ophthalmic dosage form: eye drops & ointment
TRANSCRIPT


Contents
Introduction
Anatomy and physiology of the eye
Mechanism of ocular absorption
Factors affecting intraocular bioavailability
Approaches to improve ocular drug delivery
Classification of ocular drug delivery systems
Eye drops
Eye ointment

Introduction
• Ophthalmic preparations are specialized dosage formsdesigned to be instilled onto the external surface of the eye(topical) or administered inside the eye (intraocular).
• The purpose may be therapeutic, prophylactic or palliative.
• The most commonly employed ophthalmic dosage formsare solutions, suspensions, and ointments.
• The newest dosage forms for ophthalmic drug delivery are: gels, gel-forming solutions, ocular inserts , intravitrealinjections and implants.

Anatomy & physiology of EyeHuman eye
Diameter 23 mm
Consist 3 layes-
1. Outermost coat :
The clear,
transparent cornea
and the white,
opaque sclera.
2. Middle layer :
The iris anteriorly,
the choroid
posteriorly, and
the ciliary body at
the intermediate
part.
3. Inner layer :
Retina (extension
of CNS).

The Cornea:
The cornea is transparent and allows light to enter the eye. It is a
powerful refracting surface, providing much of the eye's focusing
power.
Epithelium-stroma-endothelium (fat-water-fat structure).
Penetration of the drug depends on oil-water partition coefficient.
The sclera: The protective outer layer of the eye, referred to as the
“white of the eye” and it maintains the shape of the eye.
The choroids is the second layer of the eye and lies between the sclera
and the retina. It contains the blood vessels that provide nourishment to
the outer layers of the retina.
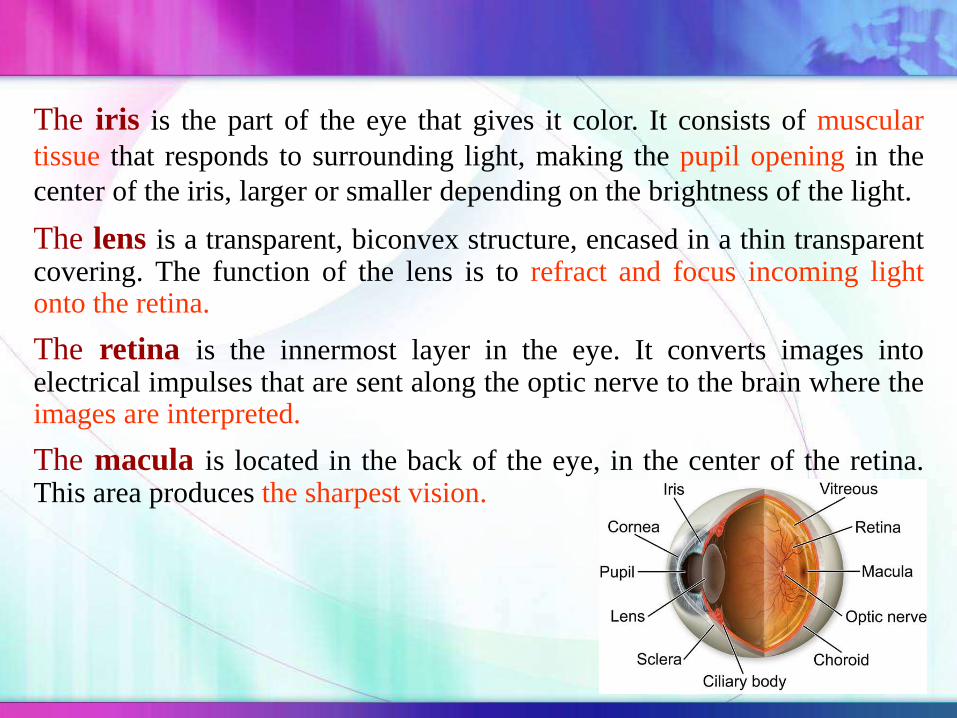
The iris is the part of the eye that gives it color. It consists of muscular
tissue that responds to surrounding light, making the pupil opening in the
center of the iris, larger or smaller depending on the brightness of the light.
The lens is a transparent, biconvex structure, encased in a thin transparentcovering. The function of the lens is to refract and focus incoming lightonto the retina.
The retina is the innermost layer in the eye. It converts images intoelectrical impulses that are sent along the optic nerve to the brain where theimages are interpreted.
The macula is located in the back of the eye, in the center of the retina.This area produces the sharpest vision.

