november 2007 - eprints.qut.edu.au · fever management information was learnt from numerous...
TRANSCRIPT
i
Queensland University of Technology
School of Nursing
Faculty of Health
Institute of Health and Biomedical Innovation
Parents’ Management of Childhood Fever
Anne Majella Walsh
RN, EM, Dip App Sci, BA, Grad Dip HProm, MHSc
This thesis is submitted to fulfil the requirements for
degree of Doctor of Philosophy at the
Queensland University of Technology
November 2007

ii
iii
KEY WORDS Childhood illness; child nursing; community care, decision making; evidence-based
practice; fever; focus groups; general paediatrics; health education; information
needs; instrument development; literature review; medications; medication
management; parental attitudes; parenting; public health nursing; subjective norms;
Theory of Planned Behavior.
iv
ABSTRACT
Despite decades of research about educational interventions to correct parents’
childhood fever management their knowledge remains poor and practices continue to
be based on beliefs about harmful outcomes. The purpose of this thesis was to 1)
identify Australian parents’ fever management knowledge, attitudes, practices and
methods of learning to manage fever and 2) undertake a theoretical exploration of the
determinants of parents’ intentions to reduce fever using the Theory of Planned
Behavior (TPB). Two studies were undertaken: a qualitative study with 15 parents;
and survey of 401 Queensland parents with a child aged between 6 months and 5
years.
Parents determine childhood fever through behavioural changes they have learnt to
associate with fever. Few were aware of the immunological beneficial effects
associated with fever and most believed fever harmful causing febrile convulsions
and brain damage. To prevent harm they monitored temperatures, used antipyretics,
dressed children in light clothing and sponged them with tepid, cool or cold water.
Despite believing antipyretics harmful most parents reduced temperatures of 38.3°C
± 0.6ºC with antipyretics, alternating two antipyretics when fever was not reduced or
returned. In addition to temperature reduction antipyretics were used to reduce
distress or general unwellness and pain or discomfort. Multiple factors were used to
determine antipyretic dosage including temperature, irritability and illness severity.
Over one-third of parents had overdosed their child with too frequent antipyretic
administration; more frequently with ibuprofen than paracetamol, 12:1.
v
Fever management information was learnt from numerous sources. Doctors were the
most frequently reported followed by personal experience. With the variety of
information sources nearly half received conflicting information about how to
manage fever increasing concerns and creating uncertainty about how to best care for
their child. Despite this many believed they knew how to manage fever.
Some parents’ practices changed over time as a result of either positive or negative
experiences with fever indicating more positive or negative attitudes toward fever.
Positive experiences reduced antipyretic and medical service use; negative ones had
the adverse effect with increase in antipyretic use including alternating antipyretics
and double dosing with one antipyretic. Child medication behaviours also influenced
attitudes and practice intentions. Parents of children who readily took antipyretics
had more negative attitudes and intended to reduce their child’s next fever with
antipyretics. Negative attitudes were a significant determinant of fever management
intentions.
Parents’ practices were strongly influenced by their perception that doctors and
partners expected them to reduce fever. This expectation from partners is
understandable; from doctors it is not and indicates doctors’ propensity to
recommend reducing fever. There is an urgent need to identify doctors’ fever
management beliefs and rationales for practice recommendations. Parents also learn
to manage fever from nurses and pharmacists; their beliefs and management
rationales must also be determined and addressed.
vi
There is an urgent need to educate parents about evidence-based fever management
and reduce their unnecessary antipyretic use. They must be encouraged to delay
antipyretic administration using them to reduce pain rather than fever. Findings from
this thesis have identified the determinants of parents’ intentions to reduce fever;
negative attitudes and normative influences and positive child medication
behaviours. Future studies should examine the efficiency and cost effectiveness of
fever management educational programs for parents using different presentation
methods in multiple settings.
vii
TABLE OF CONTENTS
Key words iii
Abstract iv
Table of Contents vii
Table of Tables xii
Table of Figures xii
Declaration of Authorship xiii
Glossary of Acronyms and Terms xv
Publications Arising from the Research Program xvi
Conference Papers Arising from the Research Program xvii
Funding Attracted by the Research Program xviii
Examples of Media Interest Arising from the Research Program xix
Acknowledgements xx
CHAPTER 1 – INTRODUCTION AND SIGNIFICANCE OF THE STUDY 1
1.1 Introduction 1
1.2 Parents and Childhood Fever 1
1.2.1 Childhood Fever 2
1.2.2 Parents’ Fever Management 3
1.3 Health Professionals and Childhood Fever Management 6
1.4 Febrile Convulsions 7
1.5 Theoretical Framework 8
1.6 Thesis Outline 9
1.7 Purpose 10
1.8 Aims 11
1.9 Research Questions 11
1.10 Hypotheses 12
1.11 Summary 13
CHAPTER 2 – BACKGROUND 15
2.1 Introduction 15
2.2 Thermoregulation 15
2.2.1 Fever 16
2.2.2 Phases of Fever 21
2.2.3 Benefits of Fever 22

viii
2.3 Fever in Children 23
2.3.1 Febrile Convulsions 27
2.3.2 Antipyretics 35
2.3.3 Management of Childhood Fever 43
2.3.4 Health Professionals and Childhood Fever 46
2.4 Summary 47
CHAPTER 3 – PARENTS AND FEVER 49
3.1 Article – Management of Childhood Fever by Parents: Literature Review 50
3.1.1 Introduction 52
3.1.2 Search Method 53
3.1.3 Findings 54
3.1.4 Discussion 68
3.1.5 Conclusions 70
3.1.6 References 73
3.2 Summary of the Literature Review 79
3.3 Need for a Theoretical Framework 79
3.3.1 Determining a Theory 80
3.4 Theory of Planned Behavior 81
3.4.1 Applications of the Theory of Planned Behavior 85
3.5 Summary 87
CHAPTER 4 – METHODS 89
4.1 Introduction 89
4.2 Needs Assessment 90
4.3 Study Aims 92
4.4 Research Plan 93
4.4.1 Study1 – Focused Discussions 94
4.4.2 Study 2 – Survey 101
4.5 Summary 116
CHAPTER 5 – STUDY 1 117
5.1 Introduction 118
5.1.1 Literature Review 119
5.1.2 Aims 120
5.2 Method 121
5.2.1 Study Design 121

ix
5.2.2 Sample 121
5.2.3 Focused Questions 122
5.2.4 Recruitment and Procedure 122
5.2.5 Data Analysis 124
5.3 Findings 124
5.3.1 My Child has a Fever 124
5.3.2 Fever is Beneficial 125
5.3.3 High Fever is Harmful 126
5.3.4 Influencing Factors 127
5.3.5 Learning to Manage Fever 132
5.3.6 Managing Fever 133
5.3.7 Need for Timely, Consistent Information 134
5.4 Discussion 135
5.4.1 Influence of Beliefs 135
5.4.2 Influence of Parental Role 136
5.4.3 Influence of Experience 137
5.4.4 Influence of Knowledge 138
5.4.5 Implications for Health Professionals 138
5.4.6 Strengths and Limitations 139
5.5 Conclusions 139
5.6 Acknowledgments 139
5.7 Funding 140
5.8 References 140
CHAPTER 6 – STUDY 2 – DESCRIPTIVE FINDINGS 144
6.1 Article 1 – Underpinned by fear: a community study of parents’ fever management with young children
145
6.1.1 Introduction 147
6.1.2 The Study 150
6.1.3 Results 155
6.1.4 Discussion 166
6.1.5 Conclusions and Recommendations 171
6.1.6 Acknowledgements 172
6.1.7 References 172
6.2 Article 2 – Over-the-counter medication use for childhood fever: a crossectional study of Australian parents
177
6.2.1 Introduction 179
6.2.2 Methods 180
x
6.2.3 Results 184
6.2.4 Discussion 189
6.2.5 Acknowledgements 193
6.2.6 References 194
6.3 Summary 196
CHAPTER 7 – DETERMINANTS OF PARENTS’ INTENTIONS TO REDUCE FEVER
198
7.1 Introduction 198
7.1.1 Theoretical Framework 199
7.2 Hypotheses for the Fever Model 201
7.3 Hypotheses for the Medication Model 204
7.4 Approach to Analysis 206
7.5 Model Estimation 208
7.6 Assessing Model Fit 209
7.6.1 Chi-square Goodness-of-fit Statistic 209
7.6.2 Goodness-of-fit Index 210
7.6.3 Adjusted Goodness-of-fit Index 211
7.6.4 Comparative Fit Index 211
7.6.5 Root Mean Square Error Approximation 211
7.7 Preparation of Data for Analysis 212
7.7.1 Management of Missing Data 213
7.7.2 Univariate Normality Testing 213
7.7.3 Issues Due to Nonnormality 214
7.8 Results 216
7.8.1 Bivariate Exploration of Demographics 216
7.8.2 Demographics 216
7.8.3 Parents’ Intentions to reduce their Child’s next Fever 218
7.8.4 Parents’ Intentions to reduce their Child’s next Fever with Medications
238
7.8.5 Integration of Findings 254
7.8.6 Strengths and Limitations 257
7.8.7 Conclusions 258
CHAPTER 8 – INTEGRATION OF FINDINGS AND CONCLUSIONS 261
8.1 Introduction 261
8.2 Integrating of Key Findings 262
8.3 Theoretical Implications 270
xi
8.4 Strengths and Limitations 273
8.5 Practice Implications 276
8.5.1 Parents 276
8.5.2 Doctors and Other Health Professionals 279
8.6 Implications for Future Studies 281
8.6 Overall Conclusions 284
Appendix 1 – Study 1 Documents 287
Appendix 2 – Study 2 Documents 295
Appendix 3 – Statements of author co-contributions to manuscripts 325
Appendix 4 – Conference abstracts 330
Appendix 5 – Media interest arising from the research program 337
References 385
xii
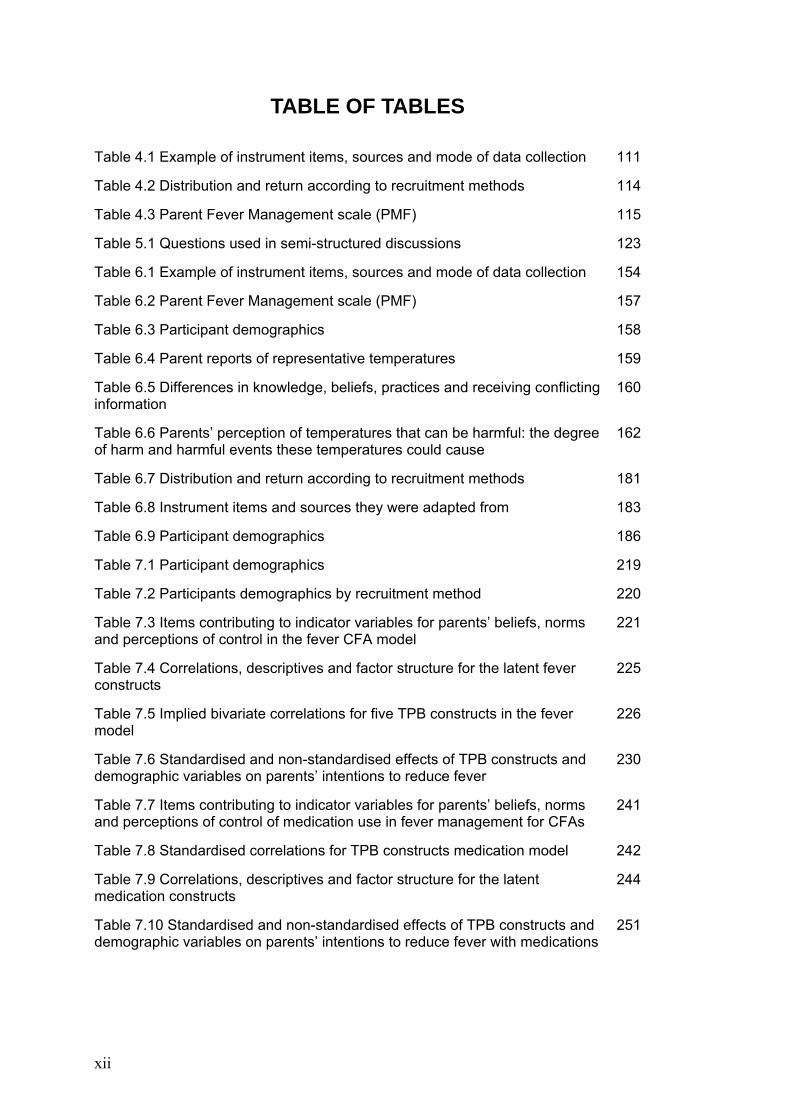
TABLE OF TABLES Table 4.1 Example of instrument items, sources and mode of data collection 111
Table 4.2 Distribution and return according to recruitment methods 114
Table 4.3 Parent Fever Management scale (PMF) 115
Table 5.1 Questions used in semi-structured discussions 123
Table 6.1 Example of instrument items, sources and mode of data collection 154
Table 6.2 Parent Fever Management scale (PMF) 157
Table 6.3 Participant demographics 158
Table 6.4 Parent reports of representative temperatures 159
Table 6.5 Differences in knowledge, beliefs, practices and receiving conflicting information
160
Table 6.6 Parents’ perception of temperatures that can be harmful: the degree of harm and harmful events these temperatures could cause
162
Table 6.7 Distribution and return according to recruitment methods 181
Table 6.8 Instrument items and sources they were adapted from 183
Table 6.9 Participant demographics 186
Table 7.1 Participant demographics 219
Table 7.2 Participants demographics by recruitment method 220
Table 7.3 Items contributing to indicator variables for parents’ beliefs, norms and perceptions of control in the fever CFA model
221
Table 7.4 Correlations, descriptives and factor structure for the latent fever constructs
225
Table 7.5 Implied bivariate correlations for five TPB constructs in the fever model
226
Table 7.6 Standardised and non-standardised effects of TPB constructs and demographic variables on parents’ intentions to reduce fever
230
Table 7.7 Items contributing to indicator variables for parents’ beliefs, norms and perceptions of control of medication use in fever management for CFAs
241
Table 7.8 Standardised correlations for TPB constructs medication model 242
Table 7.9 Correlations, descriptives and factor structure for the latent medication constructs
244
Table 7.10 Standardised and non-standardised effects of TPB constructs and demographic variables on parents’ intentions to reduce fever with medications
251
xiii
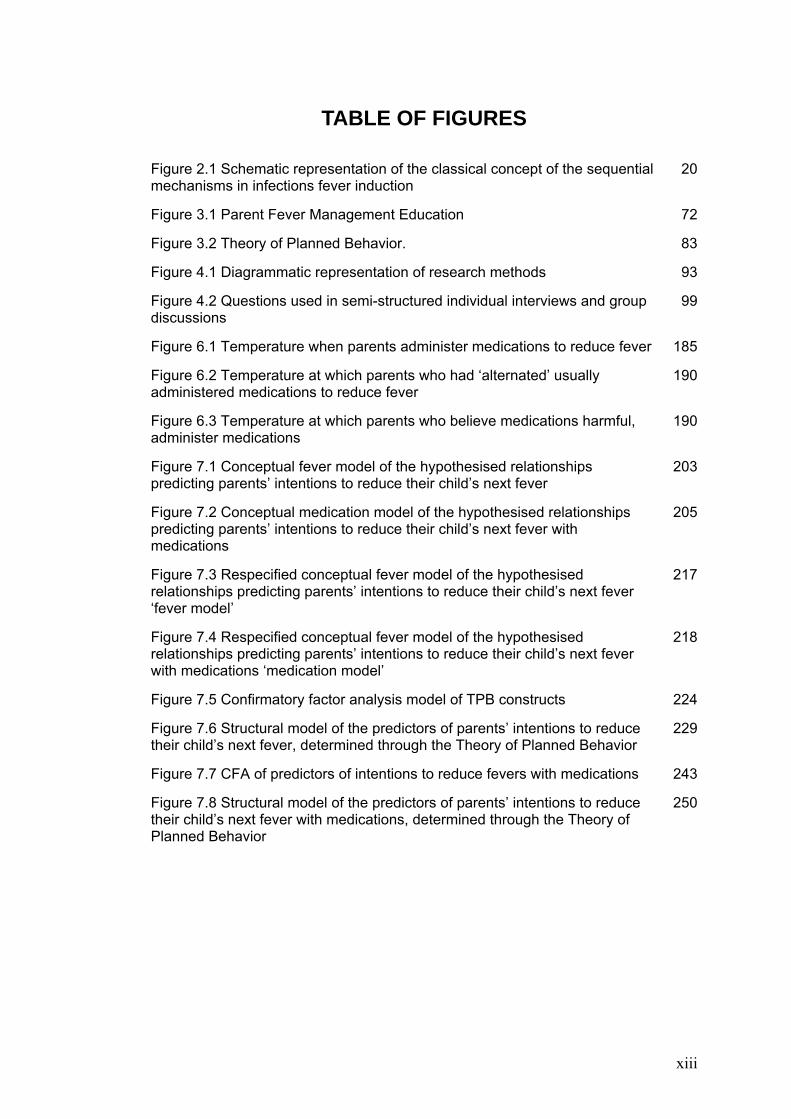
TABLE OF FIGURES Figure 2.1 Schematic representation of the classical concept of the sequential mechanisms in infections fever induction
20
Figure 3.1 Parent Fever Management Education 72
Figure 3.2 Theory of Planned Behavior. 83
Figure 4.1 Diagrammatic representation of research methods 93
Figure 4.2 Questions used in semi-structured individual interviews and group discussions
99
Figure 6.1 Temperature when parents administer medications to reduce fever 185
Figure 6.2 Temperature at which parents who had ‘alternated’ usually administered medications to reduce fever
190
Figure 6.3 Temperature at which parents who believe medications harmful, administer medications
190
Figure 7.1 Conceptual fever model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever
203
Figure 7.2 Conceptual medication model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever with medications
205
Figure 7.3 Respecified conceptual fever model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever ‘fever model’
217
Figure 7.4 Respecified conceptual fever model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever with medications ‘medication model’
218
Figure 7.5 Confirmatory factor analysis model of TPB constructs 224
Figure 7.6 Structural model of the predictors of parents’ intentions to reduce their child’s next fever, determined through the Theory of Planned Behavior
229
Figure 7.7 CFA of predictors of intentions to reduce fevers with medications 243
Figure 7.8 Structural model of the predictors of parents’ intentions to reduce their child’s next fever with medications, determined through the Theory of Planned Behavior
250
xiv
DECLARATION OF AUTHORSHIP The work contained in this thesis has not been previously submitted to meet
requirements for an award at this or any other higher education institution. To the
best of my knowledge and belief the thesis contains no material previously published
or written by another person except where due reference is made.
Signature ………………………………………… Date………………………………………………. Anne Walsh RN EM DipAppSci BA GradDipHProm MHSc
xv
GLOSSARY OF ACRONYMS AND TERMS TPB: Theory of Planned Behavior
PBC: Perceived Behavioural Control
PQ: Playgroup Queensland
CCC: Child Care Centre
ML: Maximum Likelihood
NC: Normed Chi-square-Square
GFI: Goodness-of-Fit Index
AGFI: Adjusted Goodness-of-Fit Index
AIC: Akaike Information Criterion
CFI: Comparative Fit Index
RSMEA: Root Mean Square Error of Approximation
CFA: Confirmatory Factor Analysis
SEM: Structural Equation Modelling
Health industry experience: people who had either education in a health profession
or had worked in a health setting
Antipyretics are medications with fever reduction properties, paracetamol and
ibuprofen
Medications are over-the-counter medications, antipyretics, used with childhood
fever, paracetamol and ibuprofen
xvi
PUBLICATIONS ARISING FROM THE RESEARCH PROGRAM
Walsh, A. M., & Edwards, H. E. (2006). Management of childhood fever by parents:
literature review. Journal of Advanced Nursing, 54(2), 217-227. Impact Factor 1.342
(This manuscript can be found in Chapter 3)
Walsh, A. M., Edwards, H. E., & Fraser, J. A. (2007 online early). Influences on
parents' fever management: beliefs, experiences and information sources. Journal of
Clinical Nursing. Impact Factor 1.430
(This manuscript can be found in Chapter 5)
Walsh, A. M., Edwards, H., & Fraser, J. (under review). Underpinned by fear: a
community study of parents' fever management with young children. Journal of
Advanced Nursing. Impact Factor 1.342
(This manuscript can be found in Chapter 6)
Walsh, A. M., Edwards, H. E., & Fraser, J. (in press 14th April 2007). Over-the-
counter medication use for childhood fever: a crossectional study of Australian
parents. Journal of Paediatrics and Child Health. Impact Factor 0.931
(This manuscript can be found in Chapter 6)
Walsh, A. M., Edwards, H. E., & Fraser, J. (2006). Predictors of parents' intentions
to reduce childhood fevers. International Journal of Behavioural Medicine,
13(Supp), 124. (Copy in Appendix 4)
xvii
CONFERENCE PAPERS ARISING FROM THE RESEARCH PROGRAM
Paper presented at the General Practice and Primary Health Care, Sydney, Australia, 2007:
Over-the-counter medication use for childhood fever: a crossectional study of Australian parents.
Paediatrics & Child Health Annual Meeting incorporated in the Royal Australian College of Physicians Annual Meeting, Melbourne, Australia, 2007:
Evidence-based management of uncomplicated pain and fever in children in the community setting. (Walsh third author)
23rd Quadrennial Congress of the International Council of Nurses, Taipei, Taiwan, 2005:
Febrile children: promoting evidence-based care by nurses and parents.
4th Annual Scientific Conference, Auckland, New Zealand, 2006:
Education based on the Theory of Planned Behavior promotes evidence-based fever management.
9th International Biennial Paediatric and Child Health Nurses Conference, Melbourne, Australia, 2006:
Parents' management of childhood fever - the need for evidence based education.
38th APACPH Conference 2006: Asia-Pacific Consortium for Public Health, Bangkok, Thailand, 2006:
Conflicting health information: Reducing fear and guilt for parents managing childhood fever.
9th International Congress of Behavioral Medicine, Bangkok, Thailand, 2006:
Predictors of parents' intentions to reduce childhood fevers. Poster presentation
23rd Quadrennial Congress of the International Council of Nurses, Taipei, Taiwan, 2005:
Febrile children: promoting evidence-based care by nurses and parents.
*The first author on seven of the eight conference papers was Walsh, A.M. (Abstracts in Appendix 4)
xviii
FUNDING ATTRACTED BY THE RESEARCH PROGRAM
Queensland University of Technology Postgraduate Research Award for three years
Financial assistance for the sum of:
Financial support received in the years 2004 to 2007
Institute of Health and Biomedical Innovation Queensland University of Technology
awarded for 3 years
Financial assistance for the sum of:
Confederation research funding was received for the purpose of data collection
Financial support received in the years 2005 to 2007
Australian Confederation of Paediatric and Child Health Nurses Margaret Sullivan
Scholarship
Financial assistance for the sum of:
Confederation research funding was received for the purpose of data collection
Financial support received in the year 2004
Royal College of Nursing Australia Joyce Wickham Scholarship
Financial assistance for the sum of:
Confederation research funding was received for the purpose of data collection
Financial support received in the year 2006
Grant in Aid
Financial assistance for the sum of:
Funding was received for the purpose of presenting papers at an international
conference
Financial support received in the year 2006
xix
EXAMPLES OF MEDIA INTEREST ARISING FROM THE RESEARCH PROGRAM
Parents overdose young Adelaide Advertiser, 07/04/06, General News, Page 7 Parents are overdosing children on painkillers Canberra Times, 07/04/06, General News, Page 3 Parents misusing fever medications Daily Advertiser, 07/04/06, General News, Page 8 Overdose fears Launceston Examiner, 07/04/06, General News, Page 4 Parents overdosing kids Newcastle Herald, 07/04/06, General News, Page 19 Parents feed kids too many drugs Queensland Times, 07/04/06, General News, Page 6 Parents overdose sick children West Australian, 07/04/06, General News, Page 5 Feverish kids can get too much of a good thing Sydney Morning Herald, 13/04/06, Health & Science, Page 3 Panicked parents unaware of medicine dangers Daily Telegraph, 10/04/06, General News, Page 13 ABC 720 Perth (Perth): Mornings - 06/04/06 09:24 Gillian O’Shaughnessy: Producer Ms Alicia Hanson 08 9220 2729 4BC (Brisbane): 08:30 News - 07/04/06 08:32 Newsreader: News Director Mr Steve Speziale 07 3908 8200 ABC 891 Adelaide (Adelaide): Drive - 07/04/06 04:18 Deb Tribe: Producer Mr Michael Ockerby 08 8343 4410 ABC 702 Sydney (Sydney): The World Today - 10/04/06 12:50 Eleanor Hall ABC North Coast NSW (Lismore): Afternoons - 12/04/06 02:51 Terry Sara: Station Phone 02 6627 2011
See Appendix 5 for more detail
xx
ACKNOWLEDGEMENTS
I wish to express my gratitude to Professor Helen Edwards for her guidance, support
and encouragement while undertaking and completing this thesis. I also wish to
express my gratitude to Doctor Jenny Fraser for her valuable input and
encouragement during the journey.
I would like to thank Doctor Helen Chapman and for her valuable assistance with
qualitative data analyses. I also thank Doctor Jan McDowell, Doctor Diana Battistuta
and Helen Skerman for their advice and statistical assistance during the journey.
Additionally, I would like to acknowledge the continued support and encouragement
from my fellow students and colleagues.
I thank all the parents who so generously gave of their time to participate in the
research. The Queensland University of Technology, Institute of Health and
Biomedical Innovation Australian Confederation of Paediatric Nursing and Royal
College of Nursing Australia and for their financial support in the form of
scholarships
Finally, I thank my family and friends for their support and encouragement. I
dedicate this thesis to my parents, Des and Peg Fitzgerald, and thank them for their
lifelong support and belief that I could achieve anything that I set out to.
1
CHAPTER 1
INTRODUCTION AND SIGNIFICANCE OF THE STUDY
1.1 INTRODUCTION This chapter provides an overview of the key issues and rationale for the thesis and
outlines the thesis structure. The chapter begins by introducing the reader to
childhood fever and parents’ fever management beliefs and practices. Following this
is an introduction to health professionals’ beliefs and practices then the influence of
febrile convulsions on parents and health professionals are briefly addressed. Then
theoretical framework that forms the basis of this thesis is identified and briefly
described. The chapter then mentions the research questions, hypotheses to be tested
and outlines briefly the contents of the following chapters.
1.2 PARENTS AND CHILDHOOD FEVER Despite more than three decades of literature supporting the beneficial effects of mild
to moderate fever parents continue to perceive fever as maladaptive and harmful
(Atkins, 1982; Impicciatore, Nannini, Pandolfini, & Bonati, 1998; Kluger, 1979;
Kluger, Ringler, & Anver, 1975; Lorin, 1990, 1999; Sarrell, Cohen, & Kahan, 2002;
Schmitt, 1984; Taveras, Durousseau, & Flores, 2004). Little has changed in parents’
fundamental management of fever during this period, they continue to monitor
fever’s progress and use antipyretic medications to reduce fevers, to prevent harmful
outcomes, despite recommendations to reduce the use of antipyretics (e.g., Al-Eissa,
Al-Sanie et al., 2000; Blumenthal, 1998; Kinmonth, Fulton, & Campbell, 1992;
Kramer, Naimark, & Leduc, 1985; May & Bauchner, 1992; Sarrell et al., 2002;
Schmitt, 1980; Weiss & Herskowitz, 1983). It is not always necessary to normalise a
child’s temperature during a febrile illness, however, pain or discomfort associated

2
with febrile illnesses should be reduced with analgesics (e.g., Knoebel, Narang, &
Ey, 2002; Lorin, 1999; Sadovsky, 2002; Sarrell et al., 2002). Unfortunately, the
common over-the-counter analgesics used for children, paracetamol and ibuprofen,
have antipyretic properties making this a complex issue for parents of febrile
children (eMIMS, 2007). To address this continuing problem it is imperative that
modifiable factors influencing parents’ negative beliefs about fever and inappropriate
practices are identified. Then programs can be developed to modify these factors and
promote the safe care for febrile children and over-the-counter medications use at
home. The overall aim of this research is to identify modifiable factors influencing
parents’ fever management.
1.2.1 Childhood Fever Fever is a common event during childhood and one of the most common reasons for
parents to seek medical advice with height of the fever generally the deciding factor
(Kelly, Morin, & Young, 1996; McErlean et al., 2001; Sarrell et al., 2002). During
the first two years of life children generally have between four and six febrile
episodes each year (McCarthy, 1999). These fevers are commonly a sign of self-
limiting viral infections although they signify serious illnesses in less than 10% of
cases and bacterial inflections in approximately 4% (Knoebel et al., 2002;
McCarthy). Parents (57%%) and health professionals, nurses (36%) and doctors
(14%), are concerned about fever with some parents (43%) perceiving the height of
fever an indicator of the severity of the illness (Lagerlov, Loeb, Slettevoll,
Lingjaerde, & Fetveit, 2006; Sarrell et al., 2002). However, in temperatures of 40°C
or less the temperature is more likely to be a sign of the body’s adaptive response to
the infectious process rather than the severity of illness (Blatteis, 2003;
VandenBosch, Lahaie, Rickelmann, & Gutridge, 1993). Fever does not always need
3
to be treated. However, fever should be reduced in children who would be placed at
risk from the increased physiological demands of fever, such as children with pre-
existing cardiac, respiratory and neurological conditions (Blatteis, 2006). Allowing
fever can assist in the accurate diagnosis of an illness and demonstrate a response to
antibiotics (Connell, 1997). Despite this and numerous educational programs over
the past two decades parents continue to administer antipyretics to febrile children
and alarmingly continue to be advised to do so by health professionals (e.g.,
Mayoral, Marino, Rosenfeld, & Greensher, 2000; Poirier, Davis, Gonzalez-del Rey,
& Monroe, 2000; Sarrell et al., 2002).
1.2.2 Parents’ Fever Management Fever is a source of considerable anxiety for parents; they perceive it to be harmful
(Knoebel et al., 2002) and seek advice from health professionals for self-limiting
viral infections. Parents’ concern about and inappropriate treatment of childhood
fever, is well documented and probably multifactorial (e.g., Knoebel et al., 2002;
Kramer et al., 1985; Purssell, 2000; Schmitt, 1980). Attitudes and beliefs about fever
management are influenced positively or negatively by parents’ past personal
experiences with febrile children (Poirier et al., 2000). Additional factors include
anecdotal tragic outcomes of febrile children, cultural influences and information
provided by family, friends, health professionals and other sources such as written
materials and the Internet (Poirier et al., 2000). Parents’ concerns about fever relate
to their lack of information about fever management, moderate fever in their child,
inexperience with managing febrile children and low maternal educational levels
(Crocetti, Moghbeli, & Serwint, 2001; Impicciatore et al., 1998; Singhi, Padmini, &
Sood, 1991).
4
Parents believe doctors are concerned about fever and that fevers are dangerous
(Crocetti et al., 2001). Beliefs that fever is harmful have risen since 1980 from 52%
(Schmitt, 1980) to 76% in 2001 (Crocetti et al., 2000). In 1980 parents were most
concerned about brain damage, febrile convulsions and delirium; in 2001 febrile
convulsions were the main concern followed by brain damage and death (Crocetti et
al., 2000; Schmitt, 1980). An indication of the strength of beliefs that fever is
harmful is the number of parents who would wake sleeping febrile children for an
antipyretic 79% to 93% (Crocetti et al., 2000; Schmitt, 1980). Studies exploring
parents’ definition of fever found parents define fever as temperatures ranging from
37.5ºC to 37.9ºC (Betz & Grunfeld, 2006; Karwowska, Nijssen-Jordan, Johnson, &
Davies, 2002); high fever as 38.9ºC to 39.1ºC (Karwowska et al.) and dangerous
fever 39.3ºC to 39.9ºC (Betz & Grunfeld, 2006; Karwowska et al., 2002). A number
of studies have sought to determine the prevalence of antipyretic administration and
temperature at which antipyretics are generally administered. Parents administer
antipyretics for temperatures as low as 37.8ºC to 38.2ºC (Betz & Grunfeld, 2006;
Crocetti et al., 2001; Karwowska et al., 2002; Sarrell et al., 2002) and base decisions
to reduce fever with antipyretics on temperature alone (Lagerlov et al., 2006). When
their child is febrile parents feel they need to do something, that they are not caring
appropriately for their child if they do not treat the fever (Impicciatore et al., 1998).
Aggressive antipyretic treatment of fever by parents remains common; incorrect
dosing and frequency of antipyretic administration is also common. For example, in
1993, 51% of parents administered paracetamol regularly throughout a 24-hour
period (Schnaiderman, Lahat, Sheefer, & Aladjem, 1993); 14% to 27% gave
paracetamol more frequently than fourth hourly and 33% to 50% gave ibuprofen at

5
less than six hourly intervals (Betz & Grunfeld, 2006; Crocetti et al., 2001).
Paracetamol can be administered fourth hourly and Ibuprofen sixth hourly (eMIMS,
2007). Although paracetamol is generally considered a safe medication there are
genuine concerns about hepatotoxicity in children 5 weeks to 10 years of age (e.g.,
Kearns, Leeder, & Wasserman, 1998; Knoebel et al., 2002; Miles, Kamath, Dorney,
Gaskin, & O'Loughlin, 1999; Murphy, 1992). Of most concern is that paracetamol
overdose can cause hepatic toxicity (eMIMS, 2007; Mahadevan, McKiernan, Davies,
& Kelly, 2006). Physicians (50%) recommending parents alternate antipyretics,
paracetamol and ibuprofen (Mayoral et al., 2000; Wright & Liebelt, 2007), can be
confusing for parents as different dosages and frequencies are recommended
(Goldman, 2006; Saphyakhajon & Greene, 2006; Schmitt, 2006). The practice of
alternating antipyretics has been blamed for increasing the probability of exposing
children to toxic levels of antipyretics (Knoebel et al.). Aggressive antipyretic use is
often an attempt, by parents and health professionals, to prevent febrile convulsions
and is a contributing factor to negative attitudes toward fever (e.g., Poirier et al.,
2000, Sarrell, et al., 2002; Schmitt, 2006) .
Since 1980, studies exploring parents’ knowledge of, attitudes toward and
management of fever have been conducted in United States (Schmitt, 1980), Canada
(Kramer et al., 1985) and Saudi Arabia (Abdullah, Ashong, Al Habib, Karrar, & Al
Jishi, 1987). During the 1990s studies were conducted in India (Singhi et al., 1991),
the United Kingdom (Blumenthal, 1998) and Italy (Impicciatore et al., 1998). In the
last decade there are reports of parents’ knowledge and attitudes from Israel (Sarrell
et al., 2002), Canada (Karwowska et al., 2002) the United States (Taveras et al.,
2004) and the United Arab Emirates (Betz & Grunfeld, 2006). Although studies have

6
been conducted in many countries there are some findings that differ. For example,
in Italy (Impicciatore et al.), the United States (Crocetti et al., 2001) and Canada
(Karwowska et al., 2002) more parents learn to manage fever from doctors than
family members. However in Saudi Arabia (Al-Eissa, Al-Zamil et al., 2000) parents
are equally likely to learn about fever from family, relatives, friends and doctors. No
published research identifies Australian parents’ fever management practices or their
sources of fever management information. In light of the continued concerns about
fever reported in the literature and the increase in antipyretic use with associated
incorrect dosing it is imperative that Australian parents’ fever management
knowledge, attitudes, practices and sources of information are identified. Then
educational programs can be developed to target specific modifiable factors such as
knowledge deficits; negative, inappropriate beliefs and unnecessary, unsafe practices.
1.3 HEALTH PROFESSIONALS AND CHILDHOOD FEVER MANAGEMENT There has been little change in health professionals’ negative attitudes toward fever
over the past decade (Sarrell et al., 2002; Walsh, Edwards, Courtney, Wilson, &
Monaghan, 2005). Health professionals continue to recommend fever reduction
strategies to prevent febrile convulsions and brain damage, reduce low grade fever
without other symptoms, waken sleeping febrile children for antipyretics and
administer a different antipyretic to children still febrile one hour following initial
antipyretic treatment (Abdullah et al., 1987, Poirier, et al., 2000; Sarrell, et al., 2002).
This is not surprising as the literature concerning the management of fever and
febrile convulsions is not consistent. For example, based on the evidence over the
past three decades many authors recommend supporting the role of fever in the
immunological response to an invading organism (e.g., Atkins, 1982; Duff, 1986;
7
Kluger, 1986; Lorin, 1990; 1994, 1999). Purssell (2000) advocates promoting
education, comfort and recovery rather than aggressive antipyretic therapy. On the
other hand, recommendations for nurses to advise parents to administration
paracetamol to feverish children and to continue this four to six hourly while fever is
present continue (e.g., Waterston, 2002). Parents learn to manage fever from health
professionals (Impicciatore et al., 1998; Karwowska et al., 2002) therefore health
professionals’ concerns and misconceptions about fever in addition to their overly
aggressive treatment of it contribute to parental fever phobia (e.g., May & Bauchner,
1992; Poirier et al.; Thomas et al., 1994; Weiss & Herskowitz, 1983).
1.4 FEBRILE CONVULSIONS Parents’ and health professionals’ concerns about febrile convulsions are well
documented (e.g., Huang, Liu, Huang, & Thomas, 2002; Miller, 1996; Rutter &
Metcalfe, 1978; Sarrell et al., 2002). Witnessing a febrile convulsion is a frightening
experience for parents, many of whom think their child is dying (e.g., Baumann,
2001; Purssell, 2000; Waterston, 2002). Some health professionals (11% to 22%)
report concerns about brain damage and death (6%) following a febrile convulsion
(Poirier et al., 2000; Thomas et al., 1994). Fears of the possibility of a febrile
convulsion have not only led to overaggressive treatment of fever by parents and
health professionals but have also increased parents’ anxiety and placed additional
strain on already limited community and acute health care resources through
unnecessary general practitioner and emergency department visits (Impicciatore et
al., 1998).
Traditionally antipyretics have been administered to prevent febrile convulsions,
however, there is no evidence to support that they prevent either initial or recurrent

8
febrile convulsions (van Stuijvenberg, Derksen-Lubsen, Steyerberg, Habbema, &
Moll, 1998). Febrile convulsions are benign, common events in 2% to 5% of children
aged 3 months to 5 years (D'Auria, 1997, Purssell, 2000). One-third of those who
have a febrile convulsion will have another (Offringa et al., 1994; Sadovsky, 2002).
A review of the literature in this area revealed that education about supportive care
by health professionals is more important than prophylactic treatment (Purssell,
2000). Purssell (2000) recommended health professionals focus on educating parents,
maintaining the child’s comfort and promoting recovery rather than aggressively
treating fever with antipyretics when a child is admitted to hospital following a
febrile convulsion. It is important that health professionals provide evidence-based
fever management education to parents to enable parents to safely care for their child
at home during subsequent febrile convulsions.
1.5 THEORETICAL FRAMEWORK People make decisions based on their knowledge about an action and the information
available to them. Knowledge influences beliefs, making them positive or negative
which in turn influence a person’s attitudes toward the consequences of acting in a
particular way, an evaluation of their beliefs (Ajzen, 1985). In fever management the
negative beliefs and attitudes of parents and health professionals are well known and
influence fever management. To enhance parents’ fever management practices it is
important to understand the factors behind their decision making, and the influences
on their management. The constructs of the Theory of Planned Behavior (Ajzen,
1985) identify the precursors of behaviour. This theory purports that a person’s
behaviour can be predicted from their intention to act in a certain manner.
Behavioural intention is predicted by the person’s attitudes toward, perceptions of
normative influences and control over the behaviour.
9
The Theory of Planned Behavior has been used to gain an understanding of many
health related behaviours, such as breast or testicular self-examination (McCaul,
Sandgren, O'Neil, & Hinsz, 1993), breast feeding (Janke, 1994), smoking cessation
following coronary artery bypass surgery (Bursey & Craig, 2000), fish consumption
in Belgium (Verbeke & Vackier, 2005), Jordanian married Muslim women’s
intentions to use contraceptives (Kridli & Newton, 2005) and Korean college
students’ intentions to engage in premarital sex (Cha, Doswell, Kim, Charron-
Prochownik, & Patrick, 2006). Educational programs based on this theory have
successfully changed nurses’ documentation and pain management behaviours
(Renfroe, O'Sullivan, & McGee, 1990), unsafe sexual behaviour (White, Terry, &
Hogg, 1994) and health protection behaviours (McCaul et al., 1993), surgical nurses’
post-operative opioid use (Edwards et al., 2001) and paediatric nurses’ fever
management practices (Edwards et al., in press).
The Theory of Planned Behavior is an appropriate theoretical framework to identify
the determinants of parents’ fever management practice intentions. Using this theory
the modifiable determinants of practice intentions, such as attitudes, normative
influences and perceptions of control can be targeted through educational programs.
This theoretical framework will be used to identify modifiable determinants in
parents’ intentions to reduce childhood fever and is explained in more detail in
Chapter 3.
1.6 THESIS OUTLINE This thesis consists of two studies. The first study is a qualitative study to identify
Queensland parents’ current knowledge, beliefs, practices and influences on practice.
Findings from this study assisted in the development of an instrument used in the
second study for a postal survey of Queensland parents exploring both descriptive

10
and theoretical aspects of fever management. The thesis is organised into eight
separate chapters. The overall chapter structure begins with an introduction and is
followed in Chapter 2 by more detailed background information about
thermoregulation, childhood fever and the role of antipyretics in fever management.
The next chapter, Chapter 3, is a manuscript reviewing the literature on parents’
management of childhood fever and then the need for a theoretical framework is
addressed. Manuscripts included in this thesis are presented in the format stipulated
by the journal to which they were submitted.
Chapter 4 is a detailed description of the methods used in both studies. Chapters 5 is
comprised of a manuscript reporting the findings from the first study, the qualitative
study exploring parents’ current knowledge, beliefs and practices. In Chapter 6 there
are two manuscripts describing different aspects of the descriptive data collected in
Study 2. The first manuscript addresses parents’ knowledge, beliefs and practices in
fever management; the second focuses on the use of antipyretics to reduce fever. In
Chapter 7 the methods used to prepare the theoretical data from the survey for
analysis, analytical methods and findings are presented and discussed in relation to
the literature. Chapter 8 is an integration of the key findings and their implications
for parents and health professionals. This is followed by directions for future studies
in this area then overall conclusions are drawn.
1.7 PURPOSE OF THE STUDY The purpose of this research was to investigate the current fever management
practices and influences on the practices of Queensland parents of well children aged
between 6 months and 5 years. Information gained was used to assist in the
development of an instrument to identify parents’ knowledge, beliefs, practices and
11
influences on practice determined through the Theory of Planned Behavior. Through
a crossectional community-based survey of Queensland parents’ knowledge, beliefs,
practices, antipyretic use, sources of information and determinants of intentions that
were identified. Findings identified practices were determined by poor knowledge
and negative beliefs and specific areas to target for education and future research.
1.8 AIMS The overall aim of this research was to identify parents’ knowledge, beliefs, practices
and influences on childhood fever management practices. The relationship between
parents’ attitudes, normative influences and perception of control when their child
has a fever on their fever management intentions was also investigated. The specific
aims were to:
1. Identify Queensland parents’ knowledge of fever, beliefs about fever, fever
management practices, antipyretic use, influences on practices and sources of
information about fever management. (Study 1 and 2)
2. Develop and trial a comprehensive instrument to explore parents’ childhood
fever management and the influences on fever management practices. (Study 2)
3. Identify the determinants of parents’ intentions to 1) reduce their child’s next
fever and 2) reduce their child’s next fever with medications through the Theory
of Planned Behavior. (Study 1 and 2)
1.9 RESEARCH QUESTIONS Based on the literature reviewed in the following chapters the following research
questions were proposed.
1. What do Queensland parents know about fever in young children?
2. What are Queensland parents’ beliefs about fever in young children?
3. How do Queensland parents manage fever in young children?
12
4. How do Queensland parents use antipyretic medications in fever management?
5. What influences Queensland parents’ medication use in fever management?
6. How do Queensland parents learn how to manage fever in young children?
7. What predicts Queensland parents’ intentions to reduce childhood fever?
8. What predicts Queensland parents’ intentions to reduce childhood fever with
medications?
1.10 HYPOTHESES
From the literature reviewed two theoretical models were explored. One model tested
parents’ intentions to reduce their child’s next fever, the fever model: hypotheses
tested were:
1. In accordance with the TPB, attitudes, subjective norms and perceived
behavioural control (fever management decision making and child medication
behaviour) will determine parents' intentions to reduce their child's next fever.
2. Perceived behavioural control related to child medication behaviour will
determine attitudes, subjective norms and perceived behavioural control in fever
management decision making.
3. Demographic factors, age, education, number of children and experience in the
health industry (education in a health profession or working in a health setting)
will determine parents’ attitudes, subjective norms and perceived behavioural
control (fever management decision making).
The second model explored parents’ intentions to reduce their child’s fever with
medications. Hypotheses tested in the medication model were:
13
1. In accordance with the TPB, attitudes, subjective norms and perceived
behavioural control (fever management decision making and child medication
behaviour) will determine parents' intentions to reduce their child's next fever
with medications.
2. Perceived behavioural control related to child medication behaviours will
determine attitudes, subjective norms and perceived behavioural control in fever
management decision making.
3. Demographic factors, age, education, number of children and experience in the
health industry (education or working in a health setting) will determine parents’
attitudes, subjective norms and perceived behavioural control (fever management
decision making).
1.11 SUMMARY Fever is a common event in childhood causing significant concern for health
professionals and parents. This concern has resulted in the customary use of
antipyretic therapy to reduce fever and prevent febrile convulsions. Mild to moderate
fever does not always need to be reduced, only when it places an additional burden
on children already compromised by specific pre-existing conditions. Fever is
beneficial, febrile convulsions are benign. Fevers below 40°C are associated with
immunological benefits.
Based on the literature reviewed above this fever management research, consisting of
two studies, has been developed. This research reports the knowledge, attitudes,
normative influences on, perceived control over and practices in fever management
of Queensland parents. Study 1 was conducted to identify the current knowledge,
beliefs, norms, practices and influences on practice of Queensland parents fever

14
management. This was undertaken using focused interviews and focused group
discussions. Findings from Study 1 assisted in the development of the instrument
used in Study 2, a Queensland survey of parents of children aged 6 months to 5
years.
15
CHAPTER 2 – BACKGROUND
2.1 INTRODUCTION This chapter firstly introduces the concept of thermoregulation and the physiology,
phases and immunological benefits of fever. Following this, childhood fever, febrile
convulsions and parents’ perceptions of febrile convulsions are reviewed. The final
section addresses the use of antipyretics in fever management, evidence-based fever
management and health professionals’ perceptions of fever and fever management.
Parents’ perceptions of fever are addressed in the next chapter.
2.2 THERMOREGULATION Thermoregulation is considered an integrated complex physiological process
involving a continuum of neural structures and connections extending from the
hypothalamus and limbic system through the lower brain stem and reticular
formation to the spinal cord and spinal ganglia (Boulant, 2000; Mackowiak, 2000b).
The area generally referred to as the preoptic region, in and near the rostral
hypothalamus, is thought to be pivotal in thermoregulation and senses subtle
deviations in body temperature. In this role the preoptic region acts as the
coordinating centre for thermoregulation receiving afferent sensory input from
thermoreceptors throughout the body and strongly influencing lower effector areas
throughout the brain stem and spinal cord (Boulant, 2000).
Thermoregulation is believed to maintain the body at a constant core temperature, at
a set-point, through activation of warm and cold sensitive neurones throughout the
body and skin despite changes in ambient temperature and motor activity
(Zeisberger, 1999). In this manner thermoregulation is achieved through a balance in

16
the firing rate of cold-and warm-sensitive neurons to control the temperature set-
point (Ng, Lam, & Chow, 2002). Heat loss responses (e.g., panting and sweating) are
controlled by warm-sensitive neurones which increases proportionally with preoptic
temperature once a threshold or the set-point temperature has been reached. Cold-
sensitive neurones receive synaptic inhibition from nearby warm-sensitive neurones.
During preoptic cooling, the firing rates of warm-sensitive neurones decrease
reducing synaptic inhibition and allowing cold-sensitive neurones to increase firing
rates (Boulant, 2000; Ng et al., 2002).
The belief that all humans maintain the same temperature in normal conditions has
been challenged (Connell, 1997; Mackowiak, Wasserman, & Levine, 1992). In
healthy adults normal temperature has been found to vary from 35.6ºC to 38.2ºC with
a mean of 36.8ºC ± 0.4ºC; and it is thought that very few adults have a normal
temperature of 37.0ºC (Mackowiak et al. 1992). In 1997, following a review of the
literature, Connell (1997) determined normal body temperature’s set-point to range
from 36.5°C to 38.0°C. Additionally, body temperature is subject to diurnal circadian
rhythms associated with the sleep-wake cycle and varies up to 1°C daily with a
plateau at about 1400 to 2000 hours and a minimum about halfway through sleep,
between 0200 and 0400 hours (Anderson, 1988; Dershewitz, 1993; Samples, 1985;
Waterhouse et al., 2005).
2.2.1 Fever Fever is considered an intentional elevation of the body’s core temperature in
response to an invasion of an exogenous organism. During fever, core temperature
rise is the deliberate result of a regulated operation of active thermogenic effectors.
Hyperthermia, passive heat gain greater than the body’s capability to dissipate heat is
17
distinct from fever and the two should not be confused. Fever is believed to be a host
defence response to invasion from exogenous pyrogens including microbial
pathogens, such as bacteria, viruses, mycobacteria and fungi as well as non-microbial
antigens, such as inflammatory agents and drugs (Blatteis, 2006).
There has been a substantial increase in understanding the physiology of fever over
the past decade which was documented in a review by Blatteis (2006) who, himself,
has undertaken considerable work in this area (e.g., Blatteis, 2003, 2006; Blatteis,
Sehic, & Li, 1998). Blatteis (2006), Boulant (2000) and Mackowiak ( 2000b)
discovered that, when exogenous pyrogens enter the body through a break in the
skin, or through the respiratory, digestive or urinogenital systems, a concentration of
non-specific, local reactions occur to protect the host and preserve normal body
functioning. Initially, there is a local inflammatory response initiated by the release
by various cell types activated by the invading pathogens such as soluble, vasoactive
and chemoactive mediators. Among these are immunoglobulins which activate
mononuclear phagocytes to remove the microbes and release additional mediators
such as cytokines and other prostaglandins which enhance the inflammatory process.
These effects are further augmented by more compounds released by other local
sensitised cells; limited by counter-regulatory factors (e.g., interleukin [IL]-4, IL-6
and IL-10). Following this cellular debris, microbial products and mediators in the
inflamed area drain via the lymphatic vessels and are filtered by macrophages in the
lymph system. However, some of these materials stimulate local sensory nerves or
escape and are absorbed into the circulation. Local inflammatory effects now extend
throughout the body evoking a range of systemic reactions collectively called the
‘acute phase reaction’ mediated largely by the central nervous system.
18
The acute phase reaction has been found to be extensive and includes, for example,
increased pituitary hormone release (e.g., ACTH, GH), increased plasma iron levels,
reduced erythropoiesis, increased neutrophils, increased sympathetic nervous
activity, release of acute phase proteins (increased C-reactive proteins, reduced
albumin, increased haemoglobin), increased lipogenesis and increased pancreatic
insulin and glucagon. These responses, occurring as an organised integrated series of
regulated events, are an integral part of a highly coherent, interconnected
physiological phenomena that together constitute the primary, early non-specific host
defence response (Blatteis, 2006; Blatteis, Feleder, Perlik, & Li, 2004; Zeisberger,
1999). During the acute phase response a number of sickness behaviours or
alterations in physiological functions occur, such as fever, hyperalgesia, lethargy,
somnolence, hypophagia, weakness, malaise, reduced locomotor activity, and an
inability to concentrate which impact general host homeostasis (Blatteis, 2006;
Zeisberger, 1999).
The immuno-protective effects of fever are believed to occur during the subsequent
adaptive or later phase of fever. These effects protect the host from infection by the
same micro-organism. The immune benefits of fever activated during the late phase
include enhanced neutrophils and monocyte motility and emigration; enhanced
phagocytosis and pinocytosis; increased oxygen radical production by phagocytes;
increased interferon production; increased antiviral, antiproliferative and natural
killer cell-stimulating activities; increased antibody production and increased killing
of intracellular bacteria (Blatteis, 2003; Blatteis, 2006; Zeisberger, 1999).

19
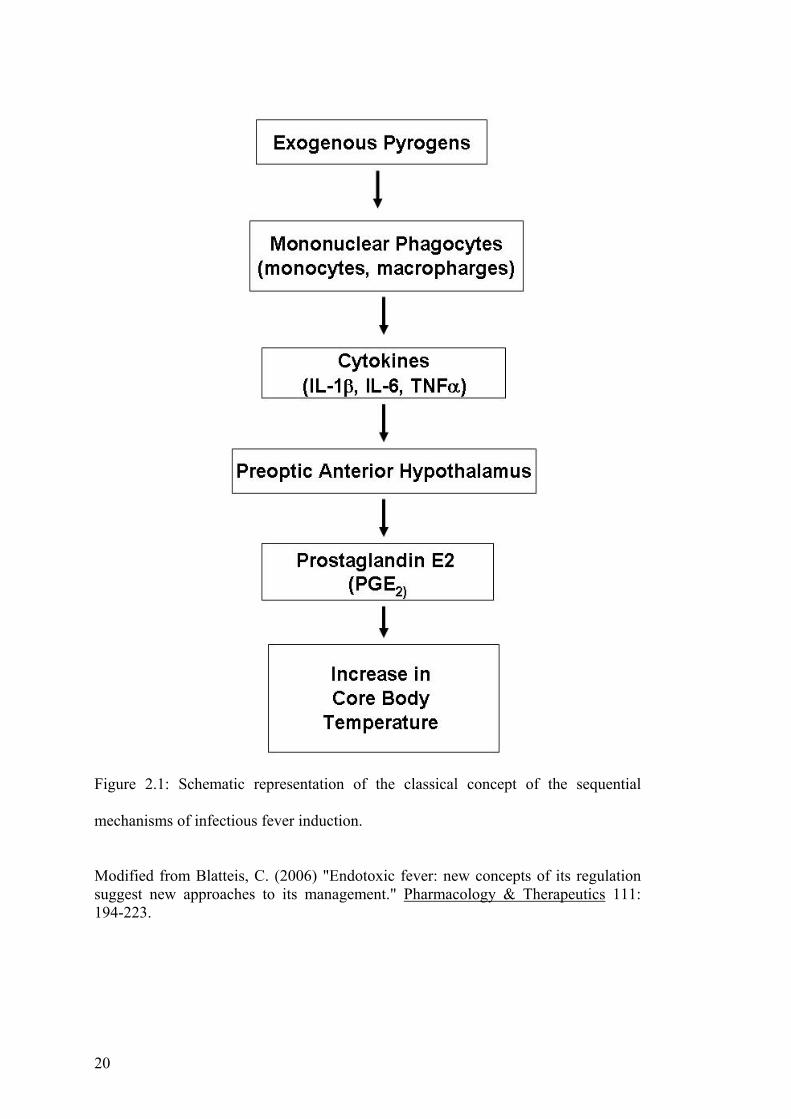
The generally held view of the genesis of pathogen-induced fever, or the febrile
response, occurs in sequential steps, see Figure 2.1. Fever begins with the production
by peripheral mononuclear phagocytes, activated by the exogenous pyrogens, of
pyrogenic cytokines, principally tumour necrosis factor (TNF)-α, interleukin (IL)-1β,
and IL-6, interferons (IFN) and other cytokines and chemokines (Blatteis, 2006). The
release of these cytokines into the bloodstream and their transport to the preoptic-
anterior hypothalamic area (POA), the brain site of the primary thermoregulatory
controller; the ventromedial preoptic nucleus is thought to be the fever-producing
locus where they act (Boulant, 2000; Mackowiak, 2000b). Prostaglandin E2 (PGE2)
is considered to be the final fever mediator in the POA, induced by these cytokines.
In the laboratory setting febrile responses are promptly evoked when these cytokines
or PGE2 are microinjected into this site, and it is now generally accepted that
thermosensitive neurons contained in this region modulate the thermoregulatory
mechanisms that effect the development of fever (Boulant, 2000; Mackowiak,
2000b).
In humans and most mammals fever has an upper limit ranging from 41.0ºC to
42.0ºC (Mackowiak & Boulant, 1996). When humans are in a thermoneutral
environment febrile rises in body temperature tend to range from 0.5ºC to 3.0ºC with
most infections producing fevers between 38.5ºC and 40.5ºC with an average fever
of 39.5ºC. Mechanisms involved in temperature regulation may lie in the intrinsic
properties of the neurons in the rostral hypothalamus or the release of endogenous
antipyretic substances that antagonise the effects of the pyrogens on these neurones
(Mackowiak & Boulant, 1996).
20
Figure 2.1: Schematic representation of the classical concept of the sequential
mechanisms of infectious fever induction.
Modified from Blatteis, C. (2006) "Endotoxic fever: new concepts of its regulation suggest new approaches to its management." Pharmacology & Therapeutics 111: 194-223.
21
2.2.2 Phases of Fever Three phases of fever have been identified by a number of authors, a cold, hot and
defervescence phase (e.g., Bruce & Grove, 1992; Connell, 1997; Fruthaler, 1985;
Holtzclaw, 1992; McCarron, 1986). The cold phase begins when the set-point is reset
to a higher level. This phase lasts approximately 10 to 40 minutes during which all
heat-producing mechanisms are activated and there is a rapid steady rise in
temperature. Heat production increases oxygen demands by three to five times
normal resting levels contributing to a hypermetabolic state. In this state there are
associated increases in heart and respiratory rates and thirst. Vasoconstriction causes
the skin to look pale with cyanotic nail beds and to feel cool and dry.
During the hot phase the body has reached a new set-point and maintains the body
temperature at this new higher temperature. The length of this phase depends on the
time it takes to eradicate the pyrogenic cytokines responsible for the raised set-point.
Higher temperatures in this phase are maintained through a balance in heat
production and heat loss. Skin is flushed and warm and the individual feels hot.
Basal metabolic rate remains high so tachycardia and thirst continue. Other
symptoms associated with this phase include drowsiness, headache, photophobia,
reduced activity and appetite, feelings of weakness and/or restlessness and
sometimes convulsions. This phase ends when the underlying cause of fever has been
treated and/or eliminated by the body resulting in a decrease in set-point to normal.
The defervescence phase, the dramatic ‘breaking’ of the fever occurs when there is a
sudden decline in circulating pyrogenic cytokines and resetting of the hypothalamic
set-point back to normal. Heat loss mechanisms take over and heat production is
inhibited. The skin feels warm and is flushed due to vasodilation and sweating,
22
which can exacerbate existing dehydration. Finally the temperature returns to
normal.
2.2.3 Benefits of Fever Fever evolved long ago in phylogeny (evolutionary biology) and is widespread in the
animal kingdom in mammals, reptiles, amphibians and fish (Blatteis, 2006; Kluger,
1979; Mackowiak, 2000b). The widespread and continued prevalence of the febrile
response offers some of the strongest evidence that fever is an adaptive response
even though it places substantial demands on the body through increased metabolic
demands. This response would not have evolved and/or been so faithfully preserved
in the animal kingdom unless there was some net benefit to the host (Mackowiak,
2000b). Upon reviewing the thermophysiological and immunological literature,
Blatteis (2006), Mackowiak (2000b) and Zeisberger (1999) concluded fever to be
beneficial.
Evidence for fever’s beneficial role is found in the enhanced resistance of animals to
infection associated with increases in body temperature within a physiologically safe
range (Blatteis, 2006; Mackowiak, 2000b). Kluger and associates demonstrated not
only a direct correlation between body temperature and survival but that suppression
of the febrile response with sodium salicylate was associated with substantial
increases in mortality (Kluger, Kozak, Conn, Leon, & Soszynski, 1996; Kluger,
1979; Kluger, et al., 1975). In humans positive correlations have been found between
maximal temperature on the day bacteraemia was diagnosed and survival;
temperature greater than 38.0ºC associated with spontaneous bacterial peritonitis was
positively correlated with survival (Weinstein, Iannini, Stratton, & Eickhoff, 1978).
Reduced amount and length of viral shedding from rhinovirus have been reported

23
(Graham, Burrell, & Douglas, 1990; Stanley, Jackson, Panusarn, Rubenis, & Dirda,
1975). When this is considered in association with the phylogeny of the febrile
response there is strong evidence that fever is an adaptive response in most
circumstances (e.g., Blatteis, 2006;. Mackowiak, 2000b; Zeisberger, 1999).
As earlier stated, the mechanisms involved in the febrile response are believed to be
integral to the functioning of the febrile response, not an accidental biological effect.
Demonstrated benefits include the enhancement of phagocytosis, neutrophil
migration, T-cell proliferation and O2-radical production, the increased synthesis of
interferon and the augmented antiviral and antitumour activities of their cytokine and
the decreased growth rate and viability of iron-dependent bacteria (Blatteis, 2003;
Mackowiak, 1994, 2000b). Immunological enhancements occur at most elevated
temperatures and are present in low and moderate fevers but reduce to below
baseline levels as temperatures approach 40°C (Lorin, 1990). However, at
temperatures of 40°C certain bacterial and viral growth is impaired (Lorin, 1999).
Neurologically, slow-wave sleep patterns are produced when temperature is raised,
reducing the body’s energy requirements and conserving the energy needed to fight
infection (Blatteis, 2006).
2.3 FEVER IN CHILDREN
No definitive temperatures for normal fever or high fever are consistently reported in
the childhood fever literature although some have been suggested. In 1994, El-Radhi
and Carroll (1994) defined fever as “body temperature 1.0°C (1.8ºF) or greater above
the mean standard deviation at the site of recording”: that is, a rectal, oral or an
axillary temperature of 38.0ºC, 37.6ºC and 37.2°C respectively. Sarrell et al. (2002)
supported these definitions in 2002. Watts, Robertson and Thomas (2003) gave a
24
range of temperatures when undertaking a systematic review of literature in relation
to paediatric nursing care of childhood fever. They defined oral temperature of 37.6º
to 37.8ºC and rectal temperature from 38.0ºC to 38.3ºC as fever. Crocetti and
Serwint (2005) were the first to report tympanic temperatures, their definitions of
fever include a temperature of 37.8ºC orally, 38.0ºC for tympanic and rectal methods
and 37.2ºC when taken in the axilla.
Prior to these common definitions, a retrospective audit of 691 temperatures in
charts of well infants (less than 3 months) attending well-baby visits found infants’
normal temperature to be 37.5ºC ± 0.3ºC (Herzog & Coyne, 1993). These infants’
temperatures demonstrated a 0.3ºC seasonal variation between summer and winter
and a 0.1ºC per month increase from 1 month to 3 months of age. Herzog and Coyne
(1993) concluded 38.2ºC or greater would indicate fever in a 3 month infant.
However, infant’s body temperature can also be raised 1°C to 1.5°C by excessive
clothing, physical activity, hot weather, digestion including bottle or breast feeding,
hot baths, damage to body tissues and hyperpyrexia (Holtzclaw, 1992; McCarthy,
1999; Ng et al., 2002).
The range of body temperature in children has been found to be higher than adults
and decreases to adult levels from about one year onwards continuing through
puberty and stabilises at 13 to 14 years in girls and 17 to 18 years in boys (Lorin,
1999). This indicates that children also have higher temperatures when febrile than
adults due to higher metabolic rates and smaller body masses; children generate more
heat and have less body surface from which to lose it. Consequently the normal
processes of heat generation and heat removal can be more readily disrupted in
febrile children (Casey, 2000).
25
Childhood fever with infection seldom exceeds 40.0°C and poses negligible risk of
brain injury unless it exceeds 41.7ºC, harmful or dangerous fever; endogenous
antipyretics prevent this occurring (Mackowiak & Boulant, 1996). However,
although rare, temporary neuronal dysfunction may occur with high fever resulting in
delirium (Okumura, Uemura, Suzuki, Itomi, & Watanabe, 2004; Scheifele, 1994). A
Japanese study found 65% of children exhibiting febrile delirium had temperatures
greater than 39.0ºC (Onoe & Nisigaki, 2004). In this study an association between
febrile delirium in a current febrile illness and history of febrile convulsions, 20%, or
previous febrile delirium, 15%, was found. No serious brain dysfunction has been
found in children exhibiting febrile delirium. Febrile delirium usually occurs during
the first 3 days of illness, lasts for about 3 days, is a transient disturbance (10 minutes
or less) usually occurring at night and sometimes repeatedly within the same night
(Onoe & Nishigaki, 2004). Delirious behaviour associated with a febrile convulsion
is rare, 2%. It generally appears prior to febrile convulsions, usually short convulsion
less than 3 minutes in duration (Okumura et al., 2004).
It has been reported that many children tolerate low grade fevers, to 39.0°C, with
remarkable ease and there is consensus in the literature that temperatures of 40°C and
higher should be avoided (e.g., Connell, 1997; Holtzclaw, 1992; Lorin, 1999). This
combined with the beneficial effects of fever indicate that mild to moderate fever,
temperatures up to 40°C should not be routinely suppressed. High fevers in young
children, 40.5ºC or over, generally indicate a serious illness or bacteraemia (Schmitt,
1994), however, temperature is not the determining factor in illness severity. Active
children with temperatures of 40.0ºC do not require as close monitoring and urgent
medical advice as a lethargic, irritable, anorexic child with a temperature of 38.3ºC
26
(Bruhn, Lelyveld, & Ludwig, 1991). Seriously ill children behave differently to those
with a self-limiting viral infection, they are unusually quiet, drowsy or irritable and
cry differently, moaning or have an inconsolable loud cry (Van den Bruel et al.,
2005). However, serious illness from bacterial infections is becoming rare. It was
recently reported that only one in 200 children with acute fevers, 39.0ºC or higher
and white cell counts of 15,000/µL or more, had occult bacteraemia; Streptococcus
pneumoniae was the most common cause (Steele & Garrison, 2005).
Fever is beneficial in normal healthy children in the home setting, but seriously ill
children can become severely compromised by the additional physiological strain of
fever. For every 1°C above normal temperature there are associated physiological
changes. Metabolic, heart and respiratory rates increase 13%, 20 beats per minute
and four to five respirations per minute respectively. There is an associated increase
in oxygen consumption of 10% to 12% and an insensible fluid loss of 20%
(Goldberger, 1986). Increased fluid loss associated with reduced intake leads to
dehydration, the most common and dangerous side effect of fever (Holtzclaw, 1992).
During the cold stage blood pressure increases and glomerular filtration rates
decrease; this reverses during the hot phase (El-Radhi & Carrol, 1994; Gildea, 1992;
Holtzclaw, 1992). Increased urine output assists in the removal of the additional
metabolic wastes from the catabolic febrile state (Holtzclaw, 1992).
When fever is prolonged the risk of dehydration increases and anorexia, secondary to
generalised weakness and malaise, is common. Psychological effects include apathy,
confusion, delirium and withdrawal from people and activities (Bruce & Grove,
1992). These physiological and psychological effects of fever are important
27
considerations for parents caring for febrile children. Fever may trigger convulsions
in those with a seizure disorder or predisposition to febrile convulsions (Scheifele,
1994) and should be reduced in those for whom the additional physiological burden
places at risk (e.g., Holtzclaw, 1992, McCarthy, 1999). This includes children who
are seriously ill and children who have cardiorespiratory, neurological or metabolic
disorders are malnourished, dehydrated or have epileptic lesions who may not
tolerate the additional physiological demands during fever (Blatteis, 2006). It is
recommended fever in these children be reduced.
2.3.1 Febrile Convulsions Febrile convulsions are not a true epileptic disease but rather a special syndrome
characterised by a provoking factor (fever) and a typical range of 6 months to 6 years
(Nakayama & Arinami, 2006; Waruiru & Appleton, 2004). They were defined as ‘a
seizure in association with a febrile illness in the absence of any central nervous
system infection or acute electrolyte imbalance in children older than one month of
age with no prior afebrile seizures’ by the International League Against Epilepsy
(Commission on Classification and Terminology of the International League Against
Epilepsy, 1989). Approximately 30% to 40% of children who have one febrile
convulsion will have another (Berg et al., 1997).
Most febrile convulsions (75% to 85%) are simple lasting less than 10 minutes
(Annegers, Hauser, Shirts, & Kurland, 1987; Berg et al., 1997). Febrile convulsions
lasting longer than 15 minutes, complex febrile convulsions, occur in 9% of children
(Berg et al., 1997). Simple febrile convulsions are brief (<15 minutes), bilateral,
tonic-clonic seizures of short duration followed by a brief post-ictal period after
which the child readily returns to their pre-morbid baseline state (Baumann, 2001;
28
Kluger & Johnson, 1998). Complex febrile convulsions are focal, unilateral or
prolonged seizures lasting longer than 15 minutes or multiple convulsions within the
same illness ( Berg & Shinnar, 1996a; Shinnar & O'Dell, 2004). Febrile convulsions
longer than 30 minutes indicate febrile status epilepticus and occur in 5% of febrile
convulsions (Berg et al., 1997). Large epidemiological studies concluded simple
febrile convulsions to be benign, common events in children without a history of
afebrile convulsions or intracranial involvement (D'Auria, 1997) associated with
rectal temperatures above 38°C (Kudsen, Paerregaard, Andersen & Anderson, 1996).
In the United States of America and Europe febrile convulsions occur in 2% to 5% of
young children, aged 1 month to 5 years, and resolve before the age of 6 years
(D'Auria, 1997; Nelson & Ellenberg, 1978). Higher incidence rates have been
reported in Japan, 8.8%, India 5% to 10% and in Guam and the Marianna Islands 14
% of children have febrile convulsions (Kluger & Johnson, 1998). Interestingly,
lower incidence and recurrence rates were reported in a Chinese population, 0.4%
and 21% respectively, over a three year period. However, this study reported higher
rates of complex febrile convulsions, 16% (Chung, Wat, & Wong, 2006).
Febrile convulsions are precipitated by any febrile illness, for example, otitis media,
pneumonia, tonsillitis, influenza, or environmental factors that raise the body
temperature (Nelson & Ellenberg, 1983). Immunisations such as diphtheria–
pertussis–tetanus and measles are environmental precipitants of febrile convulsions.
In children who have an environmentally precipitated febrile convulsion 50% have a
genetic predisposition to febrile convulsions (Hirtz, Nelson, & Ellenberg, 1983).
Influenza A is associated with prolonged post ictal impairment of consciousness

29
which may suggest influenza effects state of consciousness at the same time as it
induces the febrile convulsion (Hara et al., 2007). Sudden Infant Death Syndrome
(SIDS) was not associated with febrile convulsions in a large Danish epidemiological
study (Vestergaard, Basso, Henriksen, Ostergaard, & Olsen, 2002). The rate of SIDS
in children who had had a febrile convulsion was .002%; children with a first degree
relative who had a febrile convulsion had no overall increased risk of SIDS.
Febrile convulsions were thought to be associated with a rapidly rising temperature;
this has been disproved in both human and animal studies (Berg, 1993; Shinnar &
O'Dell, 2004). There is increasing evidence from human and animal studies that
Interlukin-1, a key cytokine in the production of the febrile response may be
implicated in the pathophysiology of febrile convulsions as it is also a proconvulsant
agent (Baram & Shinnar, 2002). Current treatment for febrile convulsions recognises
both simple and complex febrile convulsions are benign. No specific medical
treatment is recommended for simple febrile convulsions (Baumann, 2001). Parent
education is recommended for all parents of children who have a febrile convulsion
to reduce anxiety and enable parents to safely manage any recurrent febrile
convulsions. Sometimes the use of oral or rectal diazepam is recommended during
febrile episodes for children who have complex, prolonged or multiple febrile
convulsions that have a high risk of recurrence or live in remote geographical
locations (Shinnar & O'Dell, 2004).
In a review of the molecular genetics of febrile convulsions Nakayama and Arinami
(2006) concluded these convulsions have a significant genetic component. Six
susceptibility febrile convulsion loci have been identified on chromosomes 8q13–q21

30
(FEB1), 19p (FEB2), 2q23–q24 (FEB3), 5q14–q15 (FEB4), 6q22–q24 (FEB5), and
18p11 (FEB6). This genetically complex disorder is believed to be influenced by
variations in several of the susceptibility genes. Findings from recent studies report
varying results and no consistent or convincing febrile convulsion susceptibility
genes have emerged (Nakayama & Arinami, 2006).
2.3.1.1 Predictors of Febrile Convulsions Risk factors for initial and recurrent febrile convulsions have been identified in well-
designed studies (Shinnar & O'Dell, 2004). It is thought that febrile convulsions are
precipitated by a number of factors including a lower seizure threshold of the
developing cortex (normal seizure threshold is higher than 41.5°C (Kudsen et al.,
1996), susceptibility to infections, tendency to have high fevers and a genetic
component affecting the seizure threshold (Baumann, 2001; Freeman, 1992; Nelson
& Ellenberg, 1981). During the last decade febrile convulsion susceptibility genes
have been identified in regions of a number of chromosomes (Johnson et al., 1998;
Kluger & Johnson, 1998; Nakayama & Arinami, 2006; Thoman, Duffner, &
Shucard, 2004; Wallace, Berkovic, Howell, Sutherland, & Mulley, 1996).
Although strong correlations have been identified between the height of fever and the
occurrence of febrile convulsions in children who have 40.0°C to 41.1°C
temperatures, febrile convulsions also occur at lower temperatures, for example
38.0ºC (McCarthy, 1999). Febrile convulsions have been found more common in
boys, to peak between 10 and 20 months of age, and occur more frequently in
association with respiratory illnesses during winter and gastroenteritis in summer
(D'Auria, 1997). However, at least 50% of children who present following a febrile
31
convulsion have no identified risk factors for febrile convulsions (Waruiru &
Appleton, 2004).
There is consensus in the literature that the predictors of an initial febrile convulsion
are a febrile convulsion in a first or second degree relative, neonatal discharge at 30
days or later, very pre-term birth, parental report of slow development, more febrile
episodes per year or attending day care (Bethune, Gordon, Dooley, Camfield, &
Camfield, 1993; Herrgard et al., 2006; Huang et al., 1999; Mukherjee & Mukherjee,
2002). In children with a febrile illness additional factors include the peak
temperature during the illness and the underlying illness (Berg et al., 1995). For
example, gastroenteritis has a lower risk for febrile convulsions than otitis media or
other causes of fever (Berg et al., 1995). In children with two risk factors, 3% of the
population, the risk of an initial febrile convulsions is higher, approximately 28%
(Bethune et al., 1993).
Predictors of recurrent febrile convulsions include younger age at initial febrile
convulsion, history of febrile convulsions in a first degree relative, low peak
temperature during the fever, short duration of recognised fever and initial febrile
convulsions and the duration of the fever (Berg & Shinnar, 1996b; Berg et al., 1997;
Berg et al., 1992; Offringa et al., 1994). Recurrent febrile convulsions are more
likely to occur within the first 2 hours of fever onset in a subsequent febrile illness
and are more common in younger children (van Stuijvenberg, et al., 1998). The
length of fever prior to the initial febrile convulsion influences recurrence rates
within the following year. A prolonged febrile seizure is a risk factor for further
prolonged attacks (Berg et al., 1997). The risk of a recurrence for fevers lasting less
32
than one hour prior to the initial febrile convulsion is 44%, 23% for fevers between
one and 24 hours and there is a 13% risk of recurrence in the following year in fevers
which occurred 24 hours prior to the initial febrile convulsion (Berg et al., 1992).
Risks for recurrent febrile convulsions are cumulative as with initial febrile
convulsions. In a child younger than 1 year the cumulative risk is 25% and 30% in a
child younger than 2 years (Berg et al., 1992). A decreased risk of recurrence is
associated with a temperature of 39°C or higher at the time of the initial febrile
convulsion (Laditan, 1994).
More recent studies have examined circadian and genetic relationships with febrile
convulsions. In Italy first febrile convulsions occurred more frequently during the
winter months (December to February) peaking in January (Manfredini, Vergine,
Boari, Faggioli, & Borgna-Pignatti, 2004). They were more commonly associated
with upper respiratory tract infections and occurred most frequently between 1800
and 2400 hours peaking at 1831 hours. In males febrile convulsions peaked at 1755
hours and in females at 1932 hours. A study in the Netherlands found a positive
relationship between influenza and febrile convulsions (van Zeijl, Mullart, Borm, &
Galama, 2004). In a twin study of febrile convulsions, monozygotic twins were
significantly more likely to have a febrile convulsion if their pair did than dizygotic
twins supporting the genetic predisposition to febrile convulsions (Kjeldsen, Kyvik,
Friis, & Christensen, 2002).
2.3.1.2 Outcomes Following Febrile Convulsions No long-term effects have been identified in children aged 6 to 12 years following
febrile convulsions. Areas of health and intellect studied include attention, working
memory, scholastic ability and behaviour (Chang, Guo, Huang, Wang, & Tsai, 2000;

