ophthalmic in - metrovision.fr · pinel, 69003lyon, france. acceptedforpublication ... in all the...
TRANSCRIPT
BritishJ7ournal ofOphthalmology 1993; 77: 785-788
Ophthalmic results in patients withmacroprolactinomas treated with a new prolactininhibitor CV 205-502
Michele Grochowicki, Yad Khalfallah, Alain Vighetto, Serge Berquet, Genevieve Sassolas
AbstractMacroprolactinomas are pituitary tumourswhich have been effectively treated medicallysince the introduction of bromocriptine. Thevisual function of 13 patients treated with a newprolactin (PRL) inhibitor CV 205-502 (SandozBasle), a potent and selective dopamine D2receptor agonist, was evaluated. This is thefirst detailed ophthalmic report of the use ofthis drug in macroprolactinomas. Patientswere enrolled from June 1988 to July 1990(mean follow up 30 months). Visual functionincluding visual acuity, ocular pressure, andvisual fields was regularly controlled. Visualfields (VF) were tested with Goldmann andautomatic static perimetry (Vision Monitor).Treatment was globally effective. No modifica-tions of the visual function were observed innine patients (six normal, three previous VFlosses after surgery). In four other patients,visual function dramatically improved (regres-sion ofa III paresis, one case; disappearance ofa chiasmatic syndrome, three cases). A pitu-itary necrosis was observed in one case andsuccessfully cured. CV 205-502 seems to be aneffective and weli tolerated treatment ofmacroprolactinomas.(Br3r Ophthalmol 1993; 77: 785-788)
(Basle, Switzerland) and approved by our institu-tional ethics committee. Thirteen patients with
H6pital Neurologique etNeurochirurgical PierreWertheimer, Lyon,France
Consultationd'OphtalmologieM GrochowickiA VighettoS Berquet
Centre de MedecineNucleaireY KhalfallahG SassolasCorrespondence to:Dr M Grochowicki,Consultationd'Ophtalmologie, H6pitalNeurologique etNeurochirurgical PierreWertheimer, 59 BoulevardPinel, 69 003 Lyon, France.Accepted for publication29 June 1993
For 10 years, dopamine agonists have been usedin the treatment ofmacroprolactinomas, either asa preparation for surgical removal, or as a uniquetreatment.' CV 205-502 (octahydrobenzo [g]quinoline) is a new non-ergot long acting pro-lactin inhibitor, a pure D2 agonist. For 2 yearsseveral clinical teams have reported the firstresults in the treatment of macroprolactino-mas.2- It was shown that CV 205-502 was effec-tive in the treatment of macroprolactinomas incases in which bromocriptine was poorly toler-ated or ineffective.8 CV 205-502 is well toleratedand its long action makes one dose a day possible.CV 205-502 can induce normalisation of prolac-tin (PRL) secretion and a noticeable reduction intumour size. In the control of tumour volume,ophthalmic controls are essential. In this studywe present the ophthalmic results in 13 patientstreated with this new drug, with a mean follow upof 30 months. The early results in eight patientsafter 9 months of treatment have been publishedpreviously.3 To our knowledge, this is the firstdetailed ophthalmic report of the use of this drugin macroprolactinomas.
