nutrition without harm: feeding the critically ill patient
TRANSCRIPT

NUTRITION WITHOUT HARM: FEEDING THE CRITICALLY ILL PATIENT
NUTRITION SANS PREJUDICE: NOURRIR LE PATIENT EN ETAT CRITIQUE
Wednesday, March 11 2015Mercredi 11 Mars 2015

Your Hosts & PresentersVos hôtes et présentateurs
Leanne Couves, Improvement Advisor
L. John Hoffer, MD, PhD, FRCPC; Professor of Medicine, McGill University; Attending PhysicianJewish General Hospital.
Paule Bernier, P.DT., MSc.; Présidente, Ordre professionnel des diététistes du Québec; Sir MB David Jewish General Hospital (McGill University), Montreal
Ardis Eliason, Technical Host
Hélène Riverin, French Language Support, CPSI
211/03/2015

Interacting in WebEx: Today’s ToolsInteragir dans Webex : outils à utiliser
3
Be prepared to use:‐ Pointer ‐ Raise hand‐ CHAT‐ Text Tool “writing on the slide”‐ Shape Tools
Have you used WebEx before?Avez‐vous déjà utilisé WebEx? YES / OUI NO / NON
Soyez prêts à utiliser les outils :‐ le pointeur ‐ lever la main‐ clavardage‐ Outil textuel pour « écrire sur la diapo »‐ Outils de forme11/03/2015
Type your message & click ‘send’
Select ‘send to’

4
Who’s Online? Qui est en ligne?
POINTER
11/03/2015

What professions are represented?Quelles professions sont représentées?
Nurse MD
Educator / Quality Improvement Professional
Infection Control
Administrator / Senior Leader
Other
POINTER
RespiratoryTherapist
Nutritionist
511/03/2015

11/03/2015 6
Objectives of the Call
To understand the current evidence on ICU nutrition. To translate this evidence into practice for
energy. To translate this evidence into practice for
macronutrients.

Dr. John Hoffer
NUTRITION WITHOUT HARM: FEEDING THE CRITICALLY ILL PATIENT
NUTRITION SANS PREJUDICE: NOURRIR LE PATIENT EN ETAT CRITIQUE

Canadian Patient Safety Institute
Nutrition Without Harm: Feeding the Critically Ill Patient ~ Protein and Energy Requirements
L. John Hoffer, MD PhD FRCPCMcGill University
March 11, 2015

Objectives
• Describe shortcomings and misunderstanding of the evidence regarding optimal protein and energy provision in critical illness with attention to the relationships between protein and energy provision
• Highlight contradictory recommendations for protein provision in critical illness
• Suggest a rational and testable approach to protein provision in the ICU
Financial Interest Disclosure
No relevant financial relationships with any commercial interests