33
Chang, Guo, Wang, Huang, & Tsai, 2001); neurophysical and neurological
functioning (Kolfen, Pehle, & Konig, 1998) and health problems, speech, sleep,
overactivity and other behavioural concerns (Hutt, Trueman, & Hutt, 1999). Large
epidemiological studies report that measures to prevent additional febrile convulsions
are unlikely to alter the long-term outcome of most children who have a febrile
convulsion (e.g., Autret et al., 1990; Uhari, Rantala, Vainionpaa, & Kurttila, 1995).
A single febrile convulsion has not been found to increase the risk of epilepsy and no
causal relationship has been discovered between febrile convulsions and subsequent
epilepsy (Berg, 1992; Mukherjee & Mukherjee, 2002; Shinnar & O'Dell, 2004).
However, between 2% and 10% of children who have febrile convulsions
subsequently develop epilepsy; two to ten times the general population (Annegers et
al., 1987; Berg & Shinnar, 1996a,b). Risk factors for epilepsy following a febrile
convulsion are a complex or prolonged febrile convulsion, neurodevelopmental
abnormality, family history of epilepsy, three or more febrile convulsions and
duration of recognised fever less than one hour prior to febrile convulsion (Annegers
et al., 1987; Berg & Shinnar, 1996a; MacDonald, Johnson, Sander, & Shorvon, 1999;
Nelson & Ellenberg, 1983 ; Shinnar & O'Dell, 2004; Verity & Golding, 1991). A
family history of epilepsy and the presence of a neurodevelopmental abnormality are
recognised risk factors of epilepsy independent of febrile convulsions (Shinnar &
O'Dell, 2004).
2.3.1.3 Parents and Febrile Convulsions Parents may be very anxious when their child has a febrile convulsion. Actions
during febrile convulsions are often inappropriate and include sponging or
medicating the convulsing child to reduce fever; holding the child or lying the child

34
on their side, supine or prone; mouth to mouth resuscitation; hitting the child on the
back or shaking the child to arouse it, forcing an object, spoon or fingers, into their
child’s mouth to prevent them swallowing their tongue and some restrain the
convulsing child (Deng, Zulkifli, & Azizi, 1996; Flury, Aebi, & Donati, 2001;
Huang, et al., 2002; Ling, 2000). Some parents report believing febrile convulsions
to be harmful, causing death or damaging their child; they believe their child has
changed or looks damaged following a febrile convulsion (Flury et al., 2001; Huang
et al., 2002; Parmar, Shau, & Bavdekar, 2001; van Stuijvenberg et al., 1999). Parents
thought their child would or had died when they were convulsing, they also felt
helpless and panicked (Miller, 1996). Particular fears associated with febrile
convulsions include death, brain damage, paralysis, physical handicap later in life,
epilepsy, a recurrence and febrile convulsion in other children (Deng et al., 1996;
Parmar et al., 2001; van Stuijvenberg et al., 1999).
Most parents seek medical advice during or immediately following a febrile
convulsion (e.g., Deng et al., 1996; Ling, 2000; Miller, 1996; Parmar et al., 2001).
For parents, witnessing a febrile convulsion generates long lasting fears about
recurrences, they are very anxious with subsequent febrile episodes; monitor afebrile
children at night and report sleep disturbances including insomnia (Flury et al., 2001;
Miller, 1996). During subsequent febrile episodes parents frequently check their
child, sleep in the same bed or room as the child or leave the child’s door open (van
Stuijvenberg et al., 1999).
Although parents of children with recurrent febrile convulsion were more
knowledgeable about and had more positive attitudes toward febrile convulsions they
35
had similar concerns about febrile convulsions as parents of children following an
initial convulsion (Huang et al., 2002). Parents most frequently learn about febrile
convulsions from friends and relatives (Deng et al., 1996; Ling, 2000). Other sources
of information are health professionals, television, newspapers, magazines and radio
(Deng et al., 1996). Educational interventions have successfully improved parents’
poor knowledge, reduced negative attitudes, anxiety towards and inadequate first-aid
measures during febrile convulsions (Huang, 2001; Huang, Liu, & Huang, 1998;
Wassmer & Hanlon, 1999). Face to face educational programs are associated with
greater long term effectiveness than mailed information pamphlets (Huang, 2001).
2.3.2 Antipyretics In a historical review of antipyretics Duff (1986) wrote that when aspirin became
available in the late 19th century it was used by doctors to reduce the discomfort
associated with inflammation, at this time antipyresis was of secondary interest.
Following this the indiscriminate reduction of fever became a common medical
practice with the immediate symptomatic gains apparently outweighing any risks.
The use of antipyretics for fever reduction involves two critical assumptions; that
fever is at least in part harmful and suppressing fever will reduce if not eliminate
fever’s harmful effects. However, neither of these assumptions has been validated
experimentally (Mackowiak, 2000a). Fever is often perceived as a syndrome, or
illness in itself, that can initiate a dangerous, potentially life-threatening illness
(Blumenthal, 1998).
Other rationales for reducing fever with antipyretics include preventing febrile
convulsions, increasing comfort and reducing the metabolic costs of fever (e.g.,
Isaacs, Axelrod, & Lorber, 1990; Mackowiak, 2000a). Arguments for the use of
antipyretics in preventing febrile convulsions stem from beliefs that febrile
36
convulsions are caused by rapidly rising temperatures. In 1993, after reviewing the
evidence of the rate of rise of temperature and height of temperature and their roles
in febrile convulsions, Berg (1993) concluded that there was no evidence that the rate
of rise of temperature had any role in provoking febrile convulsions. Numerous
experimental studies exploring the effect of antipyretics in preventing an initial or
recurrent febrile convulsions conclude antipyretics ineffective in preventing febrile
convulsions (e.g., Baumann, 2001; Sagraves, 1999; Uhari et al., 1995; Van Esch et
al., 1995; van Stuijvenberg, et al., 1998). However, some reduction of risk of
recurrence may be achieved under optimal circumstances, namely that fever is
noticed at once and that antipyretics can be administered on time (van Esch et al.,
2000). Many initial and recurrent febrile convulsions occur within the first one to
two hours of a febrile illness making it difficult for parents to achieve this.
Carefully controlled experiments have not established the validity of the claim that
antipyretics improve comfort (Isaacs et al., 1990; Mackowiak, 2000a). Antipyretics
do reduce discomfort associated with hyperalgesia in the cold phase of fever to some
extent. Common antipyretics, paracetamol and ibuprofen have analgesic properties
(eMIMS, 2007). When a febrile child in pain is given an analgesic the medication
will reduce the child’s pain, making them more comfortable. This can cause parental
confusion or belief that the increase in comfort is associated with temperature
reduction rather than pain reduction (eMIMS, 2007). The improvement is not due to
reduced fever or reduction in circulating pathogens but to the analgesic properties of
most antipyretic medications. Nevertheless, it is important to remember that all
drugs, including antipyretics, have potentially noxious side effects. There was a
seven fold increase in the use of ibuprofen in an Australian metropolitan paediatric
37
hospital between 1999 and 2003 (Titchen, Cranswick, & Beggs, 2005). During this
period there were 10 adverse drug reactions from ibuprofen compared with 6 from
paracetamol. With the availability of ibuprofen and paracetamol in Australian
supermarkets there is an urgent need for parents to become aware of the need for
caution with the use of these drugs. Their use and advice about their use should be
directed by competent health professionals (Blatteis, 2006; Mackowiak, 2000b).
Fever reduction with antipyretics is recommended when the metabolic costs of fever
are greater than the physiological benefits. Although recommended, it is necessary to
be cautious, ensuring the symptomatic relief provided by the antipyretic does not
adversely affect the course of the febrile illness. Additionally, it is necessary to
ensure the toxicological costs (side effects) of an antipyretic regime are considerably
lower than fever’s beneficial efforts. When administering antipyretics parents and
health professionals must be careful not to induce shivering, shivering will further
increase both the temperature and metabolic rate (Mackowiak, 2000a). Although
antipyretics are recommended in certain situations the risk-benefit ratio of metabolic
cost and beneficial benefits from fever have not been determined (Blatteis, 2006;
Mackowiak, 2000a).
Paracetamol has been the standard treatment for fever since the discovery of an
association between aspirin and Reye’s syndrome (Starko, Ray, & Dominguez,
1980). It retains this status due to its effectiveness, low cost and minimal side effects
(McCarthy, 1999) although ibuprofen, a more expensive alternative, is increasing in
popularity (Knoebel et al., 2002). Ibuprofen is often used to treat fevers unresponsive
to paracetamol. Any additional benefit derived from ibuprofen in these situations is

38
probably small and must be weighed against ibuprofen’s potential toxicity, which
includes an antiplatelet effect, potential hypersensitivity, and gastrointestinal
irritation (eMIMS, 2007; Titchen et al., 2005).
Paracetamol and ibuprofen are believed to inhibit prostaglandin synthesis in the
thermoregulatory control area of the brain blocking the conversion of arachidonic
acid to prostaglandins such as PGE2 by inhibiting prostaglandin synthesis (Knoebel
et al., 2002; McCarthy, 1999; Vane & Botting, 1998). This effect is thought to be
critical in their antipyretic activity; the production of PGE2, at key sites in the
hypothalamus. PGE2 production is a widely regulated and critical step in
thermoregulation and for temperature increase and control when the febrile response
is activated (Blatteis & Sehic, 1997). Refer to Figure 2.1. Parents and health
professionals reducing childhood fever with antipyretics may unknowingly reducing
prostaglandin synthesis, altering the body’s intricate protective response to invading
pyrogens. There are studies demonstrating a negative effect of antipyretics on
recovery by prolonging illnesses. For example, viral shedding in rhinovirus (Stanley
et al., 1975) and crusting time of varicella lesions (Doran, De Angelis, Baumgardner,
& Mellits, 1989). They also inhibit the maturation of monocytes into macrophages
and interfere with lymphocyte activation and antibody production (Graham et al.,
1990).
2.3.2.1 Effectiveness of Antipyretics in Fever Reduction Antipyretics reduce temperature by 0.9°C to 1.3°C and when tepid sponging is
conducted 30 minutes following antipyretic administration temperature reduction
increases to between 1.3°C and 1.7°C (Friedman & Barton, 1990; Hunter, 1973;
Kinmonth et al., 1992; Sharber, 1997). Traditionally antipyretics were used to

39
prevent rises in temperature and by association febrile convulsions as febrile
convulsions were thought to be precipitated by the rapid rise in temperature
(Ouellette, 1993); this was unsubstantiated (Berg, 1993). It has been found that
controlling fever rarely, if ever, prevents an initial or a recurrent febrile convulsions
(e.g., Baumann, 1999, 2001; Rantala, Tarkka, & Uhari, 2000; Uhari et al., 1995; van
Esch et al., 2000; van Stuijvenberg, et al., 1998). However, temperature reduction is
recommended in some cases. For example, children with pre-existing cardiac,
respiratory, neurological, metabolic, renal or hepatic conditions are placed ‘at risk’
by the debilitating effects of an increased metabolic rate which include increased
pulse and respiratory rates, oxygen demand and insensible fluid loss (Holtzclaw,
1992; Reeves-Swift, 1990). Other children fever places at risk are those who are fluid
depleted, have low protein levels or an electrolyte imbalance (e.g., Betz et al., 1994;
D'Auria, 1997; McCullough, 1998; Stone, 1990).
Many studies have compared the efficiency of paracetamol compared with ibuprofen
in fever reduction. However, comparison of findings is difficult as in many of the
studies the inclusion criteria, definition of fever and the dosages of paracetamol and
ibuprofen compared differ. Limited research has been conducted using Australian
recommended dosage and administration frequencies for paracetamol and ibuprofen
(Beggs, Carroll, Walsh, & Palmer, under review). However, Walson et al. (1992) did
compared the Australian recommended doses 15mg/kg paracetamol and 10mg/kg
ibuprofen (eMIMS, 2007). They found no statistically significant difference in
temperature reduction between the two medications. A review by Goldman et al.
(2004) and Beggs et al. (under review) of single and multiple mono-therapy studies
comparing the efficacy and safety of paracetamol and ibuprofen concluded ibuprofen
40
significantly more effective after a single dose and after six hours. However, similar
efficacy and effectiveness were found when multiple mono-therapies of paracetamol
and ibuprofen in recommended doses were compared.
Reports of parents alternating antipyretics, paracetamol and ibuprofen, when fever is
not sufficiently reduced or returns are becoming more frequent, particularly over the
past decade. This is not a new practice, 53% of paediatric house officers’ alternated
aspirin and paracetamol in 1983 (Weiss & Herskowitz, 1983). In 2000 and 2001
reports indicated 7% to 27% of parents alternated (Crocetti, Moghbeli, & Serwint,
2001; Li, Lacher, & Crain, 2000)). This has increased significantly in the past year to
30% to 67% parents reporting they have alternated antipyretics (Nabulis et al., 2006;
Wright & Liebelt, 2007).
Until recently no experimental studies had explored the efficacy of alternating
antipyretics on fever reduction. In 2006 three studies were reported (Erlewyn-
Lajeunesse et al., 2006; Nabulis et al., 2006; Sarrell, Wielunsky, & Cohen, 2006).
Again, these studies used different alternating methods, dosages and frequencies of
medication administration. One study compared combined paracetamol and
ibuprofen with paracetamol or ibuprofen alone (Erlewyn-Lajeunesse et al., 2006).
Combined administration resulted in significantly greater temperature reduction than
paracetamol alone 0.35ºC but not the ibuprofen alone 0.25ºC. Another study
compared alternate-therapy with mono-therapy. An initial administration of
ibuprofen 10mg/kg was followed by either ibuprofen 10mg/kg (mono-therapy) or
paracetamol 15mg/kg (alternate-therapy) (Nabulis et al., 2006). Similar temperatures
were discovered four hours after the initial ibuprofen dose 37.5ºC in alternate-
41
therapy group and 37.7ºC in the mono-therapy group. Over an eight hour period
there was similar maximum temperature reduction of 2.2ºC ± 0.7ºC in the alternate-
therapy group and 2.1ºC ± 1.2ºC in the mono-therapy group. The third study,
conducted over a three day period, used loading doses followed by different
alternating doses and frequencies (Sarrell et al., 2006). In this study there was a 1.0ºC
additional reduction in temperature in the alternating medication group. Overall in
these studies the additional temperature reduction was between 0.3ºC and 1.0ºC
(Erlewyn-Lajeunesse et al., 2006; Nabulis et al., 2006; Sarrell et al., 2006).
2.3.2.2 Dangers of Antipyretics Although paracetamol is considered a safe medication liver failure is a well
recognised consequence of paracetamol overdose (Russell, Shann, Curtis, &
Mulholand, 2003) and there are genuine concerns about hepatotoxicity in children 5
weeks to 10 years of age (e.g., Kearns et al., 1998; Knoebel et al., 2002; Miles et al.,
1999; Murphy, 1992). Multiple doses of 60mg/kg/day from 1 to 8 days have been
associated with hepatic failure (Heubi, Barbacci, & Zimmerman, 1998). There are
reports of rare adverse reactions to paracetamol which have been neither confirmed
nor refuted: dyspepsia, nausea, allergic and haematological reactions. Caution must
be taken with paracetamol administration in children with hepatic or renal
dysfunction. Paracetamol overdose can result in severe liver damage and sometimes
acute renal tubular necrosis (eMIMS, 2007).
The most common reactions to ibuprofen are gastrointestinal disturbances such as
nausea, epigastric pain, heartburn, diarrhoea, abdominal distress, nausea and
vomiting, indigestion, constipation, abdominal cramps or pain and fullness of the
gastrointestinal tract (bloating and flatulence). Others include tinnitus, oedema, fluid
42
retention, dizziness, headaches, nervousness, maculopapular rashes and decreased
appetite. Caution should be taken in the administration of ibuprofen in children with
impaired renal or hepatic function or a history of gastrointestinal haemorrhage or
ulcer or inflammation of the lining of the stomach or bowel as in conditions such as
Crohn's disease or ulcerative colitis. Ibuprofen overdose causes depression of the
central nervous and the respiratory systems (eMIMS, 2007) .
Serious toxicity, from paracetamol has been reported in children with a febrile illness
who were unwell, anorexic, vomiting and/or dehydrated and who received fourth
hourly paracetamol 90mg/kg/day or greater for more than one day. Most at risk are
children under 2 years of age (Miles et al., 1999) and children who are both febrile
and acutely malnourished (Heubi et al., 1998). Analgesics/antipyretics are the most
frequently reported substances responsible for unintentional overdose in children
under the age of 12 years in the United States (Watson et al., 2004). Most, 76%,
paracetamol overdoses in children less than 19 years of age occur in children
younger than 6 years and all (100%) overdoses in children younger than 6 years were
unintentional (Angalakuditi, Coley, & Krenzelok, 2006). Although younger children
are likely to have a lower dose compared with older children and adolescents; the
impact is usually more severe and likely to be fatal (Angalakuditi et al., 2006).
Potential for dosing errors and overdosing increases with alternating antipyretics
(Mayoral et al., 2000). Toxicity and poison control centres receive many calls
regarding this practice and parental confusion is common (Knoebel et al., 2002).
Those particularly at risk are children younger than 1 year; the age where inaccurate
antipyretic dosing has been found to occur more frequently (Li et al., 2000).
43
McCullough (1998) recommends that the practice of alternating antipyretics be
confined to specialised units, under professional supervision, following careful
consideration of the risks and benefits of exposing the sick child to two drugs with
different half-lives.
There have been strong warnings about the dangers of alternating since the recent
publication of experiments in alternating antipyretics in febrile children (Goldman,
2006; Saphyakhajon & Greene, 2006; Schmitt, 2006). Alternating increases the risk
of incorrect dosing, more likely with ibuprofen than paracetamol, in both dosage and
frequency (Lagerlov, Helseth, & Holager, 2003; Li et al., 2000) and fever phobia.
This practice focuses on a need to ‘get fever under control’ and will increase parental
preoccupation with the height of the fever, their fear of fever and increase
unnecessary phone calls and medical service use (Schmitt, 2006).
2.3.3 Management of Childhood Fever Many papers have been published on the management of febrile children in the past
35 years. The risks and benefits of fever have been debated for more than two
decades along with the efficacy and necessity of reducing fevers with antipyretics.
Not all studies reach the same conclusion creating confusion as to the best practice in
caring for a febrile child. For the past two decades the normal value for human
temperature, 37.0°C, has had very little scientific support. A study of 148 adults
suggests that normal temperature in healthy subjects ranges from 35.6°C to 38.2°C
and only eight percent of those studied recording a temperature of 37.0°C
(Mackowiak et al., 1992).
44
Advice on the temperature at which fever should be treated varies. Cunha et al.
(1984) recommend treating fevers greater than 38.9°C, Thomas 38.3°C (1995) and
McCarthy 39.4°C (1999) while Lorin (1994; 1999) and Connell (1997) advocate
treating only fevers greater than 40°C when the physiological benefits of fever
diminish. Information relating to febrile convulsions and the use of antipyretics in
fever management also varies. A genetic predisposition toward febrile convulsions
was identified in the early 1990s (Freeman, 1992). Yet, in 1993 reducing fever with
antipyretics, tepid sponging and treating the underlying cause of the fever was
recommended to prevent febrile convulsions (Ouellette, 1993).
Since the early 1970s inconsistent results have been reported on the effectiveness of
antipyretics in combination with tepid sponging (e.g., Friedman & Barton, 1990;
Hunter, 1973; Mahar et al., 1994; Sharber, 1997) and any additional temperature
reduction is queried in relation to the discomfort caused, that is, crying, goose bumps
and shivering, which in themselves cause an increase in temperature (Connell, 1997;
Holtzclaw, 1992; McCarthy, 1999; Scheifele, 1994; Sharber, 1997). A recent
systematic review of the efficacy of tepid sponging in fever management determined
little benefit from tepid sponging (Watts, Robertson, Thomas, & Panel, 2001).
However, recommendations for tepid sponging in association with antipyretics still
occur in the literature (Bernath, Anderson, & Silagy, 2002; Chandra & Bhatnagar,
2002) along with advice to control the fever and reassure the family (McCarthy,
1999).
Current management of febrile convulsions depends heavily on studies from the
United States and United Kingdom where the latest practice in fever management is
45
the use of alternating antipyretics (Mayoral et al., 2000) even though strategies to
reduce fever to prevent febrile convulsions have been proven ineffective (Baumann,
2001; Camfield & Camfield, 1997). Fever, per se, does not always need to be treated,
although it should be treated in those it places at risk of further complications. The
latest scientific evidence supports the notion that fever has a role to play in
supporting the body’s defence against invading pyrogens and there is consensus that
temperatures above 40°C should be avoided, as there are reduced immunological
benefits at these temperatures (Connell, 1997).
Based on the literature above appropriate management of childhood fever includes
careful observation of the child’s response to fever, preventing dehydration,
supporting the febrile response and reducing distressing symptoms such as pain and
discomfort with recommended doses of analgesics (Connell, 1997). McCarthy (1999)
recommends determining the degree of illness from the child’s interactions with the
environment. This is achieved through observing the child’s alertness, playfulness or
irritability and consolability in addition to physical observations such as petechiae,
bulging fontanelle, nasal flaring and response to stimuli. Parents are anxious about
fever. If a child is shivering and vasoconstricted in a warm environment, it is safe to
assume their thermostatic set-point has been raised. If they become flushed and
perspire, cooling mechanisms are functioning.
The literature recommends avoiding temperatures above 40°C and temperature
reduction is mandatory above the upper limit of physiologic thermoregulation 41.1°C
(McCarthy, 1999). It is important for parents to be watchful when administering
antipyretics to dehydrated or severely malnourished children (Robertson, 2002) and
46
those with hepatic or renal impairment (eMIMS, 2007). In the more usual
temperature range, indicators for temperature control are less clear. In a febrile,
irritable, uncomfortable child, analgesia is warranted. Antipyresis is warranted in
children with underlying neurological or cardiopulmonary disease (McCarthy, 1999).
Parents learn to manage fever from health professionals, drawing on their knowledge
(Crocetti et al., 2001; Karwowska, et al., 2002). Therefore, health professionals’
current knowledge and attitudes toward fever contribute to parents’ knowledge of,
attitudes toward and management of fever. This makes it imperative that health
professionals have current fever management knowledge based on the latest
scientific evidence. They must challenge their negative beliefs and attitudes so that
they will be positioned to provide evidence-based fever management information to
parents of young children, allay parents’ inaccurate beliefs and reduce their fears of
harmful outcomes from childhood fever (Edwards et al., in press).
2.3.4 Health Professionals and Childhood Fever Parents report learning to manage fever from numerous sources with health
professionals being considered a reliable source of health information (e.g., Al-Eissa,
Al-Zamil et al., 2000; Barrett & Norton, 2000; Karwowska et al., 2002; McErlean et
al., 2001; Singhi et al., 1991). There are many reports about health professionals’
incorrect, phobic beliefs and practices, their knowledge, beliefs and fever
management practices are not always based on the latest scientific evidence.
Internationally, there are reports indicating health professionals, doctors and nurses,
believe fever to be harmful, causing febrile convulsions and brain damage
irrespective of country of research. For example, Canada (Ipp & Jaffe, 1993),
Switzerland (Gehri et al., 2005), Israel (Sarrell et al., 2002), Saudi Arabia (Al-Eissa
et al., 2001), Australia (Edwards, Courtney, Wilson, Monaghan, & Walsh, 2001b;
47
Walsh, et al., 2005) and the United States (Poirier, et al., 2000; Thomas et al., 1994).
Health professionals’ negative attitudes toward fever have remained unchanged over
the past 20 years (e.g., Abdullah, et al., 1987; Sarrell et al., 2002) despite strong
evidence for the beneficial effects of mild fever available for 30 years (e.g., Knoebel
et al., 2002; Lorin, 1999; Poirier et al., 2000; Sadovsky, 2001; Sarrell et al., 2002).
Health professionals as well as parents use the height of fever as a determinant of
illness severity (Sarrell et al., 2002; Walsh et al., 2005) and report that temperatures
as low as 38.3°C to 38.5°C require reduction to prevent febrile convulsions despite
evidence that febrile convulsions are benign events in young children which are not
prevented by antipyretics (D'Auria, 1997; Kudsen et al., 1996; May & Bauchner,
1992; Poirier et al., 2000; Sarrell et al., 2002; Van Esch et al., 1995). Health
professionals’ use of antipyretics to reduce low grade fever and recommendations to
parents to practice similarly continue (May & Bauchner, 1992; Mayoral et al., 2000;
Poirier et al., 2000; Sarrell et al., 2002; Sarrell & Kahan, 2003; Thomas et al., 1994;
Walsh et al., 2005; Waterston, 2002). Reports of health professionals alternating
antipyretics to reduce fever are widespread (Edwards, Courtney, Wilson, Monaghan,
& Walsh, 2003; May & Bauchner, 1992; Mayoral et al., 2000; Sarrell & Kahan,
2003). Health professionals and paediatricians also recommend parents alternate
antipyretics to reduce and maintain normal temperatures in children with a febrile
illness (Mayoral et al., 2000).
2.4 SUMMARY In humans, body temperature for each individual is maintained at a set temperature
‘set-point’ in the anterior hypothalamus through a highly orchestrated series of heat
production and conservation measures. When the set-point is raised by invading
48
micro-organisms the febrile response, a coordinated series of events to defend the
body against the organisms, is activated. Benefits of this response are evident in
children with temperatures up to 40°C and include enhancement of the
immunological system, reductions in serum iron and increases in phagocytic activity.
Associated with raised temperatures are incremental increases in heart, respiratory
and metabolic rates which place undue strain on some children. Fever should be
reduced in these children and in children with temperatures of 40°C or greater.
Benign convulsions associated with fever occur in 2% to 5% of children aged 3
months to 5 years. Aggressive antipyretic therapy has not been shown to prevent
these convulsions; it reinforces parents’ fever phobias and contributes to overdosing.
Parents are very concerned about the probability of febrile convulsions. They use
unsafe practices during febrile convulsions such as shaking, mouth to mouth
resuscitation, supine positioning and administering oral medications during a
convulsion. Health professionals, parents’ educators, hold negative attitudes toward
fever and recommend temperature reduction to prevent febrile convulsions. Health
professionals are responsible for educating parents about home fever management;
their negative attitudes might influence parents care of febrile children. It is
important for health professionals to educate parents about evidence-based fever
management, assessing and monitoring the child and treating the child, not the fever.
In the next chapter there is a published article exploring parents’ knowledge,
attitudes and practices in fever management, their sources of information and the
efficacy of educational interventions that have been trialled to improve parents’ fever
management practices. Following the article the need for a theoretical exploration of
the determinants of parents fever management is addressed.
49
CHAPTER 3 - PARENTS AND FEVER
This chapter begins with a published article reviewing the international literature
about parents’ management of childhood fever. The article reviews parents’
knowledge, attitudes and practices in fever management. Initially parents’ knowledge
of temperature and fever and antipyretics and the predictors of knowledge are
explored. Following this attitudes toward fever and predictors of attitudes are
discussed. Next parents’ practices in relation to fever management are reviewed.
These include temperature taking and fever management. The limitations of studies
exploring these areas are then discussed. Following this the information sources
parents use to learn to about fever management and antipyretics are explored. Finally
educational interventions developed and trialled to improve parents’ fever
management are discussed along with limitations of these studies.
The discussion following the article explores the lack of theoretically based research
into parents’ management of childhood fever as a reason for the continued reports of
parents’ concerns about harmful outcomes from fever despite successful educational
programs. An appropriate theory is chosen, the Theory of Planned Behavior, and its
assumptions and constructs discussed.
50
3.1 MANAGEMENT OF CHILDHOOD FEVER BY PARENTS: LITERATURE REVIEW Walsh, A., Edwards, H. (2006) Management of childhood fever by parents: literature
review. Journal of Advanced Nursing 54 (2), 217-227. Journal Impact Factor: 1.342
Abstract Aim. This paper reports a review which draws together findings from studies
targeting parents’ temperature-taking, antipyretic administration, attitudes, practices
and information-seeking behaviours.
Background. Parents’ concerns about the harmful effects of fever have been
reported for more than two decades. These concerns remain despite successful
educational interventions.
Method. Medline, CINAHL, PsycINFO, PsycARTICLES and Web of Science
databases were searched from 1980 to 2004 during November 2004. The search
terms were fever, child, parent, education, knowledge, belief, concern, temperature,
antipyretic and information, and combinations of these.
Findings. In the 1980s, studies were mainly descriptive of small single site samples
of parents with a febrile child seeking assistance from healthcare professionals. From
1990, sample sizes increased and multi-site studies were reported. Educational
interventions were designed to increase knowledge and reduce unnecessary use of
health services. One 2003 study targeted knowledge and attitudes. Parental
knowledge about normal body temperature and the temperature that indicates fever is
poor. Mild fever is misclassified by many as high, and parents actively reduce mild
fever with incorrect doses of antipyretics. Although some parents acknowledge the
benefits of mild fever, concerns about brain damage, febrile convulsions and death
from mild to moderate fever persist irrespective of parental education or socio-
51
economic status. Many base their fever management practices on inaccurate
temperature readings. Increased use of antipyretics to reduce fever and waking
sleeping febrile children for antipyretics or sponging reflects heightened concern
about harmful effects of fever. Educational interventions have reduced unnecessary
use of healthcare services, improved knowledge about fever and when to implement
management strategies, and reduced incorrect parental accuracy of antipyretic
dosing. Information-seeking behaviours in fever management differ according to
country of origin.
Conclusion. Despite successful educational interventions, little has changed in
parents’ fever management knowledge, attitudes and practices. There is a need for
interventions based on behaviour change theories to target the precursors of
behaviour, namely knowledge, attitudes, normative influences and parents’
perceptions of control.
Summary Statement What is already known about the topic
• Parents’ concerns about fever and its potential harm continue to be reported after
two decades of research and educational interventions.
• Parents’ decisions to seek medical assistance are frequently based on temperature
alone.
• Knowledge-based educational interventions have reduced parents’ inappropriate
use of healthcare services, increased knowledge and targeted inappropriate fever
management practices.
What this paper adds
• Parents are now more concerned about febrile convulsions than about brain damage
resulting from fever.
52
• Decisions to seek medical assistance are based on inaccurate temperature-taking
and use of low antipyretic doses.
• Educational programmes must be theoretically-based and target not only knowledge
but also the influences on parents’ and healthcare professionals’ attitudes,
normative influences and fever management practices.
3.1.1 Introduction
Parents are very concerned when they have a sick child, and often have difficulty
assessing the severity of the illness (Kai 1996a). Fever, a main indicator of illness, is
considered harmful by many parents (Crocetti et al. 2001) and a disease in itself
(Singhi et al. 1991). They often feel disempowered when their child is ill, and
believe they are not caring appropriately for their child if they do not treat the fever
(Kai 1996a). Papers describing parents' concern about and inappropriate management
of fever have been published in the healthcare literature over the past few decades,
and educational programmes developed to assist parents manage childhood fever
have proven effective (Casey et al. 1984, Crocetti et al. 2001, Sarrell & Kahan
2003). However, parents remain concerned about and mismanage fever, and seek
information and reassurance about their fever management practices from family,
friends, healthcare professionals, books, magazines and the Internet (e.g.
Impicciatore et al. 1998, Crocetti et al. 2001, Karwowska et al. 2002).
An article written in 1980 by Schmitt (1980) instigated interest in parents'
management of fever in the medical literature. Schmitt (1980) coined the phrase
'fever phobia' to describe parents' unrealistic fears about fever. This term has been
adopted to describe unrealistic fears about fever by both parents and healthcare
professionals (e.g. Abdullah et al. 1987, Sarrell et al. 2002). Since 1980, parents'
53
fever phobia, confirmed by their over-consultation of medical practitioners for minor
febrile illnesses, has been the impetus for most research in this area. Studies
conducted in the 1980s were descriptive and undertaken predominantly in the United
States of America (USA), with some in Canada and Saudi Arabia. During this
decade, only two controlled intervention studies were reported from the USA. The
1990s brought international interest in fever phobia, and descriptive studies were
published from the United Kingdom (UK), Italy, India and Israel and intervention
studies from the USA and UK. The quest to understand and enhance parental
management of fever continues into the 21st century as researchers try to understand
parents' concerns about fever and trial new methods to improve their fever
management. The aim of this paper is to review the literature reporting parents'
knowledge about fever, their attitudes towards it and their practices in the
management of childhood fever. Reports of educational interventions implemented
to assist parents' management of febrile children at home are also reviewed.
3.1.2 Search Method
During November 2004, Medline, CINAHL, PsycINFO, PsycARTICLES and Web
of Science databases were searched from January 1980 to October 2004. Papers were
included if they were from the developed world, written in English, explored fever in
common childhood illnesses (excluding, for example, meningitis and malaria) and, in
the case of quantitative studies, had sample sizes greater than 30. The search terms
were fever, child, parent, education, knowledge, belief, concern, temperature,
antipyretic and information, and combinations of these.
54
3.1.3 Findings
In this paper, we discuss the findings under the themes of parents' knowledge,
attitudes and practices in fever management, parents' sources of information about
fever management and educational interventions to improve parents' management of
childhood fever.
3.1.3.1 Parents’ Knowledge Temperature
Many people, healthcare professionals included, use body temperature to determine
state of health (e.g. Grossman et al. 1995, Blumenthal 2000, Edwards et al. 2001a,
Sarrell et al. 2002). Parents measure temperature by feeling body parts and/or using a
thermometer, but their knowledge of normal temperature and fever is poor. They
report that normal body temperature ranges from 35·0°C to 37·2°C (Singhi et al.
1991, Blumenthal 1998). Blumenthal (1998) found many parents in the UK did not
expect body temperature to rise on a hot summer day.
Although parents define temperatures between 37·0°C and 39·0°C as fever, 38·0°C
was the most commonly reported level they used for this (Kelly et al. 1996,
Blumenthal 1998, Impicciatore et al. 1998, Porter & Wenger 2000). High fever is
generally defined at temperatures around 39·0°C (Schmitt 1980, Singhi et al. 1991,
Karwowska et al. 2002); however, some parents recently reported high fever as
temperatures between 39·0°C and 40·0°C (Al-Eissa et al. 2000a, Crocetti et al.
2001). In the 1980s, 48% of parents reported that untreated temperatures could rise to
between 41·7°C and 43·3°C (Schmitt 1980, Kramer et al. 1985).
There has been limited exploration of the predictors of parental knowledge about
fever. In the 1980s, Kramer et al. (1985) discovered an inverse relationship between
55
the child's age and the minimum temperature considered as fever. Parents of younger
children considered higher temperatures to indicate fever than did parents of older
children. No differences were found in the temperature parents thought to indicate a
fever in a culturally-diverse population in the USA between Latinos, African
Americans and white Americans (Taveras et al. 2004). However, the height of fever
is commonly the deciding factor behind parents presenting at an emergency
department (McErlean et al. 2001).
Antipyretics
Parental knowledge about the effectiveness and appropriate dosing of antipyretics is
questionable. Knowledge about concentration differences between liquid
paracetamol and paracetamol drops is often incorrect (65%) (Barrett & Norton
2000), and some parents have reported that paracetamol and aspirin have
antihistamine, antiviral and decongestant properties (Ames et al. 1982) and that
paracetamol improves well-being (46%), prevents febrile convulsions (20%) or
prevents febrile convulsions and brain damage (28%) (Sarrell et al. 2002).
Although many parents are aware that an overdose of paracetamol could be
dangerous (62%) (Linder et al. 1999) or lethal (53%) (Kapasi et al. 1980), few are
aware of the possibility of liver toxicity (26%) (Linder et al. 1999). They (45%)
expect antipyretics to reduce temperatures to normal (Linder et al. 1999) and to
remain lowered for longer than the therapeutic time period (Kelly et al. 1996).
Knowledge about the effectiveness of antipyretics influences their decisions to seek
medical assistance. The failure of fever to respond to antipyretics is frequently the
reason parents attend emergency departments (Kelly et al. 1996, McErlean et al.
2001, Goldman & Scolnik 2004).
56
Many parents administer antipyretics in too low, too high or too frequent doses (Li
et al. 2000, Goldman & Scolnik 2004). Underdosing is more common in younger
and low weight children (Gribetz & Cronley 1987, Li et al. 2000), and incorrect
antipyretic dosing has been reported for nearly two decades. In 1987, 39% of parents
underdosed, 12% overdosed and only 32–35% correctly dosed febrile children with
paracetamol (Gribetz & Cronley 1987, Kilmon 1987). More recently, 47–49% of
febrile children presenting at emergency departments had received an appropriate
antipyretic doses prior to presentation (Li et al. 2000, McErlean et al. 2001, Goldman
& Scolnik 2004). Antipyretic doses administered by parents range between
6 mg/kg/dose (Gribetz & Cronley 1987) and 120 mg/kg/day (Linder et al. 1999).
Recently, the mean paracetamol dose administered by parents has been reported as
8·3 mg/kg/dose (Goldman & Scolnik 2004). Underdosing is associated with parents'
belief that a 5 mL teaspoon holds only 3 mL (Hyam et al. 1989, Linder et al. 1999),
not increasing dosages with the child's weight (Linder et al. 1999), incorrect beliefs
about the concentrations of children's paracetamol liquid and drops (Barrett &
Norton 2000) and determining the dose based on the child's age or temperature (Li
et al. 2000). Although there has been some improvement in correct antipyretic
dosing over the past two decades, overdosing has increased. In Linder et al.'s (1999)
study, 43% of parents correctly dosed their child, 24% underdosed and 33%
overdosed.
Alternating antipyretics is the latest reported parental method for controlling fever.
When parents do not perceive the antipyresis from one antipyretic (e.g. paracetamol)
to be satisfactory, they administer another (e.g. ibuprofen) 1–2 hours later. This
introduces another avenue for incorrect antipyretic usage (Crocetti et al. 2001).
Crocetti et al. (2001) found that 27% of parents alternate antipyretics. Li et al. (2000)
57
reported that parents incorrectly dosed children with one or both the antipyretics
paracetamol and/or ibuprofen, 7% of children (14 out of 200) received alternating
antipyretics, and only one child received correct doses of both. Overdosing was more
likely with ibuprofen than paracetamol both in dosage and frequency. Fever
legitimizes parents' use of antipyretics for fever-related problems such as helping the
child during illness, alleviating suffering, providing comfort, enabling the child to
sleep and giving parents a feeling of coping (Lagerlov et al. 2003).
Predictors of parental knowledge about antipyretics and correct dosing were
identified in the 1980s, education, income and age predicting antipyretic knowledge
(Ames et al. 1982). Less knowledge was associated with lower educational levels (7–
12 years of formal education), age between 15 and 30 years, lower income levels or
use of subsidized public health care. However, in the late 1990s it was reported that
younger mothers were more likely to read the instructions included with the bottle
and comply with recommended dosages (Linder et al. 1999). These differences have
not been found in the 21st century. More recent studies have focused on antipyretic
use rather than knowledge per se. Learning about antipyretics from doctors made no
difference to parents' antipyretic knowledge. Neither parent nor child variables have
been found to predict parental antipyretic knowledge (Barrett & Norton 2000) or
accurate antipyretic usage (McErlean et al. 2001).
Summary
In summary, parents' knowledge about normal body temperature and the temperature
that defines fever is poor. They classify mild fever as high and actively reduce
temperatures, sometimes normal temperatures, with incorrect doses of antipyretics.
When underdosed children's temperatures are not reduced to a level parents consider
58
satisfactory, they seek professional assistance, placing additional burdens on already
strained healthcare systems.
3.1.3.2 Attitudes
Parental fever phobia, concern about, and inappropriate treatment of, childhood fever
are well documented and possibly multifactorially caused (e.g. Schmitt 1980, Kramer
et al. 1985, Knoebel et al. 2002). This may be caused by past personal experience
with febrile children, anecdotal tragic outcomes of febrile children, cultural
influences and information from family, healthcare professionals and other sources
(Poirier et al. 2000). Over the 24 years of literature reviewed, many parents were
reported as believing fever to be harmful and being very worried about these
perceived harmful effects, despite numerous reports of the benefits of mild to
moderate fever in the medical and scientific literature (e.g. Kluger 1986, Lorin 1986,
1999, Zeisberger 1999, Mackowiak 2000, Blatteis 2003, Roth et al. 2004).
Parents' perceptions of the temperature at which fever is harmful have changed over
time. In the 1980s, although in the USA 94% of American parents of well children
(n = 100) believed fever to be harmful, only 4% believed temperatures in a normal
range, 37·8°C or lower, to be harmful; 48% believed temperatures below 40°C
(moderate fever) to be harmful (Schmitt 1980). In a recent Israeli study, 43%
(n = 1000) believed in the beneficial effects of low grade fever (37–38°C) during
infection; however, 57% believed that low grade fevers (38°C or lower) were
harmful (Sarrell et al. 2002).
Parental ratings of the harmful effects of fever have changed from 1980 to 2004,
although their main concerns continue to be brain damage, febrile convulsions and
death (e.g. Schmitt 1980, Kramer et al. 1985, Al-Eissa et al. 2000a, Crocetti et al.
59
2001, Karwowska et al. 2002). In the 1980s, they were more concerned about brain
damage (38–46%) than febrile convulsions (15–39%) (Schmitt 1980, Abdullah et al.
1987). More recently, although concerns about brain damage remain (21–53%),
concerns about febrile convulsions have increased dramatically (32–70%) (Al-Eissa
et al. 2000a, Crocetti et al. 2001, Karwowska et al. 2002). Reports of concerns that
fever is a sign of serious illness have reduced from 12–43% in the 1980s (Schmitt
1980, Abdullah et al. 1987) to 2–28% in the 2000s (Al-Eissa et al. 2000a, Crocetti
et al. 2001). Interestingly, an increase in parental concern about dehydration (80%)
and discomfort (75%) was recently reported by Canadian parents (Karwowska et al.
2002), compared with 4–8% in the 1980s (Schmitt 1980, Anderson 1988).
Although most research exploring parental attitudes and practices in fever
management has been quantitative, some qualitative studies during the past decade
have explored their perceptions of fever. Kai (1996b) found that these concerns were
influenced by the perceived threat of the illness and anxieties about fever, coughs
and the possibility of meningitis. These anxieties were heightened by the knowledge
that non-specific symptoms could precede a rapidly-progressing, serious illness. The
degree of parental concern about a symptom (e.g. fever or cough) was dependent on
the perception of the symptom hurting their child. Parents' personal control is
threatened by their child's illness, and attempts to maintain control include
monitoring symptoms and minimising discomfort. Lagerlov et al. (2003) has
reported that, although parents acknowledge that low to moderate fever reflects the
body's immunological response, they consider high or rapidly rising fever dangerous.
Predictors for parents' concerns about fever have been identified. Italian mothers'
concerns were positively associated with lack of information about fever
60
management, moderate fever in their child, inexperience with managing febrile
children and low maternal educational levels (Impicciatore et al. 1998). Other studies
corroborate these predictors, even among highly educated people and those in higher
socioeconomic classes (Kramer et al. 1985, Singhi et al. 1991). There has been little
change in these predictors over the last two decades (Crocetti et al. 2001).
Summary
In summary, although there is a move toward acknowledging the benefits of mild
fever, attitudes toward it remain negative. Beliefs about its harmful outcomes
identified in the 1980s (e.g. brain damage, febrile convulsions and death) persist,
irrespective of parental education or socio-economic status. Concerns about febrile
convulsions, dehydration and discomfort associated with fever have increased, and
attitudes toward fever seem to be similar irrespective of country of origin.
3.1.3.3 Practices Temperature-Taking
Although parents are concerned about the height of their child's temperature, not all
have a thermometer (38–44%) (Fischer et al. 1985). Owning a thermometer does not
predict ability to accurately take a temperature or read a thermometer. Several reports
state that few parents (30–46%) can accurately take a temperature and read a
thermometer (Fischer et al. 1985, Porter & Wenger 2000, Taveras et al. 2004).
Despite this, parents take febrile children's temperatures regularly, often hourly
(Crocetti et al. 2001), and initiate activities to reduce temperatures; sometimes this is
done with temperatures within a normal range (Schmitt 1980, Kilmon 1987,
Blumenthal 1998, Crocetti et al. 2001, Sarrell et al. 2002).
61
Correlations between inability to take a temperature accurately and parent variables
have been examined. Lower socioeconomic status and not owning a thermometer
predict an inability to read a thermometer accurately (Fischer et al. 1985). Fischer et
al. found no relationship between maternal age or the presence of other children in
the home and ability to read a thermometer. Banco and Jayasherkaramurthy (1990)
discovered that younger parents and those with higher socioeconomic backgrounds
and higher educational levels were more likely to own and accurately read a mercury
thermometer. This was corroborated by Porter and Wenger (2000), who found that
maternal age, educational level and socioeconomic status predicted accuracy of
temperature-talking.
3.1.3.4 Fever Management
Antipyretics have been and remain, for many parents, the preferred method for
reducing fevers (e.g. Kramer et al. 1985, Anderson 1988, Kelly et al. 1996,
Impicciatore et al. 1998, Linder et al. 1999, McErlean et al. 2001). They prefer to
treat fever with antipyretics rather than removing clothing or tepid sponging
(Kinmonth et al. 1992). Antipyretic use in fever management has increased from
67% of parents in 1980 (Schmitt 1980) to 95% in 2002 (Karwowska et al. 2002). In
the 1980s, parents administered antipyretics to children with normal temperatures
(67%) (Schmitt 1980) and temperatures below 38·3°C (71%) (Casey et al. 1984).
More recently, only 23% of parents reported treating fevers below 37·8°C with
antipyretics (Crocetti et al. 2001). Today, parents (46%) use antipyretics to promote
their child's well-being during a febrile episode (Sarrell et al. 2002), and this gives
them a feeling of mastery when their child is ill (Lagerlov et al. 2003).

62
Parents' practices have not changed. Waking sleeping febrile children for an
antipyretic was one of the early factors describing fever phobia (Schmitt 1980). In
1980, 48–53% of parents woke sleeping febrile children (Schmitt 1980, Kramer et al.
1985), and today this has increased to between 66% and 92% (Al-Eissa et al. 2000b,
Crocetti et al. 2001, Sarrell et al. 2002). Parents need reassurance that they are
managing their febrile child appropriately and often contact doctors about low fevers
or those of short duration (Kramer et al. 1985, Singhi et al. 1991, Kelly et al. 1996,
Impicciatore et al. 1998). Although this creates guilt in some parents, they feel that
they have little choice and need to share responsibility for their febrile child (Kai
1996b).
Other fever management practices in the 1980s included the use of tepid, cold or ice-
cold water and alcohol rubs (Schmitt 1980, Kramer et al. 1985, Abdullah et al. 1987,
Anderson 1988). Although tepid sponging has continued into the early 2000s (Al-
Eissa et al. 2000b, Crocetti et al. 2001, Karwowska et al. 2002), the use of cold or
ice-cold water and alcohol rubs has reduced considerably (Karwowska et al. 2002).
However, in Saudi Arabia, some parents continue to keep their febrile child warm by
controlling the ambient temperature or using additional clothing (Abdullah et al.
1987, Al-Eissa et al. 2000b), and continue to combine treatments such as tepid
sponging and antipyretic administration (Kramer et al. 1985, Blumenthal 1998, Al-
Eissa et al. 2000a). One fever management practice that has changed since the
documented association between Reye syndrome, aspirin and influenza is the use of
aspirin as an antipyretic; this has almost disappeared, along with a decline in the
incidence of Reye syndrome (Drwal-Klein & Phelps 1992, Cranswick 2000).
63
Summary
Although parents do not take accurate temperatures, they continue to base their fever
management practices on temperature. Today, fewer aim to reduce temperatures in
normal ranges, and some practices, such as the use of aspirin and cold or iced water
to reduce fever, have reduced. Other practices reflect an increased concern about
harmful effects of fever and the need for control during this frightening time. These
include increased use of antipyretics and waking sleeping febrile children for
antipyretics or sponging.
3.1.3.5 Limitations
The data above describe parents' knowledge, attitudes and practices in fever
management. Similar findings have been found in a number of different countries
and cultures; however, in most studies data were collected from concerned parents
seeking medical assistance for a concern such as fever or injury. Therefore the
findings might not be generalisable. Longitudinal studies have not been reported.
Parents' knowledge, attitudes and practices could change over time as the child ages
or with the birth of subsequent children.
Most studies in the 1980s exploring parents' management of fever were descriptive
cross-sectional studies using small single-site, convenience samples (36–249) from
hospitals or health clinics (e.g. Schmitt 1980, Ames et al. 1982, Kramer et al. 1985,
Abdullah et al. 1987). Instruments were researcher-developed (e.g. Schmitt 1980,
Casey et al. 1984, Kramer et al. 1985), sometimes the questions were reported (e.g.
Schmitt 1980, Kramer et al. 1985), and only one study compared findings with
earlier studies by using previously-developed questions (Anderson 1988). However,
64
instrument reliability, validity and data analysis were generally not reported (e.g.
Schmitt 1980, Kramer et al. 1985, Abdullah et al. 1987).
Larger samples (100–1237) were explored from 1990 onwards. Multi-site studies
were reported more frequently than single-site studies. Again, descriptive, cross-
sectional, comparative and multi-site studies compared the perceptions of
convenience samples of parents with febrile and afebrile children (e.g. Banco &
Jayasherkaramurthy 1990, Impicciatore et al. 1998, Linder et al. 1999). Community-
based studies were reported more frequently – three from 1990 to 2004 (Kai 1996b,
Impicciatore et al. 1998, Linder et al. 1999) – compared with one in the 1980s
(Anderson 1988). Instrument reliability and data analysis were reported more
frequently in the 1990s (e.g., Kai 1996b, Kelly et al. 1996, Impicciatore et al. 1998)
and in most studies from 2000 onwards.
3.1.3.6 Information Sources Fever
Parents learn to manage fever from different sources. In India, they were more likely
to learn from parents and relatives than doctors, friends or reading. However,
educated parents from higher socioeconomic backgrounds are more likely to learn
from reading and doctors (Singhi et al. 1991). Saudi Arabian parents are equally
likely to learn fever management from relatives and friends, doctors and reading (Al-
Eissa et al. 2000b). Italian mothers are more likely to learn to manage fever from
doctors during a febrile episode than during a visit when the child is well
(Impicciatore et al. 1998). More parents in the USA learn from doctors and nurses
than friends and relatives, experience, reading or television (Crocetti et al. 2001).
Canadian parents are most likely to learn from doctors (Karwowska et al. 2002),

65
while other regular sources are family, nurses, books, magazines, and some gather
information from the Internet and television.
Antipyretics
In the USA in the 1980s, parents learnt antipyretic dosing from doctors, previous
experience, friends, product advertising and medical reference books (Ames et al.
1982). In the 21st century, they are more likely to gather medication information
from doctors and packaging (Li et al. 2000). However, the source of antipyretic
information does not lead to a significant difference between correct and incorrect
doses in the USA (Li et al. 2000). Israeli parents learn from doctors,
mothers/grandmothers and instructions on containers (Linder et al. 1999).
3.1.3.7 Educational Interventions
Controlled educational interventions have effectively enhanced parents' knowledge
and fever management practices, reduced fever-related anxiety, fever-related clinic
visits and telephone calls to doctors. During the 1980s, experimental studies were
undertaken in health clinics to reduce inappropriate visits by educating parents about
fever management (Casey et al. 1984, Robinson et al. 1989). These studies
effectively increased the knowledge of parents from middle socioeconomic
background and reduced antipyretic use for temperatures below 38·3°C, dosing
errors and physician visits and telephone calls (Casey et al. 1984, Robinson et al.
1989). These positive changes were still evident 6 months after the intervention.
A randomized, controlled community-based study in the UK determined the effect
on general practice clinic visits of an educational booklet explaining the symptoms
and management of childhood illnesses such as fever, cough, sore throat and
diarrhoea (Usherwood 1991). Although it did not reduce clinic visits for fever, home
66
visits and out-of-hours calls for febrile children were statistically significantly
reduced. A paediatrician-administered intervention about the benefits of fever and
appropriate fever management practice was successful in Israel (Sarrell & Kahan
2003); parents' definitions of the different levels of fever (low, moderate and high)
were corrected, knowledge of when to initiate non-pharmacological rather than
pharmacological fever management reduction strategies was improved, and the
number of visits to paediatricians and emergency departments for febrile concerns
was reduced.
Nursing interventions have also been implemented. A comparative, pre- and post-test
study explored the effectiveness of educational interventions among minority groups
with lower socioeconomic backgrounds using an instruction sheet focused on aspects
of fever and its management (Kelly et al. 1996). Although unsuccessful in altering
knowledge of the temperature at which an antipyretic should be administered, the
intervention did improve accuracy of medication dosing. Quasi-experimental
interventions in emergency departments have successfully reduced parental anxiety,
improved caretakers' home management of fever and reduced emergency department
visits for fever (Murphy & Liebman 1995, O'Neill-Murphy et al. 2001).
Murphy and Liebman (1995) explored the efficacy of different teaching methods in
reducing parental anxiety, increasing ability to read a thermometer and managing
fever at home. Demonstration, discussion and written educational methods were
equally effective. O'Neill-Murphy et al. (2001) found a standard written fever
pamphlet and interactive educational intervention equally effective. A recent
American study by Broome et al. (2003) attempted a theoretically-based
intervention. Based on the attitudinal construct of the Theory of Planned Behavior
67
(Ajzen 1985), they explored influence of knowledge and attitudes on decision-
making. They claimed that increasing parents' knowledge about assessing childhood
fevers, communicating with healthcare professionals and implementing prescribed
fever management therapies would change parents' attitudes toward and knowledge
about fever management. Their experimental group had statistically significantly
more knowledge and an increase, though not statistically significant, in confidence in
fever management. However, changes in attitudes were not reported.
Summary
Educational interventions have successfully reduced parents' unnecessary use of
healthcare services for childhood fever. Additionally, they have improved knowledge
about fever, when to implement management strategies and accuracy of antipyretic
dosing through various mediums. Different educational media (e.g. discussion with
healthcare professionals, videos, pamphlets and booklets) and a combination of these
have not influenced outcomes. Only one intervention was theoretically-based and
addressed attitudes; all others targeted knowledge to change fever management
behaviours. There is a need for theoretically-based interventions to target not only
knowledge, but also attitudes, intentions and practices in fever management.
Limitations
Many intervention studies have targeted knowledge only and used potentially biased
convenience samples of parents concerned about fever and those attending
paediatricians (Sarrell & Kahan 2003) and emergency departments (e.g. Murphy &
Liebman 1995, O'Neill-Murphy et al. 2001) for fever related concerns. Some studies
reported reduced inappropriate healthcare professional contact for childhood fevers
and increased parental knowledge (e.g. Casey et al. 1984, Robinson et al. 1989,
68
Broome et al. 2003), although not all did (Kelly et al. 1996). Samples in comparative
studies were small (52–156) (Kinmonth et al. 1992, Kelly et al. 1996). Quasi-
experimental studies had similarly-sized samples (87–130) (Casey et al. 1984,
Murphy & Liebman 1995, O'Neill-Murphy et al. 2001, Sarrell & Kahan 2003), and
samples in randomized controlled trials ranged from 216–497 (Robinson et al. 1989,
Usherwood 1991, Broome et al. 2003).
3.1.4 Discussion
There have been few changes in parents' knowledge, attitudes and practices over the
past two decades. They continue actively to reduce low grade fevers despite
persistent recommendations in the literature that only temperatures of 40°C or higher
be reduced; temperatures below 40°C support immunological activities associated
with fever (Lorin 1994, 1999, Connell 1997). Definitions of high fever, although
moving in the right direction, remain low at 40°C. Sarrell et al. (2002) defined
moderate fever as 40·0°C. Height of fever remains a common deciding factor in
seeking medical assistance and when, associated with antipyretic underdosing and
unrealistic expectations from antipyretics, overuse of medical services for febrile
children is understandable. The incidence of antipyretic overdosing has nearly
trebled in the last 20 years and concerns about overdosing, particularly in connection
with alternating antipyretics, are appropriate. An important issue for healthcare
professionals is the lack of association between parents' appropriate antipyretic use
and learning about antipyretics from healthcare professionals. This needs further
exploration.
Parental fever phobia, or unrealistic concerns about fever, persists. Increased
concerns about meningitis could result from the extensive media coverage of rare,
69
serious childhood illnesses, such as meningococcal meningitis. However, the reasons
for increased concerns need to be explored.
Educational interventions have improved parental knowledge and practices. Why,
then, are there no great changes in parents' knowledge, attitudes and practices over
the past two decades? Many educational programmes had specific goals, such as
reduction in parents' use of medical services for self-limiting viral infections. In order
to change behaviour, these interventions targeted knowledge and not attitudes or
environmental factors such as social influences and parental control when a child has
fever. Descriptive studies were often just that, rather than precursors of educational
interventions targeting parents' specific needs. There is a need to identify parental
knowledge, attitudes and practices and then to develop educational interventions
based on a behaviour change theory proven to be effective in situations where people
have an emotional involvement in a behaviour that is not always totally under their
control. The Theory of Planned Behavior (Ajzen 1985) has identified the predictors
of behaviours such as safe sex (McCamish et al. 1994) and nurses' management of
postoperative pain (Edwards et al. 2001a,b), and guided the development and
implementation of successful educational interventions. Predictors of other health
behaviours identified by this theory include smoking cessation following coronary
artery bypass surgery (Bursey & Craig 2000), breastfeeding (Janke 1994), breast or
testicular self-examination (McCaul et al. 1993), parents use of booster seats in cars
(Ferraro 2004) and pregnant adolescents' intentions to breastfeed (Wambach 1997,
Wambach & Koehn 2004).
The constancy of knowledge, attitudes and practices in countries where new parents
learn from their parents to manage fever is understandable. However, this is

70
unacceptable in countries where parents learn from healthcare professionals. An
exploration of the literature reporting healthcare professionals' knowledge, attitudes
and practices in this area sheds some light, and professional concerns about harmful
effects of fever (Abdullah et al. 1987, Thomas et al. 1994, Walsh et al. 2005) and
fever phobia (May & Bauchner 1992, Poirier et al. 2000, Sarrell et al. 2002) continue
to be reported. This could explain similarities in fever-related concerns between
parents who learn to manage fever from professionals and from previous generations.
Health education is a responsibility of all healthcare professionals. Fever education
must be based on the latest scientific evidence, and professionals' attitudes toward the
benefits of mild to moderate fever must be positive. To ensure that parents are
equipped to manage a febrile episode, health education should be included in clinic
visits when the child is well, preferably prior to a febrile episode. Parents must be
advised about accurate temperature-taking, how to care safely for a febrile child,
when to seek professional advice, the role of fever in the immunological process,
when to reduce fever with antipyretics, and how to administer antipyretics safely.
Reports in the literature highlight the need for parental and healthcare professional
education about fever and fever management to ensure that children are cared for
safely at home without seeking medical advice and reassurance for each febrile
episode.
3.1.5 Conclusion
Caring for a febrile child is emotionally challenging for parents, and limited
improvements in knowledge, attitudes and practices highlight the need for structured
research programmes. To develop such programmes, an assessment of parents'
knowledge, attitudes, practices and educational needs must precede the development
71
of theoretically-based interventions. Evidence-based health education by healthcare
professionals, and particularly by nurses delivering maternal-child health care,
should aim to precede a child's first febrile episode. Fever management education
must highlight the benefits of fever and equip parents with appropriate knowledge
and skills to manage mild to moderate fevers without unnecessary health professional
consultation. Figure 3.1 describes the components necessary for effective fever
management education.
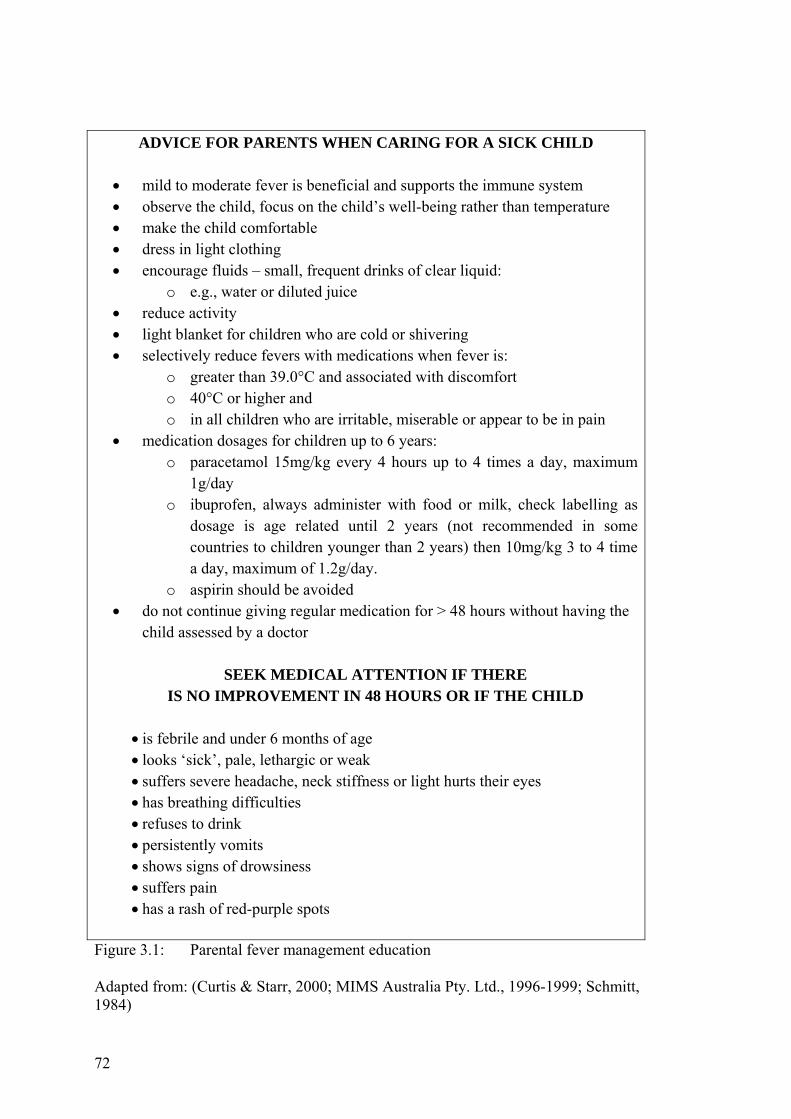
72
ADVICE FOR PARENTS WHEN CARING FOR A SICK CHILD
• mild to moderate fever is beneficial and supports the immune system • observe the child, focus on the child’s well-being rather than temperature • make the child comfortable • dress in light clothing • encourage fluids – small, frequent drinks of clear liquid:
o e.g., water or diluted juice • reduce activity • light blanket for children who are cold or shivering • selectively reduce fevers with medications when fever is:
o greater than 39.0°C and associated with discomfort o 40°C or higher and o in all children who are irritable, miserable or appear to be in pain
• medication dosages for children up to 6 years: o paracetamol 15mg/kg every 4 hours up to 4 times a day, maximum
1g/day o ibuprofen, always administer with food or milk, check labelling as
dosage is age related until 2 years (not recommended in some countries to children younger than 2 years) then 10mg/kg 3 to 4 time a day, maximum of 1.2g/day.
o aspirin should be avoided • do not continue giving regular medication for > 48 hours without having the
child assessed by a doctor
SEEK MEDICAL ATTENTION IF THERE IS NO IMPROVEMENT IN 48 HOURS OR IF THE CHILD
• is febrile and under 6 months of age • looks ‘sick’, pale, lethargic or weak • suffers severe headache, neck stiffness or light hurts their eyes • has breathing difficulties • refuses to drink • persistently vomits • shows signs of drowsiness • suffers pain • has a rash of red-purple spots
Figure 3.1: Parental fever management education Adapted from: (Curtis & Starr, 2000; MIMS Australia Pty. Ltd., 1996-1999; Schmitt, 1984)
73
3.1.6 References Abdullah, M. A., Ashong, E. F., Al Habib, S. A., Karrar, Z. A., & Al Jishi, N.
M. (1987). Fever in children: diagnosis and management by nurses, medical students, doctors and parents. Annals of Tropical Paediatrics, 7(3), 194-199.
Ajzen, I. (1985). From intentions to actions: a theory of planned behavior. In J.
Kuhl & J. Beckmann (Eds.), Action control: from cognition to behavior (pp. 11-39). Berlin: Springer Verlag.
Al-Eissa, Y. A., Al-Sanie, A. M., Al-Alola, S. A., Al-Shaalan, M. A., Ghazal,
S. S., Al-Harbi, A. H., et al. (2000). Parental perceptions of fever in children. Annals of Saudi Medicine, 20(3-4), 202-205.
Al-Eissa, Y. A., Al-Zamil, F. A., Al-Sanie, A. M., Al-Salloum, A. A., Al-
Tuwaijri, H. M., Al-Abdali, N. M., et al. (2000). Home management of fever in children: rational or ritual? International Journal of Clinical Practice, 54(3), 138-142.
Allen, J., Dyas, J., & Jones, M. (2002). Minor illnesses in children: parent's
views and use of health services. British Journal of Community Nursing, 7(9), 462-468.
Allotey, P., Reidpath, D. D., & Elsisha, D. (2004). "Social medication" and the
control of children: a qualitative study of over-the-counter medication among Australian children. Pediatrics, 114(3), e378-e383.
Ames, J. T., Hayden, G. F., Campbell, R. E., & Lohr, J. A. (1982). Parents'
conception of their use of over-the-counter medicines. Clinical Pediatrics, 21(5), 298-301.
Anderson, A. R. (1988). Parental perception and management of school-age
children's fevers. Nurse Practitioner, 5(May), 8-18. Banco, L., & Jayasherkaramurthy, S. (1990). The ability of mothers to read a
thermometer. Clinical Pediatrics, 29, 343-345. Barrett, T. W., & Norton, V. C. (2000). Parental Knowledge of Different
Acetaminophen Concentrations for Infants and Children. Academy of Emergency Medicine, 7(6), 718-721.
Baumann, R. J. (2001). Prevention and management of febrile seizures.
Paediatric Drugs, 3(8), 585-592.
74
Blatteis, C. M. (2003). Fever: pathological or physiological, injurious or beneficial? Journal of Thermal Biology, 28(1), 1-13.
Blumenthal, I. (1998). What parents think of fever. Family Practice, 15(6),
513-518. Blumenthal, I. (2000). Fever and the practice nurse: management and
treatment. Community Practitioner, 73(3), 519-521. Broome, M. E., Dokken, D. L., Broome, C. D., Woodring, B., & Stegelman,
M. F. (2003). A study of parent/grandparent education for managing a febrile illness using the CALM approach. Journal of Pediatric Health Care, 17(4), 176-183.
Casey, R., McMahon, F., McCormick, M. C., Pasquariello, P. S., Zavod, W.,
& King, F. H. (1984). Fever therapy: an educational intervention for parents. Pediatrics, 73(5), 600-605.
Connell, F. (1997). The causes and treatment of fever: a literature review.
Nursing Standard, 12(11), 40-43. Cranswick, N. C., D. (2000). Paracetamol efficacy and safety in children: the
first 40 years. American Journal of Therapeutics, 7(2), 135-141. Crocetti, M., Moghbeli, N., & Serwint, J. (2001). Fever phobia revisited: have
parental misconceptions about fever changed in 20 years? Pediatrics, 107(8), 1241-1246.
Curtis, N., & Starr, M. (2000). Infectious diseases. In J. Smart & T. Nolan
(Eds.), Paediatric handbook (6th ed., pp. 365-405). Calton South, Victoria: Blackwell Science.
D'Auria, J. P. (1997). Fever. In J. A. Fox (Ed.), Primary health care of
children (pp. 770-776). New York: Mosby. Dawson, K. P., & Capaldi, N. (1994). The initial hospital management of
childhood febrile convulsions: an audit. Journal of Quality Clinical Practice, 14(2), 111-114.
Drwal-Klein, L. A., & Phelps, S. J. (1992). Antipyretic therapy in the febrile
child. Clinical pharmacy, 11(12), 1005-1021. Edwards, H. E., Courtney, M. D., Wilson, J. E., Monaghan, S. J., & Walsh, A.
M. (2001). Fever management practices: what pediatric nurses say. Nursing and Health Sciences, 3(3), 119-130.
75
Fischer, H., Moore, K., & Roaman, R. R. (1985). Can mothers of infants read a thermometer? Clinical Pediatrics, 24, 120.
Freeman, J. M. (1992). The best medicine for febrile seizures. The New
England Journal of Medicine, 327(16), 1161 - 1163. Goldman, R. D., & Scolnik, D. (2004). Underdosing of acetaminophen by
parents and emergency utilization. Pediatric Emergency Care, 20(2), 89-93.
Gribetz, B., & Cronley, S. A. (1987). Underdosing of Acetaminophen by
parents. Pediatrics, 80(5), 630-633. Grossman, D., Keen, M. F., Singer, M., & Asher, M. (1995). Current nursing
practices in fever management. MEDSURG Nursing, 4(3), 193-198. Haddow, G., & Watts, R. (2003). Caring for a febrile child: the quality of
Internet information. Collegian, 10(2), 7-12. Hyam, E., Brawer, M., Herman, J., & Zviele, S. (1989). What's in a teaspoon?
Underdosing with acetaminophen in family practice. Family Practice, 6, 221-223.
Impicciatore, P., Nannini, S., Pandolfini, C., & Bonati, M. (1998). Mothers'
knowledge of, attitudes toward, and management of fever in preschool children in Italy. Preventive Medicine, 27(2), 268-273.
Johnson, E. W., Dubovsky, J., Rich, S. S., O'Donovan, C. A., Orr, H. T.,
Anderson, V. E., et al. (1998). Evidence for a novel gene for familial febrile convulsions, FEB2, linked to chromosome 19p in an extended family from the Midwest. Human Molecular Genetics, 7(1), 63-67.
Kai, J. (1996a). Parents' difficulties and information needs in coping with
acute illnesses in preschool children: a qualitative study. British Journal of Medicine, 313, 987-990.
Kai, J. (1996b). What worries parents when their preschool children are
acutely ill, and why: a qualitative study. British Medical Journal, 313, 983-986.
Kapasi, A. A., Lorin, M. I., Nirken, M. H., & Yudovich, M. (1980). Parents'
knowledge and sources of knowledge about antipyretic drugs. Journal of Pediatrics, 97, 1035-1037.
76
Karwowska, A., Nijssen-Jordan, C., Johnson, D., & Davies, H. (2002). Parental and health care provider understanding of childhood fever: a Canadian perspective. Canadian Journal of Emergency Medicine, 4(6), 394-400.
Kelly, L., Morin, K., & Young, D. (1996). Improving caretakers' knowledge of
fever management in preschool children: is it possible? Journal of Pediatric Health Care, 10(4), 167-173.
Kilmon, C. (1987). Parents' knowledge and practices related to fever
management. Journal of Pediatric Health Care, 1(4), 173-179. Kinmonth, A., Fulton, Y., & Campbell, M. J. (1992). Management of feverish
children at home. British Medical Journal, 305(7), 1134-1136. Kluger, M. (1986). Is fever beneficial. The Yale Journal of Biology and
Medicine, 59(2), 89-95. Kluger, S. L., & Johnson, W. G. (1998). Genetics of the febrile seizure
susceptibility trait. Brain and Development, 20, 265-274. Knoebel, E. E., Narang, A. S., & Ey, J. L. (2002). Fever: to treat or not to
treat. Clinical Pediatrics, 41(1), 9-16. Kramer, M. S., Naimark, L. E., & Leduc, D. G. (1985). Parental fever phobia
and its correlates. Pediatrics, 75(6), 1110-1113. Krantz, C. (2001). Childhood fevers: developing an evidence-based
anticipatory guidance tool for parents. Pediatric Nursing, 27(6), 567-573.
Lagerlov, P., Helseth, S., & Holager, T. (2003). Childhood illnesses and the
use of paracetamol (acetaminophen): a qualitative study of parents' management of common childhood illnesses. Family Practice, 20(6), 717-723.
Li, S. F., Lacher, B., & Crain, E. F. (2000). Acetaminophen and ibuprofen
dosing by parents. Pediatric Emergency Care, 16(6), 394-397. Linder, N., Sirota, L., Snapir, A., Eisen, I., Davidovitch, N., Kaplan, G., et al.
(1999). Parental knowledge of the treatment of fever in children. Israel Medical Association Journal: IMAJ, 1(3), 158-160.
Lorin, M. I. (1986). Is fever a friend or a foe? Contemporary Pediatircs, 3, 35-
46.
77
Lorin, M. I. (1994). Pathogenesis of fever and its treatment. In F. Oski, DeAngellis, C.D., Feigin, R.D., McMillan, J.A., Warshaw, J.B. (Ed.), Principles and practice of pediatrics (2nd ed., pp. 1111-1113). Philadelphia PA: J.B. Lippincott.
Lorin, M. I. (1999). Pathogenesis of fever and its treatment. In J. B. McMillan,
C. DeAngelis, R. D. Feigin & J. B. Warshaw (Eds.), Oski's Pediatrics: principles and practices (3rd ed., pp. 848-850). Philadelphia: Lippincott, Williams & Wilkins.
Mackowiak, P. A. (2000). Diagnostic implications and clinical consequences
of antipyretic therapy. Clinical Infectious Diseases, 31, S230-S233. May, A., & Bauchner, H. (1992). Fever phobia: the pediatrician's contribution.
Pediatrics, 90(6), 851-854. McErlean, M. A., Bartfield, J. M., Kennedy, D. A., Gilman, E. A., Stram, R.
L., & Raccio-Robak, N. (2001). Home antipyretic use in children brought to the emergency department. Pediatric Emergency Care, 17(4), 249-251.
MIMS Australia Pty. Ltd. (1996-1999). E-MIMS 4.0 Australia (1996-1999).
Retrieved 2000, 20/5/2000, from www.mims.com.au Murphy, K. A., & Liebman, M. (1995). Fever care: does nursing instruction
make a difference? Journal of Emergency Nursing, 21(5), 461-463. O'Neill-Murphy, K., Liebman, M., & Barnsteiner, J. H. (2001). Fever
education: does it reduce parent fever anxiety? Pediatric Emergency Care, 17(1), 47-51.
Poirier, M. P., Davis, P. H., Gonzalez-del Rey, J. A., & Monroe, K. W. (2000).
Pediatric emergency department nurses' perspectives on fever in children. Pediatric Emergency Care, 16(1), 9-12.
Porter, R. S., & Wenger, F. G. (2000). Diagnosis and treatment of pediatric
fever by caretakers. Journal of Emergency Medicine, 19(1), 1-4. Purssell, E. (2000). The use of antipyretic medications in the prevention of
febrile convulsions in children. Journal of Clinical Nursing, 9(4), 473-480.
Robinson, J. S., Schwartz, M., Magwene, K. S., Kreugel, S. A., & Tamburello,
D. (1989). The impact of fever education on clinic utilization. American Journal of Diseases in Children, 143, 698-704.

