ordering radiology exams (and cases)nevadaosteopathic.org/attachments/article/33/snyder...
TRANSCRIPT

Ordering Radiology Exams (and cases)
5/4/18 NOMA LectureTravis Snyder, D.O.
Touro University NV Class of 2009
Assistant Adjunct Professor of Radiology and Neuroradiology Touro University NV
SimonMed Radiologist Las Vegas
Objectives
• Ordering X-ray (plus cases)
• Ordering CT (plus cases)
• Ordering US (plus cases)
• Ordering Nuclear Medicine (plus cases)
• Ordering MRI (plus cases)

X-ray

Chest X-rayIndications:
¨ Do a CXR if there is a new/abnormal physical exam finding in the chest (i.e., rales, rhonchi, wheezing, dullness to percussion, chest wall tenderness, tracheal deviation)
¨ New chest symptoms (i.e., cough, SOB, wheezing, chest pain, fever of unknown origin)
¨ Not Overutilized!!

Chest X-ray Positioning: Rotation Concerns
• One can identify malrotation by looking at the symmetry of the clavicles.
• Proper, upright positioning and proper inspiration are also important for a good X-ray.

CXR Technique
• CXR should be performed when the patient is “holding in” a full inhalation.• There should be at least 10 ribs visible (counting from top to bottom).

CXR Technique
• Underexposed film will cause the structures to appear too white.• Overexposed film will cause the blood vessels to appear too dark, which
prevents accurate assessment of the blood vessels.

Normal CXR

Who gets AP vs PA CXRs?
• AP –Ill patients, ICU
• PA- everyone else

Anterior-Posterior (AP) Films
• Although AP films are less accurate, sometimes they must be done in patients who are too ill or are too unstable to stand up. (ICU).
• AP films make heart size look artificially enlarged since it is more anterior and will cast a wider shadow.
• Heart Failure ‘cured’ when leave ICU!!!

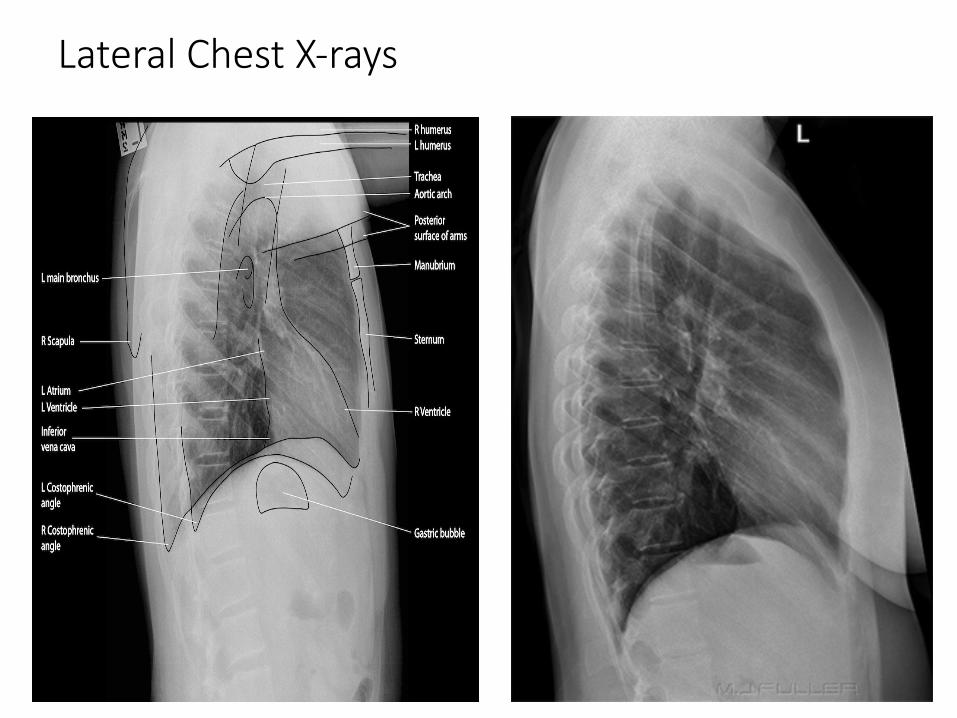
Lateral Chest X-rays

Lateral Chest X-Rays
• Lateral chest X-rays are useful for localizing pathology. Perform on all patients if possible (personal opinion). • Posterior vs anterior • “Pneumonia Spine Rule”: increased lucency in the inferior lung fields

Lateral Chest X-rays• Help determine whether a structure is more anterior or posterior.• Have a greater sensitivity for the detection of small pleural effusions• Can identify retrocardiac pneumonia hidden on PA view

Other chest Xray
• Rib Series• Decubitus, Expiratory, inlet views? Rarely used

Abdomen/Decubitus
•Decubitus view of the abdomen should be done with the patient on his or her left side. •Used to rule out free intraperitoneal air
(pneumoperitoneum) and air/fluid levels (obstruction).


