originalarticle - canadian journal of...
TRANSCRIPT



Return undeliverable Canadian Addresses to:
115 King Street West, Suite 220, Dundas, ON L9H 1V1
For Instructions to Authors, please visit http://www.andrewjohnpublishing.com/CJP/instructionstoauthors.html
Canadian Journal of P athology S3Supplement 2, Winter 2015
OriginalArticle
Selectiveprogesteronereceptormodulators:Clinicalrolesandeffectsonendometrialhistology
S4 Abstract/Resumé
S5 Introduction
S6 MedicalManagementofUterineLeiomyomata
S6 UlipristalAcetateintheManagementofUterineLeiomyomata
S7 HistologicEffectsofUlipristalAcetateandOtherSelective ProgesteroneReceptorModulators
S12 ProgesteroneReceptorModulator–AssociatedEndometrialChange inClinicalTrialsofUlipristalAcetate
S19 EndometrialHistologyinWomenTreatedforUterineLeiomyomata withUlipristalAcetate:PostmarketingExperienceatSt.Michael’s Hospital
S20 ADigitalReferenceToolforProgesteroneReceptor Modulator–AssociatedEndometrialChange
S20 Conclusion
S23 AppendixA:AccesstoSlidesDemonstratingProgesterone ReceptorModulator-AssociatedEndometrialChange
Canadian Journal of Pathology is published four times annually by Andrew John Publishing Inc., with offices at 115 King Street West, Dundas, ON, Canada L9H 1V1.
We welcome editorial submissions but cannot assume responsibility or commitment for unsolicited material. Any editorial material, including photographs that are accepted from an unsolicited contributor, will become the property of Andrew John Publishing Inc.
FEEDBACKWe welcome your views and comments. Please send them to Andrew John Publishing Inc., 115 King Street West, Dundas, ON, Canada L9H 1V1.
Copyright 2014 by Andrew John Publishing Inc. All rights reserved. Reprinting in part or in whole is forbidden without express written consent from the publisher.
Publications Agreement Number 40025049 • ISSN 1918-915X
EDITOR-IN-CHIEFGeorge M Yousef, MD PhD FRCPC (Path)
INTERIM EDITORMarie Abi Daoud, MD, MHSc, FRCPC
EDITORIAL BOARDManon Auger, MD, FRCPC, Cytopathology;
Calvino Cheng, BSc, MD, FRCPC, Pathology Informaticsand Quality Management;
Pierre Douville, MD, FRCPC, Medical Biochemistry;David K. Driman, MB ChB, FRCPC, Anatomical Pathology;
Lawrence Haley, MD, FRCPC, Hematopathology;Todd F. Hatchette, BSc, MD, FRCPC, Medical Microbiology;
Michael J. Shkrum, MD, FRCPC, Forensic Pathology;
FOUNDING EDITORJagdish Butany, MBBS, MS, FRCPC
MANAGING EDITORRose Simpson
COPY EDITORMichael Peebles
PROOFREADERScott Bryant
ART DIRECTORAmanda Zylstra, [email protected]
TRANSLATORAnouk Jaccarini
SALES AND CIRCULATION COORDINATORBrenda Robinson, [email protected]
ACCOUNTINGSusan McClung
GROUP PUBLISHERJohn D. Birkby, [email protected]
SUPPLEMENT 2, WINTER 2015
Contents
Hysterectomy sample showing Progesterone Receptor Modulator-Associated Endometrial Change in a patient receiving 5 mg UPA daily for almost 3 months.Note extensive cyst formation, a common finding in patients treated with UPA (H&E x25).
AbouttheCover

Supplement 2, Winter 2015S4 Canadian Journal of P athology
Selectiveprogesteronereceptormodulators:ClinicalrolesandeffectsonendometrialhistologyEleanor Latta MD FRCPC,1 Guylaine Lefebvre MD FRCSC,2 Alex Ferenczy MD3
ABSTRACTUlipristal Acetate (UPA), marketed as Fibristal in Canada and Esmya in Europe, was approved by Health Canada in 2013 for the treatment of moderate-to-severe symptoms and signs of uterine leiomyomata (fibroids) in adult women of reproductive age who are eligible for surgery. Ulipristal acetate belongs to a family of molecules called selective progesterone receptor modulators (SPRMs), which act differentially in various progesterone-responsive tissues and specifically induce the regression of uterine leiomyomata (ULs). Two phase III randomized controlled trials showed that 13 weeks of UPA treatment resulted in effective control of heavy menstrual bleeding and decreased UL size. These trials also showed that, as with other SPRM regimens, 3 months of daily UPA treatment resulted in mild thickening of the endometrium (40%) and in a histologic pattern of benign, nonphysiological endometria (70%). This response has been described as progesterone receptor modulator–associated endometrial change (PAEC). In most instances, normal endometrial histology returns within 6 months of UPA discontinuation. Differential diagnosis of PAEC includes disordered proliferative-pattern endometrium and endometrial hyperplasia; both conditions are associated with unopposed estrogen effects. This supplement was developed to assist pathologists in recognizing PAEC in order to facilitate the accurate diagnosis of this benign, reversible condition in patients receiving UPA or other SPRMs.
RÉSUMÉ L’acétate d’ulipristal (UPA, commercialisé sous le nom de Fibristal au Canada et d’Esmya en Europe) a été approuvé en 2013 par Santé Canada pour le traitement des signes et symptômes modérés a sévères des léiomyomes utérins (fibromes) chez les femmes adultes en âge de procréer et opérables. L’UPA appartient à la famille des modulateurs sélectifs des récepteurs de la progestérone (SPRM), qui agissent sur divers tissus sensibles à la progestérone et induisent spécifiquement une régression des léiomyomes. Deux essais cliniques de phase III contrôlés et randomisés ont démontré qu’un traitement de 13 semaines à l’UPA a permis de réduire efficacement les saignements menstruels excessifs et la taille des léiomyomes. Les essais montrent également que, comme pour d’autres SPRM, l’administration quotidienne d’UPA pendant trois mois entraîne un léger épaississement de l’endomètre (40 %) et des changements histologiques non physiologiques bénins de l’endomètre (70 %). Cette réaction est décrite comme une modification de l’endomètre associée aux modulateurs des récepteurs de la progestérone (PRM-associated endometrial changes, ou PAEC). Dans la plupart des cas, l’histologie de l’endomètre redevient normale dans les six mois qui suivent l’arrêt du traitement. Le diagnostic différentiel de la PAEC comprend un endomètre prolifératif désordonné et une hyperplasie endométriale; les deux affections sont associées aux effets des œstrogènes sans la présence de la progéstérone. Le présent supplément aidera les pathologistes à reconnaître la PAEC afin de faciliter le diagnostic de cette affection bénigne et réversible chez les patientes recevant de l’UPA ou un autre SPRM.
ORIGINAL ARTICLE
1Department of Laboratory Medicine, St. Michael’s Hospital, Toronto, Ontario2Department of Obstetrics and Gynecology, St. Michael’s Hospital, Toronto, Ontario3Department of Pathology, Jewish General Hospital, Montréal, QuébecCorrespondence may be directed to Eleanor Latta at [email protected] article has been peer reviewed.Competing interests: Eleanor Latta, Guylaine Lefebvre, and Alex Ferenczy have advised for Actavis Specialty Pharmaceuticals. Alex Ferenczy is a member of the pathology panel in the PEARL I, II, and III studies. Some of the material discussed here was presented in July 2014 at the Annual Congress of the Canadian Association of Pathologists, in Toronto, Ontario.