78
Roth, J., Rummel, C., Harre, E.-M., Voss, T., Mutze, J., Gerstberger, R., et al. (2004). Is interleukin-6 the necessary pyrogenic cytokine? Journal of Thermal Biology, 29(7-8), 383-389.
Sadovsky, R. (2002). Managing seizures associated with fever in children.
American Family Physician, 65(10), 2155. Sarrell, M., Cohen, H. A., & Kahan, E. (2002). Physicians', nurses', and
parents' attitudes to and knowledge about fever in early childhood. Patient Education and Counselling, 46, 61-65.
Sarrell, M., & Kahan, E. (2003). Impact of a single-session education program
on parental knowledge of and approach to childhood fever. Patient Education and Counseling, 51, 59-63.
Schmitt, B. D. (1980). Fever phobia: misconceptions of parents about fevers.
American Journal of Diseases in Children, 134(2), 176-181. Schmitt, B. D. (1984). Fever in childhood. Pediatrics, 74 (Suppl), 929-936. Singhi, S., Padmini, P., & Sood, V. (1991). Urban parents' understanding of
fever in children: its danger and treatment practices. Indian Pediatrics, 28(5), 501-505.
Taveras, E. M., Durousseau, S., & Flores, G. (2004). Parents' beliefs and
practices regarding childhood fever - A study of a multiethnic and socioeconomically diverse sample of parents. Pediatric Emergency Care, 20(9), 579-587.
Thomas, V., Riegel, B., Andrea, J., Murray, P., Gerhart, A., & Gocka, I.
(1994). National survey of pediatric fever management practices among emergency department nurses. Journal of Emergency Nurses, 20(6), 505.
Usherwood, T. P. (1991). Development and randomised controlled trial of a
booklet of advice for parents. British Journal of General Practice, 41, 58-62.
Woollard, M., & Pitt, K. (2003). Antipyretic prehospital therapy for febrile
convulsions: does the treatment fit? A literature review. Health Education Journal, 62(1), 23-28.
Zeisberger, E. (1999). From humoral fever to neuroimmunological control of
fever. Journal of Thermal Biology, 24(5-6), 287-326.
79
3.2 SUMMARY OF LITERATURE REVIEW ARTICLE The article reviewed the literature about parents’ knowledge, attitudes and practices
in and sources of information about fever management. There have been few changes
over the past two decades with some practises, e.g., the use of antipyretics to reduce
fever and alternating antipyretics, increasing in prevalence. Concerns about harmful
outcomes from fever remain high with a shift in concern from brain damage to
febrile convulsions. Knowledge based educational interventions to assist parents
manage fever in an evidence-based manner have been reported as successful.
However, evidence of these changes is not apparent in baseline data from more
recent studies. Early interventions targeted parents’ knowledge to reduce
unnecessary health service utilisation. One study was loosely based on a behaviour
change theory targeting one of the theoretical constructs of the theory, attitudes, in
addition to knowledge.
3.3 NEED FOR A THEORETICAL BASE Parents continued fear of and perceived need to reduce fever highlight deficits in the
reportedly successful knowledge based education programs. Changes have been
neither sustainable over time nor from one generation to the next. The lack of
theoretically based educational interventions could be a contributing factor in parents
continued concern about fever and its perceived harmful effects. Kok (1993),
suggests the reason health educational interventions are ineffective is their lack of
theoretical base, adequate planning and evaluation. Whitehead (2004) has extended
this by including health educators’ poor understanding of the behaviour change
processes and the complexity of behaviour change and emphasises a need for careful
consideration of the theoretical and practical constructs underpinning health
education programs.
80
Parents’ fever management is determined during febrile episodes; it is an individual
behaviour. Therefore, theories focusing on the characteristics of the individual were
explored to determine fit for this research. The dominant individual behavioural
theories in the health education arena include the Health Belief Model (Rosenstock,
1974), Social Cognitive Theory (Bandura, 1977), Transtheoretical Model
(Prochaska, Johnson, & Lee, 1998) and the Theories of Reasoned Action (Fishbein &
Ajzen, 1975) and Planned Behavior (Ajzen, 1985). Newly emerging theories such as
the Information Motivation Behavioral Skills model (Fisher & Fisher, 2002) extend
earlier theories such as the Health Belief Model and Theories of Reasoned Action
and Planned Behavior. These dominant theories account for the majority of theory
based research and interventions in the health education literature.
3.3.1 Determining a Theory To determine an appropriate theoretical framework it is necessary to revisit the
currently identified predictors of parents’ fever management practices. Influences on
parents’ fever management are multifactorial and include knowledge, beliefs,
attitudes, sources of information and past experience with fever (e.g., Knoebel et al,
2002; Kramer et al., 1985; Schmitt, 1980). Additionally, childhood fever is not an
everyday occurrence. Febrile children make parents anxious (Betz & Grunfeld, 2006;
Goldman & Scolnik, 2004). Influences identified during a febrile episode could
differ according to the specific context and height of fever and be confounded by
parental anxiety related to these. It is therefore more appropriate to explore the
determinants of parents’ fever management when children are afebrile. To achieve
this it is necessary to explore behavioural intentions rather than behaviours,
behaviours that could be influenced by a specific febrile episode.
81
Following a review of the fever management and health educational literature the
Theory of Planned Behavior was deemed the most appropriate theoretical basis for
the research as it identifies the determinants of behavioral intention. This theory
provides the constructs appropriate for identifying parents’ beliefs, attitudes, the
normative influences on them and their control over their fever management. An
earlier study conducted in the United States used one construct of the Theory of
Planned Behavior, attitudes, in an intervention to enhance parents’ management of
fever (Broome et al. 2003). This will be the first study to undertake a comprehensive
theoretical exploration of the determinants of parents’ fever management practices.
3.4 THEORY OF PLANNED BEHAVIOR The Theory of Planned Behavior (TPB) (Ajzen, 1985; 1991) is an extension of the
earlier Theory of Reasoned Action (TRA) (Fishbein & Ajzen, 1975). Both are
deliberative processing models and based on the assumption that when making
behavioural decisions, people rationally consider all information available and
implicitly or explicitly consider the implications of their actions. The TRA and TPB
postulate that a person’s intention to perform (or not perform) a behaviour is the
most important immediate determinant of that action (Ajzen, 2005). Within both
theories is the principal of compatibility which purports that each attitude and
behaviour has four elements: action, target, context and time. Attitudes and
behaviour are more likely to correspond when both are measured with the same
degree of specificity with respect to each element (Ajzen, 2005). Therefore fever
management behaviour consists of:
• an action or behaviour (using, or not using, medications to reduce fever)
• performed on or toward a target or object (febrile child, a child is a different
target each time they have a fever)

82
• in a particular context (temperature 38.0ºC or greater)
• at a specified time or occasion (at home, going to child care, on vacation) (Ajzen,
2005).
The TRA was based on a compensatory, expectancy-value model of attitude which
proposed a person’s attitude towards an object was a function of their beliefs about
the object (characteristics, qualities and attributes) and evaluation of those beliefs.
The TRA purports the key predictor of performing behaviours under volitional
control are intentions to perform the behaviour. The underlying determinants of
intention are attitudes and subjective norms and the relative weighting given to each
of these varies according to the behaviour and population being studied (Fishbein &
Ajzen, 1975). The TPB extends the TRA to include situations under which a person
does not have complete volitional control over behaviour, this extension offers
insight into individuals’ situation specific behaviour (Ajzen, 1985, 1991, 2005).
According to the TPB there are three basic determinants to a person’s intention (and
behaviour) one personal in nature (attitudes), one reflecting social influence
(subjective norms) and a third dealing with issues of control (perceived behaviour
control). A person intends to perform a behaviour when they evaluate it positively,
experience social pressure to perform it and believe they have the means and
opportunity to do so. See Figure 3.1.
Attitudes toward a behaviour are determined by salient (accessible) beliefs about the
consequences of the behaviour – behavioural beliefs. Each behavioural belief is
linked to an attribute, such as the outcome or cost of performing the behaviour
(Ajzen, 2005; Conner & Sparks, 2005). For example a parent might believe it
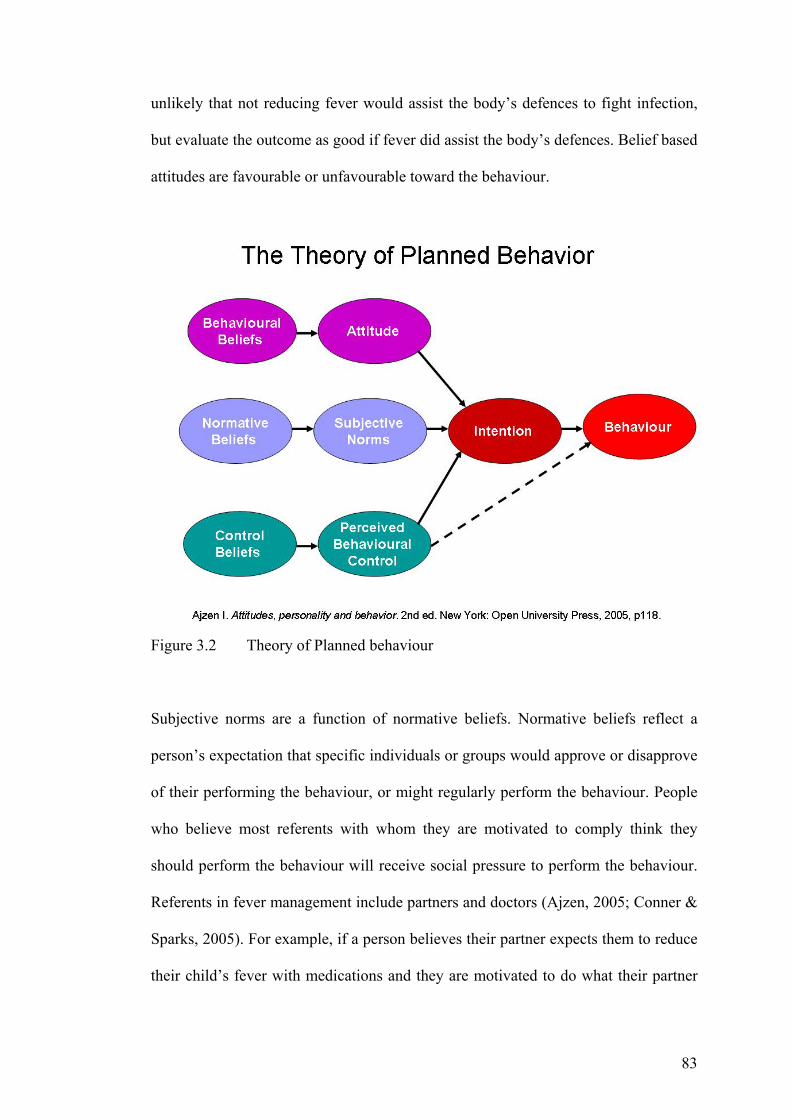
83
unlikely that not reducing fever would assist the body’s defences to fight infection,
but evaluate the outcome as good if fever did assist the body’s defences. Belief based
attitudes are favourable or unfavourable toward the behaviour.
Figure 3.2 Theory of Planned behaviour
Subjective norms are a function of normative beliefs. Normative beliefs reflect a
person’s expectation that specific individuals or groups would approve or disapprove
of their performing the behaviour, or might regularly perform the behaviour. People
who believe most referents with whom they are motivated to comply think they
should perform the behaviour will receive social pressure to perform the behaviour.
Referents in fever management include partners and doctors (Ajzen, 2005; Conner &
Sparks, 2005). For example, if a person believes their partner expects them to reduce
their child’s fever with medications and they are motivated to do what their partner
84
wishes, then they are likely to reduce the fever with medications. Subjective norms
are supportive or unsupportive of the behaviour.
Perceived behavioural control is a function of beliefs about the presence or absence
of factors that facilitate or impede performance of a behaviour. Perceived
behavioural control beliefs may be based on past experience, experiences of others
and factors that reduce or increase their perceived difficulty of performing the
behaviour (Ajzen, 2005; Conner & Sparks, 2005). For example, parents would not
have high perceived behavioural control over administering paracetamol to their
febrile child if the parent believed fever should be managed with paracetamol but
their child regularly refused to take oral paracetamol when febrile.
Background factors can also influence behavioural, normative and control beliefs.
Many variables may be related to or influence the beliefs people hold such as age,
gender, marital status, ethnicity, socio-economic status, education, occupation,
religion, nationality and so on. In childhood fever management age, education and
inexperience in fever management have been identified as influencing knowledge
and concerns about fever (Ames et al. 1982; Crocetti et al. 2001; Impicciatore et al.,
1998; Kramer et al., 1985; Singhi et al., 1991). The potential influence of these
factors is recognised by the TPB, however, without a theoretical guide the specific
background factors influencing beliefs are unknown. Additional background factors
that could influence parents’ fever management include the number of children they
have, the age of their children, whether they have had employment in a health setting
and sources of fever management information.
85
The TPB has been applied to a variety of behavioural domains over the past 20 years
and there is considerable support for the theory. Intentions to perform a behaviour
can be predicted from attitudes, subjective norms and perceptions of behavioural
control and behaviour can generally be predicted with considerable accuracy from
intentions and perceptions of perceived behavioural control (Ajzen, 2005). Meta-
analyses of the TPB literature provide good support for the TPB (e.g., Armitage &
Conner, 2001; Downs & Hausenblas, 2005; Godin & Kok, 1996; Rivis & Sheeran,
2003)
3.4.1 Applications of Theory of Planned Behavior The TPB has predicted intention to perform a variety of everyday behaviours. These
include, for example, pedestrians’ intentions to violate traffic regulations (Diaz,
2002), mobile phone use (Wang, Lin, & Luarn, 2006), young males’ intentions to
drink and drive (Marcil, Bergeron, & Audet, 2001) and blue collar workers’
intentions to exercise (Blue, Wilbur, & Marston-Scott, 2001). Health behaviours
predicted by the TPB include young adolescents’ fruit and vegetable consumption
(Lien, Lytle, & Komro, 2002), eating and activity behaviours (Wood Baker, Little, &
Brownell, 2003), breakfast eating behaviours (Gummeson, Jonsson, & Conner,
1997), fish consumption (Verbeke & Vackier, 2005), exercise intention (Rhodes &
Courneya, 2005; Rhodes, Courneya, & Jones, 2005) and purchasing foods enriched
with omega-3 fatty acids (Patch, Tapsell, & Williams, 2005).
However, few TPB studies have explored predictors of parent child rearing
behaviours. Studies have found parents’ attitudes toward booster seat use predict
booster seat use (Ferraro, 2004), adolescents’ attitudes, social norms and perceived
control influence pregnant adolescents’ intentions to breastfeed (Wambach & Koehn,
2004). Perceived control was found to influence breast feeding among new mothers
86
in Hong Kong (Dodgson, Henly, Duckett, & Tarrant, 2003) and subjective norms
were the best predictors of Peruvian mothers’ intentions to seek medical help for
children with signs of pneumonia (Galvez, 2001). Identifying predictors of parents’
intentions allows for targeted interventions to be developed to improve parents’
practices. The dearth of research in this area exploring both the predictors of parents’
child health behaviours and interventions to improve parents’ child health behaviours
highlights the urgent need for theoretical research in this area.
Recommendations from the research on ‘Planned Behavior’ during the past two
decades (Ajzen & Madden, 1986; Anderson et al., 1998; Edwards, Nash et al., 2001;
Fishbein, 2000; Fishbein et al., 2001; Godin & Kok, 1996; McCaul et al., 1993;
Terry & O'Leary, 1995; White et al., 1994), assert the TPB contains variables
necessary to predict health behaviours and for the development of successful
interventions aimed at increasing intention to perform a particular health behaviour.
The TPB demonstrates that a person’s intention to perform a behaviour is the most
reliable predictor of behaviour. Therefore, research aimed at identifying the
predictors of intention and interventions aimed at changing behaviour must focus on
changing the specific behavioural antecedents influencing intention, namely
perceived control, attitudes and subjective norms in order to promote lasting
behavioural changes.
The TPB has been successfully used as a basis for educational interventions targeting
the predictors of behavioural intention. Positive results have been reported in
changing HIV/AIDS protection (McCamish, Timmins, Terry, & Gallois, 1993;
McCaul et al., 1993; White et al., 1994), use the bus instead of driving the car
(Bamberg, Ajzen, & Schmidt, 2003), wear bicycle safety helmets (Quine, Rutter, &
87
Arnold, 2001), increase regular condom use (Fishbein et al., 2001) and change job-
seeking strategies (Van Ryn & Vinokur, 1992).
The TPB has also been used to identify predictors of intentions and behaviour and as
a guide for developing educational interventions. Successful applications of the TPB
to initially identify the predictors of intentions and then develop educational
interventions to change intentions are reported. For example, surgical nurses’
intentions to administer as required opioid analgesia to post-surgical patients with
pain (Edwards, Nash, Najman et al., 2001; Edwards, Nash et al., 2001) and paediatric
nurses’ intentions to reduce childhood fever with paracetamol (Edwards et al., in
press; Edwards et al., 2003; Walsh et al., 2005).
Prior to developing interventions to promote parents’ rational, consistent fever
management it is imperative that a comprehensive exploration of parents’ current
practices and the influences on those practices is undertaken. As factors influencing
parents’ fever management practices have been identified as multifactorial the TPB
provides an excellent theoretical basis upon which to explore the predictors of their
intentions. When predictors of intentions have been identified targeted educational
interventions can be developed and trialled to determine their effectiveness in
addressing identified needs.
3.5 SUMMARY Through this chapter the fever management and health educational literature were
examined to identify an appropriate theoretical framework to explore the
determinants of parents’ fever management practices. It was deemed appropriate to
examine the determinants of parents’ intentions as their practices could be situation

88
specific. The Theory of Planned Behavior was deemed fitting as this theory purports
behaviour to be predicted by behavioural intention. This theory identifies the salient
(most accessible) beliefs and social influences and also considered perceptions of
control over the behaviour, which could be influenced by a number of factors.
89
CHAPTER 4 – METHODS
4.1 INTRODUCTION This chapter describes the research designs, ethical considerations, samples,
instrument development and data collection methods for the two studies undertaken
for this thesis. Data preparation and methods of analysis are also discussed. The first
study, an elicitation study, was guided by Theory of Planned Behavior (TPB)
recommendations to identify the salient or accessible behavioural, normative and
control beliefs under study (Ajzen, 2006a; Francis et al., 2004). In addition to
gathering information about parents’ behavioural, normative and control beliefs in
fever management, data were also collected about parents’ fever management
knowledge, attitudes, practices and methods of searching for information about how
to manage childhood fever to inform survey item development.
The second study, a crossectional survey, was conducted to explore Queensland
parents’ fever management. The survey had three components. The first explored
parents’ knowledge about fever, fever management practices, beliefs about fever and
methods of learning to manage fever. The second targeted parents’ use of
medications in fever management. Finally parents’ intentions to reduce fever were
explored in the third section through the tenets of the TPB. Demographic information
was also collected. Queensland parents of children aged 6-months to 5-years were
targeted for this research because febrile convulsions have been identified in the
literature as parents’ major concern when children are febrile and febrile convulsions
generally occur in children aged between 6-months and 6-years (see Chapter 2). In
90
these studies the term ‘medications’ was used to represent antipyretics, over-the-
counter medications that reduce fever.
As no Australian research has been conducted in this area two frameworks were used
to ensure comprehensive, complementary data were collected: a health promotion
needs assessment framework (Ewles & Simnett, 2003) and a theoretical framework
based on the Theory of Planned Behavior (Ajzen, 1985, 1991). A needs assessment
framework ensures comprehensive valid data are collected using multiple data
collection methods (Ewles & Simnett, 2003). The theoretical framework facilitated
the identification of specific predictors of parents’ behavioural intentions to reduce
fever and has been described in detail in Chapter 3. Research based on these
frameworks ensured the studies provided a comprehensive examination of parents’
knowledge, attitudes and fever management practices. When parents’ needs are
identified then educational programs can be developed to address these needs. Then
parents will be equipped to care of febrile children at home. Salient behavioural,
normative and perceived control beliefs in fever management were also identified.
4.2 NEEDS ASSESSMENT Ewles and Simnett’s (Ewles & Simnett, 2003) needs assessment framework drawn
from the work of Bradshaw (Bradshaw, 1972) targets four distinct types of needs:
normative, felt, expressed and comparative. Normative needs are the needs of most
parents in the area and are defined by professionals or experts. These were assessed
during the literature reviewed in Chapter 3. Felt needs are defined by the individuals
themselves. These will be determined through the focused interviews, group
discussions and survey. Parents’ felt fever management needs are shaped by their
circumstances, experiences, knowledge and understanding of fever. Expressed needs,
91
those expressed by parents, will initially be identified through the focused interviews
and group discussions and then further explored through the survey. Finally,
comparative needs, comparing differences in needs by age, number of children,
educational attainment and experience in the health industry (education in a health
profession or having worked in a health setting) were explored through the survey
(Ewles & Simnett, 2003).
Based on the literature in Chapter 3 describing parents’ fever management practices
it was determined that a behavioural approach, focusing on the individual with data
collected from the target population, would be appropriate for the needs assessment
(Lawton, 1999). Collecting both qualitative and quantitative data ensures that the
phenomenon discovered by social scientists in relation to self-reported data, public
and private levels of responding, would not influence the findings (Lawton, 1999).
Public level data represents information parents think health professionals might
want to hear. This is often gathered through surveys. Private level data is information
parents would discuss with their family and friends. The inclusion of focused
individual interviews and group discussions ensured private level data were also
collected (Lawton, 1999). Examining both private and public accounts of parents’
beliefs and practices via focused interviews, group discussions and surveys provides
a more accurate and truer account of parents’ knowledge, attitudes, practices,
information gathering activities and fever management intentions. Additionally, an
initial qualitative study allows for exploration of the topic, is recommended by Ajzen
(2006a) to identify salient predictors of intention through the TPB, and ensures the
survey contains relevant, culturally appropriate items modified from previously
developed instruments and developed specifically for Study 2.
92
4.3 STUDY AIMS The aims of Study 1 were to explore Queensland parents’ current knowledge of and
beliefs about fever, fever management practices; salient behavioural, normative and
perceived control beliefs; influences on fever management practices and sources of
fever management information. Findings from this study were used to develop
relevant, culturally appropriate questionnaire items and to modify items from
developed instruments for they survey conducted in Study 2.
Aims of Study 2 were to:
1. Identify Queensland parents’ knowledge of and beliefs about fever, fever
management practices and influences on practices.
2. Identify Queensland parents’ knowledge of appropriate medication dosage
and frequency, medication use in fever management and beliefs of harm from
medications used in fever management.
3. Discover where Queensland parents learnt about childhood fever
management and the impact of this on their practices.
4. Identify the predictors of Queensland parents’ intentions to reduce fever
according to the tenets of the TPB.
5. Develop and trial a comprehensive instrument to explore parents’
management of childhood fever and influences on fever management.
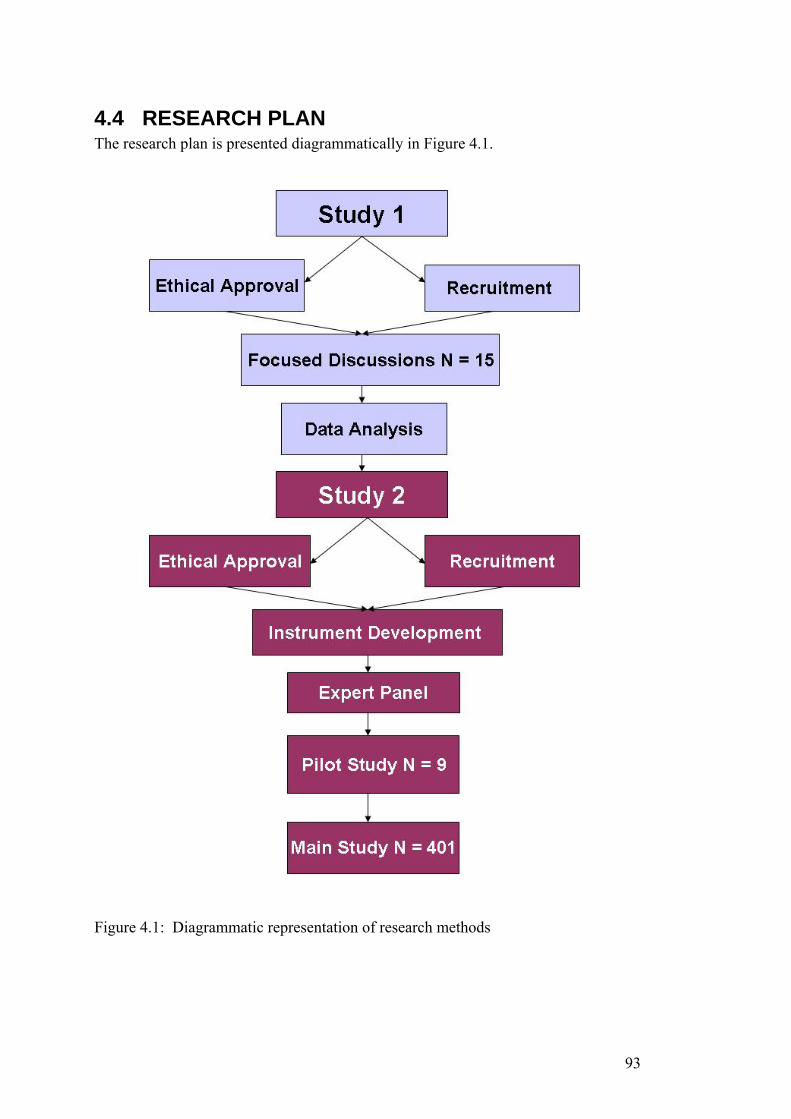
93
4.4 RESEARCH PLAN The research plan is presented diagrammatically in Figure 4.1.
Figure 4.1: Diagrammatic representation of research methods
94
4.4.1 Study 1 – Focused Discussions
4.4.1.1 Study Design Qualitative study using semi-structured focused interviews and group discussions.
4.4.1.2 Rationale The dearth of literature describing Australian parents’ management of childhood
fever and the need to elicit parents’ salient beliefs highlighted the need for an initial
exploratory study. Focused discussions were conducted, with parents of children
aged 6-months to 5-years at a time and place suitable to those indicating an interest
in participating. As all targeted parents had young children discussions therefore
were conducted at a time and in an environment suitable to those interested in
participating. This determined whether interested parents participated in a group
discussion or individual interview. Factors influencing participation in an interview
were a preference to be interviewed when their child was asleep, interviewed at
home so that children could play happily during the interview or at work during
lunch time. Discussions were conducted with natural groups such as a playgroup
meeting, child care centre and workplace. Discussions elicited parents’ salient
behavioural, normative and control beliefs and their knowledge about fever, fever
management practices and how parents learn to manage childhood fever.
4.4.1.3 Semi-Structured Focused Individual Interviews and Group Discussions Semi-structured focused interviews and semi-structured focused group discussions
were conducted using the same topic guide to direct discussions (Millward, 2006).
Both these methods involve participant participation and explanation of the specific
topic and provide insight into sources of complex behaviours and motivations. They
are appropriate to use in areas of limited research (Morgan, 2004) and have become
popular in health research as they produce rich, comprehensive, credible, valid
95
information (Morrison-Beedy, Cote-Arsenault, & Fischeck Feinstein, 2001; Polit &
Beck, 2006). In psychological research these methods are commonly used to develop
or operationalise constructs, as a first step in questionnaire development and to test
the viability of a construct (Millward, 2006). A limitation of these methods is that
self-report data are collected. Self report data reflect what participants say not what
they do (Polit & Beck, 2006).
Focused Individual Interviews Focused interviews have been found to generate more data and better quality of data
per participant than group discussions. Interviews place a greater burden on the
participant to explain themselves to the researcher than group settings (Morgan,
2004). During interviews researchers have an opportunity to probe participant
experiences and beliefs in more depth. Additionally, participants may be more
willing to share their experiences in interviews than in a group setting, particularly
on sensitive topics such as their care of their children (Greenbaum, 2000; Morgan,
2004).
Focused Group Discussions During focused group discussions there is greater breadth of data collection (Morgan,
2004), participants are encouraged to query each other and to explain their thinking
(Morgan, 2004). The use of group processes during discussions encourages
participants to explore and clarify their views, ensuring comprehensive data are
collected (Morrison-Beedy et al., 2001). In this study natural groups of people who
knew each other were used. Natural groups are useful when the researcher wants to
understand how participants’ social knowledge about a subject, in this study
childhood fever management, was generated (Green & Thorogood, 2004).
96
Two Data Collection Methods: Advantages and Disadvantages An advantage of using two methods to collect qualitative data is the quality
(interviews) and breadth (groups) of data generated (Morgan, 2004). Data collected
by interviews and groups were similar and data collection continued in both methods
until data saturation was achieved (Green & Thorogood, 2004). To confirm
saturation an additional group discussion was conducted. A disadvantage of using
two methods could be reflected in the data quality and breadth, although saturation
was achieved. However, group discussions offset some of the disadvantages of
individual interviews as the interviewer had access to interaction between
participants as well as between the interviewer and participant (Green & Thorogood,
2004).
4.4.1.4 Research Questions Research questions addressed by the focused interviews and group discussions were:
1. What do Queensland parents know about fever in young children?
2. What are Queensland parents’ beliefs about fever in young children?
3. How do Queensland parents manage fever in young children?
4. How do Queensland parents learn how to manage fever in young children?
Through the research questions behavioural, normative and perceived control beliefs
were identified.
4.4.1.5 Sample A convenient sample of Queensland parents of children aged between 6-months and
5-years was targeted to generate appropriate data (Green & Thorogood, 2004).
Parents of children enrolled at metropolitan child care centres and parents registered
with Playgroup Queensland were targeted. Eligibility criteria included being over 18
years of age, able to read and converse in English and being a parent/primary
caregiver for a child aged between 6-months and 5-years.
97
4.4.1.6 Settings and Procedures Parents were recruited from two metropolitan child care centres and Playgroup
Queensland. At child care centres a letter of invitation to participate and an
information sheet about the study were given to parents of all children enrolled in the
child care centres. A copy of the Information sheet is available in Appendix 1.
Metropolitan members of Playgroup Queensland were recruited through an invitation
to participate in the Playgroup Queensland monthly online newsletter. A copy of the
invitation is in Appendix 1. Interested parents from child care centres and Playgroup
Queensland contacted the researcher by telephone or email. Parents’ contact details
and availability for group or individual discussion was discussed and arranged. Six
individual interviews and three group discussions were conducted. Both group and
individual discussions were conducted with parents recruited from child care centres
and Playgroup Queensland.
All discussions were audio taped and simultaneously recorded by a data recorder,
experienced in court data recording. A word document of the discussion was sent to
the researcher within two weeks following each discussion. Transcripts were sent to
participating parents through the child care centre director or posted directly to
parents for data checking to ensure transcript accurately reflected parents’
recollection of the discussion. All participants read the transcripts and reported they
represented their recollection of the discussion, beliefs and practices. No additional
information was contributed through this process.
4.4.1.7 Question Guide Semi-structured questions for the individual interviews and group discussions were
guided by an extensive review of the literature, the researcher’s past experience
educating paediatric nurses about evidence-based fever management (Edwards,
98
Courtney et al., 2001b, 2003; Edwards, Walsh, et al., 2007, in press; Walsh &
Edwards, 2006; Walsh et a., 2005, 2006) and the constructs of the Theory of Planned
Behavior (Ajzen, 1985, 1991) (TPB). Four main areas were targeted through the
interviews and discussions: parents’ beliefs and concerns about fever, knowledge of
fever management, fever management practices and sources of information about
fever management. Figure 4.2 portrays the semi-structured questions and prompt
questions used for both interviews and group discussions.
4.4.1.6 Ethical Considerations Ethical approval was granted by the Queensland University of Technology Human
Research Ethics Committee prior to the commencement of participant recruitment
for this study. Parents were not pressured to participate as the researcher was an
outsider to the child care centres or Playgroup Queensland and was not in a position
for parents’ non-participation to impact children’s care. When participants contacted
the researcher to indicate interest they were informed about the study, that the
discussion would be audio taped and a data recorder would be attending the
discussion with the researcher. Prior to participating in a discussion, participant
confidentiality and anonymity were assured and written consent obtained. A copy of
the consent form is available in Appendix 1. Transcripts were returned to participants
for data checking to ensure the data accurately reported participants’ perception of
the discussion.
4.4.1.7 Data Analysis Wilkinson (2003) suggests there is no single or preferred method for analysing focus
group data and that data analysis is dependent on the data of interest, the content or
process. In this study the content was of interest. Content analysis, supplemented
with systematic quotations from the interviews to illustrate conclusions, was
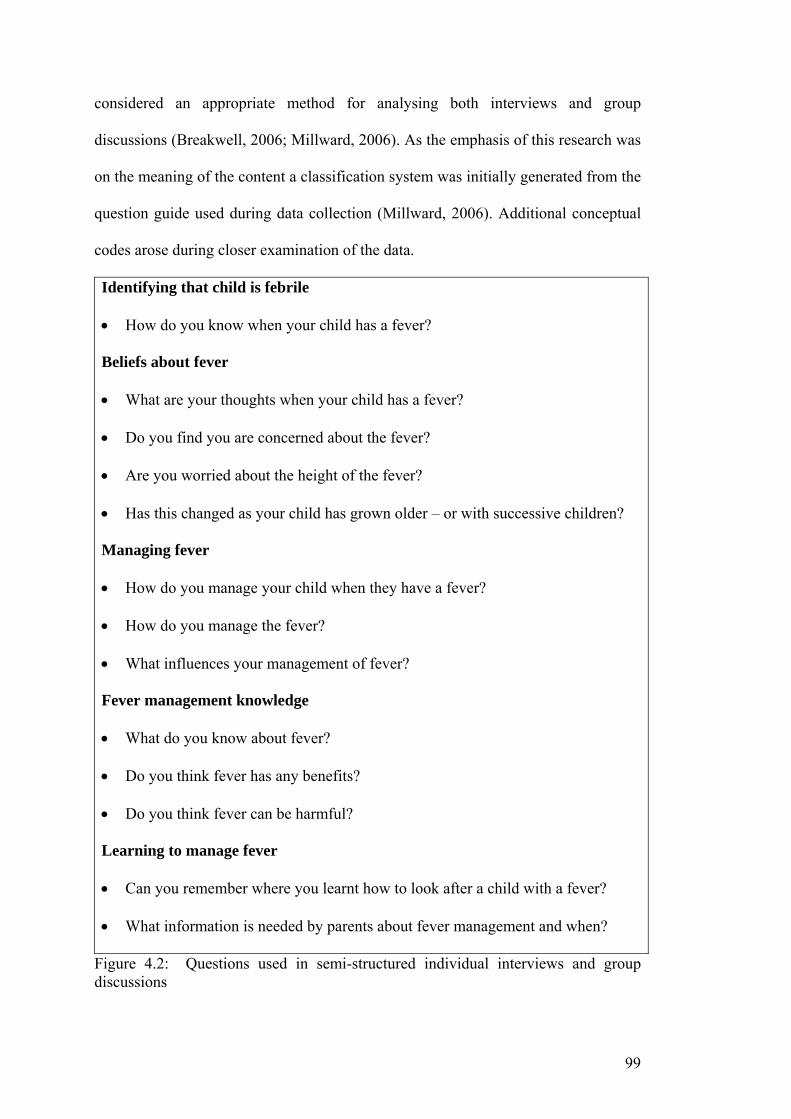
99
considered an appropriate method for analysing both interviews and group
discussions (Breakwell, 2006; Millward, 2006). As the emphasis of this research was
on the meaning of the content a classification system was initially generated from the
question guide used during data collection (Millward, 2006). Additional conceptual
codes arose during closer examination of the data.
Identifying that child is febrile
• How do you know when your child has a fever?
Beliefs about fever
• What are your thoughts when your child has a fever?
• Do you find you are concerned about the fever?
• Are you worried about the height of the fever?
• Has this changed as your child has grown older – or with successive children?
Managing fever
• How do you manage your child when they have a fever?
• How do you manage the fever?
• What influences your management of fever?
Fever management knowledge
• What do you know about fever?
• Do you think fever has any benefits?
• Do you think fever can be harmful?
Learning to manage fever
• Can you remember where you learnt how to look after a child with a fever?
• What information is needed by parents about fever management and when?
Figure 4.2: Questions used in semi-structured individual interviews and group discussions
100
To ensure trustworthiness of the findings Burnard’s (1991) 14 stage content analysis
method was used. Using Burnard’s method transcripts were initially read and re-read
and the researcher became immersed in the data. Emergent headings or categories
were identified and linked to develop a category system. Following this the
researcher and an experienced qualitative researcher independently identified themes,
categories and sub-categories for two transcripts. These were checked and found
consistent. The remaining transcripts were then analysed by the researcher according
to identified themes and categories. Similar themes were collated into a WORD
document under the appropriate headings. It was not possible to involve participants
in checking the category system. They were however, involved in transcript
checking. In the final stages the findings are written up and examples linked together
and to the literature. See Chapter 5.
To ensure data trustworthiness and that comprehensive valid data were collected
multiple interviews and discussions were conducted until data saturation was
achieved and confirmed (Green & Thorogood, 2004; Morgan, 2004). A detailed
interview guide was used for all discussions, verbatim transcripts crosschecked with
the audiotape and transcripts returned to participants to determine data accuracy.
Data trustworthiness was assessed through credibility, dependability, confirmability
and transferability (Polit & Beck, 2006).
1. Data credibility was determined through triangulation and researcher
credibility. Triangulation was achieved by collecting data from multiple
participants and having two researchers independently develop categories and
themes from two transcripts and compare findings (Ploit & Beck, 2006).
Researcher credibility was assured as the researcher collecting and analysing
101
the data was experienced in conducting and analysing focused interviews and
group discussions.
2. Dependability was determined through an inquiry audit with two researchers
scrutinising two transcripts as discussed under data credibility.
3. Confirmability was achieved through the development of an audit and
decision trail and inter-rater reliability by the independent coding of two
transcripts by two researchers (Polit & Beck, 2006).
4. Transferability was confirmed through data saturation (achieved after two
group and six interview discussions; a final group discussion confirmed
saturation) in both interviews and group discussions and the thorough
description of the research setting (Morgan, 2004; Polit & Beck, 2006).
4.4.2 Study 2 – Survey
4.4.2.1 Rationale The focused interviews and group discussions identified knowledge of and beliefs
about fever similar to parents internationally (see Chapter 5). However, some
practices and factors influencing practices, behavioural, normative and perceived
control beliefs had not been previously reported (see Chapter 5 and Chapter 7). To
identify the prevalence, distribution and interrelatedness of the interview and group
discussion findings a community based crossectional survey of Queensland parents
of well children was conducted.
Surveys are an appropriate method for gathering population data and are commonly
conducted when descriptive information about populations is unknown. Descriptive
information about a population’s specific knowledge, beliefs, opinions, attitudes,
practices and intentions of performing the specific practice as well as disease status
102
and demographics is gathered through surveys (Minicheillo, Sullivan, Greenwood, &
Axford, 2004). Survey data provide a broader understanding of prevalence of a
health issues or factors influencing health behaviour (Minicheillo et al., 2004; Polit
& Beck, 2006). Surveys also assist in identifying the need for further research or
health education about specific health practices (Webster & Osborne, 2005).
Community based crossectional surveys are a quick and economical method of
collecting data from people not seeking health care (Minicheillo et al., 2004).
Through this crossectional survey a description of the knowledge, beliefs, practices
and influences on practices of Queensland parents of well children was gained.
Surveys are traditionally used in research based on the Theory of Planned Behavior
(Ajzen, 2006a) to identify attitudes, subjective norms perceived control and
behavioural intentions.
4.4.2.2 Research Design A postal, self administered, self report, crossectional survey was conducted.
4.4.2.3 Research Questions Research questions addressed by the survey were:
1. What do Queensland parents know about childhood fever?
2. What do Queensland parents believe about childhood fever?
3. How do Queensland parents manage fever in young children?
4. How do Queensland parents use medications in fever management?
5. What influences Queensland parents’ medication use in fever management?
6. How do Queensland parents learn how to manage fever in young children?
7. What predicts Queensland parents’ intentions to reduce childhood fever?
103
8. What predicts Queensland parents’ intentions to reduce childhood fever with
medications?
4.4.2.4 Ethical Considerations Ethical approval was granted from the Queensland University of Technology Human
Research Ethics Committee to conduct the pilot and main survey. Parents self-
selected to participate and were free to withdraw at any time. The researcher had no
associated with the recruitment centres. Therefore parents’ participation or non-
participation in the research had no impact on the parents or the care of their
children. Participants were informed about the study through the recruitment
processes and an information sheet attached to the questionnaire. A copy of the
information sheet used in the pilot study is available in Appendix 2 and the main
study in Appendix 2. The information sheet explained that the participant’s
confidentiality and anonymity was assured and return of a completed questionnaire
would indicate consent to participate in the study. Prior to recruiting for the survey
the researcher obtained a Blue Card from the Employment Screening Services Unit
Commission for Children and Young People.
4.4.2.5 Instrument Development Initially an extensive search of the literature using CINAHL, Medline and
PsycArticles and PubMed databases was conducted. Only articles published, in
English, between the years 1980 and 2004 were examined. Databases were searched
for terms such as fever, child, seizure, convulsion, paracetamol, acetaminophen,
ibuprofen, parent, beliefs, temperature and health information and combinations of
these. A number of published articles had survey items included in the article (e.g.,
Abdullah, et al., 1987; Al-Eissa, Al-Sanie et al., 2000; Al-Eissa, Al-Zamil et al.,
2000; Birchley & Conroy, 2002; Blumenthal, 1998; Kapasi et al., 1980; Karwowska,
104
et al., 2002; Li, et al., 2000; Sarrell, et al., 2002; Schmitt, 1980). Authors of other
developed instruments were contacted and instruments were obtained from Crocetti
(2001) and Kelly (1996). Items from developed instruments were adapted and other
items were developed from the information gained through Study 1 (Walsh,
Edwards, & Fraser, 2007a), to suit an Australian audience. Ajzen’s website was
explored for information about the development of items to address the tenets of the
Theory of Planned Behavior (TPB). Additional items were developed to target the
constructs of the TPB, namely parents’ beliefs about and attitudes toward fever, the
normative influences on and their perceptions of control over fever management and
fever management intentions. No developed scales targeting parents’ fever
management practices or beliefs were found during the literature search.
A pilot instrument was developed and had three sections. In the first section 14 items
explored parents’ fever management practices, four explored knowledge of fever,
five explored beliefs about fever, 12 recorded medication uses and four gathered
information about where parents learnt to manage fever. In the focused individual
interviews and group discussions parents used the terminology fever, high fever and
very high fever to describe mild, moderate and high fever. Therefore this
terminology was used in the instrument. This instrument is attached in Appendix 2.
In the second section 55 items targeted the tenets of the TPB and Section 3 recorded
demographic information on 21 items. Prior to piloting, the instrument was examined
for content and face validity and response bias by an expert panel consisting of two
clinical paediatric nurses, a paediatric nurse researcher, two nurse academics and a
nurse academic who was also a psychologist and familiar with the TPB (Polit &
105
Beck, 2006). The panel confirmed the instrument was valid and items were placed in
a manner that would not cause response bias.
Pilot Test A test-retest study was conducted to determine the reliability of items in the survey
instrument (Polit & Beck, 2006).
Sample A convenient sample of parents was recruited. To be eligible for inclusion in the pilot
study parents were 18 years and older, able to read and write in English and had a
child aged between 6 months and 5 years of age.
Settings and Procedures Parents who participated in Study 1 indicated an interest in participating in the pilot
study. These parents were contacted by phone and if still interested in participating
were informed about the pilot study and their potential involvement. Additionally
paediatric nurses and nurse academics known to the researcher who met the
eligibility criteria were approached to determine interest in participating. Interested
parents were posted a survey package containing a letter describing the pilot study
and their potential involvement, a plain language statement about the research, a
questionnaire, a survey evaluation form and a reply paid envelope. These documents
are available in Appendix 2. The evaluation form was included to determine the
instrument’s readability, ease of completion and clarity of questions. Two weeks
following return of the first questionnaire a second identical questionnaire and reply
paid envelope were sent to participating parents. When questionnaires were not
returned within two weeks the researcher contacted the participant to enquire about
their interest in continued participation.
106
Data Analysis Initially qualitative data were coded. All data were then entered into SPSS version 13
(SPSS, 2004) searched for outliers and irregularities and 25% of data rechecked for
data entry errors. No errors were detected. Item reliability on categorical items was
determined by Cohen’s Kappa and on continuous items by Bland Altman analysis.
Cohen’s Kappa is an appropriate measure of reliability or stability for nominal data,
the closer a score is to 1.0 the greater the item reliability and stability (Minicheillo et
al., 2004). Cohen’s Kappa takes into account the problem of chance responding, a
person responding in a particular manner by chance. Bland Altman analysis
compares two continuous measures (temperature in this study) by plotting the
differences between the two measures against the averages of the two measures
(Bland & Altman, 1986). Measures falling within limits of agreement (mean
difference ± 2SD) are considered reliable.
Results Nine parents participated in the test-retest study and included two clinical paediatric
nurses, a nurse academic and six parents from the semi-structured discussion study
(Walsh et al., 2007a). All participants were female. Their mean age was 34.4 years
(SD 11.1), most were in a partnered relationship (88.9%), had two children (66.7%),
an undergraduate or postgraduate degree (22.2% and 55.6% respectively), experience
in a health industry (66.7%, this includes education in a health profession or worked
in a health setting), were employed part-time (55.6%) and born in Australia (77.8%).
Feedback from participants indicated the instructions preceding each section were
clear, sufficient response space had been allocated to open-ended items and all but
one item was easily understood. In the final instrument the confusing item “How
harmful do you believe fever is” was preceded by a lead item “Can fever ever be
107
harmful”. Additionally, an item was included to explore decision making in seeking
medical assistance and another reporting examples of the conflicting information
they had received, if they reported receiving conflicting information.
Test-retest (2-weeks) reliability of categorical data, determined by Kappa analysis,
ranged from 0.55 (on one item) to 1.00. Bland Altman analysis on continuous items
indicated responses for temperature representative of normal temperature, high, very
high and harmful fever temperatures when antipyretics were administered and items
targeting fever management practices were within the limits of agreement (mean
difference ± 2SD). One respondent’s responses on temperature for fever were outside
the limits of agreement (Bland & Altman, 1986). The questionnaire was deemed
suitable for use in the main study.
Final Instrument Following some minor adjustments to the pilot instrument the final instrument
consisted of 103 items in three sections. Section 1 included items targeting parents’:
o knowledge of temperature perceived to represent normal, fever, high and very
high fever (four items),
o beliefs about fever (six items) and beliefs about fever management
knowledge (one item),
o general fever management practices and practice changes over time (18
items),
o sources of fever management information (five items)
o medication administration (eight items),
o influences on medication administration (seven items) and
o beliefs about medication safety (two items).
108
Section 2 targeted parents’:
o beliefs about fever being harmful (20 items) and outcome expectations of
those beliefs (20 items),
o normative beliefs about fever (eight items) and motivation to comply with
referents (four items),
o perceived behavioural control in fever management decision making (four
items), perceived behavioural control influenced by child medication
behaviour (whether febrile children were compliant or non-compliant with
medication administration) (four items) and
o intentions to reduce their child’s next fever (three items) and intentions to
reduce their child’s next fever with medications (three items).
In Section 3 22 items recorded demographic information about the participant, their
children, partner and sources of assistance in deciding on fever management. Table
4.1 presents an example of how constructs in Section 1 were developed to items. The
full instrument is available in Appendix 2.
As this was an exploratory study many items in Section 1 collected qualitative or
categorical data. Eight items exploring fever management practices were specifically
developed to create a parents’ fever management practice scale. Responses to these
items were recoded on Likert scales. This scale addressed a gap in the literature as no
developed scales had been found during the literature review to explore parents’
fever management knowledge, beliefs or practices.
109
4.4.2.6 Survey Design A postal, self administered, self report crossectional study was conducted with
Queensland parents of children aged between 6-monhts and 5-years.
Sample A convenient sample of Queensland parents were targeted to participate in the
survey. Recruitment was conducted over a three-month period during February,
March and April 2005 and continued until the target of at least 384 participants had
been recruited. Parents were recruited through child care centres, kindergartens and
preschools, Playgroup Queensland online newsletter and quarterly magazine, Family
Day Care – Queensland and the monthly parenting magazines ‘Brisbane’s Child’ and
‘Mother and Child’ available freely to parents in the metropolitan and outer
metropolitan areas. To be eligible for inclusion in the study parents had to be 18
years and older, able to read and write in English and had a child aged between 6
months and 5 years of age.
Sample Size The sample size for the present survey was calculated by estimating the population
proportion with specified absolute precision (Lwanga & Lemeshow, 1991 p1,2,25).
Two key items used by Sarrell et al. (2002) in their sample size calculations a) the
temperature at which parents considered a child had a fever and b) the temperature at
which parents administered antipyretics were considered. A study conducted in Saudi
Arabia reported 46% of 560 parents believed fever to be a temperature between
37.0°C and 38.0°C (Al-Eissa, Al-Sanie et al. 2000). In a similar United Kingdom
study, Blumenthal (1998) reported 49% of 392 parents believed a temperature of
38.0°C to indicate fever. Eighty eight percent of the 392 parents studied by
110
Blumenthal (1998) administered antipyretics for temperatures of 38.0°C or lower, as
did 78% of 650 parents in an Israeli study by Linder et al. (1999).
The following sample estimates were calculated using Lwanga and Lemeshow’s
estimating the population proportion with specified absolute precision (1991,
p1,2,25). If the true percentage of parents who consider temperatures of 38°C or less
to be fever is 50% with a relative precision of 45% at the 95% level of significance
and power of 90% a minimum number of 384 parents are needed. For a true
percentage of parents who administer antipyretics to children with temperatures of
38.0°C or lower of 90% with a relative precision of 85% at the 95% level of
significance and power of 90%, 138 parents are required to participate in the survey.
Therefore, a sample of 384 parents was the target sample size for the study.
Advertising Advertising was conducted through child care centres, kindergartens and preschools,
Playgroup Queensland, Family Day Care service and parenting magazines.
1) Contact was made with directors of privately owned child care centres and
kindergartens in the metropolitan and outer metropolitan area. Seven child care
centres or kindergartens and preschools agreed to advertise the study. Posters were
placed strategically around these centres and a letter describing the survey’s
rationale, parents’ potential involvement and researcher contacts was distributed to
all parents with children enrolled at the centre. One child care centre advertised the
survey in their weekly email newsletter and distributed the survey to all parents as an
attachment to a weekly newsletter. Interestingly this method had the lowest response
rate.
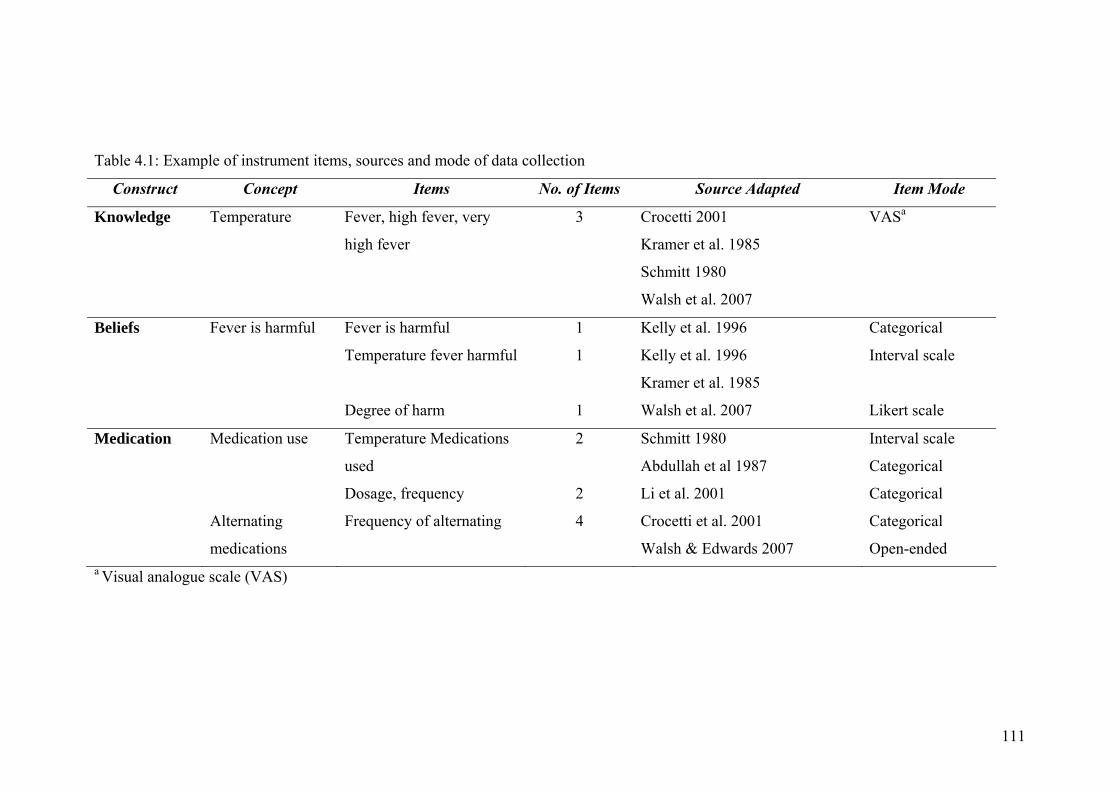
111
Table 4.1: Example of instrument items, sources and mode of data collection
Construct Concept Items No. of Items Source Adapted Item Mode
Knowledge Temperature Fever, high fever, very
high fever
3 Crocetti 2001
Kramer et al. 1985
Schmitt 1980
Walsh et al. 2007
VASa
Beliefs Fever is harmful Fever is harmful 1 Kelly et al. 1996 Categorical
Temperature fever harmful 1 Kelly et al. 1996
Kramer et al. 1985
Interval scale
Degree of harm 1 Walsh et al. 2007 Likert scale
Medication Medication use Temperature Medications
used
2 Schmitt 1980
Abdullah et al 1987
Interval scale
Categorical
Dosage, frequency 2 Li et al. 2001 Categorical
Alternating
medications
Frequency of alternating 4 Crocetti et al. 2001
Walsh & Edwards 2007
Categorical
Open-ended a Visual analogue scale (VAS)
112
2) Parents registered with Playgroup Queensland were informed of the survey
via the Playgroup Queensland online monthly newsletter during February, March and
April 2005 and the first quarterly magazine for 2005, distributed during February.
3) Advertisements were placed in ‘Brisbane’s Child’ during February, March
and April 2005 and ‘Woman and Child’ during March and April 2005 to alert parents
in the metropolitan and outer metropolitan area of the research.
4) Parents registered with Family Day Care Queensland were recruited through
the 80 Family Day Care centres throughout Queensland. Posters and informational
letters were sent to the centres who forwarded them to individual registered carers.
Carers then alerted parents to the study.
Interested parents, responding to advertising, contacted the researcher by phone
(49.6%) or email (50.4%). When contact was made the researcher, using a prepared
script, recorded contact details including telephone, email (if applicable) and postal
address. A survey package including a letter of introduction from the researcher,
plain language statement, survey and reply paid envelope were posted to each
interested parent. Examples of these are available in Appendix 2. Reminders letters
or emails were sent one month following the survey when a completed questionnaire
had not been returned (see Appendix 2).
Face-to-face Four child care centres or kindergartens and preschools agreed to participate in face-
to-face recruitment for the survey. Following negotiation with the director
recruitment dates were arranged, posters advertising the survey and recruitment days
were placed strategically in the centres. Additionally, a letter describing the survey
rationale, potential involvement and recruitment days was sent to the parents of each
113
child enrolled in the centre. The researcher approached eligible parents at the agreed
times, introduced herself and the research and asked parents if they are interested in
participating. Interested parents were given a package containing a plain language
statement about the research; a questionnaire and an envelope (see Appendix 2).
Parents were asked to complete the questionnaire within a week and return it to a
sealed box in the director’s office. The researcher collected completed surveys for a
three week period following recruitment.
Snowball Methods Snowball recruitment was through researcher and participant contacts who recruited
parents within their social networks to the study. Survey packages were posted to and
distributed by the contacts and completed surveys returned to the researcher by mail.
Overall 401 parents were recruited through 1) advertising in parenting magazines
(92.4% returned); 2) face-to-face in childcare centres, kindergartens (60.0%
returned); and 3) snowball technique (57.3% returned). The overall response rate was
69%. See Table 4.2 for survey distribution and response rates.
Data Analysis – Sections 1 and 3 Prior to data entry responses to open-ended items were coded. Data were entered
twice into SPSS Version 13 (SPSS, 2004) and crosschecked for entry errors using
SPSS Data Entry Builder 4.0 software (SPSS, 1996-2003). Identified inconsistencies
were checked with raw data and corrected. Demographics were examined for
frequency and distribution. Categorical data were explored for frequency; the interval
scale for distribution, normality and outliers. Temperatures, recorded on six scales,
were checked for distribution normality and outliers. One extreme outlier, a report of
the temperature at which fever could be harmful (100ºC), was removed.
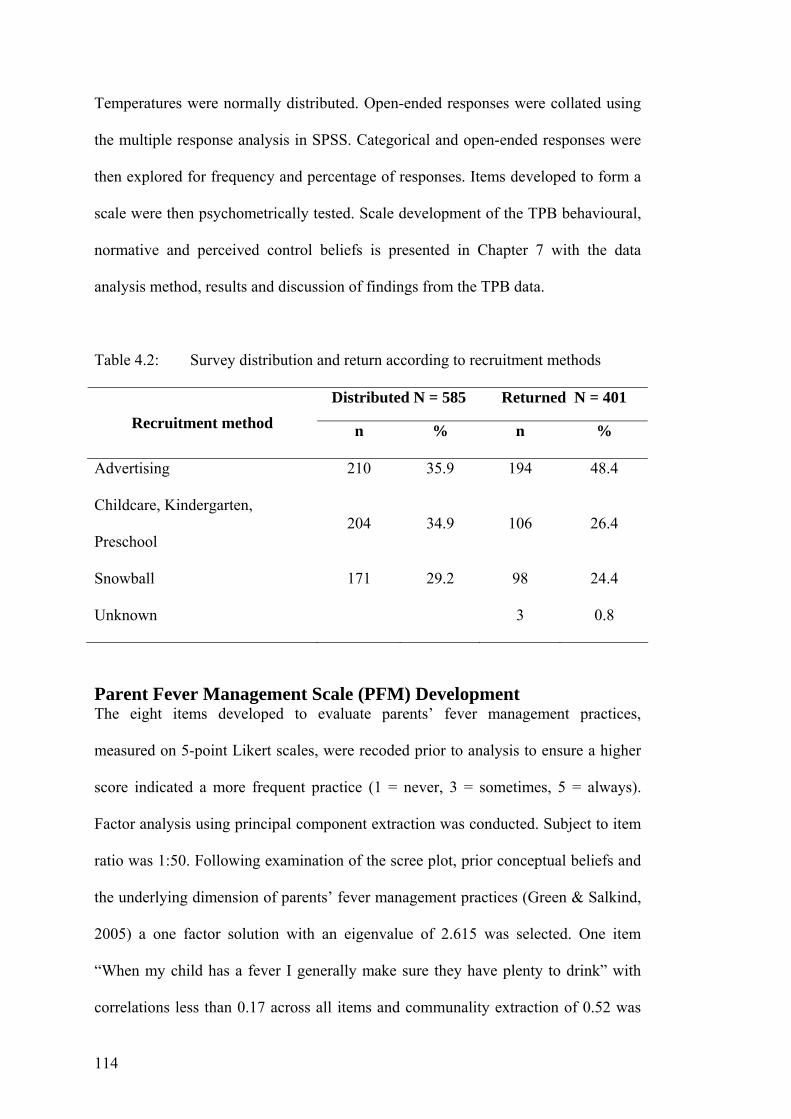
114
Temperatures were normally distributed. Open-ended responses were collated using
the multiple response analysis in SPSS. Categorical and open-ended responses were
then explored for frequency and percentage of responses. Items developed to form a
scale were then psychometrically tested. Scale development of the TPB behavioural,
normative and perceived control beliefs is presented in Chapter 7 with the data
analysis method, results and discussion of findings from the TPB data.
Table 4.2: Survey distribution and return according to recruitment methods
Distributed N = 585 Returned N = 401 Recruitment method n % n %
Advertising 210 35.9 194 48.4
Childcare, Kindergarten,
Preschool 204 34.9 106 26.4
Snowball 171 29.2 98 24.4
Unknown 3 0.8
Parent Fever Management Scale (PFM) Development The eight items developed to evaluate parents’ fever management practices,
measured on 5-point Likert scales, were recoded prior to analysis to ensure a higher
score indicated a more frequent practice (1 = never, 3 = sometimes, 5 = always).
Factor analysis using principal component extraction was conducted. Subject to item
ratio was 1:50. Following examination of the scree plot, prior conceptual beliefs and
the underlying dimension of parents’ fever management practices (Green & Salkind,
2005) a one factor solution with an eigenvalue of 2.615 was selected. One item
“When my child has a fever I generally make sure they have plenty to drink” with
correlations less than 0.17 across all items and communality extraction of 0.52 was
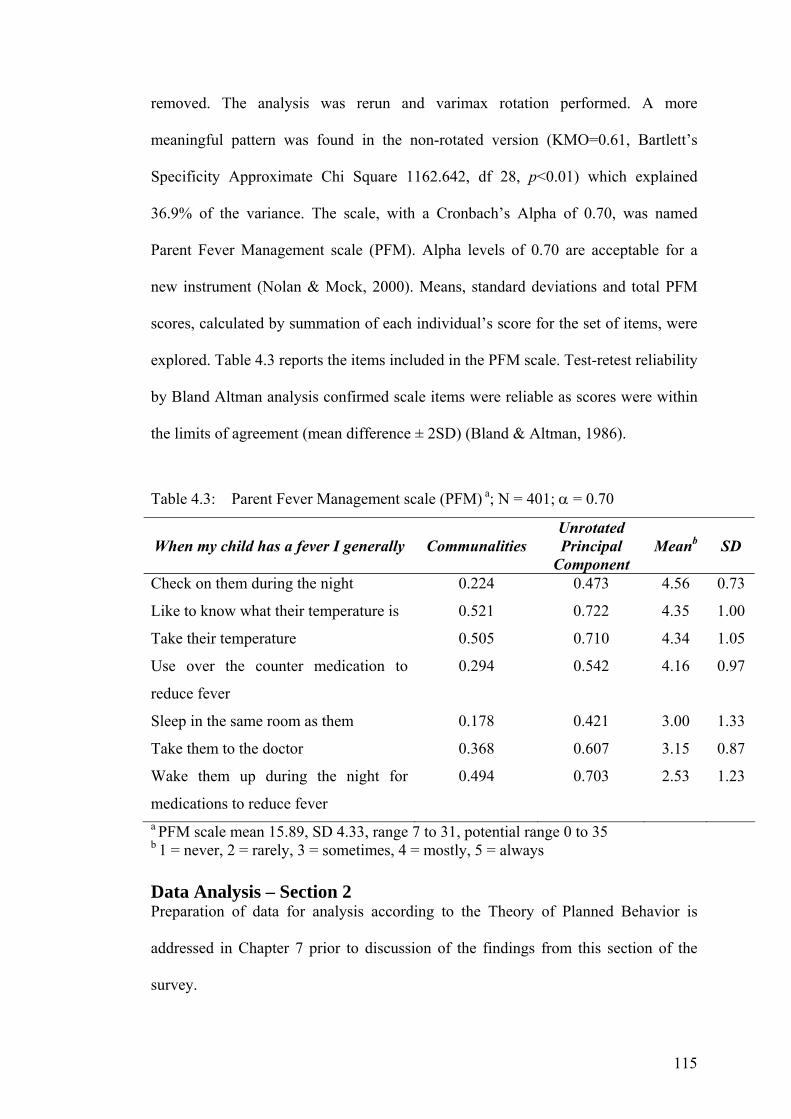
115
removed. The analysis was rerun and varimax rotation performed. A more
meaningful pattern was found in the non-rotated version (KMO=0.61, Bartlett’s
Specificity Approximate Chi Square 1162.642, df 28, p<0.01) which explained
36.9% of the variance. The scale, with a Cronbach’s Alpha of 0.70, was named
Parent Fever Management scale (PFM). Alpha levels of 0.70 are acceptable for a
new instrument (Nolan & Mock, 2000). Means, standard deviations and total PFM
scores, calculated by summation of each individual’s score for the set of items, were
explored. Table 4.3 reports the items included in the PFM scale. Test-retest reliability
by Bland Altman analysis confirmed scale items were reliable as scores were within
the limits of agreement (mean difference ± 2SD) (Bland & Altman, 1986).
Table 4.3: Parent Fever Management scale (PFM) a; N = 401; α = 0.70
When my child has a fever I generally Communalities Unrotated Principal
Component Meanb SD
Check on them during the night 0.224 0.473 4.56 0.73
Like to know what their temperature is 0.521 0.722 4.35 1.00
Take their temperature 0.505 0.710 4.34 1.05
Use over the counter medication to
reduce fever
0.294 0.542 4.16 0.97
Sleep in the same room as them 0.178 0.421 3.00 1.33
Take them to the doctor 0.368 0.607 3.15 0.87
Wake them up during the night for
medications to reduce fever
0.494 0.703 2.53 1.23
a PFM scale mean 15.89, SD 4.33, range 7 to 31, potential range 0 to 35 b 1 = never, 2 = rarely, 3 = sometimes, 4 = mostly, 5 = always Data Analysis – Section 2 Preparation of data for analysis according to the Theory of Planned Behavior is
addressed in Chapter 7 prior to discussion of the findings from this section of the
survey.

116
4.5 SUMMARY This chapter has described the research plan, aims and research questions each study
addresses. Rationales for undertaking the two studies and study designs are discussed
along with the samples, settings and procedures and the development of questions
and instruments used to conduct the studies. Ethical considerations necessary before
conducting the studies and methods of analysing the data analyses were also
described. The next chapter contains an article describing the semi-structured
individual interviews and group discussions.
117
CHAPTER 5 – STUDY 1
FOCUSED DISCUSSIONS
This chapter reports the findings from the qualitative study, undertaken in Study 1, to
determine Queensland parents’ current knowledge of and beliefs about fever, fever
management practices and methods of learning how to manage fever.
Influences on Parents' Fever Management: Beliefs, Experiences and Information Sources Walsh, A., Edwards, H. & Fraser, J. (2007). Influences on parents' fever
management: beliefs, experiences and information sources. Journal of Clinical
Nursing, doi: 10.1111/j.1365-2702.2006.01890.x. Journal Impact Factor: 1.430
Journal of Clinical Nursing 16(12): 2331-2340 (c)2007 Blackwell Publishing
Abstract Aims. Identify parents’ knowledge, beliefs, management and sources of information
about fever management.
Background. Despite numerous studies exploring parents’ management of
childhood fever, negative beliefs about fever and overuse of antipyretics and health
services for mild fevers and self-limiting viral illnesses continue to be reported.
Design. Qualitative design using semi-structured interviews and discussions.
Method. Fifteen metropolitan parents of children aged 6-months to 5-years self-
selected to participate in individual interviews or group discussions. Recruitment was
through Playgroup Queensland’s online newsletter and letters to all parents from two
childcare centres. Verbatim and audio data were collected by an experienced
moderator using a semi-structured interview guide.
118
Data analysis: two transcripts were independently analysed by two researchers,
categories, sub-headings and codes were independently developed, crosschecked and
found comparable. Remaining transcripts were analysed using developed categories
and codes.
Findings. Fever, determined through behavioural changes, was perceived as ‘good’,
a warning something was wrong. High fever, reported as 38.0ºC to 39.1ºC, was
considered harmful; it must be prevented or reduced irrespective of concerns about
antipyretics. Positive febrile experiences reduced concern about fever. Negative
experiences such as febrile convulsions, media reports of harm, not receiving a
definitive diagnosis, inaccessibility to regular doctors and receiving conflicting
information about fever management increased concerns. Parents seek information
about fever from multiple sources such as doctors, books and other parents.
Conclusions. Parents’ experiences with and information sources about fever and
fever management influenced their knowledge, beliefs and practices. Positive
experiences reduce concerns, health service usage and sometimes antipyretic usage.
Negative experiences increase concerns, monitoring and antipyretic and health
service usage.
Relevance to clinical practice. Health professionals need to update their fever
management knowledge ensuring it is based on the latest scientific knowledge. They
must provide parents of young children with consistent, reliable information
preferably before their first child’s first febrile episode.
5.1 INTRODUCTION In 1980 Barton Schmitt (1980) coined the term ‘fever phobia’ to describe parents’
unrealistic concerns about childhood fever. Despite nearly three decades of education
and research parents’ concerns about and fever management practices remain

119
virtually unchanged (Crocetti et al. 2001). Most studies focus on parents of febrile or
injured children; their knowledge, beliefs, practices and demographic predictors of
these (e.g. Ames et al. 1982, Impicciatore et al. 1998, McErlean et al, 2001). Reports
of factors influencing knowledge, beliefs and practices are scarce as is research on
parents of well children. For health professionals, particularly those working in well-
child clinics, this study provides a comprehensive assessment of fever management
practices useful for assisting parents make health related decisions for their children.
5.1.1 Literature review Numerous quantitative studies have described the knowledge, beliefs and practices
of parents with febrile or injured children seeking medical assistance from accident
and emergency departments, hospitals or community based clinics (e.g. Blumenthal
1998, Al-Eissa et al. 2000, Sarrell et al. 2002). Temperatures of 38.0ºC and below
continue to be considered representative of fever (e.g. Blumenthal et al., 1998,
Sarrell et al. 2002). Beliefs that fever is harmful causing febrile convulsions and
brain damage abound (e.g., Schmitt, 1980, Al-Eissa et al. 2000; Karwowska et al
.2002;). Antipyretic administration as the preferred method of reducing fever has
increased from 67% in 1980 (Schmitt 1980) to 95% in 2002 (Karwowska et al.
2002). Similarly, overdosing with antipyretics increased from 12% in 1987 (Kilmon
1987) to 33% in 1999 (Linder et al. 1999). Alternating antipyretics, a potentially
unsafe practice reported since 2000, increases the opportunity for overdosing with
either or both antipyretics (Mayoral et al. 2000, Carson 2003). However, the use of
cold/ice-cold sponging/bathing, alcohol rubs and Aspirin have reduced significantly
(Drwal-Klein & Phelps 1992, Cranswick & Coghlan 2000, Karwowska et al. 2002).
120
Qualitative studies are few and report parental concerns, difficulties and practices
and factors influencing these (Kai, 1996a,b, Lagerlov et al. 2003). Kai (1996a,b)
concluded practices were influenced by the parenting role; to protect children from
suffering and harm. Childhood illnesses disempower parents. Monitoring
temperatures and reducing fevers with antipyretics gives a feeling of mastery and
medical assistance is sought for reassurance (Kai, 1996a,b, Lagerlov et al. 2003).
Fever legitimises the use of antipyretics; they calm the child allowing family
members to get some sleep (Lagerlov et al. 2003).
These studies provide a broad picture of parental fever management practices but
little insight into the reasons behind them. Data are needed to assist community-
based health professionals positively influence parents’ health decisions. Identifying
the knowledge, beliefs, practices of, and influencing factors on, parents of well
children’s practices enables health professionals target these parents’ education
toward reducing deficits and negative influences and reinforcing positive influences.
Learning to manage fever at a non-threatening time, when their child is well, would
assist the reduction of parents’ mismanagement of fever.
5.1.2 Aims The aim of the study was to investigate influences on fever management practices of
parents of well children aged between 6-months and 5-years. More specifically,
parents’ knowledge and beliefs about fever and fever management, methods of
managing fever, mode of learning to manage fever and the influences of these on
knowledge, beliefs and practices were explored.

