nutrition supply chain workshop kenya experience · pdf filenutrition supply chain workshop...
TRANSCRIPT

Nutrition Supply Chain Workshop
KENYA Experience
Presented by:
Dr Patrick Amoth
Head, Division of Family Health
Ministry of Health, Kenya
21st June 2016

OVERVIEW OF KENYA NUTRITION SITUATION
30.3
35.3
26
19.9
16.1
11
5.6 6.74
0
5
10
15
20
25
30
35
40
2003 2008 2014
% c
hild
ren
Trends of under nutrition in Kenya(KDHS 2003-2014)
Stunting Underweight Wasting
•Reduction in stunting from 35.3% to 26%, however huge disparities exist
among counties, with some rates exceeding 40%
•MDG target for underweight (11%) achieved.
•According to the Global Nutrition Report 2015, Only 1 country—Kenya—is
on course for all five WHA undernutrition targets.
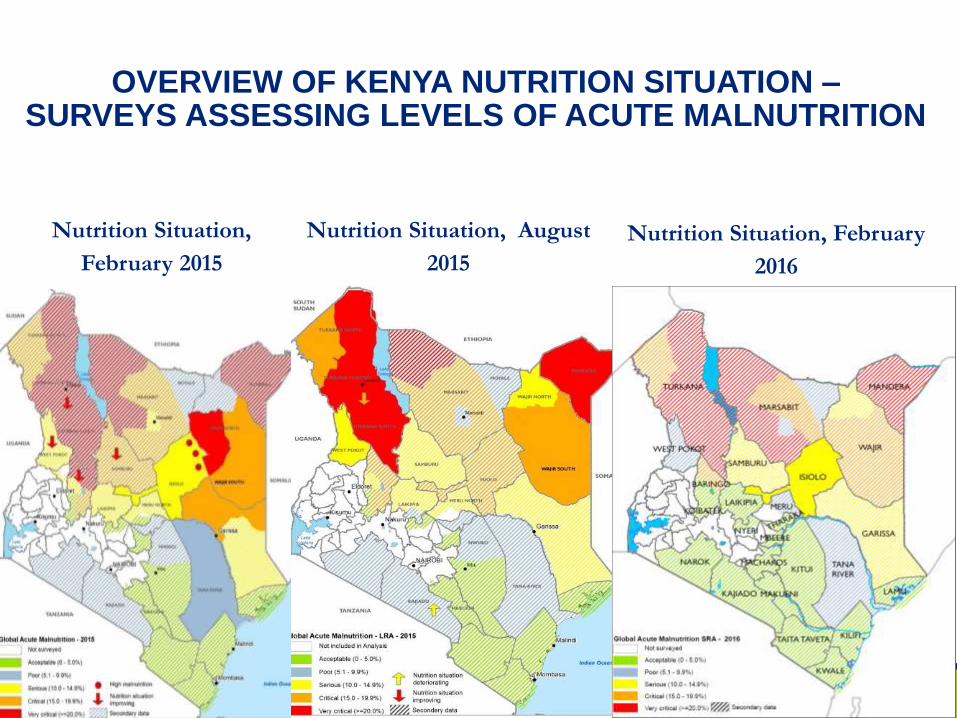
Nutrition Situation,
February 2015
Nutrition Situation, August
2015
Nutrition Situation, February
2016
OVERVIEW OF KENYA NUTRITION SITUATION –SURVEYS ASSESSING LEVELS OF ACUTE MALNUTRITION
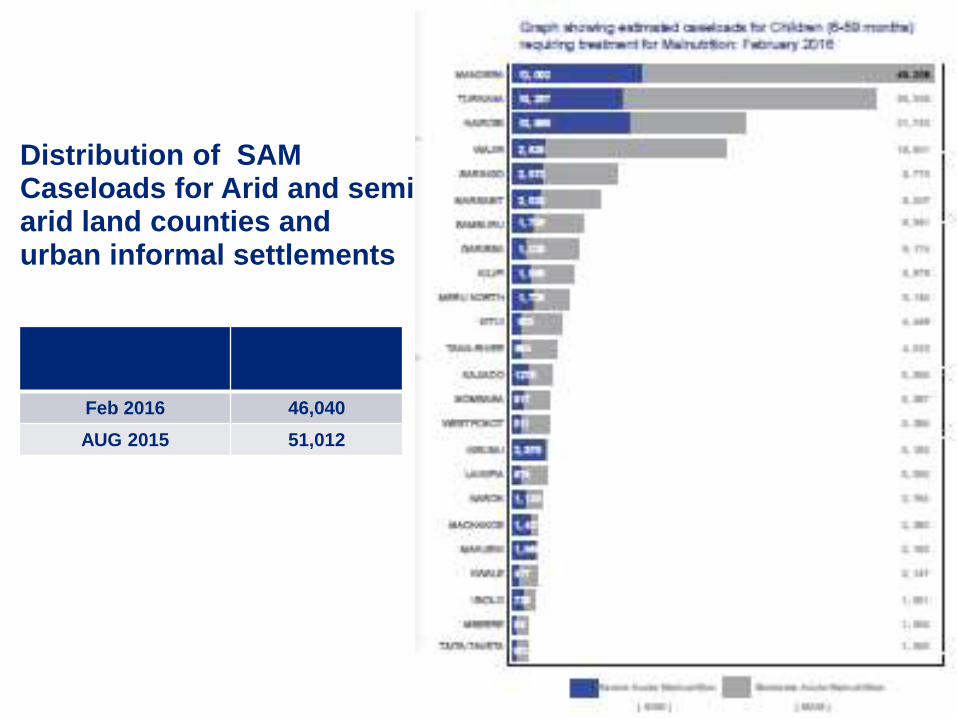
Distribution of SAM Caseloads for Arid and semi arid land counties and urban informal settlements
DATE SAM
Feb 2016 46,040
AUG 2015 51,012

TREATMENT OF SEVERE ACUTE MALNUTRITION
Therapeutic milks – F75 & F100
Ready to Use Therapeutic Food (Plumpy Nut)
ReSoMal
• Each severely malnourished child
requires about 150 sachets of Ready
to Use therapeutic foods until full
recovery
• Each year over 56,000 children living
in Arid and Semi Arid Counties of
Kenya are severely malnourished and
