occupational heath and safety in residential aged care
TRANSCRIPT

Occupational Health andSafety in Residential Aged CareFirst Steps
October 1999
Department of Health and Aged Care

2 OHS in Residential Aged Care First Steps
DisclaimerOHS in Residential Aged Care: First Steps (First Steps) has been developed to
provide information to assist small aged care facilities to develop their own
occupational health and safety program.
The material takes into account the special circumstances of aged care facilities and
must be considered with the relevant State OHS Legislation.
The Commonwealth of Australia and the authors disclaim all and any liability to
any person, whether a purchaser of this publication or not, in respect of anything
and of the consequences of anything done or omitted to be done by any person in
reliance, whether in whole or in part, upon the contents of First Steps.
Copyright
© 1999, Commonwealth of Australia
This work is copyright. Apart from use and reproduction by aged care facilities and
related agencies for the purpose of developing an occupational health and safety
program for an aged care facility (but not for the purpose of commercial gain) or
any other use as permitted under the Copyright Act 1968, no part may, in any form
or by any means be reproduced without prior written permission.
Development of First StepsOHS in Residential Aged Care: First Steps was produced by Marion Pocock
Consultancy, under contract to the South Australian WorkCover Corporation and the
Commonwealth Department of Health and Aged Care. Marion Pocock wishes to
acknowledge the input of Christine Aickin of Workability (Self-Assessment and 4.2),
Carla Baron, N&C Baron & Associates and Verna Blewett, New Horizon Consulting
Pty Ltd, the Flexible Learning Centre of the University of South Australia, the
support of the Steering Committee for the project and the contribution of each
person and organisation who gave feedback during the consultation phases.

Contents Section 1: Using First Steps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
1.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
1.2 Who should use the First Steps? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
1.3 What’s in First Steps? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
1.4 Factors affecting effective OHS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
1.4.1 Leadership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
1.4.2 Employee participation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
1.4.3 Designing better environments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
1.4.4 Training and communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
1.4.5 Continuous improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
1.5 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Section 2: Getting started . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
2.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
2.2 Where are we now? (self-assessment) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
Form 2.1 Sample Checklist for Self Assessment against OHS
related Expected Outcomes of the Standards and Guidelines
for Residential Aged Care Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
2.3 What to do with the self-assessment results (planning) . . . . . . . . . . . . . . . . . . . . . .16
Form 2.2 – Sample OHS Action Plan Worksheet . . . . . . . . . . . . . . . . . . . . . . . . . . .17
2.4 Implementation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
2.5 Continuous improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
2.6 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Section 3: Managing hazards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
3.2 Hazard identification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
3.2.1 Hazard audits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Form 3.1 – Sample Hazard Log . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
3.3 Risk assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
3.3.1 Using a risk table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
3.4 Risk control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25
3.4.1 Hierachy of controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26
3.4.2 Implementing controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
3.5 Monitoring and review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
3.6 Tools for identifying hazards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29
3.6.1 Hazard reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29
Form 3.2 – Sample hazard Report Form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30
3.6.2 Workplace inspections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
Form 3.3 – Sample Workplace Inspection sheet . . . . . . . . . . . . . . . . . . . . . . . . . . .34
3.6.3 Incident reports/investigation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
Form 3.4 – Sample Incident/Injury Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40
Section 4: Major hazards of the aged care industry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .43
4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .43
4.2 Manual handling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .44
4.2.1 Identify the hazards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .44
4.2.2 Assess the risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .44
4.2.3 Control the risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .44
4.2.4 Record actions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .45
4.2.5 Monitor/evaluate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .45
4.2.6 Case studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46
Form 4.1 - Sample Manual Handling Risk Assessment and Control Action Plan . . . . . .47
Form 4.2 - Sample Resident Manual Handling Risk Assessment Checklist . . . . . . . . . .50
3OHS in Residential Aged Care First Steps
C o n t e n t s

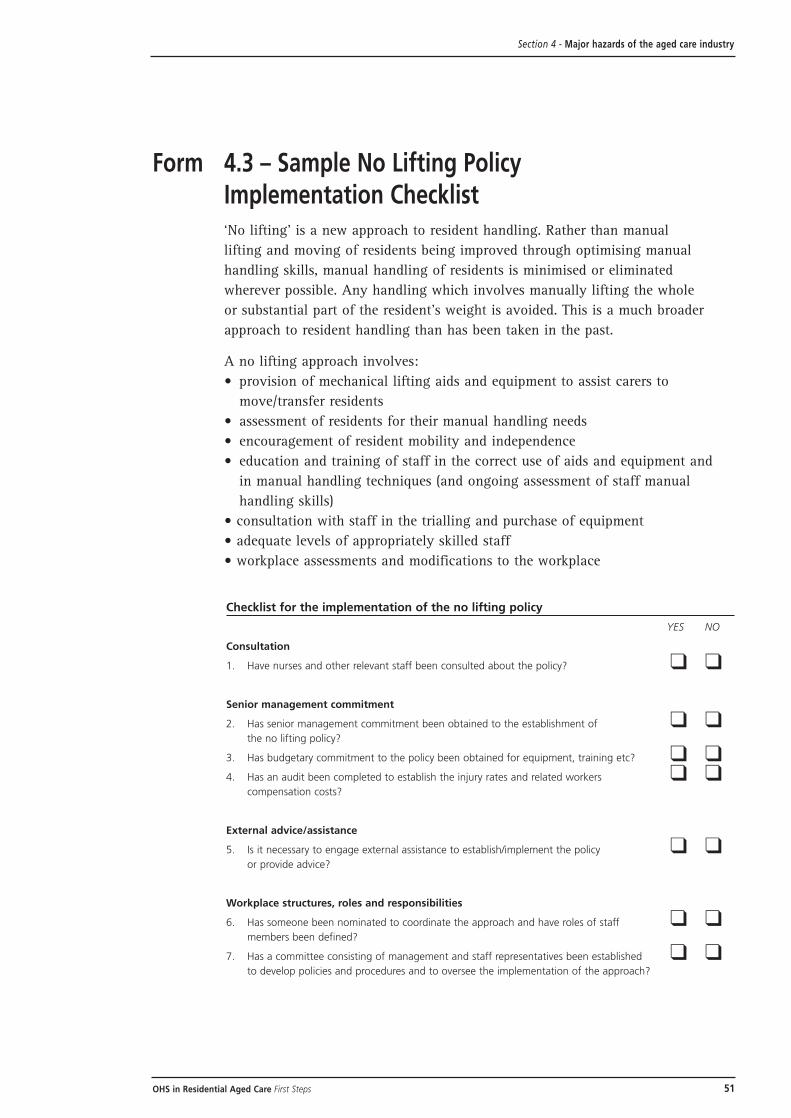
Form 4.3 - Sample No Lifting Policy Implementation Checklist . . . . . . . . . . . . . . . . . . .51
Table 4.1 - Resident handling using hoists and non-mechanical aids . . . . . . . . . . . . . .53
4.3 Slips, trips and falls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55
4.4 Resident aggression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .56
4.4.1 Identify the causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .56
4.4.2 Assess the risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .56
4.4.3 Develop and implement risk controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57
4.4.4 Monitor, evaluate and improve the strategies . . . . . . . . . . . . . . . . . . . . . . .58
Form 4.4 – Sample Aggression Incident report . . . . . . . . . . . . . . . . . . . . . . . . . . . .59
4.5 Plant and equipment hazards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .60
Form 4.5 – Sample Selecting Equipment – Pre-purchase Assessment . . . . . . . . . . . . .62
4.6 Living environment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .63
4.7 Fire, security and other emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .64
4.8 Infection control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .65
4.9 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .66
Section 5: Occupational Health and Safety management systems
5.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .67
5.2 Continuous improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .68
5.3 Compliance with OHS legislation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .71
5.4 Education and staff development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .72
5.5 OHS records . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .74
Form 5.1 – Sample monthly OHS statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .75
5.6 Occupational injury management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .76
5.7 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .78
Section 6: Occupational Health and Safety review - preparing for accreditation
6.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .79
6.2 Reviewing progress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .79
6.3 Preparing for accreditation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .79
Form 6.1 – Sample Standards Review Form – Preparing for Accreditation . . . . . . . . .80
6.3.1 Criteria (a) – Managing the Risks – 1st Stage . . . . . . . . . . . . . . . . . . . . . . . .83
6.3.1 Criteria (a) – Managing the Risks – 2nd Stage . . . . . . . . . . . . . . . . . . . . . . . .84
6.3.1 Criteria (a) – Managing the Risks – 3rd Stage . . . . . . . . . . . . . . . . . . . . . . . . .85
6.3.2 Criterion (b) – Involving Employees – 1st Stage . . . . . . . . . . . . . . . . . . . . . . .86
6.3.2 Criterion (b) – Involving Employees – 2nd Stage . . . . . . . . . . . . . . . . . . . . . . .87
6.3.3 Criterion (c) – Reporting and Acting on Incidents . . . . . . . . . . . . . . . . . . . . . .88
6.3.4 Criterion (d) – Equipment Fit for Purpose – 1st Stage . . . . . . . . . . . . . . . . . .89
6.3.4 Criterion (d) – Equipment Fit for Purpose – 2nd Stage . . . . . . . . . . . . . . . . . .90
6.4 Continuous improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .91
Form 6.2 – Sample OHS Policy/Procedure Document Review . . . . . . . . . . . . . . . . .92
Section 7: Resources
7.1 Legislation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .93
7.2 OHS authorities/contacts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .94
7.3 Hazard specific information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .96
Section 8: OHS Fact Sheets
8.1 OHS legal requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .99
8.2 OHS responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .100
8.3 Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .102
8.4 Fire, security and other emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .103
8.5 Hazardous substances and dangerous goods . . . . . . . . . . . . . . . . . . . . . . . . . . . . .104
Appendix 1: Project Steering Committee Members . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .105
Appendix 2: Feedback sheet . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .106
4 OHS in Residential Aged Care First Steps
Contents
Using First Steps
1.1 IntroductionOccupational Health and Safety in Residential Aged Care: First Steps has been
designed to assist you, as staff working in small aged care facilities, to improve
your management of Occupational Health and Safety, and to meet the OHS
requirements for the accreditation of your facility.
Under the Federal Government’s Aged Care Act 1997 all residential aged care
facilities in Australia will need to become accredited by 1 January 2001, if they
wish to continue to receive residential care subsidies. The requirements and
processes for gaining accreditation are set out in the Standards and Guidelines for
Residential Aged Care Services, the Aged Care Standards Agency Accreditation
Guide for Residential Aged Care Service, and the Application Kit for Accreditation.
Of the 44 Expected Outcomes specified in the Standards and Guidelines which
facilities are required to meet to gain accreditation, seven relate to OHS. Expected
Outcome 4.5 – Occupational Health and Safety is the major one, but Expected
Outcomes 4.1 to 4.7 all have OHS requirements.
To help you meet the OHS requirements for accreditation we have cross referenced
First Steps with these documents. In particular, if you complete the self-assessment
checklist contained in First Steps this will assist you to complete the OHS related
criteria in the worksheets of the Application Kit for Accreditation.
Throughout First Steps the relevant Expected Outcomes from the Standards and
Guidelines have been quoted to provide you with the links between OHS and the
Standards and Guidelines. Section 5 pays particular attention to accreditaion.
(Of course there are many other requirements for accreditation besides the OHS
ones. You will still need to be working with the Standards and Guidelines to make
sure you meet all those other requirements as well.)
In summary, First Steps can help you:
• implement priority Occupational Health and Safety (OHS) management systems
• address the major hazards facing aged care facilities
• reduce work related injuries and illness (and associated costs)
• meet the OHS requirements of accreditation
Section 1 Using First Steps
5OHS in Residential Aged Care First Steps
1.2 Who should use the First Steps?First Steps is designed as a management guide for owners, employers, directors,
managers and employees of small aged care facilities who are involved in the
process of reviewing and improving OHS. First Steps also aims to assist you
to reduce accidents and the human and economic costs of work related injuries
or illness.
1.3 What’s in First Steps?First Steps outlines simple steps you can follow to improve the management
of OHS and prepare your facility to meet the OHS requirements for accreditation.
Flowcharts are used to summarise the major steps required, with more information
included in the text. You may also use the flowcharts to develop your facility’s OHS
procedures (if required).
First Steps also includes a number of sample tools (i.e. checklists and forms). They
may be used in their current form or adapted to meet the needs of your facility.
They occur throughout First Steps immediately after the section in which they are
discussed. The development and systematic use of well designed checklists and
forms is a central element in an effective OHS program.
In the final sections of First Steps you will also find contacts for further
information and a range of Fact Sheets which may be used to inform staff
or further develop OHS.
Section 1 sets out a summary of the content of First Steps (summarised in
flowchart 1.1), and describes the five major principles necessary for an effective
OHS program, as background information for the remainder of First Steps.
6
Section 1 Using First Steps
OHS in Residential Aged Care First Steps

Section 1 Using First Steps
7OHS in Residential Aged Care First Steps
More information• State OHS Authorities
• Resources [Section 7]
• Fact sheets [Section 8]
Review progress - are weready for Accreditation?
[Section 6]
Improve OHS management systems
[Section 5]
Major hazards of aged care[Section 4]
Manage hazards [Section 3]
Set up program(4 stage process)
[Section 2]
Background [Section 1]
Flowchart 1.1 – Using First Steps

1.4 Factors affecting effective OHSTo be effective OHS must be integrated into the day-to-day operations of your
facility. Its success will depend on 5 major principles:1
• leadership demonstrated by managers
• employee participation
• designing better environments
• training and communication
• continuous improvement
Let’s consider each of these in turn.
1.4.1 Leadership
Leadership and commitment from senior management must be visible.
This requires managers to:
• allocate resources
• allocate responsibility, authority and accountability
• plan and follow through decisions
• assess performance and implement continuous improvement
• regularly review OHS
• integrate OHS into all decision making
• consult with employees
• develop written policies and procedures
1.4.2 Employee participation
Consultation with employees/health and safety representatives is a
requirement of each State’s OHS Legislation. Employee participation is
crucial for you to achieve a successful and effective OHS program.
Some reasons why consultation and participation are likely to lead to
a successful program are:
• people are more likely to change if they are involved in the process
• common goals can be identified when working together
• participation can provide a more fulfilling role for employees
• employees have detailed knowledge of any hazards in their work and often
have ideas of how problems can be solved
Details of the legal requirements for consultation methods are included in
Fact Sheet 3 in Section 8.
8 OHS in Residential Aged Care First Steps
Section 1 Using First Steps
1 WorkSafe Australia, (1995), “OHS Good for Business”, AGPS, Canberra. ‘Commonwealth of Australia, copyright reproduced by permission’.

1.4.3 Designing better environments
To design better environments you need to consider OHS:
• prior to designing new facilities or redesigning current facilities
• when making decisions to purchase new equipment
• restructuring your staffing arrangements
• when identifying, assessing and controlling risks
This process is described further in Section 3.
1.4.4 Training and communication
OHS should be part of all training. When training new staff you should
include workplace OHS policies and procedures, quality expectations, and
similar OHS issues.
Communication with employees on OHS issues is crucial to:
• raise awareness of OHS
• ensure people know what they are required to do
• encourage the exchange of ideas
• update people on changes and procedures
More detail of training requirements is included in Section 5.
1.4.5 Continuous improvement
Continuous improvement is an essential component of an effective OHS
program. This involves you and your staff constantly asking the questions
'Are we doing it right?' and 'How can we do this better?'.
The continuous improvement requirements of the relevant Standards and
Guidelines for Residential Aged Care Services are included in Section 5.
1.5 SummaryIn this opening section we have described the purpose and content of First Steps,
and also provided an overview of the 5 major principles on which any effective
OHS program needs to be based. In the next section we will look at the practical
steps required to set up or improve such a program.
9OHS in Residential Aged Care First Steps
Section 1 Using First Steps

11OHS in Residential Aged Care First Steps
Getting started
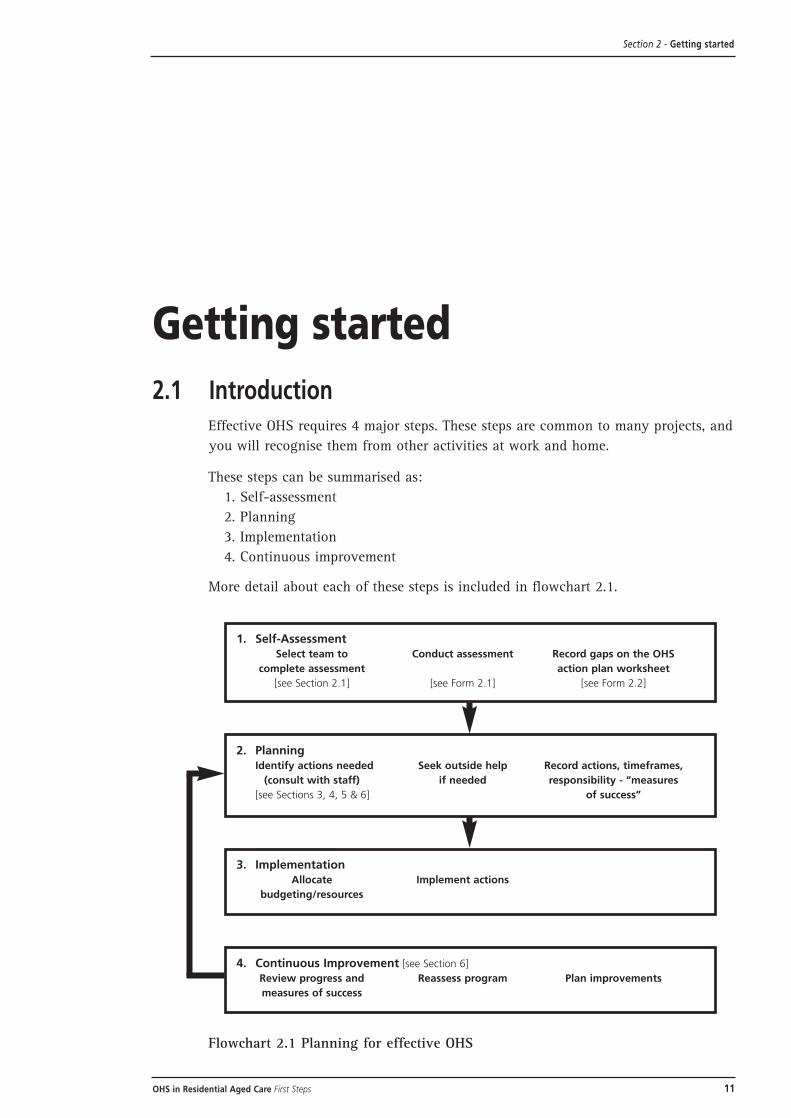
2.1 IntroductionEffective OHS requires 4 major steps. These steps are common to many projects, and
you will recognise them from other activities at work and home.
These steps can be summarised as:
1. Self-assessment
2. Planning
3. Implementation
4. Continuous improvement
More detail about each of these steps is included in flowchart 2.1.
Flowchart 2.1 Planning for effective OHS
Section 2 - Getting started
1. Self-AssessmentSelect team to Conduct assessment Record gaps on the OHS
complete assessment action plan worksheet
[see Section 2.1] [see Form 2.1] [see Form 2.2]
4. Continuous Improvement [see Section 6]
Review progress and Reassess program Plan improvements
measures of success
3. ImplementationAllocate Implement actions
budgeting/resources
2. PlanningIdentify actions needed Seek outside help Record actions, timeframes,
(consult with staff) if needed responsibility - “measures
[see Sections 3, 4, 5 & 6] of success”