121
5.2 METHOD
5.2.1 Design A qualitative study using semi-structured discussions with individuals and groups
was undertaken to explore parents of well children’s fever management, gain an
understanding of their thinking and generate new knowledge (Minicheillo et al.
2004). Both methods involve participant explanation, provide insight into sources of
complex behaviours and motivations and are appropriate in areas of limited research
(Morgan 2004). Interview dynamics place a burden on interviewees to explain
themselves to the interviewer; in group discussions group members query each other
and explain themselves to each other (Morgan 2004).
Ethical approval was obtained from the university human research ethics committee.
Voluntary participation was by informed written consent with assurances of
confidentiality and anonymity.
5.2.2 Sample A purposive convenience sample of 15 metropolitan parents self selected to
participate. Eligibility criteria included aged 18 years or older, able to read and
converse in English and being a parent and primary caregiver for a child aged
between 6-months and 5-years. All participants were female, married (86.7%) and
aged between 29 and 42 years (mean 34.1, SD 3.63). Most were the primary
caregiver of two or more children (66.7%). They majority had either a university
degree (53.3%) or Technical And Further Education (TAFE) certificate (40%) and
were employed (93.3%) predominantly part-time (86.7%).
122
5.2.3 Focused Questions Semi-structured questions were developed from an extensive review of the literature
and the author’s past experience in fever management research ( Edwards et al.
2001b, 2003; Walsh et al. 2005, 2006). Four areas were targeted: parents’ knowledge
and beliefs about fever, method of fever management and sources of information
about fever management. Questions are displayed in Table 1.
5.2.4 Recruitment and Procedure An advertisement in Playgroup Queensland’s monthly online newsletter and letters
distributed to parents of children enrolled at two Childcare centres resulted in
recruitment of five parents from each area. Interested parents contacted the
researcher and discussion mode (group or interview) was determined by parent’s
employment and parenting responsibilities. Six interviews and three group
discussions were conducted in naturalistic settings (home, office, childcare centre)
(Green & Thorogood 2004). Both interviews and discussions were conducted with
parents recruited from Playgroup Queensland or Childcare Centres.
To ensure data comparability, data collection was conducted by one moderator,
experienced in group discussions and interviewing. All discussions were facilitated
by the use a semi-structured interview guide finalised following an initial exploratory
interview (Morgan 2004). See Table 1. Predetermined prompt questions stimulated
discussion when necessary. Data saturation was reached after two group and six
interview discussions. A final group discussion with five parents confirmed
saturation. The moderator ensured equality in group participant’s involvement.
Group discussions were between 50 and 90 minutes, interviews 20 to 30 minutes.
Natural groups were used with participants acquainted through work or childcare
connections (Green & Thorogood 2004). Data reliability was ensured through
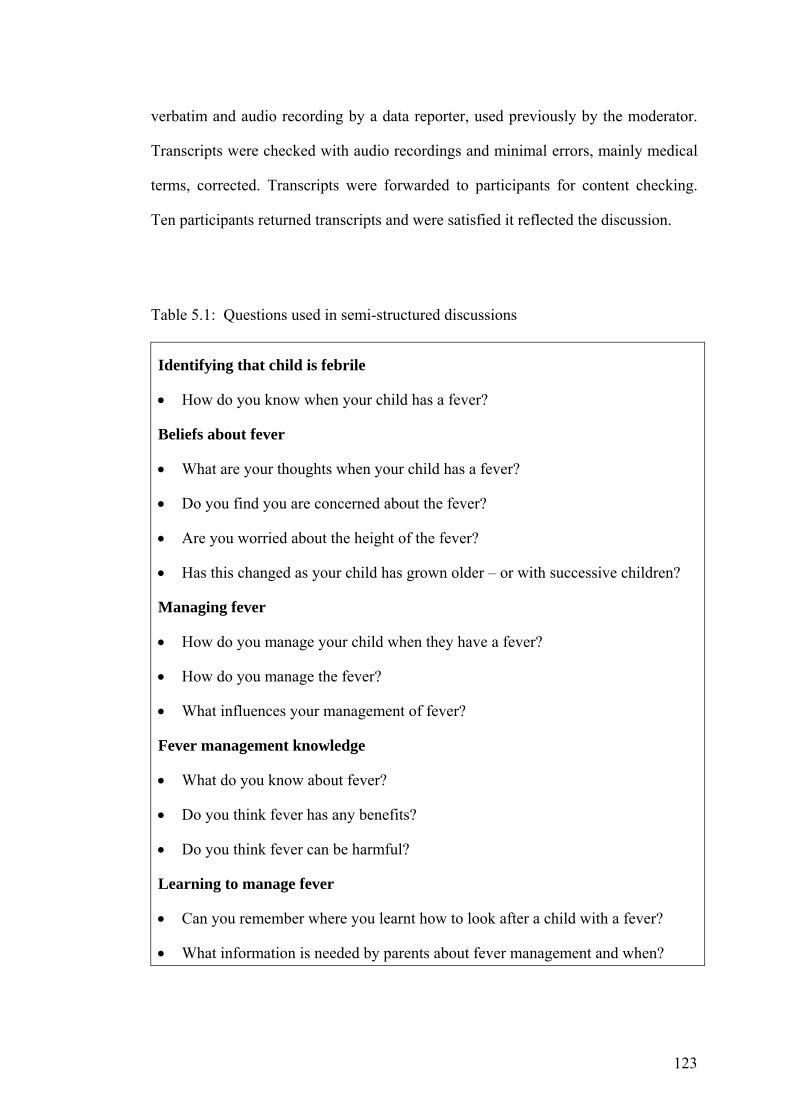
123
verbatim and audio recording by a data reporter, used previously by the moderator.
Transcripts were checked with audio recordings and minimal errors, mainly medical
terms, corrected. Transcripts were forwarded to participants for content checking.
Ten participants returned transcripts and were satisfied it reflected the discussion.
Table 5.1: Questions used in semi-structured discussions
Identifying that child is febrile
• How do you know when your child has a fever?
Beliefs about fever
• What are your thoughts when your child has a fever?
• Do you find you are concerned about the fever?
• Are you worried about the height of the fever?
• Has this changed as your child has grown older – or with successive children?
Managing fever
• How do you manage your child when they have a fever?
• How do you manage the fever?
• What influences your management of fever?
Fever management knowledge
• What do you know about fever?
• Do you think fever has any benefits?
• Do you think fever can be harmful?
Learning to manage fever
• Can you remember where you learnt how to look after a child with a fever?
• What information is needed by parents about fever management and when?
124
5.2.5 Data Analysis To ensure data trustworthiness and that comprehensive valid data were
collected multiple discussions were conducted until data saturation was
achieved and confirmed (Morgan 2004). Data were analysed thematically in
accordance with Burnard’s (1991) 14 stage method. Emergent themes were
then linked to develop a category system. The first author and an experienced
qualitative researcher independently identified themes, categories and sub-
categories for two transcripts. These were checked and deemed to be
consistent. Remaining transcripts were analysed by the first author according
to identified themes and categories.
5.3 FINDINGS Findings will be discussed according to the six themes: my child has a fever; fever is
beneficial, high fever is harmful, influencing factors, managing fever and learning to
manage fever.
5.3.1 My Child has a Fever Parents associate specific changes in their child’s normal behaviour with fever.
These include lethargy, agitation or restlessness, irritability, listlessness, withdrawal,
wanting to be comforted or stay close to a parent, refusing food, babbling in a
feverish manner or becoming very quiet verbally. Not sleeping well, pulling at the
ears or flushed cheeks were also reported as signs of fever. Children able to
communicate verbally tell parents they feel unwell. These behaviours cause parents
to touch their child to see if they are ‘hot’, indicating a fever.
P9. With my kids it is that they don't have the energy, usually that's the first sign.
They get a bit whiny. They won't eat and you go to give them breakfast or something
125
to eat and they won't eat. They just are clingy, my daughter is ‘Velcro’…hanging off
your body.
5.3.2 Fever is Beneficial Fever was considered a warning signal, alerting parents that something was wrong
with their child’s body. This was considered to be ‘good’. Some thought fever was
part of the body’s defence mechanism for combating invading organisms. Most were
unaware of immunological benefits associated with fever; those who were had learnt
from health professionals. Knowledge of temperature representative of fever was
poor, ranging from 37.5ºC to 39.1ºC (mean 38.1ºC, SD 0.5). Parents believed
temperatures would continue to rise if they were not actively reduced; there was no
ceiling for temperatures resulting from infection. The discussion below highlights
that although fever is beneficial there is concern about the height of the fever.
P12. My doctor has told me that fever is good. He said "Don't panic about fever;
that is your body is trying to fight whatever is going on in there." Even though it is
bad, it is good. It is trying to get it (the infection) out of the system.
P15. I think it is good. It is the natural way of trying to confront or work over the
virus.
P14. If it is natural and I am only asking a question here - if it is natural, how come
we give Panadol (paracetamol) to take it down then? Do you see what I am saying?
P15. Yes.
P13. I might be able to answer that one. From where I stand, the reason I give
them the Nurofen (ibuprofen), Panadol or whatever when they have their
temperature is because the temperature gets to the level that I don't feel comfortable
126
with. I start thinking of potential fitting or the fact that you know their head is going
to explode or ---
P14. They could end up with brain damage.
P13. And so to that extreme, that's why, because the temperature and all the rest is
good, I ignore it and that's just my way of doing things. That's not to say they are not
scary. Temperatures are scary. Temperatures can be very scary.
5.3.3 High Fever is Harmful Harm from high fever included febrile convulsions, death, dehydration, a stroke and
cardiac problems. Most parents indicated high fever, ranging from 38.0ºC to 39.1ºC
was harmful. All believed temperatures of 40.0ºC and over harmful. To prevent harm
high fever must be prevented, controlled and reduced. Children were monitored
closely and antipyretics administered when temperatures did not reduce or continued
to rise. Medical assistance was sought for temperatures unable to be reduced,
recurrent and high fevers. In an attempt to prevent harm advice was sought from the
family general practitioner (GP) prior to a weekend or public holiday, if a child
remained febrile for more than one day, became listless or lethargic or there was a
probability of dehydration.
P7. 39 something, 40… I would be concerned if I couldn't get that fever down, that
whole seizure thing, whether that would cause some sort of brain damage, something
with the brain.
127
5.3.4 Influencing Factors Factors reducing and increasing concerns about fever were reported.
5.3.4.1 Positive Factors Reduce Concern Most parents reported their concerns reduced over time as they learnt to identify
illness behaviours and differentiate between serious and minor self-limiting illness.
High temperatures unrelated to illness behaviours were not as worrying.
P1. It’s quite different now from the first new baby I think. It really does change
after you have had the second one, I think. Now I don’t worry so much. If you had
spoken to me in the first six months of my first child, my responses would have been
quite different.
Behaviours associated with specific illnesses (e.g., tonsillitis and otitis media) were
learned through consultations with health professionals. Receiving definitive
diagnoses and consistent medical advice increases parents’ confidence in their GP.
Parents receiving reassurance of their ability to judge illness severity, use appropriate
fever management practices and determine when medical assistance is necessary feel
confident in their own abilities to manage childhood fevers appropriately.
P6. But because they were so young I went to the GP more for reassurance more
than anything, more to see what I was planning on doing, for reassurance. So I
received that reassurance.
Parnets believed that immunised children were unlikely to contract serious illnesses
and that older children are stronger and less likely to convulse. Parents can
128
communicate with verbal children. Learning appropriate antipyretic dosage and
frequency and that antipyretics can be alternated increases perceptions of control
over fever, reducing concerns. Medication information was gathered from
medication labels, health professionals and pharmacists.
P2. The real beauty was you can give Panadol and Nurofen. Because they are two
different types of medication they won't overdose. You can only give Panadol four or
six hourly, he would be all right for two hours, then – up again, whereas if you gave
him Nurofen you could manage it pretty much the whole time without him spiking.
That was really useful information and I didn't know that to start with.
5.3.4.2 Negative Factors Increase Concern High Temperatures The first childhood fever, fever in babies, the firstborn and very young children were
reported as very worrying. Temperatures that rose rapidly or were not reduced by
antipyretics and fevers persisting for two or more days increased concerns for all
parents. In addition to temperature, rashes, high fevers associated with lethargy or
listlessness, potential serious illnesses and febrile convulsions added to parental
concern.
P7. …if they got really sort of quiet, listless kind of, couldn't rouse them or they
seemed a bit strange. If they were like that and they have high fever then I would be
worried.
Fear of Serious Illness External influences such as media reports, conflicting perceptions of illness severity
between GP and parent and when GPs do not give a definitive diagnosis increase
129
parents’ concerns. Media reports reinforce beliefs that fever is harmful and indicates
a serious illness. Reports of children seriously ill with meningococcal disease, rapid
deterioration of a febrile child with dire consequences and negative outcomes
following misdiagnosis increase concerns.
P7. Meningococcal, like every other mother, because you see all these things on
Today Tonight and A Current Affair (national current affair shows) like that because
I suppose, right or wrong, they have kind of honed in that message, that you
probably don't always have a lot of time.
When a definitive diagnosis is not found, parents are told ‘ít’s a virus´, or parental
concern and belief in illness severity is not reflected by the GP then parents become
increasingly concerned and their confidence in the GP reduces. Dissatisfied parents
sometimes sought a second or even third opinion from another GP or paediatric
emergency department. Receiving a different diagnosis or recommended treatment
from another GP can reduce parents’ confidence in GPs and increase their use of
emergency departments.
P9. "It's just a virus." I think how can you just look at them and say "It's just a
virus." How do you know it's not meningitis?
P14. I took him to the doctor and I expressed my concern and they said everything
was all right and I walked out, knowing he wasn't all right, and he ended up in
hospital that night for a week and a half so I just don't have a lot of faith in doctors.
130
Inaccessible family GPs on weekends or public holidays increase concerns about
their child deteriorating; this causes some to seek medical advice earlier than usual.
Others wait until their GP is available and worry about their child in the interim.
Some seek advice from an emergency department.
P5. If it is coming up to a weekend, I won't let her go for the, say if it is Friday I
won't let it go for the weekend. I will get it checked in case its something like a sore
throat, ears or coming down with a virus. It is reassurance for yourself.
Inconsistent Information Conflicting information about how to manage fever increased concerns, especially
when the information came from sources considered reliable and trustworthy, e.g., a
child health help-line, pharmacist, GP or emergency department. Conflicting GP
information included definitions of fever (38.0°C to 40.0°C), fever is beneficial – not
harmful versus administer antipyretics every four hours febrile children.
Misinformation from other parents included febrile convulsions at 38.0ºC;
temperatures of 39.0ºC – 40.0°C cause febrile convulsions with resulting brain
damage. When this occurs worried, anxious parents still need to decide how to
manage the fever; where to go for information, who to trust.
P3 … one doctor will tell you something different to the nurse or tell you something
different to the chemist. That sort of does make it a bit hard sometimes.
Parental Protective Role - Protecting from Harm All parents believed fever could precipitate a febrile convulsion. They had incorrect
knowledge of risk factors for febrile convulsions learnt from, e.g., mothers groups,
child health books. Parents reported a strong need to control and reduce fever to
protect children from the harm associated with fever.
131
P5. My immediate thought is basically to control the fever so they don't end up
having febrile convulsions or something like that.
Although antipyretics were used to reduce fever and thereby protect from harm some
had concerns about antipyretics. Concerns were expressed about medication dosages,
the possibility of overdosing and the safe length of time to use antipyretics, e.g., five
days for a young child. Conflicting beliefs make fever management difficult; beliefs
that fever must be controlled and reduced conflict with beliefs that antipyretics have
harmful side effects. However, beliefs about the harmfulness of fever were stronger
and antipyretics were used to reduce fevers. Media reports of accidental paracetamol
overdosing contributed to this dilemma. However, by alternating antipyretics parents
were able to reduce high fevers reducing this concern. Alternating antipyretics was
considered a safe practice; fever was reduced and overdosing with one antipyretic
prevented.
P2. I worry about what effect the drugs have on them. I do try not to use them but
you have to. The flipside of that is that I worry about whether it gets too high. If that
is going to happen there are those two concerns, kind of balancing each other out.
Negative events associated with fever increase perceptions of harm causing parental
guilt. Parents assumed responsibility for delaying seeking medical assistance for
illnesses believed inconsequential, e.g., tonsillitis diagnosed as glandular fever, and
precipitating a febrile convulsion by tepid bathing a febrile child (40°C). Children of
three parents (20%) had a febrile convulsion increasing antipyretic use and the belief
fever is harmful. One parent introduced a safe guard mechanism to prevent continued
132
accidental overdosing with antipyretics by recording medication administration
during febrile episodes.
P9. We write it on the notice board now because there were two times when I had
given it to her and half an hour later he had.
Antipyretics are believed to reduce temperatures and therefore prevent febrile
convulsions. Following a febrile convulsion, parents administered antipyretics as
soon as they were aware a child was febrile. Only one parent, when the child did not
have a recurrent febrile convulsion, returned to pre-febrile convulsion management
using non-pharmacological methods first. Others continued to reduce all fevers with
antipyretics.
P9. Antipyretics at 38 and a half probably! I don't let it go too high. My daughter
had a fit once from a high temperature and I was quite frightened by that so I don't
usually let it hang around for too long.
5.3.5 Learning to Manage Fever Parents reported learning about fever and its management from child health books,
doctors, child health nurses and help lines, hospitals, emergency departments,
professional education, biology or physiology lectures at school or university, other
mothers, own mother, sisters, friends with children and pharmacists. Information
from health professionals was most trusted. The Internet was not generally a source
of child health information. The accuracy of information and reliable sites was
questioned. Books or a phone call are easier information sources, than the Internet,
with a child is febrile.
133
P3 We had phone calls to Mum, we had phone calls to the child health people, visits
to the chemist, to see what they thought down at the chemist. We were at the doctor's
once. The doctor said "It will be gone in 24 hours." Finally, the second doctor's was
after the hospital visit.
5.3.6 Managing Fever Fever management includes identifying the cause for the fever and symptoms
necessitating medical intervention. They are controlled or reduced by both non-
pharmacological and pharmacological methods. Children able to communicate
verbally were asked how they felt. Most parents used non-pharmacological methods
initially. These included removing additional clothing, monitoring to ensure the child
did not get chilled, cold drinks or ice blocks and cool/tepid cloths or baths. During
hot tropical summers environmental cooling included opening windows, using fans
and air-conditioners. Most offered fluids although some report febrile children were
reluctant to drink. Comforting the child, monitoring behaviour and encouraging rest
were reported by some.
Antipyretics were the first line of treatment for some irrespective of temperature.
Others used them when non-pharmacological methods were ineffective. Additional
methods are incorporated when temperatures were not reduced sufficiently within 30
minutes to two hours following an antipyretic. These included additional non-
pharmacological methods or an alternate antipyretic was administered. Some
preferred a specific antipyretic, for example ibuprofen; others avoided ibuprofen
because of side effects, gastrointestinal bleeding and triggering asthma. Antipyretic
administration ranged from one dose, regular doses of the same antipyretic and
alternating antipyretics. Antipyretics were administered for temperatures ranging

134
from 37.0°C to 40.0°C (mean 38.3°C, SD 0.78°C) and for pain. All parents had used
antipyretic to reduced temperatures of 39.0°C.
P6. Generally check their forehead then take temperature, ask them how long they
have felt this way, try to think of a probably cause, temperature of 38 would probably
keep a closer eye on them, 37.5 doesn’t worry me. Lie them down, keep them
comfortable, remove extra clothing, make sure they don’t get chilled, monitor, if
distressed/crying/complaining of a headache give paracetamol, otherwise offer lots
of fluids, cuddle them, sit down next to them and pat them, keep them calm, just keep
an eye on the temperature, take temperature every couple of hours, use a wet flannel,
cool/lukewarm bath, prior to medications. Do keep an eye on them because one had
a febrile convulsion.
Decisions to seek medical advice were influenced by distance to and availability of
preferred GP. Weekends and close physical proximity increased GP use for advice
and reassurance. Others living a distance, e.g. 30 minute drive, from their GP delay
seeking assistance until it is ‘really’ necessary. Parents not confident in local GPs
seek advice and reassurance from emergency departments.
5.3.7 Need for Timely, Consistent Information Parents considered it important for all parents, particularly new parents, to have
accurate information about fever, common childhood illnesses, signs and symptoms
of illness and managing a febrile child. Perceptions of the ideal time to receive
information were mixed. Some recommended during antenatal classes, ‘you are very
busy with the baby postnatally’. A 2-week old firstborn had a febrile illness. Others
135
recommended post-delivery, before the first febrile illness, from a doctor or child
health nurse at a well-baby visit or with the first immunisation.
5.4 DISCUSSION Parents’ fever management practices were influenced by their knowledge, beliefs and
information sources about fever management. They had limited knowledge of the
physiological changes and associated immunological benefits of fever. Fever was
believed to be harmful, requiring active reduction. Some parents dressed febrile
children in light clothing, encouraged fluids and monitored them prior to
antipyretics; others used antipyretics as a first line of treatment. Negative experiences
during febrile episodes influenced management increasing antipyretic use and
concern. Initially fever management was learnt from a variety of sources. Conflicting
information made management decisions difficult causing parents to seek further
advice, often medical. For most, concerns about fever reduced over time or
uneventful febrile illnesses.
5.4.1 Influence of Beliefs Parents believed fever needed to be controlled, treated quickly to prevent it rising
any higher or harming their child. The range of temperatures considered fever varied
1.6ºC (37.5ºC to 39.1ºC). Although some believed mild fever beneficial, they were
reluctant to allow fever to get too high. Parents reported concern about and actively
reduced temperatures of 38.0ºC to 39.0ºC (mild fever) with antipyretics, all reduced
temperatures of 40ºC (moderate fever). Beliefs of potential harm from fever have
been reported previously, febrile convulsions, dehydration, brain damage and death
(e.g. Crocetti et al. 2001, Karwowska et al. 2002, Sarrell i2002). Additional harmful
beliefs of stroke and cardiac problems were reported indicating transference of harm
to other major organs highlights parental fears; fears that are increasing rather than

136
decreasing fever phobia. Fever is not harmful, has a natural upper limit and
convulsions resulting from fever are benign (e.g. Chang et al. 2000, Chang et al.
2001, Kolfen et al. 1998, Lorin 1986).
Beliefs that fever indicates a serious illness were reinforced by media reports of
meningitis and meningococcal disease and occasions where misdiagnosis resulted in
a life-threatening event. Kai (1996b) reported this in 1996. Media influences may be
greater now than ten years ago. Increased media coverage and easy access to
information via the Internet could be responsible for maintaining and possibly
strengthening these beliefs. Interestingly beliefs about serious illnesses was tempered
with perceptions that older children, three years or older, were stronger and therefore
more resistant to serious illness than younger children. Although appropriate
immunisations were believed to protect children from serious illnesses, parents were
still concerned about meningitis in general and meningococcal meningitis
specifically.
5.4.2 Influence of Parental Role Parental protective role creates conflict. Parents believe fever is harmful and must be
reduced but are worried about side effects from, or overdosing their child with,
antipyretics. Despite this, beliefs about the potential harm of fever make antipyretic
use essential. Most parents alternated antipyretics. This practice increased control
over fever, reduced fever, maintained fevers at a temperature considered safe.
Concerns about overdosing with one antipyretic and side effects of each antipyretic
are also reduced by alternating antipyretics. Similarly to parents studied by Lagerlov
et al. (2003) antipyretics gave parents a feeling of control, they helped parents
believe they were preventing harm.
137
5.4.3 Influence of Experience Similar to earlier work by Kai (1996a) behaviours associated with fever were learnt
through experience with fevers. Identification of a cause for fever, fever management
strategies and illness severity were sought from books, friends and health
professionals. Parents perceived their need for reassurance from health professionals
with early febrile episodes as a learning experience enabling them to differentiate
between minor and serious illnesses and illnesses requiring medical intervention,
e.g., otitis media, tonsillitis. Positive influences of experience were evident in
comparisons between earlier negative beliefs, with the first baby, and current more
positive beliefs. For example, febrile convulsions and brain damage are not
associated with temperatures of 38.0ºC and high temperatures (39.0ºC) unrelated to
illness behaviours are not harmful and do not require antipyretics.
Negative experiences during a febrile episode were associated with increased
monitoring and antipyretic use. Feelings of guilt were associated with perceived
inappropriate home management, precipitating a febrile convulsion and delays in
seeking medical assistance for a fever requiring medial intervention, e.g., antibiotics,
reflecting a strong sense of responsibility to be competent parents (Kai, 1996a).
Experiences with missed or unsatisfactory diagnosis or being told ‘it’s a virus’
continue to cause confusion and anxiety (Kai, 1996a). Parents reporting these
experiences frequently sought a second opinion. When beliefs the child was ill and/or
required treatment were confirmed, trust in general practitioners reduced and
paediatric emergency departments became the preferred source for medical advice
influencing both private and public health service use.
138
5.4.4 Influences of Knowledge and Information Sources Influences of parents’ limited knowledge about benefits of fever are evident in their
beliefs and fever reduction practices. Knowledge of fever’s benefits, although
limited, was learnt from doctors. The endless search for information from a variety of
sources created additional problems. Information from family, friends, books and
health professionals was often contradictory. Conflicting information increases
concerns about management promoting feelings of insecurity. Parents either seek
additional information from health professionals and literature or base management
decisions on past experiences, not necessarily positive experiences.
5.4.5 Implications for Health Professionals Conflicting information about fever management from health professionals is
unacceptable. Evidence about the benefits of mild to moderate fever and
recommendations for antipyretic use based on the child’s well-being have been
reported in health literature for more than two decades (e.g. Schmitt 1984, Kluger,
1986, Lorin, 1986, 1999, Zeisberger 1999, Mackowiak 2000, Blatteis 2003, Roth et
al. 2004). Health professional encouragement of unnecessary fever reduction
reinforces negative beliefs and can prolong illnesses (Graham et al. 1990).
Unnecessary antipyretic administration and alternating antipyretics increase the
probability of overdosing with potentially serious consequences (Kearns et al. 1998).
It is necessary to raise health professionals’ awareness of these issues. Health
professionals must update their knowledge and encourage parents to practice in a
manner based on the latest scientific evidence. Education must target individual
parent’s knowledge deficits, beliefs and practices. Current myths and misconceptions
must be addressed to enable parents to respond with evidence-based information
when confronted. Evidence-based guidelines for the use of antipyretics in mild to
moderate fever are necessary.
139
5.4.6 Strengths and Limitations This study detailed the fever management practices of parents of well children; the
aim was achieved and important influences identified. However, qualitative research
is not generalisable and parents who participated had tertiary education and were
from metropolitan areas. Therefore findings need to be interpreted with caution.
Future studies with larger and more representative samples are needed to confirm the
findings of this study.
5.5 CONCLUSIONS Mixed experiences with and information sources about childhood fevers influenced
parental knowledge, beliefs and practices. For most, beliefs and concerns about and
negative consequences of fever reduced over time through experiences with
uneventful febrile episodes, learning to identify differences between minor self-
limiting viral infections and serious illnesses, beliefs that serious illnesses were
unlikely in immunised children and perceptions of increased knowledge. For some,
reduced antipyretic use was associated with reduced concerns. Negative experiences
during a febrile episode, such as a febrile convulsion, delayed medical intervention,
being told ‘it’s a virus’, receiving conflicting advice and media reports of serious
illnesses reinforced negative beliefs. Negative beliefs encouraged increased
antipyretic administration, monitoring and health service usage. Health professionals
must ensure fever management information provided to parents is consistent, based
on the latest scientific evidence and made available to parents before their first
experience with a childhood fever.
5.6 ACKNOWLEDGEMENTS The authors would like to thank Dr Helen Chapman from the School of Nursing,
Queensland University of Technology for expert assistance with data analysis and
140
the Australian Confederation of Paediatric and Child Health Nurses for their support
through the Margaret Sullivan Scholarship which assisted in data collection. We
would also like to thank the parents who gave their valuable time to participate.
5.7 FUNDING Margaret Sullivan Scholarship from the Australian Confederation of Paediatric and
Child Health Nursing Queensland Inc.
5.8 REFERENCES Al-Eissa Y, Al-Zamil F, Al-Sanie A, Al-Salloum A, Al-Tuwaijri H, Al-Abdali N &
Al-Azzam S (2000a). Home management of fever in children: rational or ritual? International Journal of Clinical Practice, 54, 138-142.
Al-Eissa Y, Al-Sanie A, Al-Alola S, Al-Shaalan M, Ghazal S, Al-Harbi A & Al-
Wakeel A (2000b) Parental perceptions of fever in children. Annals of Saudi Medicine, 20, 202-205.
Ames J, Hayden G, Campbell R & Lohr, J. A. (1982) Parents' conception of their use
of over-the-counter medicines. Clinical Pediatrics, 21, 298-301. Blatteis C (2003) Fever: pathological or physiological, injurious or beneficial?
Journal of Thermal Biology, 28, 1-13. Blumenthal I (1998) What parents think of fever. Family Practice, 15, 513-518. Burnard P (1991) A method of analysing interview transcripts in qualitative research.
Nurse Education Today, 11, 461-466. Carson S (2003) Alternating acetaminophen and ibuprofen in the febrile child:
Examination of the evidence regarding efficacy and safety. Pediatric Nursing, 29, 379.
Chang Y, Guo N, Huang C, Wang S & Tsai J (2000) Neurocognitive attention and
behavior outcome of school-age children with a history of febrile convulsions: a population study. Epilepsia, 41, 412-420.
Chang, Y. C., Guo, N. W., Wang, S. T., Huang, C. C., & Tsai, J. J. (2001). Working
memory of school-aged children with a history of febrile convulsions: a population study. Neurology, 57(1), 37-42.
Cranswick, N., & Coghlan, D. (2000). Paracetamol efficacy and safety in children:
the first 40 years. American Journal of Therapeutics, 7(2), 135-141.
141
Crocetti, M., Moghbeli, N., & Serwint, J. (2001). Fever phobia revisited: have parental misconceptions about fever changed in 20 years? Pediatrics, 107(8), 1241-1246.
Drwal-Klein, L. A., & Phelps, S. J. (1992). Antipyretic therapy in the febrile child.
Clinical Pharmacy, 11(12), 1005-1021. Edwards, H. E., Courtney, M. D., Wilson, J. E., Monaghan, S. J., & Walsh, A. M.
(2001). Fever management practices: what pediatric nurses say. Nursing and Health Sciences, 3(3), 119-130.
Edwards, H. E., Courtney, M. D., Wilson, J. E., Monaghan, S. J., & Walsh, A. M.
(2003). Fever management audit: Australian nurses antipyretic usage. Pediatric Nursing, 29(1), 31-37.
Graham, M. H., Burrell, C. J., & Douglas, R. M. (1990). Adverse effects of aspirin,
acetaminophen, and ibuprofen on immune function, viral shedding, and clinical status in rhinovirus-infected volunteers. Journal of Infectious Diseases, 162, 1277.
Green, J. L., & Thorogood, N. (2004). Qualitative methods in health research.
London: Sage. Impicciatore, P., Nannini, S., Pandolfini, C., & Bonati, M. (1998). Mothers'
knowledge of, attitudes toward, and management of fever in preschool children in Italy. Preventive Medicine, 27(2), 268-273.
Kai, J. (1996a). Parents' difficulties and information needs in coping with acute
illnesses in preschool children: a qualitative study. British Journal of Medicine, 313, 987-990.
Kai, J. (1996b). What worries parents when their preschool children are acutely ill,
and why: a qualitative study. British medical Journal, 313, 983-986. Karwowska, A., Nijssen-Jordan, C., Johnson, D., & Davies, H. (2002). Parental and
health care provider understanding of childhood fever: a Canadian perspective. Canadian Journal of Emergency Medicine, 4(6), 394-400.
Kearns, G. L., Leeder, J. S., & Wasserman, G. S. (1998). Acetaminophen overdose
with therapeutic intent. The Journal of Pediatrics, 132(1), 5-8. Kilmon, C. (1987). Parents' knowledge and practices related to fever management.
Journal of Pediatric Health Care, 1(4), 173-179. Kluger, M. (1986). Is fever beneficial. The Yale Journal of Biology and Medicine,
59(2), 89-95. Kolfen, W., Pehle, K., & Konig, S. (1998). Is the long-term outcome of children
following febrile convulsions favorable? Developmental Medicine & Child Neurology, 40(10), 667-671.
142
Lagerlov, P., Helseth, S., & Holager, T. (2003). Childhood illnesses and the use of paracetamol (acetaminophen): a qualitative study of parents' management of common childhood illnesses. Family Practice, 20(6), 717-723.
Linder, N., Sirota, L., Snapir, A., Eisen, I., Davidovitch, N., Kaplan, G., et al. (1999).
Parental knowledge of the treatment of fever in children. Israel Medical Association Journal: IMAJ, 1(3), 158-160.
Lorin, M. I. (1986). Is fever a friend or a foe? Contemporary Pediatircs, 3, 35-46. Lorin, M. I. (1999). Pathogenesis of fever and its treatment. In J. B. McMillan, C.
DeAngelis, R. D. Feigin & J. B. Warshaw (Eds.), Oski's Pediatrics: principles and practices (3rd ed., pp. 848-850). Philadelphia: Lippincott, Williams & Wilkins.
Mackowiak, P. A. (2000). Diagnostic implications and clinical consequences of
antipyretic therapy. Clinical Infectious Diseases, 31, S230-S233. Mayoral, C. E., Marino, R. V., Rosenfeld, W., & Greensher, J. (2000). Alternating
antipyretics: is this an alternative. Pediatrics, 105(5), 1009-1012. McErlean, M. A., Bartfield, J. M., Kennedy, D. A., Gilman, E. A., Stram, R. L., &
Raccio-Robak, N. (2001). Home antipyretic use in children brought to the emergency department. Pediatric Emergency Care, 17(4), 249-251.
Minicheillo, V., Sullivan, G., Greenwood, K., & Axford, R. (Eds.). (2004).
Handbook of research methods for nursing and health science (2nd ed.). Frenchs Forest, NSW: Pearson Education Australia.
Morgan, D. L. (2004). Focus groups. In S. N. Hesse-Biber & P. Leavy (Eds.),
Approaches to qualitative research: a reader on theory and practice (pp. 263-285). Qxford: Oxford University Press.
Roth, J., Rummel, C., Harre, E.-M., Voss, T., Mutze, J., Gerstberger, R., et al.
(2004). Is interleukin-6 the necessary pyrogenic cytokine? Journal of Thermal Biology, 29(7-8), 383-389.
Sarrell, M., Cohen, H. A., & Kahan, E. (2002). Physicians', nurses', and parents'
attitudes to and knowledge about fever in early childhood. Patient Education and Counselling, 46, 61-65.
Schmitt, B. D. (1980). Fever phobia: misconceptions of parents about fevers. American Journal of Diseases in Children, 134(2), 176-181. Schmitt, B. D. (1984). Fever in childhood. Pediatrics, 74 (Suppl), 929-936. Walsh, A. M., Edwards, H. E., Courtney, M. D., Wilson, J. E., & Monaghan, S. J.
(2005). Fever management: paediatric nurses' knowledge, attitudes and influencing factors. Journal of Advanced Nursing, 49(5), 453-464.

143
Walsh, A. M., Edwards, H. E., Courtney, M. D., Wilson, J. E., & Monaghan, S. J. (2006). Paediatric fever management: Continuing education for clinical nurses. Nurse Education Today, 26, 71-77.
Zeisberger, E. (1999). From humoral fever to neuroimmunological control of fever.
Journal of Thermal Biology, 24(5-6), 287-326.
144
CHAPTER 6 – STUDY 2
DESCRIPTIVE FINDINGS
This chapter presents two articles reporting the descriptive findings from Section 1 of
Study 2, the survey of Queensland parents. The instrument developed for use in
Study 2 was based on the literature and findings from Study 1, the qualitative study
reported in the previous chapter. In the first article parents’ fever management
knowledge, beliefs, practices and sources of fever management information are
reported. Specific areas included in the first article, developed from findings from
Study 1, explored changes in fever management practices over time and the
influences on these, temperatures considered harmful and the harm these
temperatures could cause, specific concerns when a child is febrile, influences on
alternating antipyretics and receiving conflicting information.
The second article focuses on the use of over-the-counter medications in childhood
fever management. Specific areas included in article 2 developed from the findings
from Study 1 are difficulties in medication administration, temperatures at which
parents alternate antipyretics and reasons for alternating, whether medications were
perceived as harmful and the harm these medications could cause. Items targeting the
type of medications used to reduce fever identified paracetamol and ibuprofen and
included space for parents to include additional over-the-counter preparations such as
homeopathic, herbal and additional analgesic/antipyretics.
145
6.1 ARTICLE 1 Underpinned by fear: a community study of parents' fever management with young children Walsh, A. M., Edwards, H., & Fraser, J. (under review). Underpinned by fear: a
community study of parents' fever management with young children. Journal of
Advanced Nursing. Journal Impact Factor: 1.342
Abstract Aims. Explore Australian parents’ knowledge, beliefs, practices and information
sources about fever management and develop a scale to measure parents’ fever
management practices.
Background. Internationally, parental fever phobia and overuse of antipyretics to
reduce fever continues. No developed scales are available. Australian parents’ beliefs
and practices are unknown.
Method. A community-based, postal survey of 401 Australian parents of well-
children aged 6-months to 5-years during 2005 were recruited through advertising
(48.4%), face-to-face (26.4%) and snowball (24.4%) methods. A 33 item instrument
was developed; construct and content validity determined by an expert panel and
item reliability by test-retest with nine parents.
Results. Most respondents were female, had university education and lived in a
major city. Moderate fever (40.0ºC ± 1.0ºC) was reported harmful (88%), causing
febrile convulsions (77.7%). Usual practices targeted temperature reduction,
antipyretic administration (87.8%), temperature monitoring (52.5%) and 51.8% had
alternated antipyretics. Fewer evidence-based practices such as encouraging fluids
(49.0%) and light clothing (43.8%) were reported. Positive changes over time
(36.4%) included less concern; delayed or reduced antipyretic use. Negative practice
146
changes (22.7%) included greater concern and increased antipyretic use. Medical
advice was sought for illness symptoms (48.7%), high (37.4%) or persistent (41.5%)
fevers. Fever management was learnt from doctors, family and friends and
experience; receiving conflicting information (41.9%) increased concerns and
created uncertainty about best practice.
Conclusions. Australian parents’ practices are influenced by concerns about fever
indicated by preferences for antipyretic use and the percentage who had alternated
antipyretics. Conflicting information increases concerns identifying a need for
consistent evidence-based information from health professionals.
What is already known about this topic:
o Internationally, parents are overly concerned about harmful outcomes from
childhood fever.
o Antipyretic use, as parents’ preferred method of reducing fever, has
increased.
o Parents often incorrectly dose febrile children with antipyretics.
o No known tools to measure the physical burden of care on parents during
childhood fever.
What this paper adds: o Australian parents have similar concerns about harmful outcomes from
childhood fever as their international counterparts.
o More than half the parents surveyed had alternated antipyretics.
o Parents receive conflicting information about how to manage fever causing
confusion and increasing concerns and best practice in fever management.
o Development of a scale to measure parents’ fever management practices.

147
6.1.1 Introduction Internationally, little has changed in parents’ concerns about childhood fever since
Schmitt (1980) coined the term ‘fever phobia’ describing parents’ irrational concerns
about fever. Parents continue to reduce fever to prevent febrile convulsions and brain
damage and more recently to prevent discomfort and improve general well-being
(Crocetti et al. 2001, Karwowska et al. 2002). Childhood fever has a socioeconomic,
physical and emotional influence on parents who take time off work, seek medical
advice, purchase pharmaceuticals and need more assistance at home (Principi et al.,
2004). Fever phobia increases the physical and emotional burden through constant
temperature taking, worry and sleepless nights and could influence parents’ practices
(Impicciatore et al. 1997, Lagerlov et al. 2003). Internationally, although many
studies are reported, studies replicating earlier studies allowing comparisons are
scarce (Crocetti et al. 2001, Taveras et al. 2004) and scales appropriate for fever
management research unavailable. This paper begins to address this deficit and the
dearth of literature reporting Australian parents’ knowledge, beliefs, practices and
methods of learning to manage fever.
6.1.1.1 Background Fever No definitive temperatures considered to be normal, fever or high fever are
consistently reported in the literature. Normal temperature in infants ranges from
37.5ºC ± 0.3ºC with 0.3ºC seasonal variation between summer and winter and a
0.1ºC per month increase from 1-month to 3-months of age (Herzog & Coyne, 1993).
Hertzog and Coyne (1993) concluded 38.2ºC or greater would indicate fever in a 3-
month infant. Others report 38.0ºC, indicates childhood fever (Chamberlain et al.
1995, Schmitt 1984). More recently Sarrell et al. (2002), agreeing with El-Radhi and
Carroll (1994), defined fever as 38.0°C rectally or an axillary temperature of 37.2°C.
148
Moderate fevers, up to 40.0ºC are associated with immunological benefits (Connell
1997, Holtzclaw 1992, Lorin 1999). High fevers, 40.5ºC or over, generally indicate
bacterial infection (Schmitt 1984). Brain damage is unlikely unless fever exceeds
41.7ºC, harmful or dangerous fever; exogenous antipyretics prevent this occurring in
infectious fever (Mackowiak & Boulant 1996).
Parents and Fever Parents seeking medical assistance in an emergency department in the United Arab
Emirates recently reported 37.5ºC to indicate fever (Betz & Grunfeld 2006).
Canadian parents of febrile children reported fever to be 37.9ºC (SD 0.7ºC), high
fever 39.2ºC (SD 0.7ºC) and dangerous fever 39.9ºC (SD 0.8ºC) (Karwowska et al.,
2002). Other studies reported parent definitions of fever between 37.0°C and 39.0°C
with 38.0°C most common (Blumenthal 1998, Impicciatore et al. 1998, Porter &
Wenger 2000) and high fever between 39.0°C and 40.0°C (Al-Eissa et al. 2000a,
Crocetti et al. 2001).
Parents reduce mild low grade fevers, 38.2ºC to 38.9ºC, to prevent harmful outcomes
(Al-Eissa et al. 2000b, Crocetti et al. 2001, Karwowska et al. 2002). Antipyretic use,
the preferred fever reduction method, has increased from 67% (Schmitt 1980) to 95%
(Karwowska et al. 2002). In the last decade the practice of alternating antipyretics
when temperature reduction is insufficient or fever returns has become more popular
(Crocetti et al. 2001, Li et al. 2000); recently 67% of parents in Alabama, United
States, alternated (Wright & Liebelt 2007). This is disturbing in relation to continued
reports of parents’ incorrect antipyretic dosing (Goldman & Scolnik 2004, Kilmon
1987). Recently, less than half, 47% to 49%, the children presenting at emergency
departments had received the correct antipyretic dose (Goldman & Scolnik 2004,
149
McErlean et al, 2001). Underdosing with antipyretics increases health service usage
as parents perceive fever not sufficiently reduced or returning too soon (Li et al.
2000, McErlean et al. 2001). Overdosing has trebled from 12% (Kilmon 1987) to
33% (Linder et al. 1999). Younger children, under two years, are at greater risk of
unintentional overdosing (Alander et al. 2000, Kozer et al. 2002). Paracetamol is
among the most common over-the-counter medications associated with unintentional
overdose in Australian children younger than five years (Chien et al. 2003).
Fever is Beneficial There is overwhelming evidence that fever is an adaptive response in all vertebrates
(Kluger 1979). Mild to moderate fevers during febrile illnesses are associated with
enhanced immunological responses (Blatteis et al. 1998, Kluger 1986, Lorin 1999,
Mackowiak 1998). Fever plays a pivotal role in the anti-inflammatory response;
antipyretics may interfere with this response and should be avoided unless overriding
conditions exist (Blatteis 2003, Klein & Cunha 1996, Mackowiak 1998). Reducing
fever to prevent febrile convulsions is ineffective and unwarranted (Chang et al.
2001, Hutt et al. 1999). Large epidemiological studies concluded febrile convulsions
are benign events occurring in 5% of children aged three months to five years
(Chang et al. 2001, Kolfen et al. 1998).
Most recent research targeted parents of febrile children and parents seeking advice
at health clinics (Karwowska et al. 2002, Sarrell et al. 2002). Having an ill child or
being in a health environment could influence parents’ perceptions or responses. In
light of the dearth of Australian literature and community-based studies it was timely
for a comprehensive community-based investigation of Australian parents’ fever
150
management. This study builds on findings from a qualitative study to identify
Australian parents’ current knowledge, beliefs and practices (Walsh et al. 2007a).
6.1.2 The Study
6.1.2.1 Aims The aims of this study were to identify the knowledge, beliefs, practices and methods
of managing fever in a crossectional community-based sample of Australian parents
of young children and develop a scale to explore parents’ fever management
practices. Parents’ antipyretic use is discussed in detail elsewhere (Walsh et al.
2007b).
6.1.2.2 Design A self-report, self-administered, crossectional survey was undertaken in 2005.
6.1.2.3 Sample A convenient sample of parents of children aged between 6-months and 5-years
living in Queensland, Australia was recruited. Recruitment was through a range of
strategies: 1) advertising in parenting magazines (210 distributed, 194 returned;
92.4%); 2) face-to-face in child care centres, kindergartens and preschools (204
distributed, 104 returned; 60.0%); and 3) snowball technique (171 distributed, 98
returned; 57.3%). Nearly half were recruited through advertising (48.4%) and similar
percentages through childcare centres (26.4%) and snowball (24.4%). Three (0.8%)
returned completed questionnaires with the identifying number removed.
6.1.2.4 Data Collection In an attempt to recruit a representative sample three recruitment methods were
employed; 1) advertising, 2) face-to-face and 3) snowball.
1) Over a 3-month period advertisements were placed in parenting magazines
accessible freely to parents in metropolitan and outer metropolitan areas.

151
Playgroup Queensland members were targeted through the monthly online
newsletter and quarterly magazine. Queensland parents using Family Day
Care were targeted through care providers. Interested parents contacted the
researcher by phone (49.6%) or email (50.4%). Survey packages, containing
a letter of introduction, information sheet, survey and reply paid envelope,
were posted to interested parents.
2) Parents from metropolitan and outer metropolitan childcare centres,
kindergartens and preschools were informed of the study through posters and
individual letters. Interested parents received a survey package following
face-to-face recruitment and returned completed surveys to a sealed box in
the centre.
3) Queensland wide snowball recruitment was conducted through respondents
and researcher networks. Completed surveys were returned by mail or
collected by the initial contact and returned to the researcher.
6.1.2.5 Instrument An extensive search of the literature was conducted through Medline, CINAHL,
PsycINFO, PsycARTICLES and Web of Science databases from 1980 to 2004 for
articles from the developed world published in English. Instrument items were
developed from published and unpublished instruments and information gained
through semi-structured discussions with Australian parents of young children
(Walsh et al. 2007a). The instrument was piloted and the final instrument consisted
of 33 items. It explored parents’ knowledge (five items), beliefs about fever (six
items), general fever management practices (18 items) and sources of fever
management information (four items). See Table 6.1 for examples of constructs to
item development.
152
Appropriate terminology was determined through an earlier study (Walsh et al.
2007a); ‘medication’ was used for antipyretics and other over-the-counter
medications used to reduce fever; ‘fever’ for mild fever, ‘high fever’ for moderate
fever and ‘very high fever’ for high fever. To begin to address the deficit of
psychometrically tested scales for use in fever management research eight of the 18
fever management practices targeted parents’ physical burden of care during
childhood fever. Twenty-two demographic items were included.
6.1.2.6 Validity and Reliability Sample size was calculated by estimating the population proportion with specified
absolute precision (Lwanga & Lemeshow 1991). Calculations were based on
findings from other studies. Forty-six to 49% of parents believed a temperature of
38.0ºC represented fever (Al-Eissa et al. 2000a, Blumenthal 1988) and 78% to 80%
administered antipyretics for temperatures of 38.0ºC (Blumenthal 1998, Linder et al.
1999). For relative precision of the results at the 95% significance level and power of
90% a minimum sample of 384 parents were required.
Instrument content and face validity were confirmed by an expert panel consisting of
two clinical paediatric nurses, a paediatric nurse researcher and two nurse academics
(Polit & Hungler 1999). Item reliability was determined by test-retest (2-weeks) with
nine parents of children aged 6-months to 5-years. Kappa on categorical items ranged
from 0.55 (on one item) to 1.00. Bland Altman analysis (Bland & Altman 1986) on
all continuous items indicated responses were within the limits of agreement (mean
difference ± 2SD). One respondent’s responses on temperature for fever were outside
the limits of agreement. Following minor adjustments the instrument was deemed
suitable.
153
6.1.2.7 Ethical Considerations Ethical approval was obtained from the Queensland University of Technology
human research ethics committee. Voluntary participation in the study was by
informed consent with assurances of confidentiality and anonymity for all
participants. The return of a completed survey was considered consent to participate
in the study.
6.1.2.8 Data Analysis Responses to open-ended questions were coded and entered into SPSS Version 13
(SPSS 2004). Entry errors were checked and corrected using SPSS Data Entry
Builder 4.0 (SPSS 1996-2003). Demographic variables were examined for frequency
and distribution. Items measuring perceptions of temperatures representative of
fever, recorded on six scales, were checked for distribution normality and outliers.
An extreme outlier, fever is harmful at 100ºC, was removed (Tabachnick & Fidell
2007). Open-ended responses were collated using the multiple response analysis in
SPSS. Categorical and open-ended responses were then explored for frequency and
percentage of responses. Demographic influences of recruitment method, age,
number of children, educational attainment and experience in the health industry
were explored using ANOVA and Tukey post hoc tests, t-test and chi-square tests as
appropriate. Interestingly no correlations between age and dependent variables were
discovered.
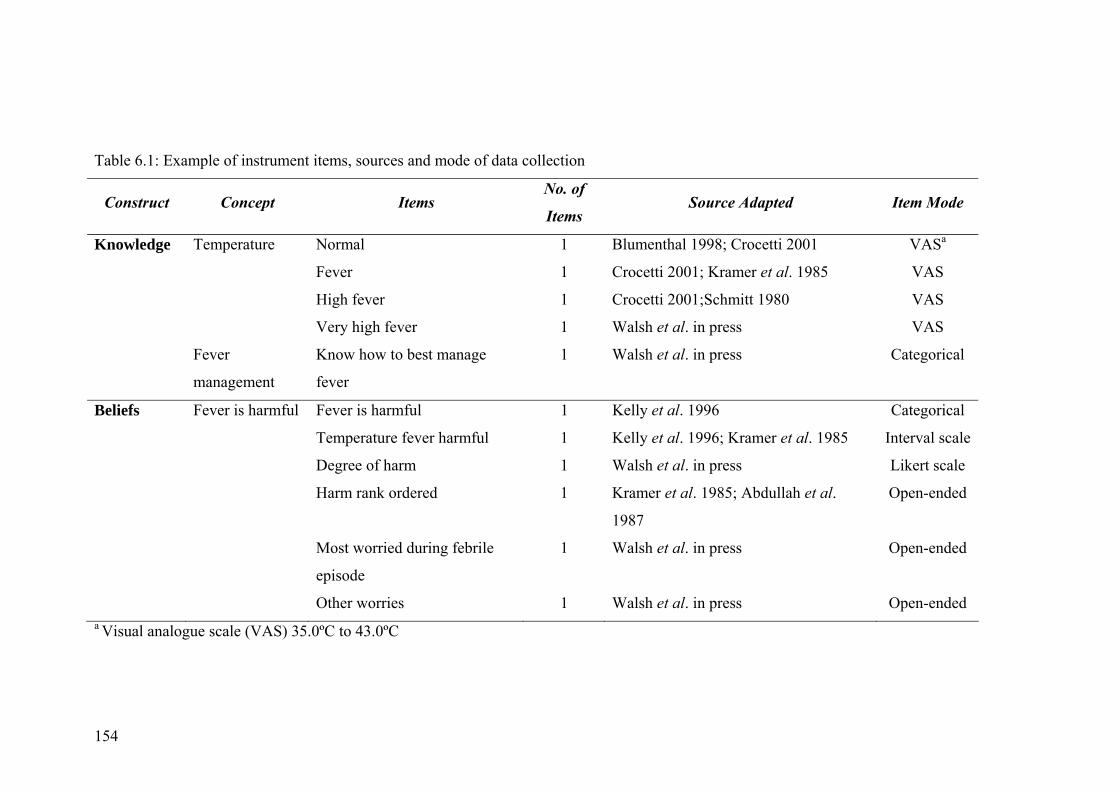
154
Table 6.1: Example of instrument items, sources and mode of data collection
Construct Concept Items No. of
Items Source Adapted Item Mode
Knowledge Temperature Normal 1 Blumenthal 1998; Crocetti 2001 VASa
Fever 1 Crocetti 2001; Kramer et al. 1985 VAS
High fever 1 Crocetti 2001;Schmitt 1980 VAS
Very high fever 1 Walsh et al. in press VAS
Fever
management
Know how to best manage
fever
1 Walsh et al. in press Categorical
Beliefs Fever is harmful Fever is harmful 1 Kelly et al. 1996 Categorical
Temperature fever harmful 1 Kelly et al. 1996; Kramer et al. 1985 Interval scale
Degree of harm 1 Walsh et al. in press Likert scale
Harm rank ordered 1 Kramer et al. 1985; Abdullah et al.
1987
Open-ended
Most worried during febrile
episode
1 Walsh et al. in press Open-ended
Other worries 1 Walsh et al. in press Open-ended a Visual analogue scale (VAS) 35.0ºC to 43.0ºC
155
Parent Fever Management Scale Development (PFM) The eight items developed to evaluate parents’ fever management, measured on 5-
point Likert scales, were recoded prior to analysis to ensure a higher score indicated
a more frequent practice (1 = never, 3 = sometimes, 5 = always). Factor analysis
using principal component extraction was conducted. Subject to item ratio was 1:50.
Following examination of the scree plot, prior conceptual beliefs and the underlying
dimension of parents’ fever management practices (Green & Salkind, 2005) a one
factor solution with an eigenvalue of 2.615 was selected. One item “When my child
has a fever I generally make sure they have plenty to drink” with correlations less
than 0.17 across all items and communality extraction of 0.52 was removed. The
analysis was rerun and varimax rotation performed. A more meaningful pattern was
found in the non-rotated version (KMO=0.61, Bartlett’s Specificity Approximate Chi
Square 1162.642, df 28, p<0.01) which explained 36.9% of the variance. The scale,
with a Cronbach’s Alpha of 0.70, was named Parent Fever Management scale
(PFM). Alpha levels of 0.70 are acceptable for a new instrument (Nolan & Mock
2000). Means, standard deviations and total PFM scores, calculated by summation of
each individual’s score for the set of items, were explored. Table 6.2 reports the
items included in the PFM scale. Test-retest reliability by Bland Altman analysis
confirmed scale items were reliable as scores were within the limits of agreement
(mean difference ± 2SD). See Table 6.2 for items in the PFM scale.
6.1.3 Results Respondents were aged between 20 and 52 years (mean 34.58, SD 4.83), female
(97.5%), in a married or defacto relationship (93.5%) and a child who had had at
least one fever (99.7%). Forty-one (10.2%) had a child who had had a febrile
convulsion; nine a child with epilepsy (2.2%). Most had a university education; two
or more children, were born in Australia and lived in a major city. See Table 6.3 for
156
additional demographic information. There were no significant differences between
recruitment methods in age, educational achievement or employment status. Those
recruited through advertising were less likely to come from a major city
(χ2[396]=44.97,p<0.01) and had fewer children (F[2,395]=4.380,p=0.01).
6.1.3.1 Knowledge Temperatures reported to represent normal temperature ranged from 35.2ºC to
38.7ºC (mean 36.8ºC, SD 0.5ºC) with 96.4% of the sample reporting between 36.0ºC
and 38.0ºC as normal. Temperatures representing ‘fever’ ranged from 36.7ºC to
40.5ºC (mean 38.2ºC, SD 0.6ºC). One third (33.3%) reported between 38.1ºC and
39.0ºC indicated fever and 56.3% reported 38.0ºC or lower. Reports of ‘high fever’
ranged from 37.5ºC to 42.6ºC (mean 39.4ºC, SD 0.8ºC); 38.4% reported between
39.1ºC and 40.0ºC and 47% identified 39.0ºC or lower. ‘Very high fever’ was
reported to range from 38.0ºC to 43.0ºC (mean 40.3ºC, SD 1.0ºC); 43.4% of the
sample reported 40.1ºC and above. See Table 6.4 for more detail.
Educational attainment and experience in the health industry influenced knowledge.
Specifically, educational attainment made significant differences to reports of high
(F[3,393]=3.243, p=.02) and very high fever (F[3,394]=4.062, p=.01). Parents with a
degree or higher degree reported lower temperatures for high (p=.06 and p=.02
respectively) and very high fever (p=.03 and p=.01 respectively) than those with
secondary education. Parents with health industry experience reported lower
temperatures representing fever (t(389)=3.260, p=.01) high (t(391)=2.233, p=.03) and
very high fever (t(392) = 2.496, p = .01) than parents without this experience. See
Table 6.5.
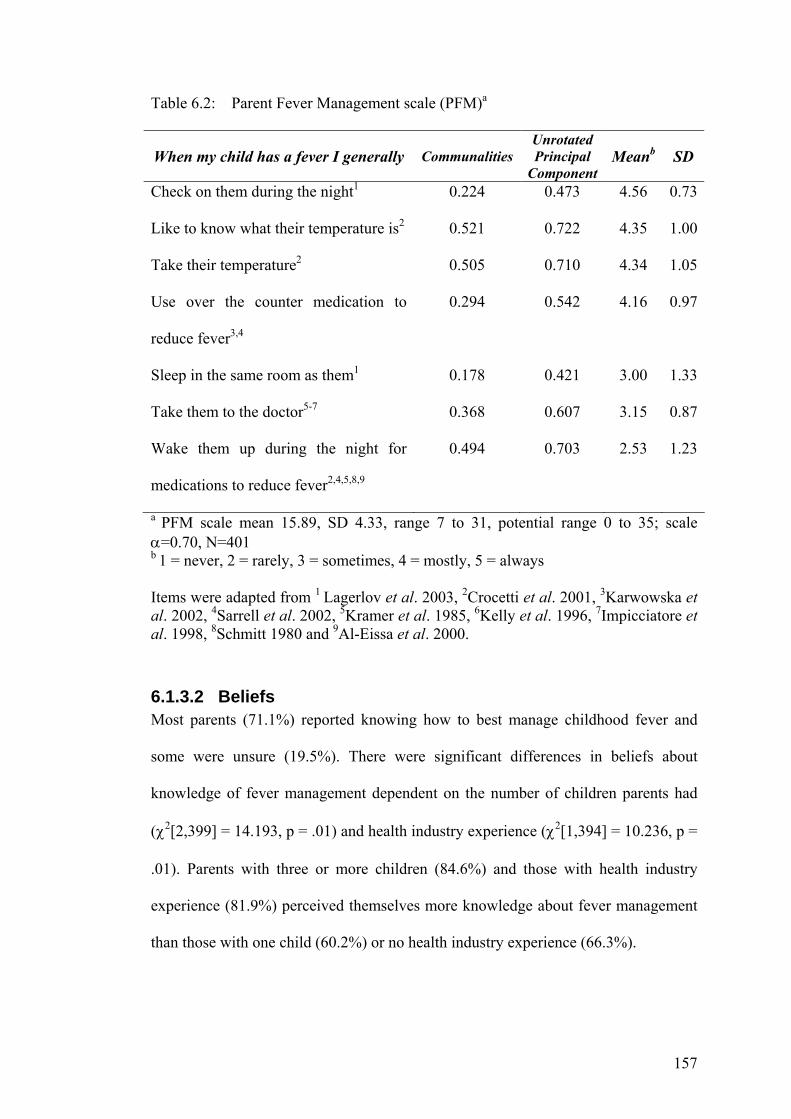
157
Table 6.2: Parent Fever Management scale (PFM)a
When my child has a fever I generally CommunalitiesUnrotated Principal
Component Meanb SD
Check on them during the night1 0.224 0.473 4.56 0.73
Like to know what their temperature is2 0.521 0.722 4.35 1.00
Take their temperature2 0.505 0.710 4.34 1.05
Use over the counter medication to
reduce fever3,4
0.294 0.542 4.16 0.97
Sleep in the same room as them1 0.178 0.421 3.00 1.33
Take them to the doctor5-7 0.368 0.607 3.15 0.87
Wake them up during the night for
medications to reduce fever2,4,5,8,9
0.494 0.703 2.53 1.23
a PFM scale mean 15.89, SD 4.33, range 7 to 31, potential range 0 to 35; scale α=0.70, N=401 b 1 = never, 2 = rarely, 3 = sometimes, 4 = mostly, 5 = always Items were adapted from 1 Lagerlov et al. 2003, 2Crocetti et al. 2001, 3Karwowska et al. 2002, 4Sarrell et al. 2002, 5Kramer et al. 1985, 6Kelly et al. 1996, 7Impicciatore et al. 1998, 8Schmitt 1980 and 9Al-Eissa et al. 2000.
6.1.3.2 Beliefs Most parents (71.1%) reported knowing how to best manage childhood fever and
some were unsure (19.5%). There were significant differences in beliefs about
knowledge of fever management dependent on the number of children parents had
(χ2[2,399] = 14.193, p = .01) and health industry experience (χ2[1,394] = 10.236, p =
.01). Parents with three or more children (84.6%) and those with health industry
experience (81.9%) perceived themselves more knowledge about fever management
than those with one child (60.2%) or no health industry experience (66.3%).
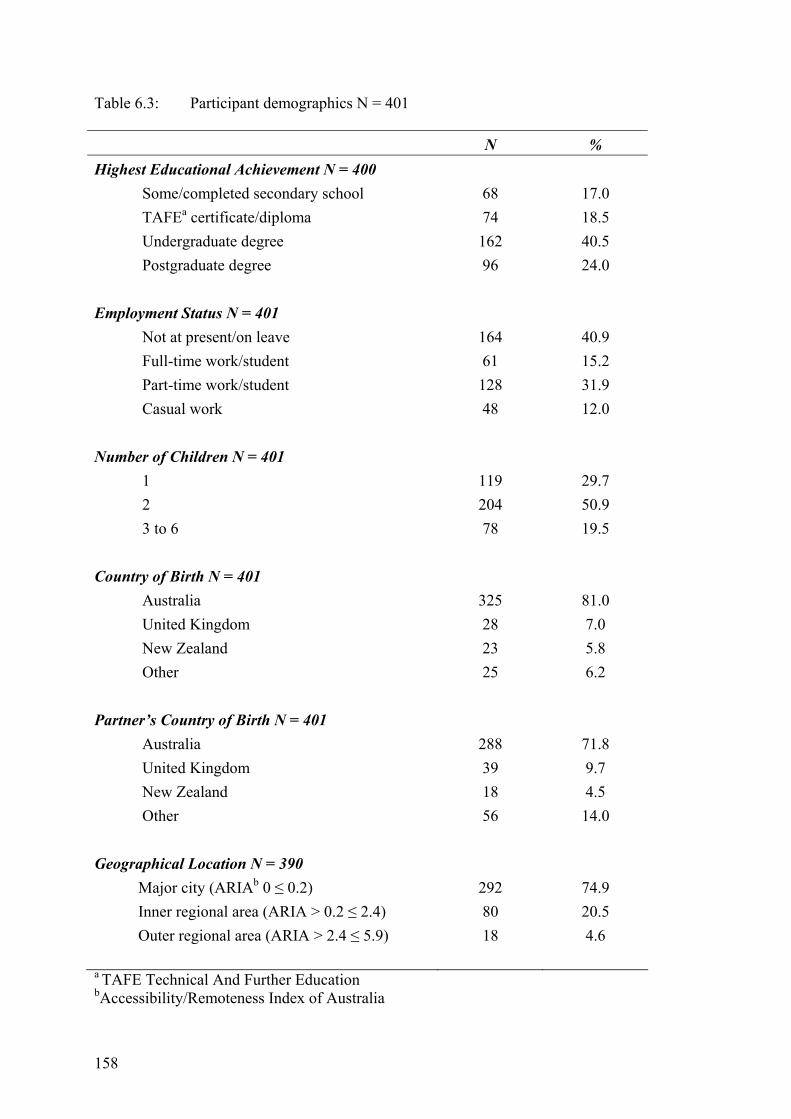
158
Table 6.3: Participant demographics N = 401
N % Highest Educational Achievement N = 400
Some/completed secondary school TAFEa certificate/diploma Undergraduate degree Postgraduate degree
68 74 162 96
17.0 18.5 40.5 24.0
Employment Status N = 401
Not at present/on leave Full-time work/student Part-time work/student Casual work
164 61 128 48
40.9 15.2 31.9 12.0
Number of Children N = 401 1 2 3 to 6
119 204 78
29.7 50.9 19.5
Country of Birth N = 401 Australia United Kingdom New Zealand Other
325 28 23 25
81.0 7.0 5.8 6.2
Partner’s Country of Birth N = 401 Australia United Kingdom New Zealand Other
288 39 18 56
71.8 9.7 4.5 14.0
Geographical Location N = 390 Major city (ARIAb 0 ≤ 0.2) Inner regional area (ARIA > 0.2 ≤ 2.4) Outer regional area (ARIA > 2.4 ≤ 5.9)
292 80 18
74.9 20.5 4.6
a TAFE Technical And Further Education bAccessibility/Remoteness Index of Australia
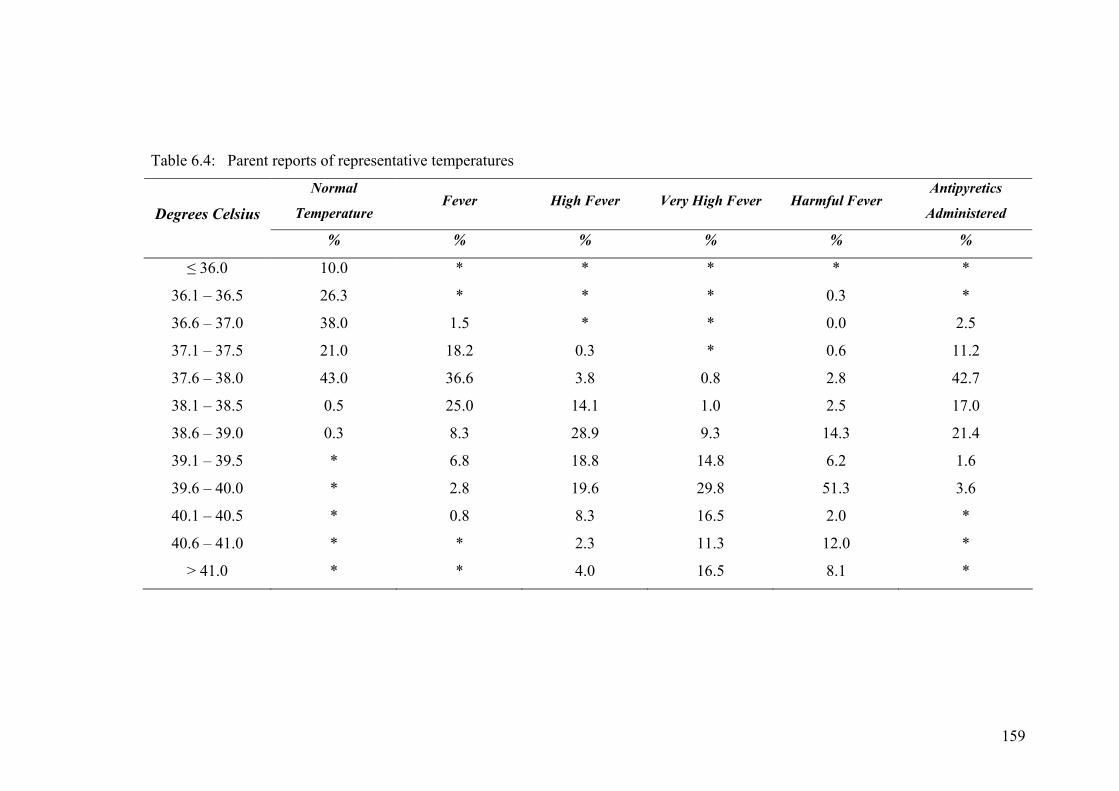
159
Table 6.4: Parent reports of representative temperatures
Normal
Temperature Fever High Fever Very High Fever Harmful Fever
Antipyretics
Administered Degrees Celsius % % % % % %
≤ 36.0 10.0 * * * * *
36.1 – 36.5 26.3 * * * 0.3 *
36.6 – 37.0 38.0 1.5 * * 0.0 2.5
37.1 – 37.5 21.0 18.2 0.3 * 0.6 11.2
37.6 – 38.0 43.0 36.6 3.8 0.8 2.8 42.7
38.1 – 38.5 0.5 25.0 14.1 1.0 2.5 17.0
38.6 – 39.0 0.3 8.3 28.9 9.3 14.3 21.4
39.1 – 39.5 * 6.8 18.8 14.8 6.2 1.6
39.6 – 40.0 * 2.8 19.6 29.8 51.3 3.6
40.1 – 40.5 * 0.8 8.3 16.5 2.0 *
40.6 – 41.0 * * 2.3 11.3 12.0 *
> 41.0 * * 4.0 16.5 8.1 *
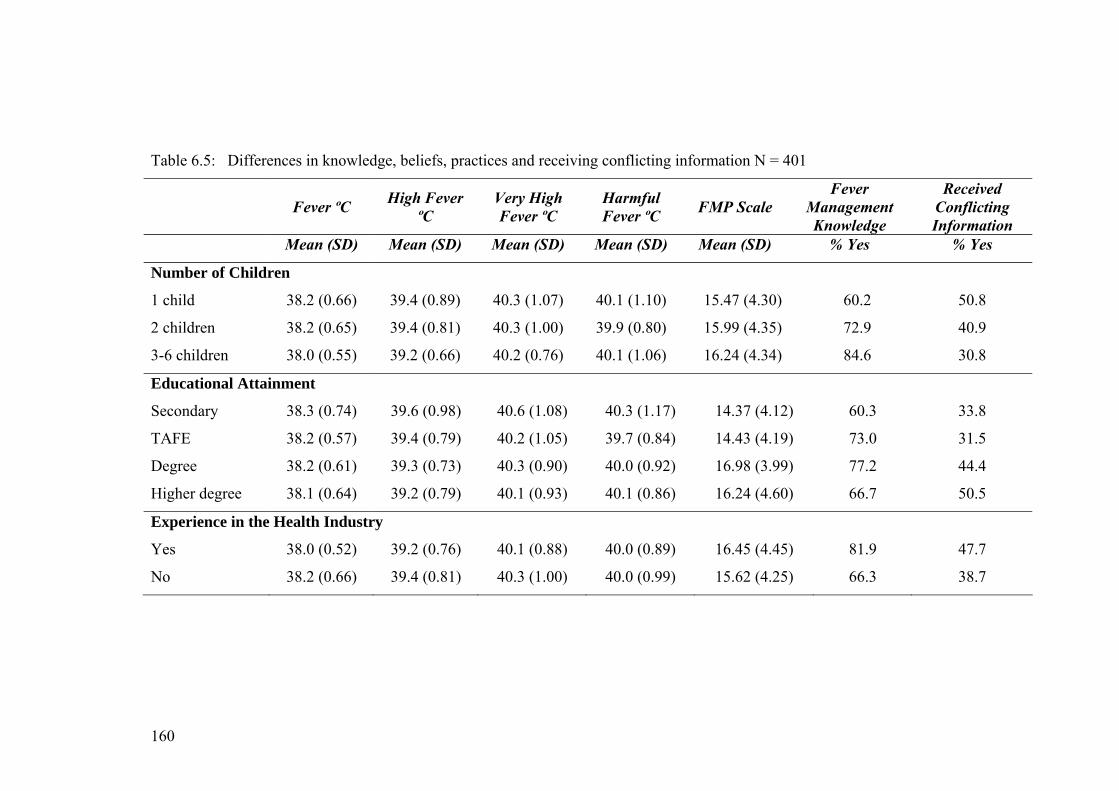
160
Table 6.5: Differences in knowledge, beliefs, practices and receiving conflicting information N = 401
Fever ºC High Fever ºC
Very High Fever ºC
Harmful Fever ºC FMP Scale
Fever Management Knowledge
Received Conflicting Information
Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD) % Yes % Yes
Number of Children
1 child
2 children
3-6 children
38.2 (0.66)
38.2 (0.65)
38.0 (0.55)
39.4 (0.89)
39.4 (0.81)
39.2 (0.66)
40.3 (1.07)
40.3 (1.00)
40.2 (0.76)
40.1 (1.10)
39.9 (0.80)
40.1 (1.06)
15.47 (4.30)
15.99 (4.35)
16.24 (4.34)
60.2
72.9
84.6
50.8
40.9
30.8
Educational Attainment
Secondary
TAFE
Degree
Higher degree
38.3 (0.74)
38.2 (0.57)
38.2 (0.61)
38.1 (0.64)
39.6 (0.98)
39.4 (0.79)
39.3 (0.73)
39.2 (0.79)
40.6 (1.08)
40.2 (1.05)
40.3 (0.90)
40.1 (0.93)
40.3 (1.17)
39.7 (0.84)
40.0 (0.92)
40.1 (0.86)
14.37 (4.12)
14.43 (4.19)
16.98 (3.99)
16.24 (4.60)
60.3
73.0
77.2
66.7
33.8
31.5
44.4
50.5
Experience in the Health Industry
Yes
No
38.0 (0.52)
38.2 (0.66)
39.2 (0.76)
39.4 (0.81)
40.1 (0.88)
40.3 (1.00)
40.0 (0.89)
40.0 (0.99)
16.45 (4.45)
15.62 (4.25)
81.9
66.3
47.7
38.7
161
Parents were asked if fever could be harmful, at what temperature, how harmful
these fevers could be and the harm that fevers at this temperature could cause. Most
parents (88.8%) believed fever could be harmful, few believed it was not harmful
(2.5%). Educational attainment influenced perceptions of the temperature that could
cause harm (F[3,352] = 5.266, p = .01). Parents with secondary education reported a
higher temperature than those TAFE (p = .01) or a degree (p = .05). See Table 6.5.
Temperatures considered harmful ranged from 36.5ºC to 43.0ºC (mean 40.0ºC, SD
1.0ºC). This was explored to determine how harmful this temperature could be and
the outcomes that could occur at the harmful temperature. Of the 87.6% who
reported a temperature that could be harmful 59.2% reported this very or reasonably
harmful. It is important to note that 14.4% of parents believed temperatures of 39.0ºC
and lower could be harmful to very harmful; 50.3% reported this for temperatures of
40.0ºC or lower. See Table 6.6 for reports of harmful fevers. Specific harmful
outcomes at the identified harmful temperature were reported in rank order (1-3; 1 =
the most harm) by 91.8%. Febrile convulsions, brain damage, and dehydration, an
indication of serious/fatal illnesses and loss of consciousness were most frequently
reported. Table 6.6 presents parents’ reports the degree of harm from harmful
temperatures and harmful events that could occur at the temperature considered
harmful.
During febrile episodes parents (N=394) were most concerned about febrile
convulsions (35.0%) and the underlying cause of the fever (20.1%). In addition to
their main concern parents (N=705, multiple responses) were also concerned about
the cause of the fever (29.7%), serious/fatal illnesses (23.2%), their child’s well-
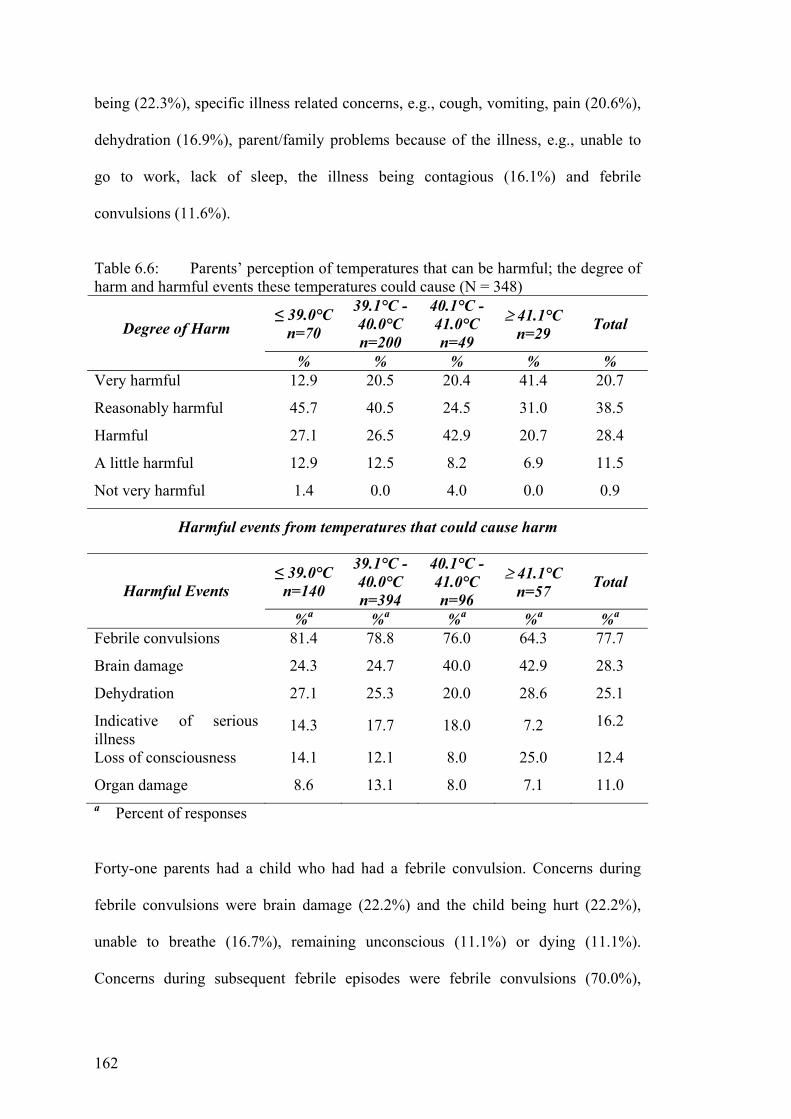
162
being (22.3%), specific illness related concerns, e.g., cough, vomiting, pain (20.6%),
dehydration (16.9%), parent/family problems because of the illness, e.g., unable to
go to work, lack of sleep, the illness being contagious (16.1%) and febrile
convulsions (11.6%).
Table 6.6: Parents’ perception of temperatures that can be harmful; the degree of harm and harmful events these temperatures could cause (N = 348)
≤ 39.0°C n=70
39.1°C - 40.0°C n=200
40.1°C - 41.0°C n=49
≥ 41.1°C n=29 Total Degree of Harm
% % % % % Very harmful 12.9 20.5 20.4 41.4 20.7
Reasonably harmful 45.7 40.5 24.5 31.0 38.5
Harmful 27.1 26.5 42.9 20.7 28.4
A little harmful 12.9 12.5 8.2 6.9 11.5
Not very harmful 1.4 0.0 4.0 0.0 0.9
Harmful events from temperatures that could cause harm
≤ 39.0°C n=140
39.1°C - 40.0°C n=394
40.1°C - 41.0°C n=96
≥ 41.1°C n=57 Total
Harmful Events
%a %a %a %a %a
Febrile convulsions 81.4 78.8 76.0 64.3 77.7
Brain damage 24.3 24.7 40.0 42.9 28.3
Dehydration 27.1 25.3 20.0 28.6 25.1
Indicative of serious illness
14.3 17.7 18.0 7.2 16.2
Loss of consciousness 14.1 12.1 8.0 25.0 12.4
Organ damage 8.6 13.1 8.0 7.1 11.0 a Percent of responses
Forty-one parents had a child who had had a febrile convulsion. Concerns during
febrile convulsions were brain damage (22.2%) and the child being hurt (22.2%),
unable to breathe (16.7%), remaining unconscious (11.1%) or dying (11.1%).
Concerns during subsequent febrile episodes were febrile convulsions (70.0%),
163
temperature reduction (25.0%), the underlying cause (25.0%) and brain damage
(10.0%).
6.1.3.3 Practices Fever management practices were explored qualitatively to explore the most salient
practices, and were reported by 400 parents. Most frequent practices reported were
administering antipyretics (87.8%), temperature monitoring (52.5%), offering fluids
(49.0%) and dressing the child in light clothing (43.8%). Some comforted distressed
children (38.8%), ensured the child was comfortable, for example, lying on a sofa
(27.3%), used tepid (23.8%) or cool sponging/bathing (14.0%). Only 14% sought
medical advice. When fever was considered ‘very high’ additional practices were
reported by 46.9%. These included seeking medical advice (63.7%), using
antipyretics (35.2%), tepid or cool sponging/bathing (15.0% and 8.8% respectively).
Ninety-two percent of parents (N=365) reported ‘usually’ using antipyretics to
reduce fevers ranging from 37.0ºC to 40.0ºC (mean 38.3ºC, SD 0.6). Of these 57.3%
used antipyretics for temperatures below 38.5ºC and 17.1% below 38.0ºC. More than
half 51.8% had alternated antipyretics. Of these 39.8% sometimes, 11.7% mostly and
0.5% always alternated antipyretics. Influences on alternating antipyretics were
advice from a doctor or at a hospital (49.5%), child febrile post-antipyretic (41.7%)
and therapeutic qualities of the different antipyretics (21.6%). Medication use and
influences on use are reported in detail elsewhere (Walsh et al. 2007b).
The literature reports parents’ overuse of medical services for febrile children.
Parents’ (N=398) decisions to seek medical advice were influenced by specific
illness symptoms such as pain or a cough (49.7%), persistent fever (41.5%), high

