orthostatic hypotension and nicotine sensitivity a …jnnp.bmj.com/content/jnnp/32/1/28.full.pdfone...
TRANSCRIPT
J. Neurol. Neurosurg. Psychiat., 1969, 32, 28-34
Orthostatic hypotension and nicotine sensitivityin a case of multiple system atrophy
J. G. GRAHAM AND D. R. OPPENHEIMER
From the Department of Neurology, Cardiff Royal Infirmary, and the Department of Neuropathology,the Radcliffe Infirmary, Oxford
Shy and Drager (1960), on the basis of some 40published case reports, described a clinical syndrometo which their names have subsequently beenattached. The complete syndrome includes ortho-static hypotension, anhidrosis, urinary and faecalincontinence, sexual impotence, Parkinsonian signs,external ocular palsies, amyotrophy, and irisatrophy. A detailed post-mortem examination ofone of their cases showed neuronal degeneration atmany sites, including the intermediolateral columnsof the spinal cord. They did not comment on therelation of this finding to the autonomic features oftheir patient's disorder.
In 1965, Fichefet, Sternon, Franken, Demanet,and Vanderhaeghen described a case presenting withorthostatic hypotension, with subsequent develop-ment of Parkinsonism. The pathology was that ofidiopathic paralysis agitans, with Lewy-type cyto-plasmic inclusions and loss of pigmented nerve cells.In addition, the authors observed some cell loss inthe anterior and lateral horns of the spinal cord.
In 1966, Johnson, Lee, Oppenheimer, andSpalding described the clinical, physiological, andpathological findings in two cases of orthostatichypotension. In the first of these, the only associateddisturbances were sexual impotence and loss ofsweating. Lewy-type inclusions were found in thepigmented nuclei and elsewhere, but there was nodetectable loss of pigmented cells. Cell loss in theintermediolateral columns was estimated at nearly90%. In the second case, the autonomic disorderwas followed, after a few years, by a progressivedisorder of motor and cerebellar function. Thelesions were those of olivo-ponto-cerebellar atrophy;in addition, there was cell loss, estimated at about75 %, in the intermediolateral columns. Since then,there have been four reports on cases that have goneto necropsy-that of Nick, Contamin, Escourolle,Guillard, and Marcantoni (1967) and the two casesof Schwarz (1967)-all of which showed neuronaldegeneration at various sites, including the inter-
28
mediolateral columns; and the case of Martin,Travis, and van den Noort (1968), which showed norelevant CNS pathology.The case reported here showed certain features of
the Shy-Drager syndrome, including orthostatichypotension, impotence, and incontinence. Thepatient also suffered from a cerebellar type of ataxia,which was temporarily made very much worse bysmoking a cigarette. This type of sensitivity tonicotine has been reported by Spillane (1955) inpatients with spino-cerebellar disease, but not,hitherto, in association with the Shy-Drager syn-drome. The object of this paper is to provideevidence that (1) in this, as in other cases of theShy-Drager syndrome, the basic disease is a primaryatrophy of a selection of neurones in the CNS;(2) the features of sympathetic failure, includingorthostatic hypotension, are attributable to cell lossin the intermediolateral columns; (3) nicotinesensitivity is associated with cerebellar system dis-orders, which are present in some cases of theShy-Drager syndrome. There does not appear to bea direct connection between nicotine sensitivity andautonomic failure.