CXR Terminology• Consolidation – any pathologic process that fills the alveoli with fluid, pus,
blood, tumor cells, or other substances• Results in lobar, diffuse, or multifocal ill-defined opacities
• Interstitial – involvement of the supporting tissue of the lung parenchyma • Results in fine or coarse reticular opacities or small nodules
• Nodule or mass – any space occupying lesion either solitary or multifocal• Atelectasis – collapse of part of lung due to decreased air in the alveoli

Pneumonia• Lobar pneumonia: causes a white density of the lobe due to greater density
of the lung.• +Silhouette sign (affected lobe obscures surrounding structures – i.e. the
heart border).• Lower lobe pneumonia obscures: diaphragm.• Right middle-lobe pneumonia obscures : right heart border.• Upper lobe infiltration will not pass the major fissure


Interstitial Infiltrates
• Fine, lacy appearance• Seen in diseases outside the airspace, but in the
interstitial membrane• Nonspecific, large differential• As the disorder worsens so does the fibrosis.
which leads to greater membrane thickening (reticular-nodular, honeycombing appearance)

Atelectasis
• Atelectasis: loss of lung volume secondary to lung collapse• Etiology: bronchial obstruction – inflammation, infection, foreign body,
cancer• Appearance: increased density and decreased volume of lung• +/- shift of trachea to ipsilateral side, elevation of ipsilateral hemidiaphragm• Linear and wedge shaped in appearance
• Don’t confuse with pneumonia:• Space occupying opacification with no volume loss • Consolidation appearance due to air space etiology
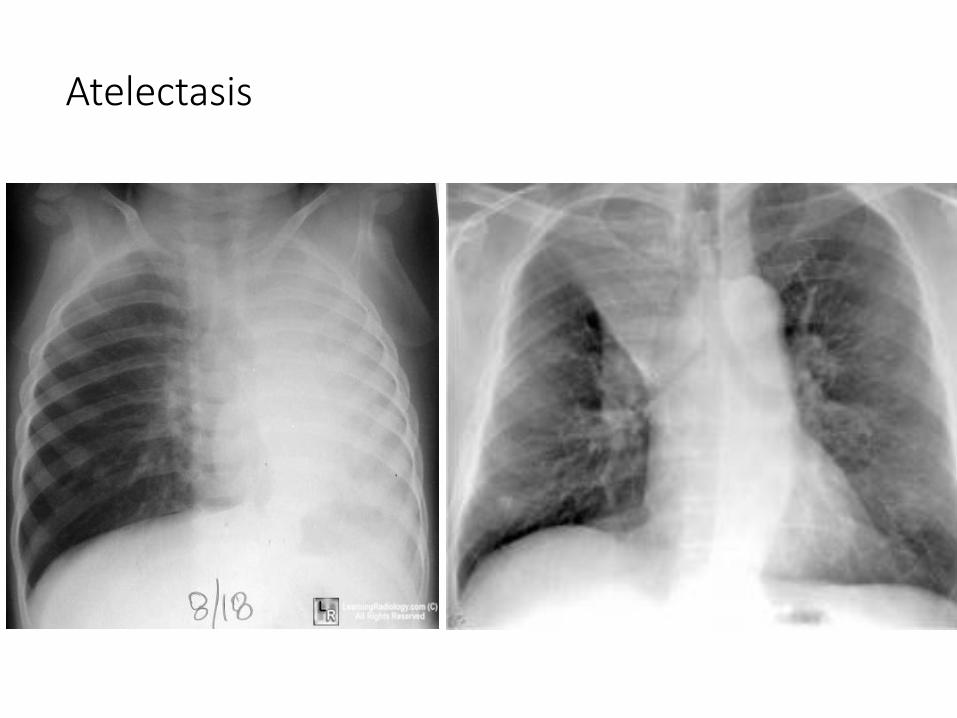
Atelectasis

