oncology highlights from asco 2009 melanoma … web… · oncology highlights from asco 2009...
TRANSCRIPT

Oncology Highlights from
ASCO 2009
Melanoma
August 1, 2009
Santa Monica, CA
Jeffrey Weber M.D. Ph.D.
Moffitt Cancer Center
Tampa, FL
COI Disclaimers
• Honoraria from Novartis, Roche, Medarex
and BMS, all less than $10,000 dollars in
any year
• I was named on a patent relating to
ipilimumab that was assigned to the Univ
of Southern California and later was
abandoned by the filer

ASCO 2009 Theme:
Melanoma enters the era of
personalized, targeted therapy

Phase I study of PLX4032:Proof of concept for V600E BRAF
mutation as a therapeutic target
in human cancer: abstract #9000
K. Flaherty,1 I. Puzanov2, J. Sosman2, K. Kim3, A. Ribas4, G. McArthur5, R. Lee6, J. Grippo6, K. Nolop7,
P. Chapman8
1University of Pennsylvania 5Peter MacCallum Cancer Centre2Vanderbilt University 6Hoffmann-La Roche Inc3MD Anderson Cancer Center 7Plexxikon Inc4University of Califorinia, Los Angeles 8Memorial Sloan-Kettering Cancer Center

PLX4032: novel, small molecule inhibitor
Selectivity for BRAFV600E in vitro and in vivo
Phospho-ERK IC50 (nM)
A375
COLO829
COLO205
SW620
SKMEL2
20
10
30
>40,000
14,000
Selective in cellular assays
V600E
WT
Selective regression of V600E tumors
Selective for BRAFV600E kinase
among 70 kinases screened
1205Lu
V600E
+ PLX4032
C8161
WT
+ PLX4032
Tumor
Size
100 mm3
10–100
IC50 (nM)
100–1000
1000–10000
PLX4720 co-structure with kinase domain of
BRAFV600E (Tsai J et al. 2008 PNAS)
Kinase domain binding
2006 EORTC-NCI-AACR Molecular Targets & Cancer Therapeutics
BRAF

PLX4032: phase I study
Design:
Open-label, sequential dose escalation study
Intra-patient dose escalation permitted
Primary objectives:
• Evaluate safety and PK of PLX4032 in patients with solid tumors
• Measure activity, including response and symptom improvement
Secondary objectives:
• Measure PD activity of PLX4032 via inhibition of biomarkers
- pMEK, pERK & Ki67 in paired tumor biopsy samples
- 18FDG uptake
Eligibility standard for phase I trials; no requirement for BRAFV600E

3 patients
4 pts
4 pts
3 pts
4 pts4 pts
4 pts
100 200 400 800 1600
Daily Dose (mg) BID
160 240 360Daily Dose (mg)
BID
All Comers
n = 18
Max Dose: 1600 (Bid)
720
100
600
500
400
300
200
shrinkage
stasis
700
PK Bridging
Study
1200
1000
900
1400
1600
1800
2000
2200
2400
2600
2800
AUC ( μM
*hr)
900
1000
800
1100
1200
1300
1400
1500
1600
1700
1800
1900
1120
100
500
400
300
200
600
700 5 pts
7 pts
4 pts
2000
2100
2200
2300
2400
2500
2600
2700
2800
2900
3000
AUC ( μM
*hr)
900
1000
800
1100
1200
1300
1400
1500
1600
1700
1800
1900
500
600
700
2000
2100
2200
2300
2400
2500
2600
2700
2800
2900
3000
960
4 pts
PLX4032 optimized formulation achieves
preclinical target exposure for tumor regression
Initial Formulation Optimized Formulation
1000
2000
3000
AU
C 0
-24
hr
(uM
*hr)
Daily BID dose (mg)
100 200 400 800 1600
Daily BID dose (mg)
160 240 360 720 1120 960
100
400
720 BID
960 BID
1120 BID
Target for regression
1000
2000
3000
AU
C 0
-24 h
r (u
M*h
r)
Target for stasis
400
100

BRAFV600E melanoma patients treated with
PLX4032 > 240 mg BID
% change from baseline (sum of lesion size)
*
100
75
50
25
0
-25
-50
-75
-100
(RECIST cutoff for PR, 30%)
Patients (n=15)*
M1a/M1b patients
M1c patients
* One M1c patient had 55% reduction in target lesions, but PD in non-target lesions;
died before end C2 (not included above)