2.2 Where are we now? (self-assessment)The first step is to select a team to review your facility’s current performance in
OHS to identify achievements and any gaps.
The team may include the Director and Health and Safety Representative [HSR]
if one is elected, or the OHS Committee [if one is in place] or with one or
more employees.
Once your team is selected, it should inform all staff about the review prior
to commencing and invite them to be involved. As we have seen, employee
participation is a major principle of effective OHS.
Form 2.1-The Self Assessment checklist on the next page will guide your team
through the process of assessing OHS. The form includes the major OHS
requirements, but you will need to review your State OHS legislation to make
sure you comply with all requirements.
Answering the questions in Form 2.1 will require you to review physical locations,
policies and procedures, meeting minutes, incidents and hazard reports and any
other documentation to provide evidence for your answers. Record relevant
information in the comments section of the checklist.
12 OHS in Residential Aged Care First Steps
Section 2 - Getting started

Section 2 - Getting started
13OHS in Residential Aged Care First Steps
Form 2.1 Sample Checklist for Self Assessment against OHS related Expected Outcomes of the Standardsand Guidelines for Residential Aged Care Services
Yes No Comments
1. Continuous improvement (expected outcome 4.1)
a) Does your facility have an OHS plan? ❑ ❑
b) Is OHS information (such as hazard/incident ❑ ❑reports, maintenance reports and minutes)
collected and used as the basis of
review/planning?
c) Is there a budget allocation for OHS? ❑ ❑
d) Does your facility have a written OHS policy? ❑ ❑
e) Does the policy include responsibilities of ❑ ❑employees and managers?
f) Is there a written rehabilitation policy? ❑ ❑
g) Are OHS policies and procedures ❑ ❑reviewed regularly?
2. OHS legislation (expected outcome 4.2)
a) Is your facility aware of State OHS ❑ ❑legislative requirements?
3. Consultation/participation (expected outcome 4.5)
a) Are there effective means of consultation/ ❑ ❑participation of employees in OHS decision
making that meets State legislative requirements?
b) Is OHS a regular agenda item at management, ❑ ❑board, staff and resident information meetings?
c) Where applicable, are the language needs of ❑ ❑employees and residents considered when
consulting on OHS?
14 OHS in Residential Aged Care First Steps
Form 2.1 – Sample Checklist for Self Assessment [cont]
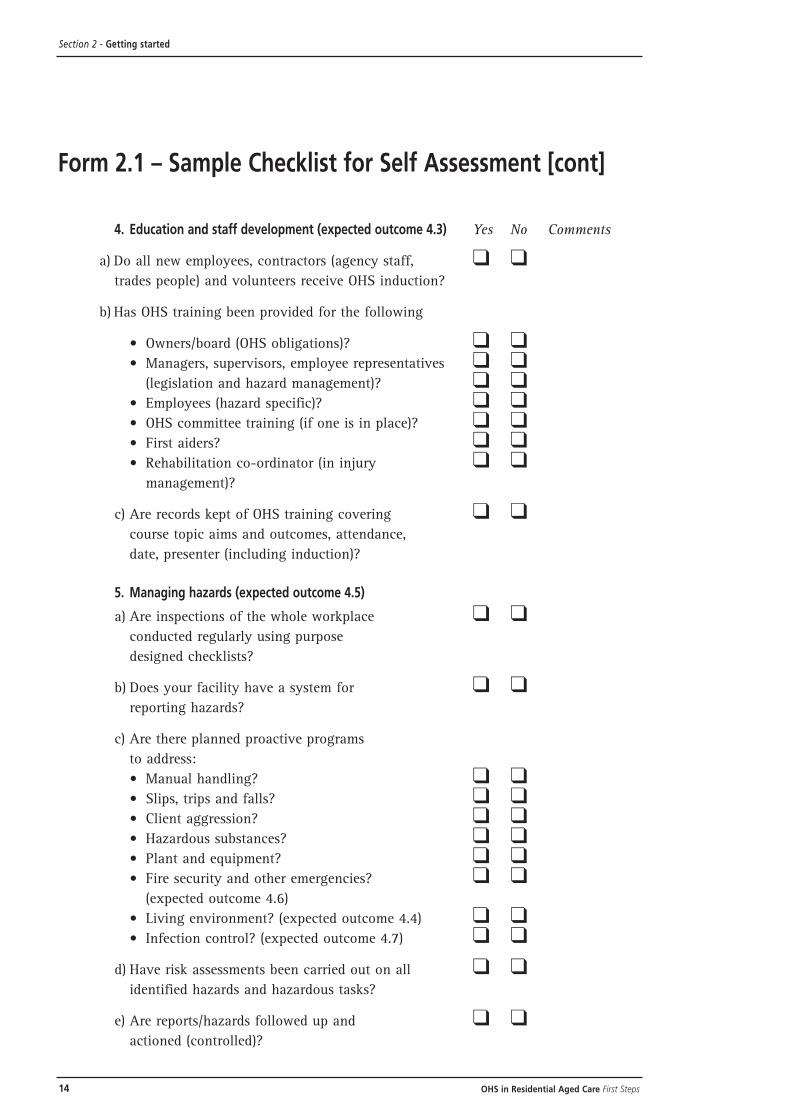
4. Education and staff development (expected outcome 4.3) Yes No Comments
a) Do all new employees, contractors (agency staff, ❑ ❑trades people) and volunteers receive OHS induction?
b) Has OHS training been provided for the following
• Owners/board (OHS obligations)? ❑ ❑• Managers, supervisors, employee representatives ❑ ❑
(legislation and hazard management)? ❑ ❑• Employees (hazard specific)? ❑ ❑• OHS committee training (if one is in place)? ❑ ❑• First aiders? ❑ ❑• Rehabilitation co-ordinator (in injury ❑ ❑
management)?
c) Are records kept of OHS training covering ❑ ❑course topic aims and outcomes, attendance,
date, presenter (including induction)?
5. Managing hazards (expected outcome 4.5)
a) Are inspections of the whole workplace ❑ ❑conducted regularly using purpose
designed checklists?
b) Does your facility have a system for ❑ ❑reporting hazards?
c) Are there planned proactive programs
to address:
• Manual handling? ❑ ❑• Slips, trips and falls? ❑ ❑• Client aggression? ❑ ❑• Hazardous substances? ❑ ❑• Plant and equipment? ❑ ❑• Fire security and other emergencies? ❑ ❑
(expected outcome 4.6)
• Living environment? (expected outcome 4.4) ❑ ❑• Infection control? (expected outcome 4.7) ❑ ❑
d) Have risk assessments been carried out on all ❑ ❑identified hazards and hazardous tasks?
e) Are reports/hazards followed up and ❑ ❑actioned (controlled)?
Section 2 - Getting started

15OHS in Residential Aged Care First Steps
Section 2 - Getting started
Form 2.1 – Sample Checklist for Self Assessment [cont]
Yes No Comments
f) Is the action taken reviewed to ❑ ❑ensure effectiveness?
g) Are staff and residents considered when ❑ ❑managing risks and developing safe
work procedures?
h) Are OHS implications considered when ❑ ❑purchasing or hiring equipment/
furniture etc?
6. Incident reporting/investigation (expected
outcome 4.5)
a) Does the facility have a standard form ❑ ❑for reporting/investigating incidents/
injuries that complies with relevant State
Legislation and Codes of Practice?
b) Are staff aware of the reporting procedure? ❑ ❑
c) Are incidents investigated and documented? ❑ ❑
7. Injury management (no cross reference
to standards)
a) Is there a procedure to manage workers ❑ ❑compensation claims?
b) Is there a process to manage early and ❑ ❑effective return to work following
an injury?

2.3 What to do with the self-assessment results (planning)Any ‘no’ answers recorded when filling in your Self-assessment checklist (Form 2.1)
demonstrate a gap in the OHS system and the need for improvement. Record these
on Form 2.2-Action plan worksheet (see next page). This worksheet is based on
those in the Application Kit for Accreditation. You will need to document the
actions required, what your outcome (or improved result) will be, who is responsible
for the actions and the timeframe. The remainder of First Steps will help you decide
on the actions required.
It is vital to involve staff in the planning process in order to achieve successful
outcomes (and meet the legal requirements for consultation). Discuss the required
actions with employees and their representatives. Record the actions on the OHS
action plan worksheet (Form 2.2) (or your own action plan if you already have one).
Next you will need to decide who will be responsible for the tasks, and timeframes.
Record these also on Form 2.2. Obtain outside help for carrying out tasks, if needed.
Refer to the relevant State OHS Legislation while developing the action plan to
ensure legislative compliance and to meet Expected Outcome 4.2 of the Standards
and Guidelines for Residential Aged Care Services.
You may need to include short and long term objectives in the plan. Some may be
completed within one month while others require one or even two years.
Next you will need to decide what resources are needed to implement the plan.
Determine how you will measure the success of the plan; for example, through
better reporting of hazards, regular maintenance of equipment, reduction in injuries.
This will require the development of ‘measures of success’ such as ‘90% of
equipment checked by the due date’. Record these measures of success in the ‘What
will be the improved result?’ column of the action plan (Form 2.2).
You will also need to prioritise activities recorded on your action plan, so that you
start by addressing priority hazards first.
For effective prioritisation you will need to take into account:
• the particular needs of your facility
• your major hazards (see Section 4)
• legislative compliance
• resource/budget requirements
• training and staff development needs
16 OHS in Residential Aged Care First Steps
Section 2 - Getting started

17OHS in Residential Aged Care First Steps
Section 2 - Getting start e d
Form 2.2 – Sample OHS Action Plan Worksheet
S o u rce: Adapted from Aged Care Accreditation Agency Guide for Residential Aged Care
2.4 ImplementationNow you have an action plan in place the next step is to make it happen.
• arrange any resource/budgeting needs for implementing the action plan
• implement the required actions (if additional information is needed to
implement the improvements, contact your employer association, union
or State OHS Authority)
• provide any required training (Expected Outcome 4.3)
• record the “improved result” on the action plan worksheet
2.5 Continuous improvement(Expected Outcome 4.1)
To achieve continuous improvement you and your team will need to:
• review progress against the action plan at the OHS committee or staff meetings
at regular intervals, for example monthly, to ensure timeframes are being met,
that the changes made have been effective and to identify any difficulties in
implementing the plan
• reassess your OHS program on a regular basis (e.g. annually), using the self-
assessment checklist (Form 2.1) and your ‘measures of success’ entries in the
‘What will be improved result?’ column of your action plan
• use the findings to develop an annual OHS plan (continuous improvement) and
to complete the worksheets in the Application Kit for Accreditation
2.6 SummaryCompletion of the self assessment sheet and recording the required tasks on the
action plan has started you and your team on the path to continuously improve
OHS within your facility.
The next section of First Steps will provide you with more detail on how to manage
your hazards by firstly identifying them, then assessing and eliminating or
minimising the risks.
18 OHS in Residential Aged Care First Steps
Section 2 - Getting started

19OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
Managing hazards
3.1 IntroductionA key element in any effective OHS program is the management of hazards.
Managing hazards involves 4 major steps:
• hazard identification
• risk assessment
• risk control
• monitoring and review
In this Section we will go through each of these steps in turn, outlining a range of
strategies and tools to assist in the management process. Sample forms related to
each step are included immediately after the relevant discussion.
Using these strategies and tools will also assist you to meet Expected Outcome 4.5
of the Standards and Guidelines for Residential Aged Care Services, which requires
‘Management to actively work to provide a safe working environment that meets
regulatory requirements’.
There must be policies and practices which provide:
• for the management of hazards identified in the workplace
• for management and staff involvement in identifying and resolving OHS issues
• incident report mechanisms that are present, functional and acted upon
• equipment that is fit for the purpose intended, is well maintained, and which
staff are trained to use
Hazards are defined as anything that has the potential to cause injury or illness,
such as:
• physical hazards, for example, sharp edges, slippery floors
• chemicals
• work practices such as repetitive jobs, including manual handling
• aspects of workplace design, for example restricted access to toilets, poor lighting,
steep stairs
Risk is defined as the likelihood (probability) that injury/illness will occur and the
potential severity (consequences).
The steps involved in managing hazards are shown in the following flowchart
(Flowchart 3.1).

20 OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
Monitor/reviewoutcomes
Implement controls
Develop control plan(who,when, how,
training etc)
Select risk controlsolutions
Conduct a riskassessment
List on hazard log
Hazard identified(audit, inspection
report/incident etc)
see Section 3.2
see Section 3.3
see Section 3.3
see Section 3.4
see Section 3.4.2
see Section 3.4.2
see Section 3.5
Each step must include consultation with staff and feedback
Flowchart 3.1 Hazard Management Process

21OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
3.2 Hazard identificationThe first step in managing hazards is to identify your hazards. It is important to
involve everyone in this task.
Tools that can assist you to identify and address hazards are a hazard log (Form
3.1), hazard or incident reports (Form 3.2), and a structured workplace inspection
using a workplace inspection sheet (Form 3.3).
Strategies for identifying hazards may be continuous, that is integrated into day
to day activities, or specifically planned for the purpose. Examples of each are
listed below.
Continuous strategies• hazard reports completed by staff
• incident reports and investigation
• informal observations
• OHS discussion at staff meetings/OHS committee
• ‘breakdown’ maintenance records
Planned strategies• regular workplace inspections
• monthly review of data
• conducting a hazard audit, for example, brain-storming to consider all aspects
of the facility and the things which could cause injury/illness
• considering potential hazards prior to purchasing new equipment or chemicals
• use of industry information from employer organisations and unions to highlight
issues which have not been considered
3.2.1 Hazard audits
One useful planned activity to identify hazards is to conduct a hazard audit
(‘hunting for hazards’). This can be done in a number of ways. Use a small
group of staff from a range of positions to conduct the survey but involve
everyone. One way to organise the survey is to draw a map of the site and
then to look at and discuss the potential hazards within each area, for
example, kitchen, storeroom, resident rooms, office, maintenance shed,
garden, delivery area.

22 OHS in Residential Aged Care First Steps
Record all the hazards identified in a hazard log. A sample hazard log has been
included (Form 3.1 – see next page). A hazard log should include a summary of
hazards including the level of risk, actions taken, responsibility, completion date
and follow-up date.
The next step is to decide which hazards present the greatest risk in order to
prioritise which hazards to address first. Hazards which are simple to fix (and
at small, or no cost) should be rectified at the time or soon after the audit.
Keep a record of the actions and consider whether the same or a similar problem
may exist in other areas of the facility.
Section 3 - Managing hazards
Consider: 2
• substances used - for example, cleaning and laundry products,
photocopier toner
• equipment used - suitability of hoists, maintenance tools, ovens,
washing machines, dryers, irons, lawnmowers etc and any hazards
associated with the way they are used or maintained
• moveable items - vehicles, store boxes, linen and food trolleys,
shower chairs, wheelchairs (manual and electric), lifters
• people - do they have the skills, information, training and
equipment necessary to perform tasks safely? Do they comply
with the procedures? Are there potential hazards for staff who
are new and/or inexperienced? How could they be affected?
2 Victorian Occupational Health and Safety Authority, “An Accident at Work Hurts Everyone Around You – Making OHS Matter”, October 1994, pp 7-8

23OHS in Residential Aged Care First Steps
Form 3.1 – Sample Hazard Log
Section 3 - Managing hazards
Date of
Nature of hazard
Priority A
ction requiredBy
By D
ate actionFollow
report(risk identification)
(risk (risk control)
whom
when
completed
up dateassess-m
ent)

24 OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
3.3 Risk assessmentRisk assessment is the second major step you need to take in managing hazards,
once you have identified hazards by any of the continuous or planned methods
listed above, and entered them in your hazard log (Form 3.1).
Risk assessment is the process in which you and your staff consider two things:
• the degree of seriousness of injury or illness which could be caused by a hazard
• the likelihood of such injury or illness occurring.
There are a number of tools which you could use to assist in conducting risk
assessments. One example is the risk table3 on the next page.
3.3.1 Using a risk table
Consider the following:
What might be the consequences of the hazard?
• fatality
• major injuries (normally irreversible injury or damage to health)
• minor injuries (could require several days off work)
• negligible injuries (first aid)
How likely is it the hazard will cause an injury or illness?
• very likely – could happen frequently
• likely – could happen occasionally
• unlikely – could happen but only rarely
• highly unlikely – could happen but probably never will
3 National Occupational Health and Safety Commission (1995), “Plant in the Work Place - Making it Safe”, Australian Goverment Publishing Service, Canberra

25OHS in Residential Aged Care First Steps
Consequence Likelihood
Very likely Likely Unlikely Highly
Unlikely
Fatality High High High Medium
Major Injury High Medium Medium Low
Minor injury High Medium Medium Low
Negligible Medium Medium Low Low
The risk table matrix is used to determine the level of risk based on the assessment
of likelihood and consequence. For example, a frequently used slippery bathroom
floor could be assessed as very likely to result in a major injury. Using the risk table
this would be assessed as high risk.
Conduct a risk assessment on each of the hazards listed in the hazard log and
record the results. This will then help to prioritise which hazards should be
addressed first.
3.4 Risk controlAfter hazard identification and risk assessment, the third major step in managing
hazards is risk control. This requires you to plan actions to eliminate or reduce the
risks of injury or illness starting with the high priority hazards.
The recognised method for controlling risks is to apply the ‘Hierarchy of controls.’
Section 3 - Managing hazards
Table 3.1 Risk Table

