osteoarthritis 2013
TRANSCRIPT

OSTEOARTHRITIS
Blondina Marpaung
Rheumatology DivisionInternal MedicineDepartment
Medical Faculty Sumatera Utara University

The most common degenerative joint had been seen in :
•Human
•Rats
•Whales
•Dinosaur fossil
It had been recognice since 5000 years ago

* Over 40 years old
* Woman : man = 4 : 1
• The most common joint disease
in Indonesia
* Weight bearing joints

Chronic disease due to articular Chronic disease due to articular cartilage damage with a new bone cartilage damage with a new bone
formation.formation.
OsteoarthritisOsteoarthritis

• Degenerative joint disease
• Cartilage and sub chondral damage
• Imbalance between synthesa and
degradation
• Cartilage erosives, cyst formation, osteophytes formation
• Synovial inflammation
OsteoarthritisOsteoarthritis
FUNCTONAL IMPAIRMENT:
Restricted movement
Intermitten
Mild at early phase
Joint stiffness:
- localized / temporary - in the morning before activity - weather alteration
Crepitation :
-The sensation of bone rubbing against bone
- palpable at knee joint
Helpful for diagnosis

GAIT DISORDER
* ANTALGIC GAIT (PAIN AT WEIGHT BEARING JOINT)
* TRENDELENBURG GAIT ( HIP )
* STIFF KNEE GAIT
* LUMBAR CLAUDICATION (VERTEBRA LUMBAL)

RISK FACTOR
Knee joint: * Body weight- linier association- obese woman 7 x fold risk
* Activity- menekuk sendi lutut- weight bearing
Panggul : * obesitas kurang berperan* hubungan erat dgn aktivitas (petani)
* Race Kaukasia >> Asia (orang Asia sering jongkok)

Joint Predilection Joint Predilection Joint Predilection Joint Predilection Most common : weight bearing joint - knee - lumbal - cervical
Generalized OA DIP ( Heberden node )

thickening capsule
OA KNEENORMAL KNEE
Cyst formation
Subchondral bone sclerosis
Cartilge articular fibrillation
Synovium hypertrophy
Osteofphyte formation
capsule
cartilageArticular
Synovium
bone
ACRFP
NORMAL versus OA JOINT


