oab made simple for the primary care provider (pcp): how...
TRANSCRIPT

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 1
Emerging Challenges In Primary Care: 2014
!
Faculty
OAB Made Simple for the Primary Care Provider (PCP):
How to Identify, When to Treat and When to
Refer
Matt T. Rosenberg, MD Medical Director of Mid-Michigan Health Centers
Jackson, MI Section Editor of
Urology, International Journal of Clinical
Practice
Louis Kuritzky, MD Clinical Assistant
Professor Department of
Community Health & Family Medicine
University of Florida Gainesville, FL
Pamela Ellsworth, MD Professor of Urology
Department of Urology UMass Memorial Medical
Center/University of Massachusetts Medical
School Worcester, MA
² Pamela Ellsworth, MD - Speaker/Advisory Board – Pfizer, Allergan - Advisory Board – Astellas
² Louis Kuritzky, MD - No relevant relationships to disclose
² Matt T. Rosenberg, MD - Speaker/Consultant – Astellas, Horizon, Pfizer - Speaker – Forest, Ortho-McNeil - Consultant – Easai, Ferring, Lilly, Bayer
FACULTY DISCLOSURES
2

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 2
LEARNING OBJECTIVES
After participating in this educational activity, clinicians should be better able to:
1. Recognize the role of simple questioning for identifying patients with overactive bladder (OAB)
2. Discuss the essential components of the evaluation of the patient with OAB symptoms
3. Develop a management plan for patients with OAB that emphasizes the incorporation of behavioral therapy and setting appropriate expectations, optimizes efficacy and minimizes side effects to improve patient compliance and adherence with pharmacologic therapy
4. Describe the role of recently approved second line therapies, third line therapies and future therapies in patients with OAB who are unsatisfied with antimuscarinic therapy 3
On a scale of 1 to 5, please rate how confident you would be in the diagnosis and management
of a patient with OAB.
1. Not at all confident 2. Slightly confident 3. Moderately confident 4. Pretty much confident 5. Very confident
4
PRE-TEST QUESTION 1

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 3
1. OAB is less prevalent than chronic sinusitis 2. An 80 year old patient should know that it is normal
to get up several times per night to empty their bladder
3. At least 50% of symptomatic patients are offered medical treatment for their symptoms of OAB
4. Understanding volume voided is a helpful point of distinction when evaluating LUTS symptoms for OAB
PRE-TEST QUESTION 2
Mary is a 80 year old patient who admits during her yearly exam that she wears a diaper “just in case” she can’t make it to the bathroom in time. Which of
the following is true regarding OAB?
5
When you tell Mary she may have OAB, she asks about the evaluation. Which is test is not
recommended by the AUA in the initial evaluation of OAB in the uncomplicated patient?
1. Urinalysis 2. Bladder ultrasound 3. Voiding diary 4. Genital exam
PRE-TEST QUESTION 3
6

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 4
After an appropriate evaluation you discuss treatment options with Mary. Which of the following statements regarding
expectations of OAB therapy is false?
1. It is appropriate to tell the patient that urinary urgency may be reduced with the correct therapy
2. It may take titration or changes in the pharmacologic therapy before an adequate response in attained
3. Therapeutic efficacy is enhanced with the combination of behavioral therapy and pharmacologic therapy as opposed to either alone
4. The risk of urinary retention in the male increases with longer duration on pharmacologic therapy for OAB
PRE-TEST QUESTION 4
7
Mary is very interested in efficacy but wants to limit side effects. Which of the following is true regarding OAB
pharmacologic therapy with either an antimuscarinic or a beta 3 adenergic agonist?
1. Both classes have a high rate of dry mouth 2. The efficacy of the antimuscarinic medications are higher
than the beta 3 adrenergic agonist medication 3. The efficacy of the beta 3 adrenergic agonist medication is
higher than the antimuscarinic medication 4. One agent blocks contraction while the other stimulates
relaxation
PRE-TEST QUESTION 5
8

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 5
DEFINITION OF OAB
OAB is syndrome or symptom complex defined as: “Urgency, with or without urgency incontinence, usually with frequency and nocturia”
Urgency is the key symptom of OAB
Urgency is defined as “a sudden compelling desire to void, which is difficult to defer”
Abrams P, et al. Urology. 2003;61:37-49. Rosenberg MT, et al. Int J Clin Pract. 2007;61:1535-1546. 9
PREVALENCE OF OAB SYMPTOMS
Coyne S, et al. Urology. 2011;77:1081-1087.
1 in 3 US adults ≥40 years of age reported symptoms of OAB at least “sometimes”
Age (years)
Resp
onde
nts
(%)
10