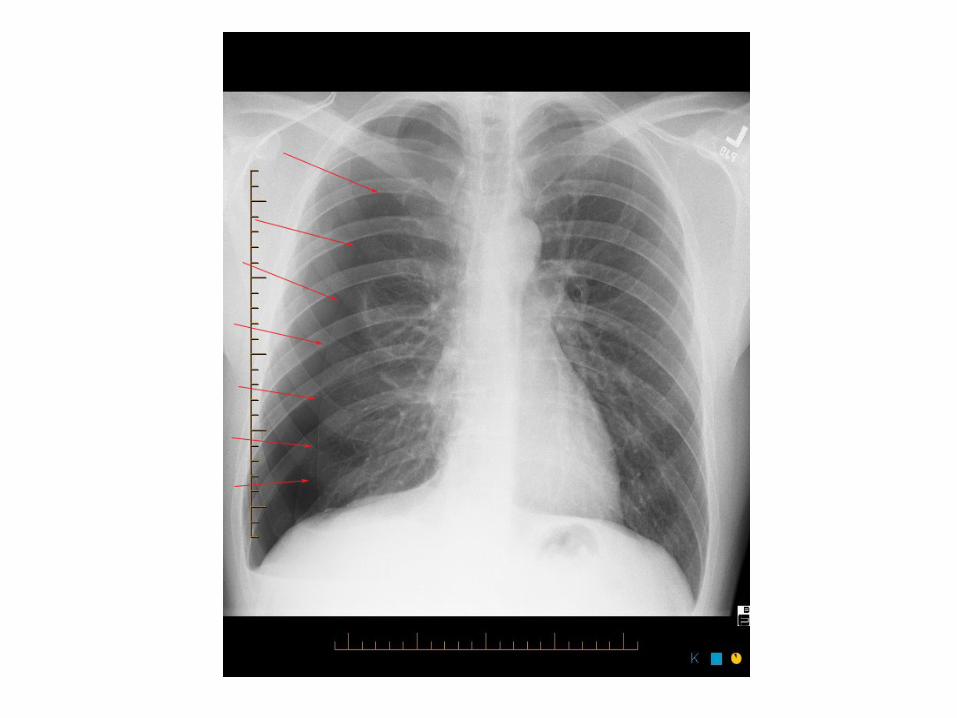
Pneumothorax
• Presence of air in the pleural space • Etiology: • Primary spontaneous• Secondary spontaneous: bullae, blebs, emphysema, abscess, radiation
necrosis• Trauma: pulmonary laceration• Iatrogenic - percutaneous biopsy, central line placement
• Appearance:• Decreased density, pleural edge (thin white line) with no lung markings
peripheral to the edge• Shift of trachea to ipsilateral side• Tension pneumothorax: shift of trachea to contralateral side

Tension Pneumothorax• Air enters pleural space and is trapped during expiration causing
increased intrathoracic pressure• Compromised venous filling of heart can lead to death• XR = shift of mediastinum to contralateral side• Treatment: emergent needle thoracostomy


COPD/EMPHYSEMA
• Hyperinflation of the lung.• Lung fields appear darker due to presence of
more air.• The trapped air “flattens” the diaphragm and the
heart appears elongated.• There is increased AP diameter (aka: Barrel chest)• May have bullae (large, air filled cavities that
create thin, white lines on CXR as the walls of the cavities press up against each other)

COPD/Emphysema


Congestive Heart Failure
• Other CXR findings: Cardiomegaly, effusions
• When fluid overload exists, blood vessels toward the lung apices become fuller (known as “pulmonary vascular congestion” or “cephalization” of flow).