require treatment plus a further
12,000 from the 2 refugee camps and
12,000 in the urban informal
settlements
• In 2015 about 82,000 cartons of
Ready To use Therapeutic foods was
required costing about USD 4.6M
excluding transport

-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
2012 2013 2014 2015
Valu
e (
US
D)
Year
Ready To Use Therapeutic Foods (2012 – 2015)
TREATMENT OF ACUTE MALNUTRITION
It costs 130$ to treat One
(1) Severely
malnourished child
RUTF costs approx.
52USD/ treatment plus
programme costs

PREVIOUS NUTRITION SUPPLY CHAIN DISTRIBUTION SYSTEM IN KENYA
UNICEF store
National level
UNICEF Supply
and logistic unit
County and Sub-
county stores
County & Sub
county level
CNO/DNO/CHMT/
SCHMT
Storeman/
Commodity officers
Health facilities
Officer in
charge/nurse
Outreach
sites
Request
Flow of RUTF
UNICEF Supply
division-
Copenhagen

Contra-
ceptives and
RH
equipment
STI
DrugsEssential
Drugs
Vaccines
and
Vitamin A
TB/Leprosy
Blood
Safety
Reagents
(inc. HIV
tests)
D
F
I
D
K
f
W
UNICEF
J
I
C
A
GOK, WB/
IDA
Source of
funds for
commodities
Commodity
Type(colour coded) MOH
Equip-
ment
Point of first
warehousingKEMSA Central Warehouse
KEMSA
Regional
Depots
Organization
responsible
for delivery to
district levels
KEMSA and KEMSA Regional Depots
(essential drugs, malaria drugs,
consumable supplies)
Procurement
Agent/BodyCrown
Agents
Government
of Kenya
GOK
GTZ(procurement
implementation
unit)
JSI/DELIVER/KEMSA Logistics
Management Unit (contraceptives,
