orthopaedic surgery & sports medicine surgery... · to discuss the principles of ... during the...
TRANSCRIPT

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ORTHOPAEDIC SURGERY & SPORTS MEDICINE
ARTROS, CENTRE FOR ORTHOPAEDIC
SURGERY & SPORTS MEDICINE
LJUBLJANA, SLOVENIA
BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
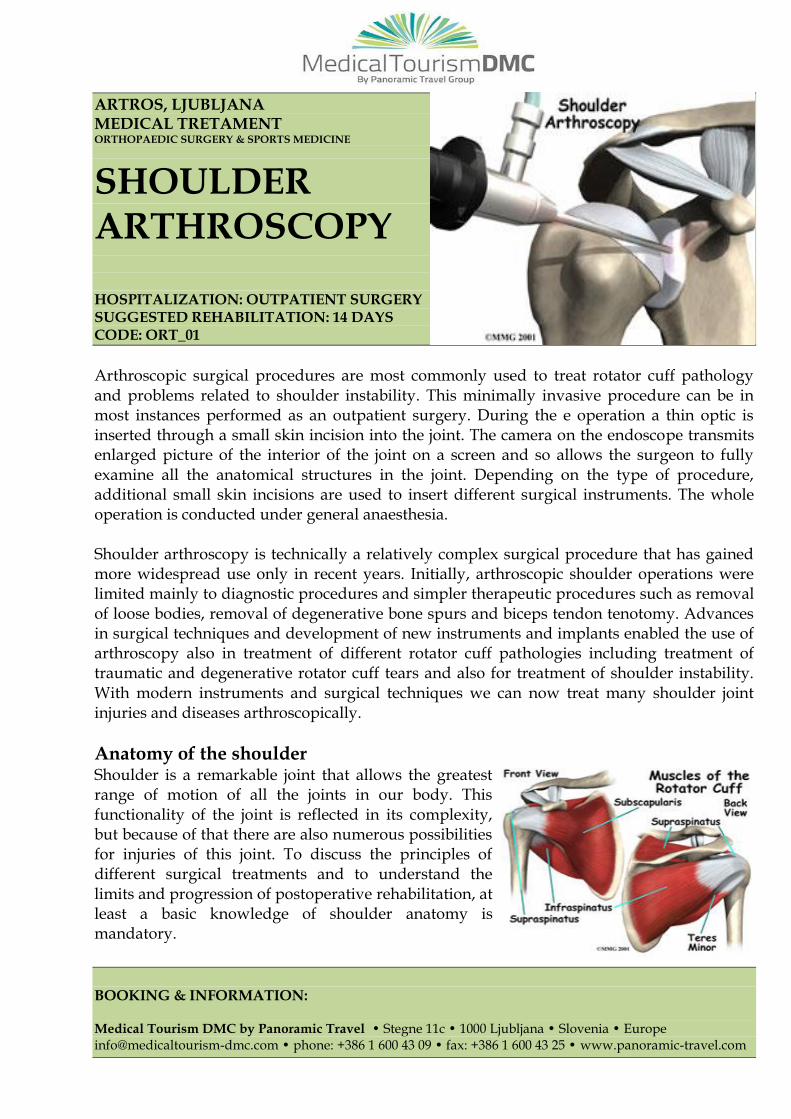
SHOULDER ARTHROSCOPY HOSPITALIZATION: OUTPATIENT SURGERY SUGGESTED REHABILITATION: 14 DAYS CODE: ORT_01
Arthroscopic surgical procedures are most commonly used to treat rotator cuff pathology and problems related to shoulder instability. This minimally invasive procedure can be in most instances performed as an outpatient surgery. During the e operation a thin optic is inserted through a small skin incision into the joint. The camera on the endoscope transmits enlarged picture of the interior of the joint on a screen and so allows the surgeon to fully examine all the anatomical structures in the joint. Depending on the type of procedure, additional small skin incisions are used to insert different surgical instruments. The whole operation is conducted under general anaesthesia. Shoulder arthroscopy is technically a relatively complex surgical procedure that has gained more widespread use only in recent years. Initially, arthroscopic shoulder operations were limited mainly to diagnostic procedures and simpler therapeutic procedures such as removal of loose bodies, removal of degenerative bone spurs and biceps tendon tenotomy. Advances in surgical techniques and development of new instruments and implants enabled the use of arthroscopy also in treatment of different rotator cuff pathologies including treatment of traumatic and degenerative rotator cuff tears and also for treatment of shoulder instability. With modern instruments and surgical techniques we can now treat many shoulder joint injuries and diseases arthroscopically.
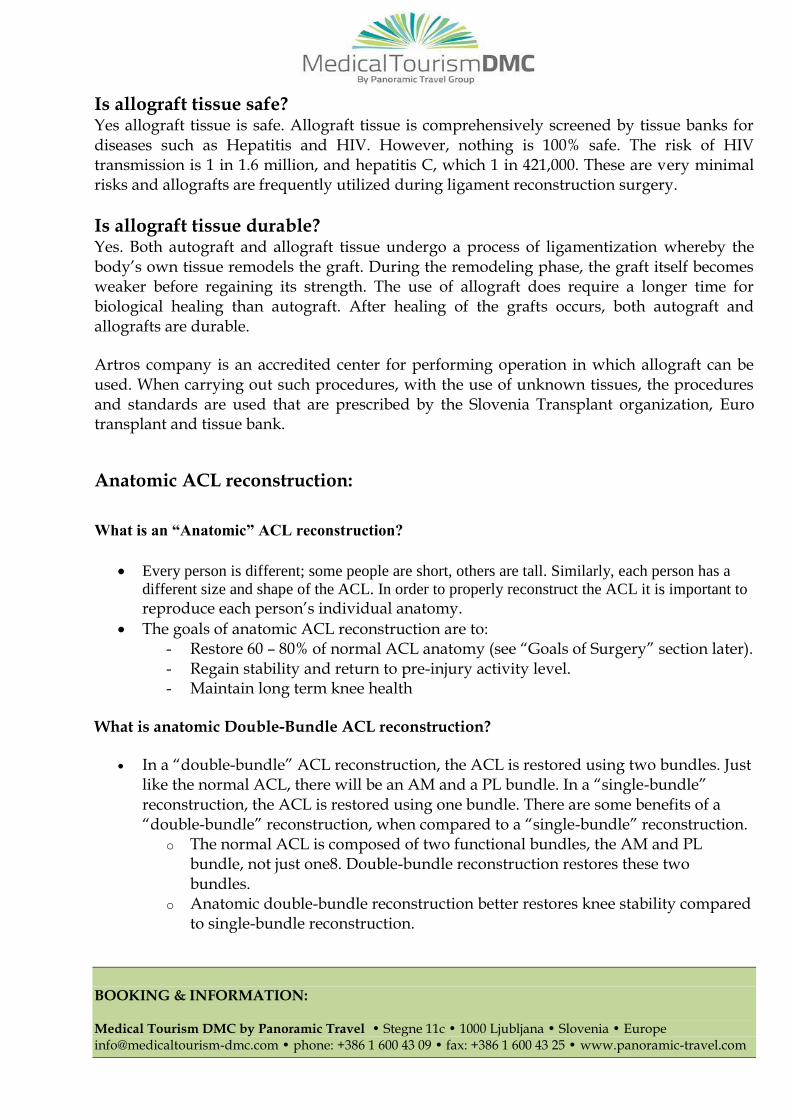
Anatomy of the shoulder Shoulder is a remarkable joint that allows the greatest range of motion of all the joints in our body. This functionality of the joint is reflected in its complexity, but because of that there are also numerous possibilities for injuries of this joint. To discuss the principles of different surgical treatments and to understand the limits and progression of postoperative rehabilitation, at least a basic knowledge of shoulder anatomy is mandatory.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
The bony anatomy of the shoulder joint is formed by the scapula (shoulder blade), proximal humerus and the clavicle. It principally consist of three joints - the joint between humeral head and the shoulder blade (glenohumeral joint), the joint between shoulder blade acromial processes and the clavicle (acromioclavicular joint) and a connection between the thorax and scapula (scapulothoracic joint). In physiologic conditions with normal functioning shoulder, movements in all three joints are coordinated. Disease or injury in each of the joints can lead to disturbed function of the whole shoulder.
Surgical procedure Shoulder arthroscopy is carried out under general anesthesia. At the beginning of the procedure usually two small skin incisions are made, one on the back and one on the front of the shoulder. They are used to introduce the optic and a palpation probe into the joint. Following this, a diagnostic joint examination is performed and all pathologic changes in the shoulder joint are identified and evaluated. In case of complex procedures one to three additional skin incisions are made, through which additional operating instruments are introduced. Similar to knee arthroscopy, shoulder joint is also filled with sterile saline during surgery. It is a solution of NaCl, which flushes out joint, expands it a bit and in this way provides good visibility inside the joint. Shoulder arthroscopy is usually done in two steps. In the first part of the procedure the arthroscope is introduced into glenohumeral joint, this is the main joint of the shoulder, where the articular surfaces of the humerus and the shoulder blade articulate. At this step usually pathology associated with shoulder instability, lesions of the long head of biceps tendon, cartilage damage and rotator cuff tendon tears are identified. Diagnostic arthroscopy is than continued by introducing the arthroscope into the subacromial bursa – space between undersurface of the acromion and the outside surface of the rotator cuff. At this step mainly the degenerative changes on the undersurface of the acromion and in the region of the acromioclavicular joint are identified. After initial diagnostic joint evaluation, operation is usually followed by therapeutic procedure, where the important pathology is addressed and treated adequately. Most common procedures performed during shoulder arthroscopy include rotator cuff tear reconstruction, treatment of chronic long biceps tendon inflammation or instability, treatment of degenerative changes or acute injury of the acromioclavicular joint, treatment of different shoulder joint instability problems, just to name a few. Depending on the complexity of the procedure, the operation time can vary from 30 minutes to two hours. After the procedure the patient has to stay for a short time in the recovery room where for appropriate postoperative pain control is taken care. Usually the patient is discharged on the same day.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
The advantages of arthroscopic shoulder procedures
Arthroscopic surgical techniques that allow minimally invasive treatment of joint problems have several advantages over the traditional surgery. Similar to arthroscopy in the other joints the inside of the shoulder joint can be inspected in much more detailed fashion. A significant advantage of arthroscopic procedures on the shoulder is also the preservation of the deltoid muscle. This is the main muscle that covers the entire surface of the shoulder joint and assures the main force for the shoulder abduction and arm elevation. Preservation of the deltoid muscle is associated with less postoperative pain, diminished scarring and less risk for postoperative adhesion formation. Arthroscopic procedures have also significantly lower risk for postoperative infection and neurovascular injuries. Due to the small skin cuts the cosmetic effect of the operation is also significantly better.