CASE REPORT
A 60-year-old unmarried male street photographer wasadmitted to hospital in April 1964 complaining ofunsteadiness of gait, which had developed over the pastfour months. For 18 months, he had had urinary hesit-ancy, dribbling, and nocturnal incontinence, and sexualimpotence. He had noticed that cigarette smoking madethe unsteadiness very much worse, and made his legsfeel 'wooden'. A year before, in a cinema, he had goneto the back of the auditorium for a smoke. He re-membered lighting a cigarette, and the next memory wasof regaining his senses in the manager's office, feelingunwell, but rapidly returning to normal. It is not knownwhether he struck his head in falling. Witnesses made nomention of convulsive movements.Apart from three attacks of chest pain at rest, each
lasting a quarter of an hour, there was no relevant past
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from
Orthostatic hypotension and nicotine sensitivity in a case of multiple system atrophy
medical history. His mother died aged 35, of unknowncauses, and his father aged 56, of Bright's disease. Hisfamily consisted of one half-brother and one aunt, bothhealthy.On admission, he was unkempt and slovenly, but of
high intelligence and lively wit. The pulse was regularat 100/min, and the blood pressure (taken lying down),was 170/100mm Hg. The bladder was palpably distended,without distress. The gait was broad-based and ataxic,and walking heel to toe was impossible. Speech wasslurred, and there were permanent small collections ofsaliva at the angles of the mouth. There were no cranialnerve lesions, and no nystagmus. In the upper limbs tone,power and co-ordination were normal; the reflexes weresymmetrically hyperactive, with brisk finger jerks, butnegative Hoffmann's and Wartenberg's signs. The lowerlimbs, especially the left, were ataxic, with slight proximalweakness. The right plantar response was absent, theleft flexor. All modalities of sensation were normal.
Investigations included a full blood count, blood urea,serum cholesterol, serum proteins and electrophoresis,midstream urine analysis, liver function tests, bloodWassermann reaction, radiography of chest (withscreening), abdomen, skull, dorsal and lumbar spine,electrocardiography and electroencephalography (EEG).The only abnormalities were an ESR of 38 mm in 1 hr,a trace of albuminuria with sterile culture, and slightlyraised serum a and P globulin concentrations. A diagnosisof spinocerebellar degeneration was made, and vitaminsB1 and B12 prescribed as a placebo.He was not seen again until July 1966, when he was
readmitted, all the earlier symptoms and signs havingworsened. His speech was now barely intelligible, andbecame quite unintelligible after smoking a cigarette. Hewas unable to walk without assistance and had to weara portable urinal. He was more unkempt than ever, buthis intellect was quite unimpaired and contrasted evenmore sharply with his physical state. There was nonystagmus. He had gross ataxia with slight proximalweakness in all four limbs; reflexes remained sym-metrically hyperactive, abdominal reflexes were absent,and plantar responses were equivocal. There was impair-
ment of vibration sense in both feet, but no other sensorydisturbance. He had bilateral dependent oedema.
In addition he complained of about six attacks ofabrupt loss of consciousness, all of which occurred onrising out of a chair, usually resulting in his falling backinto the chair, and once to the floor. Observers had toldhim that unconsciousness lasted only a few seconds,during which he was pale, with open glazed eyes. He didnot become rigid or convulse. His blood pressure wasrecorded lying and standing over a period of days, andwas persistently lower on standing, often by as muchas 50 to 60 mm Hg systolic.
