observing best practice in parent-infant psychotherapy y... · afc anna freud centre afc anna freud...
TRANSCRIPT

Observing Best
Practice in
Parent-Infant
Psychotherapy
Yvonne Osafo
Parent-Infant Psychoanalytic
Psychotherapist (UKCP)
2016 Fellow

ii
Copyright © 2018 by Yvonne M Osafo. The moral right of the author has been asserted.
The views and opinions expressed in this report and its content are those of the author and not of the
Winston Churchill Memorial Trust, which has no responsibility or liability for any part of the report.
iii
Contents
Declaration ii
Contents iii
Abbreviations iv
Acknowledgements 1
Executive Summary 2
My Background 3
Introduction to the Project 4
Context 4
What is Parent-Infant Psychotherapy 4
Aims, Objectives and Purpose of the Project 5
Approach 6
Overview of my Fellowship Travels 6
Lessons from Sweden 10
Lessons from Norway 15
Lessons from Michigan 23
Lessons from California 33
Recommendations for the UK 37
Dissemination 39
References 41
Itinerary 42

iv
Abbreviations
AAIMH Alliance for the Advancement of Infant Mental Health
AFC Anna Freud Centre
AFC Anna Freud Centre
AIMH UK Association for Infant Mental Health UK
ASQ Ages & Stages Questionnaire
ASQ-SE Ages & Stages Questionnaire-Social Emotional
BEES Building Early Emotional Skills
BSID The Bayley Scales of Infant Development
CBSPIP Croydon Best Start Parent-Infant Partnership
CCAP College for Child and Adolescent Psychotherapy
CNC Centre for Natural Connections
COS Circle of Security
CPP Child Parent Psychotherapy (Alicia Lieberman’s model)
CUPID Collaborative for Understanding Pedagogy in Infant and Toddler Development
EPDS Edinburgh Postnatal Depression Scale
ESC Engagement Scholarship Consortium
FNP Family Nurse Partnership
FPHC Faculty for the Psychological Health of Children
HCI Hair Combing Interactions
HMB Hearts and Minds on Babies
IDEA Individuals with Disabilities Act
IMH Infant Mental Health
IMHCF Infant Mental Health Competencies Framework
IMH-DTP Infant Mental Health Dual Title Program
IMH-E Infant Mental Health Endorsement
IPP Infant Parent Program
LBS Blue Cross Lade Treatment Centre
Mi-AIMH Michigan Association of Infant Mental Health
MM Marte Meo
v
MPSI Merrill Palmer Skillman Institute
MSU Michigan State University
NBO Brazelton’s Newborn Observation
NHS National Health Service
PIC Parent Infant Centre
PIP Parent-Infant Psychotherapy
PIP UK Parent Infant Partnerships UK
PIP UK Parent-Infant Partnership UK
PRIDE Pre-Service Foster and Adoptive Parent Training
RBUP Regional Centre for Children and Young People's Mental Health (RBUP East and
South)
SETs Standards of Education and Training in Psychotherapy
SIMH School of Infant Mental Health
UKCP United Kingdom Council for Psychotherapy
USA United Sates of America
USFC University of San Francisco, California
VIG Video Interaction Guidance
WAIMH World Association for Infant Mental Health
WCMT Winston Churchill Memorial Trust
WLAC West London Action for Children
WSU Wayne State University
1
Acknowledgements
What a privilege it has been to have borne the name of Winston Churchill on my Fellowship travels;
and what a journey it has been. My heartfelt thanks to the WCMT and the Dulverton Trust for their
sponsorship.
I did not travel alone. My husband, Reverend Kofi-
William Osafo, who is also a Systemic Family
Practitioner, travelled with me every step of the
journey and made the adventure even more special
by sharing it with me; debriefing after every meeting,
taking care of practical details so I could focus on my
goals and enriching conversations with his pastoral
and systemic perspective. A big THANK YOU to you
darling.
At every stop on my journey; from Prague, Sweden,
Norway, Michigan and California; I have received a
warm welcome and hospitality from my hosts. Your
names are listed in my itinerary at the end of this
document. I take this opportunity to emphasize just
how much I have appreciated meeting each one.
Thanks also to my clinical supervisor at PIP UK, Robin
Balbernie, who encouraged me to apply for the Fellowship, and connected me with Deborah
Weatherston, who patiently and sensitively guided me with kind and encouraging words and
responded to my numerous emails in the midst of her very busy schedule.
Thank you Deborah for connecting me with the team from the Merrill Palmer Skillman Institute;
Anne, Carla, Rebecca and Carolyn, who accompanied and advised me from the early stages of
planning my travels, and continue to offer support by publishing reports of my visit. Your help and
hospitality is much appreciated.
I look forward to continuing this journey with you in the coming years as I put my findings into
practice.

2
Executive summary
My WCMT Fellowship took me to Prague, Sweden, Norway and the USA to observe best practice in
parent-infant psychotherapy (PIP), and to learn from giants in this field, in order to contribute to the
practice of parent-infant psychotherapy in the UK and the training of parent-infant psychotherapists.
I explored:
The historical development of PIP within the context of the nation
The different methods of delivery of PIP, the tools and measures used
The training and ongoing professional development of the PIP workforce
The way PIP teams are cared for and supported to manage the trauma of the work
To achieve my goals, I met with pioneers, policy makers, clinicians, academics and service users of
projects that are working with the parent-infant relationship (0-2 years).
I established meaningful links across the continents and shared good practice with my hosts during
and after my travels.
My main findings were:
That there are clear links between the historical development of PIP within each
country’s context and the current mental health of the nation.
Each country or State brings something unique with regard to their methods of
delivery of PIP (groups, residential care, etc.) and what works in one country does not
necessarily work in another. It is therefore necessary to research what is best suited
to one’s particular context.
The training and ongoing professional development of the PIP workforce is also
context specific. A well-funded, integrated national strategy for PIP has a much better
impact on the mental well-being of the nation than a fragmented approach.
The tools and measures used to help clinicians to ‘see the baby’ and to measure
outcomes, can either enhance the work or feel cumbersome and intrusive.
PIP teams that feel nurtured and well cared for enjoy longevity; are more productive
and are better able to manage the trauma of the work.
Based on my findings I feel that the model of PIP practiced in the UK; grounded in psychodynamic
practice and developmental science; is a good model, and this is also the view of the professionals
that I met. However, I feel that an increased focus on group and residential interventions could result
in better outcomes. A competency framework and a national strategy would also improve IMH
outcomes, as well as the establishing of a ‘centre that holds’ together the strategy for IMH in the UK.
I have set out my recommendations for an ideal practice at the end of this report.

3
My Background
My interest in parent-infant psychotherapy was nurtured at the School of Infant Mental
Health & Parent Infant Centre in Hampstead where I trained as a psychoanalytic parent
infant psychotherapist under the mentorship of Dr Stella Acquarone. There, I participated
in numerous intensive family treatments, which honed my skills as a clinician.
The WCMT Fellowship opportunity came at a turning point in my career. I had
recently been appointed Clinical Lead of the Croydon Best Start Parent-Infant
Partnership (CBSPIP) and was determined that the service would be an example
of good practice. CBSPIP is a collaboration of the local council, Croydon Drop-In
(CDI), a voluntary sector counselling organization and Parent Infant Partnership
UK (PIPUK), which is a national, umbrella organization to a network of Parent-
Infant Partnerships (PIPs) that provide specialist psychotherapeutic services to babies and their
relationships (primary caregiver - mother, father, grandparent, foster carer, adoptive parent).
I felt confident about the clinical approach used at CBSPIP; having worked with many extreme cases
at the Parent Infant Centre using that model. Nevertheless, I wanted to be sure that I was up to date
in my knowledge to ensure that the clinical work was being built on the best possible foundations.
I had also been a member of the team at West London Action for Children (WLAC) for several years,
taking a lead in early intervention in the first two years of life. WLAC is an independent charity in West
London, that has supported families in the boroughs of Kensington and Chelsea, Hammersmith and
Fulham, for the past 100 years. The charity offers a range of counselling and
therapy services for children in need, and their families; supporting families under
emotional and financial stress to develop their confidence and skills to cope with
the ordinary and extraordinary challenges of family life. I had never before felt so
fulfilled and cared for by an organization. I was able to transfer the good practice
experienced at WLAC to CBSPIP.
At the time when I heard of the Fellowship opportunity I was two years into a doctorate research in
psychoanalytic parent-infant psychotherapy, and the design of my research provided a good model
on which to base the clinical practice within the CBSPIP team.
The opportunity to travel the world to observe best practice came at time when I was already
stretched in many directions. But as this would be the only opportunity to receive funding under the
WCMT category of Early Intervention and Prevention, I took the risk to apply, and I have no regrets.
This has been a life-changing adventure that has informed my practice and my research. The
interpretation of my findings is best explained in my recommendations for the UK, summarised at the
end of this report; which is a culmination of lessons learned from my life’s work and my Fellowship
travels.
I have big dreams for the future and a determination to make a significant contribution to the work of
psychoanalytic parent-infant psychotherapy in the UK and further afield.

4
Introduction to the project
Context
My project falls under the category of Early Intervention and
Prevention, which is aimed at professionals who are involved
in policy and delivering programmes that give children aged
zero to three years the social and emotional bedrock they
need to reach their full potential?
As a parent-infant psychotherapist, the focus of my work is
on parents-to-be and parents of babies up to 24 months (the
first 1001 critical days), helping them to build stronger bonds
and positive relationships with their babies. Caregivers are able to talk through their worries about
their baby, think together about how past experiences might be affecting the parent-infant
relationship, receive information on child development and helped to see their child’s point of view.
The intervention is grounded in psychodynamic theory and developmental science and involves a
collaboration with key community services, such as health visiting, midwifery, perinatal services,
children’s centers, early years and the voluntary sector.
What is Parent-Infant Psychotherapy?
Parent-infant psychotherapy (PIP) is a dyadic intervention that works with parent and
infant together, with the aim of improving the parent-infant relationship and promoting
infant attachment and optimal infant development. It aims to achieve this by targeting
the mother’s view of her infant, which may be affected by her own experiences, and
linking them to her current relationship to her child, in order to improve the parent-infant
relationship directly.
Cochrane Review, 2015; Abstract
The practice of parent-infant psychotherapy is growing
rapidly across the UK and politicians from across the
political spectrum have come together to promote early
intervention in the first two years of life through the
1001 Critical Days all party manifesto (Leadsom, 2013).
The national organization, PIP UK, is instrumental in the
delivery of the government agenda. They achieve this
by setting up parent infant partnerships across the UK
with the aim of making psychotherapeutic support
available to all families who are struggling to form a secure relationship with their baby.
The evidence accrued over recent years supports the view that early
intervention with parent and infant in the first two years has a lifetime
impact on the quality of their relationship and well-being. However,
there is a need for accredited and competent clinicians to do the work
of early intervention.

5
Aims, objectives and purpose of the project
What difference do I hope to make as a result of the learning from my travels?
Well, I'm a bit of a dreamer and I have some big dreams about the practice of parent-infant
psychotherapy in the UK. My travels have taken me to like-minded dreamers, many of whom have
been on this road for thirty to forty years and have left a legacy in their nations. According to Isaac
Newton:
"If I have seen a little further it is by standing on the shoulders of Giants" (Newton to Hooke, 5 Feb.
1676; Corres I, 416).
Newton probably learned this truth from theologian John of Salisbury who said in the 12th century:
"We are like dwarfs sitting on the shoulders of
giants. We see more, and things that are more
distant, than they did, not because our sight is
superior or because we are taller than they,
but because they raise us up, and by their
great stature add to ours."
The Metalogicon of John of Salisbury:
A Twelfth-Century Defence of the Verbal and
Logical Arts of the Trivium
My aim in undertaking these travels was to become equipped to push new boundaries in my work
with parents and infants in the UK. I hoped to learn from the experiences of pioneers and giants in
their field, in order to contribute to the training of parent-infant psychotherapists and to grow the
workforce of accredited professionals, who will be equipped with well-researched tools for their work
with vulnerable families. In particular, I wished to learn about the historical development of PIP within
the country’s context; how they are training their workforce; the tools they use to achieve their goals;
and how they support their teams. I planned to achieve this by meeting with pioneers, workers and
clients of projects that are working with parents and infants (0-2 years).
I chose to visit Scandinavia and America because they have made a vast contribution to the
development of parent-infant psychotherapy, producing prolific writings and leading the world with
good practice. My long-term objective is to apply the learning from these continents to the
development of my clinical practice in the UK; in order to improve the experience of my clients as well
as the clinicians in my team. It is normal for parent-infant psychotherapists to hold highly complex
caseloads. I therefore wished to observe how clinicians are held and supported in their practice in
order to transfer the experience of being held and supported to the families in their care.
Finally, I wished to build links across the continents in order to continue sharing good practice after
my travels. I spent three weeks in Scandinavia and four weeks in the USA, meeting the professionals
that I had read about for many years.
6
Approach
In preparation for my travels I consulted widely among leading Infant Mental Health (IMH)
professionals in the UK network for their recommendations about experts in my chosen destinations.
I contacted Bjorn Salomonsson from Sweden via his website, introducing myself and the Fellowship
opportunity. His writings had been a major influence in my practice and he is well quoted amongst
UK parent-infant psychotherapists. I was encouraged by Bjorn’s positive reply and willingness to host
me and this spurred me on to contact other professionals in Scandinavia.
Also helpful was Robin Balbernie, a 1998 Winston Churchill Memorial Trust (WCMT) Fellow, who
connected me with Deborah Weatherston, from the Michigan Association for Infant Mental Health
(Mi AIMH) in the USA. Deborah had been supportive to Robin during his
Fellowship, and she kindly introduced me to significant members of the Mi
AIMH network who are based at the three main universities in Michigan.
This enthusiastic team arranged a Skype meeting with me to help me plan
my itinerary. Present online were Ann Michele Stacks, Carolyn Dayton, Carla
Baron and Rebecca Wheeler from Wayne State University, who prepared a
rich itinerary for me in the USA. Our SKYPE meeting was very productive
and I was able to map out my USA journey by the end of it.
The USA team suggested that I attend the World Association of Infant Mental Health (WAIMH)
conference in Prague, where I would be able to meet IMH professionals from around the world, in
order to flesh out my plans further.
An Overview of my Fellowship Travels
My Fellowship was undertaken in three phases, arranged around my UK work commitments; starting
with the five-day WAIMH conference in Prague, Czech Republic, from 29th May to 2nd June, 2016.
The trip to the Prague conference enabled me to hear and meet potential hosts before making a final
decision whether to visit their projects. The conference was rich and very inspiring; but also inspiring
was the beautiful Old Town of Prague (below). I had only a few hours to explore but I vowed to return
one day to see more.

