oral and dental abnormalities in barber–say syndrome
TRANSCRIPT

CLINICAL REPORT
Oral and Dental Abnormalities in Barber–SaySyndromeFabiana Martins, Karem Lopez Ortega, Cybelle Hiraoka, Patricia Ricardo, and Marina Magalh~aes*Department of Oral Pathology, Special Care Dentistry Center, School of Dentistry, University of S~ao Paulo, S~ao Paulo, Brazil
Received 10 November 2008; Accepted 9 March 2009
A previously unreported case of Barber–Say syndrome is de-
scribedwith special attention to dentalmanifestations. A 7-year-
old female with multiple congenital anomalies such mammary
gland hypoplasia, hypertrichosis, ectropion, and redundant skin
was seen at the School ofDentistry of theUniversity of S~aoPaulo.Oral examination revealed macrostomia, broad alveolar ridges,
gingival fibromatosis, taurodontism, delayed tooth eruption,
and malocclusion. Dental treatment included gingivoplasty and
orthodontic treatment. � 2010 Wiley-Liss, Inc.
Key words: Barber–Say syndrome; taurodontism; ectropion;
hypertrichosis; macrostomia
INTRODUCTION
In 1982, Barber et al. described a 31/2-year-old girl with multiple
congenital anomalies such as macrostomia, ectropion, atrophic
skin, hypertrichosis, and growth retardation. The nameBarber–Saysyndrome (BSS, OMIM 209885) was used for the first time by
Martinez-Santana and coworkers in 1993 [Barber et al., 1982;
Martinez-Santana et al., 1993].
The etiology of this rare condition is as yet unclear. Dinulos and
Pagon [1999] suggested an X-linked or autosomal dominant
inheritance, while Martinez-Santana et al. [1993] associated the
syndrome with an autosomal recessive pattern.
Only nine cases have been reported in the scientific literature.
The clinical features of BSS include a ‘‘senile’’ appearance caused by
dry, loose, redundant skin particularly on the forehead, neck and
trunk, as well as in the antecubital and popliteal areas; hypoplasia of
the mammary glands and nipples; hypoplastic genitalia; ectropion;
atrophic skin; hypertrichosis; and growth retardation [Sod et al.,
1997; Mazzanti et al., 1998]. Histopathological analysis of the skin
shows atrophic epidermis with slight orthohyperkeratosis; thin,
reticular dermis; almost complete absence of elastic fibers and
hypocollagenosis [David et al., 1991; Tenea and Jacyk, 2006].
The differential diagnosis of BSS includes ablepharon–macrostomia syndrome (AMS, OMIM 20011). AMS and BBS are
both characterized by macrostomia, hypertelorism, or telecanthus;
abnormal nose and ears; aplasia or hypoplasia of nipples; and
redundancy of the skin. However AMS ablepharon is characterized
by no hair at birth, late development of sparse, thin hair, and total
absence of lanugo [Cesarino et al., 1988;Mazzanti et al., 1998;Tenea
and Jacyk, 2006]. According to Mazzanti et al. [1998] and to
Pellegrino et al. [1996], patients with AMS share many phenotypic
features with BSS patients, suggesting that these disorders may be
allelic. Pelegrinno et al. [1995] demonstrated a complex rearrange-
ment involving chromosome 18, in a BSS patient, and proposed
that the gene(s) for AMS and BSS may lie on chromosome 18.
The craniofacial characteristics of BSS include sparse eyebrows
and eyelashes, ocular hypertelorism or telecanthus, ectropion, low-
set, small andabnormal-shaped ears, bulbousnosewithhypoplastic
nasal alae, thin lips, and hirsutism [Barber et al., 1982]. To our
knowledge, only three studies have reported oral manifestations
such as macrostomia, malocclusion and prognathism [David et al.,
1991; Dinulos and Pagon, 1999], and delayed teeth eruption
[Mazzanti et al., 1998] in patients with BSS.
