optimizing environmental hygiene: the key to c. difficile control philip c. carling, m.d. carney...
TRANSCRIPT
Optimizing Environmental Hygiene: The Key to C. Difficile Control
Philip C. Carling, M.D.
Carney Hospital and
Boston University School of MedicineMassachusetts CDI Preventative
Collaboration
June 24, 2010
Consultant – Ecolab, Steris, ASHES
Pending Patent License - [email protected]
Presentation Objectives
A. Understand current issues related to the roe of the environment in CDI transmission
B. Understand the basis for suboptimal healthcare environmental cleaning
C. Appreciate the complexity of making practice recommendations without modern evidenced based studies
Background: Epidemiology
Risk Factors
• Antimicrobial exposure
• Acquisition of C. difficile
• Advanced age
• Underlying illness
• Immunosuppression
• Tube feeds
• ? Gastric acid suppression
Main modifiable risk factors

How contaminated is the hospital environment?

Contaminated Surfaces
Bed Rails +++++++ + +++Bed Table ++++++ + Door Knobs ++ ++ +Doors +++ + Call Button +++ + ++Chair ++ + ++Tray Table +++ ++ Toilet Surface + ++++Sink Surface + + +++Bedpan Cleaner +
VRE MRSA C. difficile
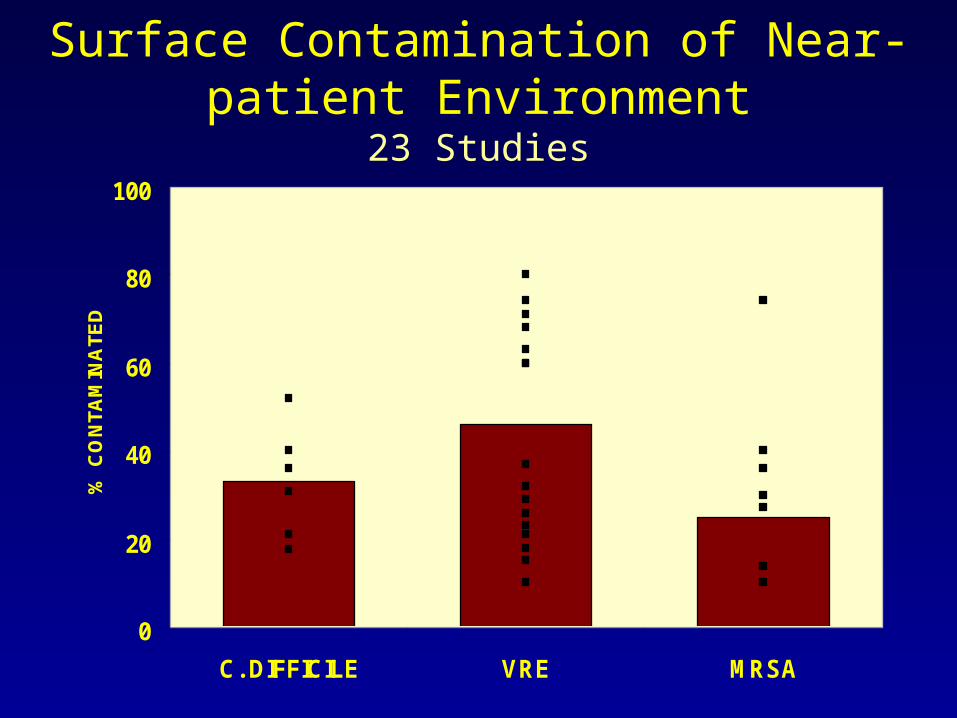
Surface Contamination of Near-patient Environment
23 Studies
0
20
40
60
80
100
C. DIFFICILE VRE MRSA
% C
ON
TAM
INA
TED
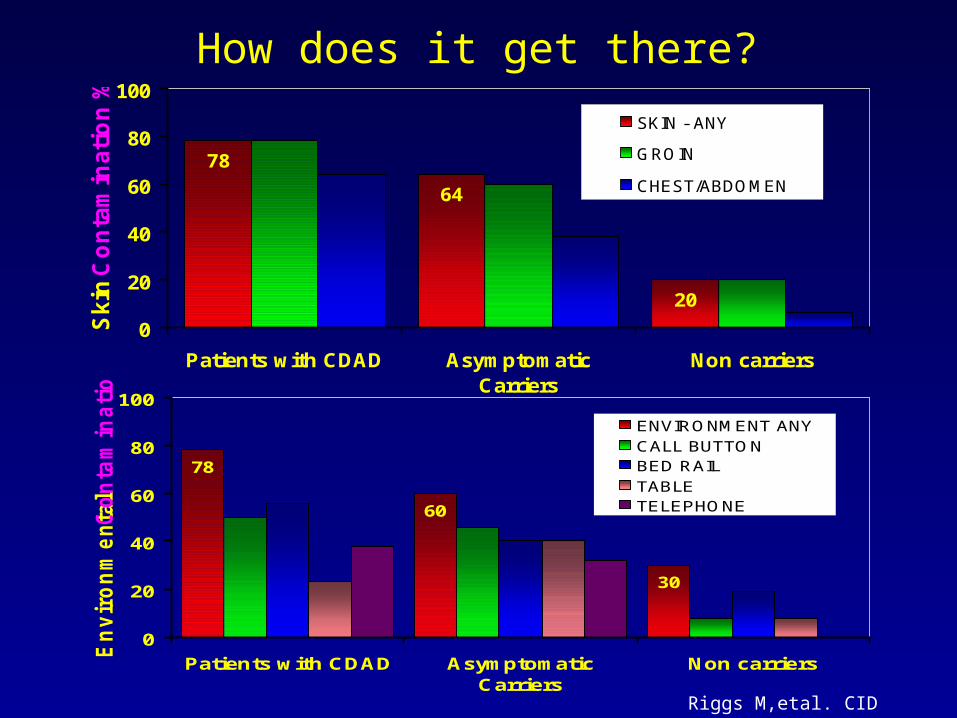
How does it get there?
78
60
30
0
20
40
60
80
100
Patients with CDAD AsymptomaticCarriers
Non carriers
En
vir
on
me
nta
l C
on
tam
ina
tio
n %
ENVIRONMENT ANY
CALL BUTTONBED RAIL
TABLETELEPHONE
78
64
20
0
20
40
60
80
100
Patients with CDAD AsymptomaticCarriers
Non carriers
Sk
in C
on
tam
ina
tio
n %
SKIN - ANY
GROIN
CHEST/ABDOMEN
Riggs M,etal. CID 2007;45:592

C. Difficile Environmental Contamination
0
3000
6000
PT HANDS NEARENVIRONMENT
DISTANTENVIRONMENT
HCW HANDS
PCR
COLO
NY C
OUN
TS/1
0cm
2
CDAD POS. PATIENT ROOMS
CDAD NEG. PATIENT ROOMS
Mutters R, etal. J Hosp Infect. 2009; 71: 43-48

