oral workshop
TRANSCRIPT

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 1/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 2/99
60 yr old male, mass buccal mucosa

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 3/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 4/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 5/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 6/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 7/99
Differential diagnosis?????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 8/99
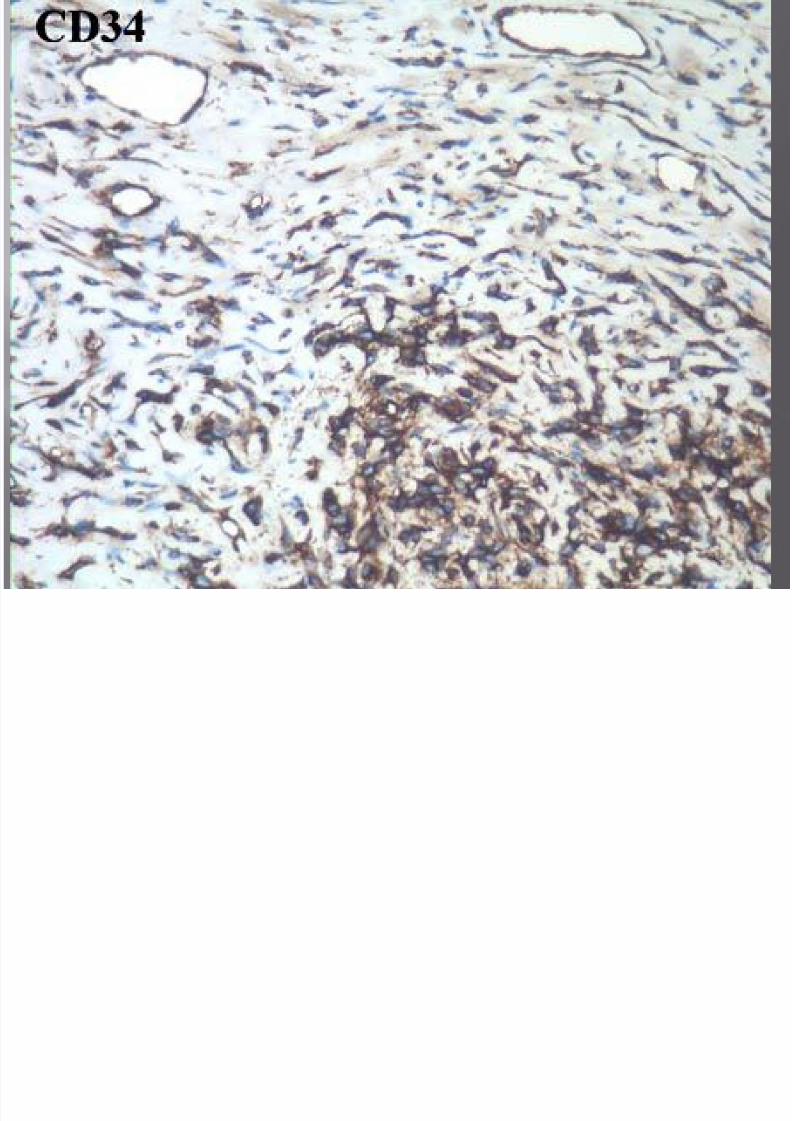
Solitary fibrous tumor
Leiomyoma
Fibroma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 9/99
Recent explosion of reports citing SFT at unrecognizedsites.
Region of head and neck is one of the more commonsites.
SFT is not very aggressive in head and neck sites. In the head and neck buccal mucosa is the commonest
site.
Fibroblast like cells with patternless pattern, thin strip-
like bands of collagen and gaping vessels. IHC; CD34, bcl2+ Fibroma CD34-, Leiomyoma ; actin/desmin+
CD34-

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 10/99
40 year female ulcer lip

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 11/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 12/99
8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 13/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 14/99
Differential diagnosis????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 15/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 16/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 17/99
Well differentiated squamous cell carcinoma
Granular cell tumor