Tulang subkhondral Tulang subkhondral
menebal dan ireguler, menebal dan ireguler,
tampak sklerostik dan tampak sklerostik dan
pembentukan kistapembentukan kista
Kapsul mengalami Kapsul mengalami fibrosis, distorsi dan fibrosis, distorsi dan penebalanpenebalan
Fibrilasi, kerusakan dan Fibrilasi, kerusakan dan berkurangnya volume berkurangnya volume rawan sendirawan sendi
Sinovitis kronikSinovitis kronik
Pertumbuhan osteofit, Pertumbuhan osteofit, dan penebalan jaringan dan penebalan jaringan ikat lunakikat lunak
Sendi Normal dan Perubahannya Pada
OATekstur tulang Tekstur tulang
subkhondral normal subkhondral normal
Rawan sendi Rawan sendi normal, tebal dan normal, tebal dan
ratarata
Ujung tulang rataUjung tulang rata
Sinovium normal Sinovium normal dengan selapis sel dengan selapis sel
tunggaltunggal
Kapsul sendi tebalKapsul sendi tebal
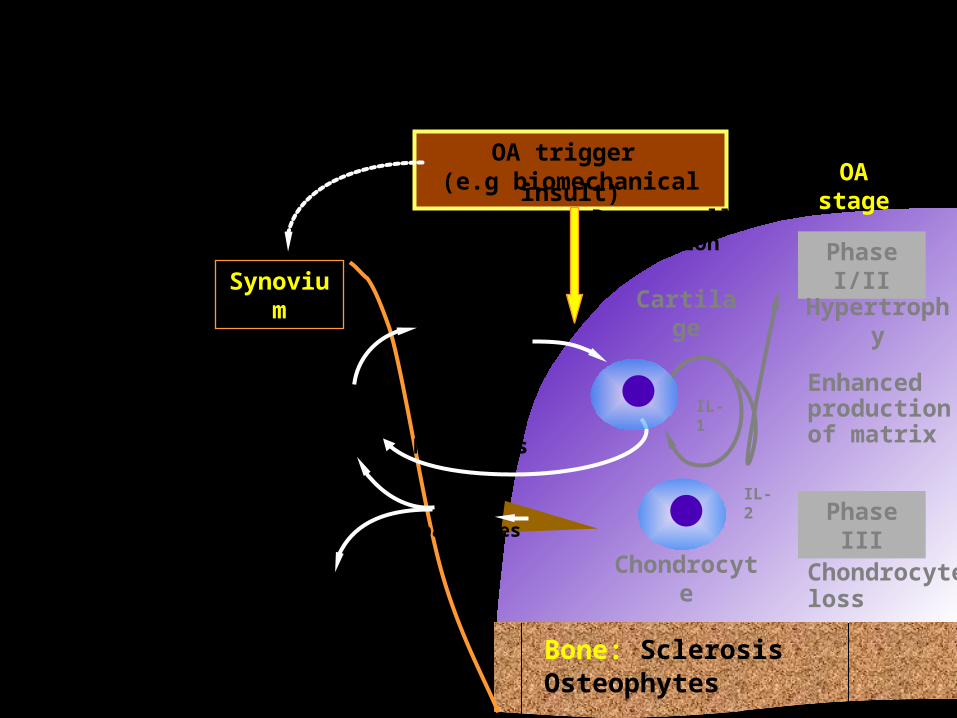
The role of cytokines
OA stage
Phase I/II
Hypertrophy
Enhanced production of matrix
Phase III
Chondrocyte loss
Bone: SclerosisOsteophytes
Synovium
OA trigger (e.g biomechanical insult)
Damage cell activation
Cartilage
Chondrocyte
IL-1, IL-2, TNF, GF enzymes
Fibroblast, macrophage
Mediators
Immune infiltrate
?
IL-1
IL-2Wear
particles
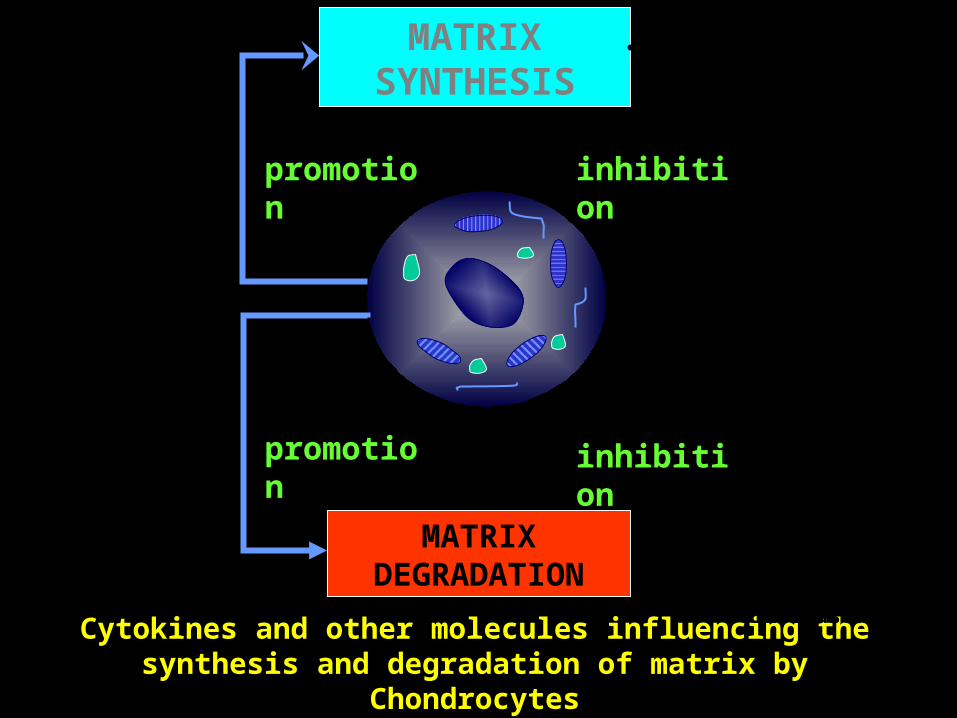
Cytokines and other molecules influencing the synthesis and degradation of matrix by Chondrocytes
MATRIX SYNTHESIS
MATRIX DEGRADATION
promotion
promotion
inhibition
inhibition
TGF-
IGF-1
bFGF
PDGF
IL-1,
TNF-
IL-1 + bFGF or PDGF
(IL-1 effect enhanced)
Glucocorticoid
IL-1,
IL-1 + PDGF (IL-1 effect inhibited)
TNF
-IFN
Retinoids
IL-1 + -IFN (IL-1 effect inhibited)
Glucocorticoid
IL-1+ TGF- or IGF-1 or -IFN (IL-1 effect inhibited)
TGF- (TIMP increased)