Conclusions
PLX4032 Phase I dose escalation study
• Twice daily administration tolerable up to 720 mg
• 960 mg BID dose under evaluation as MTD
• Pharmacokinetics show limited variability and exposure adequate to
inhibit target in animal models
• Responses observed in V600E+ melanoma patients > 240 mg BID:
• 9 PRs (7 confirmed 49% - 100%, 2 unconfirmed 31% - 62%)
• Regression of liver, lung and bone lesions
• Symptom improvement in many patients
• Interim PFS ~ 6 months, with many patients still on therapy
• In 3 V600E+ thyroid patients, 1 confirmed PR and 2 SD
A Phase II Study of Imatinib Mesylate
(IM) for Patients with Advanced
Melanoma Harboring Somatic
Alterations of KIT (Abst ID: 9001)
R. D. Carvajal, P. B. Chapman, J. D. Wolchok, L.
Cane, J. B. Teitcher, J. Lutzky, A. C. Pavlick, B. C.
Bastian, C. R. Antonescu, G. K. Schwartz
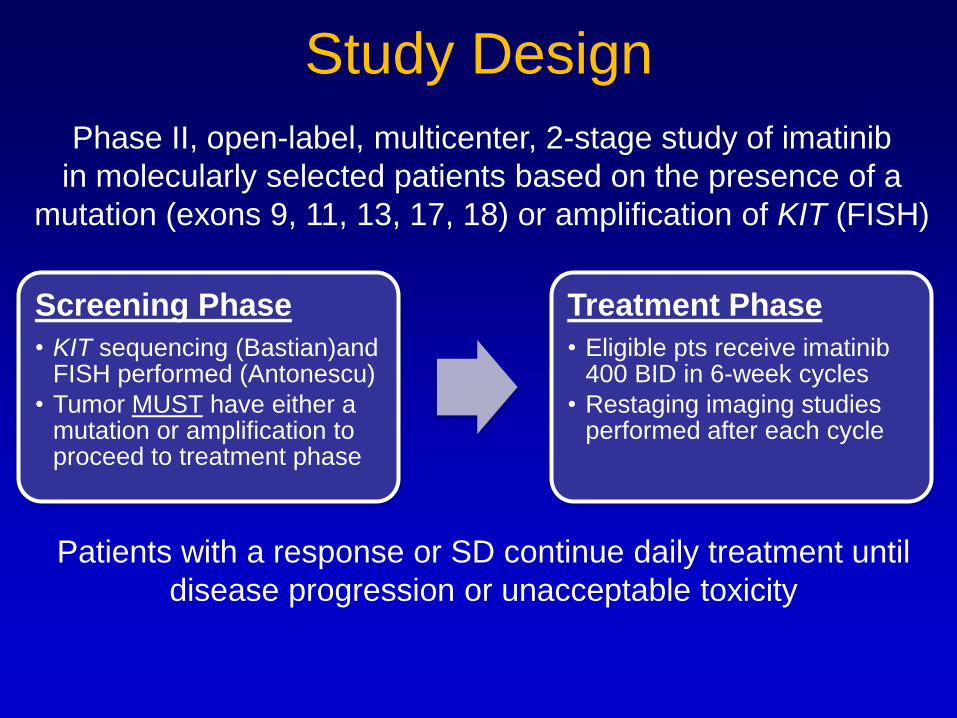
Study Design
Phase II, open-label, multicenter, 2-stage study of imatinib
in molecularly selected patients based on the presence of a
mutation (exons 9, 11, 13, 17, 18) or amplification of KIT (FISH)
Screening Phase
• KIT sequencing (Bastian)and FISH performed (Antonescu)
• Tumor MUST have either a mutation or amplification to proceed to treatment phase
Treatment Phase
• Eligible pts receive imatinib 400 BID in 6-week cycles
• Restaging imaging studies performed after each cycle
Patients with a response or SD continue daily treatment until
disease progression or unacceptable toxicity

Key Eligibility Criteria
• Inoperable melanoma arising from acral, mucosal, or chronically sun-damaged sites
• Tumor must harbor KIT amplification by FISH or a detectable mutation in KIT by sequencing
• No prior therapy with other KIT tyrosine kinase inhibitors
• Other standard eligibility criteria apply

Response Data (n = 12)
n %
Complete Response 2 17%
Partial Response 2 17%
Stable Disease 6 50%
Progression 2 17%
Overall RECIST RR 4/12 33%
(Updated 5/12/09)

# Melanoma
Subtype
KIT Mutation KIT Amp Best
Response
Cycles Wks
1 Mucosal Exon 11 L576P Yes CR 7 37+
2 Acral Exon 11 L576P Yes CR 4 18+
3 Mucosal Exon 11 L576P No PR 7 40+
4 Acral Exon 13 K642E No PR 3 13+
5 Mucosal Exon 13 K642E No SD 3 18
6 Mucosal Exon 11 L576P No SD 2 12
7 Mucosal None Yes SD 2 11
8 Mucosal None Yes SD 2 11
9 Acral Exon 13 K642E No SD 2 8+
10 Acral Exon 13 K643X Yes SD 2 6+
11 Mucosal Exon 13 V654A No POD 1 6
12 Mucosal Exon 9 N463S
Exon13 N655S
No POD 1 4
KIT Alteration and Response
(Updated 5/18/09)Red – on study; Blue – off study

Conclusions• There is 21% prevalence of a KIT mutation and/or
amplification in this selected cohort.
• We have observed 4 responses in 12 evaluable
patients thus far, allowing expansion to the second
stage of the study (ongoing).
• The 2 CRs were in tumors with both an exon 11
L576P mutation and amplification of KIT.
• It is feasible to identify appropriate patients
prospectively for treatment with imatinib.
• Only molecularly appropriate patients with melanoma
should be treated with imatinib.

Clinical relevance of miRNA expression in metastatic melanoma
Abstract #9006Eva Hernando, Ph.D.
Interdisciplinary Melanoma Program

microRNAs: small, non-coding RNAs
with a critical role in cancer
• miRNA genes are frequently located at fragile sites and chromosomal regions
frequently altered in human cancer (e.g. amplifications, deletions,
translocations)
• miRNA patterns are able to sub-classify tumor types (Calin and Croce,2006)
• miRNAs can act as tumor suppressors (e.g. let-7) or oncogenes (e.g. miR-17-92)
• Some miRNAs are known to contribute to metastasis (e.g. miR-10b, miR-335).
ADVANTAGES TO THEIR ANALYSIS
Tissue/cell-type specificity
Stable in formalin-fixed paraffin-embedded tissues.
Can be tested by standardized methods (qRT-PCR)
Represent closely the functional level of the gene.

