objectives primary prevention of heart disease · 9/29/2015 2 impact of ascvd in women • single...
TRANSCRIPT

9/29/2015
1
Samia Mora, MD, MHSAssociate Professor, Harvard Medical School
Associate Physician, Brigham and Women’s Hospital
October 2, 2015
Financial disclosures: Dr Mora has received
research grant support from Atherotech Diagnostics,
served as consultant to Pfizer, Lilly, Cerenis Therapeutics
Primary Prevention of Heart Disease:
What works? What doesn’’’’t?1. To review current challenges for atherosclerotic
cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
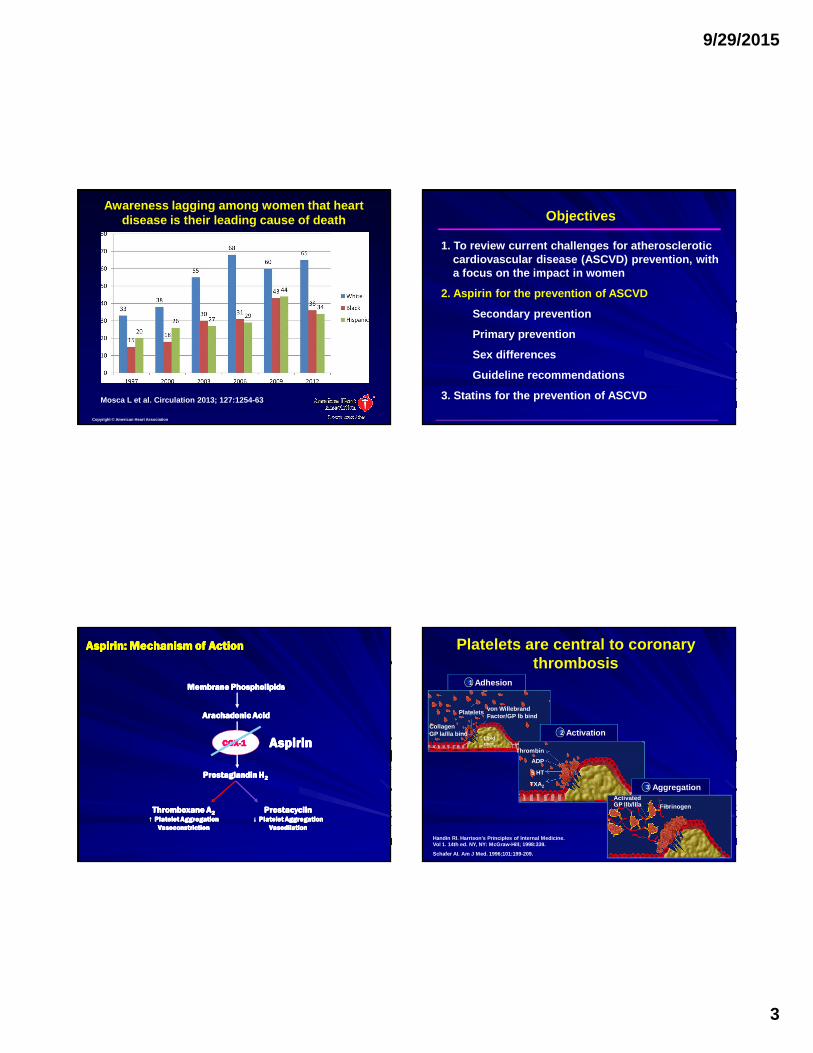
Objectives
1. To review current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
ObjectivesCardiovascular disease is the leading cause of
death in women and men (US: 1979–2009)
Mozaffarian et al. Circulation 2015;131:e29-e322Copyright © American Heart Association
Women
Men

9/29/2015
2
Impact of ASCVD in Women
• Single largest killer of women in US
• One in 30 women will die of breast cancer, vs. one in 3 will die from CVD
• One woman dies from CVD every minute
• CVD deaths in women = all deaths from cancer, lung disease, and Alzheimer disease combined
Impact of ASCVD in Women
•Black women ~ 40% more likely to die from CVD compared with White women
•Death rate in US women ages 35-54 is increasing, possibly due to obesity
•Two thirds of women who die suddenly had no prior symptoms (vs. ~ half of men)
•More women than men will have a second heart attack after their first heart attack
Impact of ASCVD in Women• More strokes than coronary heart disease (CHD) in women (opposite in men)
• Gestational diabetes (2-10% of pregnancies): increases risk of future diabetes by 30 to 60%
•Unique risk factors for stroke in women:
• pregnancy
• hormone therapy
• more hypertension at >age 65
Lifetime Risk of ASCVD Death for Women by Risk Factors at Age 45
Berry et al. NEJM 2012;366:321-9
4 Major Risk Factors:
Smk, DM, TC>240, BP>160/100 or HTN
Optimal Risk Factors:
Non-smk, non-DM, TC<180, BP <120/80
9/29/2015
3
Awareness lagging among women that heart disease is their leading cause of death
Mosca L et al. Circulation 2013; 127:1254-63
Copyright © American Heart Association
1. To review current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