Clinical featuresClinical featuresClinical featuresClinical features





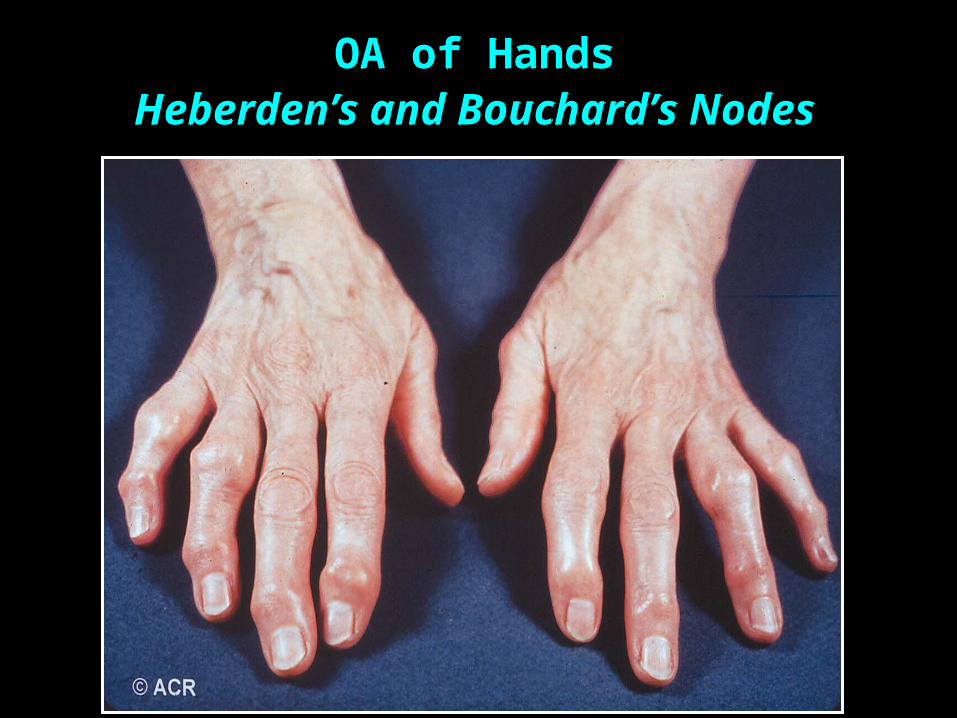
OA of HandsOA of HandsHeberden’s and Bouchard’s NodesHeberden’s and Bouchard’s Nodes
OA of HandsOA of HandsHeberden’s and Bouchard’s NodesHeberden’s and Bouchard’s Nodes



Chondrocyte :
Play role in collagen and proteoglycan synthesis
Articular Cartilage
MATRIX EXTRACELLULER :
Water (65-85 %)
Collagen type I (15-25 %)
Proteoglycan (10 %)
Collagen type VI, IX, XI and XIV
Connective Protein etc

Mature chondrocyte cell
Produces Collagen & proteoglycan
CHONDROCYTE
Function : produces syntheses and degradates articular cartilage enzymes
Stabil and balance articular cartilage

COLLAGEN
a protein with strenght and elastic fibre Play role as tissue skeleton
Function : perekat yang membangun matriks rawan
sendi
PROTEOGLYCANMacromolecule yang dibangun oleh protein & gula
Terdiri dari :
Inti protein
Glycosaminoglycan
Chondroitin sulphate
Keratan sulphate
menyokong stabilitas dan kekuatan rawan sendiProteoglikan membentuk kesatuan dgn asam hialuronat
Fungsi :
menghisap dan mengeluarkan air sesuai dgn gerakan sendi
Evaluation Konventional Radiology
cant assess early OA
because : cartilage thickening can assessbut surface alteration cant
- Cartilage thinning / narrowing joint cleave
OA process had been 10 year
Clinical Presentation of OA Clinical Presentation of OA
Symptoms*Pain–initially with use
Stiffness
Limitation of motion
Symptoms*Pain–initially with use
Stiffness
Limitation of motion
SignsCrepitus
Bony hypertrophy
Bony tenderness
Limitation of range of motion
Malalignment
Altered gait
SignsCrepitus
Bony hypertrophy
Bony tenderness
Limitation of range of motion
Malalignment
Altered gait*Insidious onset*Insidious onset
Risk factor for osteoarthritis
Non-modifiable Age Race Genetics (Col 2A1 gene) Female sex Metabolic and endocrine
disease Congenital defect Neurological defect
Modifiable Major trauma Repetitive stress Inflammatory joint
disease Obesity Smoking Hormone Quadriceps muscle
weakness
Hochberg MC. J Rheumatol 1991; 18: 1438-40.

Therapy principle
• Pain Reduction / elimination
•Functional impairment prevention/
reduction
•Disability prevention

Management of Osteoarthritis
• Non-pharmacological therapyNon-pharmacological therapy
• Pharmacological therapyPharmacological therapy
• SurgerySurgery
Non-pharmacological therapy
• Patients education, self-management program
• Weight control
• Physical therapy, occupational therapy
• Exercise program
• Assistive devices
• Joint protection
• Appropriate foot ware
Modified from ACR subcommittee. A&R 2000; 43:1905-15.

