of the billing process for pediatric cardiology analysis ...ioe481/ioe481_past_reports/f9604.pdf ·...
TRANSCRIPT
Analysis and Recommendationsof the Billing Process for
Pediatric CardiologyFinal Report
December 16, 1996Industrial and Operations Engineering, Hospital Practicum
University of Michigan, Ann Arbor
by:Melissa Petrucci
Gary SchwartzbardC. Elena Szymanski

cm
*

Table of Contents
Executive Summary - Page 2
Introduction Page 3
Background Page 3
Purpose Page 3
Method Page 3
Current System Page 5
Alternatives Page 5
Findings Page 6
Conclusions Page 8
Recommendations Page 9
Action Plan Page 11
Appendix Page 13
1

Executive Summary
This report will focus on the billing process for Pediatric Cardiology at the University of Michigan MedicalCenter. The motivation of the project is to achieve 100% billing of non-invasive procedures, minor procedures, andcatheterization laboratoxy hospital charges. With this goal in mind, we will look to improve the accuracy of thecharge ticket information and increase the efficiency of the billing process. Obtaining 100% billing is not onlyimportant because of the loss of charges but also from a budget standpoint. The division’s hospital budget is basedon the number of procedures that are billed. Therefore missed billing also reduces the division’s hospital budget.This report will illustrate the current system and define the problems through the analysis of data for the month ofJuly.
In the current system, for each patient that enters the clinic the clerk creates a charge ticket. On this ticketan office visit charge as well as any necessary procedural activities should be identified by placing a check in theappropriate box. All of charge tickets are located at the nurses station. At the end of each day the charge tickets arecollected and entered into the University’s billing system the following morning.
The first step in our approach to improving the billing process was to identify how many procedures werenot being billed. More specifically we wanted to find out which laboratories were affected and the financial impactof the missed procedures. The time period from 1, 1996 through July 30, 1996 was audited.
The first aspect of billing that was looked at was the general office visit. However, the Medical ServicePlan (MSP) component will not be addressed either in the process nor in the lost charges because the necessarypatient specific data was not available. The MSP portion of the billing should be reviewed in the future.
Next, the laboratory procedures were analyzed for lost billing. The echocardiogram report and the logbooks were then compared against the Falcon billing sheets for each patient. The days surrounding the date ofservice were also checked to ensure the patient’s billing had actually been missed and not posted on a later date.Patients that had procedures that were not billed were identified.
This analysis revealed that the division does not bill for all procedures performed but the reason why stillremained in question. The problem had to be further identified. For each patient that had not been billed, theircharge ticket for the date of service in question was reviewed. Three possible situations were found. First there wasno check mark in the box. This clearly shows the patient was not billed because the person who performed theprocedure did not mark it. Secondly, there were many cases in which the procedure had been checked but had notbeen billed. This was attributed to a data inputting error. Lastly, the charge ticket was missing. The cause of this isalmost impossible to identify. Since for the echocardiogram laboratory a list of reports that were generated was usedin place of the log books, an additional check was performed to ensure the validity of the data.
Using the data we analyzed for the targeted procedures we have found that Pediatric Cardiology is onlybilling 89% of their procedures. The total amount of monetary facility charges that has been found to have been lostbased on the audit of July’s activity comes to a total of $28,085. Assuming that July is fairly representative of anaverage amount of activity the total charges lost over the span of a year would equal $337,020. The actual loss tothe clinic is more than shown due to the fact that the expense budget provided to the division from the University ofMichigan Hospital is based on the activity that is billed.
After close scrutiny and meticulous collection of all of the data it has been determined that an electronicbilling system directly tied to the billing system of the University of Michigan should be implemented. This type ofsystem is currently used for 80% of the billing at the Hospital. There are some problems that are inherent to anelectronic system. These problems are not a common occurrence and can be remedied if the proper backups areinstituted.
The log books should be electronic and be the point of entry for a charge to be electronically sent to theUniversity’s billing system. This is the only possibility that would eliminated the three sources of missed billing. Itwould also reduce the workload as well as offer additional capacities.
The action plan for the system would begin with the benchmarking of a current system. From here all of thenecessary fields and functionality needed for the Pediatric Clinic would have to be identified. The interaction withother software both within the clinic and with the Hospital will also need to be recognized. Once this preliminarydesign has been completed the system must then be designed, tested, implemented, and maintained. All users shouldalso be trained.
2

Introduction
This report will focus on the billing process for Pediatric Cardiology at the University of Michigan Medical Center.It will illustrate the current system and define the problems through the analysis of data for the month of July. Themethod for this study and the conclusions reached will also be included. Finally, in consideration of all the data, arecommendation will be made and an implenientatIon plan will be provided.
Background
Over the past few years, Pediatric Cardiology has been attempting to identify an efficient billing process. Thecurrent system uses a charge ticket that has information about a patient as well as the procedures that wereperformed. When a patient has a procedure performed the appropriate box is to be checked off.
The billing process is composed of two components. The University of Michigan Hospital side (facility) and theMedical Service Plan (MSP) side. At the request of our client, an audit of missed billing for the office visits will bedone. However, the MSP component will not be addressed either in the process nor in the lost charges because thenecessary patient specific confirmatory data was not available from the MSP billing office. The scope of the projectwas limited to the Hospital billing aspect and the true loss may actually be more because of the omission of the MSPcomponent.
Achieving 100% billing is not only important because of the loss of charges but also because of budgetconsiderations. The division’s hospital budget is based on the number of procedures that are billed. Thereforemissed billing also reduces the division’s hospital budget.
Purpose
The motivation of the project is to achieve 100% billing of non-invasive procedures, minor procedures, andcatheterization laboratory hospital charges. With this goal in mind, we will look to improve the accuracy of thecharge ticket information and increase the efficiency of the billing process. The systems involved are the billingprocess and possibly the procedure log books. Along with the modification of these processes, the responsibilitiesof the employees may shift under a new system. Our final outcome will be a recommendation for a more efficientbilling process for Pediatric Cardiology. The major implication of this process will be the elimination of lostcharges. Additionally, the hospital budget will be reflective of the true workload of the unit.
Method
The first step in our approach to improving the billing process was to identify how many procedures were not beingbilled. More specifically we wanted to find out which laboratories were affected and the financial impact of themissed procedures. Our client suggested that we audit the month of July and provided us with the necessaryinformation for July 1, 1996 through July 30, 1996. The hospital billing data for July 31, 1996 was not available.Although July is a change over month it should not have influenced our data since the technicians, faculty, and dataentry positions did not change.
The first aspect of billing we looked at was the general office visit. Each patient that came into the clinic shouldhave an office visit charge. Since the specific patient billing data needed from the billing office was not available,
( the patient’s charge ticket was used. The clinic scheduling sheets for July were also used because they containedevery patient that arrived for an appointment. The patients that were marked as cancelled or as “no-shows” weredisregarded. For each patient that arrived their charge ticket was reviewed to see if a consultation or return visit box
3

was checked for the given date of service. All office visits that were not billed were identified to be either asmissing the entire charge ticket or missing the check on the charge ticket in the related box. For each missing ticketor missing charge on the ticket the name of the patient, the resource, the date, the time, and the day of the week werenoted. Our client will follow up with the billing office to verify these charges are not in the MSP system.
Next, the laboratory procedures were analyze.d for lost billing. The most accurate account of the activity in theselaboratories was identified to be the log books, with the exception of the echocardiogram lab. With the help of Dr.Vermillion, it was decided that the most complete data was that of the reports generated for the echocardiogramprocedure. The log books from the other labs and list of patients from the echocardiogram lab that had a reportgenerated for the month of July were used. A copy of the Falcon billing compiled by the University of Michigan’sbilling system was also used. It contained names and procedure descriptions for every patient that had a laboratoryprocedure billed during the month of July. The echocardiogram report and the log books were then comparedagainst the Falcon billing sheets for each patient. The days surrounding the date of service were also checked toensure the patient’s billing had actually been missed and not posted later due to a technician delay, a data entry erroror an inefficiency in the University’s billing system. Patients that had procedures that were not billed wereidentified. Since our data only went until July 31, 1996, our client is currently checking to see if any of the patientsthat are identified as having procedures that were not billed may have been billed at a later date.
This analysis revealed that the division does not bill for all procedures performed but the reason why still remainedin question. The problem had to be further identified. For each patient that had not been billed, their charge ticketfor the date of service in question was reviewed. Three possible situations were found. First there was no checkmark in the box. This clearly shows the patient was not billed because the person who performed the procedure didnot mark it. Very infrequently there was a check mark that was hard to identify. It was either very faint or it wasnot in the box and was difficult to tell which procedure was checked. This error was also attributed to the personperforming the procedure. Secondly, there were many cases in which the procedure had been checked but had notbeen billed. This was attributed to a data inputting error. Lastly, the charge ticket was missing. It is almostimpossible to identify the cause of this.
Since for the echocardiogram laboratory a list of reports that were generated was used in place of the log books, anadditional check to ensure the validity of the data was necessary. Dr. Vermilion looked over the list of missedbilling and compared it to the log books to make sure that the procedures were supposed to be billed. An additionalfactor that was checked was that each patient identified had a valid name and a valid report.
There is a safeguard in place in the current system in which the person is to indicate in the log book that a procedurewas checked on the charge ticket. To evaluate the effectiveness of this, for those patients that were not billed for theprocedure and the corresponding box was not checked on the charge ticket, the log book was again looked at. Thosethat were marked as having been checked on the charge ticket but in reality had not been checked were identified.In the case of the echocardiogram laboratory, the actual log books were looked at to see if the technician had placedan “M” or an initial in it, indicating that it had been billed.
Using the gathered information we were able to identify the procedures that needed to be targeted. Severalprocedures were eliminated from our project. The catherterization laboratory and minor procedures were not lookedat further because all of their procedures were checked and they appeared on Falcon. The ProTime procedure wasalso ignored because the procedure did not generate a facility charge. The ECG-UH procedure was also notaddressed because it did not appear on the Falcon billing sheets. Lastly the Holter analysis procedure was notincluded because of the variable and possibly extensive time period from the beginning of a test to the end of it.Although these procedures are not specifically addressed in this report the recommendations provided are for theentire clinic and would apply to these procedures as well.
Interviews with the employees of Pediatric Cardiology were also conducted. The interviews were done withdifferent positions throughout the division so as to receive information from different perspectives and because the
4