Canadian Journal of P athology S5Supplement 2, Winter 2015
IntroductionSelective progesterone receptor modulators (SPRMs) are progesterone receptor (PR) ligands that act in a tissue-specific manner to activate or repress PR-modulated responses in target organs, such as the uterus, the breast, and the ovary. Because of their tissue selectivity, SPRMs have physiological effects that are distinct from those of endogenous progesterones or pure antiprogestins.1,2
By definition, SPRMs have mixed activity, acting as PR agonists or antagonists, depending on cellular context. The molecular basis of this differential effect appears to reflect at least two differences among cell types: (1) the ratio between two alternative spliced PR isoforms (PR-A and PR-B) and (2) the expression of different transcriptional
co-activators and co-repressors.3-5 Deletion of the individual PR isoforms in mice suggests that these receptors have distinct roles; PR-B by itself can drive progestin responses in the mammary gland,6 whereas both PR isoforms are needed to mediate the various effects of progestins in the uterus.6,7
Conformational change in the PRs after SPRM binding is thought to account for the mixed agonistic (progestational) and antagonistic (estrogenic) effects of these drugs, as the PR/SPRM complex binds regulatory factors (co-activators and co-repressors) that are present in various levels in different target cell types (Figure 1).1, 3
Figure 1: Selective progesterone receptor modulators (SPRMs) have mixed activity as progesterone agonists and antagonists. The binding of SPRMs to progesterone receptor (PR) results in a conformational change in the PR, the dimerization of PR, and the binding of the SPRM/PR complex to the progesterone response element. The bound SPRM/PR/PR-E can interact with co-activators to increase transcription (agonism). The bound PR can also interact with co-repressors to prevent transcription activation (antagonism). The precise activity of each SPRM varies by tissue, based on the relative levels of co-activators and co-repressors. Adapted from Bouchard et al.3
LATTA ET AL.

Supplement 2, Winter 2015S6 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY
Medical Management of Uterine LeiomyomataUterine leiomyoma (UL) is a common benign uterine tumour that develops in women of reproductive age.8 The prevalence of ULs varies by age and ethnicity and is easily underestimated, depending on the diagnostic approach. Studies using ultrasound imaging indicate that 51% have evidence of ULs.9 Although many ULs are asymptomatic,10
common symptoms include heavy menstrual bleeding (sometimes leading to anemia), as well as pelvic pressure and pain. These symptoms can be debilitating, restricting the ability to work and to carry out daily activities.11 In some cases, depending on the size and location of the ULs, women may experience difficulties conceiving and may experience obstetric complications as well.12,13
The management of ULs depends on the nature and severity of the symptoms and on the patient’s age, priorities, and preferences. For instance, hysterectomy offers a definitive cure but cannot be considered for a woman wishing to retain her fertility. Myomectomy and uterine artery embolization preserve the uterus; however, 10% and 14%, respectively, of women who undergo a myomectomy or uterine artery embolization will require a hysterectomy within 5 years of the initial procedure.13,14
The medical management of ULs has traditionally aimed at alleviating symptoms. Until recently, no medication for the reduction of ULs was approved in Canada, although gonadotropin-releasing hormone (GnRH) agonists, such as leuprolide acetate (LPA), are often used off-label for this purpose.15 In a placebo-controlled trial, women treated with LPA showed significantly decreased uterus and UL size when compared to placebo controls, as well as a decrease in menstrual bleeding.16 As LPA suppresses estrogen to postmenopausal levels, women may experience menopause-like symptoms, including hot flashes, bone loss, and diminished libido. Estrogen or a combination of low-dose estrogen and progestin may be added to offset these symptoms.8 Uterus and UL size return to baseline after the discontinuation of treatment.17
Uterine leiomyomata develop under the influence of estrogen and progesterone.18,19 The primary role of estrogen signalling in UL development is to induce PR expression, thus sensitizing the leiomyomatous tissue to respond to progesterone secreted by the ovaries.18 Progesterone and PRs in turn contribute to UL growth by increasing cell proliferation and decreasing apoptosis. Antagonizing PR function with SPRMs has several distinct effects on UL cells, including suppression of neovascularization, cell proliferation, and extracellular collagen synthesis, as well as the activation of apoptosis.2
Ulipristal Acetate in the Management of Uterine LeiomyomataThe SPRM ulipristal acetate (UPA) was approved by Health Canada in 2013 for the treatment of moderate-to-severe signs and symptoms of leiomyomata in adult women of reproductive age who are eligible for surgery. Three large randomized controlled clinical trials of UPA for this indication have been reported to date, including two trials – PEARL I and PEARL II – that assessed the safety and efficacy of up to 13 weeks of daily UPA (5 mg and 10 mg daily doses) compared to placebo or LPA in women with symptomatic ULs and excessive bleeding.20,21 A follow-up trial, PEARL III, was a long-term open-label phase III study evaluating the efficacy and safety of multiple rounds of UPA in women with ULs.22
PEARL I and PEARL II included premenopausal women (18–50 years of age) with at least one UL at least 3 cm in diameter (as measured by ultrasound) but no ULs larger than 10 cm in diameter. In both studies, patients were included only if they were expected to be eligible for UL surgery following 3 months of treatment. In these studies, most women in the UPA arms reported amenorrhea. The median time to amenorrhea was less than 10 days, and menstruation resumed approximately 30 days following the end of UPA treatment.20,21
Uterine bleeding was controlled at week 13 in ≥90% of women receiving UPA, significantly better than placebo and not inferior to LPA. In PEARL I, both UPA doses resulted in a significant reduction in UL size when compared to placebo: −21%, −12%, and +3% change in total UL size for 5 mg UPA, 10 mg UPA, and placebo, respectively. In PEARL II, all treatments resulted in a size reduction of the largest three ULs, along with no significant between-group differences. However, in contrast to LPA patients, the majority of UPA patients maintained a reduced UL size for at least 6 months after UPA was discontinued.
In PEARL III, women received a 3-month open-label course of 10 mg of UPA taken once daily. After the completion of this first cycle, they could leave the study and attend a final follow-up visit 12 weeks later, or they could choose to continue in the PEARL III extension study, in which case they would receive three further 3-month courses of UPA along with the progestin norethindrone acetate or a placebo. Courses were separated by an interval of a full menstrual cycle up to the start of the second menstruation, during which time patients received neither UPA nor hormonal treatment.22 The median rates of amenorrhea were 79%, 89%, 88%, and 90% for the 209, 131, 119, and 107 women who received treatment courses 1, 2, 3, and 4, respectively; median UL size reductions were −45%, −63%, −67%, and −72%, respectively.22

