optimising the high risk bariatric patient for surgery - laparoscopic
TRANSCRIPT

Optimising the High Risk Bariatric Patient for Surgery
Mr Andrew Jenkinson MS FRCS Consultant Surgeon The London Clinic
Quality and Safety Lead University College Hospital London Chairman Bariatric Development The London Clinic

Worldwide Prevalence of Obesity
Worldwide Obesity League Table

Conditions Associated with Obesity
Obstructive Sleep Apnoea
• Type II Diabetes • Hypertension • Hypercholesterolaemia
Metabolic Syndrome
Ischaemic Heart Disease

Pre-assessment Clinic
Rationale
3. Assessment of Fitness for Surgery
1. Screening tool for Occult Disease
2. Optimisation of Preexisting Conditions

CPX fitness/triage
Specialist investigations
Routine investigations
Sur
gica
l Clin
ic
Pre-
asse
ssm
ent
Clin
ic
Nurse
Anaesthetist MDT
1. Unfit; risks>benefits
2. Unfit; benefits>risks
Fit if optimised
3. Fit
2-6 weeks
Pre-assessment Clinics
STOP BANG
Sleep Study
Endocrinology Cardiology Respiratory Psychology
Pre-assessment Clinic
Rationale
Assessment of Fitness for Surgery
Screening tool for Occult Disease
Optimisation of Preexisting Conditions
SLEEP APNOEA
CPEX

Bone Airway Soft tissue
The Airway
From Watanabe et al Copyright © 2009, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Obstructive Sleep Apnoea
APNOEAS - Abnormal pauses in breathing
HYPOAPNOEAS - Abnormal episodes of shallow breathing

Bone Airway Soft tissue
The Airway
Obstructive Sleep Apnoea
APNOEAS - Abnormal pauses in breathing
HYPOAPNOEAS - Abnormal episodes of shallow breathing
Reduced Luminal Diameter Inc Airway Resistance
Greater Insp Effort Required Negative Insp Pressure
Further Airway Narrowing Airway Occlusion

Obstructive Sleep Apnoea
Symptoms Daytime somnolence, fatigue Impaired Alertness, slower reactions, vision problems Leads to Behavioral changes – moodiness, decreased attention and drive Morning Headache
Often Symptoms Ignored by Patient Often Symptoms Misdiagnosed
Recent Interest in Effect of Sleep Disturbance on Appetite Regulation and Glycaemic Control
Incidence of OSA Mild 20% Moderate / Severe 7%

STOP BANG
Chung F, Yegneswaran B, Liao P, Chung SA, Vairavanathan S, Islam S, Khajehdehi A, Shapiro CM. Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology 2008; 108: 822-30. [Conclusion; STOP Sens 65.6%, Spec 60% (PPV 78; NPV 44). BANG Sens 83.6%, Spec 56.4% (PPV 81; NPV61). Combined 91% and 74% respectivelly. Grade C recommendation]
STOP S (snore) Loud Snoring T (tired) Daytime Tiredness O (observed) Cessation of Breathing During Sleep P (blood Pressure) Have or being treated for High Blood
Pressure BANG B (body mass index) BMI >35kgs/m2 A (age) Age >50 years N (neck) Neck Circumference >40cm G (gender) Male
Predictor for Sleep Apnoea
Sensitivity 65% Specificity 60%
Sensitivity 84% Specificity 56%
STOP-BANG Combined Sensitivity 91% Specificity 74%

! Snores at night ! Has morning headache ! Tires during the day
Your typical patient with OSA
“Under diagnosed” Validation of the American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology 2008; 108: 822-30

! Male ! Past 40 ! Overweight
Your typical patient with OSA

Nocturnal oximetry
1. 4% sats drop/ hr = 86/hr = AHI index 2. Average sats [=81%] 3. Lowest sats [=50%]
1 2
3
Your typical patient with OSA

Nocturnal oximetry
1. 4% sats drop/ hr = 86/hr = AHI index 2. Average sats [=81%] 3. Lowest sats [=50%]
1 2
3
Apnoea Hypopnoea Index (AHI)
5-15 mild 15-30 moderate >30 severe
Your typical patient with OSA

Assessment of Fitness for Surgery
After Optimisation of Pre existing Conditions
Is Patient Fit to Withstand General Anaesthetic?
Is Patient fit to Survive a Complication of Surgery?
Quantify Risk of Surviving Surgery
What is the Anaerobic Threshold?