INDICATIONS FOR SHOULDER ARTHROSCOPY
Chronic subacromial impingement Rotator cuff tear Recurring shoulder dislocations Biceps tendonitis Calcific tendonitis Injuries and osteoarthritis of the AC joint Labral injuries Adhesive capsulitis
Recovery after shoulder arthroscopy
Postoperative recovery after shoulder arthroscopy is due to the minimal invasiveness of the procedure in many ways easier and faster. After these procedures there is less pain and in some cases shoulder joint function returns quicker. The expected actual recovery time depends on the pathology treated and type of procedure that was performed. It can be relatively short in simpler procedures as subacromial decompression, biceps tendon tenotomy or tenodesis, removal of free bodies and calcific deposits, resection of the distal clavicle. The rehabilitation is more demanding after reconstructive operations such as rotator cuff repair and shoulder stabilization procedures. In these procedures biologic healing of the reconstructed tissues is the limiting factor that has to be observed in progression of postoperative rehabilitation. Usually after these complex procedures the whole process of postoperative rehabilitation lasts about 4 to 6 months. During early postoperative period, most of the rehabilitation is done under the supervision of a physiotherapist. Later in the course of recovery, the patient himself can do many of the prescribed exercises at home. If advanced degenerative changes are already present in the joint or soft tissues that have been reconstructed, this can lead to even more slow recovery and can have negative influence on the final treatment outcome.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
KNEE ARTHROSCOPY HOSPITALIZATION: OUTPATIENT SURGERY SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_02 & ORT_03
Arthroscopic surgery is a procedure in which the inside of the joint can be evaluated and treated using surgical instruments placed into the joint through small incisions measuring few millimetres. The arthroscopic equipment consists of the scope and small surgical instruments which allow the surgeon to probe, cut, or shave tissues inside the knee. The scope itself is a small tube 4-5 millimetres in diameter (smaller than a pencil) which has a fiber optic light source and a magnifying lens. Attached to this is a camera and cable which projects the image from inside the knee onto a television screen or monitor. The knee joint is filled with sterile fluid and the scope is moved around the inside of the knee joint by the surgeon so that various areas and structures can be seen and evaluated on the monitor. The small surgical instruments (biters, shavers, probes, scissors, etc.), also measuring few millimetres, are placed into the joint through separate incisions to remove torn cartilage, trim torn structures, or do other procedures. Two to three small incisions are usually needed for knee arthroscopy. The arthroscope allows the surgeon see many structures inside the knee such like cartilage, meniscus or cruciate ligaments. If torn or damaged, surgical reconstruction can be done in selected patients by arthroscope - assisted techniques.
Basic Knee Anatomy The knee is the largest joint in the body. The knee joint is made up of the femur, tibia and patella (knee cap). All these bones are lined with articular surface cartilage. This articular cartilage acts like a shock absorber and allows a smooth low friction surface for the knee to move on. Between the tibia and femur lie two floating cartilages called menisci. The medial (inner) meniscus and the Lateral (outer) meniscus rest on the tibial surface cartilage and are mobile. The menisci also act as shock absorbers and stabilizers. The knee is stabilized by ligaments that are both in and outside the joint. The medial and lateral collateral ligaments support the knee from excessive side-to-side movement. The anterior and posterior cruciate ligaments support the knee from buckling and giving way. The knee joint is surrounded by a capsule (envelope) that produces a small amount of synovial (lubrication) fluid to help with smooth motion. Thigh muscles are important secondary knee stabilizers.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
The procedure of knee arthroscopy Knee Arthroscopy can be performed under local, regional, or general anesthesia.
Local anesthesia numbs just knee Regional anesthesia numbs patient below his waist General anesthesia puts patient to sleep
After placing the patient on the operating table we prepare and drape the knee in sterile fashion. A compression cuff is placed on the thigh, which allows blood stasis in the leg during surgery, if necessary. During the surgery, the knee joint is filled with sterile saline. It is a solution of NaCl, which flushes out joint, expands it a bit and in this way provides good visibility inside the joint. During the surgery, depending on the type of pathology in the knee the damaged structures can be removed or repaired. The ruptured ligaments can be reconstructed. Considering the extent and complexity of the procedure, time of operation varies and ranges from 20 minutes to two hours. After the procedure the patient rests in recovery room for a shorter time, and the same day released to home care.
The advantages of arthroscopic procedures on the knee Arthroscopic surgical techniques that allow minimally invasive treatment of injuries and diseases of joints have over classic surgery several advantages. In knee arthroscopy allows much more detailed and comprehensive review of all structures in the joint Many of those in conventional surgeries are not even reachable to evaluate. The great advantage of arthroscopic precedure is minimal traumatization surrounding healthy tissues, which are associated with significantly less pain in the postoperative period. All of the above advantages improve the functional results of surgical treatment, risk of postoperative complications. Finally, due to the small skin cuts is the cosmetic effect of the operation operations also significantly better.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
INDICATIONS FOR KNEE ARTHROSCOPY
Torn Meniscus Loose bodies in the joint Torn anterior or posterior cruciate ligament Mild degenerative changes Cartilage injury Patellar pain and disorders Chronic inflammation of the synovial membrane
Recovery from knee arthroscopy Recovery from knee arthroscopy is much faster than recovery from traditional open knee surgery. The actual recovery time depends on the type of the procedure; usually there is a minimum recovery after the partial resection of the ruptured meniscus, and the longest is in complex knee ligaments reconstruction. If degenerative changes in the knee are already present the following may contribute to a substantial extension of the recovery. Still, it is important to follow your orthopedic surgeon's instructions carefully after you return home. Swelling Keep your leg elevated as much as possible for the first few days after surgery. Apply ice is recommended to relieve swelling and pain. Bearing Weight Normally is a partial weight loading of the operated legs allowed immediately after surgery as tolerated by pain. But some patients need crutches or other assistance after arthroscopic surgery. Your surgeon will tell you when it is safe to put weight on your foot and leg. Medications Your doctor will prescribe pain medication to help relieve discomfort following your surgery. He may also recommend medication to lessen the risk of blood clots. Exercises to Strengthen Your Knee You should exercise your knee regularly for several weeks after surgery. This will restore motion and strengthen the muscles of your leg and knee. Exercise will play an important role in how well you recover. A formal physical therapy program may improve your final result.
Side-effects These are the unwanted, but mostly mild and temporary effects of a successful treatment, for example feeling sick as a result of the general anesthetic. After a knee arthroscopy you will have small scars on your knee from the cuts.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Complications This is when problems occur during or after the operation. Most people aren't affected. The possible complications of any operation include an unexpected reaction to the anesthetic, a wound infection, excessive bleeding or developing a blood clot, usually in a vein in the leg (DVT). Arthroscopy complications can include:
accidental damage to the inside of your joint infection loss of feeling in the skin over your knee bleeding into joint the surgery may not be successful or it may have to be repeated
Warning Signs:
Contact your surgeon immediately if you experience any of the following: Fever Chills Persistent warmth or redness around the knee Persistent or increased pain Significant swelling in your knee Increasing pain in your calf muscle

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA
MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
ANTERIOR CRUCIATE
LIGAMENT
RECONSTRUCTION HOSPITALIZATION: OUTPATIENT SURGERY SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_04
The anterior cruciate ligament (ACL) is one of the major ligaments in the knee that connects the
thigh bone (femur) to the shin bone (tibia). Is an important stabilizing ligament of the knee The
ACL provides stability to the knee, while also allowing for normal knee movement. It is located
deep inside the knee joint and provides almost 90% of the stability to forward force on the joint.
Although the ACL is referred to as one ligament, it consists of two functional bundles. These two
bundles are named for the place where they attach on the tibia. There is an anteromedial (AM)
bundle, which inserts more anterior (Towards the front) and medial (towards the inside) of the
tibia. The posterolateral (PL) bundle inserts most posterior (towards the back) and lateral
(towards the outside) of the tibia.
Injuries to this ligament are very common ACL tears are very common. Over 200,000 ACL tears
occur each year in the United States. However, ACL tears can occur at all ages and in all sporting
activities after either contact or non-contact injuries. The highest occurrence is in individuals
between 15 to 25 years of age who participate in pivoting and cutting sports. In aggressive sports
such as skiing and basketball. Injury to the ACL usually occurs with a sudden hyperextension or
rotational force to the joint. The exact mechanism differs for different sports. Typically the
injured athlete will hear or feel a "pop", and will have sudden onset of pain, instability and
swelling.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
The physical examination in clinic is used to make the diagnosis. This is done through a thorough history of injury as well as through a variety of physical exams which include anterior drawer test, Lachman, pivot shift and KT-2000 measurements. Each of these tests aids in determining the functional status of the ACL. MRI scans are used to image the ACL, confirm the diagnosis and evaluate for other possible injuries, like meniscus tears. Below we show an MRI of a normal ACL. We also take x-rays of the knee. You cannot see the ACL on x-ray, but we do this to make sure there is no problem with the bones, such as a fracture.
When ACL is torn, do we absolutely need surgery?
No. There are some patients who are able to function without an intact ACL. These patients modify their lifestyle by eliminating sporting activities that require pivoting and cutting. However, sometimes during everyday activities the ACL-deficient knee can buckle or “give way” (subluxate) resulting in painful episodes with swelling.
Importantly, there is a risk of damage to the menisci (the cartilage shock absorbers) and articular cartilage (the slippery gliding surface on the ends of the bones) with each subluxation event. This damage can lead to degenerative arthritis and subsequent meniscus tears.
Because of these concerns a majority of active patients elect to undergo ACL surgery when the ligament tears.
When knee will be ready for surgery?
In general, there are three criteria that must be met before the ACL can be surgically reconstructed:
o Swelling in the knee must go down to near-normal levels o Range-of-motion (bending and straightening) of the injured knee must be
nearly equal to the uninjured knee o Good Quadriceps muscle strength must be present. This means that while lying
flat on your back you should be able to raise your leg off the ground while holding it is straight. We call this a “straight leg raise”.
Usually it takes a couple of weeks after injury before ACL reconstruction can be performed.
The presence of any associated injuries to the knee joint involving cartilage, meniscus, or other ligaments may change the time-frame for surgery.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Surgical procedure Arthroscopic anterior cruciate ligament has many advantages over conventional open reconstruction. It allows much more precise positioning of the reconstructed ligament in the joint, preserves the soft tissues surrounding the joint, with less pain and risk of infections. It is usually performed under general or regional anesthesia. The surgical procedure itself takes between 60 and 90 minutes. You will be in the operating room between 90 and 120 minutes because we repeat the physical examination of your knee when you are in the operating room. To reconstruct the ACL, arthroscopy is performed. This means we look inside the joint with a small camera using small incisions and instrumentation. We typically use four small incisions (3 arthroscopic):
LP (lateral portal = incision towards the outside of the knee), MP (medial portal = incision towards the inside of the knee) and AMP (accessory medial portal = incision even further on the inside of the knee)
In the picture above the small incisions are used for the camera and the surgical instrumentation.
One incision over the tibia is used to attach the new ACL to the tibia. (Lower, longer Incision).
Occasionally, an additional incision is made on the outer aspect of the knee joint over the femur to help attach the new ACL to the femur.
After placing the patient on the operating table we prepare and drape the knee in sterile fashion. A compression cuff is placed on the thigh, which allows blood stasis in the leg during surgery, if necessary. During the surgery, the knee joint is filled with sterile saline. It is a solution of NaCl, which flushes out joint, expands it a bit and in this way provides good visibility inside the joint. In case of a detection of associated injuries, of other joint structures, such as medial and lateral meniscus, cartilage surface and rear posterior cruciate ligament. If possible, we give appropriate surgical treatment. In meniscus tear, this may involve partial removal of the meniscus or meniscus repair with sutures or arrows.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Where do the grafts for ACL reconstruction come from? Arthroscopic reconstruction of the cruciate ligaments with autologous tendon graft is a gold standard for the treatment of anterior cruciate ligament rupture. The surgeon replaces the ruptured anterior cruciate ligament with tendon graft, usually with autologous tendon of hamstring muscles, which is taken during the surgery from the back of the thigh. Otherwise:
The graft tissue can come from your own body (autograft) or from a cadaver (allograft).
Autograft options include different tendons from different muscles: Hamstrings Tendons, Quadriceps Tendon, and Patellar Tendon (BTB).
o Advantages to autograft include no risk of disease transmission and potentially quicker healing of the new ACL.
o Disadvantages to autograft tissue primarily relate to harvesting of the tissue, which can cause pain after the surgery. The operating time is also longer because the tissue has to be obtained before the reconstruction.