condoms, STI kits, HIV test kits, TB
drugs, RH equipment etc)
E
U
K
f
W
UNICEF
KEPI Cold
Store
KEPI(vaccines
and
vitamin A)
Malaria
U
S
A
I
D
U
S
A
I
D
U
N
F
P
A
E
U
R
O
P
A
Condoms
for STI/
HIV/AIDS
prevention
C
I
D
A
U
N
F
P
A
US
Gov
C
D
C
NPHLS store
MEDS(to Mission
facilities)
Private
Drug
Source
G
D
F
Government
NGO/Private
Bilateral Donor
Multilateral Donor
World Bank Loan
Organization Key
Japanese
Private
Company
W
H
O
G
A
V
I
S
I
D
A
NLTP(TB/
Leprosy
drugs
Commodity Logistics System in Kenya (as of April 2004)Constructed and produced by Steve Kinzett, JSI/Kenya - please communicate
any inaccuracies to [email protected] or telephone 2727210
Anti-
Retro
Virals
(ARVs)
Labor-
atory
supp-
lies
Global
Fund for
AIDS, TB
and Malaria
The
"Consortium"
(Crown Agents,
GTZ, JSI and
KEMSA)
B
T
C
MEDS
D
A
N
I
D
A
Mainly District level staff: DPHO, DPHN, DTLP, DASCO, DPHO, etc or staff from the Health Centres,
Dispensaries come up and collect from the District level
MEDS
Provincial and
District
Hospital
Laboratory
Staff
Organization
responsible for
delivery to sub-
district levels
K
N
C
V
MSF
MSF
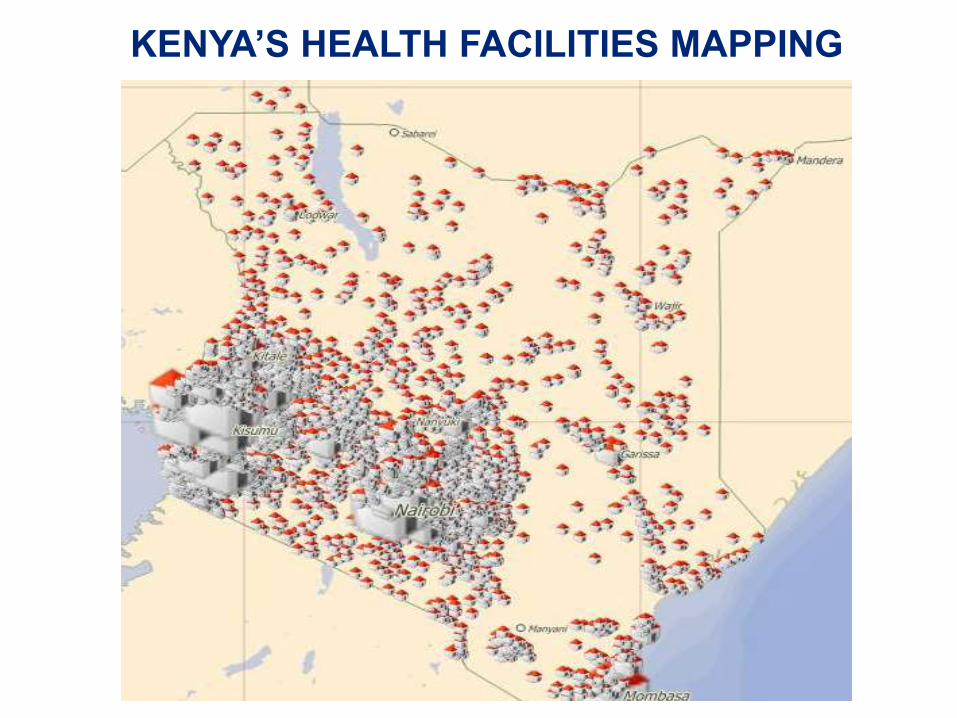
KENYA’S HEALTH FACILITIES MAPPING

Overview of Current Project
• Supply of nutritional commodities is
currently done via parallel logistic
chains by various donors and
stakeholders.
• These parallel systems make it difficult
to coordinate and manage the nutrition
program supply chains since they
require parallel reporting and parallel
logistics systems.