Pharmacologic Management of OA
Systemic therapySystemic therapy• Nonopioid analgesics• NSAIDs / Cox 2 inhibitor• Opioid analgesics • DMOAD’s / SYSADOA’s:
Chondroitin & Glucosamine DoxicyclineChloroquine visco suplement
• Diacerine
Local therapyLocal therapyTopical agents Topical agents Intra-articular Intra-articular
agentsagents

Pharmacological therapy of osteoarthritisACR Recommendation(Arthritis Rheum 2000;43:1905-15)
• Oral– Acetaminophen– COX-2 inhibitor– Nonselective NSAIDs plus misoprostol or a PPI– Nonacetylated salicylate– Others: tramadol, opioids
• Intra-articular– Corticosteroids– Hylauronan
• Topical– Capsaicin– Methylsalicylate

OARSI guidelines
Eight pharmacological recommendations– Acetaminophen– cyclooxygenase-2 (COX-2) non-selective and selective
oral non-steroidal anti-inflammatory drugs (NSAIDs)– topical NSAIDs and capsaicin– intra-articular injections of corticosteroids and
hyaluronates– glucosamine and/or chondroitin sulphate for symptom
relief– glucosamine sulphate, chondroitin sulphate and
diacerein for possible structure-modifying effects– opioid analgesics for refractory pain

CAUSAL DRUGS / DMOADS
• Visco supplementation
Hyaluronan / Hyalgan Intra articular
- Main molecule of proteoglycan - Activates repairing cartilage process.
- Normalyzed synovial fluid quality.
* Intra articular inj. 20 mg (1 amp) weekly, 5-7 weeks

• Chloroquin
- inhibits IL-1 expression
- inhibits supression of prostaglandin synthese-Slowing progression of OA stage-Repairs OA pathology
• Chondroitin Sulphate
- matrix proteoglycan formation-Dose : per-oral 400 mg , 3 x / day

OA: Intra-articular Therapy
• Intra-articular steroid• Good pain relief • Most often used in knees, up
to q 3 mo• With frequent injections, risk
infection, worsening diabetes, or CHF
• Joint lavage• Significant symptomatic
benefit demonstrated
• Hyaluronate injection• Symptomatic relief • Improved function• Expensive• Require series of injections• No evidence of long- term
benefit• Limited to knees
* Altman, et al. J Rheumatol. 1998;25:2203.

Surgical Therapy for OASurgical Therapy for OA• ArthroscopyArthroscopy
• May reveal unsuspected focal abnormalitiesMay reveal unsuspected focal abnormalities• Results in tidal lavageResults in tidal lavage
• Osteotomy: May delay need for TKR for 2 to 10 yearsOsteotomy: May delay need for TKR for 2 to 10 years
• Total joint replacement: When pain severe and Total joint replacement: When pain severe and function significantly limitedfunction significantly limited

OARSI guidelines
– five surgical modalities• total joint replacements
• unicompartmental knee replacement
• osteotomy and joint preserving surgical procedures
• joint lavage and arthroscopic debridement in knee OA

PHARMACOLOGICAL THERAPY OF OSTEOARTHRITIS
EULAR Recommendation(Ann Rheum Dis 2003;62:1145-55)
• Analgesics Acetaminophen NSAIDs and COX-2 inhibitors Tramadol and opioids
• Topical Capsaicin and topical NSAIDs
• Intra-articular Corticosteroids Hyaluronan
• Symptomatic slow acting drugs Glucosamine sulfate Chondroitin sulfate Diacerein

Treatment of osteoarthritis (of the knee)
Education, PT, OT, weight reduction, topic analgesics
Simple analgesics
IA co
rtico
stero
ids,
IA h
yalu
ronan
SurgeryExercise, assistive devices
NSAIDs or specific COX-2 inhibitors, or tramadol, or
opioids analgesics
SYSADOAs

Glucosamin:o Stimulates chonrocytes to produces more
and faster collagen and proteoglycan o Normalyzed metabolism of cartilage articular
o Eliminates of pain
o Supports joint movement
GLUCOSAMIN & KONDROITIN GLUCOSAMIN & KONDROITIN FUNCTIONFUNCTION

Chondroitin:
o Role as liquid magnet membantu menarik cairan ke dalam molekul-molekul proteoglikan sehingga membantu jalannya nutrisi kartilago dan juga berperan sebagai Spongy Shock Absorber
o Mempercepat penyembuhan luka dan tukak

Glucosamine
• A building block for articular cartilage’s extracellular matrix
• Used to produce GAGs and proteoglycans
• Synthesized by chondrocytes
• 90% absorption by oral administration
• 26% available for processing by the body’s tissue

Claims
• Treatment of knee osteoarthritis
• Repair and maintenance of joint cartilage
• Aid glycosaminoglycan (GAGs) synthesis
• Reduce joint pain