The 18 miRNA signature clusters melanoma
patients
based on post-recurrence survival

A 6-miRNA subset separates melanoma patients based onpost-recurrence survival
p=0.001
Low Risk
High Risk
n=29
n=30
0 500 1000 1500 2000
Survival (days)
0.0
0.2
0.4
0.6
0.8
1.0
Surv
ival
Pro
bab
ility
miRNA predictor:
miR-150 miR-455-3p miR-145 miR-497 miR-155miR-342-3p

The 6 miRNA signature retains its predictive
value in an optimized multivariate model

Conclusions
A miRNA signature associates with post-recurrence
survival of a cohort of 61 melanoma patients
miRNAs add to the power of clinicopathological
parameters (Stage, site of metastasis) in predicting post-
recurrence survival.
miRNA profiles discriminate between Stages IIIB and IIIC.
A model that integrates a miRNA predictor and Stage
accurately predicts post-recurrence survival.
Certain miRNAs might hold prognostic information at the
time of diagnosis.

A Phase III Multi-institutional Randomized Study of
Immunization with gp100:209-217(210M) Peptide
Followed by High Dose IL-2 vs High Dose IL-2 Alone
in Patients With Metastatic Melanoma CRA #9011
Doug Schwartzentruber, MD, FACS
Medical Director, Goshen Center for Cancer Care
Clinical Associate Professor of Surgery Indiana
UniversityAuthors: D. Schwartzentruber, D. Lawson, J. Richards, R. Conry, D. Miller,
J. Treisman, F. Gailani, L. Riley, D. Vena, P. Hwu
Support: NCI, Chiron, Novartis, Goshen Health System, Goshen Hospital
and Health Care Foundation, Luke Brennen Research Fund

BackgroundTreatment of Patients with Metastatic Melanoma
• gp100 209-217 (210M) in Montanide ISA 51 + HD IL-2
(720K) every 3 weeks, RR 42% (13/31).1
• gp100 209-217 (210M) in Montanide ISA 51 every 3 weeks
+ HD IL-2 (600K) on a variable schedule.2
Trial 1 (IL-2 C1 and C2 only) RR 23.8% (n=42)
Trial 2 (IL-2 C3 and C4 only) RR 12.5% (n=40)
Trial 3 (IL-2 C1 through C4) RR 12.8% (n=39)
• Retrospective results Surgery Branch: HD IL-2 alone
(n=305) RR 12.8%; gp100 + HD IL-2 (n=49) RR 25.0%.3
1. Rosenberg S.A., et. al., Nature Medicine 4: 321-327, 1998.
2. Sosman J.A., et. al., J Clin Oncol 26: 2292-2298, 2008.
3. Smith F.O., et. Al., Clin Cancer Res 14:5610-5618, 2008.

Objectives of Study
• Primary
Compare RR of HD IL-2 with and without
gp100 vaccine.
• Secondary
Evaluate toxicity.
Compare disease and progression free survival.
Immunologic monitoring (PBL and serum)
QOL measurements (before and after 2 cycles of
treatment)

Study Design
• Prospective, randomized (1:1), multi-institutional.
• Stratified for cutaneous / SQ disease only vs. all other.
• Arm A: HD IL-2 (720K) IV q 8hrs, max 12 doses,
repeated every 3 weeks.
• Arm B: gp100 209-217 (210M) in Montanide ISA 51 SQ
and HD IL-2 as in Arm A, starting day after vaccine.
• Response assessment (WHO criteria) after 2 cycles of
treatment.
• Re-treatment with 2 cycles when disease stable.
• IL-2 obtained commercially.
• gp100 and Montanide provided by CTEP, NCI (IND
holder).

Central Response Assessment
ResponseIL-2
N (%)
IL-2 + gp100
N (%)
P Value
CR + PR 6 (6.5) 16 (18.6) 0.013
SD + PD 87 (93.5) 70 (81.4)
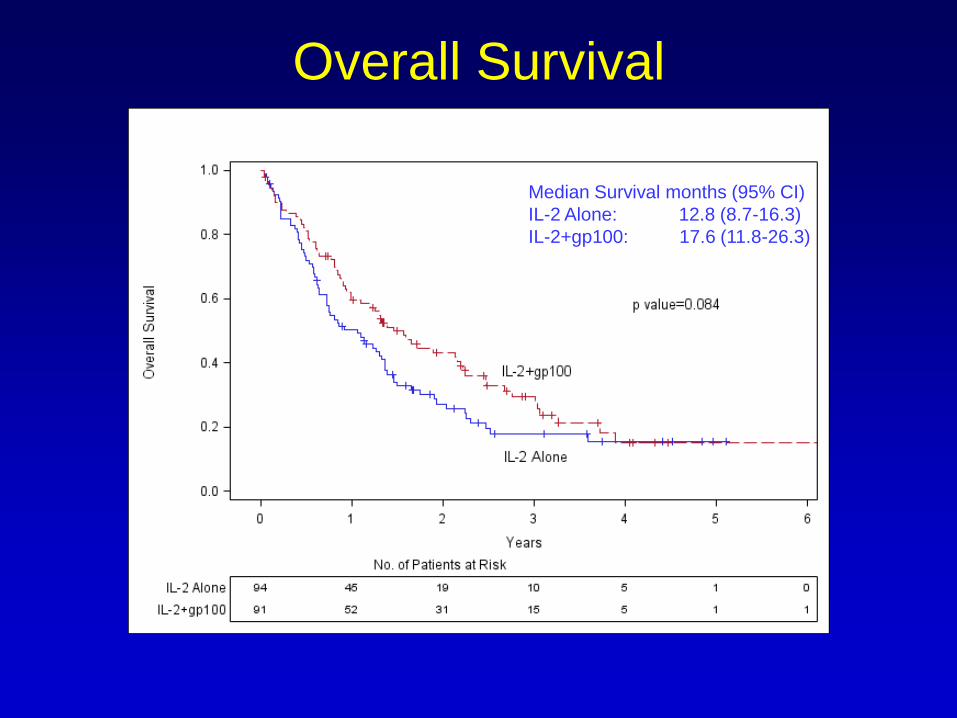
Overall Survival
Median Survival months (95% CI)
IL-2 Alone: 12.8 (8.7-16.3)
IL-2+gp100: 17.6 (11.8-26.3)
p value: 0.084
Median Survival months (95% CI)
IL-2 Alone: 12.8 (8.7-16.3)
IL-2+gp100: 17.6 (11.8-26.3)
p value: 0.084
Median Survival months (95% CI)
IL-2 Alone: 12.8 (8.7-16.3)
IL-2+gp100: 17.6 (11.8-26.3)