26 OHS in Residential Aged Care First Steps
3.4.1 Hierarchy of controls
The hierarchy of controls is a graded list of four strategies:
The first of these, eliminating the hazard completely, is the most desirable,
but if this is not possible the second can be applied, and so on down the
hierarchy to the least satisfactory option, the use of personal protective
clothing or equipment. In practice, if it is not possible to eliminate the hazard
completely, it is often necessary to use some combination of the remaining
three controls.
Methods used should be in compliance with the relevant State OHS
Regulations and Codes of Practice.
Elimination
Examples of elimination are:
• repairing or replacing faulty equipment
• redesigning the workplace or work practices, for example, not doing
unnecessary high risk tasks or designing new facilities (or redesigning old
ones) to allow sufficient space for manual handling tasks
If the hazard can’t be eliminated the next option is to minimise the risk
of injury.
Minimise the risk of injury
There are a number of options you may be able to use alone or in
combination to minimise the risks of injury and illness.
Section 3 - Managing hazards
Eliminate the Hazard
Minimise the Risk – Engineering, Substitution etc
Implement Adminstrative Controls
Provide PersonalProtective Clothing
or Equipment (PPCE)

Substitution
Substitution requires replacing hazardous substances or procedures with
those which are safer, for example by:
• replacing a hazardous cleaning product with one which is non-hazardous
and environmentally friendly
• replacing tiles in the bathroom with non slip tiles
Modification
You may be able to modify the workplace or work practices to minimise risk,
for example by:
• rearranging the layout of a resident’s room to allow free access with a hoist
• improving drainage in bathrooms
Isolation
You may be able to isolate hazards to minimise the risk, for example by:
• moving a photocopier away from the desk area
• locking up chemicals to prevent access by residents or visitors
Engineering controls
Engineering controls include the use of:
• hoists and trolleys
• spring loaded bases in linen baskets
• electric or manually raising beds
If risks can’t be minimised the next option is to consider implementing
administrative controls.
Administrative controls
Administrative controls include:
• changing the way the work is done
• implementing Safe Work Practices or Standard Operating Procedures (SOPs)
• training
• increasing the supervision of staff
Examples include:
• written procedures for higher risk tasks
• safe procedures to be followed during maintenance
• signs warning of hazards
• rest breaks for people like computer operators doing repetitive tasks
• job rotation
• regular training on, for example, manual handling
27OHS in Residential Aged Care First Steps
Section 3 - Managing hazards

Personal Protective Clothing and Equipment (PPCE)
PPCE is a means of protecting the worker’s body from the hazard,
and may include:
• gloves (for example vinyl, rubber, mesh)
• respirators/masks
• safety glasses/goggles
• hearing protection
• non-slip shoes, rubber boots
• aprons
PPCE must be:
• carefully selected to be suitable for the task
• correctly fitted
• comfortable to wear
• always worn where indicated
You must train staff in the use and maintenance of PPCE and they must be
supervised to ensure they do wear/use and maintain it.
3.4.2 Implementing controls
When you have considered options for controlling risks and chosen a
solution, your next step is to document it on the hazard log (Form 3.1) and
develop an implementation plan, including who is responsible for tasks
and the time frames.
Employees and their representatives must be involved in the process
of selecting controls and trained in any new procedures required.
3.5 Monitoring and review
(Expected Outcome 4.1)
You have now identified your hazards, and assessed and controlled the risks they
present. The fourth step in managing hazards is, in consultation with your staff, to
monitor and review the changes made to control the hazard to ensure they have
been effective, and have not introduced additional hazards.
The hazard log (Form 3.1) is a key tool for monitoring and review. Record the action
completed and follow up dates on the hazard log. During review you may identify
further improvement strategies which need to be implemented. These should be
recorded as a new item on the hazard log.
28 OHS in Residential Aged Care First Steps
Section 3 - Managing hazards

3.6 Tools for identifying hazards
3.6.1 Hazard reports
Effective hazard reporting is essential for successful hazard management and
to meet Expected Outcome 4.5. Implementing the use of hazard report forms
(Form 3.2 on the next page) will encourage your staff to identify and report
hazards. You can then implement controls before an injury occurs.
Encourage staff to complete hazard report forms for any situation which
requires actions beyond simple maintenance. For example, a maintenance
request may be completed for a wheel sticking on one shower chair. Repeated
occasions of wheels sticking on a number of shower chairs has identified a
hazard and a hazard report form should be completed.
Hazard report forms should be:
• completed by anyone-employees, managers, contractors, volunteers
or residents/families
• investigated and improvements planned and implemented by the
director/supervisor (in consultation with staff)
• signed by the health and safety or employee representative (if there is one)
• discussed at an OHS committee/staff meeting
After discussion at a meeting you should include comments on the
effectiveness of action taken on the hazard report form and hazard log.
Provide feedback to the staff member who reported the hazard.
The steps for resolving hazards are summarised in Flowchart
29OHS in Residential Aged Care First Steps
Section 3 - Managing hazards

30 OHS in Residential Aged Care First Steps
Risk Rating(See Risk
Table)
Name (optional): Date:
Description of hazard(include area and task involved, and any equipment, tools, people involved. Use sketches if necessary):
Suggested actions(list any suggestions you have for reducing or eliminating the problem e.g. redesign, use of mechanical devices, training etc):
Report to (Name) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Position . . . . . . . . . . . . . . . . . . . . . . . . . . . .Give this report to Manager/Supervisor
Action taken(to be completed by a Manager/Supervisor in consultation with employees and include action at local level):
Supervisor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Date . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Outcome evaluation: Hazard eliminated ❑ Risk controlled ❑
Further actions, by who, when? ❑ Response to person reporting
Date of response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
❑ Response to staff meeting/ OHS Committee
Date of response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Director . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Date . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Employee representative . . . . . . . . . . . . . . . . . . . . . . . . . . .Date . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Form 3.2 - Sample Hazard Report form
Section 3 - Managing hazards
To b
e co
mpl
eted
by
man
agem
ent
To b
e co
mpl
eted
by
pers
on id
enti
fyin
g ha
zard

31OHS in Residential Aged Care First Steps
Person identifies hazard
Complete hazard report form
Report to Supervisor/Managerand/or Health & Safety
Representative
Discuss/resolve issue andoutcome at staff and/or OHS
committee meeting
Feedback to person reporting hazard
Record on hazard log
Assess and control risks
Implement actions
Monitor/review
Section 3 - Managing hazards
Flowchart 3.2 Steps in resolving hazards

32 OHS in Residential Aged Care First Steps
3.6.2 Workplace inspections
Regular workplace inspections using a checklist provide you with a chance to
identify hazards not noticed on a day-to-day basis.
The objective is to identify hazards, monitor OHS standards and ensure that
corrective action is taken within an agreed time frame.
Inspections should be conducted by a manager and an employee representative
or OHS committee member. It is a good idea to rotate the people conducting the
inspections and bring in people from different areas as they may see different
hazards. This also helps to encourage participation by all staff in the facility.
A flowchart of the process is shown in Flowchart 3.3.
Monitor/review outcomes
Implement action plan
Record hazards/actions onhazard log
Conduct risk assessment
Identify hazards
Inspect workplace using checklist
Section 3 - Managing hazards
Flowchart 3.3 Workplace inspections
Select inspection team

You should decide how often to conduct inspections in consultation with employees,
considering how quickly hazards could arise, for example, every two months.
Inspections should include a wide range of issues such as housekeeping, emergency
equipment, lighting, equipment, storage and hazardous substances, and should
involve staff working in the area.
A sample Workplace Inspection sheet or checklist is included (see Form 3.3 on the
next page). You will need to adapt this to suit your facility. A small facility may
only need to have one checklist, or it may be more practical to have more than one
and complete them at staggered regular intervals, for example, kitchen/dining areas,
laundry, offices, resident rooms, garden and maintenance areas.
Following workplace inspections you must take action to address identified hazards
or issues. Document the actions on the checklist, along with who is to take action
and the timeframe. Rectify anything which can be immediately fixed but still record
it on the checklist as it may indicate a trend, for example, blocked fire exits.
Once actions have been completed record the completion date on the checklist. You
may wish to record major hazards on the hazard log, to keep all information in one
place (see Form 3.3).
Long term actions should be included in the OHS Action Plan worksheet (Form 2.2).
33OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
34 OHS in Residential Aged Care First Steps
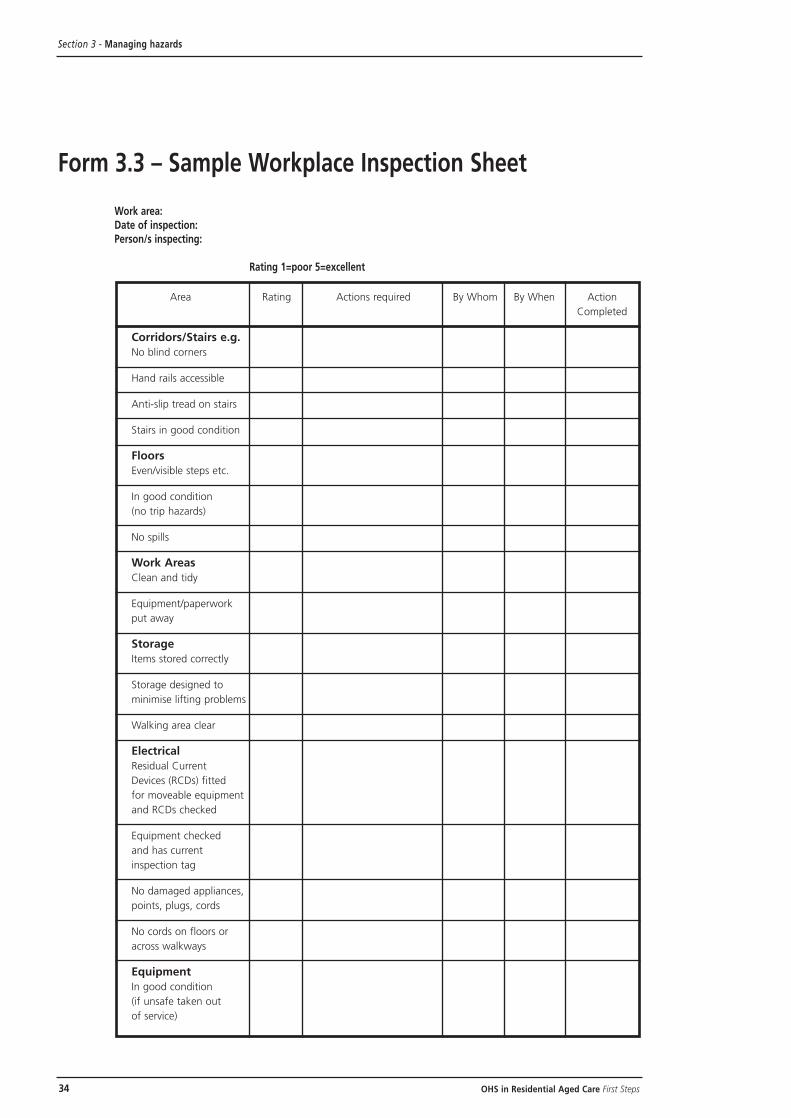
Form 3.3 – Sample Workplace Inspection Sheet
Work area:Date of inspection:Person/s inspecting:
Rating 1=poor 5=excellent
Area Rating Actions required By Whom By When Action
Completed
Corridors/Stairs e.g.
No blind corners
Hand rails accessible
Anti-slip tread on stairs
Stairs in good condition
Floors
Even/visible steps etc.
In good condition
(no trip hazards)
No spills
Work Areas
Clean and tidy
Equipment/paperwork
put away
Storage
Items stored correctly
Storage designed to
minimise lifting problems
Walking area clear
Electrical
Residual Current
Devices (RCDs) fitted
for moveable equipment
and RCDs checked
Equipment checked
and has current
inspection tag
No damaged appliances,
points, plugs, cords
No cords on floors or
across walkways
Equipment
In good condition
(if unsafe taken out
of service)
Section 3 - Managing hazards
35OHS in Residential Aged Care First Steps
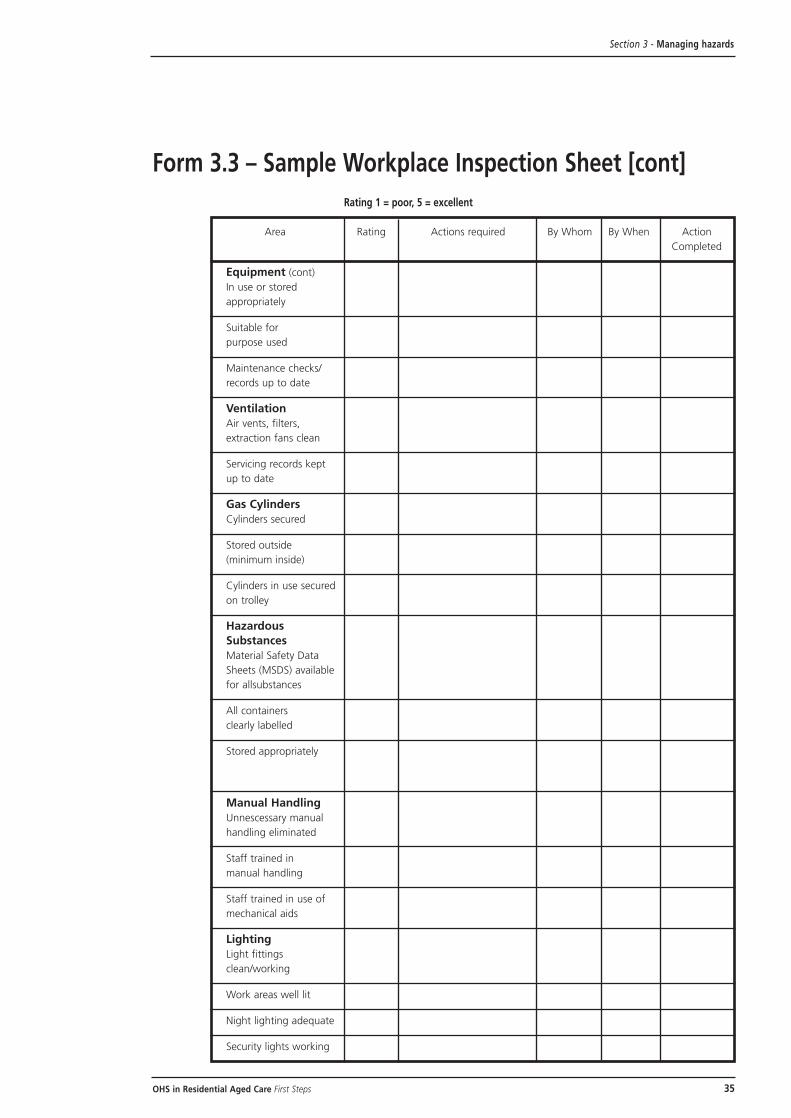
Form 3.3 – Sample Workplace Inspection Sheet [cont]
Rating 1 = poor, 5 = excellent
Area Rating Actions required By Whom By When Action
Completed
Equipment (cont)
In use or stored
appropriately
Suitable for
purpose used
Maintenance checks/
records up to date
Ventilation
Air vents, filters,
extraction fans clean
Servicing records kept
up to date
Gas Cylinders
Cylinders secured
Stored outside
(minimum inside)
Cylinders in use secured
on trolley
Hazardous
Substances
Material Safety Data
Sheets (MSDS) available
for allsubstances
All containers
clearly labelled
Stored appropriately
Manual Handling
Unnescessary manual
handling eliminated
Staff trained in
manual handling
Staff trained in use of
mechanical aids
Lighting
Light fittings
clean/working
Work areas well lit
Night lighting adequate
Security lights working
Section 3 - Managing hazards

36 OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
Form 3.3 – Sample Workplace Inspection Sheet [cont]
Rating 1 = poor, 5 = excellent
Area Rating Actions required By Whom By When Action
Completed
Employee amenities
Toilets/handbasins clean/
soap available
Lunch room clean
Safety signs
OHS policy dispalyed
First Aid, Protective and
Fire Equipment, signs
etc posted
Waste disposal
Bin regularly
emptied/cleaned
Food scraps in vermin
proof bins
Infectious waste
disposal
Sharps containers
available (close to area
of use)
Infectious waste
disposed of appropriately
Fire/Emergencies
Extinguishers in place,
serviced/not blocked
Exits clearly
marked/clear
Exit/Emergency
lighting works
Action cards/emergency
numbers displayed
Smoke detectors tested
Fire blanket accessible
Employees know
procedures (ask a
sample of staff)
First aid kit available,
well stocked and clean
Records kept of first
aid provided
37OHS in Residential Aged Care First Steps
3.6.3 Incident reports/investigation
OHS Legislation in all States requires incidents resulting in injury to be
recorded. Serious injuries must be reported to the appropriate authority.
The requirements differ from State to State so you must refer to the State
Legislation or State OHS authority to check specific requirements. The
process for incident investigation is summarised in Flowchart 3.4 on
the opposite page.
Section 3 - Managing hazards
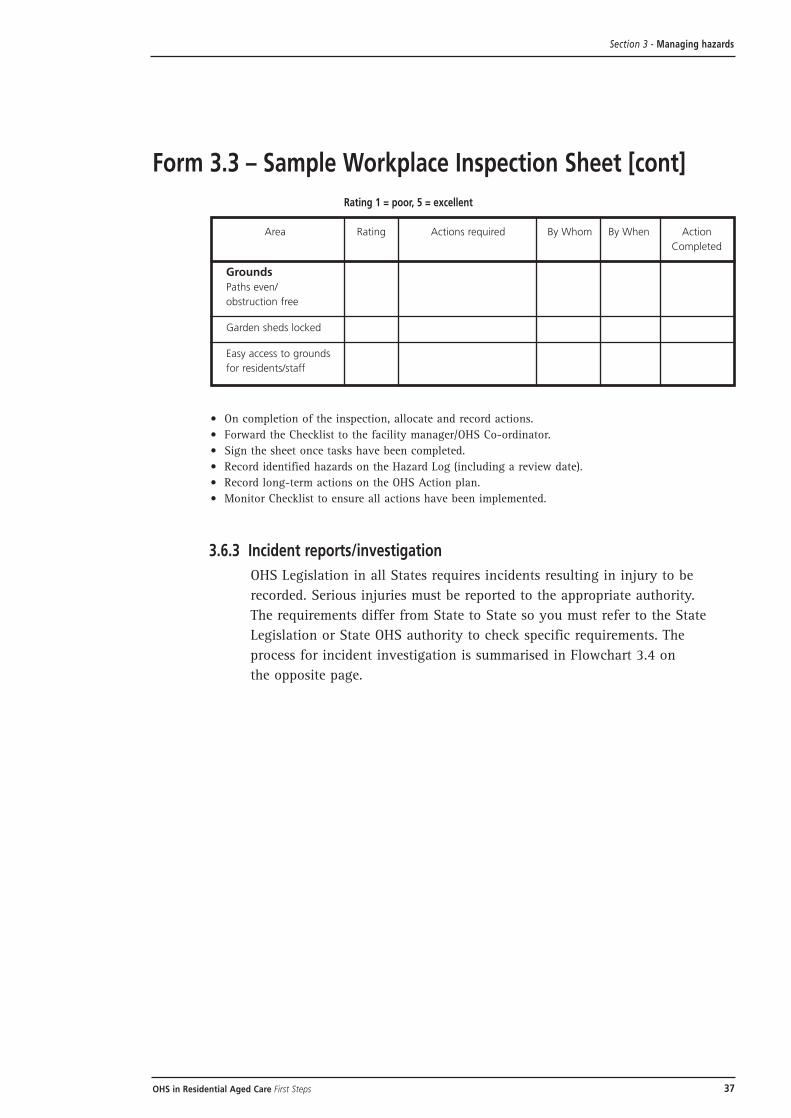
Form 3.3 – Sample Workplace Inspection Sheet [cont]
Rating 1 = poor, 5 = excellent
Area Rating Actions required By Whom By When Action
Completed
Grounds
Paths even/
obstruction free
Garden sheds locked
Easy access to grounds
for residents/staff
• On completion of the inspection, allocate and record actions.
• Forward the Checklist to the facility manager/OHS Co-ordinator.
• Sign the sheet once tasks have been completed.
• Record identified hazards on the Hazard Log (including a review date).
• Record long-term actions on the OHS Action plan.
• Monitor Checklist to ensure all actions have been implemented.