Allograft options also include a variety of different tendons from different muscles: Hamstrings Tendons, Tibialis Anterior Tendon, Posterior Tibialis Tendon, Patellar Tendon, Quadriceps Tendon, Achilles Tendon, and the Tensor Fascia Lata.
BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Is allograft tissue safe? Yes allograft tissue is safe. Allograft tissue is comprehensively screened by tissue banks for diseases such as Hepatitis and HIV. However, nothing is 100% safe. The risk of HIV transmission is 1 in 1.6 million, and hepatitis C, which 1 in 421,000. These are very minimal risks and allografts are frequently utilized during ligament reconstruction surgery.
Is allograft tissue durable? Yes. Both autograft and allograft tissue undergo a process of ligamentization whereby the body’s own tissue remodels the graft. During the remodeling phase, the graft itself becomes weaker before regaining its strength. The use of allograft does require a longer time for biological healing than autograft. After healing of the grafts occurs, both autograft and allografts are durable.
Artros company is an accredited center for performing operation in which allograft can be used. When carrying out such procedures, with the use of unknown tissues, the procedures and standards are used that are prescribed by the Slovenia Transplant organization, Euro transplant and tissue bank.
Anatomic ACL reconstruction:
What is an “Anatomic” ACL reconstruction?
Every person is different; some people are short, others are tall. Similarly, each person has a
different size and shape of the ACL. In order to properly reconstruct the ACL it is important to
reproduce each person’s individual anatomy.
The goals of anatomic ACL reconstruction are to: - Restore 60 – 80% of normal ACL anatomy (see “Goals of Surgery” section later). - Regain stability and return to pre-injury activity level. - Maintain long term knee health
What is anatomic Double-Bundle ACL reconstruction?
In a “double-bundle” ACL reconstruction, the ACL is restored using two bundles. Just like the normal ACL, there will be an AM and a PL bundle. In a “single-bundle” reconstruction, the ACL is restored using one bundle. There are some benefits of a “double-bundle” reconstruction, when compared to a “single-bundle” reconstruction.
o The normal ACL is composed of two functional bundles, the AM and PL bundle, not just one8. Double-bundle reconstruction restores these two bundles.
o Anatomic double-bundle reconstruction better restores knee stability compared to single-bundle reconstruction.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
o Because anatomic double-bundle reconstruction uses two bundles to restore the ACL, it allows for a replacement of a larger size ACL. For example in the picture below, the patient on the left has a 12 mm ACL, but the patient on the right has a 23 mm ACL. Using two bundles on the patient on the right can help to restore more of the normal ACL, where using only a single bundle on this patient might only restore half of the native ACL size.
What is the surgical procedure for an anatomic double-bundle reconstruction?
When the camera (arthroscope) is place inside the knee, we look carefully at the injured ACL. We determine where and how it is torn. It can be partially or completely torn, and torn from the top, in the middle or on the bottom. Sometimes, the ACL is still attached to the bones, but often it is stretched out and has lost its function.
The insertion sites of the AM and PL bundle are then carefully measured with a small ruler. These measurements will determine the size of the new ACL.
A new AM and PL bundle are created using “a graft”, which can be from donor tissue or from your own body. The sizes of these grafts are based on your own ACL size. More about the graft will be explain explained later in this hand-out.
To attach the ACL graft to the bone, tunnels are dilled in the bone. For a double-bundle procedure (shown below), 4 tunnels total will be drilled: 2 tunnels in the femur and 2 tunnels for the tibia for the AM and PL bundles.
The ACL grafts are then placed into the tunnels and fixed to the femur and tibia bones with a combination of special fasteners, screws and sometimes staples.
Do we also perform anatomic single bundle ACL reconstruction? Yes. We perform single bundle ACL reconstruction in approximately 40% of our
patients. However, our anatomic single-bundle reconstruction is very different from the
traditional non-anatomic ACL reconstruction that used to be performed. We have learned a great deal from the development of the anatomic double-bundle technique. We use all of the same principles to perform an “Anatomic Single Bundle” ACL reconstruction.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Anatomic single bundle There are a few scenarios where we actually prefer to perform single bundle surgery over double bundle surgery:
The patient has a very small native ACL size, usually less than 14 mm. This can be estimated on MRI, but can only be confirmed at the time of surgery.
The patient is still growing and his or her growth plate is not closed. The patient has severe arthritis of the knee. The patient has multiple knee ligament injuries or a knee dislocation and multiple
other ligaments need to be reconstructed at the same time. The patient has bone that is severely bruised. The patient has a small “notch”. This is the open space in the femur bone where the
ACL houses.
The procedure is very similar to anatomic double-bundle reconstruction. However, instead of drilling 4 tunnels for the 2 bundles, we only drill 2 tunnels because there will be only one bundle. One tunnel is drilled in the center of the attachment of the old ACL on the tibia, right between the AM and PL bundle. The other tunnel in the center of the attachment of the old ACL on the femur (see below).
Anatomic single-bundle reconstruction has some limitations when compared to anatomic double-bundle reconstruction.
It cannot recreate the two functional bundles (AM and PL) of the ACL. It can cover less of the size of the normal ACL, typically 65-85% of the ACL insertion
site recreated, vs. 80-90% in double-bundle reconstruction.
The Primary Goal of Anatomic ACL Reconstructive Surgery: Restoring Native Anatomy
The goal of anatomic ACL reconstruction is to reproduce 60 – 80% of the native ACL insertion site area.
We take very careful measurements in the operating room and use a mathematical formula to calculate the area of the native ACL insertion site that we reproduce during surgery.
In rare cases, during the diagnostic arthroscopy is founded that a part of the anterior cruciate ligament is still preserved. In this case, the surgeon might decide to reconstruct the torn part and to preserve the other one. The course of this operation is very similar to the anterior cruciate ligament reconstruction with double bundle technique, only in this case only single bundle in reconstructed, the preserved part of the cruciate ligament, in this case represents the second bundle.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Recovery after the arthroscopic reconstruction of anterior cruciate ligament Due to the minimal invasive nature of arthroscopic reconstruction of anterior cruciate ligament the recovery is faster comparing to the conventional surgery. It is very important that the patient is aware and understands that the absence of the knee swelling and pain and full mobility of the knee does not mean that the knee has fully healed and capable of full loading. With Arthroscopic surgery we do achieve minor post-operative pain, that knee swelling disappears quickly, and that the full range of motion returns faster comparing to the conventional open surgery, but we cannot speed up the in growing of the tendon graft in the bone or the process of tendon revascularization. The above mentioned process need few months. It is a biological process of healing, which we normally stimulate with appropriate physical therapy and controlled loading, but we cannot significantly reduce it. Only a complete ingrowths of bone tendon graft and revascularization that has a vitally recovered cruciate ligament as an outcome enables that this type of reconstructed cruciate ligament is capable of withstanding burdens that occur at full burdening of the knee and demanding activities. Usually this is achieved in 9 months after surgery. Early uncontrolled or excessive movement of the knee in the first few months after surgery may lead to elongation of the tendon graft and the consequently an instability of the knee or even failure of the graft. Rehabilitation after the anterior cruciate ligament reconstruction is complex. It is crucial that is controlled and under the supervision of a physiotherapist, who is suitably qualified and knows the limits and objectives of the various phase of recovery very well. It is strongly recommended that the physical therapy is individual and that the program adapts to progress and to capabilities of individual, to the extent of biological processes and tissue healing can be permitted. Immediately after the operation, it is necessary to cool the knee with ice cooling several times a day, which reduces swelling and pain. A after the surgery a weight bearing on the operated leg is allowed as. First few days patients usually help themselves with crutches. Due to weakening of the leg muscles when walking with support, it is recommended to give up the support as soon as possible. On discharge each patient receives instructions regarding post-operative checkups and early rehabilitation.
ACL Surgery Complications No procedure is ever completely free of risks. However, ACL reconstruction is a safe procedure that is performed thousands of times each year. Complications occur in less than 2 out of 100 procedures. With ACL surgery, complications can either be minor or major. Most complications are minor, meaning they are temporary and, in most cases, can be treated by your healthcare provider without difficulty.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Minor ACL surgery complications include:
Bleeding Infection Numbness around the incision Instrument failure, including breakage Painful or abnormal scar formation Knee stiffness Ligament or cartilage injury Allergic skin reaction to tape, dressing, or latex.
Major ACL Surgery Complications
There are several major complications that can also occur during or after uncommon, but your overall health will play a role in your likelihood of developing them, as well as your ability to recover from them should they happen. For example, patients with lung or kidney disease, severe heart disease, or diabetes may have a higher chance of complications occurring than those who are healthier. Major ACL surgery complications include, but are not limited to:
Serious infections Fracture of the kneecap or thighbone Rupture or failure of the graft Blood clots in the legs, pelvis, or lungs Nerve injury Serious bleeding from blood vessel injury Serious reaction to anesthesia Allergic reaction to medication Persistent pain or numbness Long-term decreased knee motion Persistent swelling of the knee Transmission of disease (if a cadaver ACL is used) Thighbone fracture (if a hamstring graft is used) Continued knee looseness or return of the original symptoms Loss of life Other rare and improbable events.
Depending on the individual situation, a major complication may lead to a longer hospital stay, a repeat surgery, or, in infrequent cases, permanent disability or even loss of life.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA
MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
ARTHROSCOPIC RECONSTRUCTION OF THE ROTATOR CUFF WITH TRANSOSSEOUS SUTURES HOSPITALIZATION: OUTPATIENT TRETAMENTS, DURING STAY IN SELECTED HEALTH RESORT SUGGESTED STAY IN SLOVENIA: 14 DAYS CODE: ORT_05
Rotator cuff tear is the most common cause of shoulder pain in patients after 40 years of age. Usually a surgical treatment is proposed for this condition in active individuals. In Artros center, they were among the first to introduce a new biological method of arthroscopic rotator cuff suturing without the use of suture anchors. This new technique completely eliminates the risk for suture anchor related complications such as bone osteolysis and suture anchor migration. In addition the preservation of the bony surface to which tendon is sutured offers improved healing potential and increases the chance for complete recovery. The rotator cuff is formed by tendons of four muscles originating from different surfaces of the shoulder blade to attach around the humeral head. Its main function is dynamic stabilization of the shoulder joint and support of large superficial shoulder muscles during active moves of shoulder abduction and arm elevation. With aging, the blood circulation in the rotator cuff tendons gradually diminishes and tendon resistance to tensile loads decreases. With repetitive loading and overuse or with already a small injury this can lead to a tear of some of the tendons. In advanced cases of rotator cuff degeneration, tendon tear can develop spontaneously.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Shoulder pain at rest and especially during the night is usually the presenting symptom of rotator cuff tear. With progression of tendon tearing a decrease in active range of motion and in strength of abduction and later also in external and internal rotation can be observed. Surgical repair with cuff reattachment is the most effective method of treatment. Early diagnosis and anatomic repair are important factors influencing the final functional outcome. With delay in treatment a gradual enlargement of tear size with progressive tendon retraction can be anticipated. This can eventually lead to irreversible shoulder damage. Arthroscopic minimally invasive tendon repair is the predominant mode of treatment of this condition. With use of endoscopic camera inserted into the joint the tendons are attached back to their bony insertion on the humeral head. For years during arthroscopic rotator cuff repair, small implants loaded with sutures were used to attach the torn tendons to the bone. The advantage of using these implants is that they offer a relatively simple way of arthroscopic tendon reattachment. With broader use of these implants it became obvious, that they can cause also complications, among them bone osteolysis around the implants with weakening of bone and implant migration potentially causing additional damage in the joint.