new system will most likely affect staff in many areas. Members of the faculty, such as Dr. Rosenthal and Dr.Vermillion, provided much guidance as to how the division’s billing process works now and how it should ideallywork. We also met with Mike Pearistein, a senior laboratory technician. He helped to document the technician’srole in the current billing process. We frequently met with Dorothy Nalepa, our client. She helped us to attain andcompile the information as well as provided us with direction.
The results of the data from the remaining laboratories was then tallied and entered into a spreadsheet using Exceland charts were made to graphically represent the findings.
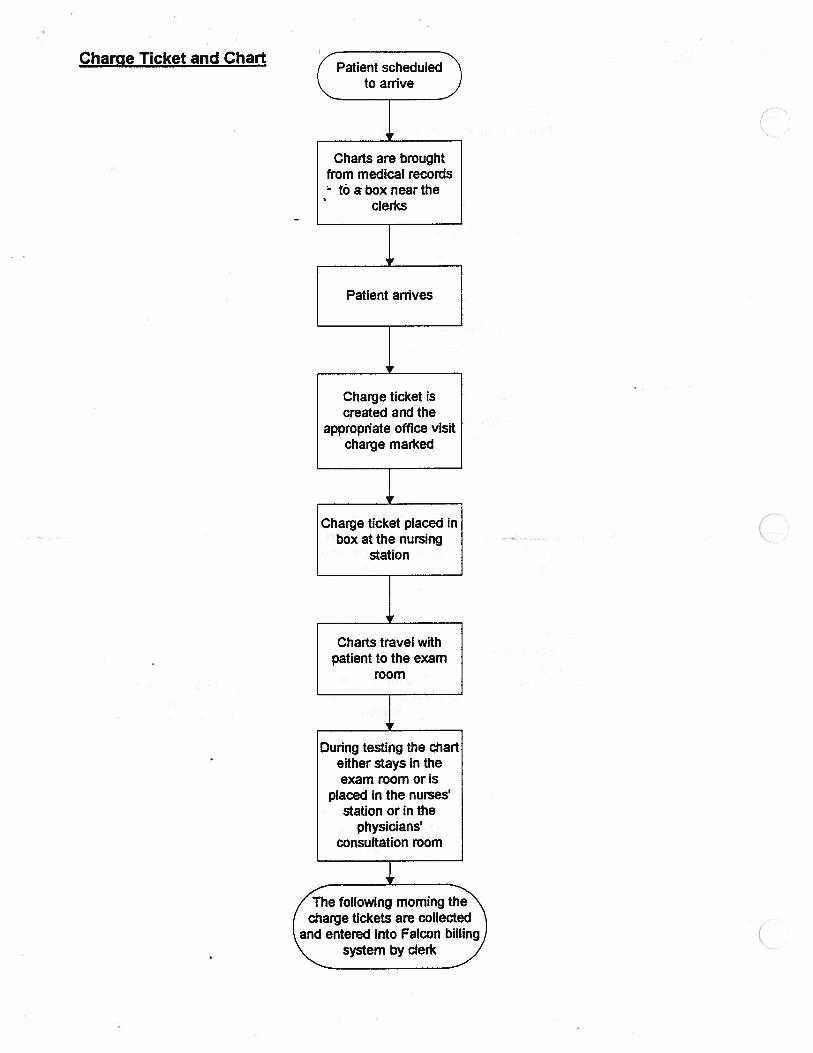
The information regarding the process flow that was collected through interviews was then documented. The flowof the charge ticket for each of the procedures was flow charted using Visio software. The flow charts may be foundin Appendix C.
A rough layout of the clinic was drawn in Visio. This was done so that the interaction between the charge ticketlocated at the nurse’s station and the various laboratories could be shown. This drawing may be found in AppendixD.
Current System
For each patient that enters the clinic the clerk creates a charge ticket. On this ticket an office visit charge as well asany necessary procedural activities should be identified by placing a check in the appropriate box. The person thatperforms a procedure is responsible for marking the charge ticket accordingly. All of charge tickets are located atthe nurses station. After the charge ticket is marked for the procedure performed the log books should be markedwith an M or an initial to indicate that the procedure was billed. For the echocardiogram lab throughout the day, astim& permits, the log books are compared to the charge tickets and the log books are marked indicating that theprocedures were billed. The flow of the billing process and the interaction with the charge ticket that is presently inplace has been documented for each of the targeted laboratories. The charts are included in Appendix A.
The most accurate account of the patients activity are the log books. Each procedure and in some cases, i.e. theechocardiogram lab, each machine has it’s own paper log book that is located in the appropriate room. Thetechnicians manually log in each patient.
At the end of each day the charge tickets are collected and entered into the University’s billing system the followingmorning. The day after they have been entered the division will receive two reports. One of which is an error reportspecifying any inconsistencies that were detected. These errors are then at this point to be corrected. The secondreport is the accepted procedures that have been posted to a patients account. Recently the clinic has instituted aprocedure to check the charge tickets that were entered the day before to the report of charges posted. Any of theprocedures that were missed are to be put in. This causes some problems because the system may simply not haveprocessed a patient and the patient may be billed twice if another charge is entered.
Alternatives
Their were two paths that we felt that we could follow in our recommendations for Pediatric Cardiology. The firstwe considered was to carefully examine the process that we had charted. We brainstormed many alternatives forthis type of direction. Possibly come up with standard procedures that must be followed for each laboratory. Placereminders or checklists in each of the laboratories. Examine the flow of the process and find the trouble spots in theprocess and fix them. Implement some type of a double checking throughout the process. Possibly even scratch theentire process and come up with a new one or revert back to a variation of their previous system in which the chargeticket followed the patient’s chart. This alternative could significantly reduce the technician error but could not
5

absolutely eliminate it, nor could it eliminate the problems of data entry error or missing charge tickets. It wouldalso create more work that would need to be distributed.
The second path we saw was one that would take considerably more effort to develop and implement but would bedramatically more efficient than any other. It would also reduce the workload of the clerk, technician and data entrypersonnel. This path was to automate the process electronically by having the log books be on-line and having thembe the point of entry for a charge to be electronically sent to the University’s billing system. This would eliminatethe technician error since it would no longer be necessary to go find the charge ticket to check off. The datainputting error would also be eliminated because this part of the process would be removed. This alternative was notwithout hesitations. The development of such a system would be time consuming to develop and then to maintain.It would also be something that would be very unfamiliar to the entire clinic.
Findings
After the data had been compiled it became clear that something strange had occurred on July 22, 1996. Almost allof the procedures that had occurred on that day had not been billed. This significantly altered the data and did notcontribute to helping us identify the standard causes of missed billing. Statistically the date in question was anoutlier and was eliminated to show a more accurate representation. The findings that include this date can be foundin Appendix B. Except for this Appendix, the recommendations and findings in the report do not include this date.This does bring about the possibility that the data used may have slightly more missed billing than actually shownbecause what was meant to have been billed on that day is not known.
The data in Table 1.1 shows a breakdown of the procedures that were not billed by the specific laboratories. Theactual number may be found in Appendix A. The echocardiogram laboratory is losing the greatest number ofcharges, but all of the laboratories must be considered. The fmal recommendation will apply to them all..
Total #Procedure Performed
Oxygen Saturation 118Transtelephonic 28
Echo 389EKG 502Pace Maker 21AnalysisExercise Lab 18Catheterization 42Minor Procedure 22
TOTALS 1140
Not checked on Charge Ticket
NotChecked in Checked inLog Book Log Book
5.1% 5.9%0.00% 0.0%3.1% 2.1%8.0% 0.0%
0:00% 4.8%
N/A N/A0.0% 0.0%N/A N/A
5.1% 1.4%
Table 1.1 Laboratory Procedures Percentages That Were Not Billed
C.6
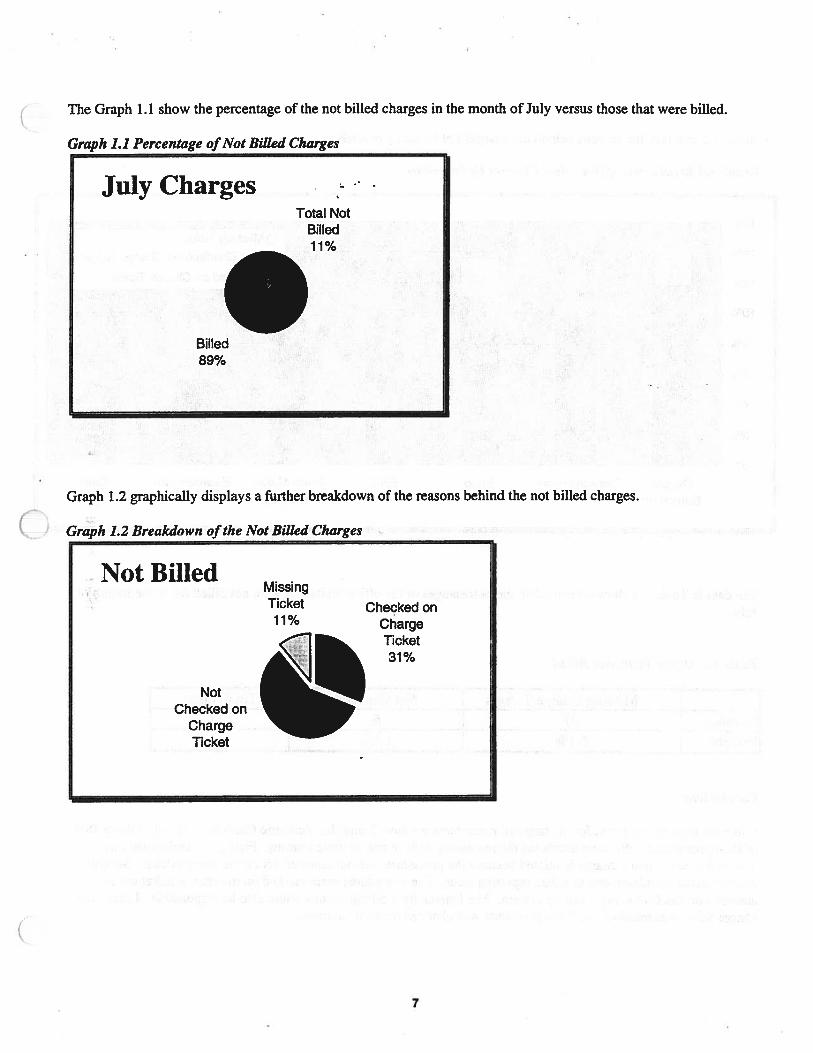
The Graph 1.1 show the percentage of the not billed charges in the month of July versus those that were billed.
Graph 1.1 Percentage ofNot Billed Charges
Graph 1.2 graphically displays a further breakdown of the reasons behind the not billed charges.
Graph 1.2 Breakdown of the Not Billed Charges:
July ChargesTotal Not
Billed11%
Billed89%
Not BilledMissingTicket Checked on11% Charge
Ticket31%
NotChecked on
ChargeTicket
7

Graph 1.3 displays the reasons behind the charges not billed by procedure.
Graph 1.3 Breakdown ofNot Billed Charges by Procedure
The data in Table 1.2 shows the number and percentages of the office visits that were not billed for in the month ofJuly.
Table 1.2 Office Visits Not Billed
Missing Charge Tickets Not Checked Total VisitsNumber 27 6 531
Percent 5.1% 1.1%
Conclusions
Using the data we analyzed for the targeted procedures we have found that Pediatric Cardiology is only billing 89%of their procedures. We have attributed the remaining 11% to one of three reasons. First is the technician error.This is the case when a charge is missed because the procedure was not checked off on the charge ticket. Secondlycharges could be missed due to a data inputting error. The procedures were marked on the charge ticket but notentered into the University’s billing system. The University’s billing system could also be responsible. Lastly, thecharge ticket was missing and if the procedure was checked or not is unknown.
16%D Missing Ticket
• Not Checked on Charge Ticket
• Checked on Charge Ticket
Oxygen Transtelephonic Echo EKG Pace Maker Exercise Lab CathSaturation Analysis
8

The data also suggest that the mark made when the charge ticket is reconciled against the log books is not effective.Many of those that were indicated in the log books as having been marked in fact were not. This safety check hasnot proved to resolve the problem.
These numbers and percentages may also be translated into actual monetary loss of facility charges. Table 1.3converts the missed billing numbers into actual lost hospital charges.
Table 1.3 Charges Lost in July
_________ _________
Facility Total # Total NotProcedure Charges Performed Billed
Echocardiogram $445 389 13.62%
Electrocardiogram $37 502 10.16%
Catheterization $1621 42 2.4%
Oxygen Saturation $34 118 14.41%
Exercise Lab $180 18 5.56%
Transtelephonic $37 28 14.29%
Pace Maker Analysis $43 21 9.52%
Minor Procedures $1,621 22 0.00%
TOTAL 1,140 11.3%
The total amount of charges that has been found to have been lost based on the audit of July’s activity comes to atotal of $28,085. See Table 1.3 for a breakdown by procedure. Assuming that July is fairly representative of anaverage amount of activity the total charges lost over the span of a year would equal $337,020.
The loss to the division from these findings is greater than simply the lost charges. The expense budget provided tothe division from the University of Michigan Hospital is based on the activity that they bill. Since they are missing11% of their billing their budget is much lower than it should be to cover the procedures that actually are performedin the division.
The data from the office visit audit show that there is potentially a problem in this area. From our data collected wefound no correlation between missing charges and day of the week, time, or resource. Lack of patient specific datafrom the MSP billing office prohibited us from proceeding further.
Recommendations
After close scrutiny and meticulous collection of all of the data it has been determined that an electronic billingsystem directly tied to the billing system of the University of Michigan should be implemented. This is the only waythat both the technician billing errors, lost charge tickets, and the data entry errors may be corrected and the ultimategoal of 100% billing be achieved. Simply improving the process would still not ensure that the charge tickets wouldindeed be checked nor would it ensure that a mistake in the entry of the data into the University’s billing systemwould not occur.
The physical requirements for this system would not be extensive. Their are currently IBM computers in each of thelaboratories. The program would be loaded onto a server and be accessible from all of them.
In April of 1997 the University of Michigan’s facility billing system will be switching from FALCON billing toHQ3.0 (Healthquest 3.0). This is an on-line system that will allow for charges to be posted directly to a patients
9

