obesity and diabetes - future management · 75 drugs currently licensed for reducing hba1c int2dm...
TRANSCRIPT

Obesity and Diabetes -
Future Management
Professor Mike LeanHuman Nutrition University of Glasgow and Otago
Edinburgh 12th September 2016
Disclosures:
• Research/conference support and advisory boards:
(Novo Nordisk, Orexigen, Janssen, Cambridge Weight Plan)
• Medical consultancy for Counterweight Ltd
• I have never tasted Coca Cola, Pepsi or any other cola
• I have never owned a TV
• I have bought shares costing £10 in Eat Balanced Ltd


Proportions of UK overweight (BMI>25) adults
with and without ‘obesity-related’ diseases
Comorbidities: Diabetes, Hypertension, Stroke, Angina, MI.
Vlassopoulos, Combet & Lean 2014, ICO in KL
Data from the SHS (2008-11) n=24,831


Life expectancy with obesity:
BMI 30-35: reduced 2-4 years
BMI 40-50: reduced 8-10 years
Prospective Studies Collaboration (Whitlock et al)
Lancet 2009 (cf, Fontaine et al 2003)
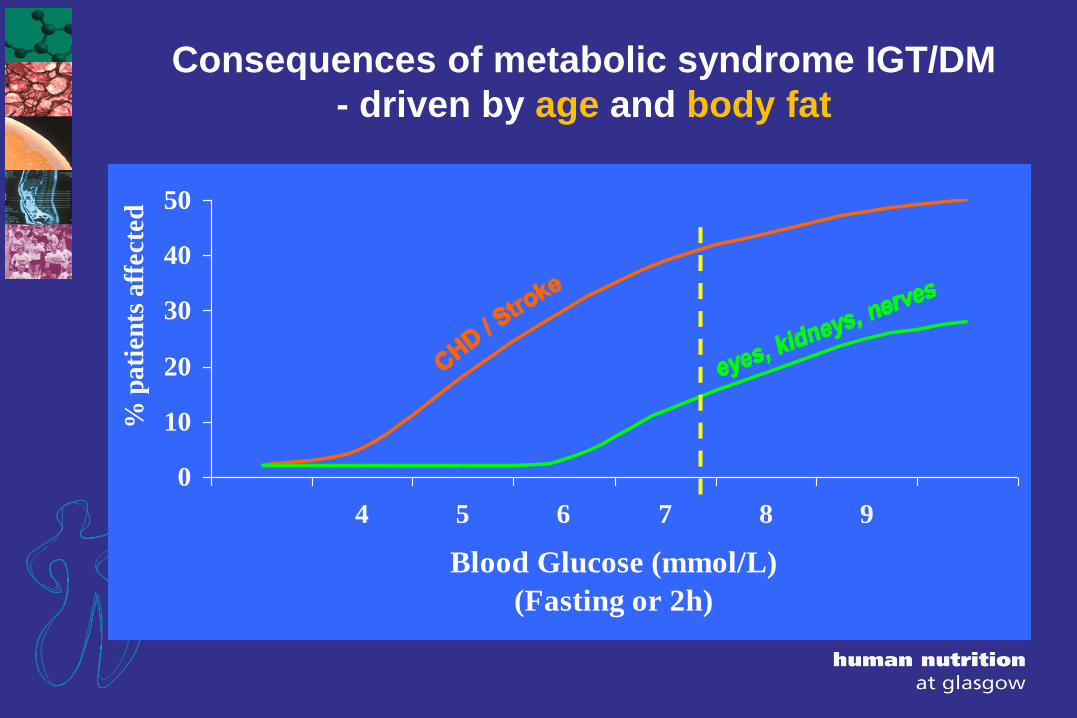
Consequences of metabolic syndrome IGT/DM
- driven by age and body fat
0
10
20
30
40
50
4 5 6 7 8 9
Blood Glucose (mmol/L)
(Fasting or 2h)
% p
ati
en
ts a
ffecte
d
Current management priorities for
Metabolic Syndrome/T2DM
1. Reduce HbA1c
2. Delay vascular complications
3. Arrest the underlying disease process
– Prevention
– Remission from diabetes
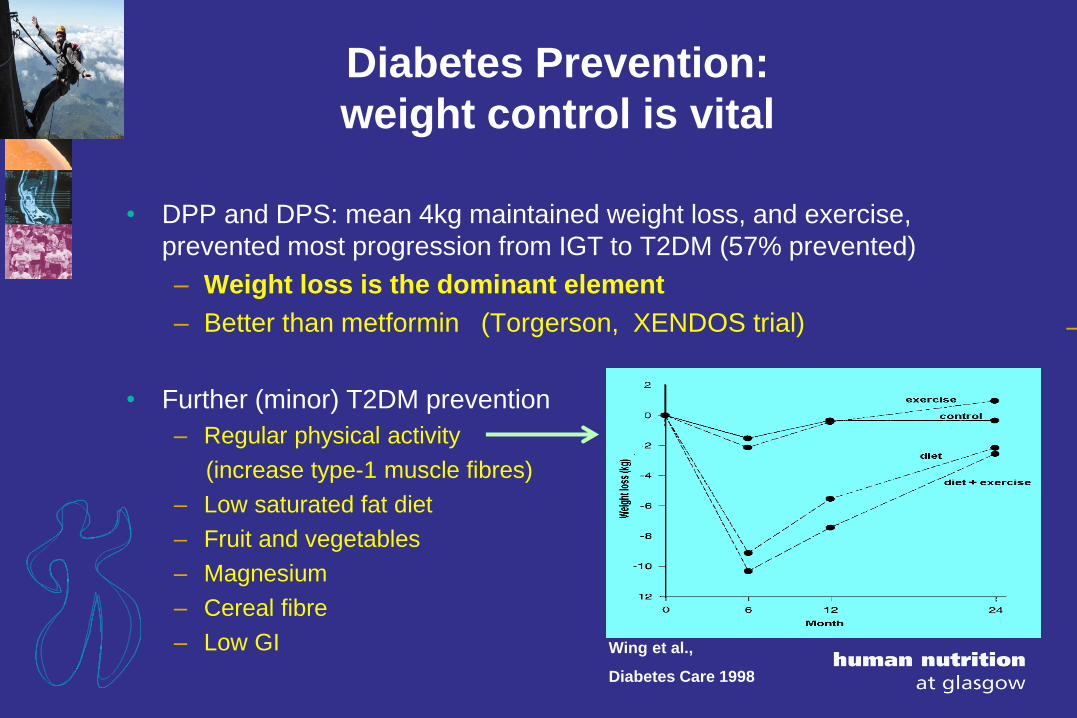
Diabetes Prevention:
weight control is vital
• DPP and DPS: mean 4kg maintained weight loss, and exercise,
prevented most progression from IGT to T2DM (57% prevented)
– Weight loss is the dominant element
– Better than metformin (Torgerson, XENDOS trial)
• Further (minor) T2DM prevention
– Regular physical activity
(increase type-1 muscle fibres)
– Low saturated fat diet
– Fruit and vegetables
– Magnesium
– Cereal fibre
– Low GI Wing et al.,
Diabetes Care 1998
–