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 6
Stewart WF, et al. World J Urol. 2003;20(6):327-336. Pleis JR, Coles R. Summary health statistics for U.S. adults: National Health Interview Survey, 1998. Vital Health Stat 10. 2002;209:1-113. Centers for Disease Control and Prevention/National Center for Health Statistics. Vital and Health Statistics. Hyattsville, MD: U.S. Department of Health and Human Services; 1997. DHHS Publication No. (PHS) 97-1522. «http://www.cdc.gov/nchs/data/series/sr_10/sr10_194.pdf».
Overactive Bladder Chronic Sinusitis
Arthritic Symptoms
Hay Fever/Allergic Rhinitis Heart Disease
Asthma
Chronic Bronchitis Diabetes
Ulcer
0 10 20 30 40Millions
OAB & OTHER DISORDERS
11
To cope with symptoms of OAB, many patients
employ elaborate behaviors aimed at hiding and managing urine loss
Rosenberg MT. Curr Urol Rep. 2008. Abrams et al. Am J Manag Care. 2000 Jul;6(11 Suppl):S580-S590. Ricci JA, et al. Clin Ther. 2001;23:1245-1259.
Restrict fluid intake
Carry extra clothes in case of wetting accident
Try to urinate on a schedule
Bathroom mapping
Wear dark, baggy clothes to hide wet
spots or wear diapers
Use diapers or other
absorbent products
COPING STRATEGIES
12
OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 7
² 33.3 million US adults are said to have OAB ² Less than 50% will discuss with healthcare
provider ² Only a minority will be diagnosed and offered
treatment ² A smaller proportion will stay on therapy
Stewart WF et al. World J Urol. 2003;20:327-336. Rovner E, Wein A. Curr Urol Rep. 2002;3:434-438. Milsom I et al. BJU Int. 2001;87:760-766. Benner J et al. J Urol. 2009;181:2591-2598. Rosenberg M et al. Cleve Clinic J Med. 2007;74:S21-S29. Goepel M et al. Eur Urol. 2002;41:234-239. Dmochowski RR et al. Curr Med Res Opin. 2007;23:65-76.
OAB IS PREVALENT, UNDIAGNOSED AND UNDERTREATED
13
The Reality is We Can Do Better in the Identification
and Treatment of OAB
14

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 8
The answer is education and communication
Unfortunately, if we don’t understand the disease, we may not identify it
even to refer, let alone treat!!!!!!
WHY IS OAB UNDERDIAGNOSED AND UNDERTREATED?
15
Rosenberg MT. Curr Urol Rep. 2008;9:428-432.Yu YF, et al. Value Health. 2005;8:495-505.
IDENTIFYING OAB TAKES A VILLAGE
16

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 9
PATIENTS DON’T DISCUSS BLADDER ISSUES WITH THE PROVIDER
² Embarrassment ² Fear of invasive procedures or need for
surgery ² Perception of lack of available and effective
treatment
Ricci JA, et al. Clin Ther 2001;23:1245–1259. Milsom I, et al. BJU Int 2001;87:760–766. 17
² I have had this problem and did not know who to talk to
² My previous doctor told me it was part of aging
² It became a problem only when my diaper overflowed
² I thought it was normal as my sister and mother had this
² You mean going to the bathroom every hour is not normal?
² I am too embarrassed
MacDiarmid S, Rosenberg, M. Curr Med Res Opin. 2005; 21:1413-1421.
WHAT DO PATIENTS SAY?
18

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 10
THE UROLOGIST AND THE UROGYNECOLOGIST ROLE IN THE PARTNERSHIP
² Identification and initial evaluation of OAB starts in the office of the PCP
² There is a significant amount of medically related LUTS
² The diagnosis of OAB does not require an extensive or complicated evaluation
Stewart WF, et al. World J Urol. 2003;20:327-336. Darkov T, et al. Pharmacotherapy. 2005;25:511-519. Ailinger RL, et al. J Comm Health Nurs. 2005;22:135-142. Rosenberg M et al. Cleve Clinic J Med. 2007;74:S21-S29. 19
POTENTIAL MISCONCEPTIONS IN OAB
² OAB is a natural part of aging ² Diagnosis and treatment of genitourinary
disease is to be determined by a specialist
² Diagnosis and treatment is outside the realm of the PCP setting
MacDiarmid S, Rosenberg, M. Curr Med Res Opin. 2005;21(9):1413-1421. 20

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 11
WHAT DO DOCTORS SAY?
² No time ² Treatments are not all that effective ² If it was a problem for the patient, he or she
would bring it up ² Your bladder/penis/kidney won’t kill you, your
heart will, so I need to focus
MacDiarmid S, Rosenberg, M. Curr Med Res Opin. 2005;21(9):1413-1421. 21
NOT SO! ² What is the outcome of an elderly patient
falling and breaking a extremity?
² What is one of the primary drivers for nursing home admission?
Brown et al. J Am Geriatr Soc. 2000;48:721-725. 22