CLINICAL REPORT
A 7-year-old girl with unremarkable family history was diagnosed
with BSS at birth. She was born of a first-degree consanguineous
marriage after an uncomplicated first full-term pregnancy, to a
28-year-old mother. The patient was referred to the Special Care
Dentistry Center with a complaint of malocclusion and delayed
eruption of most permanent teeth. Physical examination showed
hypoplastic nipples and telangiectases on the chest, severe hyper-
trichosis affecting the back and neck, as well as lanugo covering
the patient’s entire body (Fig. 1). Other features included facial
dysmorphism, low hairline, hypertelorism, eyelid atrophy, sparse
*Correspondence to:
MarinaMagalh~aes, Universidade de S~ao Paulo, Faculdade deOdontologia,
Av. Prof. Lineu Prestes 2227, Departamento de Patologia Bucal, Cidade
Universit�aria-05508-900, S~aoPaulo, SP, Brazil. E-mail:[email protected]
Published online 9 September 2010 in Wiley Online Library
(wileyonlinelibrary.com)
DOI 10.1002/ajmg.a.32898
How to Cite this Article:Martins F, Ortega KL, Hiraoka C, Ricardo P,
Magalh~aes M. 2010. Oral and dental
abnormalities in Barber–Say syndrome.
Am J Med Genet Part A 152A:2569–2573.
� 2010 Wiley-Liss, Inc. 2569

eyelashes and eyebrows, telecanthus, bulbous nose, hypoplastic
nasal alae, and low-set ears of abnormal shape (Fig. 1).
At oral examination, anomalies of tooth number, tooth size, and
tooth structure were not noticed. The following teeth were present:
all permanent incisors, except for right superior lateral incisor,
two superior deciduous canines, two inferior permanent canines
partially erupted, all deciduousmolars teeth, and all first permanent
molars. Inmaxilla the canines, premolars, and secondmolars germs
were present. Inmandible the pre molars and secondmolars germs
were present.
Regarding tooth shapes anomalies, we observed abnormal cusps
pattern in molars, taurodontic molars, and shovel-shaped upper
incisors.
Dental history revealed delayed tooth eruption, with the first
deciduous tooth erupting at the age of 2. Oral examination revealed
macrostomia, thin upper lip, increased dental arch perimeter, as
well as a hypotonic tongue. The patient presented with anterior
open bite, infraoccludedmolars, overjet, broad alveolar ridges, and
tongue thrust. The crowns of the permanent teeth were partially
covered by gingiva. Less than one third of the clinical crowns of the
upper incisors were visible, and half of the clinical crowns of the
molars were visible (Fig. 2).
Radiographic examination had shown widening of the pulp
cavity of posterior permanent teeth and absence of constriction
in the cementum junction. The first lower permanent molars and
the lower deciduous molar presented an apical displacement of
the roots bifurcation, conferring a rectangular aspect to the pulp
cavities characterizing taurodontism [Constant and Grine, 2001].
Premature apical closure was seen in anterior teeth; the patient was
7 years old and this process should only begin at the age of 9 [Rafter,
2005]. Radiographic examination also revealed atypical incisors
with enhanced marginal ridges and a distinctive shovel-shaped
appearance (Fig. 3).
FIG. 1. Frontal (A) and lateral (B) viewof the patient’s face, forehead
hirsutism, low set and malformed ears, bulbous nose, eyebrows,
and macrostomia were observed. View (C) severe hypertricosis is
observed in back and neck. Thoracic region of the patient from the
front view (D)presenting redundant and thick skin, telangiectasis,
and absence of nipples.
FIG. 2. Intra-oral examination demonstrated macrostomia (A),
partial exposition of the crow of permanent teeth (B), and
morphological alteration of molars (C).
FIG. 3. Panoramic radiography showedmolar taurodontism (A) early
apical closure in permanent anterior teeth (B), shovel-shaped
incisors (C).