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 18/99
Benign neoplasms very rarely malignant
Female prdilection.
Can occur in a variety of sites in head and neck
region.Tongue is the commonest site. H/P; border of lesion ; ill defined with tumor
infiltrating in the stroma.
When the tumor arises in the muscle , granular
cells can be difficult to recognize Cytology; bland, distinct cytoplasmic borders,
fine granulations

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 19/99
Closely associated with nerves.
N.B. If a graular cell tumor is present, adiagnosis of squamous cell carcinoma should
not be rendered; no matter how closely thesquamous proliferation resembles squamouscell carcinoma.
IHC; S100+, inhibin+
CD68+, Alpha 1 antitrypsin +

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 20/99
66 yr old man treated with radiation forcarcinoma oral cavity. Polypoid noduleradiation site.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 21/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 22/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 23/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 24/99
Differential diagnosis?????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 25/99
Reactive fibroblastic proliferation
Pseudosarcomatous reaction to an associatedcarcinoma or radiation
True sarcoma Sarcomatoid carcinoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 26/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 27/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 28/99
Rare, diagnostically challenging esp in head andneck region.
May show prominent or exclusively spindle cellcomponent.
Cellular atypia is highly variable. IHC may help but not always relaible. Cytokeratin 50 -75% but absence of CK +vty does
not excludes sarcomatoid SCC
CK +vty does not confirm presence of sarcomatoidSCC. p63 is very useful as its expression is not
encoutered in most sarcomas or benign spindle celllesions.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 29/99
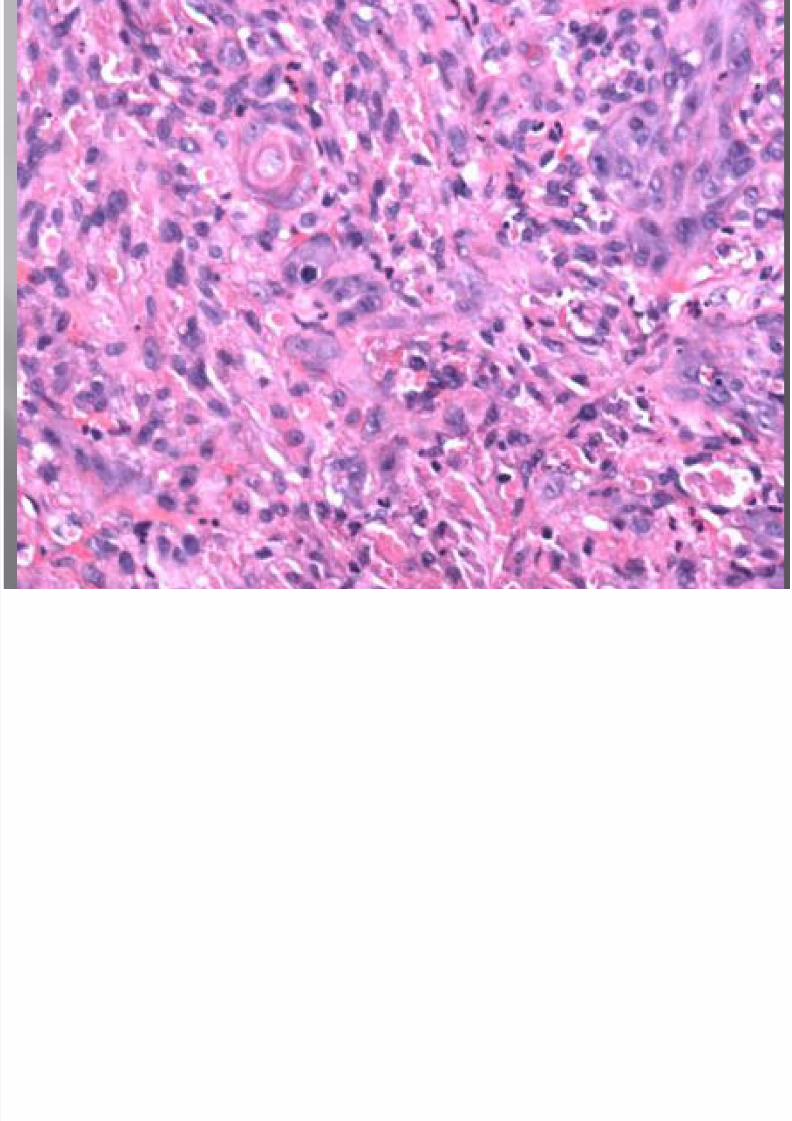
60 yr old male ,mandible resection for recurrentsquamous cell carcinoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 30/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 31/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 32/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 33/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 34/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 35/99
Differential diagnosis?????
8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 36/99
Silaometaplasia
Squamous cell carcinoma
Jxtaoral organ of chievitz