164
fever (37.4%) and general unwellness, deterioration or lethargy (34.7%). Other
influences were an inability to reduce the fever or fever recurring post antipyretic
(29.4%), a need for advice or reassurance (20.4%).
Our earlier study identified practices do change over time and with subsequent
children (Walsh & Edwards 2007). In this study one third (39.4%) of parents
reported practice changes over time, some changes were positive or evidence-based,
others negative or phobic. Positive changes reflected reduced concern about fever
(36.4%), delaying or rarely using medications (34.4%) and delaying seeking medical
advice (19.5%). Of concern is that 22.7% reported increased antipyretic use which
included alternating antipyretics and a double dose of antipyretics.
6.1.3.4 Parent Fever Management Scale (PFM) Responses to items on the PFM scale confirm parents’ qualitative reports above
(refer to Table 6.2). Parents usually take the child’s temperature, use antipyretics to
reduce fever and sometimes take febrile children to the doctor. These include usually
checking on febrile children at night, sometimes sleeping in the same room and
waking febrile children for an antipyretic during the night. Total scale scores ranged
from 7 to 31 (potential range 7 – 35); mean 15.89 (SD 4.33). Mean score above the
median indicates a febrile child places a moderate burden on parents. Those with a
university education reported greater burden (F[3,399]=172.449, p ≤.001) than those
with secondary (degree, p ≤ 0.001; higher degree p = .03) or TAFE education (degree
p ≤ 0.001; higher degree p = .03 (see Table 65). There is scope for this scale to be
further developed as a useful tool to determine the burden of childhood fever places
on parents.
165
6.1.3.5 How Parents Learnt to Manage Fever Parents learnt to manage fever from multiple sources. Most frequently reported were
doctors (60.9%), personal experience or trial and error learning (39.1%), childcare
books and magazines (26.0%), peers, other mothers and friends (24.0%) and their
own mothers (22.5%). Fever management was also learnt from nurses (19.2%),
personal professional knowledge (12.1%) and other family members (12.9%). Some
actively researched fever management (12.1%); others learnt from pharmacists
(7.3%) and a few learnt about fever from alternative therapists (2.3%) and medical
help lines (1.3%).
Nearly half the parents (41.9%) had received conflicting information about managing
fever. For example, always reduce fever versus fever is good for the body, regular
antipyretics versus as required and do not alternate antipyretics versus alternate
antipyretics. Some received different advice from general practitioners and paediatric
emergency departments. Receiving conflicting information created feelings of
uncertainty and confusion (77.1%), anger and frustration (16.6%) and concern about
best management (14.6%). Some parents continued to make their own decisions
(17.8%) or sought further information from an expert such as a paediatrician,
pharmacist or general practitioner (7.6%). A number of demographic variables were
associated with receiving conflicting information; recruitment method
(χ2[2,N=396]=7.104, p=.03), number of children (χ2[2,399]=7.938, p=.02) and
educational attainment (χ[3,398]=8.401, p=.04). Parents recruited face-to-face were
least likely to report receiving conflicting information (32.1%) compared with
advertising (47.9%) and snowball methods (40.8%). Those with one child; TAFE or
degree education were more likely to report receiving conflicting information. See
Table 6.5.
166
6.1.4 Discussion This study identified Australian parents’ knowledge, beliefs and practices in
childhood fever management. Parents, perceiving they are knowledgeable, reported
normal temperatures indicated fever, believed moderate fever harmful causing febrile
convulsions and usually reduced normal temperatures and mild fevers with
antipyretics. Usual fever management practices, checking and medicating febrile
children throughout the night, place an additional burden on parents. Fever
management was learnt from numerous sources including doctors as well as trial and
error, peers and own mothers; receiving conflicting information from these varied
sources is not surprising. Caring for a febrile child is worrying; the additional
disruptions to parents’ life during this time and attempting to determine best practice
contribute to making this an even more daunting experience. Health professionals
have a responsibility to ensure parents not only know how to best care for febrile
children but also receive the necessary and timely support and reassurance.
6.1.4.1 Knowledge In this community-based study parents identified a wide range of temperatures
representative of normal, fever, high and very high fever. Interestingly the mean
temperature for fever, 38.2ºC and high fever, 39.4ºC reported were higher than those
reported by parents in other studies recruited from health care facilities or schools,
37.6ºC to 38.0ºC and 37.8ºC to 39.2ºC respectively (Betz & Grunfeld 2006,
Karwowska et al. 2002, Soon et al. 2003). Are Australian parents more
knowledgeable or do these findings reflect differences in perceptions when children
are well. If the latter, then educating parents when perceptions are more positive
could increase evidence-based practice. More research is needed to explore this
phenomenon.
167
6.1.4.2 Beliefs Parents in this study, similar to their international counterparts, believed fever
harmful causing febrile convulsions, brain damage and dehydration (Al-Eissa et al.
2000a, Betz & Grunfeld 2006, Crocetti et al. 2001, Karwowska et al. 2002) with
febrile convulsions their main concern. Parents of today are more concerned about
febrile convulsions than previously reported (Crocetti et al. 2001, Karwowska et al.
2002). These convulsions are rare occurring in less than 5% of children under the age
of five years (Kira et al. 2005, Vestergaard et al. 2002). Parent education has been
found effective in reducing concerns in parents of children who have had a febrile
convulsion (Huang et al. 2001, Wassmer & Hanlon 1999). Education about the
prevalence and predictors of febrile convulsions and safely caring for a child during a
febrile convulsion is necessary and may contribute to reducing fever phobia and
unnecessary fever reduction.
6.1.4.3 Practices The most common practices reported, antipyretics and temperature monitoring,
indicate parents’ focus on the need to reduce fever. Less than half the parents
reported practices supported by the literature, encouraging fluids, dressing in light
clothing and reducing activity (Connell 1997, Schmitt 1994, Watts et al. 2003).
Decisions to seek medical assistance were equally influenced by a need to reduce
temperature and specific illness related factors. These findings reflect a stronger
focus on the child’s temperature than on the child’s general well-being, indicating the
care of febrile children was motivated by fever phobia. Reports of very high and
harmful fever were similar and corroborate earlier studies reporting parents’
perception of harmful fevers, between 39.3ºC and 40.0ºC (Betz & Grunfeld 2006,
Sarrell et al. 2002). This is concerning, parents perceive moderate fever, fever with
immunological benefits to be harmful.
168
Importantly, practices did change over time for some parents. This is an important
finding specifically as positive changes indicated reduced concerns about fever and
negative changes more concern. Our pilot work found a negative experience with
childhood fever, febrile convulsion, increased concerns and antipyretic use (Walsh et
al. 2007a). Negative practice changes indicate a need for parents who have had
negative experiences to receive advice and reassurance from health professionals
following these negative experiences.
Reducing fever with antipyretics was common and consistent with recent studies
(Sarrell et al, 2002). However, the number of parents who had alternated antipyretics
is disturbing; more than half had alternated, a significant increase from rates reported
in the last few years, 7% to 27% (Crocetti et al. 2001, Li et al. 2000). Is this
becoming a common practice? Warnings about the dangers of alternating, increasing
fever phobia and antipyretic overdosing, abound (Goldman 2006, Saphyakhajon &
Greene 2006, Schmitt 2006). Alternating increases the risk of incorrect dosing, more
likely with ibuprofen than paracetamol, in both dosage and frequency (Lagerlov et
al. 2003, Li et al. 2000). Recent experimental studies comparing mono and
alternating therapies report an increased reduction of approximately 1.0ºC, over a 24
hour period, with alternating therapies (Erlewyn-Lajeunesse et al. 2006, Nabulis et
al. 2006, Sarrell et al. 2006). Is the risk of increasing parents’ focus on temperature
and antipyretic overdosing warranted for a 1.0ºC temperature reduction?
6.1.4.4 Parent Fever Management Scale The development of this scale assisted in determining parents’ usual practices and
reflects their concerns. Parents wanted to know their child’s temperature, checked
them during the night, gave antipyretics during the night and sometimes slept in the
169
same room. These practices indicate phobic beliefs and place additional demands on
parents causing tiredness and risking physical exhaustion during febrile episodes.
Australian parents use paracetamol to promote children’s sleep thereby allowing
parents to sleep (Allotey et al. 2004). Fear of negative outcomes influences
antipyretic use. Understanding parents’ concerns and the impact childhood fever has
on parents is important to assist health professionals target education and provide
appropriate reassurance.
6.1.4.5 Demographic Influences Interestingly, parents’ demography had little influence on their knowledge, beliefs
and practices. Our findings related to higher educational attainment conflict with
previous reports. However, that more than half of the sample had university
education must be considered; a more heterogeneous sample could have resulted in
different findings and needs further investigation. Nevertheless, some studies do
report lower educational levels associated with increased concerns about febrile
children (Impicciatore et al. 1998) and some report no educational influence (Kramer
et al. 1985, Singhi et al. 1991). The negative influence of a higher educational level
has not been reported. That more than half the parents had a university education
could explain our findings, however, this requires further exploration.
Health industry experience, not previously explored, had the greatest negative
influence on beliefs and practices. Most parents with either health education or
experience working in a health setting reported knowing how to manage fever.
However, they reported lower temperatures for fever, high and very high fever, a
greater physical burden of care and were more likely to have received conflicting
information indicating greater concern about fever than parents without health
170
industry experience. Health professionals’ fever phobia continues to be reported
(Karwowska et al. 2002, Sarrell et al. 2002, Walsh et al. 2005) despite evidence of
the beneficial role of fever and lack of support for antipyretic use to prevent febrile
convulsions (Chang et al. 2001, Hutt et al. 1999, Lorin 1999). Do health
professionals’ negative beliefs and practices influence others in the health industry,
irrespective of position?
6.1.4.6 Practice Implications Parents concerns about managing their febrile child were evident by their quest for
information. Inaccurate information from friends and relatives is understandable and
multifactorial (Purssell 2000, Schmitt 1980). Information from health professionals is
expected to be accurate and reliable (Walsh et al. 2007a). That this is not so is
evident in reports from parents with health industry experience. Reports of some
health professionals’ concern about harmful outcomes from fever, febrile
convulsions, persist (Karwowska et al, 2002, Sarrell et al. 2002, Walsh et al. 2005).
Information from phobic health professionals and those practicing in line with the
latest scientific evidence will be incongruent, increasing parental concern.
Additionally, more parents in this study reported learning to manage fever by
experience than previously, 39% versus 14% (Crocetti et al. 2001).
Health professionals must update their knowledge and recommend practices in
accordance with the latest scientific evidence. It is imperative all health professionals
provide evidence-based information not only to parents but also to peers and
colleagues. Childhood fever, a frightening experience for parents, is inevitable.
Health professionals have a responsibility to assist parents care safely for febrile
children without undue demands on parents’ own health. The development and use

171
of guidelines for evidence-based fever management and dissemination through
reliable sources is essential. Scientifically based advice, for parents, on how to care
for a febrile child and when to seek medical advice has been available since 1984
(Schmitt 1984, El-Radhi & Carroll 1994) and must be distributed by health
professionals to parents.
6.1.4.7 Strengths and Limitations This large, comprehensive, community-based study of parents’ fever management
highlights the need for evidence-based education of not only parents but also the
health professionals from whom parents reported learning to manage fever (80%).
Care must be taken in generalisation of these findings as the sample was self-
selected, most had university education and lived in major cities and data were
collected by self-report. Findings were not influenced by recruitment method but
were by educational attainment.
6.1.5 Conclusions and Recommendations Fever management remains a challenging time for parents of young children. Their
knowledge is inaccurate and incorrect beliefs about fever being harmful strongly
influence practices with alternating antipyretics to reduce fever becoming a common
practice. Parents with higher education or health industry experience reported greater
concern. There is an urgent need to ensure health professionals’ knowledge is in line
with the latest scientific evidence; parents receiving inconsistent information from
health professionals is unacceptable. Additionally, the development of fever
management guidelines and evidence-based education programs and literature and
consistent use of these tools with all parents of young children is recommended.
172
Further research is needed to determine whether parents’ perceptions about fever
differ when their child is well and febrile, the influences on practice change over
time, the influence of education about febrile convulsions prevalence, predictors and
management of febrile convulsions and the development of fever management
guidelines and their influence on parents’ practices,
6.1.6 Acknowledgements The authors would like to thank the expert panel and parents who gave their valuable
time to participate. This study was supported in part by the Joyce Wickham
Scholarship awarded by the Royal College of Nursing Australia.
6.1.7 References Alander, S. W., Dowd, M. D., Bratton, S. L., & Kearns, G. L. (2000). Pediatric
acetaminophen overdose - Risk factors associated with hepatocellular injury. Archives of Pediatrics & Adolescent Medicine, 154(4), 346-350.
Al-Eissa, Y. A., Al-Sanie, A. M., Al-Alola, S. A., Al-Shaalan, M. A., Ghazal, S. S.,
Al-Harbi, A. H., et al. (2000a). Parental perceptions of fever in children. Annals of Saudi Medicine, 20(3-4), 202-205.
Al-Eissa, Y. A., Al-Zamil, F. A., Al-Sanie, A. M., Al-Salloum, A. A., Al-Tuwaijri,
H. M., Al-Abdali, N. M., et al. (2000b). Home management of fever in children: rational or ritual? International Journal of Clinical Practice, 54(3), 138-142.
Allotey, P., Reidpath, D. D., & Elsisha, D. (2004). "Social medication" and the
control of children: a qualitative study of over-the-counter medication among Australian children. Pediatrics, 114(3), e378-e383.
Betz, C. L., & Grunfeld, A. F. (2006). Fever phobia in the emergency department: a
survey of children's caregivers. European Journal of Emergency Medicine, 13(3), 129-133.
Bland, M. J., & Altman, D. G. (1986). Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet, i, 307-310. Blatteis, C. M. (2003). Fever: pathological or physiological, injurious or beneficial?
Journal of Thermal Biology, 28(1), 1-13. Blatteis, C. M., Sehic, E., & Li, S. (1998). Afferent pathways of pyrogen signaling.
Annals of the New York Academy of Sciences, 856(1), 95-107.
173
Blumenthal, I. (1998). What parents think of fever. Family Practice, 15(6), 513-518. Chamberlain, J. M., Terndrup, T. E., & Alexander, D. T. (1995). Determination of
normal ear temperature with an infrared emission detection thermometer. Annals of Emergency Medicine, 25, 15.
Chang, Y. C., Guo, N. W., Wang, S. T., Huang, C. C., & Tsai, J. J. (2001). Working
memory of school-aged children with a history of febrile convulsions: a population study. Neurology, 57(1), 37-42.
Chien, C., Marriott, J., Ashby, K., & Ozanne-Smith, J. (2003). Unintentional
ingestion of over the counter medications in children less than 5 years old doi:10.1046/j.1440-1754.2003.00148.x. Journal of Paediatrics and Child Health, 39(4), 264-269.
Connell, F. (1997). The causes and treatment of fever: a literature review. Nursing
Standard, 12(11), 40-43. Crocetti, M., Moghbeli, N., & Serwint, J. (2001). Fever phobia revisited: have
parental misconceptions about fever changed in 20 years? Pediatrics, 107(8), 1241-1246.
El-Radhi, A. S., & Carrol, J. (1994). Fever in pediatric practice. Oxford: Blackwell
Science. Erlewyn-Lajeunesse, M. D. S., Coppens, K., Hunt, L. P., Chinnick, P. J., Davies, P.,
Higginson, I. M., et al. (2006). Randomised controlled trial of combined paracetamol and ibuprofen. Archives of Disease in Childhood, 91, 414-416.
Goldman, R. D. (2006). Alternating ibuprofen and acetaminophen may be more
effective in the treatment of fever in children. The Journal of Pediatrics, 149(1), 140-141.
Goldman, R. D., & Scolnik, D. (2004). Underdosing of acetaminophen by parents
and emergency utilization. Pediatric Emergency Care, 20(2), 89-93. Green, S. B., & Salkind, N. J. (2005). Using SPSS for Windows ad Mackintosh:
analysing and understanding data (4th ed.). Upper Saddle River, New Jersey: Pearson Education.
Herzog, L. W., & Coyne, L. J. (1993). What Is Fever - Normal Temperature in
Infants Less Than 3 Months Old. Clinical Pediatrics, 32(3), 142-146. Holtzclaw, B. J. (1992). The febrile response in critical care: state of the science.
Heart & Lung, 21(5), 482 - 501. Huang, M. C., Liu, C. C., Chi, Y. C., Huang, C. C., & Cain, K. (2001). Parental
concerns for the child with febrile convulsion: long-term effects of educational interventions. Acta Neurologica Scandinavica, 103(5), 288-293.
174
Hutt, M. J., Trueman, M., & Hutt, S. J. (1999). Parental perceptions of pre-adolescent children who have experienced a febrile convulsion: effects of social class and gender. British Journal of Clinical Psychology, 38(Pt 1), 59-72.
Impicciatore, P., Nannini, S., Pandolfini, C., & Bonati, M. (1998). Mothers'
knowledge of, attitudes toward, and management of fever in preschool children in Italy. Preventive Medicine, 27(2), 268-273.
Impicciatore, P., Violante, A., & Bonati, M. (1997). Helping parents to cope when
their preschool children are acutely ill. British Medical Journal, 314, 373. Karwowska, A., Nijssen-Jordan, C., Johnson, D., & Davies, H. (2002). Parental and
health care provider understanding of childhood fever: a Canadian perspective. Canadian Journal of Emergency Medicine, 4(6), 394-400.
Kilmon, C. (1987). Parents' knowledge and practices related to fever management.
Journal of Pediatric Health Care, 1(4), 173-179. Kira, R., Torisu, H., Takemoto, M., Nomura, A., Sakai, Y., Sanefuji, M., et al.
(2005). Genetic susceptibility to simple febrile seizures: Interleukin-1[beta] promoter polymorphisms are associated with sporadic cases. Neuroscience Letters, 384(3), 239-244.
Klein, N. C., & Cunha, B. A. (1996). Treatment of fever. Infectious Disease Clinics
of North America, 10(1), 211-216. Kluger, M. (1986). Is fever beneficial. The Yale Journal of Biology and Medicine,
59(2), 89-95. Kluger, M. J. (1979). Phylogeny of fever. Federation Proceedings, 38(1), 30-34. Kolfen, W., Pehle, K., & Konig, S. (1998). Is the long-term outcome of children
following febrile convulsions favorable? Developmental Medicine & Child Neurology, 40(10), 667-671.
Kozer, E., Barr, J., Bulkowestein, M., Avgil, M., Greenberg, R., Matias, A., et al.
(2002). A prospective study of multiple supratherapeutic acetaminophen doses in febrile children. Veterinary and Human Toxicology, 44(2), 106-109.
Kramer, M. S., Naimark, L. E., & Leduc, D. G. (1985). Parental fever phobia and its
correlates. Pediatrics, 75(6), 1110-1113. Lagerlov, P., Helseth, S., & Holager, T. (2003). Childhood illnesses and the use of
paracetamol (acetaminophen): a qualitative study of parents' management of common childhood illnesses. Family Practice, 20(6), 717-723.
Li, S. F., Lacher, B., & Crain, E. F. (2000). Acetaminophen and ibuprofen dosing by
parents. Pediatric Emergency Care, 16(6), 394-397.
175
Linder, N., Sirota, L., Snapir, A., Eisen, I., Davidovitch, N., Kaplan, G., et al. (1999). Parental knowledge of the treatment of fever in children. Israel Medical Association Journal: IMAJ, 1(3), 158-160.
Lorin, M. I. (1999). Pathogenesis of fever and its treatment. In J. B. McMillan, C.
DeAngelis, R. D. Feigin & J. B. Warshaw (Eds.), Oski's Pediatrics: principles and practices (3rd ed., pp. 848-850). Philadelphia: Lippincott, Williams & Wilkins.
Lwanga, S. K., & Lemeshow, S. (1991). Sample size determination in health studies.
Geneva: World Health Organization. Mackowiak, P. A. (1998). Concepts of fever. Archives of Internal Medicine, 158(17),
1870-1882. Mackowiak, P. A., & Boulant, J. A. (1996). Fever's glass ceiling. Clinical Infectious
Diseases, 22(3), 525-536. McErlean, M. A., Bartfield, J. M., Kennedy, D. A., Gilman, E. A., Stram, R. L., &
Raccio-Robak, N. (2001). Home antipyretic use in children brought to the emergency department. Pediatric Emergency Care, 17(4), 249-251.
Nabulis, M. N., Tamin, H., Mahfoud, Z., Itani, M., Sabra, R., Chamseddine, F., et al.
(2006). Alternating ibuprofen and acetaminophen in the treatment of febrile children: a pilot study. BMC Medicine.
Nolan, M. T., & Mock, V. (2000). Measuring patient outcomes. Thousand Oaks:
Sage Publications. Polit, D. F., & Hungler, B. P. (1999). Nursing research: principles and methods.
New York: Lippincott. Porter, R. S., & Wenger, F. G. (2000). Diagnosis and treatment of pediatric fever by
caretakers. Journal of Emergency Medicine, 19(1), 1-4. Principi, N., Esposito, S., Gasparini, R., Marchisio, P., & Crovari, P. (2004). Burden
of influenza in healthy children and their households. Archives of Disease in Childhood, 89(11), 1002-1007.
Purssell, E. (2000). The use of antipyretic medications in the prevention of febrile
convulsions in children. Journal of Clinical Nursing, 9(4), 473-480. Saphyakhajon, P., & Greene, G. (2006). Alternating acetaminophen and ibuprofen in
children may cause parental confusion and is dangerous. Archives of Pediatric Adolescent Medicine, 160(July), 757.
Sarrell, E. M., Wielunsky, E., & Cohen, H. A. (2006). Antipyretic Treatment in
Young Children With Fever: Acetaminophen, Ibuprofen, or Both Alternating in a Randomized, Double-blind Study. Archives of Pediatrics & Adolescent Medicine, 160(2), 197.
176
Sarrell, M., Cohen, H. A., & Kahan, E. (2002). Physicians', nurses', and parents' attitudes to and knowledge about fever in early childhood. Patient Education and Counselling, 46, 61-65.
Schmitt, B. D. (1980). Fever phobia: misconceptions of parents about fevers.
American Journal of Diseases in Children, 134(2), 176-181. Schmitt, B. D. (1984). Fever in childhood. Pediatrics, 74 (Suppl), 929-936. Schmitt, B. D. (2006). Concerns Over Alternating Acetaminophen and Ibuprofen for
Fever. Archives of Pediatrics and Adolescent Medicine, 160(7), 160-757. Singhi, S., Padmini, P., & Sood, V. (1991). Urban parents' understanding of fever in
children: its danger and treatment practices. Indian Pediatrics, 28(5), 501-505.
Soon, W. S., Cheong, S. K., & Hong, C. Y. (2003). Fever phobia in a primary
healthcare setting: a Singapore perspective. Annals Academy of Medical Journal, Singapore, 32(2 Supp), S26-27.
SPSS. (1996-2003). Data Entry Builder Release 4.0.0 (Version 4.0). Chicago, IL,
US: SPSS Inc. SPSS. (2004). SPSS for Windows, Version 13.0 (Version 11.0). Chicago, IL, US:
SPSS Inc. Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.).
Boston, MA: Pearson Education Inc. Taveras, E. M., Durousseau, S., & Flores, G. (2004). Parents' beliefs and practices
regarding childhood fever - A study of a multiethnic and socioeconomically diverse sample of parents. Pediatric Emergency Care, 20(9), 579-587.
Vestergaard, M., Basso, O., Henriksen, T. B., Ostergaard, J., & Olsen, J. (2002). Risk
factors for febrile convulsions. Epidemiology, 13(3), 282-287. Walsh, A. M., Edwards, H. E., Courtney, M. D., Wilson, J. E., & Monaghan, S. J.
(2005). Fever management: paediatric nurses' knowledge, attitudes and influencing factors. Journal of Advanced Nursing, 49(5), 453-464.
Walsh, A. M., Edwards, H. E., & Fraser, J. A. (2007a). Influences on parents' fever
management: beliefs, experiences and information sources. Journal of Clinical Nursing. doi: 10.1111/j.1365-2702.2006.01890.x.
Walsh, A. M., Edwards, H. E., & Fraser, J. (2007b). Over-the-counter medication use
for childhood fever: a crossectional study of Australian parents. Journal of Paediatrics and Child Health. doi:10.1111/j.1440-1754.2007.01161.x.
Wassmer, E., & Hanlon, M. (1999). Effects of information on parental knowledge of
febrile convulsions. Seizure, 8(7), 421-423.
177
Wright, A. D., & Liebelt, E. L. (2007). Alternating antipyretics for fever reduction in children: an unfounded practice passed down to parents from paediatricians. Clinical Pediatrics, 46, 146-150.
6.2 ARTICLE 2
Over-the-counter medication use for childhood fever: a crossectional study of Australian parents. Walsh, A., Edwards, H., & Fraser, J. (2007). Over-the-counter medication use for
childhood fever: A cross-sectional study of Australian parents. Journal of
Paediatrics and Child Health, doi:10.1111/j.1440-1754.2007.01161.x.
Journal of Paediatrics and Child Health 43(9): 601-606 (c) 2007 Blackwell Publishing
ABSTRACT
Aim: To report Australian parents’ medication (paracetamol, ibuprofen and
homeopathic) use in childhood fever management.
Methods: A cross-sectional survey of 401 Queensland parents of children aged
between 6 months and 5 years recruited through advertising (48.4%), face-to-face
(26.4%) and snowball (24.4%) methods was conducted. A 17-item instrument was
developed; construct and content validity were determined by an expert panel, and
item reliability by test–retest with nine parents. Areas targeted were medication use,
influences on, and barriers to medication use.
Results: Most participants were female, had tertiary education and lived in a major
city (mean age 34.6 years). Reducing children’s fever with over-the-counter
medications was common (91%): 94% of parents reported using paracetamol and
77% reported using ibuprofen. A few (3.7%) used homeopathic remedies. Dosage
178
was determined by weight (86.3%), age (84.3%), temperature (32.4%), illness
severity (31.4%) and lethargy (20.9%). Frequency was determined by instructions on
the medication label (55.3%), temperature (40.6%) and well-being (27.7%).
Ibuprofen was administered too frequently by 31.5% (four hourly by 22.8%), and
paracetamol by 3.8%. Fifty-two per cent had alternated medications, 65.8% of these
for temperatures below 38.5°C. Decisions to alternate were influenced by
information from doctors/hospitals (49.5%) and children remaining febrile post-
antipyretic (41.7%). Most parents reported over-the-counter medications as
potentially harmful (73.2%), citing liver (38.2%), stomach (26.4%) and kidney
(18.6%) damage and overdose (35.7%) as concerns. When medications were refused
or spat out (44.0%), parents used force (62.4%), different methods (29.5%) or
suppositories (20.8%).
Conclusions: Most parents used over-the-counter medications to reduce fever,
often below 38.5°C. The belief that these medications were harmful was overridden
by fears of harmful outcomes from fever.
Key Points o Parents believe over-the-counter medications may harm children but still use
them to reduce low grade fevers.
o Influences on alternating medications include recommendations from and
observing heath professionals’ practices and children remaining febrile post-
medication.
o Ibuprofen administration four hourly indicates confusion with paracetamol
administration.
179
6.2.1 Introduction Despite more than two decades of literature reporting fever as beneficial.1,2 parents
continue to reduce mild fever, below 38.5ºC, with medications to prevent febrile
convulsions, brain damage and dehydration.3-6 Incorrect antipyretic dosing and
frequency is common, reports of parents overdosing febrile children increased 21%
from 1987 to 1999.7-10 Although literature reporting parents’ beliefs about fever and
medication use abounds literature reporting Australian parents’ fever management
practices is scarce. This paper addresses this deficit by reporting findings from a
crossectional survey of a community based sample of Queensland parents of young
children. Findings will assist Australian health professionals develop and target
education to ensure correct antipyretic use by parents and address parental concerns
about fever.
Antipyretics as parents’ preferred method of managing fever has increased
significantly from 67% in 198011 to 95% in 2002.5 Over the past decade alternating
antipyretics has becoming an accepted practice in controlling fever.4,12 This is
disturbing13,14 as reports of parents’ administration of antipyretics at too low, high, or
frequent doses is common.7,12,15 Recent reports indicated that 45% to 53% of parents
of febrile children had administered incorrect doses of antipyretics prior to seeking
medical assistance.7,12
In addition to reducing temperatures with antipyretics parents also use them to
promote their child’s wellbeing during a febrile episode.3 Using antipyretics
increases parents’ control when their child is ill.16 Temperature reduction is not
always necessary. Many children tolerate low grade fevers to 39.0°C with
remarkable ease.1,17 There is consensus in the literature to reduce temperatures as

180
they approach 40°C (moderate fever) as the immunological benefits of fever are
reduced at 40.0ºC.1,17 There is little indication for medication administration below
38.3ºC, excepting to relieve pain.18
In Australia, paracetamol is one of the most common over-the-counter medications
associated with unintentional overdose in children younger than five years of age.19
When Australian parents use paracetamol to calm upset children, lift children’s mood
and to sedate children so that parents can get some sleep, this is not surprising.20
Paracetamol has been attributed with magical qualities and is perceived as a safe
drug; it increases parents’ control and time management during childhood
illnesses.16,20 The increase in antipyretic use internationally4,5 and reports of
Australian parents misuse of paracetamol20 highlight the importance of identifying
Australian parents’ antipyretic use in fever management and the factors influencing
antipyretic use.
This paper describes Australian parents’ medication usage and influences on
medication use for childhood fever management in a community based sample of
Australian parents with children aged between 6-months and 5-years. It reports part
of a larger study exploring parents’ knowledge, beliefs, practices, influences on
practices and medication use, information sources about fever management, reported
elsewhere,21 and predictors of intentions to reduce fever with medications.
6.2.2 Methods
6.2.2.1 Design A self report crossectional survey was conducted.
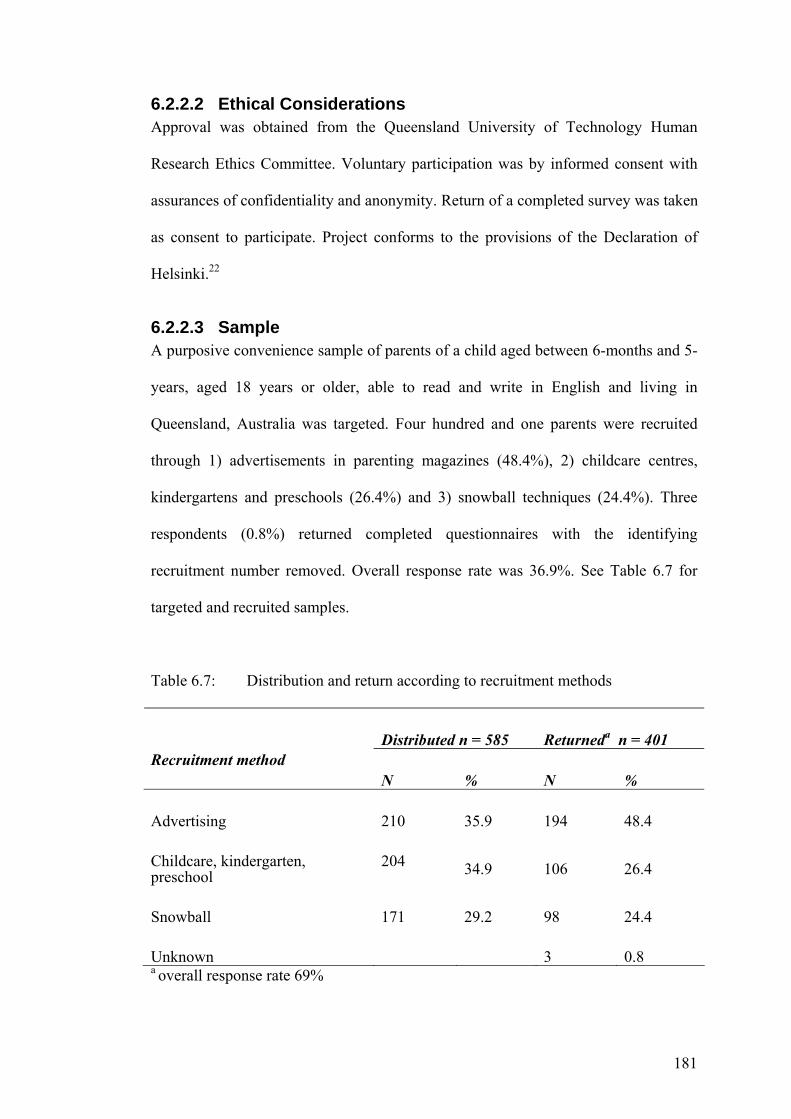
181
6.2.2.2 Ethical Considerations Approval was obtained from the Queensland University of Technology Human
Research Ethics Committee. Voluntary participation was by informed consent with
assurances of confidentiality and anonymity. Return of a completed survey was taken
as consent to participate. Project conforms to the provisions of the Declaration of
Helsinki.22
6.2.2.3 Sample A purposive convenience sample of parents of a child aged between 6-months and 5-
years, aged 18 years or older, able to read and write in English and living in
Queensland, Australia was targeted. Four hundred and one parents were recruited
through 1) advertisements in parenting magazines (48.4%), 2) childcare centres,
kindergartens and preschools (26.4%) and 3) snowball techniques (24.4%). Three
respondents (0.8%) returned completed questionnaires with the identifying
recruitment number removed. Overall response rate was 36.9%. See Table 6.7 for
targeted and recruited samples.
Table 6.7: Distribution and return according to recruitment methods
Distributed n = 585 Returneda n = 401 Recruitment method
N % N %
Advertising 210 35.9 194 48.4
Childcare, kindergarten, preschool
204 34.9 106 26.4
Snowball 171 29.2 98 24.4
Unknown 3 0.8 a overall response rate 69%
182
6.2.2.4 Procedures In an attempt to recruit a representative sample three recruitment methods were
employed; 1) advertising, 2) face-to-face and 3) snowball.
1. Over a 3-month period advertisements were placed in parenting magazines
accessible free of charge to parents in metropolitan and outer metropolitan areas.
Playgroup Queensland members were targeted through the monthly online
newsletter and quarterly magazine. Queensland parents using Family Day Care
were targeted through care providers. Interested parents contacted the researcher
by phone (49.6%) or email (50.4%). Survey packages, containing a letter of
introduction, information sheet, survey and reply paid envelope, were posted to
interested parents.
2. Parents from metropolitan and outer metropolitan childcare centres,
kindergartens and preschools were informed of the study through posters and
individual letters. Interested parents received a survey package following face-to-
face recruitment and returned completed surveys to a sealed box in the centre.
3. Queensland wide snowball recruitment was conducted through respondents and
researcher networks. Completed surveys were returned by mail or collected by
the initial contact and returned to the researcher.
6.2.2.5 Instrument A self-report questionnaire was developed from the international literature and
discussions with Queensland parents.23 See Table 6.8 for sources. The developed
instrument addressed parents’ medication use, influences on medication use and
perceptions of the safety of medications used for fever management on 17 items. The
term medication was used to indicate over-the-counter medications (e.g.,
paracetamol and ibuprofen) and include homeopathic or non-traditional medications.
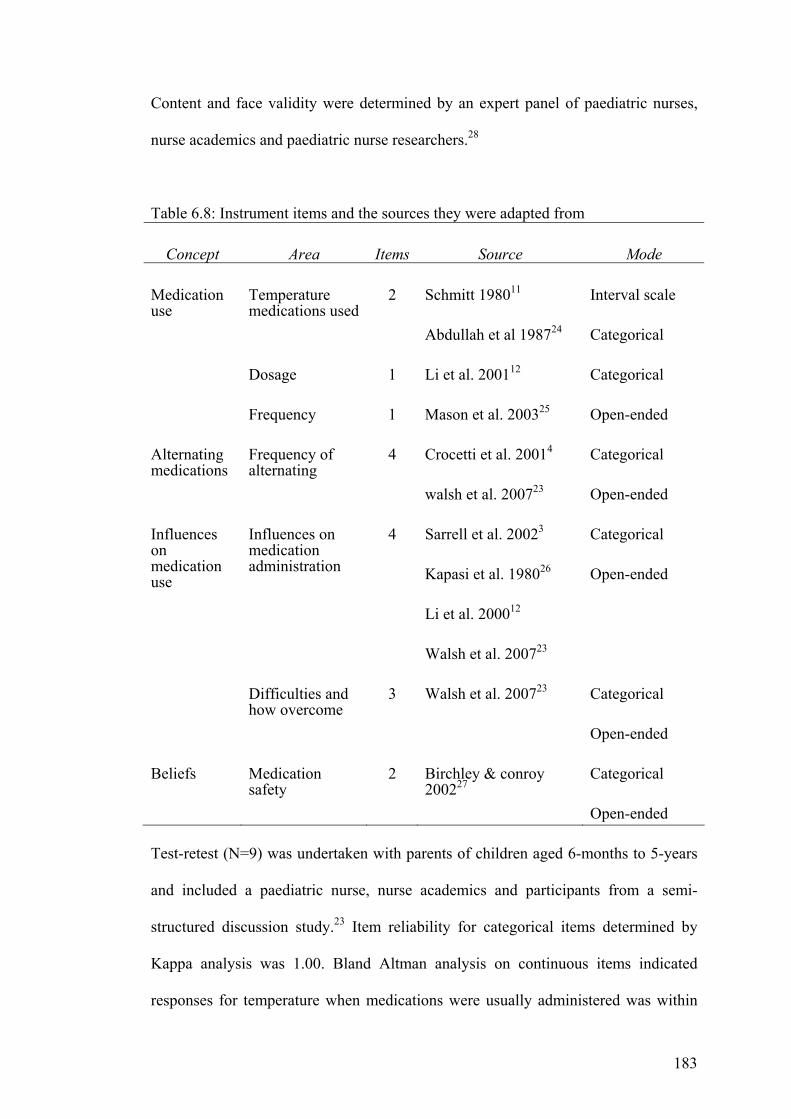
183
Content and face validity were determined by an expert panel of paediatric nurses,
nurse academics and paediatric nurse researchers.28
Table 6.8: Instrument items and the sources they were adapted from
Concept Area Items Source Mode
Medication use
Temperature medications used
2 Schmitt 198011
Abdullah et al 198724
Interval scale
Categorical
Dosage 1 Li et al. 200112 Categorical
Frequency 1 Mason et al. 200325 Open-ended
Alternating medications
Frequency of alternating
4 Crocetti et al. 20014
walsh et al. 200723
Categorical
Open-ended
Influences on medication use
Influences on medication administration
4 Sarrell et al. 20023
Kapasi et al. 198026
Li et al. 200012
Walsh et al. 200723
Categorical
Open-ended
Difficulties and how overcome
3
Walsh et al. 200723 Categorical
Open-ended
Beliefs Medication safety
2 Birchley & conroy 200227
Categorical
Open-ended Test-retest (N=9) was undertaken with parents of children aged 6-months to 5-years
and included a paediatric nurse, nurse academics and participants from a semi-
structured discussion study.23 Item reliability for categorical items determined by
Kappa analysis was 1.00. Bland Altman analysis on continuous items indicated
responses for temperature when medications were usually administered was within

184
the limits of agreement (mean difference ± 2SD).29 Instructions and items were clear
and easily understood.
The final instrument explored parents’ medication administration (eight items),
influences on medication administration (seven items) and beliefs about medication
safety (two items). Demographic information was also collected. This was an
exploratory study and categorical items (e.g., yes, no, unsure) often preceded open-
ended items. Table 6.8 provides the items and source.
6.2.2.6 Data Management and Aanalysis Data were entered into SPSS Version 13 (SPSS Inc., Chicago,IL, USA).30 Responses
to open-ended questions were coded prior to entry. Data entry accuracy was ensured
by SPSS Data Entry Builder 4.0 (SPSS Inc., Chicago,IL, USA).31 Demographics
were examined for frequency and distribution. Open-ended items were examined for
frequency of response. Categorical data were explored for frequency; the interval
scale for distribution, normality and outliers. ANOVA and chi-square analyses were
conducted to explore for demographic differences in alternating medications and
frequency of medication administration.
6.2.3 Results Participants (N=401) were aged between 20 and 52 years (mean 34.58, SD 4.83),
female (N=401, 97.5%) and most in a married or defacto relationship (N=375,
93.5%). Some parents (N=401, 11.2%) reported having a child with a chronic illness,
identified as asthma by 77.3% (N=44) of cases. Experience in a health industry
(education in health care or worked in a health setting) was reported by 32.3%
(N=401). Most respondents had tertiary education; more than one child, were born in
Australia and lived in a major city. See Table 6.9 for additional demographic
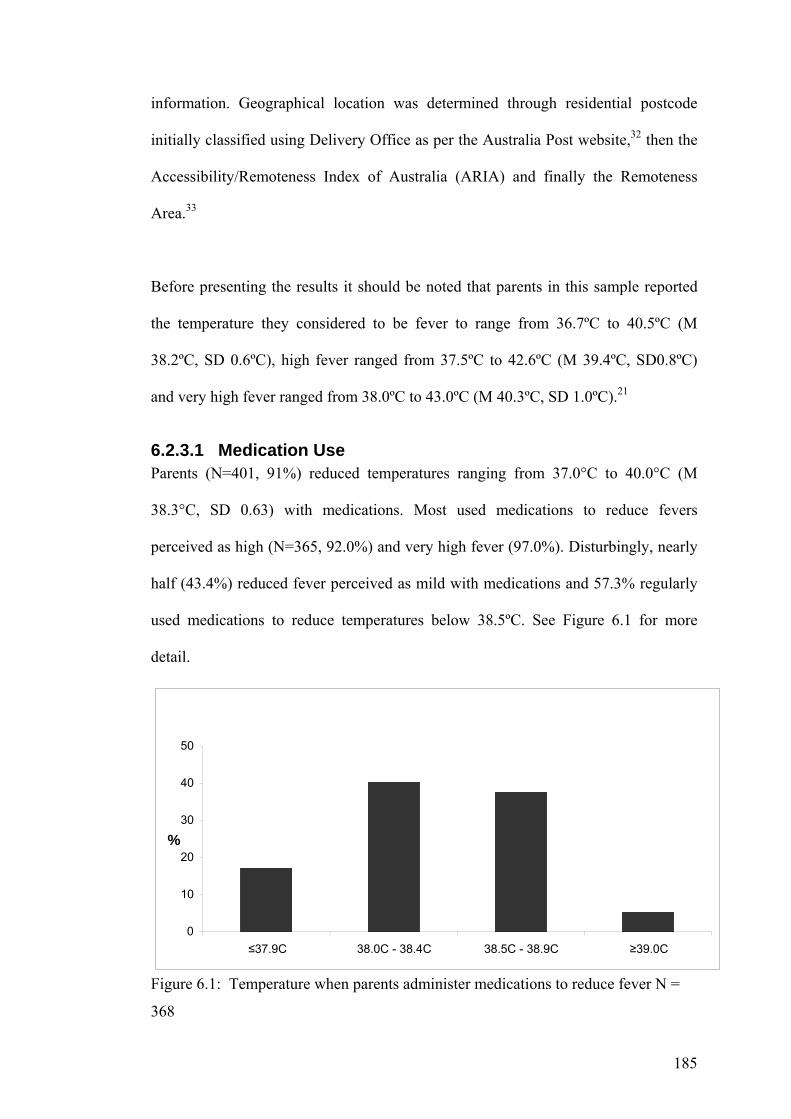
185
information. Geographical location was determined through residential postcode
initially classified using Delivery Office as per the Australia Post website,32 then the
Accessibility/Remoteness Index of Australia (ARIA) and finally the Remoteness
Area.33
Before presenting the results it should be noted that parents in this sample reported
the temperature they considered to be fever to range from 36.7ºC to 40.5ºC (M
38.2ºC, SD 0.6ºC), high fever ranged from 37.5ºC to 42.6ºC (M 39.4ºC, SD0.8ºC)
and very high fever ranged from 38.0ºC to 43.0ºC (M 40.3ºC, SD 1.0ºC).21
6.2.3.1 Medication Use Parents (N=401, 91%) reduced temperatures ranging from 37.0°C to 40.0°C (M
38.3°C, SD 0.63) with medications. Most used medications to reduce fevers
perceived as high (N=365, 92.0%) and very high fever (97.0%). Disturbingly, nearly
half (43.4%) reduced fever perceived as mild with medications and 57.3% regularly
used medications to reduce temperatures below 38.5ºC. See Figure 6.1 for more
detail.
Figure 6.1: Temperature when parents administer medications to reduce fever N =
368
0
10
20
30
40
50
≤37.9C 38.0C - 38.4C 38.5C - 38.9C ≥39.0C
%
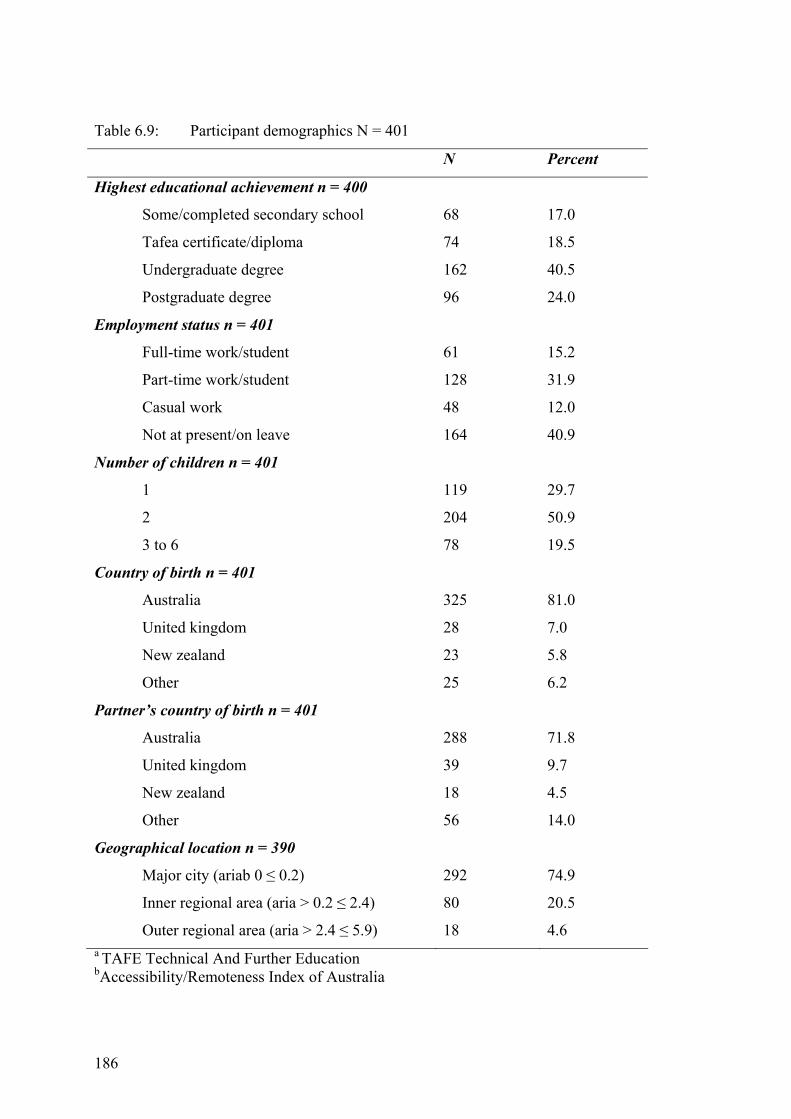
186
Table 6.9: Participant demographics N = 401
N Percent
Highest educational achievement n = 400
Some/completed secondary school
Tafea certificate/diploma
Undergraduate degree
Postgraduate degree
68
74
162
96
17.0
18.5
40.5
24.0
Employment status n = 401
Full-time work/student
Part-time work/student
Casual work
Not at present/on leave
61
128
48
164
15.2
31.9
12.0
40.9
Number of children n = 401
1
2
3 to 6
119
204
78
29.7
50.9
19.5
Country of birth n = 401
Australia
United kingdom
New zealand
Other
325
28
23
25
81.0
7.0
5.8
6.2
Partner’s country of birth n = 401
Australia
United kingdom
New zealand
Other
288
39
18
56
71.8
9.7
4.5
14.0
Geographical location n = 390
Major city (ariab 0 ≤ 0.2)
Inner regional area (aria > 0.2 ≤ 2.4)
Outer regional area (aria > 2.4 ≤ 5.9)
292
80
18
74.9
20.5
4.6 a TAFE Technical And Further Education bAccessibility/Remoteness Index of Australia
187
A small number of parents (N=401, 3.7%) reported using homeopathic preparations
to reduce fever; paracetamol was used by 94% and ibuprofen by 77.1%. Although
decisions to use medications were primarily influenced by temperature many
reported additional factors (N=401, 67.9%). These included the child’s altered
behaviour and/or general wellbeing (57.6%), the presence of pain or discomfort
(32.0%), illness symptoms (22.6%) (e.g., vomiting, cough, cold, rhinitis), sleeping
problems (15.8%) and not eating or drinking (4.1%). Medications were also used
when children had a history of febrile convulsions (3.7%) and non-pharmacological
or homeopathic methods were ineffective (3.3%).
In response to our question regarding frequency of medication administration parents
reported administering paracetamol at one to eight hourly intervals (N=368).
Although most (73.9%) reported four hourly intervals, 3.8% reported more frequent
intervals. Ibuprofen was administered at three to eight hourly intervals (N=260); one-
third (38.6%) reported six hourly administration. Alarmingly, 31.5% reported more
frequent intervals three to five hourly; 22.8% administered ibuprofen four hourly.
Parents with one child (43.3%) reported incorrect ibuprofen administration more
frequently than those with three or more children (15.1%) (F[2,257]=4.114,p=0.02).
A tendency toward incorrect ibuprofen administration was found in parents recruited
through advertising (33.3%) and face-to-face (32.4%) compared with those recruited
by snowball methods (18.9%) (F[2,256]=2.512,p=.08).
Factors influencing medication dosage (N=401) included the child’s weight (86.3%),
age (84.3%), temperature (32.4%), illness severity (31.4%), presence of
lethargy/listlessness (20.9%) and irritability (18.0%). Frequency of administration
188
(N=401) was influenced by instructions on the medication label (55.3%), child’s
temperature (40.6%), wellbeing (27.7%), doctor’s advice (10.7%) and time of day
(4.3%) (e.g., at bedtime to assist sleep).
6.2.3.2 Alternating Medications The practice of alternating medications, paracetamol and ibuprofen, was common
(N=401, 51.8%). Parents alternated to reduce mild (5.8%), high (55.6%) and very
high fever (91.8%) (see Figure 6.2). Frequency of alternating ranged from once
(N=207, 19.9%), to rarely (28.2%), sometimes (39.8%), mostly (11.7%) and always
(0.5%). Disturbingly 65.8% of parents who alternated did so to reduce mild fever,
temperatures below 38.5ºC. Decisions to alternate were influenced by advice from a
doctor or at a hospital (49.5%), a child febrile post-medication (41.7%), different
therapeutic qualities of the medications (21.6%) and advice from others (8.8%).
Medications were also alternated to increase comfort (7.8%), for children with a
history of febrile convulsions (2.0%) and to encourage fluid intake (1.5%). Again
parents recruited through advertising (66.7%) reported alternating medications more
frequently than those recruited through face-to-face (58.2%) or snowball (48.1%)
methods (χ2[2, N=397]=7.331,p=.03). Parents who had exposure to the health
industry (61.7%) were more likely (χ2[1,N=396]=7.884,p=.01) to alternate
medications than those with no exposure (46.6%).
6.2.3.3 Medications are Harmful Most parents believed medications used to reduce fever were harmful (N=401,
73.2%). Some were unsure of this (16.3%) and 10.5% believed them not to be
harmful. Parents reported harmful outcomes from these medications to be liver
damage (38.2%), overdose (35.7%), stomach (26.4%) or kidney damage (18.6%),
reduced immunity (7.9%) and allergic reactions (7.5%). Figure 6.3 presents the
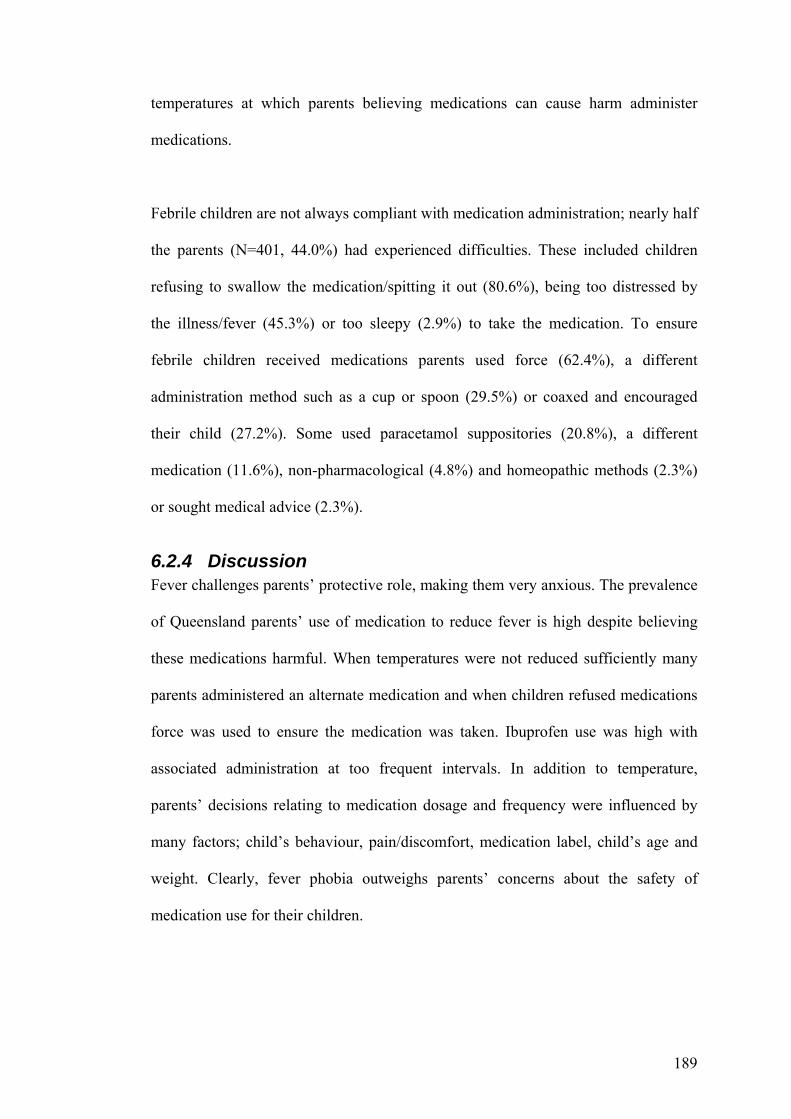
189
temperatures at which parents believing medications can cause harm administer
medications.
Febrile children are not always compliant with medication administration; nearly half
the parents (N=401, 44.0%) had experienced difficulties. These included children
refusing to swallow the medication/spitting it out (80.6%), being too distressed by
the illness/fever (45.3%) or too sleepy (2.9%) to take the medication. To ensure
febrile children received medications parents used force (62.4%), a different
administration method such as a cup or spoon (29.5%) or coaxed and encouraged
their child (27.2%). Some used paracetamol suppositories (20.8%), a different
medication (11.6%), non-pharmacological (4.8%) and homeopathic methods (2.3%)
or sought medical advice (2.3%).
6.2.4 Discussion Fever challenges parents’ protective role, making them very anxious. The prevalence
of Queensland parents’ use of medication to reduce fever is high despite believing
these medications harmful. When temperatures were not reduced sufficiently many
parents administered an alternate medication and when children refused medications
force was used to ensure the medication was taken. Ibuprofen use was high with
associated administration at too frequent intervals. In addition to temperature,
parents’ decisions relating to medication dosage and frequency were influenced by
many factors; child’s behaviour, pain/discomfort, medication label, child’s age and
weight. Clearly, fever phobia outweighs parents’ concerns about the safety of
medication use for their children.
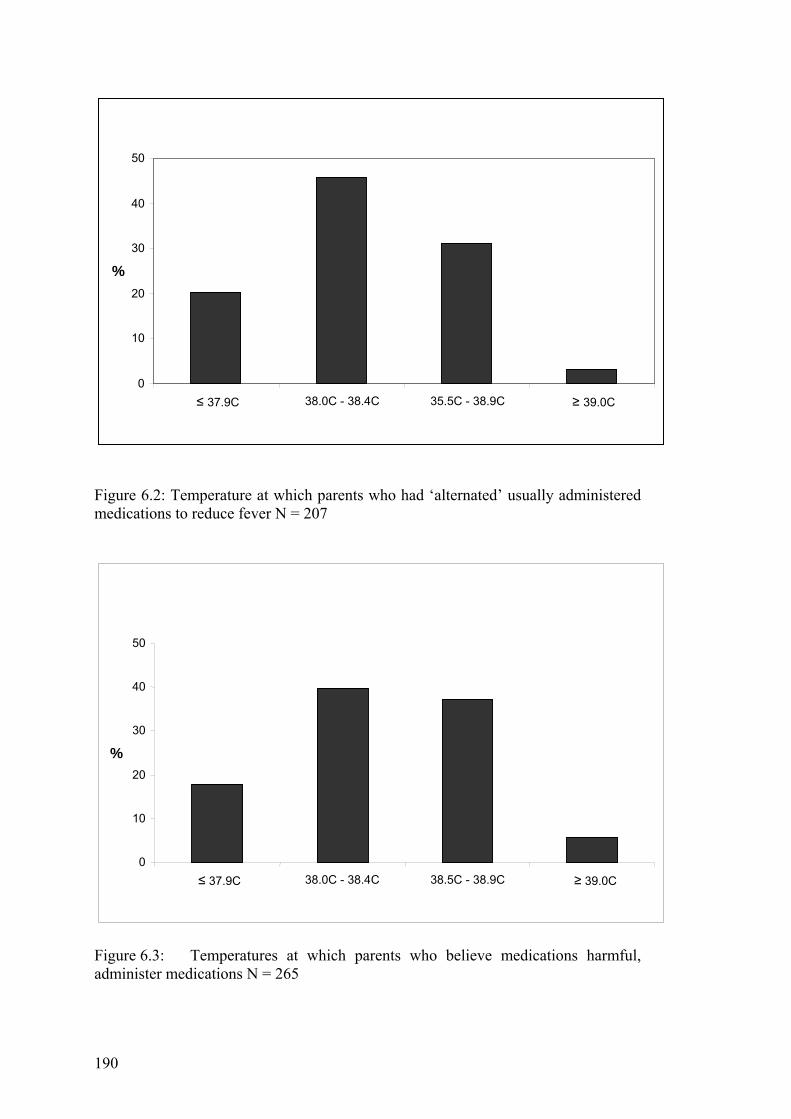
190
Figure 6.2: Temperature at which parents who had ‘alternated’ usually administered medications to reduce fever N = 207
Figure 6.3: Temperatures at which parents who believe medications harmful, administer medications N = 265
0
10
20
30
40
50
≤ 37.9C 38.0C - 38.4C 35.5C - 38.9C ≥ 39.0C
%
0
10
20
30
40
50
≤ 37.9C 38.0C - 38.4C 38.5C - 38.9C ≥ 39.0C
%
191
6.2.4.1 Medication Use We found parents medicated to reduce mean temperatures of 38.3ºC, a temperature
similar to their definition of fever 38.2ºC.21 Similar findings have been reported.
American34 parents define fever as 38.0ºC and medicate at 38.1ºC and Canadian5
parents define fever as 37.9ºC and medicate 38.2ºC. Parents reducing temperatures
defined as fever highlight their concerns about fever. More than half the parents in
this study medicated temperatures below 38.5ºC, mild fever, and alternated
medications at temperatures below 39.5ºC, moderate fever.
Although paracetamol was the most frequently used medication, most parents also
used ibuprofen. Internationally, other studies report much lower rates of ibuprofen
use.3,8 This is disturbing as more parents indicated administering ibuprofen at too
frequent intervals with four hourly most common implying there may be confusion
when parents use multiple medications. However, these findings do align with those
from other studies, too frequent administration is more likely with ibuprofen.4,15
The use of antipyretics for behaviour control, improving well-being and sleeping
have been previously reported.3-5, 8,20 Queensland parents’ reports were similar
indicating an urgent need for health professionals to educate parents about
antipyretics’ actions. The attribution of magical qualities to antipyretics encourages
their use, increasing fever phobia and the probability of overdosing. Providing
parents with appropriate fever management strategies such as encouraging fluids and
rest, keeping febrile children comfortable and guidelines of when to use medications
and seek medical advice is needed to reduce phobias and overdosing.