Summary and Conclusions
• Investigator assessed Response Rate in the vaccine arm is
significantly higher: 22.1% vs. 9.7% (p=0.022).
• Patients with lung metastases (M1b) accounted for the
majority of the response difference (p=0.002).
• Central review: Response Rate in the vaccine arm is
significantly higher: 18.6% vs. 6.5% (p=0.013).
• Progression Free Survival is significantly higher in the
vaccine arm: 2.9 vs. 1.6 months (p=0.01).
• Trend for greater Overall Survival in the vaccine arm: 17.6
vs. 12.8 months (p=0.084). Median follow up for surviving
patients is 28.7 months.

A Randomized, Double-blind, Phase 3 Trial of STA-
4783 (elesclomol) in Combination with Paclitaxel
versus Paclitaxel Alone for Treatment of Patients
with Stage IV Metastatic Melanoma (SYMMETRY)
Review of Preliminary Data abstract # LBA 9012
A. Hauschild, A.M. Eggermont, E. Jacobson, S. O’Day. University of Kiel, Kiel, Germany; Erasmus University Medical Center, Rotterdam, The Netherlands; Synta Pharmaceuticals,
Lexington, MA; The Angeles Clinic and Research Institute, Santa Monica, CA
On behalf of the SYMMETRY Trial Investigators
Elesclomol: Mechanism of Action
• Elesclomol is an investigational drug candidate that induces oxidative
stress (reactive oxygen species, ROS)1
• Oxidative stress induction represents a potential novel way of
selectively targeting and killing cancer cells
• Cancer cells produce higher levels of reactive oxygen species (ROS)
than normal cells, making them potentially more susceptible to further
oxidative stress and ROS mediated apoptosis2
• Elevation of ROS may facilitate the ability of taxanes to induce
apoptosis through the intrinsic mitochondrial pathway3
• Preclinical in vivo studies demonstrated synergistic efficacy of
paclitaxel and elesclomol in a variety of solid tumor models, including
melanoma1. Kirshner et al. (2008) Molecular Cancer Therapy 7:2319-2327
2. Kong et al. (2000) Medical Hypothesis 55:29-35; Pelicano et al. (2004)
Drug Resistance Updates 7:97-110
3. Ramanathan et al. (2005) Cancer Research 65:8455-8460

SYMMETRY Study design
• 160 centers in 15 countries
• Tumor Assessment: at baseline and every 8 weeks from time of
randomization (RECIST)
• No patient cross-over
Study
Population
• Stage IV
metastatic
melanoma
• Chemo-naïve
• LDH ≤ 2x ULN
• ECOG PS 0-2
• Absence of
CNS mets
paclitaxel 80mg/m2
+
elesclomol 213 mg/m2
(N=315)
Randomization
1:1
(N=630)
Stratification Factors
• LDH status
• M1 subclass
• Prior permitted
(non-chemo) therapy*paclitaxel 80mg/m2
(N=315)
Primary
endpoint:
Progression-
free survival
qw for 3 weeks; 1 week off
* Kinase inhibitor, immunotherapy, biologic therapy, vaccine, or investigational non-chemo
Study Steering Committee: Steven O’Day, Axel Hauschild, Alexander Eggermont

PFS Analysis Methodology
• The protocol assumption was that treatment with ELPAC
would extend PFS by two months (3 vs. 5)
– 2-sided alpha 0.05, power 90%
– required number of PFS events = 164
• There were a total of 219 PFS events at the time of the
February 23rd, 2009 DMC meeting which exceeded the
required number of events by 34%
• Follow-up for disease progression stopped at time of study
stop; patients were censored at last valid tumor
assessment prior to stopping the treatment phase of the
study on February 26th, 2009

