occupational asthma - cecity.com fileoccupational asthma pier is copyrighted ©2014 by the american...
TRANSCRIPT
Evidence Ratings: Practice recommendations in PIER are given a strength of evidence rating (A,B,C):
= Preponderance of data supporting this statement is derived from high quality studies with minimal bias, including treatment issues (randomized
trials and systematic reviews or meta-analyses), diagnostic issues (cohort studies with appropriate reference standards), and prognosis issues
(observational studies with adequate controlling for confounders).
= The preponderance of data supporting this statement is derived from suboptimal quality studies, such as observational data for treatment issue
or others not meeting the criteria above.
= The preponderance of data supporting this statement is derived from non-experimental evidence such as case series or from expert opinion.
Disclosures: Craig S. Glazer, MD, MSPH, current author of this module, has no financial relationships with pharmaceutical companies, biomedical device manufacturers, or health-care related organizations. Deborah Korenstein, MD, FACP, Editor-in-Chief, PIER, has no financial relationships with
pharmaceutical companies, biomedical device manufacturers, or health-care related organizations. Richard B. Lynn, MD, FACP, Editor, PIER, has no
financial relationships with pharmaceutical companies, biomedical device manufacturers, or health-care related organizations.
CME Information: The American College of Physicians is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing education for physicians. The American College of Physicians designates this enduring material for a maximum of 1 AMA PRA
Category 1 CreditTM. Physicians should claim only credit commensurate with the extent of their participation in the activity.
Purpose: This activity has been developed for internists to facilitate the highest quality professional work in clinical applications, teaching,
consultation, or research. Upon completion of the CME activity, participants should be able to demonstrate an increase in the skills and knowledge
required to maintain competence, strengthen their habits of critical inquiry and balanced judgement, and to contribute to better patient care.
Disclaimer: The information included herein should never be used as a substitute for clinical judgement and does not represent an official position of the American College of Physicians. Because all PIER modules are updated regularly, printed web pages or PDFs may rapidly become obsolete.
Therefore, PIER users should compare the module updated date on the offical web site with any printout to ensure that the information is the most
current available.
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Occupational Asthma View online at http://pier.acponline.org/physicians/diseases/d278/d278.html
Module Updated: 2014-05-21
CME Expiration: 2017-05-21
Author
Craig S. Glazer, MD, MSPH
Table of Contents
1. Prevention .........................................................................................................................2
2. Screening ..........................................................................................................................4
3. Diagnosis ..........................................................................................................................6
4. Consultation ......................................................................................................................16
5. Hospitalization ...................................................................................................................17
6. Therapy ............................................................................................................................18
7. Patient Counseling ..............................................................................................................22
8. Follow-up ..........................................................................................................................23
References ............................................................................................................................26
Glossary................................................................................................................................29
Tables ...................................................................................................................................30
Figures .................................................................................................................................45
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 2 of 29
1. Prevention Top
Take primary preventive measures and report patients with occupational asthma to surveillance programs to prevent progressive disease and additional cases.
1.1 Take measures to prevent occupational asthma.
Recommendations
• Take primary preventive measures that focus on reducing exposures:
Eliminate potential sensitizers or substitute other substances with lower risk profiles
Implement engineering controls, including improved ventilation or process modification, or both, that
would reduce exposure levels
Consider administrative controls to limit the number of exposed workers or their time in exposure, and improve worker education regarding risks and alarm symptoms for which they should seek medical attention
Provide respiratory protection when the above options fail to eliminate exposure
• Take the following measures once occupational asthma has been identified:
Screen other exposed workers for sensitization (when possible) or early disease
Implement a medical surveillance program. These programs typically include medical screening but also use screening data to define interventions that can reduce exposure and prevent disease
Evidence
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended that work sites with potential exposures to sensitizers
implement secondary prevention, including medical surveillance (1).
• A 2005 guideline from the British Occupational Health Research Foundation on occupational asthma
emphasized the need to reduce workplace exposure as the most important factor in preventing the
development of occupational asthma (2).
• A 2012 systematic review of medical screening and surveillance in the workplace included 72
studies. Overall, the predictive value of pre-employment screening for individual risk factors was
too low to justify excluding those individuals from employment. There were few systematic studies
of medical surveillance programs, but there was some evidence that such programs may prevent
disease (3).
• A 2006 systematic review of primary prevention of latex sensitivity and occupational asthma
included eight studies, most of which were observational. The use of powder-free nonlatex gloves
appeared to reduce the incidence of latex allergy and asthma (4).
• A 2005 literature review of studies of the prevention of occupational asthma highlighted the
importance of various preventive measures in the development and prognosis of occupational
asthma. Primary prevention was effective for occupational asthma related to natural latex and
diisocyanate asthma. Secondary prevention, such as medical health surveillance, has been
effective in occupational asthma related to detergent enzymes, platinum salts, and diisocyanates.
Tertiary prevention is thought to improve the prognosis of workers who already have occupational
asthma (5).
Rationale
• Occupational asthma is a preventable illness. Identifying a case of occupational asthma is a
sentinel health event indicating an opportunity for preventive measures in the workplace.
Comments

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 3 of 29
• People with a laboratory diagnosis of only atopy characterized by positive prick-test results to
common allergens probably should not be removed from their jobs but should be provided with an
individual program of medical prevention (6).
• According to NIOSH, respiratory protection is generally a less effective method of exposure
reduction than elimination, substitution, or engineering controls. Most studies of respiratory
protective devices have examined occupational asthma in circumstances in which workers have
already been sensitized to a particular agent (7). However, these devices are not always successful
in preventing occupational asthma (8).
• National occupational disease surveillance programs have been developed in the U.S. (SENSOR),
Great Britain (SWORD), and other countries (9; 10). SENSOR programs provide workers and
physicians with workplace investigations to facilitate preventive surveillance.
• In the detergent industry, process modification dramatically reduced occupational asthma, using
measures such as encapsulating enzymes, improving ventilation, and screening to detect
sensitization (11).

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 4 of 29
2. Screening Top
Screen all patients with asthma for workplace-related asthma.
2.1 Ask all patients with asthma about occupational factors.
Recommendations
• Record occupational history in all patients with asthma.
• Ask whether other workers are similarly affected with asthma.
• Determine whether risk factors (smoking, atopy, occupational rhinitis) for the development of
occupational asthma are present.
• See table Select Agents Associated with Occupational Asthma with or without a Latency.
• See table Questionnaire: Determining Whether Asthma Symptoms Are Work-Related.
Evidence
• The 2007 Expert Panel 3 guidelines on asthma from the National Heart, Lung, and Blood Institute
and National Asthma Education and Prevention Program recommended that clinicians ask all
patients with asthma about occupational exacerbating factors (12).
• A 2003 statement from the American Thoracic Society on the occupational contribution to the
burden of airway disease reviewed the evidence regarding factors that contribute to the
pathogenesis of obstructive airway disease and reported the population attributable risk to range
from 4% to 58%, with a median value of 15% (13).
• A cross-sectional study evaluated the prevalence of occupational rhinitis among 596 individuals
with occupational asthma. Overall, 58.4% of those with occupational asthma had occupational
rhinitis (14).
• A retrospective case series described outcomes after inhalation exposure in 323 patients.
Symptoms lasting 14 or more days were reported by 6% of patients. Risk factors for persistent
symptoms included preexisting lung disease (RR, 2.4 [CI, 14 to 4.2]) and cigarette smoking (RR,
1.7 [CI, 1.3 to 2.2]) (15).
• A prospective study evaluated the prevalence of new-onset occupational asthma in a European
population and identified risk factors. Between 10% and 25% of new adult asthma was attributable
to occupational exposures; risk factors included exposure to a substance known to cause
occupational asthma (RR, 1.6 [CI, 1.1 to 2.3]), a symptomatic inhalation event (RR, 3.3 [CI, 1.0 to
11.1]), and working as a nurse (RR, 2.2 [CI, 1.3 to 4.0]) (16).
• NHANES III showed the prevalence of work-related asthma, defined as an affirmative response to
questions on self-reported, physician-diagnosed asthma and work-related symptoms of rhinitis,
conjunctivitis, and asthma, was 3.7% (CI, 2.88% to 4.52%), and the prevalence of work-related
wheezing was 11.46% (CI, 9.87% to 13.05%). The main industries at risk for work-related asthma
and wheeze included the entertainment industry, agriculture, forestry, fishing, construction,
electrical machinery repair services, and lodging places. The population attributable risk for work-
related wheezing was 28.5% (17).
• A large population-based study in Finland combined data from individuals with persistent asthma
with population census data to estimate the attributable fraction of work in adult-onset persistent
asthma. The attributable fraction of occupation in males was 29% (CI, 25% to 33%) and in
females was 17% (CI, 15% to 19%). The risk increased especially in agricultural, manufacturing,
and service work. Among manufacturing jobs, high risks were recorded in food and beverage work,
and also in smelting, metallurgical, foundry, painting, and lacquering work. Among service workers,

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 5 of 29
high risks were recorded in hygiene and beauty treatment, pressing, dry cleaning, and laundering
work (18).
• A prospective study evaluated the accuracy of specific questions for the diagnosis of occupational
asthma in 212 patients who underwent challenge testing. Overall, 72 patients (34%) were
diagnosed with occupational asthma. In the multivariate analysis, symptoms at work that were
independently associated with occupational asthma included wheezing (OR, 3.39 [CI, 1.43 to 8.0]),
nasal itching (OR, 3.7 [CI, 1.8 to 7.8]), and eye itching (OR, 2.37 [CI, 1.06 to 5.30]). Loss of voice
at work made occupational asthma less likely (OR, 0.39 [CI, 0.18 to 0.86]) (19).
• A prospective study among subjects exposed to high-molecular-weight occupational allergens
showed that of three potential factors for the development of respiratory symptoms—atopy,
rhinoconjunctivitis, and PC20 (the level of provocational concentration of methacholine causing a
change in FEV1 of 20%)—having a measurable PC20 level was the most significant (20).
• A cross-sectional study of 799 female Finnish dental assistants (response rate, 87%) showed an
increased risk for adult-onset asthma among those with daily methacrylate exposure vs. those with
less than daily exposure (adjusted OR, 2.65 [CI, 1.14 to 7.24]). Nasal symptoms (OR, 1.37 [CI,
1.02 to 1.84]) and work-related cough or phlegm (OR, 1.69 [CI, 1.08 to 2.71]) were also increased
(21).
• A 2006 narrative review discussed six epidemiologic studies on professional cleaners and noted an
increased risk for occupational asthma, even after adjusting for age and smoking history. The
review noted that using bleach, especially in cleaning windows and washing dishes, has been
implicated (22).
• A 2011 narrative review of occupational asthma discussed known environmental risk factors and
possible cofactors, such as exposure to cigarette smoke (23).
Rationale
• Asthma may frequently be related to occupational exposure.
• The identification of a case of occupational asthma may lead to the detection of other cases in the
same work site.
• Smoking has been identified as a risk factor for some types of occupational asthma (lab animal
workers and snow-crab workers).
• Atopic workers are more at risk for the development of IgE-mediated occupational asthma (latex,
lab animal proteins).
• Occupational rhinitis is common among people with occupational asthma and may precede the
development of lower airway disease.
Comments
• A retrospective review of medical records indicated that physicians take incomplete occupational
histories among adults with new-onset asthma. The implications of such underrecognition may
result in underdiagnosis and undermanagement of potentially modifiable workplace exposure (24).

