ntsb and osa acoem 2014 · 3/28/14 2 evaluation of osa accident investigation cumulative level of...
TRANSCRIPT

3/28/14
1
Obstructive Sleep Apnea and
Fatal Transportation Accidents
1
Mary Pat McKay, MD, MPH Chief Medical Officer
Disclosure
• Nothing to disclose
2
Outline • Relationship between fatigue and
accident risk • Investigation of sleep and fatigue
after a fatal accident • Current state of NTSB’s OSA
recommendations
3
Why should the NTSB care?
OSA causes extreme daytime sleepiness; the affected individual can be observed to fall asleep within a few minutes in a quiet or monotonous environment.
4
OSA Transportation Risks
• Up to 7-fold increase in the risk of a motor vehicle crash • Falling asleep • Fatigue-related decrements in
psychomotor and cognitive function, particularly vigilance tasks
• Significant reduction of risk with CPAP 5
Multi-modal Problem • Marine:
• Port Arthur, TX, January, 2010 • Rail
• Clarkston, MI, November, 2001 • Newton, MA, May 2008 • Red Oak, IA, April, 2011
• Highway • Memphis, TN, April, 2002 • Miami, OK, June, 2009
• Aviation • Hilo, Hawaii, February, 2008

3/28/14
2
Evaluation of OSA Accident Investigation Cumulative Level of Fatigue
• Length and timing of sleep opportunities
• Circadian rhythm • Medical conditions & treatments • Family sleep issues • Personal stressors 8
11/15/2001 Clarkston, MI • Head on freight train collision, ~ 5:45am • Engineer
• Working 7:30 pm – 8:40 am x 7 days • Hypertension • Diabetes • 1998: ENT evaluation for snoring, daytime
somnolence – failed to follow up • Known for falling asleep
9
2001 Clarkston, MI
• Conductor • Night before worked at 11:30pm
• Home at 11:30am • Called at 5:30pm to return to work at 7:30pm
• Diabetes • Being treated for obstructive sleep apnea
10
Clarkston: Probable Cause
Due to the engineer’s untreated and the conductor’s insufficiently treated obstructive sleep apnea
11
WPR09LA016: Parowan, UT
• Heisler Lancair Legacy • 59 year old pilot
• >4,400 hours • ATP single engine • Commercial multi-engine, rotor, balloon
• 2nd class medical certificate • Gout, high cholesterol
12

3/28/14
3
Parowan, UT
• Low altitude after take off • Objects flew out during left turn
• Clothing item(s) retrieved • Likely canopy opened
• Turn continued into the ground
13
Medical issues
• Moderate-severe hypertension • Multiple medications
• Lumbar disc disease • Coronary artery stenosis
• 100% LAD; collateralized • Told FAA “precautionary” angiogram
was “normal” 14
Toxicology: Blood • ACETAMINOPHEN (Tylenol)
• 10.01 ug/ml
• DIAZEPAM (Valium) • 0.055 ug/ml (Low 0.1480) • 0.094 ug/ml NORDIAZEPAM
• HYDROCODONE (Vicodin, Lorcet, Norco) • 0.152 ug/ml (High 0.050) • 0.031 ug/mL DIHYDROCODEINE
• TRAMADOL (Ultram) • 0.428 ug/mL (High 0.500)
15
? Obstructive sleep apnea?
• Obese: BMI = 33.8 • Hypertension • Enlarged right heart • Benzodiazepines (50%) • Coronary artery disease
16
Probable Cause
• Failed to secure canopy • Unable to respond to emergency
successfully • Contributing:
• Impairing prescription medications • Possible fatigue from OSA
17
NTSB Recommendations on OSA
• By mode: • 7 Marine • 4 Aviation • 2 Highway • 5 Rail
• Topics: • Educate operator • Educate examiner • Ask for existing diagnosis • Ask for symptoms/screen • Treat/ensure adequate
treatment
18