7
I left the WAIMH conference with a list of professionals to contact. As I followed them up via email, I
was pleasantly surprised that most were already familiar with the WCMT Fellowship opportunity and
felt honoured to assist me.
Phase two of my travels to Scandinavia took place six months after the Prague conference. The
Scandinavian countries are known for excellent outcomes with regard to child care and infant mental
health.
Sweden
My Scandinavian adventure started in Stockholm, where I met with Pia Risholm Mothander, who is
respected Internationally and nationally in the Nordic countries; having played a significant role in the
formation and activity of the Nordic Association for Infant Mental Health. Pia gave me an overview
of the national strategy with regard to IMH and her dreams for future developments.
My next contacts in Sweden, Anna Malmquist and Camilla Wachtmeister, worked within the Infant-
Child-Parent unit at the Child and Adolescent Psychiatry department in Stockholm. Anna shared some
inspiring stories about her group work with parents and infants and particularly her studies
about Infant to Infant interactions over the past 30 years.
My final stop in Sweden was with Dr Bjorn Solomonsson; a psychoanalyst, perinatal consultant,
researcher, prolific writer and grandfather. Bjorn explained how the Swedish health system, which
is one of the world’s best systems, is organized; how it has changed over the years and the impact of
change on the role and training of parent-infant professionals.
Norway
After Sweden I moved on to Trondheim in Norway to meet with Anne Margrete Rostad and Hege
Welde, who shared research and strategies for early IMH interventions across Trondheim; taking me
to visit projects in the community to see how 35 years of research works in practice.

8
From Trondheim, I flew to Oslo in the South, and then on to Tonsberg, where Berit Lande, head of the
child psychiatric unit in Tonsberg, leads a team that is dedicated to working with infants/children up
to the age of three years old (including during pregnancy). This team demonstrated the impact of the
national training strategy for IMH across Norway.
Marit Bergum Hansen, was my host for the last two days in Norway. She is a special advisor at
the Centre for Child and Adolescent Mental Health (RBUP) East and South Norway. Established in
1998 by the Ministry of Health, RBUP runs educational programmes for professionals, conducts
research, arranges international conferences and houses the National Network for Infant Mental
Health. Marit explained RBUP's work with 0 - 5s across 380 municipalities; training midwives, doctors,
psychologists, etc. in the 12 most important hospitals in Norway.
Marit introduced me to Gro Vatne Brean, a member of the RBUP network who specialises in working
with parents through pregnancy and childbirth as well as with infants and young children. Gro
provides training around pregnancy issues, neurobiology, developmental psychology and attachment
and the implementation of DC 0-3 diagnostic system.
The University of Oslo was my next stop in Norway, where I met with Unni Tanum Johns and Vibeke
Moe, who are members of the teaching faculty in the psychology department. Vibeke is a
researcher and clinician with a particular interest in developmental psychology and psychopathology,
as well as the earliest interaction and development in the first years of life.
On my last day in Oslo I met with Mette Sund Sjøvold who works at the Aline Polyclinic with 0-5 year
olds and their caregivers, supporting them to care for their child rather than to remove the child.
My final appointment in Norway was is with Tove Walstrom, General Secretary of the Norwegian
Foster Care Association, which works to improve quality at all levels within foster care. It is a national
and independent organization in relation to political parties and religious communities.
Michigan - USA
The third phase of my travels was to the USA; six months after my visit to Scandinavia. I started in
Michigan, the birthplace of parent infant psychotherapy; which presents a contrasting picture to that
of Scandinavia, where the structure of the health care system is highly integrated and well-
funded. The USA depends on individual projects and funding is not easy to find. Research based
evidence is key in order to convince funders, so not all projects are able to survive the competition.
9
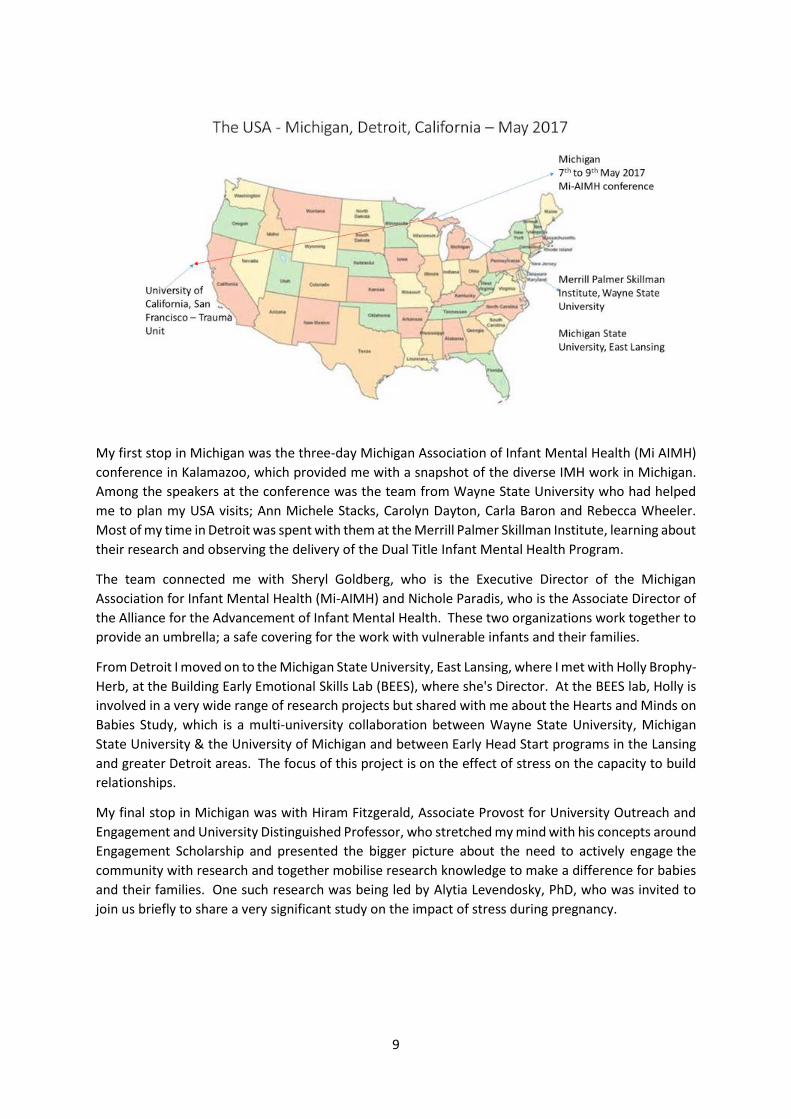
My first stop in Michigan was the three-day Michigan Association of Infant Mental Health (Mi AIMH)
conference in Kalamazoo, which provided me with a snapshot of the diverse IMH work in Michigan.
Among the speakers at the conference was the team from Wayne State University who had helped
me to plan my USA visits; Ann Michele Stacks, Carolyn Dayton, Carla Baron and Rebecca Wheeler.
Most of my time in Detroit was spent with them at the Merrill Palmer Skillman Institute, learning about
their research and observing the delivery of the Dual Title Infant Mental Health Program.
The team connected me with Sheryl Goldberg, who is the Executive Director of the Michigan
Association for Infant Mental Health (Mi-AIMH) and Nichole Paradis, who is the Associate Director of
the Alliance for the Advancement of Infant Mental Health. These two organizations work together to
provide an umbrella; a safe covering for the work with vulnerable infants and their families.
From Detroit I moved on to the Michigan State University, East Lansing, where I met with Holly Brophy-
Herb, at the Building Early Emotional Skills Lab (BEES), where she's Director. At the BEES lab, Holly is
involved in a very wide range of research projects but shared with me about the Hearts and Minds on
Babies Study, which is a multi-university collaboration between Wayne State University, Michigan
State University & the University of Michigan and between Early Head Start programs in the Lansing
and greater Detroit areas. The focus of this project is on the effect of stress on the capacity to build
relationships.
My final stop in Michigan was with Hiram Fitzgerald, Associate Provost for University Outreach and
Engagement and University Distinguished Professor, who stretched my mind with his concepts around
Engagement Scholarship and presented the bigger picture about the need to actively engage the
community with research and together mobilise research knowledge to make a difference for babies
and their families. One such research was being led by Alytia Levendosky, PhD, who was invited to
join us briefly to share a very significant study on the impact of stress during pregnancy.

10
California
From Michigan, I followed the path of Selma Fraiburg, the pioneer of parent-infant psychotherapy to
California, where I spent two weeks, visiting the Infant-Parent Program (IPP) that is based at the
University of California San Francisco’s trauma hospital. Here I learned about the training and
supervision of parent-infant psychotherapists and how they are equipped and supported to manage
very traumatic cases.
My hosts in California were, Kadija Johnston and Maria St John, who are based at the Zuckerberg San
Francisco General Hospital and Trauma Centre, which is unique in San Francisco as it serves the poor,
elderly people, uninsured working families, and immigrants. Most patients receive Medicare. The
homeless, are also welcome at the hospital, which is the only acute hospital in San Francisco that
provides twenty-four-hour psychiatric emergency services.
Maria St John, Associate Clinical Professor and Director of Training at the IPP and Kadija Johnson,
Director of U.C.S.F. Infant-Parent Program/Day-care Consultants, allowed me to experience the
normal life of the IPP, without any frills added; welcoming me behind the scenes as they discussed in-
house business and inviting me to participate in the supervision of extremely traumatic cases.
It was useful to understand the significance of Day-care at the IPP. Maria and Kadija arranged for me
to meet with Kristin Reinsberg, Director of Day-care Consultants, who explained how the program
aims to help the adults caring for the children to understand and respond to challenging behaviours
appropriately, despite being overworked, underpaid and stressed. Many children spend more than
40 hours a week in day care, therefore the day-care staff spend more time with them than their own
parents.
The work with homeless families is also a significant part of life in California, where homelessness is a
chronic issue. Andrea Scott, an Early Childhood Mental Health Consultant at the Infant Parent
Programme, provides support to a variety of community based organisations. Andrea took me to see
some of the projects that work with homeless families; the Hamilton Project for homeless families,
and Compass Children's Centre. Hamilton houses over 50 families each night and provides support
for up to 25 families at high risk for chronic homelessness for 6 to 18 months. Sometimes we forget
that infants and toddlers are among the homeless population.
After two weeks in California, I ended my travels with a final meeting with Maria St John, where she
presented me with a treasure from the archives of the university; one of the original copies of the
famous article, 'Ghosts in the Nursery' by Selma Fraiberg. Having been inspired by Selma and after
having followed her footsteps from Michigan to California, this was an apt way to end my travels.
Lessons from Sweden
Historical Development in Sweden
As one of the world’s best systems, Sweden provides excellent care for infants and children, especially
in the first six years of life. In Stockholm 96% of women attend the perinatal clinics. Up until 10 years
ago each clinic had its own psychologist; so it was possible to intervene early where there were
psychological issues affecting the parent-infant relationship. However, things have now changed due
to the institution of big child psychiatry units, which have an increased focus on disorders such as
ADHD and autism, and a decreasing focus on infant mental health and early intervention. The