Investigations at this time included an ESR of 28millimetres, bilateral high tone deafness, worse on theright, a normal EEG, normal cerebrospinal fluid, normalchest and skull radiographs, and an air encephalogramshowing normal posterior fossa anatomy but slightventricular dilatation and a slight excess of air in thecerebral cortical sulci.A histamine infusion test showed that he was almost
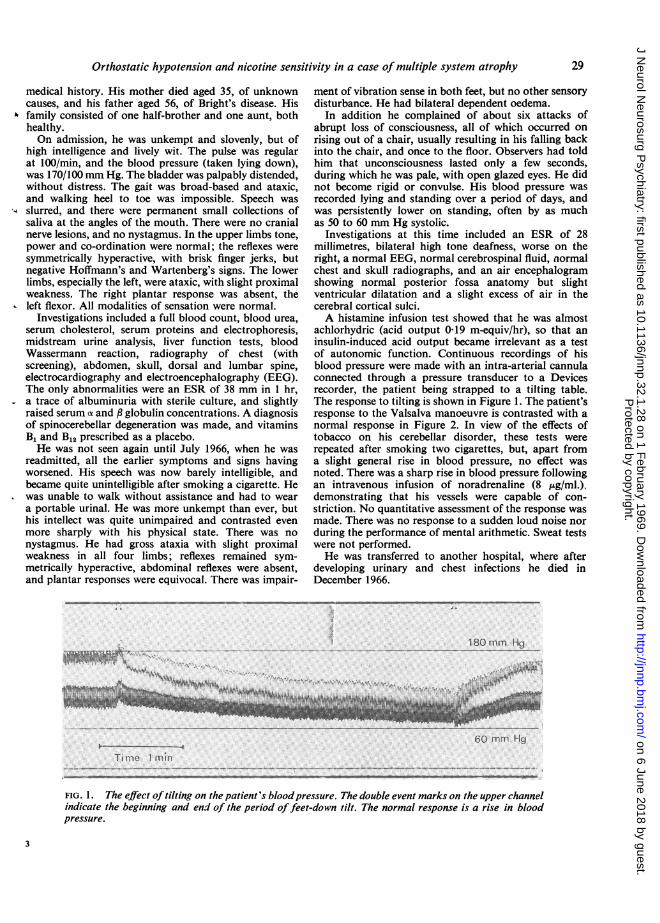
achlorhydric (acid output 0-19 m-equiv/hr), so that aninsulin-induced acid output became irrelevant as a testof autonomic function. Continuous recordings of hisblood pressure were made with an intra-arterial cannulaconnected through a pressure transducer to a Devicesrecorder, the patient being strapped to a tilting table.The response to tilting is shown in Figure 1. The patient'sresponse to the Valsalva manoeuvre is contrasted with anormal response in Figure 2. In view of the effects oftobacco on his cerebellar disorder, these tests wererepeated after smoking two cigarettes, but, apart froma slight general rise in blood pressure, no effect wasnoted. There was a sharp rise in blood pressure followingan intravenous infusion of noradrenaline (8 ug/ml.),demonstrating that his vessels were capable of con-striction. No quantitative assessment of the response wasmade. There was no response to a sudden loud noise norduring the performance of mental arithmetic. Sweat testswere not performed.He was transferred to another hospital, where after
developing urinary and chest infections he died inDecember 1966.
^. 180mm HgS ......~~~~~~~~~~~~~~~~~~~........ ..... S.
i\
60 nmtmi HgTL me 1 men
. ...
FIG. 1. The effect oftilting on the patient's bloodpressure. The double event marks on the upper channelindicate the beginning and end of the period offeet-down tilt. The normal response is a rise in bloodpressure.
29
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from

J. G. Graham and D. R. Oppenheimer
rTirfe it,S
FIG. 2a.
_A
L
T - "I' .,i F ..
FIG. 2b.
FIG. 2. Blood pressure response to the Valsalva manoeuvre. Normal response in upper
recording. Note the failure of 'rebound' in the patient's record.
4. fitU,I.1111,111111[itmI
30
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from

Orthostatic hypotension and nicotine sensitivity in a case of multiple system atrophy
PATHOLOGY
Necropsy was carried out by Dr. K. M. Laurence, whovery kindly supplied us with the brain, spinal cord, andother tissues. The gross findings were of purulent tracheo-bronchitis, bilateral bronchopneumonia, old pleurisy,old apical tuberculosis, and atheroma of the aorta andother main arteries. The brain (1,370 g; hind brain alone150 g) was externally unremarkable, apart from an oldtraumatic scar, 2 cm in diameter, in the right orbitalcortex. The cerebral vessels were healthy. On sectionthere were no naked-eye abnormalities in the brain,spinal cord or nerve roots.