• Objective of the project is to to asses
the Parallel Nutrition Logistics Chains
for Integration into the GoK National
SCM System.
• The assessment focused on RUTF,
RUSF, F-75 and F-100 commodities.
The parallel chains assessed included
UNICEF, WFP and KEMSA.
• The assessment focused on the
activities within the supply chain
functions which include planning,
sourcing, storage, distribution,
monitoring and evaluation.
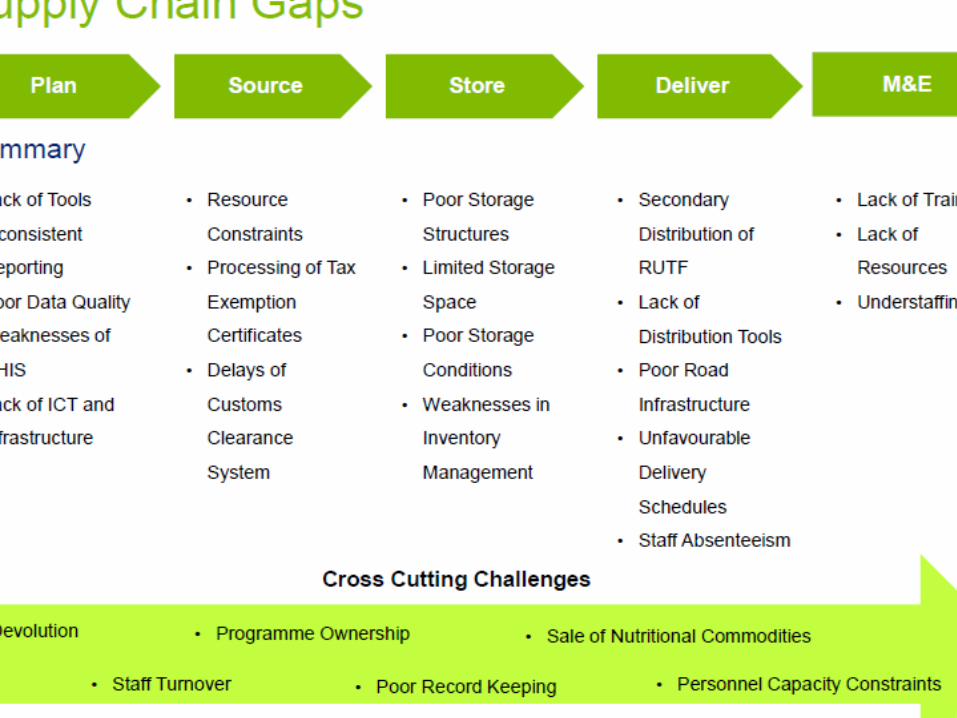
Supply Chain Gaps Supply Chain Recommendations
Deliver
Source
Store
Plan
M&E
• Lack of planning tools
• Inconsistent Reporting
• Poor Data Quality
• Weaknesses in DHIS
• Lack of ICT and
Infrastructure
• Develop Standardized Reporting Tools
• Investment in ICT Infrastructure
• Development of a Resource Mobilization
Strategy
• Lobbying for a blanket Commodity Exemptions
for Nutritional Commodities
• Rehabilitating and Upgrading of Existing Stores
• Design of Suitable Storage Structure
• Provision of Buffer Stocks
• Integration into the National Government
Supply Chain
• Provision of Continuous Training
• Resource Constraints
• Processing of Tax
Exemption Certificates
• Delays of
Customs
Clearance
System
• Poor Storage
Structures
• Weaknesses in
Inventory Management
• Limited Storage Space
• Poor Storage Conditions
• Secondary Distribution of
RUTF
• Lack of Distribution Tools
• Staff Absenteeism
• Poor Road
Infrastructure
• Unscheduled
Deliveries
• Lack of Training
• Lack of
Resources
• Understaffing
Cross Cutting Challenges
• Devolution
• Programme Ownership
• Staff Turnover
• Sale of Nutritional Commodities
Cross Cutting Recommendations
• County Government involvement
• Capacity Building
• Community Engagement and
Sensitization
• Branding and Serialization
Supply Chain Functions
Project Phases
Assessing the parallel
nutritional supply chains
and identifying the
bottlenecks within the
system.