account. This system differs significantly from the current system and all interfaces between the recommendedelectronic system and the University’s billing system should be done with respect to HQ3.0 and not FALCON.
The point of entry for the system will be the log books since every patient that has a test must be logged in. In thecurrent process, the patient is logged in so an extra step would not need to be added. A major change with the newsystem is that instead of manually writing in the patient’s information they would enter it into a computer. Thiswould eliminate the technician having to remember to check the charge ticket, walk over to the charge ticket, andthen mark it clearly in the appropriate box. This eliminates the possibility of the charge ticket not being checked aswell as the possibility of missed billing due to a lost charge ticket.
The electronic log book would be standard procedure for each laboratory. The main screen for each laboratorywould look the same except for the fact that the field would be individually tailored to meet their specific needs.Each employee would be given a name and password to gain access into the system. Depending on their accessprivileges, they would be allowed into different parts of the system.
The change to an electronic system is significant but many aspects would remain similar. The electronic log bookwould look and function similarly to the log books currently in place. All of the fields that are in the current logbooks would be designed into the electronic system. The relevant information concerning they type of procedurewould also be available. Their would still be a list of the patients with the option to add the most recent patient at thebottom of the list. Once a patient is entered their information will be stored in a database.
The time spent to log in a patient would be decreased because all of the information would not need to be added.Simply entering one field would bring up the necessary information from the database relating to the patient. Thiswould not only decrease the time but the accuracy as well. Safety checks in the program would catch any mistakesmade about a patient. For example if a registration number was not valid an error message would appear indicatingthis. The patient name would also be automatically entered and any confusion caused by misspelling would beeliminated.
The entire step of having to reconcile the log books with the charge tickets would also be eliminated. Each patientin the log books would no longer have to be initialed as having been billed. This step was shown in the data to beineffective.
Additional capacities could also be added that are not possible in the current system. The option to count thenumber of a procedure performed in specified months could be available. In addition, reports could be generatedthat show any specified compilation of data that would be useful to the employees in the division. For example areport could be made to display all of the procedures a patient had for a given date of service. Queries concerningany aspect of the database could also be made. Another possibility is to included additional fields that do not occurin the log books but would be useful, such as the diagnostic code. The above are only possibilities to demonstratethe capacity of the suggested system. The actual capacities should be decided upon by the division.
After the essential information had been entered it is then to be sent directly to the University of Michigan’s billingsystem. This bypasses the necessity for a clerk to manually input all of the days activities into the system. Bysending them directly it will not only eliminate the time spent but will eliminate the chance of a data entry error.
This type of direct electronic system is currently used in 80% of the clinics at the University of Michigan Hospitalincluding the Adult Cardiology Clinic. The transfer process is already known, so the clinic needs only to follow theformat of the other clinics. In general terms, after the patients data has been logged in and stored in a database itwill need to be formatted in a standard way specified by the Hospital. For example the registration number wouldneed to be eight characters in length, the visit number 4 characters, etc. From here the formatted information wouldbe saved as a file and sent by a file transfer program to the mainframes of the Hospital. This formatting and sendingof files would be done after each working day. To ensure that the billing had been accurate a report of the activity
10

of the given day could be generated from the new system and reconciled against the printout from the Hospital’sbilling system.
There are some problems that are inherent to an electronic system. These problems are not a common occurrenceand can be remedied if the proper back ups are instituted. The server that Pediatric Cardiology uses at the presenttime backs up all of its information once a daS’. This process should be continued. A hard copy of the logbooksshould also be printed out at the end of the week so if something were to happen to the system a copy of all of thepatients for each laboratory would still be available. Additionally a paper log book having the same fields as theelectronic system should be kept in each of the laboratories. This is in case the system is ever down and it isnecessary to log in a patient. However once the system is up again, the information should be transferred from thelog book into the system.
The automated system would make many jobs in the division a lot easier. Those employees that would experiencethis reduction in work load could then focus their time in other areas. The extra time would not go to waste, butshift the focus into areas that my have been previously neglected.
It is additionally recommended that the Medical Service Plan portion of the billing be reviewed. This includes theMSP portion of the laboratory procedures as well as the office visit charge in it’s entirety. The loss of billing due todata entry error was not able to be quantified but should be in the future. The automatic billing should be astandard procedure that applies to all aspect of the billing process including eventually the MSP side. We wouldassume that if a charge ticket was not checked then the MSP side would also not get the charge contributing to agreater loss.
All of the above recommendations will assist in the attainment of the goal of 100% billing as well as improve
( accuracy, data and report generation and budgetary planning. Assuming July is a typical month, they will assist incapmring at the least, the $28,085 of lost charges for a month and the $337,020 lost annually.
Action Plan
The Pediatric Cardiology Clinic should immediately begin planning for the electronic system. There are severalareas that need exploring in the development and implementation of the new system.
A project team will be necessary. The project manager should be named that will plan a feasible time schedule,oversee the progress, and help to have a timely completion. There will also have to be members that have technicalknowledge in the following fields; database management systems, programming languages, server knowledge, andgeneral networking knowledge. These technical members will have a number of responsibilities. They will set upthe database, design, program, debug, test, and implement the system. There should be several technical membersdue to the amount of work that will be required in this area. The input of the entire clinic will be needed, especiallythose that will be significantly effected.
As a beginning point, Adult Cardiology’s electronic system should be benchmarked. The construction of theirsystem should be closely examined. The interaction between their interface and the Hospital’s mainframes shouldbe documented. Contact should be kept with the clinic throughout the project when complications arise since theAdult clinic already has a proven system. It may even be possible to replicate some of the system for pediatrics.
The next information source that should be contacted is one that could define the requirements for the file transfermethod and formatting that are required by the University of Michigan Hospital’s billing. There are several relateddepartments that may need to be contacted. The system should be created to interact with the new HQ3.0 billing
( system. The possibility of verifying that files have been received should also be investigated. Once this iscompleted the focus can then shift to the construction of the electronic billing system.
11

The specific needs of Pediatric Cardiology will need to be identified. This includes the state of the current logbooks as well as any additional features that would be desired. Each of the laboratories needs to submit exactlywhat fields they think would be useful in the new system. This would included the columns that are currently inplace. They would also include any additional information that would be helpful. They would also submit any typeof report that would be helpful to them if generated by the system.
The physicians should also contribute their suggestions. Additional fields should be added, such as diagnosticcodes. They would also request that the system have the capacity to generate certain types of reports that would behelpful to them.
The other positions in the clinic should also be consulted as to any capabilities they may need.
Once all of the suggestions had been collected and compiled, the design of the system should be outlined. Thisdocumentation should be flow charted and all of the relationships in the program defined. The design should thenbe shown to the faculty and senior laboratory technicians to receive any additional input.
The database management system should then be decided upon. The type of software that is desired should beinstalled. The database relationships among the desired fields should then be made, From these relationships themost optimal database should be constructed.
With the database constructed and the system design complete, the development phase of the project may begin.This will be one of the most difficult and time consuming aspect to the project. The programming in the chosenlanguage should begin. This coding should be broken down into different phases and a timeline set for thecompletion of each. This breakdown will make the progranmiing more manageable. As the program is developeddebugging should be occurring simultaneously. After the program is able to run, error handling should be invoked.
After a version of the program is ready a fairly extensive amount of testing should be performed. A testing softwaremay be purchased or manual testing may be done. Every possible combination of information and every avenuepossible should be explored. This is critical step in the quality of a system once it has been implemented.
Once all of the above steps have been executed the system is ready to “go live”, or in other words ready to be used.The fully developed program should be placed onto the server at Pediatric Cardiology so that all of the computersthrough out the facility will have access. Training sessions should be held so that all employees are aware of thechange and understand how to use the system. A manual should also be written so that it may be referenced shouldproblems occur.
During the first few weeks of implementation the hand written log book and checking of the charge tickets as well asthe electronic system should be run simultaneously. This is to test the system in a real situation and this is also sothat if a problem occurs no data will be lost.
After the system is running without problems the hand written log books should be filed away. A single log bookshould be placed in each lab in case the system goes down. A binder for the weekly printouts should also be placedin each laboratory.
The final documentation and code should also be filed and a copy of the program stored. This is so that ifadjustments or additions need to be made in the future they may be done.
The last hurdle that the new system will encounter is the maintenance of the system. This is not a small job and anemployee should be responsible for it. The division will hold the responsibility for the system and will be primarilyresponsible for handling all maintenance concerns internally.
12

Appendix A• • Actual Numbers
Appendix BData with July 22, 1996
Appendix CFlow Charts
Appendix D
c Diagram of the Pediatric Cardiology Clinic
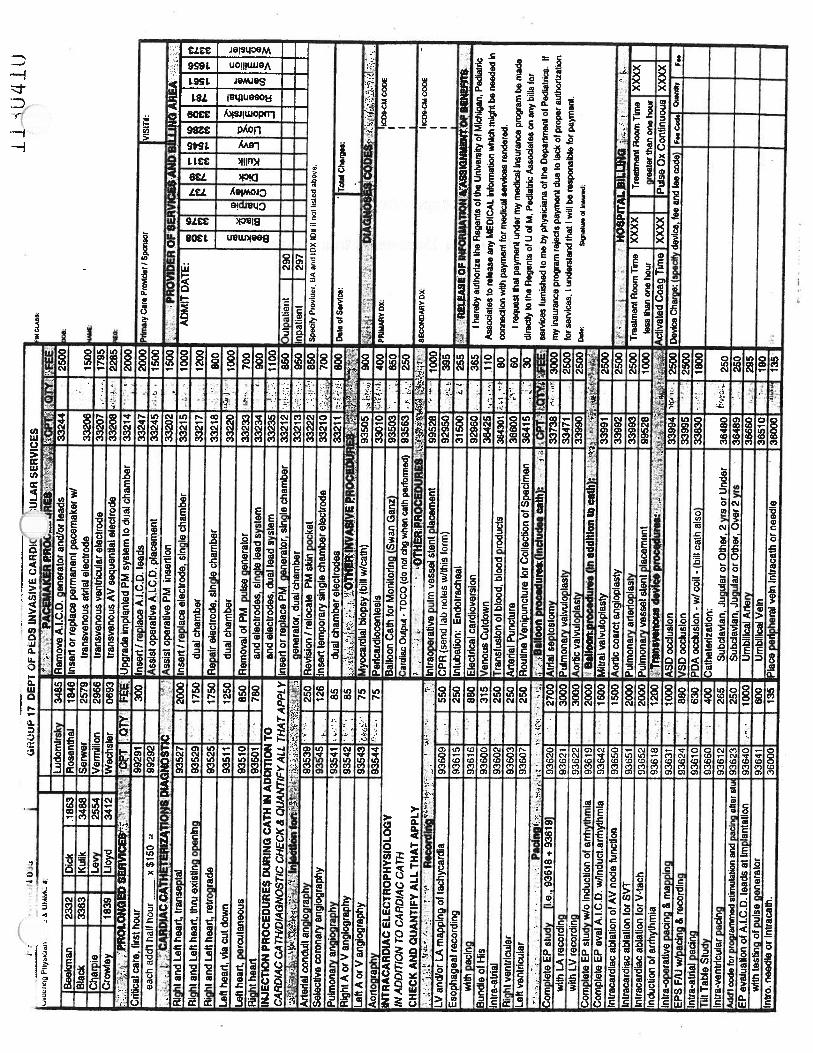
Appendix EPediatric Cardiology Charge Ticket
Appendix FSource Code for Demonstration Program
13

Appendix A
Actual Numbers
Actual Numbers for the percentages found in Table 1.1
Not checked on Charge Ticket
Test Checked on Checked in Not Total Not Missing Total Not Total #Charge Log Book Checked in Checked Ticket Billed PerformedTicket Log Book
Echo 23 12 8 20 10 53 389Pace Maker 1 0 1 1 0 2 21AnalysisTTX 4 0 0 0 0 4 28
02 1 6 7 13 3 17 118Minor 0 N/A N/A 0 0 0 22ProcedureExercise Lab 0 N/A N/A 1 0 1 18Catheterization 1 0 0 0 0 1 42EKG 10 40 0 40 1 51 502TOTALS 40 I 58 16 75 14 129 1140

Appendix F: MD Data Collection Form for Establishing andMonitoring Scheduling Templates
fr_d___’ jI -
r
— t “..-J--,.‘,
.. .
—V—.
Cardiology - Page 17

Patient type: -
Indirect• Date Begin
• 1
___ ___
.2.
___
‘.4
___
• ...• .• •..
.. .1
6’_•..
_____
8.
_____
•
.
11
_____ _____
13___
___
14 •.
15
______
• 16
______
17
____
19r.,..
____
20
______
21:22
__
____
____
2.._____
_____
•• •2
______
Data Cal1ction Form for Establishing & Monitofing Scheduling Template
Doctor:
_____________
IndirectEnd
• TotalIndirectService
DirectTime-tn
DirectTime-Out
/ —
• (‘••
TotalDirect
Service
TotalServiceTime

Appendix B
Actual Count
Data with July 22, 1996
Not checked on Charge Ticket
Test Total # Checked on Checked in Not Checked Total Not Missing Total NotPerformed Charge Ticket Log Book in Log Book Checked Ticket Billed
Oxygen Saturation 128 10 6 7 13 4 27
Echo 408 41 12 9 21 10 72
Transtelephonic 29 5 0 0 0 0 5
Pace Maker 22 2 0 1 1 0 3AnalysisEKG 531 10 40 0 40 1 51
Minor Procedure 24 0 N/A N/A 2 0 2
Exercise Lab 18 0 N/A N/A 1 0 1
Catheterization 44 2 0 0 0 0 2
TOTALS 1204 70 58 17 78 15 163
Percentage
Not checked on Charge Ticket
Test Total # Checked on Checked in Not Checked Total Not Missing Total NotPerformed Charge Ticket Log Book in Log Book Checked Ticket Billed
Oxygen Saturation 128 7.8% 4.7% 5.5% 10.2% 3.1% 21.1%
Echo 408 10.0% 2.9% 2.2% 5.1% 2.5% 17.6%
Transtelephonic 29 17.2% 0.0% 0.0% 0.0% 0.0% 17.2%
Pace Maker 22 9.1% 0.0% 4.5% 4.5% 0.0% 13.6%AnalysisEKO 531 1.9% 7.5% 0.0% 7.5% 0.2% 9.6%Minor Procedure 24 0.0% N/A N/A 8.3% 0.0% 8.3%
Exercise Lab 18 0.0% N/A N/A 5.6% 0.0% 5.6%
Catheterization 44 4.6% 0.0% 0.0% 0.0% 0.0% 4.6%
TOTALS 1204 5.8% 4.8% 1.4% . 6.5% 1.3% 13.5%

