operating policy for the continuing healthcare and complex
TRANSCRIPT
Page 1 of 101
Operating Policy for the Continuing Healthcare and Complex Care Team
Including arrangements for:
Continuing Healthcare, NHS-Funded Nursing Care (FNC), Complex Care,
Mental Health and Rehabilitation Service Provision.
Image taken from the National Framework - https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213137/National-Framework-for-NHS-CHC-NHS-FNC-JUN-2016.pdf
Page 2 of 101
DOCUMENT CONTROL SHEET
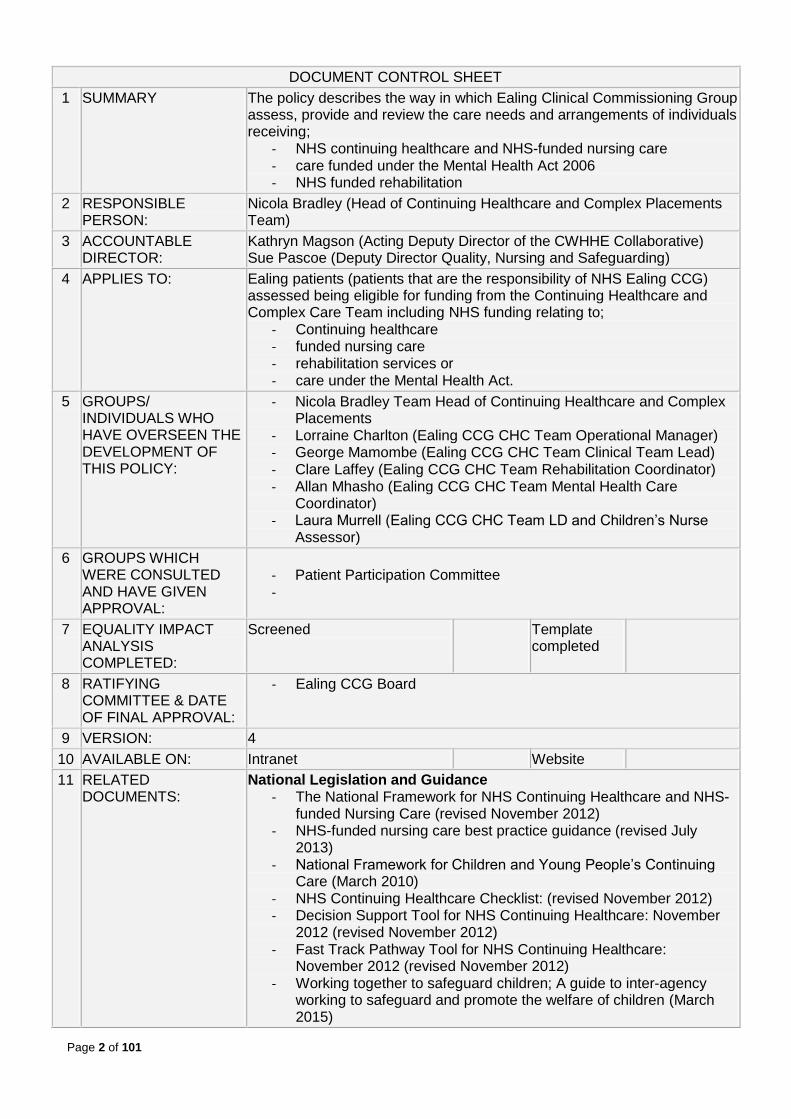
1 SUMMARY The policy describes the way in which Ealing Clinical Commissioning Group assess, provide and review the care needs and arrangements of individuals receiving;
- NHS continuing healthcare and NHS-funded nursing care - care funded under the Mental Health Act 2006 - NHS funded rehabilitation
2 RESPONSIBLE PERSON:
Nicola Bradley (Head of Continuing Healthcare and Complex Placements Team)
3 ACCOUNTABLE DIRECTOR:
Kathryn Magson (Acting Deputy Director of the CWHHE Collaborative) Sue Pascoe (Deputy Director Quality, Nursing and Safeguarding)
4 APPLIES TO: Ealing patients (patients that are the responsibility of NHS Ealing CCG) assessed being eligible for funding from the Continuing Healthcare and Complex Care Team including NHS funding relating to;
- Continuing healthcare - funded nursing care - rehabilitation services or - care under the Mental Health Act.
5 GROUPS/ INDIVIDUALS WHO HAVE OVERSEEN THE DEVELOPMENT OF THIS POLICY:
- Nicola Bradley Team Head of Continuing Healthcare and Complex Placements
- Lorraine Charlton (Ealing CCG CHC Team Operational Manager) - George Mamombe (Ealing CCG CHC Team Clinical Team Lead) - Clare Laffey (Ealing CCG CHC Team Rehabilitation Coordinator) - Allan Mhasho (Ealing CCG CHC Team Mental Health Care
Coordinator) - Laura Murrell (Ealing CCG CHC Team LD and Children’s Nurse
Assessor)
6 GROUPS WHICH WERE CONSULTED AND HAVE GIVEN APPROVAL:
- Patient Participation Committee -
7 EQUALITY IMPACT ANALYSIS COMPLETED:
Screened Template completed
8 RATIFYING COMMITTEE & DATE OF FINAL APPROVAL:
- Ealing CCG Board
9 VERSION: 4
10 AVAILABLE ON: Intranet Website
11 RELATED DOCUMENTS:
National Legislation and Guidance - The National Framework for NHS Continuing Healthcare and NHS-
funded Nursing Care (revised November 2012) - NHS-funded nursing care best practice guidance (revised July
2013) - National Framework for Children and Young People’s Continuing
Care (March 2010) - NHS Continuing Healthcare Checklist: (revised November 2012) - Decision Support Tool for NHS Continuing Healthcare: November
2012 (revised November 2012) - Fast Track Pathway Tool for NHS Continuing Healthcare:
November 2012 (revised November 2012) - Working together to safeguard children; A guide to inter-agency
working to safeguard and promote the welfare of children (March 2015)

Page 3 of 101
- The Delayed Discharges (Continuing Care) Directions 2013 - Who pays? Determining responsibility for payments to providers
(August 2013) - Rules and guidance for clinical commissioning groups - Mental Capacity Act 2005 - Mental Health Act 2009 - The Care Act 2014 - The National Health Service Commissioning Board and Clinical
Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012
- NHS Ealing Continuing Healthcare Refreshed Redress Guidance (April 2015)
- Better Care Closer to Home. Our three year strategy for coordinated, high quality care out of hospital 2012-2015 NHS Ealing Clinical Commissioning Group(2012)
- Policy paper; 2010 to 2015 government policy: choice in health and social care (revised May 2015)
- Policy paper 2010 to 2015 government policy: long term health conditions (revised May 2015)
Local Documents
- Learning Disability Section 75 arrangements - Continuing Healthcare Funding Protocol - Personal Health Budget Policy and Procedure - Information Sharing Policy - Pan London Safeguarding Policy (in Draft) - NHS Ealing CCG Safeguarding Policy (in Draft)
12 DISSEMINATED TO: NHS Ealing CCG, CNWL, Continuing Healthcare Team, London Borough of Ealing, Patients, Voluntary Sector Groups (MIND, Age UK)
13 DATE OF IMPLEMENTATION:
- 1st April 2016
14 DATE OF NEXT FORMAL REVIEW:
- July 2017
Version Date Released Change Notice
Pages Affected
Remarks
0.1 Internally Draft Comments from Rehab Co-ordinator
0.2 Internally Draft Comments from LD Nurse Assessor
0.3 Internally Draft Comments from Mental Health Care Co-ordinator
0.4 Internally Draft

Page 4 of 101
1. Index
Contents 1. Index ............................................................................................................................................ 4 2. Introduction to this policy.............................................................................................................. 7
1.1 Context ................................................................................................................................. 7 1.2 Contact Details for the Team ................................................................................................ 7 1.3 Abbreviations and Meaning................................................................................................... 7 1.4 Other inter-relating policies ................................................................................................... 9 1.5 Responsible Commissioner .................................................................................................. 9 1.6 Safeguarding (Adults and Children) ...................................................................................... 9 1.7 Consent .............................................................................................................................. 10 1.8 Mental Capacity .................................................................................................................. 10 1.9 Depravation of Liberty Safeguards (DoLS) .......................................................................... 11 1.10 Quality Assurance ............................................................................................................... 11 1.11 Duty of Candor.................................................................................................................... 11 1.12 Training............................................................................................................................... 12 1.13 Timeframes ......................................................................................................................... 13 1.14 Team Structure and Responsibilities ................................................................................... 13 1.15 Changes to Policy and Protocol .......................................................................................... 14 1.16 Equality Impact Assessment ............................................................................................... 14 1.17 Information Governance ..................................................................................................... 14
3. Definitions – NHS Continuing Healthcare and Funded Nursing Care ......................................... 15 3.1. Adult NHS continuing Healthcare - Definition ...................................................................... 15 3.2. Adult NHS-Funded Nursing Care (FNC) Definition .............................................................. 15 3.3. Equalities Impact Assessment ............................................................................................ 15
4. The CHC Assessment Process for Adults .................................................................................. 16 4.1. Referral ............................................................................................................................... 17 4.2. Who is eligible for a continuing healthcare assessment? (Checklist) ................................... 17
4.2.1. Checklist - to establish whether a full assessment is required ..................................... 17
4.2.2. When is a full assessment required? ........................................................................... 18
4.2.3. Outcome ...................................................................................................................... 18
4.2.4. Ratification of the Checklist outcome ........................................................................... 18
4.2.5. Informing the outcome following a checklist ................................................................. 19
4.2.6. Keeping a record of the checklist findings .................................................................... 19
4.2.7. What happens if the individual disagrees with the checklist outcome? ......................... 19
4.3. Continuing Healthcare Assessment .................................................................................... 19 4.3.1. Patients’ requiring rehabilitation ................................................................................... 20
4.3.2. Arranging a Continuing Healthcare Assessment .......................................................... 20
4.3.3. Establishing Capacity................................................................................................... 20
4.3.4. Establishing the Individual’s needs (Health Needs Assessment) ................................. 20
4.3.5. Decision Support Tool.................................................................................................. 21
4.3.6. Fast Track tool ............................................................................................................. 21
4.3.7. Recommendation (eligible for NHS continuing healthcare?) ........................................ 21
4.4. Determination (Ratification of decision) ............................................................................... 22 4.4.1. Keeping a record regarding eligibility for NHS funding ................................................. 23
4.5. Refusing NHS Continuing Healthcare ................................................................................. 23 4.6. Appeal ................................................................................................................................ 23 4.6.1. Requesting an Appeal ..................................................................................................... 24

Page 5 of 101
4.6.2. Responding to the Request ............................................................................................. 24 4.6.3. Local Review ................................................................................................................... 24 4.6.3.1. Meeting Processs ........................................................................................................ 24 4.6.3.2. Purpose ....................................................................................................................... 25 4.6.3.3. Outcome ...................................................................................................................... 25 4.6.3.4. Informing the Appellant of the Ouctome ....................................................................... 25 4.6.3.5. Minutes ........................................................................................................................ 25 4.6.4. External Review .............................................................................................................. 26 4.6.4.1. Independent Review Panel .......................................................................................... 26 4.6.4.2. Ombudsman ................................................................................................................ 26 4.6.5. Complaints ...................................................................................................................... 26 4.7. Local Authority and Clinical Commissioning Disputes ......................................................... 26
5. Previously Unassessed Periods of Care (PUPoC) ..................................................................... 28 5.1. Determining Eligibility for PUPoC Assessment.................................................................... 28 5.2. Collating Evidence .............................................................................................................. 28 5.3. Care Needs Portrayal ......................................................................................................... 28 5.4. Meeting with the Family ...................................................................................................... 29 5.5. PUPoC Panel ..................................................................................................................... 29 5.6. Continuing Healthcare Panel .............................................................................................. 29 5.7. Outcome Letter ................................................................................................................... 29 5.8. Keeping a Record ............................................................................................................... 29 5.9. Appealing the Decision ....................................................................................................... 29 5.9.1. Local Resolution .............................................................................................................. 29 5.10. Independent Review ........................................................................................................ 30
6. Redress ..................................................................................................................................... 31 7. Commissioning of Care .............................................................................................................. 32
7.1. Funding Principals .............................................................................................................. 32 7.2. Top Up ................................................................................................................................ 33 7.3. Capacity to decide preferred place of residence ................................................................. 33 7.4. Personal Health Budget ...................................................................................................... 34
7.4.1. Options – Types of Personal Health Budget ....................................................................... 34 7.4.2. Access Criteria .................................................................................................................... 35 7.4.3. Exemption Criteria .............................................................................................................. 35 7.4.4. Process to obtain a PHB ..................................................................................................... 35
7.5. Discharge Planning ............................................................................................................. 36 7.6. Commissioned Care (Adults) .............................................................................................. 37 7.7. Nursing Home Placement ................................................................................................... 37
7.7.1. Criteria to establish an appropriate placement .................................................................... 37 7.7.2. Procedure to find a suitable placement ............................................................................... 38
7.8. Homecare Package (Domiciliary Care) ............................................................................... 39 7.8.1. Criteria to access domiciliary care (Care at Home) ............................................................. 39 7.8.2. Risk and environmental Assessments ................................................................................ 40 7.8.3. Memorandum of Understanding for Domiciliary Care Provision .......................................... 40 7.8.4. Termination of home care (domiciliary) provision ................................................................ 40
7.9. Review ................................................................................................................................ 41 8. Transition from Children to Adults’ Services ............................................................................... 42 9. Access to Equipment & Other NHS Services ............................................................................. 43 10. Children and Young People’s Continuing Care ...................................................................... 44
10.1. Objective ......................................................................................................................... 44 10.2. The Continuing Healthcare Pathway for children and young people ................................ 45 10.3. Step 1 - Identification of Children who may be eligible ..................................................... 45 10.4. Step 2 – Assessing Need ................................................................................................ 45 10.5. Step 3 - Recommendation to the panel ........................................................................... 46 10.6. Step 4 – Decision Making ................................................................................................ 47 10.7. Step 5 - Informing the relevant parties ............................................................................. 47 10.8. Step 6 - Appealing the decision ....................................................................................... 47 10.9. Step 7 - Delivering Care .................................................................................................. 48

Page 6 of 101
10.10. Step 8 - Review ............................................................................................................... 49 10.11. Step 9 - Transition to adult services of closure of a package ........................................... 49 10.12. Special Circumstances .................................................................................................... 50
11. Mental health Assessment and Funding Arrangements .......................................................... 51 11.1. Context ............................................................................................................................ 51 11.2. Assessment & Preparation for Panel ............................................................................... 51 11.3. Panel ............................................................................................................................... 52 11.4. Commissioning Placement .............................................................................................. 52 11.5. Review ............................................................................................................................ 52 11.6. Appeal ............................................................................................................................. 53 11.7. Disputes .......................................................................................................................... 53
12. Learning Disability Assessment and Funding Arrangement .................................................... 54 13. Community Bedded General Rehabilitation Service ............................................................... 55
13.1. Rehabilitation Service Pathway ....................................................................................... 55 13.2. Referral Criteria ............................................................................................................... 56 13.3. Acceptance Criteria ......................................................................................................... 56 13.4. Exclusion Criteria ............................................................................................................ 56 13.5. Referral Process ............................................................................................................. 57 13.6. Discharge Process .......................................................................................................... 58
14. APPENDIX ............................................................................................................................. 59 Appendix 1 – CHC history ................................................................................................................. 60 Appendix 2 – Team Structure ........................................................................................................... 61 Appendix 3 – CHC referral form ........................................................................................................ 62 Appendix 4 – Council Brokerage ....................................................................................................... 65 Appendix 5 – Equalities Impact Assessment for NHS continuing Healthcare .................................... 74 Appendix 6 – Community Rehabilitation Referral Form ..................................................................... 75 Appendix 7 – Continuing Healthcare Process (Adults) ...................................................................... 81 Appendix 8 – CHC Older People’s Panel ToR .................................................................................. 82 Appendix 9 – CHC Children Process ............................................................................................... 84 Appendix 10 – Memorandum of Understanding ............................................................................... 85 Appendix 11 – Children’s Panel ToR................................................................................................. 87 Appendix 12 – MH Panel ToR ........................................................................................................... 90 Appendix 13 – Physical Disability and Learning Disability Panel Terms of Reference ....................... 91 Appendix 14 – Children’s Continuing Care Leaflet ............................................................................ 94 Appendix 15 – Information Sheet for Parents/Carers of Children ...................................................... 96 Appendix 16 – Appeal Process Flow ................................................................................................ 98 Appendix 17 – Community Bedded Rehabilitation Discharge Summary ............................................ 99 Appendix 18 – Rehabilitation Referral Pathway .............................................................................. 101

Page 7 of 101
2. Introduction to this policy
This policy describes the way in which NHS Ealing Clinical Commissioning Group (Ealing CCG) will assess, make provision for and review the care of people who have been assessed as eligible for funding from this department. There are 3 areas of funding covered by the Continuing Healthcare and Complex Placements Team (Continuing Healthcare Team) included within this Local Policy Document:
- NHS Continuing Healthcare (CHC) and Funded Nursing Care (FNC) for Adults aged 18 or over
- NHS Continuing Care for Children and Young People - Mental Health - Rehabilitation Services
Each area has been described in a separate section within this document.
1.1 Context Every effort has been made to align this policy with the five clinical commissioning groups within north central London. The CCG has developed and agreed this policy to guide decision making that reflects the preferences of individuals but balances the need for the CCG to commission care that is safe and effective and makes best use of the resources available to the CCG. The policy sets out to ensure that decisions will,
be robust, fair, consistent and transparent. be based on the objective assessment of the patient’s holistic clinical needs, safety and
where appropriate best interests. will have regard for the safety and appropriateness of care packages to those involved in
care delivery. will involve the individual and their family or advocate where possible and appropriate. take into account the need for the CCG to allocate its financial resources in the most cost
effective way whilst supporting patient choice to the extent possible in the light of these constraints.
be consistent with the principles and values of the NHS Constitution. take into account an individual’s needs for both their health and their wellbeing.
1.2 Contact Details for the Team The Team are based in their own offices within the NHS Ealing CCG at the address below:
Continuing Healthcare Team NHS Ealing CCG Level 3 Perceval House 14/16 Uxbridge Road Ealing W5 2HL
Tel: 020 8280 8091 Fax: 020 8280 8189 E: [email protected]
1.3 Abbreviations and Meaning

Page 8 of 101
The following abbreviations are used throughout the document and for the purposes of clarity have been defined below. Copies of all these documents are available from the Team (see 1.2) Continuing Healthcare Or CHC
Abbreviation for ‘NHS funded continuing healthcare’ as determined in accordance with the “National Framework for continuing healthcare and NHS-funded nursing care” (revised 2012)
National Framework
National Framework for continuing healthcare and NHS-funded nursing care” (revised 2012) https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213137/National-Framework-for-NHS-CHC-NHS-FNC-Nov-2016.pdf
Ealing CCG
NHS Ealing Clinical Commissioning Group
Checklist
The NHS Continuing Healthcare checklist is a tool to help practitioners identify people who need a full assessment for NHS Continuing Healthcare. It is applied in line with the National Framework. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213138/NHS-CHC-Checklist-FINAL.pdf
Decision Support Tool
The purpose of the Decision Support Tool is to support the application of the National Framework for NHS Continuing Healthcare and inform consistent decision making. It is used in conjunction with the guidance supplied in the National Framework for NHS Continuing Healthcare. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213139/Decision-Support-Tool-for-NHS-Continuing-Healthcare.pdf
CCG Standing Regulations
The National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012 http://www.nhs.uk/choiceintheNHS/Rightsandpledges/Waitingtimes/Documents/nhs-england-and-ccg-regulations.pdf Typically in reference to NHS Continuing Healthcare – Part 6; Standing rules: NHS Continuing Healthcare and NHS funded nursing care
Funded Nursing Care Practice Guidance
NHS-funded Nursing Care Practice Guide July 2013 (Revised) https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/211256/NHS-funded_Nursing_Care_Best_Practice_Guidance.pdf
Health Needs Assessment
A tool developed by NHS London in conjunction with CCGs to capture evidence of an individual’s care needs. It acts as a prompt for clinicians to consider aspects of an individual and how their needs present.
LHNA_blank.doc
Redress Guidance This guidance from NHS England explains the process to be followed
by CCGs with regards to “refunding” individuals who have paid for care

Page 9 of 101
that were eligible for NHS Continuing Healthcare. The update now reflects guidance from the Parliamentary and Health Ombudsman for all public sector bodies, on calculating interest on redress payments. This It supersedes the previous version. http://www.england.nhs.uk/wp-content/uploads/2015/04/nhs-cont-hlthcr-rdress-guid-fin.pdf
CWHHE Collaborative Collaborative of CCGs in North West London including Chelsea and Westminster, Harrow, Hounslow and Ealing
1.4 Other inter-relating policies This policy does not stand alone and has been created in the spirit of existing legislation and policy. It should be read in conjunction with the documents listed on the Document Control Sheet (pages 1-2) including:
The National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012
The National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care: November 2012 (revised) – for adults and individual’s in transition.
National Framework for Children’s and Young People’s Continuing Care NHS Continuing Healthcare Checklist: November 2012 (revised) Decision Support Tool for NHS Continuing Healthcare: November 2012 (revised) Fast Track Pathway Tool for NHS Continuing Healthcare: November 2012 (revised) The Delayed Discharges (Continuing Care) Directions 2013 Who pays? Determining responsibility for payments to providers (August 2013)
1.5 Responsible Commissioner The CCG is responsible for those patients who have a Ealing General Practitioner (GP) at the time of assessment even if they do not reside in Ealing. If those patients have been placed out of borough, the CCG will be responsible either until death or until they no longer meet the criteria for NHS Continuing Healthcare. However if a patient independently moves out of the borough without the assistance of the CCG then they become the responsibility of the receiving borough. Therefore if a patient is placed in Ealing by another Local Authority (LA), registers with a Ealing GP, and after three months meets the criteria for NHS Continuing Healthcare, then they will be the responsibility of Ealing CCG. The reverse is true of those placed by Ealing LA into another borough.
1.6 Safeguarding (Adults and Children) Local Authorities remain the responsible organisation for coordinating Safeguarding matters. The Care Act 2014 redefines safeguarding and responsibilities Local Authorities have. Ealing Council have published the following page for more information regarding safeguarding: http://www.ealing.gov.uk/info/200050/help_for_adults/147/safeguarding_adults_at_risk There is an existing Policy “Protecting adults at risk: London multi-agency policy and procedures to safeguard adults from abuse” which staff are expected to adhere to. This is currently being revised to reflect changes brought in by the Care Act. A final version anticipated later in 2015. Once approved, this policy will be updated to reflect any necessary changes. The team work closely with the CWHHE Safeguarding leads to ensure that concerns are escalated and risks mitigated appropriately. There is also a draft policy which is due for approval by the governing body later in 2015.