Progression-Free Survival - ITT Population
ELPAC PAC
Events/Number at risk 170/309 192/312
Median (months)
95% CI
3.4
(2.6 - 3.6)
1.9
(1.9 - 2.9)
6 Month PFS Rate 23% 17%
HR (ELPAC vs. PAC)
95% CI
0.84
(0.68 – 1.04)
p-value (Stratified Log-
Rank)
0.1107
PAC 312 200 87 42 20 8 2 2 1 0 0
ELPAC 309 187 107 53 21 10 6 3 2 2 0
Subjects at Risk
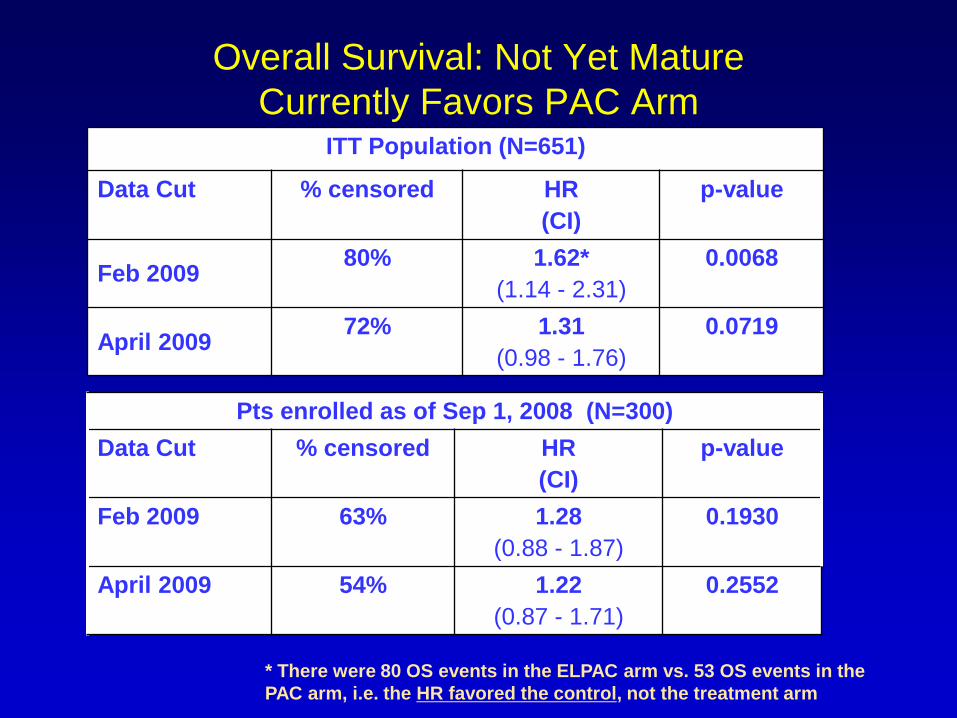
Overall Survival: Not Yet Mature
Currently Favors PAC ArmITT Population (N=651)
Data Cut % censored HR
(CI)
p-value
Feb 200980% 1.62*
(1.14 - 2.31)
0.0068
April 200972% 1.31
(0.98 - 1.76)
0.0719
* There were 80 OS events in the ELPAC arm vs. 53 OS events in the
PAC arm, i.e. the HR favored the control, not the treatment arm
Pts enrolled as of Sep 1, 2008 (N=300)
Data Cut % censored HR
(CI)
p-value
Feb 2009 63% 1.28
(0.88 - 1.87)
0.1930
April 2009 54% 1.22
(0.87 - 1.71)
0.2552
Conclusions
• Despite a trend in improvement of PFS, elesclomol in combination with
paclitaxel (ELPAC) failed to demonstrate a statistically significant
improvement when compared with paclitaxel alone in chemo-naive
patients with metastatic melanoma
• There was a statistically significant increase in PFS with ELPAC in the
subgroup of patients with normal LDH (68% of the ITT, pre-specified
exploratory analysis)
• An imbalance in deaths favoring the paclitaxel arm was observed,
leading to early study termination
• No organ-specific toxicities have been identified that explain the
observed imbalance in deaths at this time; safety data is continuing to
be evaluated
• At this point OS data is not mature; mature data will be presented at a
future scientific meeting

Phase II Study of Aflibercept (VEGF Trap) in
Recurrent Inoperable Stage III or Stage IV
Melanoma of Cutaneous or Ocular origin
abstract #9028
Ahmad A. Tarhini, Scott Christensen, Kim Margolin, Paul Frankel, Christopher Ruel, Stergios Moschos, Hussein Tawbi, Janice Shipe-
Spotloe, John M. Kirkwood
Support: NCI, Sanofi-aventis, Regeneron, UPCI CTRC
University of Pittsburgh, Pittsburgh, PA
City of Hope National Medical Center, Duarte CA
USC/Norris Comprehensive Cancer Center, Los Angeles
University of California, Davis Cancer Center, Sacramento

Introduction• Aflibercept (VEGF Trap) is a unique fusion protein combining
the Fc portion of human IgG1 with the principal extracellular
ligand-binding domains of human VEGFR1 & VEGFR2
• Acts as a high-affinity soluble decoy VEGF receptor and potent
angiogenesis inhibitor
• Aflibercept has highest binding affinity for VEGF described to date.
Dissociation constant 0.5 pM

Treatment Plan
• Schedule of administration
– Aflibercept 4 mg/kg I.V. every 2 wks for 8 wks
(4 cycles; 1 cycle=14 days)
– Response assessment every 8 wks
• Correlative Studies– Pharmacokinetics
– Anti-VEGF Trap Antibody

Efficacy Summary: Responses (N=41)**
No.
Pts
(%)
Primary
No. Pts (%)
Classification
No. Pts (%)
Cutaneous Ocular Unknown M1a,
N3
M1b M1c
RR* 1
(2)
1
(100)
1
(100)
SD 20 (49) 13
(65)
5
(25)
2
(10)
4
(20)
5
(25)
11
(55)
PD 13
(32)
9
(69)
3
(23)
1
(8)
1
(8)
2
(15)
10
(77)
Not
Eval
5
(12)
Too
Early
2
(5)