38 OHS in Residential Aged Care First Steps
Section 3 - Managing hazards
First Aid/
medical care
Complete First
Aid Report
Notify
supervisor
Is injury
serious?
Notify
employer/
employee
representative
Complete
compensation
claim form
(if required)
Lost time/
medical costs?
Complete incident report
Manager/HSR/employees
review reports
Recommend and implement
corrective action
Discuss at staff meeting/
OHS committee
Hazard controlled
Monitor/review
Report to
OHS authority
(if required)
Incident
occurs
Injury
Property
damage
Damage
significant
Report to
manager
No
No
No
No
No No
Yes
Yes
Yes
Yes
Yes
Yes
Flowchart 3.4
Incident reporting/investigation procedure
39OHS in Residential Aged Care First Steps
Reporting and investigating ‘near miss’ incidents where no injury occurred will also
assist you to identify hazards. Where an injury results in lost time or medical costs,
workers compensation claim forms must be completed.
Incident report forms are legal documents and must be completed thoroughly and
objectively. An example form is included on the next page (Form 3.4).
You will need to adapt this to suit your facility and your State legislation.
Investigating incidents is essential for identifying and addressing hazards. This
requires investigators (a manager and health and safety/employee representative) to
be trained in the task. A detailed approach must be used, particularly for long-term
incidents or symptoms where underlying causes may be hard to identify.
Things you should consider include:
• who was involved?
• where and when did the incident occur?
• what task or work was being performed?
• how did the incident occur, for example, was a chemical, client, process
or equipment involved?
• what were the events leading up to the incident?
Look for problems related to equipment, the task, work environment or procedures
(not just what a person did wrong).
You can use this information to identify the underlying causes (hazards). You will
then need to conduct a risk assessment on each hazard.
Next, develop a plan for controlling the hazards identified, including time frames
and responsibilities and record the outcomes on the incident report form (Form 3.4)
and the hazard log (Form 3.1).
Discuss the injury statistics and actions taken at the OHS committee/staff meetings.
Document the discussion in the minutes, including a review of the effectiveness of
the actions taken.
You may choose to use separate incident report forms for staff and residents or to
use the same form. Where the same form is used, confidentiality of resident records
must be protected. Staff reports must also be kept confidential with incidents
discussed at meetings but without individuals involved being identified.
For more information about the management of employee injuries see Section 5.6.
Section 3 - Managing hazards

40 OHS in Residential Aged Care First Steps
Status:
Employee ❑ Visitor ❑ Contractor ❑ Volunteer ❑ Student ❑ Resident ❑
1. Details of injured person
Surname: Phone: (h) (w)
First name: Sex: M ❑ F ❑Address: Date of birth:
1st Language:
Experience in job: Work arrangement:
❑ 0-3 months ❑ 3-5 years ❑ Casual ❑ Full time
❑ 4-12 months ❑ 5 years plus ❑ Permanent P/T ❑ Other
❑ 1-2 years
2. Details of witnesses:
Name: Phone: (h) (w)
Address:
Name: Phone: (h) (w)
Address:
3. Details of incident or accident:
Date: Time of Injury:
Activity engaged in:
Location of incident/accident:
Describe how and what happened:
4. Details of injury (the assistance of a supervisor may be required to complete this section):
Nature of injury/illness (eg burn, sprain, cut etc):
Mechanism (eg fall, grabbed by person, muscular stress):
Location on body (eg back, right thumb, left arm etc):
Agency (eg furniture, another person, hot water):
5. Treatment administered:
First Aid Administered Yes ❑ No ❑Treatment:
Referred to:
First Aid Attendant (Print name): (Signature):
Form 3.4 – Sample Incident/Injury Report
Section 3 - Managing hazards

41OHS in Residential Aged Care First Steps
Sections 6-9 must be completed by Supervisor
6. Did the injured person stop work:
Yes ❑ No ❑ If yes, state date: Time:
Outcome:
❑ Treated by doctor ❑ Lodged Workers Comp Claim ❑ Referred to Rehab Co-ord
❑ OHS Authority notified ❑ Returned to normal duties ❑ Referred to OHS Officer
❑ Hospitalised ❑ Returned to alternative duties and/or OHS Committee
7. Incident or accident investigation
(comments to include identified causal factors):
Name and Signature (supervisor): Date:
8. Remedial actions:
❑ Conduct task ❑ Reinstruct persons ❑ Improve design/
analysis involved construction/guarding
❑ Conduct hazard ❑ Improve resident ❑ Add to inspection program
systems audit /staff skills mix
❑ Develop/review ❑ Provide debriefing ❑ Improve communication/
tasks/procedures and/or counselling reporting procedures
❑ Improve work ❑ Request maintenance ❑ Improve security
environment
❑ Review OHS ❑ Improve personal ❑ Temporarily relocate
policy/programs protection employees involved
❑ Replace ❑ Improve work congestion/ ❑ Other (specify)
equipment/tools housekeeping
❑ Improve work ❑ Investigate safer
organisation alternatives
❑ Develop and/or ❑ Request Material Safety
provide training Data Sheets (MSDS)
What, in your own words, has been implemented or planned to prevent recurrence:
9. Remedial actions completed:
Signed (supervisor): Title: Date:
10. Review comments
(OHS Committee/staff meeting):
Reviewed by DON/Director/Site Manager (Signed) (Date)
Source: Adapted from WorkCover NSW/Baptist Community Services, “Managing Resident Aggression in Aged CareFacilities” - 1st Edition, November 1998.
Section 3 - Managing hazards
Form 3.4 – Sample Incident/Injury Report [cont]

43OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
43OHS in Residential Aged Care First Steps
Major hazards of the agedcare industry
4.1 IntroductionWhat are the hazards most commonly encountered in aged care facilities which
must be eliminated or minimised to prevent or reduce the occurrence and severity
of staff injuries or illness?
Seven major hazards which have been identified are:
• manual handling
• slips, trips and falls
• resident aggression
• plant and equipment
• the living environment
• fire, security and other emergencies
• infection control
The first three of these hazards make up more than 80% of all claims for workers
compensation, according to statistics from the National Occupational Health and
Safety Commission [NOHSC] for aged care in 1996-1997. The latter four reflect
major hazards referred to in the Standards and Guidelines for Aged Care Services.
However, these are not the only hazards in aged care and other examples are
detailed in the Practical Guide to OHS in Residential Aged Care.
In this section the information, strategies and tools that were introduced in the
preceding sections will be applied to each of these seven major hazards in turn,
using the appropriate hazard management approaches.

44 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
4.2 Manual handlingManual handling is the most common cause of injuries for employees
working in aged care facilities, accounting for 58% of all injuries. Nurses, carers,
cleaners, laundry, maintenance, administration and kitchen staff have all been
injured during manual handling.
Statistics from the National Occupational Health and Safety Commission [NOHSC]
for aged care in 1996-1997 showed strains and sprains made up three quarters of
all the workers compensation injuries that occurred.
It is important to remember that manual handling injuries can be the result of
lots of stresses and strains over time. Often the immediate cause is only part
of the picture.
The most commonly injured part of the body is the back, followed by the shoulder,
arm, hand and neck.
The following steps are required to reduce the number of injuries.
4.2.1 Identify the hazards
Identify manual handling hazards by:
• reviewing injury and near miss data
• reviewing potential manual handling problem areas and tasks during
workplace inspections
• talking to staff to find out what the difficult manual handling jobs are
• observing tasks, for example, pushing a linen trolley or shower chair with
poorly maintained wheels, getting a non-weight bearing resident out of
bed, moving beds around, lifting and carrying a pot of soup in the kitchen,
leaning over for long periods while feeding residents in bed or at a low
table, mopping floors for prolonged periods
4.2.2 Assess the risks
In consultation with Health and Safety Representatives and employees assess
the risk of each task. You can use a manual handling task risk assessment
(Form 4.1) or resident risk assessment (Form 4.2). Refer to your State Code
of Manual Handling Practice for more details.
4.2.3 Control the risks
Based on the risk assessment, consider options to control the risks (using
the four step ‘hierarchy of controls’ we looked at in Section 3.4, eliminate,
minimise, administrative strategies, personal protective clothing and
equipment (PPCE)).

Some examples include:
• ensure that bathroom design allows sufficient space for shower trolleys,
hoists and commodes
• install overhead railing, hoists in rooms used for heavy or non weight
bearing residents
• purchase height adjustable electric beds
• maintain all wheels on linen trolleys, commodes, hoists etc
• ensure that the wheels on trolleys are compatible with the floor coverings
• implement a No Lifting policy
(see Form 4.3 for an implementation checklist)
• select the appropriate lifting aid for the resident and the task (see
Table 4.1 for a selection table of aids for non-weight bearing and weight
bearing residents)
• provide height adjustable trolleys in kitchens
• reduce the size and weight of pots used in kitchens
• ensure washing machines and dryers are at a suitable height
4.2.4 Record actions
Record actions on the hazard log (Form 3.1) and/or OHS action plan
worksheet (Form 2.2) (longer term items).
4.2.5 Monitor/evaluate
Monitor and evaluate the controls selected. This should occur both before,
during and after implementing controls.
You can:
• re-do the task risk assessment with the control measure in place
• trial new equipment prior to purchase (for example beds, trolleys)
After controls have been implemented you can:
• monitor hazard reports, inspection reports and incident investigations
to see if the number reduces
• monitor Workers’ Compensation payments to see if they reduce
45OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry

46 OHS in Residential Aged Care First Steps
4.2.6 Case studies
Kitchen case study
A member of the kitchen staff working in an aged care facility noticed
that it was difficult to move bulk dry food and flour containers around
the kitchen. The bulk dry food and flour containers were very heavy
and because there was a shortage of storage space they had to be
pushed around the kitchen from time to time. The staff member let the
chef know that the containers were awkward to move and presented
a manual handling hazard.
The chef assessed the risk with the help of the staff member and
decided to take immediate action. She bought dolleys for the base
of the containers to make them easier to move around. The risk
was reduced. 4
In this case study the chef used the manual handling risk assessment
checklist (Form 4.1). She went through every question with the employee
who had to move the containers. Where the employee answered ‘yes’, they
knew they had a risk. In this case, it was lifting over 16 kg and pushing an
object which had an awkward shape in a restricted space. They worked out a
way to reduce the risk. By putting wheels on the containers they eliminated
the need to lift and made it easier to push. They still had the space problem
but the job was much improved. (In the longer term extra storage space was
planned to eliminate that problem).
No lifting approach case study
Cyril Jewell House is an aged care facility which introduced a ‘no
lifting approach’ as a result of staff, management and resident
consultation. The key to the success of the program is that all residents
are assessed on admittance by the physiotherapist and carers and a
plan established for minimising manual handling. The emphasis is on
the use of appropriate equipment for each resident taking into account
risk factors, resident condition and resident/family wishes. Daily care
requirements are detailed in the care plans. There is also a written
handover that highlights any changes in care plans.
As a result of the program, overhead lifting systems have been
installed in a number of rooms and others are planned. Overhead
systems are installed in the bathrooms and toilets while lifting and
standing machines and pivot boards are also available. All beds are
now of the adjustable height hydraulic type.
Induction and ongoing training in safe manual handling techniques
and use of equipment is provided for all staff.
The OHS objectives relating to the no lifting approach have been
incorporated into the centre’s quality improvement plan objectives. 5
Section 4 - Major hazards of the aged care industry
4&5 Hesta Better Health and Safety Case Studies, 1997, pp10-11

47OHS in Residential Aged Care First Steps
Form 4.1 – Sample Manual Handling Risk Assessment and Control Action Plan
Section 4 - Major hazards of the aged care industry
Part A. Task: Date:
Name:
(person(s) carrying out identification/assessment)
Position:
Part B. Description of activity and location
Include the way the activity fits in with the overall work process eg. getting residents out of bed as part of the process of
taking them to the bathroom or lifting heavy kitchen supplies as part of preparing meals
.
Part C. How was the task identified?
Hazard report ❑ Direct observation ❑Incident records ❑ Resident assessment ❑Consultation ❑
Part D. Movements and posture during Manual Handling
YES
1. Is there frequent or prolonged bending down where the hands pass below mid thigh
level of the employee? ❑2. Is there frequent or prolonged reaching above the head? ❑3. Is there frequent or prolonged bending due to extended reach forwards? ❑4. Is there frequent or prolonged twisting of the back? ❑5. Are awkward postures adopted that are not forward facing and upright? ❑
Part E. Task and load
YES
6. Is the manual handling performed frequently or for long periods of time by the employee? ❑7. Are the loads moved or carried over long distances? ❑8. Is the weight of the load:
a) more than 4.5 kg handled from the seated position? ❑b) more than 16 kg and handled in a posture other than seated? ❑c) more than 55 kg? ❑
9. Are large pushing or pulling forces required? ❑10. Is the load difficult or awkward to handle due to? ❑
a) size? ❑b) shape? ❑c) temperature? ❑d) instability? ❑e) unpredictability? ❑f) restricted vision? ❑
11. Is it difficult or unsafe to obtain adequate grip? ❑

48 OHS in Residential Aged Care First Steps
Form 4.1 – Sample Manual Handling Risk Assessment and Control Action Plan [cont]
Section 4 - Major hazards of the aged care industry
Part F. Work environment
YES
12. Is the activity performed in a restricted space (eg bathroom, hallway access)? ❑13. Is the lighting inadequate? ❑14. Is the climate hot or cold (eg is manual handling affected by bulky clothes, cold stiff ❑
hands or slippery perspiring hands)?
15. Are the floor surfaces cluttered, uneven, slippery or otherwise unsafe (eg ❑obstacles, electrical cords, rugs, ridges, carpeted making pushing/steering
difficult, steps)?
Part G. Individual factors
YES
16. Is the employee new to the work or returning from extended period away? ❑17. Are there age-related factors, disabilities, pregnancy factors? ❑18. Does the employee’s clothing, or lack of waterproof clothing, footwear or personal ❑
protective equipment interfere with manual handling performance?
Part H. Equipment
YES
19. Is equipment incompatible with furniture or other equipment? ❑20. Is equipment unsuitable for the task it is being used for? ❑21. Is equipment inefficient and slow to use? ❑22. Is equipment poor quality? ❑23. Is equipment difficult to use or understand how to use? ❑24. Is equipment poorly maintained? ❑25. Is equipment unavailable or difficult to obtain when needed? ❑
Part I. Work organisation
YES
26. Are there bottlenecks, deadlines or periods of peak activity? ❑27. Is the work affected by insufficient staff numbers to complete tasks within deadline? ❑28. Are there inefficiencies in the systems of work and/or double handling? ❑
Part J. Skills and experience
YES
29. Are employees untrained in manual handling? ❑30. Are employees untrained in recognition and reporting of risks? ❑31 Are employees untrained in how to perform specific tasks? ❑32. Has there been a failure to provide employees with an induction into work practices ❑
and safety requirements?
33. Are employees inexperienced in manual handling? ❑34. Are work demands beyond the physical capacity of employees? ❑

49OHS in Residential Aged Care First Steps
Part K. Risk control options
Consider short, medium and long-term solutions and record options.
Part L. Control strategy details and action plan
Record the control measures to be implemented, timeframe and person responsible.
Source: Adapted from Manual Handling Guide for Nurses, WorkCover NSW, 1998, p 12-15.
Section 4 - Major hazards of the aged care industry
Form 4.1 – Sample Manual Handling Risk Assessment and Control Action Plan [cont]

50 OHS in Residential Aged Care First Steps
Form 4.2 – Sample Resident Manual Handling Risk Assessment Checklist
Section 4 - Major hazards of the aged care industry
Physical function Mental status and cognition
❑ Control of arms and legs ❑ Aggression
❑ Weight ❑ Unpredictable
❑ Height ❑ Resisting
❑ Subluxed shoulder ❑ Confused
❑ Balance ❑ Agitated
❑ Tone ❑ Judgement
❑ Sensation ❑ Memory
❑ Vision ❑ Concentration
❑ Body awareness
❑ Hearing
❑ Range of movement
Medical Condition Communication
❑ Pain ❑ Ability to speak
❑ Fractures ❑ Ability to understand
❑ Medication ❑ Language barriers
❑ Recent change ❑ Body language
❑ Fatigue ❑ Confidence
❑ Delicate skin
Summary of factors affecting manual handling
Source: Adapted from the Queensland Nurses Union Back Pain Prevention Package & Manual Handling Guide for Nurses,WorkCover NSW, 1998, p 38
51OHS in Residential Aged Care First Steps
Form 4.3 – Sample No Lifting Policy Implementation Checklist‘No lifting’ is a new approach to resident handling. Rather than manual
lifting and moving of residents being improved through optimising manual
handling skills, manual handling of residents is minimised or eliminated
wherever possible. Any handling which involves manually lifting the whole
or substantial part of the resident’s weight is avoided. This is a much broader
approach to resident handling than has been taken in the past.
A no lifting approach involves:
• provision of mechanical lifting aids and equipment to assist carers to
move/transfer residents
• assessment of residents for their manual handling needs
• encouragement of resident mobility and independence
• education and training of staff in the correct use of aids and equipment and
in manual handling techniques (and ongoing assessment of staff manual
handling skills)
• consultation with staff in the trialling and purchase of equipment
• adequate levels of appropriately skilled staff
• workplace assessments and modifications to the workplace
Section 4 - Major hazards of the aged care industry
Checklist for the implementation of the no lifting policy
YES NO
Consultation
1. Have nurses and other relevant staff been consulted about the policy? ❑ ❑
Senior management commitment
2. Has senior management commitment been obtained to the establishment of ❑ ❑the no lifting policy?
3. Has budgetary commitment to the policy been obtained for equipment, training etc? ❑ ❑4. Has an audit been completed to establish the injury rates and related workers ❑ ❑
compensation costs?
External advice/assistance
5. Is it necessary to engage external assistance to establish/implement the policy ❑ ❑or provide advice?
Workplace structures, roles and responsibilities
6. Has someone been nominated to coordinate the approach and have roles of staff ❑ ❑members been defined?
7. Has a committee consisting of management and staff representatives been established ❑ ❑to develop policies and procedures and to oversee the implementation of the approach?