Recently a new biologic fixation technique for arthroscopic rotator cuff repair has been developed. It is based on the fixation of the tendon to bone with transosseous sutures without the use of any additional implants. This new technique has many important advantages. It allows us to fully preserve the bone underneath the attached tendon without any disturbance in blood supply needed for tendon healing. In addition there is no risk for bone osteolysis or implant pullout, especially the last complication being very concerning as it can severely damage the joint. Several studies have already proven the safety, reliability and efficacy of this new rotator cuff repair technique. Dou to this significant changes we have adopted this technique as a standard mode of rotator cuff repair in our practice.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
ELBOW
ARTHROSCOPY HOSPITALIZATION: OUTPATIENT SURGERY SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_06
Arthroscopic procedures on the elbow can be used to treat a variety of injuries and conditions, most common among them include Tennis elbow, contracture release, removal of loose bodies, treatment of early osteoarthritis, synovectomy in rheumatoid arthritis. The procedure is conducted under general anesthesia. Symilar to arthroscopy of other joints, a small optico of the arthroscope is introduced through a skin incision into the joint. The joint is filled with a saline solution that distends it and improves visualization. Due to close relation of numerous vessels and nerves, elbow arthroscopy is regarded as technically demanding procedure. Despite this, it is a safe and reliable operation if performed by a skilled and experienced surgeon. Diagnostic elbow arthroscopy is carried out usually through for small skin incisions measuring each about 5 millimeters. In the first part of the procedure, the anterior part of the joint in the front of the elbow is examined. This is followed by the introduction of the arthroscope and instruments into the posterior part of the elbow, where we examine the dorsal joint surfaces. Similar to knee arthroscopy, shoulder joints during surgery is also filled with sterile saline. It is a solution of NaCl, which flushes out joint, expands it a bit and in this way provides good visibility inside the joint.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Depending on the condition for which the arthroscopic procedure is done, the adequate treatment is undertaken. In case of early osteoarthritis, degenerative bone spurs in the joint and loose bodies are removed, in patients with contracture the joint capsule is released, in chronic synovitis the synovial membrane is resected, in patients with Tennis elbow a degenerated part of the Extensor carpi radialis brevis tendon is resected. Depending on the complexity of the procedure, the operation time varies from 20 minutes to two hours. After the procedure the patient has to rest for a short period of time in the recovery room before being released home on the same day.
Advantages of the arthroscopic procedures on the elbow joint Due to its minimal invasiveness that enables the preservation of the muscles and other soft tissues around elbow joint, the arthroscopic procedures of the elbow offer numerous advantages. There is less postoperative paint, less soft tissue scaring and potential for quicker recovery. All procedures can be done on an outpatient basis and the risk of a perioperative joint infection is significantly reduced. Finally, due to the small skin incisions the cosmetic effect of the operation is also significantly better.
INDICATIONS FOR ELBOW ARTHROSCOPY
Chronic synovitis with joint swelling Epicondylitis (Tennis elbow) Elbow contracture Moderate degenerative changes Radial plica syndrome Loose joint bodies
Recovery after elbow arthroscopy The actual recovery time after elbow arthroscopy depends on the type of procedure and the preoperative condition of the joint. It is relatively short after smaller procedures, such as removal of loose bodies or degenerative spurs in the joint. The rehabilitation is more demanding after synovectomy, tennis elbow surgery, or the release of contractures. Rehabilitation after these procedures can take from 3-6 months, depending on the extent of joint disease. Coexistent advanced degenerative changes can prolong the recovery process and also negatively influence the treatment outcome.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
HIP REPLACEMENT
SURGERY HOSPITALIZATION: 3 – 5 DAYS SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_07
Hip replacement surgery, also called total hip arthroplasty, involves removing a diseased hip joint and replacing it with an artificial joint, called prosthesis. Hip prostheses consist of a ball component, made of metal or ceramic, and a socket, which has an insert or liner made of plastic, ceramic or metal. The implants used in hip replacement are biocompatible — meaning they're designed to be accepted by your body — and they're made to resist corrosion, degradation and wear. Hip replacement is typically used for people with hip joint damage from arthritis or an injury. Followed by rehabilitation, hip replacement can relieve pain and restore range of motion and function of your hip joint.
The goal of hip replacement surgery is to relieve pain and increase the mobility and function of a damaged hip joint. If a stiff, painful hip joint has forced you to cut back on everyday activities, successful surgery may allow you to resume them. Before thinking about surgery, though, your doctor may recommend other treatments, such as pain medications, physical therapy, exercise, and use of a cane or walker. If these treatments are not enough, hip replacement may be the right option for you.
Conditions that can damage the hip joint, sometimes necessitating hip replacement surgery, include:
Osteoarthritis Rheumatoid arthritis Broken hip Bone tumor Osteonecrosis, which occurs when there is inadequate blood supply to the ball portion
of the hip joint

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
INDICATIONS FOR HIP REPLACEMENT SURGERY
Persistent pain, despite pain medication
Pain exacerbated by walking, even with a cane or walker
Poor sleep due to pain
Difficulty going up or down stairs
Trouble rising from a seated position
Inability to participate in formerly enjoyable activities because of pain
The hip is a ball and socket type joint comprising the femoral head (ball) and acetabulum (socket). The bearing surfaces of the femoral head and acetabulum are covered by hyaline cartilage, which forms a very low friction surface allowing free and painless motion. Hip arthritis is a disease that involves the degeneration and loss of the cartilage bearing surface leading to bone-on-bone contact between the femoral head and acetabulum. The patient suffers pain, loss of hip motion and impairment of activities. Total hip replacement is a definitive and effective treatment for hip arthritis. Surgical technique for hip arthroplasty – the advantage of anterior minimal invasive approach The popularity of the anterior approach for total hip replacement is rapidly growing because of its definite advantages for patients, even those in need of bilateral procedures. Rehabilitation is simplified and accelerated, dislocation risk is reduced, leg length is more accurately controlled, and the incision is small. The anterior approach is an approach to the front of the hip joint as opposed to a lateral (side) approach to the hip or posterior (back) approach. Rehabilitation is accelerated and hospital time decreased because the hip is replaced without detachment of muscle from the pelvis or femur. Other surgical approaches necessitate detachment of muscle from the femur during surgery. In the anterior approach, by contrast, the hip is approached and replaced through a natural interval between muscles.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
The most important muscles for hip function, the gluteal muscles that attach to the posterior and lateral pelvis and femur, are left undisturbed.
Lack of disturbance of the lateral and posterior soft tissues also accounts for immediate stability of the hip and a low risk of dislocation. It is normal for patients undergoing lateral or posterior incisions to follow strict precautions that limit hip motion for the first two months after surgery. Most importantly, they are instructed to limit hip flexion to no more than 90 degrees. These limitations complicate a patient's simple daily activities such as sitting in a chair or on the toilet or getting in a car. Following the anterior approach, however, patients are immediately allowed to bend their hip freely and avoid these cumbersome restrictions. They are instructed to use their hip. Additionally, if patients are sexually active before surgery, there are no limitations on resumption of normal sexual activity after surgery.
The normal incision is about 4 inches but may vary (shorter or longer) according to a patient's body size. Though small incisions are often considered desirable by patients, it should be kept in mind that the degree and type of tissue disturbance beneath the skin is a more important factor. Incisions of adequate length allow the necessary side-to-side separation of the incision without undue force. Too small an incision can be more traumatic to the tissues, particularly to muscles that can be damaged by stretching too hard. With the anterior approach the patient lies supine (on their back) during surgery.
The anterior approach does not limit the patient's and surgeon's options regarding type of hip prosthesis. Hip prostheses that are implanted with or without cement are applicable as well as all modern bearing surfaces including ultra high-density polyethylene, metal and ceramic. Surface replacement arthroplasty is also possible through the anterior approach. After the exposure the femoral neck is cut and the arthritic femoral head and neck are removed.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Femoral Preparation After dropping the foot towards the floor through the lowering of the operating table foot section, a broach is inserted into the femoral canal. Progressively larger broaches are then inserted. The broach size is limited by the hard outer cortical bone. Sizing Following insertion of the final broach, the driving handle is removed. The broach is temporarily left in as a "trial" femoral prosthesis and its upper end is capped with a trial femoral head. The table repositions the leg to its normal position and the trial head is "reduced" into the acetabulum. The leg and hip are moved by the table to check for stability (resistance to dislocation). If the initial trial shows undesirable leg length, offset or stability adjustments are made The Femoral Prosthesis A femoral prosthesis of specific size is accurately inserted to reproduce the sizing indicated by the trial phase.
The Final Result The prosthetic hip is reduced by moving the leg into its normal position as the femoral head is placed into the acetabulum. The wound is washed with antibiotic solution and closed.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Risks and Complications Hip replacement surgery is generally safe, but as with any surgery, complications can occur. Although some complications are serious, most can be treated successfully. Complications of hip replacement include: Blood clots. Clots can form in your leg veins as a result of decreased leg movement after surgery, as well as from pressure on the veins during surgery. Your doctor usually gives you blood-thinning medications after your surgery to try to prevent clots from forming. Compression devices, such as elastic stockings, and exercise to increase blood flow through the veins in your legs also can reduce your risk. Infection. Infections can occur at the site of your incision and in the deeper tissue near your new hip. Most infections are treated with antibiotics, but a major infection near your prosthesis may require surgery to remove and replace the prosthesis. Fracture. During surgery, healthy portions of your hip joint may fracture. Sometimes the fractures are so small that they heal on their own, but larger fractures may be corrected during surgery with wires, cables or bone grafts. Dislocation. Certain positions can cause the ball of your new joint to become dislodged. To avoid this, it is often recommended that after surgery you don't bend more than 90 degrees at the hip and don't let your leg cross the midline of your body. If the hip dislocates, your doctor may fit you with a brace to keep the hip in the correct position. If your hip keeps dislocating, surgery is often required to stabilize it. Loosening. Although this complication is rare with newer implants, your new joint may not become solidly fixed to your bone or may loosen over time, causing pain in your hip. Surgery might be needed to fix the problem. Breakage of the prosthesis. Another rare possibility is that your artificial hip could break several years after surgery. Another surgery would be required to replace the broken joint. Change in leg length. Your surgeon takes steps to avoid the problem, but occasionally a new hip may make one leg longer or shorter than the other. Sometimes this is caused by weakness in the muscles surrounding the hip. In this case, progressively strengthening and stretching those muscles can make the hip more stable.
Joint stiffening. Sometimes the soft tissues around your joint harden (called ossification), making it difficult to move your hip. This usually isn't painful. If you're at risk of ossification, your doctor may recommend medications or radiation therapy to prevent it. Wear and tear over time. Your prosthetic hip joint may wear out eventually, so if you have hip replacement surgery when you're relatively young and active, you may need a second hip replacement within your lifetime. However, new materials are making implants last longer, so a second replacement may not be needed for many years.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Before surgery you'll meet with your orthopedic surgeon for an examination. The surgeon will:
Ask about your medical history and current medications Do a brief general physical examination to make sure you're healthy enough to
undergo surgery Examine your hip, paying attention to the range of motion in your joint and the
strength of the surrounding muscles Order blood tests, an X-ray and possibly an MRI if deemed necessary
This preoperative evaluation is a good opportunity for you to ask questions about the procedure. If you have any concerns about the surgery, be sure to ask. Your doctor or surgeon may also recommend that you begin an exercise program in preparation for your surgery. Some doctors believe that people who have an established muscle-building and flexibility program before surgery have better outcomes and faster recovery time following surgery. Preoperative exercise programs may have less effect in those with advanced osteoarthritis, however. Talk to your doctor before starting any exercise program. When you check in for your surgery, you'll be asked to remove your clothes and put on a hospital gown. The first member of the medical team to visit may be the anesthesiologist. You'll be given either a general anesthetic or a spinal block, which numbs the lower half of your body.