Can C. diff be transmitted from the environment to patients?
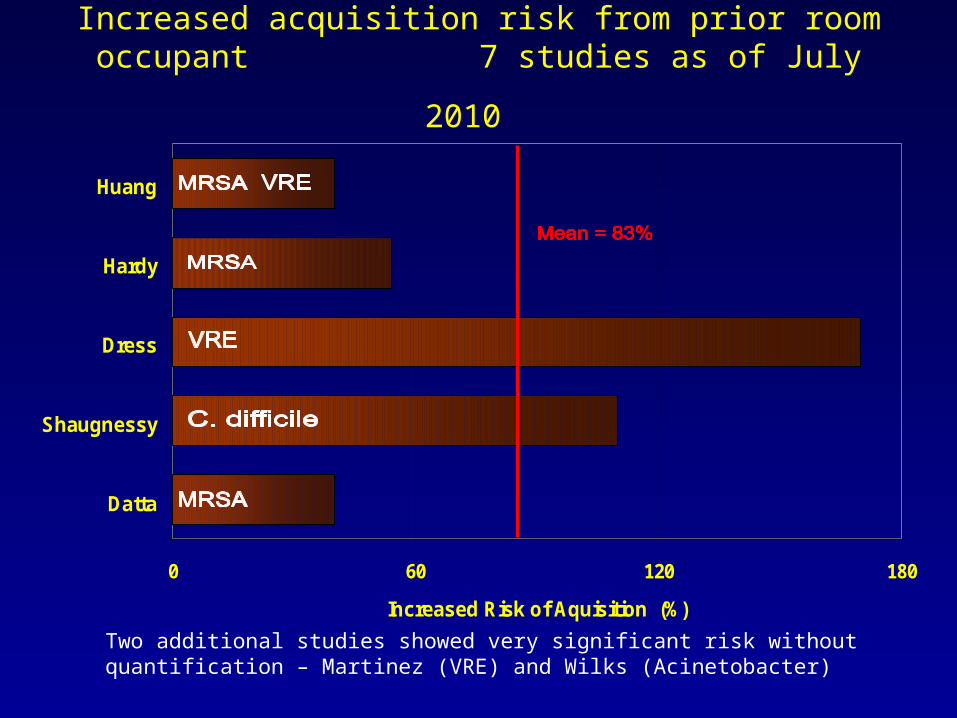
Increased acquisition risk from prior room occupant
7 studies as of July 2010
0 60 120 180
Datta
Shaugnessy
Dress
Hardy
Huang
Increased Risk of Aquisition (%)
Two additional studies showed very significant risk without quantification – Martinez (VRE) and Wilks (Acinetobacter)
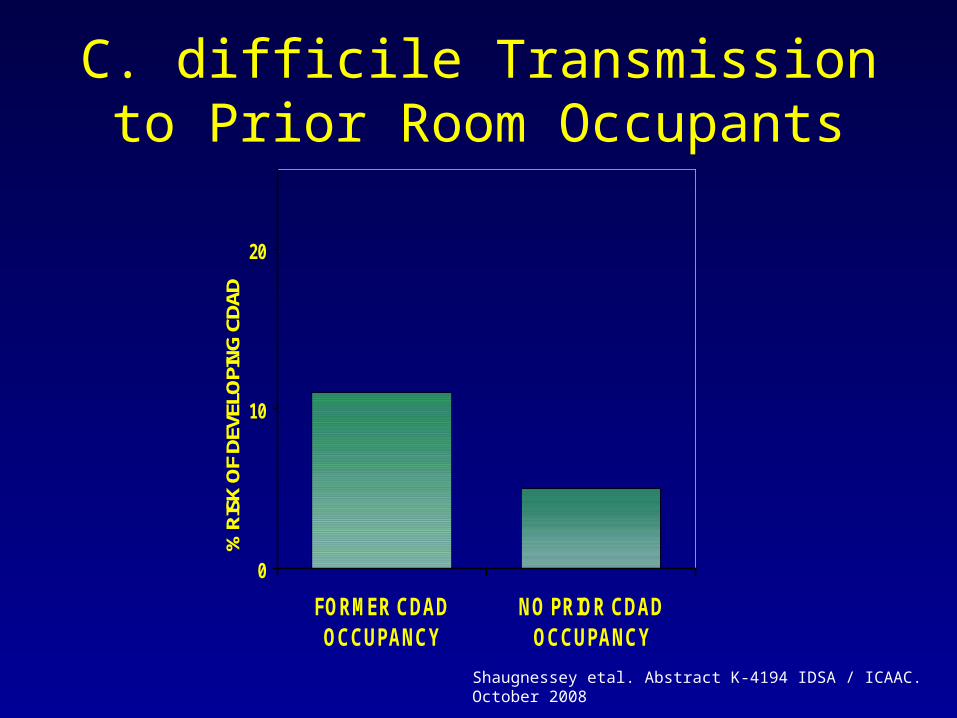
C. difficile Transmission to Prior Room Occupants
0
10
20
FORMER CDADOCCUPANCY
NO PRIOR CDADOCCUPANCY
% R
ISK
OF
DEVE
LOPI
NG C
DAD
Shaugnessey etal. Abstract K-4194 IDSA / ICAAC. October 2008
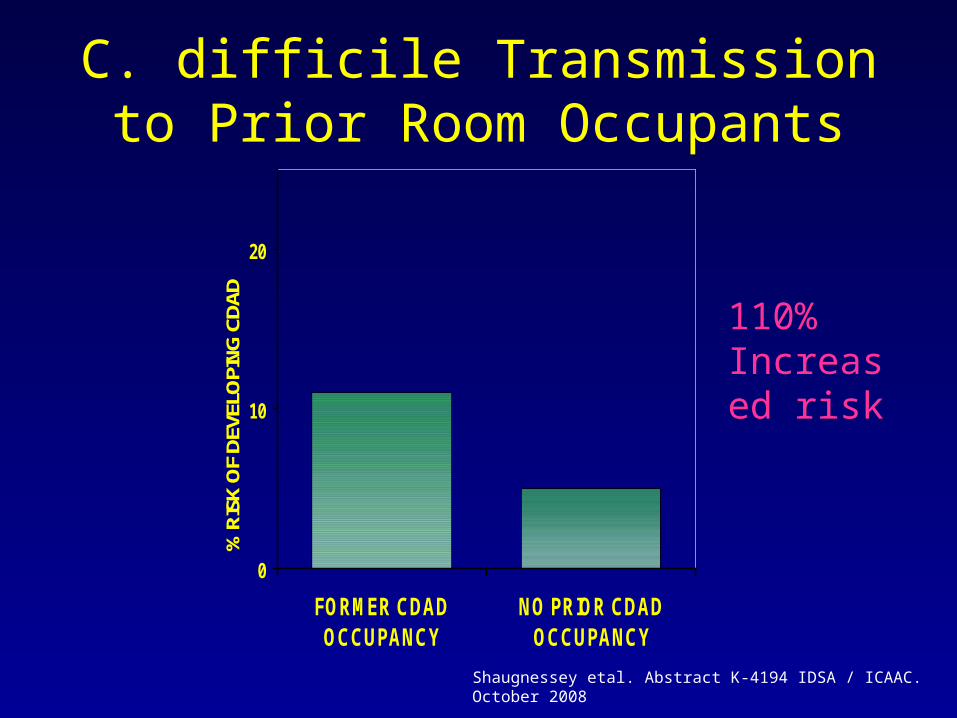
C. difficile Transmission to Prior Room Occupants
0
10
20
FORMER CDADOCCUPANCY
NO PRIOR CDADOCCUPANCY
% R
ISK
OF
DEVE
LOPI
NG C
DAD
Shaugnessey etal. Abstract K-4194 IDSA / ICAAC. October 2008
110% Increased risk
Can better cleaning favorably impact environmental contamination with C.
diff ?
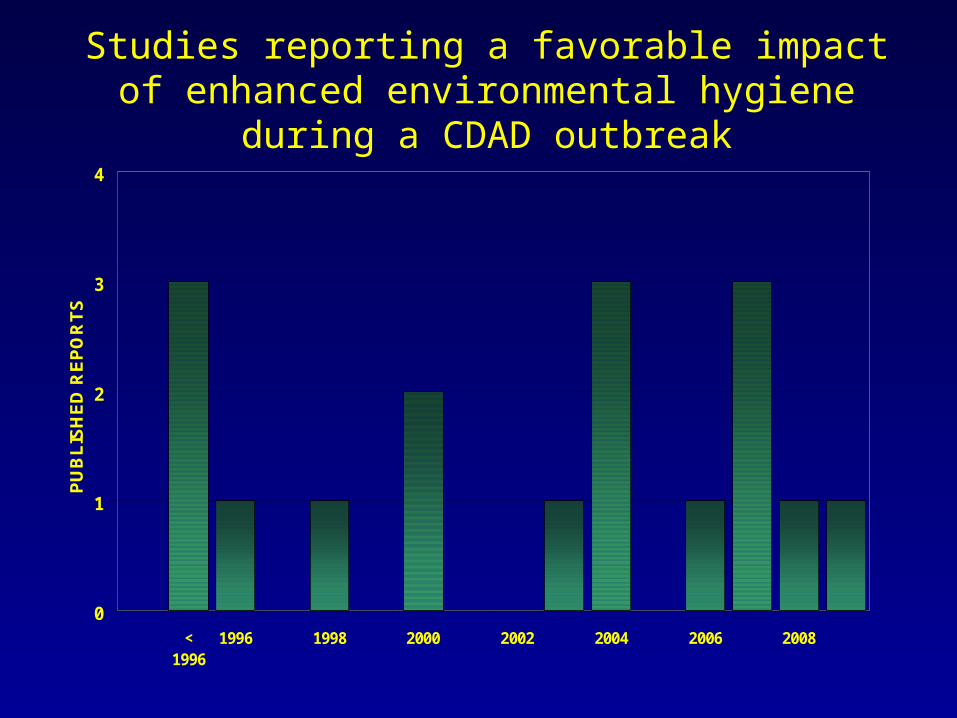
