orthotics … taping … bracing - home page - continuing ed - orthotics taping bracing... ·...
TRANSCRIPT

Orthotics … Taping … Bracing
Ed Mulligan, PT, DPT, OCS, SCS, ATCClinical Orthopedic Rehabilitation Education

Other STJ Neutral Capture Methods
Foam Trays Scanning Systems Slipper Sock

foam tray casting impression
1. Bottom out the heel with the foot mildly supinated2. Depress the lateral side of the foot from the base of the 5th
metatarsal to the 5th toe3. Push the toes into the foam4. Press the met heads from lateral to medial to the bottom of
the foam tray5. Using the web space of your hand, push the talonavicular
area in a posterolateral direction along the STJ axis
Use the “pen” test to check for parallel bottoming out

Starting Position:The patient needs is seated so their knee is at a right angle keeping the leg vertical to the top of the foam tray.
Carefully Lift their feet from the foam. A deep impression of the foot should be seen in the foam. Before you seal the box remember to enclose the prescription form that is provided with each tray. Impression trays can be purchased by the case, each case contains six self-addressed trays.
Do one foot at a time. Position the foot over top the foam area. Make sure your patient maintains a right angle in their leg. Place your finger on their ankle and find the neutral position
Grasp the ankle with your opposite hand and push straight down. Be careful not to let your finger become a part of the impression. Press firmly down until the foot is at the lowest point in the foam. Next, take your finger and press down each toe until the foot is completely flat. Remember, do not let the patient stand in the foam as it will allow the foot to collapse in the arch and the heel to rotate.
Repeat the procedure with the opposite foot. Remember to push the foot to the bottom of the foam tray. Each toe and metatarsal head can be pushed individually to the trays bottom as well as the heel and forefoot. Do not allow the patient to help push down the foam

Scanning Systems
Pedascan– Foot Management’s 2‐D System
Xtremity One– Podiatry Art’s (PAL) 3‐D System
Digital scanning capture system with on‐line forms and ordering systems

Slipper Socks
Resin‐impregnated slipper sock– www.stssox.com for detailed instructions and information
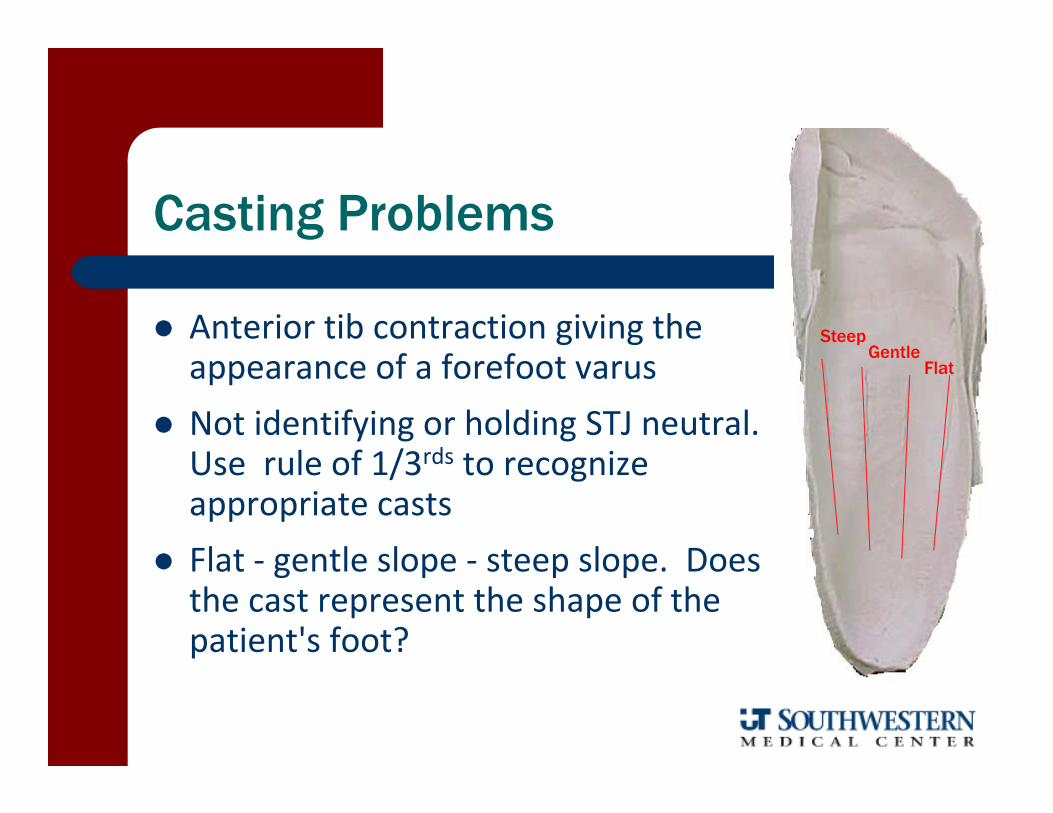
Casting Problems
Anterior tib contraction giving the appearance of a forefoot varus
Not identifying or holding STJ neutral. Use rule of 1/3rds to recognize appropriate casts
Flat ‐ gentle slope ‐ steep slope. Does the cast represent the shape of the patient's foot?
SteepGentle
Flat