192
6.2.4.2 Alternating Medications – Clinical Implications The rate of alternating medications is increasing and influenced by information from
doctors and hospitals, temperatures not reduced sufficiently after an initial
medication, medication properties and advice from others. Observing health
professionals alternate medications and receiving advice to alternate from doctors
significantly influenced parents’ practices.13,23,35 Alternating has been reported since
the 1980s when aspirin and paracetamol were alternated.36 The influence of the
health profession in alternating is evidenced by the higher percentage of parents with
exposure to this industry alternating. This is possibly understandable when
considered in association of continued reports of health professionals’ concerns
about fever and recommendations to alternate antipyretics.3,5,13 Recent experimental
studies exploring the efficacy of alternating antipyretics in febrile children35,37,38
found minimal additional temperature reduction, that is from 0.3ºC to 1.0ºC as a
result of a combined dose38 from alternating medications over a 24-h period.37
Caution is recommended in advising parents to alternate emphasising the risk of
parental confusion and dosage errors.14,39 Additionally, identifying a need to alternate
to ‘get fever under control’ will increase parental preoccupation with and fear of
fever increasing unnecessary phone calls and medical service use.14 Increased
medication use could produce an associated increase in accidental overdosing. Over-
the-counter medications are readily available; marketing includes recommendations
from celebrity and health professional mothers. Health professionals, especially
doctors and nurses, have a responsibility in child advocacy to make parents more
competent in the use of such easily available and potentially harmful drugs.
193
6.2.4.3 Strengths and Limitations This large, comprehensive study highlights the need for evidence-based education for
parents and the health professionals from whom parents’ information is sourced.
However, care must be taken in generalisation of these findings as the sample was
self-selected and most had tertiary education and lived in major cities and data were
collected by self-report. That those recruited through advertising were more likely to
overdose and alternate medications indicates the sample could be biased toward
medication use. It was not within the scope of this study to collect data relating to
the medication dosages parents administered.
6.2.4.4 Conclusions Health professionals have a vital role in ensuring parents appropriately medicate their
children. The inappropriate and overuse of antipyretics by Queensland parents
highlights the need for parental education about medication dosage and actions.
Fever phobia, implied by Queensland parents’ rate of alternating antipyretics and use
of medications believed harmful to reduce fever, must be addressed. Education based
on the latest scientific evidence is needed for all parents of young children. Ideally all
parents should learn how to manage fever prior to their first child’s first febrile
episode. Findings from this study may not be confined to Queensland. Therefore,
replication of this study in other Australian states is recommended to determine the
extent of parental fever phobia and medication misuse in Australia.
6.2.5 Acknowledgements The authors would like to acknowledge the support of the Royal College of Nursing,
Australia for the Joyce Wickham Memorial Scholarship which assisted in the
undertaking of this study. We would also like to thank those involved in the expert
panel and all the parents who so generously gave of their time to complete the pilot
and main study.
194
6.2.6 References 1 Lorin M. Pathogenesis of fever and its treatment. In: McMillan JB, DeAngelis C,
Feigin RD, Warshaw JB, eds. Oski’s Pediatrics: Principles and Practices, 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins, 1999; 848–50.
2 Lorin M. Is fever a friend or a foe? Contemp. Pediatr. 1986; 3: 35–46. 3 Sarrell M, Cohen H, Kahan E. Physicians’, nurses’, and parents’ attitudes to and
knowledge about fever in early childhood. Patient Educ. Coun. 2002; 46: 61–5.
4 Crocetti M, Moghbeli N, Serwint J. Fever phobia revisited: have parental
misconceptions about fever changed in 20 years? Pediatrics 2001; 107: 1241–6.
5 Karwowska A, Nijssen-Jordan C, Johnson D, Davies H. Parental and health care
provider understanding of childhood fever: a Canadian perspective. Can. J. Emerg. Med. 2002; 4: 394–400.
6 van Stuijvenberg M, de Vos S, Tjiang G, Steyerberg E, Derksen-Lubsen G, Moll
H. Parents’ fear regarding fever and febrile seizures. Acta Paediatr. 1999; 88: 618–22.
7 Goldman R, Scolnik D. Underdosing of acetaminophen by parents and emergency
utilization. Pediatr. Emerg. Care 2004; 20: 89–93. 8 Betz C, Grunfeld A. Fever phobia in the emergency department: a survey of
children’s caregivers. Eur. J. Emerg. Med. 2006; 13: 129–33. 9 Kilmon C. Parents’ knowledge and practices related to fever management. J.
Pediatr. Health Care 1987; 1: 173–9. 10 Linder N, Sirota L, Snapir A et al. Parental knowledge of the treatment of fever
in children. IMAJ 1999; 1: 158–60. 11 Schmitt B. Fever phobia: misconceptions of parents about fevers. Am. J. Dis.
Child. 1980; 134: 176–81. 12 Li S, Lacher B, Crain E. Acetaminophen and ibuprofen dosing by parents.
Pediatr. Emerg. Car. 2000; 16: 394–7. 13 Mayoral C, Marino R, Rosenfeld W, Greensher J. Alternating antipyretics: is this
an alternative. Pediatrics 2000; 105: 1009–12. 14 Schmitt B. Concerns over alternating acetaminophen and ibuprofen for fever.
Arch. Pediatr. Adolesc. Med. 2006; 160: 757. 15 Bilenko N, Tessler H, Okbe R, Press J, Gorodischer R. Determinants of
antipyretic misuse in children up to 5 years of age: a cross-sectional study. Clin. Ther. 2006; 28: 783–93.
195
16 Lagerlov P, Helseth S, Holager T. Childhood illnesses and the use of paracetamol (acetaminophen): a qualitative study of parents’ management of common childhood illnesses. Fam. Pract. 2003; 20: 717–23.
17 Connell F. The causes and treatment of fever: a literature review. Nurs. Stand.
1997; 12: 40–3. 18 Dlugosz C. CE test appropriate use of nonprescription analgesics in pediatric
patients. J. Pediatr. Health Care 2006; 20: 326–8. 19 Chien C, Marriott J, Ashby K, Ozanne-Smith J. Unintentional ingestion of over
the counter medications in children less than 5 years old. J. Paediatr. Child Health 2003; 39: 264–9.
20 Allotey P, Reidpath D, Elsisha D. ‘Social medication’ and the control of children:
a qualitative study of over-the-counter medication among Australian children. Pediatrics 2004; 114: e378–83.
21 Walsh A, Edwards H, Fraser J. Underpinned by fear: a community study of
parents’ fever management with young children. Int. J. Nurs. Stud. (in press). 22 World Medical Association. World Medical Association Declaration of Helsinki:
ethical principles for medical research involving human subjects. In: WMA The Global Representative Body of Physicians: Document 17.C. Available from: http://www.wma.net/e/policy/b3.html [accessed 21 August 2006].
23 Walsh A, Edwards H, Fraser J. Influences on parents’ fever management: beliefs,
experiences and information sources. J. Clin. Nurs. 2007. doi:10.1111/j.1365-2702.2006.01890.x.
24 Abdullah M, Ashong E, Al Habib S, Karrar Z, Al Jishi N. Fever in children:
diagnosis and management by nurses, medical students, doctors and parents. Ann. Trop. Paediatr. 1987; 7: 194–9.
25 Mason S, Thorp S, Burke D. Prehospital use of paracetamol among children
attending the accident and emergency department. Emerg. Med. J. 2003; 20: 88–9.
26 Kapasi A, Lorin M, Nirken M, Yudovich M. Parents’ knowledge and sources of
knowledge about antipyretic drugs. J. Pediatr. 1980; 97: 1035–7. 27 Birchley N, Conroy S. Parental management of over-the-counter medicines.
Paediatr. Nurs. 2002; 14: 24–8. 28 Polit D, Hungler B. Nursing Research: Principles and Methods. New York:
Lippincott, 1999. 29 Bland M, Altman D. Statistical methods for assessing agreement between two
methods of clinical measurement. Lancet 1986; i: 307–10.
196
30 SPSS Inc. SPSS for Windows Version 13.0 [program], 11.0 version. Chicago, IL: SPSS Inc., 2004.
31 SPSS Inc. SPSS Data Entry Builder Release 4.0.0 [program] (version 4.0).
Chicago, IL, USA: SPSS Inc. 1996 to 2003. 32 Australia Post. Australia Post Postcode Datafile pc-full_20051206, 2006.
Available from: http://www1.auspost.com.au/postcodes/ [accessed 8 January 2007].
33 Trewin D. Australian Standard Geographical Classification (ASGC). Canberra:
Australian Bureau of Statistics, 2005. 34 Porter R, Wenger F. Diagnosis and treatment of pediatric fever by caretakers. J.
Emerg. Med. 2000; 19: 1–4. 35 Nabulis M, Tamin H, Mahfoud Z et al. Alternating ibuprofen and acetaminophen
in the treatment of febrile children: a pilot study. BMC Med. 2006. Available from: http://www.biomedcentral.com/1741-7015/4/4 [accessed 10 December 2006].
36 Weiss J, Herskowitz L. House officer management of the febrile child. A survey.
Clin. Pediatr. 1983; 22: 766–9. 37 Sarrell E, Wielunsky E, Cohen H. Antipyretic treatment in young children with
fever: acetaminophen, ibuprofen, or both alternating in a randomized, double-blind study. Arch. Pediatr. Adolesc. Med. 2006; 160: 197.
38 Erlewyn-Lajeunesse M, Coppens K, Hunt L et al. Randomised controlled trial of
combined paracetamol and ibuprofen. Arch. Dis. Child. 2006; 91: 414–6. 39 Saphyakhajon P, Greene G. Alternating acetaminophen and ibuprofen in children
may cause parental confusion and is dangerous. Arch. Pediatr. Adolesc. Med. 2006; 160: 757.
6.3 SUMMARY Parents have negative beliefs about fever and reduce fever to prevent harmful
outcomes, principally febrile convulsions. Temperature reducing strategies were
dependent on the height of fever as was seeking medical advice. Doctors were the
most frequently reported source for learning to manage fever followed by past
experience. Experience influenced practice change. Positive experiences reduced
antipyretic and medical service use, negative experiences increased antipyretic and
medical service use. Antipyretics were the preferred method of fever reduction for

197
mean temperatures of 38.3ºC. Half the parents had alternated antipyretics on the
recommendation of doctors and hospitals.
198
CHAPTER 7
DETERMINANTS OF PARENTS’ INTENTIONS TO REDUCE FEVER
7.1 INTRODUCTION This chapter describes the methods, results and discussion of findings from the
second section of the survey, the theoretical data. The survey used in Study 2 was
completed by 401 parents and is available for perusal in Appendix 2. Two conceptual
models were examined to identify the influence of demographic factors and
theoretical constructs to the Theory of Planned Behavior (TPB) on parents’ fever
management intentions.
The chapter begins by identifying the hypotheses to be tested for each model and the
conceptual frameworks for each model are depicted. Next the approach to analysis,
structural equation modelling, and its appropriateness is discussed. Following this the
method of model estimation and statistical methods for assessing model fit are
described. Preparation of data for analysis including the management of missing
values, normality testing and issues due to nonnormality are then addressed.
Following this bivariate correlations of the demographic variables are described then
the theoretical models tested. The fever model, results and discussion are addressed
first. The medication model is similarly reported. Finally there is a discussion of the
overall findings and comparisons between the models. Implications of the findings
and recommendations for future research are addressed in Chapter 8.
199
7.1.1 Theoretical framework The Theory of Planned Behavior (TPB) (Ajzen, 1985) described in Chapter 3 forms
the theoretical framework used to determine the predictors of parents’ fever
management intentions. Two specific intentions were explored: 1) parents’ intention
to reduce their child’s next fever (fever model) and 2) parents’ intention to reduce
their child’s next fever with over-the-counter medications (medication model).
Central to the TPB is the premise that an individual’s overt behaviour is related to
their intention to perform the behaviour. Behavioural intention is determined by the
person’s attitudes toward the behaviour (an individual’s positive or negative
evaluation of the behaviour), subjective norms (individual’s perception of social
pressure from significant referents) and perceived behavioural control (perceived
potential constraints, both internal and external, on the individual performing the
behaviour) (Ajzen, 2006a,b). In accordance with the TPB, parents’ fever
management intentions were determined by their attitudes toward the benefits or
harmful outcomes from fever, perceived expectations of significant others about
fever reduction, perceptions of control over fever management decision making (self-
efficacy; internal or direct control) and of child medication behaviour
(controllability; external or indirect control) on managing fever. Background
influences contributing to parents’ intentions explored in this study through the TPB
were age, educational level, number of children and experience in the health
industry.
This section of the instrument has a strong theoretical basis. Directions for
developing items to address theoretical constructs of the TPB are well established
and were used to develop the instrument items (Ajzen, 2006a; Francis et al., 2004).
Ajzen (2006a) advises the development of TPB instruments be guided by an
200
elicitation study. This was undertaken through a qualitative, elicitation study, Study 1
which is reported in Chapter 5, to determine salient beliefs about fever and fever
management, principal referents in fever management and perceptions of control and
perceived barriers to control when managing fever (Ajzen, 2006a). Findings from the
elicitation study and the fever management literature from 1980 to 2004 directed
item development for use in this section of the instrument.
Parents’ fever management behavioural intentions have not been previously explored
either theoretically or through the TPB. Therefore, theoretical constructs of the TPB,
in relation to parents’ fever management intentions have not been previously
developed. To ensure high reliability of survey items (indicator variables) and correct
estimations of the associations between the theoretical constructs, Ajzen (2006a)
advises the use of indirect measures of the TPB’s constructs. Therefore, the
development of items exploring the theoretical constructs was guided by Ajzen’s
recommendations of the necessary conceptual and methodological considerations
when constructing a TPB instrument (Ajzen, 2006a). Items targeting attitudes
included behavioural beliefs, beliefs about the likely outcome of the behaviour and
the evaluations of these outcomes. Those exploring subjective norms included
normative beliefs, beliefs about the normative expectations of others and motivation
to comply with these expectations. Both internal and external dimensions of
perceived behavioural control (PBC) were explored (Ajzen, 2006a; Frances et al.,
2004). The internal dimensions (direct control) explored were parents’ self-efficacy
in relation to controlling fever management decision making. External dimensions
(indirect control) explored whether child medication behaviour, if a child took
medications easily, made managing fever easier. Several direct items were used to

201
measure intention and measured whether parents intended, planned or would try to
reduce the next fever and reduce their child’s next fever with medications (Ajzen,
2006a).
TPB instrument validity and reliability were determined both theoretically and
statistically. When using the TPB construct validity is determined through the
theoretically determined constructs (Ajzen, 2006a). Face and content validity of
instrument items were determined by an expert panel including a psychologist
familiar with TPB research, a paediatric nurse researcher, clinical paediatric nurses
and nurse academics. Analytical methods using confirmatory factor analysis
explored convergent and discriminant validity through the extent to which items
converge on a construct or share a high proportion of variance in common and
construct reliability (Hair, Black, Babin, Anderson & Tatham, 2006). The use of
indirect measures rather than direct measures has been shown to increase TPB
construct reliability (Ajzen, 2006a). Construct and discriminant validity and
construct reliability are discussed later in the chapter in sections addressing each
model.
7.2 HYPOTHESES FOR THE FEVER MODEL Parents’ intentions to reduce their child’s next fever were explored through their:
• Attitudes toward reducing fever to prevent harmful outcomes from fever (fever
beliefs – six items). See attitudes fever in Figure 7.1,
• Normative influences from partner, mother, friends and doctor to reduce fever
(normative beliefs – eight items). See norms fever in Figure 7.1,
202
• Perceived behavioural control in decision making related to fever management
(perceived control beliefs, direct control – four items). See PBC decision making
in Figure 7.1,
• Perceived behavioural control related to child medication behaviour (child
behaviours beliefs, indirect control– four items). See PBC child medication
behaviour in Figure 7.1,
• Intentions to reduce their child’s next fever (intentions – three items). See
intentions to reduce fever in Figure 7.1 and
• Demographic factors: age (one item), educational level (one item), number of
children (one item) and experience in the health industry (one item). See Figure
7.1 for age, education, number of children and health industry.
The hypotheses tested in the fever model were:
5 In accordance with the TPB, attitudes, subjective norms and perceived
behavioural control (fever management decision making and child medication
behaviour) will determine parents' intentions to reduce their child's next fever.
6 Perceived behavioural control related to child medication behaviour will
determine attitudes, subjective norms and perceived behavioural control in fever
management decision making.
7 Demographic factors, age, education, number of children and experience in the
health industry (education in a health profession or working in a health setting)
will determine parents’ attitudes, subjective norms and perceived behavioural
control (fever management decision making).
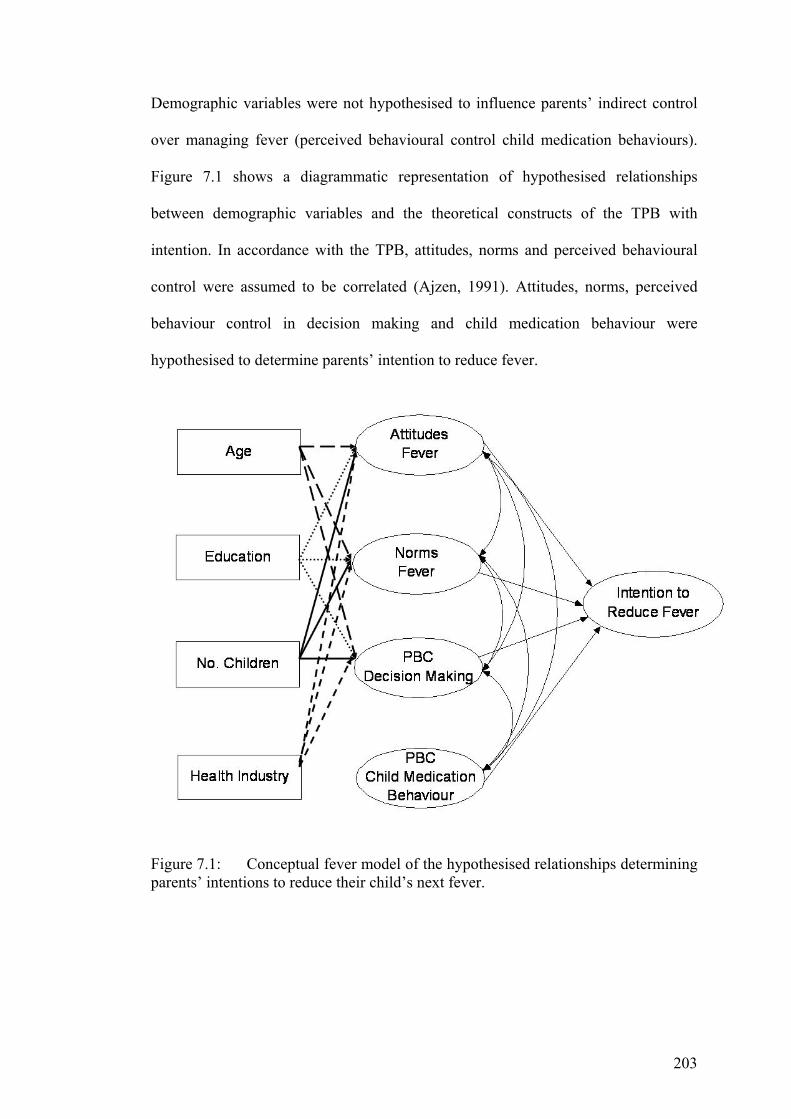
203
Demographic variables were not hypothesised to influence parents’ indirect control
over managing fever (perceived behavioural control child medication behaviours).
Figure 7.1 shows a diagrammatic representation of hypothesised relationships
between demographic variables and the theoretical constructs of the TPB with
intention. In accordance with the TPB, attitudes, norms and perceived behavioural
control were assumed to be correlated (Ajzen, 1991). Attitudes, norms, perceived
behaviour control in decision making and child medication behaviour were
hypothesised to determine parents’ intention to reduce fever.
Figure 7.1: Conceptual fever model of the hypothesised relationships determining parents’ intentions to reduce their child’s next fever.
204
7.3 HYPOTHESES FOR THE MEDICATION MODEL Parents’ intentions to reduce their child’s next fever with medications were explored
through their:
• Attitudes toward reducing fever with medications to prevent harmful outcomes
from fever (beliefs about reducing fever with medications – eight items). See
attitudes medications in Figure 7.2,
• Normative influences from partner, mother, friends and doctor to reduce fever
with medications (normative beliefs about reducing fever with medications –
eight items). See norms medications in Figure 7.2,
• Perception of control in decision making related to fever management (perceived
control beliefs – four items). See PBC decision making in Figure 7.2,
• Perceived behavioural control related to child medication behaviours (child
behaviours – four items). See PBC child medication behaviour in Figure 7.2,
• Intentions to reduce their child’s next fever with medications (intentions – three
items). See intentions to reduce fever with medications in Figure 7.2 and,
• Demographic factors: age (one item), educational level (one item), number of
children (one item) and experience in the health industry (one item). See Figure
7.2 for age, education, number of children and health industry.
The hypotheses tested in the medication model were:
4. In accordance with the TPB, attitudes, subjective norms and perceived
behavioural control (fever management decision making and child medication
behaviour) will determine parents' intentions to reduce their child's next fever
with medications.
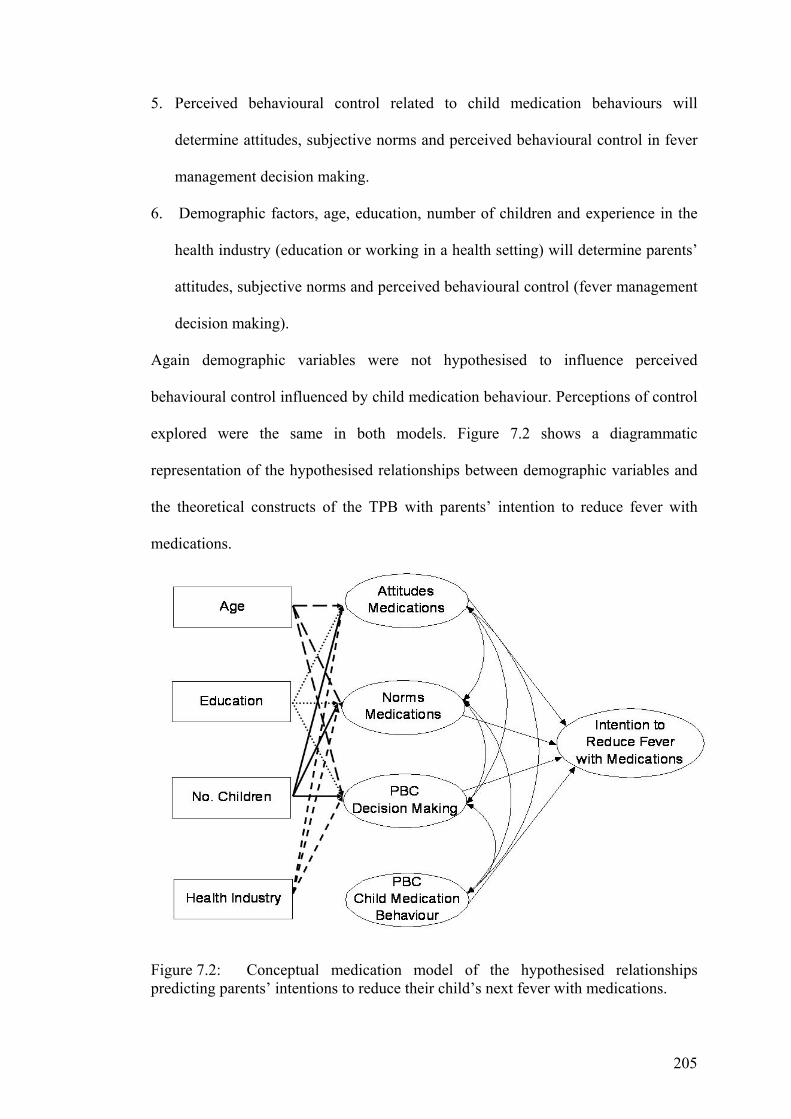
205
5. Perceived behavioural control related to child medication behaviours will
determine attitudes, subjective norms and perceived behavioural control in fever
management decision making.
6. Demographic factors, age, education, number of children and experience in the
health industry (education or working in a health setting) will determine parents’
attitudes, subjective norms and perceived behavioural control (fever management
decision making).
Again demographic variables were not hypothesised to influence perceived
behavioural control influenced by child medication behaviour. Perceptions of control
explored were the same in both models. Figure 7.2 shows a diagrammatic
representation of the hypothesised relationships between demographic variables and
the theoretical constructs of the TPB with parents’ intention to reduce fever with
medications.
Figure 7.2: Conceptual medication model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever with medications.
206
7.4 APPROACH TO ANALYSIS When using the TPB, Hankins, French and Horne (2000) recommend the use of
multiple regression or structural equation modelling to determine the relative
contributions of attitudes, norms and perceived control in the prediction of intention.
Regression and structural equation modelling are used for different levels of model
complexity. Regression, with its modelling of direct relationships, is a subset of the
complex models with which structural equation modelling can cope (Tabachinck &
Fidell, 2007). With the development of user-friendly computer programs structural
equation modelling has become more popular and is particularly relevant where
constructs that can not be directly measured, such as personality traits and attitudes,
are inferred from test or questionnaire items (Fife-Shaw, 2006). The TPB infers a
person’s attitudes, subjective norms, perceived control and intentions from cross-
products of questionnaire items. Structural equation modelling (SEM) is an
appropriate analytical method for correlational and experimental studies, however
crossectional designs are reported more frequently (Hair et al., 2006).
SEM approaches use two types of models (measurement and structural) to determine
a priori relationships between questionnaire items that define latent constructs
(measurement) and relationships between independent and dependent variables
(structural). In this way the models represent confirmatory modelling of a theory
rather than exploratory modelling using factor analysis and multiple regression
analyses. The measurement model, confirmatory factor analysis (CFA), models the
relationships between observed items and unobserved, or latent variables; confirms
item inclusion in a factor (scale); and whether the items and factor have a predefined
unidimensional or multidimensional relationship. The second model, the structural
model, models the relationships between the unobserved latent variables, developed
207
through CFA as well as their relationship to any additional observed variables.
Cross-sectional studies exploring latent variable or measurement models are common
in TPB literature (MacCallum & Austin, 2000).
CFA and exploratory factor analysis answer different research questions. CFA is
used when confirming an established model while exploratory factor analysis is used
to establish a likely model. In accordance with the TPB a full latent variable CFA
model specifies the relationships of the indicator variables to the latent variables and
relationships between latent variables (MacCallum & Austin, 2000).
Both SEM and multiple regression are general linear models valid only if specific
assumptions are met and the hypothesised causal relationships have been determined
by sound underlying theory and research design (Weston & Gore, 2006). Similarly to
regression, SEM allows for the identification of linear relationships between
independent and dependent constructs or directly observed variables. The
assumptions of SEM are:
o interval data are assumed,
o multivariate normality of the indicators – violation leads to large differences
in the chi-square test (χ2) undermining its utility,
o linear relationships between indicator and latent variables,
o theoretically under-identified or just-identified models are inappropriate (the
number of free parameters must be less than or equal to the number of
observations)
o sample size is dependent on the number of parameters and should be greater
than 200 (complex models require larger samples) and
208
o single factors should have at least three indicators for a model to be identified
(Kline, 2005).
An exception to the last assumption is when models have more than one factor there
can be a minimum of two indicator variables per factor (Bollen, 1989) in samples
greater than 150 (Marsh & Hau, 1999).
In summary, the analytical capabilities of CFA and SEM make it a more appropriate
method for confirming relationships between questionnaire items and constructs
(CFA) and between both independent and dependent constructs (SEM) in TPB
research when assumptions are met.
7.5 MODEL ESTIMATION The most commonly used estimation method in SEM is maximum likelihood
estimation. It is the statistical principle underlying the derivation of parameter
estimates: the estimates maximising the likelihood (the continuous generalisation)
that the data (the observed covariances) are drawn from a population assumed to be
the same as that reflected in the coefficient estimates. Maximum likelihood
estimation selects estimates with the greatest chance of reproducing the observed
data (Kline, 2005). It is a ‘normal theory’ method and assumes the population
distribution for the errors associated with the indicator variables are multivariate
normal. Generally, if these distributions are severely nonnormal corrections should
be made (Kline, 2005).
In large samples with severely nonnormal distributions on continuous variables the
maximum likelihood parameter estimates are generally accurate. However, estimated
standard errors can be too low (negatively biased) by as much as 25-50% (depending
on data and model) resulting in inappropriate rejection of the null hypothesis and
209
hence an inflated Type I error rate. Additionally, in the presence of nonnormality, the
rate of Type II error may be up to 50% compared to an expected 5% when normal
distributions are assumed, again depending upon the data and model (Chou &
Bentler, 1995; Curran, West & Finch, 1997).
Despite this, parameter estimates generated by maximum likelihood estimations have
been found to be relatively robust against violations of normality assumptions (Hair
et al., 2006; Kline, 2005). Maximum likelihood estimations on nonnormal data have
been compared with generalised least squares and weighted least squares to explore
the effects on fit indices and parameter bias in different sample sizes. Reliable results
have been produced under many circumstances (Olsson, Foss, & Breivik, 2004;
Olsson, Foss, Troye, & Howell, 2000).
7.6 ASSESSING MODEL FIT There are many statistical methods available to determine how well a structural
equation model fits the observed data; these generally assess model goodness-of-fit
(model saturation) and badness-of-fit (model parsimony). Generally both goodness
and badness-of-fit statistics are reported (Hair et al., 2006). Fit statistics used in the
following analyses are discussed below along with the rationale for choosing each
statistic. Goodness-of-fit statistics to be reported are the chi-square goodness-of-fit
statistic, normed chi-square goodness-of-fit index, adjusted goodness-of-fit index and
comparative fit index. The badness-of-fit statistic reported is the root mean square
error approximation.
7.6.1 Chi-Square Goodness-of-Fit Statistic (χ2 GOF)
The most common goodness-of-fit index is the χ2 GOF which assumes multivariate
normality and tests difference in estimated and actual observed covariance matrices.
210
A significant χ2 suggests the model does not fit the sample data, alternatively a
nonsignificant χ2 indicates the model fits the data well. However, finding an exact fit
is rare and as with most statistics large sample sizes increase power resulting in
significance of negligible effect sizes (Weston & Gore, 2006). In SEM χ2 values
increase as sample sizes (degrees of freedom) increase influencing the model χ2 GOF
(Hair et al., 2006; Kline, 2005). To reduce the sensitivity of χ2 to sample size and
model complexity it has been suggested the χ2 value be divided by the degrees of
freedom (df) resulting in a normed chi-square (NC), a lower value. Although there
are no clear guidelines for minimally acceptable NC values, Bollen (1989)
recommended NC ratios of 2:1, 3:1 or even as high as 5:1 as indicating reasonable
fit. More recently Hair et al. (2006) suggested a χ2/df ratio of 3:1 or less to be
associated with better fitting models. However, SEM models reflect an a priori
theory; χ2 GOF might not be important as a measure of model fit (Hair et al., 2006).
Therefore, in the following analyses if χ2 GOF is significant then NC with a ratio
less than 3:1 was used to determine model goodness-of-fit.
7.6.2 Goodness-of-Fit Index (GFI) The GFI is similar to R2 used in regression to summarise the variance explained in a
dependent variable by the independent variables. In SEM it explains the variance
accounted for in the entire model (Weston & Gore, 2006). It is an absolute fit index
and is less sensitive to sample size or χ2. Possible ranges of GFI values are 0 to 1
with higher values indicating better fit. Generally GFI values of .90 have been
accepted as good, others argue for .95 (Hair et al., 2006). In this study, values greater
than .90 are accepted as indicating good fit of model to data.
211
7.6.3 Adjusted Goodness of Fit Index (AGFI) The AGFI accounts for model complexity by adjusting the GFI by a ratio of the
degrees of freedom used in the model and the degrees of freedom available. The
AGFI penalises complex models in favour of models with the minimum number of
free paths (fewer degrees of freedom). AGFI values from 0 to 1 are generally lower
than GFI in proportion to model complexity, again greater than .90 is accepted as a
good fit of model to data and was used in this study (Hair et al., 2006).
7.6.4 Comparative Fit Index (CFI) CFI, an incremental fit statistic, is relatively insensitive to model complexity and is a
widely used index (Hair et al., 2006; Weston & Gore, 2006). It assesses the relative
improvement in fit of the model compared with the baseline model (independence
model or null model which assumes zero population covariances among observed
variables). The CFI is normed so that values range from 0 to 1 with higher values
indicating a better fit; values less than .90 are not usually associated with well fitting
models (Hair et al., 2006; Hu and Bentler 1999; Weston & Gore, 2006). Although
values greater than .90 are considered a reasonably good fit of the researcher’s model
to reduce the probability of Type II error with acceptable rates of Type I error CFI
values of .95 and above are used in this study (Hu & Bentler 1999).
7.6.5 Root Mean Square Error Approximation (RMSEA) RMSEA is a parsimony-adjusted index in that its formula includes a measure that
attempts to correct for model complexity and approximates a noncentral χ2
distribution. An added parameter, the non-centrality parameter, measures the degree
of inconsistency of the data with the null hypothesis (Hair et al., 2006; Kline, 2005).
The fit of the researcher’s model is not assumed to be perfect (Hair et al., 2006;
Kline, 2005). In contrast to the preceding, RMSEA is a badness-of-fit index
212
measuring model parsimony. Generally values of .10 or less are acceptable, however,
Hu and Bentler (1999) found RSMEA values of .06 and lower resulted in lower and
acceptable rates of Type II error in simple and complex misspecified models under
both robustness and nonrobustness conditions.
Precision of the RSMEA is assessed by confidence intervals (90%) which provide
additional assistance in evaluation of model fit. A narrow confidence interval
indicates good fit of the RSMEA value in reflecting model fit to the population. If
the lower boundary is less than .05 the model has a close approximate fit; 90%
confidence intervals have a maximum boundary of .10 (Hair et al., 2006). For this
study RMSEA values of .06 and confidence intervals of below .05 to .10 are
accepted as representing close fitting models.
7.7 PREPARATION OF DATA FOR ANALYSIS Prior to analysis, TPB data were recoded to ensure a higher score indicated a
positive, favourable or supportive response representing evidence-based fever
management. Items forming beliefs, norms and perceived control were prepared in
accordance with the TPB (Ajzen, 1991; Ajzen & Fishbein, 1980). Belief indicator
items were created by multiplying the individual’s expectancy and value beliefs,
creating new variables. Subjective norm indicator items were created similarly by
cross-multiplying each individual’s perceived likelihood of a particular individual or
group approving of the behaviour and their motivation to comply with this individual
or group. Perceived behavioural control in fever management decision making (PBC
decision making) indicator items were developed by multiplying each respondent’s
decision making beliefs with their perceptions of the power that making fever
management decision had on managing fever. Perceived behavioural control related
213
to child medication behaviours (PBC child medication behaviour) were created by
multiplying the child’s medication behaviour with its influence on fever
management. As CFA and SEM analyses were to be conducted, belief, norm,
decision making, perceived control child factors and intention items were not
summed.
7.7.1 Management of Missing Data Cases with more than 10% of data missing (10 cases) were excluded from this
analysis leaving a sample of N = 391. The remaining surveys had less than .002% of
data missing completely at random and were included in the analysis (Hair et al.,
2006). On the 14 belief items missing data were replaced with a midpoint response,
indicating a neutral belief. No subjective norm or perceived behavioural control
responses were missing. When participants had indicated a normative response was
not applicable (e.g., they did not have a partner as a referent) this response was
replaced with a median response indicating a theoretically appropriate neutral
normative effect. Two cases had missing data on an intention item; these data were
replaced with the case mean from the other two intention items. Missing
demographic items were replaced prior to SEM analysis. This included replacing
eight age responses with the mean (34), one educational attainment responses with
the median (a degree) and one in experience in the health industry was replaced with
a negative response.
7.7.2 Univariate Normality Testing All variables for inclusion in the analysis were checked for univariate normality
using skewness and kurtosis. Data were not normally distributed on the indicator
items for either independent or dependent latent variables. On 15 of the 19 indicator
items for independent variables, standard deviations were not half the mean and three
214
variables demonstrated positive skewness (greater than + 3.0). Nine items
demonstrated leptokurtic kurtosis (greater than ± 3) (Hair et al., 2006a) with kurtosis
greater than 10 indicating a potential problem on three of these nine items (Kline,
2005). All six outcome indicator variables had standard deviations greater than half
the mean and two demonstrated leptokurtic kurtosis greater than ± 3 (Hair et al.,
2006a). Items with potentially problematic kurtosis were checked for response
congruence and found representative of people who had positive beliefs and practices
in fever management. They did not think fever harmful, administered antipyretics at
39.0ºC to 40.0ºC or did not have a specific temperature at which they administered
antipyretics. These cases represented logical, valid responses from the sample
population and were not removed (Weston & Gore, 2006).
In an attempt to improve univariate normality, square root transformations were
calculated. This is an appropriate method to correct positive skewness (Tabachnick
& Fidell, 2007). Following transformation three belief indicator items retained
minimal leptokurtic kurtosis 3.0, 4.0 and 4.1. As the transformed data did not
demonstrate skewness or extreme kurtosis the transformed data were used in the
following modelling.
7.7.3 Issues Due to Nonnormality There is conflicting information about the effect on nonnormal data in SEM. Hair et
al. (2006) report that in large samples, 250 or greater, violations of univariate
normality have little impact and acceptance of a misspecified model is less likely
when CFI is .95 or higher and standardised root mean residual (SMRS) greater than
.06. SMRS is a badness-of-fit statistic measuring the differences between the
standardised sample variances and covariances with model estimated variances and
215
covariances (Hair, et al., 2006). Although SMRS was not available in the statistical
package used for the analysis, AMOS 6 (Arbuckle, 2005), a similar badness of fit
index, RSMEA was available and was defined earlier. A complex analysis of
conventional and new GOF indices by Hu and Bentler (1999) found that when
RSMEA was less than .05 (or .06) and SRMR less than .06 (.07, .08, .09, .10 or .11)
reasonable proportions (94% to 100%) of misspecified models were rejected.
Additionally, combinations of RSMEA less than .06 and SMRS less than .09 (or .10)
resulted in the least number of Type I and Type II error rates. Bentler (1990) reported
large χ2 and underestimated CFIs to be problems with nonnormally distributed data
in SEM. However, modifying hypothesised models to gain a better χ2 fit of the model
to the data is not recommended as SEM tests predetermined, a priori models.
Modifying theoretical hypotheses could lead to inappropriate non-replicable
modifications in otherwise theoretically adequate models (Byrne, 2001). Models
tested in this study were theoretically sound therefore CFI of .95 or greater, RMSEA
of .06 or less were used to determine model fit.
Another method of accommodating nonnormality is bootstrapping (Yung & Bentler,
1996). Bootstrapping creates multiple sub-samples from an original database and
compares the parametric values over repeated samples drawn with replacement from
the original sample. Bootstrapping allows for the estimation of parameters, standard
errors, and model test statistics to be tested in empirical sampling distributions from
large numbers of generated samples (Kline, 2005; Yung & Bentler, 1996). Bootstrap
estimates are less biased than maximum likelihood estimates when underlying
distributions are nonnormal (Byrne, 2001). In the following analysis 1000 bootstrap
samples automatically generated in AMOS 6 were drawn to determine model fit.

216
In summary, with consideration of the normality issues and complexity of the models
the analyses were conducted using maximum likelihood estimation with
bootstrapping (1000). Model fit to data will be estimated using NC less than 3:1
ratio, GFI greater than .90, AGFI greater than .90, CFI greater than .95 and RMSEA
of .06 or less. Although χ2GOF will be reported in the findings it will not be used as
the method of determining statistical fit of the models to the data.
7.8 RESULTS
7.8.1 Bivariate Exploration of Demographics Initially relationships between demographic variables of those included in the
theoretical analysis (N = 391) were explored through bivariate correlations using
Pearson’s r. Age was significantly correlated with educational attainment (r = .29, p
< .01), number of children (r = .24, p < .01) and experience in the health industry (r
= .19, p < .01). Educational attainment was significantly correlated with experience
in the health industry (r = .16, p < .01). As age was significantly related to all other
demographics being explored it was removed from the conceptual frameworks.
Demographic variables included in the final conceptual models were educational
attainment, number of children and health industry experience. Theoretical variables
were attitudes, subjective norms, PBC decision making and PBC child medication
behaviour. The re-specified conceptual models are presented in Figures 7.3 and 7.4.
7.8.2 Demographics Respondents (N = 391) were aged between 20 and 52 years (mean 34.5, SD 4.7),
female (97.4%) and in a married or defacto relationship (93.3%). Forty-one (10.5%)
had a child who had experienced a febrile convulsion and nine a child with epilepsy
(2.3%). Nearly one third, 32%, had experience in a health setting (either health
education or worked in a health environment). Most had a university education; two

217
or more children, were born in Australia and lived in a major city. See Table 7.1 for
additional demographic information.
Figure 7.3: Re-specified conceptual model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever, ‘fever model’
There were no statically significant differences between participants based on their
age, educational achievement or employment status. Parents recruited through
advertising were significantly more likely to come from an inner regional area than
those recruited through face-to-face and snowball (p < 0.01 and < 0.01 respectively)
and less likely to come from a major city (p < 0.01) than those recruited through
face-to-face (F[2,383] = 10.642, p < .01). Recruitment method also influenced
number of children with those recruited through advertising significantly more likely
to have fewer children (p < 0.01) than those recruited through face-to-face (F[2,385]
= 6.208, p < .01). Table 7.2 displays additional recruitment information.
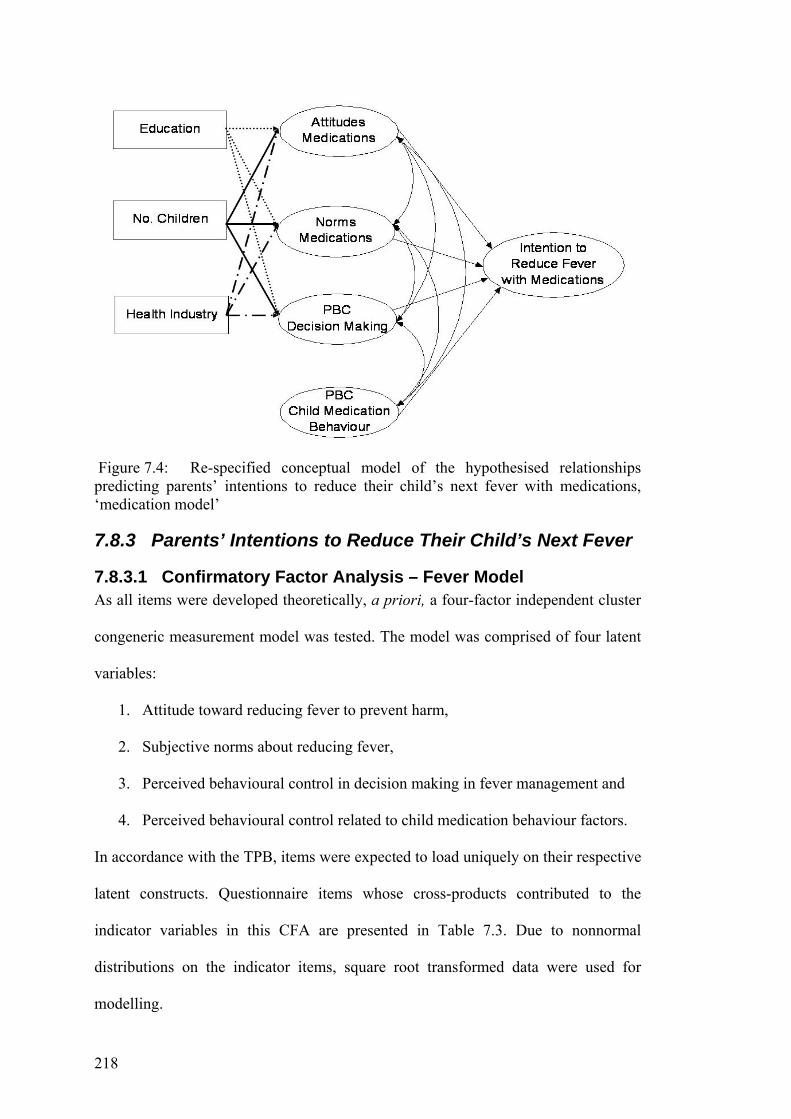
218
Figure 7.4: Re-specified conceptual model of the hypothesised relationships predicting parents’ intentions to reduce their child’s next fever with medications, ‘medication model’
7.8.3 Parents’ Intentions to Reduce Their Child’s Next Fever
7.8.3.1 Confirmatory Factor Analysis – Fever Model As all items were developed theoretically, a priori, a four-factor independent cluster
congeneric measurement model was tested. The model was comprised of four latent
variables:
1. Attitude toward reducing fever to prevent harm,
2. Subjective norms about reducing fever,
3. Perceived behavioural control in decision making in fever management and
4. Perceived behavioural control related to child medication behaviour factors.
In accordance with the TPB, items were expected to load uniquely on their respective
latent constructs. Questionnaire items whose cross-products contributed to the
indicator variables in this CFA are presented in Table 7.3. Due to nonnormal
distributions on the indicator items, square root transformed data were used for
modelling.
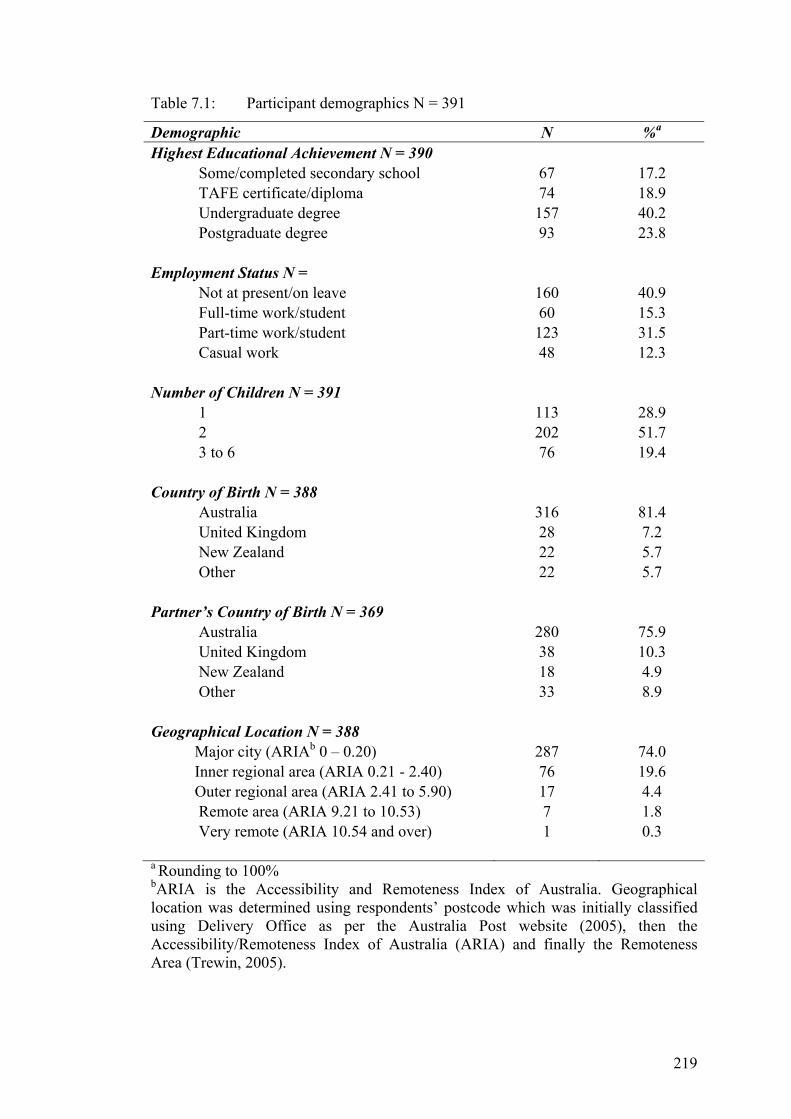
219
Table 7.1: Participant demographics N = 391
Demographic N %a
Highest Educational Achievement N = 390 Some/completed secondary school TAFE certificate/diploma Undergraduate degree Postgraduate degree
67 74 157 93
17.2 18.9 40.2 23.8
Employment Status N = Not at present/on leave Full-time work/student Part-time work/student Casual work
160 60 123 48
40.9 15.3 31.5 12.3
Number of Children N = 391 1 2 3 to 6
113 202 76
28.9 51.7 19.4
Country of Birth N = 388 Australia United Kingdom New Zealand Other
316 28 22 22
81.4 7.2 5.7 5.7
Partner’s Country of Birth N = 369
Australia United Kingdom New Zealand Other
280 38 18 33
75.9 10.3 4.9 8.9
Geographical Location N = 388 Major city (ARIAb 0 – 0.20) Inner regional area (ARIA 0.21 - 2.40) Outer regional area (ARIA 2.41 to 5.90)
Remote area (ARIA 9.21 to 10.53) Very remote (ARIA 10.54 and over)
287 76 17 7 1
74.0 19.6 4.4 1.8 0.3
a Rounding to 100% bARIA is the Accessibility and Remoteness Index of Australia. Geographical location was determined using respondents’ postcode which was initially classified using Delivery Office as per the Australia Post website (2005), then the Accessibility/Remoteness Index of Australia (ARIA) and finally the Remoteness Area (Trewin, 2005).
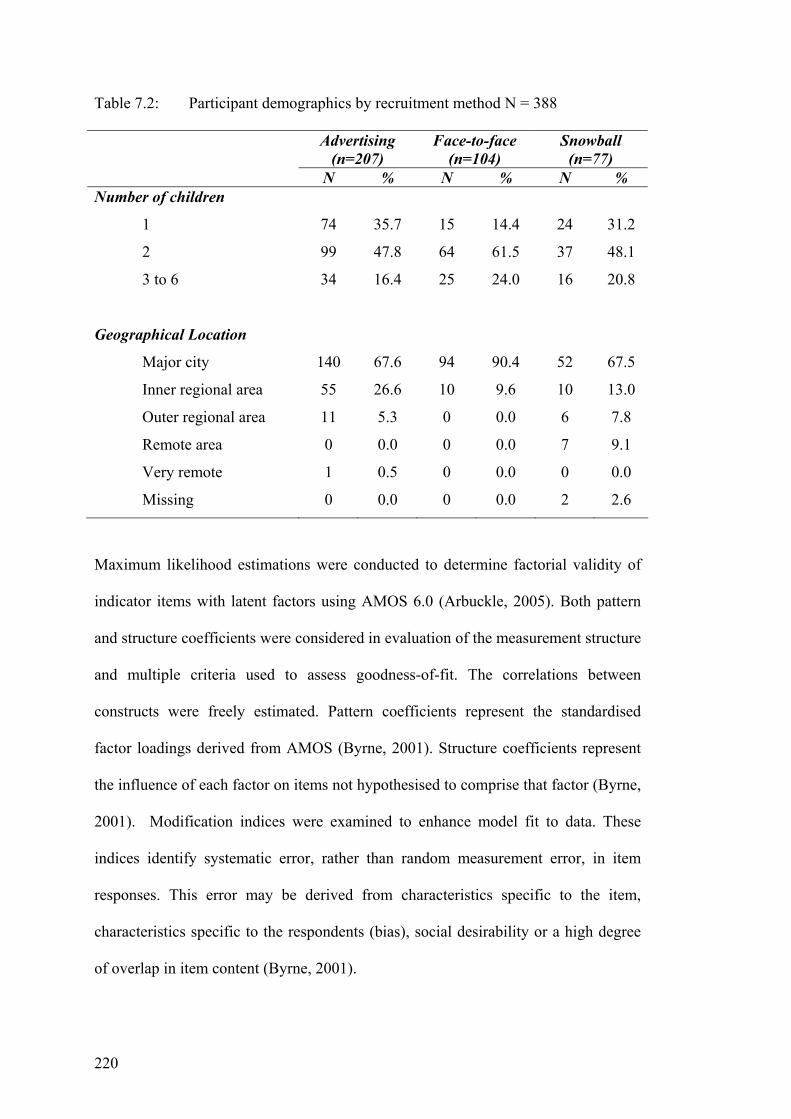
220
Table 7.2: Participant demographics by recruitment method N = 388
Advertising (n=207)
Face-to-face (n=104)
Snowball (n=77)
N % N % N % Number of children
1
2
3 to 6
74
99
34
35.7
47.8
16.4
15
64
25
14.4
61.5
24.0
24
37
16
31.2
48.1
20.8
Geographical Location
Major city
Inner regional area
Outer regional area
Remote area
Very remote
Missing
140
55
11
0
1
0
67.6
26.6
5.3
0.0
0.5
0.0
94
10
0
0
0
0
90.4
9.6
0.0
0.0
0.0
0.0
52
10
6
7
0
2
67.5
13.0
7.8
9.1
0.0
2.6
Maximum likelihood estimations were conducted to determine factorial validity of
indicator items with latent factors using AMOS 6.0 (Arbuckle, 2005). Both pattern
and structure coefficients were considered in evaluation of the measurement structure
and multiple criteria used to assess goodness-of-fit. The correlations between
constructs were freely estimated. Pattern coefficients represent the standardised
factor loadings derived from AMOS (Byrne, 2001). Structure coefficients represent
the influence of each factor on items not hypothesised to comprise that factor (Byrne,
2001). Modification indices were examined to enhance model fit to data. These
indices identify systematic error, rather than random measurement error, in item
responses. This error may be derived from characteristics specific to the item,
characteristics specific to the respondents (bias), social desirability or a high degree
of overlap in item content (Byrne, 2001).
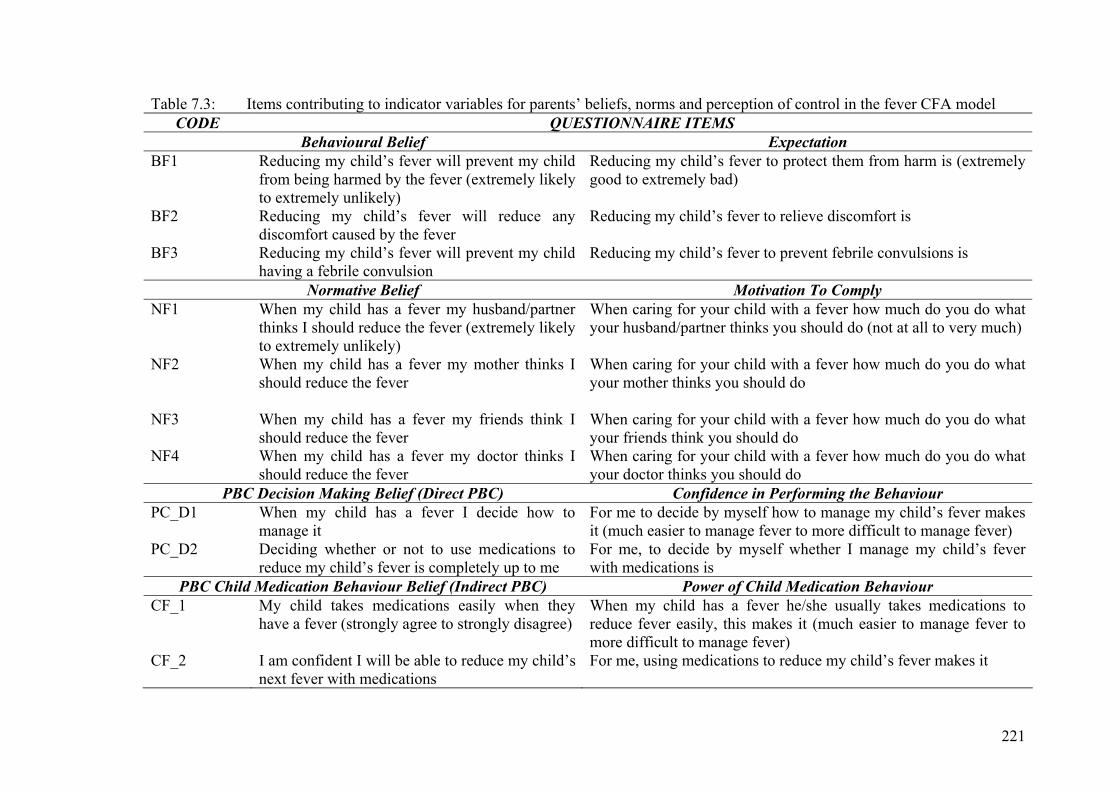
221
Table 7.3: Items contributing to indicator variables for parents’ beliefs, norms and perception of control in the fever CFA model CODE QUESTIONNAIRE ITEMS
Behavioural Belief Expectation BF1 Reducing my child’s fever will prevent my child
from being harmed by the fever (extremely likely to extremely unlikely)
Reducing my child’s fever to protect them from harm is (extremely good to extremely bad)
BF2 Reducing my child’s fever will reduce any discomfort caused by the fever
Reducing my child’s fever to relieve discomfort is
BF3 Reducing my child’s fever will prevent my child having a febrile convulsion
Reducing my child’s fever to prevent febrile convulsions is
Normative Belief Motivation To Comply NF1 When my child has a fever my husband/partner
thinks I should reduce the fever (extremely likely to extremely unlikely)
When caring for your child with a fever how much do you do what your husband/partner thinks you should do (not at all to very much)
NF2 When my child has a fever my mother thinks I should reduce the fever
When caring for your child with a fever how much do you do what your mother thinks you should do
NF3 When my child has a fever my friends think I should reduce the fever
When caring for your child with a fever how much do you do what your friends think you should do
NF4 When my child has a fever my doctor thinks I should reduce the fever
When caring for your child with a fever how much do you do what your doctor thinks you should do
PBC Decision Making Belief (Direct PBC) Confidence in Performing the Behaviour PC_D1 When my child has a fever I decide how to
manage it For me to decide by myself how to manage my child’s fever makes it (much easier to manage fever to more difficult to manage fever)
PC_D2 Deciding whether or not to use medications to reduce my child’s fever is completely up to me
For me, to decide by myself whether I manage my child’s fever with medications is
PBC Child Medication Behaviour Belief (Indirect PBC) Power of Child Medication Behaviour CF_1 My child takes medications easily when they
have a fever (strongly agree to strongly disagree) When my child has a fever he/she usually takes medications to reduce fever easily, this makes it (much easier to manage fever to more difficult to manage fever)
CF_2 I am confident I will be able to reduce my child’s next fever with medications
For me, using medications to reduce my child’s fever makes it

222
In reviewing the modification indices output it was evident that the only
measurement error of any substantial note appeared in the covariances portion of the
output. The largest modification index of 28.88 represented error covariance between
normative influences from mother and friends. Normative means (ranges 1-7)
indicated an unsupportive normative influence; however the means for mother (3.18,
SD 1.24) and friend (3.44, SD 1.17) were more supportive than partner (2.61, SD
1.12) and doctor (2.17, SD 0.99). In this instance there may be a high degree of
overlap in item content or a similar normative influence from these sources, mothers
and friends (Byrne, 2001). If the model was re-estimated with this parameter
specified as free, the overall χ2 would be expected to reduce by 29 and the value of
the estimate itself to reduce by 0.25 (Byrne, 2001). Therefore, the model was
respecified with the error terms for mother and friends allowed to covary.
The resultant model was a good fit to the data in both statistical and practical terms.
GOF indices were χ2(37, N = 391) = 70.26, p = .001, NC 1.90; GFI .97, AGFI .95,
CFI .97 and RMSEA .05 (.03 to .07; 90% CI). The factor structure coefficients for
the estimated parameters are presented in Table 7.4. All indicator variables
demonstrated unidimensional loading onto their respective factors. Loadings ranged
from .48 to .91 and were statistically significant at the .001 level, indicating
discriminant validity. Factor construct reliability was determined by Cronbach’s
Alpha. Reliability of the attitudes toward fever construct was .80, subjective norm in
reducing fever .74, perceived behavioural control (PBC) decision making .78 and
PBC child medication behaviour .65 on the transformed data. See Figure 7.5 for the
CFA fever model. This model demonstrates the relationships between indicator
variables and TPB latent constructs, standardised parameters are reported.
223
Parents’ attitudes toward fever were unfavourable; they believed fever should be
reduced to prevent harm, febrile convulsions and discomfort. Beliefs about reducing
fever to prevent discomfort and febrile convulsions were more unfavourable than
those related to reducing fever to prevent harm, although these were still
unfavourable. Parents perceived the strongest normative influence from doctors, an
unsupportive normative influence; they perceive doctors expected fever to be
reduced and were willing to reduce fever based on this perception. Normative
influences from partners were also unsupportive, though not as extreme as doctors.
Interestingly normative influences in reducing fever from their own mother and
friends were ambivalent, more supportive of evidence-based fever management than
that from doctors and partners. Reports of behavioural control over fever
management were positive. Parents believed making fever management decisions
made fever management easier (direct PBC). When children took medications easily
parents found it easier to manage fever (indirect PBC). See Table 7.4 for the factor
structure of the latent constructs and correlations and descriptives for the indicator
variables in the CFA fever model.
7.8.3.2 Structural Equation Model – Fever Model In accordance with the TPB a five-factor cluster measurement model incorporating
parents’ intentions to reduce the next fever and the four constructs (attitudes, norms,
PBC decision making and PBC child medication behaviours) was tested to explore
relationships between the constructs and intention. Following this a structural model
of parents’ intentions to reduce their child’s next fever was tested. The main purpose
of this analysis was to ensure that the constructs under consideration determined
discriminant validity when intention items were included in the model. The latent
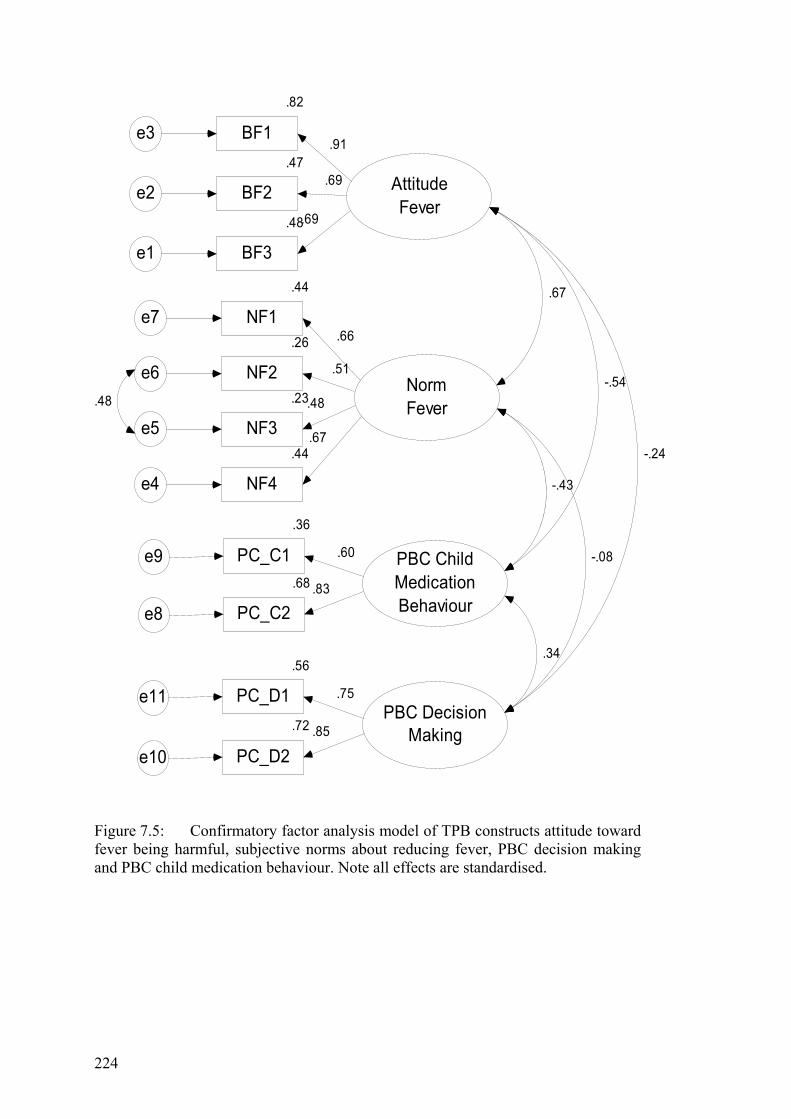
224
AttitudeFever
.48
BF3e1
.69
.47
BF2e2.69
.82
BF1e3.91
NormFever
.44
NF4e4
.23
NF3e5
.26
NF2e6
.44
NF1e7
.67
.48
.51
.66
PBC ChildMedicationBehaviour
.68
PC_C2e8
.36
PC_C1e9
.83
.60
PBC DecisionMaking.72
PC_D2e10
.56
PC_D1e11
.85
.75
.67
-.54
-.24
-.43
-.08
.34
.48
Figure 7.5: Confirmatory factor analysis model of TPB constructs attitude toward fever being harmful, subjective norms about reducing fever, PBC decision making and PBC child medication behaviour. Note all effects are standardised.
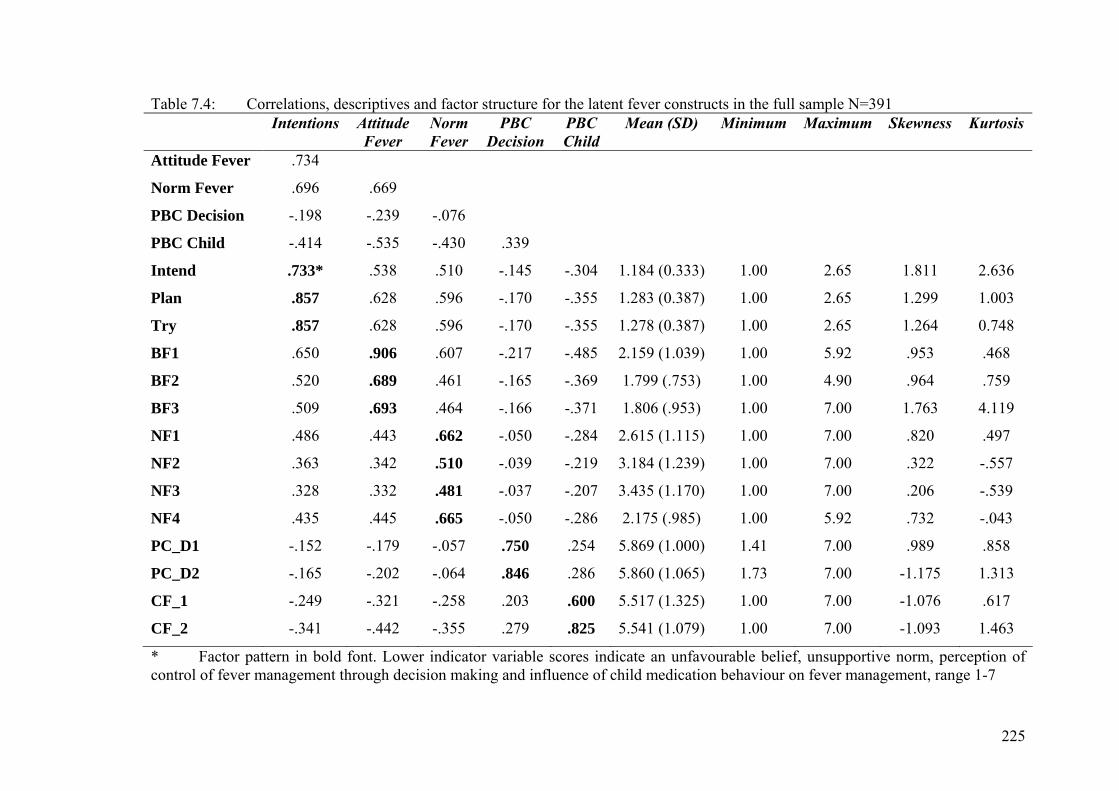
225
Table 7.4: Correlations, descriptives and factor structure for the latent fever constructs in the full sample N=391 Intentions Attitude
Fever Norm Fever
PBC Decision
PBC Child
Mean (SD) Minimum Maximum Skewness Kurtosis
Attitude Fever .734
Norm Fever .696 .669
PBC Decision -.198 -.239 -.076
PBC Child -.414 -.535 -.430 .339
Intend .733* .538 .510 -.145 -.304 1.184 (0.333) 1.00 2.65 1.811 2.636
Plan .857 .628 .596 -.170 -.355 1.283 (0.387) 1.00 2.65 1.299 1.003
Try .857 .628 .596 -.170 -.355 1.278 (0.387) 1.00 2.65 1.264 0.748
BF1 .650 .906 .607 -.217 -.485 2.159 (1.039) 1.00 5.92 .953 .468
BF2 .520 .689 .461 -.165 -.369 1.799 (.753) 1.00 4.90 .964 .759
BF3 .509 .693 .464 -.166 -.371 1.806 (.953) 1.00 7.00 1.763 4.119
NF1 .486 .443 .662 -.050 -.284 2.615 (1.115) 1.00 7.00 .820 .497
NF2 .363 .342 .510 -.039 -.219 3.184 (1.239) 1.00 7.00 .322 -.557
NF3 .328 .332 .481 -.037 -.207 3.435 (1.170) 1.00 7.00 .206 -.539
NF4 .435 .445 .665 -.050 -.286 2.175 (.985) 1.00 5.92 .732 -.043
PC_D1 -.152 -.179 -.057 .750 .254 5.869 (1.000) 1.41 7.00 .989 .858
PC_D2 -.165 -.202 -.064 .846 .286 5.860 (1.065) 1.73 7.00 -1.175 1.313
CF_1 -.249 -.321 -.258 .203 .600 5.517 (1.325) 1.00 7.00 -1.076 .617
CF_2 -.341 -.442 -.355 .279 .825 5.541 (1.079) 1.00 7.00 -1.093 1.463
* Factor pattern in bold font. Lower indicator variable scores indicate an unfavourable belief, unsupportive norm, perception of control of fever management through decision making and influence of child medication behaviour on fever management, range 1-7

226
variable for intention to reduce the next fever (α .85) was represented by three
indicator items with a stem ‘The next time my child has a fever’ and items ‘I will try
to reduce my child’s fever,’ ‘I intend to reduce my child’s fever’ and I plan to reduce
my child’s fever’. See Table 7.4 for intention indicator item correlations and
descriptives. All indicator items loaded significantly on their construct (p ≤ .001) and
all constructs loaded significantly on each other excepting fever norms and PBC
decision making (p = .28). The model was found to fit the data well χ2(66, N = 391)
= 107.20, p = .001, NC 1.62; GFI .96, AGFI .94, CFI .98 and RMSEA .04 (.03 to
.05; 90% CI). See Table 7.5 for correlations of all variables included in the final CFA
fever model.
Table 7.5: Standardised bivariate correlations for TPB constructs – fever model
Attitudes Norms PBC Decision PBC Child
Norms .68
PBC decision -.24 -.08
PBC child -.55 -.42 .34
Intention to reduce fever
.73 .70 -.20 -.41
Consistent with the TPB a structural model hypothesising relationships between
intentions and attitudes, subjective norms and perceived behavioural control was
tested. The model was also explored for demographic influences of educational
attainment, number of children and experience in the health industry on parents’
attitudes, subjective norms and PBC decision making. The model fitted the data well:
χ2 (102, N = 391) = 180.11, df 102, p ≤.000, NC 1.77, GFI .95, AGFI .93, CFI .96,
RMSEA .04 (.03 to .06; 90% CI). The structural model is presented in Figure 7.6.
227
For interpretation of the model, standardised beta weights of .10 and above will be
deemed of practical significance as this area has not been previously explored. Weak
relationships are defined as a standardised beta weight ranging from .10 to .29;
moderate relationships from .30 to .49 and strong relationships from .50 and greater
for this study. With the exception of the pathways from PBC decision making to
intention (β -.07, p = 0.16), attitudes to PBC decision making (β -.18, p = 0.10),
subjective norms to PBC decision making (β .17, p = 0.12) and PBC child factors to
intention (β .03, p = 0.69) all TPB pathways were significant at the 0.05 level.
However, although not statistically significant, attitudes and subjective norms made a
substantive practical contribution to PBC decisions making.
There were some significant, though weak, pathways from demographic variables to
TPB variables (Cohen, 1992). Educational attainment had a significant pathway to
subjective norms (β .12, p = 0.05), attitudes (β .11, p = 0.02) and PBC decision
making (β -.18, p = 0.01). The pathways from experience in the health industry to
subjective norms (β .12, p = 0.05) and number of children to PBC decision making
(β .17, p = 0.01) were also significant. All other pathways from demographic
variables to TPB variables were neither statically nor practically significant. See the
structural model in Figure 7.6 for a clearer presentation of the SEM findings.
The significant statistical and practical contributions discussed here are the
standardised parameters (see Table 7.6). Attitudes had a direct effect on PBC
decision making -.18 (p < 0.001) and parents’ intention to reduce their child’s next
fever .47 (p < 0.001); attitudes total effect on intentions was .40. Subjective norms
had the strongest direct effect on attitudes .53 (p < 0.001) and intention .38 (p <

228
0.001) and a total effect on intention of .62. PBC child medication behaviour factors
had a total indirect effect on intention of -.42, mediated through attitudes (indirect -
.21). Although the direct effect of PBC child medication behaviour factors on
intention was not significant, .03, their total effect on intention was -.41. Educational
attainment had a total effect on intention of .14 mediated through attitudes (indirect
.06, non-significant; direct .11, p < 0.05), subjective norms (direct .12, p < 0.05) and
PBC decision making (direct -.18, p < 0.01). However the total effects of educational
attainment were weak: attitude.17; subjective norms .12; PBC decision making -.19
and intention .14. This model explains 60% of the variance in parents’ intentions to
reduce their child’s next fever. The complete record of the standardised and
nonstandardised effects in the fever SEM is available in the Table 7.6.
Hypothesis 1 postulated that in accordance with the TPB, attitudes, subjective norms
and perceived behavioural control would determine parents' intentions to reduce their
child's next fever and was supported, though some of the influence was indirect.
Hypothesis 2 postulated that PBC child medication behaviours would determine
attitudes, subjective norms and BPC decision making and was supported.
Hypothesis 3 postulated that demographic factors would determine attitudes,
subjective norms and PBC decision making. The postulated hypothesis relating to
educational attainment was supported; educational attainment determined attitudes,
subjective norms and PBC decision making. Hypotheses relating to the number of
children and experience in the health industry were unsupported.