52 OHS in Residential Aged Care First Steps
Form 4.3 – Sample No Lifting Policy Implementation Checklist [cont]
Section 4 - Major hazards of the aged care industry
YES NO
Equipment
8. Has an audit of manual handling equipment been conducted to determine ❑ ❑equipment needs?
9. Have suppliers been contacted to provide advice and to arrange demonstrations ❑ ❑of equipment?
10. Has equipment been trialled? ❑ ❑11. Has equipment been selected and purchased in consultation with staff? ❑ ❑12. Is there a maintenance program for equipment? ❑ ❑13. Is there adequate appropriate storage space for equipment? ❑ ❑14. Is equipment easily accessible to staff? ❑ ❑
Staff training
15. Have staff been educated in the policy and procedures of the no lifting approach? ❑ ❑16. Have staff been trained in the correct use of equipment and manual handling techniques ❑ ❑
based on the no lifting approach? Has training been provided to all staff including casual
and agency staff?
17. Does an appropriate trainer/educator need to be engaged to provide the training? ❑ ❑18. Is the training competency based and does it include the no lifting approach? ❑ ❑
Resident/advocate information and education
19. Have residents and their families been informed of the approach and their ❑ ❑co-operation gained?
Worksite assessment
20. Has a worksite assessment of the work areas and the physical environment been ❑ ❑conducted to determine whether workplace modifications are required?
Staffing levels
21. Is there an adequate number of appropriately skilled staff to enable the no lifting ❑ ❑policy to be properly implemented?
Risk assessment of manual handling tasks
22. Have risk assessments of manual handling tasks been conducted and control ❑ ❑measures implemented?
23. Are the manual handling needs of residents assessed and are they incorporated ❑ ❑into individual resident care plans?
Cultural change
24. Have policies and procedures been established to ensure full compliance and cooperation ❑ ❑by staff with the no lifting procedures and manual handling methods taught in training?
Policy monitoring and evaluation
25. Have procedures been established for the evaluation of the policy? ❑ ❑
Source: Adapted from the ANF (Vic Branch) No Lifting Implementation Guide & Checklist, 1998.

53OHS in Residential Aged Care First Steps
Table 4.1 – Resident handling using hoists and non - mechanical aidsThe following information provides practical assistance to help with the selection
of appropriate equipment for lifting and moving residents. Hoists are obviously
very useful for handling people, but they are not always available. The following
tables provide assistance in selecting hoists and non-mechanical aids that can
assist carers to handle residents more safely.
1. Choosing a hoist for resident handling
2. Non-mechanical aids for weight bearing resident
★★★ Best available choice ★★ Can be done but involves some risk
★ Can be done but requires advanced skills No symbol indicates that the aid is not
applicable for this task.
Transfer type Buckle Belt Velcro Belt Blue Sling PAT slide Slide sheet
Chair to bed ★★★ ★★★ ★
Toiletting/commode ★★★ ★★★ ★
Repositioning in bed ★★ ★★★
Helping up from floor ★★★
Bed to trolley ★★★
Section 4 - Major hazards of the aged care industry
Task Stand up hoist General purpose “Process hoist”
hoist with chair
attachment etc
Lying in bed to use full harness applied useful for this task commode chair placed
chair commode, in lying to pull resident in bed
wheelchair up to sitting in bed
Bed to toilet with toilet useful useful
seat attachment
Dressing useful
Off the floor some hoists only; sling or Jordan boom attachment for
use four point sling frame attachment sling or Jordan frame
Into waterchair long booms only useful
Walking with fold up footboard
Complete bed to chair attachment,
bath, shower or no slings needed
toilet in hoist

54 OHS in Residential Aged Care First Steps
Table 4.1 – Resident handling using hoists and non-mechanical aids [cont]
3. Non-mechanical aids and hoists for non-weight bearing resident
Transfer type Hoist PAT slide Slide sheet
Chair to bed ★★★
Toiletting/commode ★★★
Repositioning in bed ✜ ★★★
Helping up from the floor ★★★
Bed to trolley ★★★
★★★ Best available choice
✜ Good for high dependency residents who require continuous repositioning. Need to ensure
that the sling is comfortable for continuous use.
Adapted from: Lifting and moving people: Choosing the right equipment, (1998) WorkCover NSW,
Catalogue no. 752
Section 4 - Major hazards of the aged care industry
55OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
4.3 Slips, trips and fallsSlips, trips and falls are a common cause of injury for employees working in aged
care facilities.
Statistics from the National Occupational Health and Safety Commission (NOHSC)
showed slips, trips and falls as a cause of injury increased from 10.8% of all injuries
in 1992-19936 to 15% in 1996-19977.
The 1992-1993 statistics showed that over 80% of falls were on the same level
caused by slips on wet or oily internal floor surfaces. The other 20% were classed
as falls from a height, such as down steps or stairs.
In order to reduce the number of injuries it is necessary to:
Identify the hazards
Identify potential slip, trip or fall hazards, for example, water on bathroom floors
and near outer doors, freezer rooms, or bedrooms where residents may be
incontinent when standing, worn or slippery steps or stairs. (Outside paths should
also be checked.)
Review injury/near miss data, talk to staff (to identify unreported near misses) and
review potential problem areas during workplace inspections. Record potential
hazards on a hazard report form (Form 3.2).
Assess the risks
Assess the risks of each potential hazard using the risk assessment table (Table 3.1)
Control the risks
Control the risks using the ‘hierarchy of controls’ (Section 3.4). For example:
• apply a non slip surface in bathrooms and kitchens
• ensure spills and wet floors are sign-posted and dried quickly
• clean vinyl corridors/floors in a way to allow a dry surface for walking
• mark the edges of steps and ramps (where needed)
• use non-slip mats (at doors and beside beds)
• prevent the use of talcum powder in bathrooms
• mop bathroom floors after use
• use non-slip shoes, rubber boots in bathrooms
Record actions required in the hazard log (Form 3.1)
6 WorkSafe Australia, “Occupational Health and Safety Performance Overviews, Selected Industries”, Issue No.7. Hospitals, Nursing Homes and Related Industries, July 1995, AGPS, Canberra.
7 Ellis N and Stiller L, “Evaluation of the National OHS Strategy for Residential Aged Care”. Draft report for the Commonwealth Department of Health and Aged Care, December 1998.

56 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
Monitor and evaluate
Monitor and evaluate the outcomes of the controls, for example, during reviews
of monthly data and workplace inspections
It may be necessary to implement short-term solutions while more expensive long-
term solutions are planned, for example, mopping the bathroom floor after each use
until non-slip tiles can be fitted.
4.4 Resident aggressionThe National Occupational Health and Safety Commission injury statistics for the
Aged Care Industry showed 7.2% (1992-1993) and 8% (1996-1997) of injuries were
as a result of being “hit by moving objects”. Over a third of the injuries within the
1992-1993 group were as a result of being hit by another person, either accidentally
or deliberately. It was believed there might be significant under-reporting, further
demonstrating that resident aggression is a major hazard within aged care facilities.
Reducing the risk of injuries requires a systematic approach including a number
of strategies. The strategies that need to be developed, in consultation with
staff, include:8
• identifying the causes of aggressive behaviour
• assessment of risks
• developing and implementing risk controls
• monitoring, evaluating and improving the strategies
4.4.1 Identify the causes of aggressive behaviour
Identifying the causes of aggression requires:
• a regular review of incident reporting (which depends on the use of
effective aggression incident report forms) to determine the time and details
of incidents, possible triggers and the severity of incidents (Form 4.4)
• ongoing review of the physical, personal and social needs of all residents
• review of the way work is organised, for example, are residents woken,
showered, toileted and fed rapidly, causing confusion and frustration?
4.4.2 Assess the risks
Following identification of the causes the next step is to assess the level
of risk, considering how severe the aggression is and how often staff are
exposed to the aggression. This will assist to prioritise the most serious risks.
8 Baptist Community Services and WorkCover NSW. “Managing Resident Aggression in Aged Care Facilities”. First edition, November 1998.

4.4.3 Develop and implement risk controls
Some examples of control strategies are outlined below:
Staff
• train managers in record keeping, analysing reports and
hazard management
• employee discussions and problem solving
• work in pairs/teams and avoid rotating employees between residents
• don’t wake residents suddenly and always approach them from the front
• provide training in identifying areas of work where aggression may occur,
actions to minimise risk, what to do during and after incidents and how to
prevent them
• train employees to protect themselves by defusing situations using
negotiation and anger management skills
• be aware of burnout and reducing fatigue or stress
• establish policies and procedures for emergency situations including
effective communication systems
• deal with the effects of aggression
• provide team and management support, for example, via team discussions
• provide access to debriefing and counselling services
• carry out ongoing monitoring and review of aggressive incidents
Residents
• find out resident likes and dislikes and plan care with their family
• plan activities to meet their needs and preferences
• review resident health – pain, effects of medication
• don’t rush or hurry residents
Environment
• use aromatherapy, music, pastel colours, pleasant pictures
• reduce potential weapons where possible, for example, sticks, frames,
furniture and fittings
• ensure clothing and footwear can be put on and removed easily
• provide a secure garden or walking area including points of interest
• keep the atmosphere as calm as possible, avoiding large gatherings
• minimise noise levels (for example, radios)
57OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry

Case study
St Catherines, a small aged care facility, identified resident aggression as a
significant OHS issue. Using a proactive approach they have created a calm
environment for residents and staff using aromatherapy with vapourisers
and scented oils, sensory boards and doll therapy. They play nature videos,
calming music and monitor the television to avoid loud game shows. They
have also painted the exit doorways to create scenic images.
Changes to resident routines are documented and short-term problem sheets
are read at the beginning of each shift.
These simple, cost effective initiatives have resulted in increased productivity
with happier staff and residents. There have been no staff injuries from
resident aggression in the last 12 months. 9
4.4.4 Monitor, evaluate and improve the strategies
It is also important that you monitor and evaluate the strategies used, and
look for ways to improve.
This requires:
• ensuring incidents are reported
• ongoing review and updating of systems/procedures
• team review of all aggressive incidents
• regular case reviews of all residents with challenging behaviour, focusing
on incidents and preventative measures
• ongoing review of training
58 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
9 SA WorkCover Corporation SAfer Industries Aged Care Industry Newsletter. Issue 2, April 1999, p2.

59OHS in Residential Aged Care First Steps
Your name:
Resident’s name:
Residential care facility/wing:
Date Time of incident Your sex Resident’s sex Has resident been
aggressive to you before?
/ / am/pm F ❑ M ❑ F ❑ M ❑ Yes ❑ No ❑
Tick what activity you were engaged in when the aggression occurred.
❑ Feeding ❑ Transporting ❑ Toileting
❑ Lifting ❑ Bathing ❑ Redirecting
❑ Turning ❑ Grooming ❑ Other activities
❑ Dressing/changing ❑ Awaking from sleep
Did the aggression come from the resident you were attending? ❑ Yes ❑ No
Tick the type of aggression involved.
❑ Hit ❑ Unwelcomed touching ❑ Hair pulling
❑ Punch ❑ Trip ❑ Pushing
❑ Scratch ❑ Yell (insult) ❑ Bent fingers back
❑ Kick ❑ Yell (noise) ❑ Bite
❑ Spit ❑ Abusive comments ❑ Throwing object
❑ Sexual harassment ❑ Offensive comments ❑ Grabbing
❑ Sexual comments ❑ Racial abuse ❑ Other
Were you injured? ❑ Yes ❑ No
If yes, please fill out an Incident/Injury Report.
In your opinion was there a “trigger” to this incident? ❑ Yes ❑ No
What was the “trigger” e.g. pain, other person, personal care?
Indicate the seriousness of the incident from your perspective by circling the appropriate number.
0 1 2 3 4 5
Not at all serious Extremely serious
Would you like to talk about this incident? ❑ Yes ❑ No
Section 4 - Major hazards of the aged care industry
Form 4.4 – Sample Aggression Incident ReportTo assist management to prevent resident aggression it is important that
employees record incident details on this form. It is vital that all employees’
concerns are addressed.
Source: WorkCover NSW/Baptist Community Services, “Managing Resident Aggression in Aged Care Facilities”, 1st edition, November 1998.

60 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
4.5 Plant and equipment hazardsExpected Outcome 4.5 (Criteria d) requires that equipment used is fit for the purpose
intended and well maintained and that staff are trained in its use. Examples of
equipment are hoists, wheelchairs, trolleys, vacuum cleaners, stoves, lawn mowers
and workshop tools.
Maintenance
You must have a maintenance system in place to ensure routine and preventative
maintenance is undertaken and recorded.
Your maintenance system should include:
• documentation of breakdown maintenance
• a documented program for routine preventative maintenance
• documentation of completed preventative maintenance including the date
and signature of the person who performed the task (including external
maintenance programs)
• records of work needed as a result of routine inspection and maintenance and
breakdowns for each item of equipment
Routine inspections and maintenance must be conducted by competent personnel,
and in line with suppliers’ recommendations and relevant State Standards
and Regulations.
Some equipment may not have a specified frequency of maintenance. You should
review relevant maintenance records and decide on a reasonable frequency period
for maintenance to make sure breakdowns are prevented, for example, servicing of
shower chair wheels.
‘Flagging’ dates for routine maintenance can be managed by a manual diary or
card system or on a computerised database.
Maintenance records must be reviewed regularly to ensure the maintenance has
been conducted and to identify a need for more frequent preventative maintenance
or replacement of equipment. This information will also be useful to guide you
when selecting new equipment.
Fit for purpose
Ensuring equipment is fit for the purpose requires you to use a number
of approaches including:
• purchase of suitable equipment
• assessment of the equipment and the task prior to use, for example, hoists
• training staff in the skills required to select the correct equipment

61OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
Purchase of suitable equipment requires a pre-purchase assessment to ensure it is
suitable for the task, the area in which it will be used and stored and for the people
who will use it.
A sample checklist has been included for you to adapt for this purpose (Form 4.5-
Selecting equipment-pre-purchase assessment, on the next page). Other more
detailed checklists are available from WorkCover NSW, for example for selecting
hoists or beds10. Australian Standards may also apply.
New equipment must be checked for safety on arrival and there must be a system
for the safe disposal of replaced equipment.
10 WorkCover NSW, Checklist for Evaluating Mobile Hoists (Catalogue Number 741)

Form 4.5 – Sample Selecting Equipment – Pre -purchase Assessment
Item: Date of Assessment/Trial:
Design
❑ Meets relevant Australian Standards?
❑ Durable and reliable?
❑ Easily cleaned and maintained?
❑ Compatible with existing environment/equipment e.g. hoists fit under beds, through doorways etc.?
❑ Easily manoeuvrable and adjustable (if applicable)?
❑ Controls and displays visible, legible, easily operable?
❑ Facilitates good postures/safe use in handling?
❑ Safe design e.g. no “pinch points”?
Performance
❑ Does it perform the required functions?
❑ What training is needed for correct use?
❑ Is training provided by the supplier?
❑ Does the item suit the residents e.g. weight, height, fragile skin etc?
❑ Does it provide enough support?
Usability
❑ What accessories are available?
❑ Can it be operated by one person?
❑ Is there adequate storage space?
❑ Is an emergency repair and maintenance service agreement available?
❑ Is a “user friendly” instruction manual provided?
❑ Is a trial period available?
❑ Brakes fitted (where necessary)?
Risk assessment
❑ All associated risks with equipment and parts identified and assessed?
❑ Would any alternative product be better?
Other Comments:
Checked by Maintenance Personnel:
Signature (Manager):
Signature (Employee Representative):
Adapted from QNU BackPain Prevention Package, 1990.
62 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry

63OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry
4.6 Living environmentExpected Outcome 4.4 of the Standards and Guidelines for Residential Aged Care
Services requires managers to actively work to provide a safe and comfortable
environment consistent with resident care needs, and to have the following policies
and practices in place (only those directly affecting OHS are included):
• grounds of the service are safe, well maintained and easily accessible
to residents, staff and visitors
• consideration of resident and staff needs in the management of environmental
risks and the development of safe work procedures
• a restraint free environment whenever possible
• any restraints be the least restrictive type possible and used only after all
reasonable alternatives are explored
• decisions to restrain made in partnership between the resident and/or
representative and the health care team
To achieve safe grounds you will need to identify any potential hazards, conduct
risk assessments and control the risks.
Potential hazards may include:
• uneven paths or ground surfaces
• low overhanging bushes or trees obstructing paths
• contents of garden or workshop sheds (which may contain tools and chemicals)
• poor lighting in carpark areas
Assessing the risks, as described earlier, will assist to prioritise required actions.
Risk controls may include:
• repair of uneven paths or ground surfaces
• regular trimming of bushes and trees
• keeping sheds locked to prevent access by residents or visitors
• improved lighting
• sitting areas (for residents to sit if tired)
• secure areas within the garden (if required)
When developing safe work practices and managing environmental risks you must
consider both resident and staff needs. For example, when setting up resident rooms
to ensure safety of staff and residents, or if fitting a keypad within secure areas to
prevent egress by residents, you need to consider and meet the egress needs of
independent residents, staff and visitors.
Making decisions to use resident restraints must, like other potential hazards,
be based on an assessment of risk to residents and staff.