The inside of the eyeball is divided by the lens into two fluid-filledsections.
The larger section at the back of the eye is filled with a colorlessgelatinous mass called the vitreous humor.
The smaller section in the front contains a clear, water-like materialcalled aqueous humor.
The conjunctiva is a mucous membrane that begins at the edge of thecornea and lines the inside surface of the eyelids and sclera, whichserves to lubricate the eye.
Lacrimal glands
Secrete tears & wash foreign bodies.
Moistens the cornea & prevent
from drying out.conjunctiva

Non-Corneal Absorption
Penetration across Sclera & Conjuctiva into Intra Ocular tissues
Non-Productive: because penetrated drug is
absorbed by general circulation
Corneal Absorption
Outer Epithelium: rate limiting barrier, with
pore size 60å, Only access to small ionic & lipohillic molecules.
Trans cellular transport: transport between corneal epithelium &
stroma.
Mechanism of ocular absorption

Corneal absorption
Poor Bioavailability
Protective mechanism (short
residence time)
Blinking
Reflex lacrymation,
Nasolacrimal drainage
Anatomy of eye
Barrier properties of cornea

Factors affecting drug availability:
1. Rapid solution drainage by gravity, induced lachrymation, blinking
reflex, and normal tear turnover.
The normal volume of tear = 7 µl
The blinking eye can accommodate a volume of up to 30 µl without
spillage
The drop volume = 50 µl
2. Superficial absorption of drug into the conjunctiva and sclera and rapid
removal by the peripheral blood flow

3. Low corneal permeability (act as lipid barrier)
In general:
-Transport of hydrophillic and macromolecular drugs occurs
through scleral route.
-Lipophillic agents of low molecular weight follow transcorneal
transport by passive diffusion.
4. Metabolism
Enzymatic biotransformation
Esterases, oxidoreductases, Peptidases, Glucuronide
Sulfate transferases, Lysosomal enzymes.


1. Viscosity enhancers
2. Eye ointments
3. Gel
4. Prodrug
5. Penetration enhancers
6. Liposomes
7. Niosomes
8. Nanosuspension
9. Microemulsion
10. Nanoparticles/nanospheres
11. In situ-forming gel
Approaches to improve ocular drug delivery

Enhancement of bioavailability
1. Increase in viscosity of formulation leads to decrease in drainage.
2. Slows elimination rate from the precorneal area and enhance contact
time.
3. Generally hydrophilic polymers, eg. Methyl cellulose, polyvinyl
alcohols, polyacrylic acids, sodium carboxy methyl cellulose,
carbomer are used.
4. A minimum viscosity of 20 cp is needed for optimum corneal
absorption.

Use of penetration enhancers
1. Substances which increases the permeability characteristics of the
cornea by modifying the integrity of corneal epithelium are known
as penetration enhancers.
2. Act by increasing corneal uptake by modifying the integrity of
the corneal epithelium.
Modes of actions
1. By increasing the permeability of the cell membrane.
2. Acting mainly on tight junctions.
e.g. dimetylsulfoxide(DMSO), laurocapram.
Prodrugs
1. Prodrugs enhance corneal drug permeability through modification
of the hydrophilicity or lipophilicity of the drug.
2. The method includes modification of chemical structure of the drug
molecule, thus making it selective, site specific and a safe ocular
drug delivery system.
3. Drugs with increased penetrability through prodrug formulations are
epinehrine, phenylephrine, timolol, pilocarpine.