Page 10 of 101
With regards to children, the Continuing Healthcare Team work closely with the Children’s Safeguarding Lead and follow the guidance “Working together to safeguard children; A guide to inter-agency working to safeguard and promote the welfare of children” (March 2015) which can be found in the following location: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/419595/Working_Together_to_Safeguard_Children.pdf The Continuing Healthcare Team will provide information and evidence to the local safeguarding team where concerns about care quality from any provider exist. This will include Local Authorities outside Ealing on occasions. The Continuing Healthcare Service will review existing patients in placements where concerns about care quality arise, and will take appropriate action in conjunction with the local authority to safeguard the patients. Continuing Healthcare staff will undertake training in line with the CWHHE mandatory training policy, (which includes safeguarding) and be familiar with the adult safeguarding process. Once published the revised Safeguarding (local or national) policies must be adhered to. The team and actively partake in Safeguarding proceedings as required. Individual training needs may vary and can be reviewed by the Clinical Team Leader for the Continuing Healthcare Team, who may facilitate further training in conjunction with the CWHHE Safeguarding Lead(s).
1.7 Consent Before any assessment or decision is made regarding an individual, the CCG will establish consent from the individual or their representative.
1.8 Mental Capacity Mental capacity should be ascertained at various stages of this process and must always be assessed based on decision being made at that time. A major placement or treatment decision may accompany the assessment for NHS continuing healthcare. Capacity should always be assumed. If the patient lacks capacity to make a decision and does not have an individual to advocate on their behalf, an Independent Mental Capacity Advocate (IMCA) will be allocated. A best interests decision should made. When making decisions on behalf of an individual, the least restrictive option should always be applied. This policy works in parallel with the Mental Capacity Act 2005 and the National Framework for Continuing Healthcare and NHS-funded nursing care. These documents describe in full the processes that should be applied by the CCG. To avoid repetition, this policy intentionally does not contain full details, as these can be obtained from the relevant sections of the Mental Capacity Act and National Framework. Essentially:
The CCG will support an individual in making the decision as to where they wish to live. However, if concerns remain that an individual does not have the mental capacity to make the decision as to where they live, a mental capacity assessment (as defined in the Mental Capacity Act) will be undertaken.
Where the individual is found to lack capacity to make the decision and there is a personal welfare deputy has been appointed by the Court of Protection under the Mental Capacity Act or a Lasting Power of Attorney with powers extending to healthcare decisions, the CCG will consult with that person and obtain a decision from the appointed person on the preferred outcome.

Page 11 of 101
Where the individual is found to lack capacity to make the decision and there is no individual/organisation appointed to legally act on their behalf with regard to welfare matters, an Independent Mental Capacity Advocate will be instructed.
A best interests meeting will be held and consideration given to the views of the family/carers/representatives.
The CCG will need to consider whether there is a requirement for a deprivation of liberty safeguards (DoLS) authorisation.
1.9 Depravation of Liberty Safeguards (DoLS) The Continuing Healthcare Team may become aware during an assessment that an individual’s liberty may be deprived. In this instance, the Nurse Assessor or relevant professional will advise the provider to make a DoLS referral to Ealing Council. Since 1st April 2013 the Local Authorities hold the Supervisory Body function for Deprivation of Liberty Safeguards. Therefore it is not the role of the CCG to complete assessments in this regard. The onus remains on the Provider to ensure they comply with legislation. During the commissioning process of individual placements, there may be a requirement for the provider to, for example, provide one-to-one observations on an individual. In this instance, the CCG would ordinarily advise the provider of the circumstances where they may be required to make a DoLS application.
1.10 Quality Assurance The team has a dedicated member of staff allocated to work with providers to:
Ensuring a person centered approach to quality assurance framework for services commissioned in nursing homes and homecare.
Support and monitor provider performance to ensure compliance with the Health and Social care Act 2008 (Regulated Activities) Regulations 2011; The Care Act 2014 and The duty of Candour, putting safety at the heart of service delivery.
Work collaboratively with the Ealing Council, CQC and the providers to share intelligence, improve care and support practice and processes.
Coordinate access to appropriate training and support for care staff. Monitor providers to ensure that care regulations are complied with. Offer support to providers to up skill staff to deliver safe and effective practice in order to meet
the needs of the individual. Encourage providers to drive up quality standards within their services. Support providers in constructing and delivering management plans in the instance of provider
failures. Local Authorities hold the overarching responsibility to support providers in financial failure.
Support and monitor provider performance to ensure compliance with the Care Act 2014 and the duty of Candour, putting safety at the heart of service delivery.
The CCG works in partnership with the Local Authority, CQC and providers in this regard.
1.11 Duty of Candor The final report of the Independent Inquiry into the care provided by Mid Staffordshire NHS Foundation Trust was published in February 2013. The inquiry’s Chairman, Mr. Robert Francis QC

Page 12 of 101
made a number of recommendations. One of which recommended that the obligation on healthcare staff to be truthful when things go wrong is currently not taken seriously in all cases. The report called for a statutory Duty of Candour on organisations and individuals to ensure healthcare staff are required to disclose information where an episode of care has resulted in serious harm or death. In response to these recommendations the Department of Health has revised the NHS Standard Contract 2014/15 to include clauses and a quality indicator with regard to the Duty of Candour for all providers of commissioned health services. Candour is defined in the Independent Inquiry report as ‘the volunteering of all relevant information to persons who have or may have been harmed by the provision of services, whether or not the information has been requested and whether or not a complaint or a report about that provision has been made’. However, in relation to an organisation’s commitment to the Duty of Candour, it is about being honest and truthful and making sure that people are told what went wrong and why, apologizing and explaining what will be done to stop it happening again. Principles of the Duty of Candour to be adopted by NHS Ealing CCG NHS Ealing CCG fully supports the Duty of Candour. We place Governance at the top of our agenda not only in the commissioning of high quality and safe care for all our commissioned services but also on ourselves internally. We believe that good governance fosters inward facing scrutiny, honesty and transparency. The Team continually strive to assure ourselves that as commissioners we are open and transparent in the business we do and all our providers are open, honest and transparent in all contact with patients and the public. Our accountability and responsibility to the people of NHS Ealing CCG in relation to the provision of health services The people of NHS Ealing CCG expect and deserve that as a commissioner of health services we must be honest, open and truthful in all our dealings with them. We listen to the views of patients and the public through a number of public engagement events. We share our operational plans that set out a commitment to commission healthcare services that will fulfil the needs of the people of Ealing
1.12 Training All staff receive training beyond the legal requirements (i.e. Health and Safety, Fire, Moving and Handling, Safeguarding Adults and Children, Equality and Diversity, Infection Control etc.); these generic training modules are monitored and enforced by the Assistant Director for Operations and Governance. Nursing Staff come with transferrable assessment skills required to complete NHS Continuing Healthcare Assessments. Continuing Healthcare Training is offered on a regular basis to educate staff about the processes, familiarise staff with existing, new and developing policy (e.g. Mental Capacity Act and Direct Payments Regulations) and provide an opportunity for staff to familiarise themselves with the relevant documents. The process of training a new member of staff involves the following. Development to the next stage will only take place once the individual demonstrates competence in the training component.
- Read the department’s Operational Policy (this document) and (Internal Operating Protocols) - Read the National Framework (see section 1.8 for an electronic link, or a copy can be
obtained from the Continuing Healthcare Team) , make notes and highlight crucial sections for ease of reference.
- Familiarise themselves with London Health Needs Assessment (see section 1.8 for an electronic link), make notes and highlight crucial sections for ease of reference.

Page 13 of 101
- Read the Decision Support Tool (see section 1.8 for an electronic link), in full alongside instructions make notes and highlight crucial sections for ease of reference.
- Read the Checklist (see section 1.8 for an electronic link) in full alongside instructions, make notes and highlight crucial sections for ease of reference.
- Undertake the e-learning module on NHS Continuing Healthcare - Shadow 3 assessments with a colleague. Following the 3rd assessment, write up all
documentation as part of the process. - Take the lead on 2 assessments, complete all paperwork, present the case to the relevant
panel with their colleague shadowing them. - Take part in regular clinical supervision and review - Take part in case study learning sessions - Receive additional support when required.
In addition staff partake in training relevant to their role which is arranged when needed. Recent training includes the Mental Capacity Act and Care Act.
1.13 Timeframes The following are considered good practice timeframes to achieve: The National Framework makes clear the following timeframes should be aimed for:
28 days for a decision – this is the length of time from when the CCG is aware that a full continuing healthcare assessment is required, e.g. from a completed Checklist to the determination being made
Continuing Healthcare reviewed 3 months after the initial decision and
Yearly (every 12 months) thereafter Local timeframes include:
Fast-track applications - decisions made within 24 hours (working days only)
Length of time from between ratification and the outcome letter being sent; 3 working days
1.14 Team Structure and Responsibilities The organisational and reporting structure of the NHS Ealing CCG Continuing Healthcare Team has been included in Appendix 2. The Continuing Healthcare and Complex Placements Team contains the following:
Head of Continuing Healthcare – responsible for the overall management of the department processes in Ealing. Manages the team and develops services across Ealing. Responsible for the quality of the services provided, commissioning arrangements, safeguarding, complaints and appeals. CHC Business Support (Admin) – Provides support to the Head of Continuing Healthcare and Complex Placements. Co-ordinates the PUPoC process. Service Coordinator – Organises continuing healthcare assessments, manages the generic email box, manages incoming and outgoing mail. Is the first point of contact when someone contacts the team. PUPoC Administrator – Responsible for collating evidence for PUPoC cases (section
Page 14 of 101
Operational Manager - Responsible for the day to day running of the Team, ensuring compliance with local and national policies, recruitment. Development of Personal Health Budgets and Integrated Personalisation. Clinical Lead Nurse – Manages the clinical staff. Responsible for ensuring the consistency and quality of assessments completed by the team. Co-chair of the Older Peoples’ Continuing Healthcare Panel. Quality Assurance Nurse - Responsible for ensuring the quality of care provided within care homes in Ealing. Highlighting concerns to the Head of Continuing Healthcare and Quality and Safety Committee. Closely working with the Safeguarding Team. Nurse Assessors – Responsible for leading the continuing healthcare assessment process in the community. Case Management of individuals receiving continuing healthcare (Learning Disability, Children’s and Physical Disability only). Active participation in Safeguarding matters including case conferences and strategy meetings. Mental Health Case Manager - Case Management of individuals funded by the service – continuing healthcare, mental health act (for example sections, forensic step-down, aftercare) Care Home Selection – Brokers responsible for finding appropriate nursing home placements to meet the needs for those eligible for NHS continuing healthcare. Invoice validation, contract approval, quality monitoring. Ealing Council Homecare Team - Brokers responsible for finding appropriate home care providers to meet the needs or those eligible for NHS continuing healthcare.
1.15 Changes to Policy and Protocol NHC Continuing Healthcare is subject to Case Law, Recommendations from the Ombudsman and Independent Review Panel. Scope to improve policy and procedures within Ealing CCG is paramount to the Continuing Healthcare Team and the individuals that the team serve. From time to time findings will impact on local policy and procedures, and hence this document will be reviewed every two years and at times when required. In a weekly meeting, the team review performance, hold clinical supervision and case studies, along with revising standard operating procedures in a strive to deliver an exemplary service.
1.16 Equality Impact Assessment A formal assessment is required in respect of all new service and policy proposals to ensure that vulnerable and minority groups are not disadvantaged in their access to and experience of services provided.
1.17 Information Governance The Continuing Healthcare Team is expected to comply with Information Governance requirements. For this reason, all paper files are stored in locked cupboards and a “clear desk” policy is in place. A copy of the CCG’s information governance policy can be obtained from the Team (see 1.2 above).
Page 15 of 101
3. Definitions – NHS Continuing Healthcare and Funded Nursing Care
Funding arrangements for on-going care is a complex and highly sensitive area, which can affect individuals at a very vulnerable stage of their lives. To see a brief history of NHS continuing healthcare, please refer to appendix 1. Since October 2007 There has been national guidance available which sets out a single, National Framework for determining eligibility for NHS continuing healthcare and for NHS-funded nursing care. The purpose of the National Framework is to provide for fair and consistent access to NHS funding across England, regardless of location, so that individuals with similar needs should have an equal likelihood of getting all of their health and nursing care provided free of charge.
3.1. Adult NHS continuing Healthcare - Definition NHS continuing healthcare is the name given to a care funded by the NHS for individuals outside of hospital who have on-going health care needs. It can be funded in any setting, including an individual’s own home or in a care home. NHS continuing healthcare is free, unlike support provided by local authorities which is means tested and for which there may be a financial charge depending on an individual’s income and savings. Eligibility for NHS continuing healthcare is based on an individual’s assessed health needs. The diagnosis of a particular disease or condition is not in itself a determinant of eligibility for NHS continuing healthcare. As part of the assessment, the CCG will consider the nature, intensity, complexity and unpredictability of an individual’s condition in deciding whether they have a primary health need. Home care If eligible for NHS continuing healthcare and provision is made in the individual’s own home, the NHS will pay for healthcare (e.g. services from a community nurse or specialist therapist) and associated social care needs (e.g. personal care and domestic tasks, help with bathing, dressing, food preparation). If In a care home, the NHS also pays care home fees, including board and accommodation.
3.2. Adult NHS-Funded Nursing Care (FNC) Definition For individuals in care homes with nursing, registered nurses are usually employed by the care home itself and, in order to fund this nursing care, the NHS makes a payment direct to the care home. This is called ‘NHS-funded nursing care’ (FNC) and is a standard rate contribution towards the cost of providing registered nursing care for those individuals who are eligible. Registered nursing care can involve many different aspects of care. It can include direct nursing tasks as well as the planning, supervision and monitoring of nursing and healthcare tasks to meet your needs. The process for determining eligibility for FNC is described within the policy. Essentially if an individual;
is resident within a care home registered to provide nursing care and they have been assessed for and do not qualify for NHS continuing healthcare but
have been assessed as requiring the services of a registered nurse they are eligible for NHS-funded nursing care.
3.3. Equalities Impact Assessment
Page 16 of 101
Referral Checklist CHC
Assessment Determin-
ation Appeal
Commission-ing of Care
Review
The Department of Health completed a qualities impact assessment for the introduction of the National Framework for continuing care and NHS-funded nursing care. This can be found in Appendix 5, or a copy can be obtained from the Continuing Healthcare Team.
4. The CHC Assessment Process for Adults Ealing CCG applies this policy in accordance with The National Framework for Continuing Healthcare and NHS-funded nursing care (The National Framework). When it is identified that an individual may have on-going healthcare needs, they should be assessed by appropriate professionals to consider eligibility for Continuing Healthcare. This process uses the tools provided within the National Framework. Appendix 7 summarises the decision making process in a flow chart. This section describes the process followed by the CCG in terms of assessing an individual for NHS continuing healthcare, provision and review. Essentially the pathway involves:
- Referral – anyone can make a request to the team for an assessment of eligibility (see
section 3.1 for more details).
- Checklist – a screening tool used to help practitioners identify individuals who require referral for a full Continuing Healthcare Assessment (section 3.2).
- Continuing Healthcare Assessment (section 3.3) – this may include either a
o Health Needs Assessment and Decision Support Tool completed by a multi-disciplinary team, or
o alternatively individuals may be assessed under the Fast Track tool, applied to individual’s that have a rapidly deteriorating condition thought to be entering a terminal phase.
In both process, the primary health needs test is applied.
- Determination – this is process to ratify the recommendation (Section 3.4).
- Appeal – the process for an individual to appeal if they disagree with the outcome (see section 3.6 for more details)
- Commissioning of Care – this includes directly procured services and Personal Health
Budgets (Section 3).
- Review – of eligibility and appropriateness of care provision (section 4.9). Whilst the team manages the throughput of all continuing healthcare assessments that take place for individual’s that remain the responsibility of NHS Ealing, they do not complete all the assessments. Local hospitals complete the full continuing healthcare assessment process internally and send the paperwork to NHS Ealing CCG for determination. Some assessments are received from other CCGs for example when an individual is moving into the area. With regards to end of life, In the case of a fast track assessment, an appropriate clinician can complete the tool and send it to the CCG for determination. Arrangements for applying the National Framework form an integral part of the hospital discharge policy, and is implemented in such a way that delayed discharges are minimized. Ealing CCG has

Page 17 of 101
Referral Checklist CHC Assessment Determination Appeal Commissioning
of Care Review
Referral Checklist CHC Assessment Determination Commissioning
of Care Appeal Review
arrangements with Hospital Trusts and other NHS bodies to ensure the continuing healthcare process fits their discharge pathway.
4.1. Referral Any patient in any setting is entitled to a full Continuing Healthcare assessment if Nurse Assessor(s), social worker or patient themselves consider that needs may be sufficient to warrant a full
assessment. The Continuing Healthcare Team has a referral form for professionals and individual’s requesting an assessment (see Appendix 2). There is an expectation that Social Workers and Hospital Discharge Co-ordinators will apply a checklist before making a referral.
4.2. Who is eligible for a continuing healthcare assessment? (Checklist) The National Framework provides a ‘Checklist’ (see section 1.3) for trained practitioners to establish whether a full continuing healthcare assessment should be completed. A continuing healthcare checklist should only be completed by a trained individual in conjunction with the patient and/or their relative and carer. This tool typically forms part of the discharge process from a hospital setting. Alternatively for example a GP, nurse, social worker or other allied health professional could use it in an individual’s home.
Patients can be identified as requiring a continuing healthcare assessment in a number of settings; acute hospitals, the community or in care homes. Some of these patients will already have allocated social workers and/or district nursing staff. In these instances it is these staff members who will be responsible for completing the Checklist by collating information provided by professionals involved, the patient, and/or their carer. These examples are not an exhaustive list of people that may use this tool, because in some cases it may be appropriate for different or multiple professional(s) to be involved in the assessment process. Some patients will not yet be known to services, in these cases, the Continuing Healthcare Nurse Assessor will be the responsible assessor for leading the full process following the referral.
4.2.1. Checklist - to establish whether a full assessment is required Only a professional trained in NHS Continuing Healthcare assessments should complete the checklist as their judgement is required in cases where the weightings do not apparently trigger for an assessment, but a full assessment may be appropriate. The professional(s) will complete all the domains, which purposely mimic the Decision Support Tool (DST). There are 11 domains covering; behaviour, cognition, psychological and emotional needs,

Page 18 of 101
communication, mobility, nutrition, continence, skin integrity, breathing, drug therapies and medication: symptom control and altered states of consciousness. Each of these domains has a statement A, B or C. The professional(s) involved will complete the checklist with evidence to support the selected statement. If patients are in hospital, the Discharge Co-ordinator/ward staff will be responsible for coordinating the assessment. If they are in care homes, the Continuing Healthcare Team’s Nurse Assessor will be the responsible lead health co-ordinator. By mapping out responsibilities in this way Ealing CCG endeavours to prevent gaps or duplication of the process.
4.2.2. When is a full assessment required? A full assessment for NHS continuing healthcare is required if there are:
- two or more statements selected in column A; - five or more statements selected in column B, or - one selected in A and four in B; or - one statement selected in column A in one of the boxes marked with an asterisk (i.e. those
domains that carry a priority level in the Decision Support Tool), with any number of selections in B or C.
4.2.3. Outcome There are only 2 possible outcomes from completion of a checklist:
- A full continuing healthcare assessment is required or - A full continuing healthcare assessment is not required
The individual completing the checklist should complete the recommendation on (page 19 of the checklist) to confirm whether a full assessment is required and the rationale.
4.2.4. Ratification of the Checklist outcome When a Checklist is completed, a copy of it should be given to the individual or (where appropriate) their representative in a timely manner. The Checklist should include enough information to understand how the decision was made. If the Checklist indicates that a full consideration for Continuing Healthcare is not required, then the individual does have the right to request a review of the decision if they disagree with it. CCG contact details are included with the Checklist. The CCG receives checklists from a variety of sources. What happens next in the process will depend on where the checklist has come from and whether the CCG needs to act. The Clinical Team Leader or delegated individual is required to complete the ratification process. The purpose of ratification is to ensure that decisions regarding eligibility for a continuing healthcare assessment are:
- consistent - evidence based and - in line with the National Framework.
Any concerns regarding the content will be discussed with the individual leading the checklist process. Checklists received from Hospital When a checklist is applied to an individual in a hospital as part of their discharge planning process, the CCG is forwarded a copy of the checklist (usually by the discharge planning teams). If the checklist states that:
- A full assessment is required; the hospital is expected to complete the full continuing healthcare assessment.