Objectives
Aspirin: Mechanism of ActionAspirin: Mechanism of ActionAspirin: Mechanism of ActionAspirin: Mechanism of Action
Membrane PhospholipidsMembrane PhospholipidsMembrane PhospholipidsMembrane Phospholipids
Arachadonic AcidArachadonic AcidArachadonic AcidArachadonic Acid
Prostaglandin HProstaglandin HProstaglandin HProstaglandin H2222
COXCOXCOXCOX----1111
Thromboxane AThromboxane AThromboxane AThromboxane A2222
↑↑↑↑ Platelet AggregationPlatelet AggregationPlatelet AggregationPlatelet Aggregation
VasoconstrictionVasoconstrictionVasoconstrictionVasoconstriction
ProstacyclinProstacyclinProstacyclinProstacyclin↓↓↓↓ Platelet AggregationPlatelet AggregationPlatelet AggregationPlatelet Aggregation
VasodilationVasodilationVasodilationVasodilation
AspirinAspirinAspirinAspirin
Adhesion1
Platelets
Lipidcore
CollagenGP la/lla bind
von WillebrandFactor/GP lb bind
Activation2
Thrombin
ADP
5 HT
TXA2 Aggregation3
FibrinogenActivatedGP llb/llla
Handin RI. Harrison’s Principles of Internal Medici ne. Vol 1. 14th ed. NY, NY: McGraw-Hill; 1998:339.
Schafer AI. Am J Med. 1996;101:199-209.
Platelets are central to coronary thrombosis

9/29/2015
4
Meta-analysis of 16 randomized trials of aspirin(N=17,000 participants, 3306 serious vascular events)
• ���� 31%, nonfatal MI
• ���� 20%, major CHD events
• ���� 19%, total stroke
• ���� 19%, any serious vascular event
(Results similar in men and women)
Aspirin Evidence: Secondary Prevention of ASCVDAspirin Evidence: Secondary Prevention of ASCVDAspirin Evidence: Secondary Prevention of ASCVDAspirin Evidence: Secondary Prevention of ASCVD
Antithrombotic Trialist Collaboration. Antithrombotic Trialist Collaboration. Antithrombotic Trialist Collaboration. Antithrombotic Trialist Collaboration. LancetLancetLancetLancet 2009;373:18492009;373:18492009;373:18492009;373:1849
Antithrombotic Trialists’ (ATT) Collaboration 1. To review current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
Objectives
• The role of aspirin in primary prevention has not been as clear, particularly among women.
• The assessment of the benefits of aspirin in primary prevention is more complicated, since the absolute risks of vascular events are lower than in secondary prevention while complication rates (eg., bleeding) are comparable.
Aspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary Prevention
Number of Events (Aspirin vs. Control)
Rate ratio (95% CI) (Aspirin vs. Control)
Major coronary event 934 vs. 1115 0.82 (0.75-0.90)
Non-fatal MI 596 vs. 756 0.77 (0.69-0.86)
CHD mortality 372 vs. 393 0.95 (0.82-1.10)
Stroke 655 vs 682 0.95 (0.85-1.06)
Hemorrhagic 116 vs. 89 1.32 (1.00-1.75)
Ischemic 317 vs. 367 0.86 (0.74-1.00)
Unknown cause 222 vs. 226 0.97 (0.80-1.18)
Vascular death 619 vs. 637 0.97 (0.87-1.09)
Any serious vascular event 1671 vs. 1883 0.88 (0.82 vs 0.94)
Major extracranial bleed 335 vs. 219 1.54 (1.30-1.82)
Antithrombotic Trialists’ (ATT) Collaboration
Antithrombotic Trialists’ Collaboration. Lancet 2009;373:1849-60
Aspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary Prevention
Meta-analysis of 95,456 low risk patients randomized to aspirin
(100 mg every other day to 500 mg daily) vs. placebo for 4 to 10 years
Aspirin reduces the risk of ischemic events, but with a higher rate of bleedingAspirin reduces the risk of ischemic events, but with a higher rate of bleedingAspirin reduces the risk of ischemic events, but with a higher rate of bleedingAspirin reduces the risk of ischemic events, but with a higher rate of bleeding

9/29/2015
5
0.5 1.0 1.5 2.0
Non-fatal MI
Vascular Mortality
Major GI and extracranial bleeds
Serious Vascular Events
Antiplatelet Better Antiplatelet Worse
Rate Ratios for
Vascular Events
0
P=0.0001
Effect of antiplatelet treatment on vascular events
Antithrombotic Trialist Collaboration. Lancet 2009;373:1849
Stroke
Aspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary Prevention Aspirin Evidence: Dose and EfficacyAspirin Evidence: Dose and EfficacyAspirin Evidence: Dose and EfficacyAspirin Evidence: Dose and Efficacy
0.50.50.50.5 1.01.01.01.0 1.51.51.51.5 2.02.02.02.0
500500500500----1500 mg1500 mg1500 mg1500 mg 34343434 19191919
160160160160----325 mg325 mg325 mg325 mg 19191919 26262626
75757575----150 mg150 mg150 mg150 mg 12121212 32323232
<75 mg<75 mg<75 mg<75 mg 3333 13131313
Any aspirinAny aspirinAny aspirinAny aspirin 65656565 23232323
Antiplatelet BetterAntiplatelet BetterAntiplatelet BetterAntiplatelet Better Antiplatelet WorseAntiplatelet WorseAntiplatelet WorseAntiplatelet Worse
Aspirin DoseAspirin DoseAspirin DoseAspirin Dose No. of Trials (%)No. of Trials (%)No. of Trials (%)No. of Trials (%)Odds Ratio for Odds Ratio for Odds Ratio for Odds Ratio for
Vascular EventsVascular EventsVascular EventsVascular Events
0000
Indirect comparisons of aspirin doses on vascular events in Indirect comparisons of aspirin doses on vascular events in Indirect comparisons of aspirin doses on vascular events in Indirect comparisons of aspirin doses on vascular events in
highhighhighhigh----risk patientsrisk patientsrisk patientsrisk patients
Antithrombotic Trialist Collaboration. BMJ 2002;324:71-86
Aspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary Prevention
2015 U.S. Preventive Task Force Services updated meta2015 U.S. Preventive Task Force Services updated meta2015 U.S. Preventive Task Force Services updated meta2015 U.S. Preventive Task Force Services updated meta----analysisanalysisanalysisanalysis
Outcome No. trials No. individuals Summary Relative Risk
Nonfatal MI 10 114,734 0.78 (0.71-0.87)
Nonfatal stroke 10 99,655 0.95 (0.85-1.06)
CVD mortality 11 118,445 0.94 (0.86-1.03)
Total mortality 11 118,445 0.94(0.89-0.99)
Guiruis-Blake JM et al. 2015 www.uspreventiveserv icestaskforce.org
Aspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary PreventionAspirin Evidence: Primary Prevention
2015 U.S. Preventive Task Force Services updated meta2015 U.S. Preventive Task Force Services updated meta2015 U.S. Preventive Task Force Services updated meta2015 U.S. Preventive Task Force Services updated meta----analysisanalysisanalysisanalysis
Outcome No. trials No. individuals Summary Relative Risk
Nonfatal MI 10 114,734 0.78 (0.71-0.87)
8 (≤100 mg) 87,524 0.83 (0.74-0.94)
Nonfatal stroke 10 99,655 0.95 (0.85-1.06)
7 (≤100 mg) 68,734 0.86 (0.76-0.98)
CVD mortality 11 118,445 0.94 (0.86-1.03)
8 (≤100 mg) 87,524 0.97 (0.85-1.10)
Total mortality 11 118,445 0.94(0.89-0.99)
8 (≤100 mg) 87,524 0.95 (0.89-1.01)
Guiruis-Blake JM et al. 2015 www.uspreventiveservi cestaskforce.org

9/29/2015
6
Bleeding risks with aspirin
Risk factors for bleeding
Age
Male sex
GI hospitalization
Excess alcohol use
Current smoking
Hypertension
Diabetes
Liver / renal disease
Concomitant meds(NSAIDs, anticoagulants)
Whitlock E et al. 2015 www.uspreventiveservicesta skforce.org
Proton Pump Inhibitors (PPIs) may decrease risk of GI bleeding on aspirin
Tran-Duy A. et al. 2015 Int J Clin Pract doi:10. 1111/ijcp.12634
GI: Gastrointestinal
1. To review current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
Objectives
Aspirin in Primary Prevention: Sex differences?