Canadian Journal of P athology S7Supplement 2, Winter 2015
The findings of PEARL III suggest that in addition to the now-established role of UPA as a bridge to surgery, intermittent UPA dosing may be appropriate as a longer-term strategy for the medical management of ULs. Although further studies of intermittent use are ongoing, Canadian labelling currently restricts UPA treatment to a single 13-week cycle.23 In Canada, the approved dose of UPA is 5 mg daily, and treatment is indicated for adult women who are eligible for UL surgery.
Histologic Effects of Ulipristal Acetate and Other Selective Progesterone Receptor ModulatorsStudies of SPRMs have shown a spectrum of endometrial changes that range from normal physiological to nonphysiological, some of the latter resembling endometrial hyperplasia.24–26 In 2006, the National Institutes of Health) sponsored a workshop titled “Progesterone Receptor Modulators and the Endometrium” to evaluate a series of endometrial specimens from premenopausal women who had received one of four progesterone receptor modulators in clinical trials: mifepristone, asoprisnil, UPA, and JNJ17072341.27 Biopsy samples were read by seven gynecologic pathologists who were blind to the type and dose of drugs and to the duration of use. All samples, including some with endometrial polyps, were judged to be benign; none contained hyperplastic or neoplastic endometria.27
A subset of cases exhibited a novel combination of endometrial changes. These changes, which had not previously been encountered in routine practice, required new terminology and diagnostic criteria to prevent their being misclassified as hyperplasia.27 The panel suggested the term “progesterone receptor modulator–associated endometrial change” (PAEC) to describe a constellation of three of the nonphysiological endometrial histologic features observed in SPRM-treated individuals. Only when the three main features are found in the same endometrial tissue are they suggestive of PAEC.
Architectural AlterationsThe endometrial background is characterized by an admixture of estrogenic (mitosis) and progestogenic (secretory) effects (Figures 2 to 6). The endometrial architecture varies from a polypoid disordered proliferative pattern type (with extensive cyst formation) to a nonphysiological, poorly developed secretory-type endometrium. The gland-stroma ratio is normal. Typically, many of the cysts have a ragged, collapsed contour rather than a smooth, dilated contour. Cyst formation is the key histologic alteration of PAEC.
LATTA ET AL.
Figure 2: Hysterectomy sample showing PAEC in a patient receiving 5 mg UPA daily for almost 3 months. Note cyst formation, a common finding in patients treated with UPA (H&E ×25).

Supplement 2, Winter 2015S8 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY
Figure 3. (A) and (B) Hysterectomy samples showing collapsed cyst formation in a patient with progesterone receptor modulator–associated endometrial changes following 3 months of daily 5 mg doses of ulipristal acetate. The cystic glands are lined by a single layer of inactive cuboidal epithelium. (Hematoxylin and eosin. (A) ×50; (B) ×200)
Figure 4. Hysterectomy specimen from a patient treated with ulipristal acetate (5 mg) for 3 months. Time from end of treatment to surgery was 2 months. The endometrium is thickened and somewhat polypoid. It contains a cystically dilated gland and is surrounded by haphazardly distributed architecturally atypical glands with intraluminal projections, producing irregular luminal contours. (Hematoxylin and eosin, ×25)
A B
Canadian Journal of P athology S9Supplement 2, Winter 2015
LATTA ET AL.
BA
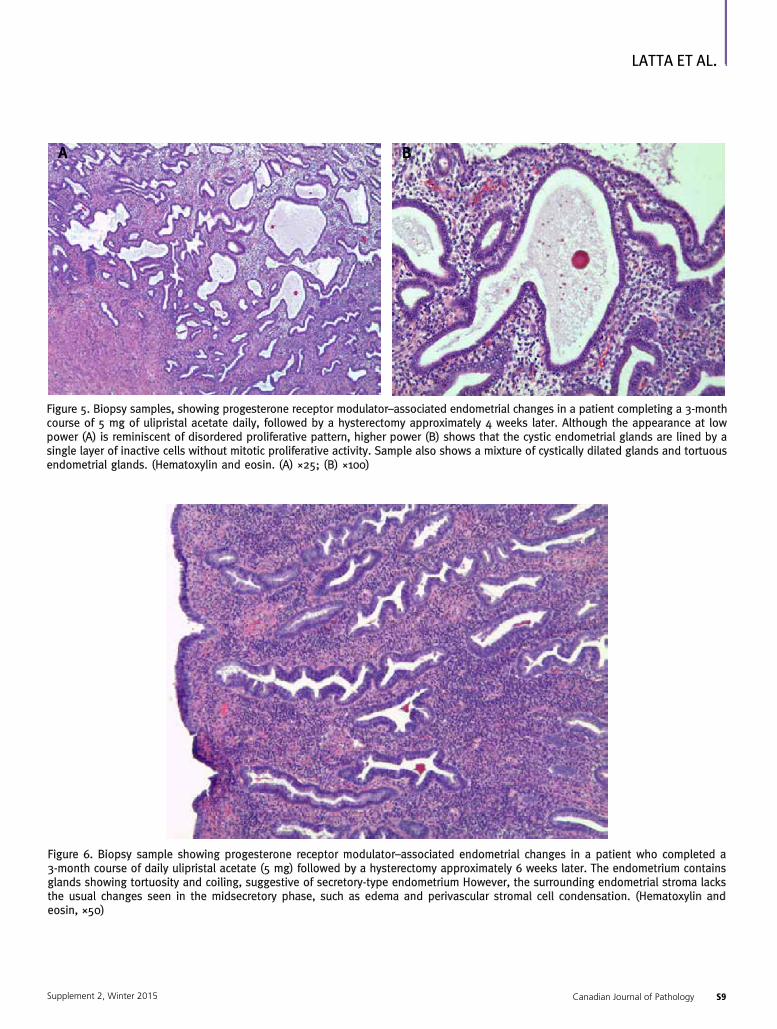
Figure 5. Biopsy samples, showing progesterone receptor modulator–associated endometrial changes in a patient completing a 3-month course of 5 mg of ulipristal acetate daily, followed by a hysterectomy approximately 4 weeks later. Although the appearance at low power (A) is reminiscent of disordered proliferative pattern, higher power (B) shows that the cystic endometrial glands are lined by a single layer of inactive cells without mitotic proliferative activity. Sample also shows a mixture of cystically dilated glands and tortuous endometrial glands. (Hematoxylin and eosin. (A) ×25; (B) ×100)
Figure 6. Biopsy sample showing progesterone receptor modulator–associated endometrial changes in a patient who completed a 3-month course of daily ulipristal acetate (5 mg) followed by a hysterectomy approximately 6 weeks later. The endometrium contains glands showing tortuosity and coiling, suggestive of secretory-type endometrium However, the surrounding endometrial stroma lacks the usual changes seen in the midsecretory phase, such as edema and perivascular stromal cell condensation. (Hematoxylin and eosin, ×50)