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 6 of 29
3. Diagnosis Top
Confirm the diagnosis of occupational asthma through a careful history, a physical exam, and lab testing.
3.1 Ask about classic symptoms of asthma in patients with suspected occupational asthma.
Recommendations
• Ask about the following classic symptoms of asthma:
Cough, particularly if worse at night
Recurrent wheeze
Recurrent difficulty in breathing
Recurrent chest tightness
• Look for symptoms that occur or worsen in the presence of
Exercise
Viral infection
Exposure to allergens, such as animal fur or feathers, dust mites, mold, smoke, or pollen
Changes in weather
Emotional expression (laughing)
Menses
Airborne chemicals, dusts, or other irritants, including those in the workplace
• Look for symptoms that occur or worsen at night, waking the patient.
• See table Diagnostic Criteria for Asthma.
• See module Asthma.
Evidence
• The 2007 Expert Panel 3 guidelines on asthma from the National Heart, Lung, and Blood Institute
and National Asthma Education and Prevention Program recommended criteria for the diagnosis of
asthma. Key indicators for the diagnosis include history of recurrent wheeze, cough (especially if
worse at night), chest tightness, or shortness of breath with worse symptoms in the setting of
exercise, viral infection, allergens (animal fur, mold, smoke, pollen, dust), weather change,
menstruation, or strong emotion (12).
• A prospective study evaluated the accuracy of specific questions for the diagnosis of occupational
asthma in 212 patients who underwent challenge testing. Overall, 72 patients (34%) were
diagnosed with occupational asthma. In the multivariate analysis, symptoms at work that were
independently associated with occupational asthma included wheezing (OR, 3.39 [CI, 1.43 to 8.0]),
nasal itching (OR, 3.7 [CI, 1.8 to 7.8]), and eye itching (OR, 2.37 [CI, 1.06 to 5.30]). Loss of voice
at work made occupational asthma less likely (OR, 0.39 [CI, 0.18 to 0.86]) (19).
Rationale
• The presence of multiple key indicators increases the probability of a diagnosis of asthma.
• The socioeconomic consequences of occupational asthma can be severe. In addition, the specificity
of history alone is inadequate for the diagnosis of occupational asthma.
3.2 Look for findings on the lung exam consistent with asthma, such as wheezing, prolonged expiratory phase, or chest hyperexpansion, and examine
the skin and nose.
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 7 of 29
Recommendations
• Examine the respiratory system, the nose, and the skin:
Look for wheezing during normal breathing, use of accessory muscles of respiration, hyperexpansion of the thorax, and prolongation of forced exhalation
Examine the nose for increased nasal secretion, mucosal swelling, and nasal polyps
Examine the skin for evidence of atopic dermatitis or eczema
• See table Diagnostic Criteria for Asthma.
Evidence
• The 2007 Expert Panel 3 guidelines on asthma from the National Heart, Lung, and Blood Institute
and National Asthma Education and Prevention Program noted that a physical exam for asthma
includes the upper respiratory tract, chest, and skin, and stated that findings that increase the
likelihood of asthma include chest hyperexpansion; wheezing during normal breathing; prolonged
expiratory phase; nasal secretions, swelling, or polyps; and atopic dermatitis or eczema (12).
• A prospective study evaluated the accuracy of history and physical exam findings in 85 patients
with chronic dyspnea. Wheezing on physical exam had a PPV of 33% and an NPV of 72% for
asthma, and spirometry had a PPV of 18% and an NPV of 72% for asthma (25).
Rationale
• The presence of certain physical findings helps confirm the diagnosis of asthma.
Comments
• Wheezing during forced exhalation is not a reliable indicator of airflow limitation. Wheezing may be
undetectable in mild asthma, very severe asthma, or between exacerbations. In general,
physicians have limited ability in assessing the degree of airflow limitation or to predict whether the
obstruction is reversible.
3.3 Use spirometry to confirm a diagnosis of asthma.
Recommendations
• Obtain spirometry to measure inspiratory and expiratory flow curves and establish FEV1 before and
after bronchodilators.
Obtain baseline spirometry to assess the degree of airway obstruction and the severity of the illness
Obtain postbronchodilator FEV1 to confirm the diagnosis
Note that reversible obstruction confirms asthma
• If spirometry is normal, then perform nonspecific airway responsiveness testing (e.g.,
methacholine challenge) to document airway hyperresponsiveness.
• High-value care: Do not diagnose or manage asthma without spirometry.
Evidence
• The 2007 Expert Panel 3 guidelines on asthma from the National Heart, Lung, and Blood Institute
and National Asthma Education and Prevention Program stated that spirometry is essential for the
diagnosis and treatment of asthma (12).
• A 1999 American Thoracic Society guideline discussed the indications for methacholine challenge
testing and described the details of its performance (26).
Rationale
• Confirming bronchial hyperresponsiveness or reversible airflow obstruction is crucial for objective
confirmation of asthma.
• An empiric therapeutic trial with asthma therapy may confound the evaluation for occupational
asthma and is discouraged when occupational asthma is a consideration.
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 8 of 29
• Spirometry determines whether there is reversible airflow obstruction; however, normal testing
does not rule out asthma.
• A normal methacholine challenge performed when the patient is still working has a high NPV for
active asthma.
3.4 Ask adult patients with newly diagnosed or worsening asthma about patterns of respiratory symptoms and signs that suggest a relationship to
their work.
Recommendations
• Ask about specific symptom patterns, or use a respiratory questionnaire to record occupational
histories.
• At the completion of the history and physical exam, ask about
The circumstances around the onset of the patient's asthma
The temporal relationships between relevant exposures at the time of symptom onset and with disease
exacerbations
The current severity of the disease
• In patients whose asthma began or worsened during their working life, ask the following:
Were there changes in work processes in the period preceding the onset of symptoms?
Was there an unusual work exposure within 24 hours before the onset of initial asthma symptoms?
Do asthma symptoms differ during times away from work, such as weekends or holidays, or other
extended times away from work?
Are there allergic rhinitis or conjunctivitis symptoms, or both, that are worse with work?
• See table Specific Symptom Patterns and Patterns of Exposure for Occupational Asthma.
Evidence
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended screening patients with newly diagnosed or worsening
asthma for work-related factors, including asking about job duties, exposures, use of protective
equipment, and the timing of symptoms in relation to work (1).
• The 2007 Expert Panel 3 guidelines on asthma from the National Heart, Lung, and Blood Institute
and National Asthma Education and Prevention Program recommended that clinicians ask all
patients with asthma about occupational exacerbating factors (12).
• A 2003 statement from the American Thoracic Society on the occupational contribution to the
burden of airway disease reviewed the evidence implicating factors on the pathogenesis of
obstructive airway disease and reported the population attributable risk to range from 4% to 58%,
with a median value of 15% (13).
• A cross-sectional study evaluated the prevalence of occupational rhinitis among 596 individuals
with occupational asthma. Overall, 58.4% of patients with occupational asthma had occupational
rhinitis (14).
• A prospective study evaluated the prevalence of new-onset occupational asthma in a European
population and identified risk factors. Between 10% and 25% of new adult asthma was attributable
to occupational exposures; risk factors included exposure to a substance known to cause
occupational asthma (RR, 1.6 [CI, 1.1 to 2.3]), a symptomatic inhalation event (RR, 3.3 [CI, 1.0 to
11.1]), and working as a nurse (RR, 2.2 [CI, 1.3 to 4.0]) (16).
• NHANES III showed the prevalence of work-related asthma, defined as an affirmative response to
questions on self-reported, physician-diagnosed asthma and work-related symptoms of rhinitis,
conjunctivitis, and asthma, was 3.7% (CI, 2.88% to 4.52%), and the prevalence of work-related

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 9 of 29
wheezing was 11.46% (CI, 9.87% to 13.05%). The main industries at risk for work-related asthma
and wheeze included the entertainment industry, agriculture, forestry, fishing, construction,
electrical machinery repair services, and lodging places. The population attributable risk for work-
related wheezing was 28.5% (17).
• A large population-based study in Finland combined data from individuals with persistent asthma
with population census data to estimate the attributable fraction of work in adult-onset persistent
asthma. The attributable fraction of occupation in males was 29% (CI, 25% to 33%) and in
females was 17% (CI, 15% to 19%). The risk increased especially in agricultural, manufacturing,
and service work. Among manufacturing jobs, high risks were recorded in food and beverage work
and in smelting, metallurgical, foundry, painting, and lacquering work. Among service workers,
high risks were recorded in hygiene and beauty treatment, pressing, dry cleaning, and laundering
work (18).
• A prospective study evaluated the accuracy of specific questions for the diagnosis of occupational
asthma in 212 patients who underwent challenge testing. Overall, 72 patients (34%) were
diagnosed with occupational asthma. In the multivariate analysis, symptoms at work that were
independently associated with occupational asthma included wheezing (OR, 3.39 [CI, 1.43 to 8.0]),
nasal itching (OR, 3.7 [CI, 1.8 to 7.8]), and eye itching (OR, 2.37 [CI, 1.06 to 5.30]). Loss of voice
at work made occupational asthma less likely (OR, 0.39 [CI, 0.18 to 0.86]) (19).
• A cross-sectional study assessed the prevalence of work-related asthma in 17,637 adults with
asthma and a history of employment from a national sample of U.S. residents. Overall, 9.7% had
work-related asthma. Compared with patients with non-work-related asthma, those with work-
related asthma had lower household income (OR, 2.2 [CI, 1.6 to 3.1] for the lowest income group
compared with the highest income group) and were more likely to be 45 to 64 years old (OR, 1.9
[CI, 1.5 to 2.4] compared with those aged 18 to 44 years) (27).
Rationale
• The occupational history taken by an experienced clinician or by questionnaire either given by an
interviewer or self-administered is a sensitive tool.
• Workplace exposure may worsen bronchial asthma or aggravate subclinical or mild asthma.
• Work-related asthma accounts for a significant portion of adult asthma.
• There are important non-drug interventions for work-related asthma.
Comments
• Several different reporting systems demonstrate incidences of occupational asthma ranging from 1
to 18/100,000 per year (28; 29; 18).
3.5 In patients whose asthma symptoms are related to their work environments, ask about specific exposures.
Recommendations
• Ask patients with apparent occupational asthma about specific exposures.
Focus on exposures at the time the disease began or initially started to worsen
Assess the duration, concentration, frequency, and peak concentration of any exposures
Ask the worker to obtain the material safety data sheets kept on file by the employer, and discuss all the agents to which the worker may be exposed, including data on composition, physical characteristics, and health-related information
• Note that agents that can cause occupational asthma include
Smoke, wood dust, acrylates, and paper dust
Solvents, isocyanates, aldehydes, glues, epoxy resins, and paint
Ammonia, bleach, acids, bases, cleaning materials, metalworking fluid, and oxidizers