-
Appendix C
Flow Charts
C,

Echocardiogram Patient requiresEchocardiogram
Exit lab and findcharge ticket while
finding chart to placereport
Check off log book that patient was billed(Does not occur immediately)
Place report with chartand place charge ticket
in outbox

Electrocardiogram
rohate box
C
(
Patient requiresElectrocardiogram
Yes
Make a new chargeticket and place tracing
in chart
Take tracing to chartand find charge ticket
ticket
Yes
V

Exercise Test
Report place in box forreviewing and to be
typed
Find charge ticketwhile placing report in
chart
Mark appropriate boxon charge ticket
Charge Ticket and Chart(enedule
______
nCharts are brought
from medical recordstôaboxnearthe
clerks
Patient arrives
V
Charge ticket iscreated and the
appropriate office visitcharge marked
Charge ticket placed inbox atthe nursing : V
station
Charts travel withpatient to the exam
room
1.During testing the chart
either stays in theexam room or is
placed in the nurses’station or in the
physicians’consultation room
The following morning thecharge tickets are collected
V
and entered into Falcon billing (system by clerk
•w’r
J
-.
I
4.’-.
t)
£2ojojpaT41PdaqjoiuSujq
crxwuaddv
C)

Diagram of Pediatric Cardiology Clinic
________________
Physicians’LibraryConsultation Room
Echo
__________ _________________ ____________
NurseEKG
Clinicians
ExamRooms
_________
Charge Tickets
NursingStation
ExerciseLab
WaitingRoom
ClerksCheck-In
* Not to scale

CD z. n n Mt o a.’ o n CD n CD

Ip.d
b,O
td.i
irr
Ptiy
eIcl
enN
ame
&U
tV4G
5or
ctw
ckon.
relo
w:
Ana
lysi
sof
anti
-tac
hy
card
iaPM
syst
em
incl
udes
EG
G.
prog
ram
min
g,in
duct
ion
and
lam
inat
ion
ofta
chyc
ardl
law
ith
Inte
rpre
tatio
nof
reco
rdin
gs
R18
46
Ele
ctro
card
iogr
am:
..—
—
:Hof
ler,
tipt
o24H
rs.
.as
s0
4—
:Ho
Iter
,Lp
toi2
Hrt
aeio
4
:Eso
chaa
eal
Flec
ordi
na
1863
1IL
ucba
drek
y34
851
PCT
UE
CG
’’’—
-..—
..—-.
,,“-‘
V
Bla
ck3363
Kul
ik3488
Russ
ell
46
20
:Sta
ndar
d(1
2le
ad)
35.0
1
33
87
Ly
2554
Ser
wer
25
79
Lat
ePo
tent
ial
EG
Gau
O2
—
Cro
wle
y18
39U
cyd
34
12
Ver
mil
ion
29
66
Rhy
thm
Ship
-.
—
,1rR
OC
ED
UR
ES
c’
tallo
onC
di.
frr
Moi
iteri
ng(w
an-G
aiiz
)-
Me
19
Wec
hsl
er-
0693
ass
01
V.V
•-
--
ass
23
ee
01
0107
3ntr
aIP
eflQ
Jo
wn
2Y
rsor
Un
der
CP
R’-
-Att
ach
rep
ort
&-
--
:-O
FSE
RV
ICE
SA
ND
BIL
LIN
GA
RE
A
áxC
ulao
iw
Ov
er2
Yrs
--.1
-i..
E1et
hvec
ardker
sion,e
lech
ical
ord
rug
..
SIT
E:
003
p..
-—
:xi-T
DC
X)
35020
——
Inhi
batio
n:E
ndot
rath
eal..V
tPIy
ian
esc.
inc
aco
inin
ath
eaab
cft
‘-rr
eadi
nill
Tes
t3
eo
and
Sub-
5db
—!
ri1
.i
T,e
adm
iWan
dEC
G—
—o
ng
rid
bel
ow
:•
:Sub
davi
an,J
ugL
daro
rOth
er,O
ver2
Yrs
•.•
Oxy
gen
Upt
ake
orC
ardi
acO
utpu
t—
-=
>
:Lic
alA
rlery
...
:..
;.-.
A.I
.C.D
.inqu
iiyl
anal
ysis
3a.
27
—--
-J
-
.:L
kthl
llcal
Vei
n•.•
‘....
r.iP
4-.
i’w
ith
repro
gra
mm
ing
a27
CC>
‘
Aze
del
Caj
irsd
atjo
nP
ercu
t.-
.:--“-.‘•
-•‘
s;‘
Pac
emak
er,
Ele
ctro
nic
Ana
lysi
s,D
ual
aae2
7—
.-In
patie
nt18
0-
MC
a&
nwtcun
‘.‘
with
repr
ogra
mrr
ilng
_‘-.
-
unt
,..
‘i:
’P
acem
aker
,E
lect
roni
cA
naly
sis,
Sin
gle
359
27V
.tc
)bse
4v:
159
nh
roN
..ec
rIn
trac
aIV
ein
i.;:,‘
,.;i-
-I’
‘:.‘
with
repr
ogra
mm
ing
3ê27
—-•
Sp.
cdyP
ror.
BA
md
IDX
IDa
Sii.d
aio
v.:
enot
asC
u)d
,V
ecto
rcar
dllo
gram
as.
12
ttai
cti
Blo
od&
8lo
od
Pro
duct
s,-:.
iPu
lse
Oxi
met
ry,
Sing
le36
930
-:
dm
atyC
..P
roid
.IS
pon.o
p.J
)ijj
-‘‘
=H
OSP
ITA
LB
ILLI
NG
CPT
OTY
Ven
ipis
ictu
mU
nder
SYrs
.:O
ther
Vei
n--
--.
--.
reah
nent
Roo
mT
ime
Ihour
3730
1—
oe.ir
rDA
TE
Ven
ipLa
ictu
reti
nder
3Yrs
.:S
calp
Vei
n:::...
-—
reat
men
tR
oom
Tim
e>1
hour
3730
2—
.;-
empL
mcU
eJ.ln
der
3çr
s.(,
hcc
One
.J,
...A
ctiv
ated
Coai
lahon
lim
ev.
at&
.no.
Tcsa
l cIi
u.s
Fem
orsi
.“
‘?‘
Sa
11W
Sin
u-.:
jP
.,
.P
uls
eO
xim
etry
,co
nli
nous
mon
itor
ing
ass
31.
eqlp
mci.
.__
yrsN
oB
14C
i‘--
kitt
onC
losu
reD
evic
e—
,k)
evic
eC
harg
e(s
ç.dly
devi
cele
een
d1
..co
deD
IAG
NO
SIS
CO
DE
S
itinV
eax
Col
lect
ion
ofS
ped
men
/:-
r..c.
1-C
MC
OO
S
ass
14
2D-
V-
——
ssoo
en*y
ox
Dop
pler
V
I
Dopple
rOobM
——
Ech
ogra
phy,
Com
plet
eM
ater
nal &
Feta
l35
.14
,.
DIS
CO
UN
TED
CH
AR
(ES
:
tres
sEdi
oWw
itei
p&R
epod
3501
4‘V
VV
Reason
.
Dcb
iAam
ineS
bess
Ech
o(m
terp
&R
epor
t35
01—
-—
——
.D
lsco
unIt
he’
char
gby
‘-%
‘a’P
iofC
oui-
tesy
SV
)TE
:F3
69
l4is
chec
ked
abcv
eom
1t3
89
36
3.03
6—
:‘:,
•.
..,.,,....
V
)TE
:F38
914i
chec
ked
abov
e,om
it38
936
3503
6—
•:
——
—
)TE
:IF
38914
Isch
ecke
dab
ove,
omit
3893
7as
s37
34.
911
res
ixol
ocoU
iion
ofba
Dee
nt-
1
)TE
F3
8O
l4is
chec
ked
abov
e,om
it38
937
3.03
7—
——
s-
mne
e.op
bege
.lE
tho-
2D,w
cww
’oM
-Mod
e35
014
Pro
be
ilac
ein
enl
kn
eg.
&re
port
——
——
—,.
1,‘
..
Pla
cem
ent
ofpro
be
only
ass
14.
,Z’
Imag
eaj
ssib
ori
lnte
rp&
repo
rtas
s14
——
—4’
‘
OT
Ell
TH
IS18
CH
ECK
EDT
hEN
OIl
TBL
LIN
G38
914
310
16V
;,i
aJ(
th
Icw
ho
Ne.
d.o
rbit
rmca
th.v
.ln
V—
V—
—•j
,•-... F
AL
CO
N
‘‘Ir
!‘4
I

i..g
jI
lNattj
cT—
CA
Br
,tC
1A
LT
Ysv
t.;,
iF.
LL
lN
,-
UL
TA
TIO
NS
Init1
alC
o..
-Lev
ell
Lev
el2
•Lev
al4
You
may
loiw
sid
IN.t
oyo
urbw
,wen
c.ce
nter
Io#
rsl.
.bum
am.n
t.U
i*.m
lIy
atU
lchl.
aH
.aII
hS
yste
mC
om
er
Serv
Ice
(31
3)14
7422
5or
1400
-Il4
4581
TA
XID
#3
8-6
00
63
09
DR
.lo
xII
CO
DE
OTY
FEE
145
1992
02‘--
155
I
pecI
tyO
rd.f
lnQ
Phy
&cl
anN
ame
&
-Lev
el3(
Fet
alIm
agrn
g)I°
E:i
I336
31It<
uikI9
9244.4
’22
0
IIo
ick
lCha
rvie
_udo
mir
skv
1863
I338
71IL
evv
18
2554
46:
-Lev
el5
I[9
9245
°18
391
IUoy
d34
12B
LU
6SH
IEL
D;
hIc
bis
nL
ic.n
..an
b.1
—PR
OC
ED
UR
ESN
ON
INV
ASI
VE
DR
-ID
XI
Las
t:(2
tstb
s.I
dgte
)E
choc
ardl
ogra
phy,
com
plet
e(af
l3
code
s)Fi
rst
MED
ICA
ID:
74g4
PSI’
ocP
rovi
d.r
Nw
r4er
2D($
300)
Add
ress
:D
oppl
er($
180)
Dop
pler
Col
orFk
n($
150)
OFF
ICE
VIS
ITS
—Ir
anse
sop
hag
eal
Ech
oN
ewP
atie
ntO
ffic
eV
isit
-L
evel
199
555.i;
50P
robe
plac
emen
t,Im
age,
&re
port
(N
eav.hsdno
-Lev
el2
9951
2:4
60P
lace
mer
aof
prob
eon
ly
iNC
LA
SS
25on
os(o
r)0
&
1F
EE
[;::
?;$f
:JI..
—
PDC
e.v
ces
thir
mpa
st3
yr.)
-L
evel
399
203‘
80Im
age
aqui
sitio
n,in
terp
,&re
port
630
850
400
450
0228
3• L
evel
4ö4
47Z
ii’
Ech
o,co
mpl
ete
mat
erna
l&
feta
lst
udy
-L
evel
S99
205
t15
0S
tres
sE
cho
ReV
Isits
•L
evel
I(M
Dno
tre
qd)
9921
1A
135
Oob
utam
ine
Str
ess
Ech
o-
Lev
el2
9951
640
Dup
lex
scan
,LE
a,le
nes,
bila
tera
l-
Lev
el3
9921
3iji
Follo
wup
orlim
ited
stud
y-
Lev
el4
9921
495
Dup
lex
scan
,LE
vein
s,bi
late
ral
-L
evel
599
215
125
Follo
wup
orlim
ited
stud
y—
PRE
VE
N11
ON
CU
NIC
——
Ele
ciro
card
togr
am-
Sta
ndar
d.12
lead
%Iew
Patie
nt(C
onsu
l--n
eed
refe
rrin
g)88a88(:
...i
422
5L
ate
Pote
ntia
lE
CG
Est
abls
hed
Patie
nt95
Rhy
thm
Stri
pro
up
Ses
sIon
(12
sess
Ions)
9941
2.L
j—
Hol
ier,
upto
24ho
urs
Indi
vidu
alC
ouns
ehng
(ind
icat
ele
e)99
400
upto
12ho
urs
PRO
LO
NG
ED
PHY
SIC
IAN
SE
RV
Idi’
—T
reed
mill
Tes
tan
dE
CG
Cho
ose
thes
eco
des
Inad
diti
onto
Con
sult
orV
IsIT
d.
—O
xyge
nup
take
orca
rdia
cou
tput
Prol
onge
dF
ace-
lo4a
ce30
-60m
mIn
troN
eedl
e,in
trac
ath
for
echo
cont
rast
Eac
had
dlon
&30
min
utes
9935
550
Vec
toro
ardt
ogra
mPr
olon
ged
non-
lace
-lo4
aoe
30-6
0mm
99
35
8.
100
frJ.
C.D
.In
quiry
Iana
lysi
sE
ach
addi
onaI
30m
inut
es99
359
50w
ithre
prog
ram
mm
:
CO
NFE
RE
NC
ES
—A
nti-
tach
yPM
anal
ysis
,w/p
rogr
amm
ing
Brie
fP
hone
Cal
l-
Pt/
Par
ent
9937
125
Pac
emak
er,
oled
roni
can
alys
is,
dual
inte
rmed
iate
Pho
neC
alP
t/P
aren
t99
372
-35
with
repr
ogra
mm
ing
Com
plex
Pho
neC
al-
Pt/
Par
ent
9937
3‘:.-
50P
acem
aker
,el
edro
mc
anal
ysis
,si
ngle
Tea
mC
onfe
renc
e(1
/2)
9936
1.
50w
ithre
prog
ram
mm
gN
UR
SIN
GI
OT
hER
CA
RE
....
Fran
stel
epho
nic
pace
mak
er,
dual
Nur
sing
VisI
t--
Rou
tIne
9951
930
-si
ngle
-C
ompr
ehen
sive
9952
045
rran
sih
onic
Rhy
thm
Mm
lnls
trel
lon
ofT
hera
peut
icM
uds:
9079
9O
xim
etry
. sin
gle
(Fee
v.d
sNe$
7t0
$15)
Spe
dfy
Dru
g:A
‘:•
,C
US
HO
SPIT
AL
BIW
NG
’U
FC
IIe
code
-
,C
ompr
ehen
sIve
CM
SV
IsIt
.M
anag
emen
t/Fol
low
-up
CM
SV
isit
.Su
ppor
tC
MS
VIs
1-N
wal
ng.
Supp
ort
CM
SV
iel
-D
iste
tic,
.Su
ppor
tC
MS
VII
-S
odai
Wor
k.
Supp
ortC
MS
VII
-Ps
ycho
logy
SIT
E,
SUB
-SIT
E&
PHY
SIC
IAN
IDX
IN
um
ber
s60
0S
Ite:
003
Sub
-Sit
es:
600
PH
YS
ICiA
Ns
lox
Num
bers
:IC
tlnIc
ill
125
Bla
ck33
78O
bser
vatI
on15
975
Ch
arp
le33
87L
udom
irek
y33
0912
5C
row
l.y
737
Ros.
nth
al78
175
DIc
k73
9R
uss
ell
3399
kL
.440
Kul
Ik33
11$
ii-w
ar15
841;
30L
evy
1545
V.h
nll
ton
1658
25L
loyd
3286
S.W
.chsi
.r33
731
‘20
0D
AT
AEN
TRY
NO
TE
:P
ut
offi
cevI
sIt
orco
nsu
lton
one
-
150
invo
Ice,
loca
tion
1 1..
Get
new
Invo
ice,
ente
rp
roce
di.
r.s
loca
tion
—2.
T16
0D
ate
ofS
wvi
c.:
Tou
tChar.
s
135
DIA
GN
OS
ISan
dIC
D-9
-CM
Code
iR
--
esr..
120
i-
ned
êig
cu
i.ca..
.r.I
idie
,
I!ai
500
Ii:]:
I11
0C
AS
HIE
RU
SE
ON
LY
90T
.11
0Pm
tC
ode
Pay
men
tB
alD
ue_
__
__
__
_I.
o-P
ay_[:J
Pald
Che
ckN
o._
__
__
__
__
40I:
35ash
_V
Isa_M
ast
erc
ard
_D
lscover_
Am
Ex
p_
20:
-15
BUI I
nsur
ance
[]A
ssIg
ned
[]co
urte
sy39
5U
nkno
wn
reti
prnvld
ed36
5R
efer
rall
]it
pi.v.o
u.vi.
*
LB
1LL
ING
••.
DIS
CO
UN
TE
DC
HA
RG
ES
ho
ur
XX
XX
XX
Xon
eho
urX
XX
XX
XX
Dis
coun
tth
ech
arge
by%
asPr
ofes
sion
alC
ourt
esy
I.e
and
I.e
code
Hoe
ptb
spB
itIn
sura
nce
only
-D
ono
tse
nda
NI
toth
epa
tient
Pie
Ced
.B
itre
sear
chpr
otoc
ol-
dono
tbi
llpa
tient
iped
V:
——
ffP
tiy
sk
SàrR
ép
imd
#o
ren
yc(t
hab
áv
e
DA
TAEN
TRY