Diabetes Prevention:
weight control is vital
• DPP and DPS: mean 4kg maintained weight loss, and exercise,
prevented most progression from IGT to T2DM (57% prevented)
– Better than metformin
– Weight loss is the dominant element (Torgerson, XENDOS trial)
• Further (minor) T2DM prevention
– Regular physical activity
– (increase type-1 muscle fibres)
– Low saturated fat diet
– Fruit and vegetables
– Magnesium
– Cereal fibre
– Low GI Wing et al.,
Diabetes Care 1998

75 drugs currently licensed for reducing HbA1c inT2DM (with multiple trade names)
(plus 25 in the licensing pipeline)
(plus countless more in development)
Alpha-Glucosidase Inhibitors:
acarbose
miglitol
Biguanides
metformin
metformin-alogliptin
metformin-canagliflozin
metformin-glipizide
metformin-glyburide
metformin-linagliptin
metformin-pioglitazone
metformin-repaglinide
metformin-saxagliptin
metformin-sitagliptin
Dopamine Agonist
bromocriptine
DPP-4 Inhibitors
alogliptin
alogliptin and pioglitazone
linagliptin
saxagliptin
sitagliptin
sitagliptin and simvastatin
Glucagon-Like Peptides
albiglutide
dulaglutide
exenatide
liraglutide
Meglitinides
nateglinide
repaglinide
SGLT2 Inhibitors 40 listeddapagliflozin
canagliflozin
empagliflozin
Sulfonylureas
glimepiride
glimepiride and pioglitazone
glimeperide and rosiglitazone
gliclazide
glipizide
glyburide
chlorpropamide
tolazamide
tolbutamide
Thiazolidinediones
rosiglitazone
pioglitazone