HISTOLOGICAL FINDINGS 1. Cerebral hemispheres Theonly striking abnormality was a symmetrical heavy cellloss, with astrocytic gliosis, in the putamen, affectingparticularly the dorsal and lateral parts. The ventralparts of the putamen, and the caudate nuclei, appearednormal. There was a corresponding loss of myelin, andgliosis without cell loss, in the globus pallidus on bothsides. Cortex, hippocampus, thalamus and amygdaloidnuclei appeared normal; the hypothalamus, examinedat 1 mm intervals, was unremarkable.
2. Brain-stem and cerebellum There was no gross
atrophy of the pons, but there was loss of cells and oftransverse fibres in a narrow strip over the ventralsurface of the pons, and astrocytic gliosis of the remainingpontine nuclei. Symmetrical cell loss and gliosis wereseen in the lateral thirds of the substantia nigra, thedorsal laminae of the inferior olives, the medial vestibularnuclei, the lateral reticular nuclei of the lower medulla,and the dorsal vagal nuclei (Fig. 3). Cranial motor nucleiappeared intact. In the cerebellum there was a severe lossof Purkinje cells in all parts of the vermis, accompaniedby abundant torpedo formations, Bergmann gliosis, andfibrillary gliosis of the white matter. Basket and granulecells were preserved. Purkinje cell loss was patchy andnot very severe in the cerebellar hemispheres. There was
,.7
*r 4
..P.
*..N
FIG. 3. Upper medulla, showing gliosis in the medialvestibular and dorsal vagal nuclei. Holzer stain for fibroglia.
no obvious cell loss in the dentate and roof nuclei, butthese nuclei showed active microgliosis, and a diffusestippling with Sudanophil lipid. The central white mattershowed astrocytic gliosis and slight Sudanophil stippling.There was no demonstrable loss of fibres in the superiorcerebellar peduncles.
3. Spinal cord There was a mild degeneration in bothcrossed and uncrossed pyramidal tracts, more marked inthe lower segments, and not detectable in the medullarypyramids. The spinocerebellar tracts appeared intact.There was no obvious loss of motor cells in the anteriorhorns, but many of them were small and pyknotic. Thecells of Clarke's columns showed an unusual degree ofloading with lipochrome. In the thoracic segments therewas a very severe loss of cells in the intermediolateralcolumns. Cell counts were carried out on six 20,u sectionsfrom each thoracic segment (except TI 1, which wasdamaged post mortem) and the first lumbar segment.The figures (Table I) were compared with pooled controlmaterial, as in Johnson et al. (1966), and with the casesdescribed there. They showed an overall loss of about80% of these cells. The loss was much more severe onthe right than on the left.
TABLE I1MEAN COUNTS OF NUMBER OF CELLS IN EACH LATERAL HORN
IN 20,u SECTIONS, WITH STANDARD ERRORS*
Level Pooled Johnson Johnson Presentcontrols et al. et al. case
(case 1) (case 2)
TI-4 15-8 ± 10 13 ± 03 4-3 ± 05 4-2 ± 0-6(48) (36) (36) (48)
T5-8 9-2 ± 0 7 1-0 ± 0-2 1 9 + 0-2 1-3 ± 0-2(48) (36) (48) (48)
T9-12 9-5 ± 0 7 2-0 i 0 3 2-7 + 0 3 1-3 + 0 2t(48) (36) (48) (48)
*Figures in brackets show the number of counts made at each level.tT9, T10, T12, and LI.
4. Peripheral nervous system There were no detectablechanges in the right vagus nerve. Sections of varioussympathetic ganglia showed loss of fibres in some of thenerve bundles, but no loss of, or morphological changesin, ganglion cells (Fig. 4). Samples of tongue and neckmuscles showed no sign of denervation.
In summary, the pathological findings were of selectiveneuronal degeneration at multiple sites in the centralnervous system. Since no changes were found in thehypothalamus or in peripheral autonomic ganglia, it isreasonable to ascribe the patient's autonomic disorder tothe observed loss of preganglionic autonomic cells.'Schwarz (1967) has expressed doubt as to the possibility ofmaking significant evaluations of cell loss by counting methods.Variations in cell density certainly exist from level to level and fromsection to section. The standard errors, shown above, reflect thisvariation. We are satisfied that the figures obtained in these threeeases show a devastating loss of intermediolateral cells. Loss offunctioning cells is probably still greater, since many shrunken,pyknotic cells were included in the counts.