Page 19 of 101
Referral Checklist CHC Assessment Determination Appeal Commissioning
of Care Review
- A full assessment is not required; the CCG will email the referrer and social services to confirm that the individual is not eligible for an NHS continuing healthcare assessment. In this instance, the CCG will need determine whether the individual has needs that would qualify them for NHS-funded nursing care (see section 2.2 for a definition). This would be included in the outcome email.
Checklists received from Social Care When a checklist is led by a social worker, this is typically in conjunction with a Social Care Assessment. The CCG is forwarded a copy of the checklist, Social Care Assessment, and Referral form (section 3.1). In this circumstance, if the checklist states that:
- A full assessment is required; the CCG will allocate the case to a Nurse Assessor who will lead the assessment process in completing the multi-disciplinary continuing healthcare assessment.
- A full assessment is not required; the CCG will email the referrer and social services to confirm that the individual is not eligible for an NHS continuing healthcare assessment. In this instance, the CCG will need determine whether the individual has needs that would qualify them for NHS-funded nursing care (see section 2.2 for a definition). This would be included in the outcome email.
4.2.5. Informing the outcome following a checklist The referrer and social services are informed of the decision by email. The CCG then writes to the individual explaining the outcome and their right to appeal this decision.
4.2.6. Keeping a record of the checklist findings Regardless of the outcome, the checklist will be kept on file/ in the patient records. This acts as evidence that the CCG has considered whether an individual’s care needs and whether they should have a continuing healthcare assessment. This record is useful in establishing whether a Previously Unassessed Period of Care (PUPoC) exists. Please see section 3.8 for more information regarding Previously Unassessed Periods of Care.
4.2.7. What happens if the individual disagrees with the checklist outcome? If the patient and/or their representative are dissatisfied with the decision not to complete a full Continuing Healthcare assessment, they should inform the CCG. The CCG will give such requests due consideration, taking account of all the information available, including additional information from the individual or his or her carer or representative. On review, the CCG may determine that a full continuing healthcare assessment should be completed if there is evidence to suggest it is required. Alternatively the CCG may decide to uphold the decision not to complete a full continuing healthcare assessment. In this instance a written response (including how to make a complaint) will be provided to the individual or their representative within 4 working weeks.
4.3. Continuing Healthcare Assessment
Page 20 of 101
Eligibility for NHS continuing healthcare is based on an individual’s assessed health needs. The diagnosis of a particular disease or condition is not in itself a determinant of eligibility for NHS continuing healthcare. The National Framework and Decision Support Tool describe in full the guidelines to be followed by CCGs in relation to assessing eligibility. There are a number of matters to consider before completing a Continuing Healthcare Assessment including consent, capacity (see National Framework Practice Guidance 7 & 8 – page 58-60) and responsible commissioner (see section 1.3, 1.4 and 1.5 for more details) along with whether the individual has any rehabilitation potential. Once these matters have been clarified and the individual requires an assessment, the Clinical Lead Nurse allocates a Nurse Assessor to lead the assessment process for the named individual.
4.3.1. Patients’ requiring rehabilitation Patients who are deemed to require a period of rehabilitation will not be allocated for a continuing healthcare assessment until the full rehabilitation potential has been reached.
4.3.2. Arranging a Continuing Healthcare Assessment Continuing healthcare assessments are arranged by the Team Co-ordinator. The co-ordinator will confirm the date and time of the assessment in writing to all those invited. Individuals and/or their relative or representative will be given a copy of the Department of Health’s public information leaflet The leaflet can be downloaded at https://www.gov.uk/government/publications/nhs-continuing-healthcare-and-nhs-funded-nursing-care-public-information-leaflet or a copy can be requested from the Team – see section 1.2 for details. This leaflet provides information about NHS continuing healthcare and NHS-funded nursing care. At the beginning of the assessment the Nurse Assessor will supply patients and/or relatives and carers with this booklet to guide them through the process. They will explain what NHS continuing healthcare and NHS-funded nursing care is. They will talk attendees through the process that will be followed, and explain that individuals have the right to appeal in the event that they are unhappy with the outcome or the process followed by the CCG. The individual or their representative will also be provided with a feedback questionnaire, this is used to establish the quality of service provided by the team and address areas for improvement when they arrive.
4.3.3. Establishing Capacity A mental capacity assessment should always be carried out for the Decision Support Tool. Capacity should always be assessed based on decision being made at that time. A major placement or treatment decision may accompany the assessment for Continuing Healthcare; if the patient lacks capacity to make such a decision and does not have a relative to act in their best interests, an Independent Mental Capacity Advocate (IMCA) may be required.
4.3.4. Establishing the Individual’s needs (Health Needs Assessment) For those patients who meet the threshold of the check list, a full assessment is required to ascertain if a patient has a primary health need and therefore meets the criteria for NHS continuing healthcare. The CCG Nurse Assessor leads a multi-professional assessment. This included the completion of the London Health Needs Assessment (See section 1.3); completed to establish what an individual’s needs are. This document is completed using information from the patient, care records and information from people involved in currently providing care who are familiar with the individual being assessed. This may include assessments or information from a Social Worker, District Nurse or
Page 21 of 101
Referral Checklist CHC Assessment Determination Recourse Commissioning
of Care Review
other Allied Healthcare Professional (e.g. Speech and Language Therapist, Occupational Therapist, Physiotherapist).
4.3.5. Decision Support Tool Once the assessment of needs is completed the Multidisciplinary Team (as defined by the CCG Standing Regulations 2012) should then complete an assessment of continuing healthcare eligibility. The Decision Support Tool used to capture how an individual’s needs present, the type of care required to meet the arising needs, and how the needs are managed. In this holistic assessment for eligibility process, the Decision Support Tool covers 12 domains:
- Behaviour - Cognition - Psychological and emotional needs - Communication - Continence - Mobility - Nutrition - Continence - Tissue Viability - Drugs therapies and medication - Altered states of consciousness, - Breathing and - Other need not described within the tool.
When completing the Decision Support Tool, it is essential to involve both the patient and their relatives/carers in the assessment process. Good patient, relative, representative and carer involvement throughout the process improves satisfaction and prevents undue appeals at a later stage. The process involves considering whether someone has a primary health need based on the nature, intensity, complexity or unpredictability of an individual’s needs.
4.3.6. Fast Track tool Individuals who are believed by an appropriate clinician (as defined by CCG Standing Regulations Part 6, section 21.13) to have a rapidly deteriorating condition that is entering a terminal phase can receive a Fast Track continuing Healthcare Assessment. This is a faster assessment process (see section 1.3 for a copy of this tool) and can be completed by an appropriate clinician. It is used when there is an urgent need to commission care for an individual that is thought to be dying. It may be used, for example, in order to enable discharge from hospital for an individual to die at home. The ratification process for these assessments are as described in 3.2.4 above (rather than 3.38 below as this would cause undue delay) and therefore takes place outside of the Ratification Panel. Fast Track assessments are taken to the relevant Panel’s as “for information” items. This enables
the Panel to consider consistency in the application of the National Framework, and to discuss any matters arising.
4.3.7. Recommendation (eligible for NHS continuing healthcare?)
Page 22 of 101
The MDT is then required to make a recommendation to the CCG as to whether the individual is eligible, including the reasons for making this recommendation. The recommendation should be clear, make reference to the complexity, intensity, unpredictability and nature of the individual’s needs and apply the primary health needs test.
Whether someone has a ‘primary health need’ is assessed by looking at all of their care needs and relating them to four key indicators:
nature – this describes the characteristics and type of the individual’s needs and the overall effect these needs have on the individual, including the type of interventions required to manage those needs
complexity – this is about how the individual’s needs present and interact and the level of skill required to monitor the symptoms, treat the condition and/or manage the care.
intensity – this is the extent and severity of the individual’s needs and the support needed to meet them, which includes the need for sustained/on-going care
unpredictability – this is about how hard it is to predict changes in an individual’s needs that might create challenges in managing them, including the risks to the individual’s health if adequate and timely care is not provided
If the individual is considered not eligible for NHS continuing healthcare, the Multi-disciplinary team should consider whether the individual is eligible for NHS-funded nursing care in line with the Funded Nursing Care Practice Guidance.
4.4. Determination (Ratification of decision) This section describes how the CCG accepts or declines the recommendation of the multi-disciplinary team with regards to eligibility for NHS continuing healthcare. The role of the Continuing Healthcare Panel is to ratify recommendations made by the multi-disciplinary team. The Panel has oversight of all assessments that are completed for individuals relating to a specific category of care. There are a number of Continuing Healthcare Ratification Panels held in Ealing depending on the individual’s overriding condition. In Ealing, the following Panels are held:
- Older People’s Risk Panel; Social Services and the CCG co-chair, this panel considers all community assessments led by the Continuing Healthcare Nurse Assessors for individuals that are physically frail, or have a predominant organic mental health diagnosis such as dementia.
- Disabilities Risk Panel; Chaired by a Director of Social Services, this panel covers adult and young people with Physical Disabilities and Learning disabilities;
- Adult Mental Health. Each Panel has their own Terms of Reference which can be found in the appendix. There are 4 categories of care that hold their own specific Panels:
Mental Health – terms of reference can be found in Appendix 12. Older People (including palliative care, organic mental health and physical disabilities) – see
appendix 8. Physical Disabilities and Learning Disabilities Appendix 13 Children and young people – see appendix 11.
Panels must be quorate in order to make ratify or overturn decisions. They meet regularly. A ratification panel may, for example consist of the following representatives:
A chair

Page 23 of 101
Referral Checklist CHC Assessment Determination Appeal Commissioning
of Care Review
A Senior Manager
A clinical representative
A Social Worker The Panel will ratify the eligibility recommendation made by the multidisciplinary team. They carefully consider the evidence provided and host a discussion for each domain and the Primary Health Needs test. Usually the Panel will ratify immediately. In some circumstances insufficient evidence or a disagreement may mean the case is deferred. Delays in decision-making will not usually delay the patient’s care provision. This is because one organisation will agree to “temporarily fund” provision under the proviso that the cost will be recharged if they are wrongly funding after the decision is concluded.
4.4.1. Keeping a record regarding eligibility for NHS funding At the end of Panel the appointed Panel Secretary circulates details of all clients, the considerations made and the outcome. It is the role of the attending Nurse Assessor to make a record of the Panel’s decision (outcome) on the Team’s database (Caretrack). And updating all relevant data on this database as it arises. The CCG will write to all individuals who have been considered for Continuing Healthcare explaining that the panel have ratified the recommendation. The letter will be sent within 10 working days and will include the details of who to contact if they disagree with the decision or would like more information. Letters are also sent to the patient’s General Practitioner and where appropriate; Care Provider and Local Authority and their representative. The letter will then be uploaded onto CareTrack.
4.5. Refusing NHS Continuing Healthcare Ealing CCG is only obliged to provide services that meet the assessed needs and reasonable requirements of an individual. A patient has the right to decline NHS funded services and make their own private arrangements. If an individual is eligible for NHS Continuing Healthcare, and refuses NHS Funding, they will no longer be able to receive funding from the Local Authority towards their care. In this circumstance, it will be explained to the individual that they can request support from the NHS at any point in the future. If the individual’s needs change, the CCG may be required to complete an NHS continuing healthcare assessment, to determine whether they are eligible for NHS funding before any service can be commissioned.
4.6. Appeal NHS Ealing works closely with patients and their representatives to ensure they are closely involved in the continuing healthcare process. We use questionnaires to ascertain the quality of the service
Page 24 of 101
we provide to the end user. When a response is received, the information is fed back directly to the Clinical Team Leader and into the operational processes as described in 1.10. Once a decision has been made with regards to an individual’s eligibility, and letter has been sent confirming the decision, individuals have the right to request a review. Staff should be familiar with the internal protocol for Appeals. A process flow has been included in Appendix 16.
4.6.1. Requesting an Appeal In the event that an individual is dissatisfied with
a) the procedure followed by Ealing CCG in reaching an individual’s eligibility decision or b) the eligibility decision for NHS continuing healthcare or NHS-funded nursing care
they have a right to request a review in accordance with the National Framework (paragraph 147) and CCG Standing Regulations (Part 6 23.3). This right is made explicit in the outcome letter sent to the individual and/or their relative to inform them of the continuing healthcare assessment outcome. If there is a disagreement, the individual will be asked to put their dispute in writing within 4 weeks of the outcome being written to them. The disagreement must be clearly stated along with the reasons why a) or b) above apply. If the issue is a complaint, it must be dealt with via the complaints procedure described in section 4.6.5 below.
4.6.2. Responding to the Request In response the CCG will write to them using the standard template in Appendix 5 (usually within 2 working days). This letter will invite the individual to meet with the Operational Manager (within 2-4 weeks – notice period required for all individuals attending) and discuss the reasons for their disagreement.
4.6.3. Local Review In line with sections 145-151 of the National Framework Ealing CCG offers local resolution as the first stage of disagreement. The appellant must be the patient or an individual with authority to act on behalf of the individual if they lack capacity. Once the CCG has confirmed that the case is for an appeal rather than complaint. The applicant will always be invited to attend the Local Review Meeting, with adequate notice being given to the applicant and enough time allocated in the meeging for the applicant’s full involvement with the discussion. The purpose of this meeting is to ensure the CCG has explained how the National Framework for NHS conginuing healthcare is applied in Ealing. To ensure that the CCG has applied the National Framework appropriately, has given due attention to the reasons for appeal and satisfy itself that the process followed and decision made were appropriate. The meeting will include a description of the assessment process, primary health needs test and appeals process.
4.6.3.1. Meeting Processs This meeting will be chaired by the Head of Continuing Healthfcare and Completx Placemetnts or nominated individual who is is literate in the National Framework and ideally has experience in dealing with appeals. During the meeting, the CCG will try to ascertain whether:
All appropriate evidence has been made available and been scrutinised properly
Page 25 of 101
the health needs assessment was an accurate reflection of the individual’s needs at the time
there is further information that needs to be considered
During these meetings, individuals may receive advice regarding how to complain about services they have received, where to obtain help and support in caring for their loved one.
4.6.3.2. Purpose The purpose of the local review meeting is for;
the CCG to provide clear information regarding the National Framework and how it is applied
locally. This would include for example an explination of tools used and ulrimately the primary
health needs test.
the CCG to listen to the concerns made by the appellant and considers their views.
both parties to either resolve the disagreement or agree on a resolution process
4.6.3.3. Outcome The CCG may decide following or during this meeting:
That the outcome reached by the Multi Disciplinary Team may not have been robust in which
case:
o The CCG may overturn the decision or
o The CCG may request additional evidence before reviewing the process or outcome.
And then re-present the case to the appropriate care category’s Continuing Healthcare
Panel.
That an independent assessment is required from an individual/organisation not previously
involved in the case.
Altternatively the appellant may decide:
They are satisfied that the CCG has applied the Natioinal Framework appropriately and that
the decision made was appropriate.
If this meeting is unable to resolve queries, concerns or more directly the outcome of the original decision, the appellant may choose to request an independent review.
4.6.3.4. Informing the Appellant of the Ouctome The CCG will notify the applicant of the decision in writing within 10 working days. This letter will include a detailed rationale for how the decision was made. This letter will also give details of how to proceed with the appeal via NHS England’s Independent Review Panel if they remain dissatisfied.
4.6.3.5. Minutes Minutes are taken for these meetings in order to ensure Ealing CCG captures all the information and considers the appeal carefully. Once agreed, a copy will be stored.
Page 26 of 101
4.6.4. External Review If following completion of local resolution, the appellant remains dissatisfied with the outcome, they can proceed through the external review stages, of which there are two. Firstly the Independent Review Panel and secondly the Ombudsman. Individuals are made aware of these stages when the CCG replies to their letter of appeal.
4.6.4.1. Independent Review Panel Independent Review Panel
If after completing local resolution the appellant remains dissatisfied with the CCG’s decision, they can request an Independent Review Panel (IRP) consider the case. Requests should be made in writing to:
Karen Scarsbrook Continuing Healthcare Manager (London Region) NHS England Southside, 105 Victoria Street, London, SW1E 6QT
Requests of this nature must be made within 6 months of local resolution being completed. Agreements for an IRP by NHS England to proceed are subject to approval by the Independent Chair appointed by NHS England to consider the case. The appellant will need to provide reasons in writing as to why they believe the decision should be reviewed, clearly stating why they believe the CCG’s decision was wrong. If the Independent Review Panel agrees to review the case, they will write to Ealing CCG Managing Director. After the review, the IRP may make a recommendation to the CCG with regards to the outcome, or procedures which have been followed. In all but exceptional circumstances, the CCG will agree to accept these recommendations.
4.6.4.2. Ombudsman If once the Independent Review Panel has considered the case, the appellant remains dissatisfied, they can contact the Health Investigations Directorate, The Parliamentary and Health Service Ombudsman; Milbank Tower, Milbank, London, SW1P 4QP. Recommendations from the Ombudsman are shared with the NHS England (London Branch) Continuing Healthcare Leads. This information id disseminated to the London Leads Meeting of all the Continuing Healthcare Leads across London. This information influences policy and practice locally.
4.6.5. Complaints Individuals have the right to make a complaint. Any complaint for NSH Ealing CCG should be put in writing to the: Complaints Manager CWHHE Clinical Commissioning Groups, 15 Marylebone Road, London, NW1 5JD.
4.7. Local Authority and Clinical Commissioning Disputes The process for dealing a dispute (whereby the CCG and Local Authority are not able to agree with on an eligibility decision, or there is disagreement with regards to which CCG should be involved) is

Page 27 of 101
well documented within the National Framework in paragraphs 159-160). The process for Ealing CCG and Ealing Council can be found in the Panel’s Terms of Reference in Appendix 8.

Page 28 of 101
5. Previously Unassessed Periods of Care (PUPoC) The CCG received a number of requests following the The Department of Health’s deadline for PUPoC claims during the period 1st April 2011 – 31st March 2012 (and previous closures). The team has been working to address each request and there is an action plan in progress for every request received. In many cases, PUPoC requests relate to an individual who are deceased. For this reason the CHC Team has taken the decision to prioritise requests relating to individuals that are alive. There process is similar to a traditional assessment as described in section 3, however there are a few key differences as demonstrated below.
5.1. Determining Eligibility for PUPoC Assessment
In deciding whether an individual is eligible for a PUPoC assessment, the CCG is required to
establish whether:
o The application was made before the deadline
o There is a PUPoC, or if the CCG completed robust assessments during the specified
timescale
o The individual requesting an assessment has the right to make this request. This may
be the beneficiary of a will if the individual is deceased. Or it may be an individual with
Lasting Power of Attorney for Welfare and Finance if the individual is alive. Some
applicants opt for an advocate or solicitor to represent them or support them through
this process.
5.2. Collating Evidence
The PUPoC Administrator is responsible for collating all evidence required for a robust assessment to
take place. This may include:
The Registered General Practitioner
The Care Home(s) or Care Provider
Secondary Care (hospitals)
Community Services (including dieticians, district nurses, Occupational Therapists,
Physiotherapists etc.)
Social Services
Mental Health Providers
Contact should be made with the Solicitor or Advocate in the event that they may hold
records.
The CCG will consider the relevance of any additional evidence that an individual
wishes to submit.
5.3. Care Needs Portrayal The Nurse Assessor will complete a health needs assessment using the “Needs Portrayal”
Document as issued by NHS England. The purpose of this document is to ensure that all evidence is
captured based on the records available. During this process it may be identified that further
evidence or information is required.
Page 29 of 101
Once all the information has been included, a draft Needs Portrayal will be sent to the family
for consideration and comment.
5.4. Meeting with the Family This meeting is an opportunity for Assessor to explain what NHS continuing healthcare is and how eligibility for NHS continuing healthcare is determined. The family will be given the opportunity to provide any additional comments regarding the individual’s care needs and how they presented at the time. Any amendments will be made and sent to the family for review. Once this document is finalised, it can be discussed at the PUPoC Panel
5.5. PUPoC Panel The Panel is held in two halves. During the first half, the family/representative are invited to attend.
Attendees will discuss the Needs Portrayal and the family/representative will be given an opportunity
to comment on the content.
During the second half, the family are invited to leave. At this point, the Decision Support Tool is
completed by the Multi-disciplinary Team and the primary health needs test applied. A
recommendation is made.
Minutes are taken at the meeting, provided to the attendees and are stored as a record.
5.6. Continuing Healthcare Panel
The case will then be presented to the relevant Continuing Healthcare Panel as described in section
3.4 above.
5.7. Outcome Letter Once ratified by the Panel, the family/representative will be written to explaining the outcome and the
appeal process should they wish to appeal.
5.8. Keeping a Record A copy of the outcome letter will be retained by the CCG.
5.9. Appealing the Decision If, following receipt of the outcome letter, an individual wishes to appeal the decision, they are invited
to proceed to local resolution (see section 4.6)
5.9.1. Local Resolution The appellant and their representative (if they have one) will be invited to meet with the head of the
Continuing Healthcare and Complex Placements Team in order to discuss their areas of
Page 30 of 101
disagreement, as described in 3.6.3.1. Minutes will be take of this meeting as an accurate record of
the discussion that took place. They will be sent with a covering letter detailing the appeals process
and contact details to the appellant.
5.10. Independent Review
If after this meeting the individual still wishes to appeal, they can do so via NHS England as
described in section 4.6.4.1 above. If they remain dissatisfied, they can contact the ombudsman as
described in section 4.6.4.2 of this document.
Page 31 of 101
6. Redress There is clear guidance (see section 1.3) from NHS England with regards to redress. The CCG will request evidence from the appellant as follows:
The individual has authority to act in terms of receiving funds Invoices from the Care Provider to demonstrate what the cost applied to. There are instances
where nursing home provide additional services such as hairdressing and newspapers, that the CCG would not be responsible to pay for.
Bank statements to show that funds left the appropriate account The CCG will calculate the interest and consider whether any further redress should be provided. A letter is sent to the appellant confirming what the amount is for, and that it relates to the care services provided to the named individual for the defined period. The appellant is required to return a signed form as a full and final settlement of the case. Once the CCG is satisfied that it has all the information required, a bank transfer is completed.

Page 32 of 101
Referral Checklist CHC Assessment Determination Appeal Commissioning
of Care Review
7. Commissioning of Care Some patients in receipt of continuing healthcare will receive it in a specialised environment. The treatments, care and equipment required to meet complex, intense and unpredictable health needs may depend on trained professionals for safe delivery, management and clinical supervision. Specialised care, particularly for people with complex disabilities may be required in specialist setting and may be distant from the patient’s ordinary place of residence. Placements can be very costly. The complexity of an individual’s needs may result in a limited choice for safe and affordable provision. NHS Ealing holds the responsibility to promote a comprehensive health service on behalf of the Secretary of State and to not exceed the defined financial allocations. It is expected to take account of patient choice, but must do so in the context of those two responsibilities. In the light of these constraints, the CCG has developed and agreed this policy to guide decision making on the provision of continuing care, in a manner that reflects the choice and preferences of individuals but balances the need for the CCG to commission care that is safe and effective and makes best use of the resources available to the CCG.
7.1. Funding Principals NHS Ealing CCG is responsible for promoting a comprehensive health service on behalf of the Secretary of State. The CCG must not exceed its financial allocations. In addition the CGG is expected to take account of patient choice, but must do so in the context of those two responsibilities. In the light of these constraints, NHS Ealing CCG has agreed this policy to guide decision making with regards to the care commissioned. The policy sets out to ensure that decisions will;
take into account the need for the CCG to allocate its financial resources in the most cost effective way.
offer appropriate choice where available and suitable in the light of the above factors. involve the individual and their family or advocate where possible and appropriate. be robust, fair, consistent and transparent. be based on the objective assessment of the patient’s clinical need, safety and, where
appropriate, best interests. Be based on the homes’ suitability to meet the individual’s needs
While there is no set upper limit on expenditure, the expectation is that placements/care packages will not be agreed where costs exceed 10% over the most cost effective package that has been assessed as able to meet an individual’s needs. This is the most effective, fair and sustainable use of finite resources, as set out in the principles and values of the NHS Constitution. Ealing CCT must promote a comprehensive health service on behalf of the Secretary of State and to not exceed its financial allocations. As a service, the team are expected to take account of patient choice, but must do so in the context of those two responsibilities.
Page 33 of 101
An assessment of need will be undertaken by Ealing Social Care and will include a review of the psychological and personal care needs and the impact on home and family life as well as the individual’s healthcare needs. For the avoidance of doubt, a patient will not be treated on a different basis to another NHS patient because the individual previously received privately funded treatment. Where a care package requested by an individual is not the most cost effective, the CCG, taking into account the considerations set out below, may agree to fund such a package of care in exceptional circumstances:
Circumstances of overall placement/ package Clinical need Psychological need Risk Patient preference Available alternatives Overall cost to CCG
A discussion will take place between the Senior Nurse and the Broker (Care Home Selection) the patient and family on the respective merits of the alternatives. Where the patient and family preference is consistent with the most cost effective package, the placement will be negotiated and the arrangements made and reviewed by the Continuing Healthcare team.
7.2. Top Up Where an individual is eligible for NHS Continuing Healthcare, the CCG is required to provide services to meet those assessed needs, free of charge. In the context of care home placements this will be limited to the cost of providing accommodation, care and support necessary to meet the assessed needs of the patient. For domiciliary arrangements this will be the cost of providing the services to meet the assessed needs of the individual. Where an individual wishes to augment any NHS-funded care provisions to meet their personal preferences they are at liberty to do so. However, this is only provided that it does not constitute a “subsidy” to the package required to meet the individual’s needs as identified by the CCG.
Example: Mrs Brown would like to purchase the services of a hairdresser and a daily paper in the home. Statement: If an individual chooses to purchase for example additional hotel services within a care home placement, these arrangements must be separate from dealings with the NHS and invoices sent directly to the individual. Invoices must clearly state the service/item that the payment relates to in order to demonstrate that payment is not subsidising the CCG's core package. As a general rule individuals can purchase services or equipment where these are optional, non-essential items which an individual has chosen (but was not obliged) to receive and are not items which are necessary to meet the individual's assessed needs. Examples include private hairdressers or a personal television.
7.3. Capacity to decide preferred place of residence