Casting Problems
Incomplete or no "loading" of the 4th and 5th metatarsal heads
– Must dorsiflex the plantar surface of the foot until mild tissue resistance is felt.
– The caster may notice a mild thumb indent from where this loading occurred during casting It can be punched out after the cast is removed
Excessive loading can be avoided by placing traction at the 4th and 5th met heads once the initial tissue resistance is met

Casting Problems
Proper loading of the forefoot means ensuring that both the 4th and 5th met heads are loaded and the loading is not proximally on the metatarsal shaft or distally on the phalange

Cast Evaluation
Minimal wrinkles Cast height
– up to the lateral malleolus assists lab in calcaneal bisection but makes it more difficult to remove
Flat dell in calcaneocuboid area with gradual incline beginning 1/3 of the way across the plantar aspect– Pronated cast – flat dell is larger than 1/3 of the distance
– Supinated cast – flat dell is smaller than 1/3 of the distance

Ed Mulligan, PT, DPT, OCS, SCS, ATC

injuries typically related to or effected by pathological hyperpronation
Lower Leg Tendinopathies– posterior tib, anterior tib, peroneal, and Achilles tendinitis
Hallux Abductovalgus Metatarsal Stress Fractures Morton’s Neuroma Plantar Fasciitis Patellofemoral Syndrome (malalignment) Anterior Cruciate Ligament Injury Low Back Injuries

“Podiatric” -biomechanical

orthotic therapy
• PURPOSE− allow the subtalar joint to function near and around its neutral position
• ACCOMPLISHED by− balancing the forefoot to the rearfoot− balancing the rearfoot to the supporting surface
orthotic therapyalternative theories
• Provides a means for medial longitudinal arch support
• Pre‐positions the foot so that as it enters the propulsive phase it minimizes deleterious stresses
• Proprioceptive influence to control the amount and rate of pronation

orthotic indications
1. Support or correct structural deformities of the rearfoot and forefoot
2. Influence, support, or restrict range of motion3. Treatment of postural abnormalities4. Dissipate pathological ground reaction forces5. Decrease shear forces or tender spots on the plantar surface
of the foot by redistribution of weight bearing to more tolerant areas
6. Control abnormal transverse plane rotation of the lower extremity

Who really benefits from an orthotic device?
1. Recent IDF changes in ADLs or recreation activities have been minimal
2. Significant navicular drop relative to Feiss line from non‐weight bearing to weight bearing posture
3. Difficult to detect stiffening of midfoot and/or forefoot when STJ is supinated
4. Structural RF or FF abnormality that causes pathological hyperpronation compensation

orthotic contraindications
Lack of intrinsic or structural foot abnormality– i.e. – soft tissue induced equinas (tight Achilles)– Muscle imbalances
Incomplete lower quarter biomechanical examination

orthotic anatomy
• Module or Shell− The body of the orthotic that conforms
to the patient’s plantar contours
• Post− The “shim” placed on the front or rear
of the shell to bring the ground up to− the foot and place the STJ in its neutral position

