nyp/q dsrip executive committee meeting thursday april 21
TRANSCRIPT

NYP/Q DSRIP Executive Committee Meeting Thursday April 21, 2016- 4:30p.m.-5:00p.m. – Conference Call
EXECUTIVE COMMITTEE MEMBERS: Maureen Buglino (Chair) - NewYork-Presbyterian/Queens Anthony Somogyi M.D. (Vice-Chair) - NewYork-Presbyterian/Queens Maria D’Urso - NewYork-Presbyterian/Queens Frank Hagan - NewYork-Presbyterian/Queens John Lavin - Mental Health Provider of Western Queens Daniel Muskin - The Grand Nursing Home Lorraine Orlando - NewYork-Presbyterian/Queens Faivish Pewzner - Americare Ashook Ramsaran - PAC Member Michael Tretola - Silvercrest Center for Nursing and Rehabilitation Paul Vitale - Queens Coordinated Care Partners AGENDA:
I. Welcome M. Buglino
II. Review & Approve Minutes of Previous Meeting – Action Item M. Buglino
III. DY1 Q3 Dashboard A. Simmons
IV. DY1 Q4 Reporting Progress A. Simmons
V. IT Change Management Strategy – Action Item M. Greaker
VI. IT Future State & Roadmap – Action Item M. Greaker
VII. IT Security Enhancement Recommendations – Action Item M. Greaker
VIII. Committee Seat Updates – Action Item M. Buglino a. IT (Committee Chair / Co Chair / EC Seat) b. Cultural Comp (Committee Chair)
IX. Next Meeting – April 21, 2016 M. Buglino
X. Questions / Open Discussion
XI. Adjourn


New York State Department of Health
Delivery System Reform Incentive Payment (DSRIP) Program
Achievement Value (AV) Scorecard
The New York Presbyterian Hospital of Queens
Quarter
PPS
PPS Number
AVs Available AVs AwardedAV
Adjustment
Net AVs
Awarded
Payment
Available
Payment
Earned
High
Performance
Funds
Total
Payment
Earned
5.00 5.00 0.00 5.00
21.00 21.00 0.00 21.00 -$ -$ -$ -$
21.00 21.00 0.00 21.00 -$ -$ -$ -$
21.00 21.00 0.00 21.00 -$ -$ -$ -$
21.00 21.00 0.00 21.00 -$ -$ -$ -$
16.00 16.00 0.00 16.00 -$ -$ -$ -$
13.00 13.00 0.00 13.00 -$ -$ -$ -$
10.00 10.00 0.00 10.00 -$ -$ -$ -$
11.00 11.00 0.00 11.00 -$ -$ -$ -$
16.00 16.00 0.00 16.00 -$ -$ -$ -$
DY1, Q3 October 1, 2015 - December 31, 2015
PPS Information
Organizational funds are embedded within each
project's payment
Achievement Value (AV) Scorecard Summary
AV Data Payment DataProject Link (click on the purple link below to access
each individual project report)
The New York Presbyterian Hospital of Queens
40
Domain I - Organizational (All Projects)
2.a.ii
Print Summary
Print All
2.b.v
2.b.vii
2.b.viii
3.a.i
3.b.i
3.d.ii
3.g.ii
4.c.ii
New York State Department of Health
Delivery System Reform Incentive Payment (DSRIP) Program
Achievement Value (AV) Scorecard
The New York Presbyterian Hospital of Queens
Print Summary
Print All
150.00 150.00 0.00 150.00 -$ -$ -$ -$ Total
AV Adjustments (Column F)

CHANGE MANAGEMENT PLAN NYPQ DSRIP PPS
NEW YORK PRESBYTERIAN QUEENS 56-45 MAIN STREET FLUSHING, NY 11355
DATE 3/28/16

NPYQ- MILESTONE # 2
1
TABLE OF CONTENTS INTRODUCTION ................................................................................................................................ 2 CHANGE MANAGEMENT APPROACH ................................................................................................ 2 DEFINITIONS OF CHANGE ................................................................................................................. 2 CHANGE CONTROL BOARD .............................................................................................................. 3 ROLES AND RESPONSIBILITIES ......................................................................................................... 3 CHANGE CONTROL PROCESS ........................................................................................................... 4

