oct applications in optometry · oct applications in optometry chuck aldridge, o.d. ... fdt, swap ,...
TRANSCRIPT

5/18/16
1
OCTApplicationsinOptometry
ChuckAldridge,O.D.,M.B.A.
FellowAmericanAcademyofOptometry
MemberofOptometricGlaucomaSociety
AldridgeEyeInstitute
Burnsville,NC
• The content of this course was prepared independently by myself without commercial influence from members of the ophthalmic industry.
• I am on the Speaker Bureau’s of Allergan, Alcon and Optovue. I am a clinical investigator for Bausch & Lomb and CIBA. I am on Clinical Advisory Board for TearLab. However, I have no direct financial or proprietary interest in any company, product or service mentioned in this presentation.
• I have not received commercial support in any form (honorarium, etc.)
for this presentation. • The content and format of this course will be presented without
commercial bias and will not claim superiority of any commercial product or service.
COMMERCIAL DISCLOSURE Mandatory Slide
OCTGettherightonefortherightreason! WhichOCT?
• TimeDomain
• Fourier(Spectral)Domain
TimeDomainvs.Spectral“CirrusOCThasbetterscanqualitythanStratusOCT,
especiallyinglaucomatouseyes.Incaseswithgood-
qualityscans,thesensitivityandspecificity,andAUCs
weresimilar.Thebestagreementwasintheglobal
averageRNFLclassification.Thewidthsoflimitsof
agreementsexceedthelimitsofresolutionoftheOCTs.”
JavierMoreno-Montañés,NataliaOlma,etal.CirrusHigh-DefinitionOpticalCoherenceTomographyComparedwithStratusOpticalCoherenceTomographyinGlaucomaDiagnosis.IOVS;Jan2010,Vol51,no.1,335-343
FOURIERDOMAINOCTADVANTAGE
• FDOCThastwicethedepthresolutionasTDOCT(5microns
vs10microns)
• Allowsimagingandsegmentationofganglioncelllayers
• Fasterspeedalsoallowsforgreaterdensityofsampling
pointsandreducesartifactsfromeye-movements(FDOCT
has26,000Ascans/secvsStratusTDOCTwith400Ascans/
sec)

5/18/16
2
EvaluationoftheCorneaandAnteriorChamber
PachymetryMapsKeratoconus Analysis Thickness Parameters
B-Scans
Thickness Map color coded
6 mm diameter average thickness values by region Central circle 0-2mm Middle circle 2-5 mm Outer circle 5-6 mm
Power Calculations
Keratoconus
IMAGINGANDMEASUREMENTOFTHECORNEA
AngleCalculationsMEASUREDOCCLUDABLEANGLE

5/18/16
3
Pre-CataractNarrowAngle
Post-CataractOpenAngle
OCTandGlaucoma
HowDoTheyCompare?
FDT,SWAP,flickerperimetry,andOCTareall
usefulmethodsfordiscriminatingbetweenhealthy
eyesandeyeswithearlyglaucoma.Amongall10
OCTparameters,NFLThasthehighestsensitivity
fordetectingearlyglaucomatouschangesinGS
patients.Nomoto,Hiroki;Matsumoto,Chota;Takada,Sonoko;Hashimoto,Shigeki;Arimura,Eiko;Okuyama,Sachiko;
Shimomura,Yoshikaz.DetectabilityofGlaucomatousChangesUsingSAP,FDT,FlickerPerimetryandOCT.Journalof
Glaucoma.18(2):165-71,Feb2009.
OVERLAYOFTHERNFLANDGCC(OS)WITHFDOCT
pRNFL
GCC
DENDRITICSHRINKAGE
Normal Ganglion cells (Primate) Glaucoma model Ganglion cells (Primate)
• The first structural change from glaucoma was a shrinkage of the ganglion cell dendritic fields
GANGLIONCELLLOSSINTHEMACULA
• Histologicstudieshaveshownganglioncelllossinthe
macula
• Desatniketal.(1996)foundmacularganglioncellsare
lostinearlyglaucoma
• Yuceletal.(2003)showedlossofcellsinthe
parvocellularlayersoftheLGNimplicatingcentral
ganglioncellloss
Desatnik H, Quigley HA, Glovisnky Y. J Glaucoma 1996; 5: 46-53. Yucel YH, Zhang Q, Weinreb RN, Kaufman PL, Gupta N. Prog Retin Eye Res 2003; 22:465-481