SIGN 115 Obesity (2010)
Dietary interventions in adults
• Calculated to produce a 600 kcal/day deficit
• Tailored to the dietary preferences of the individual
• Emphasise achievable and sustainable healthy eating
• Very Low Calorie Diets for rapid weight loss, under medical supervision
Drugs
• Orlistat should be considered as an adjunct to lifestyle interventions
Surgery
• BMI ≥35 kg/mƒƒ2 & severe comorbidities expected to improve ƒƒsignificantly
with weight reduction (eg severe mobility problems, arthritis, T2 diabetes).
• AND completion of a structured weight management programme involving
diet, ƒƒphysical activity, psychological and drug interventions,
without significant and sustained improvement in the comorbidities.
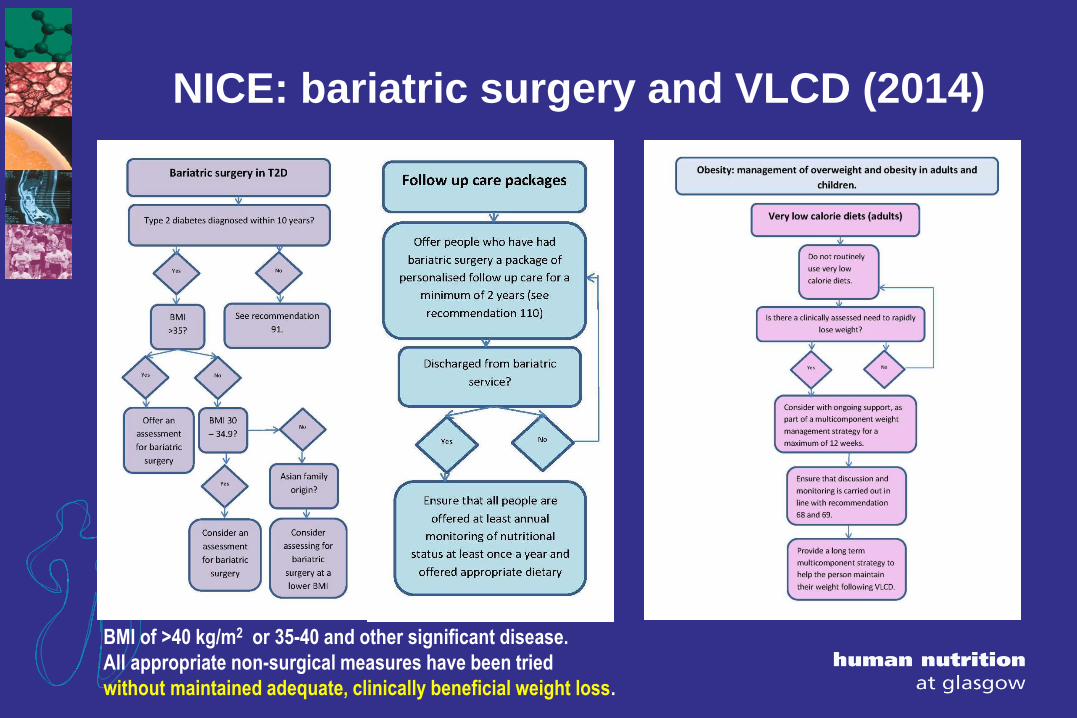
NICE: bariatric surgery and VLCD (2014)
BMI of >40 kg/m2 or 35-40 and other significant disease.
All appropriate non-surgical measures have been tried
without maintained adequate, clinically beneficial weight loss.
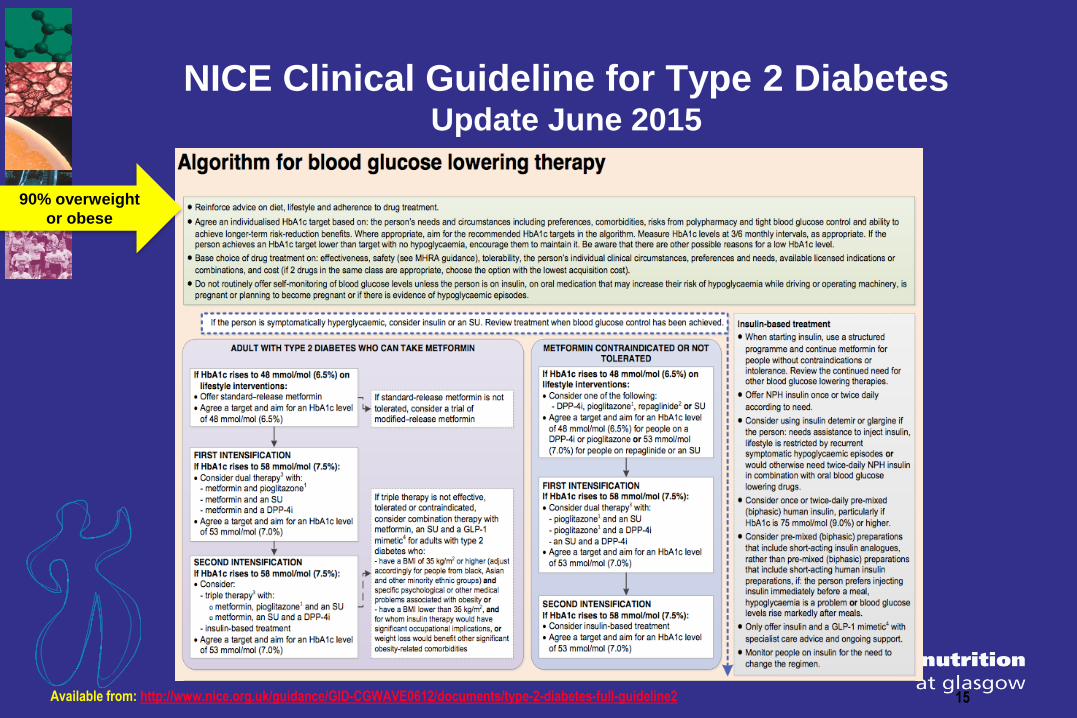
NICE Clinical Guideline for Type 2 Diabetes Update June 2015
15Available from: http://www.nice.org.uk/guidance/GID-CGWAVE0612/documents/type-2-diabetes-full-guideline2
90% overweight
or obese