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 37/99
Vestigial epithelial remnant
Site; medial aspect of mandible along the angle.
May serve some mechanosensory function (
some suggest that it is a neuroendocrinereceptor)
Resemblance to squamous cell carcinoma but
lack cytologic atypia May undergo hyperplasia

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 38/99
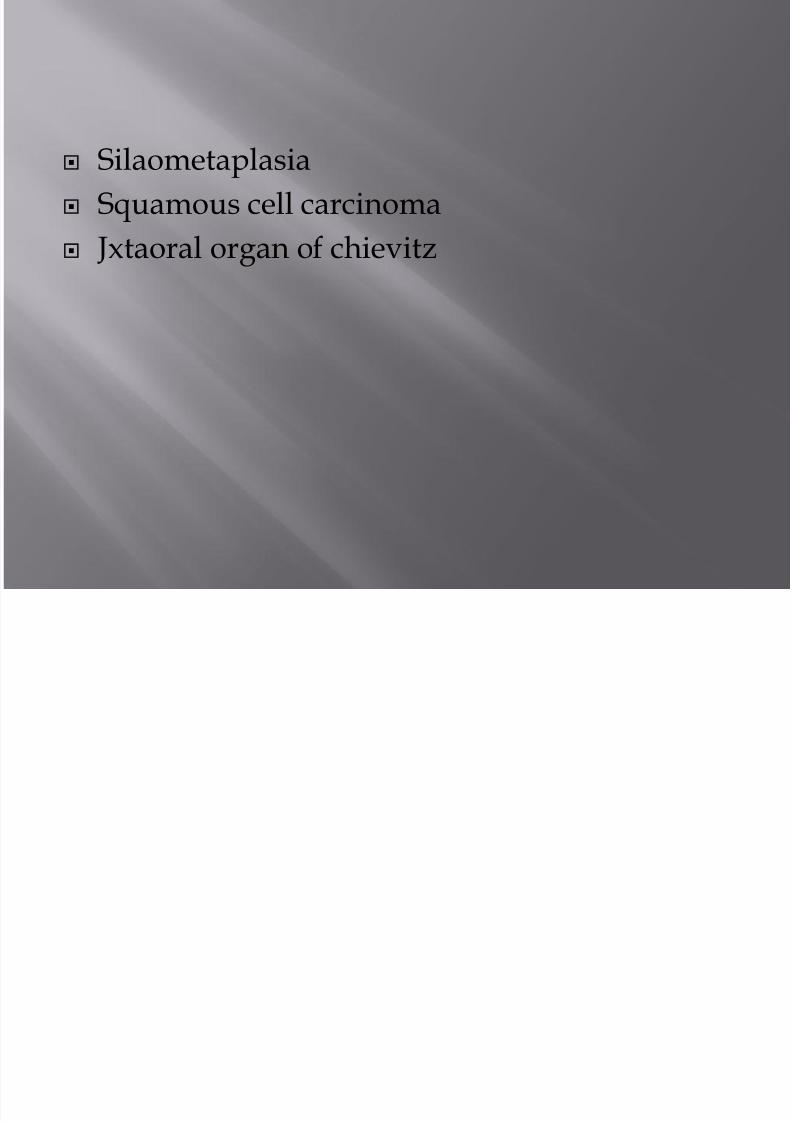
68 yr old female, large solid pale yellowswelling soft palate, tumor excision done