Conclusions• Aflibercept has promising clinical activity
in metastatic melanoma of cutaneous or ocular origin in 41 pts
• It is highly likely that we will meet the 4-months PFS milestone of at least 17 instances of 4-month PFS with longer follow up
• Serious adverse events noted with this class of drugs such as hypertension require close follow up and monitoring of patients

Ipilimumab Treatment May Be Associated With A
Long-term Survival Benefit: 18-month* Survival Rate Of
Patients With Advanced Melanoma Treated With
10 mg/kg Ipilimumab In Three Phase II Clinical Trials
*24-month survival data is also presented
Steven J. O’Day,1 Jeffrey Weber,2 Celeste Lebbé,3
Michele Maio,4 Hubert Pehamberger,5
Kaan Harmankaya,5 Jonathan Siegel,6 Axel Hoos,6
Rachel Humphrey,7 and Jedd Wolchok,8
ASCO 2009
Poster Discussion
Abstract 9033
1The Angeles Clinic and Research Institute, Santa Monica, CA USA; 2H. Lee Moffitt Cancer Center and Research Institute, Tampa,
FL USA; 3Saint-Louis Hospital Department of Dermatology, Center of Clinical Investigation, Paris, France; 4Division of Medical
Oncology and Immunotherapy Department of Oncology University Hospital of Siena, Istituto Toscano Tumori, Siena, Italy; 5Univ. of
Vienna, Department of General Clinical Dermatology, Vienna, Austria; 6Bristol-Myers Squibb Company, Wallingford, CT, USA; 7Bristol-Myers Squibb Company, Princeton, NJ, USA; 8Memorial Sloan-Kettering Cancer Center, New York, NY, USA
Email: [email protected]

Overall Survival Rates In
CA184-008, CA184-022, And CA184-007a
Study
12-month
survival rate
% (95% CI)
18-month
survival rate
% (95% CI)
24-month
survival rate
% (95% CI)
CA184-008 (N=155)
(previously treated)47.2 (39.5-55.1) 39.4 (31.7-47.2) 32.8 (25.4-40.5)
CA184-022 (N=217)b, c
10 mg/kg (n=72)
(previously treated)
48.6 (36.8-60.4) 34.5 (23.6-46.2) 29.8 (19.1-41.1)
CA184-007 (N=115)
Ipilimumab + placebo (n=57) 62.4 (49.4-75.1) 50.9 (37.5-64.1) 41.8 (28.3-55.5)
Treatment-naive (n=32) 71.4 (55.2-87.2) 61.0 (43.4-77.7) 56.6 (38.4-74.3)
Previously treated (n=25) 50.8 (31.5-71.1) 38.1 (20.0-57.6) 24.2 (8.0–42.8)
Ipilimumab + budesonide (n=58) 55.9 (42.7-68.8) 47.9 (34.7-61.2) 40.6 (27.1-54.4)
Treatment-naive (n=21) 65.9 (45.0-85.7) 65.9 (45.0-85.7) 56.5 (30.6-81.0)
Previously treated (n=37) 49.9 (33.3-66.6) 37.9 (22.2-54.3) 31.6 (16.5-47.6)
aStatistics are based on randomized patients in studies -007 and -022, and treated patients in study -008. For study -022, the statistics are for patients in
the 10 mg/kg arm only bIn study -022, there were 217 patients randomized and 214 treated patientscFor the 10 mg/kg arm of study -022, there were 72 patients randomized and 71 treated patients
CI = confidence interval

Median Survival Times In Studies CA184-
008, CA184-022, And CA184-007
Study
Median Survival Time
months (95% CI)
CA184-008 (N=155) 10.2 (7.6 - 16.3)
CA184-022 (N=217)a
10 mg/kg (n=72)b 11.4 (6.9 - 16.1)
CA184-007 (N=115)
Ipilimumab + placebo (n=57)
Ipilimumab + budesonide (n=58)
19.3 (12.0 - NR)
17.7 (6.8 - NR)
aIn study -022, there were 217 randomized and 214 treated patients bFor the 10 mg/kg arm of study -022, there were 72 patients randomized and 71 treated patients;
CI = confidence interval; NR = not reached
Conclusions
• With a median follow-up of 10.1 to 16.3 months, and with a
range reaching up to 37.5 months, patients receiving
ipilimumab 10 mg/kg showed durable survival
• Across 3 studies, 12-month OS was >47%, 18-month OS
was >34%, 24-month OS was ≥30% and median survival
was >10 months
• Long-term survivors include patients with PD according to mWHO
criteria
– Reassessment and confirmation of PD is recommended to
prevent premature discontinuation of ipilimumab treatment
• Updated phase II trial survival results with ipilimumab 10 mg/kg in
advanced melanoma encourage continued investigation of this
therapy, and patients continue to be followed to evaluate long-term
survival
Ipilimumab Exerts Disease Control And Survival
Benefits In Advanced Melanoma Patients With
And Without Immune-related Adverse Events
(irAEs)
Jose Lutzky,1 Jedd Wolchok,2 Omid Hamid,3
Celeste Lebbé,4 Hubert Pehamberger,5 Gerald Linette,6
Veerle De Pril,7 Ramy Ibrahim,8 Axel Hoos,8
and Steven O’Day3
E-mail: [email protected]
1Mt. Sinai Comprehensive Cancer Center, Miami Beach, FL, US; 2Memorial Sloan-Kettering
Cancer Center, New York, NY, US; 3The Angeles Clinic and Research Institute, Los Angeles, CA,
US; 4Saint-Louis Hospital, Paris, France; 5Department of Dermatology, University of Vienna,
Vienna, Austria; 6Washington University School of Medicine, St. Louis, MO, US; 7Bristol-Myers
Squibb, Braine-l’Alleud, Belgium; 8Bristol-Myers Squibb, Wallingford, CT, US
Abstract 9034