Studies reporting a favorable impact of enhanced environmental hygiene during a CDAD outbreak
0
1
2
3
4
<1996
1996 1998 2000 2002 2004 2006 2008
PU
BL
ISH
ED
RE
PO
RT
S
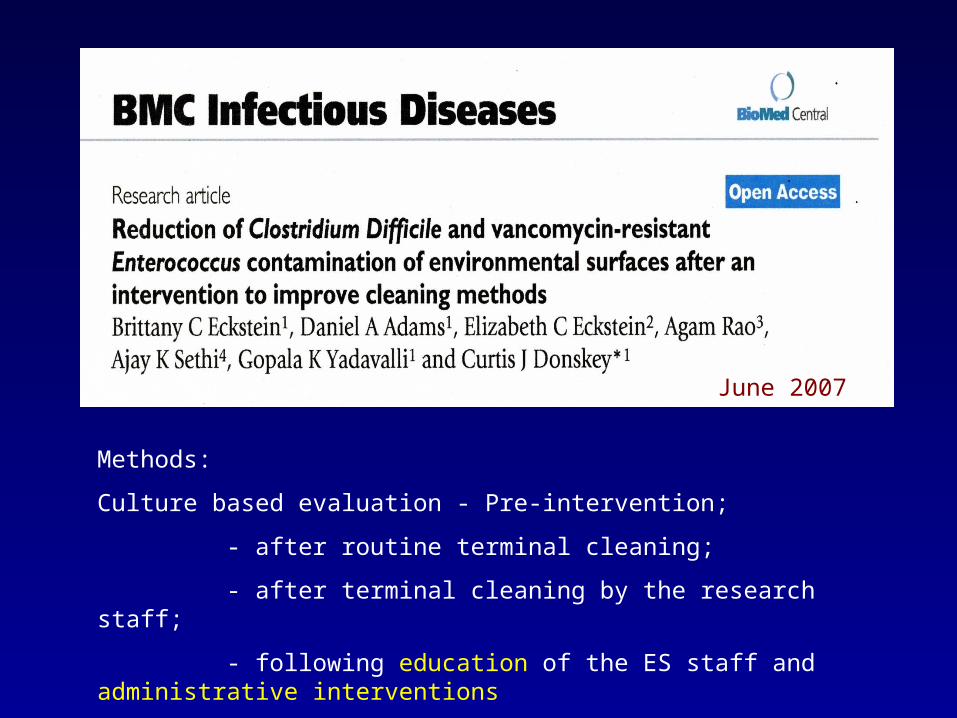
June 2007
Methods:
Culture based evaluation - Pre-intervention;
- after routine terminal cleaning;
- after terminal cleaning by the research staff;
- following education of the ES staff and administrative interventions
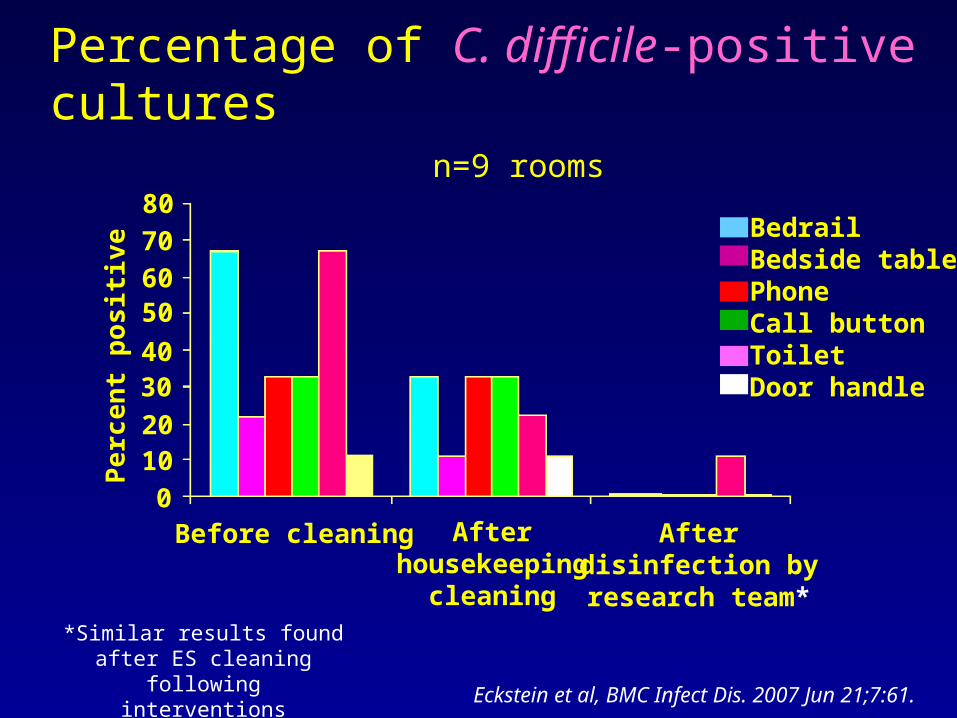
Percentage of C. difficile-positive cultures n=9 rooms
80
706050
4030
2010
0
Pe
rce
nt
po
sit
ive
Before cleaning Afterhousekeeping
cleaning
Afterdisinfection byresearch team*
BedrailBedside tablePhoneCall buttonToiletDoor handle
Eckstein et al, BMC Infect Dis. 2007 Jun 21;7:61.
*Similar results found after ES cleaning following
interventions
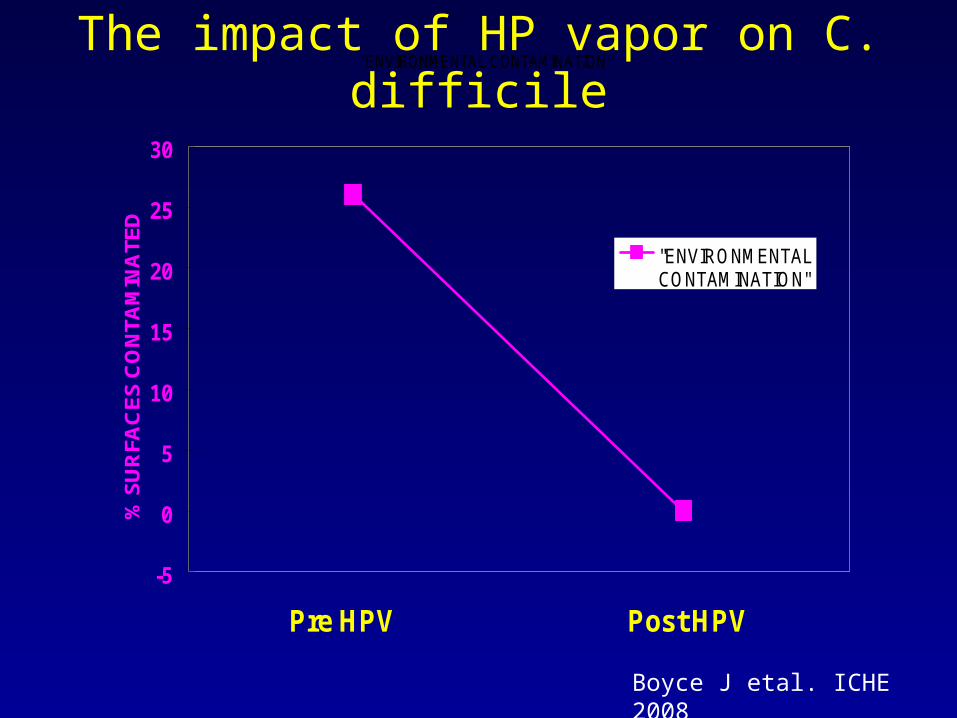
The impact of HP vapor on C. difficile"ENVIRONMENTAL CONTAMINATION"
-5
0
5
10
15
20
25
30
Pre HPV Post HPV
% S
UR
FAC
ES
CO
NTA
MIN
ATE
D
"ENVIRONMENTALCONTAMINATION"
Boyce J etal. ICHE 2008