• Cycle ergometer
• On-mouth pneumotachograph to measure flow of gases
• Gas sampling to O2 and CO2 sensors to record O2 used and CO2 produced in ml/kg/min
• Continuous 12 lead ECG and ST segment analysis
• Exercise increased till the rise in CO2 exceeds the slope of the O2 supply. This O2/CO2 crossover is referred to as the anaerobic threshold (AT)
Cardio pulmonary exercise test (CPX)

Results • Degree of exercise or tolerance
• ECG changes: heart rate, arrhythmias and their type, ST levels
• Pulmonary function test - dynamic
• Anaerobic Threshold (AT)
Cardio pulmonary exercise test (CPX)

VO2 (ml/min)
The Physiological Principle
Anaerobic Contribution To Metabolism
Aerobic Metabolism
Anaerobic Threshold
CO2
Prod
uction
(ml/min)
O2 Consumption (ml/min)

AT >11 – No recommendation of augmented level of care on the basis of CPEX results
AT < 11 – Consider Intensive recovery, PACU,
HDU or ICU AT < 8, – Consider/prepare for extended
stay on ICU
Level of care triage
Normal Anaerobic Threshold (AT) - >16mls/kg/min
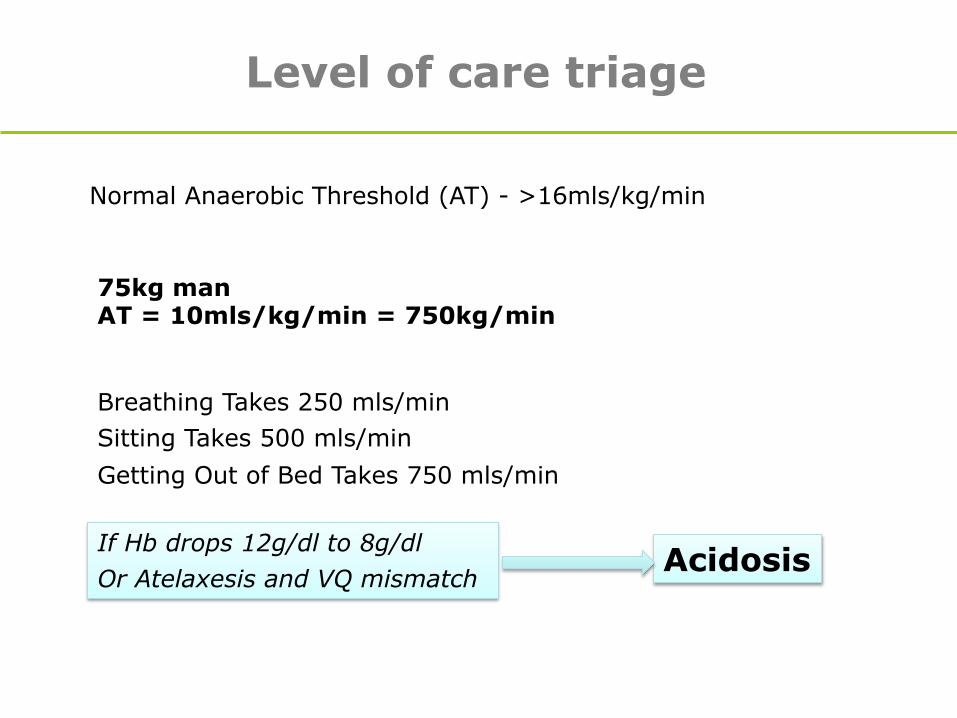
Level of care triage
Normal Anaerobic Threshold (AT) - >16mls/kg/min
75kg man AT = 10mls/kg/min = 750kg/min
Breathing Takes 250 mls/min Sitting Takes 500 mls/min Getting Out of Bed Takes 750 mls/min
If Hb drops 12g/dl to 8g/dl Or Atelaxesis and VQ mismatch
Acidosis

Advice on risk of surgery
AT >11 - periop mortality less than 1%; AT < 11- periop CVS mortality 18%; AT < 8 - periop CVS mortality 50%; in
patients> 65yrs

One Stop Proforma
Diabetes Optimisation
• Poor preoperative glycaemic control is associated with increased postoperative morbidity and mortality
• Optimisation of DM control can reduce postoperative mortality by 50%
• Aim for HbA1C < 69 mmol/mol (8.5%) prior to surgery

Lifestyle Changes
• Stop Smoking • Increase Activity Levels
• Preoperative Diet • Psychological Counselling

Summary
• Pre-assessment Essential for All Surgical Patients
• Be Aware of Sleep Apnoea
• Use CPEX Assessment to Quantify Risk