NPYQ- MILESTONE # 2
2
INTRODUCTION The Change Management strategy was created by the PPS CMIO, for the NYPQ DSRIP Project in order to set expectations on how the approach to changes will be managed, what defines a change, the purpose and role of the change control board, and the overall change management process. All stakeholders will be expected to submit or request changes to the DSRIP Project in accordance with this Change Management Plan and all requests and submissions will follow the process detailed herein. CHANGE MANAGEMENT APPROACH The Change Management approach for the NYPQ DSRIP Project will ensure that all proposed changes are defined, reviewed, and agreed upon so they can be properly implemented and communicated to all stakeholders. This approach will also ensure that only changes within the scope of this project are approved and implemented. The Change Management approach is not to be confused with the Change Management Process which will be detailed later in this strategy. The Change Management approach consists of three areas:
• Ensure changes are within scope and beneficial to the project • Determine how the change will be implemented • Manage the change as it is implemented
The Change Management process has been designed to make sure this approach is followed for all changes. By using this approach methodology, the NYPQ DSRIP PMO will prevent unnecessary changes from occurring and focus its resources only on beneficial changes within the project scope. DEFINITIONS OF CHANGE
There are several types of changes which may be requested and considered for the NYPQ DSRIP Project. Depending on the extent and type of proposed changes, changes project documentation and the communication of these changes will be required to include any approved changes into the project plan and ensure all stakeholders are notified. Types of changes include:
• Scheduling Changes: changes which will impact the approved project schedule. These
changes may require fast tracking, crashing, or re-baselining the schedule depending on the significance of the impact.
• Budget Changes: changes which will impact the approved project budget. These changes may require requesting additional funding, releasing funding which would no longer be required or adding to project or management reserves. May require changes to the cost baseline.
• Scope Changes: changes which are necessary and impact the project’s scope which may be the result of unforeseen requirements which were not initially planned for. These changes may also impact budget and schedule. These changes may require revision to WBS, project scope statement, and other project documentation as necessary.

NPYQ- MILESTONE # 2
3
The project manager will ensure that all approved changes are communicated to the project stakeholders. Additionally, as changes are approved, the project manager will ensure that the changes are captured in Performance Logic (PMIS) and project documentation where necessary. These document updates must then be communicated to the project team and stakeholders as well. CHANGE CONTROL BOARD The Change Control Board (CCB) is the approval authority for all proposed change requests pertaining to the IS Project. The purpose of the CCB is to review all change requests, determine their impacts on the project risk, scope, cost, and schedule, and to approve or deny each change request. The following chart provides a list of the CCB members for the NYP/Q- DSRIP Project: Name Position CCB Role M. Greaker IS Project Sponsor CCB Chair M. Durso DSRIP Executive Lead CCB Member Maurine Buglino DSRIP Executive Lead CCB Member K. Weiner NYPQ Compliance Officer CCB Member As change requests are submitted to the IS Project Manager by the project team/stakeholders, the Project Manager will log the requests in a change log and the CCB will convene every other Friday to review all change requests. For a change request to be approved, all CCB members must vote in favor. In the event more information is needed for a particular change request, the request will be deferred and sent back to the requestor for more information or clarification. If a change is deemed critical, an ad hoc CCB meeting can be called in order to review the change prior to the next scheduled bi-weekly CCB meeting. ROLES AND RESPONSIBILITIES The following are the roles and responsibilities for all change management efforts related to the NYPQ DSRIP Project: Project Sponsor:
• Approve all changes to budget/funding allocations • Approve all changes to schedule baseline • Approve any changes in project scope • Chair the CCB
Project Manager:
• Receive and log all change requests from project stakeholders/Network partners • Conduct preliminary risk, cost, schedule, scope analysis of change prior to CCB • Seek clarification from change requestors on any open issues or concerns • Make documentation revisions/edits as necessary for all approved changes