31
WWIs
I't!::.. .-. io'l
I / I
p.:,--N p
I. ;,.
IL '\.
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from

J. G. Graham and D. R. Oppenheimer
FIG. 4. Thoracic sympathetic ganglion, showingnormal ganglion cells. There is some loss offibresin the bundle on the left. Frozen: Bielschowsky,modified Schofield, x 190.
DISCUSSION
We know of eight previously reported cases ofso-called idiopathic orthostatic hypotension in whicha neuropathological examination has been made. Areport has recently been published by Martin et al.(1968) on a man aged 59 with orthostatic hypo-tension, urinary incontinence, laryngeal and externalocular palsies, unilateral hypoalgesia, and spasticlegs. The authors were unable to demonstrate any
significant lesions in the central or peripheralnervous systems, and are reluctant to believe thatanyone else has succeeded in doing so. The remainingseven consist of case 2 of Shy and Drager (1960);the case of Fichefet et al. (1965); cases 1 and 2 ofJohnson et al. (1966); the case of Nick et al. (1967);cases 1 and 2 of Schwarz (1967). Intermediolateralcolumn degeneration of some degree has been notedin all these; apart from this, the cases appear to fallinto two groups.
In the first group are the case of Fichefet et al.(1965) and case 1 of Johnson et al. (1966), in bothof which there were numerous Lewy-type inclusionbodies in pigmented nuclei and elsewhere. In theformer, clinical Parkinsonism developed beforedeath, and there was marked cell loss in the pig-mented nuclei. In the latter, Parkinsonism did notdevelop, and no pigmented cell loss was seen.Neither case showed cell loss in the basal gangliaor in the cerebellar system; and neither case canproperly be regarded as an example of the Shy-Drager syndrome.The remaining five cases, and the case reported
here, form the second group. The main clinical andpathological features of these are shown in Table II.
The similarities are obvious, and it would be
unreasonable to attach different diagnostic labels tothese cases-for instance, to label four of them'olivo-ponto-cerebellar atrophy' (OPCA) and theother two 'striato-nigral degeneration' (Adams,van Bogaert, and van der Eecken, 1964; Jellingerand Danielcyzk, 1968). The disadvantages of thistype of labelling are apparent from the fact thatAdams et al. (1964) diagnosed one of their cases as'striato-nigral degeneration and olivo-ponto-cere-bellar degeneration'.
Welte (1939), in a review of the pathology ofOPCA, clearly pointed out that the lesions inreported cases were commonly widespread, and veryfrequently, but not always, included the striatumand pigmented nuclei. He commented 'Thesemanifold combinations [of lesions] argue for a closerelationship between all types and sub-types ofsystem atrophies of the central nervous system'. Bythis he presumably meant that these conditionsshared some common aetiological factor. We wouldmake the same point in a different way. There is agroup of progressive neurological conditions, mostoften arising during middle life, with symptoms andsigns of lesions affecting several central nervousstructures, more or less