on the major trend towards personalised medicine – and other visions: the public health genomics...
TRANSCRIPT

On the major trend towards personalised medicine – and other visions: the Public Health Genomics (PHG) perspective
Prof. Dr. Angela Brand MD PhD MPH, Director of the European Centre for Public Health Genomics (ECPHG), Coordinator of PHGEN (DG Sanco)Institute for Public Health Genomics@Maastricht University, The Netherlands
9th Swiss Congress on Health Economics and Health Sciences (Bern 26.10.2012)

“Public Health Genomics (PHG) is the responsible and effective translation of genome-based knowledge and technologies into public policy and health services for the benefit of population health.”
[Bellagio Statement 2005: GRAPHInt, PHGEN, IPHG]
Public Health Genomics (PHG): translational research„from cell to society“

1. What do we need to translate?
2. How do we translate (innovations into healthcare systems)?

1. What do we need to translate?

… genomics is a „moving target“ …

… from the
Human Genome Project
to the
Personal Genome Project …
… from
single and linear systems
to
non-linear networks in systems biology and systems medicine …

Not only 4 P‘s …

… not only beyond the 4 P’s, but also (A. Brand, 2008) …
1. from common complex diseases to “multiple rare diseases”
2. from diseases to “diseasomes”
3. from risk factor to “risk pattern”
4. from clinical utility to “personal utility”



… obesity story (21.08.2012)

….. and also
(1) highly (in space & time) dynamic personal (health) information
(2) from statistical risks within groups to “individualized evidence”
(3) “virtual individual models”
ITFoM (www.itfom.eu) – ”ICT for health & health for ICT”:a radically new vision for healthcare!

The Idea –Oganism = Computer
Life is the translation of the information in the genome into the
phenotype of the organism:
The organism ‚computes‘ this phenotype from its genotype, given a
specific environment (PentiumV) (neuronal net visualisation)
Genome
Phenotype


“From Stratified Medicine to truly Individualized Medicine“
• No existing groups, only individuals Every test will be part of treatment. No result can be transferred to
another patient. Every therapy is unique, not reproducible.
• No existing method on how to evaluate the new kind of technology How can we fulfill the hierarchy of evidence, the golden standard to
prove the efficacy of a treatment?• The patient is not only consumer of the technology, but also part of it
There is no boundary between patient and treatment. The patient is a unique part of the technology itself.

“The contemporary clinical trials development process is like a duck-billed platypus, an organism that no rational person would have designed a priori.”
[[David Steensma, DFCI, JCO, 2009]

2. How do we translate innovations into healthcare systems?

Translation in daily life
• Direct / timely implementation in healthcare quite low (Literature, Patents, Market data)
• Identify 3 phases:
• Lab Industrial application
• Industrial application Market
•Market Healthcare integration
• Focus generally on first two phases
19

Technology Transfer (TT)
• Addresses 1st two phases• Activity of the migration of
academic discoveries to useful application in the development of marketable products or processes
• TTO or valorization office• Most widely used activity in
business development or academic research
• Process, technique, method, tool, activity

Public Health Trias (3rd phase)
[IOM, 1988]

innovation & awareness & society

Public Health Assessment Tools (PHAT)
• HNA: systematic method of reviewing the health issues facing a population, leading to agreed priorities and resource allocation that will improve health and reduce inequalities
• HTA: multidisciplinary process that summarizes information about the medical, social, economic, legal and ethical issues related to the use of a health technology in a systematic, transparent, unbiased, robust manner.
• HIA: combination of procedures, methods and tools by which a policy, program, or project may be judged as to its potential effects on the health of a population, and the distribution of those effects within the population
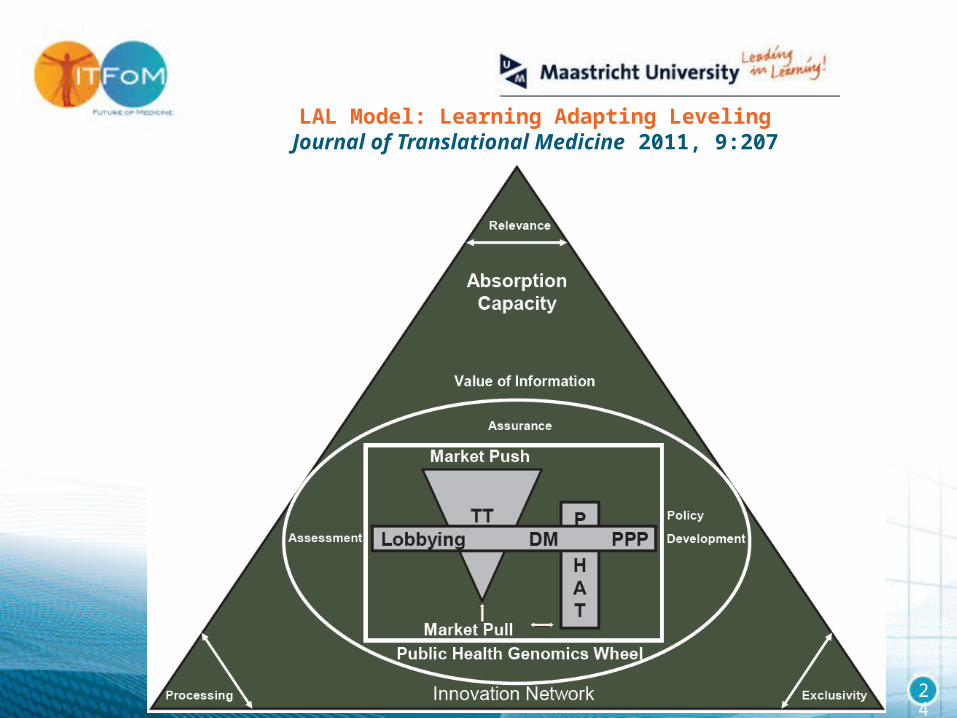
LAL Model: Learning Adapting LevelingJournal of Translational Medicine 2011, 9:207
24