Developed an integration
roadmap that entails the
activities, roles of
stakeholders, KPIs to guide
the implementation process.
Piloting the
integration model to
evaluate its
feasibility and
generate lessons
learnt
Assessment of Parallel Nutrition Logistics Chains for Integration into the GoK National SCM System
2013 - 2014
Phase 1: Assessment Phase 2: Integration Design Phase 3: Pilot

Why Need for integration of system
• Too many parallel nutrition supply chains by
DPs.
• Opportunity to optimize parallel supply chain
systems
Also consider:
• Increased risk of losses
• Poor supply chain management
• Supplies component is a Nutrition Sector
priority: need for better planning and resource
management
• RUTF is on the essential supplies list
KEY BENEFITS OF INTEGRATION
12
• Direct delivery of nutritional commodities to health facilities
• Increased collaboration in forecasting and quantification of needs
• Dedicated warehousing and distribution partner
• Continuous flow of commodities from Mombasa (port) to satellite facilities
(no supply chain breaks)
• Commodity tracking information system
• Trained personnel
• Increased accountability
13

Capacity BuildingFull Integration
The roll out of the integrated supply chain to other counties
will occur after the successful completion of the pilot
project. The full integration will require the following
initiatives for its successful implementation.
Roll out of integrated supply chain
in the country
Standardized reporting tools
Steering committee / Coordinating
entity to guide the implementation
Establishment of funding
mechanism
Establishment of project
management office for
implementation
Capacity Building
This will address the downstream supply chain bottlenecks to have a fully
integrated supply chain model. It will involve training of targeted personnel
from the entities involved in the integration process equipping them to
effectively participate in the integration process. The focus of the training
will be on integrated supply chain management. The approach to undertake
capacity building will involve:
Identify
Audience
Needs
Assessment
Content
Development
Capacity
Development
Scale Up
Identifying the targeted personnel and