orthotic types
• Biomechanical− controls and resists abnormal compensatory foot forces
• Accommodative− supports the foot− allows the foot to compensate and yields to abnormal foot forces− posting is referred to as “bias”
• Diabetic− total foot contact to disperse weight as evenly as possible on the
plantar surfaces− reduce pressure in ulcer prone areas
biomechanical orthotics
Rigid – maximal control
– minimal flexibility
– normally met head length
– rohadur, graphite, polypropylene, fiberglass

biomechanical orthotics
Semi‐rigid– partial control
– semi‐flexible or flexible
– normally toe sulcus length
– thermoplastics or cork

accommodative orthotics
Soft– shock absorption
– normally full length
– plastizote or PPT

orthotic posting
LOCATION rearfoot and forefoot
TYPES tip and bar
ANGULATION varus (medial angulation)valgus (lateral angulation)
CONSTRUCTION Intrinsic‐post within the moduleExtrinsic‐post external to the module

RF Medial Wedge RF Lateral Wedge FF Medial Wedge FF Lateral Wedge FF Bar
Tip Post Bar Post
Modular Orthotic Systems
www.vasylimedical.com/products/product_additions.html
www.palhealth.com/underdogs.php
www.footmanagement.com/acc.php
www.alimed.com/Alimed/catalog/Orthotic-Arch-Supports,259.htm

Over-the-Counter Insoles
www.superfeet.com
temporary orthotic demo

primary considerations in selecting an orthotic
• Physiological Age− not chronological age ‐ older/softer
• Mobility/Restriction Foot Motion− general foot mobility− hypo‐normal‐hyper
• Primary activity for orthotics − sport vs. street− straight ahead vs. pivots

• Chief Complaint/Diagnosis• specific complaint − need for accommodations
• Control of STJ/MTJ motions− control vs. bias
• Shock absorption provided/necessary− dissipation of ground reaction forces − proximal injury
primary considerations in selecting an orthotic

Weight of Patient – consider durometer or flex code – rigidity and firmness
Neurological or Anatomical Abnormalities − need for accommodation, top covers, etc
primary considerations in selecting an orthotic

decision making continuum
rigidsemi-rigidsoft
accommodative biomechanical
age patient size motion control shock absorption activities shoes chief complaint specific problem

SOFTER ORTHOTIC
Higher arch Stiff foot Older Patient Support
RIGID ORTHOTIC
Lower Arch Mobile Foot Younger Patient Control
Orthotic decision making summary

orthotic prescription forms
• Patient Information− Weight, shoe size‐style, activities, occupation
• Product Selection− type of orthotic
• Orthotic Instructions− Width, forefoot and rearfoot posting
− “Post to cast and standard RF post”

orthotic instructions
SHELL WIDTH Narrow
– Ladies dress, bicycling shoes, skates, ski boots
– 5/16” “in” ‐ (normal is 3/16” “in”)
Wide– Lateral motion sports, children– Flush with most medial and lateral aspect of 1st and 5th met heads

• Patient Information− Weight, shoe size‐style, activities, occupation
• Product Selection− type of orthotic
• Orthotic Instructions− Width, forefoot and rearfoot posting
• Extensions (Covers)− Materials, length, pockets
• Specialties− Specific accommodations
• Comments:− General history, diagnosis, specific requests
orthotic prescription forms

Met Head Length Sulcus Length Full Length Wide Grind Athletic
Narrow Grind Street Morton’s Extension Medial Clip Lateral Clip
Cobra Pad Neutral Shell Heel Lift Heel Spur Pad

Dancer’s Pad Med Pad (Rise) Met Bar Sesamoid Cut-Out
Forefoot Varus Post Forefoot Valgus Post Rearfoot Varus Post Rearfoot Valgus Post

orthotic accommodations-modifications
SHELL DEPTH Shallow
– Ladies dress or narrow width Normal
– Casual and athletic shoes Deep
– High impact athletic shoes– Increased rearfoot control