NPYQ- MILESTONE # 2
4
• Coordinate change request trainings and communicate changes as appropriate. Project Team/Stakeholders:
• Submit all change requests on standard organizational change request forms • Provide all applicable information and detail on change request forms • Be prepared to address questions regarding any submitted change requests • Provide feedback as necessary on impact of proposed changes
CHANGE CONTROL PROCESS The Change Control Process for the NYPQ DSRIP Project will follow the organizational standard change process for all projects. The project manager has overall responsibility for executing the change management process for each change request.
1) Identify the need for a change (Stakeholders) – Change requestor will submit a completed change request form to the project manager.
2) Log change in the change request register (Project Manager) – The project manager will keep a log of all submitted change requests throughout the project’s lifecycle.
3) Evaluate the change (Project Manager, Team, and Requestor) – The project manager will conduct a preliminary analysis on the impact of the IT system change to risk, cost, schedule, and scope and seek clarification from team members and the change requestor.
4) Submit change request to CCB (Project Manager) – The project manager will submit the change request, as well as the preliminary analysis, to the CCB for review.
5) Obtain Decision on change request (CCB) – The CCB will discuss the proposed change and decide whether or not it will be approved based on all submitted information.
6) Implement change (Project Manager) – If a change is approved by the CCB, the project manager will update and re-baseline project documentation as necessary.
7) All approved changes will be shared with the Executive and IT committees to ensure that all stakeholders have knowledge of a change and its impact.

NPYQ- MILESTONE # 2
5
SPONSOR ACCEPTANCE Approved by the Project Sponsor: __________________________________________ Date: ___________________ <Project Sponsor> <Project Sponsor Title>
IT Future State & Roadmap
1
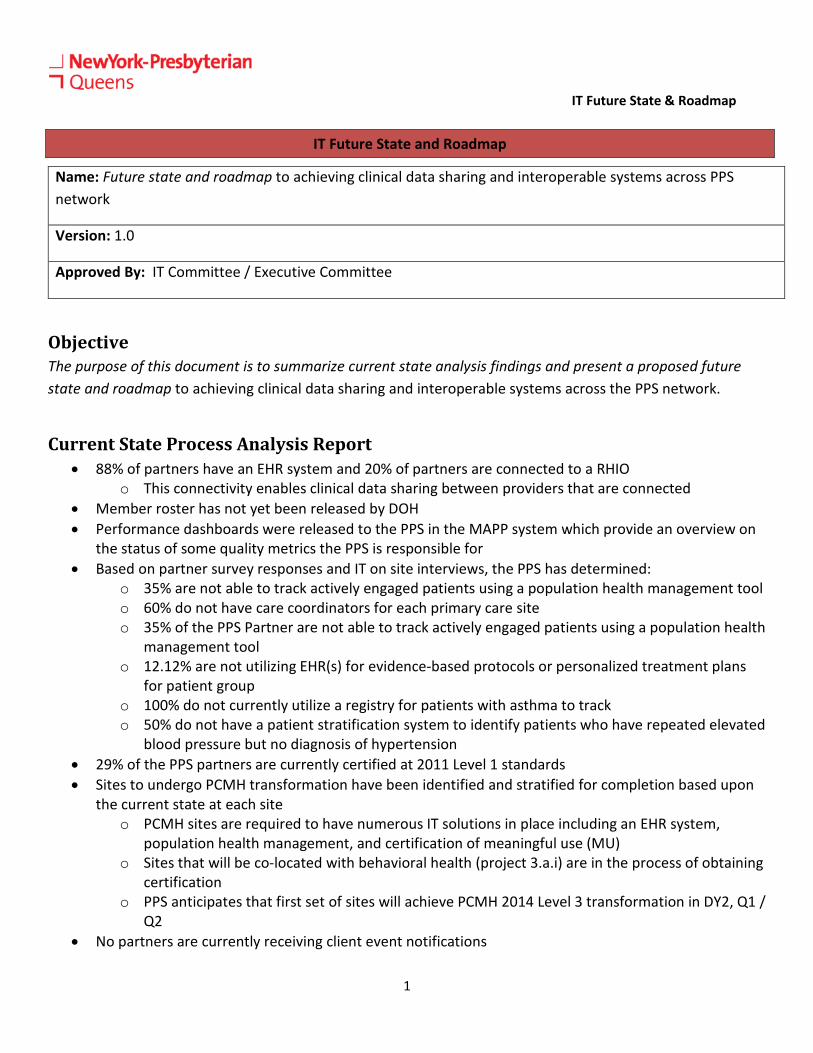
IT Future State and Roadmap
Name: Future state and roadmap to achieving clinical data sharing and interoperable systems across PPS network
Version: 1.0
Approved By: IT Committee / Executive Committee
Objective The purpose of this document is to summarize current state analysis findings and present a proposed future state and roadmap to achieving clinical data sharing and interoperable systems across the PPS network.
Current State Process Analysis Report • 88% of partners have an EHR system and 20% of partners are connected to a RHIO
o This connectivity enables clinical data sharing between providers that are connected • Member roster has not yet been released by DOH • Performance dashboards were released to the PPS in the MAPP system which provide an overview on
the status of some quality metrics the PPS is responsible for • Based on partner survey responses and IT on site interviews, the PPS has determined:
o 35% are not able to track actively engaged patients using a population health management tool o 60% do not have care coordinators for each primary care site o 35% of the PPS Partner are not able to track actively engaged patients using a population health
management tool o 12.12% are not utilizing EHR(s) for evidence-based protocols or personalized treatment plans
for patient group o 100% do not currently utilize a registry for patients with asthma to track o 50% do not have a patient stratification system to identify patients who have repeated elevated
blood pressure but no diagnosis of hypertension • 29% of the PPS partners are currently certified at 2011 Level 1 standards • Sites to undergo PCMH transformation have been identified and stratified for completion based upon
the current state at each site o PCMH sites are required to have numerous IT solutions in place including an EHR system,
population health management, and certification of meaningful use (MU) o Sites that will be co-located with behavioral health (project 3.a.i) are in the process of obtaining
certification o PPS anticipates that first set of sites will achieve PCMH 2014 Level 3 transformation in DY2, Q1 /
Q2 • No partners are currently receiving client event notifications