After the procedure.After surgery, you'll be moved to a recovery area for a few hours while your anesthesia wears off. Nurses or other anesthesia aides will watch your blood pressure, pulse, alertness, pain or comfort level, and your need for medications.
Blood clot preventionAfter your surgery, you'll be at increased risk of blood clots in your legs. Possible measures to prevent this complication include: Early mobilization. You'll be encouraged to sit up and even try walking with crutches or a walker soon after surgery. This will likely happen the same day as your surgery or on the following day. Pressure application. Both during and after surgery, you may wear elastic compression stockings or inflatable air sleeves similar to a blood pressure cuff on your lower legs. The pressure exerted by the inflated sleeves helps keep blood from pooling in the leg veins, reducing the chance that clots will form. Blood-thinning medication. Your surgeon may prescribe an injected or oral blood thinner after surgery. Depending on how soon you walk, how active you are and your overall risk of blood clots, you may need blood thinners for several more weeks after surgery.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Physical therapy Evaluation and treatment by a physical therapist begins following surgery and leads to walking and functional activities. Patients may go home after achieving an initial degree of independence in walking with crutches or a walker, as well as capabilities in basic day to day activities. Patients are commonly discharged 1 to 3 days following surgery depending on their degree of disability prior to surgery and their overall capabilities. Activity and exercise must be a regular part of your day to regain the use of your joint and muscles. Your physical therapist will recommend strengthening and mobility exercises and will help you learn how to use a walking aid, such as a walker, a cane or crutches. As therapy progresses, you'll gradually increase the weight you put on your leg until you're able to walk without assistance.
Home recovery and follow-up careBefore you leave the hospital, you and your caregivers will get tips on caring for your new hip. For a smooth transition:
Arrange to have a friend or relative prepare some meals for you Place everyday items at waist level, so you can avoid having to bend down or reach
up Consider making some modifications to your home, such as getting a raised toilet seat
About six to eight weeks after surgery, you'll have a follow-up appointment with your surgeon to make sure your hip is healing properly. If recovery is progressing well, most people resume their normal activities by this time — even if in a limited fashion.
Hip replacement surgery is successful more than 90 percent of the time. Expect your new hip joint to reduce the pain you felt before your surgery and increase the range of motion in your joint. But don't expect to do anything you couldn't do before surgery. High-impact activities — such as running or playing basketball — may never get your doctor's approval. But in time, you may be able to swim, play golf, walk or ride a bike comfortably.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
KNEE
REPLACEMENT HOSPITALIZATION: 3-5 DAYS SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_08
In knee replacement surgery (arthroplasty), a damaged, worn or diseased knee is replaced with an artificial joint. Knee replacement is a routine operation for knee pain when the knee joint has been severely damaged, most commonly by arthritis. There are two main types of surgery, depending on the condition of the knee: total knee replacement and partial (half) knee replacement. More than 70,000 knee replacements are carried out in England and Wales each year, and the number is rising. Most people who have a total knee replacement are over 65, and just over half of all patients are women.Candidates for knee replacement surgery need to be well enough for both a major operation and the rehabilitation afterwards.
Long-term outlook Wear and tear through everyday use means that your replacement knee will not last forever. However, for most people it will last for at least 15-20 years, especially if the new knee is cared for properly and not put under too much strain. Revision knee replacement surgery (replacing the replacement knee) is usually more complicated and a longer procedure than the original surgery. There is no set limit to the number of times you can have revision surgery, but it is widely accepted that the artificial knee joint becomes less effective each time it is replaced. Research has also shown that patients become less satisfied with their artificial knee each time it is replaced. This is one reason why knee replacement is less likely to be recommended for younger patients.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
INDICATIONS FOR KNEE REPLACEMENT SURGERY
Knee replacement surgery (arthroplasty) is usually necessary when a health condition or injury disrupts the normal working of the knee joint so that:
Your mobility is severely reduced You experience pain even while resting
Knee anatomy The knee joint acts as a hinge between the bones of the leg. It is really two joints. The major joint is between the thigh bone of the upper leg (femur) and the shin bone of the lower leg (tibia). The smaller joint is between the kneecap (patella) and the upper leg (femur). A smooth, tough tissue called articular cartilage usually covers the ends of the bones within the knee joint. This protects the ends of the bones and allows them to slide smoothly over each other without pain or too much effort. The synovial membrane that covers the other surfaces of the knee joint produces synovial fluid, which lubricates the joint, reducing friction to further help movement.
Osteoarthritis The most common reason for knee replacement surgery is osteoarthritis. Osteoarthritis in the knee occurs when the articular cartilage becomes damaged or wastes away through natural wear and tear. The bones have little or no protection to prevent them rubbing against each other when the knee moves, causing pain. The bones may compensate by growing thicker and producing bony outgrowths to try to repair themselves, but this can cause more friction and pain.
Preoperative consultation
Before surgery, the joints adjacent to the diseased knee (hip and ankle) are carefully evaluated. This is important to ensure optimal outcome from the surgery. Replacing a knee joint that is adjacent to a severely damaged joint may not yield significant improvement in function as the nearby joint may become more painful. Furthermore, all medications, which the patient is taking, are reviewed. Blood-thinning medications such as warfarin (Coumadin) and anti-inflammatory medications such as aspirin may have to be adjusted or discontinued prior to surgery.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Routine blood tests of liver and kidney function and urine tests are evaluated for signs of anemia, infection, or abnormal metabolism. Chest X-ray and EKG are performed to exclude significant heart and lung disease, which may preclude surgery or anesthesia. Finally, a knee replacement surgery is less likely to have good long-term outcome if the patient's weight is greater than 200 pounds. Excess body weight simply puts the replaced knee at an increased risk of loosening and/or dislocation.
Replacing a damaged knee Pain and difficulty moving the knee joint are common when the articular cartilage has become damaged or worn away. The ends of the bones start to rub or grind together, instead of smoothly sliding over each other. During a total knee replacement, the end of the femur bone is removed and replaced with a metal shell. The end of the lower leg bone (tibia) is also removed and replaced with a channeled plastic piece with a metal stem. Depending on the condition of the kneecap portion of the knee joint, a plastic "button" may also be added under the kneecap surface. The artificial components of a total knee replacement are referred to as the prosthesis. Replacing the damaged knee joint with an artificial one can help reduce pain and increase mobility.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Surgical alternatives to a knee replacement
There are alternative surgeries to knee replacement, but results are not as good in the long term.
Arthroscopic washout and debridement An arthroscope (tiny telescope) is inserted through small incisions in the knee. The knee is washed out with saline and any bits of bone or cartilage are cleared away. It is not recommended if you have severe arthritis. Microfracturing This is a keyhole (minimally invasive) operation in which small holes are made in the surface layer of bone with a small, sharp ‘pick’. This allows cells from the deeper, more blood-rich bone beneath to come to the surface and stimulate cartilage growth. It can be a good option if you have just a small area of damaged cartilage. However, the benefits are not well proven and the results are not as good as knee replacement for severe arthritis.
Osteotomy This is an open operation in which the surgeon cuts the shin bone and realigns it so that weight is no longer focused on the damaged part of the knee. It is sometimes used for younger people with limited arthritis, where it may enable a knee replacement to be postponed. However, you will usually need a knee replacement at a later date, and the operation may make knee replacement surgery more difficult if it is needed.
Autologous chondrocyte implantation (ACI) This is when new cartilage from your own cells is grown in a test tube and introduced into the damaged area. This method may be used for accidental injury to the knee with limited cartilage damage in younger patients. It is not successful for treatment of generalized osteoarthritis.
Mosaicplasty (cartilage replacement) This is a keyhole (minimally invasive) procedure that involves transferring plugs of hard cartilage, together with some underlying bone from another part of your knee, to repair the damaged surface. This method is successful for restoring small cartilage defect in younger patients but it can not be used in generalized advanced osteoarthritis.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Non-surgical treatment options These options include:
Physiotherapy to improve the flexibility, mobility and strength of your knee joint Painkillers to reduce pain in your joint so movement is easier Anti-inflammatory medicines to reduce swelling within the joint, increasing mobility Steroid injections into your joint to help relieve pain and swelling Temporarily losing excess weight to reduce the strain on your knees, thereby reducing
pain and improving mobility Using walking aids, such as a cane or crutch
You will normally be offered a knee replacement if you have severe pain, swelling and stiffness in your knee joint and your ability to move the joint is significantly reduced. A knee replacement is major surgery, so is normally only recommended if non-surgical options have not helped reduce pain or improve mobility. Knee replacement may be considered for adults of all ages, although young, physically active people are more likely to wear out their replacement joint. As a result, knee replacement is typically recommended for older, less active people, as the replacement joint is less likely to wear out and need to be replaced. Most people who have a total knee replacement are between the ages of 60 and 80. They need to be well enough to cope with both a major operation and the rehabilitation afterwards. The earlier you have a knee replacement, the greater the chance you will eventually need further surgery. However, there is some evidence that having treatment before the knee becomes very stiff leads to a better surgical outcome. If you are having a knee replacement because of arthritis and also need a hip replacement, the hip should be replaced first as you will need a flexible hip to do the exercises that are necessary after a knee replacement operation.
Risks and complications
As with any operation, knee replacement surgery has risks as well as benefits. Most people
who have a knee replacement have no problems at all. Complications occur in about 1 in 20
cases, but most of these are minor and can be successfully treated. Your anesthetist and
surgeon can answer any questions you may have about your personal risks from anesthetic
and the surgery itself.
Risks include:
Infection of the wound. This will usually be treated with antibiotics, but occasionally the wound can become deeply infected and require further surgery. Very occasionally, it requires replacement of the artificial knee joint.
Fracture in the bone around the artificial joint during or after surgery. Treatment will depend on the location and extent of the fracture.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Excess bone forming around the artificial knee joint and restricting movement of the knee. Further surgery may be able to remove this and restore movement.
Excess scar tissue forming and restricting movement of the knee. Further surgery may be able to remove this and restore movement.
The kneecap becoming dislocated. Surgery can usually repair this. Numbness in the area around the wound scar. Allergic reaction. You may have an allergic reaction to the bone cement if this is used
in your procedure. Unexpected bleeding into the knee joint. Ligament, artery or nerve damage in the area around the knee joint. Blood clots or deep vein thrombosis (DVT). Clots may form in the leg veins as a result
of reduced movement in the leg during the first few weeks after surgery. They can be prevented by using special support stockings, starting to walk or exercise soon after surgery, and by using anticoagulant medicines.
In some cases, the new knee joint may not be completely stable and further surgery may be needed to correct it.
A total knee replacement generally requires between one and a half to three hours of operative time. After surgery, patients are taken to a recovery room, where vital organs are frequently monitored. When stabilized, patients are returned to their hospital room.
Back in the ward, the team will continue to monitor you carefully. You will have a large dressing on your knee to protect your wound. A drain will siphon off blood from the operation site to prevent it collecting inside the wound. You may also be given oxygen through a mask or tubes. If necessary, you will be given a blood transfusion.
You may be allowed to have a drink about an hour after returning to the ward and, depending on your condition, you will also be allowed to have food. You will need help moving position and using a bed pan. Your wound dressing will be changed regularly until it has healed over.