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 12
Current Thinking Is a Myth
23
REALITIES OF OAB MANAGEMENT
² The PCP is the first line of contact ² Diagnosis and treatment is within the realm of
the PCP setting
² Current treatments offer significant improvement of patient symptoms and patient quality of life
24

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 13
What we have here is a
failure to communicate. Initially stated by the Warden in Cool Hand Luke
repeated by Jackie Gleason in Smokey and the Bandit And now just shamelessly used by me for lecturing amusement
25
WHAT DOES THE PCP NEED?
² Keep It Simple
26

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 14
WHAT DOES THE PCP NEED?
² Keep It Simple
² Keep It Effective
27
WHAT DOES THE PCP NEED?
² Keep It Simple
² Keep It Effective
² Keep Us From Harming Our Patients
28

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 15
IT ALL COMES DOWN TO “NORMAL”
² How many times a day does a normal person need to urinate?
² What is the normal volume of urine voided per micturition?
² Is it normal for older people to get up during the night to use the bathroom?
29
What are the normal functions of the bladder?
30

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 16
² Normal Function - Storage capacity (300 – 500 ml of fluid)
• Adequate low pressure urinary storage (bladder) • Adequate outlet resistance (sphincter)
- Empty to completion (minimal residual) • Adequate bladder contraction • Absence of outlet obstruction
² Abnormal Function (failure to store or empty) - Voiding frequently small amounts - Uncontrollable urge (urgency) - Incomplete emptying - Hesitancy, poor stream Wein AJ. Pathophysiology and categorization of voiding dysfunction. In: Wein AJ, Kavoussi LR, Novick AC, et al, eds.
Campbell-Walsh Urology. 9th ed. Philadelphia, PA: W. B. Saunders/Elsevier; 2007:1973-1985.
FUNCTION OF THE BLADDER
31
What are the normal functions of the prostate?
32

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 17
² Normal Function - Does not grow (enlarge) into the urethra thereby
allowing unobstructed flow - It is intimately associated with the continence
mechanism - Produces fluid for seminal emission
² Abnormal Function (failure of flow) - Obstruction of urinary flow (“obstruction” “retention”) - Sphincteric damage /usually surgical - (“stress
incontinence”)
Wein AJ. Pathophysiology and categorization of voiding dysfunction. In: Wein AJ, Kavoussi LR, Novick AC, et al, eds. Campbell-Walsh Urology. 9th ed. Philadelphia, PA: W. B. Saunders/Elsevier; 2007:1973-1985.
FUNCTION OF THE PROSTATE
33
LOWER URINARY TRACT SYMPTOMS (LUTS): BLADDER OR PROSTATE?
Storage (bladder) Voiding (prostate) Urgency Hesitancy
Frequency Poor flow/weak stream Nocturia Intermittency
Urge incontinence Straining to void Stress incontinence Terminal dribble Mixed incontinence Prolonged urination
Overflow incontinence Urinary retention
Chapple CR, et al. Eur Urol. 2006;49:651-658. 34

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 18
It is all about VOLUME VOIDED
and FLOW
Rosenberg MT, et al. Int J Clin Pract. 2010; 64(4):488-496. 35
Guess What Happens When You Understand
What is Normal?
36

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 19
Guess What Happens When You Understand
What is Normal? ² Your patients will understand what is normal, and
subsequently, what is abnormal
37
Guess What Happens When You Understand
What is Normal? ² Your patients will understand what is normal, and
subsequently, what is abnormal ² You recognize when you have something to fix
38

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 20
Treat or Refer
LUTS
Focused HPE UA/PSA Blood Sugar
Desires Treatment?
Watchful Wai@ng
Treat for BPH Con@nue Meds
Assess and Treat OAB/SI
Con@nue Meds
Refer
Unlikely OAB/BPH/SI
Likely OAB/BPH/SI
No
Yes Provisional BPH Provisional OAB/SI
Effec@ve
Ineffec@ve
Effec@ve
Ineffec@ve
Modified from Rosenberg MT, Staskin DR, Kaplan SA, et al. Int J Clin Pract. 2007;61(9):1535-1546.
THE LUTS ALGORITHM Key:
LUTS – lower urinary tract symptoms HPE – history, physical examination UA – urinalysis PSA – prostate specific antigen BPH – benign prostatic hyperplasia OAB – overactive bladder SI – stress incontinence
39
DEFINING LUTS
Frequency • Patient considers that he/she voids too
often by day • Normal is < 8 times per 24 hours
Nocturia • Waking to urinate during sleep hours • Considered a clinical problem if
frequency is greater than twice a night
Urgency • Sudden compelling desire to pass urine that is difficult to defer
UUI • Involuntary leakage accompanied by, or immediately preceded by, urgency
OAB “Wet” • OAB with UUI
OAB “Dry” • OAB without UUI
Warning Time • Time from first sensation of urgency to voiding
Abrams P, et al. Neurourol Urodyn. 2002;21:167-78; Wein A, et al. J Urol. 2006;175:S5-10; Zinner N, et al. Int J Clin Pract. 2006;60:119-26; Wein AJ. Am J Manag Care. 2000;6:S559-64.
40