Life-expectancy is still reduced 6-10 years by T2DM,
despite all our drug treatments (Wirral)
Nwaneri et al Postgrad Med J 2012)

Once you have T2 Diabetes…….
Treatment aims:
• To reduce HbA1c
• ?To reduce vascular complications
• ??To arrest the underlying disease process
– (Remission from diabetes)

Multiple clinical benefits from major weight loss4 y after laparoscopic adjustable gastric banding
0
20
40
60
80
100
120
Hyperte
nsion
Sleep a
pnoea
Dyspnoea
General p
hysica
l act
ivity
Self
esteem
Diabete
s
Perip
heral O
edema
Join
t pain
Reflux
Improved
Cured
Frigg et al. Obes Surg, 2004
T2DM ‘cured’
in 75%
T2DM ‘resolved’ in 78%
N=4070, mean age 40, BMI 48,
Systematic review and
meta-analysis
Buchwald et al Am J Med, 2009


• “....since my surgery I felt that ‘I wanna die’ feeling..... It was
HORRIBLE...”
• “If I eat too many carbs at one time, I get so tired immediately
after and almost feel drunk and may even slur my words”
• Treating Dumping syndrome: Acarbose, Octreotide.....
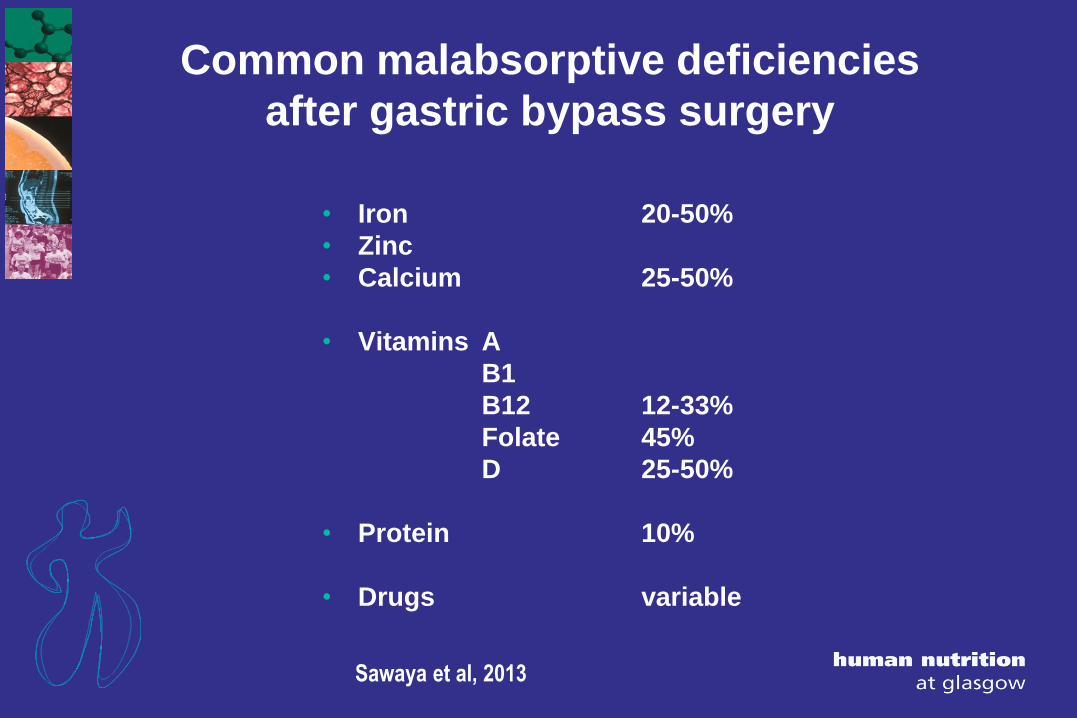
Common malabsorptive deficiencies
after gastric bypass surgery
• Iron 20-50%
• Zinc
• Calcium 25-50%
• Vitamins A
B1
B12 12-33%
Folate 45%
D 25-50%
• Protein 10%
• Drugs variable
Sawaya et al, 2013

weight loss interventions should be targeted to improving these comorbidities; in many individuals a greater than 15-20kg weight loss (will always be over 10%) will be required to obtain a sustained improvement in comorbidity”.
The new epidemic: Severe and complicated obesity
SIGN 115: Management of Obesity 2010