The impact of HP vapor on C. difficile
-5
0
5
10
15
20
25
30
Pre HPV Post HPV
% S
UR
FA
CE
S C
ON
TA
MIN
AT
ED
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
C. D
IFF
RA
TE
/ 10
00 P
TD
"ENVIRONMENTALCONTAMINATION"
"C. DIFF RATE"
Boyce J etal. ICHE 2008
Does improving environmental hygiene have a measurable Impact on
environmental contamination with C. difficile?
Eckstein – 2007Boyce – 2008
Impact on Transmission?
Quasi-experimental support – Substantial but limited by study design and evaluation in outbreak settings
Why is C. being transmitted to susceptible patients in our
hospitals ?

Don’t forget the Rutala Equation
Product + Practice

Don’t forget the Rutala Equation
Product + Practice
The other name for Hygienic Practice ?
The other name for Hygienic Practice
The Missing Link

The other name for Hygienic Practice
The Missing Link
Why?

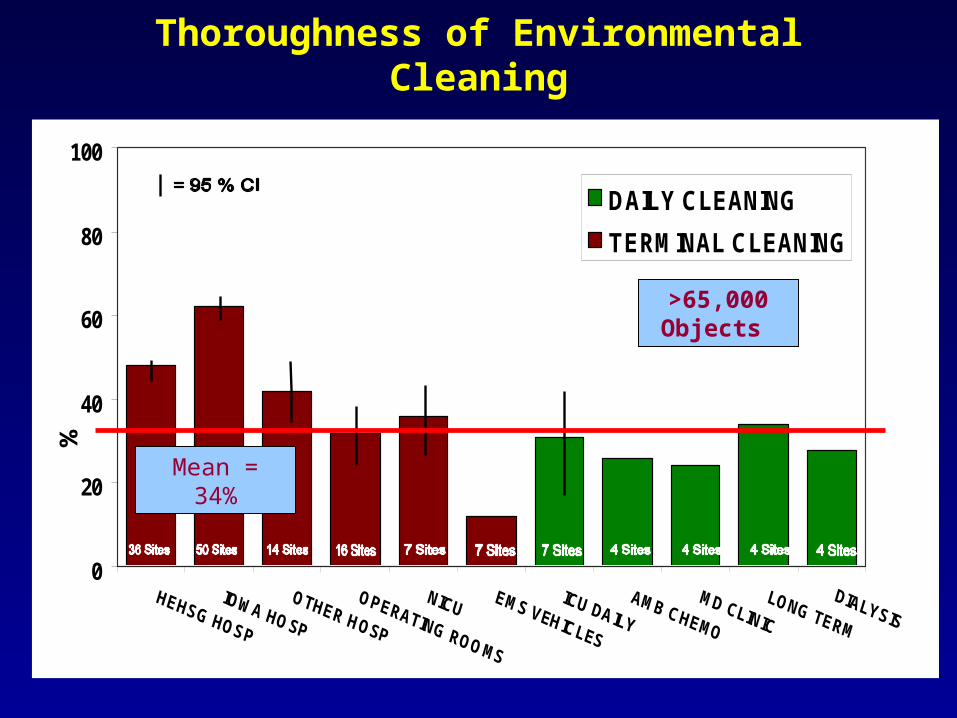
Thoroughness of Environmental Cleaning
0
20
40
60
80
100
%
DAILY CLEANING
TERMINAL CLEANING
Cle
aned
Thoroughness of Environmental Cleaning
0
20
40
60
80
100
%
DAILY CLEANING
TERMINAL CLEANING
Cle
aned
Mean = 34%
>65,000 Objects
0 20 40 60 80 100
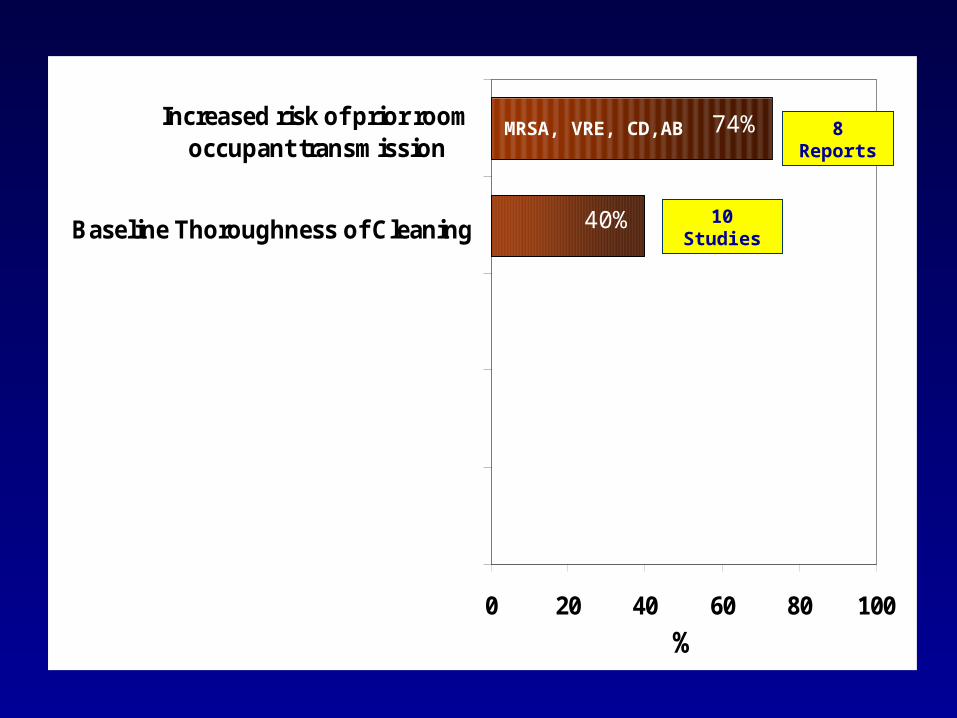
Baseline Thoroughness of Cleaning
Increased risk of prior roomoccupant transmission
%
10 Studies
8 ReportsMRSA, VRE, CD,AB
40%
74%
Why is environmental cleaning not being done thoroughly ?