stakeholders to be trained in supply chain
management
Conducting a high level analysis of the capacity
gaps of identified personnel and stakeholders
To include order processing, forecasting,
inventory management, stores management,
reporting, M&E, etc.
Use of various approaches to build capacity for
targeted individuals. The trained individuals are
expected to cascade the knowledge to other
personnel and stakeholders
Develop a Capacity Development Scale-Up
Strategy for the country
• Direct delivery of nutritional commodities to health facilities and Commodity tracking information system
• Dedicated warehousing and distribution partner – KEMSA
• Trained personnel and Increased accountability
• Continuous flow of commodities from Mombasa (port) to satellite
facilities (no supply chain breaks)
• Increased collaboration in forecasting and quantification of needs
Stakeholders
NUTRITION SUPPLY CHAIN INTEGRATION
Anticipated Benefits of the Integrated Supply Chain
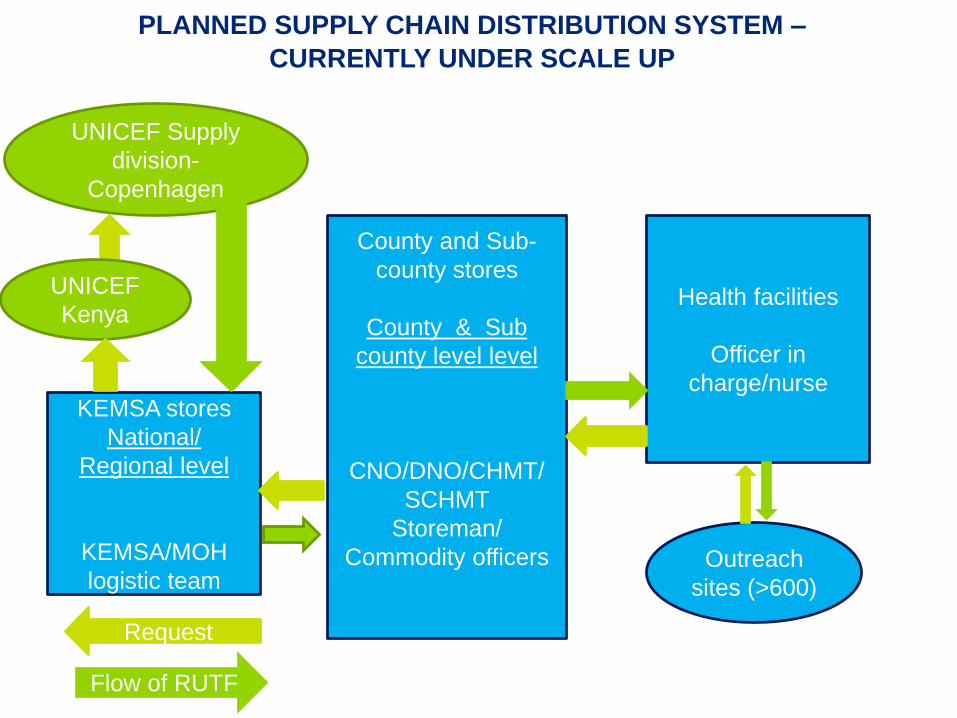
PLANNED SUPPLY CHAIN DISTRIBUTION SYSTEM –
CURRENTLY UNDER SCALE UP
KEMSA stores
National/
Regional level
KEMSA/MOH
logistic team
County and Sub-
county stores
County & Sub
county level level
CNO/DNO/CHMT/
SCHMT
Storeman/
Commodity officers
Health facilities
Officer in
charge/nurse
Outreach
sites (>600)
Request
Flow of RUTF
UNICEF Supply
division-
Copenhagen
UNICEF
Kenya

ORDER REQUEST SYSTEM
16
• Current nutrition reporting structure maintained
• Standardized reporting templates – KEMSA have specific reporting tools for
nutrition
Sub-County
Request
Orders Health Facilities
KEMSA Warehouse
in Nairobi
CNC / CHMT to provide
quality assurance
DNOPhysical
Reports
MoH
Analyzed
data
Direct supply of nutritional commodities by KEMSA
Approved D-
List
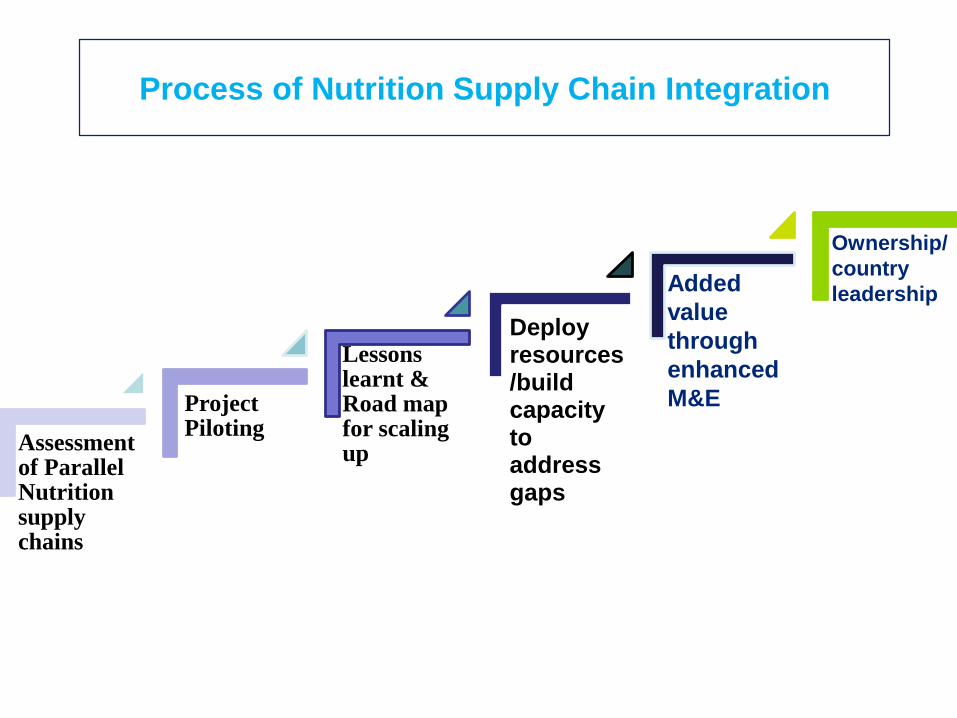
TOWARDS COUNTRY OWNED COUNTRY LED SUSTAINABLE
NUTRITION SUPPLY CHAIN SYSTEM
Assessment of Parallel Nutrition supply chains
Project Piloting
Deploy resources/build capacity to address gaps
Lessons learnt & Road map for scaling up
Ownership/
country
leadershipAdded
value
through
enhanced
M&E
Process of Nutrition Supply Chain Integration

Logistics Management Information System
LMIS- web
based system.