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 39/99
8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 40/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 41/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 42/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 43/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 44/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 45/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 46/99
Lipomatosis or fatty replacement
Lipomatous pleomorphic adenoma
Lipoadenoma of salivary glands
Hamartoma
Sialopliopma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 47/99
Slow growing painless mass
Mean age; 51 years. Male predominance
H/P; well circumscribed, may be encapsulated.
Focii of atrophic acini and ducts containedwithin lipomatous proliferation.
Ductal structures may be dilated with fibrosis
of the wall.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 48/99
40 yr old male , dome shaped nodule softpalate

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 49/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 50/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 51/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 52/99
8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 53/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 54/99
Differential diagnosis????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 55/99
Traumatic neuroma
Palisaded encapsulated neuroma
Spindle cell melanoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 56/99
Nodular neuroma consisting of schwan cells andnumerous axons with a delicate perineuralcapsule.
90% affect lips,face , oral cavity
Usually a solitary nodule May poorly or prtially encapsulate.
Retraction artefact common.
Vague palisading may be present.
Nuclear regimentation into verocay bodiesoccasionally seen.
Mitosis, atypia not seen.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 57/99
Palisaded encapsulated neuroma schwanoma
Peripheral delicate EMA positivity Completely surrounded by perineuralcapsule
Axons throught the lesion Axons when present are typicallyperipheral, subcapsular
GFAP- GFAP+
No organization into Antoni A & Bareas
common

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 58/99
Traumatic neuroma PEN
H/O trauma, surgery
Can have irregular margins Circumscribed
Numerous well formed small nervetwigs
Random proliferation of schwan cellsand axonsLack collagenous stroma
EMA+ perineurium surroundsindividual nerve twigs
EMA+ perineurium restricted toperphery of entire neuroma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 59/99
40 yr old man red patch hard palate

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 60/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 61/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 62/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 63/99
Differential diagnosis???

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 64/99
Kaposi sarcoma
Fibrosarcoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 65/99
Vascular lesion of low grade malignant potential
May originate from cell type capable ofundergoing lymphatic differentiation based on D240 staining.
Sites; skin , mucus membranes, visceral organs,lymph nodes.
IHC: FL1 (nuclear), VEGFR-3, HHV8,fVIII related
antigen,CD34,CD31 KS represents the most frequent oral malignancy
seen in association with HIV infection.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 66/99
50 year old male , mass hard palate

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 67/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 68/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 69/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 70/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 71/99
Differential diagnosis???
8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 72/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 73/99
Solitary fibrous tumor
Myoepithelioma
Inflammatory myofibroblastic tumor
Sarcomatoid carcinoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 74/99
Solitary fibrous tumor