Postoperative recovery
The staff will help you to get up and walk about as quickly as possible. If you have had minimally invasive surgery with partial prosthesis implantation, you may be able to walk on the same day as your operation. Walking with a frame or crutches is encouraged. Most people are able to walk independently with sticks after about a week.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
During your stay in hospital, a physiotherapist will teach you exercises to help strengthen your knee. You can usually begin these the day after your operation. It is very important that you follow the physiotherapist's advice to avoid complications or dislocation of your new joint.
It is normal to experience some initial discomfort while walking and exercising, and your legs and feet may be swollen. You may be put on a passive motion machine to restore movement in your knee and leg. This support will slowly move your knee while you are in bed. It helps to decrease swelling by keeping your leg raised and helps improve your circulation. Knee replacement surgery is very successful, but the success of the procedure is partly due to the rehabilitation period that follows the surgery. For patients to expect a good result from knee replacement surgery, they must be an active rehab participant.
It is important for patients to continue in an outpatient physical-therapy program along with home exercises for optimal outcome of total knee replacement surgery. Patients will be asked to continue exercising the muscles around the replaced joint to prevent scaring (contracture) and maintain muscle strength for the purposes of joint stability. These exercises after surgery can reduce recovery time and lead to optimal strength and stability. Patients should watch for warning signs of infection including abnormal redness, increasing warmth, swelling, or unusual pain. It is important to report any injury to the joint to the doctor immediately. Future activities are generally limited to those that do not risk injuring the replaced joint. Sports that involve running or contact are avoided, in favor of leisure sports, such as golf, and swimming. Swimming is the ideal form of exercise, since the sport improves muscle strength and endurance without exerting any pressure or stress on the replaced joint. Patients with joint replacements should alert their doctors and dentists that they have an artificial joint. These joints are at risk for infection by bacteria introduced by any invasive procedures such as surgery, dental or gum work, urological and endoscopic procedures, as well as from infections elsewhere in the body. The treating physician will typically prescribe antibiotics before, during, and immediately after any elective procedures in order to prevent infection of the replaced joint. Though infrequent, patients with total knee replacements can require a second operation years later. The second operation can be necessary because of loosening, fracture, or other complications of the replaced joint. Reoperations are generally not as successful as the original operation and carry higher risks of complications. Future replacement devices and techniques will improve patient outcomes and lead to fewer complications.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
SHOULDER
REPLACEMENT
HOSPITALIZATION: 3 – 5 DAYS SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_09
The shoulder joint is a ball and socket that connects the upper arm to the body. A healthy shoulder can allow you to have an active life, participate in the activities you enjoy and comfortably accomplish everyday tasks like driving, combing your hair, reaching for your wallet and getting a good night’s sleep. However, a chronic shoulder problem can limit your activities and interfere with your quality of life. Conditions that can affect your shoulder include arthritis, fracture, shoulder dislocation or rotator cuff tear.
Although shoulder joint replacement is less common than knee or hip replacement, it is just as successful in relieving joint pain. Shoulder replacement surgery was first performed in the United States in the 1950s to treat severe shoulder fractures. Over the years, shoulder joint replacement has come to be used for many other painful conditions of the shoulder, such as different forms of arthritis. If nonsurgical treatments likemedications and activity changes are no longer helpful for relieving pain, you may want to consider shoulder joint replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain and help you resume everyday activities. Whether you have just begun exploring treatment options or have already decided to have shoulder joint replacement surgery, this text will help you understand more about this valuable procedure.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Rotator cuff tear
Although shoulder joint replacement is less common than knee or hip replacement, it is just as successful in relieving joint pain. Shoulder replacement surgery was first performed in the United States in the 1950s to treat severe shoulder fractures. Over the years, shoulder joint replacement has come to be used for many other painful conditions of the shoulder, such as different forms of arthritis. If nonsurgical treatments like medications and activity changes are no longer helpful for relieving pain, you may want to consider shoulder joint replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain and help you resume everyday activities. Whether you have just begun exploring treatment options or have already decided to have shoulder joint replacement surgery, this text will help you understand more about this valuable procedure.
Anatomy
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle). The shoulder is a ball-and-socket joint: The ball, or head, of your upper arm bone fits into a shallow socket in your shoulder blade. This socket is called the glenoid. The surfaces of the bones where they touch are covered with articular cartilage, a smooth substance that protects the bones and enables them to move easily. A thin, smooth tissue called synovial membrane covers all remaining surfaces inside the shoulder joint. In a healthy shoulder, this membrane makes a small amount of fluid that lubricates the cartilage and eliminates almost any friction in your shoulder. The muscles and tendons that surround the shoulder provide stability and support. All of these structures allow the shoulder to rotate through a greater range of motion than any other joint in the body. In shoulder replacement surgery, the damaged parts of the shoulder are removed and replaced with artificial components, called prosthesis. The treatment options are either replacement of just the head of the humerus bone (ball), or replacement of both the ball and the socket (glenoid). Several conditions can cause shoulder pain and disability, and lead patients to consider shoulder joint replacement surgery.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Osteoarthritis (Degenerative Joint Disease) This is an age-related "wear and tear" type of arthritis. It usually occurs in people 50 years of age and older, but may occur in younger people, too. The cartilage that cushions the bones of the shoulder softens and wears away. The bones then rub against one another. Over time, the shoulder joint slowly becomes stiff and painful. Unfortunately, there is no way to prevent the development of osteoarthritis. It is a common reason people have shoulder replacement surgery.
Rheumatoid Arthritis This is a disease in which the synovial membrane that surrounds the joint becomes inflamed and thickened. This chronic inflammation can damage the cartilage and eventually cause cartilage loss, pain, and stiffness. Rheumatoid arthritis is the most common form of a group of disorders termed "inflammatory arthritis." Post-traumatic Arthritis This can follow a serious shoulder injury. Fractures of the bones that make up the shoulder or tears of the shoulder tendons or ligaments may damage the articular cartilage over time. This causes shoulder pain and limits shoulder function. Rotator Cuff Tear Arthropathy A patient with a very large, long-standing rotator cuff tear may develop cuff tear arthropathy. In this condition, the changes in the shoulder joint due to the rotator cuff tear may lead to arthritis and destruction of the joint cartilage. Avascular Necrosis (Osteonecrosis) Avascular necrosis is a painful condition that occurs when the blood supply to the bone is disrupted. Because bone cells die without a blood supply, osteonecrosis can ultimately cause destruction of the shoulder joint and lead to arthritis. Chronic steroid use, deep sea diving, severe fracture of the shoulder, sickle cell disease, and heavy alcohol use are risk factors for avascular necrosis. Severe Fractures A severe fracture of the shoulder is another common reason people have shoulder replacements. When the head of the upper arm bone is shattered, it may be very difficult for a doctor to put the pieces of bone back in place. In addition, the blood supply to the bone pieces can be interrupted. In this case, a surgeon may recommend a shoulder replacement. Older patients with osteoporosis are most at risk for severe shoulder fractures.
BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Failed Previous Shoulder Replacement Surgery Although uncommon, some shoulder replacements fail, most often because of implant loosening, wear, infection, and dislocation. When this occurs, a second joint replacement surgery — called a revision surgery — may be necessary.
Is Shoulder Joint Replacement for You?
The decision to have shoulder replacement surgery should be a cooperative one between you, your family, your family physician, and your orthopedic surgeon. There are several reasons why your doctor may recommend shoulder replacement surgery. People who benefit from surgery often have:
Severe shoulder pain that interferes with everyday activities, such as reaching into a cabinet, dressing, toileting, and washing.
Moderate to severe pain while resting. This pain may be severe enough to prevent a good night's sleep.
Loss of motion and/or weakness in the shoulder. Failure to substantially improve with other treatments such as anti-inflammatory
medications, cortisone injections, or physical therapy.
Your family physician may refer you to an orthopedic surgeon for a thorough evaluation to determine if you can benefit from this surgery. An evaluation with an orthopedic surgeon consists of several components:
A medical history. Your orthopedic surgeon will gather information about your general health and ask you about the extent of your shoulder pain and your ability to function. A physical examination. This will assess shoulder motion, stability, and strength. X-rays. These images help to determine the extent of damage in your shoulder. They can show loss of the normal joint space between bones, flattening or irregularity in the shape of the bone, bone spurs, and loose pieces of cartilage or bone that may be floating inside the joint. Other tests. Occasionally blood tests, a magnetic resonance imaging (MRI) scan, or a bone scan may be needed to determine the condition of the bone and soft tissues of your shoulder.
Your orthopedic surgeon will review the results of your evaluation with you and discuss whether shoulder joint replacement is the best method to relieve your pain and improve your function. Other treatment options — including medications, injections, physical therapy, or other types of surgery — will also be discussed and considered.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Shoulder Replacement Options
Shoulder replacement surgery is highly technical. It should be performed by a surgical team with experience in this procedure. There are different types of shoulder replacements. Your surgeon will evaluate your situation carefully before making any decisions. He or she will discuss with you which type of replacement would best meet your health needs. Do not hesitate to ask what type of implant will be used in your situation, and why that choice is right for you. Total Shoulder Replacement The typical total shoulder replacement involves replacing the arthritic joint surfaces with a highly polished metal ball attached to a stem, and a plastic socket. These components come in various sizes. They may be either cemented or "press fit" into the bone. If the bone is of good quality, your surgeon may choose to use a non-cemented (press-fit) humeral component. If the bone is soft, the humeral component may be implanted with bone cement. In most cases, an all-plastic glenoid (socket) component is implanted with bone cement. Implantation of a glenoid component is not advised if:
The glenoid has good cartilage The glenoid bone is severely deficient The rotator cuff tendons are irreparably torn
Patients with bone-on-bone osteoarthritis and intact rotator cuff tendons are generally good candidates for conventional total shoulder replacement.