You
aylo
iwar
dth
i.toy
kw
ur.
nc.
cri
.fo
rr.
Intb
ws.
m.n
t.U
.*ar
04
ty04
Mic
hig
anH
ealt
h8y.m
Cuom
arS
aM
e.
(31
3)
147-5
225
or14004144511
3488
2554
Serw
er25
79V
erT
ndio
n29
66DO
see
14
0228
3SI
TE
.S
UB
-SIT
EA
PHY
SIC
IAN
IDX
IN
um
ber
s
IC
ON
SUL
TA
TIO
NS
DR
.ID
XN
CO
DE
0FY
FEE
Spec
ify
Ord
eiin
gPh
ysic
ian
Nam
e&
UM
MO
N::L
udom
irsk
y34
85Il
nW
Con
sul
--L
.v*1
‘-
...
9920
1.
145
Ros
enth
al18
4699
202x
155
Dic
k18
63—
Rus
sell
4620
css
I99
243
.185
Bla
ck33
63K
uhk
________
9O
244
.-
220
Cha
ipie
3387
Lev
y
__
__
__
•L
.v5
J.;
•99
245
...
250
Cro
wle
y18
39L
loyd
3412
Wec
hsle
r06
9355xi
-:O
FF
ICE
YIS
lTS
•.
...
.T
rarm
esop
hage
a)E
cho
N.w
Pat
I.is
t041k. v
ti.
öv
etf
C.
50P
robe
plac
emen
t.im
age,
repo
rt
__
__
_
see
14—
—
:;
0061
2.
.60
Pla
cem
ento
fpro
boonly
______
i4
——
CC
.he
.fl
lgp
ms,
m)4
Ley
&3
‘9
02
03
”‘
80Im
age
aqul
sif I
onIn
terp
repo
rtse
e14
“.j
Th..
.‘.L
e,é
U4.
0020
41
15
..E
cho,
com
plet
em
aler
nal
&Ie
taI
stud
y
__
__
__
•_90005
150_S
lres
sEdio
______
RV
toIt
s-
1eié
l1’
(MD
not
reqd
)-
...
9921
135
Dob
utam
ina
Str
ess
Ech
o
__
__
__
_
.Lev
ei2.
.4,j
995lJy
.40
IF3
89
l4is
chec
ko
dab
ov
o,o
mit
38
93
6
______
..tJ3
,c•
9921
3:4y.
85
lF3
89
l4is
chec
ked
abo
ve,
om
t38
93
6
______
-Láv
eI4
9921
4,
95IF
3891
4is
chec
ked
abov
e,om
it38
937
______
9921
5‘.‘
125
IF3
8g
l4is
chec
ked
abo
ve,
om
it3
89
37
______
..
,PR
EV
E...
.E
lect
roca
rdio
gram
-Sta
ndar
d.12
lead
__
__
_
8888
8•.
...
225
LaI
ePoI
enti
alE
CG
__
__
_
E,I
aIi
ed
..
9999
995
Rhy
tlwn
Str
ip
______
GS
es&
on(1
2sssla
ns)i
Cw
‘H..
0041
2.
?‘•
Holt
er.u
pto
24hours
______
nd
MC
ow
e4
ng(kfie
);.
k99
400.
...
uplo
12ho
urs
•PR
OL
ON
GE
DPH
YSI
CIA
NS
ER
ViC
ES
_“.•
.iT
reed
mM
Tes
t_an
d_E
CG
______
Chose
.th
ea.
cod•s
Inad
dit
ion
toC
on
sult
orV
isit
Cod’:
Oxy
gen
upta
keor
card
iac
outp
utj
Pro
long
edFa
ce-1
o.Fo
nö3O
6qm
bio
le.j
ci&
9935
4,‘
4ji
100
IFT
HIS
ISC
HE
CK
ED
ou
rt
BIL
LIN
G38
014
E.c
haddll
orl
80ir
*ag.s
.vfI;’
9935
5‘5
0V
ecio
rcar
dlog
ram
__
__
_
see
12P
mL
,.g
ed
ia(e
4o
4ac.
3060
mbt
’j1
4L90
358.
100’
AIC
D.
Inqu
Iry
/an
aly
sis
__
__
_
3—
4E
eshad
dit
tiei
3&
nil
iiu1é
dL99
359
t44
(kh5
0aw
ithre
prog
ram
min
g
__
__
_
..
.v
Ant
i-tac
liyPM
anal
ysis
,w
/pro
gram
mln
g
__
__
_
see
27—
—
9037
1H
i25
Pac
emak
er,
elec
tron
ican
alys
is,
dual
__
__
_
see
27b
e’jo
njQ
iLP
t/P
aret
9937
2.3
5w
ithre
prog
ram
min
g
____
see
27—
—
Oo
roçt
oP
heC
aNcP
VP
iren
-kØ
9037
3Pa
cem
aker
,el
ectr
onic
anal
ysis
,si
ngle
__
__
_
see
27T
eem
Con
leis
nàO
Sg
O36
lJp
,’
50w
ithre
prog
ram
min
g
______
see
27—
—
NU
flS
lNQ
1O
ThE
flC
AR
E.41
. .,
Tra
nsla
leph
onic
pace
mak
er,
dual
______
see
03N
urgV
sit
J4flô
tkk
’1V
99519[:
w.V1
30si
ngle
______
•‘
—
IIC
om
j9
96
2O
Iifi
45r
Tra
nste
leph
onic
Rhyt
hm
______
see
03—
—
Pul
seor
Ear
Oxi
met
ry.
sing
le
__
__
__
_
(F-.
14
-‘
Pro-
Tim
________________
Sed
Iy’D
n)g
•‘
•,
•15
P11
-M
ach
Rep
ort
CI4
SH
OSP
ITA
LB
ILLI
NG
Car
dbes
ion
-an
ym
etho
dM
FCI t
ee
a—
.H
OSP
ITA
LB
IWN
GC
ompr
ehen
akie
CM
SV
isit
Tre
men
lR
oom
Tim
e,le
ssth
anon
eho
ur37
301
Man
agem
erit)
FoIl
ow-u
pC
MS
Vis
it‘
Tre
etm
enl
Roo
mT
ime,
less
than
one
hour
3730
2Su
ppor
tC
MS
Vis
it-
Nur
sing
Dev
ice
Cha
rge:
(spe
cify
devi
ce,I
.,ar
idI.
.co
deH
oip
Has
pSu
ppor
t CM
SV
lit
-D
iete
tics
__
__
Supp
ort C
MS
Vis
it-
Soci
alW
ork
Supp
ort C
MS
Vis
it-Ps
ycho
logy
seel4S
It•:003r
.
.4
see
14—
—P
HY
SIC
IAN
.ID
XN
um
b.r
.:j
Cli
nk16
1se
e36
—B
lack
3376
Ob..,v
atlo
n.1
59•.
see
36—
—C
har
pl.
3387
Lud
omlr
sky
3309
see
37—
Cro
wle
y73
7R
ose
nth
al78
1se
e37
——
DIc
k73
9R
uss
ell
3399
see
01—
—K
ulIk
3311
Sir
w.r
1564
sae0
2—
—L
.vy
1545
fitm
IIIo
n16
56
——
Uo
yd
3286
S.W
.ch
sler
3373
see
04D
AT
AEN
TRY
NO
TE
Putetfic.
vIil*
orco
nsu
lton
on.
see
04—
—im
moi
ce, l
ocat
ion
oi,i
1ne
wIrw
oicá
, eit
irpr
oced
irea
loca
tion
•2.
3800
5—
—D
al.o
tSoi
vice
:T
gdC
har0
e.••
i..
.
see
16—
—D
IAG
NO
SIS
and
ICD
-9-C
MC
od.
CA
SHIE
RU
SE
ON
LY
•.
..
‘.4•
‘‘t
.•.
p4,.
•i,i.
•iiifis.L
•.i,,,,.,,,,..
____
:i;
——
••
i)n
en
ce4
dE
JcQ
W
:$gS
sL
kil
moY
r04proM
èdjv
==
#_______
LsJ
.Itu
Lx
AR
QE
S.
TAX
IDN
38-6
0063
09
FA’
N
LIU
SL
iMM
U.
PRO
LO
NO
ED
SE
RC
E8’
CP
T
Jt
17D
E1’
c*P
cOS
INV
AlV
EC
AR
DIC
‘ULA
IlS
ER
VIC
S.“
iWC
EM
AK
ER
PRO
3485
Rem
ove
AJ.
C.D
.ge
nera
tor
and/
orle
ads
•QT
YFE
EU
pgra
deim
plan
ted
PMsy
stem
todu
alch
ambe
r
3324
425
00
3321
4‘
2000
N
Lud
omlr
skv
Bee
kman
2332
Dic
k.1
863
Ros
enth
al18
46In
sert
orre
plac
epe
rman
ent
pace
mak
erW
/—
Bla
ck33
63K
ulik
3488
Ser
wer
2579
tran
sver
ious
airi
alel
ectr
ode
3320
615
00C
harp
ieL
evy
2554
—V
erm
ilion
2966
tran
sven
ous
vent
ricu
lar
elec
trod
e33
207
...
1795
Cro
wle
y18
39Ll
oyd
3412
—W
echs
ler
0693
tran
sven
ous
AV
sequ
enti
alel
ectr
ode
3320
8‘tr
l,.
2285
oe
Ji
U4±
U
Cri
tical
care
,fir
stho
ur99
291-
300
Inse
rt/ r
epla
ceA
.l.C
.D.
lead
s33
247
2000
Pdm
aiy
care
Pro
’4de
rlS
pons
orIV
ISIT
Iea
chad
dl
half
hour
x$1
50=
9929
2A
ssis
top
erat
ive
A.I.
C.D
.pl
acem
ent
3324
515
00C
AH
DA
CC
AT
TE
AZ
11O
JSD
IAuN
OS1
h—
Ass
ist
oper
atIv
ePM
inse
rtio
n33
202—
1500
PRO
VID
ERO
FSE
RV
ICES
AN
DB
AR
EA-
Rig
htan
dLe
fthe
art,
tran
sept
al93
527
2000
Inse
rt/r
epla
ceel
ectr
ode,
sing
lech
ambe
r33
215
...;
-10
00A
DM
ITD
AT
E:
—R
ight
and
Left
hear
t,th
ruex
isti
ngop
enin
g93
529—
1750
dual
cham
ber
1712
00R
ight
and
Left
hear
t,re
trog
rade
9352
5.
1750
Rep
air
elec
trod
e,si
ngle
cham
ber
3321
880
0—
——
——
——
——
——
—Le
fthe
art,
via
cut
dow
n93
511
‘.
1250
dual
cham
ber
322
0‘‘‘
1000
,>
‘—
——
iS
Lef
thea
rt,p
ercu
tane
ous
9351
0—
850
Rer
nova
lofP
Mpu
lseg
ener
ator
33
33
‘.
.e
€R
ight
hear
t93
501
780
and
elec
trod
es,
sing
lele
adsy
stem
234
“90
0IN
JEC
TiO
NPR
OC
ED
UR
ES
DU
RIN
GC
ATH
INA
DD
ITIO
NTO
and
elec
trod
es,
dual
lead
syst
em23
511
00—
-—
-—
—C
AR
DIA
CC
AT
H/D
IAc3
NO
STIC
CH
EC
K8
QU
AN
TIF
YA
LLT
HA
TA
PPL
YIn
sert
orre
plac
ePM
gene
rato
r,si
ngle
cham
ber
3321.
850
)utp
atie
itt29
0—
--
——
—.
-‘r
inje
ctio
nfo
ft
——
rge
nera
tor
dual
cham
ber
321
950
Inpa
tient
297
——
——
——
Art
eria
lco
ndui
tan
giog
raph
y93
539
‘‘
250
Rev
isio
nI
relo
cate
PMsk
inpo
cket
322
2‘
850
Spec
ttyP
rov
tdr,
t3A
aid
OX
iDe
1ot
hsle
ciab
ove.
Sel
ecti
veco
rona
ryan
giog
raph
y9345
126
Inse
rtte
mpo
rary
sing
lech
ambe
rel
ectr
ode
321
700
Pul
mon
ary
angi
ogra
phy
9354
185
dual
cham
ber
elec
trod
es3
211
•-‘.
:-80
0D
ate
ofS
eMce
:‘h
otai
chat
g.e:
Rig
htA
orV
angi
ogra
phy
9354
2T
’85
.,
.‘
-O
ThE
RIN
VASI
YEF.
RO
cED
U.H
EI
Left
Aor
Van
giog
raph
y93
543—
75M
yoca
rdia
lbi
opsy
(bill
w/c
ath)
i90
0D
fAil
4O
3CO
DES
IA
orto
grap
hy93
544
75P
erlc
ardi
ocen
tesi
siL1-
400
PRiM
AR
YD
X‘I
cos-
cuC
OD
EIN
TR
AC
AR
DIA
CE
LE
CT
RO
PHY
SIO
LO
GY
Bal
loon
Cat
hfo
rM
onito
ring
(Sw
anG
anz)
J93
50
J65
0IN
AD
DIT
ION
TOC
AR
DIA
CC
AT
HC
ardi
acO
utpu
t-
TDCO
(do
notc
hgw
hen
cath
perio
rmed
)[9
35J
250
CH
EC
KA
ND
QU
AN
TIFY
ALL
THA
TA
PPL
Y—
OT
HE
RP
RO
CE
DU
RE
S‘-*
sco
no
ayri
xr
R.c
o,di
n2—
lntr
aope
rati
vepu
imve
ssel
slan
tpl
acem
ent
9952
1000
ILV
and/
orLA
map
ping
ofta
chyc
ardi
a93
609
*55
0C
PR
(sen
dla
bn
ote
sw
/this
form
)92
95.
395
Eso
phag
eal
reco
rdin
g93
615
250
Intu
batio
nE
ndot
rach
eal
3150
255
REL
EASE
OF
INFO
RU
AT1
O$
1A
SSIG
NU
ENT
OF
BEN
EFIT
$w
ithpa
cing
9361
688
0E
lect
rica
lca
rdio
vers
ion
9296
365
Iher
eby
auth
oriz
eth
eR
egen
tsof
the
Uni
vers
ityof
Mic
higa
n,Pe
diat
ric
Bun
dle
ofH
is93
600
--
.31
5V
enou
sC
utdo
wn
3642
110
Ass
ocia
tes
tore
leas
ean
yM
EDIC
AL
Inlo
mia
tion
whi
chm
ight
bene
eded
innt
ra-a
tria
l93
602
250
rans
fusi
onof
bloo
d,bl
ood
prod
ucts
3643
0180
conn
ectio
nw
ithpa
ymen
tfo
rmed
ical
seM
ces
rend
ered
.R
ight
vent
ricu
lar
9360
325
0A
rter
ial
Pun
ctur
e36
600
““
60Ir
eque
stth
atpa
ymen
tund
erm
ym
edic
alin
sura
nce
prog
ram
bem
ade
Left
vent
ricu
lar
9360
725
0R
outin
eV
anip
unct
ure
for
Col
lect
ion
ofS
peci
men
364
5.,..
30di
rect
lyto
the
Reg
ents
ofU
ofM
.Pe
diat
ric
Ass
ocia
tes
onan
ybi
llsfo
r..
..•.
Pacln
g.
-:B
ailo
onp
roced
s:(l
nd
ud
ea
cath
)C
PT
FE
Ese
rvic
esfu
rnis
hed
tom
eby
phic
ians
ofth
eD
epaf
lmen
tof
Pedi
atric
s.II
Com
plet
eE
Pst
udy
[i.e
.,93
618
+93
619]
[9362
0—
2700
Atri
alse
ptos
tom
y33
738
‘‘‘
30
00
my
insu
ranc
epro
gra
mre
jects
paym
ent
due
tota
ckof
prop
erauth
onzali
on
with
LAre
cord
in9t
621
—30
00P
ulm
onar
yva
lvul
opla
sly
3347
1—
-25
00fo
r serv
ices.
Iund
erst
and
that
Iwill
bere
spon
sibl
efo
rpa
ymen
t.w
ithLV
reco
rdin
g93
622
3000
Aor
licva
lvul
opla
sty
3399
025
00oa
t.:S
lt.i
..ol
in.u
..C
ompl
ete
EP
stud
yw
/oin
duct
ion
ofar
rhyt
hmia
1936
19—
2000
Bal
loon
proc
adur
es(I
nad
diti
onto
oath
),j
—C
ompl
ete
EP
eval
A.l.
C.D
.w
/ind
uct.a
rrhy
thm
ia19
3642
‘-
1600
Mitr
alva
lvul
opla
sty
3399
125
00nt
raca
rdia
cab
latio
nof
AV
node
func
tlor
9365
0—
1500
Aor
ticco
arct
angi
opla
sty
3399
2—
2500
HO
SPIT
AL
BIL
UN
G-.
ntra
card
iac
abla
tion
for
SV
T93
651
—20
00P
ulm
onar
yar
teri
opla
sty
3399
325
00Tr
eatm
entR
oom
Tim
eX
XX
XTr
eatm
ent
Room
Tim
eX
XX
Xnt
raca
rdia
cab
latio
nfo
rV
-tac
h93
652—
2000
Pul
mon
ary
vess
elst
ent
plac
emen
t99
528
1000
less
than
one
hour
grea
ter
than
one
hour
nduc
tion
ofar
rhyt
hmia
9361
8..
1200
Trn
sven
ous
devi
cep.:
Act
ivat
edC
oag
Tim
eX
XX
XP
ulse
OxcnuoX
ntra
.ope
rati
vepa
cing
&m
appi
ngj9
3631
1000
ASD
occl
usio
n33
994
P--
2500
Dev
ice
Cha
rge:
(spe
cify
devi
ce. f
ee
and
lee
code
)F
..co
d.
OIW
dSy
F..
EP
SF/
Uw
lpac
lng
&re
cord
ing
880
VSD
occl
usio
n33
995
‘25
00nt
ra-a
tria
lpa
cing
9361
0.
630
PDA
occl
usio
n-
WI c
oil
-(b
illca
thal
so)
3383
0--
--“f
-18
00Ti
ltT
able
Stu
dy93
660
400
Cat
hete
riza
tion
:nt
ra-v
entn
eula
rpa
cing
9361
226
5Su
bcfa
vian
,Ju
gula
ror
Oth
er,
2yr
sor
Und
er36
480
250
——
Add
’tco
de(o
rpr
ogra
mm
edst
imul
atio
nan
dpa
cing
afte
r St
9362
3—
250
Sub
clav
ian,
Jugu
lar
orO
ther
,O
ver
2yr
s38
489
-25
0E
Pev
alua
tion
ofA
.l.C
.D.
lead
sat
Impl
anta
tion
9364
0--
-•10
00U
mbi
lical
Art
ery
3666
0--
295
——
with
test
ing
ofpu
lse
gene
rato
r93
641—
600
Um
bilic
alV
ein
36
5’0
--
190
Intro
,ne
edle
orIn
trac
ath.
3600
0—
135
Pla
cepe
riph
eral
vein
intr
acat
hor
need
le‘
3600
013
5.
——
—