Use the most effective, safest alternative based on the “hierarchy of control”
(Section 3.4) following agreed procedures and guidelines.
You must monitor and review the outcomes of the risk control strategies and
improve them if required.
4.7 Fire, security and other emergenciesExpected Outcome 4.6 of the Standards and Guidelines for Residential Aged Care
Services requires management to provide an environment and safe systems of work
that minimise fire, security and emergency risks, and to have the following policies
and practices:
Tick those you have in place
❑ clear instructions related to fire safety, security and other emergencies
❑ staff induction in fire safety and the use of security and emergency equipment
❑ training linked to legislative requirements and internal policies
❑ regular testing of fire and other emergency equipment
❑ evidence of regular fire, evacuation and other emergency drills
❑ participation of management, staff and residents in identifying and addressing fire, security andother emergency situations
❑ management and staff involvement in identifying and resolving security risks
❑ chemicals and dangerous goods identified, stored and used correctly
If you don’t have any of the above practices in place improvements must be made.
These improvements and the actions, timeframes and responsibilities should be
included in the OHS action plan worksheet (Form 2.2).
More detailed considerations based on the Standards and Guidelines for Residential
Aged Care Services are included in Fact Sheet 8.4 in Section 8.
64 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry

65OHS in Residential Aged Care First Steps
4.8 Infection controlExpected Outcome 4.7 of the Standards and Guidelines for Residential Aged Care
Services requires facilities to have an effective infection control program in place
including policies and practices which provide for:
• incident reporting mechanisms which are used and acted upon
• equipment fit for the purpose intended, well maintained and staff
trained in its use
• management and staff involvement in identifying and resolving infection
control risks
• the identification of sources of infectious waste and appropriate disposal methods
• surveillance programs
Infection control strategies must be integrated into your general OHS management
systems (section 5) and included in induction and ongoing training.
You will need to consider all possible sources of infection to identify potential
hazards including:
• resident equipment such as nebulizers, glucometers, dosettes
• wound and skin care
• continence management
• management of ‘sharps’
• food storage and handling
• laundry procedures
• infectious and general waste disposal
Conduct a risk assessment on any hazards you identify and implement controls
to minimise the risk of infection.
You will also need to monitor infections and use the information to identify the
root causes and the need for changing practices. For example, an increased number
of urinary tract infections may indicate a need to change care practices or to
increase the fluid intake of residents. Monitor and review the actions you take
to address infection control hazards to ensure they are effective.
You will need to develop policies and guidelines (in consultation with staff) to make
sure standard precautions are always met when:
• treating and caring for residents
• handling food
• cleaning and laundry tasks
• managing sharps and needle stick injuries
Additional precautions are recommended when a resident is infected and standard
precautions may not prevent transmission of infection.
Section 4 - Major hazards of the aged care industry
You must also take steps to prevent infections by the appropriate handling of waste
such as soiled linen, food waste, clinical (medical) waste including sharps,
containers of blood or body fluid.
You must identify infectious waste, isolate it if necessary, place it in safe containers
and dispose of it appropriately in order to prevent infection.
More detailed information resources on infection control are listed in the resource
section (Section 7).
4.9 SummarySection 4 has provided the information, strategies and tools needed to apply the
hazard management process in a practical way to address a number of hazards.
There are a large number of other hazards present in aged care facilities which must
also be addressed using the hazard management approach. Several of these are
included in the Practical Guide to OHS in Residential Aged Care.
Managing hazards is just one of the major factors which make up an effective OHS
management system.
Other factors include consideration of legislative compliance, education and staff
development, record keeping, injury management and continuous improvement.
These are discussed in Section 5.
66 OHS in Residential Aged Care First Steps
Section 4 - Major hazards of the aged care industry

67OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems
Occupational Health & Safetymanagement systems
5.1 IntroductionThis section of First Steps provides information about the relevant Expected
Outcomes of the Standards and Guidelines for Residential Aged Care Services, and
how they relate to OHS. It also provides strategies and tools for assisting you to
meet these requirements for accreditation.
It includes a description of:
• the relevant Expected Outcomes
• requirements for continuous improvement
• the need for compliance with OHS legislation
• education and staff development requirements and a checklist
• OHS record keeping requirements
Section 5 also includes a brief outline of some of the basic requirements for
Occupational Injury Management. While this is not a direct requirement of the
Standards and Guidelines it forms a crucial part of the management systems
related to OHS.
Managing OHS within small aged care facilities should be integrated into the
systems used for managing other aspects of the facility.
Standard 4 of the Standards and Guidelines for Residential Aged Care Services
outlines the requirements of the ‘physical environment and safe systems’. Standard 4
sets the framework for managing OHS in aged care facilities including the need for:
• a process of continuous improvement in managing OHS (Expected Outcome
4.1-see Section 5.2)
• compliance with the legislation (Expected Outcome 4.2-see Section 5.3)
• education and staff development (Expected Outcome 4.3-see Section 5.4)
• ensuring that the living and working environment is safe and comfortable for
residents (Expected Outcome 4.4-see Section 4.6)

• managing hazards (Expected Outcome 4.5-see Section 3)
• involving managers and staff in identifying and resolving OHS issues (Expected
Outcome 4.5-see Section 3)
• ensuring that incident reporting mechanisms are present, functional and acted
upon (Expected Outcome 4.5-see Section 3.6.3)
• consideration of OHS during the purchase of goods and equipment and
developing preventative maintenance programs (Expected Outcome
4.5-see Section 4.5)
• minimising risks of fire, security and other emergencies (Expected Outcome
4.6-see Section 4.7)
• ensuring that an effective infection control program is in place (Expected
Outcome 4.7-see Section 4.8)
5.2 Continuous improvementThe Accreditation Guide for Residential Aged Care Services (Appendix 1) defines
continuous improvement as ‘continuous review by managers, staff, residents and
carers of policies, practices and service outcomes to identify and implement
improvements for better outcomes’.
It defines the Continuous Improvement Cycle as ‘where a service demonstrates what
it is doing now to meet an expected outcome and what it is going to do to
continuously improve on its current practice and process’.
Diagram 1: Continuous improvement cycle11
11 “Standards and Guidelines for Residential Aged Care Services”. Commonwealth Department of Health and Family Services, May 1998.
68 OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems
Monitoring
Assessment
Follow up
FeedbackAction

The Accreditation Guide for Residential Aged Services (p. B1) describes a quality
service in the aged care industry as one which:
• reflects the needs of participants (residents, relatives and staff)
• is planned and documented appropriately
• provides staff development so each part of the work is understood and practised
• recognises the need for possible cultural change to improve quality
• is structured and operating as a total concept rather than ad hoc
• is continuously reviewing its operations on the basis of customer feedback
Continuous quality improvement in OHS in your facility is demonstrated if you
can show that you review what you currently do and what you are going to do
to improve on current practices and processes.
When reviewing what you currently do consider the following (this is not a
comprehensive list but examples only):
❑ are staff involved in OHS?
❑ are lines and forms of communication for OHS identified?
❑ does staff induction include OHS?
❑ are mechanisms in place for reporting or providing feedback on OHS hazards?
❑ are steps documented for reporting OHS hazards?
❑ are actions taken when OHS hazards are raised and is feedback provided?
❑ is OHS data collected?
❑ do staff know the reason for data collection and the process for collection?
❑ are quality improvement activities in place, including a review of documents,surveys and/or questionnaires, observation and checklists (workplace inspections)and suggestion boxes?
❑ is the OHS plan resourced and regularly reviewed to ensure objectives are met(and updated if needed)?
❑ are OHS policies and procedures reviewed and updated regularly?
❑ are OHS achievements recorded and reported to proprietors and boards e.g. vianewsletters, annual reports?
❑ is an effective injury management program in place?
69OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems

70 OHS in Residential Aged Care First Steps
Continuous Improvement of OHS 12
Improvement required What could we do? Possible ways to do it?
Increase staff Include OHS on the Agenda of Report OHS to staff, seek input
involvement with OHS staff meetings/quality meetings. e.g. to policies, procedures.
Identify lines/forms of Increase staff awareness of Develop flowchart of
communication for OHS how to report OHS issues. communication channels.
Display on OHS noticeboard.
Include OHS in induction Restructure induction to Use checklist of OHS issues to be
include OHS. included (from the Practical Guide.)
Implement mechanisms Develop a hazard report form Use sample Form 3.2 First Steps.
for reporting/feedback including the need for feedback. Discuss, adapt, implement.
on hazards Develop flowchart.
OHS data collection Define data to be collected. Adapt form 5.1 Use MSDS
Inform relevant staff e.g. collect, Register from the Practical Guide.
collate MSDS, monthly incidents.
Implement Quality Define OHS QI activities eg: Include required activities
Improvement (QI) activities • document reviews in OHS action plan.
• surveys, questionnaires
• checklists
• suggestions.
OHS plan resourced, Identify resources required for Obtain costs for training etc.
reviewed each step of plan. Set dates for Include in budget preparation.
review of plan e.g. monthly at Discuss progress, delays,
staff meeting. priority changes and document.
OHS Policy and Develop a list of policy/ Adapt form 6.2 to seek
Procedures reviews procedure review dates. staff input into Policy/
Procedures reviews.
Record OHS achievements - Define information to describe Include in reports and/
feedback to “stakeholders” achievements eg: or Resident/Staff Newsletters.
• purchase of new equipment
• changes to work areas etc.
Section 5 - Occupational Health & Safety management systems
If your facility doesn’t have these initiatives in place you should discuss
them with staff, develop possible actions to improve on the current practices
and processes and include them into the action plan worksheet in order to
continuously improve.
The following chart describes some possible strategies.
12 Adapted from NOHSC Small Business Management Training: Integrating Occupational Health and Safety Competencies, Commonwealth of Australia, 1999

71OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems
5.3 Compliance with OHS legislationThe Standards and Guidelines for Residential Aged Care Services require facilities to
comply with all legislation including OHS Acts and Regulations (Expected Outcome
4.2). Each State has its own OHS Act and Regulations which specifically state the
mandatory requirements for OHS in that State, and a number of Codes of Practice
which provide guidance on how to achieve the required standards. These should
be followed when developing and implementing hazard controls unless a solution
is found which is ‘equal to’ or ‘better than’ the Standard set within the Code
of Practice.
Specific OHS Legislation is listed in Section 7 (with telephone numbers if you
require copies of the relevant legislation). Summaries of some of the major
requirements of the OHS Acts and Regulations, that is, responsibilities and roles
of OHS committees and health and safety representatives are included in Fact
Sheets in Section 8. These may be used as reference and/or displayed on staff
notice boards.
In addition to OHS Legislation the facility must comply with the relevant State
Workers Compensation and Rehabilitation Acts and Regulations (available from the
State Authorities listed in Section 7).

5.4 Education and staff developmentExpected Outcome 4.3 and its criteria requires your facility to:
• identify and document the knowledge and skills required by your staff
to perform their jobs
• regularly assess staff to identify development needs
• monitor staff development activities and outcomes
OHS training should be integrated into the overall training program for professional
development and included in the business and/or OHS plan for your facility.
Individual State OHS legislation requires specific OHS training for health and safety
representatives, health and safety committees, managers, supervisors, first aiders,
those who undertake manual handling, those working with hazardous substances
and plant and others. Check the requirements with State Authorities.
The following checklist includes OHS issues which should be considered when
planning training. Any items which you don’t currently have in place should be
included in the OHS action workplan.
OHS Training Considerations
Tick those you have in place
❑ do job descriptions and specifications include OHS?
❑ is information about OHS available to staff?
❑ is a staff induction program incorporating OHS been developed and implemented?
❑ is a staff appraisal which identifies OHS educational needs in place?
❑ are the skills and knowledge of staff including OHS assessed?
❑ are resources allocated for staff development (including OHS)?
❑ is the internal education program based on training needs, for example changes
to processes, new equipment, OHS Legislation, future needs, manual handling and
accreditation standards?
❑ is there regular review of the education program, including OHS components?
❑ is there encouragement of external education?
72 OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems
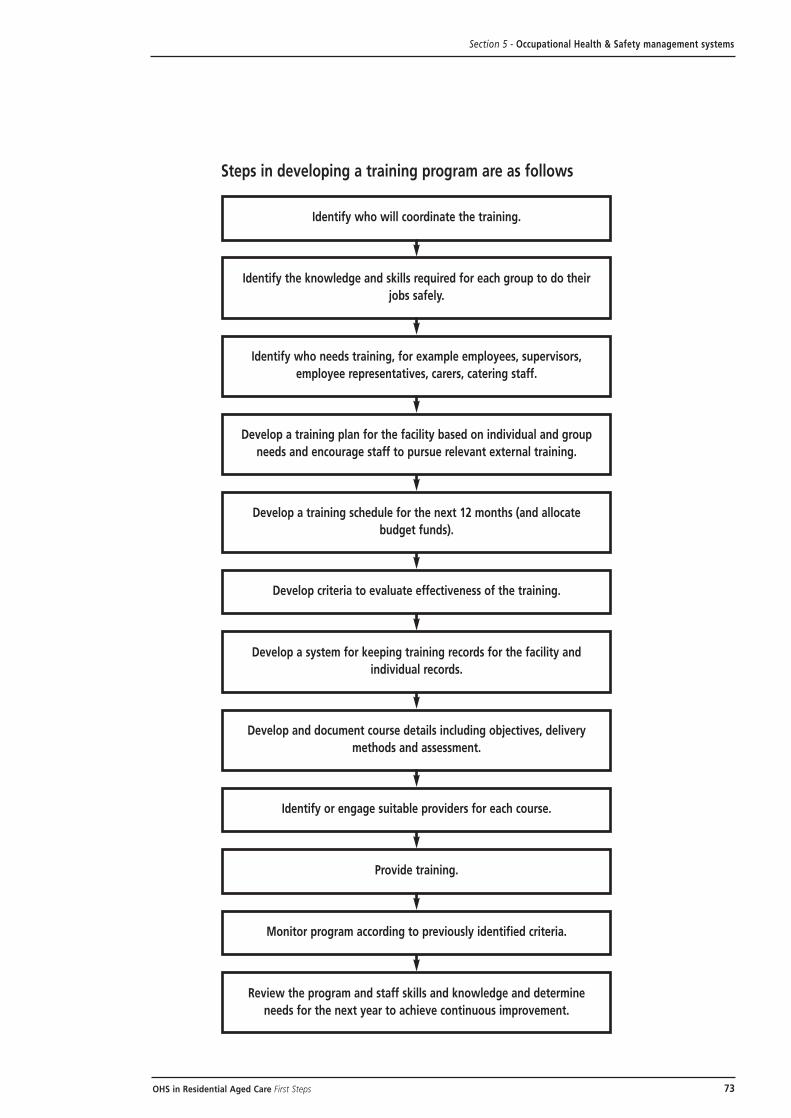
73OHS in Residential Aged Care First Steps
Steps in developing a training program are as follows
Section 5 - Occupational Health & Safety management systems
Identify the knowledge and skills required for each group to do their
jobs safely.
Identify who needs training, for example employees, supervisors,
employee representatives, carers, catering staff.
Develop a training plan for the facility based on individual and group
needs and encourage staff to pursue relevant external training.
Develop a system for keeping training records for the facility and
individual records.
Develop and document course details including objectives, delivery
methods and assessment.
Review the program and staff skills and knowledge and determine
needs for the next year to achieve continuous improvement.
Identify or engage suitable providers for each course.
Provide training.
Monitor program according to previously identified criteria.
Develop a training schedule for the next 12 months (and allocate
budget funds).
Develop criteria to evaluate effectiveness of the training.
Identify who will coordinate the training.

5.5 OHS records(Cross-references to Standard 1, Expected Outcome 1.8 - Information Systems)
Records must be kept for a range of OHS issues including those specified in
the legislation:
• *injury/incident reports and investigation
• *workers compensation and rehabilitation records
• *first aid records
• hazardous substances register
• material safety data sheets (MSDS)
• instruction/training records
• certificates and licenses
• major accident/incident notifications (to the OHS authority)
• health surveillance, atmospheric monitoring
• manufacturers and suppliers of OHS information (operating manuals etc)
• hazard report forms (and actions taken)
• workplace inspection/audit reports
• hazard log
• maintenance and testing results
• risk assessment reports
• evacuation exercise results
*These must be kept confidential with access only to authorised personnel
You should review and analyse the records regularly in consultation with staff
to assess the effectiveness of the OHS system and identify areas for improvement.
In addition, some records such as incident reports, types of injuries, first aid,
hazard reports and the hazard log should be reviewed regularly (for example
monthly) at OHS committee meetings or staff meetings. See Form 5.1 for a
sample recording sheet.
Other records would be monitored less frequently (for example, three to six
monthly) to ensure they are up-to-date, for example, that maintenance has been
completed as planned.
An overall review should be conducted on an annual basis to assess the suitability
of the records, to check compliance and identify areas for improvement.
74 OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems
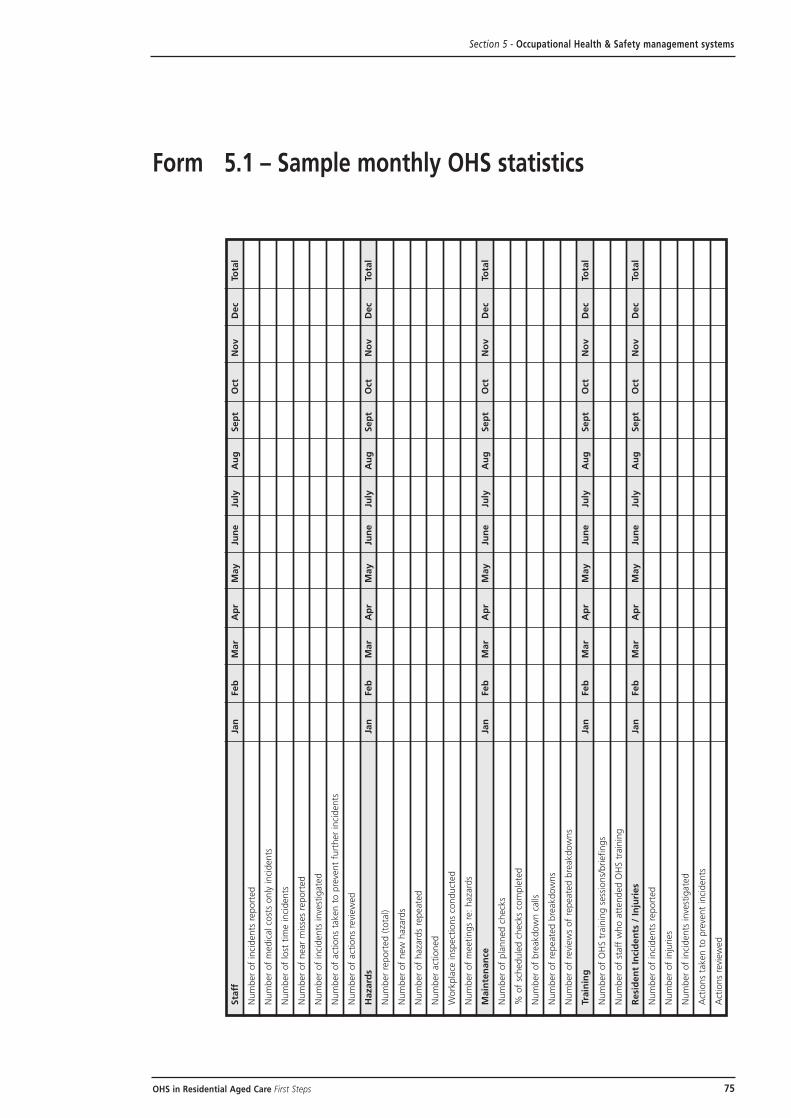
75OHS in Residential Aged Care First Steps
Sta
ffJa
nFeb
Mar
Ap
rM
ay
Jun
eJu
lyA
ug
Sep
tO
ctN
ov
Dec
Tota
l
Num
ber
of
inci
dents
report
ed
Num
ber
of
medic
al co
sts
only
inci
dents
Num
ber
of
lost
tim
e inci
dents
Num
ber
of
near
mis
ses
report
ed
Num
ber
of
inci
dents
inve
stig
ate
d
Num
ber
of
act
ions
taken t
o p
reve
nt
furt
her
inci
dents
Num
ber
of
act
ions
revi
ew
ed
Hazard
sJa
nFeb
Mar
Ap
rM
ay
Jun
eJu
lyA
ug
Sep
tO
ctN
ov
Dec
Tota
l
Num
ber
report
ed (
tota
l)
Num
ber
of
new
haza
rds
Num
ber
of
haza
rds
repeate
d
Num
ber
act
ioned
Work
pla
ce insp
ect
ions
conduct
ed
Num
ber
of
meetings
re:
haza
rds
Main
ten
an
ceJa
nFeb
Mar
Ap
rM
ay
Jun
eJu
lyA
ug
Sep
tO
ctN
ov
Dec
Tota
l
Num
ber
of
pla
nned c
heck
s
% o
f sc
hedule
d c
heck
s co
mple
ted
Num
ber
of
bre
akdow
n c
alls
Num
ber
of
repeate
d b
reakdow
ns
Num
ber
of
revi
ew
s of
repeate
d b
reakdow
ns
Train
ing
Jan
Feb
Mar
Ap
rM
ay
Jun
eJu
lyA
ug
Sep
tO
ctN
ov
Dec
Tota
l
Num
ber
of
OH
S t
rain
ing s
ess
ions/
briefings
Num
ber
of
staff
who a
ttended O
HS t
rain
ing
Resi
den
t In
cid
en
ts /
In
juri
es
Jan
Feb
Mar
Ap
rM
ay
Jun
eJu
lyA
ug
Sep
tO
ctN
ov
Dec
Tota
l
Num
ber
of
inci
dents
report
ed
Num
ber
of
inju
ries
Num
ber
of
inci
dents
inve
stig
ate
d
Act
ions
taken t
o p
reve
nt
inci
dents
Act
ions
revi
ew
ed
Form 5.1 – Sample monthly OHS statistics
Section 5 - Occupational Health & Safety management systems