“Environmental Rounds” to search for problems in cleaning
performanceor….

The search fro the Nefarious Dust Bunny
What does this finding say about disinfection cleaning at this hospital???
Finding the “Brown Spot”
What does this finding say about disinfection cleaning at this hospital???
ES Director
IPES Supervisor
Finding the “Brown Spot”
What does this finding say about disinfection cleaning at this hospital???
ES Director
IPES Supervisor
How long has this been here?
The nurses are right. ES at this hospital is terrible
Finding the “Brown Spot”
What does this finding say about disinfection cleaning at this hospital???
ES Director
IPES Supervisor
Who can I blame?
How long has this been here?
The nurses are right. ES at this hospital is terrible
Finding the “Brown Spot”
What does this finding say about disinfection cleaning at this hospital???
ES Director
IPES Supervisor
Who can I blame?
How long has this been here?
The nurses are right. ES at this hospital is terrible
I hate Environmental Rounds…. Why doesn’t this IP get a life?

Conventional monitoring of health care environmental cleaning
“Environmental Rounds”
• Subjective visual assessment
“If something looks dirty, it means housekeeping has failed”
• Deficiency oriented• Episodic evaluation• Problem detection feedback• Open definition of correctable intervention
Can the thoroughness of Hygienic Cleaning be improved?
RESULTS

Targeting Solution (AKA – Goo)
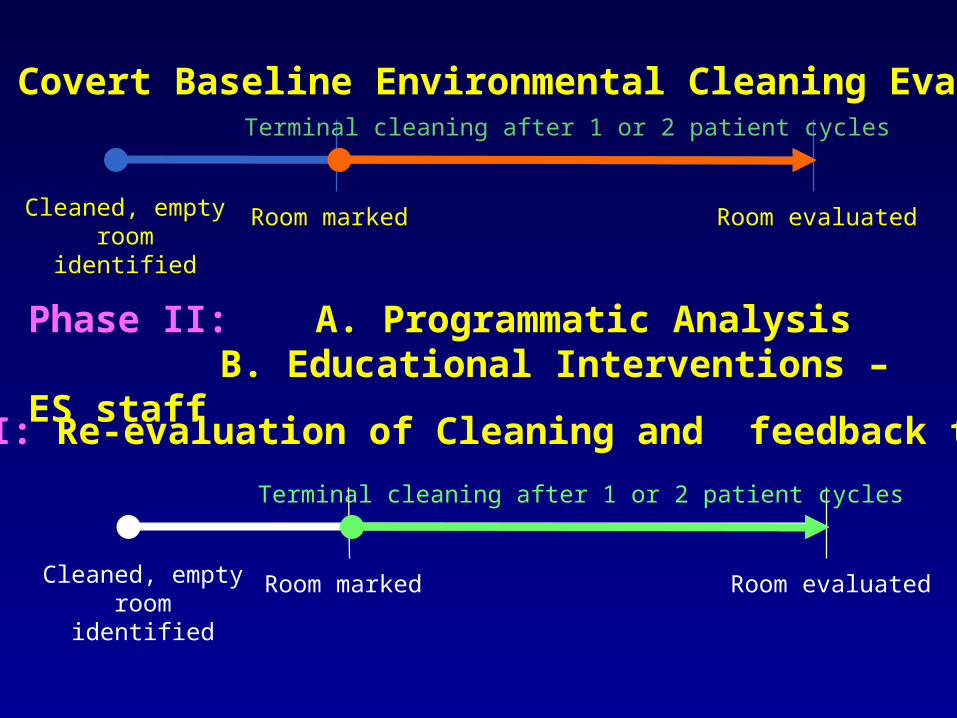
Cleaned, empty room
identified
Room marked Room evaluated
Terminal cleaning after 1 or 2 patient cycles
Phase I: Covert Baseline Environmental Cleaning Evaluation
Phase II: A. Programmatic AnalysisB. Educational Interventions – ES staff
Cleaned, empty room
identified
Room marked Room evaluated
Terminal cleaning after 1 or 2 patient cycles
Phase III: Re-evaluation of Cleaning and feedback to ES
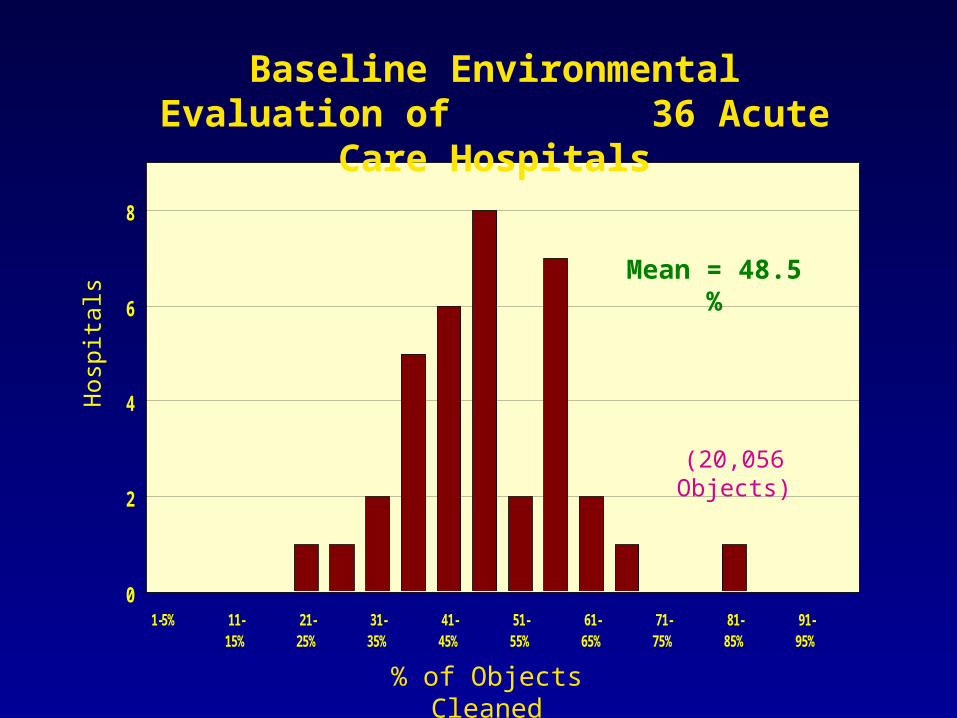
0
2
4
6
8
1-5% 11-15%
21-25%
31-35%
41-45%
51-55%
61-65%
71-75%
81-85%
91-95%
Baseline Environmental Evaluation of 36 Acute Care Hospitals
% of Objects Cleaned
Hos
pita
ls
Mean = 48.5 %
(20,056 Objects)