CHF

Dramatic CHF (pulmonary edema)
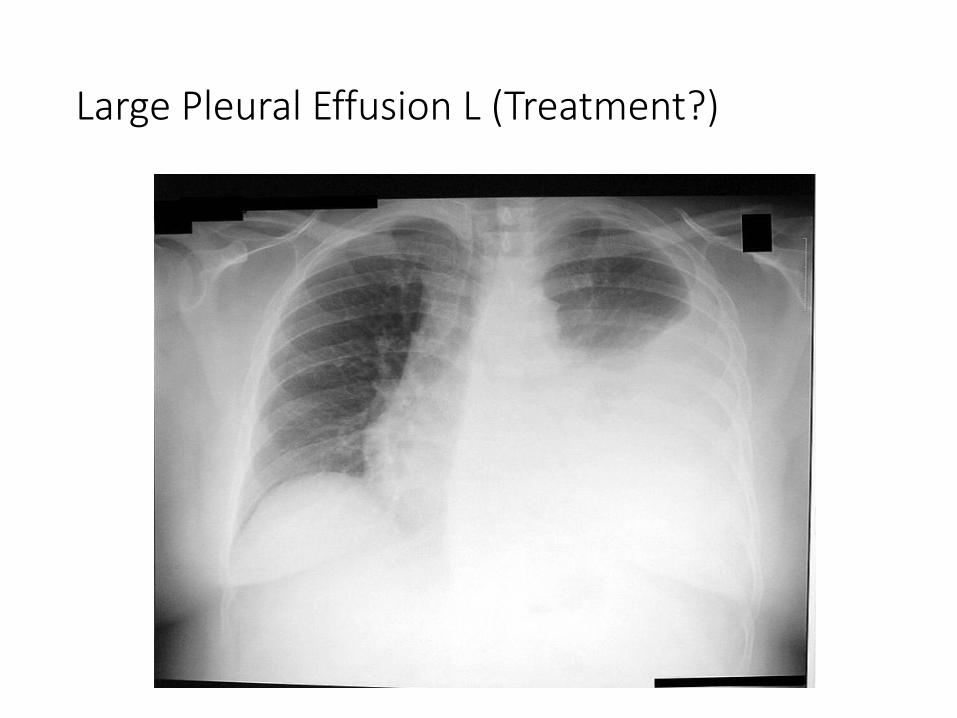
Large Pleural Effusion L (Treatment?)

What is this?

Pericardial Effusion

Aortic Dissection

Aortic Dissection

Other Chest X-ray Uses
• To ensure the appropriate position of central venous lines, endotracheal and chest tubes.
-Proper position of the tip of an endotracheal tube is 5 cm above the carina (+/- 2 cm).
-The tip of central venous lines should be at atrial caval junction

Lines


Pneumoperitoneum

Very Large Pneumoperitoneum


What Utility Do Skull X-rays Have?
• Assess for foreign body before MRI
• Gross Sinusitis (just get CT)
• Nasal Bone Fx

Abdominal X-rays
• Generally provide much less information than CTs.• Good for detecting abdominal obstructions (ileus or volvulus).• Not reliable for mass lesions, polyps, cancer, ascites, or inflammatory
bowel disease.• Can detect renal stones, but not hydronephrosis• (Noncontrast CT is best for Renal stones)

Abdomen

SBO or Ileus•Air fluid levels alone = ileus, enteritis
•Air fluid levels with dilated bowel loops = SBO especially with transition point
• If really concerned about obstruction, do CT
•SBO most common cause prev sx
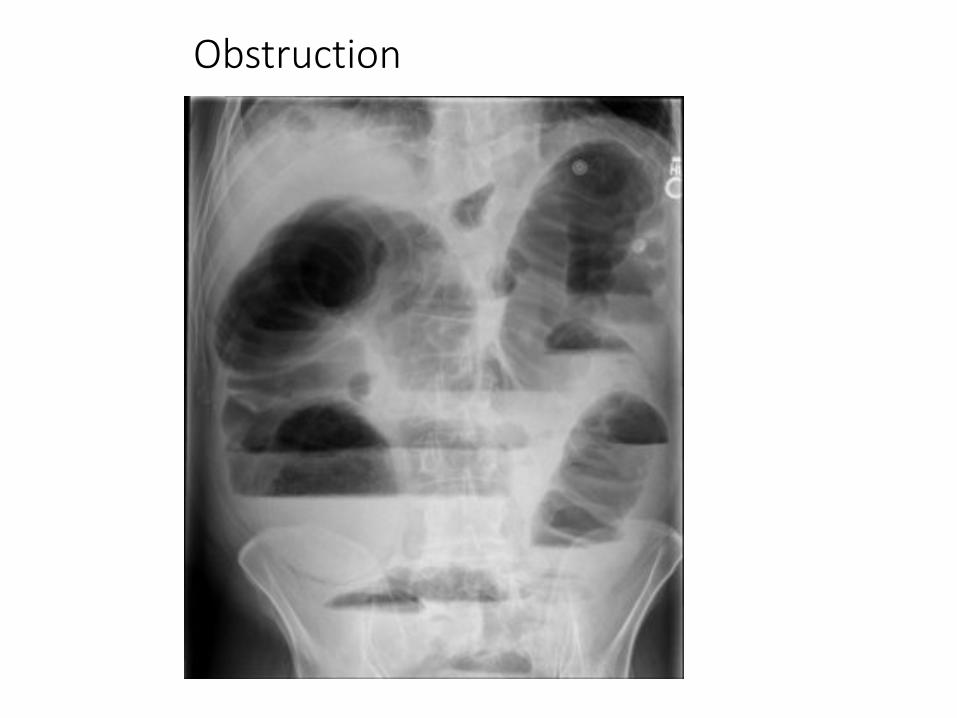
Obstruction