Page 34 of 101
The CCG will support an individual in making the decision as to where they wish to live. However, if concerns remain that an individual does not have the mental capacity to make the decision as to where they live, a mental capacity assessment (as defined in the Mental Capacity Act) will be undertaken. Where the individual lacks capacity to make the decision on where to live and there is no individual appointed to legally act on behalf on the individual legal Lasting Power of Attorney which extends to healthcare decisions then the CCG is under a duty to act in accordance with the individual's best interests in accordance with the Mental Capacity Act. The CCG will take the decision on the basis of consideration of the best interests of the individual taking into consideration the views of the family/carers. The CCG will need to consider whether there is a requirement for a deprivation of liberty authorisation.. Where the individual does not have the capacity to understand the particular decision then the CCG will consider whether it is appropriate to involve an independent advocate (IMCA) if the CCG considers that there is no one else willing and able to be consulted or that appointing an independent advocate will benefit the individual. Where a personal welfare deputy has been appointed by the Court of Protection under the Mental Capacity Act or a Lasting Power of Attorney with powers extending to healthcare decisions has been appointed then the CCG will consult with that person and obtain a decision from the appointed person on the preferred care option.
7.4. Personal Health Budget A personal health budget is an amount of money to support a person’s identified health and wellbeing needs, planned and agreed between the person and their local NHS team. Personal health budgets are to enable individuals to have greater choice, flexibility and control over the health care and support services they receive. As of April 2015, there is a “right to have” to have a personal health budget if they are eligible for NHS continuing healthcare. The purpose of the personal health budget is to enable the person to achieve a set of outcomes, it is not a budget provided to buy a specified number of hours of support as there might be better ways to achieve the agreed outcomes. NHS Ealing is currently rolling out Personal Health Budgets, in the future everyone eligible for NHS continuing healthcare will have a Personal Health Budget, even if it is simply a “nominal budget”. Individuals in receipt of a PHB (or their representative) will:
Be able to choose the health and wellbeing outcomes they want to achieve, in agreement with a healthcare professional
Know how much money they have for their health care and support Be enabled to create their own Support Plan, with support if they want it Be able to choose how their budget is held and managed, including the right to ask for
a direct payment Be able to spend the money in ways and at times that make sense to them, as agreed
with the CCG.
7.4.1. Options – Types of Personal Health Budget

Page 35 of 101
There are 3 types of Personal Health Budget available to individuals eligible for NHS continuing healthcare in Ealing;
Notional budget – No money changes hands. Individual is given the indicative budget, they then talk us about the different ways to spend that money on meeting their needs. The Continuing Healthcare Team will then arrange the agreed care and support.
Real budget held by a third party – A different organisation or trust holds the money on behalf of the individual and helps them decide what is needed. This will be agreed with our team and the third party will then buy the care and support as chosen.
Direct payment – Money is transferred into an identified account 4 weeks in advance for the individual/representative to purchase care/support. Governance mechanisms require individuals to show what money has been spent on.
7.4.2. Access Criteria Personal Health Budgets are available to anyone who consents to have one (or someone consents on their behalf if they lack capacity or are a child) where;
it is appropriate for them, it is value for money, they are eligible for NHS services, they are not subject to certain criminal justice orders and they will be able to manage one.
7.4.3. Exemption Criteria The CCG will not offer a Personal Health Budget to any individual that has been awarded funding under the Fast Track pathway. This is because it is understood that this individuals have a rapidly deteriorating condition that is entering a terminal phase. As a result the time it takes to arrange a PHB would be too long. IN the event the individual’s condition stabilises, and they remain eligible for NHS Continuing Healthcare at review, the CCG would consider offering a PHB. The CCG may also decide not offer a Direct Payment to an individual if for example it considers;
the person (or their representative) would not be able to manage a PHB; it is inappropriate for that person given their condition or the impact on that person of their
particular condition; that the benefit to that individual of having a direct payment for healthcare does not represent
value for money; that providing services in this way will not provide the same or improved outcomes; that the direct payment will not be used for the agreed purposes.
7.4.4. Process to obtain a PHB There are 8 steps to obtaining a PHB which are described below:
1. Eligible for NHS funded Continuing Healthcare Personal Health Budgets are currently only being offered to individuals that are deemed eligible for NHS continuing healthcare. NHS Ealing CCG will write to you informing you of the outcome of your assessment. This letter will enclose a leaflet giving an overview of Personal Health Budgets alongside contact details for any enquiries.
2. Requesting a PHB from the CCG If you are interested in the possibility of having a PHB, the CCG will provide you with clear information so you can make an informed decision about whether to request one. Once you have

Page 36 of 101
made a decision, the CCG should be contacted. If you decide to have a PHB, there are a number of steps to follow which are outlined below.
3. Your assessed needs (Care Plan) A Nurse Assessor from the Continuing Care Team will contact you to arrange a convenient time to visit in order to talk through what your needs are, and how they could be met with a commissioned package of care. This information will be captured in a care plan. This assessment is different to a Continuing Healthcare Assessment and is required in order for the CCG to calculate your indicative budget (step 4).
4. How much money is available (Indicative Budget) Using information from the Care Plan, the CCG will calculate your indicative budget. This is a proposed amount of money that the CCG would need to allocate in order to meet your assessed needs as defined within the care plan.
5. Understanding how your needs can be met (Support Plan) Once the indicative budget has been calculated, the Support Planner will come to meet you with the nurse assessor. Their role is to personalise your Care Plan by giving you the power obtain NHS care that best suits you. This is your opportunity to say how you would like to spend the indicative budget in order to meet your assessed needs. The support plan will then finalise the Personal Health Budget.
6. CCG Approval The Support Plan will be presented to the CCGs Continuing Care PHB Panel for consideration and approval. The role of the PHB Panel is to ensure that the plan is lawful, effective, affordable and appropriate. The CCG must be satisfied that that the assessed needs identified in the care plan can be met by the services specified in the support plan, and that the amount will be sufficient to provide for the full cost of each of the services. In the event that the Support Plan is not agreed, the Commissioner will provide feedback so the Support Plan can be amended.
7. Organising care and support (Implementation) You will now be in a position to arrange your care as agreed in the Support Plan.
8. Monitoring and review (Governance) The CCG is required to review
the making of direct payments and the health conditions of the patient in respect of which direct payments are made; at least
once within the first three months of the direct payments being made; and subsequently, at intervals not exceeding twelve months.
7.5. Discharge Planning A large number of Continuing healthcare assessments received by the team come from NHS Hospital Trusts. The Delayed Discharges (Continuing Care) Directions 2013 place certain responsibilities upon both CCGs and NHS Trusts to ensure correct discharge in this situation. Safe discharge from hospital remains the responsibility of the discharging hospital, as set out in Schedule 2, part 2 of the Standard NHS Contract for Acute Services Terms and conditions for the provision of Health Services. Hospital staff must be sure that appropriate provision will be available to meet the person’s needs after discharge, including;-
Care provision
A safe environment
Moving and handling equipment

Page 37 of 101
Medication
Continence supplies
Advance notice to the GP and DN (if applicable)
NHS Continuing Healthcare Funding & Registered Nurse Care Contribution Policy Whilst awaiting a decision on eligibility, if the person previously had Adult Services input the hospital staff may need to liaise with Ealing social care staff to continue to supply the pre-existing care package, without prejudice and to facilitate a timely discharge. Where a CCG has assessed an individual as eligible for NHS continuing healthcare the Continuing Healthcare and Complex Placements Team arrange and fund services to meet those reasonable needs as assessed by relevant professionals. There is no duty on the CCG to provide a specific package of care although the CCG will take individual choice into account when arranging a suitable package.
7.6. Commissioned Care (Adults) Continuing Healthcare can be provided in a range of settings including nursing homes and the individuals own home where appropriate. For patients with complex healthcare needs provision be required in a specialist nursing home or care facility established specifically for the purpose of skilled care in that specialist area. These settings have high levels of expertise in the successful management of complex or unusual physical and mental health care, and employ staff trained, managed and supervised in specialist interventions. They provide care significantly beyond the degree of complexity which can generally be managed safely in community settings. The most appropriate placement may not always be in the patient’s borough of residence.
7.7. Nursing Home Placement Ealing CCG commissions a brokerage service from Care Home Selection, which functions as an integrated part of the Continuing Healthcare Team. It is their responsibility to identify suitable Care Homes when the individual has decided (or it has been decided in their best interests as per the Mental Capacity Act 2005) that is the preferred location. They will work with the individual or their representative. Care Home Managers have a responsibility (under the Care Quality Commission) to ensure that the home can suitably meet the individual’s needs. The CCG expects a pre-admission to take place within 24 hours of making the request. This is in order to facilitate smooth discharge from hospital. If the home is not able to meet the individual’s needs, then it is no longer a viable option.
7.7.1. Criteria to establish an appropriate placement Care Home placements should be identified wherever possible using the criteria below.
the cost of the package; the Care Quality Commission's assessed standard; the appropriateness of the package; the clinical assessment of the individual's needs;

Page 38 of 101
the risk of any change to the individual's health; the likely length of the proposed package; and the psychological needs of the individual in determining whether the CCG will continue to
commission care at the care home.
7.7.2. Procedure to find a suitable placement The CCG will use the following procedure when making decisions about funding arrangements:
A normally commissioned provider(s) will be selected. Any offer should be within the borough of Ealing and take into full account current
commissioning arrangements of the CCG, CQC assessments, other Local Authority experience, Quality and Safeguarding concerns. It should prove value for money.
All homes must meet suitable criteria as demonstrated in CQC report. If a home frequently commissioned by NHS Ealing CCG and/or Ealing Local Authority. This
increases the footfall of statutory bodies attending the home, increasing visibility and ensuring regular contact with the home, patients and staff.
While there is no set upper limit on expenditure, the expectation is that the home will not be agreed where costs exceed 10% over the most cost effective package that has been assessed as able to meet an individual’s needs.
Where available 3 suitable providers will be offered for the patient/relatives to choose from. This not always possible due to availability of suitable homes in the area of Ealing or neighbouring authorities. If this is the case, families will be informed.
In exceptional circumstances, NHS Ealing may be consider homes outside the area of Ealing. The offer of providers outside of the area must be considered carefully with regards to the delicate balance between family wishes and the discharge of NHS Ealing’s duties to oversee ensure suitable, good quality care provision and timely review.
If the NHS and the family are unable to agree on a home, in exceptional circumstances the NHS will consider offering up to an additional 3 homes. A decision to offer additional homes must only take place when 1-6 above have failed. In this case, the CCG will write to the individual/advocate explaining which reasonable offers the CCG has offered and they have declined. It will record the potential alternative homes under discussion and set a timeframe of 2 working days (including Saturday) for the family to make a decision.
Patients and their relatives are actively encouraged by the CCG to visit the homes. NHS Ealing will anticipate confirmation regarding the home option within 2 working days following the initial offer (section 6).
In order to prevent delayed discharges from hospital, NHS Ealing will facilitate decision making process to enable patients to move into a home within 5 working days following the initial offer (section 6).
If a home is identified within the options offered by NHS Ealing, but there are no current vacancies, NHS Ealing will arrange a temporary move into a suitable alternative home. The patient will be added to the waiting list for their preferred home and move once a bed becomes available. NHS Ealing CCG will not agree to unnecessary stays in hospital.
If NHS Ealing and the family/patient are not in agreement with regards to a suitable home within 5 working days, a temporary home will be arranged for the patient to move into. The family will be requested to identify a suitable home of their wish and inform the CCG. The CCG will then carry out the relevant checks as outlined in 4.4 above. If the CCG is satisfied that this home is a suitable option, then the family will be informed. If the CCG is not satisfied that it can carry out its legal requirements as outlined or concerns remain the families will be informed. If the family are unable to agree on a home, the NHS will be unable to fulfil its obligations to provide NHS continuing healthcare. As such the CCG will advise verbally and in writing that if the individual/advocate refuses support from the CCG, they will have chosen to withdraw the patient form the services NHS continuing healthcare. If after withdrawing themselves from the process, the family decide they would like to re-enter the funding stream, the CCG will provide support to identify a home. If the individual’s needs change, it might
Page 39 of 101
warrant a review of their NHS-continuing healthcare needs before the CCG make commissioning arrangements.
An individual may appeal the decision in writing through the NHS Complaints process.
7.8. Homecare Package (Domiciliary Care)
The continuing Healthcare Team commission a brokerage service from Ealing Council “Homecare Team” for domiciliary care services. The process followed by the Council in this regard can be found in Appendix 5. Once the Council has ascertained what care should be provided, they send a purchase order to Ealing CCG for approval. The Clinical Team Leader considers the request and authorises the funding accordingly. Given the complexity of continuing care cases, it is not always possible for the CCG to provide NHS continuing care to an individual in their own home. The CCG supports the commissioning of care at home packages where they are appropriate and demonstrate value for money. The CCG aims to support patient choice but there may be situations where the CCG cannot reasonably be expected to provide the individual's choice of receiving care at home. This may for example be due to the cost or risks associated with the package. Sometimes individuals requiring high levels of support, may be more safely and appropriately provided for in another care setting. Whether a particular service should be provided by the CCG will depend on the review by the CCG of whether that particular service is required in order to meet that individual's personal or health care needs. The CCG's duty to fund services does not extend to funding for the wide variety of different, non-health and non-personal care related services that may arise in order to care for an individual at home . Should the CCG identify that such basic needs are not going to be (or have not been) properly met, the arrangement is no longer appropriate.
7.8.1. Criteria to access domiciliary care (Care at Home) Mental capacity must be established before making a decision about homecare. If a service user does not have the mental capacity to make an informed choice and is placing themself at risk by indicating choice of a care package at home a mental capacity assessment will be undertaken and the process followed as described in section 1.6. If the service user lacks capacity to make an informed choice, the CCG will complete a best interests meeting in conjunction with any advocate(s). With the intention of agreeing on the safest and most cost effective care package available. The CCG will apply the following principals when considering the provision of NHS continuing health at home:
The cost of the proposed package and whether any alternative provision can be made for the individual in a more cost efficient way i.e. where the total cost of providing care is within 10% of the equivalent cost of placement in an establishment;
The suitability, availability and suitability of alternative arrangements The individual’s capacity or expressed wishes and orientation to their surroundings Whether the individual lives alone, The individual's human rights and the rights of their family and/or carers including the right of
respect for home and family life Safety; as determined by professional assessment of risk (i.e. likelihood and consequence of
something happening or not), including appropriate equipment and clinical support agreed

Page 40 of 101
from community services (e.g. General Practitioner, District Nurse and other services relevant to the individual)
Risk management; the individual has full understanding of the risks and possible consequences and the provider accepts the risks to their staff of managing the care package
The opinion of a secondary care, specialist clinician, will be taken into account The psychological, social and physical impact on the individual; The willingness and ability of family members or friends to provide elements of care where
this is a necessary / desirable part of the care plan and the agreement of those persons to the care plan.
The likely duration of the package The extent of a patient's needs; any objections from other members of the household are taken into consideration. care can be provided by an organisation or individual under a formal agreement and meeting
standards acceptable to NHS commissioners
7.8.2. Risk and environmental Assessments In order to establish whether it is appropriate to fund a ‘care at home’ package, the CCG will undertake a number of assessments prior to agreeing to any package. Safety of the package will be determined by a formal assessment of risk, undertaken by appropriately qualified professionals. The risk assessment will include the availability of equipment and support, the appropriateness of the physical environment and availability of appropriately trained carers and/or staff to deliver care whenever it is required. The resilience of the package will be assessed and contingency arrangements will need to be put in place for each component of the package in case any component of the package fails. As part of the Continuing Healthcare Assessment, the CCG will have a clear understanding of the individual’s care needs and the extent to which that clinician considers that the proposed ‘care at home’ package meets those needs. The clinical assessment will consider the benefits of a ‘care at home’ package against the benefits of a care home placement.
7.8.3. Memorandum of Understanding for Domiciliary Care Provision When the CCG agrees to fund a ‘care at home’ package the individual and/or representative(s) may be required to enter into a Memorandum of Understanding to confirm that they accept the terms under which care is provided. This is usually only applied in the event that meeting(s) with family members and the patient have been unsuccessful in resolving the problems. This Memorandum of Understanding (appendix 6) does the following things:
Describes what the CCG will provide and what the individual and representatives have agreed to provide.
Confirms that the individual and/or their representative(s) understand that the care package is agreed on the basis of the assessed health and personal care needs
Details the required input at the date of the Memorandum. States that where the cost of meeting the assessed care needs increases for any reason, the
individual and representatives acknowledge that it may no longer be appropriate for the CCG to provide and they will work with the CCG to agree an alternative care package.
Agrees the alternative arrangements should the care package break down.
7.8.4. Termination of home care (domiciliary) provision NHS Ealing CCG will terminate any commissioned domiciliary arrangements in the following events:

Page 41 of 101
Where an individual is no longer eligible for NHS Continuing Healthcare – if following a review the individual is no longer eligible.
There are significant safeguarding concerns – and the individual requires moving to a place of safety.
NHS Ealing CCG may choose to terminate any commissioned domiciliary arrangements in the following events:
Where the CCG considers the safety of the patient, staff/contractors are at risk – in these circumstances the Continuing Healthcare Team will take such action as it considers appropriate in order to remove/reduce that risk to an acceptable level. Where this relates to the conduct of the individual or the home environment it shall request that the individual/representatives take the necessary action to remove the risk.
Harassment or bullying for example of care workers by the individual, carers or family members will not be accepted and the CCG will take any action considered necessary to protect their staff and contractors.
Compromise of safety - Where safety in providing care is likely to be compromised an appropriate action is not taken.
No longer appropriate - Where the individual is in receipt of a home care package and an assessment determines that this is no longer appropriate for any reason (section 4.8.1) then an alternative package will be discussed and agreed. If the individual declines to accept alternative suitable provision, the CCG may write formally to the individual, giving no less than 28 consecutive days notice for alternative arrangements to be put in place by the individual.
The level of need increases - Where the individual is in receipt of a home support package and the assessment determines the need for a higher level of support the criteria set out in 4.8.1 will apply. This may result in care being offered from a nursing home, hospital, whichever best meets the criteria overall.
7.9. Review In line with the National Framework, the CCG is routinely reviews individuals within the first three months of care provision starting and annually thereafter (or sooner if their care needs indicate that this is necessary). Individuals with palliative care needs may have their care reviewed more frequently in response to their medical condition. The CCG completes reviews in relation to an individual’s;
eligibility status, to ensure the CCG only funds individuals that are eligible for funding care provision to ensure it is of a standard required to be safe and appropriate.
The review may result in either an increase or a decrease in support offered and will be based on the assessed need of the individual at that time. Reviews will follow the process as described in section 3. It is possible for an individual’s condition to improve or stabilise to such an extent that they no longer meet the eligibility criteria for NHS continuing healthcare. Consequently, the individual may be referred to the Local Authority who will assess their needs against the Care Act Criteria. This may mean that the individual will be charged for all or part of their on-going care. Where possible, transition to Local Authority care will be managed by agreement between the respective authorities. However, there will be no gap in the provision and continuity of service resulting from eligibility reviews, and partners will support the reviews and transfer of responsibilities within a maximum of 28 consecutive days of being notified of the referral.

Page 42 of 101
8. Transition from Children to Adults’ Services A Continuing Healthcare representative will sit on a transition group from a care category that is most appropriately matched to the young person’s health needs to ensure NHS Continuing Healthcare continuation into adulthood is identified as early as possible. Children’s services should identify those young people for whom it is likely that adult NHS Continuing Healthcare will be necessary, this should occur when a young person reaches the age of 14. This should be followed up by a formal referral for screening at age 16 to the adult NHS continuing healthcare team. Details should be forwarded to the Continuing Healthcare team accompanied by a recent assessment including a social services report. Entitlement to adult continuing healthcare services should initially be established using the adult decision making tools. Any entitlements that are identified by means of these processes will come into effect on their 18th Birthday, subject to any change in their needs. If a young person in receipt of children’s Continuing Healthcare is not deemed eligible for adult Continuing Healthcare when they reach the age of 18, they should be advised of their non-eligibility and of their right to an appeal or to an independent review with their rationale for requesting this, as on the same basis as Continuing Healthcare decisions regarding adults. Good practice would dictate that a consistent package of support is provided during the years before and after the transition to adulthood. Children Services should at the age of 14 begin to discuss with families the difference between children and adult service provision to ensure families have a realistic expectation of what services will be continued within the adult provision. Planning for an appropriate package of care should begin at 16 with the individual and the family and should be tailored down gradually in the 2 years prior to transition to adult services. Where a young person receives support via a placement outside the Ealing area, it is important that, at an early stage in the transition planning process, there is a clear agreement as to who the responsible commissioner presently is, and whether this could potentially change. All parties with current or future responsibilities should be actively represented in the transition planning process.

Page 43 of 101
9. Access to Equipment & Other NHS Services Individuals eligible for NHS Continuing Healthcare have an entitlement on the same basis as other members of the public to access equipment and other NHS services via existing services. Where an individual is in receipt of NHS Continuing Healthcare and requires equipment to meet their care needs, there are several routes by which this may be provided:
The care home setting may provide non-specialised equipment as part of their regulatory standards under the Care Quality Commission (CQC), or as part of the contract with NHS Ealing CCG.
Some individuals may require bespoke equipment as assessed by an appropriate healthcare professional to meet specific assessed needs identified in their NHS Continuing Healthcare care plan. It is the responsibility of the Clinical Team Lead (or designated individual) to make appropriate arrangements to meet these needs.
Where an individual is going to return home with a package of care, it remains the responsibility of community services to assess for and arrange the provision of required equipment.
For further information please refer to the National Framework paragraphs 172 - 175

Page 44 of 101
10. Children and Young People’s Continuing Care In line with the National Framework for Children and Young People’s Continuing Care 2010, Ealing CCG is committed to supporting children with complex and life limiting or palliative conditions to live at home and enjoy as normal a life as possible. In practice this means bespoke packages of care for children with complex health needs at home or in the community or for a small number of children; residential placements including residential schools. Residential placements are usually jointly funded by social care and education. For Ealing CCG to fund such placements not only will the child have to meet the threshold for continuing care but the placement must provide in-house services delivered or led by health care professionals which meet the child’s health needs. For those at end of life stages, Ealing CCG aim to support families with care packages that allow their child to remain at home for as long as possible and die in a place of choice. Children who receive a continuing care package should still be able to receive appropriate support from community based health care services and social care if their need dictates. It is closely linked with the national documents below:
Every Child Matters
National Service framework for Children, Young People and Maternity Services
Better Care Better Lives
Liverpool Care of the Dying Pathway
Healthy Lives Brighter Futures
NHS Values Through all these documents there are a number of key themes:
Care at home or closer to home allowing children to enjoy a family life
High quality safe care
Services which are based on assessed needs
Working with families to deliver services in a way that is acceptable to them
Partnership working of NHS and social care for the benefit of children and families
The choice to die in their preferred place for those children nearing the end of their life
Using NHS resources wisely for the benefit of children while not compromising care quality
Provision of care NHS care is provided free to children who are eligible for NHS care for whom NHS Ealing is the responsible commissioner
10.1. Objective By implementing continuing care in Ealing the expectation is that children and young people with complex health needs can achieve the following outcomes:
Children and young people with complex health needs are able to remain in the family setting
Families feel supported to care for children with complex care needs
Children and young people are less likely to be placed in residential care or foster care for primarily health related reasons
The type of support available to families is tailored to their needs
Families caring for children and young people who have reached the end of life, are provide with a range of support that will allow the child to be cared for and die in a place of choice
The outcomes for Ealing CCG are:
Providing a process and service which meet the outcomes for families

Page 45 of 101
Evidence that resources are allocated according to need
Assurance that care provided is of high quality and safe
Ensuring that the assessment and decision making process are carried out in a timely, equitable and fair manner.
10.2. The Continuing Healthcare Pathway for children and young people The process in Ealing involves 7 steps as summarised below: Step 1: Identification of children who may be eligible Step 2: Assessing need Step 3: Recommendation to the panel Step 4: Decision making Step 5: Informing the relevant parties of the decision Step 6: Appealing the Decision Step 7: Delivering care Step 8: Reviewing care
10.3. Step 1 - Identification of Children who may be eligible Identifying children who may be eligible for continuing care is a role for a wide variety of health and social care professionals who work with children and young people. A referral form has been developed which asks questions about the needs of the child and serves as a screening tool for appropriate referrals. If the screening tool indicates that a child is unlikely to be eligible or the referral is inappropriate then the referrer is informed that an assessment will not be carried out. The referrer will be required to
1. Identify the health and social care professionals involved with the child 2. Seek permission from the child or family to undertake a referral and an assessment. 3. Provide information why the child is being referred for a Continuing Care Assessment
Families must be aware that in order to complete an assessment the continuing care assessor will require permission to seek clinical and social information from a variety of professionals and organisations, including medical notes from the GP and other hospital consultants.
10.4. Step 2 – Assessing Need The assessment process can only take place with the agreement of the parent or appropriate adult with parental authority. For older children they will be expected to be present for the assessment and their views taken into account. If an assessment is to be carried out a number of processes need to be started in rapid succession by a variety of professionals each with their own area of responsibility Role of the continuing care coordinator
To make a formal request for assessments by social worker or education processionals as required

Page 46 of 101
Collate all relevant medical information from the clinical professionals involved in the on-going health care of the child. This includes tertiary hospital consultants, community therapists, GP etc.
Liaise with the family to gather information pertaining to their child’s health needs
To undertake an initial risk assessment of the home
Present all evidence to the Continuing Care Panel
Role of social worker or social care professionals
To provide recent assessments or new assessments if none are available which provide information about the child’s needs and the families’ needs
To undertake a carers assessment if a recent one is not available
To provide evidence of why current local services are unable to meet the needs of the child Role of education professionals (this will only apply if the child or young person is attending early years services or is of school age)
To provide recent assessments or new assessments if none are available which provide information about the child’s needs and the families’ needs
To provide evidence of why current local services are unable to meet the needs of the child if a school based placement or in school support is requested
Role of health care professionals
To provide evidence and comment on the level of need within the domains
To provide recent risk assessments, clinic letters and up to date medical information relevant to their knowledge of the child
To provide evidence of why current local services are unable to meet the needs of the child For children being discharged into the community from hospital the assessment process is not an alternative to usual discharge planning arrangements but can be an additional facility to ensure the safe and timely discharge home of children with the most complex health needs. The usual discharge planning with local community services should run in parallel with the continuing care process. A summary of the assessment will be shared with the family.
10.5. Step 3 - Recommendation to the panel Assessments will be presented to the continuing care panel along with a recommendation. The recommendation will be based on
Assessments provided by health in the decision support tool
Assessments provided by education and social care
Risk assessments form the multi-disciplinary team The threshold for eligibility to continuing care is based on the health needs of the child as assessed using the decision support tool and is
high level need in 3 domains or
priority in 1 domain or
severe in 1 domain.