symmetrically. These casesare usually sporadic, but sometimes familial. Thepathological findings are of cell loss and gliosis in aselection of well-defined structures (including bothanatomical 'nuclei' such as the putamen, andextensive cellular layers, such as the Purkinje cellsof the cerebellum). In different cases, differentselections of structures are affected. Some com-binations of lesions are commoner than others;thus, familiar names, such as OPCA, have comeinto use. Nevertheless combinations are encoun-tered which do not correspond with any familiar
32
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from
Orthostatic hypotension and nicotine sensitivity in a case of multiple system atrophy
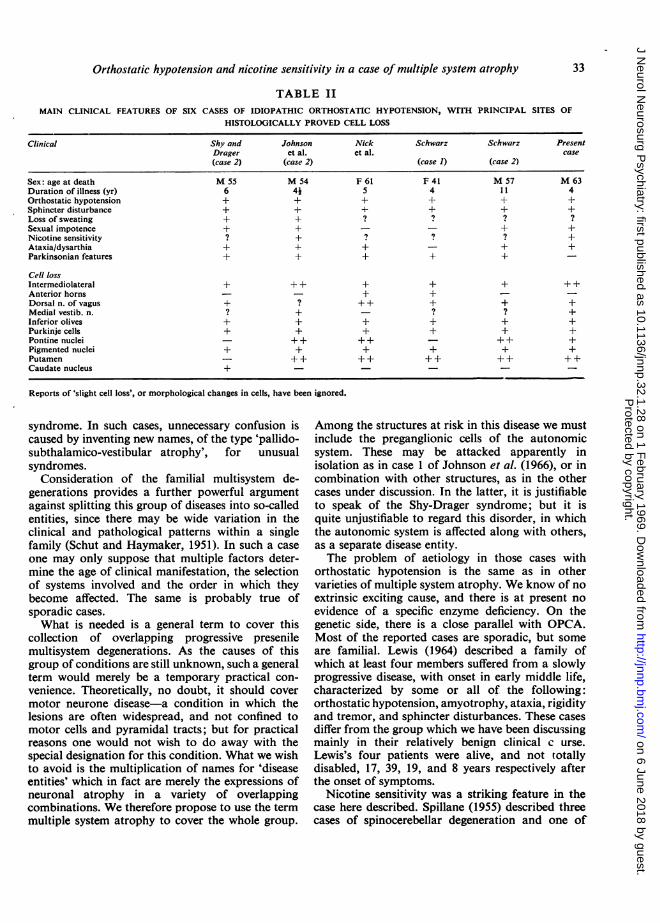
TABLE IIMAIN CLINICAL FEATURES OF SIX CASES OF IDIOPATHIC ORTHOSTATIC HYPOTENSION, WITH PRINCIPAL SITES OF
HISTOLOGICALLY PROVED CELL LOSS
Clinical Shy and Johnson Nick Schwarz Schwarz PresentDrager et al. et al. case(case 2) (case 2) (case 1) (case 2)
Sex: age at death M 55 M 54 F 61 F 41 M 57 M 63Duration of illness (yr) 6 4i 5 4 11 4Orthostatic hypotension + + + + + +Sphincter disturbance + + + + + +Loss of sweating + + ? ? ? ?Sexual impotence + + - - + +Nicotine sensitivity ? + ? ? ? +Ataxia/dysarthia + + + - + +Parkinsonian features + + + + +
Cell lossIntermediolateral + + + + + + + +Anterior horns - - + + - -Dorsal n. of vagus + ? ++ + + +Medial vestib. n. ? + - ? ? +Inferior olives + + + + + +Purkinje cells + + + + + +Pontine nuclei - ++ ++ - ++ +Pigmented nuclei + + + + + +Putamen - + + ++ ++ ++ ++Caudate nucleus +
Reports of 'slight cell loss', or morphological changes in cells, have been ignored.
syndrome. In such cases, unnecessary confusion iscaused by inventing new names, of the type 'pallido-subthalamico-vestibular atrophy', for unusualsyndromes.
Consideration of the familial multisystem de-generations provides a further powerful argumentagainst splitting this group of diseases into so-calledentities, since there may be wide variation in theclinical and pathological patterns within a singlefamily (Schut and Haymaker, 1951). In such a caseone may only suppose that multiple factors deter-mine the age of clinical manifestation, the selectionof systems involved and the order in which theybecome affected. The same is probably true ofsporadic cases.What is needed is a general term to cover this
collection of overlapping progressive presenilemultisystem degenerations. As the causes of thisgroup of conditions are still unknown, such a generalterm would merely be a temporary practical con-venience. Theoretically, no doubt, it should covermotor neurone disease-a condition in which thelesions are often widespread, and not confined tomotor cells and pyramidal tracts; but for practicalreasons one would not wish to do away with thespecial designation for this condition. What we wishto avoid is the multiplication of names for 'diseaseentities' which in fact are merely the expressions ofneuronal atrophy in a variety of overlappingcombinations. We therefore propose to use the termmultiple system atrophy to cover the whole group.