2570 AMERICAN JOURNAL OF MEDICAL GENETICS PART A
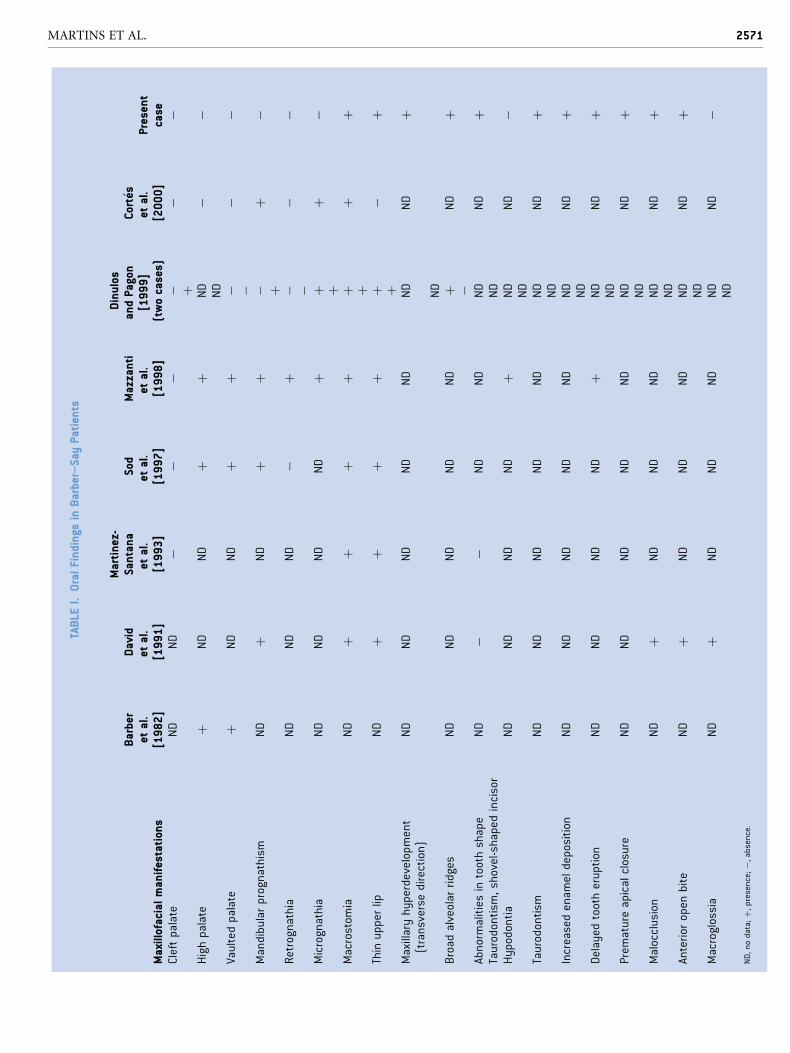
TABLE
I.OralFindings
inBarber–SayPatients
Maxillofacialmanifestations
Barber
etal.
[1982]
David
etal.
[1991]
Martinez-
Santana
etal.
[1993]
Sod
etal.
[1997]
Mazzanti
etal.
[1998]
Dinulos
andPagon
[1999]
(twocases)
Cort� es
etal.
[2000]
Present
case
Cleftpalate
ND
ND
��
��
��
þHighpalate
þND
ND
þþ
ND
��
ND
Vaultedpalate
þND
ND
þþ
��
��
Mandibularprognathism
ND
þND
þþ
�þ
�þ
Retrognathia
ND
ND
ND
�þ
��
��
Micrognathia
ND
ND
ND
ND
þþ
þ�
þMacrostom
iaND
þþ
þþ
þþ
þþ
Thinupperlip
ND
þþ
þþ
þ�
þþ
Maxillaryhyperdevelopment
(transverse
direction)
ND
ND
ND
ND
ND
ND
ND
þ
ND
Broad
alveolar
ridges
ND
ND
ND
ND
ND
þND
þ�
Abnormalitiesintoothshape
ND
��
ND
ND
ND
ND
þTaurodontism
,shovel-shapedincisor
ND
Hypodontia
ND
ND
ND
ND
þND
ND
�ND
Taurodontism
ND
ND
ND
ND
ND
ND
ND
þND
Increasedenam
eldeposition
ND
ND
ND
ND
ND
ND
ND
þND
Delayed
tootheruption
ND
ND
ND
ND
þND
ND
þND
Prem
atureapicalclosure
ND
ND
ND
ND
ND
ND
ND
þND
Malocclusion
ND
þND
ND
ND
ND
ND
þND
Anterior
open
bite
ND
þND
ND
ND
ND
ND
þND
Macroglossia
ND
þND
ND
ND
ND
ND
�ND
ND,nodata;þ,presence;�,absence.