weight loss interventions should be targeted to improving these comorbidities; in many individuals a greater than 15-20kg weight loss (will always be over 10%) will be required to obtain a sustained improvement in comorbidity”.
The new epidemic: Severe and complicated obesity
SIGN 115: Management of Obesity 2010
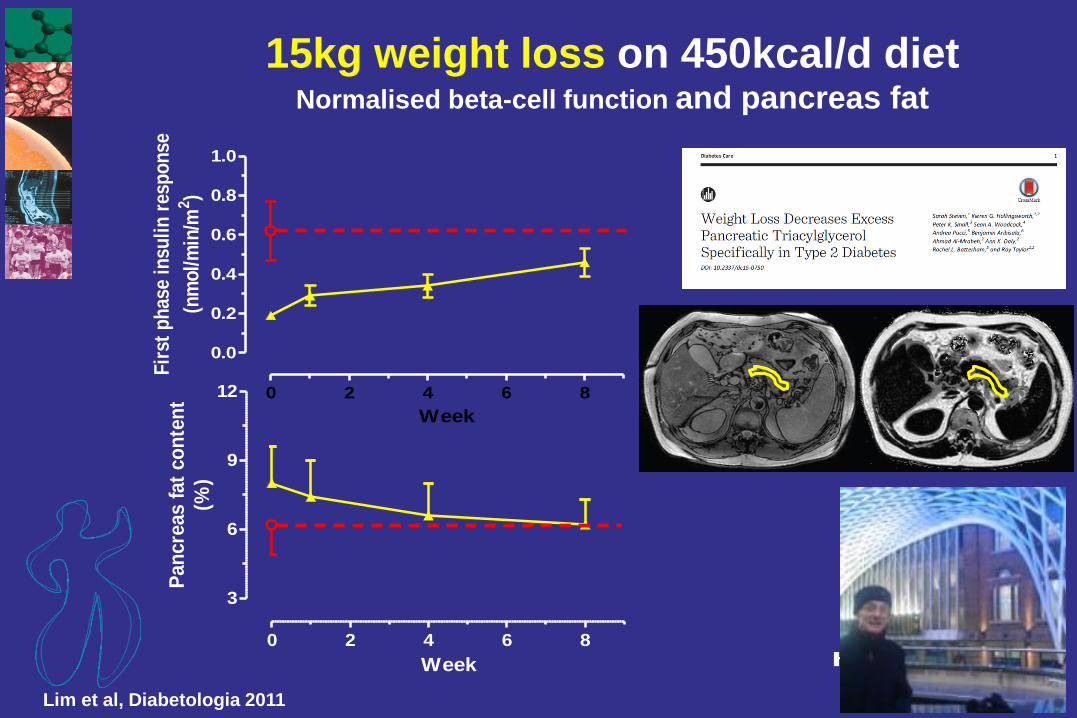
0 2 4 6 8
0.0
0.2
0.4
0.6
0.8
1.0
Week
Fir
st p
has
e in
suli
n r
esp
on
se
(nm
ol/
min
/m2)
0 2 4 6 8
3
6
9
12
Week
Pan
cre
as f
at
co
nte
nt
(%)
Lim et al, Diabetologia 2011
15kg weight loss on 450kcal/d dietNormalised beta-cell function and pancreas fat

15kg intentional loss might
normalise life expectancy
18
16
14
12
10
8
0
0 2 4 6 8 10 12 14
Weight loss (kg) in first 12 months
Lean et al. Diabetic Medicine, 1990
95% CI
↑ 95% CI
meanNormalise life expectancy
15 kgloss?
Life expectancy(mean age 64
at diagnosis)

Meta-analysis of non-surgical trials with 1-year follow-up:
BEST RESULTS WITH MOST RAPID WEIGHT LOSS
Average weight loss in subjects completing 1-year
80 studies, n = 26,455, completers =18,199 (69%) (Franz et al JADA 2007)
15 kg
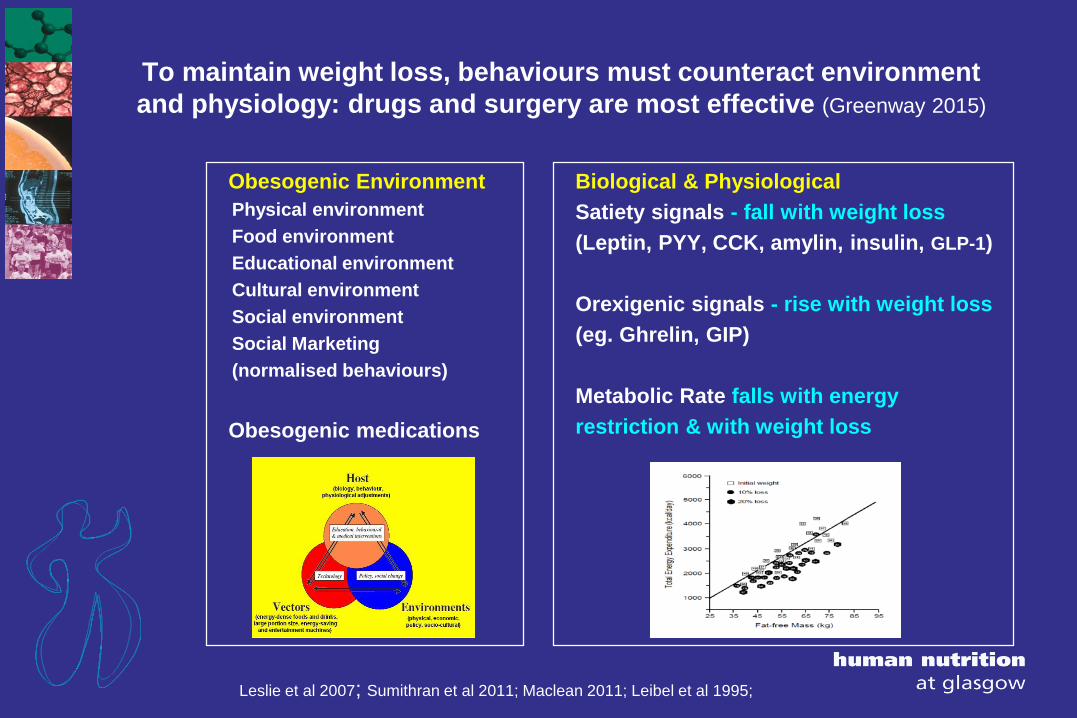
To maintain weight loss, behaviours must counteract environment
and physiology: drugs and surgery are most effective (Greenway 2015)
Obesogenic Environment
Physical environment
Food environment
Educational environment
Cultural environment
Social environment
Social Marketing
(normalised behaviours)
Obesogenic medications
Biological & Physiological
Satiety signals - fall with weight loss
(Leptin, PYY, CCK, amylin, insulin, GLP-1)
Orexigenic signals - rise with weight loss
(eg. Ghrelin, GIP)
Metabolic Rate falls with energy
restriction & with weight loss
Leslie et al 2007; Sumithran et al 2011; Maclean 2011; Leibel et al 1995;