Diagnosis?
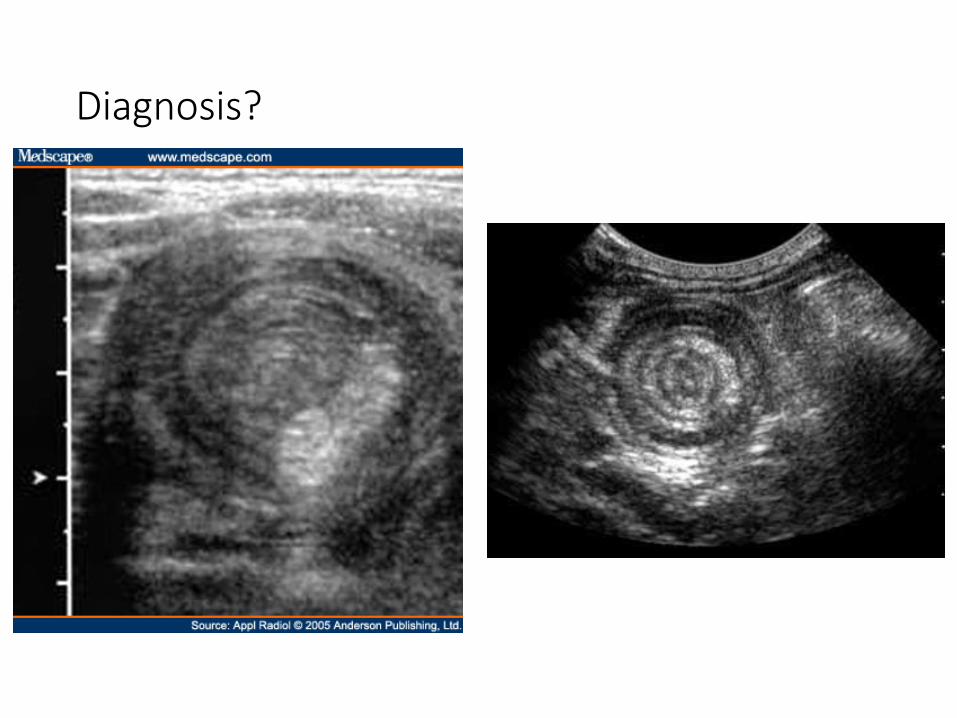
Diagnosis?


Intussusception • Bloody stool (“currant jelly”), pain, young kids• Air barium reduction is treatment• X-ray is diagnosis of choice, also US


Barium Studies• A good study to begin esophageal evaluations
-Can detect rings, webs, or Zenkers diverticulum, ulcers
Barium Enema, UGI, Esophogram, Barium Swallow(Gastrograffin if suspect perf)

Other xray indications
• Extremity Xrays• Get 3 views!!
• Spine Xrays• Flexion/Extension may be of benefit • Oblique views avail (pars in lumbar spine kids)• Open mouth dens views

Osteomyelitis
•Surrounding soft tissue swelling and loss of blurring of normal fat planes.•Periosteal reaction•Sinus tract?•Effusion may be seen• Loss of mineralization and then erosion (50% loss to
see it!)
•X-ray may be negative and if so, MRI is modality of choice (Low T1)


What do you see?

Rheumatoid ulnar deviation

Is there a problem here?

Radial fx MC adults, supracondylar fx MC kids

FOOSH, normal scaphoid, but persistent pain. What do you do next?