11
interactive perspective of the work with families has also diminished in preference for medication,
and this is a concern for all the professionals I met in Sweden. Many of these excellent and highly
skilled clinicians enjoy thriving clinics and research, which they describe as enjoyable and
satisfying. However, with the change in focus over the past 10 years and the withdrawal of
psychologists from the child health clinics, there is a concern among professionals that the skills
associated with treating the parent infant relationship will not be easily passed on to the next
generation of therapists.
Sweden is proud of its health care model, which reaches out to everyone, despite their income. The
model goes back to the 1930s when the population was very low during the recession and the
government had to support the homogenous and decreasing population of born swedes to work
outside the home. The model started with a service that supported breast feeding, known as ‘Milk
Drops’, which expanded and developed into well-baby clinics, focusing on the physical care of babies.
Psychologists were introduced into the clinics to provide
consultancy to nurses and paediatricians to enable them
to respond to the psychological problems that arose in
the parent-child relationship. My host Pia Risholm
Mothander headed up one of the first five teams of
psychologists in the 70s in Stockholm. There were 20
psychologists in each team.
Pia longs to see an integrated approach to infant mental health issues in Sweden, such as the RBUP
system in Oslo, but no-one in Sweden is interested in paying for it. There are many excellent ‘solo’
artists, but what is needed is a more collaborative approach, backed by the government.
Pia shared her vision for Sweden with me.
‘My vision and hopes for the future is that we would be more partnership oriented in Sweden.'
'Everyone is saying ‘what shall we do?’ The answer is to start at the beginning and support parents
and it will pay back.'
Pia likens her dream for the infant mental health system in
Sweden to an onion with different layers (representing social
welfare, paediatric care, infant mental health care, primary
care, well-baby clinics and pre-school; all in the same location). You
can peel the different layers of the onion but at the middle of the
onion are the children – 'because the children are the future. All the
leaves around are supporting what’s inside because that’s where it’s
growing.'
She is also aware of the impact of the changing society in Sweden.
"You have to follow the changes of society because the context is so important. You can have your
ideas about what kind of a paradise you would like to create for infant families but you can’t take that
out from the context you are living."
Perinatal Care in Sweden
My Swedish hosts explained to me why Sweden has one of the world’s best systems for taking care of
pregnant women and infants in the first year of life. Expectant mothers attend midwifery clinics,
12
about six times during pregnancy for ultrasound. After birth they are immediately followed up by a
health visitor (HV) who works at the Children’s Health Centre / well-baby clinic. The HV home visits
on day five to see that all is well; then mother goes once weekly to the well-baby clinic in the first
month, bi-weekly in the second month, monthly from 3-6 months and then bi monthly up to one year.
Nurses and HVs are trained to detect postnatal depression and provide excellent care. Paediatricians
see babies at 2 and 6 months of age and refer to consultants if they suspect something really bad.
Perinatal health care is therefore well developed in Sweden.
Despite this excellent start for the mother and baby, clinicians like my hosts, Bjorn and Pia, feel that
perinatal mental health care should be instituted with as low a threshold as possible. Along with the
decreased focus on infant mental health and the increased focus on disorders such as ADHD and
autism there is also an increased tendency to view post-natal depression as a disease that strikes the
mother; whereas the interactive perspective on these problems has diminished. Therefore, if a nurse
writes that a mother is depressed she is automatically sent to the GP to be medicated.
Models of Parent-Infant Psychotherapy
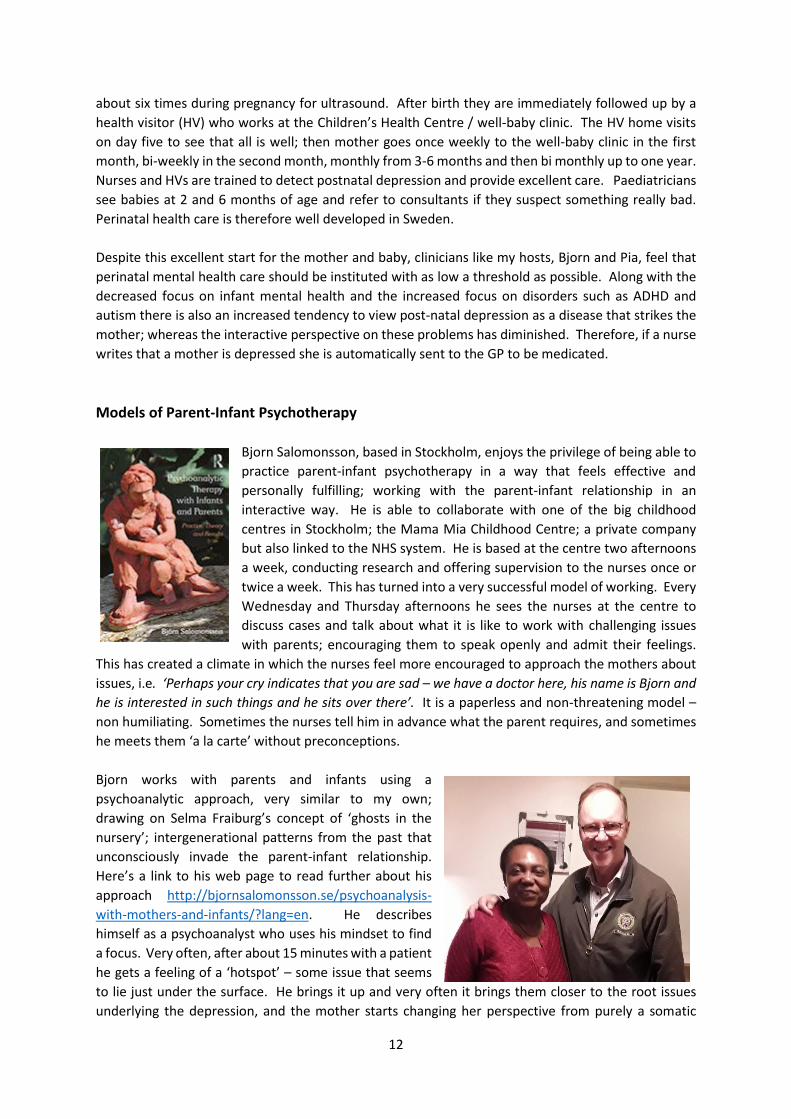
Bjorn Salomonsson, based in Stockholm, enjoys the privilege of being able to
practice parent-infant psychotherapy in a way that feels effective and
personally fulfilling; working with the parent-infant relationship in an
interactive way. He is able to collaborate with one of the big childhood
centres in Stockholm; the Mama Mia Childhood Centre; a private company
but also linked to the NHS system. He is based at the centre two afternoons
a week, conducting research and offering supervision to the nurses once or
twice a week. This has turned into a very successful model of working. Every
Wednesday and Thursday afternoons he sees the nurses at the centre to
discuss cases and talk about what it is like to work with challenging issues
with parents; encouraging them to speak openly and admit their feelings.
This has created a climate in which the nurses feel more encouraged to approach the mothers about
issues, i.e. ‘Perhaps your cry indicates that you are sad – we have a doctor here, his name is Bjorn and
he is interested in such things and he sits over there’. It is a paperless and non-threatening model –
non humiliating. Sometimes the nurses tell him in advance what the parent requires, and sometimes
he meets them ‘a la carte’ without preconceptions.
Bjorn works with parents and infants using a
psychoanalytic approach, very similar to my own;
drawing on Selma Fraiburg’s concept of ‘ghosts in the
nursery’; intergenerational patterns from the past that
unconsciously invade the parent-infant relationship.
Here’s a link to his web page to read further about his
approach http://bjornsalomonsson.se/psychoanalysis-
with-mothers-and-infants/?lang=en. He describes
himself as a psychoanalyst who uses his mindset to find
a focus. Very often, after about 15 minutes with a patient
he gets a feeling of a ‘hotspot’ – some issue that seems
to lie just under the surface. He brings it up and very often it brings them closer to the root issues
underlying the depression, and the mother starts changing her perspective from purely a somatic

13
psychiatric point of view, from ‘am I depressed?’ to seeing the links between her past experiences of
having been parented and her present relationship with her child. Bjorn tends to appreciate having
the baby present in the session sometimes, but not religiously so. Some mothers want to come alone
for the first time – ‘this is my hour’ – because they feel so ostracized. Sometimes they come with their
partners. Treatments range from one session to twenty.
To develop his approach further Bjorn received research funding from the Swedish Inheritance Fund
and allocated 10 psychoanalysts to various well-baby centres in Stockholm for three years. His long
term aim is to help the politicians understand that this is a smart system and it should be part of the
perinatal health care, which is so well developed.
Using Groups to help Babies - Infant to Infant
Learning from Sweden
Analytic group therapist, Anna Malmquist
Saracino, has been working within the Infant-Child-
Parent unit at the Child and Adolescent Psychiatry
department in Stockholm with infants since 1988.
The Unit is called Maskan, meaning ‘stitch’,
symbolizing ‘one stitch in the network, one knot in
the matrix around the baby and its family’. It also
symbolizes a dropped stitch, which must be picked
up.
Maskan used to be an independent unit before the
reorganization of the Child Guidance Clinic in Stockholm. It managed to survive by being integrated
into the Infant and Preschool Child Team, which treats children up to 17 years. The group uses
psychodynamic and psychoeducative methods to treat severe disturbances in the relationship
between infants and their parents and to promote normal development and attachment. There are
usually 13 members in a group – five babies under one year, five mothers and three therapists. They
attend twice a week for three hours from between three and ten months of age (average 5-6 months).
Anna and her colleague Camilla Wachtmeister received me at their spacious Stockholm headquarters.
After touring the lower floors, dedicated to children and adolescents and meeting the staff, we toured
the top floor, which is dedicated to parents and infants; with rooms for supervision, video interaction,
group work, a dining area where parents, infants and staff work through eating difficulties and
promote healthy habits, and much more.
There is a comfortable, homely yet professional feel to the facility, depicting quality through and
through. The space is carefully structured for parents and
infants, with a careful selection of toys. The delivery of the
programme demands hard work and a weekly
commitment to the families for many years. The window
of intervention is clear; mothers and babies up to one year
and two months. Anna shared some inspiring stories
about her group work with parents and infants and
particularly her studies about Infant to Infant interactions.
She spoke of how the child "starts to develop together as
they play together" and how "symptoms start to go away

14
when they come with their mothers continually to the group". Though she admits that the groups are
not enough and there must also be work with the individual parent infant dyad, the group provides
something immediately for the infant as he waits for his mother to change.
I love Anna's description of the group; she says, "the group matrix is also a vitalization bath".
Apart from the work within the parents and infants "there's a lot of work going on between, among
and within the therapists and there must be time to talk and process..."
Training
Over 30 years of knowledge and experience inform the work at Maskan but sadly there was no specific
training programme to pass on the skills. The ingredients of the treatment are similar to that used by
my teams in London; a combination of psychodynamic and psychoeducative methods, individual
psychotherapy for the mothers and video feedback. Activities such as singing, playing and eating
together are also included in the structure of the programme. Fathers take part in the treatment on
a continuous basis and the parents’ feedback helps to shape the provision. There is also a multi-
disciplinary collaboration between doctors, adult psychiatry, social services and children’s hospital.
The clinicians bring to the group work a solid knowledge of child development and the psychological
development of a parent; as depicted in Stern’s concept of the ‘motherhood constellation’; i.e. the
birth of three generations; baby, mother and maternal grandmother. An understanding of the
concepts of intergenerational transmission of ‘ghosts in the nursery’ (Fraiberg, et al., 1975) and the
parental internal representations are also important for the work. As in London, observational skills
are an important tool used by the therapeutic team. Psychodynamic concepts such as transference
and containment are embodied by the therapists and is a crucial part of the transformative process
within the group; the therapist becomes the tool in a different way than in other modalities
But working in this way demands specialist skills. Clinicians such as Bjorn and Anna have learned from
experience how to gauge how deep and how quickly and how far to go in addressing traumatic issues.
But how can such skills be passed on when there is no integrated and recognised training to preserve
them. The transfer of the specialist skills required to address such issues require specialist training
over several years, in order to develop competence and confidence in the clinician. But clinicians in
Sweden are immersed in their work and have difficulty finding time to convince politicians and child
psychiatry of the importance of early intervention, or to set up and run trainings without the financial
backing of the state. In a climate where everyone is preoccupied with the pressing issues such as bad
behaviour at school and suicidal adolescents, the voice of the baby is not heard.
The big concern for experts such as Bjorn, Pia and Anna in Sweden is that there are individuals who
have a lot of skill and knowledge, but how is it being passed on to the next generation. There is no
obvious channel. To start a training would mean letting go of the crucial clinical work, which is
important, enjoyable and satisfying. Bjorn is funded by the Karolina Institute to deliver a training to
nurses called ‘meeting and helping young parents with their babies – an introductory course in
perinatal psychiatry’. However, this is not enough. Skills are also passed on through supervision of
nurses and supervision of researchers, but even though the nurses and researchers are good at the
work they do with mothers and babies there is still a need to campaign for more training in order to
develop the competency of clinicians to address complex issues such as infanticide ideations, etc.