Why Such Contradictory Recommendations?
• ASPEN: Critical illness dramatically increases protein requirement; therefore provide– 1.5 g protein/kg per day + full energy provision for
non-obese patients: e.g. Ziegler NEJM 2009;361:1088
– 2.0-2.5 g protein/kg IBW + 50-75% energy for obese patients: Choban et al JPEN 2013;37:714
• Recent high profile clinical review: – Recommends hypocaloric “permissive underfeeding”– Protein is unimportant
• Casaer and van den Berghe NEJM 2014;370:1227
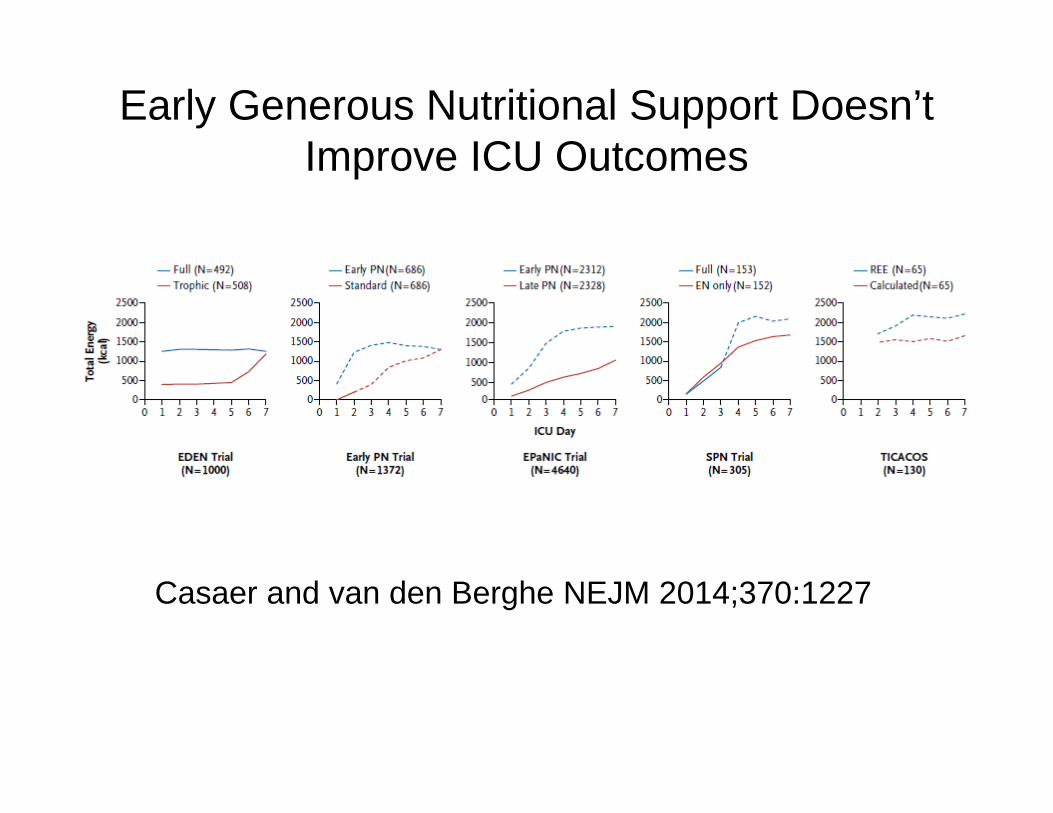
Early Generous Nutritional Support Doesn’t Improve ICU Outcomes
Casaer and van den Berghe NEJM 2014;370:1227

The Nutritional Physiology of Critical Illness
• The body cell mass (BCM) contains two compartments– peripheral (80%); muscle, slow turnover– central (20%); viscera etc, rapid turnover
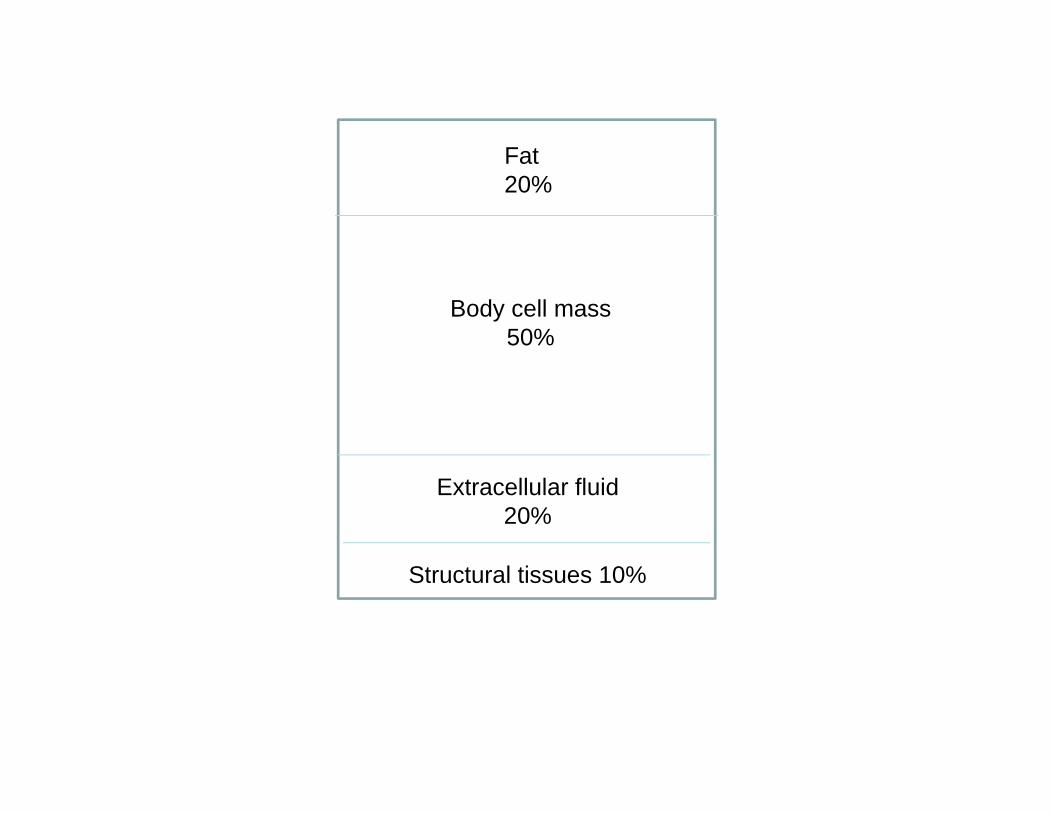
Fat 20%
Body cell mass 50%
Extracellular fluid 20%
Structural tissues 10%