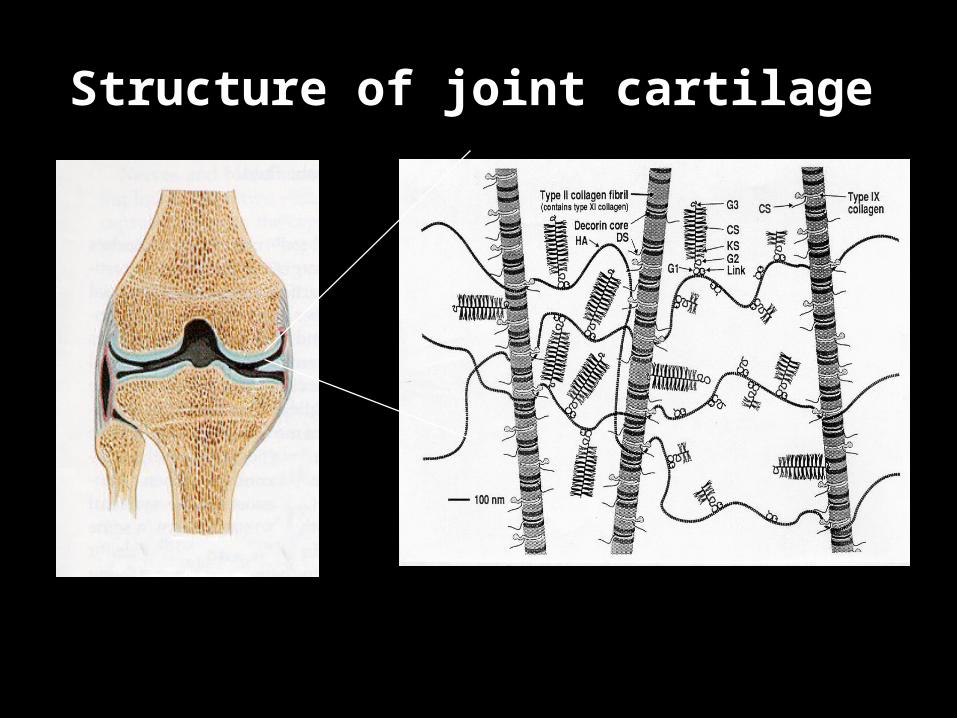
Structure of joint cartilageStructure of joint cartilage

Glucosamine
• Sulfur is an essential nutrient for the stabilization of the connective tissue matrix.
• Glucosamie sulfate stimulates the uptake of sulfate ions -> indicater of GAG synthesis by chondrocytes.
• Glucosamine also hinders hyaluronidase (tissue damaging enzyme)
• Glucosamine sulfate improves the lubricant properties of synovial fluid.

Chemical structure of glucosamine
• Aminomonosaccharide synthesized from glucose.
– Glucose + amino acid– C6H14NO5
Process in the body1. Fructose 6 phsophate+glutamine2. Glucosamine 6 phosphate3. UPD N-acetyl glucosamine

Mechanism of action

6
Glucosamine Base, Not Sulfate is Important
•Glucosamine HCl is used to make G•Sulfate which is then converted back to G•HCL in the acid environment of the stomach. 1-2
•Glucosamine that reaches chondrocytes is base, not HCL or sulfate. Sulfate component is cleaved before absorption. All glucosamine salts are 100% ionized in the low pH environment of the stomach. 1-2
1. www.wilkeresources.com/WILKEresources/GlucosamineHistorical.htm 2. www.wilkeresources.com/WILKEresources/GlucosamineHClvsSulf.htm3. Pharmacology 5:337-345, 1971

7
Glucosamine Base, Not Sulfate is Important
• One study suggested that the glucosamine base, not the sulfate was the active component in beneficially altering OA pathways in equine cartilage explants.
Conclusion: Glucosamine HCL and G•Sulfate have similar abilities to prevent or reduce cartilage degeneration in vitro.1
1. Fenton JI, et. al. Osteoarthritis and Cartilage (2000) 8, 444-451 2. Lippiello L. J. Clin. Ortho. Rel. Res. (2000) 381; 229-240

7
Glucosamine Base, Not Sulfate is Important
•The two, small, negative clinical studies on G•HCL have major flaws
• A disease-modifying, histologic animal study shows significant effects for both G•HCL and CS, with the combination yielding the best results2
1. Fenton JI, et. al. Osteoarthritis and Cartilage (2000) 8, 444-451 2. Lippiello L. J. Clin. Ortho. Rel. Res. (2000) 381; 229-240

Safety
• The clinical studies have consistently reported that glucosamine appears safe.
• No allergic reactions have been reported although glucosamine is derived from shellfish
• Allergy to shellfish may wish to avoid glucosamine.
• May not have acute oral toxicity in animal• Glucosamine may increase on insulin resistance
Glucosamine sulfate
• An optimal treatment for osteoarthritis would be one that modifies the joint structure andreturns the joint to its normal,healthy state. So far, medicine has not been able to produce such a therapy
• Some researchers think glucosamine might be a candidate
• In the case of glucosamine, some of it is deserved. But the research has been conflicting and confusing