Among the structures at risk in this disease we mustinclude the preganglionic cells of the autonomicsystem. These may be attacked apparently inisolation as in case 1 of Johnson et al. (1966), or incombination with other structures, as in the othercases under discussion. In the latter, it is justifiableto speak of the Shy-Drager syndrome; but it isquite unjustifiable to regard this disorder, in whichthe autonomic system is affected along with others,as a separate disease entity.The problem of aetiology in those cases with
orthostatic hypotension is the same as in othervarieties of multiple system atrophy. We know of noextrinsic exciting cause, and there is at present noevidence of a specific enzyme deficiency. On thegenetic side, there is a close parallel with OPCA.Most of the reported cases are sporadic, but someare familial. Lewis (1964) described a family ofwhich at least four members suffered from a slowlyprogressive disease, with onset in early middle life,characterized by some or all of the following:orthostatic hypotension, amyotrophy, ataxia, rigidityand tremor, and sphincter disturbances. These casesdiffer from the group which we have been discussingmainly in their relatively benign clinical c urse.Lewis's four patients were alive, and not totallydisabled, 17, 39, 19, and 8 years respectively afterthe onset of symptoms.
Nicotine sensitivity was a striking feature in thecase here described. Spillane (1955) described threecases of spinocerebellar degeneration and one of
33
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from
J. G. Graham and D. R. Oppenheimer
multiple sclerosis, all of whom showed sharptemporary deterioration after cigarette smoking.He established that this was due to nicotine itself.Orthostatic hypotension was not looked for, and thehistories did not suggest it. Reference to the clinicalnotes of case 2 of Johnson et al. (1966), made byDr. J. D. Spillane some years before the patient cameunder study by Johnson and co-workers, revealedthat he had had striking nicotine sensitivity and hadstopped smoking as a result. We have recentlystudied a further patient, kindly referred by Dr.Harold Edwards, who had a degenerative cerebellarsyndrome with marked orthostatic hypotension, andwho complained of nicotine sensitivity, a complaintamply confirmed by objective tests before and aftersmoking. Although anhidrosis was demonstrated shewas unwilling to submit to further tests of autonomicfunction. The nicotine effect is not mentioned inLewis's (1964) report of the familial cases, nor in thepapers of Shy and Drager (1960) and Schwarz (1967).Tripodi (1932) described a case of orthostatic hypo-tension with 'staggering' in a heavy smoker, andascribed the condition to cigarette smoking, althoughinsufficient detail is provided to assess the justificationfor doing so.
In our case cigarette smoking had no effect on thetests of vasomotor function. On theoretical grounds,the dosage of nicotine obtained from a cigarettewould, if anything, be expected to raise the bloodpressure slightly. Moreover it is clear from thehistories of the affected patients that it is the cere-bellar component of their symptomatology which isaffected. We cannot therefore relate nicotinesensitivity to the autonomic component of multiplesystem atrophy. We can only observe that twouncommon features of this range of disorders,nicotine sensitivity and orthostatic hypotension,have occurred together in two out of the three casesconfirmed by necropsy in the British literature, and afourth case mentioned above also seems to show thisassociation.
SUMMARY
A 60-year-old man developed a progressiveneurological disorder with the following features:cerebellar ataxia, which was exacerbated by smoking,orthostatic hypotension, sexual impotence, andurinary incontinence. At necropsy, he showedneuronal degeneration at multiple sites, includingthe intermediolateral columns, where the deficiencywas estimated at about 80%.Comparing this case with previously reported
cases of (a) the Shy-Drager syndrome and (b) nico-tine sensitivity, the authors conclude that:
1. This and other cases of the Shy-Drager
syndrome are examples of a group of presenileneuronal degenerations, of which olivo-ponto-cerebellar atrophy is one ofthe better-known varieties.The disease affects different selections of sites indifferent patients. The intermediolateral columnsare among the sites at risk.