IT Future State & Roadmap
2
Summary of Analysis Findings • Consent for inclusion in the RHIO needs to be completed at each partner site – there is no universal
opt-in or opt-out process at this time • There is limited data available to the PPS, including quality metrics at a partner level, for the PPS to be
able to complete rapid cycle improvements in the project implementation • Limited financial incentives for partners to join the RHIO compared to the cost of building the
integrated feeds with EHRs • A minimal number of partners are utilizing paper charts and will have a big lift to adopt an EHR • PCMH transformation is a timely and potentially costly transformation process; the PPS’s speed and
scale commitments are a risk is partners decide not to continue with the process o This risk has a potential financial impact as there are AVs associated with meeting these
commitments made to DOH • PCMH requires care coordination and many sites do not currently employ or have the bandwidth for a
dedicated care coordinator • Partners may not have the capacity to integrate all of the tools needed to complete the DSRIP
requirements in the appropriate timeframe • PPS has limited capacity to train partners on the tool • Client event notifications are a risk as there is currently no baseline or successful partner
implementation to leverage in this process

IT Future State & Roadmap
3
Proposed Future State • PPS is looking for creative way to incentivize partners to adopt an EHR and connect to Healthix
o EHR Adoption: The PPS selected ‘EHR implementation investment’ as an equity infrastructure measure
to allow funding from this initiative to pass down to participants PPS is collaborating with NYCReach to increase the number of partners with an EHR
o RHIO Connectivity: o PPS will partner with Healthix (partner RHIO) to facilitate partners joining the RHIO
PPS is conducting a RHIO connectivity pilot at this time with 10 partners • PPS is participating in the Target Operating Model (TOM) series to work with KPMG / PCG / DOH on
creating IT operating models to be utilized in the PPS and achieve true integration • PPS has contracted with HANYS consulting services to help partners become certified at the Level 3
2014 PCMH standards • Partners that undergo PCMH transformation are eligible for higher reimbursement rates for patient
encounters • PPS has purchased a population health management tool for partners to utilize for care coordination
and data reporting • PPS will work with Healthix to incorporate event notifications into the integrated EHR / RHIO data