Glucosamine sulfate• Over 20 clinical studies lasting up to 3 years and
enrolling over 2500 patients have been conducted, evaluating glucosamine for OA.
• The vast majority of these studies evaluated glucosamine SULFATE for osteoarthritis of the KNEE.
• Overall, when the findings of these studies are pooled, glucosamine appears to reduce pain scores by 28% to 41%, and to improve functionality scores by 21% to 46%.
• Poolsup N, Suthisisang C, Channark P, Kittikulsuth W. Glucosamine longterm treatment and the progression of knee osteoarthritis: systematic review of randomized controlled trials. Ann Pharmacother 2005;39:1080-7.• Towheed TE, Maxwell L, Anastassiades TP, et al. Glucosamine therapy for treating osteoarthritis. Cochrane Database Syst Rev 2005;(2):CD002946

Glucosamine sulfate
For pain relief, GS 1500 mg qd appears to be :
• comparable to ibuprofen 1200 mg daily
• comparable to piroxicam (Feldene) 20 mg daily
• comparable to acetaminophen 1000 mg three times daily
1. Lopes Vaz AL. Curr Med Res Opin 1982;8:145-9.2. Qiu GX, Gao SN, Giacovelli G, et al.. Arzneimittelforschung 1998;48:469-743. Forster K, Schmid K, Rovati L, et al.. Eur J Clin Pharmacol 1996;50:542.4. Herrero-Beaumont G, Ivorra JA, Del Carmen Trabado M, et al.. Arthritis Rheum
2007;56:555-67.

Glucosamine sulfate
• The effects of GS appear to last longer than these analgesics, but the analgesics work much faster.
• NSAIDs relieve symptoms within 2 weeks. GS takes 4‐8 weeks.
1. Lopes Vaz AL. ts. Curr Med Res Opin 1982;8:145-9.2. Qiu GX, Gao SN, Giacovelli G, et al. Arzneimittelforschung
1998;48:469-74

Glucosamine sulfate• Researchers have speculated for years that GS could
potentially modify joint structure and possibly reverse or slow disease progression
• In 2001, a study published in Lancet showed that GS might have this effect. Researchers measured joint space narrowing in patients taking GS
• After 3 years of treatment, these patients did not have further joint space narrowing, suggesting that GS might have slowed or stopped disease progression.
1. Natural Medicines in the Clinical Management of Osteoarthritis. Natural Medicines Comprehensive Database, Clinical Management Series. 2010
2. Reginster JY, Deroisy R, Rovati LC, et al. Long-term effects of glucosamine sulfate on osteoarthritis progression: a randomized, placebo-controlled trial. Lancet 2001;357:251-6.
Glucosamine sulfate• In 2002, a similar 3‐year study published in the Arch of
Internal Med showed that patients taking GS did not have increased narrowing of the joint space, again suggesting that GS slows disease progression
• A meta‐analysis of study results suggests that patients taking GS 1500 mg/day have 54% reduced risk of OA disease progression
• A retrospective analysis of patients who took GS for 1‐3 years also showed that glucosamine sulfate is associated with a 57% decreased risk of total knee replacement
1. Pavelka K, Gatterova J, Olejarova M, et al. Arch Intern Med 2002;162:2113-232. Poolsup N, Suthisisang C, Channark P, Kittikulsuth W. Ann Pharmacother 2005;39:1080-7. 3. Bruyere O, Pavelka K, Rovati LC, et al. Osteoarthritis Cartilage 2008;16:254-60.

Glucosamine sulfate
• Although most of the research has been positive, especially related to glucosamine sulfate, some research findings have been negative
• The reason for the discrepancies is not completely known; however, some experts suspect that different methodologies for assessing improvement, different product formulations, and perhaps different patients have contributed
1. McAlindon T, Formica M, LaValley M, et al. Am J Med 2004;117:643-9.2. Cibere J, Kopec JA, Thorne A, et al.. Arthritis Rheum 2004;51:738-45.3. Towheed TE, Maxwell L, Anastassiades TP, et al. Cochrane Database Syst Rev 2005;(2):CD002946..

Chondroitin Sulfate
Endogenous glycosaminoglycan incorporated into joint matrix
“Heparinoid structure”
Synthetically produced or naturally derived from animal sources
Proposed MOAStimulate chondrocyte metabolismSynthesize collagens & proteoglycansProduction of hyaluronic acid by synovial cells
Gregory PJ et al. Am Fam Physician. 2008;77(2):177-184.Image from www.fulwood.org

Chondroitin Sulfate
• Like glucosamine, chondroitin appears to serve as a substrate for the formation of the joint matrix structure.
• Chondroitin sulfate alone seems to be effective for improving symptoms of OA when used in conjunction with analgesics.
1. •McAlindon TE, LaValley MP, Gulin JP, Felson DT.. JAMA 2000;283:1469-75.2. • Leffler CT, Philippi AF, Leffler SG, et al. Mil Med 1999;164:85-91.3. • Mazieres B, Combe B, Phan Van A, et al. J Rheumatol 2001;28:173-81.