-
4Ppendi F
Source Code for Demonstr Progr
C
C.
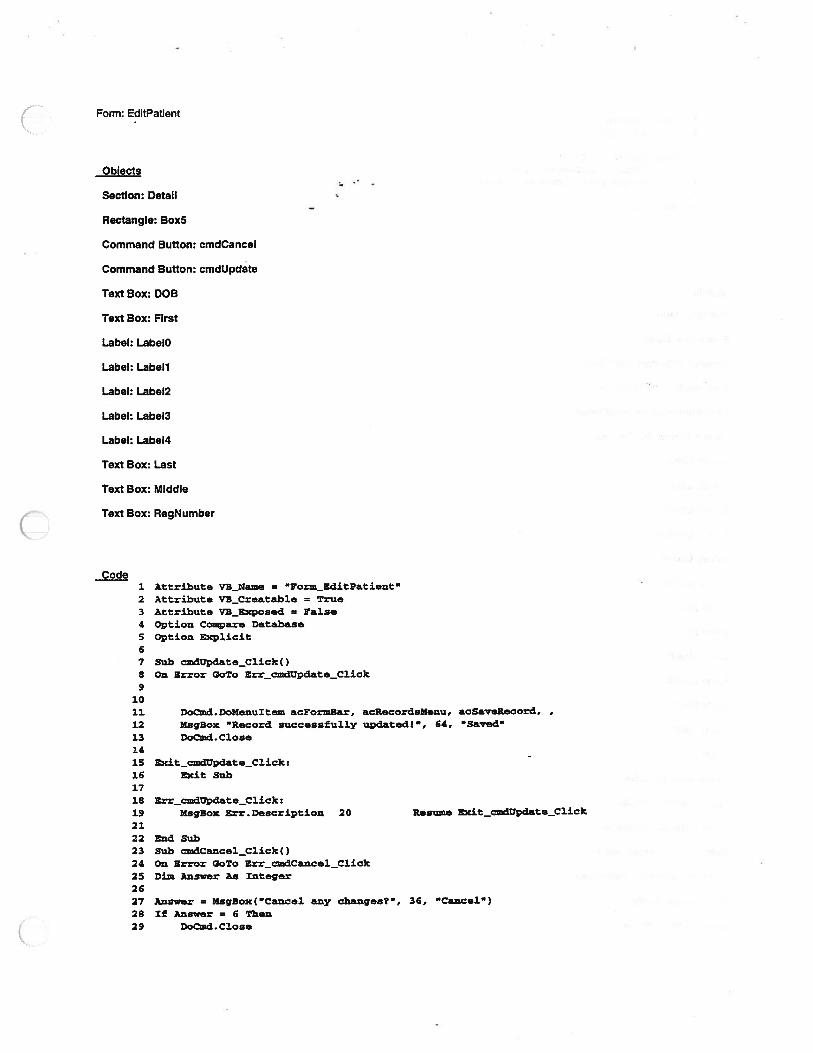
Form: EditPatient
Oblects
Section: Detail
Rectangle: Box5
Command Button: cmdCancel
Command Button: cmdupdate
Text Box: DOB
Text Box: First
Label: LabeIO
Label: Labell
Label: Label2
Label: Label3
Label: Label4
Text Box: Last
Text Box: Middle
Text Box: RegNumber
Code1 Attribute VB_Name = “Form_EitPatient”2 Attribute VE_Creatable = True3 Attribute V3_Exposecl = False4 Option Compare Database
5 Option Explicit
6
7 Sub cmdupdate_Click()8 On Error GoTo Err_cmdupdate_Click9
1011 Dod.DoNenuItem acFoziBar, acflecordsMenu, acSaeRecord,
12 MsgBox “Record successfully updatedi”, 64, “Saved
13 Dod.C1ose1415 Zxit_cmdUpdate_Click:16 Exit Sub1718 Err.dUpdate_C1ick:19 MsgBox Err.Description 20 Resie Exit_cmdUpdate_Click
2122 End Sub23 Sub cmdCancel_Click()24 On Error GoTo Err_cmdCancel_Click25 Di Answer As Integer2627 Answer = MsgBox(”Cancel any changes?”, 36, “Cancel”)28 If Answer = 6 Then29 DocmdC1ose