5/18/16
4
TDOCTSTUDYLIMITATIONS
• MajordisadvantageinthesestudiesisthatTD
OCTtypicallymeasuresfullretinalthickness
only(doesnotisolateganglioncells)
• TDOCTdoesnothaveenoughdepth
resolutiontoimageandsegmenttheganglion
cellsaccuratelyandreliably
RETINALGANGLIONCELLSEXTENDTHROUGHTHREERETINALLAYERS
RNFL
Ganglion cell bodies
Ganglion cell axons
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer
Outer plexiform layer
Outer nuclear layer
IS / OS Junction
RPE Layer
Ganglion cell dendrites
Ganglion cell complex (GCC)
GCC is: • Nerve Fiber Layer – Ganglion cell axons • Ganglion cell layer – Cell bodies • Inner-Plexiform Layer - Dendrites
IMAGINGTHEGCCWITHTHEFDOCT
ILMNFLGCLIPLINLOPLONLPRIS/OSRPEChoriocapillarisandchoroid
BloodvesselGCC Full Retina Thickness
GCC is inner retinal layers • Nerve Fiber Layer – Ganglion cell axons • Ganglion cell layer – Cell bodies • Inner-Plexiform Layer - Dendrites
DIAGNOSTICACCURACY:GCCVSTDOCTFULLRETINATHICKNESSINMACULA
• Tanetal.(2009)foundtheGCC(FDOCT)was
significantlymoreaccuratefordetectingglaucoma
comparedtofoveathickness(fullmaculathickness)
withStratusTDOCT
• Morietal.(2010)alsoshowedGCCwassignificantly
moreaccuratethanfullmaculathicknesswithTDOCT
Tan O, Chopra V, Lu AT et al. Ophthalmology 2009; 116:2305-2314. Mori S, Hangai M, et al. 2010; J Glaucoma, in press.
DIAGNOSTICACCURACY:GCCVSMACULAVFSENSITIVITYINMACULA
• GCCTdeterminedbySD-OCT(RTVue-100)
showedastatisticallysignificantstructure-
functionassociationwithmacularVF,andthe
strengthoftheassociationwasgreaterthanthat
ofthempRNFLwithmacularVFinthesuperior
centralVFarea.
JungHwaNa,MichaelKook,etal.Structure-FunctionRelationshipoftheMacularVisualFieldSensitivityandthe
GanglionCellComplexThicknessinGlaucoma.IOVS.June14,2012.11-9401
DIAGNOSTICACCURACY:GCCVSFDOCTRNFL
• Raoetal.(2010)foundGCChadsimilaraccuracylevels
asRTVueFDRNFL
• Seongetal.(2010)foundsimilarresults
• Kimetal.(2010)foundAROCvalueswerehigherfor
RNFLvsGCCinagroupofadvancedglaucoma
patients,butGCCvalueswerehigherthanRNFLina
groupofearlyglaucomapatients
RaoHL,ZangwillLM,WeinrebRNetal.Ophthalmology2010;inpress.SeongM,SungKR,ChoiEH,etal.InvestOphthalmolVisSci2010;51:1446-1452.KimNR,LeeES,SungGJ,etal.InvestOphthalmolVisSci2010;inpress