Self-service ordering
platform.
• Online ordering
• Order tracking
• Consumption data
Reporting
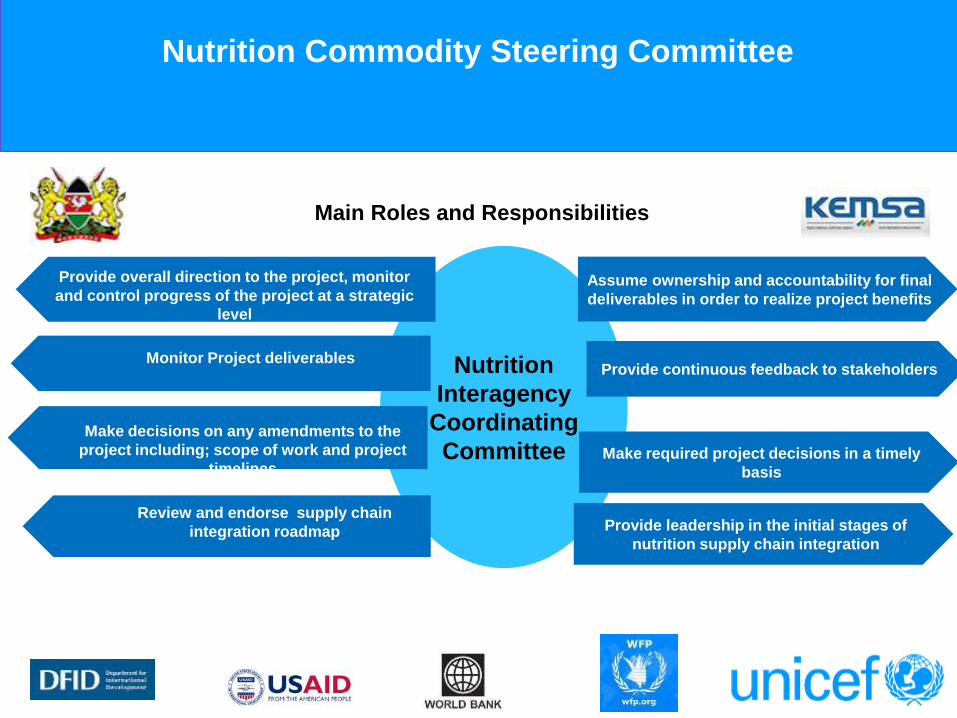
Nutrition Commodity Steering Committee
Nutrition
Interagency
Coordinating
Committee
Review and endorse supply chain
integration roadmap
Provide overall direction to the project, monitor
and control progress of the project at a strategic
level
Monitor Project deliverables
Make decisions on any amendments to the
project including; scope of work and project
timelines
Assume ownership and accountability for final
deliverables in order to realize project benefits
Provide continuous feedback to stakeholders
Make required project decisions in a timely
basis
Provide leadership in the initial stages of
nutrition supply chain integration
Main Roles and Responsibilities
WAY FORWARD ON INTEGRATION PROCESS
• Enhance M&E as a way to significantly increase transparency in the supply chain and enable a quicker response to fluctuations in demand – focus on capacity of county teams
• Support the scale up LMIS to facilitate ease in order management including order placement and reporting
• MoH, UNICEF and KEMSA and other partners to sign off on agreed KPIs that will be reviewed quarterly to monitor progress
• Integrate other partners on an ongoing basis through a national MoH led process
• Use ands regularly update the Master Facility List as provided by MoH
• Ensure and invest in adequate storage that is safe and secure for these commodities
@UNICEF/Kenya/20
11
ASANTE SANA!
THANK YOU!