15
Conclusion from Sweden
Sweden’s excellence with regard to childcare from the cradle onwards has had a positive impact on
the mental health of the nation and the general sense of well-being. This has not been the case for
the new and diverse population, many of whom have been exposed to severe trauma in their countries
of origin. Already, it is possible to see how this impacts the national picture with regard to the parent-
infant relationship in that the voice of the baby is not heard amid the more urgent cries of children,
adolescents and parents impacted by trauma, and one wonders whether there is the capacity to meet
the new and complex needs; especially among the new migrants who did not have the same privilege
as their Swedish hosts from the start of life? The physical health of the nation is well looked after and
this is a protective factor, however, the gap in the psychological provision is growing. When
‘depressed’ mothers go to Bjorn, frozen and helpless, and with the baby-self presenting, he is able to
work with the baby in the mother in a non-threatening way. Anna Malmquist also uses a similar
psychodynamic approach in her group work.
However, there is a very big responsibility on the shoulders of very few skilled professionals, to
transfer their skills through training. The concern is that there is not a specific training for parent
infant psychotherapists in Sweden and the current specialists are either retired or too busy. The
government has not yet woken up to the urgent need to bridge the gap between physical and mental
well-being in a changing and diverse population.
Despite this dilemma, Sweden still boasts an excellent child care system, which gives every child the
best physical care at the start of life.
Dr Bjorn Solomonsson reassured me that our system in Croydon Best Start Parent Infant Partnership
is a good model that is effective around the world. Bjorn also feels challenged to address the need to
train the next generation of therapists in Sweden.
By seeing what is excellent in the Swedish provision, along with the gaps, I have gained a clearer
understanding of what is good in my practice of parent-infant psychotherapy in the UK and what is
needed. Hopefully, my hosts have also been inspired to bridge the gap by establishing a good national
training to preserve and to pass on their knowledge and expertise to the next generation.
Lessons from Norway
In Norway I observed two effective regional strategies that protect the parent-infant relationship.
The first is based in Trondheim, in the middle of Norway, where the early intervention research of
Anne Margrethe Rostad serve as an organizing principle for parent-infant interventions across 18
municipalities of Trondheim.
Development of Parent-Infant Services in Trondheim
From 1986 Anne Margrethe Rostad has conducted research into Early Intervention Social Spectre
Developmental Problems (Rostad, 2008), in which she tracked 97.6% (1,217) of children born in one
16
year from 1st August 1990 to 31st July 1991 across 18 municipalities of Trondheim to explore if it is
possible to detect early signs of developmental disorders during the first year of life. Data was
collected by professionals across Trondheim on five occasions; in the birth clinics, in the first level of
health care and from parents; from pregnancy to seven months.
Anne Margrethe’s research is based on the knowledge that infants
with problems in regulation of sensorimotor function may later
develop emotional difficulties. However, the common approach
of professionals is to wait for the problems to appear rather than
to take a proactive approach. From a neurobiological perspective,
the success of early intervention strategies is due to the plasticity
of the brain in the first two years of life. Therefore, by screening
the children over a seven-month period, Anne hoped that the very
early signs of dysregulation would be detected, leading to more
hopeful interventions and outcomes.
At the age of four, data was obtained for 1,108 of the children (91%) who had been screened. Of this
number, the data for 919 children was analysed. The results showed that over 50% of participants
were predicted accurately at seven months. The screening process used in the research with parents
and professionals, generated knowledge about what the sensitive and specific risk factors are in early
infancy that are precursors of later developmental problems. Such early prediction of developmental
problems can positively influence clinical work in that it allows for preventative work to be done.
Anne Margrethe involved the professional workforce in her research, enabling them to develop an
awareness of how to identify disorders as early as possible. The findings from her research led her to
work tirelessly over 35 years, devising and implementing a cohesive strategy across Trondheim. The
findings of Anne Margrethe's research also inform work with foster children.
Models of Parent-Infant Psychotherapy Observed in Trondheim
Anne Margrethe’s early intervention model, requires careful ongoing early screening and prediction
of potential developmental issues. This has proved to be effective across Trondheim and is backed by
the authorities; serving as a safety net to catch and intervene in potential developmental issues.
Specialist Group Work for the Treatment of Complex Issues in the Parent-Infant Relationship
Apart from this strategy I observed the
impact of specialist group work in the
treatment of complex issues in the parent-
infant relationship, which build on Anne
Margrethe’s model of early intervention.
One such group in Lade, for mothers with
complex issues, requires mothers to attend
twice weekly with their babies from 10.00am
to 2.00pm. The group members became like
a family while attending the group and often
remain connected in friendship groups after the intervention. Greta, the group leader (right), has

17
been in post for over 26 years, giving a sense of permanence and security to the project. Past group
members feel that they have a secure base at the centre to which they can return.
Each group consists of 8 babies and their Mothers, who come with a wide range of symptoms such as
depression or the inability to feel for or connect with their child. Using video interaction Greta works
frame by frame to demonstrate positive aspects of the parent-infant relationship. As mothers see
moments of positive interaction their feelings for their baby become activated. In some cases, only a
few seconds of video can be used because positive moments are so few, but this increases over time.
The result of this work is that the mothers become healthier and more secure in their role and are
empowered to take care of their child. The knock on effect for the economic system of Trondheim is
a big financial saving, because the alternative would be foster care. The group allows the mothers to
discover and develop and stabilize their own internal resources to care for their child.
Apart from the group, Greta follows up the high risk mothers in their own homes. She is careful to
work alongside the mothers to empower them, without taking over or even to hold the baby, should
in case the baby responds to her in a better way. The mothers feel held and cared for by Greta in the
group and they are able to transfer this care to their babies. One mother in the group told me that
when she comes to the group she feels seen and her baby is also seen. She is also able to express her
gifts in creative ways. Mothers are referred to the group by the midwives, who have been trained to
pick up early signs of alarm.
Residential Mother and Baby Unit for Substance Abusers Before and After Birth
Some high risk families cannot be treated in the community but need residential care to ensure their
safety and the safety of their baby. Hege Weld, my co-host in Trondheim and psychologist, Lise, work
at Blue Cross Lade Treatment Center (LBS), which offers an interdisciplinary specialized treatment for
people with all types of substance related problems.
Lise and Hege work with a team of support
workers and psychologists to care for
six mothers and their babies that are based in
the apartments at the centre. During our
visit one mother who has been free of drugs for
several months, was eager to tell me about
how she has made a new start to her life, with
her partner and baby. She is full of hope for the
future and is feeling confident about how to be
a good enough mother for her baby.
The centre uses mother-baby therapy, mentalization based therapy learned at the Anna Freud Centre
(AFC) in London, couple and individual therapy and Mileau therapy. Within the centre, the Mileau
therapist is almost like a parent working alongside their child and teaching them to deal with daily life.
They shop, cook, clean and play with the families and link their work with the work of the
psychologists; directing the families to take issues to therapy.
The centre gives families a new start in life by allowing them to move away from their old location and
negative influences. They have over a year to internalise more helpful ways of being with their child.
The quality and length of stay is key and allows time for the internal shifts to take place in the parents.
18
According to psychologists Hege and Lise, ‘what you have here are other parents that they can
internalize… they can connect and have an alternative way of being and doing… ‘
It’s not over when they leave the centre. They have at least two years when they can continue to visit
the centre to receive therapy and to show their child’s progress as s/he grows. As well as being a
secure base from which to launch, the centre is a beautiful place to come back to that is part of the
family history. As they grow, children are proud to return and say, ‘this is where I was born’, because
of the beautiful setting.
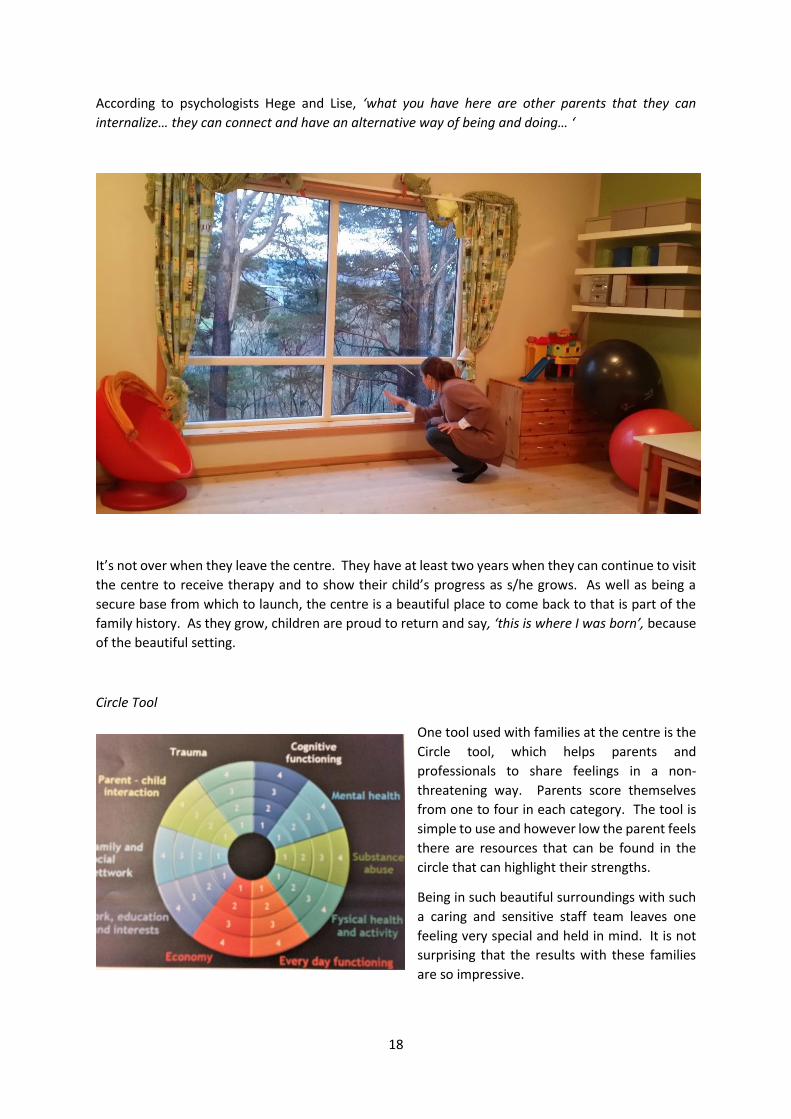
Circle Tool
One tool used with families at the centre is the
Circle tool, which helps parents and
professionals to share feelings in a non-
threatening way. Parents score themselves
from one to four in each category. The tool is
simple to use and however low the parent feels
there are resources that can be found in the
circle that can highlight their strengths.
Being in such beautiful surroundings with such
a caring and sensitive staff team leaves one
feeling very special and held in mind. It is not
surprising that the results with these families
are so impressive.
19
Development of Parent-Infant Services in Oslo
The second strategy observed in Norway is the national mental health network; the Regional Centre
for Children and Young People's Mental Health (RBUP East and South), which works to strengthen
children's and young people's mental health through
developing good services.
Established in 1998 by the Ministry of Health, RBUP
runs educational programmes for professionals,
conducts research, arranges international conferences
and houses the National Network for Infant Mental
Health.
In my travels around Sweden and Norway, most
professionals and organizations made reference to the
significance of the training provided by RBUP, which seemed to me to be a 'Centre that holds' together
the work of child mentaI health, disseminating training and good practice throughout Scandinavia and
further afield. As William Butler Yeats (1865-1939) reminds us... "Things fall apart; (when) the centre
cannot hold" (italics mine).
RBUP works with 0 - 5s across 380 municipalities in Norway; training
midwives, doctors, psychologists, etc. They aim to cover the 12 most
important hospitals in Norway with research based training, using
carefully selected programmes. However, they are not satisfied to just
adopt universal programmes; they research each programme to ensure
that they reflect the Norwegian way of life.
My host at RBUP was Marit Bergum Hansen, a special adviser in the RBUP
network who is particularly concerned with the development of children
and their mental health in the first years of life.
Trainings and Tools
The main focus of all trainings is to help professionals and parents to 'see the baby'; therefore, all the
programmes selected to be used in hospitals has this focus in mind; such as Brazelton’s Newborn
Observation (NBO) intervention programme to support parents to see the child and read the signs
from the baby. This training is delivered especially in the 12 most important hospitals in Norway. All
interventions are researched and adapted to suit the Norwegian way of life, including Circle of Security
(Virginia model), Marte Meo, a video interaction tool similar to VIG and Child Parent Psychotherapy
(Alicia Lieberman's model for working with violence and trauma). After buying into the training RBUP
quickly develops Norwegian therapists, supervisors and trainers, constantly asking the question, ‘does
this fit our culture – our way of doing things’? Also being added to the RBUP tools is the Australian
programme ‘Tuning Into Kids’, which focuses on emotional regulation, which is central to good mental
health. The programme teaches how to tune in at the child’s emotional level, similar to the work of
child psychotherapy but packaged as a tool.
Other tools include the Edinburgh Postnatal Depression Scale (EPDS), Pre-Service Foster and Adoptive
Parent Training (PRIDE) for potential foster carers, and the Family Nurse Partnership (FNP), to be used
with vulnerable dyads. The RBUP team observed FNP in England and is now piloting it for use in

20
Norway. Marit is committed to ensuring that there are enough therapists with sufficient knowledge
to do the work with infants and families.
RBUP is working on other models of interventions with autistic children, pre-school children, foster
children and adopting families.
I observed the impact of the RBUP training in operation in Tonsberg, at the
BUPA poliklinikk spesial, based at the hospital Sykehuset, Vestfold where Berit
Lande is head of the child psychiatric unit. The town of Tønsberg is 120
kilometres south of Oslo where RBUP is based.
Berit leads a team that is dedicated to working with infants/children up to the
age of three years old and their parents, and also at risk pregnancies can be
referred. This team consists of three clinical psychologists, one psychiatrist and
one clinical educational therapist.
Attachment theory and transaction models (bio-psycho-social-educational model) are strong
influences in the team's thinking and practice. A carefully selected range of programs, such as Circle
of security, Strange situation and Brazelton's Newborn Behavioural Observation along with Video
Interaction Guidance are much used methods for assessment and treatment.
The team's closest partners, when working with infants, outside the hospital are district nurses,
midwives and child welfare services. They also cooperate with the somatic infant unit in the hospital
and mental health clinics for grown-ups.
My main question to them was, what really works for them in Tonsberg. They felt that the home visits
were very effective because the balance of power rests with the parent, however they were very time
consuming. They also felt that the tools they use enables them to help the parents to focus on the
child and become more curious, or more interested in him. Also, the tools bring structure to the
session and they are adapting them in creative ways to teach parents how to cope with their children's
sleeping difficulties, etc. There seem to be a very strong link with RBUP and also with training schools
in London and the USA. The team's passion to learn and their careful selection and creative use of
their tools came across very clearly.
A Joined-Up Network
The teams across Norway work closely together
due to the RBUP network. I was privileged to
meet some of the specialists and educators
employed by RBUP to deliver training. Gro Vatne
Brean (who incidentally started the IMH team in
Tonsberg), specialises in working with parents
through pregnancy and childbirth as well as with
infants and young children. Apart from RBUP, she
works as a private practitioner, providing training
around pregnancy issues and the implementation
of DC 0-3 diagnostic system. Gro is committed to
making knowledge of neurobiology,
developmental psychology and attachment
available to everyone.