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 21
SIMPLE QUESTIONS THE PCP CAN ASK
Abrams P, et al. Neurourol Urodyn. 2002;21:167-78; Wein A, et al. J Urol. 2006;175:S5-10;Zinner N, et al. Int J Clin Pract. 2006;60:119-26; Wein AJ. Am J Manag Care. 2000;6:S559-64.
² Do you have a sudden urge to void and can barely make it to the bathroom?
² Do you wear a pad or diaper? ² Can you sit through a movie without going to
the bathroom? ² Do you leak urine? ² Do you get up at night?
41
THE EVALUATION OF LUTS
² Medical and surgical history ² Medications ² Focused physical examination ² Voiding diary ² Labs ² Urodynamics, cystoscopy, and diagnostic
renal and bladder ultrasound not necessary in initial workup of uncomplicated patients
42 Gormley EA, et al. American Urological Association (AUA) Guideline. AUA Web site. 2012. http://www.auanet.org/content/media/OAB_guideline.pdf. Accessed March 21, 2014.

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 22
EXAMPLES IN THE MEDICAL AND SURGICAL HISTORY THAT MAY CAUSE LUTS
² Diabetes (new onset or poorly controlled) - Causing polyuria/polydipsia
² Congestive heart failure - Nighttime fluid mobilization
² Recent Surgery - Catheterization during surgery, immobilization,
constipation from pain medications
A recent onset of the symptoms may provide a clue to the etiology
43
MEDICATIONS AS A CAUSE OF LUTS
Sedatives Confusion, secondary incontinence
Alcohol, Caffeine, Diuretics Diuresis
Anticholinergics Impair contractility, voiding difficulty, overflow incontinence
α – Agonists Increased outlet resistance, voiding difficulty
ß - Blockers Decreased urethral closure, stress incontinence
Calcium-Channel Blockers Reduce bladder smooth muscle contractility
ACE Inhibitors Induce cough, stress urinary incontinence
First generation antihistamines
Increase outlet resistance
Cholinesterase inhibitors Precipitate urge incontinence
Opioids Direct effect, constipation
Wyman JF, et al. Int I Clin Pract. 2009;63:1177-1191. Newman DK. Nurse Pract. 2009;34:33-45. 44

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 23
THE FOCUSED PHYSICAL EXAMINATION
² Abdominal – Tenderness, masses, distension
² Neurological – Mental and ambulatory status, neuromuscular function
² Genitourinary – Meatus and testis – Vaginal mucosal integrity, urethral mobility, bladder
prolapse ² Rectal
– Tone – Prostate size, shape, nodules and consistency
Rosenberg MT, Newman DK, Tallman CT, et al. Cleve Clin J Med. 2007;74(suppl 3):S21-S29. 45
LABORATORY TESTS
² Urinalysis – Infection, blood – The urine is not an adequate screener for diabetes since the blood
sugar must be above 180 mg/dl before it spills into the urine
² A random or fasting blood sugar – Diabetes
² Prostate specific antigen – Prostate specific not cancer specific but can be used in screening – Excellent as a surrogate marker for prostate size
§ PSA is more accurate than a DRE when estimating prostate size § A PSA of 1.5 ng/ml equates to a prostate volume of at least 30
grams(ml)
Rosenberg MT, Staskin DR, Kaplan SA, et al. Int J Clin Pract. 2007;61,9,1535-1546. Bosch J, et al. Eur Urol. 2004;46:753-759 Roerborn CG, et al. Urology. 1999;53;381-9. 46