shoe selection for orthotic use
snug, deep, stable heel counter with minimal heel height
adequate shoe depth (toe and heel) remove insoles and arch cookies straighter lasts blucher style throat with at least 3 eyelets for lacing for narrow shank dress shoes must use "cobra pad"
– entire orthotic is posting
generally, athletic shoes and work boots are wider and roomierto allow better fit and provide more support and control
shoe selectionfor orthotic use
• No one orthotic works adequately in ALL shoes− May need to have 2‐3 pairs or fit the orthotic to the shoe that is used most commonly during symptomatic periods
• Some shoes will not accommodate or are hard to fit with orthotics− Higher heels− Narrow shoes (cowboy boots)
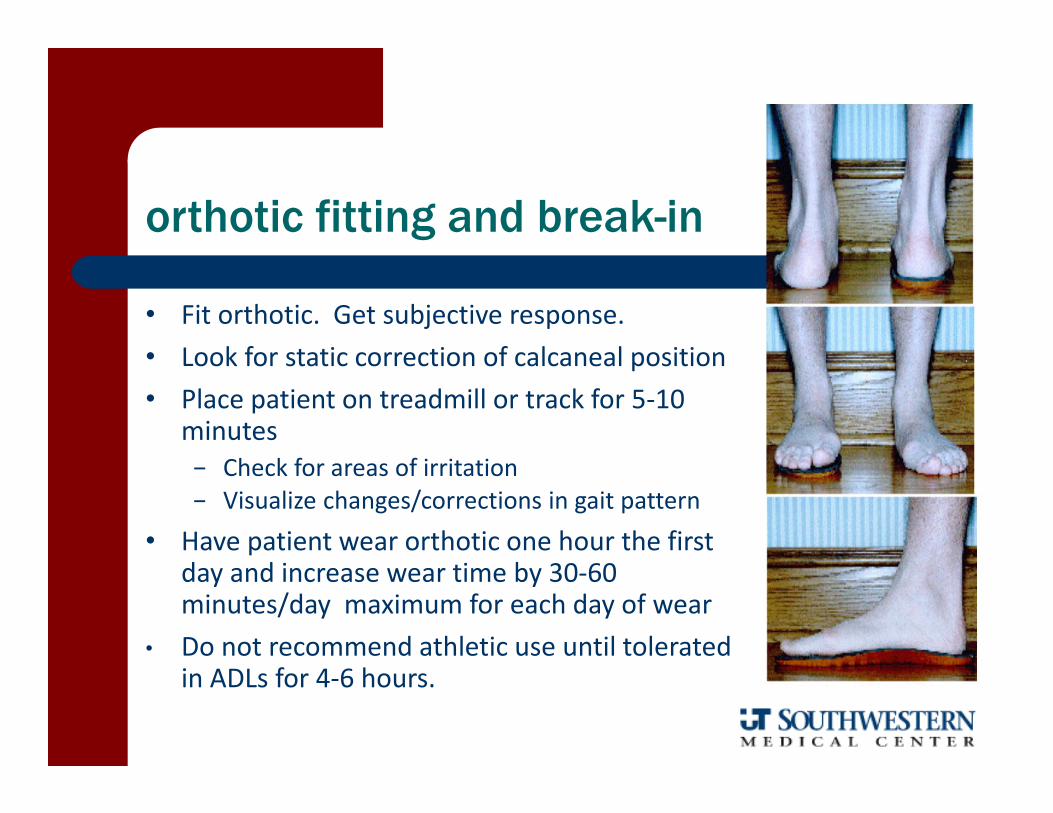
orthotic fitting and break-in
• Fit orthotic. Get subjective response.• Look for static correction of calcaneal position• Place patient on treadmill or track for 5‐10
minutes− Check for areas of irritation− Visualize changes/corrections in gait pattern
• Have patient wear orthotic one hour the first day and increase wear time by 30‐60 minutes/day maximum for each day of wear
• Do not recommend athletic use until tolerated in ADLs for 4‐6 hours.

orthotic labs and services
types of orthotics available cost preferred fitting
– casting methodology shipping additional services CUSTOMER SERVICE what labs have you had success with?