229
Figure 7.6: Structural model of the predictors of parents’ intentions to reduce their child’s next fever, determined through the Theory of Planned Behavior. Note all effects are standardised; block lines indicate a pathway significant at the 0.05 level, dotted lines indicate pathways of practical substantive influence and dashed lines indicate non-significant pathways with limited practical significance. The variation in attitudes, norms, PBC decision making and intentions are included.
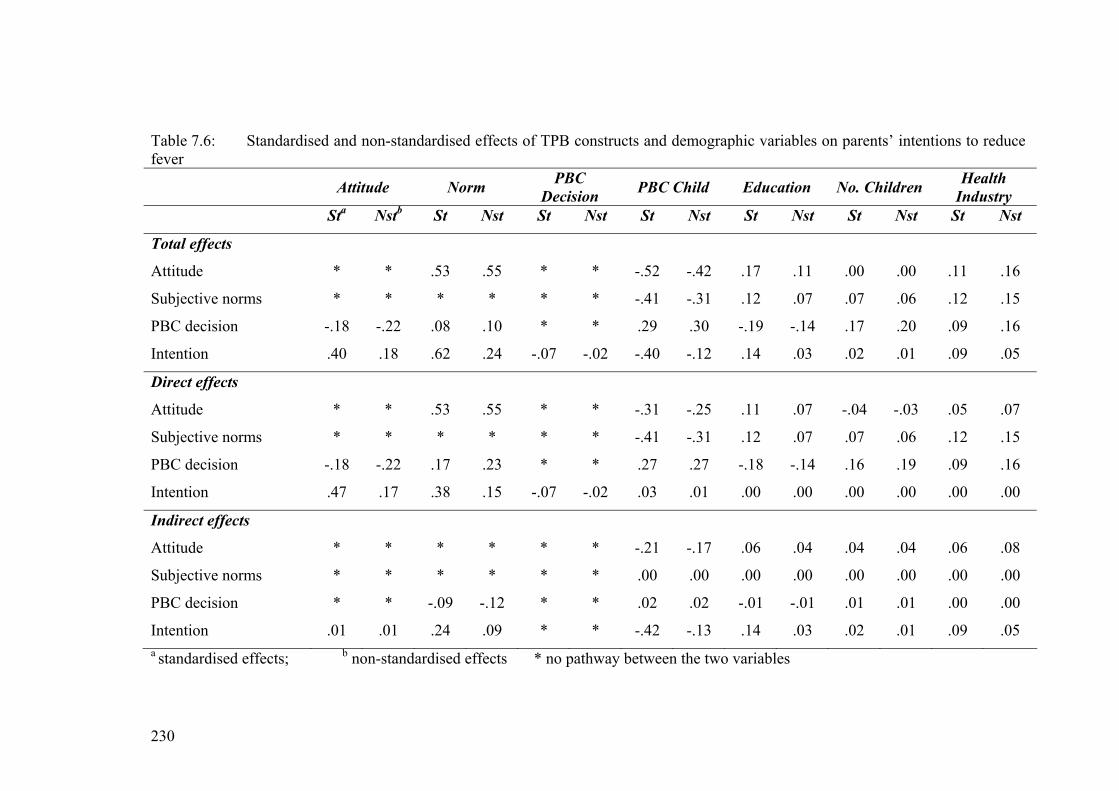
230
Table 7.6: Standardised and non-standardised effects of TPB constructs and demographic variables on parents’ intentions to reduce fever
Attitude Norm PBC Decision PBC Child Education No. Children Health
Industry Sta Nstb St Nst St Nst St Nst St Nst St Nst St Nst
Total effects
Attitude * * .53 .55 * * -.52 -.42 .17 .11 .00 .00 .11 .16
Subjective norms * * * * * * -.41 -.31 .12 .07 .07 .06 .12 .15
PBC decision -.18 -.22 .08 .10 * * .29 .30 -.19 -.14 .17 .20 .09 .16
Intention .40 .18 .62 .24 -.07 -.02 -.40 -.12 .14 .03 .02 .01 .09 .05
Direct effects
Attitude * * .53 .55 * * -.31 -.25 .11 .07 -.04 -.03 .05 .07
Subjective norms * * * * * * -.41 -.31 .12 .07 .07 .06 .12 .15
PBC decision -.18 -.22 .17 .23 * * .27 .27 -.18 -.14 .16 .19 .09 .16
Intention .47 .17 .38 .15 -.07 -.02 .03 .01 .00 .00 .00 .00 .00 .00
Indirect effects
Attitude * * * * * * -.21 -.17 .06 .04 .04 .04 .06 .08
Subjective norms * * * * * * .00 .00 .00 .00 .00 .00 .00 .00
PBC decision * * -.09 -.12 * * .02 .02 -.01 -.01 .01 .01 .00 .00
Intention .01 .01 .24 .09 * * -.42 -.13 .14 .03 .02 .01 .09 .05 a standardised effects; b non-standardised effects * no pathway between the two variables
231
7.8.3.3 Interpretation and Discussion of the Results In accordance with the TPB, intentions to reduce fever were directly determined by
attitudes and normative influences and indirectly by PBC child medication
behaviours, mediated through attitudes and subjective norms (Ajzen, 2005). Sixty
percent of the variance in parents’ intentions to reduce their child’s next fever was
explained by unfavourable attitudes, unsupportive subjective norms, positive PBC
child medication behaviours, lower educational level and having experience in the
health industry. Figure 7.6 and Table 7.6 explain these effects in more detail. Neither
PBC decision making nor the number of children parents have made a statistical or
practical significance contribution to intentions to reduce fever. Parents who 1)
believed fever should be reduced to prevent harm and that 2) others expected them to
reduce fever or 3) had children compliant with medications, making it easier for
parents to manage fever, were more likely to intend to reduce their child’s next fever.
Additionally, those with lower education levels (secondary and TAFE) or health
industry experience were more likely to intend to reduce their child’s next fever.
Attitudes Queensland parents, similarly to their international counterparts, reported negative
attitudes toward fever and reduced fever to prevent febrile convulsions, discomfort
and harm (e.g., Al-Eissa, Al-Sanie et al., 2000; Crocetti et al., 2001; Sarrell et al.,
2002; Schmitt, 1980). See Table 7.4. Beliefs related to febrile convulsions and
discomfort were more negative than those toward harm indicating specific reasons
for reducing fever. Fever phobia and undue concerns about negative outcomes from
fever have been reported for decades (e.g., Crocetti et al., 2001; Sarrell et al., 2002;
Schmitt, 1980). Concerns about febrile convulsions have increased over the past 25
years and are now parents’ main concern during febrile episodes (Al-Eissa, Al-Sanie

232
et al., 2000; Al-Eissa, Al-Zamil et al., 2000; Crocetti et al., 2001; Karwowska et al.,
2002). Interestingly parents were similarly concerned about preventing discomfort
indicating a strong desire to protect their child from harm, however, fever does not
cause discomfort (Kramer, Naimark, Roberts-Brauer, McDougall, & Leduc, 1991).
Similar influences from febrile convulsions and discomfort is worrying and parents
reporting these beliefs reported stronger intentions to reduce fever. Concern about
discomfort could reflect parents’ protective role, protecting their child from harm, to
reduce the burden of childhood illness on the family (Lagerlov et al., 2003) or a
lifestyle choice, preventing interference in family life (Allotey et al., 2004). This
requires further exploration to identify parents’ rationales for reducing fever to
prevent discomfort.
Fifty-four percent of the variance in parents’ attitude was explained by subjective
norms, PBC child medication behaviours, educational level and health industry
experience. The overall influence of subjective norms and PBC child medication
behaviours on attitudes was strong. PBC child medication behaviours both directly
and indirectly influenced attitudes, mediated through subjective norms. Background
factors of educational level and health industry experience had statistically
significant, though weak influences on attitudes. Parents, believing others expected
them to reduce fever, with children compliant with medications, lower educational
levels and health industry experience were more likely to believe fever should be
reduced to prevent harmful outcomes (unfavourable attitudes). Results from some
studies indicate lower educational levels make attitudes toward fever less favourable
(Impicciatore et al., 1998), conversely others studies found no difference in attitudes
when educational level was explored (Crocetti et al., 2001; Kramer et al., 1985;
233
Singhi et al., 1991). The majority of parents in this study had a university education;
this could cause a positive bias making attitudes toward fever more favourable
reducing the influence of education on attitudes.
The negative influence of health industry experience on attitudes has not been
reported. Conceptually, this experience should have a positive influence on attitudes;
these parents should have been exposed to evidence-based information and practices.
The negative influence from health industry experience, found in this model,
indicates the need for further exploration of this phenomenon. Findings confirm
literature reports of health professionals’ negative or unfavourable attitudes toward
fever (e.g., Karwowska, et al., 2002; Poirier, et al., 2000; Walsh, et al., 2004, Wright
& Liebelt, 2007). The strength of the influence of health professionals’ unfavourable
attitudes on those working in a health setting needs exploring.
Interestingly, when PBC child medication behaviours were negative, children were
non-compliant with medications or medication administration did not make it easier
to manage fever, attitudes toward fever were more favourable. This suggests that as
parents have positive experiences with fevers, when fever is not reduced by
medications because their child refused the medication, unfavourable beliefs about
fever, that it is harmful, reduce. The influence of PBC child medication behaviours
on attitudes is understandable. When medication administration does not make it
easier to manage fever and there are no negative outcomes from fever, then parents’
negative beliefs are challenged. With repeated similar experiences and challenges
attitudes become more favourable; parents are less likely to believe that fever must
be reduced. A comment from a parent in Study 1 (Chapter 5) highlights the influence
234
of experience on beliefs. Beliefs that temperatures of 38.0ºC cause febrile
convulsions changed after the child had a temperature of 40.0ºC and did not convulse
(Walsh et al., 2007a). This implies a change in accessible beliefs and/or evaluation of
beliefs leading to attitude change.
The role of knowledge as an antecedent of attitudes has been recognised for many
years (Fishbein, 1963). As parents acquire new information, children refusing
medications were unharmed by fever, their subjective evaluation of the attributes of
fever changes subsequently altering attitudes toward fever (Fishbein & Ajzen, 1972).
Therefore, if parents can be encouraged to appropriately defer medication
administration, their attitudes toward fever being harmful may change, becoming
more favourable. The role of education, health professional support and reassurance
to alter the unfavourable beliefs held by parents about fever is evident. Additionally,
as doctors were a significant referent for parents’ fever management decisions,
support for medication delay from doctors should have a positive influence on both
attitudes and subjective norms, making them more supportive of evidence-based
fever management.
Subjective Norms Subjective norms were unsupportive of fever being beneficial (see Table 7.4).
Parents perceived a normative influence from their main referents to reduce fever.
Interestingly, normative influences from their partner and doctors were more
unsupportive than those from their own mothers and friends. Although the influences
from referents had a moderate direct effect on intentions they made the strongest
overall effect on intentions mediated through attitudes and PBC decision making.
Those who perceived a normative influence from referents to reduce fever and were
235
motivated to comply with this perceived influence were more likely to intend to
reduce their child’s next fever.
Twenty percent of the variance in subjective norms was explained by moderate
influences from PBC child medication behaviours and weak influences from
educational attainment, experience in the health industry and PBC decision making.
Parents who reported positive PBC child medication behaviours reported greater
influence from unsupportive norms. Conversely when PBC child medication
behaviours were negative (non-compliance or medications did not made it easier to
manage fever) parents reported more supportive normative influences on intentions.
Those with lower educational levels or who had experience in the health industry
reported greater influence from unsupportive norms to reduce fever.
Childhood fever management is an emotional issue motivated by fear of harmful
outcomes (e.g., Crocetti et al., 2001; Sarrell et al., 2002). Parents perceived doctors,
partners, mothers and friends expected fever to be reduced, with greater influence
from doctors and partners. Fever is a common symptom for which parents seek
medical advice (Goldman et al., 2004; McErlean et al., 2001). Most fevers are not
serious; serious illness occurs in less than 10 percent of cases (Knoebel et al., 2002;
McCarthy, 1999). Reducing fever reduces concerns about harmful outcomes from
fever; this in turn reduces inappropriate health service usage (Impicciatore et al.,
1998; Robbins, Hundley, & Osman, 2003). The negative influence from experience
in the health industry confirms this to some degree; doctors were a significant
referent, an unsupportive referent. In health settings children are often unwell and the
association between febrile illnesses and febrile convulsions is much higher than the

236
general population (19% versus 5%) (Edwards et al., 2003). The combination of
these explains, to some extent, the unsupportive normative influence of this
experience. A normative influence from partners is understandable. Partners share
the concerns and protective role of the parent who responded to the survey. Other
contributing factors to the strong normative influence from referents possibly include
media reports of dire outcomes from missed diagnoses of febrile illnesses, higher
parental awareness of, and concern about, febrile convulsions and learning to manage
fever from these referents (e.g., Crocetti et al., 2001; Karwowska et al., 2002; Walsh
et al., 2007a; Wright & Liebelt, 2007).
Generally, attitudes or perceived behavioural control, not subjective norms, are the
strongest predictors on intention (Ajzen, 2005). The strong normative influence
found in this study is important, particularly when health professional
recommendations and use of antipyretics for fever management is considered (e.g.,
Edwards et al., 2001; May & Bauchner, 1992; Mayoral et al., 2000; Waterston,
2002). There is an urgent need for further exploration to identify specific normative
influences parents working in health settings receive and then steps can be taken to
correct the situation. In this study, the strength of normative influences on intention
could explain the lack of influence from PBC decision making.
PBC Decision Making PBC decision making was positive. Parents believed deciding how to manage fever
made managing fever easier (see Table 7.4). Conceptually, controlling fever
management decision making would influence fever management intentions ‘If I
decide how to manage fever I will either intend or not intend to reduce fever based
on my attitudes and normative influences’. However, PBC decision making made

237
neither a statistical nor practical contribution to intentions. Contributions to PBC
decision making from other variables were weak. Variance in PBC decision making
(18%) was explained by attitudes, subjective norms, PBC child medication
behaviours, educational attainment and number of children. PBC child medication
behaviours made the greatest, though weak, contribution.
Although weak, the influence from multiple variables on parents’ fever management
decision making indicates this to be a complex issue. Parents who held more
favourable attitudes, perceived others to expect fever to be reduced and had a child
compliant with medication administration reported stronger beliefs that making fever
management decisions makes it easier to manage fever. Those who have lower
education levels or more than one child also reported believing that having control
over fever management decisions made it easier to manage fever.
PBC Child Medication Behaviours PBC child medication behaviours were positive (see Table 7.4). Febrile children’s
compliance with medication administration made it easier to manage fever. Although
this had no direct influence on intentions it had a moderate overall effect on
intentions mediated through attitudes and subjective norms. PBC child medication
behaviours had an overall strong effect on attitudes mediated through subjective
norms. They made a moderate contribution to subjective norms and had a weak
effect on PBC decision making. See Figure 7.6 and Table 7.6 for more detail. Parents
reporting positive PBC child medication behaviours reported less favourable
attitudes, fewer supportive normative influences and higher perceptions that
controlling fever management decision making makes it easier to manage fever.
Alternatively, when children either did not take medications or although taking

238
medications, it did not make it easier to manage fever, reported more favourable
attitudes toward fever and more supportive normative influences.
This model identified the significant influence of indirect controlling factors, child
medication behaviour, on attitudes and subjective norms and intentions. When
children take medications easily parents intend to reduce fever. This association has
been discussed previously. The influence of experience on fever management beliefs
and intentions requires further exploration. There were similar influences from both
indicator variables in PBC child medication behaviours, which need further
exploring, possibly as individual direct items; child compliance with medications and
using medications makes it easier to manage fever.
7.8.3.4 Summary Parents’ intentions to reduce their child’s next fever were greater when they reported
unfavourable attitudes, unsupportive normative influences and child compliance with
medications making it easier to manage fever. Parents with higher educational levels
and/or experience in the health industry intended to reduce fever. In this model an
unsupportive normative influence from partners, doctors, mothers and friends had the
greatest overall influence on intentions. Child medication behaviour directly
influenced attitudes and subjective norms and had an indirect influence on intentions.
PBC decision making made little contribution to intention.
7.8.4 Parents’ Intentions to Reduce Fever with Medications
7.8.4.1 Confirmatory Factor Analysis – Medications Model An a priori, four-factor independent cluster congeneric measurement model was
tested. The model was comprised of four latent variables:
1. Attitude toward reducing fever with medications to prevent harm,
239
2. Subjective norms about reducing fever with medications,
3. Perceived behavioural control in decision making in fever management and
4. Perceived behavioural control child medication behaviours related to
medication compliance.
In accordance with the TPB, items were expected to load uniquely on their respective
latent constructs. Questionnaire items whose cross-products contributed to the
indicator variables in this CFA are presented in Table 7.7. Due to nonnormal
distributions on the indicator items, square root transformed data were used for
modelling.
In reviewing the modification indices output there was a suggestion that items ‘my
child usually takes medication easily when they have a fever’ and normative
influences from the respondent’s mother cross load. This was not conceptually
probable therefore the covariances were examined. The largest modification index
covariance of 112.05, parameter change .73, indicated a problem with the
measurement error of the above items that might be derived from characteristics
specific to the items, respondents or influenced by social desirability (Aish &
Joreskob 1990). Respecification of the model with these parameters free would
reduce the overall χ2 by 112 and the estimate itself to reduce by .73 (Byrne, 2001).
The model was respecified with these error terms allowed to covary.
When the respecified model was tested the largest modification index of 27.15,
parameter change .25, indicated measurement error covariance between normative
influence from mother and friends. Again differences were present in the normative
means indicating an unsupportive normative influence from partner and doctors and
a neutral to supportive influence from mother and friends (see Table 7.8). In this
240
instance there may be a high degree of overlap in item content or a similar influence
from mother and friends. When the model was respecified and retested with these
error terms allowed to covary no further measurement errors were indicated. The
model was a good fit to the data χ2(46, N = 391) = 116.85, p ≤ .001, NC 2.54, GFI
.95, AGFI .92, CFI .96, RMSEA .06 (.05 to .08; 90% CI). Table 7.8 presents the
factor structure of the latent constructs and correlations and descriptives for the
indicator variables in the CFA medication model and Figure 7.7 a diagrammatic
presentation of the CFA medications model.
Parents’ attitudes toward reducing fever with medications were unfavourable when
considered against the latest scientific evidence. They believed fever should be
reduced with medications to prevent harm, febrile convulsions, discomfort and
listlessness. Again the strongest unfavourable beliefs relate to discomfort and febrile
convulsions. Strong unsupportive normative influences from doctors were again
evident with those from partners, mothers and friends similar to those in the fever
model. Parents’ perceived referents expected fever to be reduced with medications.
The same PBC constructs are used in both models. As expected, correlations
between standardised constructs differed according to the model. In the medication
model there was a weaker relationship between subjective norms and attitudes than
in the fever model (.68 versus .59 respectively) and stronger relations between PBC
child medication behaviour and attitudes in the medication model (-.77 versus -.55).
See Figure 7.7 and Table 7.9 for further information about the medication CFA
model. A comparison between CFA models can be achieved by comparing Figures
7.5 and 7.7 and Tables 7.4 and 7.9.
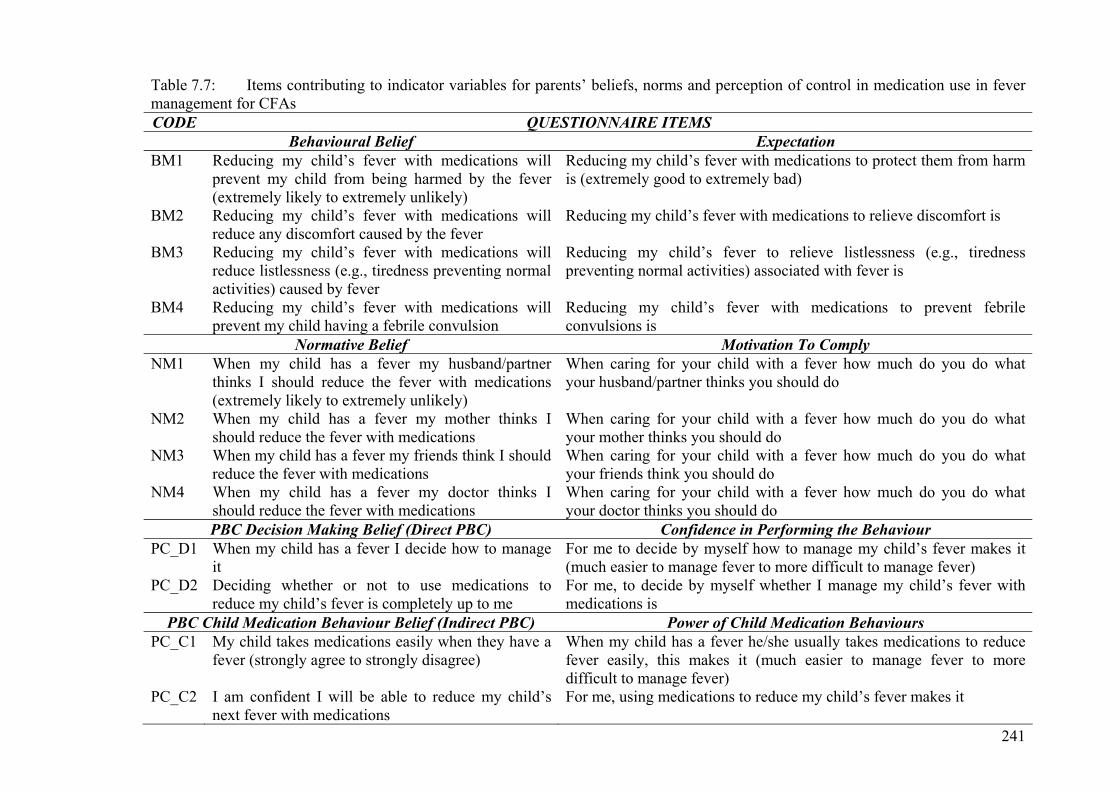
241
Table 7.7: Items contributing to indicator variables for parents’ beliefs, norms and perception of control in medication use in fever management for CFAs CODE QUESTIONNAIRE ITEMS
Behavioural Belief Expectation BM1 Reducing my child’s fever with medications will
prevent my child from being harmed by the fever (extremely likely to extremely unlikely)
Reducing my child’s fever with medications to protect them from harm is (extremely good to extremely bad)
BM2 Reducing my child’s fever with medications will reduce any discomfort caused by the fever
Reducing my child’s fever with medications to relieve discomfort is
BM3 Reducing my child’s fever with medications will reduce listlessness (e.g., tiredness preventing normal activities) caused by fever
Reducing my child’s fever to relieve listlessness (e.g., tiredness preventing normal activities) associated with fever is
BM4 Reducing my child’s fever with medications will prevent my child having a febrile convulsion
Reducing my child’s fever with medications to prevent febrile convulsions is
Normative Belief Motivation To Comply NM1 When my child has a fever my husband/partner
thinks I should reduce the fever with medications (extremely likely to extremely unlikely)
When caring for your child with a fever how much do you do what your husband/partner thinks you should do
NM2 When my child has a fever my mother thinks I should reduce the fever with medications
When caring for your child with a fever how much do you do what your mother thinks you should do
NM3 When my child has a fever my friends think I should reduce the fever with medications
When caring for your child with a fever how much do you do what your friends think you should do
NM4 When my child has a fever my doctor thinks I should reduce the fever with medications
When caring for your child with a fever how much do you do what your doctor thinks you should do
PBC Decision Making Belief (Direct PBC) Confidence in Performing the Behaviour PC_D1 When my child has a fever I decide how to manage
it For me to decide by myself how to manage my child’s fever makes it (much easier to manage fever to more difficult to manage fever)
PC_D2 Deciding whether or not to use medications to reduce my child’s fever is completely up to me
For me, to decide by myself whether I manage my child’s fever with medications is
PBC Child Medication Behaviour Belief (Indirect PBC) Power of Child Medication Behaviours PC_C1 My child takes medications easily when they have a
fever (strongly agree to strongly disagree) When my child has a fever he/she usually takes medications to reduce fever easily, this makes it (much easier to manage fever to more difficult to manage fever)
PC_C2 I am confident I will be able to reduce my child’s next fever with medications
For me, using medications to reduce my child’s fever makes it

242
7.8.4.2 Structural Equation Model – Medication Model Prior to testing the structural model a five-factor cluster measurement model of all
constructs was evaluated to ensure constructs under consideration demonstrated
discriminant validity. The latent factor for intentions to reduce fever with
medications (α = .93) was represented by a cluster of three indicator variables with a
stem “The next time my child has a fever” and items ‘I will try to reduce my child’s
fever with medications’, ‘I intend to reduce my child’s fever with medications’ and ‘I
plan to reduce my child’s fever with medications’. All indicator variables loaded
significantly on to their construct indicating construct validity. The model was a
good fit to the data χ2(78, N = 391) = 170.35, p ≤ 0.001, NC 2.18, GFI .95, AGFI .92,
CFI .97, RMSEA .06 (.04 to .07; 90% CI). Correlations for all TPB constructs
included in the final medication CFA model are presented in Table 7.8.
Table 7.8: Standardised bivariate correlations for TPB constructs medication model Attitudes Norms PBC
Decision PBC Child
Norms .59
PBC decision -.18 -.10
PBC child -.77 -.49 .36
Intention to reduce fever with medications
.74 .70 -.19 -.70
Again a TPB structural model hypothesising the relationships between intentions and
attitudes, subjective norms, PBC decision making and PBC child medication
behaviours, educational attainment, number of children and experience in the health
industry was tested. The model was a reasonable statistical fit to the data and a good
practical fit with a χ2 (117, N = 391) = 253.185, p ≤ .001, NC 2.16, GFI .93, AGFI
.90, CFI .96, RMSEA .06 (.05 to .06; 90% CI). The model was interpreted using the
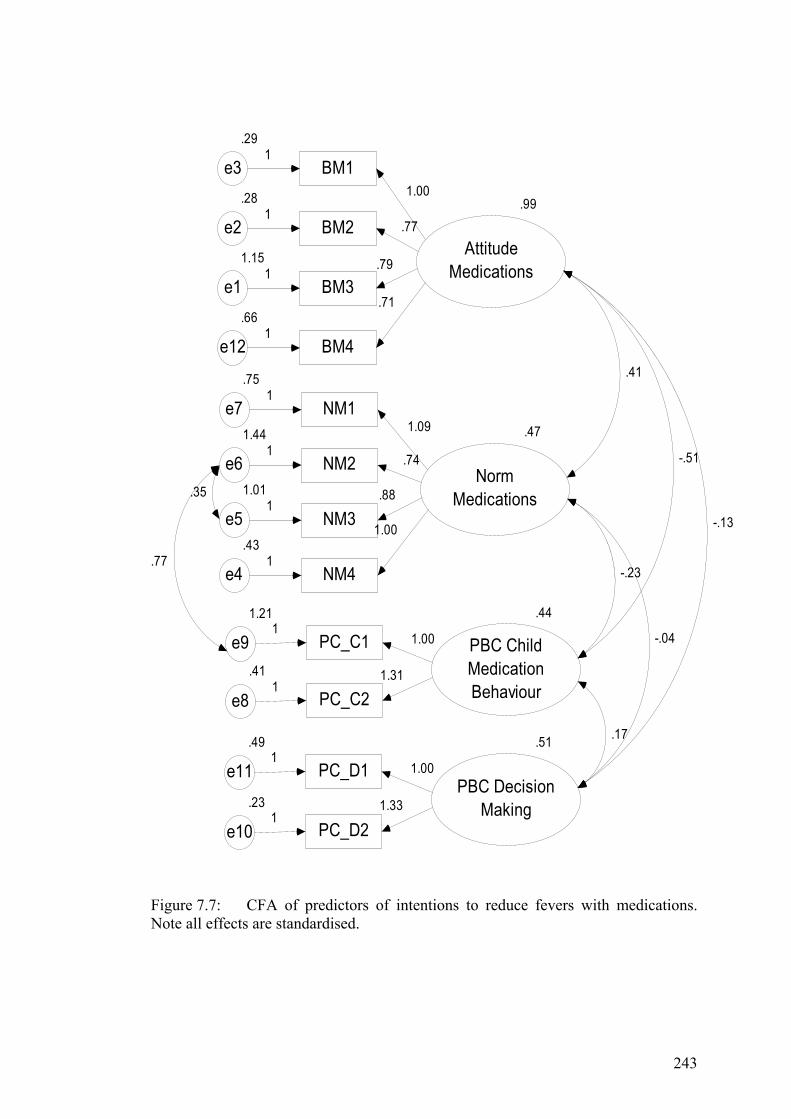
243
.99
AttitudeMedications
BM3
1.15
e1.79
1
BM2
.28
e2 .771
BM1
.29
e31.00
1
.47
NormMedications
NM4
.43
e4
NM3
1.01
e5
NM2
1.44
e6
NM1
.75
e7
1.00
1
.881
.741
1.09
1
.44
PBC ChildMedicationBehaviourPC_C2
.41
e8
PC_C11.21
e9
1.311
1.001
.51
PBC DecisionMaking
PC_D2.23
e10
PC_D1.49
e11
1.331
1.001
.41
-.51
-.13
-.23
-.04
.17
BM4
.66
e12
.71
1
.77
.35
Figure 7.7: CFA of predictors of intentions to reduce fevers with medications. Note all effects are standardised.
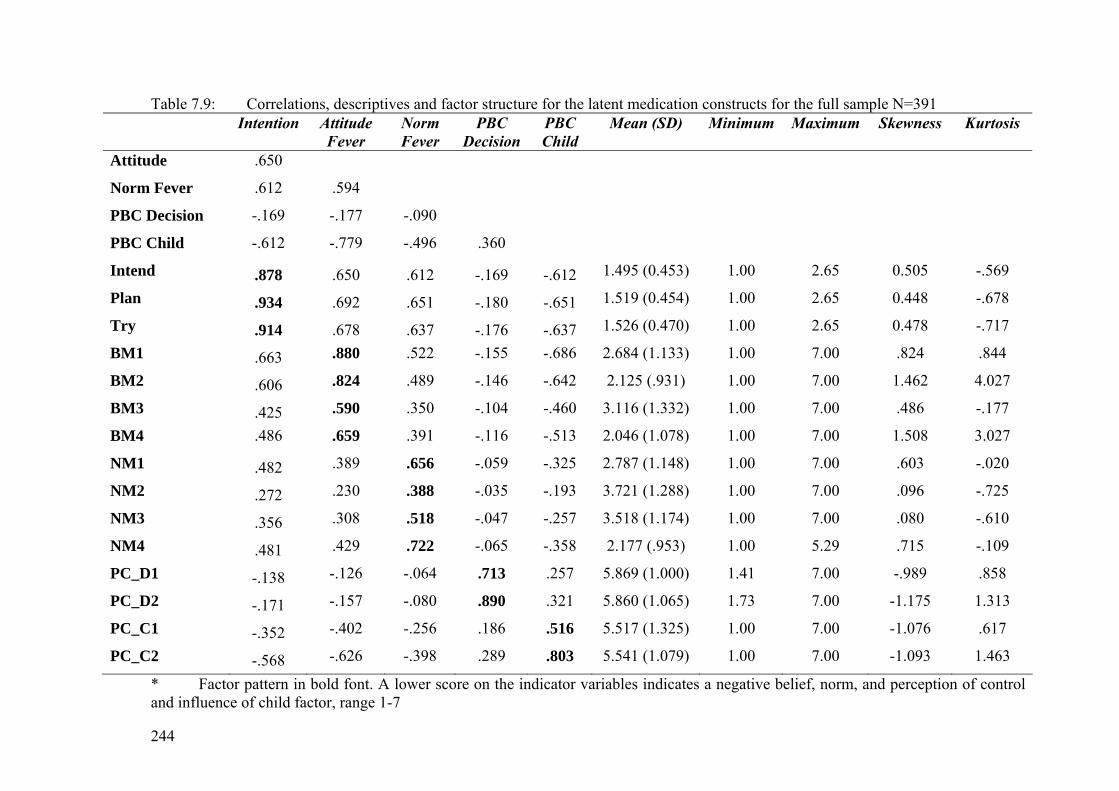
244
Table 7.9: Correlations, descriptives and factor structure for the latent medication constructs for the full sample N=391 Intention Attitude
Fever Norm Fever
PBC Decision
PBC Child
Mean (SD) Minimum Maximum Skewness Kurtosis
Attitude .650
Norm Fever .612 .594
PBC Decision -.169 -.177 -.090
PBC Child -.612 -.779 -.496 .360
Intend .878 .650 .612 -.169 -.612 1.495 (0.453) 1.00 2.65 0.505 -.569
Plan .934 .692 .651 -.180 -.651 1.519 (0.454) 1.00 2.65 0.448 -.678
Try .914 .678 .637 -.176 -.637 1.526 (0.470) 1.00 2.65 0.478 -.717
BM1 .663 .880 .522 -.155 -.686 2.684 (1.133) 1.00 7.00 .824 .844
BM2 .606 .824 .489 -.146 -.642 2.125 (.931) 1.00 7.00 1.462 4.027
BM3 .425 .590 .350 -.104 -.460 3.116 (1.332) 1.00 7.00 .486 -.177
BM4 .486 .659 .391 -.116 -.513 2.046 (1.078) 1.00 7.00 1.508 3.027
NM1 .482 .389 .656 -.059 -.325 2.787 (1.148) 1.00 7.00 .603 -.020
NM2 .272 .230 .388 -.035 -.193 3.721 (1.288) 1.00 7.00 .096 -.725
NM3 .356 .308 .518 -.047 -.257 3.518 (1.174) 1.00 7.00 .080 -.610
NM4 .481 .429 .722 -.065 -.358 2.177 (.953) 1.00 5.29 .715 -.109
PC_D1 -.138 -.126 -.064 .713 .257 5.869 (1.000) 1.41 7.00 -.989 .858
PC_D2 -.171 -.157 -.080 .890 .321 5.860 (1.065) 1.73 7.00 -1.175 1.313
PC_C1 -.352 -.402 -.256 .186 .516 5.517 (1.325) 1.00 7.00 -1.076 .617
PC_C2 -.568 -.626 -.398 .289 .803 5.541 (1.079) 1.00 7.00 -1.093 1.463
* Factor pattern in bold font. A lower score on the indicator variables indicates a negative belief, norm, and perception of control and influence of child factor, range 1-7
245
same criteria as the fever model: standardised beta weights of .10 and above were
deemed of practical significance; weak relationships were defined as a standardised
beta weight ranging from .10 to .29; moderate relationships from .30 to .49 and
strong relationships from .50 and greater. In the medication model there was
practical significance and a trend toward statistical significance between attitudes
and PBC decision making (β .26, p = .07). All other pathways were statistically
significant at the .01 level with the exception of the pathways from subjective norms
to PBC decision making (β .01, p = .91) and intention (β -.01, p = .92).
Again some significant, though weak direct, pathways from demographic variables
to TPB constructs were identified. There was a significant pathway from educational
attainment to attitudes (β .09, p = .03) and PBC decision making (β -.21, p ≤ .01).
The pathways from experience in the health industry to subjective norms (β .15, p =
.01) and number of children to PBC decision making (β .17, p = .01) were also
significant. All other pathways from demographic variables to TPB variables were
neither statistically nor practically significant. See Figure 7.8 for a clearer
presentation of the SEM findings.
The effects of TPB constructs on intention reported here are the standardised effects.
Subjective norms had a moderate total effect on intention .46, directly .38 and
indirectly through attitudes (.28). Attitudes had a moderate direct and total effect on
intention (.30) mediated by PBC decision making (.26). However, PBC decision
making has neither a total or direct effect on intentions (-.01). In this model PBC
child medication behaviours had the strongest total effect (-.70) on parents’
intentions to reduce fever with medications (indirect -.42, direct -.28). These factors
246
were mediated through attitudes (direct -.62) and subjective norms (direct -.49). PBC
child medication behaviours had a strong overall effect on attitudes of -.76, directly -
.62 and indirectly -.14, mediated through subjective norms (direct -.49). Interestingly
few demographic variables had an effect on the constructs of the TPB or parents’
intentions. Educational attainment and experience in a health environment had direct
(-.21 and .17 respectively) and total effect (-.18 and .17 respectively) on PBC
decision making. See Table 7.10 for the standardised and unstandardised effects.
Hypothesis 1 postulated that in accordance with the TPB, attitudes, subjective norms
and perceived behavioural control would determine parents' intentions to reduce their
child's next fever with medications and was supported.
Hypothesis 2 postulated that PBC child medication behaviours would determine
attitudes, subjective norms and BPC decision making and was supported.
Hypothesis 3 postulated that educational attainment, number of children and
experience in the health industry would determine attitudes, subjective norms and
PBC decision making and was unsupported.
7.8.4.3 Interpretation and Discussion of the Results Again predictive constructs of the TPB, attitudes, subjective norms and PBC child
medication behaviour (indirect PBC) predicted parents’ intentions to reduce fever
with medications (Ajzen, 2005). Sixty-eight percent of the variance in intentions to
was determined by unfavourable attitudes, unsupportive subjective norms, positive
PBC child medication behaviours and PBC decision making, having experience in
the health industry, lower educational level and more children.

247
In this model PBC decision making and background factors, educational level,
number of children and health industry experience did not contribute significantly to
parents’ intentions to reduce fever with medications. Figure 7.8 and Table 7.10
explain these effects in more detail. Parents with a child compliant with medication
administration making fever management easier, believed others expected them to
reduce fever with medications and that fever should be reduced with medications to
prevent harm intend to reduce their child’s next fever with medication.
Attitudes Again, attitudes were negative with similar beliefs about reducing fever in relation to
febrile convulsions and discomfort as in the fever model (see Tables 7.4 and 7.8).
Interestingly beliefs about reducing fever with medications to reduce listlessness
were neutral; overall, parents were ambivalent about the effect medications have on
listlessness related to fever. Attitudes toward reducing fever with medications have a
moderate influence on intentions. Parents with unfavourable attitudes who believe
fever should be reduced with medications report greater intentions to reduce their
child’s next fever with medications than those with more favourable attitudes.
The use of medications to reduce fever has increased and is now the preferred
method for most parents with as many as 95% having been reported (Karwowska et
al., 2002). In this study 91% of parents regularly used medications to reduce
temperatures of 38.3ºC ± 0.6ºC, mild fever (Walsh et al., 2007b). Over-the-counter
medication use in childhood is becoming commonplace (Allotey et al., 2004).
Australian parents report using antipyretics not only to reduce pain and fever but to
promote sleep, for mood alteration, babysitting and sending children to school
indicating their use for parental lifestyle factors (Allotey et al., 2004). The reported

248
rates of incorrect antipyretic dosing, 47% to 49%, both under and overdosing
(Goldman & Scolnik, 2004; Li et al. 2000), highlight the need for education about
not only appropriate use but also the correct dosage and frequency. In young children
the dosage is determined by weight; weight can change significantly between febrile
episodes, therefore, the correct dose during the last febrile episode is not necessarily
correct for future febrile illnesses.
Sixty-four percent of the variance in parents’ attitudes was explained by subjective
norms, PBC child factors, level of education, number of children and health industry
experience. Parents who believed others expected them to reduce fever with
medications and had a child who took medications easily, making fever management
easier, or lower educational attainment reported fewer favourable attitudes and
greater intentions to reduce their child’s next fever with medications. As in the fever
model, parents of children who did not take medications easily when febrile, reported
more evidence-based attitudes toward fever and fewer unsupportive normative
influences in fever management; fever does not need to be reduced with medications.
In this model PBC child medication behaviour had a strong influence over attitudes;
the influence of subjective norms on attitudes was moderate.
Subjective norms In the medication model subjective norms were unsupportive of evidence-based
fever management (see Table 7.8). Again, the least supportive normative influences
were from doctors. Parents who reported negative normative influence from doctors
(fever should be reduced with medications) intended to reduce their child’s next
fever with medications more frequently than those reporting more supportive norms
from doctors. Twenty-seven percent of the variance in subjective norms was
249
explained by PBC child medication behaviours, health industry experience, number
of children and educational level. The overall influence on intentions from referents
was stronger than that from attitudes (.46 versus .30). In this model PBC child
medication behaviours were again the strongest influence on subjective norms.
Health industry experience was the only background factor significantly influencing
intentions.
The literature abounds with reports of doctors advising parents to reduce fever with
medications and alternate medications to maintain fever reduction (Del Vecchio &
Sundel, 2001; May & Bauchner, 1992; Mayoral et al., 2000; Wright & Liebelt,
2007). It is therefore not surprising parents believe doctors expect fever to be
reduced with medications. Parents participating in the qualitative study, Study 1,
sought reassurance from doctors that their fever management practices were correct
and considered them a reliable source of fever management information (Walsh et
al., 2007a). Parents, receiving incorrect information, will intend to reduce fever with
medications in accordance with the advice received from their doctor.
PBC Decision Making Although parents believed making fever management decisions made fever
management easier this again had no significant or practical influence on their fever
management intentions (see Table 7.9). Eighteen percent of the variance in parents’
PBC decision making was explained by their attitudes, subjective norms, PBC child
medication behaviours, educational attainment, number of children and health
industry experience. PBC child medication behaviours, educational attainment and
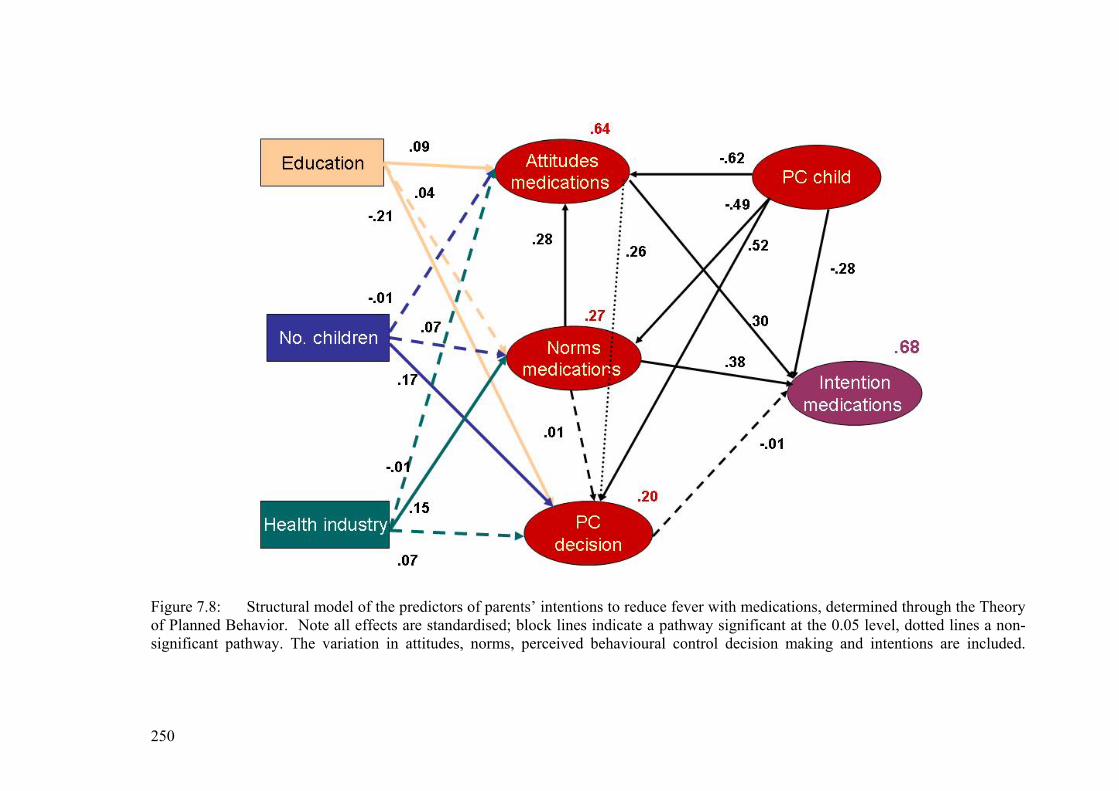
250
Figure 7.8: Structural model of the predictors of parents’ intentions to reduce fever with medications, determined through the Theory of Planned Behavior. Note all effects are standardised; block lines indicate a pathway significant at the 0.05 level, dotted lines a non-significant pathway. The variation in attitudes, norms, perceived behavioural control decision making and intentions are included.
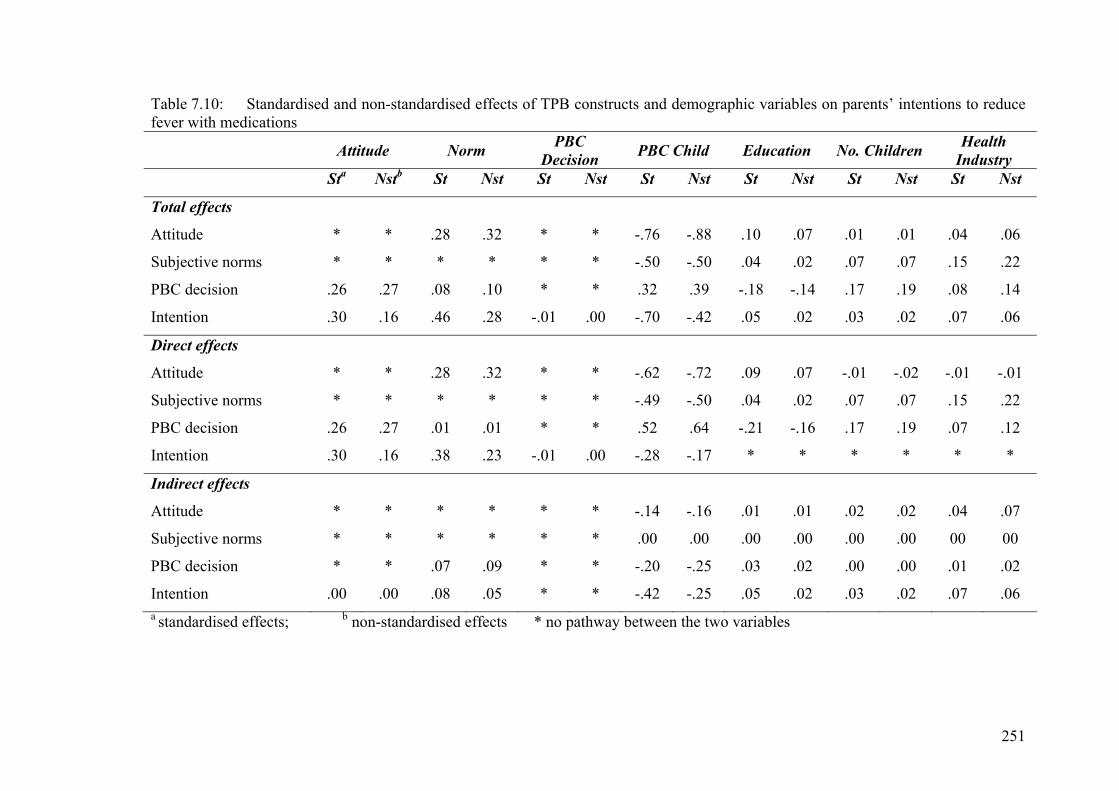
251
Table 7.10: Standardised and non-standardised effects of TPB constructs and demographic variables on parents’ intentions to reduce fever with medications
Attitude Norm PBC Decision PBC Child Education No. Children Health
Industry Sta Nstb St Nst St Nst St Nst St Nst St Nst St Nst
Total effects
Attitude * * .28 .32 * * -.76 -.88 .10 .07 .01 .01 .04 .06
Subjective norms * * * * * * -.50 -.50 .04 .02 .07 .07 .15 .22
PBC decision .26 .27 .08 .10 * * .32 .39 -.18 -.14 .17 .19 .08 .14
Intention .30 .16 .46 .28 -.01 .00 -.70 -.42 .05 .02 .03 .02 .07 .06
Direct effects
Attitude * * .28 .32 * * -.62 -.72 .09 .07 -.01 -.02 -.01 -.01
Subjective norms * * * * * * -.49 -.50 .04 .02 .07 .07 .15 .22
PBC decision .26 .27 .01 .01 * * .52 .64 -.21 -.16 .17 .19 .07 .12
Intention .30 .16 .38 .23 -.01 .00 -.28 -.17 * * * * * *
Indirect effects
Attitude * * * * * * -.14 -.16 .01 .01 .02 .02 .04 .07
Subjective norms * * * * * * .00 .00 .00 .00 .00 .00 00 00
PBC decision * * .07 .09 * * -.20 -.25 .03 .02 .00 .00 .01 .02
Intention .00 .00 .08 .05 * * -.42 -.25 .05 .02 .03 .02 .07 .06 a standardised effects; b non-standardised effects * no pathway between the two variables
252
number of children make a significant contribution to PBC decision making. Parents
reporting unfavourable attitudes reported more frequently that making fever
management decisions makes it easier to manage fever. Parents of children
compliant with medication administration who had lower education levels and more
than one child reported controlling fever management decisions made managing
fever easier.
PBC Child Medication Behaviours Again, PBC child medication behaviours were positive (see Table 7.8); when
children were compliant with medication administration it was easier to manage
fever. In this model PBC child medication behaviours had a direct negative influence
on intentions and very strong overall effect on intentions. When febrile children took
medications easily parents intended to reduce their child’s next fever with
medications more frequently than parents of children who do not take medications
easily. PBC child medication behaviours had a very strong overall influence on
attitudes, mediated through subjective norms, and a strong overall influence on
subjective norms. The moderate influence of PBC child medication behaviours on
PBC decision making was mediated through attitudes and subjective norms. See
Figure 7.8 and Table 7.10.
The strong negative influence of PBC child medication behaviours on attitudes and
subjective norms suggests experience has a significant role in not only attitude
formation (Ajzen, 2005), but also in the influence of subjective norms. When child
non-compliance with medications does not harm the child, have a negative impact on
the child, or make fever management more difficult, then parents’ attitudes toward
fever were more favourable and they report more supportive norms. Parents’

253
perception that others expect them to reduce fever with medications was also weaker.
Additionally, when a child is complaint with medications and this does not make
managing fever easier, then attitudes toward the need to reduce fever with
medications and normative influences become more supportive. The combination of
these factors contributed to fewer reports of intentions to reduce fever with
medications, these parents’ fever management practice was more evidence-based.
The strength of these associations has significant implications for parent education
which will be discussed further in the concluding section of this chapter.
Additionally, the considerable influence of child medication behaviour on attitudes,
norms and intentions is important. This has not been reported elsewhere and is
significant not only in fever management but in the general care of children; it
requires further exploration.
7.8.4.4 Summary Parents intended to reduce their child’s next fever with medications when they
reported unfavourable attitudes, fever must be reduced with medications to prevent
harmful outcomes, perceived unsupportive normative influences from doctors,
partners, mothers and friends, and their child was complaint with medications. Lower
levels of education had a negative influence on attitudes making them less favourable
and a positive influence on PBC decision making. The number of children a parent
has positively influenced PBC decision making. Experience in the health industry
again had an adverse influence on subjective norms making them less supportive. In
this model PBC child medication behaviours made the greatest contribution to
intentions.
254
7.8.5 Integration of Findings This exploratory study, conceptually based on the Theory of Planned Behavior, was
undertaken to identify predictors of parents’ intentions to 1) reduce childhood fever
and 2) reduce childhood fever with medications. TPB constructs were significant
predictors of intentions in both models predicting 60% of the variance in parents’
intentions in the fever model and 68% in the medication model. Model specific
attitudes toward reducing fever to prevent harm and normative influences to reduce
fever predicted intentions in both models highlighting differences in practice
determinants. The greatest contribution to intention also differed by model.
Unsupportive norms about reducing fever were the most significant predictor of
parents’ intentions to reduce fever with more unsupportive norms from partners and
doctors than mothers and friends. In the medication model positive PBC child
medication behaviours (indirect controlling factors) made the greatest contribution.
Both these constructs were mediated through unfavourable attitudes. Both supportive
norms and negative PBC child medication behaviours made attitudes more
favourable and intentions more evidence-based.
The greatest contribution to intentions from subjective norms, in the fever model, is
unusual (Ajzen, 2005). It highlights the important role referents play in determining a
parent’s fever management intentions. Social pressure to conform was strong.
Reliance on others for advice is understandable when parents’ concerns about fever
and fears of harmful outcomes from fever were considered. Unsupportive normative
influences were greatest from doctors and partners. The attitudes of partners could
either concur or conflict with the participant. However, the unfavourable attitudes
and unsupportive norms reported in the study indicate partners possibly have similar
255
attitudes to those who participated. Considering the significant influence from
partners on intentions partners must be included in any educational programs
targeting parents’ evidence-based fever management.
The negative influence from doctors and need for them to update their knowledge
and recommendations in accordance with the latest scientific evidence has been
addressed earlier in this thesis. Queensland doctors’ attitudes and practices have not
been reported though recommendations to reduce fever with medications have
(Pearce & Curtis, 2005). Parents’ perception that doctors expect fever to be reduced
and reduced with medications is understandable and highlights the urgent necessity
for doctors to update their knowledge and recommendations.
Attempts to address parents’ poor knowledge and negative attitudes have been
undertaken over the past few decades and were reported in Chapter 3 (Walsh &
Edwards, 2006). Most education programs reported target knowledge rather than
attitudes or specific practices to reduce unnecessary use of medical services. Despite
this fever continues to be reported as the most frequent reason for seeking medical
advice (Kelly et al., 1996; McErlean et al., 2001). When this is considered in
conjunction with the strength of the unsupportive normative influences from
partners, doctors, mothers and friends to reduce fever it suggests general concerns
about fever not only in health professions but also in the community. The need for
both health professional and community based education is evident when these
findings are considered in relation to other studies.
256
The influence of PBC child medication behaviours on intentions to reduce fever with
medications is of particular importance. It is interesting to note that PBC child
medication behaviours have no direct influence on intentions in the fever model and
only a moderate direct influence on intention in the medication model. On the
perceived behavioural control continuum, PBC child medication behaviours have a
stronger influence on intention in the medication model than the fever model (Ajzen,
2005). This construct was mediated through attitudes and subjective norms in both
models implying parents’ past experiences with fever play a role in their subjective
norms and attitudes. Parents are aware that it can be difficult to manage fever.
Therefore, despite intending to manage fever they are cognisant they may not be
successful irrespective of whether they make fever management decisions and, or,
their child was amenable to taking medications. This could help to explain the non-
significant influence of PBC decision making on intention. Although parents report
making fever management decisions makes it easier to manage fever making these
decisions had no influence on their intentions in either model. This is an important
finding and should be considered when developing educational programs to improve
parents’ fever management.
Perceptions of control explored in this study highlight the incomplete control parents
have on fever reduction. Further exploration of these constructs will assist in
determining the exact influence perceived behavioural control has on fever
management intentions. Do positive experiences with fever irrespective of child
medication behaviour influence attitudes, subjective norms and intentions? How does
being the decision maker influence fever management decisions and intentions?
257
The literature reporting parents’ fever management knowledge, attitudes and
practices and effective educational programs targeting specific knowledge, beliefs
and practices is extensive (see Chapter 3). With the exception of increased
antipyretic use and alternating antipyretics, unnecessary practices that place children
at risk of overdose, little has changed in these during the past three decades (e.g.,
Abdullah et al., 1987; Anderson, 1988; Karwowska et al., 2002; Kramer et al., 1985;
Schmitt, 1980). Specific determinants of parents’ fever management practices or
intentions have not been reported. This study makes a significant contribution to
childhood fever management and the fever management literature through the
identification of the determinants of parents’ intentions. These findings can
effectively direct educational programs targeting not only parents of young children
and their partners but also health professionals and the general public in the benefits
of fever and evidence-based fever management.
7.8.6 Strengths and Limitations This study adds to the literature reporting parents’ fever management as no
theoretically based analysis or predictors of fever management intentions have been
previously reported. A large sample of Queensland parents (N = 391) was recruited
through three recruitment methods to improve generalisability of the findings. The
questionnaire was grounded in data from preliminary findings in the qualitative
study, Study 1, (Walsh et al., 2007a). Additionally, items were specific to the target,
action, context and time elements of the population of interest (Ajzen, 1991; Ajzen &
Fishbein, 1980) increasing content validity and ensuring appropriateness for the
specific population (Blue, 1995). Construct and discriminant validity and reliability
were confirmed through the CFA. There were minimal missing data and the sample
size was fitting for complex structural equation modelling and to minimise the
258
effects from violations of normality (see SEM assumptions and model estimation)
(Kline, 2005).
On the other hand, findings and generalisations should be considered with the
following in mind. The sample was self-selected, mostly females who had a
university education and lived in a major city. Data were self-reported. Raw data
were not normally distributed and some kurtosis remained following square root
transformation. On the other hand, a sample size calculation was conducted prior to
data collection and the sample was larger than required. In addition, all efforts were
made to reduce influence on the analysis from non-Normality (see Assessing Model
Fit and Issues due to non-Normality). Multiple measures of goodness-of-fit statistics
were used to determine model fit to data and good fit was found.
7.8.7 Conclusions The TPB predicted the determinants of parents’ intentions to reduce fever and reduce
fever with medications. Interestingly, the strongest direct predictor of intentions was
not the strongest overall predictor in either model. This is important and highlights
the need for complex analyses of complex behaviours, behaviours which include an
emotional component. Different constructs make the greatest contribution to
intention in the models, subjective norms in the fever model and PBC child
medication behaviours in the medication model. PBC decision making made no
significant contribution to intention in either model. Both perceived behavioural
control constructs require further exploration to determine the specific influences
perceptions of control have over not only intentions but also attitudes and subjective
norms. Caring for a febrile child is a highly emotive experience for parents as is
attempting to medicate a sick child who refuses medications. Parents’ need to protect
their child may influence both perceived behavioural constructs explored in this

259
study. Further studies should explore parents’ emotional involvement during a febrile
illness as well as their behavioural intentions and behaviours. Exploration of moral
and descriptive norms may give more insight into the strong influence of subjective
norms in the fever model.
Parents intended to reduce fever and reduce fever with medications. Intentions were
determined by unfavourable attitudes, unsupportive subjective norms and positive
PBC child medication behaviours. Similar percentages of the variation in intention
were predicted in both models. The significant contribution of subjective norms to
attitudes and intention in both models highlight the strength of parents’ perceived
normative influence to reduce fever and the strength of this influence. Believing
doctors expect fever to be reduced identifies the need for health professionals to
upgrade their knowledge. PBC child medication behaviours contribution to intention
in the medication model was much greater than in the fever model. This requires
further exploration as medications are parents’ preferred method of fever
management. Although demographic factors have some influence on attitudes,
subjective norms and PBC decision making they have a weak overall influence on
intention in the fever model only. However, this may be influenced by sample
homogeneity.
Parents’ intentions and the determinants of intentions in both models highlight the
need for education of both parents and health professionals to reduce the strong
unsupportive normative influences which in turn influence decision making and
intentions. It is imperative health professionals consistently provide evidence-based
information about fever management, not only to parents of young children but to

260
the community as a whole. Identification of an influence on intentions of non-
compliance with antipyretics highlights an unexpected need for parents; the skill to
medicate children when necessary. Doctors order medications for children; they and
other health professionals have an important role in ensuring parents can safely
administer these medications when necessary.

261
CHAPTER 8
INTEGRATION OF FINDINGS AND CONCLUSIONS
8.1 INTRODUCTION The overall aims of this thesis were to identify parents’ knowledge, beliefs, practices
and influences on childhood fever management practices. Specific aims were to:
1. Identify Queensland parents’ knowledge of fever, beliefs about fever, fever
management practices, antipyretic use, influences on practices and sources of
information about fever management. (Study 1 & 2)
2. Develop and trial a comprehensive instrument to explore parents’ childhood
fever management and the influences on fever management practices. (Study
1 & 2)
3. Identify the determinants of parents’ intentions to 1) reduce their child’s next
fever and 2) reduce their child’s next fever with antipyretics through the
Theory of Planned Behavior. (Study 2)
The research is unique in that it provides not only a comprehensive understanding of
parents’ fever management and the underlying factors influencing their practices but
also the determinants of their behavioural intentions though the Theory of Planned
Behavior. This chapter synthesises the key findings and examines their practical
implications for parents and health professionals. Findings from each study have
been discussed in earlier chapters. This final chapter begins with an integration of the
key findings from the two studies and a discussion of the related literature. Following
this the strengths and limitations of the research are presented then the implications
262
of the findings for parents and health professionals are discussed. Finally,
recommendations for future research are made and general conclusions presented.
8.2 INTEGRATION OF KEY FINDINGS Fever was perceived as a negative event by parents in these studies and they also
believe significant others have similar perceptions. Parents believed fever was
harmful, causing febrile convulsions, brain damage, cardiac events or a stroke and
intended to reduce fever to prevent harm. Negative beliefs about fever produced
unfavourable attitudes toward fever and were a significant determinant in parents’
intentions to reduce fever.
Parents’ knowledge about fever and appropriate antipyretic administration was
limited and confounded by negative beliefs. Beliefs about the immunological
benefits of fever were vague in Study 1 and beliefs about harmful outcomes from
fever were prevalent in both studies. Confusion about beneficial effects of fever has
been previously reported. Although considering low grade fevers beneficial parents
reported it necessary to reduce low grade fevers without other symptoms (Sarrell, et
al., 2002). Beliefs about the need to reduce fever to prevent febrile convulsions and
brain damage are common (eg., Crocetti, 2001; Karwowska et al., 2002; Sarrell et
al., 2002) and were reported by participants in both studies. Correct beliefs about
fever causing dehydration (eg., Holtzclaw, 1992; Lorin 1999; Reeves-Swift, 1990;
Schmitt, 1994) were reported in Study 2 and have been reported lately indicating
parents have some evidence-based knowledge about fever (Karwowska et al., 2002).
However, parents in both studies reported that fever indicated a serious illness,
highlighting their beliefs that fever is harmful. The impact of knowledge and beliefs
on practices was evident in parents’ intentions to reduce fever. Unfavourable
263
attitudes toward fever were a significant determinant of parents’ intention to reduce
fever in both models tested in Study 2.
Fears about harmful outcomes from fever overrode parents’ beliefs that antipyretics
could be harmful. Despite believing antipyretics were harmful, the majority of
parents in both studies regularly used them to reduce fever. In Study 2 parents used
antipyretics for a mean temperature of 38.3ºC. Reducing low grade fevers with
antipyretics is not uncommon in the literature and reports of parents’ reliance on
antipyretics to control fever are increasing (Crocetti, 2001; Karwowska et al., 2002).
In 1980 in the United States only 11% of parents reported reducing low grade fevers,
37.8ºC (Schmitt, 1980), however, this increased to 25% in 2001 (Crocetti et al.,
2001). In the mid 2000s, 70% of Greek mothers reported reducing temperatures
between 37.5ºC to 38.5ºC with antipyretics (Matziou et al., in press). Antipyretics as
the preferred method of managing fever increased from 67% in 1980 to 95% in 2002
(Karwowska et al., 2002; Schmitt, 1980); 91% of parents reported this in Study 2.
Practices confirmed negative beliefs and unfavourable attitudes with more than half
those in Study 2 regularly reducing mild fevers and sometimes normal temperatures
with antipyretics.
Although parents reported reducing low grade fevers with antipyretics, the range of
temperatures reduced varied considerably, from 37.0ºC to 40.0ºC, indicating
different levels of knowledge of and beliefs about fever and some appropriate use of
antipyretics. Despite this, parents’ overall attitudes in Study 2 were strong and
unfavourable. Ajzen (2005) considers strong attitudes to be relatively stable over
time and strengthened by experience with the attitude object, in this case childhood
264
fever, and information about the issue. Factors influencing parents’ beliefs are
multifactorial (Poirier et al., 2000). Parents in both studies had experience with
childhood fever and sought information about how to manage fever from multiple
sources. Positive and negative experiences influencing practice changes were
reported in Study 1 and practice changes over time were reported in Study 2. In
Australia, catastrophic outcomes from serious febrile illnesses are newsworthy and
receive significant media attention. This can cause parents to reflect on their
attitudes. Those with unfavourable attitudes toward fever could incorporate this
information reinforcing their attitudes and intentions to reduce fever (Ajzen, 2005).
Unfavourable attitudes toward fever significantly determined intentions to reduce
fever in both models.
Parents reported learning to manage fever from doctors, past experience, family and
friends. Other studies report parents gathering fever management information from
similar sources (eg., Al-Eissa, Al-Zamil, et al., 2000; Crocetti, 2001; Karwowska et
al., 2002). In Study 2 parents’ intentions to reduce fever and reduce fever with
medications were strongly influenced by beliefs that others expected them to reduce
fever, indicating unsupportive norms. They perceived strong social pressure from
partners and doctors to reduce fever, stronger than that from their own mothers and
friends. In the fever model unsupportive norms were the strongest determinant of
intention both directly and mediated through attitudes. Different strengths in
perceived expectations highlight the conflict parents experience with childhood fever
management.
265
The impact of parents’ perceived expectations of others on their fever management
practices has not been reported previously. Unsupportive normative influences could
reflect a moral or ethical component as well as parents’ emotional involvement in
caring for a febrile child; particularly as the strongest normative influences were
from doctors in both models. Caring for a febrile child is emotionally taxing (Kai,
1996; Lagerlov et al., 2003). Concerns about their child elicit parents’ protective role
and their duty of care for their child (Kai, 1996). Mothers report preferring to stay
close to febrile children; not wanting to delegate care and postponing other duties
and social activities (Lagerlov et al., 2003). The strong influence from partners to
reduce fever indicates they possibly have similar concerns to the parents who
participated in Study 2. However, it was not within the scope of the thesis to explore
this. Stronger normative influences from partners in parenting intentions, compared
with mothers and friends, were found in a study determining the predictors of
parents’ intentions to attend parenting classes (Wellington, White & Liossis, 2006).
The need for support from partners in parenting practices may have a strong
normative influence on parenting intentions and needs further examination. The
strong unsupportive normative influence from partners indicates parents’ need for
approval from their partner when caring for a febrile child.
Doctors are presumed knowledgeable about health issues. Parents in Study 1
reported doctors as their most reliable source of fever management information
(Walsh & Edwards, 2007). In Study 2 doctors were the most frequent source of fever
management information with nurses being reported less frequently. Practices and
intentions based on beliefs of doctors’ expectations of practice should reflect the
latest scientific evidence. This was not so. Parents, believing doctors expected them
266
to, reduced fever with antipyretics; alternated antipyretics when fever was not
sufficiently reduced or returned, and intended to reduce fever with antipyretics.
Recommendations from doctors to reduce fever and alternate antipyretics to
normalise temperature during febrile illnesses continue to be reported, supporting
parents’ normative beliefs (May & Bauchner, 1992; Mayoral et al., 2000; Wright &
Leibelt, 2007). The role of health professionals was substantiated in Study 2 by the
impact that having health industry experience had on unsupportive norms. These
parents reported stronger normative influences to reduce fever and reduce fever with
antipyretics than those without this experience.
Fortunately not all authors or health professionals advise parents to reduce fever.
Some recommend evidence-based fever management and the use of antipyretics for
pain relief during febrile illnesses, not fever reduction (eg., Lorin, 1999; Mayoral et
al., 2000; Schmitt, 2006; Walsh et al., 2005; Watts et al., 2003). On the other hand,
Australian general practitioners have been advised to recommend parents normalise
fever with antipyretics despite scientific evidence recommending not reducing fever
(Pearce & Curtis, 2005). The rationale for this advice was the general practitioners’
relationship with their patients (parents in this case), which was considered to be
more important, and a stronger determinant of practice recommendations, than
scientific evidence. Although believing doctors a credible, reliable source of
information, parents in both studies received conflicting information about fever
management from doctors. Receiving conflicting information, not receiving a
definitive diagnosis and incongruence in perception of illness severity was reported
to harm the doctor-parent relationship. When unsatisfied with medical advice,
parents sought advice elsewhere: from another general practitioner or an emergency
267
department increasing health service usage. Receiving conflicting advice challenges
parents’ protective roles and to overcome this they seek further information to ensure
they are correctly caring for their child.
Although parents want to protect their child from harm their children are not always
compliant with their wishes. In Study 2, parents reported febrile children were not
always compliant with medication administration. This is an important finding
indicating a need for health professionals to ensure parents are able to medicate their
children when necessary. Some children need regular medications; others may need a
course of, for example, antibiotics or an analgesic for pain relief. When medications
are needed, it is important children receive correct doses at appropriate intervals.
Health professionals have an important role in teaching parents to medicate their
children correctly ensuring the prescribed dose is administered.
Another important finding from Study 2 was the effect child medication behaviours
have on attitudes and subjective norms. When children did not take medications
easily parents reported more favourable attitudes, supportive norms and intentions
indicative of evidence-based fever management. This indicates parents had more
positive beliefs about fever being beneficial or that fever was not harmful and that
they were less likely to believe others expected fever should be reduced with
antipyretics. Further exploration of the specific effect of child medication behaviours
on parental beliefs is necessary.
The influence of child medication behaviour has not been previously reported in
relation to childhood fever management. This finding has implications for parent
268
education indicating the positive role experience can play in fever management.
When children refusing antipyretics were unharmed during febrile episodes parents
received new information about fever and fever management which supports Ajzen’s
theory on attitude change (Ajzen, 2005). Parents’ direct personal experiences, in this
case no negative outcome from fever, produced more favourable attitudes. The
unfavourable attitudes of the parents, whose febrile children who were reluctant to
take medications, were regularly challenged.
Highlighting the importance of child medication behaviours on antipyretic
administration was the finding that these behaviours had no direct influence on
intentions in the fever model but had both a direct and the strongest overall influence
in the medication model. Medication use was parents’ preferred method of reducing
fever in these and other studies (eg., Crocetti, 2001; Karwowska et al., 2002;
Matziou et al., in press; Mc Erlean et al., 2001). In light of the rapid increase in the
practice of alternating antipyretics (Crocetti, 2001; Li et al., 2000; Wright & Leibelt,
2007; Matziou et al., in press) the influence of negative child medication behaviours
on parents’ intentions to use antipyretics is a key finding from this research.
Most parents regularly used medications, with half alternating antipyretics, and
parents intended to reduce their child’s next fever with medications. This is
worrying as many parents incorrectly determined medication dose and frequency.
They reported using the height or recurrence of fever, illness severity and the child’s
general wellbeing. Height of fever is reported to be a common determining factor in
parents’ antipyretic administration (eg., Crocetti, 2001; Karwowska et al., 2002). As
in other studies, overdosing with ibuprofen was more common (Bilenko, Tessler,
269
Okbe, Press, & Gorodischer, 2006; Li, Lacher, & Crain, 2000). In Study 2, three
quarters of the parents used both antipyretics. Confusion from using two antipyretics
was indicated through the number of parents who administered ibuprofen at four
hourly intervals (22%). There are recommendations in the literature for paracetamol
as the preferred medication for pain and fever in children as fewer adverse drug
reactions are associated with paracetamol compared with ibuprofen (Titchen,
Cranswick & Beggs, 2005).
Rationales for antipyretic use were also erroneous. Parents in Study 2 used
antipyretics: to reduce illness symptoms such as coughs, colds, rhinitis, vomiting
and pain; for sleeping problems; and to improve the child’s general wellbeing. This
reflects parents’ beliefs in the 1980s when antipyretics were believed to have
antihistamine, antiviral and decongestant properties (Ames et al., 1982). Australian
parents use paracetamol to calm upset children, improve children’s mood and
promote sleep (Allotey et al., 2004). Of concern is parents’ preference for
antipyretics to control fever and the proportion of parents who alternate antipyretics.
This indicates a normalising of medication use and the use of analgesics/antipyretics
in a preventative rather than curative role despite believing that
analgesics/antipyretics can be harmful.
Fortunately, not all parents relied on antipyretics. In both studies some parents
reported a reduction in antipyretic use over time. With experience and as their child
aged they became more confident in caring for febrile children and delayed
antipyretic use. Alternatively, some increased antipyretic use over time indicating
less favourable attitudes and unsupportive normative influences on their fever
270
management intentions. Experiences with febrile children influenced decisions about
antipyretic use in Study 1. Further exploration of specific experiences and their
influence is needed and could assist in the development of scenarios for use with
parents to promote evidence-based fever management.
However, although influenced by unfavourable attitudes and positive child
medication behaviours, making fever management decisions did not influence
parents’ intentions to reduce fever in either of the models tested in Study 2. This,
when considered with the high reported rate of antipyretic use, indicates parents
encounter difficulties when attempting to control or normalise fever. Parents’ use of
antipyretics and inability to normalise temperature prior to seeking medical advice
confirms this (Betz & Grunfield, 2006; Karwowska et al., 2002; Mason, Thorp &
Burke, 2003). Parents intended to reduce fever irrespective of their role in making
fever management decisions. The lack of influence of decision making on fever
management intentions is an important finding and of significant value when
developing education programs. Targeting parents’ decision making will not alter
their intentions or behaviour. Areas for educational programs to target, identified
through this research, are unfavourable attitudes and unsupportive normative
influences and providing parents with positive experiences with childhood fevers that
have not been reduced by antipyretics.
8.3 THEORETICAL IMPLICATIONS This thesis has a strong theoretical base through employment of the TPB, a theory
acknowledged for its ability to identify attitude-behaviour relationships and
determinants of behavioural intention in situations where people do not have
complete control (Ajzen, 1985, 1991, 2005; Armitage and Conner, 2001). Parents’
271
management of childhood fever is guided by many factors: fear of harmful
outcomes; a need to protect their child; inaccurate and/or conflicting information
about best practice; and that it is not under their volitional control. This cognitive
theory predicts the cognitive determinants of behavioural intentions in people not
necessarily motivated to or interested in changing behaviour. The predictive ability
of the TPB in health-related behaviours has been repeatedly demonstrated through a
number of reviews including meta-analyses (eg., Albarracin, Johnson, Fishbein &
Muellerleile, 2001; Armitage & Connor, 2001; Godin & Kok, 1996). Generally the
TPB explains around 40% of the variance in people’s intentions and 34% of the
variance in their health related behaviour (Armitage & Conner, 2001; Godin & Kok,
1996; Rivis & Sheeran, 2003).
Despite the volume of literature reporting TPB studies there is a dearth of literature
reporting the determinants of parents’ intentions when caring for their child’s health.
In those published, while some report the determinants of parenting intentions not all
report the predicted variance in intention. A high correlation was found between
maternal attitudes toward infant feeding methods and intentions, .67, and intentions
with behaviour, .82 (Manstead, Proffitt & Smart, 1983). Maternal attitudes toward
restricting infants’ sugar intake correlated with their intentions, .64 (Beale &
Manstead, 1991). Parental attitudes toward the use of child car restraints were
correlated with intention, .77, and predicted 67% of the variance in parents’
intentions (Ferraro, 2004). In the above studies attitudes and perceived behavioural
control predicted intentions, however, subjective norms made no significant
contribution to intentions. More recently, subjective norms were found to make a
significant contribution to parents’ intentions to attend group parenting education (β
272
.33); 37% of variance in parents’ intention was predicted in this study (Wellington &
White, 2006). Interestingly, in this study perceptions of control did not significantly
contribute to intentions and attitudes were the strongest predictor, stronger than
subjective norms.
The findings explain a significant amount of variance in factors influencing parents’
fever management intentions. In this thesis the TPB explained 60% and 68% of the
variance in parents’ fever management intentions. Parents’ attitudes toward reducing
fever to prevent harm and reducing fever with medications to prevent harm were
highly correlated, .73 and .74 respectively. Subjective norms had a high correlation,
.70, with intention in both models. Perceived control over decision making was
weakly correlated with intention, -.20 in the fever model and -.19 in the medication
model. Perceptions of control due to child medication behaviour were moderately
correlated with intention in the fever model, -.41, and highly correlated in the
medication model. -.70. Associations between behavioural intention and behaviour
were not within the scope of this thesis and need exploring in future studies.
However, this thesis makes a significant contribution to parenting and TPB literature
through the amount of variance explained in the behavioural intentions of parents in
a parenting behaviour; a behaviour that involves consideration of numerous factors
and is highly emotional.
Through the TPB this thesis has identified the difficulties parents have in caring for
an ill child. The finding of strong unsupportive normative influences implies parents
of ill children need to be perceived as caring appropriately for their child, particularly
by their partner and doctor. Are parents similarly concerned about other parenting
273
behaviours, such as, infant feeding methods, introducing solids, healthy food choices,
toilet training or immunisation? The TPB is acknowledged as an excellent theory for
identifying health related problems yet there is little research identifying
determinants of parenting styles and decision making (eg., Armitage & Conner,
2001; Albarracin et al., 2001; Ajzen 2005; Godin & Kok, 1996). Further exploration
of these areas is needed. Methods used in this thesis are appropriate for exploring the
determinants of other parenting behavioural intentions.
8.4 STRENGTHS AND LIMITATIONS The findings from this thesis are important. Australian parents’ fever management
practices and influences on their practice have not previously been reported. Decades
of research have identified parents’ knowledge, attitudes and practices but not the
determinants of these practices (see Chapter 3). No theoretical exploration of
parents’ fever management intentions has been reported. Identification of predictors
of intentions and the complex decision making involved in parents’ fever
management intentions, through a major attitude-behaviour theory, provides
important information for health professionals educating parents about childhood
fever management.
In accordance with the TPB an elicitation study was conducted to identify the current
salient beliefs, practices and referents (Ajzen, 2006). This qualitative study informed
the development of the instrument guided by advice from Ajzen (2006b) and Francis
et al. (2004) and was further refined following the piloting with nine parents. To
ensure construct reliability of indirect variables, multiple measures of subjective
norms and both direct and indirect measures of perceived behavioural control were
used (Ajzen, 2006b). Face and content validity were confirmed by an expert panel
274
and a pilot study (Polit & Beck 2006), construct and discriminant validity and
construct reliability were confirmed through confirmatory factor analysis (Hair et al.,
2006). The comprehensive instrument developed in this thesis contributes to fever
management literature, provides an instrument to enable comparison studies to be
undertaken and is suitable for evaluating educational interventions.
The thesis provides a comprehensive report of Queensland parents’ fever
management. It provides health professionals with essential information about
parents’ fever management and the influence that health professionals’ negative
beliefs and practices have on parents’ practices. This thesis adds to the literature in
two distinct ways. There is no literature reporting the determinants of parents’ fever
management and no report of Australian parents’ fever management. The variation
of intentions determined by the theoretical models was high, 60% and 68%, and
explains a considerable amount of parents’ decision making when managing a febrile
child. Many studies identify a mean of 30% of the variance in intentions (Armitage
& Conner, 2001). Additionally, there is limited literature exploring determinants of
intentions in parenting or child health behavioural intentions or practices. This thesis
contributes significantly to this area.
The major limitations of the thesis relate to the sample in Study 2. The sample was
self-selected and mostly females who had a university education and lived in major
cities. Data in this study were collected by self-report, however, data lent itself to
self-report and enabled a more diverse sample to be studied (Polit & Beck, 2006).
Participants were recruited through three distinct recruitment methods in an attempt
to reduce selection bias (Minicheillo et al., 2004; Polit & Beck, 2006) and improve
275
generalisability of the findings. Despite this, parents recruited through advertising
(half the sample) were less likely to come from a major city and more likely to have
fewer children. These parents received conflicting information about how to manage
fever and reported having alternated antipyretics more frequently than those recruited
through other methods. These experiences may have influenced the responses from
those recruited through advertising therefore caution is needed in interpreting the
findings.
Most participants were female although females were not specifically targeted. It is
possible the gender imbalance influenced the results. However, the females who did
respond reported a strong normative influence from their partners, implying their
partners had similar beliefs and practices. Most participants lived in a major city and
would therefore have ready access to medical assistance through general
practitioners and hospitals. The need to travel further distances for medical advice
may influence the fever management practices of parents living in rural and remote
areas therefore findings must be considered carefully. Limited access to health
assistance could promote the more frequent use of antipyretics in parents believing
fever harmful.
Additionally, more than half the parents had a university degree. Parents with lower
educational attainment reported different beliefs about temperatures representative of
high, very high and harmful fever; managed fever differently and were less likely to
have received conflicting information about fever management. Findings, therefore,
may be more applicable to parents with university education. The influence of
276
education on fever management intentions needs further exploration with a more
heterogeneous sample.
Although data related to the TPB were nonnormal all efforts were made to reduce
any influence on the analyses and transformed data were used for the analysis (Hu &
Bentler, 1999; Yung & Bentler, 1996). Multiple measures of goodness-of-fit
statistics were used to determine model fit to data and models were explored for both
good and bad fit. Sample bias could have influenced the impact of background
factors on intentions. A study with a heterogeneous sample, including more rural and
remote parents, those with lower educational levels and fewer with health industry
experience may have different findings. A more educationally heterogeneous sample
may report even less favourable attitudes toward fever and more influence from
unsupportive normative influences and increased intentions to reduce fever. Parents
living in rural and remote areas may have additional factors influencing their fever
management intentions due to the appropriateness of the health service available,
distances necessary to travel for medical advice and transport availability. The
findings reported in this thesis should be considered with the above in mind.
8.5 PRACTICE IMPLICATIONS
8.5.1 Parents This large study of Queensland parents identified their poor knowledge of fever,
fever’s benefits and evidence-based fever management. Although correctly seeking
fever management information from doctors and perceiving them as reliable, credible
sources of health information, parents received conflicting information which made
fever management unnecessarily taxing and complex. Parents have a right to know
the findings of the latest scientific evidence and evidence-based recommendations
277
for caring for their febrile child. Currently, many Queensland parents, while
attempting to protect their children from harmful outcomes from fever, are placing
children at risk from unnecessary antipyretic overuse and overdose.
The strong normative influence in reducing fever to prevent harm indicates the need
for broad community based education. To reduce unfavourable normative influence
from partners, education programs need to target both parents simultaneously. In
Study 1, a group of parents discussing the benefits and harm of childhood fever
began to challenge their use of antipyretics to reduce fever (see Chapter 5).
Education in groups would enable parents to discuss their fears and experiences, both
positive and negative, and learn about evidence-based fever management.
Parents’ unfavourable attitudes toward fever and intentions to reduce fever, with or
without medications, signify the need for change. The rate of antipyretic use,
alternating antipyretics and overdosing indicate the urgent need for parent education
about evidence-based fever management, appropriate antipyretic use and when to
seek medical assistance. Most parents used paracetamol but many also used
ibuprofen which is of concern particularly in relation to the proportion who
overdosed their child with ibuprofen and the harm associated with administering
ibuprofen to children who are dehydrated or have asthma (eMIMS, 2007). The rate
of Queensland parents’ ibuprofen use confirms its increasing use in Australia. A
seven-fold increase in ibuprofen use was found from 1999 to 2003 in an Australian
metropolitan paediatric hospital with associated higher rates of adverse drug
reactions compared with paracetamol (10:6) (Titchen et al., 2005). It could be
278
hypothesised that the fictitious properties attributed by Australian parents to
paracetamol (Allotey et al., 2004) are also attributed to ibuprofen.
Parents should be encouraged to delay antipyretic administration for fever reduction
and only use analgesics to relieve pain associated with febrile illnesses. Antipyretics
are unnecessary for temperatures below 39.0ºC unless associated with pain (Curtis &
Starr, 2000; Schmitt, 1994). Alternating antipyretics is unnecessary and focuses
parents’ attention to the temperature rather than child’s well-being and it must be
discouraged, particularly for mild to moderate fever (Goldman, 2006; Saphyakhajon
& Greene, 2006; Schmitt, 2006). Nearly a decade ago it was recommended
antipyretics only be alternated in specialised units under professional supervision due
to the potential risks associated with administering two drugs to an ill child
(McCullough, 1998). This recommendation needs to be taken seriously by parents
and those advising them on the care of a febrile child.
Parents’ desire to appropriately care for children with febrile illnesses is evidenced
by their search for knowledge. The impact of experience on attitudes and practice
indicates the need for parents to learn to care for a febrile child before having a
negative experience, preferably before the first febrile episode. Ideally parents will
learn to manage fever before the first immunisations are due. This will not only
prepare parents for caring for their child following immunisation it will ensure most
parents are educated before their child’s first febrile episode.
Another important outcome from this thesis is evidence that parents have difficulty
medicating their children. At times children need to take medications; parents need to
279
be taught how to administer medications to their child and advised on alternate
methods for use when children are distressed or reluctant. This responsibility lies not
only with parents and those prescribing and dispensing medications but also with
paediatric, child health and practice nurses who are ideally placed to demonstrate and
advise parents about childhood medication administration, dosage and frequency.
8.5.2 Doctors and Other Health Professionals Parents reported strong unsupportive normative influences from doctors and
alternated antipyretics on recommendations from doctors and hospitals. Fever does
not necessarily need to be reduced (Lorin, 1999; Schmitt 1994). Parents of febrile
children seek medical advice to access the doctors’ clinical skill and their ability to
discuss what is wrong with their child and how to manage them at home; they are not
seeking a prescription for antibiotics or antipyretics (Bhrolchain, 2004; Kallestrup &
Bro, 2003; Stivers, Mangione-Smith, Elliott, McDonald, & Heritage, 2003). Doctors
must respect parents’ integrity without fearing evidence-based information will harm
their therapeutic relationship. Receiving conflicting information did appear to harm
this relationship causing parents seek advice elsewhere.
The influence of experience on parents’ attitudes and fever management intentions
highlight additional areas for doctors to assist parents. When parents have, or hear of,
a negative fever experience from friends or the media, doctors have an important role
in talking with the parents, explaining the circumstances and the likelihood or
unlikelihood of the event recurring. Positive fever management and advice seeking
need to be referred to when a negative event occurs to support parents in their role as
protector of their child. Alternatively, when parents seek timely medical advice they
need to be encouraged. Additionally, when doctors prescribe medications for
280
children they should ensure parents can correctly administer the medication, provide
them with alternative methods to use should a child refuse the medication and alert
them to the consequences of a missed dose.
Parents reported they learnt to manage fever from nurses less frequently than from
doctors. Health education is an important aspect of the nurses’ role. They are ideally
placed to educate parents in hospitals, general practices where they are employed as
practice nurses, child health clinics and pharmacies where well baby clinics are
conducted. Nurses need to focus on the antecedents of parents’ intentions to reduce
fever, their unfavourable attitudes toward fever and perceptions that others expect
fever be reduced. To facilitate this education nurses should ensure their knowledge is
based on the latest scientific evidence to prevent parents receiving conflicting
information. Parents’ interest in fever management is evident from their quest for
information, from many sources.
Parents’ fears cause them to overuse and overdose children with antipyretics to
normalise mild fever and sometimes normal temperatures. Health professionals, as a
group, need to address this issue, assist parents to realise the benefits of fever and
that it is best to focus on the child’s well-being rather than the temperature and allow
the body’s immune processes to function ((National Collaborating Centre for
Women's and Children's Health [NCCWCH], 2007; Schmitt, 2000). Febrile children
should rest and allow their body to destroy the invading organism and produce
antibodies to prevent re-infection with the same organism (Blatteis, 2003, 2006;
Zeisberger, 1999).
281
Health professionals need to encourage parents to delay antipyretic administration in
children who do not exhibit pain or discomfort and have no pre-existing medical
conditions. Through experience, parents may incorporate the positive benefits of
fever into their belief system. Care of a febrile child should focus on: the child’s
well-being rather than temperature; using analgesics to relieve pain associated with
febrile illnesses; and not reducing fevers under 39.0ºC unless associated with
discomfort or pain (Schmitt, 1994; NCCWCH, 2007) .
8.6 IMPLICATIONS FOR FUTURE STUDIES The identification of determinants of intentions to reduce fever provides an excellent
basis for the development, implementation and evaluation of educational
interventions. The strongest predictors of intentions were unfavourable attitudes and
unsupportive norms. A number of different methods can be used to correct these
beliefs and create new evidence-based beliefs. Ajzen (2006b) recommends using
persuasive communications in, for example, newspapers, flyers, television, face-to-
face discussions or observational modelling. Other methods commonly used to
change incorrect beliefs are information, increasing skills, goal setting, rehearsal of
skills, modelling, planning and implementation, and social encouragement and
support (Hardeman, Johnston & Jounston et al., 2002). Ajzen (2006) also
recommends the development of implementation intentions. These are a specific plan
identifying how the next fever will be managed, when antipyretics will be
administered and how the febrile child will be managed (Gollwitzer, 1999).
Most studies reporting TPB educational interventions involve information giving
about the risks of the behaviour and the connections of behaviour and outcomes
(Hardeman et al., 2002). TPB based interventions to change health professional
282
behaviour have used information, identification of current beliefs and referents, and
the influence of these, peer group discussions, skill rehearsal (scenario) and peer
support (Edwards et al. 2001; Edwards et al., 2007, in press).
Educational programs could be developed and trialled with parents representative of
those who participated in this study. Interventions should target the identified
incorrect beliefs with scientifically determined information, such as: fever is
beneficial and does not always need to be reduced; and febrile convulsions are
benign and occur in less than 5% of children. New favourable beliefs about the use
of antipyretics for pain rather than fever need to be introduced. Other new beliefs to
introduce include when fever should be reduced and when it is necessary to seek
medical attention both urgently and within the next 24 hours. Parents with favourable
beliefs about fever who are knowledgeable about when to seek medical advice will
be more confident in their management of childhood fevers. Parents in the study
identified knowledge and experience as sources of reassurance about their fever
management practices, reducing their concerns.
Randomised controlled educational interventions need to be developed, implemented
and evaluated in paediatric hospitals and units, child health clinics and maternity
hospitals as well as child care centres and kindergartens and preschools. It is
important to include partners in these programs as partners are a significant a source
of unsupportive norms which make attitudes less favourable. Controlled trials can be
conducted by paediatric and emergency nurses modelling evidence-based fever
management and providing clear explanations of their rationales for either
283
administering an antipyretic or not administering an antipyretic to a child with a
febrile illness.
At a community level a series of brief articles could be produced targeting the
incorrect beliefs described earlier. Sources used to recruit participants for this thesis
would enable distribution of such articles throughout Queensland. These include
freely available parenting magazines, Playgroup Queensland, child care centres,
kindergartens and preschools and the Family Day Care Service. Recruitment,
baseline data collection and randomisation of parents, prior to the community project
with follow-up data collection will enable the effectiveness of community based
programs to be evaluated.
Programs should be trialled through different settings and with varied presentation
methods. Comparisons between parents’ interest in learning in the specific setting,
perceived credibility and reliability of the information, use of and ease of
understanding the information, and time and cost effectiveness of the programs need
to be examined. Varied presentation methods should reflect the parents’ lifestyle and
include interactive computer based programs in waiting rooms, pharmacies and
libraries. Other presentation methods include compact discs, booklets and take home
pamphlets to reinforce and remind parents of best practice. Anecdotally, these can be
useful when evidence-based information is challenged by others not aware of the
latest scientific evidence.
Although parents reported doctors as their main source of information, nurses and
pharmacists were also mentioned. Therefore, future studies need to identify the

284
knowledge, beliefs, and fever management recommendations of all health
professionals caring for febrile children or advising parents on the care of a febrile
child. This includes general practitioners, paediatricians, child health nurses,
paediatric, emergency and general nurses, pharmacists and pharmacy assistants, and
child care workers. Deficits identified through these studies could then be targeted
through education and evidence-based guidelines and policies for childhood fever
management developed and implemented.
8.7 OVERALL CONCLUSIONS Queensland parents have poor knowledge of evidence-based childhood fever
management. This contributes to negative beliefs about harmful outcomes from fever
and unfavourable attitudes toward fever which influence their practice and practice
intentions. The unsupportive normative influence from partners is understandable,
but from doctors it is unacceptable and should be urgently addressed. Child
medication behaviours have not been previously explored and findings indicate their
importance in parents’ fever management intentions. The strong influence of child
medication behaviour on intentions is a novel finding, not previously reported and
can be used by health professionals as a method of encouraging parents to delay
antipyretic administration.
The thesis contributes significantly to childhood fever management, paediatric care,
parenting decision making and the body of literature reporting childhood fever
management. There is an urgent need for parents to be consistently educated about
evidence-based fever management by non-phobic health professionals.
Recommendations for care must be consistently based on the latest scientific

285
evidence. Parents unnecessary overuse of, and overdose with, over-the-counter
medications for mild fever must cease.