3/28/14
4
Outcomes from NTSB OSA Recommendations
• Aviation • AME’s educated since
2008 • No increase in the rate
of OSA diagnosis
• Marine • Some educational
materials • Exam form asks
• Rail • Education performed • No medical required
• Highway • Exam form asks • “Recommendations”
19

3/28/14
1
Sleep Apnea Transportation Concerns and the
Science Behind Testing and Treatment
Natalie P. Hartenbaum, MD, MPH, FACOEM
Session 207: Monday, April 28, 2014
� None with respect to topic discussed
Disclosures
Agenda
� Dr. Hartenbaum - Introduction 8:30 – 8:35
� Dr. McKay - Findings, and recommendations from NTSB with regards to OSA - 8:35 – 9:10
� Dr. Gurubagavatula- Crash Risk and OSA, treatment and diagnosis – 9:10 – 9:45
� Dr. Hartenbaum - Current status of OSA in Highway and other transportation mode – 9:45 – 10:00
FAA and OSA
� Federal Air Surgeon’s Medical Bulletin
� “New” policy on OSA � “OSA is almost universal in obese individuals who
have a Body Mass Index (BMI) over 40 and a neck circumference of 17 inches or more,”
� FAA will be requiring Aviation Medical Examiners (AMEs) to calculate the Body Mass Index (BMI) of all airmen and ATCS.
� Airman applicants with a BMI of 40 or more would need to be evaluated by a board certified sleep specialist.
FAA and OSA � “New” policy on OSA
� Any airmen diagnosed with OSA would have to be treated prior to being medically certified.
� The testing will be expanded to ATCS shortly and once all airmen with BMI >40 are evaluated, the BMI threshold for evaluation will be lowered until “we have identified and assured treatment for every airman with OSA.” Additional details will be included in the AME Guide.
FAA and OSA � Pushback on this policy -so delay and review
� Bill introduced in the U.S. House of Representatives (H.R. 3578) - require the FAA to go through the rulemaking process before implementing new policies regarding sleep disorders
3/28/14
2
FRA and OSA Safety Advisory 2004-04: � FRA recommended:
� Railroads and representatives of employees, working together, take the following actions to promote the fitness of employees in safety-sensitive positions:
(1) Establish training & educational programs about fatigue and sleep disorders .....
(2) Ensure that employees' medical examinations include assessment and screening for possible sleep disorders and other associated medical conditions
FRA and OSA Safety Advisory 2004-04:
(3)Develop and implement rules that request employees in safety sensitive positions to voluntarily report any sleep disorder that could incapacitate, or seriously impair, their performance.
(4) When a railroad becomes aware that an employee in a safety sensitive position has an incapacitating or performance-impairing medical condition related to sleep, the railroad prohibits that employee from performing any safety-sensitive duties until that medical condition appropriately responds to treatment
FRA and OSA
(5) Implement policies, procedures, and any necessary agreements to–
(a) Promote self-reporting of sleep-related medical conditions by protecting the medical confidentiality of that information and protecting the employment relationship, provided that the employee complies with the recommended course of treatment;
(b) Encourage employees with diagnosed sleep disorders to participate in recommended evaluation and treatment; and
(c) Establish dispute resolution mechanisms that rapidly resolve any issues regarding the current fitness of employees who have reported sleep-related medical conditions and have cooperated in evaluation and prescribed treatment.
Is Sleep Apnea disqualifying? FMCSA - FAQ � Drivers should be disqualified un8l the diagnosis of sleep apnea has been ruled out or has been treated successfully.
� As a condi8on of con8nuing qualifica8on, it is recommended that a CMV driver agree to con8nue uninterrupted therapy such as CPAP, etc. / monitoring and undergo objec8ve tes8ng as required.
� A driver with a diagnosis of (probable) sleep apnea or a driver who has Excessive Day8me Somnolence(EDS) should be temporarily disqualified un8l the condi8on is either ruled out by objec8ve tes8ng or successfully treated.
10
11
Respiratory – Chronic Sleep Disorders ME Handbook
� Wai8ng period � Minimum — 1 month aPer star8ng CPAP � Minimum — 3 months symptom free aPer surgical treatment
� Maximum cer8fica8on — 1 year