Supplement 2, Winter 2015S10 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY
Gland Cell ChangesNovel gland cell alterations include the presence of subnuclear vacuoles together with occasional mitotic figures and/or apoptotic bodies. The changes resemble early, cyclic postovulatory (16th day) endometrium.
However, apoptosis is not seen in the latter. Many glands are lined by an attenuated cuboidal epithelium, whereas others display tubal and particularly eosinophilic metaplasia (Figures 7 and 8).
Figure 7. Glandular architecture in progesterone receptor modulator–associated endometrial change. (A) Closer view of endometrial gland from patient in Figure 6. Note tortuous glandular architecture devoid of cytological features characterizing the normal secretory phase. (B) Cuboidal, inactive epithelium surrounding slightly dilated glands in a sample from a patient receiving 3 months of ulipristal acetate (5 mg daily). Note absence of nuclear pseudostratification. (C) Tubal metaplasia with secretory cells, ciliated cells, clear cells, and intercalated cells (arrow). Tubal metaplasia, often seen in patients treated with ulipristal acetate (either 5 mg or 10 mg) for up to 3 months, is considered a reflection of the progesterone receptor antagonist (estrogenic) effect of ulipristal acetate. (Hematoxylin and eosin. (A) ×200; (B) ×200; (C) ×400)
A
C
B

Canadian Journal of P athology S11Supplement 2, Winter 2015
LATTA ET AL.
B
C
A
Figure 8. Vacuolization and apoptotic bodies in progesterone receptor modulator–associated endometrial change (PAEC). (A) Endometrial gland-lining cells display the simultaneous presence of subnuclear glycogen-containing vacuoles and a mitotic figure. These alterations are related to both progesterone receptor agonist and antagonist endometrial glandular effects of ulipristal acetate. (B) Example of PAEC in which the gland cells contain abortive cytoplasmic vacuolization together with mitoses. (Hematoxylin and eosin, ×300). (C) PAEC in a patient treated for 3 months with daily 10 mg UPA. Note the numerous apoptotic bodies in this field (H&E X 300).

Vascular ChangesWithin the stroma, vascular patterns include thick-walled arterioles (similar to those found in the basalis layer of normal cyclic endometrium or in benign endometrial polyps). A complex, chicken-wire-type capillary network, is also seen, as are ectatic blood vessels. None of these alterations are specific to PAEC. Typically, the stroma is devoid of decidualization as is seen with the oral contraceptive pill or other progestins. It is also devoid of vascular thrombosis and tissue breakdown, which would be characteristic of unopposed estrogen effects (Figures 9 and 10).
The histologic appearance of the study samples varied greatly, from normal physiological cycling endometria to identifiable benign pathologies to the novel combination of changes associated with PAEC. The wide spectrum of histologic changes indicated that the endometrial response to SPRMs might vary by type of agent, duration of use, and dosage, as well as by patient characteristics. As such, the panel recommended follow-up studies to fully define the natural history and presentation of PAEC.27
Figure 9. Large thick-walled blood vessel coursing through the endometrium in a patient with progesterone receptor modulator–associated endometrial change (PAEC) who completed a 3-month course of ulipristal acetate (5 mg daily) followed by a hysterectomy approximately 4 weeks later. The vessels are similar to those seen in benign endometrial polyps, and the appearance of PAEC here could be confused with that of a developing polyp, although the endometrial stroma shows no evidence of fibrosis. (Hematoxylin and eosin, ×25)
Figure 10. Vascular changes in progesterone receptor modulator–associated endometrial change. (A) Dividing and branching capillaries have produced a chicken-wire pattern. (B) Ectatic capillary with intact endothelial cell lining. (Hematoxylin and eosin, ×300)
BA
Supplement 2, Winter 2015S12 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY

Category Major classes Subclass Additional description
Adequacy AdequacyNo
No tissue; endocervix tissue only; technical issue
Yes
Primary diagnosis
BenignBenign endometrium Atrophy; inactive; proliferative;
secretory; menstrual; non-physiological; other (describe)
Hyperplasia
EH, simple, non-atypical
EH, complex, non-typical
EH, simple, atypical
EH, complex, atypical
Malignant neoplasmEndometrial adenocarcinoma Type, grade
Other malignant neoplasm Type
Observations Polyps
Absent
Present
Benign Atrophic Functional
Hyperplastic
Carcinomatous
Other observations
Non physiological epithelial changes: • secretion; mitoses; apoptotic changes
Extensive cysts present
Unusual vascular changes present: • chicken-wire capillaries; thick-walled vessels; ectatic vessels
Table 1. Rating scale used to assess endometrial biopsies in PEARL I and PEARL II. Consensus on primary diagnosis (adequate, benign, hyperplastic, malignant, neoplastic, polyp) was obtained when at least two of the three pathologists made the same diagnosis. In both PEARL I and PEARL II, over 90% of biopsy samples were adequately assessable for each treatment arm and at each time point28; EH = endometrial hyperplasia. Reproduced with permission.
Progesterone Receptor Modulator–Associated Endometrial Change in Clinical Trials of Ulipristal AcetateSystematic evaluations of endometrial changes in the PEARL I, PEARL II, and PEARL III studies have helped refine our understanding of the endometrial changes in PAEC, specifically those that manifest in women receiving UPA for ULs.20–22,28
PEARL I and PEARL IIIn both PEARL I and PEARL II, endometrial biopsies were performed at screening and at the completion of treatment at week 13.20,21 If no hysterectomy or endometrial ablation was performed, another biopsy was performed at week 38. The endometrial biopsy specimens were assessed by three independent gynecological pathologists who were blinded to the treatment, the timing of the biopsy, and each other’s assessments. Readings of the biopsy specimens were based on a rating scale of conventional descriptors of endometrial histology and additional descriptors of endometrial changes associated with PAEC (Tables 1 and 2). Representative images to assist in the differential diagnosis of PAEC are shown in Figures 11 to 14.
Canadian Journal of P athology S13Supplement 2, Winter 2015
LATTA ET AL.