LBG Corporate Headquarters450 Commack Road; Deer Park, NY 11729800‐233‐2687www.langerbiomechanics.com
PAL Health Systems1805 Riverway Drive; Pekin, IL 615441‐800‐447‐0151www.palhealth.com
Foot Management7201 Friendship Road; Pittsville, MD 218501‐410‐835‐3668www.footmanagement.com
Orthotic Labs

So, does orthotic therapy work?
Yes, only debate is how – Biomechanical correction?
Root Podiatric Perspective− Modification of Tissue Stress?
McPoil/Cornwall PT Perspective
Kinematic Change? – “minimizing muscle activity
Benno Nigg
Additional Evidence of Effectiveness
Orthotics fabricated from STJN were 78% effectiveBlake Rl, Denton JA. Functional foot orthoses for athletic injuries: a retrospective
study. J Am Podiatr Med Assoc 1985 75(7):359‐362.
91% orthotic satisfaction rateDonatelli R, Hurlbert C, Conaway D, St. Pierre R: Biomechanical foot orthotics: a
retrospective study. J Orthop Sports Phys Ther 1988;10(6):205‐212.
93% satisfaction and 95% resolution of symptomsMoranos J, Hodge W. Orthotic survey: preliminary results. J
Am Podiatr Med Assoc 1993 83(3):139‐148.
Orthotics effective for a variety of conditionsLandorf KB, Keenan A‐M. Efficacy of foot orthoses. J Am Podiatr Med
Assoc 2000;90(3):149‐158.

Systematic Review and Analysis
Orthotics (custom or prefabricated) are effective at preventing first occurrence lower extremity overuse conditions
The cost of prefabricated foot orthotics is low and few adverse effects have been reported (wear discomfort most common)
Individuals typically report decreased lower limb pain with the use of foot orthotics
We have inadequate research to definitively say that orthotics work or not but based on the low risk and potential benefits of this intervention, I believe foot orthotics are an important consideration as part of the treatment of an individual with a lower limb overuse injury
Richter RR, et al, J Athl Train, 2011Collins N, et al, Foot Ankle Int, 2007

The more poorly something isunderstood, the more theoriesthere will be about it.”
Craig PayneDepartment of Podiatry
La Trobe University
Bracing vs. Taping

What does the literature tell us about taping and bracing of the foot and ankle?
Impact on Proprioception/Balance
Seems to improve balance and proprioception but mechanism is unclear– Conflicting or no evidence for improved peroneal reaction time
– Does not seem to enhance ability to detect inv/eversion movements
Ozer D, et al, Foot, 2009Refshauge KM, et al, Am J Sports Med, 2009Shima N, et al, Intl J Sports Med, 2005Robbins S, et al, Br J Sports Med, 1995Karlsson J, et al, Am J Sports Med, 1992Konradsen L, et al, Int J Sports Med, 1991
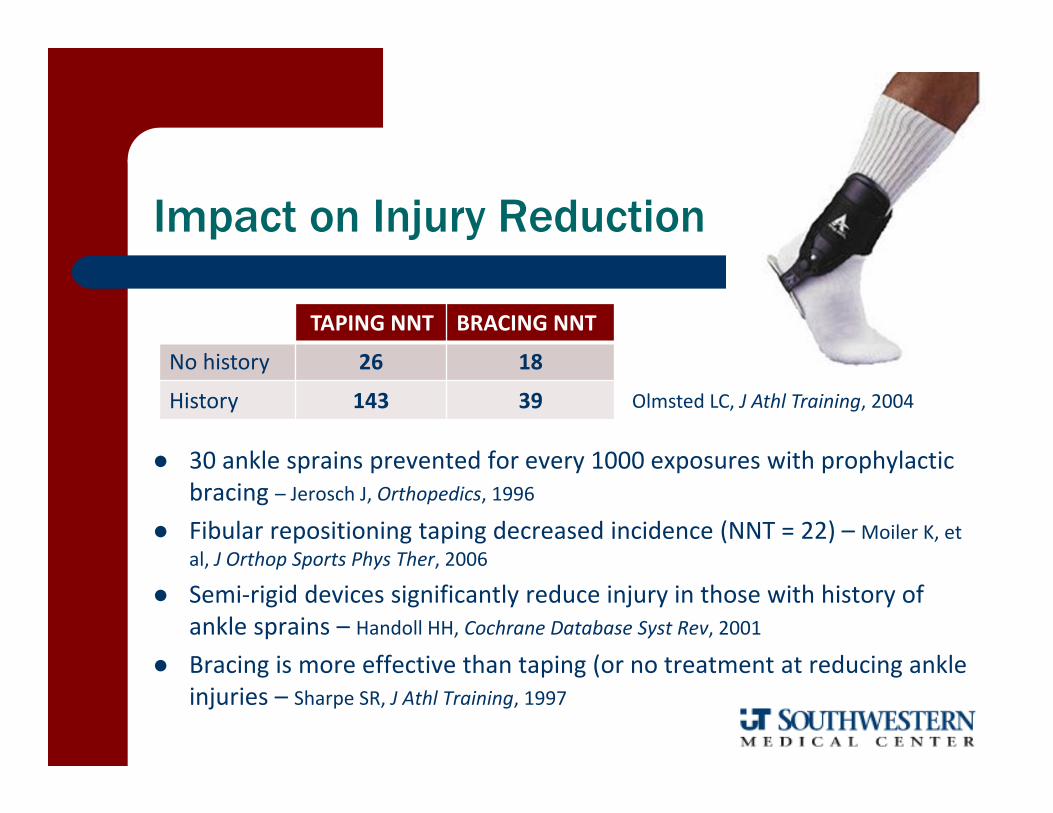
Impact on Injury Reduction
30 ankle sprains prevented for every 1000 exposures with prophylactic bracing – Jerosch J, Orthopedics, 1996
Fibular repositioning taping decreased incidence (NNT = 22) – Moiler K, et al, J Orthop Sports Phys Ther, 2006
Semi‐rigid devices significantly reduce injury in those with history of ankle sprains – Handoll HH, Cochrane Database Syst Rev, 2001
Bracing is more effective than taping (or no treatment at reducing ankle injuries – Sharpe SR, J Athl Training, 1997
TAPING NNT BRACING NNT
No history 26 18
History 143 39 Olmsted LC, J Athl Training, 2004
Impact on Function
Decreases in performance are minor and should not be used as deterrent for prophylactic support– No substantial effect on agility, sprinting, or jumping
Verbrugge JD, J Orthop Sports Phys Ther, 1996Beriau, et al, J Athl Training, 1994
– Does not impair basketball related skillsMacKean LC, et al, J Orthop Sports Phys Ther, 1995
– Does not negatively impact balance or agilityParis, J Athl Training, 1992