21
Working with Pregnancy Training
Gro is concerned that few therapists have enough knowledge to work with the issues of pregnancy.
She has therefore devised a training, which is delivered to professionals two days every second month
for 18 months. The first training day is focused on theory and the second day provides supervision
and support for the clinician. She started the first group in 2012 and at the time of my visit the third
group was ending. The cohorts consisted of 10, 25 and 15 members.
Sometimes she teaches on the neuroplasticity of the brain together
with her husband who is a neurologist.
I met other members of the RBUP team, who are also based at the
University of Oslo. Unni Tanum Johns and Vibeke Moe, are
members of the teaching faculty in the psychology department.
They believe that RBUP fills the gaps in the training of psychologists,
which can be quite theory heavy. They also provide tools for the
infant teams and filter their training to the grass roots organizations
across Norway and further afield.
Models of Parent-Infant Psychotherapy Observed in Oslo
Infants and Young Children at Risk and their Caregivers.
Mette Sund Sjøvold has worked as a lead psychologist at
the Aline Polyclinic for 18 years with infants and young
children at risk and their caregivers. The centre is part of
the children’s services in Oslo. Local child care officers
refer families with children from 0-2 years if they are
concerned about the safety of the child. Families stay for
two to three months and Mette’s team undertakes
assessments of the child’s development and the parent-
infant relationship.
The centre started in 1907 as a mother and baby unit to help unmarried mothers to learn a trade in
order to make a living to care for themselves and their child. It then changed to an orphanage and in
the 60s changed again to a parent-infant unit.
There is room at the clinic for up to 6 families at a time, who are looked after by three teams of
professionals; each team consisting of one psychologist, two Milieu therapists and a consultant senior
social worker (all working in shifts). Each of the three teams work with two families; sometimes a
mother and child or father and child or both parents and child/children. Of the children coming to the
centre, 50% of families succeed in keeping their children and 50% of children go into foster care for
further help. There's an emphasis on supporting families throughout the process as the wish is to
equip them to care for their child rather than to remove the child. If that does not work the case has
to go to court to decide the long term decisions for the child. The process takes several months and
is full of anxiety for the family.
After the family moves on from the clinic, they return for further assessment to ensure that the help
they received is still working to protect the child. Some children come to the centre from birth;
sometimes born displaying the effects of having a stressed mother during pregnancy or affected by
mother’s drug or alcohol abuse. Should the child be moved later on to permanent foster care the

22
foster family must know as much as possible about the child’s difficult history. The same psychologist
who has followed the child from birth will liaise with the foster parents. The foster carer also receives
supervision and help to manage the child.
Tools
The team works with the family using a carefully selected range of tools, which they have learned well.
They use the Brazelton’s NBO tool to ascertain how the parents take in and use the information about
the child and to assess their capacity to think about the child. They find the Working Model of the
Child Interview particularly good because it shows if the parents can mentalize about the child and
one can almost predict what the attachment pattern will be when they do the Strange Situation test
in future. Weekly Marte Meo (video feedback) is done with the parents and analysed according to the
Marte Meo principles, but the professionals also utilize the Crittenden’s Care Index for further
analysis. The Bailey Scales of Infant Development (BSID), Ages and Stages Questionnaire (ASQ) and
Ages and Stages Questionnaire – Social Emotional (ASQ-SE) are also used with the families to measure
the child’s development.
With all the instruments used it is a challenge to follow up properly with supervision and to help the
team to learn them well enough for them to be helpful tools. One can get drowned in the measures
so it’s useful to share with those who use it extensively and know it well. It’s not just about the scores
but also the observation of the parent-child interaction.
The Role of Foster Carers
My final meeting in Norway was with
Tove Walstrom, General Secretary of the
Norwegian Foster Care
Association. The Association aims to be
a driving force to improve quality at all
levels within foster care. It is a national
and independent organization in relation
to political parties and religious
communities.
Mette had shown us the role of the authorities in keeping children safe and out of foster care, but if
all efforts fail, the child must be removed to a foster home. Approximately 11,500 children are placed
in foster homes (private, municipality homes, state, specialised, religious, etc.). Only 10% are placed
in institutions such as the Aline Clinic.
Tove highlighted some of the issues of the foster carers, who are often portrayed by the media in a
negative way. The role of the association since 1981, is to challenge the media about their negative
portrayal of foster carers, including the airing a current TV series. Tove campaigns on behalf of foster
families with a relentless, pioneering spirit.
Foster carers are able to call the association with issues of concern and the association notices the
patterns of concerns presented by the carers. They are then able to lobby and campaign in order to
bring about change that will improve the experience of the carers. Carers say that they feel heard and
supported by the Association.

23
Conclusion from Norway
In many ways, Norway is very similar to Sweden in the way that they care for children in early years.
In both countries, the care from pregnancy onwards ensures the best possible start for children. The
main difference that I observed, is that there is a more cohesive IMH provision in Norway that is
generously funded by the government. This builds on the strong foundations of physical care already
in place to protect the parent-infant relationship.
The work of RBUP is a unifying factor across Norway, providing a clear model for working with the
parent-infant relationship. By using a wide range of carefully selected tools that have been researched
and adapted to suit the Norwegian way of life and embedded in the main hospitals across the country,
the professionals are able to speak the same language. Regular training by RBUP, ‘the centre that
holds’ together the national vision for IMH, ensures that tools are kept sharp and professionals are
skilled in their use. They are also freed from the pressure of using tools primarily to measure
outcomes, in order to attract funding and re-commissioning. The financial backing from the
government frees them to focus on ‘seeing the baby’.
Residential work seems to be more prevalent in Norway, providing a more concerted effort to keep
children with their families, rather than to remove them to foster care. The emphasis is on supporting
the family and carefully following their progress even after they seem to be doing well. If all fails,
parents and infants are placed together in foster care, and only if this fails are the children removed
from the parents. If this happens, the emphasis is on supporting the parents to understand and accept
that the foster placement is the best possible place for their child.
The model of parent-infant psychotherapy practiced in the UK, using psychoanalytic tools and infant
observation according to the Esther Bick Model, is not the norm in Norway. Instead, the IMH teams
depend on more concrete tools that provide a working structure for professionals, who are not usually
psychoanalytically trained. RBUP is attempting to bridge this gap by introducing Alicia Lieberman’s
Infant-Parent Psychotherapy training from California. Nevertheless, the UK emphasis on
psychoanalytically informed observational skills is still absent.
It is noticeable in Norway that clinicians remain in post for many years, providing a sense of
permanence for the mothers and babies. For instance, Anne Margrethe Rostad in Trondheim has
worked tirelessly to embed her model for over 35 years and Greta, who runs the group for mothers
with complex needs has been in post for over 26 years. The same pattern is seen in the working
patterns of staff at the residential units, which creates a secure base for the families to return to. It
seems to me that this longevity is due to the passion of the professionals and their love for mothers
and babies, combined with the high quality of the provision. The backing of the government reduces
the ongoing stress of proving one’s worth; leaving space and time to really focus on the parent-infant
relationship.
Norwegians are proud of their culture, so there is an emphasis on researching the best practice from
overseas and adapting it to suit the Norwegian way of life.

24
Lessons from Michigan, USA
I started the final phase of my travel Fellowship
adventure at the Michigan Association of Infant
Mental Health conference in Kalamazoo, which
enabled me to network with many of the
professionals working in Michigan and hear what's
really happening on the ground.
Historical Development of Parent-Infant Psychotherapy in Michigan
I decided to start my American travels in Michigan because it is the birthplace of parent-infant
psychotherapy (PIP). To be more precise, PIP was birthed out of a sharing of knowledge between the
UK and the USA... and this sharing continues today.
Selma Fraiberg
Selma Fraiberg (1918-1981) was a social worker from Michigan who was trained as a psychoanalyst
by Anna Freud, in London. She then moved back to the USA and pioneered a model of parent-infant
psychotherapy that she described in her famous paper 'Ghosts in the Nursery' (Fraiberg, et al.,
1975). She was said to have been the first to use the term parent-infant psychotherapy. I think every
parent-infant psychotherapist knows her paper inside out (perhaps). Selma's starts her paper; "In
every nursery there are ghosts. They are the visitors from the unremembered past of the parents, the
uninvited guests at the christening…"
Parent-infant psychotherapy is about expelling the ghosts from the nursery. According to Selma
Fraiberg (1975), parents bring to the task of parenting, their own experience of having been parented;
their resolved and unresolved conflicts, which become activated when they parent their own
children. Like 'Ghosts in the Nursery’ these conflicts invade the parent-infant relationship and
negatively impact feeding, toilet training, discipline, etc., by influencing the way parents interpret their
child’s behaviour.
For instance, they might have expectations of their child, which prevent
them from seeing him as a unique individual. Or perhaps the child is
seen as a replacement of someone who died. The parent might also
use the child to fulfil their own failed ambitions, leaving no room for
the child to develop in his own right.
More malicious 'ghosts' might present themselves in the nursery. For
instance, a parent might have been severely abused in childhood and
in their determination to protect their child could become merged with
the child, leaving no room for the child to separate and grow in a
healthy way, for fear that someone might hurt him. As the therapist works with the parents and child
together, the parents gain insight into these unconscious patterns of relating to their child and are able
to free the child from the unconscious baggage that they have dumped on him.
The Michigan conference celebrated the work of Selma Fraiberg (1918-1981), who devoted her career
to helping troubled children. Selma argued that all subsequent development is based on the quality
of the child's first attachments. She instilled these beliefs and values into her students and these
values have been preserved by the Michigan Association of Infant Mental Health (Mi-AIMH).

25
Mi-AIMH was set up by the first and second cohorts of community-based clinicians, who had
completed their training at Selma Fraiberg’s Child Development Project at the University of Michigan,
who wanted to share their excitement about their work. The graduates invited a respected
paediatrician, T. Barry Brazelton as their speaker at their first conference and were amazed that 800
people attended from all over the country. It was very enriching to share in the celebration of 40 years
of the Association and to be reminded of the legacy of Selma Fraiberg, who described the essentials
of infant-parent psychotherapy clearly and simply so we can understand it. One of Selma’s students,
Michael Trout, set the scene of the 2017 Mi-AIMH conference by reminding us of Selma’s values, with
a skilful presentation about the parent-infant interaction and the meaning of early experience.
Infant Mental Health ... 'a way of being with'
Using music, poetry and a soothing tone of voice Michael created a rich reflective atmosphere;
demonstrating to us the importance of being mindfully present: A quality of 'being with' the parent
and infant rather than doing. Being present and fully attentive in the moment rather than
implementing strategies or bringing our own agendas.
The biennial conference allows clinicians from all backgrounds and disciplines to showcase their work
and research, and to top up their training in the competencies (explained below) required to work
safely with infants.
A Competency Framework for Infant Mental Health Practitioners
Later on during my travels I visited the Mi-AIMH headquarters
in Southgate, Michigan, to meet with Sheryl Goldberg, who is
the Director of the Association, and Nichole Paradis, the
Associate Director of the Alliance for the Advancement of Infant
Mental Health. Sheryl explained (below) how the Association
and Alliance have managed to create a competency framework
that supports best practice in infant mental health. She gave me
a copy of the competencies (left)
History and Development of the Competencies
Sheryl explained that the Federal legislation that was the
original impetus for developing the competencies was the 1986
Individuals with Disabilities Education Act (IDEA), and a specific
section of that which focused on birth to three year olds. That
legislation gave states the mandate to develop services that
took the family relationships of the baby in context, and
required each state to develop a comprehensive professional
development system that was competency-based. The original
set of competencies was intended to cross all 11 disciplines
listed in the legislation and additional discipline-specific competencies were included for those. Infant
Mental Health was not one of those specific disciplines in the legislation, but many IMH practitioners
who were also social workers, nurses, psychologists, etc. decided to build on the transdisciplinary
competencies already in existence and create IMH-specific competencies for the growing field of
professionals interested in developing IMH knowledge and practice skills. The idea of a credential (MI-
AIMH Endorsement) that would act as an overlay to one's professional license and would acknowledge
achievement of competency was a natural step from there. The original competency work that was
supported by the Federal and State governments took many years to achieve, and then MI-AIMH's

26
Competency Guidelines and Endorsement took another 10 years to develop. These developments
took place in the late 1990's, and in 2005, Texas was the first state to purchase the right to use the
competencies (only IMH organisations can purchase the right to use the competencies). At the time
of writing more than 27 US States plus Western Australia and Ireland have bought into the
competencies.
The development of a framework ensures that each competency has the same value in every state,
involves the same number of training hours, supervision, requirements for work experience and
processes for qualification.
The federal office specified eleven competencies to which IMH professionals must adhere in order to
have access to state funds. However, over a period of ten years, Mi-AIMH has exceeded the
specifications of the state and developed a set of endorsement credentials, to ensure that
professionals graduate with enough skills to deal with matters of IMH. The Association also provide In-
service training and continuing education to support the growth of professionals after graduation and
accreditation.
Alliance for the Advancement of Infant Mental Health
Michigan is unique in that it has the largest IMH workforce in the world, of which the largest number
is concentrated in the Detroit area. The Association continues to grow and due to this rapid growth
beyond the state of Michigan the Alliance for the Advancement of Infant Mental Health
was launched on 1st July 2016... well, that was the official date but in reality, things started in 2005
when Texas came on board.
The Alliance is a global organisation that includes those states and countries whose infant mental
health associations have licensed the use of the Competency Guidelines® and Endorsement for
Culturally Sensitive, Relationship-Focused Practice Promoting Infant Mental Health® under their
associations’ names.
The idea of integrating practice with grass roots training of professionals is known as ‘Engagement
Scholarship’, which permeates the entire culture of the IMH educators and workforce.
Training and Practice
Engagement Scholarship
The phrase ‘Engagement Scholarship’, was coined by Hiram Fitzgerald, Associate Provost for
University Outreach and Engagement and University Distinguished Professor, Michigan State
University. Hiram is also active in the Engagement Scholarship Consortium (ESC). Engagement
Scholarship is scholarship-driven community engagement. In layman's language this means that
researchers and academics do not sit in their ivory towers but actively engage the community with
research and mobilise research knowledge to make a difference.
All the main universities in Michigan seek to implement Engagement Scholarship in their teaching
strategy, research and practice, including The Merrill Palmer Skillman Institute - Wayne State
University, which is the home of the Infant Mental Health Dual Title Programme. The Institute has
a three-pronged approach; namely research, community engagement, and education. The aim is to
translate valuable research back into the community as effective interventions. Hiram and his
department seek to change communities by building engagement into the core academic
mission; the outworking of which is evident in the wide range of research on matters of infancy and