Histologic feature PAEC Unopposed estrogen effectEndometrial hyperplasia (complex)
Gland architecture
Cystic dilatation Usually present PresentMay be absent, focal or widespread
Disordered architecture (as in DPP)
Focal Focal Diffuse
Complex architecture Absent Focal Diffuse
Budding into stroma Absent May be present Present
Papillation into lumen Absent May be present Present
Gland crowding Absent Focally present (DPP) Present
Gland-stroma ratio Unchanged Unchanged or focally increased (DPP)
Increased
Glandular epithelium
Cell type Flat cuboidal Tall columnar Tall columnar
Stratification of nuclei Absent Present Present
Mitoses Infrequent Usually frequent Frequent
Cytoplasmic vacuolation Common Uncommon Uncommon
Secretion in lumen Usually absent Usually absent May be present
Nuclear size Small, ovoid Small or medium Large, rounded
Nuclear shape Ovoid Ovoid or rounded Rounded
Nucleoli Usually absent Usually present Present
Nuclear atypia Absent Absent May be present or absent
Squamous metaplasia (morules)
Absent Occasional Frequent
Stroma
Stromal density Compact, moderately cellular Abundant, may be densely cellular or edematous
Usually densely cellular, may be sparse
Foam cells Absent Infrequent Present
Stromal breakdown Absent Present Present
Intravascular fibrin thrombi Absent Present Present
Table 2. Progesterone receptor-associated endometrial changes (PAEC) and mimics DPP (disordered proliferative pattern) and endometrial hyperplasia due to unopposed estrogenic stimulation.28 Reproduced with permission.
Supplement 2, Winter 2015S14 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY

Figure 11. Disordered proliferative pattern (DPP) endometrium. (A) Glands without proper (perpendicular to the surface) orientation vis-à-vis the surface epithelium (arrow); some are slightly dilated, the gland/stroma ratio is normal, and there are multiple ectatic capillaries in a compact cellular stroma. The gland-lining epithelium is cylindrical, with regular nuclear pseudostratification. (B) Another example of DPP. (C) High-magnification image of tall, cylindrical gland cells with regular, pencil-shaped, pseudostratified nuclei and numerous apoptotic bodies (arrow). Unlike in progesterone receptor modulator–associated endometrial change, the glands lack the simultaneous presence of cytoplasmic vacuoles and apoptotic bodies. (Hematoxylin and eosin. (A) ×150; (B) ×150; (C) ×400)
A
C
B
Canadian Journal of P athology S15Supplement 2, Winter 2015
LATTA ET AL.

Figure 12. Non-atypical (simple) hyperplasia (SHY). Unlike in progesterone receptor modulator–associated endometrial change, the gland-stroma ratio in SHY is in favour of the glands. (A) Sample showing several foci of stromal breakdown (arrows). Most cystically dilated cysts have a smooth nonragged contour (B) SHY with glandular crowding, resulting in a gland-stroma ratio in favour of the glands; the cylindrical lining epithelium contains regular nuclear pseudostratification devoid of atypia. (C) Detailed view of gland-lining epithelium. Many cells are ciliated with clear cytoplasm and rounded nuclei, reminiscent of tubal metaplasia. (Hematoxylin and eosin. (A) ×200; (B) ×250; (C) ×350)
Figure 13. Non-atypical (complex) hyperplasia (CHY). There is a back-to-back glandular crowding pattern and a gland-stroma ratio far in favour of the glands. (A) Sample showing that the gland cells lack cytological atypia. (B) Higher-magnification image of glandular epithelium, showing regular nuclear pseudostratification without cytological atypia. (Hematoxylin and eosin. (A) ×200; (B) ×300)
A
C
B
A B
Supplement 2, Winter 2015S16 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY

Figure 14. Atypical hyperplasia (AH). (A) Sample showing voluminous glands with intraluminal, papillary, and eosinophilic metaplasia. The stroma between glands is reduced to half compared to the greatest diameter of the glands. (B) High-magnification image of gland-lining epithelium with nuclear crowding, pleomorphism, and coarse chromatin giving rise to papillary structures made of large cells with eosinophilic cytoplasm and rounded atypical nuclei with coarse chromatin and macronucleoli. However, the nuclear-cytoplasmic ratio is normal in this cell population compared to the underlying gland-lining cells. (C) Detailed view of gland-lining cells with considerable nuclear atypia. Note rounding of pleomorphic nuclei, macronucleoli, and mitoses. Such cytological alterations are consistent with endometrioide intraepithelial neoplasia (EIN). (Hematoxylin and eosin. (A) ×200; (B) ×450; (C) ×400).
A
C
B
A total of 372 subjects (combining the 5 mg and 10 mg treatment groups) were administered UPA in PEARL I and PEARL II (Table 3). At screening, all but two patients had a diagnosis of benign endometrium, and two patients had a diagnosis of benign functional polyps. At week 13 (i.e., at the end of treatment), one patient in the total UPA treatment group was diagnosed with simple hyperplasia, and four patients were diagnosed with polyps: three benign and one with non-atypical hyperplasia (A. Ferenczy, unpublished data).28
None of the endometrial biopsy samples revealed malignant or premalignant lesions.20,21 Of the patients who had taken UPA and whose biopsy samples were adequate, one was diagnosed with a benign functional polyp, and none exhibited hyperplasia 6 months post treatment. The range of consensus primary diagnoses did not differ significantly between the UPA treatment groups and comparator groups. In contrast, one of 30 women in the placebo arm and one woman in the GnRH comparator group had atypical and non-atypical hyperplasia, respectively.
Canadian Journal of P athology S17Supplement 2, Winter 2015
LATTA ET AL.