Nutritional Pathology of Critical Illness
• Severe systemic inflammation dramatically increases net muscle proteolysis, increases central protein synthesis (rate-limited by free amino acid availability), and increases amino acid catabolism-urea synthesis
• Consequent rapid dramatic muscle atrophy leading to weakness, debilitation and inadequate central protein synthesis to support healing and immunity

Long CL Nutr Res 1993

Obesity Does Not Preclude Protein Malnutrition
• Muscle atrophy vastly outstrips fat loss in critical illness
• Most ICU patients are overweight or obese
• Severe muscle atrophy is likely very common in the ICU, but goes unnoticed, and rarely thought about
• Obesity misleads physicians into assuming their patient is “well nourished”

Recommendations for Protein Provision in Critical Illness
• ASPEN: Critical illness dramatically increases protein requirement– 1.5 g protein/kg per day + full energy provision for
non-obese patients: e.g. Ziegler NEJM 361:1088 (2009)
– 2.0-2.5 g protein/kg IBW + 50-75% energy for obese patients: Choban et al JPEN 37:714, 2013
– Normal people require ~ 0.8 g protein/kg/day


Scanty and Abysmal Clinical Evidence
• Unclear definitions of critical illness• Very low enrolments, enormous inter-group
heterogeneity, hopelessly low statistical power• Impossible to identify any average protein level as
maximally beneficial • Deliberate energy over-feeding in order to maximize
muscle protein accretion• Failure to appreciate that average intake is not “safe”
protein intake

Abysmal, ctd.• Failure to stipulate how body weight determined, and
how corrected for over-hydration and obesity
• Aqueous solutions of mixed amino acids provide 17% less protein substrate than widely assumed – Thus,1.8 g mixed free amino acids must be infused to provide
1.5 g protein substrate