27
other issues, that is being undertaken within the three main Michigan universities, and now in several
countries of the world.
The Infant Mental Health Dual Title Programme
I observed the delivery of the Dual Title Infant
Mental Health (IMH) Programme, by Ann
Michele Stacks (left), Director of the Program at
the Merrill Palmer Skillman Institute - Wayne
State University (MPSI - WSU). Ann works closely
with Carla Barron (right), Clinical Coordinator of
the IMH Program.
Trained at Michigan State University and the
University of Michigan in psychology, marriage
and family therapy, infant mental health and
family and child ecology; Ann developed the Dual Title Degree in Infant Mental Health. The course
integrates the competencies developed by the Michigan Association for Infant Mental Health (Mi-
AIMH). She has won various awards for her service and undertaken a wide range of research; such as,
'the influence of psychosocial risk on early parenting and infant development; reflective
functioning; the effect of maltreatment in infancy and infant mental health interventions.
The ten students, which comprised the class that I observed, are also registered onto other Masters
degrees at the university, mainly in social work, nursing and psychology. This additional IMH
component would equip them with the Mi-AIMH competencies to work as IMH specialists with infants
and their families. The selection process is highly competitive so those who are finally selected show
an exceptional level of commitment and motivation. The IMH modules are spread throughout their
main degree programme and are focused and intense. It made sense to me that most of the students
come from a social work background as these are the professionals most likely to meet the vulnerable
families that most need IMH interventions.
Benefits and Limitations to UK and USA Approaches.
This approach to IMH is very different from our approach in the UK, where our main IMH
professionals come from a psychotherapy background. Most of our training schools require trainees
to already be qualified therapists and have experienced personal therapy before they can specialise in
parent infant psychotherapy. In the UK there is a requirement to do a two-year observation of a
mother and baby dyad and some UK training institutions, such as the School of Infant Mental Health,
also require other forms of organisational observations in the neonatal intensive care unit, special
nurseries and other organisations working with infants. This equips the therapist to take into account
the impact of the organizational dynamics on the work with the mother-infant dyad. The
observational element is not so pronounced in the Michigan programme; not for lack of desire but
due to other constraints. I was assured that observational skills are integrated into every level of the
Mi-AIMH competencies and checklists are used to inform observation within the IMH workforce.
The UK training is more spread out whereas the US system is very focused and intense, which fits into
the way the university courses are structured and keeps training costs down. The Michigan model of
Infant Mental Health provides an ongoing structure for development and reflective supervision that
allows graduates to continue to grow in their practice as a member of the Mi-AIMH family. There is a
strong sense of connection among professionals in Mi-AIMH and a family bond that is kept alive due

28
to the bi-annual conference, which is a very important opportunity for this family to come together
and feel a sense of belonging.
The teaching style of the IMH Dual Title Programme is very dynamic and I was amazed at the volume
of work that was set for the students to do between classes. I seriously doubted that they would be
able to deliver on time. However, the following week I was proven wrong.
By the second week of the training, the students had read several papers, watched a lecture at home
and completed quizzes at different points during the lecture, which had to be emailed to Ann by
midnight on Tuesday. Watching interactive lectures online between classes and taking the quiz frees
up time in class and students can watch the fifteen-minute lecture many times and feed-back their
feelings online. They would then inform Ann of any questions that they wished to be addressed in the
next class or one to one as appropriate. Class time is devoted to discussion and in order to participate
in discussion everyone is expected to have done all the assignments before the class. There is no
room for skiving or being lazy because students are accountable to one another and score each other
in class, from zero to twenty, depending on level and quality of participation. Failure to attend class
earns a score of zero. Scores go towards the final grade. There are no surprises where grading is
concerned and the criteria is made very clear; all information is available online. With only seven
meetings in this particular module there's a sense that time is precious and must be used to the
utmost.
I was amazed at the progress of the students after just a week. Every student had delivered and
demonstrated a surprising understanding of theoretical concepts after such a short time; as if they
had been on the programme for a year rather than just a week. In the exercises set before the class
they had to start to use the theory encapsulated in the paper ‘Ghosts in the nursery’ (Fraiberg, 1975),
to tease out the different strands of IMH and to grasp the six pillars of IMH as described by the Mi-
AIMH competency framework. The teaching goes beyond parent-child psychotherapy; it includes
other aspects such as assessment, advocacy, concrete assistance, developmental guidance, emotional
support (listening emphatically and non-judgmentally; nothing is off limits), parent-infant
psychotherapy (making links from past to present).
I was also mindful of the amount of work that Ann had to put in before every class. All the questions
and responses to the students' quiz had been analysed and used to plan the class and responses fed
back to the class and discussed in detail. If students are required to put in four hours of work for every
hour in class, then I'm not sure how many hours Ann had to put in to analyse their work. During the
class she moved between the groups to assist the students to practice what they learned as they would
be required to apply the learning individually to the case studies that would be set for the coming
week. Every student was focused and engaged. I would be delighted to teach such a class. According
to Ann, they get even better as the course develops; ‘When they start clinical work they really go’.
I will be looking further into how the Dual Title IMH course is structured because it is so dynamic and
effective. When students are so hungry to learn it's a real pleasure to teach. They remind me of
the Parent-Infant Partnership (PIP) team in London, whose passion to serve and to learn makes it a
pleasure to go in to work each day.
Parent-Infant Research and Interventions in Michigan
Parent-Infant interventions in Michigan are based on the principles of scholarship-driven community
engagement, whereby nearly all interventions have been developed through research and packaged
to be delivered by the IMH workforce, such as social workers, psychologists, nurses and day-care
29
professionals, etc. I observed a range of these interventions and met with researchers who have
developed programmes that are widely used in Michigan.
Centre for Natural Connections (CNC)
One programme that I found very powerful was presented at the
Mi-AIMH conference by Marva Lewis, PhD and Kandace Thomas,
MPP. Based at the Centre for Natural Connections (CNC), the
programme promotes the positive benefits of the daily task of
combing hair as an opportunity for parents to connect with their
children, culture, and community. The programme helps parents
to fully accept their child regardless of their skin colour or hair
type, and teaches active listening using the simple, yet powerful,
daily routine of combing hair. It was quite revealing to share our
own early hair stories and what it felt like when our primary
carers combed our hair. The powerful presentation evoked a
range of positive and negative feelings in delegates.
Marva shared over a decade of research on the hair-combing task. As a result of her studies she
established a routine and ritual as a valid context to assess and intervene with African American
mother-child relationships (Lewis, 1999).
'Ten minutes per day x 365 days per year x 12 years of combing a child’s hair equals 4,380
opportunities for parents to bond with their children during this simple daily task'.
The findings from Marva's research suggest that the behaviours that occur during hair-combing
interaction (HCI) - talking, touching, and listening – are the same behaviours that strengthen the
attachment bonds between parent and children. The ritual of the hair-combing task can also be used
to re-connect and unite parents separated from children due to placement of the child into foster care
or other traumatic separations.
Marva showed us a lovely clip of a young mother in a
mother and baby unit, combing her baby's hair. Despite
the unfortunate circumstances in which she found herself
her interaction with her child demonstrated many
strengths that she had inherited from her own experience
of having been parented by a good enough mother. She
sang and played with her baby, taught nursery rhymes and
talked to her about family and friends; turning the
experience into a fun game. Afterwards, the child felt proud and pretty. A great way to connect and
build self-esteem.
Research and Interventions with Babies and their Caregivers
Carolyn is Assistant Professor and Associate Director of the Infant Mental Health Programme at the
Merrill Palmer Skillman Institute for Child and Family Development. She works closely with Anne
Michele Stacks and Carla Barron to plan and deliver the IMH Dual Title Programme.

30
Carolyn is involved in several areas of research, but as we
toured her lab we focused on her Lullaby Study and shared
stories about the power of singing to babies. Singing to Babies
in Motown! The Detroit Lullaby Study examines what happens
when parents sing to infants and how this helps to regulate the
infant.
Another area of research, entitled Baby on Board! The WSU
Early Parenting Study, aims to understand the underlying
processes that parents experience as they prepare to parent a new baby. I was particularly interested
in the aim of this research which seeks to improve intervention and support services to fathers who
are struggling to parent in the face of adversity. Carolyn's focus on fathers is also seen in another
study; Development and Implementation of a Fathering Program in Detroit, Michigan; The central aim
of this study is to develop a family-centred and culturally-informed preventive parenting intervention
for fathers and their parenting partners.
All the research mentioned above have a vast impact on the way professionals work with families to
provide the best possible outcomes for their infants. They pass on the knowledge to parents, social
workers, teachers, nurses and other professionals who work face to face with parents and infants;
packaged, manualised and easy to deliver.
Hearts and Minds on Babies
I met Holly Brophy-Herb, at Michigan State University at the Building Early Emotional Skills Lab (BEES),
where she's Director.
At the BEES lab, Holly is involved in a very wide
range of research projects but shared with me
about the Hearts and Minds on Babies Study, which
is a multi-university collaboration between Wayne
State University, Michigan State University & the
University of Michigan and between Early Head
Start programs in the Lansing and greater Detroit
areas. The focus of this project is on the effect of
stress on the capacity to build relationships.
The project consists of a 13-week programme and is built on a tree metaphor. It aims to help parents
and teachers to respond rather than react; to develop coping strategies to reduce stress
levels. Parents are helped to recognise the verbal and non-verbal cues of infants and toddlers
and their moments of connection; allow time and space for emotion to be heard rather than
distraction (emotional nurturance).
Parents learn to recognise moments for branching out
and times for exploration and how adults can support
that by giving the child opportunity to explore rather
than swooping in. The curriculum includes
information on guidance and discipline; asking what
need is driving the behaviours (kicking, biting, etc.). This project is a five-year study, in its third year
at the time of writing. The hypothesis is that the curriculum will result in reduced stress.

31
The BEES curriculum is an eight-week course designed to be used one on one at home visiting. This
study has really taken off all over Michigan. Parents can meet together weekly or participate in an
online version, which involves discussion boards. Parents move through the course at their own pace
– they love the discussion board which includes videos, etc. and is easier to monitor as researchers
can get data online by looking at the way the programme is used. A version of the course is being
developed to enable child care providers and social workers to learn about infant and toddler
development.
The BEES course aims to fill the gap in provision for children aged zero to 3 years and their families by
focusing on four main areas
1. Building parental awareness
2. Listening to and interacting with the child
3. Identifying and labelling emotions and
4. Developing self-regulation strategies over time
The main theory behind the study is that positive social emotional development, in the context of
secure, responsive relationship, provides an important foundation for later learning. If you would like
to read more you can visit Holly’s lab by video here: https://vimeo.com/180771770
Another research project that Holly is involved with is called CUPID, which is an acronym for the
Collaborative for Understanding Pedagogy in Infant and Toddler Development ... (Yes, I prefer the
shortened version too). This study involves 22 universities and aims to develop a set of competencies
to guide the training for infant and toddler workers, children, parents and anyone working with birth
to three.
The Prenatal Stress Study
This is a significant study on the impact of stress during pregnancy, led by Alytia Levendosky, PhD. We
already know that stress during pregnancy has a negative impact on the infant's brain and behavioural
development. However, Alytia's study explores whether there are sensitive periods in pregnancy
when stress is particularly harmful. The study uses intimate partner violence, one of the most common
stressors for pregnant women and their developing child, to determine precisely when during
pregnancy (early, mid, late) stress exposure has the greatest impact on infants and whether or not the
maternal stress response system changes these effects.
Alytia and her team recruited women early in pregnancy (less than 20
weeks’ gestation) and ages 18—34, who currently or recently
experienced intimate partner violence. Participants make four visits to
the research office; three during pregnancy, and one 6 months after
baby is born. At these visits, the research team collect saliva samples,
do a survey and conduct a brief public speaking task. Participants are
also asked to complete two days of home saliva sampling after each
interview and a brief questionnaire each week of pregnancy. Strict
standards of confidentiality are observed to protect the women
involved. This is asking quite a lot from these women who are already
stressed, however, they are paid generously for their involvement.