Nonphysiological changes including PAECs were recorded both by consensus diagnosis and individual readings by all three pathologists, so that each biopsy sample received three readings. At the end of UPA therapy (week 13), the rates were ~30% and ~70% of cases by consensus diagnosis and individual pathologist readings, respectively.20,21,28 At 38 weeks (6 months after the end of
treatment), the frequency of nonphysiological appearances did not differ significantly from that at baseline (Figure 15).28 Similarly, the appearance of extensive cyst formation (the main diagnostic feature of PAEC) increased from screening to week 13 but returned to baseline level at week 38 in the UPA treatment group (Figure 16).
UPA (5 mg/10 mg) Placebo GnRH agonist
n EMP EH M n EMP EH M n EMP EH M
Baseline 3720.5%(2)
0.5%*†(2)
0 48 0 0 0 911.1%(1)
0 0
Week 13 377 1.2%(4)
0.3%*(1)
0 39 0 0 0 88 1.1%(1)
0 0
Week 38 241 0.4%(1)
0 0 30 0 3.3%† (1)
0 60 0 1.7%* (1)
0
Table 3. A summary of clinically significant endometrial morphologies from PEARL I and PEARL II as per consensus diagnosis. Adapted from Williams et al., 2012.28
n = number of adequate biopsies. All other diagnoses are expressed relative to the number of adequate biopsies. EMP = endometrial polyp; EH = endometrial hyperplasia; M = malignancy; GnRH = gonadotropin releasing hormone; *non-atypical (simple) hyperplasia; † atypical hyperplasia
30
20
10
0
70
80%
60
50
40
Baseline 13 weeks 38 weeks
8.4 8.0 7.3
17.7
7.1
67.6
8.4 8.0 7.34.4
14.417.7
7.1
13.611.4 11.2
67.669.7
* 3 assessments/biopsy
Placebo
5 mg
10 mg
GnRH
Adapted from Williams et al, Int J Gynecol Pathol 2012:316
Figure 15. Nonphysiological endometrial changes in PEARL I and PEARL II studies, by individual pathologist assessment (three assessments per biopsy). GnRH = gonadotropin-releasing hormone. Adapted from Williams et al.28
Supplement 2, Winter 2015S18 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY

Figure 16. Extensive cyst formation in PEARL I and PEARL II studies, by individual pathologist assessment. GnRH = gonadotropin-releasing hormone. Adapted from Williams et al.28
PEARL IIIEndometrial biopsy samples in PEARL III were taken during screening and after courses 1 and 4. For samples diagnosed as PAEC after course 4, an additional sample was taken 3 months later. Nonphysiological histologic features were reported by at least two of three independent pathologists for 11%, 26%, and 25% of samples at screening and 6 weeks after courses 1 and 4, respectively, suggesting that nonphysiological endometrial changes do not accumulate as a result of intermittent cycles of UPA administration
Fifteen women who were diagnosed with PAEC after the fourth UPA course had repeat biopsies 3 months later. By this time, 12 of the 15 women were free of nonphysiological features. Therefore, similar to the results in PEARL I and PEARL II, PAEC in PEARL III was rapidly reversible in most women after the end of UPA treatment, despite a longer and intermittent course of treatment.22
Endometrial ThicknessPrevious studies have documented endometrial thickening, as seen on ultrasound imaging, in women who received a SPRM such as mifepristone.29,30 The relationship between this finding and the uterine histologic changes discussed above has not been studied specifically in regard to UPA, but it has been suggested that endometrial thickening correlates with cystic dilatation in women treated with the SPRM telapristone acetate.2,31
In PEARL I and II, endometrial thickness was assessed by magnetic resonance imaging and ultrasound imaging, respectively. Thickness was measured at baseline and at week 13. An arbitrary thickness of 16 mm was chosen as being outside the normal range. In these studies, up to 5% of patients had an endometrial thickness of >16 mm at screening, and 8–15% of UPA-treated patients had an endometrial thickness of >16 mm at week 13.20,21 This is of relevance for clinicians, who may rely on imaging findings to guide their decisions concerning endometrial biopsies. The results of the PEARL studies clearly indicate that the imaging findings in women who are taking SPRMs do not correlate with findings of hyperplasia or malignancy. In some patients in PEARL III, endometrial thickening was seen at the end of UPA treatment but reversed 13 weeks following the end of treatment (Table 4).
Canadian Journal of P athology S19Supplement 2, Winter 2015
LATTA ET AL.

PEARL I PEARL II PEARL III
Placebo UPA 5 mg UPA 10 mg UPA 5 mg UPA 10 mgGnRH
agonistUPA 10 mg (course 1)
Screening 0 1.1% 2.3% 5.2% 5.0% 4.0% 1.5%
Week 13 (end of treatment)
2.1% 11.2% 8.0% 11.8% 15.3% 1.1% 9.1%
Week 17 – – – 5.6% 5.3% 5.7% –
Week 26 0 6.5% 7.3% 4.5% 2.8% 2.8% 0
Week 38 4.2% 4.8% 2.6% 6.0% 2.9% 2.9% –
Table 4. Endometrial thickness ›16 mm from PEARL I, II, and III.22, 26 UPA = ulipristal acetate; GnRH = gonadotropin releasing hormone.
Endometrial Histology n = 44
Normal and known benign changes 19
PAEC and PAEC-like changes 22
Hyperplasia 3*
Cancer 0
Endometrial Histology in Women Treated for Uterine Leiomyomata with Ulipristal Acetate: Postmarketing Experience at St. Michael’s HospitalBeginning in August 2013, with Canada’s approval of UPA, patients with ULs at St. Michael’s Hospital in Toronto who were candidates for preoperation therapy were offered UPA (5 mg daily) for 3 months as a medical therapy prior to surgical treatment. In contrast to the PEARL studies, this represented a real-world use of UPA, outside of a rigid clinical trial with distinct endpoints. Although patients were prescribed the drug for 3 months, not all of them completed a full cycle, which led to variability in the actual length of treatment. As well, the interval between the completion of UPA therapy and the time of surgery varied among patients, allowing some patients to have at least one menstrual cycle prior to surgery, while other patients had none. Baseline endometrial histology was available for only a few of these women.
Between November 2013 and October 2014, 60 surgical specimens were taken from patients who had taken UPA. The specimens included hysterectomy specimens (+/− fallopian tubes or ovaries) and myomectomy specimens. In the myomectomy specimens, endometrium was rarely available for histologic assessment. Only two endometrial biopsies were performed on patients who were actively treated with UPA, in contrast to the more comprehensive use of biopsy in the PEARL studies. Where present, endometrium was sampled extensively from these surgical specimens to look for evidence of PAEC and other endometrial changes. All specimens were examined by a
pathologist who was familiar with uterine histologic responses to UPA.Of the 60 surgical specimens received, 44 included endometrium, which was assessed for the presence of PAEC or other endometrial pathology (Table 5). Three specimens showed changes consistent with hyperplasia: two showed simple non-atypical hyperplasia, and one showed complex non-atypical hyperplasia. No malignancy or premalignant lesions (i.e., complex atypical hyperplasia or endometrial intraepithelial carcinoma) were identified. Of the three patients whose surgical specimens showed endometrial hyperplasia, none had undergone an endometrial biopsy prior to starting UPA. One patient who was diagnosed with simple hyperplasia had undergone a myomectomy 2 years earlier; the endometrium was described as benign. Of interest, the patient who showed complex endometrial architecture had a follow-up endometrial biopsy 3 months after her myomectomy; at this point, her endometrium appeared unremarkable and had none of the previously noted abnormalities.
Supplement 2, Winter 2015S20 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY
Table 5. Endometrial changes seen in UPA-treated women at St Michael’s Hospital. *Two cases showed simple hyperplasia without atypia; one showed complex architecture.