But…• Every study indicated improving N balance, protein
turnover, or better clinical outcomes as protein or amino acid provision increased to the maximum provided dose of 2.5 g/kg per day
Conclusions
• Widespread view that 1.2-1.5 g protein/kg/day is “sufficient” – hence not to be exceeded – is based upon an unrepresentative biased subset of low-quality studies
• Patients were deliberately energy over-fed; appropriately limited energy provision calls for much more protein
• On balance, the existing evidence compatible with average requirement > 2.0 g/kg/day
• 2.5 - 3.0 appears safe (specific exceptions)
Contradictory Recommendations
• ASPEN: Critical illness dramatically increases protein requirement– 1.5 g protein/kg per day + full energy provision for non-obese
patients: e.g. Ziegler NEJM 361:1088 (2009)– 2.0-2.5 g protein/kg IBW + 50-75% energy for obese patients:
Choban et al JPEN 37:714, 2013
• Casaer and van den Berghe: Allow hypocaloric feeding (“permissive underfeeding”) for up to 7 days: NEJM 370:1227, 2014 – Protein unproven and not important
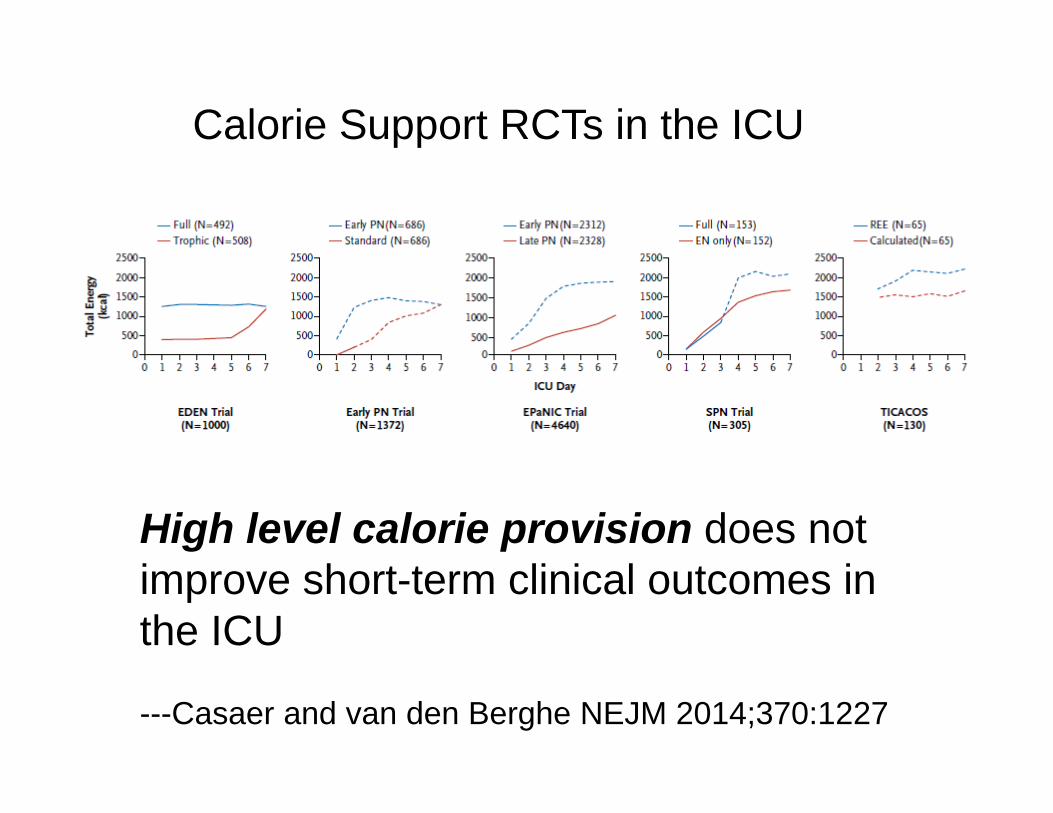
High level calorie provision does not improve short-term clinical outcomes in the ICU
---Casaer and van den Berghe NEJM 2014;370:1227
Calorie Support RCTs in the ICU