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 75/99
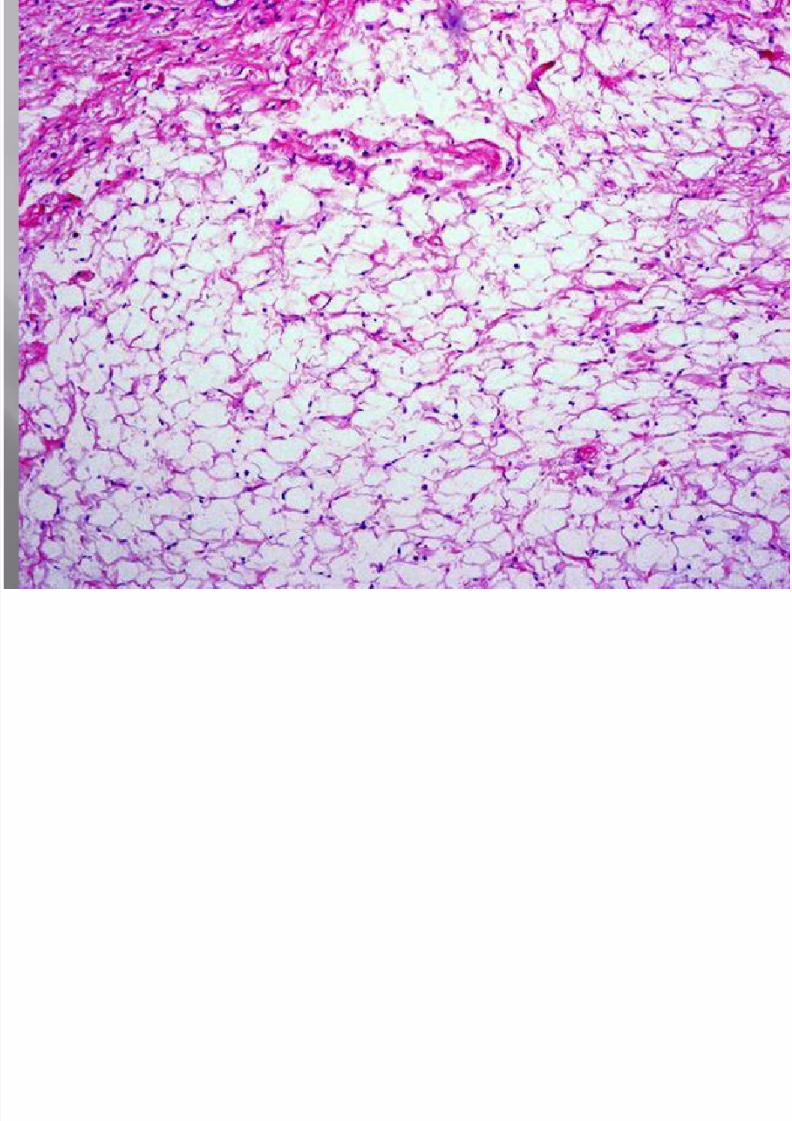
25 yr female painful swelling buccal aspect ofalveolar ridge. Xray shows radio opaque lesionsurrounded by radiolucent area connected witha tooth

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 76/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 77/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 78/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 79/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 80/99
Differential diagnosis????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 81/99
Cementoblastoma
Osteoblastoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 82/99
Def; a cementoblastoma is characterized by theformation of cementum like tissue in connectionwith the root of a tooth.
Benign tumor. Male to female ratio 2.1:1
Mostly in permanent dentition Symptomless or pain & swelling Also called true cementoma H/P; formation of sheets of cementum like tissue
cotaining a large number of basophilic reversallines and lack of mineralization at the periphery ofthe mass.
The diagnosis can not be made on the biopsyalone.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 83/99
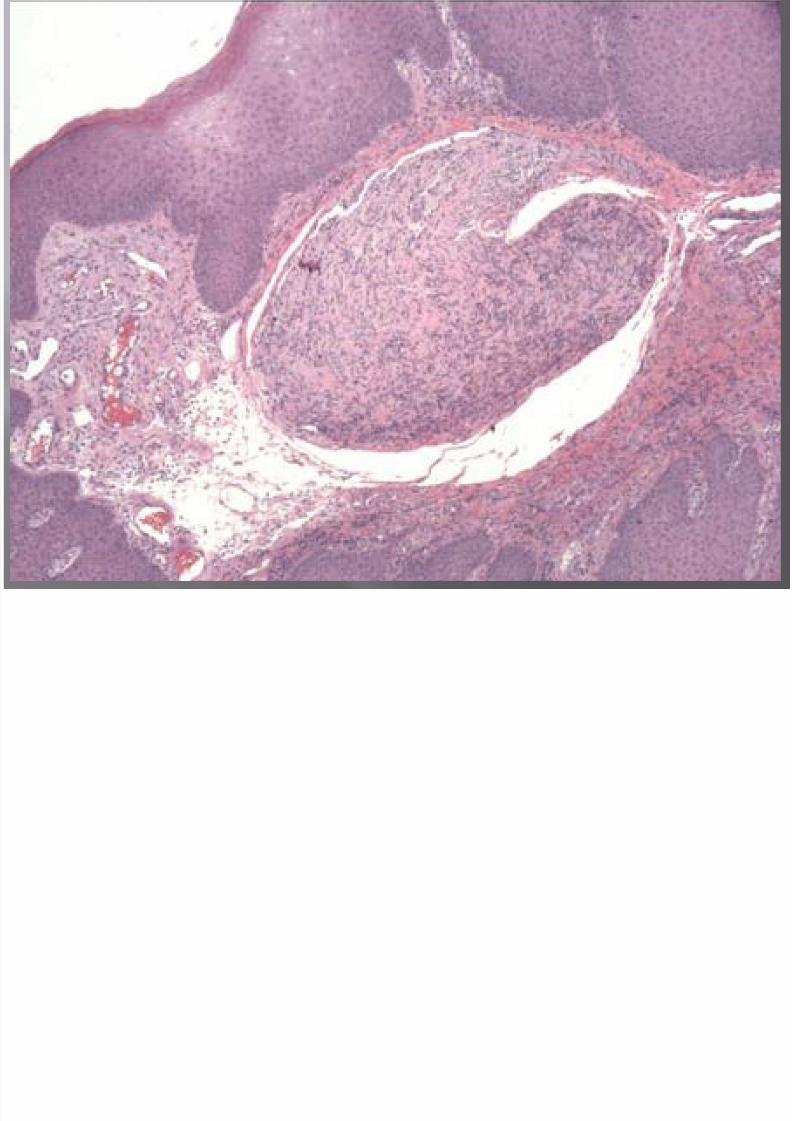
35 yr male, painless jaw swelling. Xray showsmottled mixed radio opaque/lucent lesionsuggestive of fibro osseous origin.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 84/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 85/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 86/99
Differential diagnosis????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 87/99
Desmoplastic ameloblastoma
Squamous odontogenic tumor
Odontogenic fibroma
Ameloblastic fibroma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 88/99
Ameloblastoma is the most common odontogenictumor of epithelial tissue origin.
Desmoplastic ameloblastoma is one of its variantswith specific clinical, imaging & histologicalfeatures.
Slowly growing, no gender predilection,wide agerange, locally invasive& high rate of recurrencewith incomplete removal.
Frequency slightly higher in Asian population
Show more aggressive behavior than other typesof ameloblastoma. Common location; maxilla
H/P