Material and methodsThis open study was designed by Sandoz Ltd
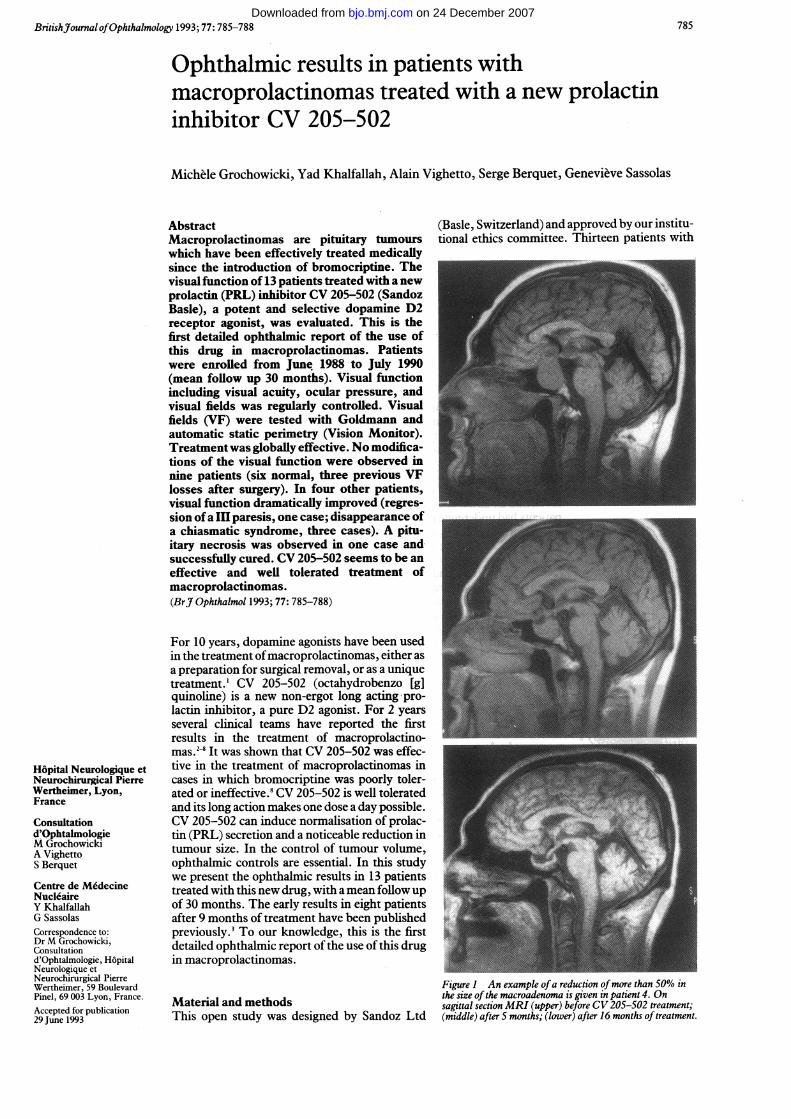
Figure I An example ofa reduction ofmore than 50% inthe size ofthe macroadenoma is given in patient 4. Onsagittal section MRI (upper) before CV 205-502 treatment;(middle) after 5 months; (lower) after 16 months of treatment.
785 on 24 December 2007 bjo.bmj.comDownloaded from
Grochowicki, Khalfallah, Vighetto, Berquet, Sassolas
Table I Visual signs of 13 patients with macroadenomas treated with CV205-502
Patient Nolsexlage Clinical Visual signs Evolution with Follow up(years) history before treatment CV 205-502 (months)
I F 25 S 2 m before Bitemporal hemianopia Unchanged 41RE: 6/6, LE: 6/9
2 M 43 S 4 m before Normal Unchanged 343 M 29 de novo Bitemporal quadrantic defect Normalised (1 m) 41
RE: 6/6, LE: 6/94 M 30 de novo Bitemporal hemianopia Improved (4 m) 40
RE: 6/9, LE: 6/65M 38 S 9 m before Normal Unchanged 436M 46 de novo Normal Unchanged 437M21 S 3 m before Normal Unchanged 398 F 33 S 9 m before Slight quadrantic defect Unchanged 35
right VF, RE:LE: 6/69 F 20 S 2 m before Normal Unchanged 3110 M 63 de novo Unitemporal scotoma Improved (1 m) 24
RE:LE: 6/6 pituitarynecrosis(16 m), RE: 6/9,LE: 6/12
11 F 35 S 8 y before Left III paresis Normalised 16RE: 6/6, LE: 6/9 (6 weeks)
12 M 38 S 5 y before Left, HLH and strabic amblyopia; Unchanged 29R, III palsy RE: 6/6, LE: 6/60
13 M 42 S 7 m before Normal Unchanged 29
S=surgery, de novo=de novo cases.m=month, y=years.RE=right eye; LE=left eye.VF=visual field, HLH=homonymous lateral hemianopia.