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 10 of 29
Phenylcyclohexene
Pesticides, animal materials, mold, and plant materials
Welding fumes
Latex
Ethanolamines
• See the list of agents that can cause occupational asthma, from the UK Health and Safety
Executive.
• See table Select Agents Reported to Be Associated with Reactive Airway Dysfunction Syndrome.
• See table Select Agents Associated with Occupational Asthma with or without a Latency.
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended asking about rhinoconjunctivitis in patients with suspected occupational asthma and
taking a detailed occupational history (30).
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended screening patients with newly diagnosed or worsening
asthma for work-related factors, including asking about job duties, exposures, use of protective
equipment, and the timing of symptoms in relation to work (1).
• A population-based study evaluated the association between work and respiratory symptoms in
15,000 adults aged 45 to 64. Overall, 11% reported wheezing and 9% were diagnosed with airway
obstruction. Compared with people with administrative or managerial jobs, those working in food
preparation and service (RR, 1.96 [CI, 1.27 to 3.01]) and as mechanics or repairers (RR, 1.83 [CI,
1.17 to 2.85]) were more likely to have asthma (31).
• From 1993 through 1995 the SENSOR surveillance program in four states (California,
Massachusetts, Michigan, and New Jersey) identified a total of 1101 persons with work-related
asthma. Of these persons, 80% to 89% were classified as having new-onset asthma and 19.1% as
having work-aggravated asthma. The most common industries associated with the condition were
transportation equipment manufacturing (19.3%), health services (14.2%), and educational
services (8.7%) (28).
• A 2000 narrative review of occupational respiratory disease included a list of common causes of
occupational airway disease, which is classified into bronchitis, bronchiolitis, asthma with latency,
asthma without latency, chronic obstructive pulmonary disease, and chronic air flow limitation (32).
Rationale
• Knowledge of the most commonly reported agents causing occupational asthma in general and in
your practice area is important when taking the occupational history.
• Information regarding the extent of exposure, site of exposure, and existent control measures is
essential in making a complete assessment.
Comments
• Work-exacerbated asthma is typically diagnosed by finding a relationship of increased symptoms
with workplace exposure in patients whose asthma was present before the onset of exposure.
• In the U.S., OSHA mandates that material safety data sheets be made available to the employee
upon request.
• The list of agents is adapted from 33.
3.6 In patients with occupational asthma, differentiate between immunologic (sensitizer-induced) and nonimmunologic (or irritant) asthma.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 11 of 29
Recommendations
• Classify the disease type in patients with occupational asthma:
Ask about a latent period, defined as the period between the onset of exposure and the onset of disease
Note that immunologic (sensitizer-induced) occupational asthma is characterized by the presence of a latent period and that occupational asthma related to an irritant is characterized by a lack of a latent period
Rule out other causes of airway symptoms
• Classify patients with sensitizer-induced occupational asthma according to the molecular weight of
the culprit antigen and the pattern of bronchial reactivity:
Note that low-molecular-weight antigens are less than 5000 kilodaltons and are typically chemicals, and that most do not induce detectable IgE responses
Note that high-molecular-weight antigens are typically proteins of animal, plant, or microbial origin, and
typically induce detectable IgE responses
Determine the pattern of bronchial reactivity:
o Immediate: usually within 1 hour of exposure (or of entering the workplace)
o Isolated late: patients develop bronchial hyperreactivity and symptoms 6 to 8 hours after exposure, generally toward the end of work shifts or in the evening of days worked
o Dual: patients in this group manifest both responses
• In patients with occupational asthma related to an irritant,
Assess whether the patient meets the criteria for RADS (nonimmunological asthma without a latent period), which is found with
o A documented absence of preceding respiratory complaints
o The onset of symptoms after a single specific high exposure
o Exposure to a particular irritating gas, fume, or vapor that was present in high concentrations
o Onset of symptoms occurring within 24 hours after the exposure
o Presence and persistence of nonspecific bronchial hyperresponsiveness (methacholine or histamine challenge test) following the exposure
o Other types of pulmonary diseases ruled out
Classify patients with longer-term irritant exposures or with symptom onset after 24 hours as having irritant-induced asthma or not-so-sudden irritant-induced asthma.
• See the list of agents that can cause occupational asthma, from the UK Health and Safety
Executive.
• See table Select Agents Associated with Occupational Asthma with or without a Latency Period.
• See table Select Agents Reported to Be Associated with Reactive Airway Dysfunction Syndrome.
Evidence
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma presented diagnostic criteria for RADS and described patterns of response
to irritant exposure (1).
• A retrospective study of 86 asthmatic patients showed that 63% had irritant-induced asthma with
two distinct clinical presentations: sudden and not-so-sudden onset. Eighty-eight percent of the
not-so-sudden group showed an atopic-allergic status. Sixteen patients with atopy and presumed
new-onset asthma had preexistent asthma. Preexisting allergic-atopic status or preexisting asthma
were significant contributors to the pathogenesis of not-so-sudden irritant-induced asthma (34).
• In a long-term follow-up study of pulmonary function, quality of life, and psychological status after
an average of 13.6 years (±5.2 years) from the time of acute irritant exposure, all 35 subjects who
had filed for compensation for work-related injuries with the medicolegal agency in Quebec still
reported respiratory symptoms, and 68% were on inhaled steroids. Measures of quality of life and
psychological status indicated that irritant-induced asthma can be a significant cause of long-term

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 12 of 29
impairment and disability. Subjects with acute irritant-induced asthma were no different from those
with allergic occupational asthma in terms of pulmonary function and markers of inflammation
(35).
• A follow-up study of 20 patients with irritant-induced asthma due to repeated exposure to chlorine
found no change in mean FEV1 after 2.5 years of follow-up; 33% of patients had improved airway
hyperresponsiveness (36).
• A 2013 narrative review discussed a diagnostic approach to suspected work-related asthma (37).
Rationale
• It is important to make the distinction between immunologically induced occupational asthma
(which occurs after a period of sensitization) and irritant-induced occupational asthma (which
occurs rapidly after exposure without sensitization).
• RADS is defined as asthma occurring after a single or multiple exposures to high levels of an
irritating gas, vapor, fume, or smoke; there is no objective test for the diagnosis and no recurrence
of symptoms after reexposure.
Comments
• The latent period can range from months to decades but is usually between 2 and 5 years in
duration.
• In individuals with significant exposure, acute irritant-induced asthma can be a long-term
impairment that may require chronic medical care.
• At the World Trade Center site where rescue workers experienced massive exposure to airborne
particulates, the development and persistence of hyperreactivity and RADS were associated
strongly and independently with exposure intensity. Hyperreactivity demonstrated shortly after
exposure predicted RADS at 6 months in highly exposed workers (1).
• Most high-molecular-weight occupational allergens and some low-molecular-weight occupational
allergens mediate asthma at least partly by a type 1 IgE-dependent mechanism, which results in
immediate symptoms, occurring within minutes but resolving usually within 1 hour; however, some
workers may have an isolated late phase (late-phase asthma) occurring 4 to 6 hours after
exposure or a dual-phase response where the immediate reaction is followed by the late-phase
response. Isolated late responses are more common with low-molecular-weight (i.e., chemical)
antigens.
• Long-term cure rates appear to be similar for acute irritant-induced asthma (17%) and allergic
occupational asthma (27%) (35; 38).
3.7 Perform confirmatory testing using serial measures of pulmonary
function, and consider immunologic testing.
Recommendations
• Measure serial PEFR in patients with occupational asthma who remain in the workplace:
Measure PEFR four times daily for 2 weeks at work and four times daily for 2 weeks outside of work
Instruct the patient to record rescue inhaler use and precipitating exposures
Recognize that patients may not accurately record or report PEFR readings obtained with portable devices (e.g., Wright mini peak flow meter); therefore, whenever possible, use an electronic device that records
PEFR or FEV1 values on a memory chip
Do not change medical therapy during the testing period
Note that positive patterns will show reduced flow or increased diurnal variability in flows, or both, when times at work are compared with times away from work in patients with sensitizer-induced occupational asthma
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 13 of 29
• Consider serial methacholine or histamine challenge testing if serial PEFR measurements cannot be
obtained or are nondiagnostic:
Do the test on the last working day of the work week and after the patient has been exposed at work for at least 2 consecutive weeks, then repeat after at least 2 weeks away from the exposure
Discontinue bronchodilators, anticholinergic medications, theophyllines, and antihistamines for 24 to 48 hours
Instruct patients to refrain from caffeine-containing beverages for 6 hours and from smoking for 2 hours before testing if methacholine is the agent used
Note that a 3 dilution or greater improvement in the PC20 when away from exposure is consistent with sensitizer-induced occupational asthma
• Consider immunologic testing in patients with suspected sensitizer-induced occupational asthma
without a clearly identified agent of exposure using one of the following:
Skin tests
Immunoassays (RAST, ELISA tests)
• Refer to a specialist for immunologic testing.
• See table Laboratory and Other Studies for Occupational Asthma.
• See table Indications for Peak Flow Monitoring.
• See table Proper Technique for Recording Portable Peak Flow Rate Recordings.
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended measuring serial PEFR at least four times per day for at least 3 consecutive weeks
during a 2-week period outside of work followed by a period after return to work. Serial PEFR
measurement had a sensitivity of 64% and a specificity of 77%. Immunologic testing is not
specific, and serial measures of bronchial responsiveness are neither sensitive nor specific (30).
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended measuring PEFR four times daily for 2 weeks during work
and four times daily outside of work in all patients with suspected occupational asthma. The
guideline recommended that patients with suspected sensitizer-induced occupational asthma
undergo immunologic testing if available (1).
• A 2005 AHRQ systematic evidence report on the diagnosis and management of work-related
asthma included 61 studies assessing the diagnostic accuracy of testing, generally compared with
specific inhalational challenges. A single nonspecific bronchoprovocational challenge test had a
pooled sensitivity of 66.7% and a specificity of 63.9%, and testing for high-molecular-weight
antigens had a pooled sensitivity of 79.3% and a specificity of 59.3%. Skin-prick testing had a
sensitivity and a specificity of 72.9% and 86.2%, respectively, in studies of low-molecular-weight
exposures; 80.6% and 59.6%, respectively, in studies of high-molecular-weight exposures; and
85.1% and 65.2%, respectively, in studies of various exposures. Serum IgE testing had a
sensitivity and a specificity of 31.2% and 88.9%, respectively, for low-molecular-weight agents;
73.3% and 79.0%, respectively, for high-molecular-weight agents; and 85.1% and 61.2%,
respectively, in studies of various agents (39).
• A prospective study evaluated the accuracy of serial PEFR measurements and serial FEV1
measurement in 20 patients with suspected occupational asthma, using inhalation challenge testing
as the reference standard. The sensitivity of flow rate recordings varied based on interpreter
between 73% and 82%, with a specificity between 89% and 100%. The sensitivity of FEV1 varied
between 45% and 55%, and the specificity varied between 56% and 100% (40).
• A prospective study using specific inhalational challenge test results to evaluate PEFR showed that
the best index for comparing results of PEFR with specific inhalational challenge testing was the
visual analysis of the PEFR (41).