MARTINS ET AL. 2571

Cephalometric analysis (Ricketts, McNamara, and Jarabak)
showed a skeletal open bite tendency, worsened by the buccal
inclination of the incisors, but still with a harmonious relationship
between the alveolar bone and the chin. Both the length and
inclination of the anterior cranial base were normal (69mm,
9 years old/5� counter-clockwise to The Frankfort Plane). The
maxilla showed normal length and a good position relative to the
cranial base. The mandible showed a slightly posterior position
relative to the cranial base. The body of the mandible was shorter
than normal (55mm), and the length and inclination of the ramus
of the mandible were within the normal range. The transverse
maxillary diameter was disproportionally wide in relation to the
mandibular arch. Anteroposterior dental examination showed that
the patient had Angle Class I malocclusion.
Generalized gingival fibromatosis, partially covering the crowns
of upper and lower anterior teeth, was observed. Gingivectomy
and gingivoplasty were performed, and histological examination
revealed that the mucosa was covered with keratinized stratified
squamous epithelium with rete ridges, and lamina propria com-
posed of fibrous connective tissue with collagen fibers organized in
thick, parallel, irregularly arranged bundles. Abundant collagen
deposition (detected by Masson’s trichrome stain) and absence of
elastic fibers (evidenced byWeigert’s stain using a staining solution
of resorcin and fuchsin) were noticed.
DISCUSSION
This is the first descriptive report of dental and occlusal features of a
patient with BSS (Table I). Themain features of BSS seem to derive
from a developmental abnormality of the skin and adnexa. The
ectodermal structures in our patient, including the teeth, were
impressively compromised, which prompted us to agree with
Martinez-Santana et al. [1993] and Cort�es et al. [2000], who
considered this disorder an ectodermal dysplasia (ED).
There aremore than 150 clinically distinct hereditary syndromes
in which an ED is present. Most syndromes are very rare and
manifest variable defects in morphogenesis of ectodermal struc-
tures, including hair, skin, nails, and teeth [Kere et al., 1996].
Our patient showed several skin and adnexa alterations as laxity
of the skin, absence of mammary glands, and sparse eyelashes and
eyebrows; otherwise, the patient did not have hypondontia or
oligodontia, which is frequent in EDs.
Finally severe hypertrichosis on the back was observed in our
patient and this aspect is not usual in ED.
The main complaint of the patient was the partially erupted
appearance of the permanent teeth. However, radiographic exami-
nation showed complete tooth eruption and premature apical
closure. Clinically, an overgrown gingiva was seen, covering two-
thirds of the clinical crowns. Gingivectomy and gingivoplasty were
performed for crown exposure, and resin was used to restore
vertical dimension in the molars. An orthodontic bracket was then
used to align upper incisors.
Some authors have reported a high vaulted palate in BSS [Sod
et al., 1997; Mazzanti et al., 1998]; our patient, however, presented
with a shallow palate with broad alveolar ridges. Although cepha-
lometric analysis showed a harmonious relationship between
the maxilla and the mandible, our patient exhibited severe facial
dysmorphism, including an anomalously large mouth and
biprotrusion.