macroprolactinomas, nine men and four womenagreed to participate in the present study andgave their informed written consent.They were referred to our institution during a
2 year period from June 1988 to July 1990. Theirages ranged from 20 to 63 years (mean 35). Sixpatients had an initial normal visual function,seven had an initial abnormal one. Nine of thesepatients had undergone pituitary surgery (Nos 1,2, 5,7,8, 9,11, 12, 13),seven as recentlyas 2 to 7months before starting the trial; the two othershad undergone surgery 8 and 5 years previously(Nos 11, 12). They had not been submitted topostoperative radiotherapy. Six ofthem had hadbromocriptine treatment. A 2 month wash outperiod before initiation ofCV 205-502 treatmentallowed plasma PRL to return to pretreatmentlevels and the tumour volume increased again.
a* a,M a
o
Oa
aa
a 8
0 0
6 8O
Oa. a
. 05
. o 0
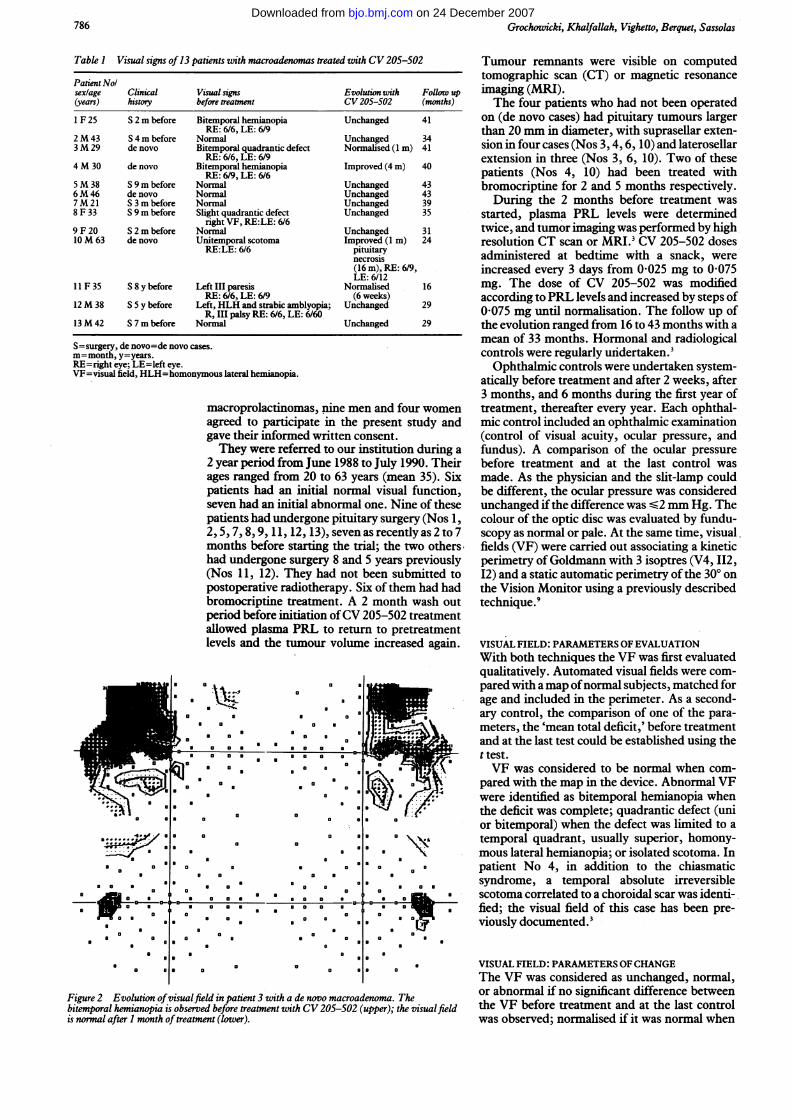
Figure 2 Evolution ofvisualfield in patient 3 with a de novo macroadenoma. Thebitemporal hemianopia is observed before treatment with CV 205-502 (upper); the visualfieldis normal after I month oftreatment (lower).