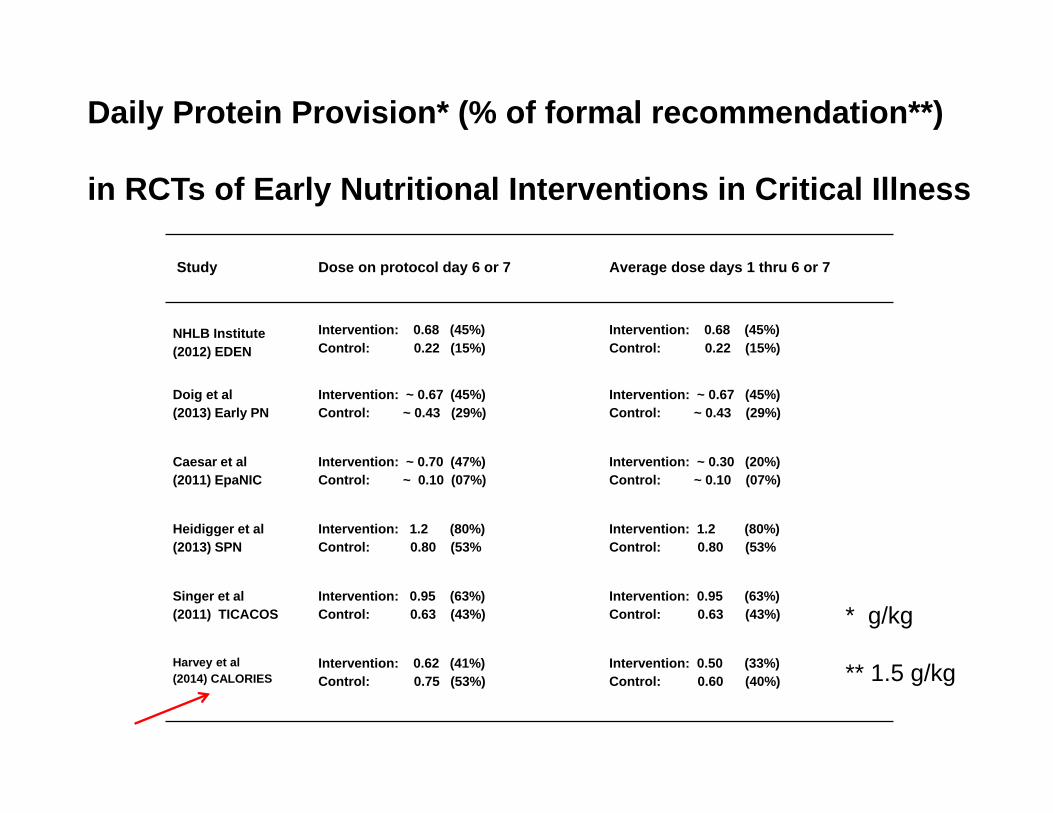
Daily Protein Provision* (% of formal recommendation**)
in RCTs of Early Nutritional Interventions in Critical Illness
Study Dose on protocol day 6 or 7 Average dose days 1 thru 6 or 7
NHLB Institute(2012) EDEN
Intervention: 0.68 (45%)Control: 0.22 (15%)
Intervention: 0.68 (45%)Control: 0.22 (15%)
Doig et al(2013) Early PN
Intervention: ~ 0.67 (45%)Control: ~ 0.43 (29%)
Intervention: ~ 0.67 (45%)Control: ~ 0.43 (29%)
Caesar et al(2011) EpaNIC
Intervention: ~ 0.70 (47%)Control: ~ 0.10 (07%)
Intervention: ~ 0.30 (20%)Control: ~ 0.10 (07%)
Heidigger et al (2013) SPN
Intervention: 1.2 (80%)Control: 0.80 (53%
Intervention: 1.2 (80%)Control: 0.80 (53%
Singer et al(2011) TICACOS
Intervention: 0.95 (63%)Control: 0.63 (43%)
Intervention: 0.95 (63%)Control: 0.63 (43%)
Harvey et al (2014) CALORIES
Intervention: 0.62 (41%)Control: 0.75 (53%)
Intervention: 0.50 (33%)Control: 0.60 (40%)
* g/kg
** 1.5 g/kg

High CALORIE provision does not improve short-term clinical outcomes in the ICU
But PROTEIN provision was grossly “inadequate” in almost every RCT

Why the Obsession with Calories?

What is the Scientific Basis for the Assertion that ICU Patients Need Lots of
Calories?
• Energy expenditure increases in critical illness
• Hypocaloric conditions promote muscle wasting
• Deficient calorie provision is associated with worse clinical outcomes
– Casaer and van den Berghe NEJM 2014;370:1227
All These Premises are Wrong
• Energy is indeed important for efficient dietary protein retention, but providing more than ~ 50% of energy expenditure improves N balance very little further, especially in critical illness

Dickerson Curr Opin Clin Nutr Metab Care 8:189,2005
False Premises Explained
• Hypocaloric states do indeed reduce the efficiency of dietary protein retention, but energy provision greater than ~ 50% of energy expenditure improves N balance very little further, especially in critical illness
• The quintessential protein-sparing nutrient is protein, not calories
• The observed association between low calorie intakes and poor outcomes is far more rationally explained by extremely low protein intakes
• Most ICU patients have at least ample body fat. Why would they need more calories?