Increasing awareness of Behavioural Therapy:
SIGN 2010 Diabetes Guidelines
• 3 pages out of 21 on Diet/Lifestyle, before drug treatment.
– improves self-management, metabolic and psychological outcomes
• Intensive, frequent contact with trained professionals
• Telephone contact, computer-assisted programmes
• Theory-based psychological interventions, motivational interviews
• Structured education curriculum, evidence-based, underpinning
philosophy, specific aims and learning objectives
• Quality-assured, independent audit assessment vs. predefined criteria
Similar emphasis is needed for obesity treatment more generally


Medical weight loss in primary care for overweight &
obese non-diabetic reduces all risk factors at 1-2 years (Naude et al meta-analysis 2014)

Weight loss maintenance programmes after VLCD/TDR:
a meta-analysis of RCTs (Johansson et al 2014)
Thin lines = control
Thick lines = intervention

Copenhagen Weight Loss in Knee Osteoarthritis trial:
more liberal TDR allowed more patients to do well
Little difference in weight loss
415kcal VLED vs. 810kcal LED
0 – 8 weeks
■ 810kcal/d liquid formula
▲ 415kcal/d liquid formula
16 – 68 weeks
■ (D) 1500kcal/d part food/part formula [average one formula meal daily]
♦ (E) Knee exercises group
● (C) Control – no intervention
88.0
90.0
92.0
94.0
96.0
98.0
100.0
102.0
104.0
106.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Time (weeks)
Bo
dy
Wei
gh
t (k
g)
n=96 per group n=64 per group
8-16 weeks 1200kcal
Part food/part formula
2 meals /day
)
D = structured food/formula maintenance
programme (No anti-obesity drug)
(Bliddal et al, secondary care, dietitian managed)

Counterweight-Plus - Protocol
Nutritionally complete
Total Diet Replacement (TDR)
• Homemade (811calories/day)
• Commercial (832calories/day)
• Cambridge Weight Plan
Plus:
• Structured patient education
– Step down approach optional
• >2.25l fluid per day (4 pints)
• Fibre supplement
Screening
TDR Stage
Food Reintroduction
Weight Loss Maintenance
Lean et al , Br J GP (2013)

Weight Loss Maintenance- Protocol
Stepped Food Reintroduction
• Introduce one 360-400 kcal meal
• Add a meal every two weeks
• Meals based on eatwell plate
• Offer Orlistat
Maintenance
• Low fat diet (30% fat)
• Estimate 500 kcal/d deficit
• 2500 kcal/d upper limit
Relapse Management
- Offer orlistat
- Second attempt LELD stage
Screening
TDR Stage
Food Reintroduction
Weight Loss Maintenance
Lean et al , Br J GP (2013)

Behavioural Strategies –
Weight Loss Maintenance
All Appointments for 12-24 months:
Review of outcome goals
Weight Tracker
- Provide feedback on performance
Rewards
- For effort or progress towards behaviour
Preventing Relapse
- Self talk- cognitive restructuring
Maintaining Change
-Provide normative information about the
-behaviours of others