5/18/16
5
FDOCT:GCCVSDISCVSRNFL
• Huangetal.(2010)comparedthediagnosticaccuracyfor
GCC,opticdisc,andRNFLfromtheRTVue
• AROCforRNFLwashighest(AROC=0.92),withGCCsecond
(AROC=0.86),andverticalC/Dratioaclosethird(AROC=
0.854)
• Theyfoundtheaccuracyimprovedwhenthey
combinedallthreestructuresinanLDF(AROC=0.97)
Huang JY, Pekmezci M, Mesiwala N, Kao A, Lin S. J of Glaucoma 2010 Epub ahead of print
GCCSUMMARY• GCCthicknesscorrelateswellwithvisualfields
• Highlyreproducible
• Morereproducibleandmoreaccuratefor
detectingglaucomathanmaculathickness
withTDOCT
• SimilaraccuracyfordetectingglaucomaasFD
OCTRNFLthickness
GCC:Arriveatthesceneofthecrimebeforethecrime
InadditiontoppRNFL
thickness,themGCC
thicknesscouldbea
structuralparameterfor
detectingpreperimetric
glaucoma
Takagi,SeijiT.MD*,†;Kita,YoshiyukiMD,PhD*,†;Yagi,FumihikoMD,PhD*,†;Tomita,Goji
MD,PhD*,†MacularRetinalGanglionCellComplexDamageintheApparentlyNormal
VisualFieldofGlaucomatousEyesWithHemifieldDefects
Takagi.JournalofGlaucoma.June/July2012.Vol21.Issue5.p318.325.
“ProofinthePudding”CaseStudies
CaseHistory(2005)• 57YOM
• Struggleswithdiabeticcontrol
• Hashadsomelasertxinprior2-3years
• CDalwayslarger;butsome?change
• Matrixscreeningfieldhasnewfinding
• IOPalwaysbeeninupperteens(17-19)
• InitiateglaucomaevaluationforNTG
• Sidenote:Approximately2009patientstartedCPAP
OpticNerveEvaluation(alsosomebackgrounddiabeticretinopathy)
Someexudates
ModerateCupping

5/18/16
6
MatrixScreeningFieldMarch2005
MatrixComprehensiveFieldMarch2005
Inferiordefects(superiorOCT?) Superiordefects(inferiorOCT?)
OS OD(ODworsethanOS)
OCTScanApril2005
OD–Inferiordamage(ConsistentwithSuperiorFieldDefect)
OS-SuperiorDamage(ConsistentwithInferiorFieldDefect)
ODworsethanOS(consistentw/VF)
RNFLProgressionEvaluation(OD)02/09-04/12
Stable
RNFLProgressionEvaluation(OS)02/09-04/12
Stable
GCCProgressionEvaluation(OD)02/09–04/12
Startingtodrop?(RepeatOCTsooner)

5/18/16
7
GCCProgressionEvaluation(OS)02/09-04/12
FairlyStable
7YearsLater(SDTOCT)April2012
Caveat
• RNFLchangesoccurearlierthanfieldchanges
• GCCchangesoccurearlierthanRNFL
• EarlyprogressivechangeinGCCisEARLY!
• RepeatOCTsoonertoverify
OCTandRetinalStuff
Patient Data • 74 yo wf
• C/O vision stress
• Non contributory history
• Baby aspirin + vitamins
• VA With Contact Lenses OD 20/30 OS 20/40
• CCT 510/516 IOP 14/15
• Long standing VM traction OS and ERM OU with a Hx of
refusing intervention
FundusPhotoswithMoreAtrophyODThanOS

5/18/16
8
StratusTimeDomainImages
NotBad….BUT
PVDERM
VMTraction
LOOKATSPECTRALDOMAIN!
Andtheproblemis….
• Examination12.14.11(29YOF)
– BCVA:OD:PL-0.50x082 20/20
OS:-0.25-1.00x097 20/20
- IOP:13,13
- EOM’s,CF,PupilsWNLOU
- C/D:OD.3/.3ROS.3/.3R
- PosteriorSegmentWNLOU
Andtheproblemis….
• 29y/ocaucasianfemale(6monthslater)
• Reports“blackspotincenterofvisioninbotheyesforoneweek”
• POH:unremarkable
• PMH:unremarkable
• SocialHistory:Cigarettes1pack/dayx10years
Andtheproblemis…• Examination6.12.2012
– BCVA:ODBCVA:OD:PL-0.50x082 20/40*
OS:-0.25-1.00x097 20/40*
*(VAw/eccentricviewing)
- IOP:15,15
- EOM’s,CFWNL.PupilsRoundReactive,OD>OSwithOD
reactionmoresluggishthanOS
- C/D:OD.3/.3ROS.3/.3R
- PosteriorSegment:
12.14.2011