“… we face a time when the taxonomy of human disease is being redefined given the existence of pathological and molecular disease subtypes…”
[Nuria Malats, CNIO 2009]
… we face a time when boundaries of disciplines are crossed and the understanding of diseases is changed as it happened before with the jump from the macroscopic view in anatomy to the microscopic view in cell structure …
Let’s get prepared in time – the future is built today!

Public Health Genomics European Network (PHGEN)

PHGEN II
"European Best Practice Guidelines for Quality Assurance, Provision and Use of Genome-based Information and Technologies”
Declaration of Rome - 19.04.2012
www.phgen.eu

PHGEN II
We have to define todaywhat kind of (policy) „guidelines“ we need for tomorrow!
… taking into account e.g.
• dynamics of the field: genomics is a „ moving target“ (from HG to PG) • genome-environment interactions changing permanantly over time and space
(incl. epigenomics: „from cell to society to cell“)• health information instead of biomarkers
• systems network thinking of biomedicine and environment (incl. social environment): e.g. „diseasomes“ and „social networks“
• P4 medicine (predictive, preemtive, personalised, participatory): „a change of view that changes everything“ • the changing roles of patients and doctors

… paradigm shift in Public Health towards Personalised Healthcare!
health promotion and prevention in public health
“one size fits all”
or
risk groups
communities
settings
prevention in public health genomics
individuals
family history
lifestyle
genomic profiling
risks for “diseasomes”
risk groups
with similar risk patterns

1. Research
• Keep up with new insights from basic sciences. • Generate evidence to demonstrate when the use of genome-based information and technologies (GBIT) in public health can improve health
outcomes in a safe, effective and cost-effective manner.
2. Monitor Health
• Develop surveillance systems of personal health data: accurate and ongoing assessment of highly dynamic health information changing over space and time on the individual level with a life-course perspective is needed.
• Promote personal files that contain comprehensive personal health information including ‘omics data and its interaction with all other health determinants.
3. Diagnose and Investigate
• Move from symptom- and phenotype-based approach to pathway-based cloud diagnostics for early identification of health problems on individual level.
• Move from “clinical utility” to “personal utility”.
4. Inform, Educate, Empower
• Promote health literacy of all stakeholders: enable citizens (including health professionals), individually and cooperatively, to access, understand, appraise, and apply information that will facilitate the application of GBIT for the benefit of individual citizens and their communities.
• Promote person-centred healthcare.
5. Mobilize Community Partnerships
• Promote Public Private Partnerships (PPP): Mechanisms, tools and models are required to link the needs of healthcare systems to those of the private sector and to foster the development of individualized technologies (e.g., Learning Adapting Levelling model).
6. Develop Policies
• Treat GBIT as the most holistic approach of health information when developing health policies.
7. Enforce Laws
• Use the dynamics of GBIT as a unique opportunity to frame and enforce laws and regulations pro-actively.
8. Link to / Provide Care
• Develop systems that sustain the interoperability between personal health management and public health management.
9. Assure Competent Workforce
• Integrate GBI and GBT into the professional training and life-long learning (LLL) curricula of health professionals.
10. Evaluate
• Establish and support a holistic and systems based evaluation of the impact of GBIT, taking into account economic issues and the different European health systems.
• Promote a system where technology transfer (TT) activities and policy-based Public Health Assessment tools (HNA, HTA, HIA) run in parallel for the timely, effective and efficient evaluation of GBIT.

Thanks for your attention!
“Future perspectivePersonal health drives a fundamental changenot just in what is known, but also in how wethink of ourselves and the way we are living,
thus redefining our society. The political will isthere, but we have to prepare for all the various
organizational changes…. in time.”
Personalized MedicineMarch 2012, Vol. 9, No. 2, Pages 115-119 , DOI 10.2217/pme.12.16
(doi:10.2217/pme.12.16)Public health perspective: from personalized medicine to personal health
Tomris Cesuroglu, Ben van Ommen, Núria Malats, Ralf Sudbrak, Hans Lehrach & Angela Brand