3/28/14
3
Respiratory – Chronic Sleep Disorders ME Handbook � Recommend to cer8fy if the driver has: � Successful nonsurgical therapy with:
� Mul8ple sleep latency tes8ng values within the normal range. � Resolu8on of apneas confirmed by repeated sleep study during
treatment.
� Con8nuous successful nonsurgical therapy for 1 month.
� Compliance with con8nuing nonsurgical therapy. � Resolu8on of symptoms following comple8on of post-‐surgical wai8ng period.
Respiratory – Chronic Sleep Disorders ME Handbook
� Recommend not to cer+fy if the driver has: � Hypoxemia at rest. � Diagnosis of: � Untreated symptoma8c OSA. � Narcolepsy. � Primary (idiopathic) alveolar hypoven8la8on syndrome.
� Idiopathic central nervous system hypersomnolence. � Restless leg syndrome associated with EDS
Respiratory – Chronic Sleep Disorders ME Handbook
� The driver who is being treated for sleep apnea should remain symptom free and agree to: � Con8nue uninterrupted therapy. � Undergo yearly objec8ve tes8ng (e.g., mul8ple sleep latency test or maintenance of wakefulness test)
� Self-‐Reported Sleepiness Surveys � NOTE: Self-‐reported sleepiness does NOT always correlate with objec8ve tes8ng (polysomnography). The driver may not perceive sleepiness as excessive or may be hesitant to disclose sleepiness.
FMCSA and Obstructive Sleep Apnea • FMCSA Medical Expert Panel - 2007
• FMCSA Medical Review Board – 2007/2008
• Motor Carrier Safety Advisory Committee/Medical Review Board – 2012
• NPRM on CMV Operators and OSA – April 2012 • withdrawn days later
Non-FMCSA Recommendations
� 2006 Tri-Medical Society Task Force
Obstructive Sleep Apnea Non-FMCSA Recommendations
� All look at BMI as primary criteria for screening � Risk factors/Objective data as additional
consideration
� All indicate that dental appliance, positional sleeping, are not acceptable treatment
� All require objective measures of compliance
� All require annual certification AFTER evidence of compliance
3/28/14
4
Obstructive Sleep Apnea Non-FMCSA Adopted Guidance
� Conditional certification or disqualification depends on risk
� Disqualify
� Diagnosed with OSA but not compliant or treated
� Fall asleep crash without evaluation
� Report excessive sleepiness while driving
� S/P surgery pending three-month post-operative evaluation (UPPP) or 6 month (Bariatric)
� Not in MRB/MCSAC
OSA and CMV Operator Bill
� "any new or revised requirement providing for the screening, testing, or treatment of individuals operating commercial motor vehicles for sleep disorders is adopted pursuant to a rulemaking proceeding”.
� This does not require that a regulation or standard be promulgated nor does it prohibit guidance, only that any REQUIREMENT be adopted through rule making. � Guidance issued by the FMCSA is not a requirement.
� FMCSA indicated that whether the agency pursues guidance or rulemaking will be addressed through the notice and comment process
OSA Current Status
� Only REQUIREMENT is what is in the regulation � 391.41(b)(5) Has no established medical history or
clinical diagnosis of a respiratory dysfunction likely to interfere with his/her ability to control and drive a commercial motor vehicle safely;
� ME Handbook is guidance
� Examiners should utilize current best practice
� So no change in what examiner and carriers should do
� Will only delay guidance/requirement from FMCSA http://www.nafmp.org/en/
NAFMP Training Modules What Examiners Should NOT Do
FMCSA and other agencies have agreed that doing nothing is not the correct approach