The novel endometrial changes seen in the patients at St. Michael’s Hospital were consistent with those described previously for PAEC. In particular, architectural alterations (including cystically dilated glands) were frequently seen, as was a combined secretory architecture that lacked the typical nuclear features or stromal changes of the postovulatory secretory phase. As previously reported, the combination of estrogenic and progestogenic features in the same specimen was seen, and vascular changes were also identified.27 However, evaluation of a hysterectomy specimen allowed a greater appreciation of the variety of changes and their heterogeneous distribution throughout the endometrium than would have been possible with an endometrial biopsy; for example, vascular changes might be prominent in one area but not in others. Similarly, some specimens showed areas typical of PAEC mixed with more normal-appearing endometrium. Finally, different characteristics of PAEC might be seen in different areas of the endometrium and not together. In contrast, nuclear changes (subnuclear vacuoles, apoptotic bodies) were not always as easy to identify, which possibly reflected differences in fixation between a large surgical specimen and a small biopsy specimen.
Including all cases that showed some characteristics of PAEC, 22 of 44 cases (50%) were described as PAEC or PAEC-like. In these 22 cases, there was a spectrum of PAEC-like changes in response to UPA therapy. This variability is important for pathologists to recognize, because as intermittent use of UPA becomes more common, they may be more likely to encounter surgical resection specimens – in addition to endometrial biopsy samples – from women previously receiving UPA therapy.
A Digital Reference Tool for Progesterone Receptor Modulator–Associated Endometrial ChangeThe novel changes in the endometrium with the use of UPA are a potential source of confusion to pathologists who are unaware of the drug and its effects; this may lead to erroneous diagnoses of hyperplasia or even of malignancy. To help pathologists become more familiar with UPA and its histologic effects, a digital reference tool that contains reference slide images of PAEC has been developed. The production of physical slide sets for distribution has numerous logistical challenges; a digital online reference tool is both more efficient and more easily accessible by pathologists across Canada.
At St. Michael’s Hospital, digital images of whole slides have been created, using digital scanning technology and digital pathology software. These images can be shared online with interested
pathologists. (See Appendix for detailed instructions on accessing this resource.) The digital slides can be viewed with freely available software. Navigation of a whole-slide image over a range of standard magnifications with this interactive viewing software emulates the examination of a slide on a light microscope offering a potentially important resource that complements the study of single-field images.32
At present, several representative images of PAEC have been posted, and there are plans to expand the reference tool to ensure adequate representation of PAEC and PAEC-like changes for viewing, study, and reference.
ConclusionUlipristal acetate (UPA), approved for the treatment of moderate-to-severe signs and symptoms of uterine leiomyomata (ULs) in adult women who are eligible for surgery, belongs to the class of selective progesterone receptor modulators (SPRMs). In randomized controlled clinical trials, 3 months of treatment with UPA was often associated with a constellation of nonphysiological endometrial features described as progesterone receptor modulator–associated endometrial change (PAEC) and characterized by architectural alterations, including extensive cyst formation, gland cell changes, and vascular changes, all found in the same sample.27 These changes were no longer evident in most patients 3 months after the discontinuation of UPA.20,21,28 With longer-term, intermittent UPA therapy, PAEC was also reversed after the cessation of treatment.22 In studies to date, UPA has not been associated with hyperplasia or malignancy.
In patients treated at St. Michael’s Hospital during a 6-month period after adoption of UPA, endometrial histology largely mirrored the clinical trial data despite considerable variability in the length of UPA treatment and in the post-UPA interval; PAEC was seen in 50% of samples, and no malignant or premalignant lesions were observed.Because a pathologist who is unfamiliar with PAEC may mistake the PAECs seen in UPA-treated patients for disordered proliferative pattern or non-atypical (simple) hyperplasia, St. Michael’s Hospital has started an educational initiative to digitize slides showing representative examples of PAEC. The digital description of PAEC is an educational and reference tool for facilitating the accurate diagnosis of this benign histologic condition, which is common in patients who are taking UPA or other SPRMs. Other means by which the pathologist can reach a correct interpretation of UPA-related endometrial histologic alterations include consultation with the clinician to inquire about prior UPA therapy if the patient’s treatment history has not been provided; consultation with a colleague with expertise in gynecological pathology; and review of the images and descriptions provided in this supplement.
Canadian Journal of P athology S21Supplement 2, Winter 2015
LATTA ET AL.