Tumour remnants were visible on computedtomographic scan (CT) or magnetic resonanceimaging (MRI).The four patients who had not been operated
on (de novo cases) had pituitary tumours largerthan 20 mm in diameter, with suprasellar exten-sion in four cases (Nos 3, 4, 6, 10) and laterosellarextension in three (Nos 3, 6, 10). Two of thesepatients (Nos 4, 10) had been treated withbromocriptine for 2 and 5 months respectively.During the 2 months before treatment was
started, plasma PRL levels were determinedtwice, and tumor imaging was performed by highresolution CT scan or MRI.3 CV 205-502 dosesadministered at bedtime with a snack, wereincreased every 3 days from 0-025 mg to 0 075mg. The dose of CV 205-502 was modifiedaccording to PRL levels and increased by steps of0-075 mg until normalisation. The follow up ofthe evolution ranged from 16 to 43 months with amean of 33 months. Hormonal and radiologicalcontrols were regularly undertaken.3Ophthalmic controls were undertaken system-
atically before treatment and after 2 weeks, after3 months, and 6 months during the first year oftreatment, thereafter every year. Each ophthal-mic control included an ophthalmic examination(control of visual acuity, ocular pressure, andfundus). A comparison of the ocular pressurebefore treatment and at the last control wasmade. As the physician and the slit-lamp couldbe different, the ocular pressure was consideredunchanged ifthe difference was -2 mm Hg. Thecolour of the optic disc was evaluated by fundu-scopy as normal or pale. At the same time, visualfields (VF) were carried out associating a kineticperimetry of Goldmann with 3 isoptres (V4, II2,I2) and a static automatic perimetry of the 300 onthe Vision Monitor using a previously describedtechnique.9
VISUAL FIELD: PARAMETERS OF EVALUATIONWith both techniques the VF was first evaluatedqualitatively. Automated visual fields were com-pared with amap ofnormal subjects, matched forage and included in the perimeter. As a second-ary control, the comparison of one of the para-meters, the 'mean total deficit,' before treatmentand at the last test could be established using thet test.VF was considered to be normal when com-
pared with the map in the device. Abnormal VFwere identified as bitemporal hemianopia whenthe deficit was complete; quadrantic defect (unior bitemporal) when the defect was limited to atemporal quadrant, usually superior, homony-mous lateral hemianopia; or isolated scotoma. Inpatient No 4, in addition to the chiasmaticsyndrome, a temporal absolute irreversiblescotoma correlated to a choroidal scar was identi-fied; the visual field of this case has been pre-viously documented.3
VISUAL FIELD: PARAMETERS OFCHANGEThe VF was considered as unchanged, normal,or abnormal if no significant difference betweenthe VF before treatment and at the last controlwas observed; normalised if it was normal when
786
a. .-:R
6.
0
a a
5 a
aa a
a0 0 0 a
a
aa
0 0a 6
a a 0
a
a 0 a a8 0
1 a 0a a
aa
0 a
0
a 00
a
0.0
00a
I
0
a
a
a
I
8
a
a
9
aa
.'.:"I a
6.A.a 0
a.......-6..0a
0
m 00
a
a n ma
a0
a0
00
9-0-0
0
0 0
sa 0
a
a a a s
I
a a
a0 5 0 0 8
I0
5 00 a
00
0 0a
0
a8
0a 0
00m 0
00
09
0
0
0
a
0
0
00
a
0
a
0
@@ a0
0
aI0 .-.
5
a
a 0
on 24 December 2007 bjo.bmj.comDownloaded from

Ophthalmic results in patients with macroprolactinomas treated with a new prolactin inhibitor CV 205-502
Figure 3 Visual field (VF)ofpatient 10; (upper) the compared with the map in thedeficit is limited to anirregular left temporal when a regression of more thascotoma after 13 months of defect was observed qualitattreatment with CV 205- titatively.502. (Lower) corresponds tothe beginning ofpituitarynecrosis after 16 months ofmedical treatment with Resultsvisualfailure (LE=6118; The overall tolerance was good.RE=619), huge centralscotoma on the RE, of prolactinaemia was observetemporal hemianopia on theLE.
device; improvedm 50% of the VFtively and quan-
.IA normalisationd in 12 out of 13
Figure 4 CT scan ofpatient 10 after 16 months oftreatment with headacheand visualfailure. Coronalsection showing theheterogeneous aspect of thetumour corresponding topituitary necrosis.