40
50
60
70
80
Hospitals Environmental Hygiene Study Group36 Hospital Results
% o
f O
bjec
ts C
lean
ed
PRE INTERVENTION POST INTERVENTION
P = <.0001Resource Neutral
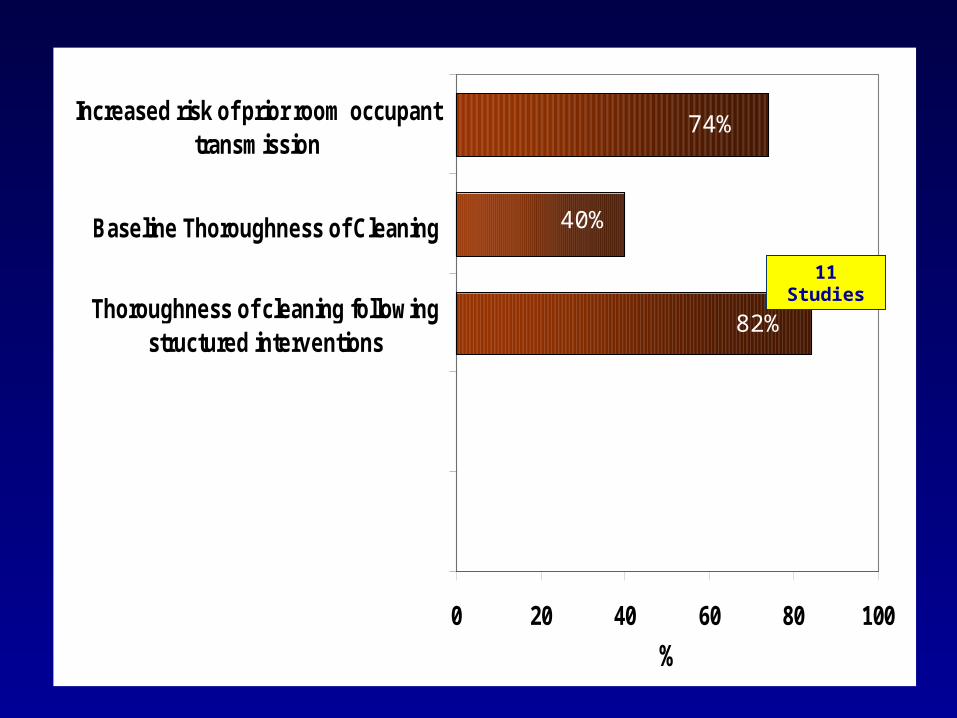
0 20 40 60 80 100
Thoroughness of cleaning followingstructured interventions
Baseline Thoroughness of Cleaning
Increased risk of prior room occupanttransmission
%
11 Studies
40%
74%
82%
Are such results sustainable?
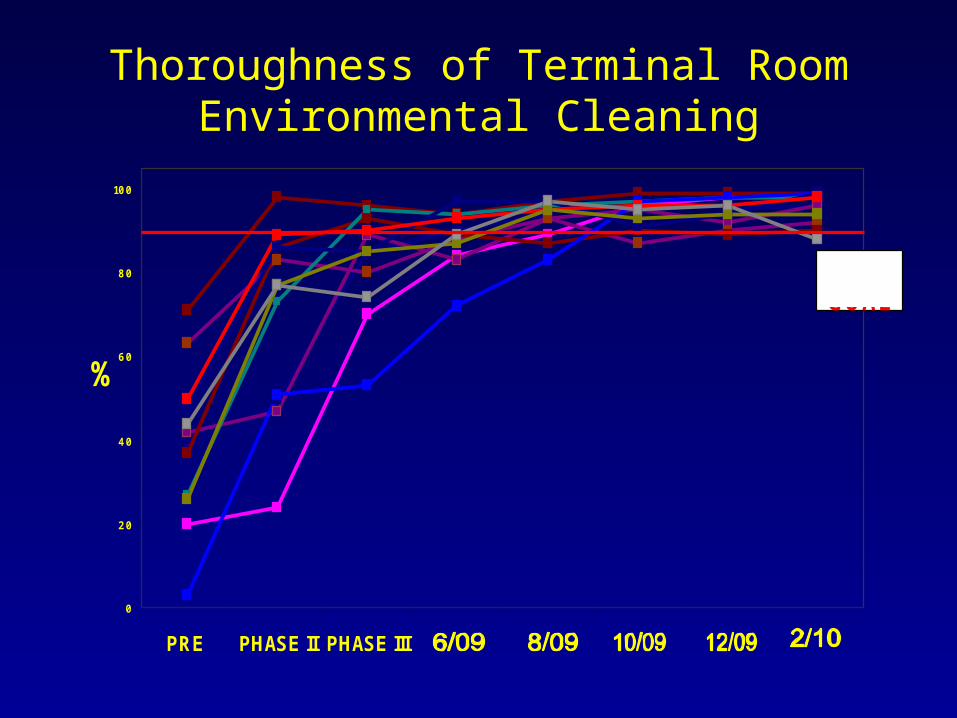
Thoroughness of Terminal Room Environmental Cleaning
0
20
40
60
80
100
PRE PHASE II PHASE III
%
90% GOAL
CLEAN