Disease control by irAE grade
(ipilimumab 10 mg/kg monotherapy)
Study
Disease control rate (PR+CR+SD)
P-value
irAE Grade
0/1
irAE Grade
≥ 2
DC
No
DC DC
No
DC
CA184-007 4 16 16 21 ≤ 0.09
CA184-008 21 73 21 40 ≤ 0.14
CA184-022 10 31 11 19 ≤ 0.3
DC = Disease Control by mWHO criteria
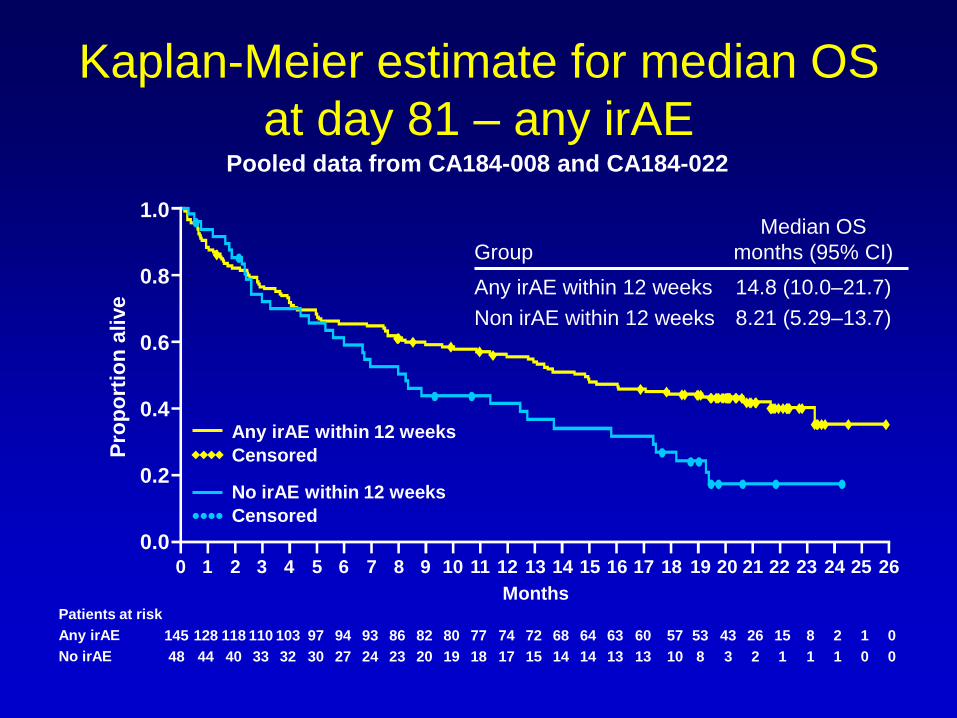
Kaplan-Meier estimate for median OS
at day 81 – any irAEPooled data from CA184-008 and CA184-022
1.0
0.8
0.6
0.4
0.2
0.0
Pro
po
rtio
n a
live
Any irAE within 12 weeks
Censored
No irAE within 12 weeks
Censored
Months
Group
Median OS
months (95% CI)
Any irAE within 12 weeks
Non irAE within 12 weeks
14.8 (10.0–21.7)
8.21 (5.29–13.7)
Patients at risk
Any irAE
No irAE
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
145 128 118 110 103 97 94 93 86 82 80 77 74 72 68 64 63 60
48 44 40 33 32 30 27 24 23 20 19 18 17 15 14 14 13 13
57 53 43 26 15 8 2 1 0
10 8 3 2 1 1 1 0 0

Conclusions
• Ipilimumab 10 mg/kg induced disease control in
patients with advanced melanoma
• Disease control and survival benefits are
observed among patients regardless of whether
they do or do not develop grade ≥2 irAEs
• Patients that do not experience an irAE by the
end of the induction dosing period (week 12)
may still demonstrate clinical benefit with
ipilimumab
A phase II trial of carboplatin and nab-paclitaxel
(ABI-007) in patients with unresectable stage IV
melanoma, final data from N057E1 abstract # 9055
L. A. Kottschade RN, MSN, CNP2; V.J.Suman, PhD2; T. Amatruda, MD3;; R.R. McWilliams,
MD2; S.R. Dakhil, MD4; D.A. Nikcevich, MD5; R.P. Morton, MD6; T.R. Fitch, MD7; A.J.
Jaslowski, MD8 ; N. Desai, PhD9; V. Trieu, PhD9; D. Knauer, PhD9; S.N Markovic,
MD, PhD2
This study was conducted as a collaborative trial of the North Central Cancer Treatment
Group and Mayo Clinic and was supported in part by Public Health Service Grants
CA-25224, CA-37404, CA-35113.
Mayo Clinic, Rochester, MN
Metro MN Community Clinical Oncology Program, St. Louis Park, MN
Wichita Community Clinical Oncology Program, Wichita, KS
Duluth Community Clinical Oncology Program, Duluth, MN
Iowa Oncology Research Association CCOP, DesMoines, IA
Mayo Clinic Scottsdale, Scottsdale, AZ
St. Vincent Regional Cancer Center CCOP, Green Bay, WI
Abraxis Bioscience LLC, Los Angeles, CA