Table 2 Visual signs in patients with macroadenomas treated with CV 205-502 in otherpublished reports
Evolution withAutlhors Cases Visual signs before treatment CV 205-502
Barnett et al' M 64 Visual failure; raised intracranial Normalised (2 m)pressure
M 59 Visual failure+hydrocephalus Normalised (2 m)Vance et al5 M Bitemporal hemianopia Partial resolution (1 m)
F Unilateral III palsy Normalised ( 1l/2m)M Bitemporal hemianopia III palsy Unchanged
post surgeryvan Verlaat et al' 1 Bitemporal hemianopia Normalised
3 Bitemporal hemianopia Normalised5 Bitemporal hemianopia Incomplete resolution (6 m)6 Bitemporal hemianopia+III palsy Normalised7 Bitemporal hemianopia Normnlised
Crottaz et al7 M 44 Left blindness secondary to optic Evolution not knownatrophy
M 60 Diplopia Evolution not knownDuranteau et al' 5 cases 'Visual field defect' Improved in 4 m
cases and a considerable reduction of the prolac-tinaemia in one. The reduction in the tumourvolume was superior or equal to 50% in eightcases out of 13 (illustrated in Fig 1). The visualtolerance was good. In all the cases the ocularpressure was -20 mm Hg. During the first yearoftreatment, modifications ofthe ocular pressurewere observed: five with a mean reduction of 4mm Hg, three with a mean increase of 3 mm Hg.These modifications were transient. There wasno difference between the ocular pressuremeasured before the treatment and at the lastcontrol. The aspect of the optic disc remainedunchanged during the treatment; 10 werenormal, three were pale. The visual resultsincluding visual acuity and visual field beforeinclusion were normal in six cases and abnormalin seven cases.
BASELINE NORMAL VISUAL FUNCTION (TABLE 1)Six patients had an initial normal visual function:visual acuity and visual fields were normal in onede novo case (No 6) and five who had undergonesurgery (Nos 2, 5, 7, 9, 13). No visual complica-tion was observed under treatment with CV 205-502 with a range of observation from 30 to 43months. A certain degree of variability in thevisual fields was observed; variable and regres-sive relative scotomas were present withoutmodifications of the prolactin levels, but therewas no significant difference between the meantotal deficit before and after treatment (t test).
BASELINE ABNORMAL VISUAL FUNCTION (TABLE 1)Four of these patients had undergone previouspituitary surgery (Nos 1, 8, 11, 12), three were denovo cases (Nos 3, 4, 10).In three patients (Nos 1, 8, 12) with alterations
of visual field, sequelae of previous pituitarysurgery, no amelioration was observed. Somevariations of the VF were observed in case 8. Incase 12, who had a left strabismic amblyopia, theleft homonymous lateral hemianopia was associ-ated with a III right palsy, sequelae of pituitarysurgery performed 5 years before. In case 11, anisolated left III paresis was observed 8 years afterthe patient had undergone pituitary surgery. Theregression of the ptosis and the diplopia wasobserved after only 6 weeks of medical treat-ment. An excellent and quick regression ofvisualfield abnormalities was observed in the three denovo cases (Nos 3, 4, 10). A complete normalisa-tion was observed in 1 month in case 3 (Fig 2). Inthe two other casesVF improved in 4 months and1 month respectively.We shall examine case No 10 in more detail.After 16 months of closely monitored treat-
ment, the reduction of the volume of the tumouron CT scan was incomplete in spite of a goodcontrol of prolactinaemia and an improved VF.The patient suddenly complained of headacheand his vision decreased bilaterally from normalto RE: 6/9, LE: 6/18 to (lower part of Fig 3) andto 'no light perception' in either eye associatedwith a right ptosis within 2 days. On the CT scana heterogeneous aspect of the macroadenomaassociated with an increase ofsize was compatiblewith the diagnosis of pituitary necrosis (Fig 4).
787 on 24 December 2007 bjo.bmj.comDownloaded from

Grochwicki, Khalfallah, Vighetto, Berquet, Sassolas
Surgical treatment with a trans-sphenoidalapproach was quickly carried out. The visualacuity of the patient rapidly improved and reach6/9 and 6/12 1 month after surgery. In spite of agood anatomical result the PRL level rose and thepatient was again treated with dopamine agonistCV 205-502. The visual field undertaken 8months later remained improved.