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 14 of 29
• A retrospective study evaluated agreement between expert interpretation of serial PEFR testing and
readings by a validated diagnostic aid (Oasys-2). For agreement between experts and Oasys-2,
median kappa values were 0.50 to 0.75 (42),
• A case-control study evaluated the accuracy of peak flow monitoring in 81 patients with
occupational asthma and 60 controls with asthma. Taking readings over 4 weeks had a sensitivity
of 81.8% and a specificity of 93.8%; taking readings over 2 weeks had a sensitivity of 70% and a
specificity of 82.4%. The sensitivity and specificity were highest with eight readings per day but
were similar with four per day (43).
Rationale
• In the setting of confirmed asthma, history alone leads to a correct diagnosis of occupational
asthma in, at most, 75% of patients.
• To ensure an accurate diagnosis and avoid the adverse socioeconomic consequences of removal
from work, additional confirmatory testing is recommended.
• Bronchial hyperresponsiveness measured by nonspecific challenge has been shown to worsen when
a patient with sensitizer-induced occupational asthma is exposed to the relevant antigen.
Comments
• As much of the testing described requires the patient to still be working, the clinician should make
every effort not to remove the patient from work until after the evaluation is completed.
• The peak flow meter should be simple to use, inexpensive, and accurate. It also needs to have the
capability to record high flows.
• Immunologic testing is available for about 40 etiologic agents but will not be feasible for most low-
molecular-weight chemical antigens because most do not induce an IgE-mediated response.
• Few of the available antigen preparations are validated and standardized. Variable antigen potency
from different manufacturers can lead to false-negative test results (44).
• Specific antibody responses wane over time, so false-negative results do occur if the patient has
been away from exposure for a prolonged time (45).
• Methacholine challenge testing should be done by a trained individual and is not generally
recommended if the FEV1 is less than 70% of the predicted result, or less than 2 L.
3.8 Consider the differential diagnosis of occupational asthma.
Recommendations
• Consider other diagnoses that may mimic occupational asthma:
Non-work-related asthma
Work-exacerbated asthma
Bronchiolitis obliterans
Hypersensitivity pneumonitis
Metal or polymer fume fever
Organic dust toxic syndrome
Byssinosis
• See table Differential Diagnosis of Occupational Asthma.
Evidence
• A 2000 narrative review of occupational respiratory disease included a list of common causes of
occupational airway disease classified into bronchitis, bronchiolitis, asthma with latency, asthma
without latency, chronic obstructive pulmonary disease, and chronic air flow limitation (32).
• Pulmonary mycotoxicosis is more common than hypersensitivity pneumonitis (46).

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 15 of 29
• A 5-year follow-up study compared cotton-thread textile workers with silk-thread textile workers.
The presence of byssinosis at the time of the first survey was 7.3%. An across-shift drop of 5% or
more at the time of the first survey was predictive of a five-year decline in FEV1 (47).
Rationale
• Other conditions can mimic occupational asthma.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 16 of 29
4. Consultation Top
Consider consultation for diagnosis in all patients suspected of having occupational asthma and for management in all patients with occupational asthma.
4.1 Consider consultation with a pulmonologist or allergist to help establish
the diagnosis.
Recommendations
• Refer patients suspected of having occupational asthma to a pulmonologist or an allergist for
assistance in the identification of specific etiologic agents and management.
• Recognize that the investigation and diagnosis of occupational asthma include testing for
nonspecific bronchial hyperresponsiveness and peak flow monitoring.
Evidence
• Consensus.
Rationale
• Patients require confirmation of a history that suggests that an occupational or environmental
inhalant is provocative or contributory to asthma.
4.2 Consider referring all patients with occupational asthma to a
pulmonologist or allergist for management.
Recommendations
• Obtain consultation with a specialist (pulmonologist, occupational medicine specialist, allergist) to
improve management in patients with poorly controlled symptoms.
• Consider referral to an allergist for desensitization therapy.
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended that patients with confirmed or suspected occupational asthma be followed at a
specialist center (30).
• A 1996 narrative review of the role of experts in asthma care noted that “expert-based” care
systems are associated with better outcomes (48).
Rationale
• A specialist is experienced in the diagnosis, treatment, or intervention required in the work
environment and in managing patients over a period of time or comanaging with the primary care
provider.
• Desensitization therapy may be helpful in controlling symptoms.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 17 of 29
5. Hospitalization Top
Consider hospitalization for severe occupational asthma.
5.1 Hospitalize patients with severe asthma symptoms. Consider hospitalization using the same determinants as for other types of asthma.
Recommendations
• Admit patients with acute asthma to the hospital if they have
Impending respiratory arrest (admit to the intensive care unit)
Severe exacerbation (peak flow or FEV1 less than 40% of predicted or best) and incomplete or poor response to initial therapy in the emergency department
Moderate exacerbation (peak flow or FEV1 40% to 69% of predicted or best) and incomplete or poor response to initial therapy in the emergency department
• Consider hospitalization in other patients with
History of severe exacerbations or multiple intubations
Medication use at the time of the exacerbation
Poor access to medical care and medications
Inadequate support or poor home conditions
Severe psychiatric illness
Evidence
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended hospitalizing patients with impending respiratory arrest and
those with mild to moderate or severe exacerbations and poor or incomplete response to
emergency department therapy (1).
Rationale
• The factors that govern the hospitalization of patients with occupational asthma are no different
from other patients with asthma.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 18 of 29
6. Therapy Top
After establishing the diagnosis of occupational asthma, develop a strategy with the patient to reduce or completely avoid exposure to the cause. Consider the use of inhaled steroids and other drugs.
6.1 For patients with sensitizer-induced occupational asthma, plan with the
patient to ensure complete removal from the source of exposure.
Recommendations
• For patients with sensitizer-induced occupational asthma, advise avoidance of all further exposure
to the causative agent through
Substitution or elimination of the causative agent from the work site
Transfer to a different position with the same employer
Job change
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended complete removal of the patient from the exposure (30).
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended removing patients with sensitizer-induced occupational
asthma from the environment, and reducing exposure and optimizing asthma therapy for those
with irritant-induced occupational asthma (1).
• A 2011 systematic review of exposure elimination or reduction for patients with occupational
asthma included 14 studies. Overall, reduction in exposure was associated with a lower rates of
asthma symptom improvement (OR, 0.16 [CI, 0.03 to 0.91]) and recovery (OR, 0.30 [CI, 0.11 to
0.84]) compared with complete exposure avoidance (49).
• A 2005 AHRQ systematic evidence report on the diagnosis and management of work-related
asthma found that workers with continued exposure generally experienced further deterioration in
FEV1 and that those for whom the exposure was eliminated generally had improvements in FEV1
(39).
Rationale
• Most patients with occupational asthma improve or stabilize with exposure removal. Some are
cured, but most will not completely recover after cessation of exposure and will worsen if exposure
is continued.
Comments
• Significant prognostic factors include both the duration of symptoms and the duration of exposure;
death has been reported with persistent exposure.
• Studies show that exposure reduction is not adequate for sensitizer-induced occupational asthma.
6.2 Reduce exposures for patients with irritant-induced occupational asthma or work-exacerbated asthma through workplace modifications.
Recommendations
• For patients with irritant-induced occupational asthma or work-exacerbated asthma, reduce
exposures through

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 19 of 29
Accommodations from the employer for workplace modifications (in the U.S., under the Americans with
Disabilities Act) and to prevent exposures that are even below the permitted NIOSH-ACGIH threshold limits
The use of a mask, respirator, or other protective equipment, especially if such irritants as nuisance dusts trigger bronchospasm
• Recognize that if symptoms continue despite modifications, complete removal of the worker from
irritant exposure is essential.
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended complete removal of the patient from the exposure (30).
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended that removing patients with sensitizer-induced occupational
asthma from the environment, and reducing exposure and optimizing asthma therapy for those
with irritant-induced occupational asthma (1).
Rationale
• Death could occur from persistent exposure to the irritant.
6.3 Use a stepwise approach to asthma therapy in patients with occupational
asthma, and treat those with mild persistent asthma symptoms with inhaled steroids.
Recommendations
• Assess symptom severity in patients with occupational asthma, and classify them as having
intermittent, mild persistent, moderate persistent, or severe persistent disease.
• Prescribe
A β2-agonist as a rescue inhaler
Inhaled steroids for all patients with more than mild symptoms
• See figure Classifying Asthma Severity.
• See figure Stepwise Approach for Managing Asthma Treatment in Youth ≥12 Years of Age and
Adults.
• See table Drug Treatment for Occupational Asthma.
• See module Asthma.
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended treating occupational asthma with the same approach to drug therapy as in
nonoccupational asthma (30).
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma recommended treating occupational asthma with the same approach as in
nonoccupational asthma (1).
• The 2007 Expert Panel 3 guidelines on asthma from the National Heart, Lung, and Blood Institute
and National Asthma Education and Prevention Program recommended a stepwise approach to
asthma therapy, starting with a β2-agonist in patients with intermittent asthma and using an
inhaled steroid in patients with moderate persistent (or more severe) symptoms (12).
• A 2005 AHRQ systematic evidence report on the diagnosis and management of work-related
asthma found few studies of medical therapy in this population (39).