Chondroitin Sulfate
• Trials evaluating a specific blend of glucosamine hydrochloride plus chondroitin sulfate have also been positive.
• Preliminary evidence also suggests that chondroitin might slow joint space narrowing.
1. Leffler CT, Philippi AF, Leffler SG, et al.. Mil Med 1999;164:85-91.2. Das A Jr, Hammad TA..Osteoarthritis Cartilage 2000;8:343-50.3. Uebelhart D, Thonar EJ, Delmas PD, et al.. Osteoarthritis Cartilage 1998;6:39-46.4. Verbruggen G, Goemaere S, Veys EM. Clin Rheumatol 2002;21:231-43.

Chondroitin: Efficacy
Reinchenbach S et al. 2007 (20 trials)Meta-analysis 1966-2006Little to no symptomatic benefit shown
Clegg DO et al. 2006 [GAIT] (n = 1583)No significant difference in symptoms, but was shown to significantly joint swelling
Kahan A et al. 2009 [STOPP] (n = 622)Two yr, randomized double-blind placebo controlled800 mg/day vs. placeboPrimary endpoint: Loss in minimum joint space widthStatistically significant in the primary endpoint & achieved pain relief faster up to 9 months

Chondroitin: Efficacy• However, a 2006 study in the New England Journal of Medicine
(GAIT) found that glucosamine HCL or chondroitin or the combination of both was ineffective for relieving symptoms of osteoarthritis.
• In a subgroup of patients with more severe osteoarthritis, the combination provided modest relief, while the single agents did not.
• Some have interpreted this study to suggest that the COMBINATION of glucosamine hydrochloride plus chondroitin could be used for more severe osteoarthritis.
Clegg DO, Reda DJ, Harris CL, et al. Glucosamine, chondroitin sulfate, andthe two in combination for painful knee osteoarthritis. N Engl J Med 2006;354:795-808.

Placebo effect in mild: 60%!
Used Glucosamine Hydrochloride
Combined tx significant change vs. placebo in Mod-Severe subgroup

8
Chondroitin Key Points
•The dose of CS shown effective is 800-1,200 mg; Glucosamine 1,500 mg 1-2
•Oral CS absorption is about 12%.3 For alendronate, an FDA-approved drug treatment for osteoporosis, oral absorption is < 1%.4 Absorption determines dose, not effect of treatment
•All Chondroitin Sulfate (CS) clinical studies are positive for either WOMAC/Lesquene Index/VAS 1-2 or radiographic outcomes
1. Arch Intern Med. 2003;163:1514-1522 2. JAMA March 15, 2000 Vol 283, No. 113. Osteoart. & Cart. (1998) 6;14-214. PDR data5. Michel BA, Stucki G, et. al. Retardation of Knee Joint Space Narrowing Through Chondroitin 4&6 Sulphate.
Arthritis & Rheumatism. Vol. 48, No. 9 (suppl) Sept. 2003 p. S77
8
Chondroitin Key Points
•The largest, single structural study for either supplement randomized 300 subjects and lasted two years. The treated group took 800 mg of CS. Minimal joint space width actually increased in the CS users and decreased in the placebo group (p < 0.05). 20% flexed X-Ray positioning guidelines were used.5
1. Arch Intern Med. 2003;163:1514-1522 2. JAMA March 15, 2000 Vol 283, No. 113. Osteoart. & Cart. (1998) 6;14-214. PDR data5. Michel BA, Stucki G, et. al. Retardation of Knee Joint Space Narrowing Through Chondroitin 4&6 Sulphate.
Arthritis & Rheumatism. Vol. 48, No. 9 (suppl) Sept. 2003 p. S77

Images from www.mirror.co.uk and www.fsinh.com
After the 1999 Oscars, actor James Coburn credited a regimen of deep tissue massage,
electromagnetic treatment, and MSM with “curing” his arthritis

Methylsulfonylmethane (MSM)): Antioxidants
• Oxidation product of DMSO• Found naturally in green plants, fruits/veggies &
human adrenal glands; commercially produced synthetically
• Upregulates the proteoglycan synthesis of chondrocytes
• Provides a sulfur source for methionine• Thought to reduce inflammation by acting as an
antioxidant (though not proven)

Methylsulfonylmethane ((MSM)
Proposed anti-inflammatory & ↓ degenerative processes
Safety: Insufficient data, as safe as placebo
Efficacy: Insufficient1,2
Two randomized double-blind, placebo-controlled trials looking at pain & physical function over 12 week period
Significantly pain & physical function
Combo w/ glucosamine more effective at pain, swelling &
physical function
Gregory PJ et al. Am Fam Physician. 2008;77(2):177-184.
1.Usha PR et al. Clin Drug Invest. 2004;24:353-363.
2.Kim LS et al. Osteoarthritis Cartilage. 2006;14(3):286-294.