feeds • PPS has selected Cureatr tool for event notifications • Perform population health management by actively using EHRs and other IT platforms, including use of
targeted patient registries, for all participating net providers • Project committee and HANYS consultant will work with partners to identify a care coordinator at each
primary care site • Develop collaborative evidence-based standards of care including medication management and care
engagement process • Include protocols, such as the Stanford Model and asthma home based registries, for chronic disease
management to ensure that reports can be pulled based on these requirements .
IT Future State & Roadmap
4
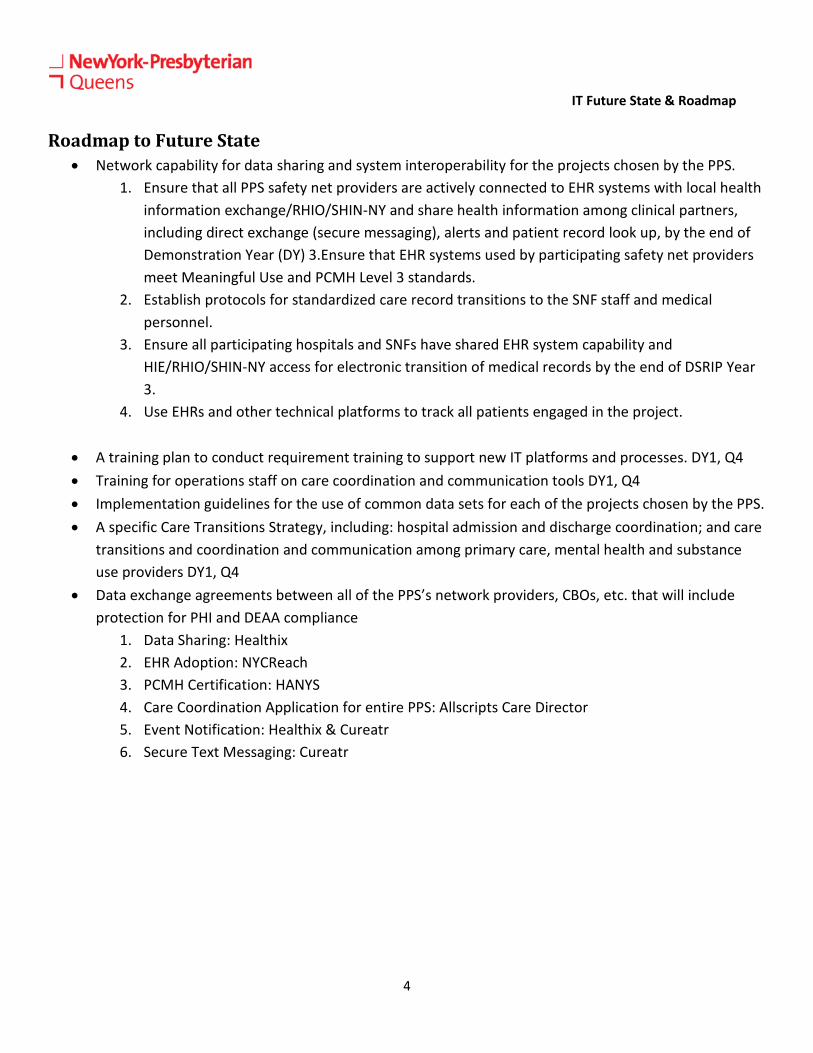
Roadmap to Future State • Network capability for data sharing and system interoperability for the projects chosen by the PPS.
1. Ensure that all PPS safety net providers are actively connected to EHR systems with local health information exchange/RHIO/SHIN-NY and share health information among clinical partners, including direct exchange (secure messaging), alerts and patient record look up, by the end of Demonstration Year (DY) 3.Ensure that EHR systems used by participating safety net providers meet Meaningful Use and PCMH Level 3 standards.
2. Establish protocols for standardized care record transitions to the SNF staff and medical personnel.
3. Ensure all participating hospitals and SNFs have shared EHR system capability and HIE/RHIO/SHIN-NY access for electronic transition of medical records by the end of DSRIP Year 3.
4. Use EHRs and other technical platforms to track all patients engaged in the project.
• A training plan to conduct requirement training to support new IT platforms and processes. DY1, Q4 • Training for operations staff on care coordination and communication tools DY1, Q4 • Implementation guidelines for the use of common data sets for each of the projects chosen by the PPS. • A specific Care Transitions Strategy, including: hospital admission and discharge coordination; and care
transitions and coordination and communication among primary care, mental health and substance use providers DY1, Q4
• Data exchange agreements between all of the PPS’s network providers, CBOs, etc. that will include protection for PHI and DEAA compliance
1. Data Sharing: Healthix 2. EHR Adoption: NYCReach 3. PCMH Certification: HANYS 4. Care Coordination Application for entire PPS: Allscripts Care Director 5. Event Notification: Healthix & Cureatr 6. Secure Text Messaging: Cureatr

IT Future State & Roadmap
5
Work Flow Future State and Roadmap Diagram for NYPQ DSRIP