Page 47 of 101
10.6. Step 4 – Decision Making The panel is health led but will include at least one NHS health care professional and a representative from social care. The panel members will be required assess the evidence and information presented and agree if the child is eligible for continuing care funding or not. They must also be assured that the local services are unable to meet the needs of the child or young person. If a child does not meet the threshold for continuing care alternative provision of support or care should be considered by the panel and recommendations made to social care services If a child meets the threshold for continuing care, the preferences of the child, young person and family members should be taken into consideration when deciding on the allocation of the package of care. Areas to be considered are
What are the preferences of the child young person and family?
In which location will care be provided?
Is the current home a suitable location in which to provide care?
What are the types of care tasks and how frequently are they necessary?
How complex are the tasks and what training would carers require?
What training or skill level would a carer require to perform the tasks?
What are the risk to the child (or to others in the case of challenging behavior) if adequate care is not provided?
Does the child need clinical intervention at night?
Is there a need for consumables and equipment to be provided?
How urgently is care needed? While these should be taken into consideration the panel should be mindful of ensuring that there is equity of provision and that NHS continuing care is not used as a substitute to appropriate provision by social care or education services. The panel should make the decision on the size of care package based on the information presented but finding an appropriate provider should remain the responsibility of Ealing CCG
10.7. Step 5 - Informing the relevant parties The decision of the panel must be made to the family in writing within 5 working days. All parties involved in the referral or assessment process should also be informed of the panel decision within 5 working days. If a package of care is allocated then a letter sent to the parents should include giving details of the package of care offered. This will be followed up with a phone conversation or home visit to discuss the finer details. There will always be some flexibility on how care is delivered for example, if parents would like care of children with palliative needs to be provided by a hospice then that can be arranged
10.8. Step 6 - Appealing the decision

Page 48 of 101
Complaints may be related to the panel decision or the quality of care provided when a package of care is in place. Complaints about the panel decision can be from the family, young person or the organisation which initiated the referral. The first point of access for any child, parent or organisation that wishes to make a complaint or challenge the panel decision will be the continuing care coordinator who can discuss the matter with the family. The appeals and complaint process should be managed using the informal process where possible. If requested a reassessment can be arranged. If there has been either inaccurate information presented to the panel or the correct process has not been followed then the informal process should be offered. The assessment can be repeated or the original assessment presented again to the panel. If the child, family or an organisation is satisfied that the assessment was accurate and the correct process has been followed then they cannot make a formal appeal or complaint. If the child, family or organisation chooses not to have a reassessment a complaint must be lodged in writing via the Ealing CCG complaints department. An Ealing CCG appeals panel can be convened which will the evidence and make a decision whether the child meets the threshold for continuing care and if they do make a recommendation about the package of care offered. Complaints about the quality of care can be made to the organisation providing care via the nurse leading the package, to the continuing care coordinator or the commissioner.
10.9. Step 7 - Delivering Care When a package of care is offered there is no obligation upon the family to accept if they feel they can care for their child without additional support. However if a child meets the threshold of need the family can request a reassessment at any time in the future. The continuing care coordinator will meet with the family to discuss the package of care offered and the stages of arranging the care All packages of care are subject to parents understanding that
Requests by families for staff who have specific language skills and or a specific gender/ culture may not always be possible and can delay the start of the package
The health needs of the child will dictate the number of hours of care provided, not the needs of the family. E.g. if the family have another baby the number of hours will not be increased unless the needs of the child receiving continuing care have also increased.
If the child’s condition improves, the type of staff providing care may change or number of hours be reduced or stopped.
The child or young person will have regular reassessments to ensure that they still have health needs which require a package of care.
The care will be provided by appropriately trained carers who may not be registered nurses.
Adult continuing care is assessed using a similar process and receiving a package as a child or young person does not an automatically guarantee eligibility or a comparable continuing care package of care as an adult.
The decision of which provider is awarded the contract for the package of care, will be based on
child focused outcomes
quality of the package that can be provided

Page 49 of 101
speed of initiation of the package
cost (start up and ongoing) The organisation providing the package of care will need to undertake a risk assessment of the location where care will be provided if this is community based package. This may include a fire assessment of the property. This is also an opportunity for the family and child to meet representatives of the care organisation who will be looking after the child and discuss arrangements. If staff will be caring for a child on oxygen there may need to be fire alarms in the home or other modifications. If the home is not considered a suitable place for care to be delivered, alternative options will be explored with the family.
10.10. Step 8 - Review Each child who is eligible for continuing care will be
Reassessed 3 months after the panel agrees they are eligible for continuing care.
Then every 12 months or earlier if the child’s needs have changed. Reassessments will be undertaken and presented to panel in the same way as the initial assessment and will include feedback from the family on how the package of care is working. The continuing care coordinator will present the case to the panel as at the initial assessment highlighting any changes in the level of need and presenting any requested changes in the care provided or problems that may have arisen. Where the child or young person is in a residential placement or school or the package of care is jointly funded the reassessment process should be coordinated with other assessments. This will require the continuing care coordinator, LAC nurse, social worker and education team to coordinate assessments. This will also prevent duplication of effort for the staff undertaking the assessments and reduce the workload for the services or organisations that are providing the care.
10.11. Step 9 - Transition to adult services of closure of a package Packages of care provided through children’s continuing care arrangements stop for a variety of reasons
Children who turn 18 years – Please see 12. Transition from Children to Adult Services
Children who’s condition improves so they no longer require a package of care
Families moving out of the area or changing GP
Children who die If a package of care is to cease because the child’s needs have reduced Ealing CCG will withdraw the package in a staged way following discussion with the family. If the family are moving out of the area and/or changing to a GP not affiliated with Ealing CCG, the needs of the child will have to be assessed by their new CCG. This can take time as some CCG’s will not asses a child until they are registered with a GP in their local area. To minimise disruption to the family Ealing CCG will work inform the new CCG at the earliest opportunity and share information (with consent) with the new CCG to ensure that the transition to a new area runs smoothly. Although we envisage that all areas in England will be using the same assessment framework in the future the local interpretation of the levels of need and therefore the allocated number of hours care may be different. Parents must be made aware of that fact in advance of moving.
Page 50 of 101
When a child reaches end of life stages, Ealing CCG will make every effort to provide the appropriate care at the end of life to support children and young people to die in a place of choice. At the end of life care needs can and do change very rapidly. In these circumstances the normal assessment and panel process is curtailed and packages of care will be changed at short notice with the panel being notified after the event. Once the child has died the continuing care coordinator will arrange with the family for equipment and surplus consumables to be collected at a single visit to minimise disruption to the family at their time of grief.
10.12. Special Circumstances End of life care and fast tracking. If there is an urgent need for a package of care and the continuing care coordinator and the commissioner agree that it is necessary it can be started without the panel having to consider the case. The panel would be informed of the decision at the next available meeting. Tier 4 Inpatient mental health services Inpatient mental health services are funded for assessment and inpatient treatment of children and young people with mental health problems. Once the admission period is complete some of these children will not be able to return home and will require a residential placement. Continuing care can be part of a jointly funded arrangement to support their placement if the child or young person’s needs are such that they are eligible for continuing care. Once fit for discharge the child or young person should be moved to a more appropriate setting. The funding of care in an inpatient mental health unit will not usually be funded through continuing care.
Page 51 of 101
11. Mental health Assessment and Funding Arrangements
11.1. Context There are three main areas that fall into this category. All categories (discussed 1-3 below) covering a functional mental health condition are considered at the Joint NHS Ealing and Local Authority Mental Health Funding and Placement Panel. Details of this panel can be found in the Appendix 12. As with all process completed by the team, staff will ensure patients are the responsibility of NHS Ealing CCG before proceeding with any assessments.
1. Continuing Healthcare This process involves individuals with a diagnosis of Functional Mental Health and the assessment under the National Framework (section 1.3) similar to that describes in section 3.
2. Mental Health Hospital and Forensic Unit discharge including; Hospital to Hospital Transfers (i.e. When the hospital cannot meet needs within
existing commissioned services) e.g. s3 or s37/41 Locked Mental Health Rehabilitation (i.e. individuals that have come through the
forensic services or have completed treatment in a locally commissioned Mental Health hospital setting and are ready for discharge, but require a period of rehabilitation in a locked/open environment) These individuals will be sectioned under the mental health act e.g. s3 or s37/41
These processes include situations when an individual requires step down following a mental health section. The Mental Health Case Manager attends the Delayed Transfer of Care (DToC) meeting at the local West London Mental Health Trust. This meeting occurs every Wednesday and is the mechanism through which the CCG works with the local hospital to prevent delayed transfers of care.
3. Section 117 (aftercare) Cases These individuals have been detained under the mental health act and since discharged by the consultant under s117 of the mental health act. This places a duty on the NHS and Local Authorities to provide aftercare services to prevent relapse or their mental health that lead to them being sectioned or readmission.
11.2. Assessment & Preparation for Panel There are a different assessment processes for the 3 work streams described above each process has been summarised below.
1. Continuing Healthcare – the process is the as described in section 3 of this document.
2. Mental Health Hospital and Forensic Unit discharge – In this instance, the Case Manager will organise a clinical meeting or Care Programme Approach (CPA) with the relevant clinical team. The purpose of this meeting is to capture the rational for the team recommending the specified placement and to understand the clinical need of the patient. The Case Manager will gather the relevant information including a copy of the; CPA report, Occupational Therapist’s report, Risk Assessment, Care Plans (no less than 6 months old). This information is then recorded on the teams’ database Care Track.

Page 52 of 101
Prior to presenting the case to Panel, the Case manager, in conjunction with the Community Psychiatric Nurse and/or Social Worker, will source placement options based on the assessed needs. They follow the process outlined in section 4.6 – 4.84 above, and encourage representatives to view before preadmission assessment takes place. The provider is given a copy of the assessment report along with proposed care and treatment plans. The provider is then requested to complete a preadmission assessment. The provider with send a copy of their proposed treatment plans and cost to the Care Co-ordinator, Social Worker and Case Manager at the CCG. The Care Coordinator compiles the above assessments and reports in preparation for panel.
3. Section 117 (aftercare) Cases – The Case Manager obtains a copy of the assessed s117 aftercare needs. This is usually in the form or a Health Needs Assessment (see section 1.3) by S/W or CPN or copy of Discharge CPA Report. Care Coordinator completes Panel paperwork
11.3. Panel
All cases for the three work streams are considered at the Joint NHS Ealing and Local Authority Mental Health Funding and Placement Panel. Full details of this panel can be found in the Appendix 12. The Panel will carefully consider requests for funding and may make recommendations back to team if there are terms of further queries to resolve. Once the Panel has agreed the funding arrangements for care provision, the Continuing Healthcare Case Manager and/or Care Manager will be charged with the responsibility of communicating the decision to all the relevant parties.
11.4. Commissioning Placement The Case Manager enters negotiations with the relevant provider(s) in order to source the best value for care provision. In the case of s117, the responsibilities of Ealing CCG have been discharged to the Local Authority in the form of a Section 75 Agreement under the National Health Service Act 2006. As a result the Local Authority is responsible for sourcing all placements.
11.5. Review The process for reviews is slightly different depending on the work stream.
1. Continuing Healthcare – these cases are reviewed in line with the national framework (see sections 1.12 and 4.9).
2. Mental Health Hospital and Forensic Unit discharge: Reviews take place as and when required using repeating the process in section 8.2 above. A London Health Needs Assessment or joint review takes place with the Social Worker/Care Coordinators for patients ready for discharge into the community.
Page 53 of 101
3. Section 117 (aftercare) Cases – A joint review takes place the Local Authority or Care Coordinator. Any change in placement or level of care needs to be present to the Joint Panel following the review.
11.6. Appeal
In the event that an individual is unhappy with a decision made by the CCG, they have the right to appeal as described in section 3.6 – 3.9 in this document.
11.7. Disputes In the event of a disagreement between health and social care, the dispute procedure will be applied as per Appendix 12.

Page 54 of 101
12. Learning Disability Assessment and Funding Arrangement The Continuing Healthcare Team has arrangements with Ealing Local Authority (via a Section 75 arrangement) to complete Continuing Healthcare Assessments on behalf of the NHS. The Learning Disability Nurses are based at:
Community Team for People with Learning Disabilities 62, Green Lane Hanwell W7 2PB Tel: (020) 8566 2360 Fax:(020) 8566 2204
The process is followed by the team is as described in section 3.3 above. This team has their own Continuing Healthcare Panel. The Terms of Reference remain in a draft format, and once approved will be submitted in Appendix 18.

Page 55 of 101
13. Community Bedded General Rehabilitation Service NHS Ealing’s ‘Better Care Closer to Home’ Out of Hospital Strategy highlights the importance of having a range of rehabilitative services including bed based provision for supported discharge from acute services. In accordance with this strategy, Ealing CCG has commissioned a Community Bedded General Rehabilitation Service that offers supported discharge for patients with rehabilitation potential requiring bedded rehabilitation who no longer require acute hospital care. To offer patients a choice of location and rehabilitation provider, the service is delivered in 2 different nurse and therapy led rehabilitation Units within the Borough of Ealing; Beech Unit in Bupa Manor Court Care Home (Southall) and Jasmin ward in Clayponds Hospital (South Ealing). The service offers tailored multidisciplinary rehabilitation encompassing Nursing, Occupational Therapy and Physiotherapy Care, with the aim of enabling patients to reach their optimum function in order to return home safely. The aims of the service are:
To enable earlier patient discharge from acute hospital
To maximise patient independence, function and mobility
To facilitate safe and timely patient discharge to their home (or anticipated discharge destination)
The objectives of the service are to provide:
Step down rehabilitation intermediate care beds in the community
Nursing care in a therapeutic environment which supports rehabilitation
Physiotherapy and Occupational Therapy to meet the patient’s needs
Access to Dietetics and Speech and Language Therapy input as and when required
Access to equipment to facilitate rehabilitation and discharge
13.1. Rehabilitation Service Pathway The pathway can be seen in Appendix 18.
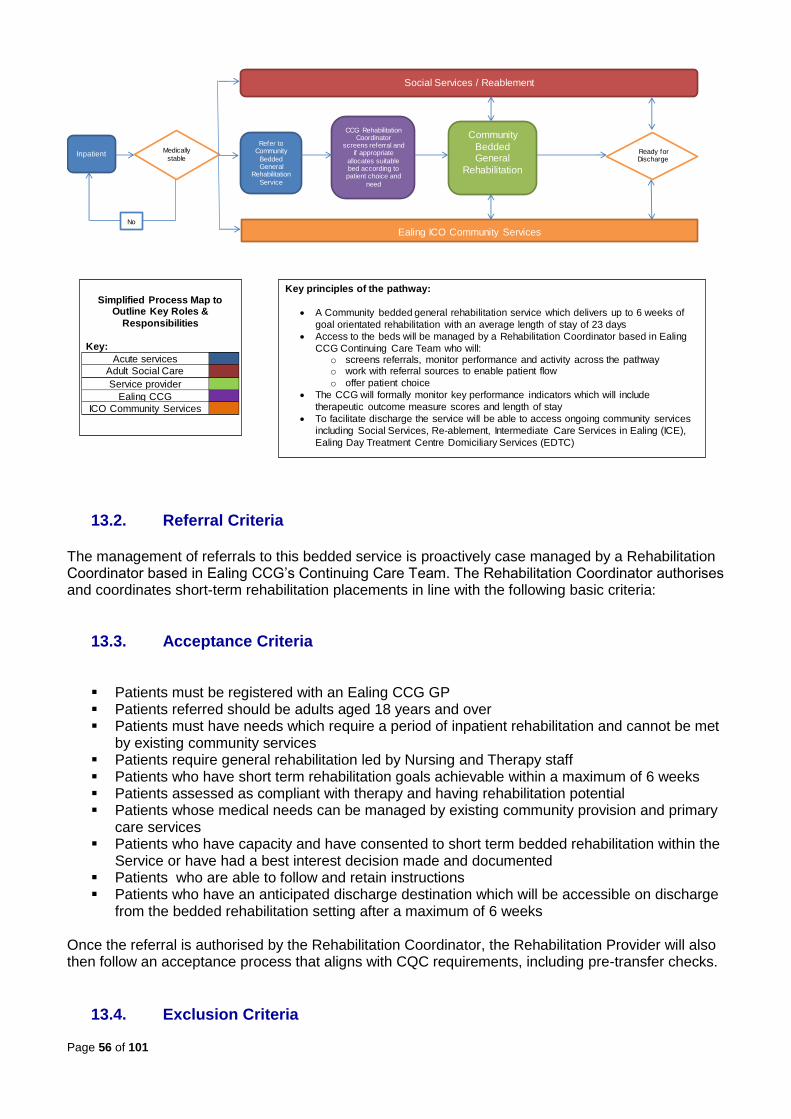
Page 56 of 101
13.2. Referral Criteria The management of referrals to this bedded service is proactively case managed by a Rehabilitation Coordinator based in Ealing CCG’s Continuing Care Team. The Rehabilitation Coordinator authorises and coordinates short-term rehabilitation placements in line with the following basic criteria:
13.3. Acceptance Criteria
Patients must be registered with an Ealing CCG GP Patients referred should be adults aged 18 years and over Patients must have needs which require a period of inpatient rehabilitation and cannot be met
by existing community services Patients require general rehabilitation led by Nursing and Therapy staff Patients who have short term rehabilitation goals achievable within a maximum of 6 weeks Patients assessed as compliant with therapy and having rehabilitation potential Patients whose medical needs can be managed by existing community provision and primary
care services Patients who have capacity and have consented to short term bedded rehabilitation within the
Service or have had a best interest decision made and documented Patients who are able to follow and retain instructions Patients who have an anticipated discharge destination which will be accessible on discharge
from the bedded rehabilitation setting after a maximum of 6 weeks
Once the referral is authorised by the Rehabilitation Coordinator, the Rehabilitation Provider will also then follow an acceptance process that aligns with CQC requirements, including pre-transfer checks.
13.4. Exclusion Criteria
Short Term Bedded Rehabilitation Care Pathway Process Map
Inpatient Medically
stable
CCG Rehabilitation Coordinator
screens referral and if appropriate
allocates suitable bed according to patient choice and
need
Community
Bedded General
Rehabilitation
Social Services / Reablement
Ready for Discharge
?
Simplified Process Map to Outline Key Roles &
Responsibilities
Key:
Acute services
Adult Social Care
Service provider
Ealing CCG
ICO Community Services
Key principles of the pathway:
A Community bedded general rehabilitation service which delivers up to 6 weeks of
goal orientated rehabilitation with an average length of stay of 23 days
Access to the beds will be managed by a Rehabilitation Coordinator based in Ealing
CCG Continuing Care Team who will: o screens referrals, monitor performance and activity across the pathway o work with referral sources to enable patient flow
o offer patient choice
The CCG will formally monitor key performance indicators which will include
therapeutic outcome measure scores and length of stay
To facilitate discharge the service will be able to access ongoing community services
including Social Services, Re-ablement, Intermediate Care Services in Ealing (ICE),
Ealing Day Treatment Centre Domiciliary Services (EDTC)
No
Ealing ICO Community Services
Refer to Community
Bedded General
Rehabilitation
Service

Page 57 of 101
Patients who do not require an in-patient setting to achieve their rehabilitation goals Patients who have not been determined as medically stable by a doctor Patients who have not consented to referral for bedded rehabilitation within the Service Patients who have not demonstrated the potential to progress with a short period of bedded
rehabilitation Patients who lack capacity to decide on agreeing to the referral to the bedded rehabilitation
service under the Mental Capacity Act 2005, and who have not had a best interests decision made and documented
Patients with cognitive difficulties which would impair their ability to participate and benefit from bedded rehabilitation
Patients under the age of 18 years Patients requiring medical led care Patients requiring specialist rehabilitation, including neuro-rehabilitation Patients with needs that cannot be safely managed by the provider of the bedded setting
following their pre-transfer assessment Patients whose needs cannot be established due to incomplete or ineligible referral forms
13.5. Referral Process
The Rehabilitation Coordinator works with referral sources to facilitate patient flow out of the acute sector
The acute hospital multidisciplinary team (MDT) identifies suitable patients for the service, and discusses potential referrals and bed availability within the bedded rehabilitation settings with the Rehabilitation Coordinator
To enable patients to make an informed choice, the acute hospital referring team discusses the rehabilitation choices available with the patient and / or their next of kin
All referrals are emailed or faxed to the Rehabilitation Coordinator based in the CCG using the CCG’s standard Community Bedded General Rehabilitation Service referral form (Appendix 6)
The Rehabilitation Coordinator screens referrals in line with the inclusion and exclusion criteria and authorises if appropriate
The Rehabilitation Coordinator informs the discharge team of the acute referring hospital if the referral has been authorised and the location of the allocated rehabilitation bed (if the referral has been declined, the discharge team will be informed and reasoning given behind this decision)
The paperwork for authorised referrals is sent by the Rehabilitation Coordinator to the provider of the allocated Rehabilitation bed
The rehabilitation provider liaises with the acute referring MDT, to carry out a pre-transfer assessment and arrange transfer of the patient
The rehabilitation provider updates the Rehabilitation Coordinator regarding the progress of the transfer
The rehabilitation provider can accept admissions from 8 am to 8 p.m., 7 days a week and will admit the patient within 24 hours of receipt of referral (once authorised by the Rehabilitation Coordinator)
The Rehabilitation Coordinator will monitor performance and activity across the pathway. In order to achieve this, the rehabilitation providers update the Rehabilitation Coordinator with:
o daily sit-rep reports on bed capacity o weekly patient progress reports including discharge plans and provisional discharge
dates o monthly KPI information including length of stay, therapy outcome measures, patient
satisfaction, readmission to acute, falls, clinical incidents o results from CQC inspections, o any changes to admission criteria, o patient discharge summaries

