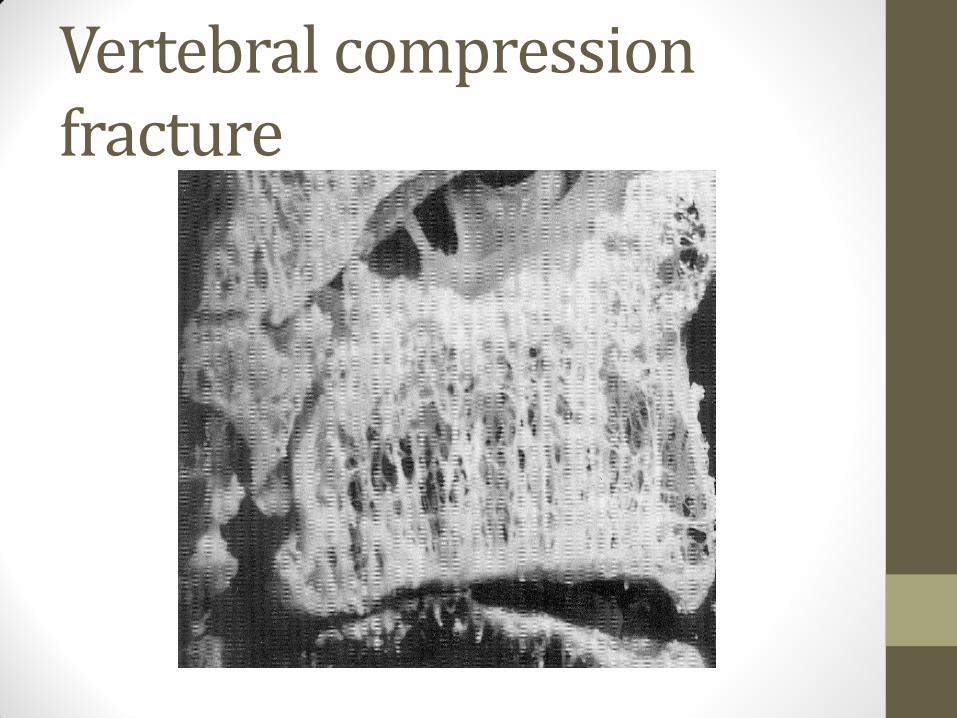
Vertebral compression fracture