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 24
THE PURPOSE OF THE VOIDING DIARY
² Identifies voiding frequency and voided volume ² Differentiates behavioral vs LUTS pathology
- Voiding frequently § excessive volume(behavioral) § small amounts as a result of always being in a rush (behavioral) § small amounts (OAB)
² Alerts patients to habits /opportunities to modify ² Can monitor effect of treatment
Wyman JF, et al. Int J Clin Pract. 2009; 63(8):1177-91 47
THE POST VOID RESIDUAL (PVR) IS ONLY NEEDED IN SELECT PATIENTS
² The fear of patients going into retention when treated for OAB leaves many patients untreated
² If PVR residual is less than 50 ml, causing retention when treating OAB is extremely unlikely - FACT: most PCPs will not have bladder scanner and will not
want to catheterize a patient - FACT: most PCPs will have access to a ultrasound unit and
can order a post void residual
² Use common sense, if you are treating the patient for voiding too frequently (OAB) and they have not voided in 6 – 8 hours or have a sense to void but cannot, have them contact you
Rosenberg MT. Curr Opin Urol. 2008;9(6):428-32. Rosenberg MT, Staskin DR, Kaplan SA, et al. Int J Clin Pract. 2007;61(9):1535-1546. 48

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 25
INDICATIONS FOR REFERRAL
² History of recurrent urinary tract infections or other infection
² Pelvic irradiation ² Microscopic or gross hematuria ² Prior genitourinary surgery ² Elevated prostate-specific antigen ² Abnormal genital exam ² Suspicion of neurological cause of symptoms ² Meatal stenosis ² History of genitourinary trauma ² Pelvic pain ² Uncertain diagnosis or patient choice
Rosenberg MT, Staskin DR, Kaplan SA, et al. Int J Clin Pract. 2007;61(9),1535-1546 49
TREATMENT NOW CAN BE EMPIRIC
² No identifiable etiology ² No reversible causes ² Is patient bothered enough for treatment?
- No, watchful waiting - Yes, consider algorithm
§ Weak flow – think Prostate § Poor voiding volumes – think Bladder § Incontinence – think Bladder/Outlet
Rosenberg MT. Cur Uro 2008;9:428–432. 50

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 26
Treat or Refer
LUTS
Focused HPE UA/PSA Blood Sugar
Desires Treatment?
Watchful Wai@ng
Treat for BPH Con@nue Meds
Assess and Treat OAB/SI
Con@nue Meds
Refer
Unlikely OAB/BPH/SI
Likely OAB/BPH/SI
No
Yes Provisional BPH Provisional OAB/SI
Effec@ve
Ineffec@ve
Effec@ve
Ineffec@ve
Modified from Rosenberg MT, Staskin DR, Kaplan SA, et al. Int J Clin Pract. 2007;61(9):1535-1546.
THE MALE (OR PROSTATE) DILEMMA
Key: LUTS – lower urinary tract symptoms HPE – history, physical examination UA – urinalysis PSA – prostate specific antigen BPH – benign prostatic hyperplasia OAB – overactive bladder SI – stress incontinence
51
TREATMENT GUIDELINES FOR OAB
Kirby M, et al. Int J Clin Pract. 2006;60:1263-1271.Burgio K, et al. J Am Geriatr Soc. 2000;48:370-374 .
² Behavioral treatment ² Pharmacologic management ² Referral for specialist management/surgery
52
Gormley EA, et al. American Urological Association (AUA) Guideline. AUA Web site. 2012. http://www.auanet.org/content/media/OAB_guideline.pdf. Accessed March 21, 2014.

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 27
BEHAVIORAL THERAPY FOR OAB
Behavioral Therapy for OAB
Bladder training
Educa:on reinforcement
Pelvic floor exercises
Biofeedback
Diaries
Timed voiding
Fluid/Dietary management
No matter what the treatment course, behavioral modification should be offered to every patient
Soda T, et al. J Urol. 2010; 184: 1000-1004 53
HABIT CHANGES: MANAGING BLADDER HEALTH
Technique
Lifestyle Modification
Diet, fluid, bowel, and weight management Smoking cessation
Timed/ Prompted Voiding
Urination at a fixed interval that avoids the symptom Useful for urgency and urinary incontinence not associated with frequency Good option in patients with cognitive impairment
Wyman JF, et al. Int J Clin Pract. 2009;63:1177-91. Wagg AS, et al. BJU Int. 2007;99:502-9. Lucas MG, et al. Eur Urol 2012;62(6):1130-42.
54