DiscussionIn our study, CV 205-502 was effective in thetreatment of macroprolactinomas. In our 13cases, six patients had a normal baseline visualfunction and maintained it during a mean followup of 30 months. Some variations of their visualfields were observed at different checks withoutstatistically significant differences. However, noclear explanation for these modifications could begiven, PRL levels remaining normal at the sametime. A transient modification of the size of thetumour could not be excluded since repeatedradiological investigations were impossible. Thevisual abnormalities we observed did not differfrom those previously published. The evolutionof visual signs under treatment is summarised inTable 2 using the authors' own, sometimesimprecise, terminology. There is an importantdifference between an intractable visual fielddefect after surgery and a visual field hemianopiain de novo cases. In our three patients who hadbeen submitted to previous surgery visual fieldlosses remained unchanged as in a case ofVance.5
In the three de novo cases, the positive andrapid effect in reduction of the visual field losswas obtained, as described previously,between 4 and 8 weeks.25 In patients with latero-sellar extension of macroprolactinoma as in case11, the use of a dopamine agonist is a goodalternative to high risk surgery. Resolution ofdiplopia is effective (case 6 ofVan Verlaat6 and inthe second case of Vance5). Despite thenormalisation of plasma PRL levels, tumoral
tissue may still be present in large amounts.There is a discrepancy between the antisecretoryand the antitumoral responses,3 which has beenpreviously reported with bromocriptine.' In ourcase 10, no complete shrinkage of the tumourwas observed in spite of a normalisation of visualfield and endocrine parameters. There were nosigns predicting pituitary necrosis. CV 205-502is an effective and well tolerated treatment ofmacroprolactinomas with few side effects. How-ever, a visual risk of pituitary necrosis remains."A regular control of ophthalmic function ismandatory as with the other dopamine agonists.
1 Molitch ME, Elton RL, Blackwel RO, Caldweil B, Chang RJ,Jaffe R, et al. Bromocriptine as primary therapy forprolactin-secreting macroadenomas: results of a prospectivemulticenter study. Jf Clin Endocrinol Metab 1985; 60:698-705.
2 Barnett PS, Dawson JM, Butler J, Coskeran PB, Maccabe JJ,McGregor AM. CV 205-502, a new non-ergot dopanineagonist, reduces prolactinoma size in man. Clin Endocrinol1990; 33: 307-16.
3 Khalfallah Y, Claustrat B, Grochowicki M, Flocard F, HorlaitS, Serusclat P, et al. Effects of a new prolactin inhibitor, CV205-502, in the treatment of human macroprolactinomas.JClinEndocrinolMetab 1990; 71: 354-9.
4 Serri 0, Beauregard H, Lesage J, Pedneault I, Comtois R,Jilwan N, et al. Long term treatment with CV 205-502 inpatients with prolactin-secreting pituitary macroadenomas.J Clin Endocrinol Metab 1990; 71: 682-7.
5 Vance ML, Lipper M, Klibanski A, Biller BMK, Samaan NA,Molitch ME. Treatment of prolactin-secreting pituitarymacroadenomas with the long-acting non-ergot dopamineagonist CV 205-502. Ann Intern Med 1990; 112: 668-73.
6 Van't Verlaat JW, Croughs RJM, Brownell J. Treatment ofmacroprolactinomas with a new non-ergot, long-actingdopaminergic drug CV 205-502. Clin Endocrinol 1990; 33:619-24.
7 Crottaz B, Uske A, Reymond MJ, Rey F, Siegel RA, BrownellJ, et al. CV 205-502 treatment of macroprolactinomas.J7EndocrinolInvest 1991; 14: 757-62.
8 Duranteau L, Chanson P, Lavoinne A, Lubetzki J, KuhnJMS. Effect of the new dopaminergic agonist CV 205-502on plasma prolactin levels and tumour size in bromocriptine-resistant prolactinomas. Clin Endocrinol 1991; 34: 25-9.
9 Grochowicki M, Vighetto A, Berquet S, Khalfallah Y, SassolasG. Pituitary adenomas: automated static perimetry andGoldmann perimetry. A comparative study of 345 visualfield charts. BrJ Ophthalmol 1991; 75: 219-21.
10 Bevan JS, Webster J, Burke CW, Scanlon MF. Dopamineagonists and pituitary tumour shrinkage. Endocrine Rev1992; 13: 22040.
11 Lawton NF. Prolactinomas: medical or surgical treatment?QJ MedNew Series 1987; 64: 557-64.
788 on 24 December 2007 bjo.bmj.comDownloaded from