Ridker, P. et al., N Engl J Med 2005; 352:1293-204 .
1.0 5.00.50.2 0.2
BDT, 1988
Combined
PPP, 2001
HOT, 1998
TPT, 1998
PHS, 1989
RR of MI Among Men
2.0
RR = 0.68 (0.54–0.86)P = .001
RR of Stroke Among Men
RR = 1.13 (0.96–1.33)P = .15
1.00.2 2.0 5.00.5
HOT, 1998
Combined
WHS, 2005
PPP, 2001
RR of MI Among Women
Aspirin Better Placebo Better
RR = 0.99 (0.83–1.19)P = .95
2.0
Aspirin Better Placebo Better
1.0
RR of Stroke Among Women
5.00.50.2
RR = 0.81 (0.69–0.96)P = .01
0.5 1.0 2.0 5.0
Berger JS et al. JAMA. 2006;295:306-313
Physicians’ Health Study (PHS)Physicians’ Health Study (PHS)Physicians’ Health Study (PHS)Physicians’ Health Study (PHS)
22,071 men randomized to aspirin (325 mg every other day) followed 22,071 men randomized to aspirin (325 mg every other day) followed 22,071 men randomized to aspirin (325 mg every other day) followed 22,071 men randomized to aspirin (325 mg every other day) followed
for an average of 5 yearsfor an average of 5 yearsfor an average of 5 yearsfor an average of 5 years
Aspirin reduces the risk of MI among men in the PHSAspirin reduces the risk of MI among men in the PHSAspirin reduces the risk of MI among men in the PHSAspirin reduces the risk of MI among men in the PHS
End pointEnd pointEnd pointEnd point Relative Risk (95% CI)Relative Risk (95% CI)Relative Risk (95% CI)Relative Risk (95% CI) P valueP valueP valueP value
CV Mortality 0.96 (0.60-1.54) NS Myocardial infarction Fatal 0.34 (0.15-0.75) 0.007 Nonfatal 0.59 (0.47-0.74) <0.00001 Total 0.56 (0.45-0.70) <0.00001 Stroke Fatal 1.51 (0.54-4.28) 0.43 Nonfatal 1.20 (0.91-1.59) 0.20 Total 1.22 (0.93-1.60) 0.15
Physicians’ Health Study Research Group. Physicians’ Health Study Research Group. Physicians’ Health Study Research Group. Physicians’ Health Study Research Group. NEJMNEJMNEJMNEJM 1989;321:1291989;321:1291989;321:1291989;321:129----35353535
CI=Confidence interval, CV=Cardiovascular, MI=Myocardial infarction, NS=NonsignificantCI=Confidence interval, CV=Cardiovascular, MI=Myocardial infarction, NS=NonsignificantCI=Confidence interval, CV=Cardiovascular, MI=Myocardial infarction, NS=NonsignificantCI=Confidence interval, CV=Cardiovascular, MI=Myocardial infarction, NS=Nonsignificant
Aspirin Evidence: Primary Prevention in MenAspirin Evidence: Primary Prevention in MenAspirin Evidence: Primary Prevention in MenAspirin Evidence: Primary Prevention in Men

9/29/2015
7
Mean Follow-Up Period of 10 years
First Major Cardiovascular Event:
Nonfatal Myocardial Infarction, Nonfatal Stroke, Ca rdiovascular Death
Aspirin(100 mg po onalternate days)
39,876 Initially healthy womenAge 45 years and older (mean age 54.6)
19,934 on Aspirin 19,942 on Placebo
Placebo
The Women’s Health Study
Aspirin Evidence: Primary Prevention in WomenAspirin Evidence: Primary Prevention in WomenAspirin Evidence: Primary Prevention in WomenAspirin Evidence: Primary Prevention in Women
Ridker P et al. N Engl J Med. 2005;352:1293-1304.