Stemmed Hemiarthroplasty Depending on the condition of your shoulder, your surgeon may replace only the ball. This procedure is called a hemiarthroplasty. In a traditional hemiarthroplasty, the head of the humerus is replaced with a metal ball and stem, similar to the component used in a total shoulder replacement. This is called a stemmed hemiarthroplasty. Some surgeons recommend hemiarthroplasty when the humeral head is severely fractured but the socket is normal. Other indications for a hemiarthroplasty include:
Arthritis that only involves the head of the humerus with a glenoid that has a healthy and intact cartilage surface
Shoulders with severely weakened bone in the glenoid Some shoulders with severely torn rotator cuff tendons and arthritis
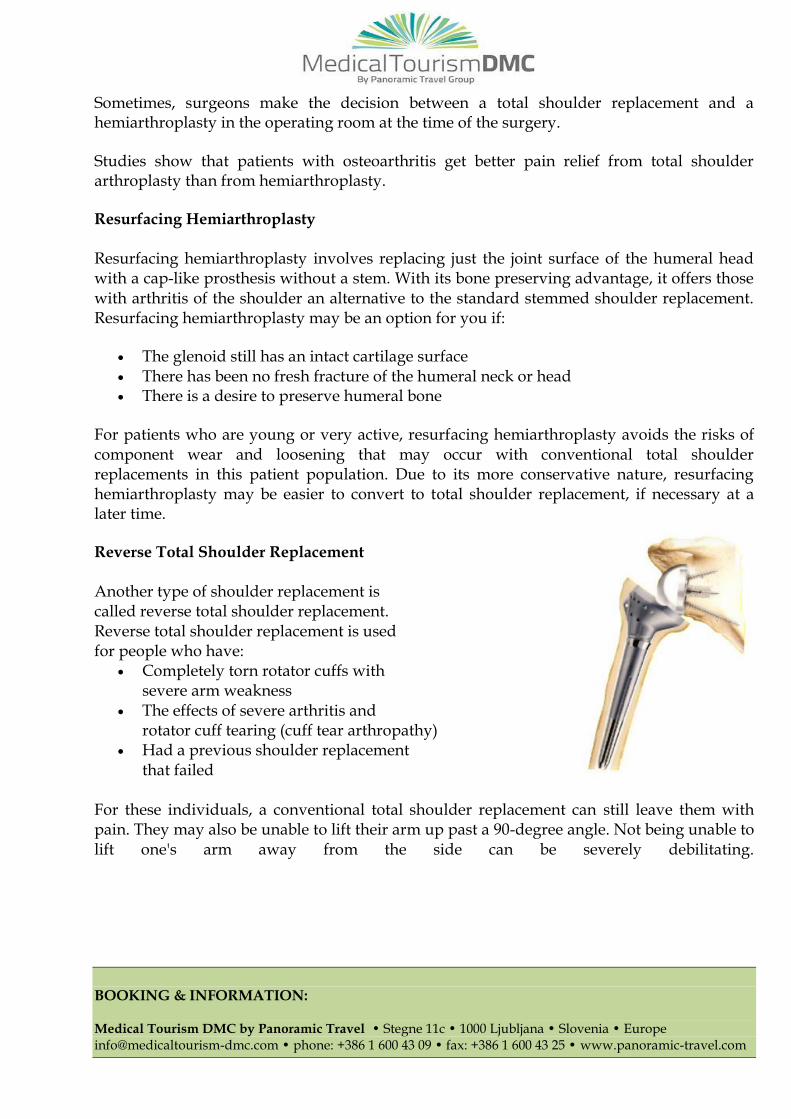
BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Sometimes, surgeons make the decision between a total shoulder replacement and a hemiarthroplasty in the operating room at the time of the surgery.
Studies show that patients with osteoarthritis get better pain relief from total shoulder arthroplasty than from hemiarthroplasty.
Resurfacing Hemiarthroplasty Resurfacing hemiarthroplasty involves replacing just the joint surface of the humeral head with a cap-like prosthesis without a stem. With its bone preserving advantage, it offers those with arthritis of the shoulder an alternative to the standard stemmed shoulder replacement. Resurfacing hemiarthroplasty may be an option for you if:
The glenoid still has an intact cartilage surface There has been no fresh fracture of the humeral neck or head There is a desire to preserve humeral bone
For patients who are young or very active, resurfacing hemiarthroplasty avoids the risks of component wear and loosening that may occur with conventional total shoulder replacements in this patient population. Due to its more conservative nature, resurfacing hemiarthroplasty may be easier to convert to total shoulder replacement, if necessary at a later time.
Reverse Total Shoulder Replacement Another type of shoulder replacement is called reverse total shoulder replacement. Reverse total shoulder replacement is used for people who have:
Completely torn rotator cuffs with severe arm weakness
The effects of severe arthritis and rotator cuff tearing (cuff tear arthropathy)
Had a previous shoulder replacement that failed
For these individuals, a conventional total shoulder replacement can still leave them with pain. They may also be unable to lift their arm up past a 90-degree angle. Not being unable to lift one's arm away from the side can be severely debilitating.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
In reverse total shoulder replacement, the socket and metal ball are switched. That means a metal ball is attached to the shoulder bone and a plastic socket is attached to the upper arm bone. The specific design of the reversed prosthesis allows for the stronger deltoid muscle to take over for the rotator cuff for function and mobility. This allows the patient to use the deltoid muscle instead of the torn rotator cuff to lift the arm.
Risks and Complications Your orthopedic surgeon will explain the potential risks and complications of shoulder joint replacement, including those related to the surgery itself and those that can occur over time after your surgery. When complications occur, most are successfully treatable. Possible complications include the following. Infection Infection is a complication of any surgery. In shoulder joint replacement, infection may occur in the wound or deep around the prosthesis. It may happen while in the hospital or after you go home. It may even occur years later. Any infection in your body can spread to your joint replacement. Infection is a very serious complication and therefore there are significant measures taken to avoid this complication. If an infection develops, the entire implanted joint may need to be removed in order to eradicate the infection. Prosthesis Problems Although prosthesis designs and materials, as well as surgical techniques, continue to advance, the prosthesis may wear down and the components may loosen. The components of a shoulder replacement may also dislocate. Excessive wear, loosening, or dislocation may require additional surgery (revision procedure). Nerve and Injury Nerves in the vicinity of the joint replacement may be damaged during surgery, although this type of injury is infrequent. Over time, these nerve injuries often improve and may completely recover.
Preparing for Surgery Medical Evaluation If you decide to have shoulder replacement surgery, your orthopedic surgeon may ask you to schedule a complete physical examination with your family physician several weeks before surgery. This is needed to make sure you are healthy enough to have the surgery and complete the recovery process. Many patients with chronic medical conditions, like heart disease, must also be evaluated by a specialist, such a cardiologist, before the surgery.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Medications Be sure to talk to your orthopedic surgeon about the medications you take. Some medications may need to be stopped before surgery. For example, the following over-the-counter medicines may cause excessive bleeding and should be stopped 2 weeks before surgery:
Non-steroidal anti-inflammatory medications, such as aspirin, ibuprofen, and naproxen sodium
Most arthritis medications
If you take blood thinners, either your primary care doctor or cardiologist will advise you about stopping these medications before surgery. Home Planning Making simple changes in your home before surgery can make your recovery period easier. For the first several weeks after your surgery, it will be hard to reach high shelves and cupboards. Before your surgery, be sure to go through your home and place any items you may need afterwards on low shelves. When you come home from the hospital, you will need help for a few weeks with some daily tasks like dressing, bathing, cooking, and laundry. If you will not have any support at home immediately after surgery, you may need a short stay in a rehabilitation facility until you become more independent.
Your Surgery
Before Your Operation Wear loose-fitting clothes and a button-front shirt when you go to the hospital for your surgery. After surgery, you will be wearing a sling and will have limited use of your arm. You will most likely be admitted to the hospital on the day of your surgery. After admission, you will be taken to the preoperative preparation area and will meet a doctor from the anesthesia department. You, your anesthesiologist, and your surgeon will discuss the type of anesthesia to be used. You may be provided a general anesthetic (you are asleep for the entire operation), a regional anesthetic (you may be awake but have no feeling around the surgical area), or a combination of both types.
Surgical Procedure The procedure to replace your shoulder joint with an artificial device usually takes about 2 hours. Shoulder replacement surgery lasts about two hours. The incision for the surgery is along the front of the shoulder joint and usually about four to six inches long. The surgery is most commonly done under general anesthesia. Time in the operating room may be more than three hours (because of anesthesia and preparation), and usually patients are in the recovery room for about an hour.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
After surgery, you will be moved to the recovery room, where you will remain for several hours while your recovery from anesthesia is monitored. After you wake up, you will be taken to your hospital room.
Surgical Procedure The procedure to replace your shoulder joint with an artificial device usually takes about 2 hours. Shoulder replacement surgery lasts about two hours. The incision for the surgery is along the front of the shoulder joint and usually about four to six inches long. The surgery is most commonly done under general anesthesia. Time in the operating room may be more than three hours (because of anesthesia and preparation), and usually patients are in the recovery room for about an hour. After surgery, you will be moved to the recovery room, where you will remain for several hours while your recovery from anesthesia is monitored. After you wake up, you will be taken to your hospital room.
Recovery
Your medical team will give you several doses of antibiotics to prevent infection. Most patients are able to eat solid food and get out of bed the day after surgery. You will most likely be able to go home on the first, second or third day after surgery.
Pain Management After surgery, you will feel some pain, but your surgeon and nurses will provide medication to make you feel as comfortable as possible. Pain management is an important part of your recovery. Physical therapy will begin soon after surgery, and when you feel less pain, you can start moving sooner and get your strength back more quickly. Talk with your surgeon if postoperative pain becomes a problem.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Rehabilitation A careful, well-planned rehabilitation program is critical to the success of a shoulder replacement. You usually start gentle physical therapy soon after the operation. Your surgeon or physical therapist will provide you with a home exercise program to strengthen your shoulder and improve flexibility.
Your Recovery At Home When you leave the hospital, your arm will be in a sling. You will need the sling to support and protect your shoulder for the first 2 to 4 weeks after surgery. Wearing a sling will protect your shoulder after surgery.
Wound care. You will have staples running along your wound or a suture beneath your skin. The staples will be removed several weeks after surgery. A suture beneath your skin will not require removal. Avoid soaking the wound in water until it has thoroughly sealed and dried. You may continue to bandage the wound to prevent irritation from clothing.
Activity. Exercise is a critical component of home care, particularly during the first few weeks after surgery. Follow your surgeon's home exercise plan to help you regain strength. Most patients are able to perform simple activities such as eating, dressing and grooming within 2 weeks after surgery. Some pain with activity and at night is common for several weeks after surgery. Usually within two to three months, patients are able to return to most normal activities and place an emphasis on strengthening the muscles around the shoulder and maintaining range of motion. Driving a car is not allowed for 2 to 4 weeks after surgery.
Do's and Don'ts
The success of your surgery will depend largely on how well you follow your orthopedic surgeon's instructions at home during the first few weeks after surgery. Here are some common do's and don'ts for when you return home:
Don't use the arm to push yourself up in bed or from a chair because this requires forceful contraction of muscles.
Do follow the program of home exercises prescribed for you. You may need to do the exercises 2 to 3 times a day for a month or more.
Don't overdo it! If your shoulder pain was severe before the surgery, the experience of pain-free motion may lull you into thinking that you can do more than is prescribed. Early overuse of the shoulder may result in severe limitations in motion.
Don't lift anything heavier than a glass of water for the first 2 to 4 weeks after surgery. Do ask for assistance. Your physician may be able to recommend an agency or facility
if you do not have home support.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Don't participate in contact sports or do any repetitive heavy lifting after your shoulder replacement.
Do avoid placing your arm in any extreme position, such as straight out to the side or behind your body for the first 6 weeks after surgery.
Many thousands of patients have experienced an improved quality of life after shoulder joint replacement surgery. They experience less pain, improved motion and strength, and better function.
Contrary to widespread belief, total surgical replacement of arthritic shoulder joints carries no greater risk of complications than replacement of other major joints, a recent Johns Hopkins study published in Clinical Orthopedics and Related research suggests. In fact, the study shows that people who undergo shoulder replacement to relieve chronic and significant pain can expect significantly fewer complications, much shorter hospital stays and less costs than patients undergoing hip or knee replacement.
The research team, led by Edward McFarland, MD, director of the Division of Adult Orthopedics at The Johns Hopkins Hospital, analyzed patient information from all arthroplasties performed in their institution to alleviate osteoarthritis pain between 1994 and 2001, including details of 15,414 hip surgeries, 34,471 knee operations and 625 shoulder
procedures."After looking at how all these patients fared, we concluded that, comparatively, total shoulder surgery is just as safe and effective as other types of arthroplasties," says McFarland. "Lower numbers of shoulder procedures done both regionally and nationally may indicate that many people live with shoulder pain because they fear that the corrective surgery is too risky. But we have found that this is just not true."
According to nationwide 2003 Medicare figures, 6,700 people had shoulder joints replaced
that year, compared to 106,887 hip replacements and 199,195 total knee replacements.Patients in the study who had shoulder surgery had far fewer in-hospital postsurgical complications (7.5 percent) compared with those patients who had their hips and knees replaced (15.5 percent and 14.7 percent, respectively).