IT Future State & Roadmap
6
DSRIP WORKFLOW ROADMAP DESCRIPTION 1. The DSRIP team will collect consent from the Life to use their data. This will be enrolled into the RHIO via an FTP or pre or post registration of the EMR. Consent will be track by the RHIO.
2. The Life is now enrolled in the RHIO Event Notification tool, if an event is posted by any of the RHIO members or PPS parties (see bottom portion of diagram to reflect the many ways), the RHIO will match the record with the enrollment (MPI) and send a message (secure email or CCDA) is sent to the DSRIP team and Population Health applications.
3. The DSRIP teat acts on this event by notifying all parties required, Case managers, remote providers and so on.
4. The event(s) will be tracked through the Population help tool. All parties will update the tool as actions are performed.
5. Analytics will be done by collecting data from the Population Health tool and MAP. Reports will come from the reporting tool and s Access
6. The RHIO will provide reporting and auditing of the said Patient information to assure secured and approved access is only being allowed.

IT Security Assessment & Action Plan
1
DSRIP IT Security Assessment and Action Plan
Approving Committee: IT Committee / Executive Committee Date: April 21, 2016 Objective: Survey the PPS partners to evaluate their IT security strengths

IT Security Assessment & Action Plan
2
Table of Contents DSRIP IT Security Assessment and Action Plan ....................................................................... 1
Strategic Objective ........................................................................................................................ 3
Procedures requiring safeguards to limit access to PHI ........................................................... 3
PPS likelihood of a threat/vulnerability affecting Their PHI ................................................... 4
PPS practice/organization that analyze the activities performed by all of its workforce and service providers to identify the extent to which each needs access to PHI ............................ 4
PPS Partners/Organization that practice identifies the security settings for each of its information systems and electronic devices that control access evidence-based standards of care including medication management and care engagement process. ................................. 5
PPS Partners/Organization that implements policies and procedures to enable access to PHI in the event of an emergency. ............................................................................................... 5
PPS Partners/Organizations that back up PHI by saving an exact copy to a magnetic disk/tape or a virtual storage, such as a cloud environment. .................................................... 6
PPS Partners/Organizations that have the capability to activate emergency access to its information systems in the event of a disaster............................................................................ 6

IT Security Assessment & Action Plan
3
Strategic Objective PMO IT staff to assess by surveying the PPS Partner who practice/organization has policies and procedures requiring safeguards to limit access to PHI to those persons and software programs appropriate for their role. Assess PPS likelihood of a threat/vulnerability affecting Their PHI. Assess PPS that practice/organization analyze the activities performed by all of its workforce and service providers to identify the extent to which each needs access to PHI. Assess PPS Partners/Organization that practice identifies the security settings for each of its information systems and electronic devices that control access evidence-based standards of care including medication management and care engagement process. Assess PPS Partners/Organization that implements policies and procedures to enable access to PHI in the event of an emergency. Assess PPS Partners/Organizations that have the capability to activate emergency access to its information systems in the event of a disaster. Assess PPS Partners/Organizations that have policies and procedures that require an authorized user’s session to be automatically logged-off after a predetermined period of inactivity. In order to maximize the IT security strengths of the partners these are the questions that needs to be addressed.
Procedures requiring safeguards to limit access to PHI
Current State: 88.89% of the PPS have policies and procedures requiring safeguards to limit access to PHI to those persons and software programs appropriate for their role. Gaps – Known and Potential: 11.11% practice/organization need to implement policies and procedures requiring safeguards to limit access to PHI to those persons and software programs appropriate for their role
Action Plan:
Per DSRIP information security policy the participating PPS will need to establish a process on getting the remaining 11.11% practice/organization to implement policies and procedures requiring safeguards to limit access to PHI to those persons and software programs appropriate for their role. NYPQ will review and reassess once these policies/measures are executed.