As Bloch-Zupan [2007] stated, ‘‘teeth abnormalities are indeed
excellent dysmorphic markers, providing visible evidence, through
their unchanging mineralized state, of earlier developmental ab-
normalities, and giving warning signs that may provide sign-posts
in syndrome diagnosis.’’ In our opinion identification of dental
alterations can be a helpful tool to assess further diagnosis and
dental management of BBS patients.We describe, for the first time,
dental anomalies such as taurodontism, shovel-shaped incisors,
delayed eruption of deciduous dentition, and premature apical
closure.
Histopathological evaluation of the gingival tissue revealed
abundant collagen deposition and absence of elastic fibers. This
pattern has been previously reported in skin biopsies of patients
with BSS [David et al., 1991; Tenea and Jacyk, 2006], and never in
oral mucosa. In skin, it has been associated with laxity. We believe
that the lack of elastic fibers in gingival tissue can cause rigidity of
the gingiva, which consequently becomes an obstacle for completed
tooth eruption.
These developmental disturbancesmay be a helpful tool to assess
further diagnosis and dental management of BBS patients. For this
reason,we encourage authors to analyze these alterations inpatients
with BSS in order to better understand the oral implications of
the syndrome and manners to prevent impaction and dental
malocclusion.
REFERENCES
Barber N, Say B, Bell RF, Mervielle OC. 1982. Macrostomia, ectropion,atrophic skin, hypertrichosis and growth retardation. Syndr Ident 8:6–9.
Bloch-Zupan A. 2007. When neuropediatrics meets odontology. Neuro-pediatrics 38:57–58.
Cesarino EJ, Pinheiro M, Freire-Maia N, Meira-Silva MC. 1988.Lid agenesis-macrostomia-psychomotor retardation-forehead hyper-trichosis–A new syndrome? Am J Med Genet 31:299–304.
Constant DA, Grine FE. 2001. A review of taurodontism with new data onindigenous southern African populations. Arch Oral Biol 46:1021–1029.
Cort�es FM, Troncoso LA, Alliende AR, Curotto BL. 2000. Barber-Saysyndrome: Further delineation of the clinical spectrum. Genet Mol Biol23:265–267.
David A, Gordeeff A, Badoual J, Delaire J. 1991. Macrostomia, ectropion,atrophic skin, hypertrichosis: Another observation. Am J Med GenetSuppl 39:112–115.
Dinulos MB, Pagon RA. 1999. Autosomal dominant inheritance of Bar-ber–Say syndrome. Am J Med Genet 86:54–56.
Kere J, Srivastava AK, Montonen O, Zonana J, Thomas N, Ferguson B,Munoz F, Morgan D, Clarke A, Baybayan P, Chen EY, Ezer S, Saarialho-Kere U, de la Chapelle A, Schlessinger D. 1996. X-linked anhidrotic(hypohidrotic) ectodermal dysplasia is caused by mutation in a noveltransmembrane protein. Nat Genet 13:409–416.
Martinez Santana S, Alvarez FP, Frias JL, Mart�ınez-Fr�ıas ML. 1993.Hypertrichosis, atrophic skin, ectropion, macrostomia (Barber–Saysyndrome): Report of a new case. Am J Med Genet 47:20–23.
2572 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

Mazzanti L, Bergamaschi R, Neri I, Perri A, Patrizi A, Cacciari E, ForaboscoA. 1998. Barber–Say syndrome: Report of a new case. Am J Med Genet78:188–191.
Pellegrino JE, Schnur RE, Boghosian-Sell L, Strathdee G, Overhauser J,Spinner NB, Stump T, Grace K, Zackai EH. 1996. Ablepharon macro-stomia syndrome with associated cutis laxa: Possible localization to 18q.Hum Genet 97:532–536.
Rafter M. 2005. Apexification: A review. Dent Traumatol 21:1–8.
Sod R, Izbizky G, Cohen-Salama M. 1997. Macrostomia, hypertelorism,atrophic skin, severe hypertrichosis without ectropion: Milder form ofBarber–Say syndrome. Am J Med Genet 73:366–367.
Tenea D, Jacyk WK. 2006. What syndrome is this? Pediatr Dermatol23:183–184.
MARTINS ET AL. 2573