Women’’’’s Health Study: Major Cardiovascular Events(Nonfatal Myocardial Infarction, Nonfatal Stroke, C ardiovascular Death)
0 2 4 6 8 10
Years of Follow -Up
0.00
0.01
0.02
0.03
Cum
ulat
ive
Eve
nt R
ate
0 2 4 6 8 10
Placebo
Aspirin
RR = 0.91 95% CI 0.80 – 1.03
P = 0.13
9 percent
Aspirin for Primary Prevention in Women?
39,876 women randomized to aspirin (100 mg every other day) or placebo
for 10 years
Ridker P et al. N Engl J Med. 2005;352:1293-1304.
0 2 4 6 8 10Years of Follow-Up
0.00
0.01
0.02
Cum
ulat
ive
Eve
nt R
ate
0 2 4 6 8 10
0.00
0.01
0.02
Placebo
Aspirin
0 2 4 6 8 10Years of Follow-Up
0.00
0.01
0.02
Cum
ulat
ive
Eve
nt R
ate
0 2 4 6 8 10
0.00
0.01
0.02
AspirinPlacebo
Years of Follow-Up
0.00
0.01
0.02
Cum
ulat
ive
Eve
nt R
ate
Aspirin
Placebo
0 2 4 6 8 10Years of Follow-Up
0.00
0.01
0.02
Cum
ulat
ive
Eve
nt R
ate
0 2 4 6 8 10
AspirinPlacebo
Total StrokeRR = 0.83 (0.69-0.99)
P = 0.04
Myocardial InfarctionRR = 1.02 (0.84-1.25)
P = 0.83
Ischemic StrokeRR = 0.76 (0.63-0.93)
P = 0.009
Hemorrhagic StrokeRR = 1.24 (0.82-1.87)
P = 0.31
0 2 4 6 8 100 2 4 6 8 10
Women’’’’s Health Study – Stroke and Myocardial Infarction
Aspirin Placebo RR 95%CI P(N=19,934) (N=19,942)
Age (years)
45–54 (24,025) 163 161 1.01 0.81-1.26 0.92
55–64 (11,754) 183 186 0.98 0.80-1.20 0.84
>65 (4,097) 131 175 0.74 0.59-0.92 0.008
Major CV Event* = Nonfatal MI, nonfatal stroke, car diovascular death
The Women’s Health Study: Subgroup Analyses, Primary Endpoint of Major CV Eve nt*
*P for interaction by age = 0.05 for total CVD and 0.03 for MI

9/29/2015
8
† Major CV Event = nonfatal MI, nonfatal stroke, ca rdiovascular death
Endpoint Aspirin Placebo RR (95%CI) P
Major CV Event† 131 175 0.74 (0.59–0.92) 0.008
Total MI 41 62 0.66 (0.44–0.97) 0.04
Total Stroke 68 86 0.78 (0.57–1.08) 0.13
44 Fewer Major CV Events16 Additional GI Hemorrhages Requiring Transfusion
Women’’’’s Health Study: Subgroup Analyses, Age > 65 years
1. To review current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
Objectives
2010 Aspirin Recommendations for Patients with Diabetes Mellitus (ADA/AHA/ACC)
• Use aspirin 75 to 162 mg/day for secondary ASCVD prevention
• Consider aspirin 75 to 162 mg/day for primary ASCVD prevention in diabetic patients at increased risk
– Those at risk for ASCVD (10-year risk >10%)—men >50 yrs, women >60 yrs, with > 1 additional risk factor (family history of premature ASCVD, HTN, smoking, dyslipidemia, albumi nuria)
• Not sufficient evidence for aspirin for primary pre vention in low risk groups
Pignone M et al JACC 2010;55:2878
2011 AHA guidelines: CVD Prevention in women
• Aspirin (75 to 325 mg/d) in high-risk womenIf aspirin-intolerant: substitute clopidogrel
• Aspirin (81 mg/d or 100 mg every other day) in at risk women ≥65 years is reasonable if BP is controlled and benefit outweighs risk
• Aspirin in at risk women <65 years for preventing
ischemic stroke may be reasonable if benefit
outweighs risk
• Not Recommended: for preventing myocardial infarction in optimal risk women <65 years
Mosca et al. Circulation 2011;123:1243-1262

9/29/2015
9
2015 U.S. Preventive Services Task ForceDraft Recommendations for low dose aspirin
Guiruis-Blake JM et al. 2015 www.uspreventiveservi cestaskforce.org
Population Recommendation Grade