Page 58 of 101
13.6. Discharge Process
The Discharge process can be found in Appendix 17. Discharge planning is an integral part of the rehabilitation process which is commenced by
the rehabilitation provider on the patients admission to the rehabilitation unit The MDT of the rehabilitation unit is responsible for planning a safe and effective discharge
for the patient, in line with the set goal timeframes, within a maximum of 6 weeks from admission
Discharge planning includes identifying and making timely referrals to on-going community services such as Intermediate Care Services in Ealing (ICE Supported Discharge or Therapy only) or Ealing Day Treatment Centre Domiciliary Therapy services, London Borough of Ealing Reablement Team and Social Services.
The rehabilitation provider is responsible for identifying and ordering the equipment needed for a safe patient discharge in a timely manner. The discharge equipment will be provided and paid for by Ealing’s Integrated Community Equipment Service
Where identified as a need, the provider ensures an Occupational Therapy home visit or access visit has been completed prior to discharge
The rehabilitation provider makes all referrals for any outstanding equipment e.g. wheelchairs and home adaptations prior to discharge
The rehabilitation provider arranges and provides transport to safely transfer the patient from the rehabilitation unit to their discharge destination
The rehabilitation provider updates the Rehabilitation Coordinator on the progress of discharge planning for all patients on a weekly basis and if there are changes to the discharge plans
The rehabilitation provider informs the Rehabilitation Coordinator regarding the date and destination of all patients discharged
The rehabilitation provider sends a completed discharge report (Appendix 14) to the patient’s GP and Ealing CCG within 24 hours of the patient’s discharge

Page 59 of 101
14. APPENDIX

Page 60 of 101
Appendix 1 – CHC history
A brief history of NHS Continuing Healthcare NHS Continuing Healthcare has been evolving since 1994 when the Health Services Ombudsman published a report on a case in Leeds entitled, ‘Failure to provide long term NHS care for a brain-damaged patient’ (Reid, 1994). In July 1999, the Court of Appeal judged in the Coughlan case that funding responsibility was dependant on the legal limit of what could lawfully be provided by a Local Authority. Local Authorities can provide nursing services under section 21 of the National Assistance Act 1948, so long as the nursing care services are capable of being properly classified as part of the social services’ responsibilities in that they are; a) merely incidental or ancillary to the provision of the accommodation that an LA is under a duty to provide, pursuant to section 21; and b) of a nature that an authority whose primary responsibility is to provide social services, can be expected to provide (i.e. health care that is merely incidental or ancillary to the provision of accommodation). This meant that in effect individuals could “fall through the gap” between health and social care provision. In March 2001, the Department of Health issued a National Framework for Older People, which referred to the provision of free nursing care in nursing homes but did not include guidance on continuing healthcare. By June 2001 the Department of Health provided guidance on funding responsibilities and laid out three categories;
1. NHS funding 2. Shared responsibility and 3. social services
By 2003, many Strategic Health Authorities had developed their own Eligibility Criteria for NHS continuing healthcare. This led to a “postcode lottery” where eligibility thresholds could be different in each area. However, there was great support for a National Framework to eliminate the postcode lottery that had developed.
The Grogan Judgement assists the process to move forward, DOH, 2007 identified; 1. the need for a clearer assessment criteria which properly identified the test or approach
to be followed in deciding whether her primary need was a health need, 2. that there was a potential in law for a gap between what the Secretary of State provided
and those ‘health services’ that the local authority could ‘lawfully’ supply. 3. That when applying the primary health need approach, this should be considered against
the limits of social services lawful provision, not just by reference to a ‘primary health need’.
On 1st October 2007, the National Framework for NHS continuing healthcare and NHS-funded nursing care was implemented after two to three years of consultation. With the introduction of the new framework came national tools to standardise the approach to continuing healthcare assessment. In 2009 the National Framework for NHS funded Continuing Healthcare and NHS-funded Nursing Care was revised. The revisions clarify the decision-making and funding process and explain more clearly the types and levels of need that should consider when completing an assessment. Best practice guidance was issued in March 2010 and provides a practical explanation of how the Framework should operate on a day-to-day basis and gives examples of good practice.
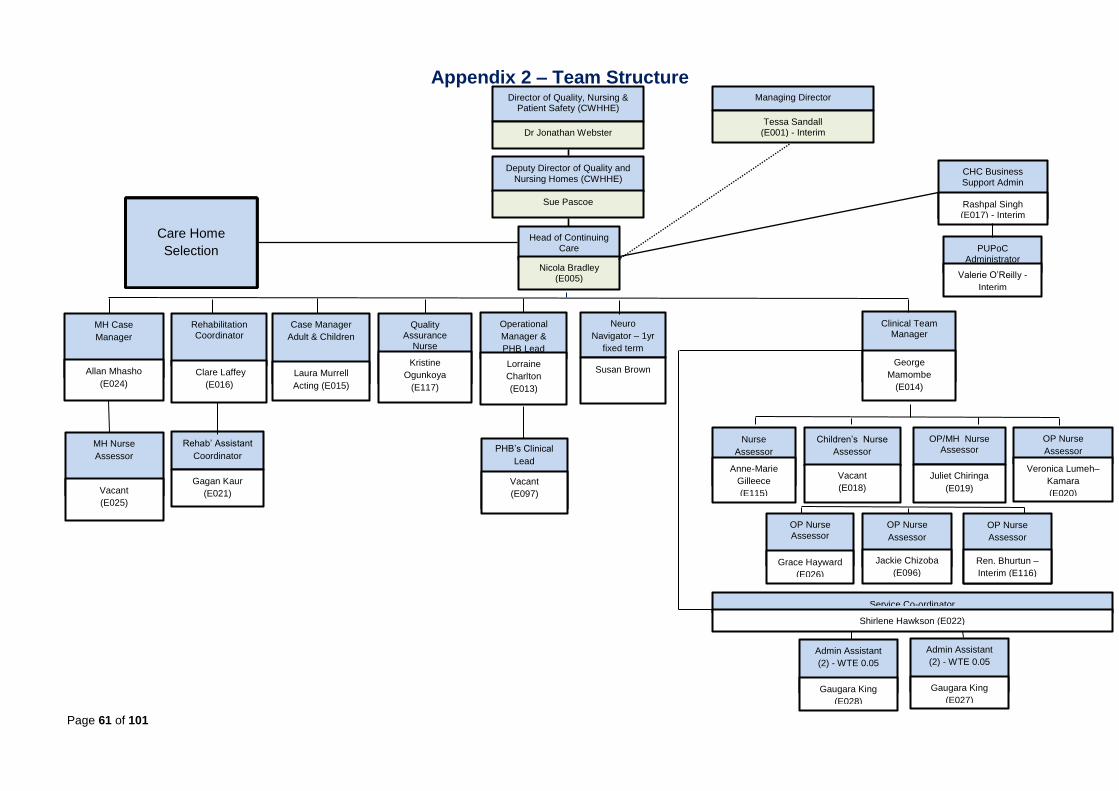
Page 61 of 101
Appendix 2 – Team Structure
Head of Continuing Care
Nicola Bradley (E005)
CHC Business Support Admin
Rashpal Singh (E017) - Interim
PUPoC Administrator
Valerie O’Reilly -
Interim
Service Co-ordinator Shirlene Hawkson (E022)
Admin Assistant (2) - WTE 0.05
Gaugara King (E028)
Children’s Nurse
Assessor
Vacant
(E018)
OP Nurse
Assessor
Jackie Chizoba
(E096)
OP Nurse
Assessor
Grace Hayward (E026)
MH Nurse
Assessor
Vacant (E025)
MH Case
Manager
Allan Mhasho (E024)
Case Manager
Adult & Children
Laura Murrell
Acting (E015)
OP/MH Nurse Assessor
Juliet Chiringa (E019)
OP Nurse
Assessor Veronica Lumeh–
Kamara (E020)
Rehab’ Assistant
Coordinator
Gagan Kaur (E021)
Clinical Team Manager
George
Mamombe
(E014)
Care Home
Selection
Rehabilitation Coordinator
Clare Laffey (E016)
Operational
Manager &
PHB Lead Lorraine
Charlton (E013)
Managing Director
Tessa Sandall (E001) - Interim
PHB’s Clinical
Lead
Vacant (E097)
Nurse
Assessor Anne-Marie
Gilleece (E115)
OP Nurse
Assessor
Ren. Bhurtun –
Interim (E116)
Quality Assurance
Nurse Kristine
Ogunkoya (E117)
Deputy Director of Quality and Nursing Homes (CWHHE)
Sue Pascoe
Director of Quality, Nursing & Patient Safety (CWHHE)
Dr Jonathan Webster
Admin Assistant (2) - WTE 0.05
Gaugara King (E027)
Neuro
Navigator – 1yr
fixed term
Susan Brown

Page 62 of 101
Appendix 3 – CHC referral form REFERRAL FOR CONTINUING HEALTHCARE ASSESSMENT FORM
First Name: Surname:
D.O.B: Date of referral:
Male Female First/preferred language:
Interpreter required Yes No
Previous Address: Tel. No:
Current Location: Address: Telephone:
Name and address of identified Nursing Home: Tel. No:
Borough of private home address: Expected / Actual date of admission to nursing home:
Current GP Name: Address: Telephone:
Previous GP: Name: Address: Telephone: Date when GP Changed:
Community Nurse Involvement?
Yes (If yes please give contact details)
No Name of nurse if known-: Address: Tel. No:
Next of Kin
Relationship: Address: Tel. No: Email:
Date of last continuing care or funded nursing care assessment if known: Assessed by which CCG?
Please indicate category of care: Elderly Frail Dementia Functional Mental Health Under 65 Physical Disability Learning Disability Child Not known Other please specify __________________
Current funding arrangements: please tick all that apply: Self-funding Social services only
APPENDIX 3 – CHC REFERRAL FORM

Page 63 of 101
NHS Clinical Commissioning Group Continuing care Other. Please specify _________________________
Name of Borough and/or CCG funding or contributing to care cost. __________________
Current Relevant Medical History, diagnosis and prognosis:
Name of Referrer: (please Print): Role/Job Title: Organisation: Address: Tel: Date:
Named Social Worker: Contact Address: Tel. No
No Allocated Social Worker
Additional Information:
Please Return to [email protected] Alternatively Fax to: 020 8080 8189. If you experience any problems when completing this form, please contact Tel: 020 8280 8080. PLEASE NOTE: Only fully completed referral forms (with a copy of the Continuing Healthcare Checklist and the Social Services Review if the referral is from a social worker) will be processed.
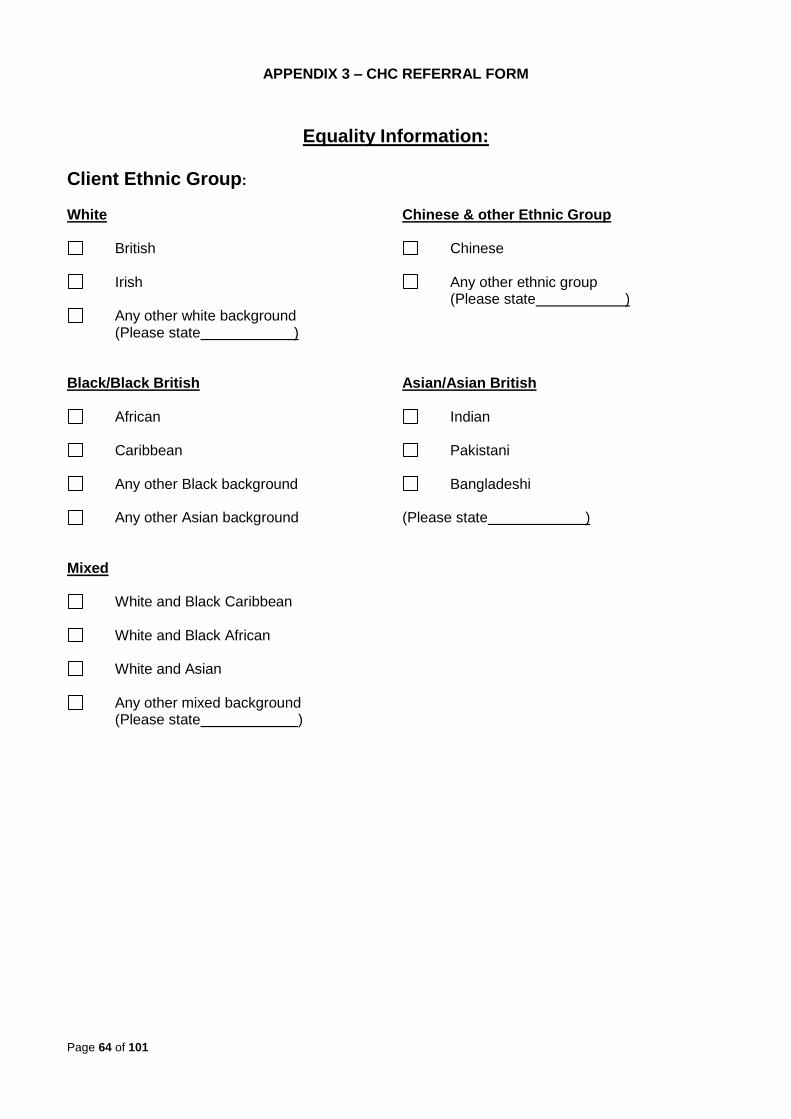
Page 64 of 101
APPENDIX 3 – CHC REFERRAL FORM
Equality Information: Client Ethnic Group:
White Chinese & other Ethnic Group
British Chinese
Irish Any other ethnic group (Please state )
Any other white background (Please state )
Black/Black British Asian/Asian British
African Indian
Caribbean Pakistani
Any other Black background Bangladeshi
Any other Asian background (Please state ) Mixed
White and Black Caribbean
White and Black African
White and Asian
Any other mixed background (Please state )

Page 65 of 101
Appendix 4 – Council Brokerage
EALING COUNCIL HOME CARE BROKERAGE PROCESS (PAGES 60 – 69)
Support at Home
Brokerage Sourcing & Purchasing Protocol
1. Following the decision to proceed with a community package social workers complete a
Brokerage Referral Form and send it to the team via FWi to action
2. The social worker is to commence completing a Care and Support Plan or Carers
Support Plan episode in parallel to sending the referral to Brokerage
3. Once received – the referral will be assigned to a named Brokerage Officer who will
undertake a matching exercise and send out a secure service request (using Egress
secure email) to those care providers who match the category requirements outlined in
the referral form. The following categories will apply to the Brokerage referral process:
Homecare
Enhanced Homecare
Reablement
Extra-care
Housing Related Support
Spot Care Agencies
Outreach
External Day Care
Independent Advocacy
Note 1 – in addition to the above categories the referral episode and form can be used
by social workers to send service requests to Brokerage for blitz-cleans
Note 2 – there is a separate FWi referral episode for social workers to request ‘floating
support’ services
4. The sourcing process will include Brokerage sending out service requests to WLA
Framework Providers in the first instance, followed by spot agencies if no ‘appropriate’
capacity is available via the framework. When sourcing services Brokerage will
incorporate the following call-off principles / arrangements:
1st
WLA Framework Providers
Brokerage will refer to the WLA call-off procedures when sourcing services from care agencies listed on the framework
Appendix 4 - page 1 of

Page 66 of 101
APPENDIX 4
2nd
Spot Care Agencies
Brokerage will select the ‘best’ option based on the following criteria:
Quality – the provider is registered with CQC and there are no concerns reported by CQC i.e. provider performance versus core quality standards.
Safeguarding – there are no current safeguarding concerns relating to the care provider
Appropriateness – the care provider can meet the service category requested; and accept the council’s terms & conditions
Capacity – the care provider has available capacity to meet the referral requirements
Value for Money – the care providers rates are in line with what the council would normally expect to pay for the requested service category
Note – Ealing Council will not normally commission services from care providers with a
CQC rating of ‘Inadequate’ or where an inadequate rating is ‘under appeal’ or the rating is ‘suspended’ – until all necessary action has been taken by the agency to address and remedy the identified service failures or the provider appeal is upheld by the CQC (see Appendix 1)
5. Care providers have 1-hour to respond to service requests issued by Brokerage –
earlier response times may be indicated if the service requirement is urgent
6. Once all ‘interested’ care providers have responded to the service request, Brokerage will
select the ‘best option’ in line with Point 4 of the sourcing protocol.
Note 1 – Brokerage will advise social workers by email – confirming the care provider,
care package details, costs and start-date; and add a case-note onto FWi
Note 2 – once notified social workers will finish the care and support plan or carers
support plan episode and request authorisation from the appropriate senior / manager; and advise Brokerage via FWi that the plan has been both completed and approved.
7. Where the request is for a cared for adult (via the Carer) then Brokerage will create a
Key Information Supplement Form in FWi, which will be used to provide the care
provider with key care and support information for the person.
8. Brokerage will purchase services on FWi and send the purchase episode to the
appropriate manager for authorisation (NHS purchases are completed using the NHS
options in the purchase episode). Authorisation requests will be sent as follows:
a) Care packages below £200.00 per week Team Manager
b) Care packages above £200.00 per week Service Manager
Appendix 4 - page 2 of
APPENDIX 4

Page 67 of 101
Brokerage will only send out an authorised purchase order (PO) once the care and support plan or key information supplement has been approved (in the case of NHS funded packages of care the PO is checked and approved by an authorised CCG manager). Care providers in turn only commence providing services following receipt of an authorised Purchase Order (PO) and Care and Support Plan or Key Information Supplement from Brokerage.
Note 1 – it is not permissible for council staff or care providers to action, vary or extend
care and support services over the phone or by email
Note 2 – in line with WLA Framework and Spot Provider Agreement criteria, care
providers will be expected to translate the support requirements outlined in the approved PO and Care and Support Plan or the Key Information Supplement into a local personalised provider support plan with the person in need.
9. Brokerage will purchase all homecare packages on the basis of Banded and Non-
Banded calls i.e. Time Specific calls. For the purposes of commissioning homecare
packages the Banded Call Structure is as follows: MORNING 07.00 11.59 AFTERNOON 12.00 17.59 EVENING 18.00 23.59 NIGHT 00.00 06.59 Non-Banded i.e. Time Specific calls are to be when a client requires a call or calls at a specific time e.g. a daily 8.30am call to assist with medication.
10. Suspensions and Re-starts – Brokerage will run a regular ‘daily suspension and re-
start report’ via FWi; and send restart and suspension PO’s to homecare agencies as
required.
Note – social workers must contact Brokerage prior to actioning the restart of a
homecare package on FWi to ascertain if the original care provider has capacity to reactivate the previous support package. If the care provider has no available capacity then a new referral to Brokerage requesting an alternate agency will be needed.
11. Requests for additional visits – care providers must contact the appropriate Duty
Team to request additional permanent or fixed term support. If agreed – duty workers are
to complete a referral form detailing the additional visits and send to Brokerage who will
complete the purchase on FWi. Brokerage will in turn issue an amended PO and revised
Care and Support Plan or Key Information Supplement to the care provider authorising
them to proceed with the agreed additional visits.
Appendix 4 - page 3 of APPENDIX 4

Page 68 of 101
Note 1 – If the request is for a one-off additional call only then there is no need to issue
a revised care and support plan with the PO. All one-off additional calls will be purchased separately by Brokerage on FWi with a clear start-date and end-date entered onto the system (this is to ensure that additional one-off support can be easily monitored, reported on, and when appropriate ended on the system)
Note 2 – financial restrictions have been lifted in FWi to allow team managers to
authorise additional calls in the event of a service manager being unavailable. However, if there continues to be a delay in authorising the ‘agreed’ additional visit, then the Brokerage Manager is authorised to send a ‘draft’ PO to the homecare agency confirming that the additional call can go ahead. Once the purchase has been subsequently authorised on FWi, Brokerage will then send out the required ‘permanent’ paperwork to the homecare agency.
12. Cost Neutral Time Changes – care providers can complete simple non-need
assessment related time-changes by agreeing these directly with the person in need or
the carer; and by amending the local provider support plan accordingly.
Note 1 – if the request, however, relates to a ‘time specific call’ or a ‘specified day’ e.g. a
change of time for a medication call or a change of day that the care package is to be provided then Brokerage must be advised of the changes as these must be reflected on FWi.
Note 2 – Brokerage will duly issue an amended PO to the care provider for all
permanent ‘time / day specific’ changes.
13. External reablement and ICE packages – beyond the initial 6-week period of
support (whilst awaiting a RAS allocation) will have a start-date with an open end-date
entered into the purchase episode on FWi – this is in line with current reablement and
ICE business processes.
14. Brokerage will purchase support at home and external community-based services for the
2 Mental Health Recovery Teams on submission of an authorised ‘hard copy’ of
the mental health referral form
15. Social care, unlike healthcare, is not free. How much the council will pay towards
persons’ care and support and how much the person will pay depends on their financial
circumstances and is subject to financial assessment. Information is available in the
booklet Determining Your Financial Contribution. Enquiries can be made to the
Financial Assessment Team on 020 8825 7066 or via
16. If a person is unhappy about the services provided or arranged for them by the Council
then they can contact the:
Appendix 4 - page of APPENDIX 4

Page 69 of 101
Customer Care Team 2nd Floor Perceval House London, W5 2HL Telephone: 020 8825 8100 E-mail: [email protected]
Appendix 4 - page 5 of
APPENDIX 4

Page 70 of 101
Appendix 1
CQC Rating System – 1st October 2014
Outstanding – the service is performing exceptionally well
Good – the service is performing well and meeting our expectations
Requires improvement – the service isn't performing as well as it
should and we have told the service how it must improve
Inadequate – the service is performing badly and we've taken
enforcement action against the provider of the service
No rating / under appeal / rating suspended – there are some
services which we can’t rate, while some might be under appeal from the provider. Suspended ratings are being reviewed by us and will be published soon
Note – Ealing Council will NOT normally commission services from registered providers
with a CQC rating of ‘Inadequate’ or where there inadequate rating is ‘under appeal’ or the providers current rating is ‘suspended’; until all necessary actions
have been taken by the provider to address and remedy the identified service failures or
where the provider rating appeal has been upheld by the CQC
Appendix 4 - page 6 of
APPENDIX 4