5.6 Occupational injury managementWhile the major focus of First Steps is to assist facilities to prevent injuries
occurring, it is also important to have an effective system in place to manage
injuries if they do occur.
The detailed legal requirements for claims management and rehabilitation vary
between States, so it is essential to contact your local regulatory authority, claims
agent or insurer for more information (see Section 7).
An injury management program aims to achieve a timely, safe and durable return to
work for injured employees. It needs to be tailored to the facility and integrate all
aspects of injury management including:
• treatment of the injury
• claims management
• rehabilitation
• return to work programs
• retraining
Generally one person will manage the rehabilitation process (this is a legal
requirement in some States). This may be an injury management or rehabilitation
co-ordinator or the director of care/facility manager.
Injury management should commence immediately after an injury occurs and be
an active process, aiming for early return to work. Effective injury management
depends on well informed employees, managers, treating doctors and other
professionals and insurers. To achieve this it is important to have:
• an injury management policy and procedures
• an employee information sheet
• authority for release of information between the people involved in rehabilitation
• a letter to the treating doctor providing information about the employee’s normal
position and duties and information about suitable alternative duties available
at the facility
The steps in injury management (following immediate treatment and accident
reporting/investigation) are as follows in Flowchart 5.1 on the next page.
76 OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems

77OHS in Residential Aged Care First Steps
Flowchart 5.1 Injury management process
Specific details of the process and examples of documentation are included
in the Practical Guide and the Occupational Injury Management in Aged
Care Facilities Manual (Department of Health and Aged Care) 1999.
Section 5 - Occupational Health & Safety management systems
Injured employee assessed
by coordinator
Establish individual rehabilitation
file (if off more than 7 days)
Initial and ongoing contact
made with relevant doctor,
insurer, supervisor and
injured employee
Develop a Return
to Work Plan
Ongoing monitoring/
review of progress
Once injury management
goals are met - close file
Review/improve Injury
Management Program

5.7 SummarySection 5 has provided some information, strategies and tools to assist you to set
up, review and/or improve OHS management systems within your facility.
Implementing or improving these systems will assist you to take further steps
towards meeting the requirements of accreditation.
Section 6 will assist you to consider the actions you have taken or planned as a
basis to prepare you to complete the OHS related information in the Application
Kit for Accreditation.
78 OHS in Residential Aged Care First Steps
Section 5 - Occupational Health & Safety management systems
79OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation
Occupational Health andSafety review – preparing for accreditation
6.1 IntroductionFirst Steps has provided you with information on how to:
• assess where your facility is in terms of OHS
• develop goals of where it wishes to be
• develop action steps for ‘how to get there’ and what needs to be done
• develop performance measures to assist in measuring success
If you have worked through the process of addressing the gaps identified in the
self-assessment checklist, it is now time to review performance and prepare for
completing Worksheet 4.5 in the Application Kit for Accreditation.
Section 6 provides the strategies and tools to lead you through the process
of reviewing your progress to date and using the information to prepare
for accreditation.
6.2 Reviewing progressThe first step is to repeat the self-assessment checklist (Form 2.2) from
Section 2 of First Steps. You should now be able to answer ‘yes’ to a greater
number of questions.
6.3 Preparing for accreditationIn preparation for completion of the Application Kit for Accreditation the next
step is to review in more detail ‘what we say we do’ and ‘what we do’ to achieve
Expected Outcome 4.5, to review the results and determine how to improve. The
outcomes may be recorded on the Standards Review form (Form 6.1 on the
next page).

80 OHS in Residential Aged Care First Steps
Expected Outcome
(Description as per Accreditation Manual):
1. What do we say we do to achieve this outcome?
• What policies are in place to address the criteria of this outcome?
List Date of Release/Review
• Is each policy clear and understandable? Yes ❑ No ❑• Is each policy current and correct? Yes ❑ No ❑• Is each policy practical? (can
be followed in the daily course of events). Yes ❑ No ❑• What other written materials address this outcome?
(e.g. staff and resident handbooks, procedures,
orientation information, standard operating
procedures etc).
List Date of Release/Review
Do these agree with or conflict with the policies on this issue?
❑Agree
❑Conflict-Initiate a continuous improvement form with suggestions to remedy the conflict.
Record actions required in the OHS action plan.
Form 6.1 - Sample Standards Review Form - Preparing for Accreditation
Section 6 - Occupational Health & Safety review - preparing for accreditation

81OHS in Residential Aged Care First Steps
2. What do we do to address this outcome?
• What evidence shows we do these things?
List with dates:
• minutes of meetings
• memos
• audits, surveys, inspections
• suggestions e.g. hazard forms, follow-ups
• anything else
List Date
• Is what we do consistent with what we say (see question 1)?
❑ Yes
❑ No - Initiate a continuous improvement form advising of problems and suggestions to bring policies
and practices into agreement. Record actions required in the OHS action plan.
3. What are the results of what we say and do?
4. How can we improve on what we say and do to achieve this outcome?
Source: Carla Baron, N&C Baron & Associates
Form 6.1 - Sample Standards Review Form – Preparing for Accreditation [cont]
Section 6 - Occupational Health & Safety review - preparing for accreditation

Expected Outcome 4.5 requires management to actively work to provide a safe
working environment that meets regulatory requirements.
Reviewing and improving OHS requires consideration of:
• management of hazards
• involvement of management and staff in resolving OHS issues
• incident reporting (and actions taken)
• equipment fit for purpose
Each of these key requirements have been described within First Steps, and
strategies and sample tools provided to assist you to improve the management
of OHS within your facility.
You may have implemented some of these strategies or plan to do so and these
activities will assist you to complete Worksheet 4.5 in the Application Kit for
Accreditation and to consider steps required to achieve continuous improvement.
The improvements may require a staged approach.
Suggestions for how you may consider these stages and complete Worksheet
4.5 follow.
These are not a complete list and you will need to consider the specific needs
of your facility to complete the worksheet.
82 OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation
83OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation
6.3.1 Criteria (a) – Managing the Risks – 1st StageThis assumes risk management is currently ad hoc.
Objective
To put in place a planned program to fix urgent problems which
present a risk.
How will we improve ‘what we say we do’?
• Develop a procedure for identifying hazards
• Implement a risk assessment tool
• Develop a hazard log
• Document the process for eliminating or minimising risk
How will we improve ‘what we do’?
• Conduct a hazard audit to identify all hazards
• Ask employees about their hazards
• Make a list and assess the risk, to rank in order of importance
• Brainstorm ideas for fixing them
• Document and implement the urgent and/or easy things
• Develop an action plan for the longer term issues
Measures of success (the improved results)
• Most urgent hazards have been addressed
• Number of hazards addressed i.e. risks eliminated or minimised
• Number of solutions implemented to plan i.e. within timeframes
• Level of interest/involvement of staff
• Level of resources provided by managers
Continuously improving
• Check the changes are made according to the action plan worksheet
(and that they fixed the problem)
• Understand why solutions didn’t work - develop an alternative solution
Once these improvements are made you can plan a second stage of improvement to
move to a more systematic approach to managing risks (this may take 3-6 months
or more depending on the size and complexity of your facility).

6.3.1 Criteria (a) – Managing the Risks – 2nd StageMoving to more Systematic Approach.
Objective
To implement a program to address high risk issues and establish a systematic
approach to identifying and addressing hazards.
How will we improve ‘what we say we do’?
• Develop a procedure to conduct regular workplace inspections
• Develop a checklist for the inspections
How will we improve ‘what we do’?
• Train staff in conducting inspections
• Conduct regular inspections, identify new hazards and ensure controls are in
place for previously identified hazards
• Regularly adjust and extend the list of hazards in the hazard log based on
the inspections
• Build a plan that addresses the risks (high risk items first)
Measures of success (the improved results)
• List of hazards regularly being amended
• Level of OHS expertise increasing
• Manager provides necessary resources
• Number of successful solutions implemented
• Documented inspection system
• Increased employee involvement in regular inspections
Continuously improving
• Quarterly review of the inspection system and documentation to see if it can
be improved
• Implement action plan and check that the changes are made according to the
plan and actually fix the problems identified
• Quarterly review/update of the action plan
Once the second stage requirements are met you can then move onto the third stage
of systematically addressing the major risks.
84 OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation

6.3.1 Criteria (a) – Managing the Risks – 3rd Stage
Objective
To systematically address all major hazards.
How will we improve ‘what we say we do’?
• Develop/adopt hazard specific policies and procedures e.g. manual handling,
hazardous substances, UV radiation (outdoor workers), resident aggression,
occupational stress etc
How will we improve ‘what we do’?
• Implement a ‘No Lifting’ policy
• Implement a program to address challenging behaviour etc
Measures of success (the improved results)
• Reduction in manual handling injuries/incidents
• Implementation of ‘No Lifting’ strategy
• Reduction in resident aggression incidents
Continuously improving
• Monitor compliance with ‘No Lifting’ policy and address reasons
for non-compliance
• Review suitability of hoists and identify need for additional equipment
• Review outcomes of resident aggression prevention strategies
See First Steps Section 4 and the Practical Guide for further assistance.
85OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation

6.3.2 Criterion (b) – Involving Employees – 1st StageAssuming employee involvement in OHS is ad hoc.
Objective
To develop a structure to involve employees in OHS.
How will we improve ‘what we say we do’?
• Include employee involvement in OHS procedures, for example, risk assessment
and control etc
How will we improve ‘what we do’?
• Add OHS to agenda of staff meetings, discuss OHS issues and
record outcomes
• Involve employees in workplace inspections
• Encourage employees to report hazards
Measures of success (the improved results)
• Most urgent hazards have been addressed
• Increased number of hazards reported
• Employees involved in all workplace inspections
• Increased employee input into solutions for hazards
• Increased level of interest/involvement of staff
Continuously improving
• Check OHS has been discussed at all staff meetings
• Check whether employee input into risk controls has been recorded
Once employee involvement is set up you can plan to move to a second stage, more
systematic approach to employee involvement.
86 OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation
6.3.2 Criterion (b) – Involving Employees – 2nd StageMoving to a more systematic approach.
Objective
To implement a structure for employee involvement in OHS.
How will we improve ‘what we say we do’?
• Develop a procedure and flowchart for the process of consultation, for example
regarding changes to the workplace, work processes, equipment (see the
Practical Guide for an example)
How will we improve ‘what we do’?
• Consider the need to implement an OHS committee or elect a health and safety
representative/employee representative (see the Practical Guide and relevant
OHS legislation for more details)
Measures of success (the improved results)
• Employee involvement in OHS initiatives documented
• OHS discussed regularly (and input sought from employees) e.g. at staff
meetings, via OHS committee etc
• Increased level of interest/involvement of staff
Continuously improving
• Review whether involvement strategies have been successful e.g. increased
hazard reporting, OHS suggestions, input into procedures etc
87OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation

6.3.3 Criterion (c) – Reporting and Acting on IncidentsAssuming there is under-reporting of incidents, for example, serious injuries
only reported.
How will we improve ‘what we say we do’?
• Review the current incident report form and any procedure e.g. is it readily
available, user friendly, provides the required information?
• Review the incident investigation procedure (if available)
• Adapt the form/s and procedures to be more user friendly
• Include incident reporting in the induction program (see the Practical Guide)
How will we improve ‘what we do’?
• Make the incident report form more accessible/simple to use
• Train employees in how to complete the form and when
• Investigate all incidents
• Discuss incidents (maintaining confidentiality) at staff meetings and address
outstanding issues
Measures of success (the improved results)
• Number of incidents reported
• % of incidents investigated and actions taken
• % of incidents discussed at staff meetings/OHS committee
• All new staff receive instructions on incident reporting
• Most urgent hazards addressed
Continuously improving• Regularly review the suitability of the incident report form
• Review incidents and trends at staff meeting/OHS committee and develop
strategies to address hazards
88 OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation

6.3.4 Criterion (d) – Equipment Fit for Purpose – 1st StageAssuming equipment management is ad hoc.
Objective
To put in place a planned program to fix urgent problems with equipment which
may present a risk.
How will we improve ‘what we say we do’?
• Develop a procedure for regular checking of equipment
• Develop an equipment inspection log (see the Practical Guide)
How will we improve ‘what we do’?
• Commence a regular equipment inspection/service schedule (by
competent persons)
• Keep and review records to ensure compliance
• Train staff in the selection of appropriate equipment for the task
Measures of success (the improved results)
• Equipment log developed
• Inspection/service schedule commenced
• Improved selection of equipment for tasks
• % of checks conducted (of those planned)
Continuously improving
• Check the equipment is in good order e.g. are checks frequent enough?
• Quarterly checks of schedule
• Review of training provided/required
Once these basic systems are implemented to ensure equipment is fit for the
purpose, you may plan to move to a second stage with a more systematic approach.
89OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation

6.3.4 Criterion (d) – Equipment Fit for Purpose – 2nd StageMoving to a more systematic approach.
Objective
To implement a systematic program to ensure that all equipment is fit for the
purpose, well maintained and that staff are trained in its use.
How will we improve ‘what we say we do’?
• Develop a procedure to be followed when purchasing new equipment (including
consultation and pre-purchase reviews)
• Include specific details of equipment to be used in care plans e.g. manual
handling equipment or in Standard Operating Procedures for laundry, kitchen,
garden equipment
• Write a procedure to be followed for faulty equipment
• Develop a training record matrix for specific equipment
How will we improve ‘what we do’?
• Trial new equipment before purchase
• Select and use appropriate equipment day-to-day
• Train staff in equipment hazard identification, risk assessment and control
Measures of success (the improved results)
• Equipment used as per care plans/Standard Operating Procedures
• Equipment checked/serviced as per schedule
• % repairs/modifications of equipment recorded
Continuously improving
• Quarterly checks of schedule
• Adapt frequency of checks if indicated e.g. if frequent breakdown maintenance
is required between checks
The process described above could be followed for each worksheet within the
Application Kit for Accreditation. As OHS is integrated into a number of other
activities within the facility, OHS will be referenced in a number of the worksheets.
90 OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation
6.4 Continuous improvementOngoing reviews of OHS are essential to achieve continuous improvement. This will
include regular review of the components of OHS, for example:
• monthly reviews of hazard reports, incident report forms, types of injuries
• annual review of the overall system using the self-assessment checklist
• review of compliance with OHS legislation
• regular review of OHS policies and procedures, for example, annually.
A sample review form is included (see Form 6.2 on the next page) which can be
used to obtain staff input.
This information then feeds into the review form (Form 6.1) which will assist you to
prepare for completion of the Application Kit for Accreditation. A separate review
may be completed for each Expected Outcome during preparation for accreditation.
The outcomes of these reviews will then form the basis of your annual OHS plan
which may be a separate plan or be incorporated into the overall business plan for
the facility.
As you progress beyond the steps included in First Steps, further assistance for
continuously improving can be found in the Practical Guide.
If you require specific OHS information contact your employer organisation, union
or the OHS Authorities listed in Section 7 or refer to the additional resources listed
in Section 7.2.
Networking with other small facilities (and larger ones) will also provide a valuable
source of information and possibly allow for joint problem solving.
91OHS in Residential Aged Care First Steps
Section 6 - Occupational Health & Safety review - preparing for accreditation