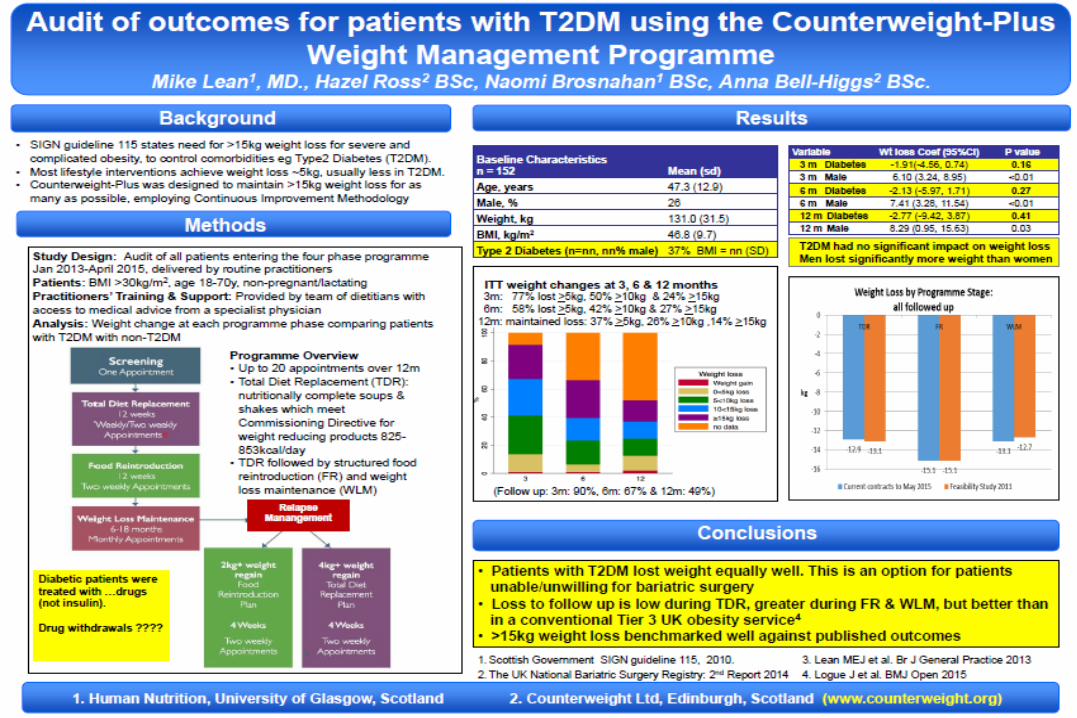
Counterweight-Plus feasibility study
in severe obesity (n = 91, mean BMI 47) (820kcal Total Diet Replacement, Food Reintroduction and Maintenance)
-60
-40
-20
0
20
10
-10
-30
0 100 200 300 400 500
Days
Wei
gtht
Cha
nge
(kg)
Lean et al , Br J General Practice (2013)

Popular Belief: Patients regain all the weight, or more
-60
-40
-20
0
20
10
-10
-30
0 100 200 300 400 500
Days
Wei
gtht
Cha
nge
(kg)
Lean et al , Br J General Practice (2013)
25%
25%
50%
In Fact:
• 25% fail to engage at all
– Lose <5kg (yet claim to be adhering to programme)
• 50% follow some or most of the programme
– Achieve and maintain 5-20kg weight loss
)
• 25% adhere fully
– Lose and maintain >20kg weight loss
Maintaining weight loss ≥15kg at 12 months:
• 33% of all 91 patients
• 44% of patients with a known 12-month weight
• 57% of those who lost >15kg on LELD
Highly cost-effective:
• 4 times more lose >15kg as with bariatric surgery

Efficiency of Obesity treatmentCost-effectiveness: Per £1 million NHS spend:
Lap Band surgery, complications and follow up @ £7,500
• 133 patients can be treated: 80% achieve >15kg 12m weight loss
• >15kg loss for 106 patients
Counterweight-Plus TDR & Maintenance programme @ £811
• 1161 patients can be treated: 30% achieve >15kg 12m weight loss
• >15kg loss for 383 patients
plus >10kg loss for 459 patients
Lean et al , Br J General Practice (2013)

2013-2018funded by DiABETES UK
to Mike Lean and Roy Taylor
• Cluster-Randomised Trial: Counterweight-Plus* 810kcal/d LELD
and weight maintenance programme vs usual care
– Both arms follow current clinical guidelines
– 280 patients, BMI >27, diagnosed T2DM <6 years, not on insulin
• Co-primary endpoints: weight loss >15kg and non-diabetic HbA1c
– at 12 & 24 months off all drugs (plus life-long clinical monitoring)
• Mechanistic and Magnetic Resonance studies
• Qualitative and process evaluation
• Planned economic analyses
* Supported by Cambridge Weight Plan
Obesity Crisis Solutions:Ethics of treatments for obesity and type 2 diabetes
• No drug should be prescribed without providing trained
professional support, for an optimal diet and lifestyle
change programme
• No clinical trial should be permitted unless an optimal
diet and lifestyle change programme is provided, to both
intervention and placebo arms

Epidemic!*
Medical Responsibility
Optimal medical care
within available resources
• Diet & lifestyle
• Drugs
• Surgery
• Palliative
Political Responsibility
Government interventions to remove
primary causes
• Catering outlets increasing
• Meals/snacks outside home increasing
• Portion sizes increasing
• Physical inactivity……
* WHO: ‘Critical Threshold for Intervention’