USE OF MUCOADHESIVES IN OCULAR DRUG DELIVERY
Polymeric mucoadhesive vehicle: Retained in the eye due to
noncovalent bonding with conjuctival mucine.
Mucine is capable of picking of 40-80 times of weight of water.
Thus prolongs the residence time of drug in the conjuctival sac.
Mucoadhesives contain the dosage form which remains adhered to
cornea until the polymer is degraded or mucus replaces itself.
Types
1. Naturally Occurring Mucoadhesives - Lectins, Fibronectins
2. Synthetic Mucoadhesives - PVA, Carbopol, carboxy methyl
cellulose, cross-linked polyacrylic acid.
Phase Transition System
1. Solution that are liquid in the container and thus can be instilled as
eye drop becomes gel on contact with the tear fluid and provide
increased contact time with the possibility of improved drug
absorption and increased duration of therapeutic effect.
2. Liquid-gel phase transition-dependent delivery system vary according
to the particular polymer employed and their mechanism for
triggering the transition to a gel phase in the eye take advantage of
change in temperature, pH, ion sensitivity, or lysozymes upon
contact with tear fluid.
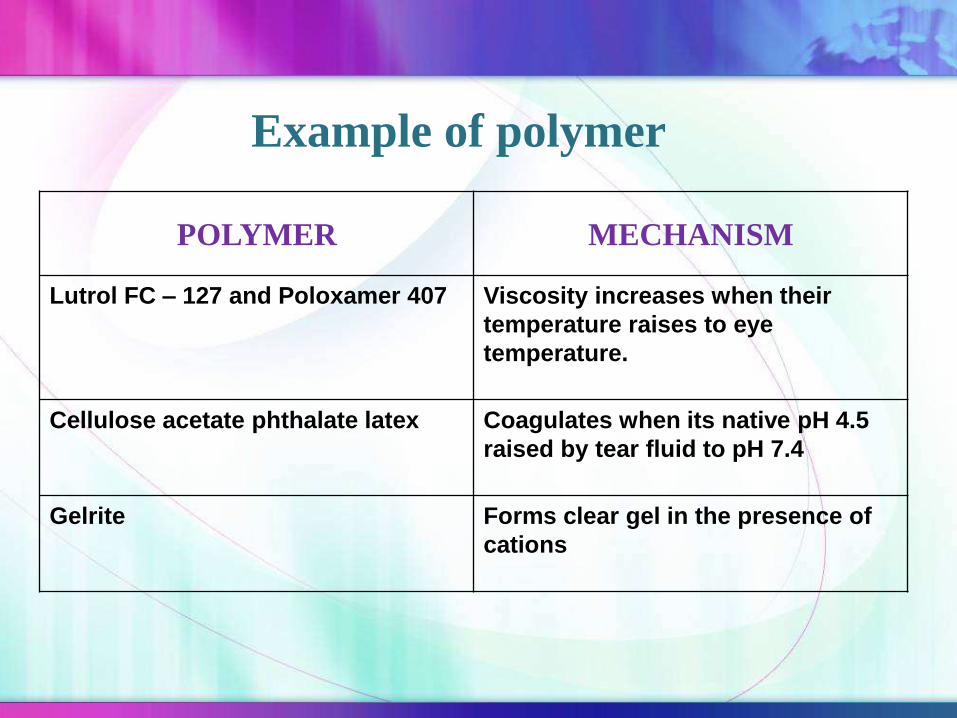
POLYMER MECHANISM
Lutrol FC – 127 and Poloxamer 407 Viscosity increases when their
temperature raises to eye
temperature.
Cellulose acetate phthalate latex Coagulates when its native pH 4.5
raised by tear fluid to pH 7.4
Gelrite Forms clear gel in the presence of
cations
Example of polymer

LIQUIDS
Solutions
Suspensions
Powders for reconstitution
Sol to gel systems
SEMISOLIDS
Ointments
Gels
SOLIDS
Ocular inserts
Contact lenses
INTRAOCULAR DOSAGE FORM
Injections
Irrigating solutions
Implants
Classification of Ocular Drug Delivery System

Ideal Ophthalmic Delivery System
Good corneal penetration.
Prolong contact time with corneal tissue.
Simplicity of instillation for the patient.
Non irritant and comfortable form.
Appropriate rheological properties.
Inert and stable.

Eye dropsEye drops are sterile solutions, suspensions or emulsions intended for
instillation in the eye.
Solutions are Manufactured by dissolution of the active ingredients and
the excipients into all portion of water and sterilization of this solution
done.
If the drug is not sufficiently soluble, it can be formulated as a
suspension.
Topical ophthalmic emulsions generally are prepared by dissolving or
dispersing the active ingredient(s) into an oil phase, adding suitable
emulsifying agent and mixing with water vigorously to form a uniform
oil-in-water emulsion.

Ophthalmic products contains drugs of various categories
including –
Miotics e.g. Pilocarpine HCl
Mydriatics e.g. Atropine
Anti-inflammatories e.g. Corticosteroids
Anti-infectives (antibiotics, antivirals and antibacterials)
Anti-glucoma drugs e.g. Pilocarpine Hcl
Diagnostic drugs e.g. Sodium fluorescein
Anesthetics e.g. Tetracaine
formulation

Eye drop should be sterile and should contain
preservatives to avoid microbial contamination when
container is open.
•The preservative for ophthalmic use includes-
benzalkonium chloride
chlorbutanol
phenylmercuric acetate
phenylmercuric nitrate etc.