92 OHS in Residential Aged Care First Steps
Form 6.2 - Sample OHS Policy/Procedure Document Review
Section 6 - Occupational Health & Safety review - preparing for accreditation
Name of Policy:
You are asked to review the attached Policy and complete the following:
Yes No
Do you believe the Policy is clear and understandable? ❑ ❑Is the Policy current and correct? ❑ ❑Is the Policy practical - that is can it be followed in daily practice? ❑ ❑
Comments/Suggestions:
Name (optional)
Source: Carla Baron, N&C Baron & Associates

93OHS in Residential Aged Care First Steps
Section 7 - Resources
Resources
7.1 Legislation
Australian Capital TerritoryOccupational Health and Safety Act 1989
New South WalesOccupational Health and Safety Act 1983
Northern TerritoryWork Health Act 1986
Work Health (Occupational Health and Safety) Regulations 1992
QueenslandWorkplace Health and Safety Act 1995
Workplace Health and Safety Regulations 1997
South AustraliaOccupational Health Safety and Welfare Act 1986
Occupational Health Safety and Welfare Regulations 1995
TasmaniaWorkplace Health and Safety Act 1995
Workplace Health and Safety Regulations 1998
VictoriaOccupational Health and Safety Act 1985
Occupational Health and Safety Regulations (contact information Victoria
Phone: 1300 366 356 for the full list of Regulations)
Western AustraliaOccupational Safety and Health Act 1984
Occupational Safety and Health Regulations 1996
• Each State also has a range of Codes of Practice and Guidelines. Contact your
OHS Authority to obtain a list of those which are relevant to your facility.
94 OHS in Residential Aged Care First Steps
Section 7 - Resources
Commonwealth Statutory Body
National Occupational Heath and
Safety Commission
92 Parramatta Road
Camperdown NSW 2050
Switch: (02) 9577 9555
1800 252 226 (outside Sydney)
Fax: (02) 9577 9202
http://www.worksafe.gov.au
Australian Public ServiceOHS Agency
COMCARE Australia
CFM Building, 12 Moore Street
Canberra ACT 2601
Switch: (02) 6275 0000
1300 366 979
Fax: (02) 6257 5634
http://www.comcare.gov.au
State & Territory GovernmentOHS Agencies
New South Wales
WorkCover Authority of NSW
400 Kent Street
Sydney NSW 2000
Switch: (02) 9370 5000
1800 451 462
Fax: (02) 9370 6120
http://www.workcover.nsw.gov.au
Western Australia
WorkSafe Western Australia
1260 Hay Street
West Perth WA 6005
Switch: (08) 9327 8777
Fax: (08) 9321 8973
http://www.safetyline.wa.gov.au
Victoria
Victorian WorkCover Authority
222 Exhibition Street
Melbourne VIC 3000
Switch: (03) 9641 1555
1800 136 089 (Vic only)
Fax: (03) 9641 1222
http://www.workcover.vic.gov.au
Australian Capital Territory
ACT WorkCover
3rd Floor
FAI House
197 London Court
Civic ACT 2601
Switch: (02) 6205 0200
Fax: (02) 6205 0797
http://www.act.gov.au
South Australia
WorkCover Corporation
100 Waymouth Street
Adelaide SA 5000
Switch: (08) 8233 2222
1800 888 508 (all States)
1800 188 000 (SA only)
Fax: (08) 8233 2466
http://www.workcover.sa.gov.au
Workplace ServicesDepartment for Administrative and
Information Services
Level 3, 1 Richmond Road
Keswick SA 5035
Switch: (08) 8303 0400
1800 777 209 (a/h emergency)
Fax: (08) 8303 0400
http://www.eric.sa.gov.au
7.2 OHS authorities/contacts

95OHS in Residential Aged Care First Steps
Section 7 - Resources
Tasmania
Workplace Standards Tasmania
Department of Infrastructure,
Energy & Resources
30 Gordons Hill Road
Rosny Park TAS 7018
Switch: (03) 6233 7657
1300 366 322 (TAS only)
Fax: (03) 6233 8338
http://www.wsa.tas.gov.au
Queensland
Division of Workplace Health
and Safety, Department of Training
and Industrial Relations
75 William Street
Brisbane QLD 4000
Switch: (07) 3247 4711
1800 177 717
Fax: (07) 3220 0143
http://www.detir.qld.gov.au
Northern Territory
Work Health Group
Minerals House
66 The Esplanade
Darwin NT 0800
Switch: (08) 8999 5010
1800 019 115
Fax: (08) 8999 5141
http://www.detir.gov.au/wha
Standards Australia
Head Office
1 The Crescent
Homebush NSW 2140
Information Centre (02) 9746 4748
Sales: (02) 9746 4600
Office in each State
7.2 OHS authorities/contacts [cont]

96 OHS in Residential Aged Care First Steps
Section 7 - Resources
7.3 Hazard specific informationThe following is not an exhaustive list of available resources but rather a guide
to assistance available in relation to the identified subject areas.
Infection control
Infection Control in the Health Care Setting. Guidelines for the prevention of
transmission of infectious diseases. National Health and Medical Research Council.
Government Info Shop, 10 Mort Street, Canberra ACT 2600. Ph: (02) 6247 7211,
Fax: (02) 6257 1797.
NSW Health Training and Information: Infection Control Resource Kit. Ellis and
Associates for NSW Health. September 1996. Ph: (02) 9332 1090.
Residential Aged Care Guidelines for Infection Control. Leaver M (ed). Kimberly
Clark Corporation. January 1999. For orders Ph: (02) 9963 8061.
Resident aggression
Management of Aggression Training Manual. Management of Client Aggression in
Aged Care. Port Adelaide Central Mission Inc, WorkCover Corporation South
Australia, GPO Box 2668, Adelaide SA 5001. Ph: (02) 8233 2222.
Managing Resident Aggression in Aged Care Facilities. Baptist Community
Service/WorkCover NSW. 1st ed November 1998. Ph: (02) 9370 5000.
Guidelines for Reducing the Risk of Violence at Work - includes a brochure
“Managing the Risks of Violence in Aged Care Facilities”. WorkCover Corporation
South Australia, GPO Box 2668, Adelaide SA 5001. Ph: (02) 8233 2222.
Manual handling
Manual Handling Codes of Practice (Contact State WorkCover).
Strategies to Reduce the Risk of Back Strain in Nursing Homes. WorkSafe WA,
1993. (See http://www.safetyline.wa.gov.au)
Manual Handling Guide for Nurses. NSW Nurses Association, WorkCover NSW.
September 1998. Ph: (02) 9550 3244.
Manual Handling Competencies for Nurses. NSW Nurses Association, WorkCover
NSW. September 1998. Ph: (02) 9550 3244.
No Lifting Implementation Guide and Checklist. Australian Nursing Federation
(ANF) (Victorian Branch) 1998. Ph: (03) 9275 9333.
Guidelines for Implementing No Lifting. Australian Nursing Federation (ANF) (SA
Branch) 1999. Ph: (08) 8363 1948.

No Lifting by the Year 2000 - Health and Safety Yearbook 1998. Queensland
Nurses Union, 1998. Ph: (07) 3840 1444.
Lifting and Moving People: Choosing the Right Equipment. WorkCover New South
Wales November 1998, Catalogue No. 752. Ph: (02) 9370 5000.
Designing Workplaces for Safer Handling of Patients/Residents - Guidelines for
the Design of Health and Aged Care Facilities. Victorian WorkCover Authority,
August 1999. Ph: (03) 9641 1555 (Publications).
Prepurchase Criteria to use in the Selection of Equipment and Furniture - Health
and Aged Care. Victorian WorkCover Authority, November 1998. See
http://www.workcover.vic.gov.au. Look under special projects- Aged Care
and Health.
Criteria for Evaluating the Core Elements that Support a Best Practice
Patient/Resident Handling Training Program in the Health and Aged Care Sector.
Victorian WorkCover Authority, December 1998. See
http://www.workcover.vic.gov.au. Look under special projects - Aged Care
and Health.
Checklist for evaluating beds for the health industry. WorkCover NSW 1998,
catalogue No. 742. Ph (02) 9370 5000
Checklist for evaluating mobile hoists. WorkCover NSW 1997, catalogue No. 741.
Ph (02) 9370 5000
Lifting and moving people: choosing the right equipment. WorkCover NSW 1998,
catalogue No. 752. Ph (02) 9370 5000
Other resources
Guidelines for the Management of Loss and Grief in the Aged Care Industry
(Draft). WorkCover NSW, June 1999. Ph: (02) 9370 5000.
97OHS in Residential Aged Care First Steps
Section 7 - Resources


Section 8 - OHS Fact Sheets
99OHS in Residential Aged Care First Steps
OHS Fact Sheets
8.1 OHS legal requirements
OHS Acts
Occupational Health and Safety Acts in each State of Australia (see Section 7 for a
complete list) place a general duty of care on the employer and employees in the
workplace and also on anyone who designs, manufactures, imports or supplies any
plant or substances to a workplace.
The Acts (which differ slightly between States) also cover issues such as how to
resolve OHS issues and the roles of (and election process where applicable) for
health and safety committees and representatives.
OHS regulations
OHS Regulations in each State set out specific requirements and standards,
which must be met. They relate to physical hazards, systems of work and/or
administrative matters.
Codes of Practice
Codes of Practice provide practical guidance that should be followed unless there
is another way to get an equal or better outcome. There is a varied number of
Codes of Practice in each State covering a range of issues e.g. Manual Handling
Code of Practice.
Guidelines
A range of Guidelines are published by State OHS Authorities and the National
Occupational Health and Safety Commission. These generally address specific
hazards and provide assistance to meet the requirements of the Acts, Regulations
and Codes of Practice.
Australian Standards
Australian Standards also provide direction about a range of OHS issues. They must
be followed if they are referenced in the Regulations. They may also be referenced
as a Code of Practice.

8.2 OHS responsibilities
Employer responsibilities
The wording of employer responsibilities within the Acts of each State varies but
in summary employers are required to:
• provide and maintain a safe working environment
• provide safe systems of work
• provide information, instruction and supervision of employees to ensure safety
• ensure the safe use, storage and handling of plant, equipment and substances
• provide adequate facilities for staff
• consult with employees/Health and Safety Representatives about OHS
• identify, assess and control hazards
Employee responsibilities
Employee responsibilities defined in the OHS Acts vary slightly between States but
in summary they are to:
• take reasonable care to ensure their own safety
• not place others at risk by any act or omission
• follow safe work procedures
• use and care for equipment as instructed
• not wilfully or recklessly interfere with safety equipment
• report hazards and injuries
• co-operate with the employer to meet OHS obligations
Managers and supervisors OHS responsibilities
Managers and supervisors have responsibilities on behalf of the employer, but must
also comply with their requirements as employees. It is their responsibility to:
• act as role models
• ensure employees have the information, instruction, training and supervision they
need to work safely
• consult with employees (and representatives) on proposed changes
• identify, assess and control hazards
• maintain a safe working environment
100 OHS in Residential Aged Care First Steps
Section 8 - OHS Fact Sheets

8.2 OHS responsibilities (cont)
OHS coordinator role
Some aged care facilities may nominate an OHS Coordinator to assist in
implementing OHS. The coordinator does not take on the management role or
responsibilities for OHS. They must be allocated time for the role. They also need
appropriate OHS training.
Their role may be to:
• assist in developing preventative strategies e.g. policies, procedures, action plans
• assist the OHS committee (if one is elected)
• assist in identifying, assessing and controlling hazards
• assist in workplace inspections, audits and incident investigation
• coordinate the collection, recording and analysis of OHS data
• coordinate training programs
Proprietors/Boards of Management responsibilities
Proprietors and boards of management have a legal responsibility for OHS.
These include:
• nominate a responsible officer (where applicable)
• ensure the legal obligations of the facility are met
OHS responsibilities of residents and their families
Residents and their families have rights within the facility, but they also have
a responsibility to ensure their actions do not put staff at risk.
Contractors
Contractors also have OHS obligations. They are to ensure their own safety and
not put others at risk. Employers have responsibility for the OHS of contractors
in relation to issues where they have control, for example, for safe access and
egress, no tripping hazards etc. Contractors including agency staff and tradespeople,
must be inducted to the site and included in training.
101OHS in Residential Aged Care First Steps
Section 8 - OHS Fact Sheets

8.3 Consultation
Health and Safety committee roles
The requirements for setting up OHS committees vary between States. Generally
small facilities would not be required to have a committee, but where they are set
up, their roles are to:
• provide a forum for management and employees to meet and discuss OHS issues
in the workplace
• bring together the employees’ practical knowledge of the job and the
management overview of the facility and work organisation
• assist to develop, monitor and review OHS policies, procedures and plans
• assist to resolve OHS issues
• develop and monitor a program for hazard identification, risk assessment
and control
• consider proposed changes which may affect OHS (for example, purchase of new
equipment, workplace changes, policy, procedure changes)
• develop and monitor an injury reporting system
• review incident reports and follow up actions
• assist to develop and evaluate training programs
• review external and internal OHS reports
• oversee the overall approach to OHS within the facility to encourage
integration of OHS into the overall management system and to promote
continuous improvement
Health and Safety Representatives’ role
The role of Health and Safety Representatives (where elected), in line with State
legislation is to:
• represent employees on OHS matters in meetings with managers, supervisors and
OHS inspectors
• participate in appropriate OHS training
• discuss OHS issues with employees within their workgroup
• participate in hazard identification, risk assessments and controlling risks
• assist to develop, implement, monitor and review agreed procedures
• participate in workplace inspections and incident investigation
• may issue Default Notices/Provisional Improvement Notices (in some States)
102 OHS in Residential Aged Care First Steps
Section 8 - OHS Fact Sheets

8.4 Fire, security and other emergencies(Expected Outcome 4.6)
Ensure the following policies and practices are in place:
• procedures for staff, residents and visitors to follow for fire, safety, security and
other emergencies, including evacuation and emergency drills which can be
understood by everyone
• emergency procedures and plan clearly displayed
• emergency contact phone numbers clearly displayed
• regular review of procedures
• staff education covers emergency procedures (and legislation)
• training data, including attendance records collated
• regular training program reviews documented
• orientation program documented and program reviewed
• qualified personnel conduct orientation and ongoing refresher programs
• alarm system operation demonstrated to staff
• identification system for staff and residents
• security measures developed
• service agreements with accredited equipment service providers and fire and
safety instructors (where necessary)
• access for staff to external programs and information, for example, videos
• program documented for planned, preventative and corrective maintenance
of fire, security and emergency equipment
• equipment testing documented and audited (and reviewed regularly)
• documented evidence of regular practice of emergency procedures (including
evacuation exercises)
• risk reporting system for staff, residents and visitors
• regular inspection of the facility to assess potential areas of risk
• quality improvement systems to identify and address deficiencies
103OHS in Residential Aged Care First Steps
Section 8 - OHS Fact Sheets

8.5 Hazardous substances & dangerous goods(Expected Outcome 4.6)
Hazardous substances are those substances which may harm health and are listed on
the National Occupational Health and Safety Commission’s List of Designated
Hazardous Substances [NOHSC:10005] or have been classified as a hazardous
substance by the manufacturer or importer in accordance with the Approved
Criteria for Classifying Hazardous Substance [NOHSC:1008(1004)].
Dangerous substances means any substance (solid, liquid or gaseous) that is toxic,
corrosive, flammable or otherwise dangerous in accordance with the Australian
Dangerous Goods Code (ADG Code) 6th edition, 1998.
Ensure the following policies and practices are in place:
• procedures for the use and storage of hazardous substances (chemicals) and
dangerous goods
• hazardous substances and dangerous goods are clearly and correctly labelled
(including decanted products)
• information and safety documentation, for example, material safety data sheets
(MSDS) obtained from suppliers
• instructions for use and dispensing of dangerous goods kept in storage area
• secure storage of hazardous substances and dangerous goods
• staff education program includes the use and storage of hazardous substances/
dangerous goods (and is documented)
• hazards of substances identified, risks addressed and controlled
• personal protective clothing and equipment (PPCE) provided (with instructions
for use)
• provision for first aid and medical attention if required
104 OHS in Residential Aged Care First Steps
Section 8 - OHS Fact Sheets

Project Steering Committee - Small Business ProjectJenny Hefford
Director Quality Assurance Workgroup
Commonwealth Department Health & Aged Care
Laurie Stiller
Manager
Sydney Operations
Niki Ellis & Associates
Mardi Webber
OHS Consultant
WorkCover Corporation
Angela Halsey
State Manager SA & NT
The Aged Care Standards Agency
ALHMW Union Representative
Sue Balde
OHS Representative
Helping Hand Aged Care
Aged Care Organisation Association Representative
Chris Racar
OHS Coordinator
Masonic Homes
Megan Williams
Senior Grants Project Officer
WorkCover Corporation
George Karlis
OHS Consultant
WorkCover Corporation
Consultant to Committee
Marion Pocock
Marion Pocock Consulting
105OHS in Residential Aged Care First Steps
Appendix 1 – Project Steering Committee
106 OHS in Residential Aged Care First Steps
As part of the evaluation of First Steps, we wouldappreciate your feedback on the contents.
Please complete the details below.
If you have additional comments and wish to attach them we would appreciate them too.
Please return your comments 3 months after receiving First Steps (or sooner if you wish).
Please send it to:
Name of Person completing the form (optional):
Facility
How long have you had First Steps?
What was your overall impression of First Steps?
(circle your response)
Comments:
Was First Steps easy to follow?
Comments:
Was the language easy to understand?
Comments:
Appendix 2 – Feedback Sheet
George Karlis
Executive Officer
Aged Care OHS Working Party
GPO Box 2668
Adelaide 5000
1 2 3 4 5 6
Poor Excellent
1 2 3 4 5 6
Poor Excellent
1 2 3 4 5 6
Poor Excellent

107OHS in Residential Aged Care First Steps
Were the flowcharts easy to understand
and follow?
Comments:
Have you used any of the sample forms? (if yes, which ones)
Were the forms useful and easy to use?
Comments:
Which parts of First Steps have you used?
Which sections did you find the most useful?
Which sections did you find the least useful?
Appendix 2 – Feedback Sheet
1 2 3 4 5 6
Poor Excellent
1 2 3 4 5 6
Poor Excellent

How could First Steps be improved?
Have you completed the Self Assessment Checklist?
How useful was it?
Have you developed an OHS Action plan using First Steps?
What OHS improvements have resulted?
Was First Steps helpful in the accreditation process?
Comments:
Individual results collated from the questionnaires will remain confidential but will be used collectively
to evaluate the effectiveness of the First Steps guide and make any improvements required.
108 OHS in Residential Aged Care First Steps
Appendix 2 – Feedback Sheet
1 2 3 4 5 6
Poor Excellent
1 2 3 4 5 6
Poor Excellent