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 28
HOW TO PERFORM PELVIC FLOOR MUSCLE EXERCISES
² Explain location of perineal muscles (anal area)
² Contract perineal muscles, squeezing upward through the pelvis
² Sit or stand with your legs apart, don’t hold your breath ² Hold the contraction for 10 seconds, then gradually relax ² Repeat at least 5 times, increase to 30-40 per day in
groups of 10 ² Relaxation is as important as contraction for muscle
rehabilitation
² Use exercises to control symptoms - eg, during urge episode, not during urination
Harv Womens Health Watch. www.health.harvard.edu/newsletters/Harvard_Womens_Health_Watch/2011/ January/how-to-perform-kegel-exercises.
The exercises can be performed anywhere 55
–100
–80
–60
–40
–20
0
Mea
n R
educ
tion
in U
I, %
Behavioral Therapy
Combined Therapy
Drug Therapy
Combined Therapy
P < .05 P = .001
–57.5%
–88.5%
–72.7%
–84.3%
ADDITIVE EFFECT OF COMBINING BEHAVIORAL AND DRUG THERAPY
Burgio KL, et al. J Am Geriatr Soc. 2000;48:370-374. 56
OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 29
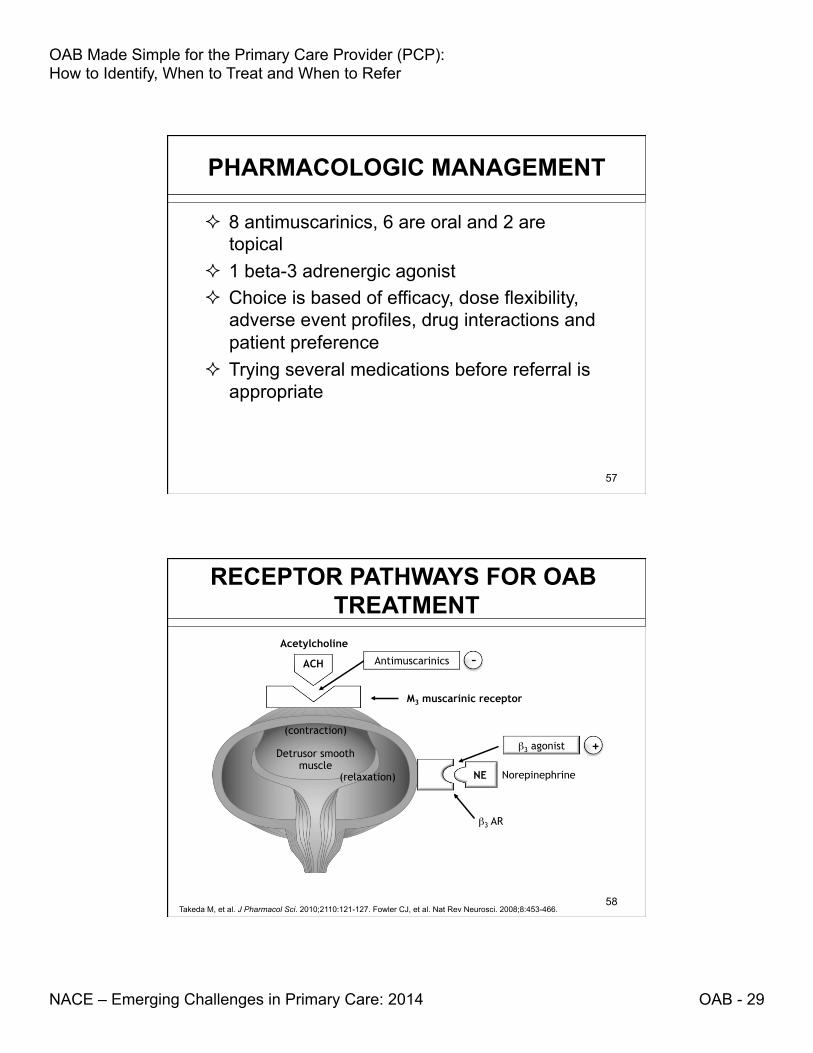
PHARMACOLOGIC MANAGEMENT
² 8 antimuscarinics, 6 are oral and 2 are topical
² 1 beta-3 adrenergic agonist ² Choice is based of efficacy, dose flexibility,
adverse event profiles, drug interactions and patient preference
² Trying several medications before referral is appropriate
57
Antimuscarinics ACH
NE
M3 muscarinic receptor
Detrusor smooth muscle
(relaxation) Norepinephrine
β3 AR
β3 agonist
–
+
Acetylcholine
(contraction)
RECEPTOR PATHWAYS FOR OAB TREATMENT
Takeda M, et al. J Pharmacol Sci. 2010;2110:121-127. Fowler CJ, et al. Nat Rev Neurosci. 2008;8:453-466. 58