32
Open Hearts, Open Homes
I had the privilege of meeting a special family in Detroit, that open their doors to mothers and their
babies; and I experienced what it feels like to be cared for in this way. Rebecca Lawlor invited me to
her home on Mother’s Day, to celebrate with her family. As a visitor, far away from home, I was
Taken from ImPrints,
Merrill Palmer Institute for Child and Family Development, July 2017

33
touched. After meeting Rebecca's mother and meeting her family, I understood where Rebecca's
generosity and hospitality came from.
Over the years, Rebecca’s parents have opened their doors to any child that needed a home and love,
adopting them if needs be. They recently started a group for mothers and babies, drafting in her
neighbours and other family members to help with clothing, food, toys, etc. Where there has been
no provision by the state, it is people like Rebecca and her family that offer food, clothing and comfort
to the needy people in their neighbourhood. According to Rebecca's mother, 'If you have no children,
all you have to do is open your doors and they will come to you'. Even as we spoke in the garden of
their home, a mother arrived at the house with her three children. They had recently joined the
parent-child group and were quite destitute. Rebecca's mother excused herself from the conversation
to attend to the family and to ensure that the children had something nutritious to eat.
Conclusion from Michigan
The delivery of parent-infant psychotherapy in Michigan looked different from the model that I know
in the UK, which is surprising because its founder, Selmer Fraiberg, was trained at the Anna Freud
Centre in the UK. I am accustomed to using myself as the main tool in the work and utilising practiced
and developed observational skills, combined with the psychoanalytic approach, to uncover
unconscious patterns that impact on the parent-infant relationship. What I observed however, were
concrete interventions based on research and embedded with the Mi-AIMH competencies.
Mi-AIMH provides an umbrella for the IMH network, in a similar way that RBUP provides a ‘centre that
holds’ together the training and regulation of practitioners. Professionals gain a sense of belonging
within the Association and feel part of a bigger family that values diversity.
It makes sense in the competitive US context that interventions are packaged in a way that makes
them accessible to be used by practitioners across many professions, such as teaching and social work.
This is how Selma Fraiburg started the practice of parent-infant psychotherapy.
Few in Michigan could afford the long, drawn out parent-infant psychotherapy training in the UK,
though many long for the privilege. After observing the effectiveness of the training and the
competitive culture of scholarship driven interventions, I cannot question the fact that the approach
works within the USA context. The field is wide open to anyone that can demonstrate a well-
researched, culturally diverse programme.
The Americans have found ways of integrating IMH training into existing degree programmes, such as
the Dual Title Programme, and adding onto their specialisms by achieving the Competencies of the
Michigan Association of Infant Mental Health. Ongoing professional development and regulation of
practice is provided by the Michigan Association and Alliance.
Also heartening to see was families like Rebecca’s, who have opened their doors to parents and infants
in the community.
Lessons from California, USA
My final stop in California brought me closer to a model of parent-infant psychotherapy with which I
am familiar in the UK: Alicia Lieberman’s model, which is used at the Infant-Parent Project in California.
34
Historical Development of Parent-Infant Psychotherapy in San Francisco, California
My USA journey followed the footsteps of Selma Fraiberg from Michigan, where parent-infant
psychotherapy was birthed through her work, to California, San Francisco, where she died.
Selma was a social worker who trained as a child psychoanalyst at
the Anna Freud Centre in London. She developed her approach to
working with families in Michigan, and relocated to San Francisco
at the invitation of the University of California, San Francisco
(UCSF), where she served as a professor before her untimely death.
Three colleagues relocated with her to help her to carry ‘the
beautiful load’; the practice of parent infant psychotherapy to
California, and to embed its principles into the curriculum at the
university. I learn from my hosts, Kadija Johnston and Maria St
John, of the traumatic outcomes for Selma and her three
colleagues.
Selma was invited to the University of California, San Francisco due to her parent-infant
expertise. Three other colleagues (Alicia Lieberman, Jeree Pawl & Judith Pakersky) uprooted
themselves from the University of Michigan to accompany her in her mission. Within two years Selma
died from a brain tumor. Without Selma, the original plan could not go ahead so her three faithful
colleagues were left high and dry, without the funding and support that Selma attracted. We can only
imagine what that must have felt like for these women and their families? Somehow, from this
traumatic situation the work of the Infant Parent Programme emerged and has been located at the
hospital’s trauma centre ever since.
Talking to Kadija, made me realise that it was not so long ago that parent infant psychotherapy was
birthed, because Judith Pakersky, one of Selma's colleagues, was one of Kadija’s professors. Alicia
Lieberman, also one of Selma's companions and pioneers of the IPP, still continues her trauma based
work in San Francisco. Later on in my visit I had a chat with Alicia, who works closely with Maria and
Kadija. Since my return from my Fellowship travels, she has also corresponded via email to connect
me with other key professionals.
The Infant Parent Programme (IPP)
Taken from The UCSF Infant-Parent Program, 2017
The U.C.S.F. Infant-Parent Program is a multifaceted infant and early childhood mental health program
specializing in serving children birth to five years of age with a particular commitment to underserved,
vulnerable and at risk populations. Based at the Zuckerberg San Francisco General Hospital and
Trauma Centre, it provides services that include infant-parent psychotherapy, perinatal mental health
service, case-centred and programmatic consultation, therapeutic play groups and therapeutic
shadowing. The aim of the Infant-Parent Program’s relationship-focused interventions is to protect
and support the natural capacity of very young children to grow up valuing themselves, caring about
others and competent to contribute to society. These capacities are shaped in the first few years of
life by the way in which children are treated by those responsible for their care. From these
relationships, they learn how to feel about themselves, how they fit into the world and what the world
has to offer them.

35
About 100 families are treated each year by the programme and nearly 90% of the work is done in the
home, unless the family chooses otherwise.
The IPP in Action
In order to understand the structure of the IPP, I participated in the
typical day to day life of the staff and students; joining seminar
groups, supervision sessions and presentations and visiting
community projects. The training, led by Professor Maria St John,
is aimed at post masters and doctoral students. Students alternate
case reviews with intensive supervision.
The students see families once a week in their homes or at the
trauma centre and the cases are taken to weekly supervision. In
order to receive this service, the families must qualify for Medicaid,
therefore participating families are usually very stressed and
traumatised. This work is not for the faint hearted as it requires
that the clinician be able to focus on the parent-infant relationship
amidst the family's stresses and strains of daily living, such as
accessing medical care, legal help on immigration, asylum seeking,
deportation preparation, domestic violence, etc.
As in Michigan, I noticed that the students come from various
professional backgrounds. The focus of the class I attended was on ending interventions with families,
which was timely for the students, because many of them were soon to finish the course. Tessa
Baradon's (2005) paper on endings from her book, 'Claiming The Baby', was the text under discussion.
After the seminar I joined Maria and one of her students who was preparing for a complex case
review. We grappled with the material in order to help the student to find new ways of thinking about
the family. I was able to understand why students received such intensive supervision; because the
level of pathology being dealt with in the families referred to the trauma centre is very high.
My third session of the day was the supervisors' meeting, where I was able to discuss with the team
about the different strands of the training offered by the university, i.e. perinatal mental health; infant
parent programme; early childhood mental health consultations and direct services, which are offered
as an extension of consultation. As a hospital that specialises in trauma, it is not an easy environment
to work in and those drawn to work here have a strong motivation and passion for this client group.
After the supervisors' meeting I took part in the supervision of a severe case. The mother and child
had been receiving help for three years and still the mother was not responding well. We explored
why it was that this mother was using the therapist so badly and not keeping appointments and how
much a therapist should cope with at the hands of clients. We discussed how the therapist could
set limits and give back responsibility to the mother, who repeatedly failed to attend meetings with
the team, yet declared her need for the service.
I considered my own attempts to engage ambivalent clients back in London. The experience of working
with emotionally unstable personalities equips you to know when to keep coming back and when to
suggest to the unwilling parent that perhaps this is not the best time for them to engage and why not
come back when it feels more convenient. For the zealous, enthusiastic trainee, eager to see change,
this was not such a simple decision, especially when the therapist comes from a position of
privilege. Her feelings of guilt were overwhelming as the client dared her to abandon her again. I

36
questioned, at what point does the patience of the therapist become the target for abuse and mitigate
against the building of a healthy, trusting therapeutic alliance?
A burden was lifted from the shoulders of the therapist as she is given permission to also look after
herself by setting limits for the client. Hopefully the client would learn gratitude, and understand
that, despite her privilege, the therapist is also a human being with feelings.
Poverty, Privilege and the Psychoanalytic Approach
I encountered the question of privileged professionals, in the Fifth Wednesday Multicultural
Gathering, where students and staff celebrate and reflect together on multicultural working. We
watched a provocative film which asks many questions: Can Latin Americans only benefit from
concrete interventions? Are Latin Americans analysable? Because they are poor does that mean that
they are not curious about themselves; or are they only occupied with poverty?
The film discussed ways of adapting psychoanalysis to non-traditional
patients; suggesting that the psychoanalytic tool will become relevant
outside the consulting room when psychoanalysts start to write papers that
more than five people understand. Can privileged psychoanalysts even
bear to hear about poverty - what it's like not to have enough food or to be
a victim of prejudice? Does the analytic setting produce the same pressures
that the clients face in society - the privileged analyst's fear of contamination? Is the couch only for
the wealthy?
We discussed some of these questions in small groups and I was humbled by the passion of group
members, who had come to the end of their training, with great prospects ahead. Will they join the
privileged or join those struggling within their cultural groups? What power do they possess to change
the status quo? Tears were shed in my small group.
Daycare
‘do unto others as you would have others do unto others’
As an offshoot of the work of the IPP, a mental health consultation programme was started about 30
years ago to bring the principles of IMH care to early care and education sites, in order to show carers
in those settings the importance of transforming relationships. The concepts have been introduced
to about 50 agencies in San Francisco that work with 0-5 year olds. Professionals include home visitors,
midwives, Neo-natal Intensive Care Unit, Obstetrics.
I met with Kristin Reinsberg, Director of Daycare Consultants at the Infant-Parent
Program. The program aims to help the adults caring for the children to understand and respond to
challenging behaviours appropriately, despite being overworked, underpaid and stressed. Many
children spend more than 40 hours a week in day care, therefore the daycare staff spend more time
with them than their own parents. The programme supports relationships between staff and
directors, staff and staff and staff and parents; helping them to think about what they want for the
children and creating a system where staff can have that also for themselves. Their motto is, ‘do unto
others as you would have others do unto others’; therefore, through the experience of being held,
heard and listened to, the staff are able to do listen to and hold fellow staff members, children and
parents. Many of the systems in which the teachers exist are ones in which their voice is not
heard. They are the unseen. Thankfully, things have changed from the 70s and the 80s. Wages and
access to education have improved, and with the introduction of reflective practice there is a stronger
emphasis on mental health consultation on a national level.

37
Homeless Families in San Francisco
Despite these improvements, there is evidence all around, of poverty and trauma in San Francisco,
such as acute homelessness, which is no respecter of persons. Of the 8,000 known homeless people
living in San Francisco, 25% are in families with infants and young children. The majority of San
Francisco’s homeless families are transient, living in shelters, cars, in cheap by-the-night hotels in the
city’s poorest neighbourhoods, or stay temporarily with friends or family. Because they are not visible
they are often forgotten.
I spent time with Andrea Scott, an Early Childhood Mental Health Consultant at the Infant Parent
Programme, whose role is to provide support to a variety of community based organisations. Andrea
took me to see two projects that work with homeless families. Her background in education and her
work with victims of severe trauma has prepared her well for this role.
Our first stop is the Hamilton Project for homeless families, where
Diana meets us and shows us around the vast property which
houses over 50 families each night and provides support for up to
25 families at high risk for chronic homelessness for 6 to 18
months. Families receive intensive social services to identify and
address factors contributing to their homelessness. The aim is for families to find and retain
permanent accommodation. Hamilton Children's Services also provides therapeutic support and
enrichment activities to strengthen children's resiliency, promote academic success and enhance the
parent-child bond. From Hamilton Housing we go to meet Lihea at Compass Children's Centre, which
is another project working with the homeless.
Though just a block away from the main centre of town I feel slightly nervous as we walk past drug
dependent individuals. The atmosphere is tense and Andrea seems to be watchful. She assures me
that she is known in the area so we are relatively safe. However, the area is known for its drugs and
shootings. The tension in the air is because it's the last day of the month and money will be received
and will be used on drugs to gain temporary relief from the miserable struggles of life.
A Treasure from the Archives of the Infant Parent Project
As I end my time at the IPP, Maria presented me with a treasure from the
archives of the University of California, San Francisco; one of the original copies
of the famous article, 'Ghosts in the Nursery' by Selma Fraiberg. I feel that I
have received a piece of history. This will be a prized possession.
Conclusion from California
The foundations of parent-infant psychotherapy in California is firmly embedded in Selma Fraiberg’s
training in the UK and her ensuing work in Michigan. This history unites the psychoanalytic approach
common in the UK, with the Engagement Scholarship approach of the USA. Born out of the trauma
of the founders, the IPP also focuses on trauma. A privileged workforce of post graduate doctorate
and PhD students from the university, immerse themselves sacrificially in the lives of those that are
less privileged.
It is not surprising that the students grapple with feelings of guilt that drive them beyond what is
reasonable, as they become targets for the clients’ projections. To avoid burnout, it is therefore