30 End I3132 Exit_dCane1_C1ick:33 Exit Sub3435 Err_Cance1_C1ick:36 MsgBox Err.Deseription37 Resume Exit cxndCa.ncel C1ik.3839 End Sub
Form: EKG
Objects
Section: Detail
Rectangle: Box32
Command Button: cmdClose
Command Button: cmdreport
Command Button: cmdReview
Option Group: frmOptions
Label: Labell
Label: Labelil
Label: Labell3
Label: Label2S
Label: Label27
Label: lblTotal
Line: LinelO
Line: Lrne36
Line: Line37
Line: Line3B
Line: Line4
Line: LineS
Line: Line9
Label: Month:_Label
Option Button: optAll
Option Button: optSome
SubformlSubreport: subAll
Subform/Subreport: subSelect
Combo Box: txtMonth ;.- .......J
Combo Box: txtYear,.,. ...... j...

Label: Year_Label
Form: EKGCode
1 Attribute ‘lB_Name = “Form_ERG”2 Attribute VB_Creatahle = True3 Attribute VB_Exposed = False4 Option Compare Database
S Option Explicit6789
10 Private Sub omdClose_Click()11 DoCmd.Clese12 End Sub13141516 Private Sub cmdrepozt_Click()
17 DoCmd.OpenFoxm “Lab Reporting”
18 Forms! [Lab Reporting] ! [ReportRequestedl .Caption = Me.Captiou
19 End Sub2021 Private Sub Form_Load 022 ‘ Initialize variables
23 t,xtMonth = Val(Format(Now, “mm”))24 txtYear = Val(Format(Now, “yyyy”))
25 lblTotal.Width = 2500
26 lblTotal.Caption = “Total 4 of Records for “ & txtMonth a “I” &
27 End Sub2829 Private Sub fmnOptions_Click()
30 If fzmOptions.Value = I. Then ‘ All records
31 subAll.Visible = True
32 subSelect.Visible = False
33 txtNonth.Enabled = False
34 txtyear.Enabled = False
35 lblTotal.Caption = “Total * of Records”
36 lblTotal.Width = 150037 End If3839 If !rmDptions.Value = 2 Then ‘ Selected month
40 subAll.Visible = False
41 subSelect.Visible = True42 txtMonth.Enabled = True
43 txtyear.Enabled = True44 lblTotal.Caption = “Total * of Records for “ a txtMonth a “/‘
a txtYear
45 lblTotal.Width = 2500
46 End If47 End Sub484950515253 Private Sub txtxonth_Change ()54 lblTotal.Caption = “Total * of Records for “ & txtMonth & “I” &
55 End Sub
5758 Private Sub txtYear_Change 059 lblTotal.Caption = “Total * of Records for “ a txtMonth a “I” a60 End Sub6162

63 Sub cmdReview_Click()64 On Error Goro Err_dReview_Click6566 Dim stDocName As String67 Dim stLinkCriteria As String “-- -
6869 stDocNasie = “Patient Into
70 Dod. OpenFozm stDocName, ,, stL.inJCriteria7172 ExitcmdReview_C1ic):73 Exit Sub7475 Err_cmdRview_C1ick:76 MsgBox Err.Description77 Resume Exit_cmdReview_Click
7879 End Sub
-
.;7-.--
(

Form: Lab Reporting
Oblects
Section: Detail
Rectangle: Box7
Check Box: Check3O
Check Box: Check32
Command Button: cmdCtose
Command Button: cmdPreview
Option Group: frmPrint
Option Group: frmsort
Label: LabelO
Label: Labell2
Label: LabeIl7
Label: LabeIl9
Label: Label2l
Label: Label25
Label: LabeI28
Label: LabeI3
Label: Label3l
Label: LabeI33
Label: LabeI6
Option Button: Optionl6
Option Button: Option 18
Option Button: Option2O
Label: ReportRequested
Text Box: txtFromDate
Text Box: txtSOL
Text Box: txtToDate
Form: Lab Reporting1 Attribute VB_Nane = “Yomjab Reporting
2 Attribute VBCreatable = true
3 Attribute VBExpesed = Ealse
4 Option Compare Database
5 Option Explicit
67 Private Sub cmdClose_Click()
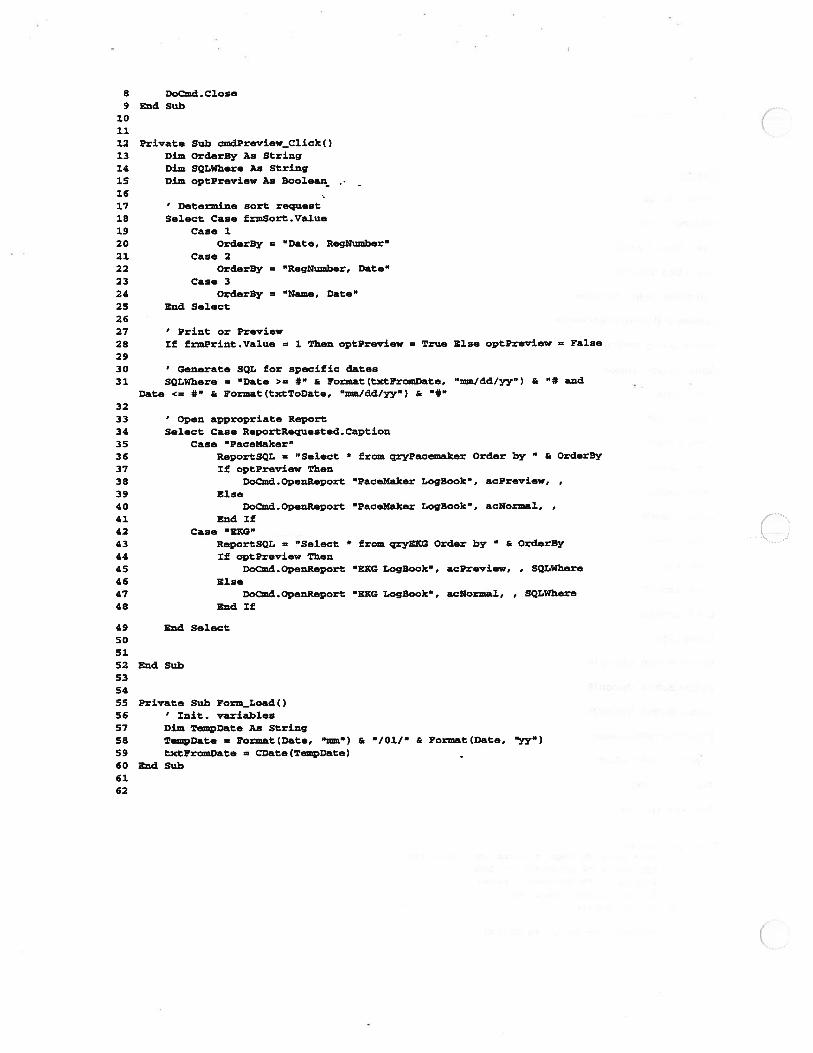
8 Dond.C1ose9 End Sub
101112 Private Sub cmdPreview_Click()
13 Dim OrderBy As String
14 Dim SQLWhere As String
15 Dim optpreviaw As Boolean
1617 ‘ Determine sort request18 Select Case frmSort.Value19 Casel
20 OrderBy = “Date, RegNumber”21 Case 222 OrderBy = ‘RegNumber, Date”
23 Case 3
24 OrderBy = “Name, Date”
25 End Select
26
27 ‘ Print or Preview28 If frmprint.Value = 1 Then optPreview = True Else optPreview = False
2930 ‘ Generate SQL for specific dates31 SQLWhere = “Date > #“ & Fornat(tzctpromDate, “tmu/dd/yy”) a * and
Date <= #“ a Format(txtToDate, “rma/dd/yy”) a “*“
3233 ‘ Open appropriate Report
34 Select Case ReportRequested.Caption
35 Case ‘PaceMaker”
36 ReportSQL = “Select * from qrypacemaker Order by a OrderBy
37 If optpreview Then
38 Docmd.OpeuReport “PaceMaker LogBook’, acPreview,
39 Else40 Dond.OpenRepert “PaceMaker LegBook’, acNormal,41 Endlf42 Case ‘EKG”43 ReportSQL = “Select * from qryEKG Order by a OrderBy
44 If optPreview Then
45 Docmd.OpenReport “EKG LogBook”, acPreview, , SQLWhere
46 Else47 Docmd. OpenReport “ERG LogBook”, acNormal, , SQLWhere
48 End If
49 End Select50
51
52 End Sub535455 Private Sub Form Load()56 ‘ Init. variables57 Dim TempDate As String58 TempDate = Pormat(Date, “om”) & “/01/” & Format(Date, “yy”)
59 txtFromDate = CDate(TempDate)
60 End Sub6162

Form: MainMenu
Objects
Section: Detail
Rectangle: Boxi
Rectangle: Box3
Command Button: cmdCath
Command Button: cmdEkg
Command Button: cmdExercise
Command Button: cmdPaceMaker
Command Button: cmdPatients
Command Button: cmdquit
Command Button: Command8
Label: LabelO
Label: Label2
Label: Label4
Image: OLEUnboundl2
Code1 Attribute VBName = “Foxm_MainNenu”2 Attribute VB_Creatabi.e = True3 Attribute yB_Exposed = False4 (ption Compare Database
5 Option Explicit67 Private Sub cmdcath_Click()8 MsgBox “tab book not yet implemented”, 16, “Under construction”
9 End Sub101112 Sub cmdEkg_Click()13 On Error Gopo Err_cmdEkg_Click1415 Dim stflocName As String16 Dim stt,inkCriteria As String1718 stDocName = “ERG”
19 Docmd OpenFom stDocName, , , stt.inkCriteria
2021 Exit_cmdBkg_Click:22 Exit Sub2324 Err_cxxzdEkg_Click:25 MsgBox Err.Description26 Resume Exit_cmdEkg_Click27