2. In such cases autonomic failure is attributableto the degeneration of the autonomic efferent cellswhich has been demonstrated in the intermedio-lateral columns.
3. Nicotine sensitivity is an occasional feature ofcases with cerebellar system degeneration. It cannotbe regarded as part of the autonomic disturbance,but its clinical association with this disturbance isrecorded.As a general term to cover the many varieties of
this disease, the authors suggest 'multiple systematrophy'. The term 'Shy-Drager syndrome' isjustified in describing those cases of multiple systematrophy with orthostatic hypotension.
We are grateful to Dr. J. D. Spillane for permission topublish this case and for his observations on case 2 ofJohnson et al., to Dr. Harold Edwards for referring thefurther case mentioned, to Dr. Sam Galloon for assistancein the autonomic tests, to Dr. John Spalding for hishelpful criticisms, to Mr. Ronald Beesley for the histo-logical preparations, and to Mr. Ralph Marshall for theillustrations.
REFERENCES
Adams, R. D., van Bogaert, L., and van der Eecken, H. (1964).Striato-nigral degeneration. J. Neuropath. exp. Neurol., 23.584-608.
Fichefet, J. P., Sternon, J. E., Franken, L., Demanet, J. C., andVanderhaeghen, J. J. Etude anatomo-clinique d'un cas d'hypo-tension orthostatique 'idiopathique'. Considerations patho-g6niques. Acta cardiol. (Brux.), 20, 332-348.
Jellinger, K., and Danielczyk, W. (1968). Striato-nigral degeneration.Acta neuropath. (Berl.), 10, 242-257.
Johnson, R. H., Lee, G. de J., Oppenheimer, D. R., and Spalding.J. M. K. (1966). Autonomic failure with orthostatic hypo-tension due to intermediolateral column degeneration. Areport of two cases with autopsies. Quart. J. Med., 35, 276-292.
Lewis, P. (1964). Familial orthostatic hypotension. Brain, 87, 719-728.Martin, J. B., Travis, R. H., and van den Noort, S. (1968). Centrally
mediated orthostatic hypotension. Arch. Neurol. (Chic.), 19,163-173.
Nick. J., Contamin, F., Escourolle, R., Guillard, A., and Marcantoni.J. P. (1967). Hypotension orthostatique idiopathique avecsyndrome neurologique complexe a predominance extra-pyramidale. Etude anatomo-clinique d'un cas. Rev. Neurol.,116, 213-227.
Schut, J. W., and Haymaker, W. (1951). Hereditary ataxia: a patho-logic study of five cases of common ancestry. J. Neuropath.clin. Neurol., 1, 183-213.
Schwarz, G. A. (1967). The orthostatic hypotension syndrome ofShy-Drager. A clinicopathologic report. Arch. Neurol. (Chic.),16, 123-139.
Shy, G. M., and Drager, G. A. (1960). A neurological syndromeassociated with orthostatic hypotension. A clinical-pathologicalstudy. Arch. Neurol., 2, 511-527.
Spillane, J. D. (1955). The effect of nicotine on spinocerebellar ataxia.Br-it. nmed J., 2, 1345-1351.
Tripodi, M. (1932). L'ipotensione arteriosa ortostatica. PoliclinicoSez. prat., 39, 797-801.
Welte, E. (1939). Die Atrophic des Systems des BruckenfuLsses unidder tinteren Oliven. Arch. PsYchiat. Nerrenkr, 109, 649-698.
34
Protected by copyright.
on 6 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.32.1.28 on 1 F
ebruary 1969. Dow
nloaded from