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 20 of 29
• A randomized trial compared inhaled beclomethasone with placebo in 32 patients with occupational
asthma. The active therapy group had small improvements in symptoms and lung function
compared with the placebo group (50).
• A randomized trial compared inhaled beclomethasone with placebo in 15 patients with occupational
asthma. During and after treatment, the beclomethasone group had decreased general airway
hyperresponsiveness but did not differ in reactivity to the specific culprit antigen (51).
• In an uncontrolled case series, 10 patients with occupational asthma and ongoing workplace
exposure were treated with beclomethasone dipropionate, 500 mcg twice daily, and salmeterol, 50
mcg twice daily. Lung function and respiratory symptoms were monitored for 3 years. At the end of
the study, no significant differences in any of the morbidity outcomes (FEV1, PC20, PEFR variability,
use of rescue salbutamol, respiratory symptom score) were found as compared with baseline or
run-in values (52).
Rationale
• Clinical trials have shown improvement in clinical and functional measurements and in nonspecific
bronchial hyperresponsiveness in patients treated early with inhaled steroids after removal from
the irritant.
Comments
• Best results are obtained with exposure modification and early (less than 1 year after cessation of
exposure) initiation of therapy with inhaled steroids; however, no cures of occupational asthma
have been documented with medical therapy alone (i.e., without removal from exposure).
• For patients with asthma in general, a 2006 meta-analysis of 19 trials with almost 34,000
participants found increased exacerbations requiring hospitalization (OR, 2.6 [CI, 1.6 to 4.3]) and
life-threatening exacerbations (OR, 1.8 [CI, 1.1 to 2.9]) among users of long-acting β-agonists
compared with placebo. Hospitalizations were also significantly increased with salmeterol (OR, 1.7
[CI, 1.1 to 2.7]) and formoterol (OR, 3.2 [CI, 1.7 to 6.0]) (53).
6.4 Recommend desensitization therapy for appropriate allergens if allergen
avoidance is impossible.
Recommendations
• Consider desensitization therapy in occasional cases of high-molecular-weight antigen-induced
occupational asthma if
Allergen avoidance cannot be accomplished
Standardized allergen extract is available for the responsible antigen
• See table Drug Treatment for Occupational Asthma.
Evidence
• A 2008 guideline from the American College of Chest Physicians on the diagnosis and management
of work-related asthma stated that immunotherapy should be considered when there is a clearly
identified allergen that cannot be avoided and for which there is a specific therapy (1).
• A 2010 Cochrane review of injection allergen immunotherapy for asthma included 88 trials
involving a variety of specific allergens. Overall, the immunotherapy had more improvement in
asthma symptom scores (mean difference, -0.59 (CI, -0.83 to -0.35]) and bronchial
hyperreactivity (54).
• A comparative study evaluated the effect of desensitization therapy compared with placebo in
patients with cat-induced asthma and found that treatment resulted in significant reductions in
bronchial sensitivity and prick-test titer compared with control treatment (55).
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 21 of 29
• A study compared immunotherapy with placebo in 24 patients with latex allergy (including 16 with
asthma). There were no differences between groups in medication use or bronchial responsiveness
(56).
Rationale
• Alleviation of allergic respiratory symptoms has been shown in animal laboratory and veterinary
workers treated with desensitization therapy.
Comments
• Desensitization therapy has not been studied extensively as a treatment modality for sensitizer-
induced occupational asthma.
6.5 Consider therapy with anti-IgE antibody in patients with IgE-mediated
occupational asthma.
Recommendations
• Consider using anti-IgE antibody in IgE-mediated occupational asthma.
• Consult with an allergist if anti-IgE therapy is considered.
Evidence
• A prospective study in 546 allergic asthmatics taking inhaled steroids showed that compared with a
placebo group, the group receiving anti-IgE antibody (omalizumab) had more than 50% fewer
exacerbations per patient. Anti-IgE antibody therapy has not been evaluated extensively (57).
Rationale
• The frequency of exacerbations and the steroid requirements may be reduced in those with allergic
asthma treated with anti-IgE antibody.
Comments
• Anti-IgE antibodies have not been studied extensively as a treatment modality.
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 22 of 29
7. Patient Counseling Top
Inform patients with occupational asthma about the disease and its management.
7.1 Inform the patient about key issues concerning occupational asthma and its causes, treatment, and prognosis.
Recommendations
• Discuss with patients the triggers of their asthma and the importance of recording symptoms,
monitoring peak flow rates, and taking all prescribed medications.
• Stress the importance of avoiding or minimizing exposures to the irritant for patients that have
irritant-induced occupational asthma.
• Inform patients that most patients continue to have respiratory symptoms and increased
nonspecific bronchial hyperresponsiveness even after removal from exposure.
• Explain that it is important to use inhaled steroids early to modify the disease course but that it will
not cure occupational asthma.
• Discuss the rationale for eliminating exposure with patients that have sensitizer-induced
occupational asthma.
Evidence
• A 2003 Cochrane review of self-management education for patients with asthma included 36 trials.
Overall, self-management education improved multiple outcomes, including reducing
hospitalizations (RR, 0.64 [CI, 0.50 to 0.82]) and nocturnal symptoms (RR, 0.67 [CI, 0.56 to
0.79]), and improving quality of life (58).
Rationale
• Patient education is essential for successful management of asthma.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 23 of 29
8. Follow-up Top
Follow up regularly to monitor treatment and response in all patients with occupational asthma.
8.1 Follow patients with occupational asthma regularly after removal from exposure to the causative agent.
Recommendations
• Follow patients with occupational asthma at least every 6 months:
Monitor symptoms, airflow limitation, and nonspecific bronchial hyperresponsiveness
Monitor response to therapy
Monitor adherence to therapy
• Evaluate for permanent impairment or disability after 2 years in patients with continuing severe
symptoms.
Evidence
• A 2012 guideline from the British Thoracic Society on the management of occupational asthma
recommended that patients with confirmed or suspected occupational asthma be followed at a
specialist center every 3 months for a year and every 6 months thereafter, and that patients be
followed for a total of 3 years after removal of the exposure (30).
• Follow-up of patients with some types of occupational asthma showed that after leaving
employment, patients who remained symptomatic had had a longer duration of exposure and
symptoms and greater abnormalities in both pulmonary function and bronchial
hyperresponsiveness at the time of diagnosis (59).
• In one study, workers with occupational asthma to soldering fluxes containing colophony were
followed for 4 years. The study showed that only 10% of affected workers became symptom free
(60).
• When 99 patients with occupational asthma who had been removed from exposure were followed
up, patients removed from exposure for more than 5 years showed significant improvement in
bronchial responsiveness when compared with those removed from exposure for less than 5 years
(P=0.01). Stepwise logistic regression showed that follow-up PC20 could be predicted from baseline
PC20, duration of exposure interval since removal from exposure, and the type of agent. Patients
with occupational asthma due to high-molecular-weight agents had a less favorable outcome
(P=0.04; OR, 0.295 [CI, 0.03 to 1.0]). Treatment with inhaled steroids was not a significant
predictor. (61)
• Thirty-one workers with occupational asthma from snow-crab processing were followed over 5
years after leaving work. Total duration of exposure was approximately 1 year (12.8 months). At
the time of diagnosis, all 31 required medication for asthma. At the end of 1 year, there was a
significant reduction in patients requiring medication; there was also an improvement in FEV1 and
FEV1/FVC percentages, but they reached a plateau thereafter (62).
Rationale
• Regular follow-up is essential to optimal management, determination of impairment, and ability to
work.
8.2 Assess factors that have prognostic significance for recovery.
Recommendations
• Review factors known to have prognostic significance:

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 24 of 29
Age
Total duration of exposure
Duration of exposure after onset of symptoms
Evidence
• Among workers with red cedar asthma followed for 3.5 years, those who remained at their jobs
after diagnosis had worsening of symptoms and increased nonspecific bronchial
hyperresponsiveness (63)
• Follow-up of patients with some types of occupational asthma showed that after leaving
employment, patients who remained symptomatic had had a longer duration of exposure and
symptoms and greater abnormalities in both pulmonary function and bronchial
hyperresponsiveness at the time of diagnosis (59).
• A study followed a cohort of 31 workers with occupational asthma caused by snow-crab processing
over a period of approximately 5 years (64.4 ± 6.3 months) after they had left this work. Diagnosis
was established in most workers by specific inhalational challenge. At the initial follow-up at 1 year
(12.8 ± 5.4 months), there was a decrease in the number of participants still requiring medication
who had a significant reduction in FEV1 and a PC20≤16 mg/mL. Interestingly, there was no further
change observed with time. The mean FEV1 and FEV1/FEV percentages improved significantly from
the diagnosis to the first follow-up but did not change thereafter (64).
Rationale
• Complete recovery requires early diagnosis and removal from the source of exposure.
8.3 Monitor all patients who remain continuously exposed to irritants.
Recommendations
• Continuously monitor patients with occupational asthma who remain exposed to the causative
agent.
Evidence
• A 2011 systematic review of exposure elimination or reduction for patients with occupational
asthma included 14 studies. Overall, reduction in exposure was associated with a lower rates of
asthma symptom improvement (OR, 0.16 [CI, 0.03 to 0.91]) and recovery (OR, 0.30 [CI, 0.11 to
0.84]) compared with complete exposure avoidance (49).
• A 2005 AHRQ systematic evidence report on the diagnosis and management of work-related
asthma found that workers with continued exposure generally experienced further deterioration in
FEV1 and that those for whom the exposure was eliminated generally had improvements in FEV1
(39).
• A follow-up study of workers with cedar asthma who were still working in the same industry after
an average of 6.5 years showed that over one third experienced deterioration in their asthma
symptoms (65).
• In one study, workers with occupational asthma to soldering fluxes containing colophony were
followed for 4 years. The study showed that only 10% of affected workers became symptom free
(60).
Rationale
• Affected workers who are continuously exposed do not recover and may deteriorate.
8.4 Recognize the importance of reporting cases of occupational asthma to government agencies.
Recommendations

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 25 of 29
• Recognize that under the OSHA act of 1970, physicians are obligated to report cases of
occupational asthma to state and county health departments.
• See table Prevention Measures Instituted by Employers.
Evidence
• Public health surveillance includes the SENSOR program, which NIOSH initiated first as a pilot
project in an effort to improve occupational disease surveillance reporting. Occupational asthma is
a target condition for the SENSOR program. Reporting guidelines and surveillance case definition
have been standardized (9).
• Approaches to the prevention of occupational asthma include primary, secondary, and tertiary
prevention strategies. Such strategies may be employed in sensitizer-induced asthma. Screening
programs have value because early detection may improve long-term prognosis (10).
Rationale
• The diagnosis of occupational asthma in a patient should be regarded as a sentinel event because
the prevalence of asthma can be high in industries where a case of occupational asthma has been
identified.
• Disease surveillance is an integral component in the prevention of occupational asthma by
providing information on how common asthma is in relationship to other occupational lung diseases
and on the relative frequency with which different agents cause asthma.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 26 of 29
References Top
1. Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, et al. Diagnosis and management of work-related asthma:
American College Of Chest Physicians Consensus Statement. Chest. 2008;134:1S-41S. (PMID: 18779187)
2. Nicholson PJ, Cullinan P, Taylor AJ, Burge PS, Boyle C. Evidence based guidelines for the prevention, identification, and management of occupational asthma. Occup Environ Med. 2005;62:290-9. (PMID: 15837849)
3. Wilken D, Baur X, Barbinova L, Preisser A, Meijer E, Rooyackers J, et al.; ERS Task Force on the Management of Work-related Asthma. What are the benefits of medical screening and surveillance? Eur Respir Rev. 2012;21:105-11. (PMID: 22654082)
4. LaMontagne AD, Radi S, Elder DS, Abramson MJ, Sim M. Primary prevention of latex related sensitisation and occupational asthma: a systematic review. Occup Environ Med. 2006;63:359-64. (PMID: 16469822)
5. Tarlo SM, Liss GM. Prevention of occupational asthma--practical implications for occupational physicians. Occup Med (Lond). 2005;55:588-94. (PMID: 16314329)
6. Górski P. Global Initiative for Asthma 2002—what concerns occupational medicine [Editorial]. Int J Occup Med Environ Health. 2002;15:207-8. (PMID: 12462447)
7. Taivainen AI, Tukiainen HO, Terho EO, Husman KR. Powered dust respirator helmets in the prevention of occupational asthma among farmers. Scand J Work Environ Health. 1998;24:503-7. (PMID: 9988093)
8. Mûller-Wening D, Neuhauss M. Protective effect of respiratory devices in farmers with occupational asthma. Eur Respir J. 1998;12:569-72. (PMID: 9762781)
9. Matte TD, Hoffman RE, Rosenman KD, Stanbury M. Surveillance of occupational asthma under the SENSOR model. Chest. 1990;98:173S-178S. (PMID: 2226005)
10. Venables KM. Prevention of occupational asthma. Eur Respir J. 1994;7:768-78. (PMID: 8005261)
11. Sarlo K. Control of occupational asthma and allergy in the detergent industry. Ann Allergy Asthma Immunol. 2003;90:32-4. (PMID: 12772949)
12. National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol. 2007;120:S94-138. (PMID: 17983880)
13. Balmes J, Becklake M, Blanc P, Henneberger P, Kreiss K, Mapp C, et al. American Thoracic Society Statement: Occupational contribution to the burden of airway disease. Am J Respir Crit Care Med. 2003;167:787-97. (PMID: 12598220)
14. Ameille J, Hamelin K, Andujar P, Bensefa-Colas L, Bonneterre V, Dupas D, et al.; members of the rnv3p. Occupational asthma and occupational rhinitis: the united airways disease model revisited. Occup Environ Med. 2013;70:471-5. (PMID: 23390199)
15. Blanc PD, Galbo M, Hiatt P, Olson KR. Morbidity following acute irritant inhalation in a population-based study. JAMA. 1991;266:664-9. (PMID: 2072476)
16. Kogevinas M, Zock JP, Jarvis D, Kromhout H, Lillienberg L, Plana E, et al. Exposure to substances in the workplace and new-onset asthma: an international prospective population-based study (ECRHS-II). Lancet. 2007;370:336-41. (PMID: 17662882)
17. Arif AA, Delclos GL, Whitehead LW, Tortolero SR, Lee ES. Occupational exposures associated with work-related asthma and work-related wheezing among U.S. workers. Am J Ind Med. 2003;44:368-76. (PMID: 14502764)
18. Karjalainen A, Kurppa K, Martikainen R, Klaukka T, Karjalainen J. Work is related to a substantial portion of adult-onset asthma incidence in the Finnish population. Am J Respir Crit Care Med. 2001;164:565-8. (PMID: 11520716)
19. Vandenplas O, Ghezzo H, Munoz X, Moscato G, Perfetti L, Lemiere C, et al. What are the questionnaire items most useful in identifying subjects with occupational asthma? Eur Respir J. 2005;26:1056-63. (PMID: 16319335)
20. Gautrin D, Ghezzo H, Malo JL. Rhinoconjunctivitis, bronchial responsiveness, and atopy as determinants for incident non-work-related asthma symptoms in apprentices exposed to high-molecular-weight allergens. Allergy. 2003;58:608-15. (PMID: 12823119)
21. Jaakkola MS, Leino T, Tammilehto L, Ylöstalo P, Kuosma E, Alanko K. Respiratory effects of exposure to methacrylates among dental assistants. Allergy. 2007;62:648-54. (PMID: 17508969)
22. Jaakkola JJ, Jaakkola MS. Professional cleaning and asthma. Curr Opin Allergy Clin Immunol. 2006;6:85-90. (PMID: 16520670)
23. Vandenplas O. Occupational asthma: etiologies and risk factors. Allergy Asthma Immunol Res. 2011;3:157-67. (PMID: 21738881)
24. Shofer S, Haus BM, Kuschner WG. Quality of occupational history assessments in working age adults with newly diagnosed asthma. Chest. 2006;130:455-62. (PMID: 16899845)
25. Pratter MR, Curley FJ, Dubois J, Irwin RS. Cause and evaluation of chronic dyspnea in a pulmonary disease clinic. Arch Intern Med. 1989;149:2277-82. (PMID: 2802893)