28 End Sub2930 Private Sub cmdxercise_C1ick()31 MsgBox Lab Book not yet implemented”, 16, “Under construction”32 End Sub3334 Private Sub cmdPaceMakerclick()35 Dod.OpenYorm “Pacemaker”36 End Sub3738 Private Sub cmdpatients_Cljck()39 Docmd.Openporm “Patient tne”40 End Sub4142 Sub dquit_C1ick()43 On Error GoTe Err_cmdquit_Cljck444546 Dod.Quit4748 Exit_cmdguit_Click:49 Exit Sub5051 Err_cmdquit_Click:52 EsgEox Err.Description53 Resume Exit_cmdquit_Click5455 End Sub5657 Private Sub Conimand8_Click()58 Dod.OpenForm “Patient Reporting”
59 End Sub6061
C
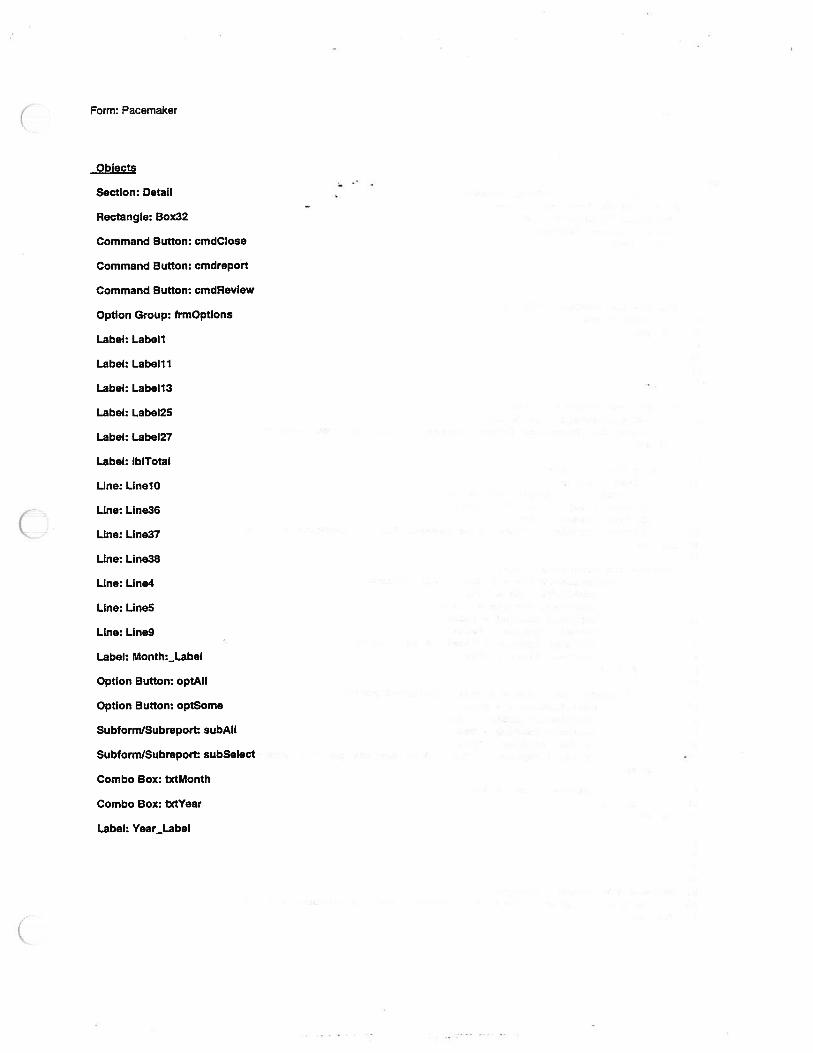
Form: Pacemaker
Objects
Section: Detail
Rectangle: Box32
Command Button: cmdClose
Command Button: cmdreport
Command Button: cmdReview
Option Group: frmOptions
Label: Labell
Label: Labell 1
Label: Labell3
Label: Label25
Label: Label27
Label: IbITotal
Line: LinelO
Line: Line36
Line: Line37
Line: Line38
Line: Line4
Line: Line5
Line: Line9
Label: Month:_Label
Option Button: optAll
Option Button: optSome
Subtorm/Subreport: subAll
Subform/Subreport: subSelect
Combo Box: txtMonth
Combo Box: txtYear
Label: Year_Label

Form: Pacemaker
Code -
1 Attribute yB_Name = “Form Pacemaker”
2 Attribute VBCreatable = True
3 Attribute VBExposed = False
4 Option Compare Database
5 Option cplicit6789
10 Private Sub cmdClose_Click()11 Dod.C1ose12 End Sub131415161718 Private Sub cmdxeport_Click()
19 Dod . OpenForm “Lab Reporting”
20 Forms (Lab Reporting I (RoportRequested] .Caption = Me.Caption
21 End Sub2223 Private Sub Form Load()24 ‘ mit. variables25 tmctMoath = Val(Pormat(Now, “un’))26 tmctYear = Val(Format(Now, “yyyy”))
27 lblTotal,Width = 250028 lblTotal.Caption = “Total * of Records for “ & txtMonth & “I” &
29 End Sub3031 Private Sub frnptions_C1ick()
32 If fxmOptions.Vaiue = 1 Then ‘ All Records
33 subAll.Visible = True
34 subSelect.Visible = False
35 txtMonth.Enabled = False
36 txtYear.Enabled = False
37 lblTotal.Caption = “Total * of Records”
38 lblTotal.Width = 1500
39 End If4041 If frxnOptions.Value = 2 Then ‘ Selected records
42 subAll.Visible = False
43 subSelect.Visible = True
44 txtNoath.Enabl.d = True
45 txtYear Enabled = True
46 lblTotaj..Caption = “Total * of Records for & txtMonth & “I”
& txtYear
47 lblTotal.Width = 2500
48 End If49 End Sub505152535455 Private Sub txtMonth_Change()56 lblTotal.Caption = “Total * of Records for “ & txtMonth & “F” &
57 End Sub58

5960 Private Sith txtYear_Chaqe 061 lblTetal.Caption = “‘ota1 # of Records for & txtMenth & /“ &
62 Ed Su
636465 Sith Review_C1ick()66 On Error GoTo Err_cmdRaview_C.ick6768 Dim stDocNae As String
69 Dim stLinkCriteria As String7071. stDocName = ‘Patient Info72 Dod . OpenFoxm stDocName, , , str4nkcriteria
7374 Exit_cmdReviewClick:75 Exit Sub
7677 Err_cmdReview_Click:78 MsgBox Err.Description79 Resume Exit_cmdReview_Click8081 End Sub

Form: Patient Info
Obiects
Section: Detail
Command Button: cmdClose
Label: Labell 1
Label: Label13
Label: Label2
Label: LabelB3
Line: LinelO
Line: Line6
Line: Line7
Line: Lineg
SubformlSubreport: Patient Data
Code1 Attribute VENaixze = Form_Patient Info’ - -
2 Attribute VE_Creatable = True
3 Attribute yB_Exposed = False4 Option Conpare Database5 Option Explicit67S Sub czndClose_Click()9 On Srror GoTo Err_ndC1ose_C1ick
101112 Docxnd.Clese1314 Exit_cmdClose_Click:15 Exit Sub1617 Err_cmdClose_Click:18 MsgBox Err.Description19 Resume Exit_zidC1ose_C1ick2021 End Sub
C
Form: Patient Reporting
Objects
Section: Detail
Rectangle: Box46
Rectangle: Box7
Check Box: Check3O
Check Box: Check32
Check Box: chkAll
Combo Box: cmbPatients
Command Button: cmdClose
Command Button: cmdPreview
Option Group: frmPrint
Label: LabelO
Label: Label28
Label: Label3
Label: Label3l
Label: Label33
Label: Label47
Label: Label48
Label: LabelSO
Label: Label6
Text Box: txtFromDate
Text Box: txtTo Date
Code1 Attribute VS_Name = ‘Pom_?atient Reporting’
2 Attribute VE_Creatable = True3 Attribute VS_Exposed = False4 Option Compare Database5 Option Explicit6
7 Private Sub chkA1l_AterOpdate()89 te chkAll.Value = True Then ‘ Disable date boxes
10 txtFromDate.Enabled = False
11 txtToDate.Eziabled = False12 Else ‘ Enable date boxes
13 txtFromDate .Enabled = True
14 txtToDate .Enabled True

15 End If16 End Sub1718 Private Sub cmbPatients_Change()19 cmdPreview.Enabled = True20 End Sub2122 Private Sub cmdCloseclick()23 Docznd.Close24 End Sub -
252627 Private Sub cmdPreview_Click()28 Dim SQLWhere As String2930 ‘ Generate SQL to select patient on form31 SQLWhere = “RegNumber = ‘“ & Format(cmbPatieats.Value) &3233 PatientWhere = “Date >= 4” & Format(tzctPromDate, “/dd/yy’) & “4 and
Date <= #“ & Format(txtToDate, “/dd/yy”) & “*“
3435 If frmPrint.Value = 1. Then36 Docmd.Openfleport ‘Patient Report”, acPreview, , SQLt’there37 Else38 Docmd. OpenReport “Patient Report’, acNormal, , SQLWhere ‘ Print39 End If40 End Sub414243 Private Sub Cozximand5lClick()44 Patientwhere = ‘Date >= 4” a Format (txtFromDate, “xzEm/dd/yy”) a “4 and
Date <= 4” a Format(txtToDate, “u/dd/yy”) a “*‘
45 End Sub4647 Private Sub Forin_Lead()48 ‘ mit. variables49 Dim Tempflate As String50 TempDate = Format(Date, “imn”) a “/01/” a Format(Date, “yy”)51 txtYromDate = CDate(TempDate)52 End Sub5354

Form: subEKG
Objects
Section: Detail
Text Box: Comments
Text Box: Date
Label: LabelO
Label: LabellO
Label: Labelli
Label: Labeil2
Label: Label4
Text Box: month
Combo Box: RegNumber
Label: RegNumber:_Label
Text Box: Technician
Text Box: Year
Code1 Attribute VS_Name = “Fom_siibERG”2 Attribute VB_Creatable = True
3 Attribute VS_Exposed = False4 Option Compare Database5 Option Explicit678 Private Sub Form_Error(DataErr As Integer, Response AS Integer)
9 ‘ Dispaly error if patient does not exist in patient table
10 If DataErr = 3201 Then
11 MsgBox “Xnvalid registration number. Patient does not exist!” &
Chr(13) & “(Hit ESC to abort record), 48, Error
12 Response = acDataErzContinue13 End If1415 End Sub1617181920 Private Sub RegNumber_DblClick(Cancel As Integer)
21 ‘ Open patient edit screen22 On Error GoTo 123 Dim SQLWhere As String2425 CuxRegnum = RegNumber26 SQLWhere = “Regnumber = ‘ & CurRegnum &
2728 DoQud.OpenPorm “EditPatient”, , , SQLWhere, , acDialog

2930 3. Exit Sub31 End Sub3233

Form: subPacemaker
Section: Detail
Text Box: Comments
Text Box: Date
Combo Box: Dual
Label: LabelO
Label: LabellO
Label: Labelil
Label: Label2
Label: Label3
Label: LabeI4
Text Box: month
Combo Box: RegNumber
Label: RegNumber:_Label
Combo Box: Single
Text Box: Year
Code1 Attribute VBName = “Form_subpacemaker2 Attribute VB_Creatable = True3 Attribute yB_Exposed = False4 Option Compare Database5 Option Explicit6 Dim SingleValue As Boolean7 Dim DualValue As Boolean89 Pri-ate Sub Dual_BeforeUpdate(Cancel As Integer)
10 If Me.Dual.Text = AYes” Then11 DualValue = True12 Else13 DualValue = False14 End If15 End Sub1617
1819 Private Sub Form_Error(DataErr As Integer, Response As Integer)
20 ‘ Display error if patient does not exist in patient table
21 If DataErr = 3201 Then22 MsgBox “Invalid registration number. Patient does not e.xist!” &
Chr(13) & “(Hit ESC to abort record)”, 48, “Error23 Response = acDataErrcontinue24 End If2526 End Sub
Private Sub Single_LostFocus()If Me.Single.Text = “Yes’ Then
SingleValue = TrueElse
SingleValue = FalseEnd If
End Sub
Private Sub R.gNutnber_DblClick(Cancel As Integer)Display petient edit form
On Error GoTo 1Dim SQLWhere As String
CurRegnum = RegNumberSQLWhere = “Regnunber = ‘ & CtrRegnum &
DoOnd.OpenForm “EditPatient”, , , SQLWhere, , aeDialog
1 Exit Sub
End Sub
272829303132333435363738394041424344
454647
484950515253
(
Form: subPatient
Objects
Section: Detail
Text Box: DOB
Text Box: First
Label: LabelO
Label: Labell
Label: Label2
Label: Label3
Label: Label4
Text Box: Last
Text Box: Middle
Text Box: RegNumber
Code1 Attribute yE same = “Form subPatient”
2 Attribute VB_Creatable = True3 Attribute VB_Exposed = False4 Option Compare Database5 Optioa Explicit
67 Private Sub Yorm_BeforeDelConfirm(Cancei As Integer, Response As Integer)
8 Response = acDataErrCoatinue9 End Sub
1011 Private Sub Fozm_Delete(Cancel As Integer)
12 ‘ Confirm deletion13 Dim Answer As Integer14 Answer = MsgBox(”Axe you sure you want to delete patient?’ & Chr(l3)
& “(All records relating to patient will be deleted!)”, 36, “Delete
15 If Answer = vbNe Then16 Cancel = True
17 End If
18 End Sub1920212223
24 Private Sub RagNumber_DblClick(Cancel As Integer)25 DocDmd.Openyorm “Patient Reporting”
26 Forms! [Patient Reporting] 1 [cmbpatiants] .SetFocus27 Formst[Patient Reporting]!fcmbPatientsl.Text = RegNumber & &
Trim(Last) & “, a Trim(First) & “ “ & Middle
28 Forms! [Patient Reporting] I [cmdPreview] 5etFocus29 End Sub3031

Form; TitieScreen
Objects
Section: Detail
Rectangle: Box7
Rectangle: Box8
Label: Label2
Label: Label3
Label: Label4
Label: Label5
Label: Label6
Image: OLEUnboundi
Code1 Attributa VBName = ‘Form_TitleScreen’2 Attribute VE_Creatable = True
3 Attribute yB_Exposed = False4 Option Compare Database5 Option ExplicitS7 Private Sub Form Click()8 Dotmd.Close9 DoCmd . OpenForm “MainZ4enu
10 End Sub111213 Private Sub Form_Timer 014 ‘ After timer is over close title screen and open main menu15 Docmd.Close16 Docmd.OpenForm ‘MainMenu17 End Sub1819