3/28/2014
1
Sleep Apnea and Transportation: Concerns and Science
Monday, April 28, 2014
Indira Gurubhagavatula, MD, MPHAssociate Professor
Director, Occupational Sleep MedicinePerelman School of Medicine, University of Pennsylvania
Director, Sleep Disorders Clinic, Philadelphia VA Medical Center
Philadelphia, PA
� Principal investigator
� Two research studies in commercial drivers regarding sleep apnea identification
▪ FMCSA (2002)
▪ NIOSH/CDC (2011)
� Perioperative management of sleep apnea
▪ loan of equipment from ResMed, Inc.
▪ loan of software from Fusion Sleep� Advisor to FMCSA in revising recommendations on OSA
screening
� OSA and crash risk
� Testing
� Subjective versus objective
� Home sleep testing versus in-lab polysomnography
� Treatment
� CPAP versus other modes
COMMERCIAL DRIVERS
FMCSA AUSTRALIA STANFORD SCHNEIDER
28% 60% 78% 80%
Pack et al: FMCSA Pub. #DOT-RT-02-030,Washington, DC, 2002
Howard et al: AJRCCM (170):1014, 2004
Stoohs et al, Chest (107):1275, 1995Berger, JOEM 54:1017, 2012
Source Study sample Risk group Odds of
crash
Truck
drivers
FMCSA N=406 with PSGs;
MCMIS crash data
Severe apnea versus
no apnea
OR = 4.6
(severecrash)
Australia,
2004
2,342 w/OSA sx
and crash hx, + 161 w/PSGs
MAP score >= 0.5 and
ESS >= 11
OR= 1.3,
95% CI (1.0-1.69)
California,
1994
N=90; MESAM IV
(HST), sleep logs
ODI3%>=10/hour;
BMI>=30/hour; sleepiness
RR=2.0
Truck
+ car drivers
Meta-
analysis
18 studies; 2 in
truck drivers
Severe OSA (n.s.),
higher BMI; sleepiness
reporting less reliable
OR=
1.21 -4.89
http://www.fmcsa.dot.gov/facts-research/research-technology/report/FMCSA-RT-04-008.pdf
Tregear et al, JCSM 2009, Dec 15 5(6); 573-581.
9 studies of crash risk in OSA patients showed that after treatment with CPAP:
� Crash risk dropped▪ risk ratio = 0.278, 95% CI: 0.22 to 0.35; P < 0.001
� Daytime sleepiness improved after one night� Simulated driving performance improved within
2-7 days
Tregear, Sleep, 33(10):1373, 2010
funded by FMCSA GS-10F-0177N/DTMC75-06-F-00039

3/28/2014
2
� OSA and crash risk
� Testing
� Subjective versus objective
� Home sleep testing versus in-lab polysomnography
� Treatment
� CPAP versus other modes
Parks, 2009 Average AHI 49/hour � Average Epworth 3.3AHI 104 � Epworth 1 AHI > 30 � normal Epworth for all but one
Talmage, 2008 187 at high risk by exam criteria, but none marked “yes” on CDME form
Berger, 2012 AHI 164, Epworth 2
Dagan, 2006 78% had OSAnone admitted to snoring or sleepiness
USE OBJECTIVE DATA (BMI, NECK SIZE, BLOOD PRESSURE, HST, PSG)
� In-lab polysomnography (PSG)� Expensive
� Requires attendance by technologist
� Wait time
� “Gold” standard
� Unattended/home sleep testing (HST)� Inexpensive
� Self-assembled
� Shorter wait time
� Abridged
• Brain waves
• Eye movement
• Chin, leg muscles
• Chest and abdomen
effort
• Airflow, snoring
• Oxygen level
85% of cases remain undiagnosed
Brain waves
Eye movement
Chin, leg muscles
• Chest and abdomen
effort
• Airflow, snoring
• Oxygen level
http://www.fette-thimm.de/img/embletta400.jpg
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy

3/28/2014
3
� Best for confirming sleep apnea if high pre-test
probability
(obese, large neck, suggestive symptoms, hypertension)
� Inappropriate for other sleep disorders
� Movement disorders (PLMS, RBD), seizures, alpha
intrusion, frequent arousals
� Sleep time is not measured � can miss apnea
� Cannot score arousal-related hypopneas
� May over-estimate sleep
� Provide confirmatory PSG, or have a
relationship with an AASM-accredited sleep lab
� Adequate follow up and care at AASM-
accredited center
http://www.aasmnet.org/ocststandards.aspx
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy
� Minimum: airflow, respiratory effort and
SaO2� Use the same biosensors, sampling frequency
and filter settings used for in-lab PSG
� Trained sleep technologists apply the sensors or educate patients on how to do so
� Perform in an accredited, comprehensive
sleep medicine program with written policies and procedures
AASM Portable Monitoring Task Force J Clin Sleep Med 2007http://www.aasmnet.org/ocststandards.aspx

3/28/2014
4
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy
� Data loss when conducted unattended, out of specialized sleep centers:� 3-18% for type 3 monitors � 7-10% for type 4 monitors
� 7% if technologist applies sensor, 33% if independent
� Pre-programmed start/stop features reduce loss
AASM recommends trained sleep technologists apply the sensors or educate patients on how to do so.
For out-of-center accreditation, must track data loss rates
AASM Portable Monitoring Task Force J Clin Sleep Med 2007http://www.aasmnet.org/ocststandards.aspx
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy
� Manual scoring � gives better agreement with PSG for mild to moderate OSA.
� Automated scoring � proprietary algorithms, not uniform
� may or may not be using all the recorded signals
� may provide results even if signal quality is poor
� may score events that are not there or miss those that are
AASM Recommendations: � all portable devices allow viewing of raw data, manual scoring
or editing of automated scoring
� trained and qualified sleep technologist should score
� Systems that rely solely on automated scoring cannot be recommended
AASM Portable Monitoring Task Force J Clin Sleep Med 2007
No similar criteria exist for unattended studies.What should the threshold be to exclude a case of sleep apnea?
AHI (events/h) Severity
0 - 5 absent
5 - 15 mild
15 - 30 moderate
>= 30 severe
AASM, Sleep, 1999
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy

3/28/2014
5
� Chain of custody solutions
� Are systems in place to confirm that unattended
portable monitors are being used on the intended subject?
Use of Type 2 studies (EEG)Technologist sets up and takes down
Deterrent letter
Securing sensors to patient with
“sticky labels” or tape
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy
� High pretest
probability of moderate to severe OSA
� Ability to comply with instructions
� No acute
mental/physical health issues
� Infection (MRSA) –
need to disinfect
� Not looking for other
sleep disorders� In-laboratory PSG is
not possible due to
shift work/scheduling� To monitor the
response to other
treatments (CPAP, intraoral device, surgery)
AASM Task Force, 2007
� Indications
� Sensor heterogeneity� Data Loss
� Scoring
� Data Integrity� Candidacy
� They are best used in combination with
clinical criteria
� Patients with high-pretest probability
▪ NC, BMI, age, gender
� Symptom data less useful in occupational settings
� Unattended studies more useful for
confirming moderate/severe cases rather
than excluding mild cases
Sleep 2012; 35(11): 1491-1501JCH 2013; 15:279-288
AJRCCM 2004; 170:370-376
3/28/2014
6
Low AHI on an unattended sleep study may need in-lab
confirmation
Affiliation with AASM-accredited sleep lab for back-up
PSG is important.
� OSA and crash risk
� Testing
� Subjective versus objective
� Home sleep testing versus in-lab polysomnography
� Treatment
� CPAP versus other modes
� CPAP preferred� FMCSA: requirement for CPAP if AHI >= 20/hour
on an in-lab PSG
� Not clear what threshold should be for HST
� If AHI<20, can try other modes� Dental appliance
� Upper airway surgery (need to retest at 3 months)
Caveat: sleep apnea can be severe even if AHI is low.
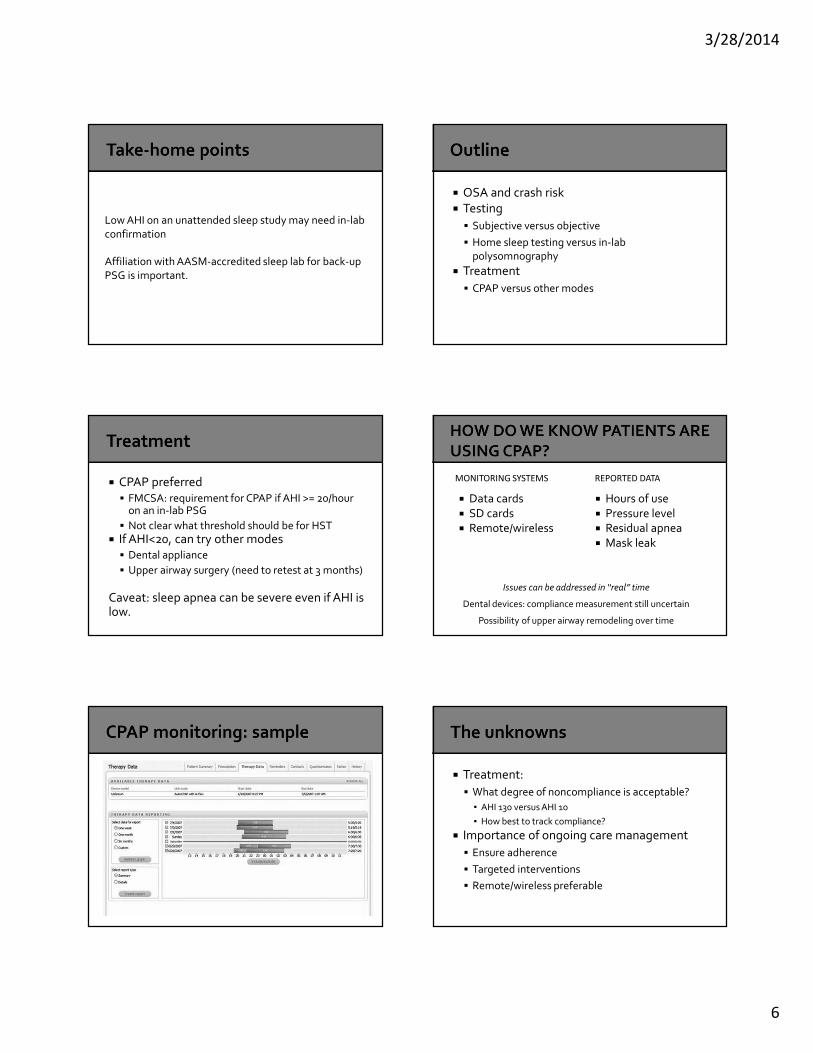
� Data cards
� SD cards� Remote/wireless
� Hours of use
� Pressure level� Residual apnea
� Mask leak
Issues can be addressed in “real” time
Dental devices: compliance measurement still uncertain
Possibility of upper airway remodeling over time
MONITORING SYSTEMS REPORTED DATA
� Treatment:
� What degree of noncompliance is acceptable?
▪ AHI 130 versus AHI 10
▪ How best to track compliance?
� Importance of ongoing care management
� Ensure adherence
� Targeted interventions
� Remote/wireless preferable

3/28/2014
7
� Be aware of chain of custody issues� If HST is negative, consider repeat testing (PSG)
� Ensure that program offers follow up care after testing
� FMCSA recommends � CPAP if AHI >= 20/hour� If AHI < 20/hour, consider dental appliance or surgery
based on severity of disease
Emphasis must be on ongoing management to ensure compliance and assess treatment response