This is what we may conclude from the current data: High CALORIE provision doesn’t improve short-term clinical outcomes in the ICU

But protein provision was inadequate in every clinical trial, even though the physiological data overwhelmingly indicate it is the crucial macronutrient to provide in this setting

Why the Obsession with Calories?
• Ignorance of nutritional principles; over-simplified and physiologically naïve therapeutic hypotheses
• Nutritional bigotry and the streetlight effect
Bigotry
• Unreflective & often unconscious oversimplification, stereotyping and labelling
Daily Protein Provision* (% of formal recommendation**)
in RCTs of Early Nutritional Interventions in Critical Illness
Study Dose on protocol day 6 or 7 Average dose days 1 thru 6 or 7
NHLB Institute(2012) EDEN
Intervention: 0.68 (45%)Control: 0.22 (15%)
Intervention: 0.68 (45%)Control: 0.22 (15%)
Doig et al(2013) Early PN
Intervention: ~ 0.67 (45%)Control: ~ 0.43 (29%)
Intervention: ~ 0.67 (45%)Control: ~ 0.43 (29%)
Caesar et al(2011) EpaNIC
Intervention: ~ 0.70 (47%)Control: ~ 0.10 (07%)
Intervention: ~ 0.30 (20%)Control: ~ 0.10 (07%)
Heidigger et al (2013) SPN
Intervention: 1.2 (80%)Control: 0.80 (53%
Intervention: 1.2 (80%)Control: 0.80 (53%
Singer et al(2011) TICACOS
Intervention: 0.95 (63%)Control: 0.63 (43%)
Intervention: 0.95 (63%)Control: 0.63 (43%)
Harvey et al (2014) CALORIES
Intervention: 0.62 (41%)Control: 0.75 (53%)
Intervention: 0.50 (33%)Control: 0.60 (40%)
* g/kg
** 1.5 g/kg

2.0-2.5 g protein/kg IBW + 50-75% energy expenditure

A Plea for Evidence-based Medicine in the ICU – Pending Adequate RCTs
• For patients who have an adequate store of body fat, hypocaloric high-protein nutrition is safest and most physiologically logical
• Therefore, follow the ASPEN guidelines for obese patients for all patients with BMI > 20
• Highest priority patients: existing low muscle mass and/or major protein catabolism
Physiologically-based Nutritional Therapy in the ICU
• Avoid toxic energy overfeeding by limiting calories to 2/3 estimated energy expenditure
• Use PN to provide 1.8 g mixed amino acids* and 3 g dextrose/kg normalized dry BW per day within 48 h of admission
• Adjust PN appropriately every 48 h as EN increases
* Equivalent to 1.5 g protein

Priority Patients
• Borderline or subnormal muscle mass – Protein energy malnutrition, cachexia, disuse atrophy,
old age, neuromuscular disease– Examine muscle mass; discount BMI
• Patients experiencing intense protein catabolism

Cautions
• Significant fat depletion (BMI < 18-20)
• Severe liver dysfunction– Advanced liver disease, hypoperfusion, ornithine
transcarbamoylase deficiency, valproic acid therapy
• Renal insufficiency if renal replacement therapy is unavailable.