Health by Stealth: Eat Balanced pizzas now
reach 32,000 Scottish children every week
PIZZA POWER KIDS by Eat Balanced
now in Primary Schools in:
• East Renfrewshire
• Moray
• Argyle and Bute
• Aberdeen City
• South Ayrshire
Trials in another 10 councils:
• Fife
• East Ayrshire
• North Ayrshire
• Clackmannanshire
• Edinburgh City
• Glasgow City
• Highland
• Tayside (includes Dundee, Perth &
Kinross, Angus)

9-month weight changes in 20,975 young adults randomised to an on-line public health intervention
Nikolaou, Hankey & Lean, Obesity 2015
Control Group
n = 2,134
‘Rational Model’
(NTICV)
n = 1,810
‘Stealth Model’
(GD)
n = 2,057

Future: Address body fat or adipose
tissue mass (not BMI)
Best R2 vs MRI
(total body fat)
R2 (m/f)
Algindan et al MRI
validation study (total
adipose tissue)
BMI 0.66-0.95 0.66/0.82
Waist 0.77-0.94 0.77/0.78
Body fat equation
(Algindan et al 2015)
0.76-0.84 0.82/0.89
DEXA 0.8-0.95 -
BIA massive
variability
-
Algindan, Hankey, Govan , Gallagher, Heymsfield, Lean
Br J Nutrition 2015
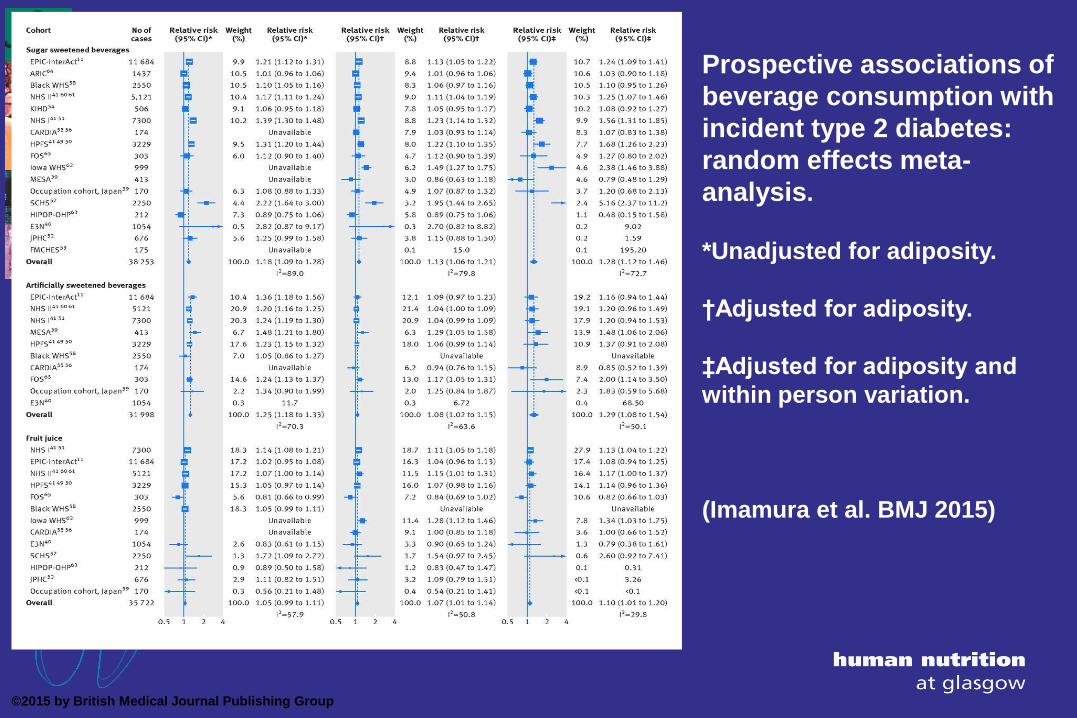
Prospective associations of
beverage consumption with
incident type 2 diabetes:
random effects meta-
analysis.
*Unadjusted for adiposity.
†Adjusted for adiposity.
‡Adjusted for adiposity and
within person variation.
(Imamura et al. BMJ 2015)
©2015 by British Medical Journal Publishing Group

Romaguera-Bosch et al. Diabetologia 56:1520, 2013
SSBs and BMI-adjusted risk of diabetes in
EPIC-Interact (Europe)

Future management: Conclusions
• Measure and deal with excess body fat, not BMI
• Direct major resources for research and routine management of
obesity, not its complications
• Target an amount of weight loss relevant to obese people and their
medical needs, not statistics
• Tackle the real problem faced by patients ie weight-loss maintenance,
not weight loss
• Provide optimal non-surgical weight-management routinely, and
accept that not all will succeed (they may not do well with surgery either)
• End manipulation of consumers, with damage to health, for profit