ForPrescribersofUlipristalAcetateWhen sending hysterectomy or endometrial biopsy specimens for histologic evaluation, it is important to inform the pathologist that the patient has been treated with ulipristal acetate.Regular assessment of endometrial thickness in patients undergoing UPA treatment with ulipristal acetate is not necessary if the increased thickness reverses after treatment is withdrawn and menstruation occurs.If endometrial thickening persists beyond 3 months after the end of treatment and the return of menstruation, the patient may need to be evaluated to exclude any underlying conditions.
AcknowledgementsThe authors gratefully acknowledge the unrestricted financial support of Actavis Canada in the development of this supplement. The authors give special thanks to Michelle Po, PhD, John Ashkenas, PhD, and Magdalena Partyka, all from SCRIPT, Toronto, Ontario, for writing, editorial, and logistic support.
References1. Chabbert-Buffet N, Pintiaux A, Bouchard P. The immninent dawn of SPRMs in
obstetrics and gynecology. Mol Cell Endocrinol 2012;358(2):232-43.2. Spitz IM. Clinical utility of progesterone receptor modulators and their effect on
the endometrium. Curr Opin Obstet Gynecol 2009;21(4):318-24.3. Bouchard P, Chabbert-Buffet N, Fauser BC. Selective progesterone receptor
modulators in reproductive medicine: pharmacology, clinical efficacy and safety. Fertil Steril 2011;96(5):1175-89.
4. Giangrande PH, Pollio G, McDonnell DP. Mapping and characterization of the functional domains responsible for the differential activity of the A and B isoforms of the human progesterone receptor. J Biol Chem 1997;272(52):32889-900.
5. Liu Z, Auboeuf D, Wong J, et al. Coactivator/corepressor ratios modulate PR-mediated transcription by the selective receptor modulator RU486. Proc Natl Acad Sci U S A 2002;99(12):7940-4.
6. Mulac-Jericevic B, Lydon JP, DeMayo FJ, Conneely OM. Defective mammary gland morphogenesis in mice lacking the progesterone receptor B isoform. Proc Natl Acad Sci U S A 2003;100(17):9744-9.
7. Conneely OM, Mulac-Jericevic B, Lydon JP, De Mayo FJ. Reproductive functions of the progesterone receptor isoforms: lessons from knock-out mice. Mol Cell Endocrinol 2001;179(1-2):97-103.
8. Bradley L. General Gynecology: The Requisites in Obstetrics and Gynecology: Elsevier Health Sciences, 2007.
9. Baird DD, Dunson DB, Hill MC, et al. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 2003;188(1):100-7.
10. Buttram VC, Jr., Reiter RC. Uterine leiomyomata: etiology, symptomatology, and management. Fertil Steril 1981;36(4):433-45.
11. Coyne KS, Margolis MK, Bradley LD, et al. Further validation of the uterine fibroid symptom and quality-of-life questionnaire. Value Health 2012;15(1):135-42.
12. Practice Committee of American Society for Reproductive Medicine in collaboration with Society of Reproductive S. Myomas and reproductive function. Fertil Steril 2008;90(5 Suppl):S125-30.
13. Fauconnier A, Chapron C, Babaki-Fard K, Dubuisson JB. Recurrence of leiomyomata after myomectomy. Hum Reprod Update 2000;6(6):595-602.
14. Spies JB, Bruno J, Czeyda-Pommersheim F, et al. Long-term outcome of uterine artery embolization of leiomyomata. Obstet Gynecol 2005;106(5 Pt 1):933-9.
15. Lefebvre G, Vilos G, Allaire C, et al. The management of uterine leiomyomas. J Obstet Gynaecol Can 2003;25(5):396-418; quiz 9-22.
16. Stovall TG, Ling FW, Henry LC, Woodruff MR. A randomized trial evaluating leuprolide acetate before hysterectomy as treatment for leiomyomas. Am J Obstet Gynecol 1991;164(6 Pt 1):1420-3; discussion 3-5.
17. Friedman AJ, Hoffman DI, Comite F, et al. Treatment of leiomyomata uteri with leuprolide acetate depot: a double-blind, placebo-controlled, multicenter study. The Leuprolide Study Group. Obstet Gynecol 1991;77(5):720-5.
18. Ishikawa H, Ishi K, Serna VA, et al. Progesterone is essential for maintenance and growth of uterine leiomyoma. Endocrinology 2010;151(6):2433-42.
19. Rosati P, Exacoustos C, Mancuso S. Longitudinal evaluation of uterine myoma growth during pregnancy. A sonographic study. J Ultrasound Med 1992;11(10):511-5.
20. Donnez J, Tatarchuk TF, Bouchard P, et al. Ulipristal acetate versus placebo for fibroid treatment before surgery. N Engl J Med 2012;366(5):409-20.
21. Donnez J, Tomaszewski J, Vazquez F, et al. Ulipristal acetate versus leuprolide acetate for uterine fibroids. N Engl J Med 2012;366(5):421-32.
22. Donnez J, Vazquez F, Tomaszewski J, et al. Long-term treatment of uterine fibroids with ulipristal acetate. Fertil Steril 2014;101(6):1565-73 e1-18.
23. Actavis Specialty Pharmaceuticals Co. Fibristal Product Monograph. 2013.24. Chabbert-Buffet N, Pintiaux-Kairis A, Bouchard P, Group VAS. Effects of the
progesterone receptor modulator VA2914 in a continuous low dose on the hypothalamic-pituitary-ovarian axis and endometrium in normal women: a prospective, randomized, placebo-controlled trial. J Clin Endocrinol Metab 2007;92(9):3582-9.
25. Murphy AA, Kettel LM, Morales AJ, et al. Endometrial effects of long-term low-dose administration of RU486. Fertil Steril 1995;63(4):761-6.
26. Williams AR, Critchley HO, Osei J, et al. The effects of the selective progesterone receptor modulator asoprisnil on the morphology of uterine tissues after 3 months treatment in patients with symptomatic uterine leiomyomata. Hum Reprod 2007;22(6):1696-704.
27. Mutter GL, Bergeron C, Deligdisch L, et al. The spectrum of endometrial pathology induced by progesterone receptor modulators. Mod Pathol 2008;21(5):591-8.
28. Williams AR, Bergeron C, Barlow DH, Ferenczy A. Endometrial morphology after treatment of uterine fibroids with the selective progesterone receptor modulator, ulipristal acetate. Int J Gynecol Pathol 2012;31(6):556-69.
29. Baird DT, Brown A, Critchley HO, et al. Effect of long-term treatment with low-dose mifepristone on the endometrium. Hum Reprod 2003;18(1):61-8.
30. Lakha F, Ho PC, Van der Spuy ZM, et al. A novel estrogen-free oral contraceptive pill for women: multicentre, double-blind, randomized controlled trial of mifepristone and progestogen-only pill (levonorgestrel). Hum Reprod 2007;22(9):2428-36.
31. Ioffe OB, Zaino RJ, Mutter GL. Endometrial changes from short-term therapy with CDB-4124, a selective progesterone receptor modulator. Mod Pathol 2009;22(3):450-9.
32. Ghaznavi F, Evans A, Madabhushi A, Feldman M. Digital imaging in pathology: whole-slide imaging and beyond. Annu Rev Pathol 2013;8:331-59.
Supplement 2, Winter 2015S22 Canadian Journal of P athology
SELECTIvE PROGESTEROnE RECEPTOR MODULATORS: CLInICAL ROLES AnD EFFECTS On EnDOMETRIAL HISTOLOGY

Appendix A. Access to Slides Demonstrating PAEC:
Slides may be viewed on your computer or iOS mobile device.
Step one: If you haven’t already done so, install ImageScope on your computer (Windows Only)
or Aperio ePathViewer on your mobile device (iOS Only)
• LinkforImageScope:http://www.leicabiosystems.com/pathology-imaging/
epathology/aperio-university/imagescope/
• LinkforAperioePathViewer:http://www.leicabiosystems.com/pathology-
imaging/epathology/aperio-university/epathviewer/
• Ifyoudonotwishorcannotdownloadthissoftware,youcanaccesstheslides
through the URL address: http://actavis.slidehosting.com/ on your browser
Step two: Access the slides using the following, Login username “pathuser” and password “paec”
(do not include quotation marks in username or password)
Access through the downloaded software
• ForImageScope:Gotohttp://actavis.slidehosting.com/andentertheabove
login credentials.
• ForAperioePathViewer:UsethesidebartoselectSlideHostingandchange
the URL to http://actavis.slidehosting.com/. Enter the above login credentials
Step three: Navigate software and launch digital slides of interest
• ForImageScope:navigatetodigitalslides.Openingslidesinyourbrowserwill
launch your ImageScope software for up to 20X viewing
• ForAperioePathViewer:navigatetodigitalslides.Openingslideswilllaunch
them in the app for up to 20X viewing
• Usingthehttp://actavis.slidehosting.com/website:Afterloginandpassword
prompt, open the slides through the eSlides icon. The website will allow views
of slides up to 20X viewing

Made possible through funding by Actavis Specialty Pharmaceuticals Co.