Was it a lot of work?
Sample Size Required to Monitor Cleaning Practice
0
100
200
300
400
500
600
20% 30% 40% 50% 60% 70% 80%
Thoroughness of Cleaning
Num
ber
of O
bjec
ts to
be
Mon
itore
d
Chow S, Shao J, Wang H. Sample size calculations in clinical research. 2ND ed. Chapman & Hall; 2007.
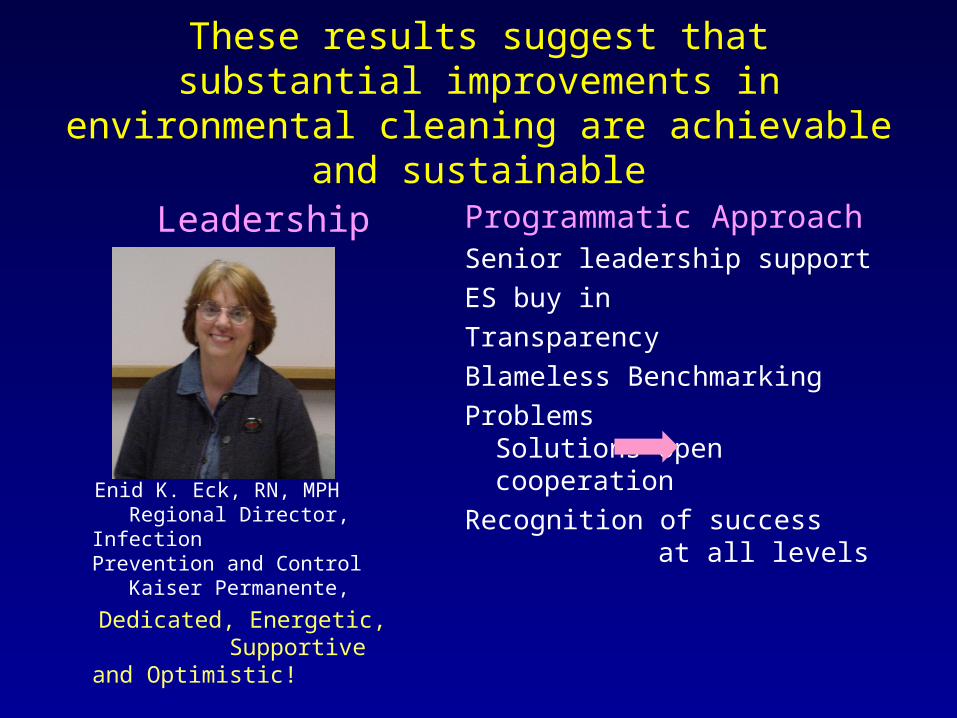
These results suggest that substantial improvements in environmental cleaning are
achievable and sustainable
Leadership
Enid K. Eck, RN, MPH Regional Director, Infection Prevention and Control Kaiser Permanente,
Dedicated, Energetic, Supportive and Optimistic!
Programmatic ApproachSenior leadership support
ES buy in
Transparency
Blameless Benchmarking
Problems Solutions open cooperation
Recognition of success at all levels

Improved Thoroughness of hygienic cleaning is a worthy goal given the billions of dollars involved…but will it impact transmission of HAPs ?
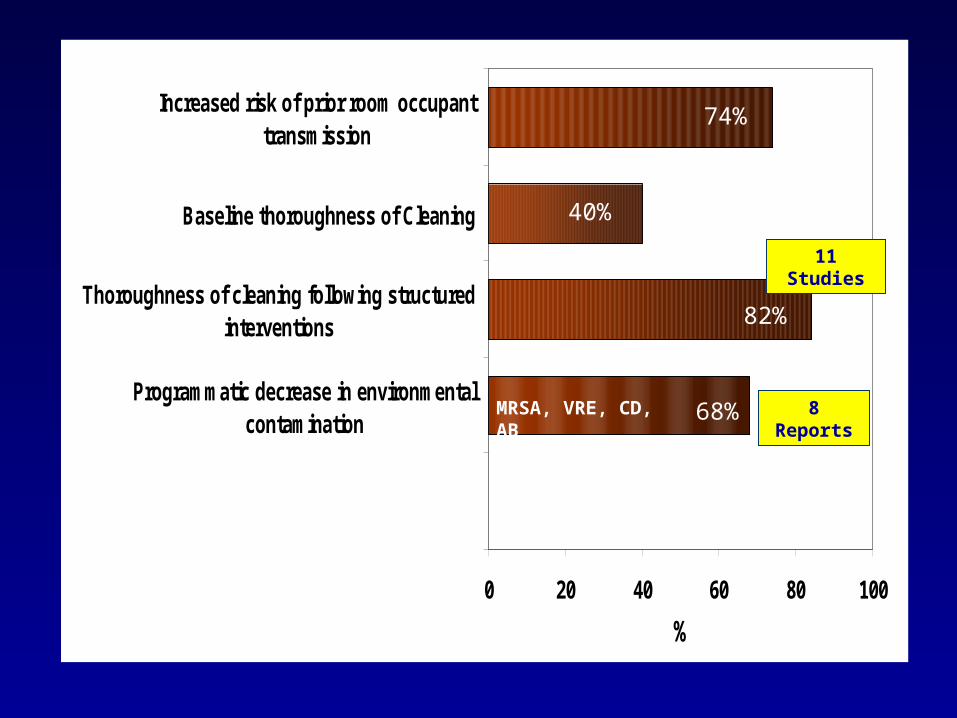
0 20 40 60 80 100
Programmatic decrease in environmentalcontamination
Thoroughness of cleaning following structuredinterventions
Baseline thoroughness of Cleaning
Increased risk of prior room occupanttransmission
%
11 Studies
8 ReportsMRSA, VRE, CD, AB
40%
74%
82%
68%
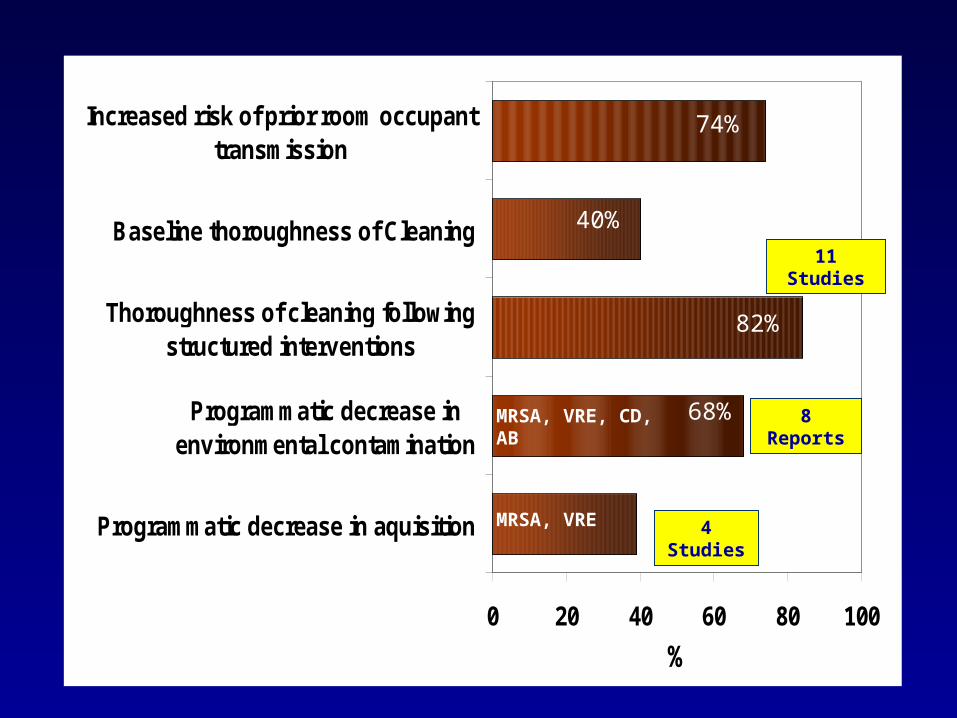
0 20 40 60 80 100
Programmatic decrease in aquisition
Programmatic decrease inenvironmental contamination
Thoroughness of cleaning followingstructured interventions
Baseline thoroughness of Cleaning
Increased risk of prior room occupanttransmission
%
11 Studies
8 Reports
4 StudiesMRSA, VRE
40%
74%
82%
68%MRSA, VRE, CD, AB
Given these results and in the context of the economic issues involved we need to seriously consider moving beyond Conventional Monitoring of health care environmental cleaning