Eye drops are sterilized by autoclaving at 121°C for 15
minutes.
• Bacterial filters are used to avoid thermal degradation.
e.g.- preservative chlorbutanol hydrolyzes at high
temperature.
The order of surfactant toxicity is :
anionic > cationic >> nonionic .
• several nonionic surfactants are used in relatively low
Concentration to aid in dispersing steroids in suspensions
and to achieve or to improve solution clarity.
• Those principally used are the sorbitan ether esters of
oleic acid ( polysorbate or tween 20 and 80 ).

pH adjustment is very important as pH affects-1- To render the formulation more stable
2- The comfort, safety and activity of the product.Eye irritation
increase in tear fluid secretion
Rapid loss of medication.
3- To enhance aqueous solubility of the drug.
4- To enhance the drug bioavailability
5- To maximize preservative efficacy
Note: If buffers are required there capacity is controlled to be as low as possible( low buffer capacity) thus enabling the tear to bring the pH of the eye back to thephysiological range .

Lachrimal fluid is isotonic with blood having an isotonicity value
Corresponding to that of 0.9% NaCl solution
e.g. Mannitol, NaCl , KCl buffer.

Polyvinyl alcohol, methylcellulose, hydroxypropyl
methylcellulose, hydroxyethylcellulose, and carbomers,are
commonly used to increase the viscosity of solution and
suspensions (to retard the rate of setting of particles) They increase
the ocular contact time , there by decreasing the drainage rate,
increase the mucoadhesiveness and Increasing the bioavailability .
Disadvantage : produce blurring vision as when dry, form a dry
film on the eye lids. make filteration more difficult .
commercial viscous vehicles are :
1. polyvinyl alcohol (liquifilm)
2. hydroxypropyl methylcellulose (isopto)
Ophthalmic drop (using purifies water USP) as the solvent.
Purified water meeting USP standards may be obtained by :
Distillation, deionization, or reverse osmosis.
Oils have been used as vehicles for several topical eye drops
products that are extremely sensitive to moisture.
When oils are used as vehicles in ophthalmic fluids, they must
be of the highest purity.
Not for injection. For external use only. Shake well before use
(if it is suspension).

Administration:-Pull down the eyelid.
-Tilting the head backwards.
-Look at the ceiling after the tip is pointed close to the lower cul-de-
sac.
-Apply a slight pressure to the rubber bulb
or plastic bottle to allow a drop to fall into
the eye.
-Do not squeeze lids.
To prevent contamination:-Clean hands
-Do not touch the dropper tip to the eye and surrounding tissue

Eye drops have been packaged almost entirely in plastic dropper
bottles
The main advantage of the Drop-Trainer are:
- Convenience of use by the patient
- Decreased contamination potential
- Lower weight
- Lower cost
The plastic bottle and dispensing tip is made of low-density
polyethylene (LDPE) resin, which provides the necessary
flexibility and inertness.
The cap is made of harder resin than the bottle.

A special plastic ophthalmic package made of polypropylene is
introduced. The bottle is filled then sterilized by steam under
pressure at 121°C.
Powder for reconstitution use glass containers , owing to their
heat-transfer characteristics, which are necessary during the freeze-
drying processes.
The glass bottle is made sterile by dry-heat or steam autoclave
sterilization.
Amber glass is used for light-resistance.

Dosage form Advantages Disadvantages
Solutions 1. Convenience
2. Usually do not interfere
with vision of patient.
1. Rapid precorneal elimination.
2. Non sustained action.
3. To be Administered at frequent
intervals.
Suspension 1. Patient compliance.
2. Best for drug with slow
dissolution.
3. Longer contact time
1. Drug properties decide
performance loss of both
solutions and suspended
particles.
2. Irritation potential due to the
particle size of the drug.
Emulsion 1. Prolonged release of
drug from vehicle
1. Blurred vision.
Advantages and Disadvantages of Eye Drops

Prolongation of drug contact time with the external ocular
surface can be achieved using ophthalmic ointment vehicle.
The ointment base is sterilized by heat and appropriately
filtered while molten to remove foreign particulate matter.
The ointment base selected for an ophthalmic ointment must be
nonirritating to the eye and must permit the diffusion of the active
ingredient throughout the secretions bathing the eye.
EYE ointment
Ointment base is sterilized by heat and filtered while molten
to remove foreign particulate matter.
It is then placed into a sterile steam jacketed
to maintain the ointment in a molten state and excipients
are added
The entire ointment may be passed
through a previously sterilized colloid mill