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 27 of 29
26. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, et al. Guidelines for methacholine and exercise challenge
testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000;161:309-29. (PMID: 10619836)
27. Knoeller GE, Mazurek JM, Moorman JE. Work-related asthma among adults with current asthma in 33 states and DC: evidence from the Asthma Call-Back Survey, 2006-2007. Public Health Rep. 2011;126:603-11. (PMID: 21800756)
28. Jajosky RA, Harrison R, Reinisch F, Flattery J, Chan J, Tumpowsky C, et al. Surveillance of work-related asthma in selected U.S. states using surveillance guidelines for state health departments—California, Massachusetts, Michigan, and New Jersey, 1993-1995. Mor Mortal Wkly Rep CDC Surveill Summ. 1999;48:1-20. (PMID: 10421216)
29. McDonald JC, Chen Y, Zekveld C, Cherry NM. Incidence by occupation and industry of acute work related respiratory diseases in the UK, 1992-2001. Occup Environ Med. 2005;62:836-42. (PMID: 16299091)
30. Fishwick D, Barber CM, Bradshaw LM, Ayres JG, Barraclough R, Burge S, et al. Standards of care for occupational asthma: an update. Thorax. 2012;67:278-80. (PMID: 22156958)
31. Mirabelli MC, London SJ, Charles LE, Pompeii LA, Wagenknecht LE. Occupation and the prevalence of respiratory health symptoms and conditions: the Atherosclerosis Risk in Communities Study. J Occup Environ Med. 2012;54:157-65. (PMID: 22157701)
32. Beckett WS. Occupational respiratory diseases. N Engl J Med. 2000;342:406-13. (PMID: 10666432)
33. Work-related lung disease: surveillance report. U.S. Dept of Health and Human Services, Division of Respiratory Disease, NIOSH; 1999:157-8.
34. Brooks SM, Hammad Y, Richards I, Giovinco-Barbas J, Jenkins K. The spectrum of irritant-induced asthma: sudden and not-so-sudden onset and the role of allergy. Chest. 1998;113:42-9. (PMID: 9440566)
35. Malo JL, L’archevêque J, Castellanos L, Lavoie K, Ghezzo H, Maghni K. Long-term outcomes of acute irritant-induced asthma. Am J Respir Crit Care Med. 2009;179:923-8. (PMID: 19234102)
36. Malo JL, Cartier A, Boulet LP, L’Archeveque J, Saint-Denis F, Bherer L, et al. Bronchial hyperresponsiveness can improve while spirometry plateaus two to three years after repeated exposure to chlorine causing respiratory symptoms. Am J Respir Crit Care Med. 1994;150:1142-5. (PMID: 7921449)
37. Aasen TB, Burge PS, Henneberger PK, Schlünssen V, Baur X; EOM Society. Diagnostic approach in cases with suspected work-related asthma. J Occup Med Toxicol. 2013;8:17. (PMID: 23768266)
38. Maghni K, Lemière C, Ghezzo H, Yuquan W, Malo JL. Airway inflammation after cessation of exposure to agents causing occupational asthma. Am J Respir Crit Care Med. 2004;169:367-72. (PMID: 14578217)
39. Beach J, Rowe BH, Blitz S, Crumley E, Hooton N, Russell K, et al. Diagnosis and management of work-related asthma. Evid Rep Technol Assess (Summ). 2005;:1-8. (PMID: 16354102)
40. Leroyer C, Perfetti L, Trudeau C, L’Archevêque J, Chan-Yeung M, Malo JL. Comparison of serial monitoring of peak expiratory flow and FEV1 in the diagnosis of occupational asthma. Am J Respir Crit Care Med. 1998;158:827-32. (PMID: 9731012)
41. Perrin B, Lagier F, L’Archevêque J, Cartier A, Boulet LP, Côté J, et al. Occupational asthma: validity of monitoring of peak expiratory flow rates and non-allergic bronchial responsiveness as compared to specific inhalation challenge. Eur Respir J. 1992;5:40-8. (PMID: 1577147)
42. Baldwin DR, Gannon P, Bright P, Newton DT, Robertson A, Venables K, et al. Interpretation of occupational peak flow records: level of agreement between expert clinicians and Oasys-2. Thorax. 2002;57:860-4. (PMID: 12324671)
43. Anees W, Gannon PF, Huggins V, Pantin CF, Burge PS. Effect of peak expiratory flow data quantity on diagnostic sensitivity and specificity in occupational asthma. Eur Respir J. 2004;23:730-4. (PMID: 15176688)
44. Sander I, Merget R, Degens PO, Goldscheid N, Brüning T, Raulf-Heimsoth M. Comparison of wheat and rye flour skin prick test solutions for diagnosis of baker's asthma. Allergy. 2004;59:95-8. (PMID: 14674940)
45. Brant A, Zekveld C, Welch J, Jones M, Taylor AN, Cullinan P. The prognosis of occupational asthma due to detergent enzymes: clinical, immunological and employment outcomes. Clin Exp Allergy. 2006;36:483-8. (PMID: 16630153)
46. Emanuel DA, Wenzel FJ, Lawton BR. Pulmonary mycotoxicosis. Chest. 1975;67:293-7. (PMID: 46192)
47. Christiani DC, Ye TT, Wegman DH, Eisen EA, Dai HL, Lu PL. Cotton dust exposure, across-shift drop in FEV1, and five-year change in lung function. Am J Respir Crit Care Med. 1994;150:1250-5. (PMID: 7952548)
48. Bartter T, Pratter MR. Asthma: better outcome at lower cost? The role of the expert in the care system. Chest. 1996;110:1589-96. (PMID: 8989082)
49. Vandenplas O, Dressel H, Wilken D, Jamart J, Heederik D, Maestrelli P, et al. Management of occupational asthma: cessation or reduction of exposure? A systematic review of available evidence. Eur Respir J. 2011;38:804-11. (PMID: 21436354)

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 28 of 29
50. Malo JL, Cartier A, Côté J, Milot J, Leblanc C, Paquette L, et al. Influence of inhaled steroids on recovery from occupational
asthma after cessation of exposure: an 18-month double-blind crossover study. Am J Respir Crit Care Med. 1996;153:953-60. (PMID: 8630579)
51. Maestrelli P, De Marzo N, Saetta M, Boscaro M, Fabbri LM, Mapp CE. Effects of inhaled beclomethasone on airway responsiveness in occupational asthma. Placebo-controlled study of subjects sensitized to toluene diisocyanate. Am Rev Respir Dis. 1993;148:407-12. (PMID: 8393638)
52. Marabini A, Siracusa A, Stopponi R, Tacconi C, Abbritti G. Outcome of occupational asthma in patients with continuous exposure: a 3-year longitudinal study during pharmacologic treatment. Chest. 2003;124:2372-6. (PMID: 14665523)
53. Salpeter SR, Buckley NS, Ormiston TM, Salpeter EE. Meta-analysis: effect of long-acting beta-agonists on severe asthma exacerbations and asthma-related deaths. Ann Intern Med. 2006;144:904-12. [Full Text] (PMID: 16754916)
54. Abramson MJ, Puy RM, Weiner JM. Injection allergen immunotherapy for asthma. Cochrane Database Syst Rev. 2010;(8):CD001186. (PMID: 20687065)
55. Ohman JL Jr, Findlay SR, Leitermann KM. Immunotherapy in cat-induced asthma. Double-blind trial with evaluation of in vivo and in vitro responses. J Allergy Clin Immunol. 1984;74:230-9. (PMID: 6206105)
56. Sastre J, Fernández-Nieto M, Rico P, Martín S, Barber D, Cuesta J, et al. Specific immunotherapy with a standardized latex extract in allergic workers: a double-blind, placebo-controlled study. J Allergy Clin Immunol. 2003;111:985-94. (PMID: 12743562)
57. Buhl R, Hanf G, Solèr M, Bensch G, Wolfe J, Everhard F, et al. The anti-IgE antibody omalizumab improves asthma-related quality of life in patients with allergic asthma. Eur Respir J. 2002;20:1088-94. (PMID: 12449159)
58. Gibson PG, Powell H, Coughlan J, Wilson AJ, Abramson M, Haywood P, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev. 2003;(1):CD001117. (PMID: 12535399)
59. Chan-Yeung M, Lam S, Koener S. Clinical features and natural history of occupational asthma due to western red cedar (Thuja plicata). Am J Med. 1982;72:411-5. (PMID: 7058838)
60. Burge PS. Occupational asthma in electronics workers caused by colophony fumes: follow-up of affected workers. Thorax. 1982;37:348-53. (PMID: 7112471)
61. Perfetti L, Cartier A, Ghezzo H, Gautrin D, Malo JL. Follow-up of occupational asthma after removal from or diminution of exposure to the responsible agent: relevance of the length of the interval from cessation of exposure. Chest. 1998;114:398-403. (PMID: 9726721)
62. Pisati G, Baruffini A, Zedda S. Toluene diisocyanate induced asthma: outcome according to persistence or cessation of exposure. Br J Ind Med. 1993;50:60-4. (PMID: 8381658)
63. Chan-Yeung M. Fate of occupational asthma. A follow-up study of patients with occupational asthma due to Western Red Cedar (Thuja plicata). Am Rev Respir Dis. 1977;116:1023-9. (PMID: 931178)
64. Malo JL, Cartier A, Ghezzo H, Lafrance M, McCants M, Lehrer SB. Patterns of improvement in spirometry, bronchial hyperresponsiveness, and specific IgE antibody levels after cessation of exposure in occupational asthma caused by snow-crab processing. Am Rev Respir Dis. 1988;138:807-12. (PMID: 3202454)
65. Cote J, Kennedy S, Chan-Yeung M. Outcome of patients with cedar asthma with continuous exposure. Am Rev Respir Dis. 1990;141:373-6. (PMID: 1689129)