Methyl Sulfonyl Methane MSM
• Systematic Review (Osteoarthritis Cartilage. 2008 Nov) MSM & DMSO in OA
• 2 MSM trials [N=168] “positive but not definitive evidence that
MSM is superior to placebo in the treatment of mild to moderate OA of the knee”
• 500-1000mg BID - TID

Dose/Time frame
Patients should be advised to take
- 1,500 mg of glucosamine daily,
- 1,200 mg of chondroitin daily,
either once daily or in divided doses two/three times daily, and to continue therapy for at least four to eight weeks to allow for onset of benefits

ConclusionAgent Glucosamine Chondroitin Sulfate
Efficacy Inconsistent resultsMay modestly
symptoms & slow disease progression
Sulfate salt = HCL
Inconsistent results; STOPP trial may influence current rec.
May modestly symptomsMay joint space narrowing thus
slowing disease progression
Dosing 1500 mg/dResponse may take ≥4 wk
1200 mg/dPain: Effective up to 9 moDisease modifying: ≥2 yr
Safety Caution w/ shellfish allergy, asthma, warfarin
Not rec. in pregnancy
Caution w/ warfarinHarvested from animal sourcesNot rec. in pregnancy
Other • Single or combined w/ other agent
• Often combined w/ other agents

ConclusionsAgent MSM Combination Products
(glucosamine/chondroitin +/- MSM)
Efficacy May modestly painNot rec. due to insufficient
evidence
Lack of clinical trialsMay modestly symptoms
& slow disease progression
Dosing 1500-6000 mg/dStudied for only 12 wk
See individual products for rec. optimal doses
Safety Well tolerated, no interactions known
See individual products
Other Usually found in combo w/ glucosamine/chondroitin
Found in many product
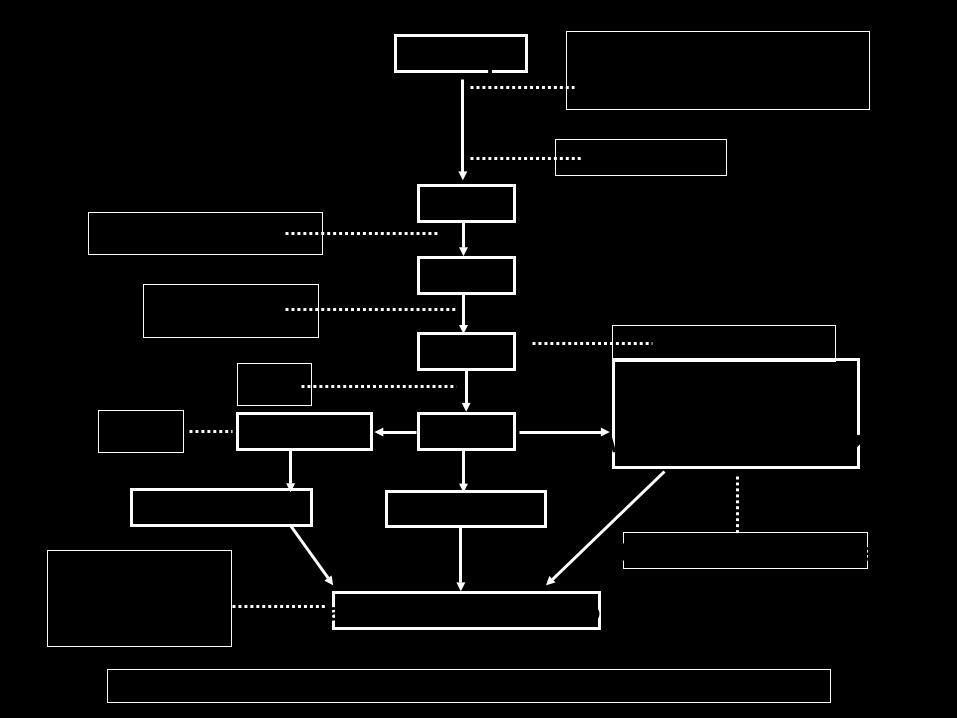
IL1
DNA
mRNA
iNOS
NO
apoptosis
Cartilago Degradation
Inhibitor sitokin( diacerhein, kloroquin ? )
Terapi gen
Inhibitor NOS
Inhibitor protease
CollagenProteoglican
Autolytic Enzyme
ChondroitinGlucosamine
Hyaluronate
Teori kerja beberapa obat pada Osteoartritis
Tetracyklin, ASA, SA
Cyclosporin,Metothrexat
ASA
COX2 NSAID ?
Inflammation

Thank You . . . .
Dr. Blondina Marpaung, SpPD - KR