Why parenteral and enteralsolutions of free amino acids provide 17% less protein and
energy than intact protein
Hoffer LJ Am J Clin Nutr 2011; 94:1396
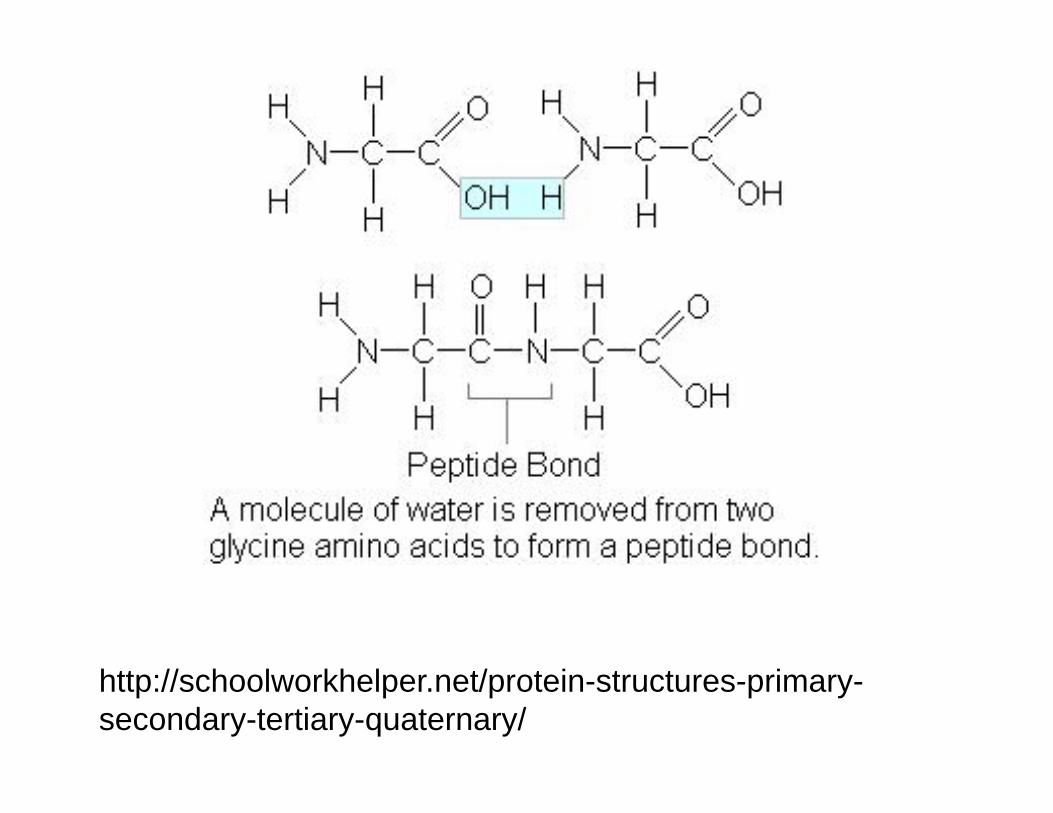
http://schoolworkhelper.net/protein-structures-primary-secondary-tertiary-quaternary/

QUESTIONS?
RAISE YOUR HAND / LEVEZ LA MAIN
OR/OU
CHAT TO “ALL PARTICIPANTS”
“Taking the Pulse” Poll
11/03/2015 49

Instructions to download certificate
1
2 3
4
5
8
9
11/03/2015 50

Canadian ICU Collaborative Faculty
Paule Bernier, P.Dt., Msc, Présidente, Ordre professionnel des diététistes du Québec; Sir MB David Jewish General Hospital (McGill University), Montreal
Paul Boiteau MD, Department Head, Critical Care Medicine, Alberta Health Services; Professor of Medicine, University of Calgary
Mike Cass, BSc, RN, MScN, Advanced Practice Nurse, Trillium Health Centre
Leanne Couves, Improvement Advisor, Improvement Associates Ltd.
Carla Williams, Patient Safety Improvement Lead, CPSI
Bruce Harries, Collaborative Director, Improvement Associates Ltd.
Denny Laporta MD, Intensivist, Department of Adult Critical Care, Jewish General Hospital; Faculty of Medicine, McGill University
Claudio Martin MD,Intensivist, London Health Sciences Centre, Critical Care Trauma Centre; Professor of Medicine and Physiology, University of Western Ontario; Chair/Chief of Critical Care Western
Cathy Mawdsley, RN, MScN, CNCC; Clinical Nurse Specialist – Critical Care, London Health Sciences Centre;
John Muscedere MD, Assistant Professor of Medicine, Queens University; Intensivist, Kingston General Hospital
Yoanna Skrobik MD, Intensivist, Hôpital Maisonneuve Rosemont, Montréal; Expert Panel for the new Pain, Sedation and Delirium Guidelines, Society of Critical Care Medline (SCCM)
5111/03/2015

RemindersRappels
Call is recorded Slides and links to
recordings will be available on Safer Healthcare Now! Communities of Practice
Additional resources are available on the SHNWebsite and Communities of Practice
L'appel est enregistré Les diapositives et liens
vers les enregistrements seront disponibles sur Des soins de santé plus sécuritaires maintenant!Communautés de pratique
Des ressources supplémentaires sont disponibles sur le site Web SSPSM et Communautés de Pratique
5211/03/2015

THANK YOU MERCI

This National Call is hosted by:
Supported by:
5411/03/2015