Cleaning House: A New Metric in the Objective Evaluation of
Environmental Cleaning

Approaches to Programmatic Environmental Cleaning Monitoring
Conventional Program
• Subjective visual assessment
• Deficiency oriented• Episodic evaluation• Problem detection
feedback• Open definition of
correctable interventions
Enhanced Program
• Objective quantitative assessment
• Performance oriented• Ongoing cyclic monitoring• Objective performance
feed back• Goal oriented structured
Process Improvement model
Carling PC, Bartley JM. AJIC (In-press)
AJIC Title Picture
Am J Infect Control 2010;38:S41-50 (June)
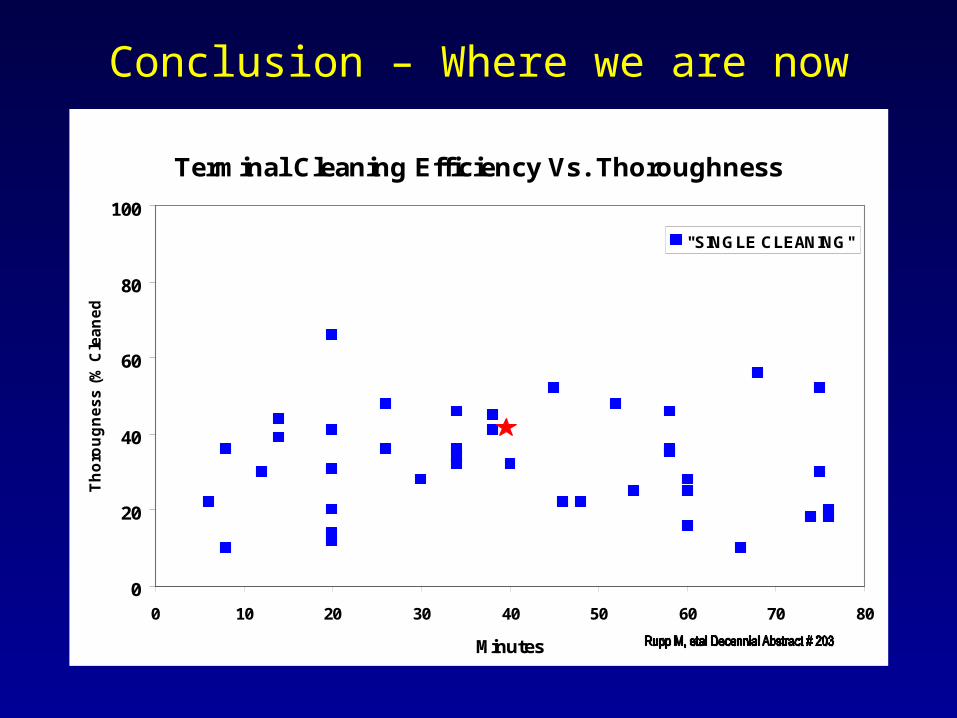
Conclusion – Where we are now
Terminal Cleaning Efficiency Vs. Thoroughness
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80
Minutes
Th
oro
ug
ne
ss
(%
Cle
an
ed
)
"SINGLE CLEANING"
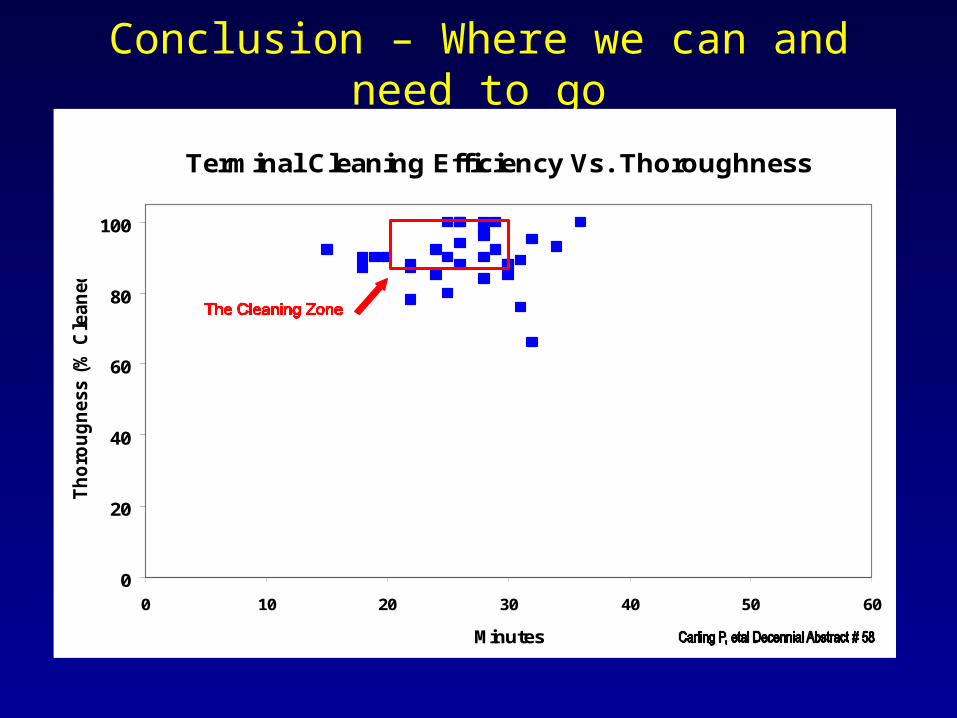
Conclusion – Where we can and need to go
Terminal Cleaning Efficiency Vs. Thoroughness
0
20
40
60
80
100
0 10 20 30 40 50 60
Minutes
Th
oro
ug
ness (
% C
lean
ed
)
So what about the disinfectant?

Don’t forget the Rutala Equation
Product + Practice

Issues with disinfectants, detergents, cloths, etc.
• What is the true role of bleach in disinfection cleaning?
• How effective will new green disinfectants be?
• When is it okay to use detergents?
• Where are we going with dwell time?
• Where does microfibre fit in?• If effective killing with bleach takes
many minutes, what is the clinical efficacy of bleach wipes?
• What is the correct amount of quat?
• Are disinfectants being mixed accurately?
Now is the time to carefully evaluate the role of product in the clinical setting
Old assumptions and new claims of effectiveness of all tools, chemicals and technological interventions must:
- be quantitatively evaluated clinically - while objectively analyzing the
thoroughness of cleaning practice
Conclusions
• It is very likely that surfaces in the Patient Zone are of relevance in the transmission of Healthcare Associated Pathogens.
• While optimizing hand hygiene and isolation practice is clearly important there is no reason why the effectiveness and thoroughness of environmental hygienic cleaning should not also be optimized, particularly since such an intervention can be essentially resource neutral.

A final thought about C. diff rates in hospitals

With respect to environmental hygiene …
can C. diff rates serve as the

With respect to environmental hygiene …
can C. diff rates serve as the
??
Presentation Objectives
A. Understand current issues related to the roe of the environment in CDI transmission
B. Understand the basis for suboptimal healthcare environmental cleaning
C. Appreciate the complexity of making practice recommendations without modern evidenced based studies