Page 71 of 101
Appendix 2
a) Equipment and telecare purchases – social workers will continue to requisition
equipment and telecare items in line with current arrangements. However, there is no
longer a need for hospital or locality teams to purchase episode these services on FWi.
The Council’s Equipment Officer will issue a report to Brokerage on monthly basis detailing all hospital and locality team requisitions. Brokerage will in turn complete the required purchase episode on FWi for recording and forecasting purposes
Note – this action only applies to hospital and locality teams. Occupational Therapy,
SVIP, and Substance Misuse Teams will continue to purchase equipment and telecare items on FWi via their existing workflow, which are not affected by these changes.
b) Non ‘support at home’ in-house provider purchases e.g. short-breaks,
day centre placements – social workers will continue to refer customers directly to
Ealing’s in-house provider services in line with current practice.
However, there is no longer a need for teams to purchase these services on FWi. Ealing’s in-house provider services will issue weekly movement reports to Brokerage, who will in turn complete the required purchase episodes on FWi for recording and forecasting purposes
Appendix 4 - page 7 of APPENDIX 4
Appendix 3
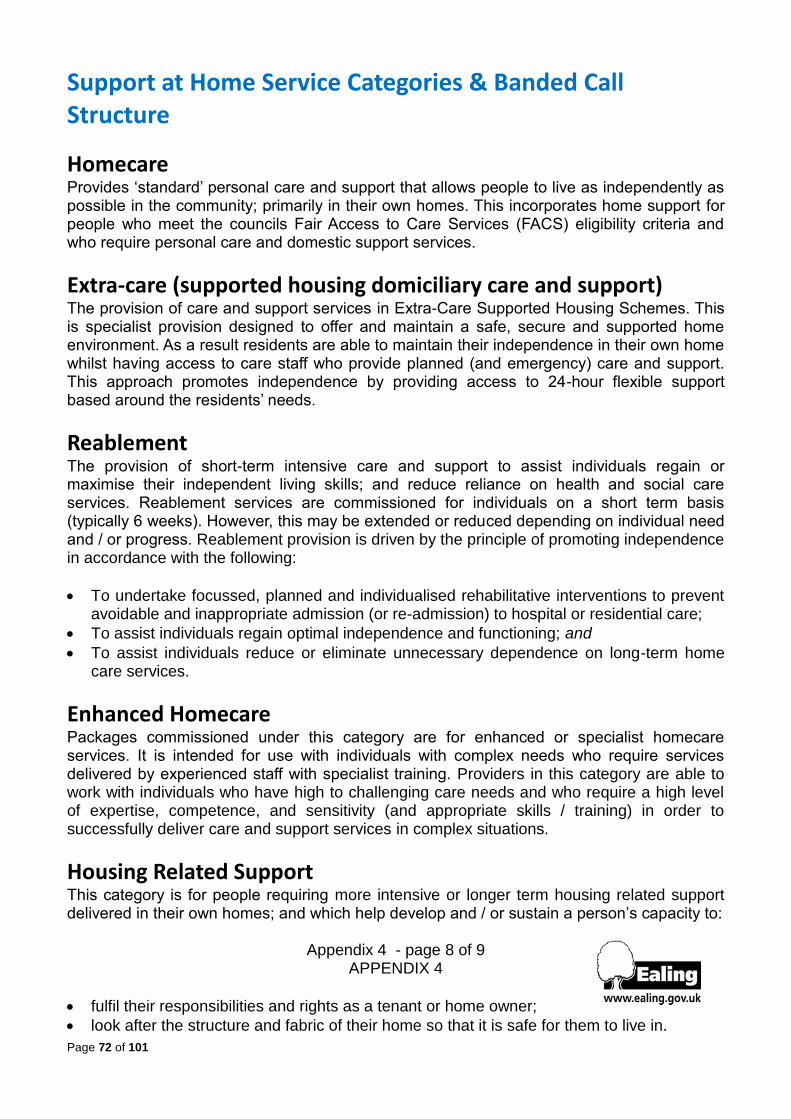
Page 72 of 101
Support at Home Service Categories & Banded Call Structure
Homecare Provides ‘standard’ personal care and support that allows people to live as independently as possible in the community; primarily in their own homes. This incorporates home support for people who meet the councils Fair Access to Care Services (FACS) eligibility criteria and who require personal care and domestic support services.
Extra-care (supported housing domiciliary care and support) The provision of care and support services in Extra-Care Supported Housing Schemes. This is specialist provision designed to offer and maintain a safe, secure and supported home environment. As a result residents are able to maintain their independence in their own home whilst having access to care staff who provide planned (and emergency) care and support. This approach promotes independence by providing access to 24-hour flexible support based around the residents’ needs.
Reablement The provision of short-term intensive care and support to assist individuals regain or maximise their independent living skills; and reduce reliance on health and social care services. Reablement services are commissioned for individuals on a short term basis (typically 6 weeks). However, this may be extended or reduced depending on individual need and / or progress. Reablement provision is driven by the principle of promoting independence in accordance with the following:
To undertake focussed, planned and individualised rehabilitative interventions to prevent avoidable and inappropriate admission (or re-admission) to hospital or residential care;
To assist individuals regain optimal independence and functioning; and
To assist individuals reduce or eliminate unnecessary dependence on long-term home care services.
Enhanced Homecare
Packages commissioned under this category are for enhanced or specialist homecare services. It is intended for use with individuals with complex needs who require services delivered by experienced staff with specialist training. Providers in this category are able to work with individuals who have high to challenging care needs and who require a high level of expertise, competence, and sensitivity (and appropriate skills / training) in order to successfully deliver care and support services in complex situations.
Housing Related Support
This category is for people requiring more intensive or longer term housing related support delivered in their own homes; and which help develop and / or sustain a person’s capacity to:
Appendix 4 - page 8 of 9 APPENDIX 4
fulfil their responsibilities and rights as a tenant or home owner;
look after the structure and fabric of their home so that it is safe for them to live in.

Page 73 of 101
understand information or access other services they may need
maintain or develop connections with local people and community facilities
learn skills that help them look after their home and live independently
Services will provide longer-term housing related support for people with eligible social care needs that include (but not restricted to) the following FACS eligible groups: People with multiple support needs; People with mental health problems; People with substance misuse problems; Older people with support needs; Homeless people and / or homeless families with eligible support needs; Ex-offenders or people at risk of offending with eligible support needs.
Banded Call Structure Banded calls will be delivered by the care agency within the following time periods:
MORNING 07.00 11.59
AFTERNOON 12.00 17.59
EVENING 18.00 23.59
NIGHT 00.00 06.59
Appendix 4 - page 9 of 9

74
Appendix 5 – Equalities Impact Assessment for NHS continuing Healthcare
Equality_Analysis.pdf

75
Appendix 6 – Community Rehabilitation Referral Form

76

77
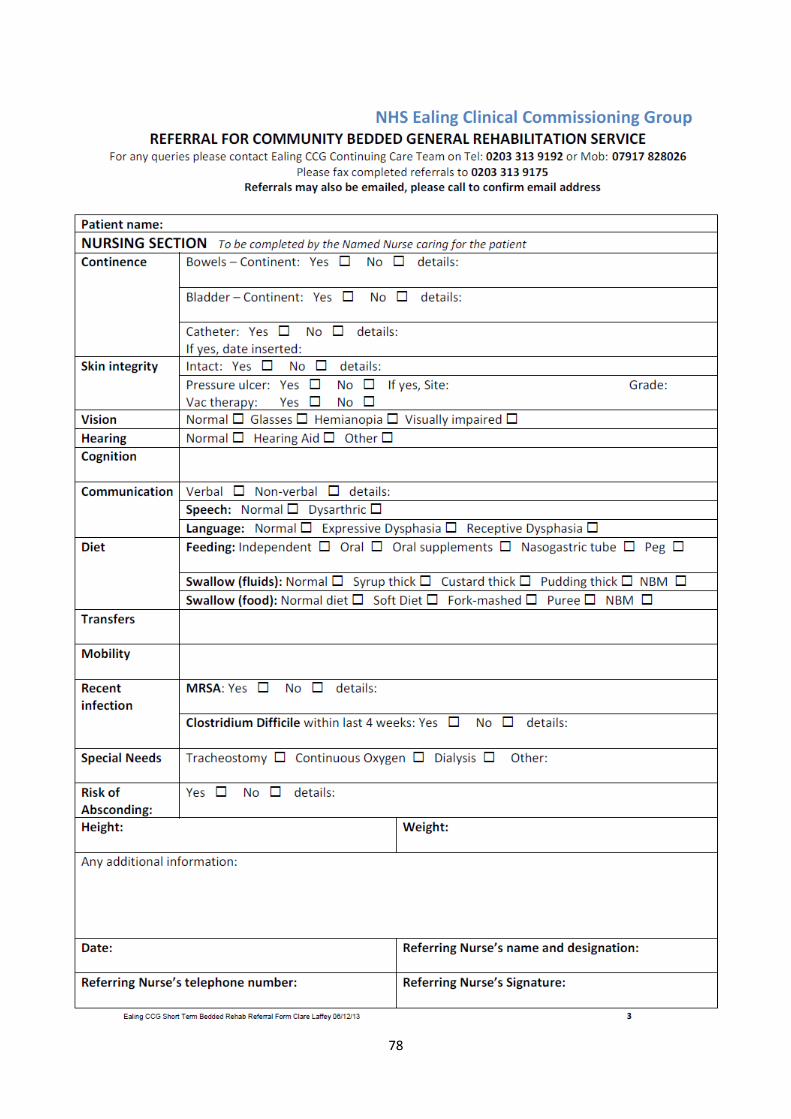
78

79
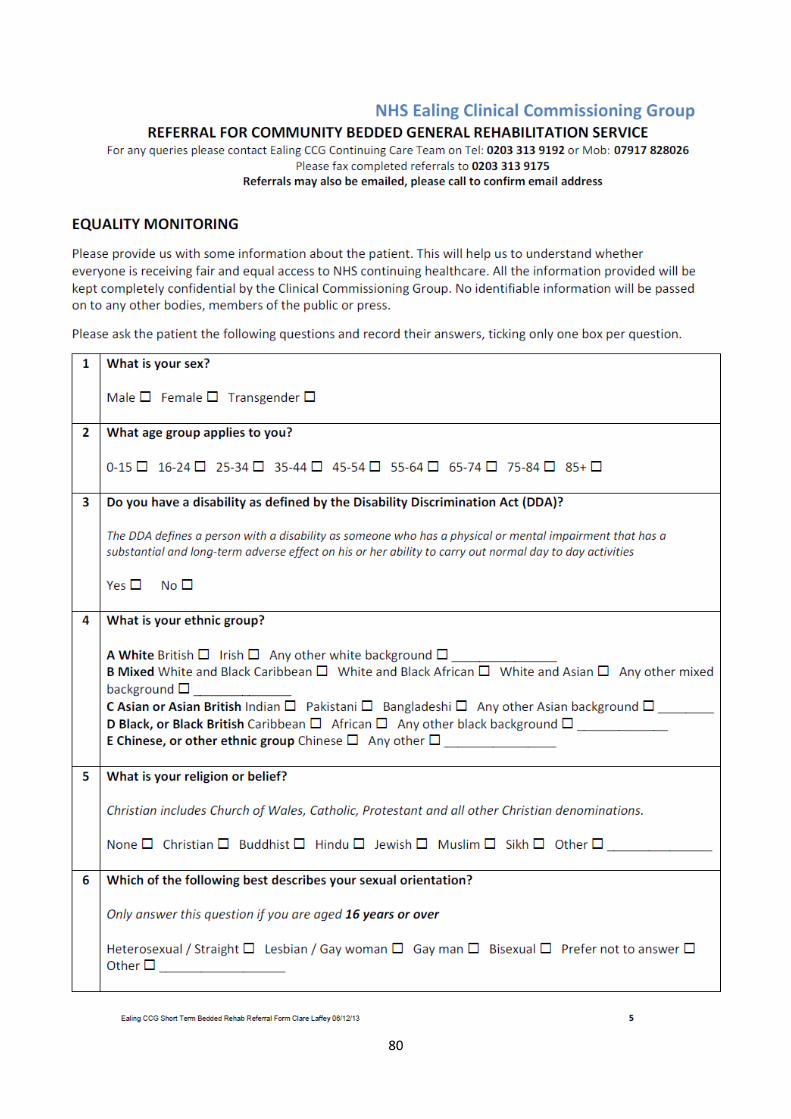
80
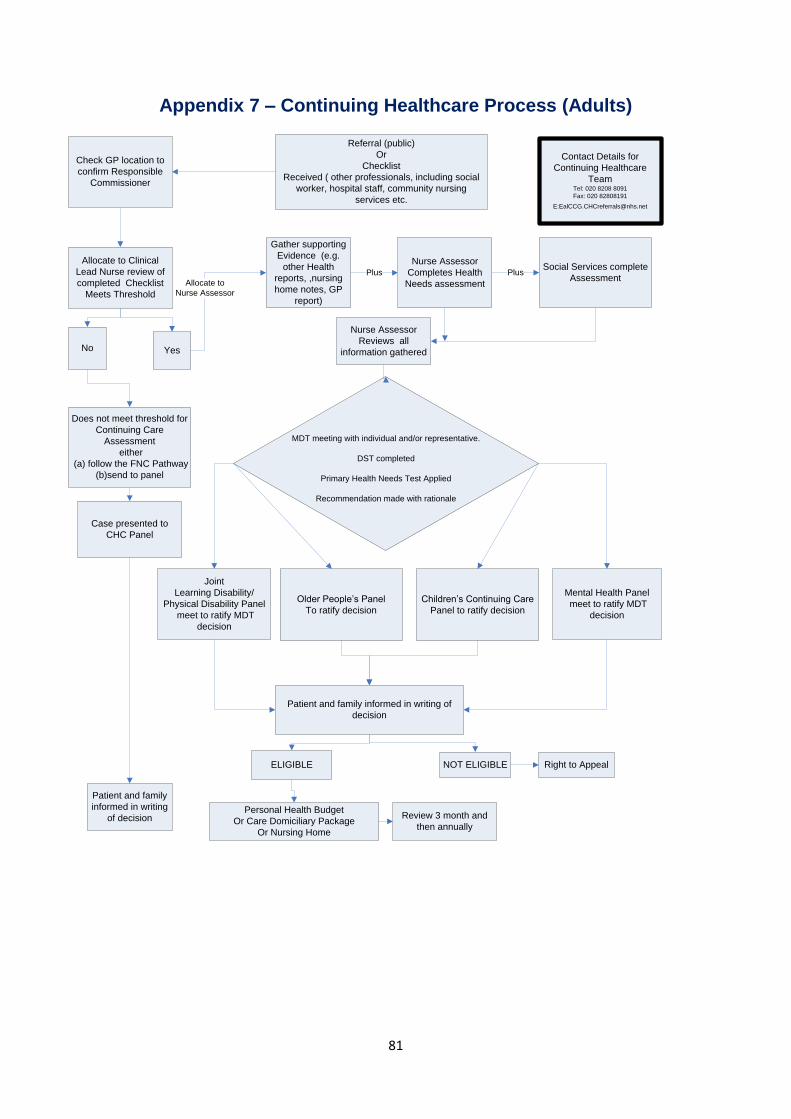
81
Appendix 7 – Continuing Healthcare Process (Adults)
Referral (public)
Or
Checklist
Received ( other professionals, including social
worker, hospital staff, community nursing
services etc.
Gather supporting
Evidence (e.g.
other Health
reports, ,nursing
home notes, GP
report)
Nurse Assessor
Completes Health
Needs assessment
Social Services complete
Assessment
Allocate to Clinical
Lead Nurse review of
completed Checklist
Meets Threshold
MDT meeting with individual and/or representative.
DST completed
Primary Health Needs Test Applied
Recommendation made with rationale
Joint
Learning Disability/
Physical Disability Panel
meet to ratify MDT
decision
Older People’s Panel
To ratify decision
Does not meet threshold for
Continuing Care
Assessment
either
(a) follow the FNC Pathway
(b)send to panel
Personal Health Budget
Or Care Domiciliary Package
Or Nursing Home
Mental Health Panel
meet to ratify MDT
decision
Nurse Assessor
Reviews all
information gathered
Patient and family
informed in writing
of decision
Check GP location to
confirm Responsible
Commissioner
No
Plus Plus
Review 3 month and
then annually
Case presented to
CHC Panel
Yes
Allocate to
Nurse Assessor
Contact Details for
Continuing Healthcare
TeamTel: 020 8208 8091
Fax: 020 82808191
Patient and family informed in writing of
decision
Children’s Continuing Care
Panel to ratify decision
ELIGIBLE NOT ELIGIBLE Right to Appeal

82
Appendix 8 – CHC Older People’s Panel ToR
NHS Ealing CCG and Ealing Social Services Joint Older Peoples Panel
Terms of Reference – for NHS Continuing Healthcare Consideration
1. Purpose
The purpose of the meeting is; a. to formally ratify community continuing healthcare assessments that have taken place,
b. to discuss community cases where there is a dispute between the Social Worker/Care
Manager and the Lead Health Co-ordinator (CCG Assessor) regarding the domain
weightings and/or the recommendation i.e. the outcome of the assessment. And
c. to ensure consistency and quality of decision-making (point 162. of the National
Framework for NHS Continuing Healthcare and NHS-funded Nursing Care.
Henceforth referred to the National Framework)
2. Frequency of Meetings
a. The Panel will meet every Tuesday morning between 09:30 – 12:30
b. Continuing Healthcare cases will be heard between 11:00 – 12:30
3. Agenda Items
a. NHS Ealing CCG will inform Ealing Social Services (Irene Byrne), by 16:00 the day
before the panel;
i. cases for information (i.e. hospital discharges that are not eligible for any
NHS funding, are eligible for FNC or eligible for Continuing Healthcare and fast
track assessments)
ii. cases for ratification e.g. cases where health and social services have
complete an assessment and are in agreement and/or
iii. cases for discussion e.g. disputes, assessments where a social worker was
not present.
4. Panel Quorum
a. Senior Manager CCG
b. Senior Manager SS
Also in attendance c. Lead Health Co-ordinator/Social Worker to present the case
d. Minute taker
5. Decisions
The Panel members will consider the evidence to ensure consistency in the decision making process and that assessments are carried out in line with the National Framework
a. The outcome – Social Services and the CCG will agree the outcome of the
assessment as follows;
i. The person is not eligible for NHS Funded Nursing Care or NHS Continuing
healthcare
ii. The person is not eligible for NHS Continuing healthcare but is eligible for
NHS-funded Nursing Care
iii. The person is eligible for NHS Continuing Healthcare
iv. An outcome could not be agreed

83
6. Disputes
This section explains the process to be followed in the event that there is a disagreement between the Social Worker and Lead Health Co-ordinator about the content or outcome of the assessment.
a. The social worker will put in writing the following and send it to the NHS Co-Chair
of the Panel (currently Lorraine Charlton) along with George Mamombe, Shirlene
Hawkson and the Lead Health Co-ordinator:
i. Specifically what they disagree with clearly stating the content, page numbers,
domains and outcome they believe should be.
ii. The full rational for their disagreement.
iii. the evidence to support their argument that this area should be reviewed. This
would include for example further medical/care home records/behaviour charts.
iv. their proposed amendment e.g. what they think the level of need should be or
what they think the outcome should be.
v. Evidence that their disagreement is congruent with the National Framework.
b. NHS Ealing allocate Panel Slot – The CCG will arrange the case to be discussed at
the Joint Panel
c. OP Panel Hearing – the Social Worker and Lead Health Co-ordinator will jointly
present the case.
i. Areas of dispute – the social worker will systematically go through each
disputed point
ii. Agree domain weightings – The panel members will agree whether the
domain “level of need” should be amended
iii. Agree outcome – The panel will apply the primary health need test and agree
the proposed outcome which will be as described in point 5 above.
7. Dispute Escalation Process
a. In the event that Social Services and the CCG cannot agree on an outcome, the Panel
members will make a decision as to whether to;
i. Complete a new up-to-date independent assessment. This might include an
assessment completed an alternative staff from the CCG and Socials Services,
or it might involve commissioning an independent organisation to complete the
review. This new assessment will be re-presented to the Panel as described in
section 1-5.
ii. Escalate the process through the Dispute Escalation Policy.
iii. In order to prevent delay the provision of the care package, the Co-chairs will
agree on a temporary funding arrangement. This usually will mean either
Health or Social Services funds the care with immediate effect, under the
proviso that they will recharge in the event that the outcome is favourable.

84
Appendix 9 – CHC Children Process Children/ Young People Continuing Healthcare Process
Referral Received with parental consent to access medical
records and carry out a CHC Assessment
Check GP location to confirm Responsible Commissioner
Assessment Process Starts. Clinical and supporting evidence gathered from professionals
involved in the child/YP health care. E.g. Community Paediatrician, therapy leads, Community Nursing, Tertiary
hospital consultants
Evidence collated and presented to continuing care panel
Eligible for continuing care
Not eligible for continuing care
Family, initial referrer and
other professionals informed of the findings and decision.
Refer to other services if appropriate
Package of Care Core Offer to family
Care begins
Re-assess at agreed time
Decision challenged
Decision explained to challenger
Resolved
Formal complaint
Referral check list to ensure appropriate referral
MDT including
representation from Social
Care and Education, where
appropriate, to discuss
Core Offer
Package of Care tailored to meet child’s
individual needs

85
Appendix 10 – Memorandum of Understanding Memorandum of Understanding for Continuing Healthcare At Home THIS AGREEMENT is made between
(1) Ealing Clinical Commissioning Group, ("the CCG") Located at: Level 3, Perceval House, 14/16 Uxbridge Road, Ealing, W5 2HL
(2) [Insert name of Individual] of [Insert Address] ("you" or "[Insert Name]);
(3) [Insert name of any carer who will be involved in the provision of the service] ("the Representative")
BACKGROUND You/[Insert Name] have been assessed as eligible to receive NHS Continuing Healthcare funding and this Memorandum of Understanding sets out the agreement reached between the CCG in relation to the provision of your care. [Insert name of patient] has been deemed not to have capacity to make the decision as to where they wish to receive care.] The [Representative] [you] has requested that you receive the care package at Home. The CCG has agreed that a home care package is provided on the terms set out in this Memorandum of Understanding. Provision of Care
The CCG has agreed to provide the Care Package as set out in your Care Plan which has been assessed to meet your current assessed care needs. The Care Package will be provided at the following address ("Home"): [Insert Address] Review The Care Package will be reviewed regularly by your care manager and the Continuing Health Care team. An initial review will take place within three months of the start of the package and at least once a year thereafter to see if your health needs are being met. Reviews will be undertaken more frequently if your needs or outcomes change substantially. You will be informed by either your Care Manager or Continuing Healthcare Nurse Adviser about the date of the review. You or your Representative may request a review to be undertaken by the CCG if you think your care needs have changed or the care package is not meeting your assessed needs. In the event that the assessed care needs have increased, the CCG will consider whether the care provision needs to change in order to meet those care needs. Where the care provision increases, the CCG will assess whether it remains appropriate for the care at home package to be provided. In doing so, the CCG will take the considerations set out in the CCG's Choice Policy and the cost of alternative care packages that would meet your assessed needs. If you are assessed as no longer eligible for receipt of NHS Continuing Healthcare then the CCG will inform the Local Authority so that a joint assessment can be carried out.
86
Patient and Representative Obligations You and your Representative agree to co-operate with a review of your needs. You and your Representative acknowledge and recognise that if your care needs change then the CCG will need to re-assess the continued provision of the care at home package. If the CCG considers that the care package is no longer appropriate or cost effective then you agree to co-operate with the CCG in choosing and moving to alternative arrangements. You and your Representative acknowledge that the CCG can issue a withdrawal of care notice if it considers that the provision of the care at home package is no longer appropriate. If you decide not to take up alternative package of care offered by the CCG then you will be considered to be refusing NHS funding. You and your Representative agree to treat all care workers with dignity and respect and will take all the action that you and your Representative are required to do in the Risk Assessment. You and your Representative will make sure that the care workers have the appropriate facilities so that they can provide your care. This includes clean and accessible bathroom and kitchen facilities. You and your Representative acknowledge that the CCG will take any action it considers necessary in the event that it considers that there is a risk to the health or safety of any of its staff or agents including withdrawing the provision of care. I have read, understand and agree with the Memorandum of Understanding, the Care Plan and Risk Assessment attached. Name of Individual receiving care: ……………………………………............................. Individual Receiving Care Signed by: …………………………………… Individual Receiving Care Printed Name …………………………………… Date……………......... Representative Signed by: …………………………………… Representative Printed Name: …………………………………… Date……………......... CCG Signed by: …………………………………………………… Date…………… Relevant Care Manager………………………Tel……………….