5/18/16
9
6.12.2012
What’sGoingonHere? It’sHereToo!
DIAGNOSIS?
• SOLARMACULOPATHY
• PATIENTWATCHEDTHEECLIPSEFOR
ABOUT30MINUTES!
“RoutineExam”
• BVA20/20ODand20/25-OS(69YOF)
• PosteriorIOLOUwithclearcapsules
• BVA20/20OU1yrearprior
• PERRLA• Hypertensive,BP118/79
• Fundus–unremarkable
• Brotherhadamaculahole
• UnexplainedacuitydecreaseOS????

5/18/16
10
OSRetina MatrixScreeningVFVFatvisittoday VFdone1.5yearprior
Maculaintact?
WhatisThis?

5/18/16
11
NormalMacula?
Thinning
AlookwithCirrus
OSwithCirrus
Thereitis
AndThinning!
FAofOS
• FAshowsdelayedreturn
inferotemporal
• Enoughtimethatany
edemaandhemresolved
onBIO
• Nocentral“window
defect”relatedtomacula
hole
DIAGNOSIS?
• OldBRVOinOS
• OS-posteriorhyaloidfacepulledawayfrom
fovea.Demonstratesasmallremnantof
hyaloid.Mayhaveabitofretinashowingon
OCT(possiblywithsomeNFL),butNOhole
• NeedtomonitorODnow
BlurryVisionCase
Lefttheirpreviousdoctorbecause“blurry
vision”notgettingbetter
5/18/16
12
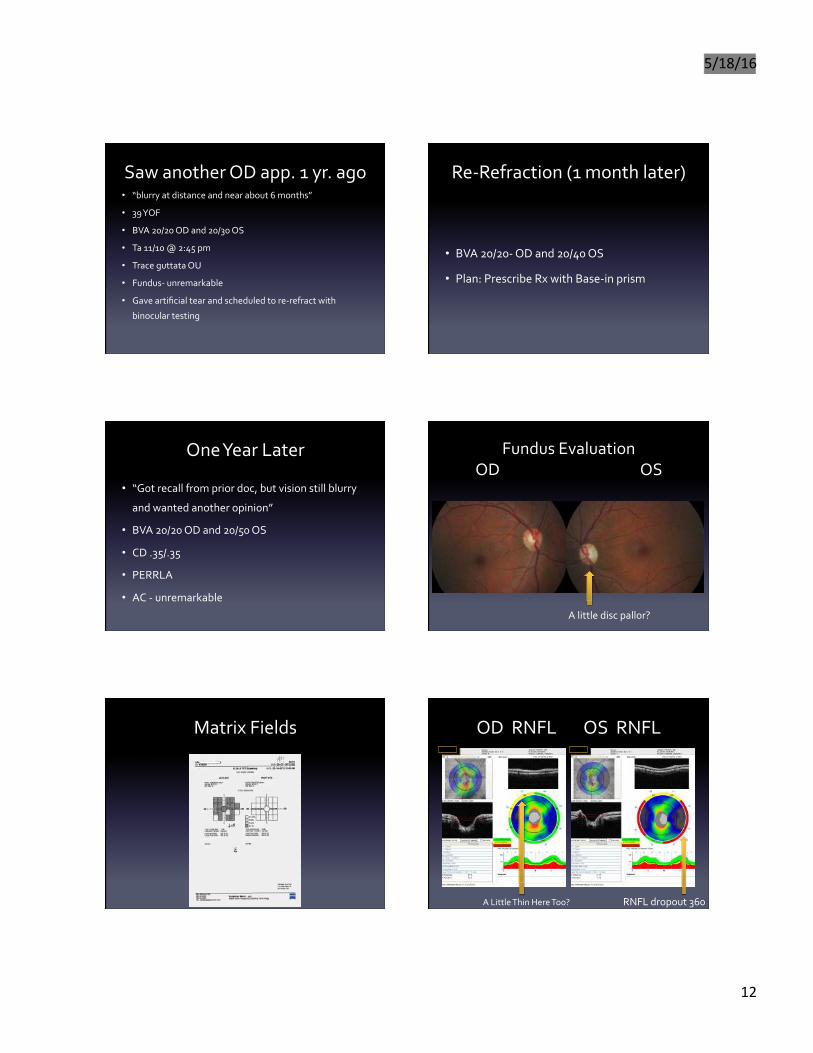
SawanotherODapp.1yr.ago• “blurryatdistanceandnearabout6months”
• 39YOF
• BVA20/20ODand20/30OS
• Ta11/10@2:45pm
• TraceguttataOU
• Fundus-unremarkable
• Gaveartificialtearandscheduledtore-refractwith
binoculartesting
Re-Refraction(1monthlater)
• BVA20/20-ODand20/40OS
• Plan:PrescribeRxwithBase-inprism
OneYearLater
• “Gotrecallfrompriordoc,butvisionstillblurry
andwantedanotheropinion”
• BVA20/20ODand20/50OS
• CD.35/.35
• PERRLA
• AC-unremarkable
FundusEvaluationODOS
Alittlediscpallor?
MatrixFields
NAME: Mcdowell, Angela
ID: 118039
LEFT EYE
PUPIL DIAMETER: 8mm VISUAL ACUITY: AX: W/o rx
30
N-30-5 FDT Screening
TEST SPEED: NORMAL
BOTH
DOB: 08-07-1973 [38]
DATE: 02-14-2012 10:43 AM
RIGHT EYE
PUPIL DIAMETER: 8mm VISUAL ACUITY: RX: W/o rx
TOTAL DEVIATION
30 30
D P>=5° /0
P<5%
1:1P<2%
P<1%
TEST DURAT ION : 1 :32 FIXAT ION TARGET: Central
TEST DURAT ION : 0 :36 F I XAT ION TARGET : Central
F IXATION ER RS : 0/3 (0 %) F IXAT ION E RRS : 0/3 (0 %)
FALSE POS ER RS : 0/3 (0 %) FALSE POS ERRS : 0/3 (0 %)
NOTES : NOTES :
30
Aldridge Eye Inst.
419 East Main St.
Burnsville, NC
SW: M02.03.01[01 S06.00.03[0] P06.00.03[0] TID: 18768.20050310154 (R1)
Humphrey Matrix with Welch Allyn Frequency Doubling Technology
ODRNFLOSRNFL
RNFLdropout360ALittleThinHereToo?