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 29 of 29
Glossary Top
ACGIH American Conference of Governmental Industrial Hygienists
AHRQ Agency for Healthcare Research and Quality
CI confidence interval
ELISA enzyme-linked immunosorbent assay
FEV1 forced expiratory volume in 1 second
FVC
forced vital capacity
IgE immunoglobulin E
NHANES III Third National Health and Nutrition Examination Survey, 1988-1994
NIOSH
National Institute of Occupational Safety and Health
NPV negative predictive value
OR odds ratio
OSHA U.S. Occupational Safety and Health Administration
PC20 provocative dose causing a 20% fall in FEV1
PEFR peak expiratory flow rate
PPV positive predictive value
RADS
reactive airway dysfunction syndrome
RAST radioallergosorbent
RR relative risk
SENSOR
Sentinel Event Notification System for Occupational Risk
SWORD Surveillance of work-related and occupational respiratory disease (UK)

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 30 of 14
Tables Top
Laboratory and Other Studies for Occupational Asthma
Test Sensitivity/Specificity (%) Notes
Pulmonary function tests Easy and inexpensive, but there is no standardized method of
interpretation. Results can vary
Serial peak flow rates over 4 weeks 81.8/93.8 If at least 4 readings per day (though 8 was optimal); based on a
case-control study
Serial peak flow rates over 2 weeks 70-82/82-100 For at least 4 readings per day; based on a case-control study and
a small prospective cohort study
Serial FEV1 over 2 weeks 45-55/56-100 Based on a small prospective cohort study
FEV1 measurement before and after work Low sensitivity
Methacholine challenge test (PC20) 66.7/63.9 Based on pooled data.
Bronchial hyperresponsiveness can also be evaluated with a
histamine challenge test.
The PC20 is defined as the provocative concentration of
methacholine inducing a 20% drop in FEV1
Immunologic tests
Skin-prick test 72.9/86.2 (low-molecular-weight antigen exposure)
80.6/59.6 (high-molecular-weight antigen exposure)
Accuracy differs if exposure was to low-molecular-weight antigens
or high-molecular-weight antigens
Serum IgE testing 31.2/88.9 (low-molecular-weight antigen exposure)
73.3/79 (high-molecular-weight antigen exposure)
Accuracy differs if exposure was to low molecular-weight-antigens
or high–molecular-weight antigens
Chest x-ray May be useful in excluding other or concomitant pulmonary
disorders
FEV1 = forced expiratory volume in 1 second; IgE = immunoglobulin E; PC20 = provocative dose causing a 20% fall in FEV1.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 31 of 14
Differential Diagnosis of Occupational Asthma
Disease Characteristics
Occupational asthma New diagnosis of asthma related to exposure in the workplace. Characterized by worsening of
symptoms during or after exposure to work environment and can be related to an irritant or an
identifiable allergen.
Associated with a wide variety of exposures
Asthma (non-work-related) Reactive airway disease unrelated to work environment. Initial diagnostic testing is the same as for
occupational asthma
Work-exacerbated asthma Preexisting asthma worsened by the work environment. Differentiated from occupational asthma based
on history
Bronchiolitis obliterans Obliterative fibrotic disease of the terminal bronchioles that can follow exposure to toxic irritants,
gases, or fumes.
Associated with ammonia, chlorine, hydrogen sulfide, nitrogen dioxide, phosgene
Hypersensitivity pneumonitis Immunologic inflammatory reaction involving the lung interstitium, terminal bronchioles, and alveoli
that is due to hypersensitivity to antigenic organic dusts encountered in some occupations.
Can also occur after exposure to certain chemicals
Metal fume fever/polymer fume fever Flulike illness occurring up to 12 hours after exposure to fumes from metal oxides (or fumes from heated fluorocarbons [Teflon]).
Symptoms resolve within 36 hours (weekends and vacations). Symptoms include fever (38.9°C
[102°F] to 40.0°C [104°F]), marked chest pains, muscle ache, and extreme weakness, sometimes with
a metallic taste in the mouth. Leukocytosis and normal chest x-ray are characteristic. Repeated attacks
are common
Byssinosis Chest tightness that develops on first returning to work in cotton or flax workers. Associated with a
decline in ventilatory capacity over the first work shift of the week
Organic dust toxic syndrome Flulike illness with symptoms that include fever, myalgia, chest tightness, cough, headache, and
dyspnea, resulting from inhalation of organic dusts or aerosols containing large quantities of
microorganisms.
Symptoms appear 3-8 hours after exposure

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 32 of 14
Drug Treatment for Occupational Asthma
Drug or Drug Class Dosing Side Effects Precautions Clinical Use
Inhaled short-acting β2-agonists Sympathomimetic effects, such as
tremor and tachycardia. Hypokalemia,
hyperglycemia, hypersensitivity
reactions
Caution with CV disease,
hyperthyroidism, diabetes, narrow-
angle glaucoma, seizure disorder
First line for mild, intermittent
symptoms
Albuterol (Proventil HFA, Ventolin HFA,
Proair HFA, Accuneb)
MDI (90 mcg/ inhalation): 2 inhalations
q4-6hr prn. Nebulizer: 2.5 mg q6-8hr
prn. For acute exacerbations, MDI can
increase to 4-8 puffs q1-4hr, or
nebulizer to 2.5-10 mg q1-4hr
Levalbuterol (Xopenex, Xopenex HFA) MDI (45 mcg/ inhalation): 2 inhalations
q4-6hr prn, Nebulizer: 0.63-1.25 mg q8hr. For acute exacerbations, MDI can
increase to 4-8 inhalations q1-4hr, or
nebulizer to 1.25-5 mg q1-4hr
Pirbuterol (Maxair) MDI (200 mcg/ inhalation): 2
inhalations q4-6hr prn. For acute
exacerbations, can increase to 4-8
inhalations q1-4hr
Inhaled corticosteroids Dose depends on previous asthma
therapy
Xerostomia, flushing, cataracts,
glaucoma, oral candidiasis, hoarseness,
purpura. Low incidence of HPA
suppression, bone loss
Caution with diabetes For mild-severe persistent asthma
Beclomethasone (QVAR) Inhaler (40, 80 mcg/inhalation): 40-
160 mcg bid
Budesonide (Pulmicort Flexhaler,
Pulmicort Turbuhaler)
DPI (90, 180 mcg/ inhalation): 360
mcg bid. DPI (200 mcg/inhalation): 200-400 mcg bid
Ciclesonide (Alvesco) MDI (80, 160 mcg/inhalation):80-320 mcg bid
Flunisolide (Aerospan HFA) Inhaler (80 mcg/inhalation): 160 mcg bid
Fluticasone (Flovent HFA, Flovent
Diskus)
MDI (44, 110, 220 mcg/inhalation):
88-440 mcg bid. DPI (50, 100, 250
mcg/inhalation): 100-1000 mcg bid
Mometasone (Asmanex Twisthaler) DPI (110, 220 mcg/inhalation): 220
mcg qd in the PM. Maximum 220-440
mcg bid
Triamcinolone (Azmacort) MDI (75 mcg/ inhalation): 150 mcg tid-
qid or 300 mcg bid. Maximum 1200
mcg total daily dose
Leukotriene modifiers Rare neuropsychiatric events Alternatives for mild-to-moderate

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 33 of 14
persistent asthma
Montelukast (Singulair) 10 mg qd in the PM Rare systemic eosinophilia
Zafirlukast (Accolate) 20 mg bid Elevated hepatic enzymes,
hypersensitivity reactions, rare
systemic eosinophilia
Avoid with hepatic disease. Inhibits
CYPs 1A2, 2C8, 2C9 and 3A4.
Increased INR with warfarin
Zileuton (Zyflo CR) Extended-release: 1200 mg bid, within
1 hr after meals
Elevated hepatic enzymes, flulike
syndrome
Avoid with hepatic disease. Check LFTs
at baseline and periodically. Substrate and potent inhibitor of CYP1A2
Respiratory anti-inflammatory
agent
Cromolyn (Intal) MDI (800 mcg/ spray): 2 sprays qid.
Nebulizer: 20 mg qid
Bronchospasm, throat irritation, cough,
severe anaphylactoid reactions
Alternative for mild persistent asthma
Inhaled long-acting β2-agonists Sympathomimetic effects, such as
tremor and tachycardia. Paradoxical
bronchospasm, hypersensitivity
reactions. Rare: hypokalemia,
hyperglycemia
Asthma-related death. Caution with
CV disease, hyperthyroidism, diabetes,
narrow-angle glaucoma, seizure
disorder. Tolerance can occur over time
For moderate to severe persistent
asthma. Must also use an asthma
controller
Formoterol (Foradil Aerolizer) Powder in capsules for use with
Aerolizer: 12 mcg q12hr
Salmeterol (Serevent Diskus) 50 mcg (1 oral inhalation) q12hr
Oral Corticosteroids Long-term use can result in HPA
suppression, immunosuppression,
hypertension, adverse neurologic
effects, glucose intolerance, weight
gain, myopathy, cataracts,
osteoporosis
For acute exacerbations. Not generally
for long-term use
Prednisone 40-80 mg total daily dose, dosed qd-bid, for a total course of 3-10 days
Prednisolone (Prelone, Flo-Pred, Orapred)
40-80 mg total daily dose, dosed qd-bid, for a total course of 3-10 days
Methylprednisolone (Medrol) PO or IV: 40-80 mg total daily dose,
dosed qd-bid, for a total course of 3-10
days
Methylxanthine
Theophylline (Theolair, Theochron,
Theo-24)
Dose must be individualized. Aim for
serum levels between 5 and 15
mcg/mL. IV: 0.2-0.4 mg/kg/hr
Immediate-release: Initially 300 mg
total daily dose, dosed q6-8hr. Can
increase to 400-1600 mg total daily
dose, dosed q6-8hr. Extended-release:
Initially 300 mg total daily dose, dosed
q8-12hr. Can increase to 400-1600 mg total daily dose, dosed q8-12hr.
GI side effects, CV adverse effects Narrow therapeutic index. Many drug
interactions due to CYP450 hepatic
metabolism. Use low dose with:
hepatic disease, HF, elderly. Caution
with cardiac disease, thyroid disease,
peptic ulcer disease, prostatic
hypertrophy, seizure disorder, smoking
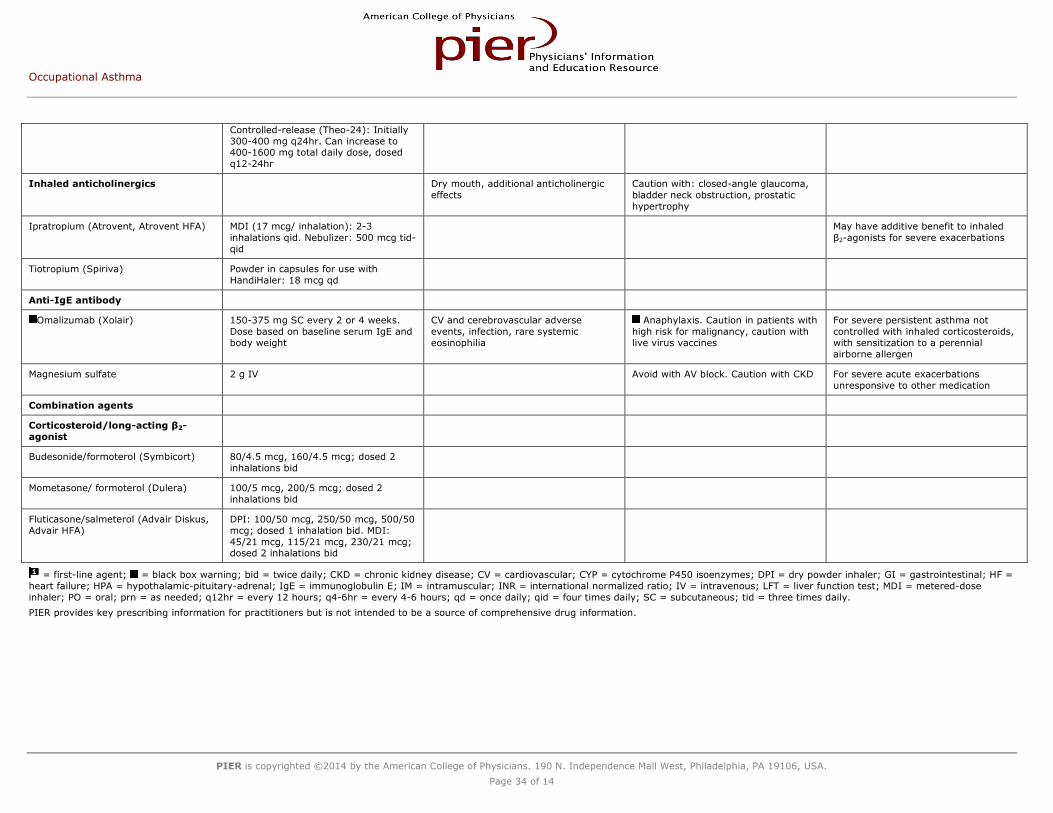
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 34 of 14
Controlled-release (Theo-24): Initially
300-400 mg q24hr. Can increase to 400-1600 mg total daily dose, dosed
q12-24hr
Inhaled anticholinergics Dry mouth, additional anticholinergic
effects
Caution with: closed-angle glaucoma,
bladder neck obstruction, prostatic
hypertrophy
Ipratropium (Atrovent, Atrovent HFA) MDI (17 mcg/ inhalation): 2-3
inhalations qid. Nebulizer: 500 mcg tid-
qid
May have additive benefit to inhaled
β2-agonists for severe exacerbations
Tiotropium (Spiriva) Powder in capsules for use with
HandiHaler: 18 mcg qd
Anti-IgE antibody
Omalizumab (Xolair) 150-375 mg SC every 2 or 4 weeks.
Dose based on baseline serum IgE and
body weight
CV and cerebrovascular adverse
events, infection, rare systemic
eosinophilia
Anaphylaxis. Caution in patients with
high risk for malignancy, caution with
live virus vaccines
For severe persistent asthma not
controlled with inhaled corticosteroids,
with sensitization to a perennial
airborne allergen
Magnesium sulfate 2 g IV Avoid with AV block. Caution with CKD For severe acute exacerbations
unresponsive to other medication
Combination agents
Corticosteroid/long-acting β2-
agonist
Budesonide/formoterol (Symbicort) 80/4.5 mcg, 160/4.5 mcg; dosed 2
inhalations bid
Mometasone/ formoterol (Dulera) 100/5 mcg, 200/5 mcg; dosed 2
inhalations bid
Fluticasone/salmeterol (Advair Diskus,
Advair HFA)
DPI: 100/50 mcg, 250/50 mcg, 500/50
mcg; dosed 1 inhalation bid. MDI:
45/21 mcg, 115/21 mcg, 230/21 mcg; dosed 2 inhalations bid
= first-line agent; = black box warning; bid = twice daily; CKD = chronic kidney disease; CV = cardiovascular; CYP = cytochrome P450 isoenzymes; DPI = dry powder inhaler; GI = gastrointestinal; HF =
heart failure; HPA = hypothalamic-pituitary-adrenal; IgE = immunoglobulin E; IM = intramuscular; INR = international normalized ratio; IV = intravenous; LFT = liver function test; MDI = metered-dose
inhaler; PO = oral; prn = as needed; q12hr = every 12 hours; q4-6hr = every 4-6 hours; qd = once daily; qid = four times daily; SC = subcutaneous; tid = three times daily.
PIER provides key prescribing information for practitioners but is not intended to be a source of comprehensive drug information.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 35 of 14
Select Agents Reported to Be Associated with Reactive Airway Dysfunction Syndrome
Uranium hexafluoride
Hydrazine (35%)
Ammonia (paint spray) fumigating fog
Metal coating remover
Smoke
Floor sealant
Sulfur dioxide
Silo dust
Acetic acid
Anhydrous ammonia
Chlorine
Toluene diisocyanate