McFarland's team also determined that the average time a person remained hospitalized after the surgery was lowest for those recovering from shoulder procedures (just 2.42 days for shoulder patients, versus more than 4 days for both the hip and knee equivalents). "Ninety-nine percent of the people who have a shoulder replacement for arthritis get pain relief and say that they wish they had done it sooner," says McFarland. "This study indicates there may be little reason to wait."
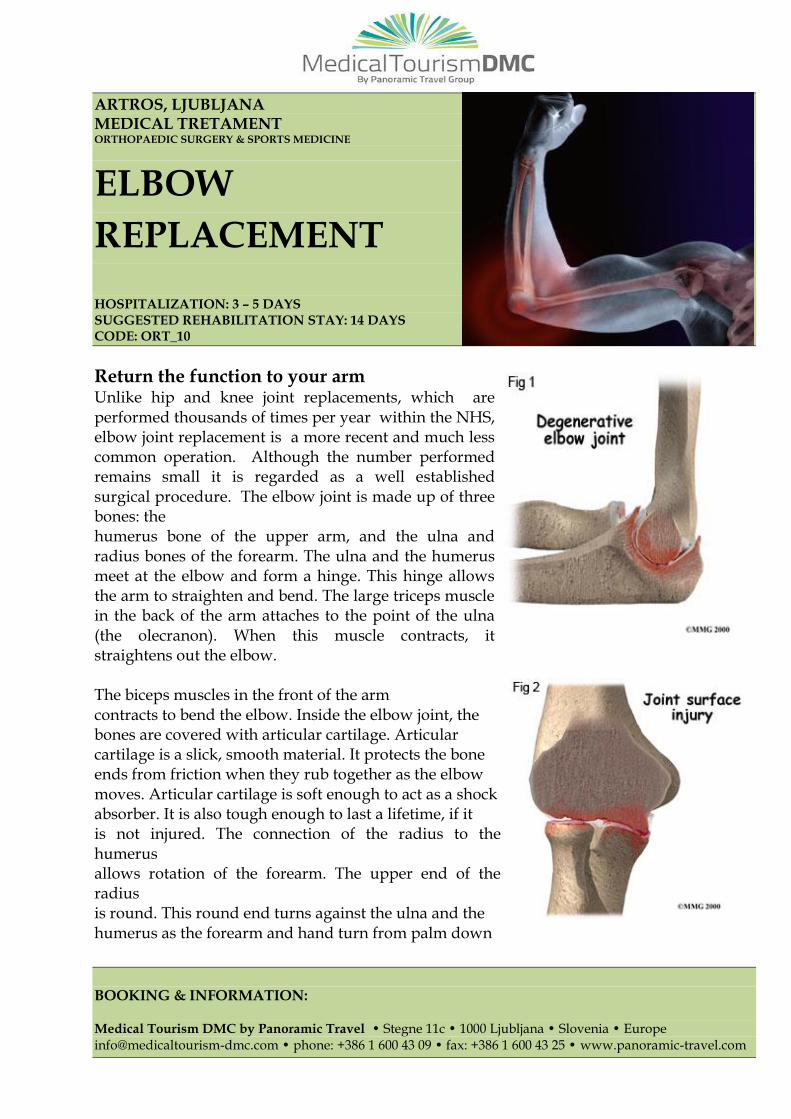
BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
ELBOW
REPLACEMENT
HOSPITALIZATION: 3 – 5 DAYS SUGGESTED REHABILITATION STAY: 14 DAYS CODE: ORT_10
Return the function to your arm Unlike hip and knee joint replacements, which are performed thousands of times per year within the NHS, elbow joint replacement is a more recent and much less common operation. Although the number performed remains small it is regarded as a well established surgical procedure. The elbow joint is made up of three bones: the humerus bone of the upper arm, and the ulna and radius bones of the forearm. The ulna and the humerus meet at the elbow and form a hinge. This hinge allows the arm to straighten and bend. The large triceps muscle in the back of the arm attaches to the point of the ulna (the olecranon). When this muscle contracts, it straightens out the elbow. The biceps muscles in the front of the arm contracts to bend the elbow. Inside the elbow joint, the bones are covered with articular cartilage. Articular cartilage is a slick, smooth material. It protects the bone ends from friction when they rub together as the elbow moves. Articular cartilage is soft enough to act as a shock absorber. It is also tough enough to last a lifetime, if it is not injured. The connection of the radius to the humerus allows rotation of the forearm. The upper end of the radius is round. This round end turns against the ulna and the humerus as the forearm and hand turn from palm down

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
(pronation) to palm up (supination). Elbow joint replacement surgery is performed when other interventions, medical and surgical, will not offer a satisfactory outcome. Underlying pathology includes:
Osteoarthritis. Rheumatoid arthritis (RA). Complex fracture of the elbow, even in the elderly. Severely damaged or torn soft tissues in the elbow resulting in instability. Malignancy in or around the elbow. Poor results from previous elbow surgery.
Indication for operation can be summarized as severe pain with radiological changes of joint destruction in the presence of failed conservative treatment. The commonest underlying pathology is RA. Before operation the disease process of the RA should be under control.
Preoperative assessment This is as for most surgery. PA and lateral X-rays of the joint are required and the usual blood tests are performed. In elderly patients the routine will include chest X-ray and ECG.
Surgery The operation usually takes about one to two hours. It is usually performed under generalanesthesia but regional anesthesia with sedation can be employed. An incision is made, usually on the dorsal side, to expose the elbow joint. The surgeon removes the lower end of the humerus and the upper end of the ulna, along with any damaged tissue. The surgeon then drills out a portion of the center of the humerus and ulna and inserts one stem of the prosthesis into each. Usually, the prosthesis is cemented into place. The two stems are joined with the hinge mechanism. The wound is closed, and a bandage is applied to splint the arm for stability. Some surgeons apply a plaster cast with the elbow extended, others with the elbow at 90°. The plaster cast is usually removed at 48 to 72 hours and gentle mobilization is commenced.
Risks and Complications There are risks attached to any form of surgery:
Hemorrhage Infection Thromboembolism is less common with upper limb surgery

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
There are specific risks to this operation:
Nerve damage during surgery, especially the ulnar nerve. Blood vessel damage during surgery. Fracture of bone during surgery. Dislocation of the prosthesis. Loosening of the implant over time. Allergic reaction to the implant. Fracture of the prosthesis is uncommon but if it can occur, results of revision surgery
are reasonably satisfactory
Postoperative management The patient will stay in hospital for about 3 or 4 days. A splint may be used after surgery to help stabilize the elbow.
Physiotherapy starts with gentle flexing exercises. Patients who have a splint typically start therapy a few weeks later than those who do not.
The patient will need help with everyday activities, such as driving, shopping, bathing, meal preparation, and household chores, for up to 6 weeks.
Some patients may begin to regain function of the elbow as soon as 12 weeks after surgery, although additional recovery can take up to a year.
The patient should not lift more than about 2.5 kg with the operated arm, even when fully recovered.
A physical or occupational therapist will direct your rehabilitation program. Recovery takes up to three months after elbow replacement surgery. The first few therapy treatments will focus on controlling the pain and swelling from surgery. Heat treatments may be used. Your therapist may also use gentle massage and other types of hands-on treatments to ease muscle spasm and pain. Then you'll begin gentle range-of-motion exercises. Strengthening exercises are used to give added stability around the elbow joint. You'll learn ways to lift and carry items in order to do your tasks safely and with the least amount of stress on your elbow joint. As with any surgery, you need to avoid doing too much, too quickly. Some of the exercises you'll do are designed get your elbow working in ways that are similar to your work tasks and daily activities. Your therapist will help you find ways to do your tasks that don't put too much stress on your new elbow joint. Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems. Your therapist's goal is to help you keep your pain under control, improve your strength and range of motion, and maximize the use of your elbow. When you are well under way, regular visits to the therapist's office will end. Your therapist will continue to be a resource for you, but you will be in charge of doing exercises as part of an ongoing home program.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
Prognosis Elbow replacement surgery relieves pain for most patients. Full benefit is not usually felt until about 6 months after operation. Alternatives to total elbow joint replacement surgery Synovectomy. This treatment option, for people with rheumatoid arthritis, involves removing the swollen (inflamed) synovial tissue that is causing pain around the elbow joint. At Mayo Clinic, this procedure is typically done using arthroscopy, a minimally invasive approach. Debridement. This surgery for osteoarthritis entails removing debris on and around the elbow joint, including bone spurs (osteophytes) and loose pieces of bone or cartilage. Surgeons at Mayo Clinic typically perform this procedure through small incisions at the elbow joint using arthroscopy. Osteocapsular arthroplasty. The procedure involves synovectomy and a more thorough form of debridement that removes bone spurs, loose bone and cartilage, and recontours bones that have become deformed or deteriorated due to arthritis. Interposition arthroplasty. This surgery involves resurfacing the elbow joint, which reduces joint pain by preventing bones from rubbing together. It is performed on people who are not candidates for osteocapsular arthroplasty or joint replacement. Partial joint (radial head) replacement. Partial replacement entails resurfacing the radial head (where the radius and humerus bones meet) and sometimes the capitellum bone joint in people with fractures from injuries. Mayo Clinic doctors developed the prosthetic replacement head for this procedure and special surgical instruments, which permit replacement with prosthesis of the same size and shape as your joint.
BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
MAGNETIC RESONANCE IMAGING CODE: ORT_11
Diagnostic imaging with magnetic resonance has become a standard examination for many orthopedic conditions. It enables very specific, noninvasive detection of injuries of soft tissue structures, such as ligaments, tendons and muscles, cartilage and also meniscus. In Artros we operate a modern dedicated musculoskeletal magnetic resonance tomograph.
Its open configuration facilitates positioning the patient and is not associated with unpleasant feeling of confinement and anxiety as can occur with some patients in closed design devices. The evaluation and interpretation of the findings is undertaken is close co-operation between treating orthopedic surgeon and a radiology specialist. Through this tight interdisciplinary cooperation we can assure the optimal clinical value of this examination.

BOOKING & INFORMATION:
Medical Tourism DMC by Panoramic Travel • Stegne 11c • 1000 Ljubljana • Slovenia • Europe [email protected] • phone: +386 1 600 43 09 • fax: +386 1 600 43 25 • www.panoramic-travel.com
ARTROS, LJUBLJANA MEDICAL TRETAMENT ORTHOPAEDIC SURGERY & SPORTS MEDICINE
ESWT NUMBER OF THERAPIES IS SUGGESED UPON FIRST DOCTOR CONSULATATION
SUGGETES STAY IN SLOVENIA: 14 DAYS CODE: ORT_12
Various tendon overuse injuries and chronic back pain syndromes with muscle spasm are among the most common orthopedic problems. Common treatments for these problems include rest, activity modification and classic physical therapy program comprising exercises, massage, stretching, ultrasound, laser and magnetic therapy.
Extracorporeal Shock Wave Therapy (ESWT) is a relatively new treatment method that has been proven as highly efficient in treatment of these problems. The basic principle of this treatment is based on a generation of pressure shock waves by the use of special shock wave inducing transmitter in contact with the body surface. The shock waves emitted cause large pressure fluctuations in the soft tissues. In this way, in case of calcifications in the soft tissues, these seek to break into smaller particles, which can then be absorbed. In tendonitis the circulation of tendons is stimulated with this therapy, which accelerates the regeneration of tendons. In case of muscle spasms and painful knots that occur in chronic back pain syndromes, this treatment will cause them to relax.
Great advantages of this treatment are its noninvasive nature and also that it is not painful. Usually it needs to be repeated 3 – 5 times with one week of rest in between each treatment.