5/18/16
13
ODGCCOSGCC
Don’tLookGood
Whatdaheckisgoingon?
• NeuroReferral:MRIdone
• 2.1x1.6cmplanumsphenoidalemeningiomaw/
meningealinvolvementofinferiororbitalgyrus,
deformationofolfactorynerves,encasementof
ant.cerebralartery,A1/A2segments,ontheleft,
right,invasionofleftcavernoussinus,and
stenosisofleftopticcanal
SurgeryPerformed
• Compressionofleftopticnerveneeded
• BVA20/40ODandNLPOS
GrowYourContactLensPracticewithOCT
Mini-Scleralbecome“mainstream”• Scleraldesign–usefulfor“sickeyes”.Havealotofvault
(fluidlayer),reducedO2
• Mini-scleral-
1. SimilarsizeandcomforttosoftCL
2. Minimalfluidlayer,greatO2
3. Greatfordryeyepatients,toricandmultifocals
4. UseofOCT“takestheartrightoutofit”withrespectto
fitting
MINI-SCLERALCONTACTS
Usethemeasuretooltoaccuratelydeterminevault288microns

5/18/16
14
MINI-SCLERALCONTACTS
291microns
MINI-SCLERALCONTACTS
Edgeevaluation- Howdoesitland?- Clearlimbus?
MINI-SCLERALCONTACTS
THANKYOU!