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 36 of 14
Indications for Peak Flow Monitoring
Patients suspected of having occupational asthma when symptoms and exposures occur
When a new agent is suspected of causing occupational asthma
As a first screening test in establishing work-related problems
When specific challenge testing in the laboratory is not possible
When specific challenge testing result is negative but the history suggests occupational asthma
To document work aggravation of asthma
To determine whether the work environment is safe for the patient
To record when a bronchodilator is used

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 37 of 14
Select Agents Associated with Occupational Asthma with or without a Latency
Onset after a Latent Period
Acid anhydrides
Aldehydes (formaldehyde, glutaraldehyde)
Acrylates
Animal proteins
Cobalt
Dusts from flour and grains
Dust from wood
Amines (ethylene diamine, monoethanolamine)
Isocyanates (toluene diisocyanate, hexamethylene diisocyanate)
Latex
Green tea/epigallocatechin
Food and cosmetic coloring/carmine
Freeze-dried raspberry powder
Fungicides/fluazinam and chlorothalonil
Onset without a Previous Latent Period
Contaminants in metalworking fluids
Chlorine gas (pulp from paper mills)
Bleach (sodium hypochlorite)
Strong acids

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 38 of 14
Prevention Measures Instituted by Employers*
Primary prevention
Elimination of the agent from the workplace either by substitution of the agent or a change in the process
Reduction of exposure through better local exhaust, isolation, and enclosure
Exclusion of susceptible individuals from high-risk workplaces after the preemployment examination
Secondary prevention
Early detection of disease using periodic examinations
Tertiary prevention
Prevention of permanent asthma with early recognition and removal from the source of exposure
* For patients with risk factors for occupational asthma including atopy, smoking, level of exposure, and possibly certain human leukocyte antigen class 2 genes, because these workers may be more
susceptible to the disease. Atopy may be defined as a personal history of allergic respiratory symptoms, cutaneous reactivity, or both to common environmental allergens.

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 39 of 14
Proper Technique for Recording Portable Peak Flow Rate Recordings
Standing upright position
No nose clip
Firm seal around the mouthpiece
Lungs filled to total capacity at the start of the test
A short forced expiratory maneuver is done as hard and fast as possible
The greatest of three consecutive measurements is recorded
The maximum mean and minimum peak flow rates over each day are plotted
Peak flow rates are recorded at least 4 times per day with 2 recordings at work and 2 away from work
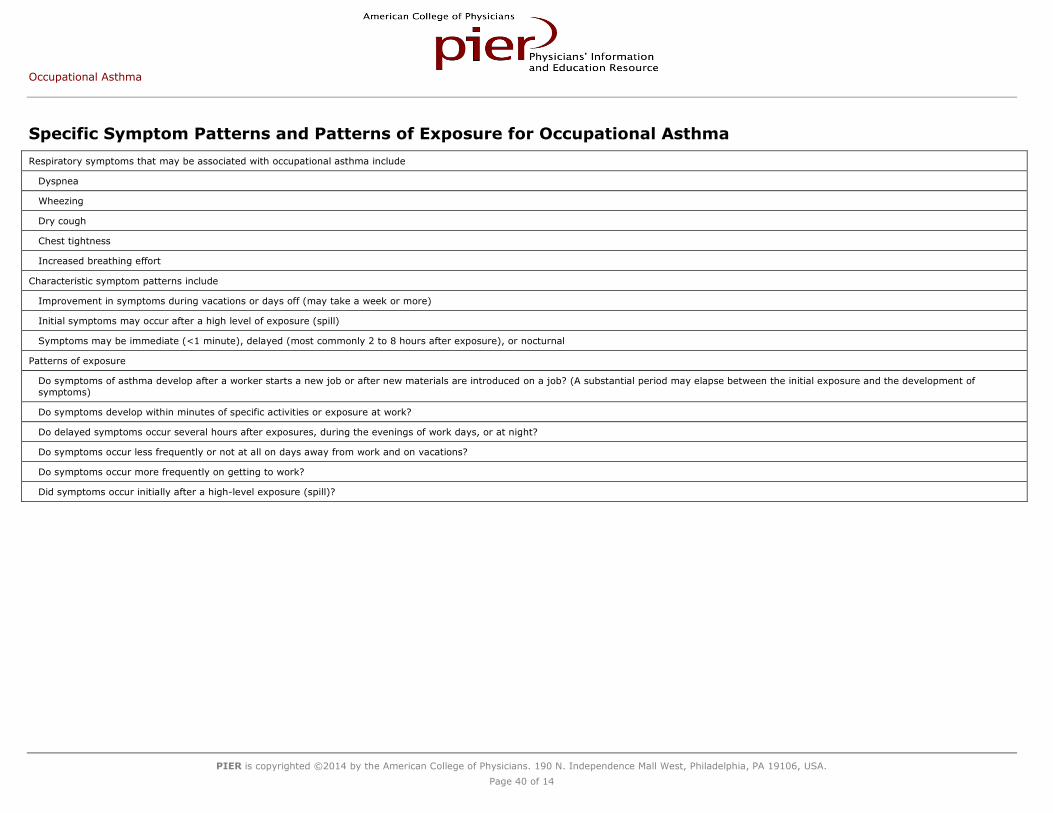
Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 40 of 14
Specific Symptom Patterns and Patterns of Exposure for Occupational Asthma
Respiratory symptoms that may be associated with occupational asthma include
Dyspnea
Wheezing
Dry cough
Chest tightness
Increased breathing effort
Characteristic symptom patterns include
Improvement in symptoms during vacations or days off (may take a week or more)
Initial symptoms may occur after a high level of exposure (spill)
Symptoms may be immediate (<1 minute), delayed (most commonly 2 to 8 hours after exposure), or nocturnal
Patterns of exposure
Do symptoms of asthma develop after a worker starts a new job or after new materials are introduced on a job? (A substantial period may elapse between the initial exposure and the development of
symptoms)
Do symptoms develop within minutes of specific activities or exposure at work?
Do delayed symptoms occur several hours after exposures, during the evenings of work days, or at night?
Do symptoms occur less frequently or not at all on days away from work and on vacations?
Do symptoms occur more frequently on getting to work?
Did symptoms occur initially after a high-level exposure (spill)?

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 41 of 14
Questionnaire: Determining Whether Asthma Symptoms Are Work Related
Did the symptoms of asthma start after you started a new job or when new materials were introduced at your job?
Do the symptoms of asthma develop within minutes after exposures or with specific activities at work?
Do symptoms occur several hours after exposures or during the evenings on workdays?
Do symptoms occur less often or not at all on days off work or on vacations?
Do symptoms occur frequently on returning to work?

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 42 of 14
Diagnostic Criteria for Asthma
A typical history, clinical features, and course must be recorded as well as a continuing regular use of asthma medication that has lasted for 6 months plus at least one of the following criteria:
A variation of more than 20% diurnal peak expiratory flow recording (reference to maximal value)
An increase of more than 15% in peak expiratory flow or FEV1 with β2 agonist
A decrease of more than 15% in peak expiratory flow or FEV1 in exercise testing

Occupational Asthma
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 43 of 14
Figures Top
Diagnostic Flowchart for Occupational Asthma