4-6 week FU X-ray to exclude fracture, some X-rays neg

Normal Suprapatellar Effusion
(MRI indicated?)

DEXA – Fracture risk, osteoporosis, osteopenia

DEXA interpretation
• 1. The International Society for Clinical Densitometry recommends categorizing the patient according to the lowest T-score from the total L-spine, total hip, and femoral neck, utilizing the following World Health Organization criteria:
Normal range: T-score of -1.0 or aboveOsteopenia: T-score of less than -1.0 but greater than -2.5Osteoporosis: T-score of -2.5 or below
2. Depending on the above results, clinical management may include calcium and vitamin D supplementation, weight-bearing exercise, and drug therapy, including bisphosphonates, Evista or hormonal replacement. Also consider followup DEXA scan in 1-2 years if clinically indicated. Preferably this should be done at the same facility. More frequent scanning may be required in the setting ofdrug-induced bone loss or metabolic bone disease.

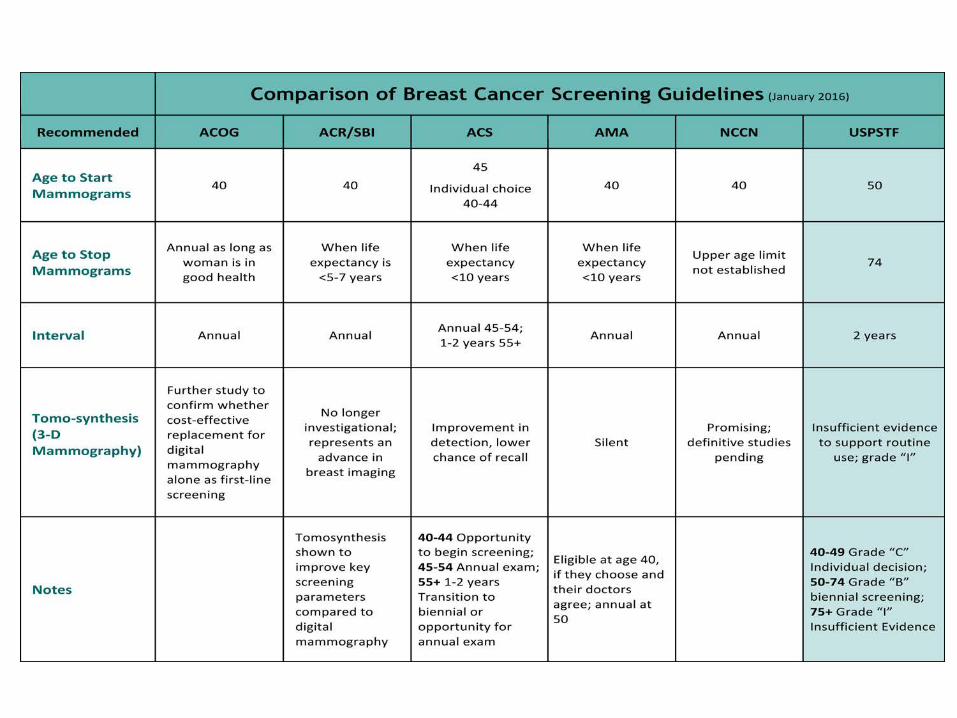
Mammography

CT

Computed Tomography
•CT number = Hounsfield unit•Air = -1024 HU•Water = 0 HU•Bone = +3000 to 4000 HU

CT Windows
Soft Tissue Lung Window Bone

Indications for CT
• Renal Stones (without contrast or IVP)• Fractures: without ER setting• Pulmonary nodules: without contrast (lung cancers w/ [lymphadenopathy])• Hernia (without, unless concern for strangulation) (US often better) • Hepatic lesions (triphasic, non-contrast arterial/delayed)• Adrenal protocol (longer triphasic)• Organ tumors/abscesses: with contrast• Appendicitis: with contrast• Bowel Obstruction: with contrast• Dissection/Pulmonary embolism: with contrast• CT neck – with contrast always• Any abdominal pain – with contrast always (also oral contrast)
• Other: Enterography, Virtual Colonoscopy
CT Brain Indications
• Trauma: CT without• Stroke: CT without, if negative and high suspicion then MRI• NPH, hydrocephalus: CT without
• CT with????
• CTA or MRA equal in efficacy for aneurysms, dissection, vascular issues
• Mets: MRI with• Infection: MRI with• Congenital: MRI without (midline anomalies, heterotopia, seizures?) • Headache: clinical discretion (MRI) almost all negative

Spine?
• Lower back pain? Degenerative disease? (MRI)
• CT: Trouble shooting osteophytes, pre-surgical planning, can’t have MRI
• Can assess hardware metallic artifact issues.