Packaging:
Ophthalmic ointment are packaged in :
1.Small collapsible tin tube usually holding 3.5g of product. the pure tin
tube is compatible with a wide range of drugs in petrolatum-based
ointments.
2.Aluminum tubes have been used because of their lower cost and as an
alternative of tin.
3.Plastic tubes made from flexible LDPE resins have also been
considered as an packaging material.
•Filled tubes may be tested for leakers.
•The screw cap is made of polyethylene or polypropylene.
•The tube can be a source of metal particles and must be cleaned
carefully before sterilization (by autoclaving or ethylene oxide).
Advantages
1. Longer contact time and greater storage stability.
2. Flexibility in drug choice.
3. Improved drug stability.
Disadvantages
1. Sticking of eyes lids.
2. Blurred vision.
3. Poor patient compliance
4. Interfere with the attachment of new corneal epithelial cells to
their normal base.
5. Matting of eyelids

Evaluation of the ophthalmic product is done by
following tests:
1. Sterility Test
2. Clarity Test
3. Leakage Test
4. Metal particles in ophthalmic ointment
Evaluation tests

Sterility Tests :
Ophthalmic products should be free from anaerobic and aerobic bacteria and fungi.
Sterility tests are therefore performed by the:
1. Membrane filtration method.
2. Direct - inoculation method.
In the Membrane filtration method :
• A solution of test product (1%) is prepared in isopropyl myristate and allowed to penetrate through cellulose nitrate filter with pore size 0.45 μ m.
• If necessary, gradual sunction or pressure is applied to aid filtration.
The membrane is then washed three times with 100 - ml quantities of sterile diluting and rinsing fluid and transferred aseptically into fluid thioglycolate medium (FTM) and soybean – casein digest medium (SBCD) .
The membrane is finally incubated for 14 days.
Growth on FTM indicates the presence of anaerobic and aerobic bacteria.
Growth on Soybean casein digest medium indicates the presence of fungi and aerobic bacteria.
Absence of any growth in both these media establishes the sterility of the product.

In the Direct - inoculation technique :
1 part of the product is diluted with 10 parts of sterile diluting and
rinsing fluid with the help of an emulsifying agent .
Incubate in Fluid thioglycolate medium (FTM) and soybean –
casein digest (SCDM) media for 14 days .
In both techniques, the number of test articles is based on the batch
size of the product.
If the batch size is less than 200 the containers, either 5% of the
containers or 2 containers (whichever is greater) are used.
If the batch size is more than 200, 10 containers are used for
sterility testing .

Clarity is tested by visual inspection of containers under light and
against a black and white background.
Instrumental methods of evaluation is based on the principles of
light scattering, light absorption and electrical resistance which are
used to count particle and particle size distribution.
Unwanted mobile insoluble matter other than gas bubbles are
present in the given product are detected.
It may be dangerous when the particle size is larger than R.B.C.
and may block the blood vessel.
Clarity Test:

This test is mandatory for ophthalmic products, which evaluates
the intactness of the ointment tube and its seal.
Ten sealed containers are selected, and their exterior surfaces are
cleaned.
They are horizontally placed over absorbent blotting paper .
maintained at 60 ± 3 ° C for 8 h.
The test passes if leakage is not observed from any container.
If leakage is observed, the test is repeated with an additional 20
tubes.
The test passes if not more than 1 container shows leakage out of 30
tubes .
Leakage test :

This test is required only for ophthalmic ointments.
The presence of metal particles will irritate the corneal or
conjunctival surfaces of the eye.
It is performed using 10 ointment tubes.
The content from each tube is completely removed onto a clean
60 - mm - diameter Petri dish which possesses a flat bottom.
The lid is closed and the product is heated at 85 °C for 2 hours.
Once the product is melted and distributed uniformly, it is cooled
to room temperature.
The lid is removed after solidification.
The bottom surface is then viewed through an optical microscope
at 30× magnification.
Test for Metal Particles:

The viewing surface is illuminated using an external light source positioned at 45 ° on the top.
The entire bottom surface of the ointment is examined, and the number of particles 50 μm or above are counted using a calibrated eyepiece micrometer.
The USP recommends that the number of such particles in 10 tubes should not exceed 50, with not more than 8 particles in any individual tube.
Limits are not met, the test is repeated with an additional 20 tubes.
In this case, the total number of particles in 30 tubes should not
exceed 150, and not more than 3 tubes are allowed to contain more
than 8 particles, the test passes.
•Carter S.J., “Dispensing for pharmaceutical by Cooper
and gunn”, CBS Publisher. p.p.634-661
•Jain N.K., Gupta G.D. “Modern dispensing pharmacy”,
Published by Pharma book syndicate. p.p. 13.3-14.9
•Mithal B.M., “Text of pharmaceutical formulation”,
Vallabh prakashan. p.p. 268-278
•Felton L., “Remington’s essential of pharmaceutics”,
published by pharmaceutical press. p.p.541-562
References