IT Security Assessment & Action Plan
4
PPS likelihood of a threat/vulnerability affecting Their PHI Current State: 83.33% of the PPS answered the survey saying that there’s very low chance of a threat/vulnerability affecting their PHI. Gaps – Known and Potential: 16.67% of the PPS answered the survey saying that there’s a possible chance of a threat/vulnerability affecting your PHI. Action Plan: Per DSRIP information security policy the participating PPS will need to establish a process on getting the remaining 16.67% practice/organization to implement policies and procedures requiring safeguards to limit access to PHI to those persons and software programs appropriate for their role. NYPQ will review and reassess once these policies/measures are executed.
PPS practice/organization that analyze the activities performed by all of its workforce and service providers to identify the extent to which each needs access to PHI Current State: 83.33% of the PPS practice/organization analyzes the activities performed by all of its workforce and service providers to identify the extent to which each needs access to PHI. Gaps – Known and Potential: 16.67% of the PPS practice/organization analyzes the activities performed by all of its workforce and service providers to identify the extent to which each needs access to PHI. Action Plan: Per DSRIP information security policy the participating PPS will need to establish a process on getting the remaining 16.67% practice/organization to analyze the activities performed by all of its workforce and service providers to identify the extent to which each needs access to PHI. NYPQ will review and reassess once these policies/measures are executed.

IT Security Assessment & Action Plan
5
PPS Partners/Organization that practice identifies the security settings for each of its information systems and electronic devices that control access evidence-based standards of care including medication management and care engagement process. Current State: 94.44 % of the PPS Partners/Organization practice identifies the security settings for each of its information systems and electronic devices that control access. Gaps – Known and Potential: 5.56% PPS Partners/Organization practice does not identify the security settings for each of its information systems and electronic devices that control access. Action Plan: Per DSRIP information security policy the participating PPS will need to establish a process on getting the remaining 5.56% PPS Partners/Organization to practice and identify the security settings for each of its information systems and electronic devices that control access. NYPQ will review and reassess once these policies/measures are executed.
PPS Partners/Organization that implements policies and procedures to enable access to PHI in the event of an emergency. Current State: 44.44% of the PPS Partners/ Organization have implemented policies and procedures to enable access to PHI in the event of an emergency. Gaps – Known and Potential: 50.00% of the PPS Partners/ Organization have not implemented policies and procedures to enable access to PHI in the event of an emergency. Action Plan: Per DSRIP information security policy the participating PPS will need to establish a process on getting the remaining 50.00% PPS Partners/Organization to implement policies and procedures to enable access to PHI in the event of an emergency. NYPQ will review and reassess once these policies/measures are executed.

IT Security Assessment & Action Plan
6
PPS Partners/Organizations that back up PHI by saving an exact copy to a magnetic disk/tape or a virtual storage, such as a cloud environment. Current State: 88.24% of the PPS Partners/Organizations back up PHI by saving an exact copy to a magnetic disk/tape or a virtual storage, such as a cloud environment. Gaps – Known and Potential: 11.76% of the PPS Partners/Organizations back up PHI by saving an exact copy to a magnetic disk/tape or a virtual storage, such as a cloud environment. Action Plan: Per DSRIP information security policy the participating PPS will need to establish a process on getting the remaining 11.76% PPS Partners/Organization to back up PHI by saving an exact copy to a magnetic disk/tape or a virtual storage, such as a cloud environment. NYPQ will review and reassess once these policies/measures are executed. PPS Partners/Organizations that have the capability to activate emergency access to its information systems in the event of a disaster. Current State: 75.00% have the capability to activate emergency access to its information systems in the event of a disaster. Gaps – Known and Potential: 25.00% does not have the capability to activate emergency access to its information systems in the event of a disaster. Action Plan: Per DSRIP information security policy the participating PPS will need the remaining 25.00% capable to activate emergency access to its information systems in the event of a disaster. NYPQ will review and reassess once these policies/measures are executed.

1 | P a g e
Document Title: Committee Seat Changes
Approval Needed: Executive Committee
Date: April 21, 2016
Document Objective/Summary:
This document outlines the changes in committee lead positions due to changes in workforce or committee needs.
The following committee lead seat changes are recommended to the NYP/Q Executive Committee:
IT & Reporting Committee Position Change From Change To Reason
Committee Chair Dr. Kenneth Ong Mark Greaker, NYP/Q Dr. Ong no longer with NYP/Q Committee Co-Chair Mark Greaker Keith Weiner, NYP/Q Moving to Chair position
Cultural Competency Committee
Position Change From Change To Reason Committee Chair Helen Lavas Maureen Buglino NYP/Q Resignation of Chair position Committee Co-Chair Medina Kurtovic Sarah Kalinowski, NYP/Q Resignation of Co-Chair
position