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 30
ANTIMUSCARINICS – IMMEDIATE RELEASE
Drug Brand Name Dose Dosing Oxybutynin IR Ditropan 5 mg 1 – 3 times per
day Tolterodine IR Detrol 1 -2 mg Twice per day Trospium Chloride Sanctura 20 mg Twice per day
Physcians’ Desk Reference. 64st ed. Montvale, NJ: Thomson PDR; 2010. 59
ANTIMUSCARINICS – EXTENDED RELEASE extended release medications have a better tolerability than their
immediate release counterparts
Drug Brand Name Dose Dosing Darifenacin Enablex 7.5 mg, 15 mg Daily Fesoterodine Toviaz 4 mg, 8 mg Daily Oxybutynin ER Ditropan XL 5 – 30 mg Daily Oxybutynin TDS Oxytrol 3.9 mg Twice per week Oxybutynin 10% gel
Gelnique 100 mg Daily
Solifenacin Vesicare 5 mg, 10 mg Daily Tolterodine ER Detrol LA 2, 4mg Daily Trospium Chloride Sanctura XR 60 mg Daily
Physcians’ Desk Reference. 64st ed. Montvale, NJ: Thomson PDR; 2010. 60

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 31
COMMON SIDE EFFECTS OF ANTIMUSCARINICS
² Dry Mouth ² Constipation ² Headaches ² Blurred vision
Clinicians should manage constipation and dry mouth before abandoning effective antimuscarinic therapy. Balance of efficacy and tolerability should be considered and discussed with each patient.
Steers WD. Urol Clin North Am. 2006;33:475-482. Erdam N, et al. Am J. Med 2006;119(suppl 1):29-36. Gormley EA, et al. American Urological Association (AUA) Guideline. AUA Web site. 2012. http://www.auanet.org/content/media/OAB_guideline.pdf. Accessed March 21, 2014. 61
CONTRAINDICATIONS, WARNINGS AND PRECAUTIONS FOR ANTIMUSCARINICS
² Contraindications- - Urinary or gastric retention - Uncontrolled narrow-angle glaucoma
² Warnings & Precautions – - Angioedema of face, lips, tongue and/or larynx - Clinically significant bladder outlet obstruction - Decreased gastrointestinal motility - Treated narrow angle glaucoma - May have CNS effects i.e., somnolence - Use with caution in patients with myasthenia
gravis Physicians’ Desk Reference. 64st ed. Montvale, NJ: Thomson PDR; 2010. Oelke M, et al. Eur Urol. 2013;64(1):118-140. 62

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 32
BETA-3 ADRENERGIC AGENTS
Drug Brand Name Dose Dosing Mirabegron Myrbetriq 25 mg, 50 mg Daily
Myrbetriq™ (mirabegron) prescribing information, Astellas Pharma US, Inc. June 2012. 63
COMMON SIDE EFFECTS OF MIRABEGRON
² Hypertension ² Nasopharyngitis ² Urinary Tract Infections ² Headaches
Balance of efficacy and tolerability should be considered and discussed with each patient.
Myrbetriq™ (mirabegron) prescribing information, Astellas Pharma US, Inc. June 2012. 64

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 33
CONTRAINDICATIONS, WARNINGS AND PRECAUTIONS FOR MIRABEGRON
² Contraindications – NONE ² Precautions & Warnings –
- Not recommended for use in severe uncontrolled hypertensive patients
- Use with caution in patients with urinary retention or bladder outlet obstruction
- Use with caution in patients taking antimuscarinic drugs for overactive bladder
- Caution with use in patients taking drugs metabolized by CYP2D6 as mirabegron is a moderate inhibitor of CYP2D6
Myrbetriq™ (mirabegron) prescribing information, Astellas Pharma US, Inc. June 2012. 65
FOLLOW UP ON THE PATIENT TREATED FOR OAB
² Review the patient after 2 – 4 weeks - Be prepared to titrate as studies show > 50 % will
increase dose if given the option - Be prepared to try different agent or class
² Consider checking PVR to ensure volume not increasing significantly in the complex patient - Studies on medication usage in males show safety
and minimal increase in post void residual over time of follow up
- The risk of urinary retention (although low) is highest during the first 30 days of treatment
Chapple CG, Rosenberg MT, Brenes FJ. Brit J Urol. 2009;104(7):960-7. Rosenberg MT, Staskin DR, Kaplan SA, et al. Int J Clin Pract. 2007;61(9):1535-1546. Martin-Merino E, et al. J Urol. 2009; 182(4):1442-8. Rosenberg M, Newman DK, Tallman CT, et al. Cleve Clin J Med. 2007;74(suppl 3):S21-S29. Myrbetriq™ (mirabegron) prescribing information, Astellas Pharma US, Inc. June 2012. 66