Adults age 50-59 yrs For primary prevention of ASCVD and colorectal cancer if:- ≥ 10% ASCVD risk *- Not at increased risk of bleeding- Life expectancy of at least 10 yrs- Willing to take aspirin for at least 10 yrs
B (Moderate)
Adults age 60-69 yrs Individualize the decision if:- ≥ 10% ASCVD risk, - Not at increased risk of bleeding- Life expectancy of at least 10 yrs- Willing to take aspirin for at least 10 yrs
C
Adults < 50 yrs Insufficient evidence I
Adults ≥ 70 yrs Insufficient evidence I
*Pooled Cohort Equations available at http://my.americanheart.org/cvriskcalculator
1. To review current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Statins for the prevention of ASCVD
Objectives
The information to estimate ASCVD risk (2013):age, sex, race, TC, HDL-C, SBP, BP Rx, diabetes ,
smoking ���� 10-yr risk of MI, fatal or nonfatal stroke, CHD dea th
���� lifetime risk
Prior (ATP III, 2001): Age, sex, TC, HDL-C, SBP, BP Rx, smoking
���� 10-yr risk of MI, CHD death
Goff et al JACC 2014;63:2935-59
*Pooled Cohort Equation available at http://my.americanheart.org/cvriskcalculator
2013 Cholesterol Guidelines
• New Equations* for ASCVD risk assessment
- Stroke included, in addition to MI
- Separate equations for blacks
• 4 Statin benefit groups
- Adults with clinical ASCVD
- Adults with LDL-C ≥190 mg/dL
- Adults 40 to 75 yrs of age with diabetes
- Adults ≥7.5% estimated 10-yr risk of ASCVD
•No LDL-C or non-HDL-C treatment targets
*Pooled Cohort Equation available at http://my.americanheart.org/cvriskcalculator
Stone et al JACC 2014;63:2889-934

9/29/2015
10
• High Risk– Clinical ASCVD* – LDL >190 mg/dL, age >21 years– Primary prevention – Diabetes: age 40-75 y,
LDL 70-189 mg/dL• Primary prevention
No diabetes, ≥7.5% 10-year ASCVD risk, age 40-75 years, LDL 70-189 mg/dL
*Acute coronary syndrome, MI, angina, coronary or o ther arterial revascularization, stroke, TIA, atherosclerotic per ipheral arterial disease (PAD)
4 Groups of High Risk Individuals
Stone et al JACC 2014;63:2889-934
Individuals Not in a Statin Benefit Group
Additional factors may inform clinical decision making
• Family history of premature ASCVD*• High lifetime risk • LDL–c ≥160 mg/dL• hs-CRP ≥ 2 mg/L• CAC score ≥ 300 or ≥75th percentile• Ankle brachial index (ABI) < 0.9
* onset <55 y first degree male or <65 first degree female
Stone et al JACC 2014;63:2889-934
Statin Evidence: Primary Prevention in WomenStatin Evidence: Primary Prevention in WomenStatin Evidence: Primary Prevention in WomenStatin Evidence: Primary Prevention in Women
.1 .5 1 5 10
AFCAPS/TexCAPS 1998
MEGA 2006
JUPITER 2008
0.63 (0.49-0.82) P<0.001P for heterogeneity 0.56ALL
Favors Statin Favors Placebo
(0.34-1.31)
(0.49-1.10)
(0.37-0.80)
21/498
56/2718
70/3375
14/499
40/2638
39/3426
RR 95% CI Placebo Statin
0.67
0.73
0.54
Year
13,154 Women; 240 CVD events
Mora S et al., Circulation 2010;121:1069
1. Reviewed current challenges for atherosclerotic cardiovascular disease (ASCVD) prevention, with a focus on the impact in women
2. Reviewed evidence on aspirin for the prevention of ASCVD
Secondary prevention
Primary prevention
Sex differences
Guideline recommendations
3. Reviewed evidence on statins for the prevention of ASCVD
Topics discussed

9/29/2015
11
Thank you!
Ongoing aspirin trials
Depta JP and Bhatt DL CCJM 2015;82:91-96