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 89/99
H/P;
1) Stromal desmoplsia (moderately cellular
fibrous connective tissue with abundantcollagen)
2)islands of different shapes in the epithelial
component. 3)peripheral layer of cuboidal cells
4)hypercellular central area composed ofspindle shaped or polygonal epithelial cells.
X ray; diffuse ill defined lesion

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 90/99
50 yr old female swelling of jaw, loosening ofteeth. Xray shows ill defined radiolucency

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 91/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 92/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 93/99

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 94/99
Differential diagnosis?????

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 95/99
Clear cell lesions of salivary glands Melanoma
Metastatic renal cell carcinoma
Clear cell odontogenic carcinoma

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 96/99
It is characterized by sheets and islands ofvacuolated and clear cells.
Strong female predilection. Older adults
On x ray ill defined radiolucency
H/P; A biphasic pattern often seen Fibrous stroma withislands of epithelial cells
having clear to faintly eosinophilic cytoplasm. Thecells have distint boundries and irregular dark
stainig nucleus. Cords of basaloid cells seen.
Ameloblastomatous islands

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 97/99
PAS +, Mucin -
IHC; CK 13,14,19,8,18, EMA+
Negative stains; vimentin, S100, desmin,SMA,HMB 45
Aggressive behavior, may metastsize.

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 98/99
Tumor histologic type and pattern Tumor size and location Tumor histologic grade Depth of invasion (not used for TNM staging) Pattern of invasion (noncohesive irregular cords, infiltrative single
cells, well defined blunt pushing borders, thick rounded invasivecords)
Tumor extension to adjacent structures Status of resection margins Vascular invasion Perineural invasion
Lymph nodes: for each level, number obtained, number involvedby tumor, size of nodal metastases, presence of extracapsularspread
Dysplasia

8/2/2019 Oral Workshop
http://slidepdf.com/reader/full/oral-workshop 99/99