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 34
HIGH DISCONTINUATION RATE FOR PATIENTS ON OAB THERAPY
*Cumulative incidence of discontinuation was determined using the Kaplan-Meier method.
Gopal M, et al. Obstet Gynecol. 2008;112:1311-1318.
Study Design: UK study. Overall drug discontinuation for all women prescribed anticholinergic medications (N=29,369). Unadjusted cumulative incidence of discontinuation (95% CI).
Months to Discontinuation
Dis
cont
inua
tion
Rat
e (%
) Fr
om
Ant
icho
liner
gics
for
OA
B (9
5% C
I)*
Adapted from Gopal et al.
67
IMPROVING PATIENT ADHERENCE BY ADDRESSING EXPECTATIONS
² Effects on urgency ² Limiting incontinence ² Decreasing nocturia ² Improved quality of life ² Tolerability of medication
Rosenberg MT. Cur Uro 2008, 9:428–432. DeCastro J, et al. Am J Med. 2008;121:S27-S33. 68

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 35
OPTIONS FOR THE UNSATISFIED PATIENT
² Sacral Nerve Stimulation ² Percutaneous Tibial Nerve Stimulation ² Onabotulinum Toxin A
Gormley EA, et al. American Urological Association (AUA) Guideline. AUA Web site. 2012. http://www.auanet.org/content/media/OAB_guideline.pdf. Accessed March 21, 2014
69
TAKE HOME MESSAGE
² Overactive bladder doesn’t take your life — it steals it from you
² The untreated 85% is in the PCP office ² OAB can be diagnosed and treated in the
primary care office efficiently, effectively and safely
70

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 36
• Be willing to discuss his/her symptoms
• Make recommended lifestyle changes
• Adhere to prescribed medication
• Diagnose OAB
• Set realistic patient expectations/goals • Provide initial treatment of OAB • Refer appropriate patients
• Treat refractory or complicated OAB • Educate PCPs to better manage OAB
Rosenberg MT. Curr Urol Rep. 2008;9:428-432.Yu YF, et al. Value Health. 2005;8:495-505.
TREATING OAB TAKES A VILLAGE
71
POST-TEST QUESTIONS
72

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 37
1. OAB is less prevalent than chronic sinusitis 2. An 80 year old patient should know that it is normal
to get up several times per night to empty their bladder
3. At least 50% of symptomatic patients are offered medical treatment for their symptoms of OAB
4. Understanding volume voided is a helpful point of distinction when evaluating LUTS symptoms for OAB
POST-TEST QUESTION 1
Mary is a 80 year old patient who admits during her yearly exam that she wears a diaper “just in case” she can’t make it to the bathroom in time. Which of
the following is true regarding OAB?
73
When you tell Mary she may have OAB, she asks about the evaluation. Which is test is not
recommended by the AUA in the initial evaluation of OAB in the uncomplicated patient?
1. Urinalysis 2. Bladder ultrasound 3. Voiding diary 4. Genital exam
POST-TEST QUESTION 2
74

OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 38
After an appropriate evaluation you discuss treatment options with Mary. Which of the following statements regarding
expectations of OAB therapy is false?
1. It is appropriate to tell the patient that urinary urgency may be reduced with the correct therapy
2. It may take titration or changes in the pharmacologic therapy before an adequate response in attained
3. Therapeutic efficacy is enhanced with the combination of behavioral therapy and pharmacologic therapy as opposed to either alone
4. The risk of urinary retention in the male increases with longer duration on pharmacologic therapy for OAB
POST-TEST QUESTION 3
75
Mary is very interested in efficacy but wants to limit side effects. Which of the following is true regarding OAB
pharmacologic therapy with either an antimuscarinic or a beta 3 adenergic agonist?
1. Both classes have a high rate of dry mouth 2. The efficacy of the antimuscarinic medications are higher
than the beta 3 adrenergic agonist medication 3. The efficacy of the beta 3 adrenergic agonist medication is
higher than the antimuscarinic medication 4. One agent blocks contraction while the other stimulates
relaxation
POST-TEST QUESTION 4
76
OAB Made Simple for the Primary Care Provider (PCP): How to Identify, When to Treat and When to Refer
NACE – Emerging Challenges in Primary Care: 2014 OAB - 39
On a scale of 1 to 5, please rate how confident you would be in the diagnosis and management
of a patient with OAB.
1. Not at all confident 2. Slightly confident 3. Moderately confident 4. Pretty much confident 5. Very confident
77
POST-TEST QUESTION 5
POST-TEST QUESTION 6 Which of the statements below describes your
approach to diagnosing and treating patients with OAB?
1. I do not diagnose or treat patients with OAB, nor do I plan to this year.
2. I did not diagnose or treat patients with OAB before this course, but as a result of attending this course I’m thinking of managing them now.
3. I do diagnose and treat patients with OAB and I now plan to change my treatment methods based on completing this course.
4. I do diagnose and treat patients with OAB and this course confirmed that I don’t need to change my treatment methods. 78