Methods• Nab-P (100 mg/m2) and Carboplatin (AUC2) were administered on
days 1, 8, and 15 of a 28 day cycle.
• A parallel phase II trial was conducted in pts who were
chemotherapy naïve (CN) or were previously treated (PT), with
unresectable stage IV melanoma.
• Testing:
– CN patients
• CR+PR rate by RECIST of ≤15% vs ≥35% with this combination
• If ≥ 9 responses (CR+PR) were seen among the first 35 evaluable patients
enrolled to this arm we would consider this regimen for further testing in this
patient population.
– PT patients
• CR+PR rate by RECIST of ≤5% vs 20% with this combination
• If ≥ 4 responses (CR+PR) were seen among the first 35 evaluable patients
enrolled to this arm we would consider this regimen for further testing in this
patient population.

Results from the CN group
• Patients were followed for a minimum of 1.7 years or until death.
• Among the first 35 patients enrolled, there were 9 (25.7%; 90%CI:
14.1-40.6%) patients who had a confirmed response (1-CR and 8
PRs).
• Among all 39 patients enrolled, there were 10 (25.6%; 90%CI: 14.6-
39.6%) patients who had a confirmed response (1-CR and 9 PRs).
• The median progression free survival time was 4.3 months and the
median overall survival was 11.1 months.
• At last contact:
– 5 patients are alive without progression of disease
– 3 patients are alive with disease progression
– 31 patients have dies from their disease

Results from the PT group
• All but one patient was followed for a minimum of 9 months or until
death.
• Among the 34 patients enrolled, there were 3 (8.8%; 90% CI: 2.5%-
21.3%) patients who had a confirmed partial response and 11
patients remained on treatment with stable disease for at least 4
cycles.
• There were no complete responses.
• The median progression-free survival time was 4.2 months.
• The median overall survival time was 10.9 months.
• At last contact:
– 1 patient is alive without progression of their disease
– 7 patients are alive with disease progression
– 26 patients have died from their disease
Discussion
• The weekly combination of nab-P and C appears to be
well tolerated and with promising clinical activity as first-
line therapy for MM.
• For patients who are previously treated the weekly
combination of nab-P and C appears to be a viable
option for salvage therapy.
• The impact of adding targeted agents (i.e bevacizumab)
to this regimen is currently being explored by our group
in a Phase II study.

nab-Paclitaxel and Bevacizumab as
First-Line Therapy in Patients with
Unresectable Stage III and IV
Melanoma
abstract # 9061
P.Boasberg1, S Cruickshank2, O.Hamid1, S.O’Day1,
R.Weber3, L. Spitler3
The Angeles Clinic and Research Institute, Los Angeles,
CA1; Scott Cruickshank and Associates, Santa Barbara, CA2;
The Northern California Melanoma Center, St. Mary’s
Medical Center, San Francisco, CA3

Background: nab-Paclitaxel and
Bevacizumab for melanoma
• nab-paclitaxel (albumin bound paclitaxel particles) delivers increased intra-tumoral concentrations of paclitaxel and has superior efficacy in the treatment of metastatic breast cancer (J Clin Oncol 2005;23:7794-7803)
• nab-paclitaxel has demonstrated single agent activity in metastatic melanoma (ASCO 2005;#7558)
• VEGF Increases vascular permeability and inhibits antigen-presenting dendritic cell function
• VEGF is over expressed by melanoma cells, and is targeted by Bevacizumab
• Bevacizumab enhances tumor responses to paclitaxel (NEJM 2007:357:2666-2676)

nab-Paclitaxel and Bevacizumab for
melanoma
Regimen
• nab-paclitaxel 150mg/m2 – Days 1, 8, 15 Bevacizumab 10mg/kg – Days 1 & 15 of a 28-day cycle
• Treated to progression, dose limiting toxicity, or 2 years
Endpoints
• Primary– Progression free survival (PFS) at 4 months
• Secondary– Progression-free survival (PFS)
– Overall Survival (OS)
– Objective Response Rate (RR)

Results
• 4-month progression-free survival 74%
• Median progression-free survival 5.8 months
• Median duration of follow-up 7.83 months
• Survival Status
Dead 9 (20.9%)
Alive 34 (79.1%)
• 6-month survival rate 91%
• 12-month survival rate 68%
• Median duration of survival Not reached yet
Complete response 1 (2.7%)
Partial response 10 (27.0%)
Stable disease (4wks) 18 (48.6%)
Progressive disease 8 (21.6%)

Conclusions
• Preliminary results suggest that:
– Combined therapy with nab-paclitaxel and bevacizumab has promise in terms of progression-free survival and overall survival benefit compared to a meta-analysis of previous Phase II studies (J Clin Oncol 2008; 26:527-534)
– The combination is safe to administer
– The number of patients and short follow-up prevent definitive conclusions to be reached concerning safety and efficacy of the combination
– The study is ongoing with continued patient treatment and follow-up.

My overall conclusions
• These data mark a new era of targeted therapy for melanoma with impressive PLX-4032 and imatinib data
• The gp100 peptide/IL-2 data are intriguing but would require a confirmatory trial unlikely to occur; it might encourage other IL-2 vaccine trials and combinations
• Overall ipilimumab survival data are very promising, bode well for its future development
• Nab-Bev and Nab-carbo are promising regimens that look at least as good as DTIC