87
Appendix 11 – Children’s Panel ToR
NHS Ealing CCG Children’s Continuing Care Panel Terms of Reference
CONSTITUTION This Group shall be known as the Ealing CCG Interim Children’s Continuing Care Panel. The Standing Orders and Standing Financial Instructions of the Trust, so far as they are applicable, shall apply to meetings and proceedings of this Committee.
ROLE OF THE PANEL
In accordance with the 2010 National Framework for Children’s continuing care the process of determining eligibility should be fair and consistent process. Ealing CCG has chosen the establishment of a panel for this reason. The continuing care coordinator will present the assessment form, health, social care, education and family comments. A recommendation and costed care options will also be presented to the panel. In exceptional circumstances and with the agreement of the chair verbal reports of the child’s needs can be presented to the panel. The panel must first consider the evidence placed before them and if there is enough information to make a decision. The initial decision on eligibility should be based on the health needs of the child or young person. In most circumstances a child or young person will be eligible if they have high needs in three care domains, severe in one or priority in one domain, or they are at the end of life This Panel will be required to:
Scrutinise and agree decisions concerning the NHS funding eligibility for continuing care funding of Children between the ages of 0 up to 18 years registered with Ealing CCG GPs or Looked after children in the care of London borough of Ealing.
Allocate hours of care Report directly to NHS Ealing Director of Strategy and commissioning. Review applications for children’s NHS continuing care submitted to NHS Ealing. Review the quality of assessments provided to the Panel, and advise where improvements
are indicated, to support good practice throughout the process. To note recommendations made by Multi-disciplinary team. To provide forum for discussion and agreement on borderline the social acre and
educational needs of the child along with the views of the family should be considered. Any decision made or upheld by the panel must be based on an accurate, comprehensive
and recent assessment (undertaken within 6 weeks of the panel date) To take a view about the quality of individual assessments and identify if the assessment
is insufficiently robust to support or reject a decisions made by MDT. Any decision regarding eligibility for NHS Continuing Care should be made independently of the decision of a package of care to be offered.
Urgent decisions can be made outside Panel but these must be subsequently scrutinised and ratified by the Panel at the next possible opportunity.
The Panel may:
Agree the application for a continuing care package of support, based on the framework for continuing care

88
Decline the application based on the recommendation of the coordinator using the framework for continuing care
Defer a decision, and refer the assessment back to the coordinator for further information or assessment.
Decline the funding of continuing care where the recommendation is not supported by the evidence presented.
Decline funding for continuing care but agree to funded nursing care for clients currently resident or planning to become resident in nursing home within the next month
MEMBERSHIP
The membership of this group will consist of: Chair, plus a commissioner and a health care professional and a social care professional. If the cases are requesting support in school an education professional will be required to sit on the panel. If the request is based primarily on challenging behaviour/ mental health needs then a children’s commissioner for CAMHS must attend the panel. The Chairperson will be appointed by the CCG and will have the responsibility of informing the family of the panel decision in writing within 5 working days.
Attendance at meetings and Nominated Deputies
Individuals will be expected to routinely attend meetings and to contribute to the decision making process for cases on the agenda. In the absence of the Chair a nominated Deputy will be identified who must be an employee of Ealing CCG. If any of the members cannot attend a meeting a nominated Deputy would be appreciated where possible.
The membership of the group may be extended to include other staff to provide specialist advice of particular cases. Observers will not be considered additional members or be able to comment on decisions unless invited to do so by the panel chair.
Additional Members
The membership of the group may be extended to include other senior managers who may from time to time be invited to attend. Communicating the Outcome The panel secretary will recorded the decisions of the panel for individual children and maintain the central record of decisions. He or she may be delegated by the chair to draft the letter of decision to the family. The continuing care coordinator will be delegated by the panel chair to inform the professionals involved in the assessment process of the panel decision. All decisions made by the panel must be documented in full on the attached reporting tool and the continuing care database.
Where the panel has chosen not to uphold the recommendation of the MDT a detailed commentary on the decision will be made available to any relevant party.

89
FREQUENCY OF MEETINGS
Meetings will be held monthly or as and when deemed necessary at the discretion of the Chair but no less than every two months unless there are no cases to consider.
REPORTING ARRANGEMENTS An aggregate review of the decisions of the panel will be undertaken on a minimum of an annual basis. It is the duty of the CCG continuing care coordinator to ensure that this review is undertaken, presented to the panel and a copy sent to the Director of Strategy. Review of the terms of reference These terms of reference will be reviewed 3 months after approval.

90
Appendix 12 – MH Panel ToR
Mental Health Complex Care Panel Terms of Reference
Draft S117 Joint Policy v2.docx

91
Appendix 13 – Physical Disability and Learning Disability Panel Terms of Reference
This document is currently in draft and will be submitted to the appendix on approval
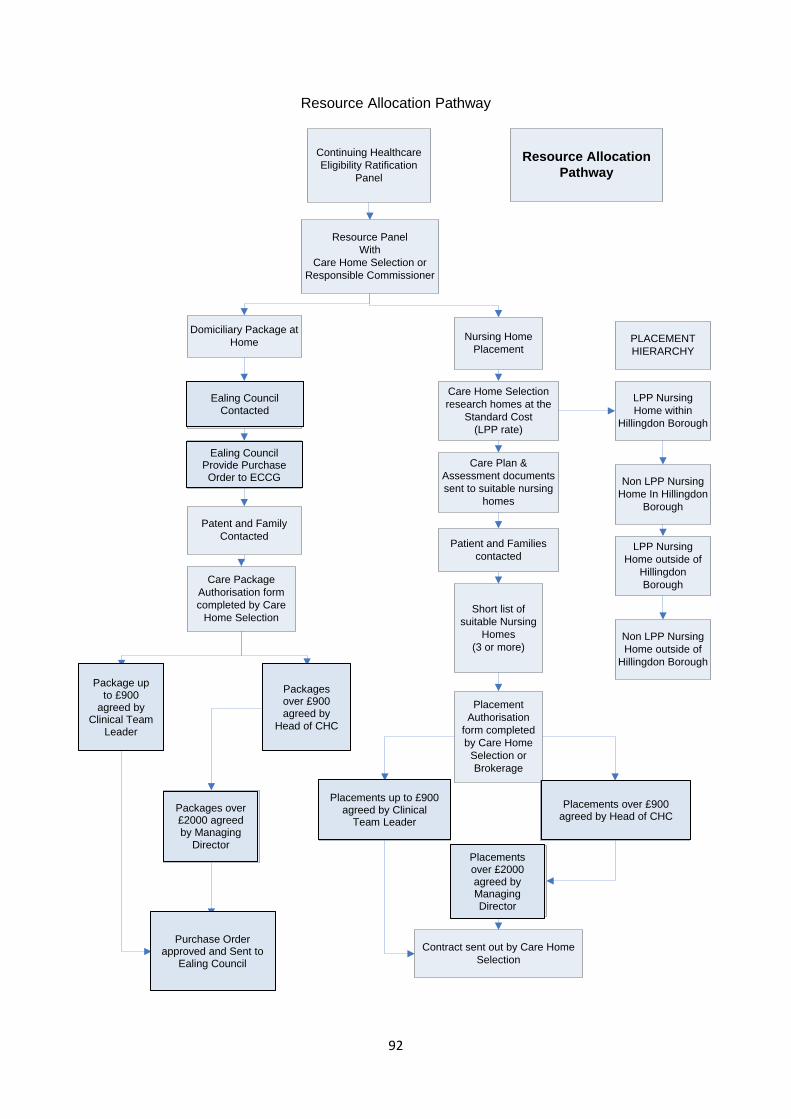
92
Resource Allocation Pathway
Continuing Healthcare
Eligibility Ratification
Panel
Resource Panel
With
Care Home Selection or
Responsible Commissioner
Domiciliary Package at
HomeNursing Home
Placement
Care Plan &
Assessment documents
sent to suitable nursing
homes
Patient and Families
contacted
Short list of
suitable Nursing
Homes
(3 or more)
Care Home Selection
research homes at the
Standard Cost
(LPP rate)
Placement
Authorisation
form completed
by Care Home
Selection or
Brokerage
Placements up to £1000
per week authorised by
Team Manager Continuing
Healthcare
Care Home Selection
research suitable
provider
Care Plan and
assessment provided
to Agency
Patent and Family
Contacted
Care Package
Authorisation form
completed by Care
Home Selection
Package up to
£1000 per week
Authorised by
Team Manager
Continuing
Healthcare
Care Package
Agreement sent to
Domicilliary Care
Agency by Care Home
Selection
Placements over £1000 per
week authorised by Head of
non acute Commissioning.
Packages over
£1000 per week
authorised by
Head on non -
Acute
Commissioning
Packages over
£1500 per week
Borough Director/
Board approval
Packages over
£1500 per week
Borough Director/
Board approval
Contract sent out by Care Home
Selection
PLACEMENT
HIERARCHY
LPP Nursing
Home within
Hillingdon Borough
Non LPP Nursing
Home In Hillingdon
Borough
LPP Nursing
Home outside of
Hillingdon
Borough
Non LPP Nursing
Home outside of
Hillingdon Borough
Resource Allocation
Pathway
Ealing Council Contacted
Ealing Council Provide Purchase Order to ECCG
Package up to £900
agreed by Clinical Team
Leader
Packages over £900 agreed by
Head of CHC
Packages over £2000 agreed by Managing
Director
Placements up to £900 agreed by Clinical
Team Leader
Placements over £900 agreed by Head of CHC
Placements over £2000 agreed by Managing Director
Purchase Order approved and Sent to
Ealing Council

93

94
A brief guide to children’s continuing care. What is continuing care? Continuing care is a generic term for a package of care that will be required when a child or young person has needs arising from disability, accident or illness that cannot be met by existing universal or specialist services alone. Continuing care packages are designed, wherever possible, to provide health care in the child or young person’s home, but it may be provided in another setting such as a residential school, residential placement or hospice. The health care will be funded by the NHS but may be provided in coordination with education and social care support. How does the continuing care process work? The continuing care process is a three-phase activity which Health services, local authorities and schools (if appropriate) work together to provide care for children and young people with complex health issues. The three phases are
1. assessment, 2. decision-making, 3. arrangement of care.
How does this work in practice?
To start an assessment a referral is made to the Ealing CCG’s Children’s Continuing Care Coordinator. The referral can come from any
Appendix 14 – Children’s Continuing Care Leaflet
health, social care or education professional involved with the child or young person. You should have been asked if an assessment can be started as it does require information about you and your child to be collected from a range of services. You will be asked to sign your consent for the referral to be sent and an assessment started. The assessment phase is led by Ealing CCG’s children’s continuing care coordinator. The four areas that should be considered in the assessment are:
The care preferences of the child or young person and their family;
A Holistic assessment of the child or young person and their family, including carer assessment;
Reports and risk assessments from the multidisciplinary team.
The children and young people’s health needs which looks at 10 different areas of your child health
How do I make my views or concerns known? You and your family will be asked about what type of care you want, where and how you would like it to be delivered. Wherever possible you will also be asked to contribute to the assessment phase by giving information regarding your child’s health and the tasks you carry out for them. Who will have to be contacted for information?
The continuing care coordinator will ask for assessments from health, social care and sometimes education. Health staff who are involved in the care of the child or young person will be asked to about the health needs of the child You will be asked to give your permission before staff are contacted What is involved in the decision making phase? Once all the information is collected a recommendation is made to a continuing care panel. The recommendation will be that the child or young person is or is not eligible for a continuing care package of support. The continuing care panel has health, social care and education representatives. The panel will look at the evidence presented and make a decision regarding whether your child meets the threshold for Continuing Care support.
95
After the panel has made a decision you will be informed in writing within 1 week of their decision. How does the arrangement of provision phase work? If the panel agrees that your child IS eligible for Continuing Care support, the continuing care coordinator will contact you to discuss the care package on offer and how it will be provided. The care will start as soon as possible but it may take some time if staff need to trained to care for your child. What happens if we are not offered continuing care? Where a child or young person is found not to have a need for continuing care, a clear explanation of the rationale for the decision should be provided to the child or young person and family. In this instance, their needs should be addressed through existing universal and specialist services using a case management approach.
Contact Details:
Children’s Continuing Healthcare NHS Ealing CCG Martin House 1 Swift Road
Southall UB2 4RP
Tel: 020 8280 8091 Fax: 020 8280 8191
Children’s Continuing Care A brief guide for families and
staff
This guide has been written for Patients, carers and children to answer some of
the most frequently asked questions about children’s continuing care in Ealing

96
Appendix 15 – Information Sheet for Parents/Carers of Children
Information for Patient and Families
Following the completion of the Continuing Healthcare Assessment
This information sheet has been put together to give you information about what happens after your Continuing Healthcare Assessment has been completed. Background Information The nurse assessor will have included you and your family in the assessment and you will have been given the opportunity of providing any additional information to help the Multi disciplinary Team make a decision about whether you are eligible for full NHS funding for your care. The nurse assessor will talk to the Multi Disciplinary Team which normally consists of other NHS staff who have been involved in your care, like your GP, District Nurse, Consultant or Specialist, they will also speak to the social worker involved with your case. Together they will make a decision on your eligibility using the Criteria and framework Tool provided by the Department of Health. (This is a nationwide practice). Once a decision has been made, you will receive a copy of the Decision Support Tool so that you and your family can read it and provide us with any comments you think should be included. Your assessment will then be considered by NHS Ealing’s Continuing Healthcare Panel who will read through the papers and ratify the Multi Disciplinary Team’s decision. The Panel can’t change the decision made by the Multi Disciplinary Team but it can ask for additional information to support the decision so in some instances cases can be deferred to a future meeting. The nurse assessor will let you know if this happens in your case. What Happens Next ? Once the Continuing Healthcare Panel has ratified the decision your case will be passed to the most appropriate team (Health or Social Services) who will make a decision about the options for meeting your care needs. NHS Ealing will write to you to confirm the outcome of your assessment and this letter will give you information on what to do if you are not happy with the decision that has been made. Below are some of the options that may apply to you 1 You are assessed as meeting the criteria for Fully Funded NHS Care Your case will be transferred to Care Home Selection who is NHS Ealing’s broker for
accessing care services. They will telephone you to discuss the type of care that is available to meet your needs. It is important that you do not make private arrangements for your care as NHS Ealing may not be able to agree to those arrangements. Please speak to Care Home Selection before making any private arrangements and they will advise you on the options that are available to you, their contact telephone number is 01895 488768.
NHS Continuing Healthcare falls into two main categories:-
97
Care in your own home. This will be provided by carers who are agency carer’s that are employed by NHS Ealing through our brokers, (Care Home Selection) to come into your home to assist you with your personal care needs, getting up and going to bed, washing, dressing and respite care, etc. Your health needs will continue to be met through your GP, District Nursing Service and any other specialist health services you need. Care Home Selection will set up the care for you and monitor the care arrangements to make sure that it is meeting your needs.
If you need 24 hours nursing care then your care can be provided in a Nursing Home within the Borough of Ealing. Care Home Selection will discuss which homes are available and can meet your needs. You and your family will be asked to view the homes that are suitable and make a decision on the one you prefer. Once you have agreed on the Nursing Home then Care Home Selection will make all the arrangements for your admission and they will regularly monitor your stay in the home.
If you or your family are unhappy with the care that is being provided to you then you should contact Care Home Selection in the first instance who will try and sort out the issues that you have. They will also tell NHS Ealing and a review of your care plan may take place. 2 You are assessed as not meeting the Continuing Healthcare Criteria but you have been
assessed as having nursing needs.
If you have a social worker, then they will discuss with you the options that are available to meet your care needs, if you remain at home then your health needs will be provided by your GP, District Nurse or Specialist Team.
However if you should be admitted to a Nursing Home then you would be eligible for a Funded Nursing Care contribution which will be paid directly to the Nursing Home.
If you are making your own private arrangements for your care in a nursing home and have a nursing need then you will still receive the Funded Nursing Care contribution, you should let the local NHS in the area where the nursing home is know and they will make arrangements for the nursing home to receive the weekly payment directly if you meet the eligibility for this following a funded nursing assessment .
3 You have been assessed as not meeting the Continuing Healthcare Criteria and you have no nursing needs.
If you have a social worker, then they will discuss with you the options that are available to meet your care needs. Any health needs would be met through your GP.
If you are making your own private arrangements for 24 hours care then you should be looking at a residential care home to meet your needs. However if you choose to go into a Nursing Home you will not be eligible for the Funded Nursing Care contribution you will have to pay the total weekly fee. In certain circumstances Social Services may be able to help you with your arrangements.
4 Further help and information
You can get further help and information on the Department of Health Web site at www.dh.gov.uk or alternatively you can contact the Continuing Healthcare Team on 01894 485500 or Care Home Selection on 01895 488760

98
Appendix 16 – Appeal Process Flow
Appeal Received
Informal Meeting
Local Resolution
Independent
Resolution
Independent Review
Panel
Health and
Parliamentary
Ombudsman
Formal Appeal Panel
RESOLVED
NOT
RESOLVED
RESOLVEDNOT
RESOLVED
RESOLVED
NOT
RESOLVED

99
Appendix 17 – Community Bedded Rehabilitation Discharge Summary
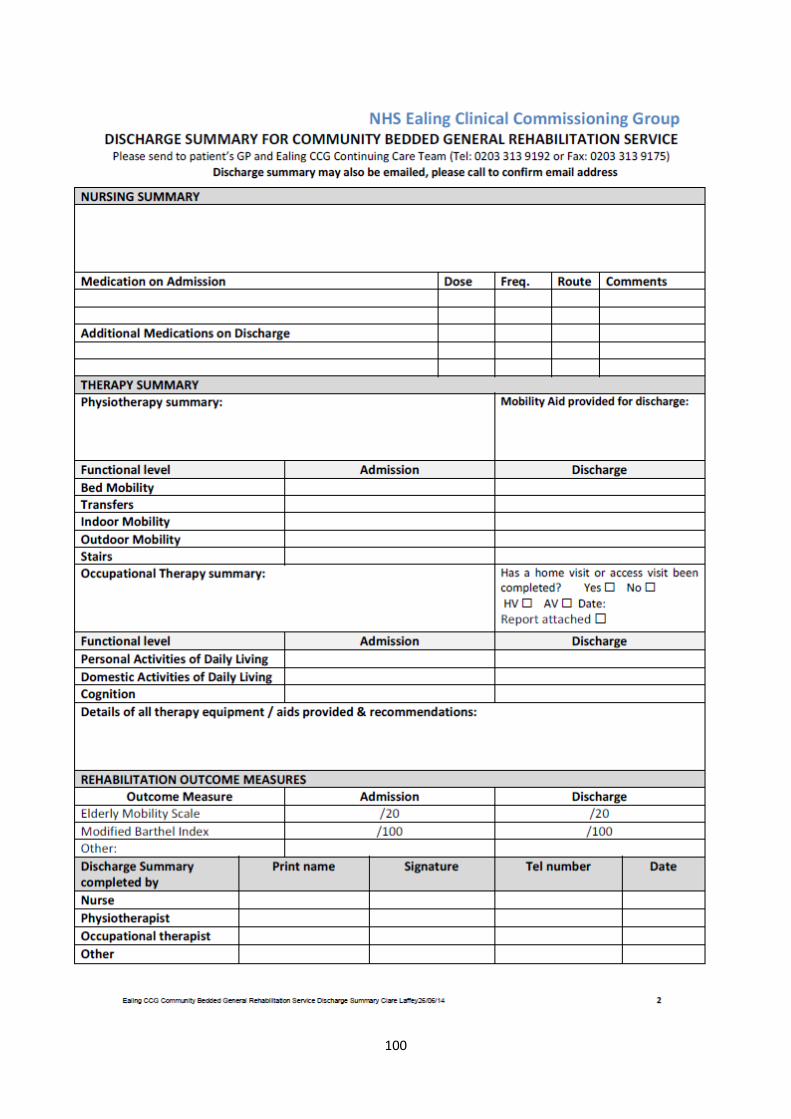
100

101
Appendix 18 – Rehabilitation Referral Pathway
REFERRAL PATHWAY FOR THE COMMUNITY BEDDED GENERAL REHABILITATION SERVICE
The patient needs a short period of in-patient general rehabilitation The patient no longer requires acute care and their rehabilitation needs cannot
be met by community rehabilitation services within their home
The patient is:
Registered with an Ealing GP
Suitable for Nurse and Therapy led care
Medically stable – no further medical input / investigations needed
Expected to achieve their rehabilitation goals within 6 weeks
ALTERNATIVE REFERRAL PATHWAYS FOR
REHABILITATION FOR EALING GP REGISTERED
PATIENTS
Please request the correct referral form for the different
services listed below
Clayponds Hospital -Specialist in-patient neurological rehabilitation -Complex general rehabilitation requiring medical management / long term rehabilitation >6/52 (Ealing Hospital only)
Tel: 0208 232 3353
Intermediate Care in Ealing (ICE)
- Rehabilitation & supported discharge within the home - Ealing Hospital patients only
Tel: 0208 967 5567
Ealing Day Treatment Centre (EDTC) -Slow stream community based rehabilitation
Tel: 0208 571 1143
ENable -Community neuro- rehabilitation for stroke & long term neurological conditions (LTC) -Supported discharge for stroke patients in NWL HASU’s & SU’s & neurological patients in Ealing Hospital & Clayponds
Stroke Team: Tel: 0208 967 5000 ext 3565 Long Term Conditions Team: Tel: 0208 568 0679
Hounslow Single Point of Access (SPA) -Patients who have a Hounslow GP and require on-going community rehabilitation
Tel: 0208 630 3943
Provide the patient (or NOK) with the patient information leaflet describing the 2 different Rehabilitation Providers who can offer this service:
Beech Unit in Manor Court Care Home in Southall
Jasmin Ward in Clayponds Hospital in South Ealing
Establish if the patient has:
A preferred choice of Rehabilitation Provider
Consented to community based inpatient rehabilitation
Consented to sharing their details with Ealing CCG Continuing Care Team for referral and monitoring their clinical care
The referral will be screened by the Ealing CCG Rehabilitation Team to assess if the Community Bedded General Rehabilitation Service is a suitable pathway
and could meet the needs of the patient
REFERRAL DECLINED
If the needs of the patient could not be met by the service, the referral will be declined and the referrer informed by Ealing CCG Rehab Team
REFERRAL ACCEPTED
The referral will be sent to the patient‘s choice of Rehabilitation Provider (or where a bed is available, if there is no preference) The Rehabilitation Provider will complete a preadmission assessment; if no issues are identified, they will arrange transfer of the patient with the referring ward
The MDT caring for the patient should complete and sign all sections of the Community Bedded General Rehabilitation Service Referral Form
The completed referral and a copy of the latest blood results should be sent to Ealing CCG Rehabilitation Team (based in the Continuing Care Team)
Fax: 0208 280 8189 or email: [email protected] Tel: 0208 280 8188