38
important that the students are held and nurtured through regular supervision, so they can be
equipped emotionally to hold the families in their care.
Some might question whether such extreme conditions of poverty merit the subtleties of the
psychoanalytic approach. I learned from the students on the verge of graduation, through their tears,
that a decision to remain working with trauma, is not an easy one. There is a temptation to flee into
greener pastures. However, like Rebecca’s family in Detroit, who resisted the ‘white flight’ from the
crumbling city; many remain and work to bring a measure of healing to suffering families in California.
Among them are my hosts, Kadija Johnson and Maria St John.
Recommendations for the UK
Competency Framework - The first recommendation for the UK as a result of my Fellowship
would be to follow the example of RBUP, Norway and Mi-AIMH, Michigan to provide a way of
measuring IMH competencies across all IMH professions. In the UK we enjoy a variety of
psychoanalytic parent-infant psychotherapy training provided by organizations such as the
Anna Freud Centre, The School of Infant Mental Health and OXPIP. However, at the time of
my travels there was no framework in place against which to measure the level of competency
of IMH professionals. Recently the Infant Mental Health Competencies Framework (IMHCF)
(Pregnancy to 2 years) was developed by The Association for Infant Mental Health (AIMH UK)
and The International School for Infancy and Early Years (ITSIEY) and is now being piloted.
Professionals will be able self-assess against the framework to find their level of competency.
AIMH (UK) will also be establishing the UK Infant Mental Health Recognition Register (IMHRR)
where practitioners will be able to gain recognition for their IMH knowledge, skills and
behaviours. This is a good step towards achieving good outcomes in the UK, but I believe that
it is necessary to undertake a careful piloting of the framework over an extended period of
time, to enable as many professionals as possible to make input. [email protected]
A Centre That Holds – Norway has demonstrated to the world that the mental well-being of
a nation requires the establishment of a 'Centre that holds' together the work of infant mentaI
health; disseminating training and good practice at grass-roots level. The UK lacks such a
strategy. PIP UK stands in a good place to fill this gap, having already established a network
of PIPs across the UK, such as the Croydon Best Start Parent-Infant Partnership. However, to
achieve noticeable impact there needs to be an investment at government level in a
nationwide strategy, such as the 1001 Critical Days agenda, that will make possible the
replication of PIPs in every locality. A response letter to the Transforming Children and Young
People’s Mental Health, Green Paper, to the Secretary of State for Health and Social Care
(http://www.pipuk.org.uk/sites/default/files/JH%20PIP%20UK%20re%20Green%20Paper%2
06.2.18.pdf) presents evidence for such a national strategy.
A Strategy for the UK – As a result of my Fellowship, I recommend a strategy for the UK that
brings together the various strands of learning from Scandinavia and the USA; including what
we know to be effective in current UK practice, as follows:
I suggest that national strategy for parent-infant psychotherapy in the UK should include;
1. Residential facilities for severe cases, where vulnerable infants and their parents or caregivers,
can receive parent-infant psychotherapy in the first 1001 critical days from pregnancy until
the parent-infant relationship is established. When baby is no longer at risk, families could be

39
discharged to independent accommodation, with regular follow-up, and return to the centre
as a secure base for ongoing support as required; as observed in Sweden and Norway.
2. Drop-in facilities for less intense cases, that provides;
a. Parent-infant psychotherapy for caregivers and their baby, who present with common
symptoms such as difficulty bonding with baby and eating and sleeping difficulties.
b. Regular groups, that act as a ‘revitalization bath’ for babies while they wait for their
mothers to become emotionally available.
3. Training facilities, embedded in research and focusing on the use of psychodynamic theory,
developmental science, and psychoanalytic observational skills; providing training for all levels
of work with parents and infants, in line with the IMHCF.
4. PIP teams in every community, that include a cross modality of experts, equipped to address
the holistic needs of the family; including parent-infant psychotherapists, trainees,
paediatrician, systemic family and couple therapist, integrative therapist, pastoral counsellor,
exercise and nutrition professional, clinical psychologist, music therapist, early years play
specialists, Milieu therapist / key workers, etc.
5. A Holistic Treatment Plan, that treats the whole person and not just a part and recognizing all
dimensions of the human experience, including physical, emotional, social and spiritual
aspects.
6. Operational teams, that will attend to the business and management of PIP projects;
overseeing fundraising, data collection to measure outcomes, budgeting and finance and daily
operations; enabling clinicians to focus on therapeutic work without distraction.
7. A Relationship Based Work Culture, that nurtures and cares for staff members through
reflective supervision and ongoing professional development; prioritizing respect and
enjoyment in their work; enabling them to pass on the experience of being cared for to
parents and infants and promoting permanence and longevity within the organization.
8. A Research-Based Culture, that utilizes the principles of Engagement Scholarship to provide a
quality, evidence-based service; using tools and measures that serve the purpose of the work
of ‘seeing the baby’ rather than the task of data collection for financial reasons.
9. A Replicable Service that can be duplicated across the UK through training, supervision and
consultancy.
10. A connected Service, that collaborates with key community services, such as health visiting,
midwifery, perinatal services, children’s centres, early years and the voluntary sector and
utilizes extensive national and international networking to disseminate findings and share
ideas in the field of parent-infant psychotherapy

40
Dissemination
I'm privileged to work with several networks of professionals in the UK and I'm hoping that they will
all benefit from my Fellowship findings.
Since returning from my travels I have been able to use my learning to
benefit my two main places of work; West London Action for Children
(WLAC), where I take a lead in early intervention and Croydon Best Start
Parent-Infant Partnership (CBSPIP), where I am the Clinical Lead.
I also aim to share my learning with the UK Council for Psychotherapy, where I am a member of
the boards of the College for Child and Adolescent Psychotherapy (CCAP), the Faculty for the
Psychological Health of Children (FPHC) and the Child Standards of Education and Training working
group (SETs). In the child college (https://www.psychotherapy.org.uk/about-ukcp/how-we-are-
structured/ukcp-colleges/college-of-child-and-adolescent-psychotherapies/), part of our work is
to monitor the standards for training of child psychotherapists. My goal within the UKCP is to ensure
that the voice of the baby can be heard in the midst of the much louder traumatic cries of children,
adolescents and adults. The children’s faculty http://www.childrensfaculty.org.uk/, aims to be
outward facing; organizing conferences and networking opportunities for professionals. Here I will be
given a platform to share my learning.
I am in the completion year of a doctorate research in parent infant psychoanalytic psychotherapy
with the University of Essex, and I am hopeful that this will lead to new platforms and opportunities
to put the findings of my research alongside my Fellowship findings, in
order to make a greater impact in this field. My research is ‘A qualitative
study of what leads to change in personal relationships in a family with a
child displaying pre-autistic behaviour’.
Other avenues for the dissemination of my findings are the training institutions with
which I am involved or teach Observational Studies, such as the School of Infant Mental
Health, http://www.infantmentalhealth.com/school and Terapia Centre,
http://terapia.co.uk/.
I look forward to making full use of the WCMT network to disseminate my findings. At the time of
writing I am preparing to speak at a conference entitled ‘Churchill’s Babies’, which will present a global
perspective on best practice in infant mental health and will address the complex needs of vulnerable
parents and their children, with insights from Churchill Fellows.
My blog has gained a big international following throughout my Fellowship and continues to be a
source of inspiration for friends, family, professionals and anyone who cares to read. I aim to continue
to link with my international hosts; sharing good practice and inspirational stories. My entire WCMT
adventure can be followed here http://www.yvonneosafopsychotherapist.com/single-
post/2016/11/03/Im-off-on-my-WCMT-travel-fellowship.

41
References
Baradon, T., & Joyce, A. (2005). The theory of psychoanalytic parent-infant psychotherapy. In T.
Baradon, C. Broughton, I. Gibbs, J. James, A. Joyce & J. Woodhead (Eds.), The Practice of
Psychoanalytic Parent-Infant Psychotherapy: Claiming the Baby. (p. 2540). London and New York:
Routledge.
Barlow, J. Bennett, C. Midgley, N. Larkin, S.K. & Wei, Y. (2015). Parent-infant psychotherapy for
improving parental and infant mental health (Review). The Cochrane Collaboration: Wiley & Sons,
Ltd.
Deep. C. (2017), MPSI Coordinator Wins Infant Mental Health Award. ImPrints. Merrill Palmer
Skillman Institute for Child & Family Development. Pg. 4. Wayne State University, July 2017
Fraiberg, S., Adelson, E. & Shapiro, V. (1975) ‘Ghosts in the nursery: a psychoanalytic approach to the
problems of impaired infant-mother relationships’. In Fraiberg, S. (ed) Clinical Studies in Infant
Mental Health. London: Tavistock 1980.
Leadsom A, Field F, Burstow, P & Lucas, C (September 2013). The 1,001 critical days: the importance
of the conception to age two period: a cross party manifesto. London: DH.
Lewis, M.L. (1999), Hair Combing Interactions: A New Pradigm for Research with African-American
Mothers. American Journal of Orthopsychiatry 69, no.4 (1999) 504-514.
Rostad, A.M. (2008), Predicting development deficiencies at the age of four based on data from the
first seven months of life. Infant Mental Health Journal 29(6):588 - 608
Salomonsson, B. (2014). Psychoanalytic Therapy with Infants and their Parents. Routledge 2014
Sander, L. (1983). Polarity, paradox and the organizing process in child development, in J. Call, E.
Galenson & R. Tyson (Eds.), Frontiers of Infant Psychiatry. New York: Basic Books.
Saracino, A.M. (2004), Relationship Treatment at a Baby-Parent Unit. The Signal. Vol. 12, No. 2.
Newsletter of the World Association for Infant Mental Health - June 2004
Turnbull, H.W, Scott, J.F. & Hall, A.R (1960). The Correspondence of Isaac Newton. Volume II 1676-
1687 (1960 552pp). Cambridge University Press, Cambridge.
42
Itinerary
Phase of Project & Date Professional / Role Organization / Event
Phase 1 – Prague 29th May – 2nd June 2016
World Association of Infant Mental Health Conference
Clarion Congress Hotel, Prague Freyova 33, Czech Republic
Phase 2 Sweden 5th -12th November 2016
Pia Risholm Motander Psychotherapist
Department of Psychology, University of Stockholm, Sweden
Anna Malmquist Saracino Psychotherapist, Group Analyst, Supervisor and Teacher in Psychotherapy Camilla Wachtmeister Child and Adolescent Psychotherapist
Infant-Child-Parent unit at the Child and Adolescent Psychiatry Department, Stockholm, Sweden
Björn Salomonsson Associate professor, M.D., researcher, specialist in general psychiatry, training in psychoanalysis and child analysis
Karolinska Institute, Stockholm, Sweden
Norway 14th – 15th November 2016 Trondheim
Anne M Rostad Hege Weld & Lise Psychologist
Blue Cross Lade Treatment Center (LBS)
16th November 2016 Tonsberg
Berit Lande Leader of Infant Mental Health CAMHS
BUPA poliklinikk spesial, Sykehuset, Vestfold Tonsberg, Norway
Oslo Marit Bergum Hansen Head od Department & Special Advisor
Regional Center for Child and Adolescent Mental Health, Eastern and Southern Norway (RBUP)
Phase 3, USA – Michigan & California 5th May–3rd June 2017
Sunday 7th -Tuesday 9th May 2017
Michigan Association of Infant Mental Health (Mi-AIMH) Biennial Conference
Radisson Plaza Hotel at Kalamazoo Center 100 W Michigan Ave Kalamazoo, MI, United States

43
Wayne State University 10th May
Ann Michele Stacks Director, IMH Dual Title Program
Participation in IMH Dual Title Class Merrill Palmer Skillman Institute Wayne State University
Thursday 11th May
Explore, rest, write
Friday 12th May
Tour of Detroit with Rebecca Wheeler & Carla Barron Clinical Coordinator, IMH Dual Title Program
Merrill Palmer Skillman Institute Wayne State University
Sunday 14th May
Exploration 2nd Baptist Church, Detroit
Monday 15th May Ann Michele Stacks, IMH faculty advisory board meeting Carolyn Dayton Researcher & Associate Director, IMH Dual Title Program
Merrill Palmer Skillman Institute Wayne State University Carolyn’s Lab - The Lullaby Study & other research
Tuesday 16th May 2017 Sheryl Goldberg Executive Director Nichole Paradis Associate Director
Michigan Association for Infant Mental Health 13101 Allen Road Southgate, Michigan 48195 www.mi-aimh.org Alliance for the Advancement of Infant Mental Health Southgate, Michigan 48195
Wednesday 17th May - 9am 12:00 - 1:30 at Ann’s office 4:30 - 7:50
IMH supervisor breakfast Ann, Carla, Carolyn Ann Michele Stacks
Talk about training programme Wayne State University Introduction to IMH Dual Title class
Thursday 18th May 2017 Travel to East Lansing
Friday 19th May 2017 Holly Brophy-Herb Director, Building Early Emotional Skills Lab (BEES)
Michigan State University 3 Human Ecology 552 West Circle Drive Michigan State University East Lansing, Michigan 48824
Saturday 20th & Sunday 21st May 2017
Writing East Lansing
Monday 22nd May 2017 Hiram Fizgerald Michigan State University East Lansing

44
Associate Provost for University Outreach and Engagement and University Distinguished Professor Alytia Levendosky Professor & Director of Clinical Training
Michigan State University East Lansing
Tuesday 23rd May 2017 Fly to San Francisco, California
California 24th May – 3rd June 2017
Maria St John & Kadija Johnston Infant Parent Program (IPP) Zuckerberg San Francisco General Hospital & Trauma Center, 1001 Potrero Avenue, Box 0852, Building 5, 6B San Francisco, CA 94110 Phone: (415) 206-44448.30
Wednesday 24th May 2017 Exploration
Thursday 25th May 2017 Maria St John Director of Training, IPP
Presentation of Infant Parent Program (IPP) to Children’s protective services
Friday 26th May 2017 Kadija Johnston Director, IPP
Overview of IPP and Lunch with Kadija
Saturday 27th to Monday 29th May 2017
Public Holiday Carnival, Exploration & Writing
Mission District
Tuesday 30th May 2017 Seminars, Case Supervision, Supervisors Meeting
IPP
Wednesday 31st May Multicultural Gathering Kristin Reinsberg, Director of Day-care Consultants
IPP IPP
Thursday 1st June 2017 Andrea Scott Early Childhood Mental Health Consultant, IPP Goodbye to Maria
Visit to Hamilton Families Homeless Project and Compass Children’s Centre
Friday 2nd June 2017 Final Explorations and Packing
Saturday 3rd June 2017 Checkout Airbnb Fly from California to London
Sunday 4th June 2017 Arrive in London