Impact of Activity on Stability Protection
Taping– Motion restriction decreases after 10‐20 minutes
Lohkamp M, et al, J Sports Rehab, 2009
– Sway control diminished after exerciseLeanderson J, et al, Knee Surg Sports Traumatol, 1996
Bracing– More effective at restricting motion (immediately
and after activity)Verhagen EA, Sports Med, 2001; Martin N, et al, J Athl Training, 1994
Bracing most effective at limiting inv/eversion and taping most effecting at limiting dorsiflexion
Cordova ML, J Orthop Sports Phys Ther, 2000

Decision
Bracing more comfortable– Stoffel KK, et al, Med Sci Sports Exer, 2010
Bracing more affordable– Mickel TJ, et al, J Foot Ankle Surg, 2006
Bracing more accessible
Bracing more effective in restricting ROM– Lindley TR, J Athl Training, 1995
Bracing more effective at reducing injury– Surve, et al, Am J Sports Med, 1994

Breg – Gridiron Ultra Ankle Brace
DonJoy Velocity Swedo
AirCastActive Ankle Support
Bauerfeind MalleolocMcDavid
Kallassy Brace
Sample Commercial Ankle Braces

Spatting
Expensive “fashion” statement or effective means of injury prevention?
external shoe support produced a significant reduction in the amount and rate of STJ inversion range when healthy subjects were exposed to an unanticipated inversion moment
No change if no tape, better motion restriction and velocity reduction with spatting alone, even better with traditional ankle strapping, and best with strapping + spatting. – This was true even after 30 minutes of exercise (although the effect on
both dependent variables began to wane)
Precaution is that this is only potentially valuable for cleated shoes– Spatting definitely alters the frictional stability/resistance to
rotational stress in court type shoes

Arch Taping

Arch (Low‐Dye) taping exerts a biomechanical anti‐pronation effect– Increases arch height 1‐2 mm that diminishes with exercise
– alters neuromuscular activity
Franettovich M, et al, Gait Posture, 2010 and Sports Med, 2008Vicenzino B, et al, Br J Sports Med, 2005Holmes CF, et al, J Orthop Sports Phys Ther, 2002Schulthies SS, et al, J Orthop Sports Phys Ther, 1991
What does the literature tell us about arch taping?

Questions?