optical recognition of polyps - conferre
TRANSCRIPT


Optical recognition of polyps
Bassioukas P. Stefanos
Department of Advanced Therapeutic Endoscopy, Bioclinic Hospital Athens

Is optical diagnosis and interpretation of colonic polyps useful?
Clinical case 1:
• 56 year-old male diagnosed with a recto-sigmoid LST-G mixed type under whitelight endoscopy, approximately 7cm

• Biopsies (10 samples) showed adenoma with low to intermediate dysplasia
• Due to tumor size CT scan and Pelvic MRI was performed
• MRI diagnosed wall thickening (possible T2 stage tumor), with a 10cm length occupying more than 50% of lumen periphery

Treatment Decision
• Surgery – low anterior resection
• But …… biopsies are negative for infiltrative malignancy….
• New image enhanced endoscopy and targeted biopsies for diagnosis



14x12 cm, Fibrosis Grade 3 Adenoma with low grade dysplasia and focal high grade
dysplasia, R0 resection

Clinical case 2
• 74 year-old female diagnosed with a 3 cm ascending colon LST-NG type polyp
• Biopsies showed high grade dysplasia

Treatment Decision
• It is not a cancer…
• Let’s try en-block removal for definite diagnosis

AdenoCa

Lesion morphologyParis Classification


Risk Stratification for Covert Invasive Cancer Among Patients Referred for Colonic Endoscopic Mucosal Resection:
A Large Multicenter Cohort Burgess N et al. Gastroenterology 2017;153:732–742


Magnification Chromoendoscopy
Kudo Pit-Pattern
Deep sm 28%
Deep sm
90%

Image Enhanced Endoscopy
overall accuracy for sm 70%


Surface/Vessel architectureMagnification virtual endoscopy






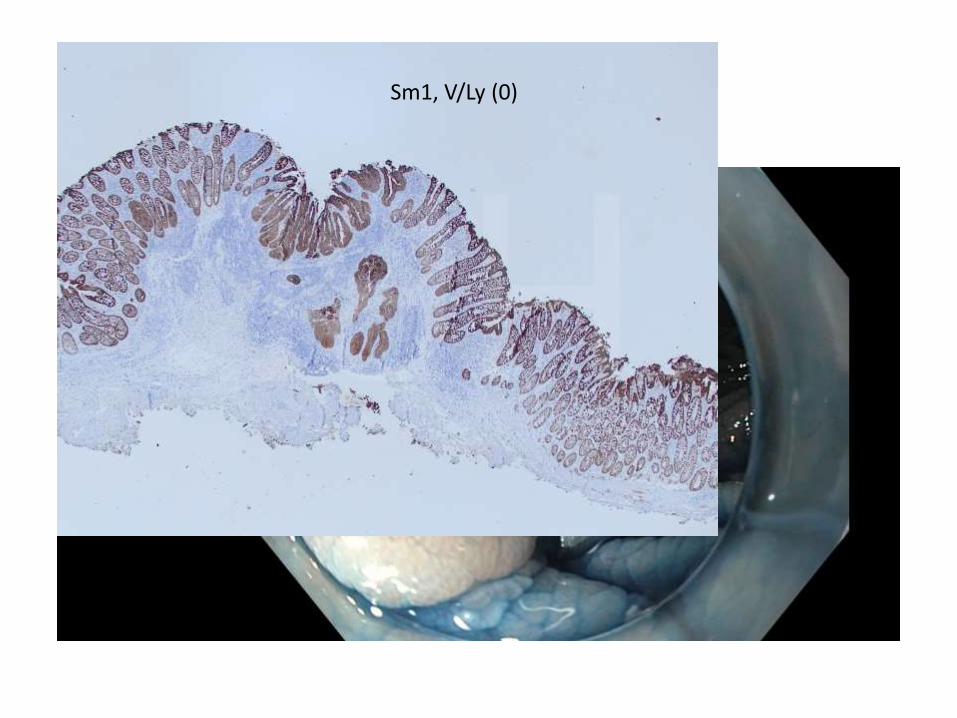
Sm1, V/Ly (0)


Conclusions
• Optical recognition is very important to determine diagnosis and choose the right therapy
• Use high definition endoscopes with image enhanced technology in cases of IIc-depressed lesions and LST-NG/G mixed types
• If this is not possible, just spray 0.3% Indigo Carmine for better interpretation
• Do not take multiple biopsies if you consider resectability. Fibrosis!! Do not tattoo under the lesion!
• One or two targeted samples are sufficient.
• Share your cases with other colleagues. We all get better endoscopists…

Optical recognition of polyps
Bassioukas P. Stefanos
Department of Advanced Therapeutic Endoscopy, Bioclinic Hospital Athens