CT
MRICheatsheets!

CT Chest
• Provides greater detail than chest x-ray.
• Indications:- Assess abnormal CXR findings-Symptomatic patients with a normal CXR-Detecting metastatic lesions, solitary nodules, bullae, bronchiectasis
and diffuse parenchymal disease-To determine the type of lung biopsy required and site of biopsy
Generally without contrast unless cancer (not nodule), embolism, dissection
High resolution CT (over ordered?) – for interstitial lung disease

Large spiculated nodule: cancer
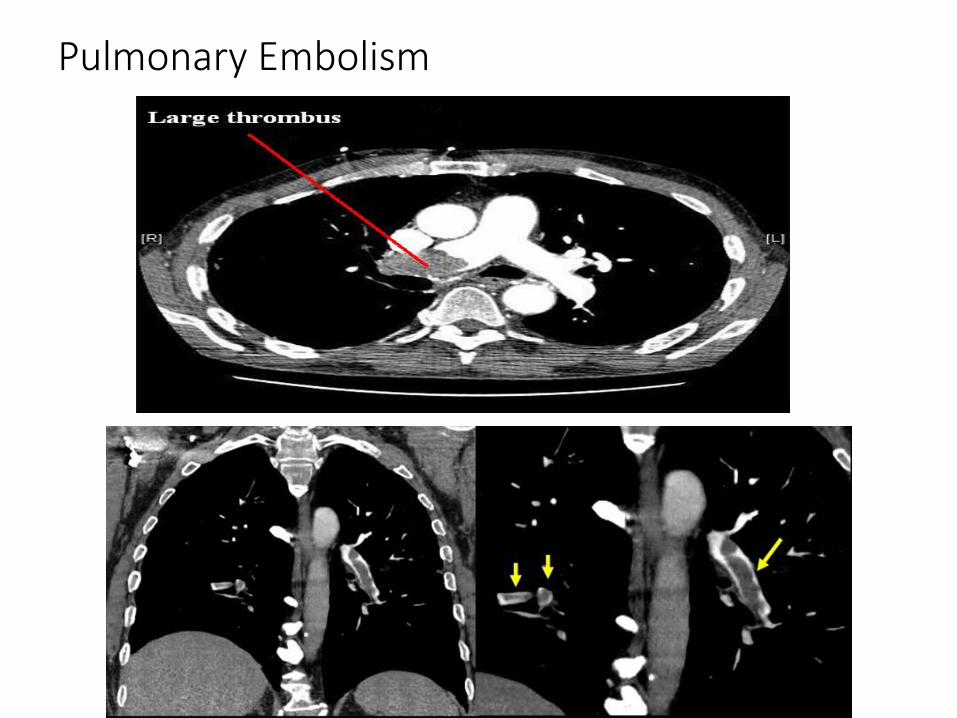
Pulmonary Embolism

This pt. has chest pain with radiation to the back Diagnosis?

Ship yard worker, Increased SOB over the last 3 months

Pleural plaques, Asbestosis exposure not malignant

Society of Thoracic Radiology recommendations for follow up of pulmonary nodules:
• Solitary nodule size: <6 mm low risk patients: no follow-up needed high risk patients: optional CT at 12 months• Solitary nodule size: 6-8 mm low risk patients: follow-up at 6-12
months, then consider further follow-up at 18-24 months high risk patients: initial follow-up CT at 6-12 months and then at 18-24 months if no change• Solitary nodule size: >8 mm either low or high risk patients consider
follow-up CT at 3 months, and/or CT-PET, and/or biopsy

Calcium Scoring


• CALCIUM SCORE/IMPLICATION/RISK OF
CORONARY ARTERY DISEASE
0: No identifiable plaque. Very low,
generally less than
5 percent.
1-10: Minimal identifiable plaque. Very
unlikely, less than 10
percent.
11-100: Definite, at least mild
atherosclerotic plaque. Mild or
minimal coronary narrowing is likely.
101-400: Definite, at least moderate
atherosclerotic plaque. Mild
coronary artery disease is highly likely,
significant narrowing is
possible.
401 or Higher: Extensive atherosclerotic
plaque. High likelihood of at least
one significant coronary narrowing.
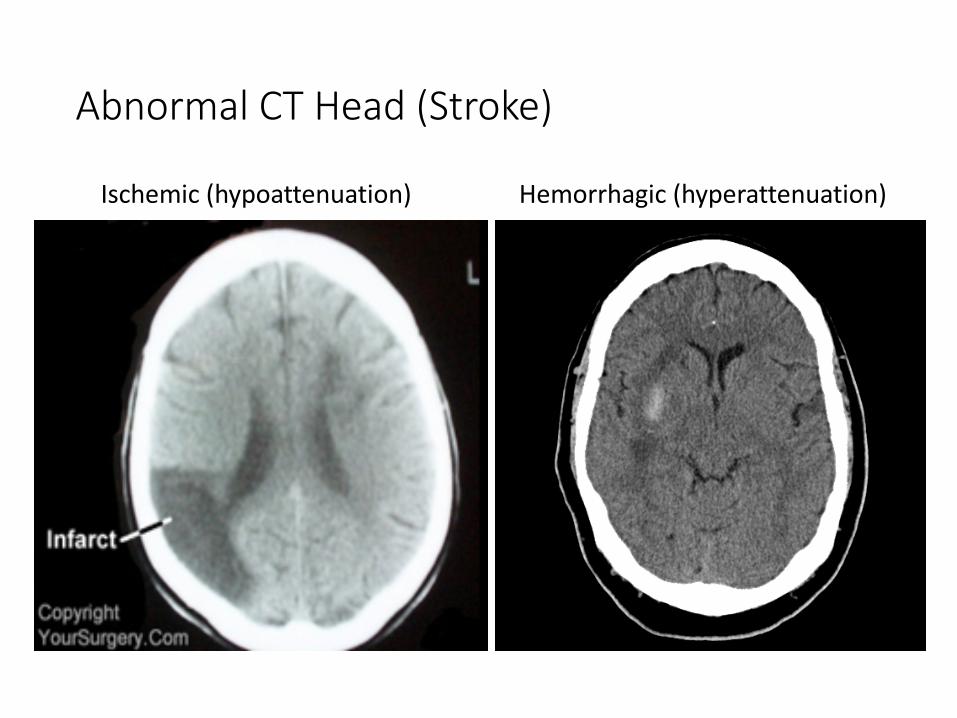
Abnormal CT Head (Stroke)
Ischemic (hypoattenuation) Hemorrhagic (hyperattenuation)

Subdural• Concave (crescent) appearance

Subarachnoid• Hyperattenuating material in subarachnoid space

What do you see?

What is the problem here? HTN bleed



Virtual Colonoscopy
• Provides a computer-simulated bi-dimensional or tri-dimensional image of the air-filled, distended colon.

Contrast Allergic Reaction
• Generally within 20 minutes: urticaria, facial edema, bronchospasm, dyspnea, cardiac symptoms. Rate as Mild/Moderate/Severe
• Treatment is corticosteriods, antihistamines; If severe = epinephrine

Myth
• “Seafood” or “iodine” allergy can receive contrast.
• A seafood allergy does not increase the risk of contrast reaction anymore than someone with any allergy. Asthma/allergic rhinitis is a small risk factor. (people with one allergy have greater risk of others)

If Patient Has Had a Prior Contrast Allergic Reaction
• Pre-medicate.
• If severe previous reaction, exam is likely contraindicated unless extreme circumstance.

Contrast Allergic Reaction Prevention
• Steroids• Methylprednisolone: one 32-mg tablet may be orally administered at 12 and
2 hours before the study• Prednisone: one 50-mg tablet may be orally administered 13 hours, 7 hours,
and 1 hour before the contrast-enhanced study.
• Serial Steroids + Antihistamine

Nephropathy Contrast Reaction
• Occurs in 1-2 % in pts with no risk factors• Risk is much higher in renal impaired pts, DM, age, current NSAIDs,
CHF: 30-100%• Creatinine peaks 3-7 days after IV contrast administration • High risk for acute kidney injury in patients with GFR < 30