286
287
Appendix 1
Study 1 Documents

288
FEVER IN YOUNG CHILDREN
INFORMATION FOR PARENTS ABOUT THE FOCUS GROUP DISCUSSION This research is being undertaken as part of a Doctor of Philosophy degree and will be conducted under the guidance of experienced researchers from the School of Nursing at the Queensland University of Technology (QUT)
Researcher: Anne Walsh, School of Nursing, (QUT), 3864 3856 Principal Supervisor: Professor Helen Edwards, Head, School of Nursing, (QUT), 3864 3844
Raising a young child is not easy and when your child becomes ill this is even more difficult. Many parents are worried about their child’s fever when they are ill. They seek advice on how best to care for their child. There is a lot of the advice available. However, advice can vary, making it hard for parents to know what the best thing to do is. This can make parents even more worried about how to care for their sick child. As you have a child aged between 6 months and 5 years you will have had to look after a child with a fever. Not much is known about how Australian parents look after their children when they have a fever. Also, little is known about how Australian parents learn how to manage fever. As this is something every parent will have to do it is important to find this out. Then nurses and doctors can help parents during this worrying time. I would like to invite you to join in a group discussion about children’s fever. The other parents in the group have children at the same child care centre as you. The discussion will be at the child care centre at a time that suits interested parents. It will take about 30 minutes. The discussion will be recorded by a person who types in shorthand, it will also be audio taped. When the discussion has been typed I will send a copy to you to make sure it is accurate. I plan to use the information from the discussions to develop a survey. This survey will be sent to parents of children aged 6 months to 5 years. By joining in a group discussion you might learn more about childhood fever. What is learnt from the discussions will be used to help Australian parents in the future when their child has a fever. I do not wish anyone to be identified through the information I collect. To make sure your records are confidential, names will not be kept on any record. To ensure the privacy of those in the discussion please do not use peoples’ names. Audio tapes will be destroyed when the information has been examined. All the information I collect will be kept secure in a locked filing cabinet. Only I and my supervisors will have access to this information. No information about the study will be published in any form that would allow you or your child care centre to be recognised. Participating in a discussion is voluntary. You are free to leave at any time without comment or penalty. Being involved in a discussion should not pose any risk to you. The only inconvenience you should experience is the use of your time. If you have any questions about this research please contact me, Anne Walsh, on 3864 3856 or my supervisor, Prof. Helen Edwards on 3864 3844. You may also contact the Queensland University of Technology’s Research Ethics Officer on 3864 2340 if you have any concerns about the ethical conduct of this research.
289
FEVER IN YOUNG CHILDREN
FOCUS GROUP MEMBER CONSENT FORM
Researcher: Anne Walsh, School of Nursing, (QUT), 3864 3856
Principal Supervisor: Professor Helen Edwards, Head, School of Nursing, (QUT), 3864 3844 I _________________________________________ (please print your full name) have read the
information sheet about “Fever in Young Children” and had any questions or queries
answered to my satisfaction by Anne Walsh.
I have read and understood the Information Statement and had any questions or queries
explained to me by Anne Walsh. I understand that:
♦ If I have any further questions I can contact the researchers at any time;
♦ My participation is voluntary and I may withdraw from this focus group discussion at
any time without comment or penalty;
♦ All information that I give during the focus group discussion will be kept in the strictest
confidence and no information will be released in any way that I could be identified.
I hereby consent to be involved in this study.
______________________________________ _________________ Signed (focus group member) Date ______________________________________ __________________ Witnessed by (please print) Date ______________________________________ Witness signature
If you have any questions about the ethical conduct of this research please contact the Queensland University of Technology Research Ethics Officer on 3864 2340.
290
FEVER IN YOUNG CHILDREN
INFORMATION FOR PARENTS ABOUT THE FOCUSED INTERVIEW
This research is being undertaken as part of a Doctor of Philosophy degree and will be conducted under the guidance of experienced researchers from the School of Nursing at the Queensland University of Technology (QUT)
Researcher: Anne Walsh, School of Nursing, (QUT), 3864 3856 Principal Supervisor: Professor Helen Edwards, Head, School of Nursing, (QUT), 3864 3844
Raising a young child is not easy and when your child becomes ill this is even more difficult. Many parents are worried about their child’s fever when they are ill. They seek advice on how best to care for their child. There is a lot of the advice available. However, advice can vary, making it hard for parents to know what the best thing to do is. This can make parents even more worried about how to care for their sick child. As you have a child aged between 6 months and 5 years you will have had to look after a child with a fever. Not much is known about how Australian parents look after their children when they have a fever. Also, little is known about how Australian parents learn how to manage fever. As this is something every parent will have to do it is important to find this out. Then nurses and doctors can help parents during this worrying time. I would like to have the opportunity to discus children’s fever with you. The discussion can take place at a venue and time that suits you. It will take about 30 minutes. The discussion will be recorded by a person who types in shorthand, it will also be audio taped. When the discussion has been typed I will send a copy to you to make sure it is accurate. I plan to use the information from the discussions to develop a survey. This survey will be sent to parents of children aged 6 months to 5 years. What is learnt from the discussions will be used to help Australian parents in the future when their child has a fever. I do not wish anyone to be identified through the information I collect. To make sure your records are confidential, names will not be kept on any record. Audio tapes will be destroyed when the information has been examined. All the information I collect will be kept secure in a locked filing cabinet. Only I and my supervisors will have access to this information. No information about the study will be published in any form that would allow you or your playgroup to be recognised. Participating in a discussion is voluntary. You are free to leave at any time without comment or penalty. Being involved in a discussion should not pose any risk to you. The only inconvenience you should experience is the use of your time. If you have any questions about this research please contact me, Anne Walsh, on 3864 3856 or my supervisor, Prof. Helen Edwards on 3864 3844. You may also contact the Queensland University of Technology’s Research Ethics Officer on 3864 2340 if you have any concerns about the ethical conduct of this research.
291
FEVER IN YOUNG CHILDREN
FOCUSSED INTERVIEW CONSENT FORM
Researcher: Anne Walsh, School of Nursing, (QUT), 3864 3856 Principal Supervisor: Professor Helen Edwards, Head, School of Nursing, (QUT), 3864 3844
I _________________________________________ (please print your full name) have read the
information sheet about “Fever in Young Children” and had any questions or queries
answered to my satisfaction by Anne Walsh.
I have read and understood the Information Statement and had any questions or queries
explained to me by Anne Walsh. I understand that:
♦ If I have any further questions I can contact the researchers at any time;
♦ My participation is voluntary and I may withdraw from this focus group discussion at
any time without comment or penalty;
♦ All information that I give during the focused interview will be kept in the strictest
confidence and no information will be released in any way that I could be identified.
I hereby consent to be involved in this study.
______________________________________ _________________ Signed (participant) Date ______________________________________ __________________ Witnessed by (please print) Date ______________________________________ Witness signature
If you have any questions about the ethical conduct of this research please contact the Queensland University of Technology’s Research Ethics Officer on 3864 2340.
FOCUS GROUP QUESTIONS FOR FACILITATOR
292
How do you know when your child has a fever?
Focus 1 – Concerns about fever
What are your thoughts when your child has a fever?
Do you find you are concerned about the fever?
Are you worried about the height of the fever?
Has this changed as your child has grown older – or with successive children?
How has this changed?
What influenced these changes?
Focus 2 – Managing fever
How do you manage your child when they have a fever?
How do you manage the fever? What else do you do?
What influences your management of fever?
Has this changed as your child has grown older – or with successive children?
How has this changed? What influenced these changes?
Focus 3 – Fever management knowledge
What do you know about fever?
Do you think fever has any benefits? Do you think fever can be harmful?
What do you know about how to manage a fever?
Focus 4 – Information gathering and reliability of information
Can you remember where you learnt how to look after a child with a fever?
Has anyone influenced how you manage fever?
Has any particular information you have influenced how you manage fever?
How accurate do you think this information is?
When do you think is the right time for parents to learn about fever?
Where would be the best place to have fever management information available?
Who from?
What type of information – a talk, leaflet, other?
Have you used the Internet or leaflets from, eg., pharmacies to assist in your management of
fever?
Do you use these sources for other medical information?
What have the most important elements of this discussion been for you?
293
FOCUS FOR CHILDHOOD FEVER RESEARCH
Participant copy
How do you know when your child has a fever?
Concerns about fever
Managing fever
How you learn to manage fever
Information sources and reliability of this information
Best place and time to learn about fever management
294
FOCUS GROUP DEMOGRAPHIC INFORMATION
Please complete the following questions about yourself
1. Your age at your last birthday Please insert the number of years
………….…..years
2. Your gender
Female Male
3. Your marital status
Single (never married) Married Defacto Divorced/Separated Widowed
4. The number of children you have Please circle the number 5. The number of children you have who are under 5 years of age Please circle the number
1 2 1 2 3 4 5 1 2 3 4 5 6 7
1 2 3 4 5
6. Your highest level of education
Please circle highest level of education completed
Completed Primary School Secondary Schooling Completed Secondary School Completed a TAFE course Completed a University Degree Completed Postgraduate Degree
Currently studying (Please specify)
……..……………………… 7. Are you currently working outside the home? No Yes If YES, is this
Full-time Part-time
8. Do you have any assistance with caring for your child or children? Yes No If YES, does this person influence your child care practices? Yes No
1 2 3 4 5 6 7 1 2 1 2 1 2 1 2
STIMULUS QUESTIONS
9. The temperature at which I consider my child has a fever is (Please specify) …..………..°C or circle Do not know
10. I generally give medication to my child when their temperature is greater than (Please specify) ………….°C or circle Do not know
295
Appendix 2
Study 2 Documents

296
Pilot Study
Documents
297
RE: PILOTING OF THE CHILDHOOD FEVER MANAGEMENT SURVEY Dear, This package has been sent to you following our discussion about the development of a questionnaire to explore parents’ management of fever in young children. I have now finalised the development of the questionnaire and would be grateful if you would complete the questionnaire and send it back to me with your feedback in the enclosed stamped envelope. I particular I am interested in whether:
all instructions are easy to read and understand, the questions are easy to read, it is easy to understand what the questions were are asking you, the questions are easy to answer, and if you think I should be asking parents about any other issues you
have experienced or feel are important in relation to managing fever in young children.
If you find an instruction or question difficult to understand or answer could you please identify it on the questionnaire. If you have a suggestion that would make it easier to understand the instruction or question or make the question easier to answer could you please write that on the questionnaire. If you would like to discuss anything about the questionnaire with me please do not hesitate to contact me during work hours on 07 3864 3856, anytime on 041 256 0182 or by email at [email protected] The number on the questionnaire is so that I will know when you return the questionnaires. I will then post you the second questionnaire when I receive this one back. Thank you for your very valuable assistance in this research and in ensuring the questionnaire will provide useful information about how parents manage fever in young children. Yours sincerely. Anne Walsh PhD Candidate School of Nursing Queensland University of Technology Victoria Park Road Kelvin Grove 4059
298
RE: PILOTING OF THE CHILDHOOD FEVER MANAGEMENT SURVEY Dear , Thank you for your feedback on the questionnaire. As we discussed
on the telephone it is necessary to determine the reliability of the
questions, that is, whether people interpreted them the same way, or
similarly, on separate occasions. If the questions are deemed reliable
by this method it can then be assumed that others will interpret
them similarly. If the questions are interpreted differently on separate
occasions then the data collected with these questions would not be a
valid representation of parents fever management. This is why I am
asking you to please complete the questionnaire again.
After returning this questionnaire would you like to receive a copy of
some best practice guidelines from the United States? These
guidelines are similar to those I will be using when I develop an
educational intervention for parents about managing fever in young
children, the final stage of this research program, which I plan to
undertake next year.
I do understand that this is very time consuming and I appreciate
and thank you for your contribution to this research. I have enclosed
for you a small token of my appreciation. Again, if you would like to
discuss anything about the questionnaire with me please do not
hesitate to contact me during work hours on 07 3864 3856, anytime
on 041 256 0182 or by email at [email protected]
Yours sincerely. Anne Walsh PhD Candidate School of Nursing Queensland University of Technology Victoria Park Road Kelvin Grove 4059
299
CHILDHOOD FEVER
MANAGEMENT
- - - INSTRUCTIONS - - -
1. The questionnaire asks for your general opinions about fever and
managing fever in children aged between 6 months and 6 years. 2. It might be an idea to do this survey when the children are asleep
and you are less likely to be interrupted. 3. Please answer every question by marking your answer with a pen as
indicated. 4. In some instances certain questions may look alike but each one is
different. 5. There are no right or wrong answers. If you are unsure how to answer a
question please give the best answer you can. 6. In this questionnaire MEDICATION only refers to over the counter
medication, eg., Panadol and Nurofen, NOT to antibiotics. 7. After you have completed the questionnaire please place it in the reply
paid envelope supplied and return it at your earliest convenience to the Queensland University of Technology.
Thank you for offering to participate in this research.
300
Section 1 The following questions relate to the times when your child has a fever.
1 What things do you usually do when your child has a fever?
(Please specify)
____________________________________________________________________ __________________________________
2 What is the very first thing you do when you discover your child has a fever? (Please specify)
__________________________________
3 If you think the fever is very high do you do these same things? (Please circle)
1. Yes Please go to Q5 2. No 3. Unsure Please go to Q5
4 If NO what other things would you do if you think the fever is very high? (Please specify)
____________________________________________________________________ __________________________________
5 Has your management of fever changed as your child has grown older OR with the birth of other children? (Please circle)
1. Yes 2. No Please go to Q7 3. Unsure Please go to Q7
6 If YES – how has your fever management changed? (Please specify)
____________________________________________________________________ __________________________________
7 Please mark with an X on the line the temperature you would consider to be NORMAL for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
8
Please mark with an X on the line the temperature you would consider to be a FEVER for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
9
Please mark with an X on the line the temperature you would consider to be a HIGH FEVER for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
10
Please mark with an X on the line the temperature you would consider to be a VERY HIGH FEVER for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
301
The following questions relate to fever in general
11
How harmful do you believe fever is? (Please circle one)
1. Very harmful 2. Reasonably harmful 3. Harmful 4. A little harmful 5. Not very harmful 6. Not harmful Please go to Q14
12 At what temperature is fever harmful? (Please specify)
_____________°C
13 In your opinion what harm can high fever cause to a child? (Please rank these in decreasing order of concern to you)
1. ______________________________ 2. ______________________________ 3. ______________________________
14 What are you MOST worried about when your child has a fever? (Please specify)
__________________________________
15 What other things do you worry about when your child has a fever? (Please specify)
____________________________________________________________________ __________________________________
The following questions ask what you GENERALLY do when your child has a fever.
Please circle the ONE number that best describes what you generally do.
When my child has a fever I generally Always Mostly Sometimes Rarely Never
16 Take their temperature 1 2 3 4 5 17 Like to know what their temperature is 1 2 3 4 5 18 Make sure they have plenty to drink 1 2 3 4 5 19 Use medication to reduce the fever 1 2 3 4 5 20 Check on them during the night 1 2 3 4 5 21 Sleep in the same room as them 1 2 3 4 5 22 Wake them up during the night for medication to
reduce their fever 1 2 3 4 5
23 Take them to the doctor 1 2 3 4 5
The following questions ask about your use of OVER THE COUNTER MEDICATIONS
(not antibiotics) to reduce fever. There are no right or wrong answers we are
interested in how you GENERALLY use this medication to reduce fever.
24 At what temperature do you USUALLY give your child medication to reduce fever? (Please specify)
____________°C
25 Do any other things influence your decision to give your child
medication to reduce fever? (Please circle)
1. Yes 2. No Please go to Q27 3. Unsure Please go to Q27
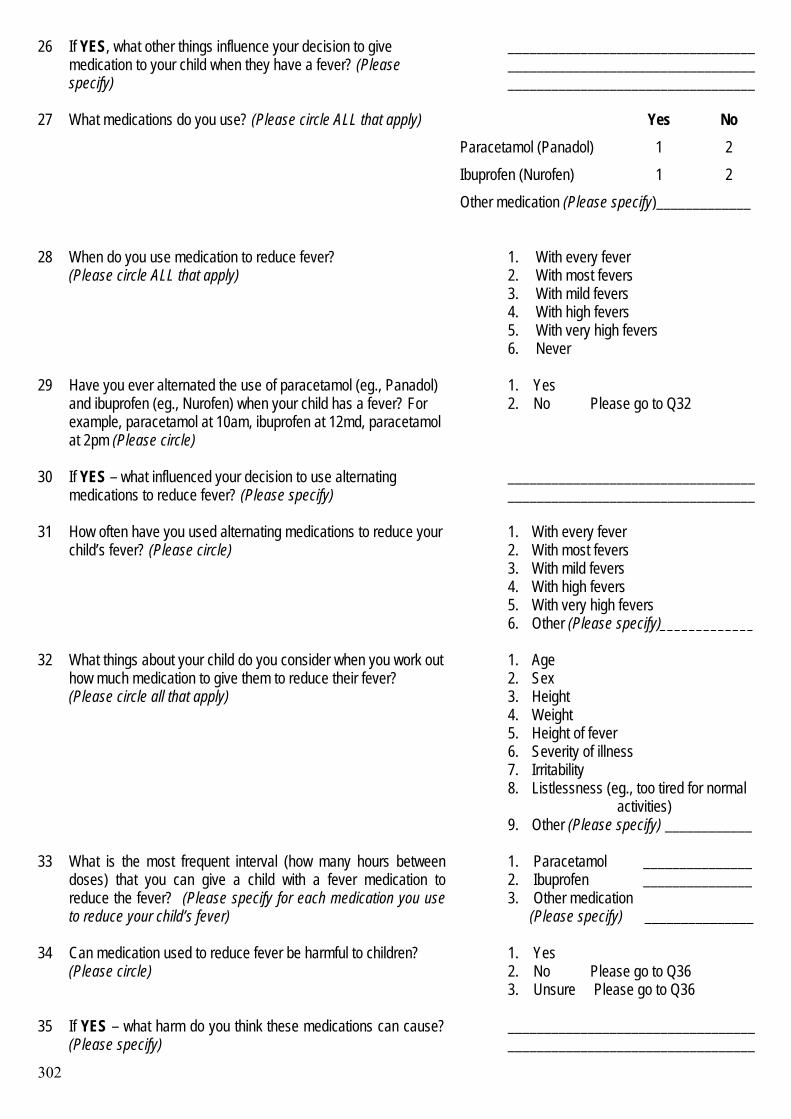
302
26 If YES, what other things influence your decision to give medication to your child when they have a fever? (Please specify)
______________________________________________________________________________________________________
Yes No Paracetamol (Panadol) 1 2 Ibuprofen (Nurofen) 1 2
27 What medications do you use? (Please circle ALL that apply)
Other medication (Please specify)_____________
28 When do you use medication to reduce fever? (Please circle ALL that apply)
1. With every fever 2. With most fevers 3. With mild fevers 4. With high fevers 5. With very high fevers 6. Never
29 Have you ever alternated the use of paracetamol (eg., Panadol) and ibuprofen (eg., Nurofen) when your child has a fever? For example, paracetamol at 10am, ibuprofen at 12md, paracetamol at 2pm (Please circle)
1. Yes 2. No Please go to Q32
30 If YES – what influenced your decision to use alternating medications to reduce fever? (Please specify)
____________________________________________________________________
31 How often have you used alternating medications to reduce your child’s fever? (Please circle)
1. With every fever 2. With most fevers 3. With mild fevers 4. With high fevers 5. With very high fevers 6. Other (Please specify)_____________
32 What things about your child do you consider when you work out how much medication to give them to reduce their fever? (Please circle all that apply)
1. Age 2. Sex 3. Height 4. Weight 5. Height of fever 6. Severity of illness 7. Irritability 8. Listlessness (eg., too tired for normal activities) 9. Other (Please specify) ____________
33 What is the most frequent interval (how many hours between doses) that you can give a child with a fever medication to reduce the fever? (Please specify for each medication you use to reduce your child’s fever)
1. Paracetamol _______________ 2. Ibuprofen _______________ 3. Other medication (Please specify) _______________
34 Can medication used to reduce fever be harmful to children? (Please circle)
1. Yes 2. No Please go to Q36 3. Unsure Please go to Q36
35 If YES – what harm do you think these medications can cause? (Please specify)
____________________________________________________________________
303
The following questions relate to how YOU learnt to manage fever.
36
Do you feel you know the best way to manage fever in your children? (Please circle)
1. Yes 2. No 3. Unsure
37 How did you learn to manage fever? (Please specify)
____________________________________________________________________ __________________________________ __________________________________
38 Have you ever received conflicting information about how to manage your child’s fever
1. Yes 2. No
39 If YES, how did this make you feel about managing your child’s
fever
__________________________________ __________________________________ __________________________________ __________________________________
Please turn over to Section 2
The next section, Section 2 may take a while, please
take your time.
Some of the questions might seem to be the
same, but they are different.
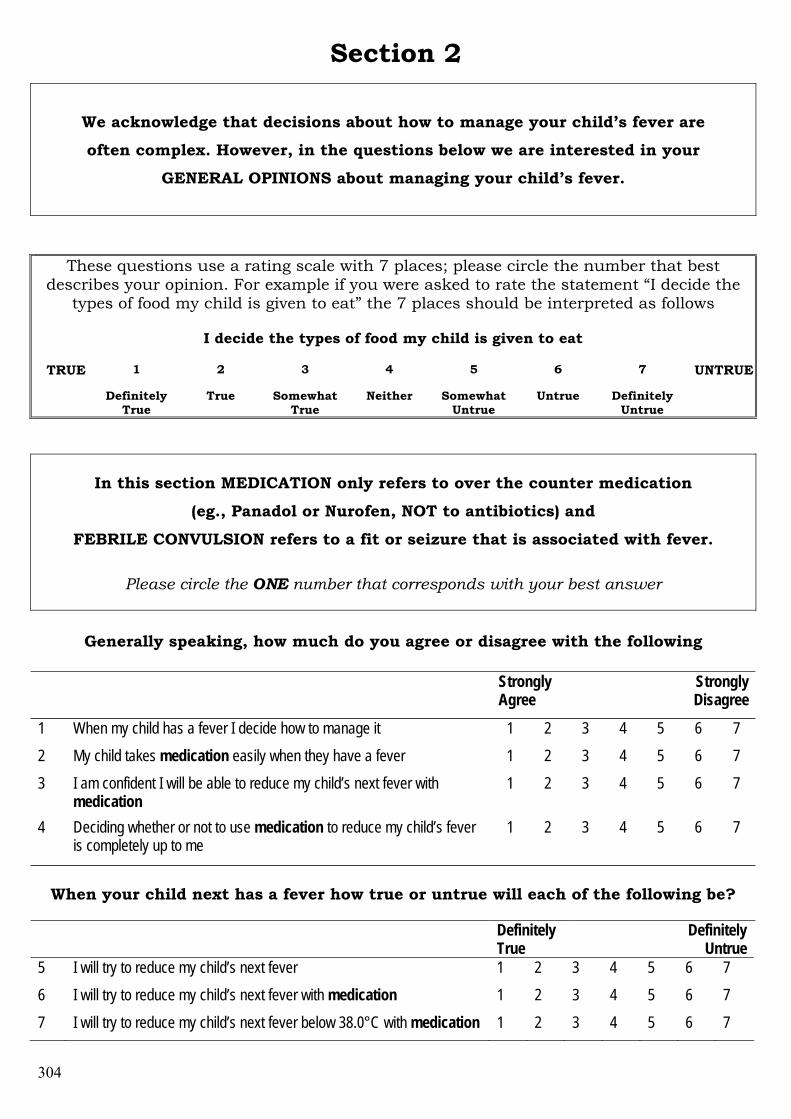
304
Section 2
We acknowledge that decisions about how to manage your child’s fever are
often complex. However, in the questions below we are interested in your
GENERAL OPINIONS about managing your child’s fever.
These questions use a rating scale with 7 places; please circle the number that best describes your opinion. For example if you were asked to rate the statement “I decide the
types of food my child is given to eat” the 7 places should be interpreted as follows
I decide the types of food my child is given to eat
1 2 3 4 5 6 7 TRUE
Definitely True
True Somewhat True
Neither Somewhat Untrue
Untrue Definitely Untrue
UNTRUE
In this section MEDICATION only refers to over the counter medication
(eg., Panadol or Nurofen, NOT to antibiotics) and
FEBRILE CONVULSION refers to a fit or seizure that is associated with fever.
Please circle the ONE number that corresponds with your best answer
Generally speaking, how much do you agree or disagree with the following
Strongly Agree
Strongly Disagree
1 When my child has a fever I decide how to manage it 1 2 3 4 5 6 7 2 My child takes medication easily when they have a fever 1 2 3 4 5 6 7 3 I am confident I will be able to reduce my child’s next fever with
medication 1 2 3 4 5 6 7
4 Deciding whether or not to use medication to reduce my child’s fever is completely up to me
1 2 3 4 5 6 7
When your child next has a fever how true or untrue will each of the following be?
Definitely
True Definitely
Untrue 5 I will try to reduce my child’s next fever 1 2 3 4 5 6 7 6 I will try to reduce my child’s next fever with medication 1 2 3 4 5 6 7 7 I will try to reduce my child’s next fever below 38.0°C with medication 1 2 3 4 5 6 7
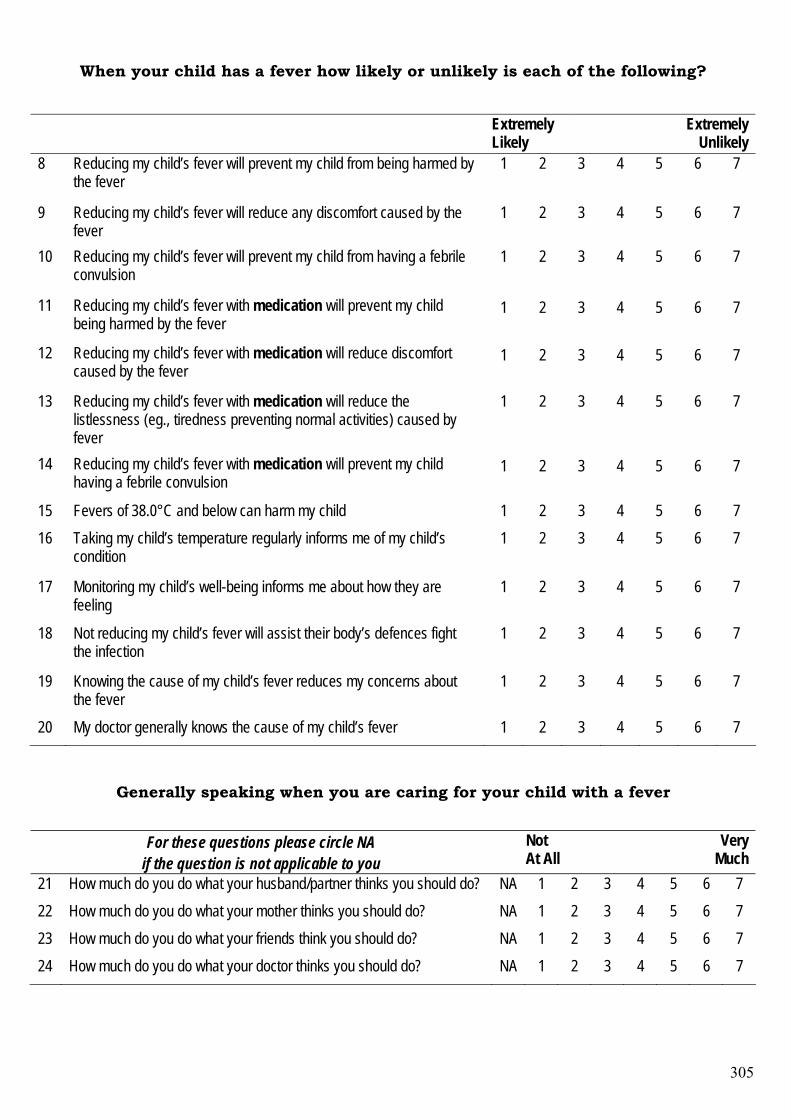
305
When your child has a fever how likely or unlikely is each of the following?
Extremely
Likely Extremely
Unlikely 8 Reducing my child’s fever will prevent my child from being harmed by
the fever 1 2 3 4 5 6 7
9 Reducing my child’s fever will reduce any discomfort caused by the fever
1 2 3 4 5 6 7
10 Reducing my child’s fever will prevent my child from having a febrile convulsion
1 2 3 4 5 6 7
11 Reducing my child’s fever with medication will prevent my child being harmed by the fever
1 2 3 4 5 6 7
12 Reducing my child’s fever with medication will reduce discomfort caused by the fever
1 2 3 4 5 6 7
13 Reducing my child’s fever with medication will reduce the listlessness (eg., tiredness preventing normal activities) caused by fever
1 2 3 4 5 6 7
14 Reducing my child’s fever with medication will prevent my child having a febrile convulsion
1 2 3 4 5 6 7
15 Fevers of 38.0°C and below can harm my child 1 2 3 4 5 6 7 16 Taking my child’s temperature regularly informs me of my child’s
condition 1 2 3 4 5 6 7
17 Monitoring my child’s well-being informs me about how they are feeling
1 2 3 4 5 6 7
18 Not reducing my child’s fever will assist their body’s defences fight the infection
1 2 3 4 5 6 7
19 Knowing the cause of my child’s fever reduces my concerns about the fever
1 2 3 4 5 6 7
20 My doctor generally knows the cause of my child’s fever 1 2 3 4 5 6 7
Generally speaking when you are caring for your child with a fever
For these questions please circle NA if the question is not applicable to you
Not At All
Very Much
21 How much do you do what your husband/partner thinks you should do? NA 1 2 3 4 5 6 7 22 How much do you do what your mother thinks you should do? NA 1 2 3 4 5 6 7 23 How much do you do what your friends think you should do? NA 1 2 3 4 5 6 7 24 How much do you do what your doctor thinks you should do? NA 1 2 3 4 5 6 7
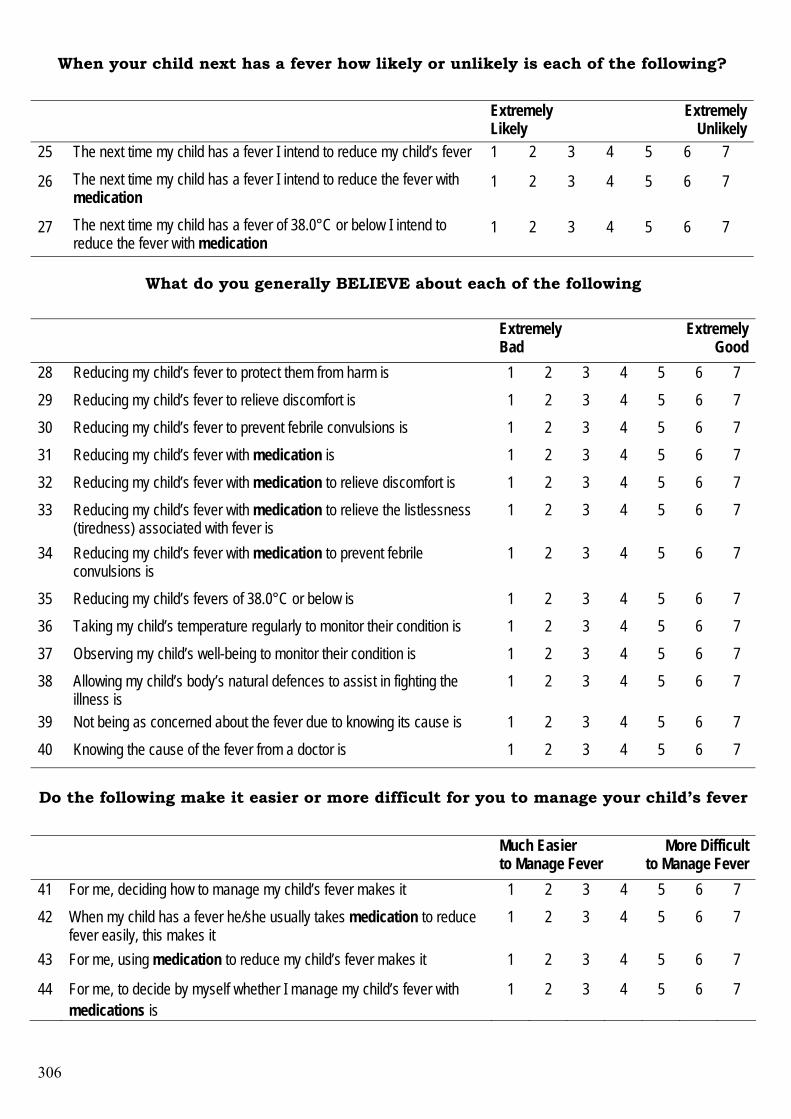
306
When your child next has a fever how likely or unlikely is each of the following?
Extremely
Likely Extremely
Unlikely 25 The next time my child has a fever I intend to reduce my child’s fever 1 2 3 4 5 6 7
26 The next time my child has a fever I intend to reduce the fever with medication
1 2 3 4 5 6 7
27 The next time my child has a fever of 38.0°C or below I intend to reduce the fever with medication
1 2 3 4 5 6 7
What do you generally BELIEVE about each of the following
Extremely Bad
Extremely Good
28 Reducing my child’s fever to protect them from harm is 1 2 3 4 5 6 7 29 Reducing my child’s fever to relieve discomfort is 1 2 3 4 5 6 7 30 Reducing my child’s fever to prevent febrile convulsions is 1 2 3 4 5 6 7 31 Reducing my child’s fever with medication is 1 2 3 4 5 6 7 32 Reducing my child’s fever with medication to relieve discomfort is 1 2 3 4 5 6 7 33 Reducing my child’s fever with medication to relieve the listlessness
(tiredness) associated with fever is 1 2 3 4 5 6 7
34 Reducing my child’s fever with medication to prevent febrile convulsions is
1 2 3 4 5 6 7
35 Reducing my child’s fevers of 38.0°C or below is 1 2 3 4 5 6 7 36 Taking my child’s temperature regularly to monitor their condition is 1 2 3 4 5 6 7 37 Observing my child’s well-being to monitor their condition is 1 2 3 4 5 6 7 38 Allowing my child’s body’s natural defences to assist in fighting the
illness is 1 2 3 4 5 6 7
39 Not being as concerned about the fever due to knowing its cause is 1 2 3 4 5 6 7 40 Knowing the cause of the fever from a doctor is 1 2 3 4 5 6 7
Do the following make it easier or more difficult for you to manage your child’s fever
Much Easier to Manage Fever
More Difficult to Manage Fever
41 For me, deciding how to manage my child’s fever makes it 1 2 3 4 5 6 7 42 When my child has a fever he/she usually takes medication to reduce
fever easily, this makes it 1 2 3 4 5 6 7
43 For me, using medication to reduce my child’s fever makes it 1 2 3 4 5 6 7
44 For me, to decide by myself whether I manage my child’s fever with medications is
1 2 3 4 5 6 7
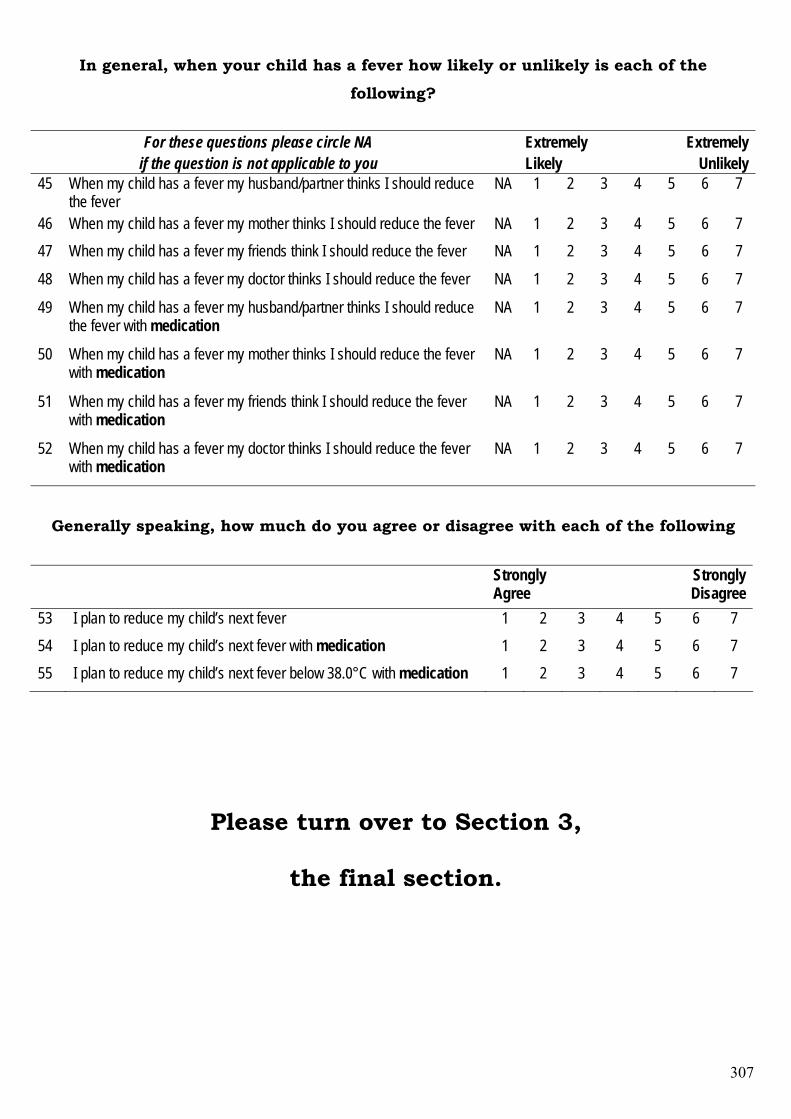
307
In general, when your child has a fever how likely or unlikely is each of the
following?
For these questions please circle NA if the question is not applicable to you
Extremely Likely
Extremely Unlikely
45 When my child has a fever my husband/partner thinks I should reduce the fever
NA 1 2 3 4 5 6 7
46 When my child has a fever my mother thinks I should reduce the fever NA 1 2 3 4 5 6 7 47 When my child has a fever my friends think I should reduce the fever NA 1 2 3 4 5 6 7
48 When my child has a fever my doctor thinks I should reduce the fever NA 1 2 3 4 5 6 7
49 When my child has a fever my husband/partner thinks I should reduce the fever with medication
NA 1 2 3 4 5 6 7
50 When my child has a fever my mother thinks I should reduce the fever with medication
NA 1 2 3 4 5 6 7
51 When my child has a fever my friends think I should reduce the fever with medication
NA 1 2 3 4 5 6 7
52 When my child has a fever my doctor thinks I should reduce the fever with medication
NA 1 2 3 4 5 6 7
Generally speaking, how much do you agree or disagree with each of the following
Strongly Agree
Strongly Disagree
53 I plan to reduce my child’s next fever 1 2 3 4 5 6 7 54 I plan to reduce my child’s next fever with medication 1 2 3 4 5 6 7 55 I plan to reduce my child’s next fever below 38.0°C with medication 1 2 3 4 5 6 7
Please turn over to Section 3,
the final section.
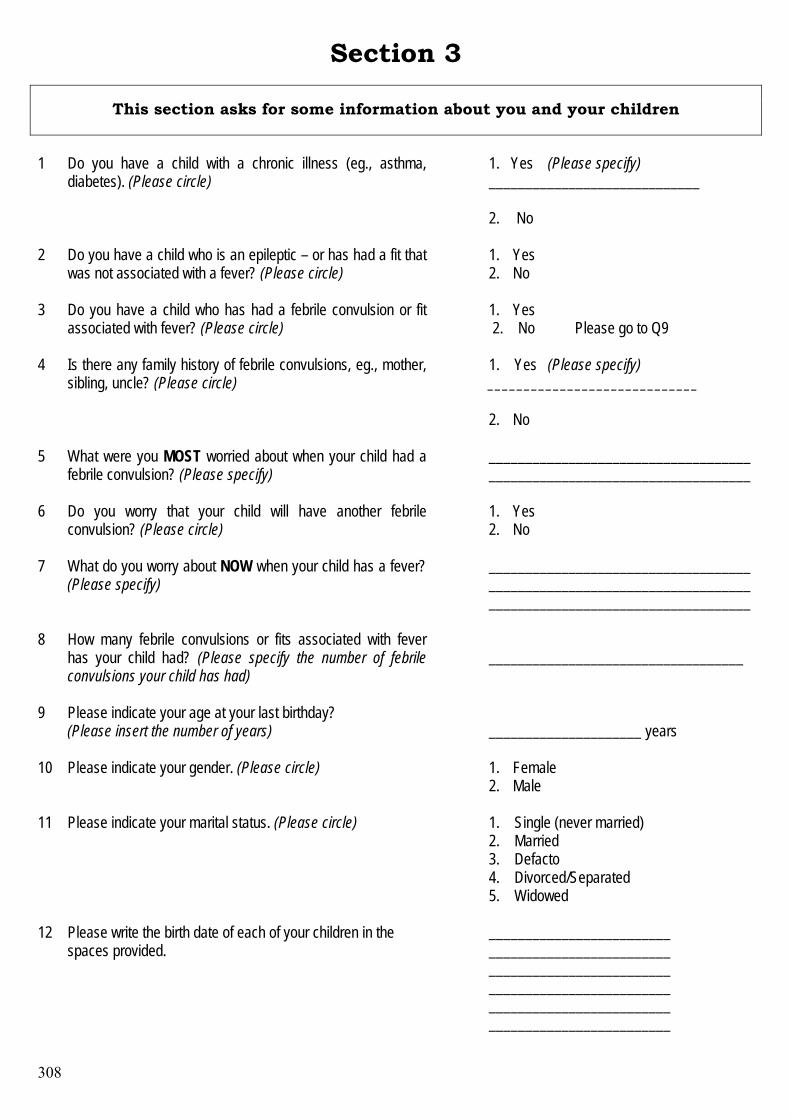
308
Section 3
This section asks for some information about you and your children 1
Do you have a child with a chronic illness (eg., asthma, diabetes). (Please circle)
1. Yes (Please specify) _____________________________ 2. No
2 Do you have a child who is an epileptic – or has had a fit that was not associated with a fever? (Please circle)
1. Yes 2. No
3 Do you have a child who has had a febrile convulsion or fit associated with fever? (Please circle)
1. Yes 2. No Please go to Q9
4 Is there any family history of febrile convulsions, eg., mother, sibling, uncle? (Please circle)
1. Yes (Please specify) _____________________________ 2. No
5 What were you MOST worried about when your child had a febrile convulsion? (Please specify)
________________________________________________________________________
6 Do you worry that your child will have another febrile convulsion? (Please circle)
1. Yes 2. No
7 What do you worry about NOW when your child has a fever? (Please specify)
________________________________________________________________________ ____________________________________
8 How many febrile convulsions or fits associated with fever has your child had? (Please specify the number of febrile convulsions your child has had)
___________________________________
9 Please indicate your age at your last birthday? (Please insert the number of years)
_____________________ years
10 Please indicate your gender. (Please circle) 1. Female 2. Male
11 Please indicate your marital status. (Please circle)
1. Single (never married) 2. Married 3. Defacto 4. Divorced/Separated 5. Widowed
12 Please write the birth date of each of your children in the spaces provided.
_________________________ _________________________ _________________________ _________________________ _________________________ _________________________
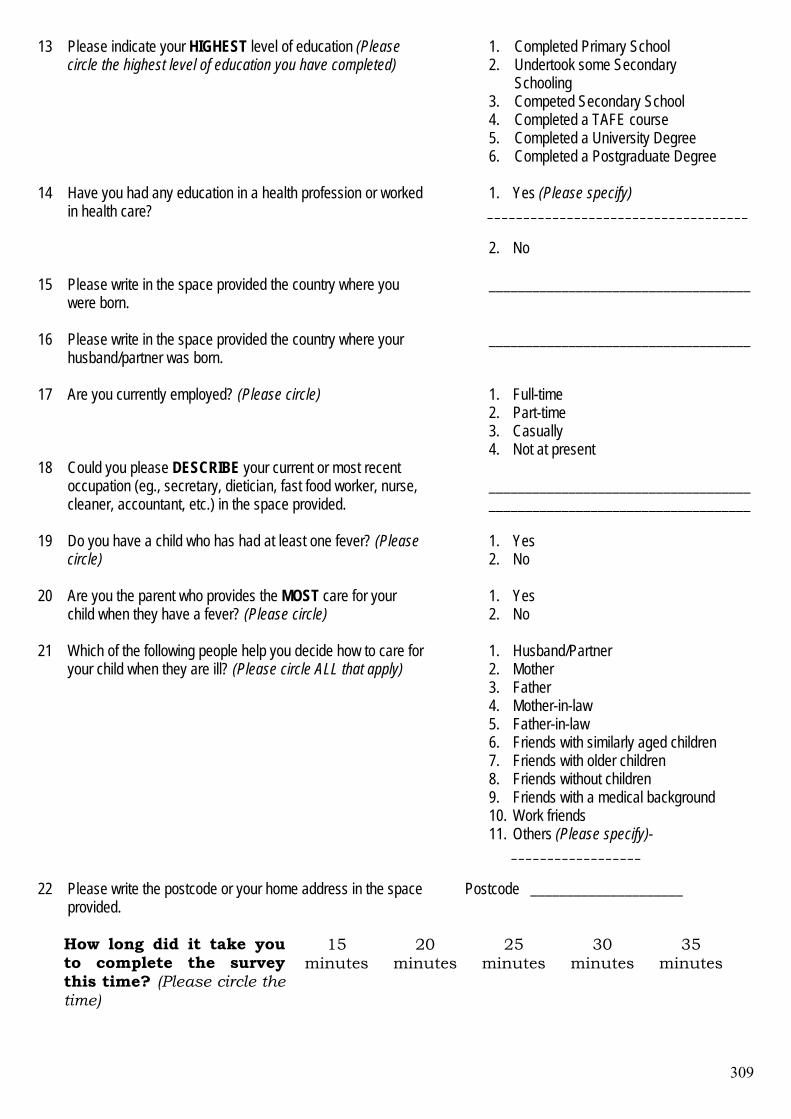
309
13 Please indicate your HIGHEST level of education (Please circle the highest level of education you have completed)
1. Completed Primary School 2. Undertook some Secondary Schooling 3. Competed Secondary School 4. Completed a TAFE course 5. Completed a University Degree 6. Completed a Postgraduate Degree
14 Have you had any education in a health profession or worked
in health care?
1. Yes (Please specify) ____________________________________ 2. No
15 Please write in the space provided the country where you were born.
____________________________________
16 Please write in the space provided the country where your husband/partner was born.
____________________________________
17 Are you currently employed? (Please circle) 1. Full-time 2. Part-time 3. Casually 4. Not at present
18 Could you please DESCRIBE your current or most recent occupation (eg., secretary, dietician, fast food worker, nurse, cleaner, accountant, etc.) in the space provided.
____________________________________ ____________________________________
19 Do you have a child who has had at least one fever? (Please circle)
1. Yes 2. No
20 Are you the parent who provides the MOST care for your child when they have a fever? (Please circle)
1. Yes 2. No
21 Which of the following people help you decide how to care for your child when they are ill? (Please circle ALL that apply)
1. Husband/Partner 2. Mother 3. Father 4. Mother-in-law 5. Father-in-law 6. Friends with similarly aged children 7. Friends with older children 8. Friends without children 9. Friends with a medical background 10. Work friends 11. Others (Please specify)-
__________________
22 Please write the postcode or your home address in the space provided.
Postcode _____________________
How long did it take you to complete the survey this time? (Please circle the time)
15
minutes
20
minutes
25
minutes
30
minutes
35
minutes
310
Main Study Documents
311
FEVER IN YOUNG CHILDREN
INFORMATION FOR PARENTS ABOUT THE SURVEY
This research is being undertaken as part of a Doctor of Philosophy degree and will be conducted under the guidance of experienced researchers from the School of Nursing at the Queensland University of Technology (QUT)
Researcher: Anne Walsh, School of Nursing, (QUT), 3864 3856 Principal Supervisor: Professor Helen Edwards, Head, School of Nursing, (QUT), 3864 3844
Raising a young child is not easy and when your child becomes ill this is even more difficult. Many parents are worried about their child’s fever when they are ill. They seek advice on how best to care for their child. There is a lot of the advice available. However, advice can vary, making it hard for parents to know what is the best thing to do. This can make parents even more worried about how to care for their sick child. As you have a child aged between 6 months and 5 years you will have had to look after a child with a fever. Not much is known about how Australian parents look after their children when they have a fever. Also, little is known about how Australian parents learn how to manage fever. As this is something every parent will have to do it is important to find this out. Then nurses and doctors can help parents during this worrying time. I would like to invite you to participate in a survey about children’s fever. The survey asks questions about how you know your child has a fever, how you manage fever in your children, what you know about fever and how you learnt to manage fever. There area also few questions asking for some personal information about you. It will take about 20 minutes to answer the questionnaire. Once you have answered the questions, or those you can, please place the questionnaire in the stamped, addressed envelope included in this package and return it to the researcher. What is learnt from the survey will be used to help Australian parents in the future when their child has a fever. I do not wish anyone to be identified through the information I collect. To make sure your records are confidential please do not write your name or address on the questionnaire. All the information I collect through the survey will be kept secure in a locked filing cabinet. Only I and my supervisors will have access to this information. No information about the study will be published in any form that would allow you to be recognised. Participating in the survey is voluntary. Answering the questionnaire should not pose any risk to you. The only inconvenience you should experience is the use of your time. If you have any questions about this research please contact me, Anne Walsh, on 3864 3856 or my supervisor, Prof. Helen Edwards on 3864 3844. You may also contact the Queensland University of Technology’s Research Ethics Officer on 3864 2340 if you have any concerns about the ethical conduct of this research.
312
FEVER IN YOUNG CHILDREN
INFORMATION FOR PARENTS ABOUT THE SURVEY
This research is being undertaken as part of a Doctor of Philosophy degree and will be conducted under the guidance of experienced researchers from the School of Nursing at the Queensland University of Technology (QUT)
Researcher: Anne Walsh, School of Nursing, (QUT), 3864 3856 Principal Supervisor: Professor Helen Edwards, Head, School of Nursing, (QUT), 3864 3844
Raising a young child is not easy and when your child becomes ill this is even more difficult. Many parents are worried about their child’s fever when they are ill. They seek advice on how best to care for their child. There is a lot of the advice available. However, advice can vary, making it hard for parents to know what is the best thing to do. This can make parents even more worried about how to care for their sick child. As you have a child aged between 6 months and 5 years you will have had to look after a child with a fever. Not much is known about how Australian parents look after their children when they have a fever. Also, little is known about how Australian parents learn how to manage fever. As this is something every parent will have to do it is important to find this out. Then nurses and doctors can help parents during this worrying time. I would like to invite you to participate in a survey about children’s fever. The survey asks questions about how you know your child has a fever, how you manage fever in your children, what you know about fever and how you learnt to manage fever. There are also a few questions asking for some personal information about you. It will take about 20 minutes to answer the questionnaire. Once you have answered the questions, or those you can, please place the questionnaire in the envelope included in this package and return it to the researcher at the child care centre this afternoon. If you prefer to take a few days to complete the questionnaire it can be returned in the enclosed envelope to the child care centre and placed in the sealed box in the director’s office. What is learnt from the survey will be used to help Australian parents in the future when their child has a fever. I do not wish anyone to be identified through the information I collect. To make sure your records are confidential please do not write your name or address on the questionnaire. All the information I collect through the survey will be kept secure in a locked filing cabinet. Only I and my supervisors will have access to this information. No information about the study will be published in any form that would allow you or your child care centre to be recognised. Participating in the survey is voluntary. Answering the questionnaire should not pose any risk to you. The only inconvenience you should experience is the use of your time. If you have any questions about this research please contact me, Anne Walsh, on 3864 3856 or my supervisor, Prof. Helen Edwards on 3864 3844. You may also contact the Queensland University of Technology’s Research Ethics Officer on 3864 2340 if you have any concerns about the ethical conduct of this research.
313
CHILDHOOD FEVER
MANAGEMENT
- - - INSTRUCTIONS - - -
1. The questionnaire asks for your general opinions about fever and managing fever in children aged between 6 months and 6 years.
2. It might be an idea to do this survey when the children are asleep and you
are less likely to be interrupted, it will take about 20 minutes to complete.
3. Please answer every question by marking your answer with a pen as
indicated. 4. In some instances certain questions may look alike but each one is
different. 5. There are no right or wrong answers. If you are unsure how to answer a
question please give the best answer you can. 6. In this questionnaire MEDICATION only refers to over the counter
medication, eg., Panadol and Nurofen, NOT to antibiotics. 7. After you have completed the questionnaire please place it in the box
provided in the Director’s office or return it at your earliest convenience to the Queensland University of Technology in the reply paid envelope supplied.
Thank you for offering to participate in this research.
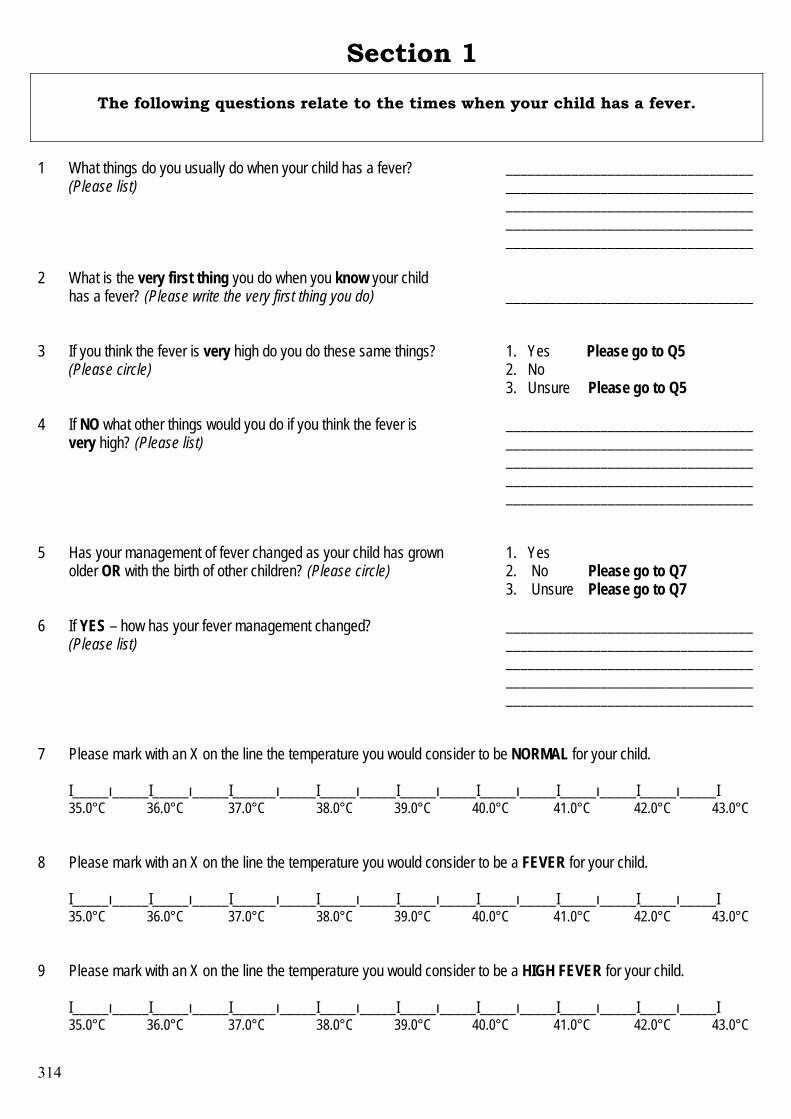
314
Section 1 The following questions relate to the times when your child has a fever.
1 What things do you usually do when your child has a fever?
(Please list)
____________________________________________________________________ __________________________________ __________________________________ __________________________________
2 What is the very first thing you do when you know your child has a fever? (Please write the very first thing you do)
__________________________________
3 If you think the fever is very high do you do these same things? (Please circle)
1. Yes Please go to Q5 2. No 3. Unsure Please go to Q5
4 If NO what other things would you do if you think the fever is very high? (Please list)
____________________________________________________________________ __________________________________ __________________________________ __________________________________
5 Has your management of fever changed as your child has grown older OR with the birth of other children? (Please circle)
1. Yes 2. No Please go to Q7 3. Unsure Please go to Q7
6 If YES – how has your fever management changed? (Please list)
____________________________________________________________________ __________________________________ __________________________________ __________________________________
7 Please mark with an X on the line the temperature you would consider to be NORMAL for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
8
Please mark with an X on the line the temperature you would consider to be a FEVER for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
9
Please mark with an X on the line the temperature you would consider to be a HIGH FEVER for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
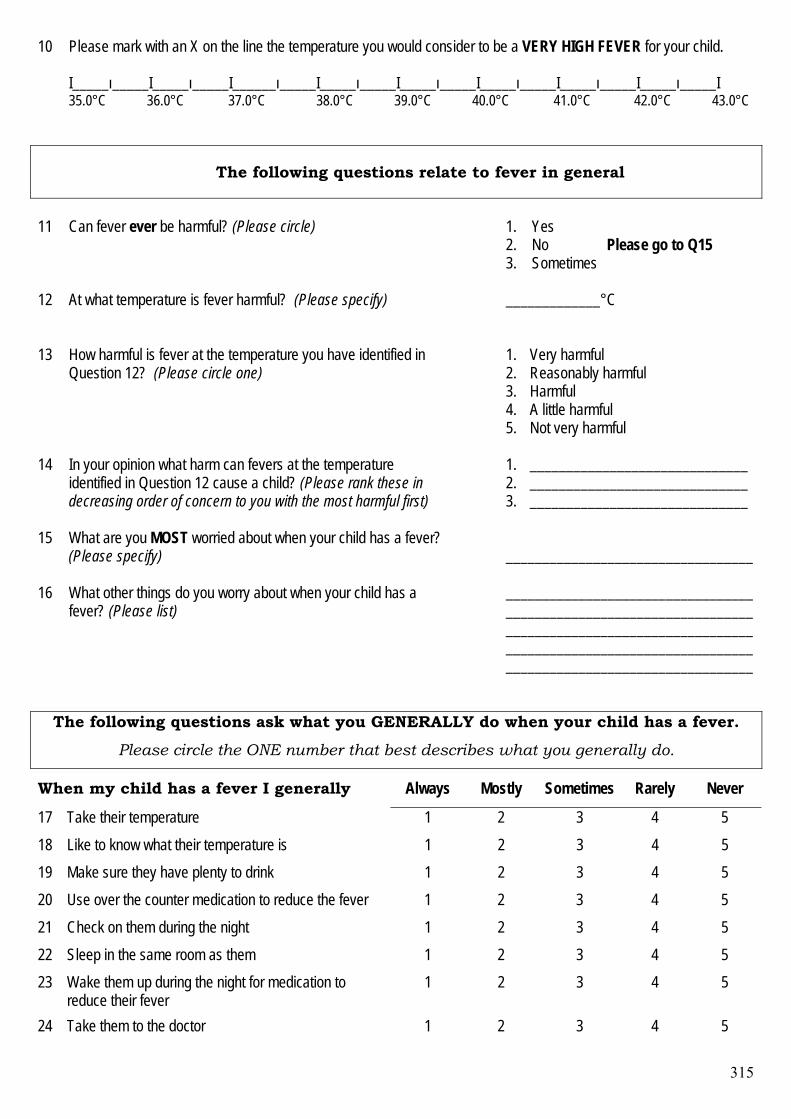
315
10 Please mark with an X on the line the temperature you would consider to be a VERY HIGH FEVER for your child.
I_____ı_____I_____ı_____I______ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I_____ı_____I 35.0°C 36.0°C 37.0°C 38.0°C 39.0°C 40.0°C 41.0°C 42.0°C 43.0°C
The following questions relate to fever in general
11
Can fever ever be harmful? (Please circle)
1. Yes 2. No Please go to Q15 3. Sometimes
12
At what temperature is fever harmful? (Please specify)
_____________°C
13
How harmful is fever at the temperature you have identified in Question 12? (Please circle one)
1. Very harmful 2. Reasonably harmful 3. Harmful 4. A little harmful 5. Not very harmful
14 In your opinion what harm can fevers at the temperature identified in Question 12 cause a child? (Please rank these in decreasing order of concern to you with the most harmful first)
1. ______________________________ 2. ______________________________ 3. ______________________________
15 What are you MOST worried about when your child has a fever? (Please specify)
__________________________________
16 What other things do you worry about when your child has a fever? (Please list)
____________________________________________________________________ __________________________________ __________________________________ __________________________________
The following questions ask what you GENERALLY do when your child has a fever.
Please circle the ONE number that best describes what you generally do.
When my child has a fever I generally Always Mostly Sometimes Rarely Never
17 Take their temperature 1 2 3 4 5 18 Like to know what their temperature is 1 2 3 4 5 19 Make sure they have plenty to drink 1 2 3 4 5 20 Use over the counter medication to reduce the fever 1 2 3 4 5 21 Check on them during the night 1 2 3 4 5 22 Sleep in the same room as them 1 2 3 4 5 23 Wake them up during the night for medication to
reduce their fever 1 2 3 4 5
24 Take them to the doctor 1 2 3 4 5
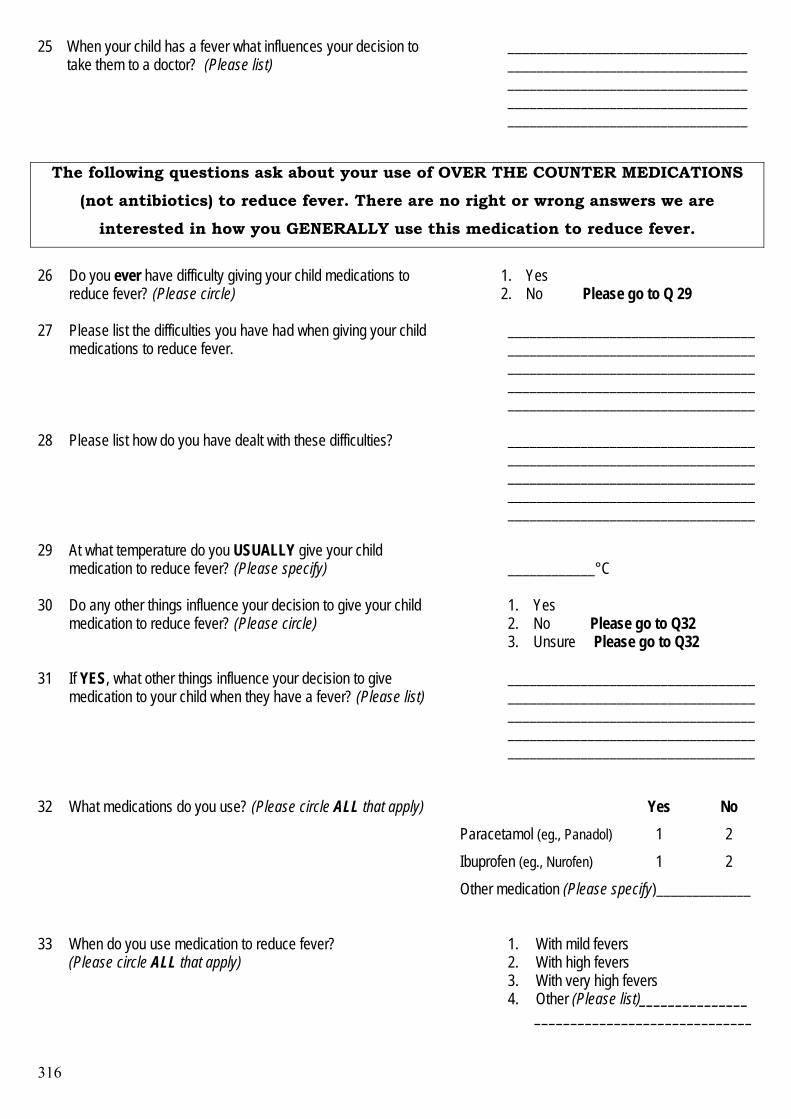
316
25 When your child has a fever what influences your decision to take them to a doctor? (Please list)
_____________________________________________________________________________________________________________________________________________________________________
The following questions ask about your use of OVER THE COUNTER MEDICATIONS
(not antibiotics) to reduce fever. There are no right or wrong answers we are
interested in how you GENERALLY use this medication to reduce fever.
26
Do you ever have difficulty giving your child medications to reduce fever? (Please circle)
1. Yes 2. No Please go to Q 29
27 Please list the difficulties you have had when giving your child
medications to reduce fever. __________________________________________________________________________________________________________________________________________________________________________
28 Please list how do you have dealt with these difficulties?
__________________________________________________________________________________________________________________________________________________________________________
29 At what temperature do you USUALLY give your child medication to reduce fever? (Please specify)
____________°C
30 Do any other things influence your decision to give your child
medication to reduce fever? (Please circle)
1. Yes 2. No Please go to Q32 3. Unsure Please go to Q32
31 If YES, what other things influence your decision to give medication to your child when they have a fever? (Please list)
______________________________________________________________________________________________________ ____________________________________________________________________
Yes No Paracetamol (eg., Panadol) 1 2 Ibuprofen (eg., Nurofen) 1 2
32 What medications do you use? (Please circle ALL that apply)
Other medication (Please specify)_____________
33 When do you use medication to reduce fever? (Please circle ALL that apply)
1. With mild fevers 2. With high fevers 3. With very high fevers 4. Other (Please list)_______________
______________________________
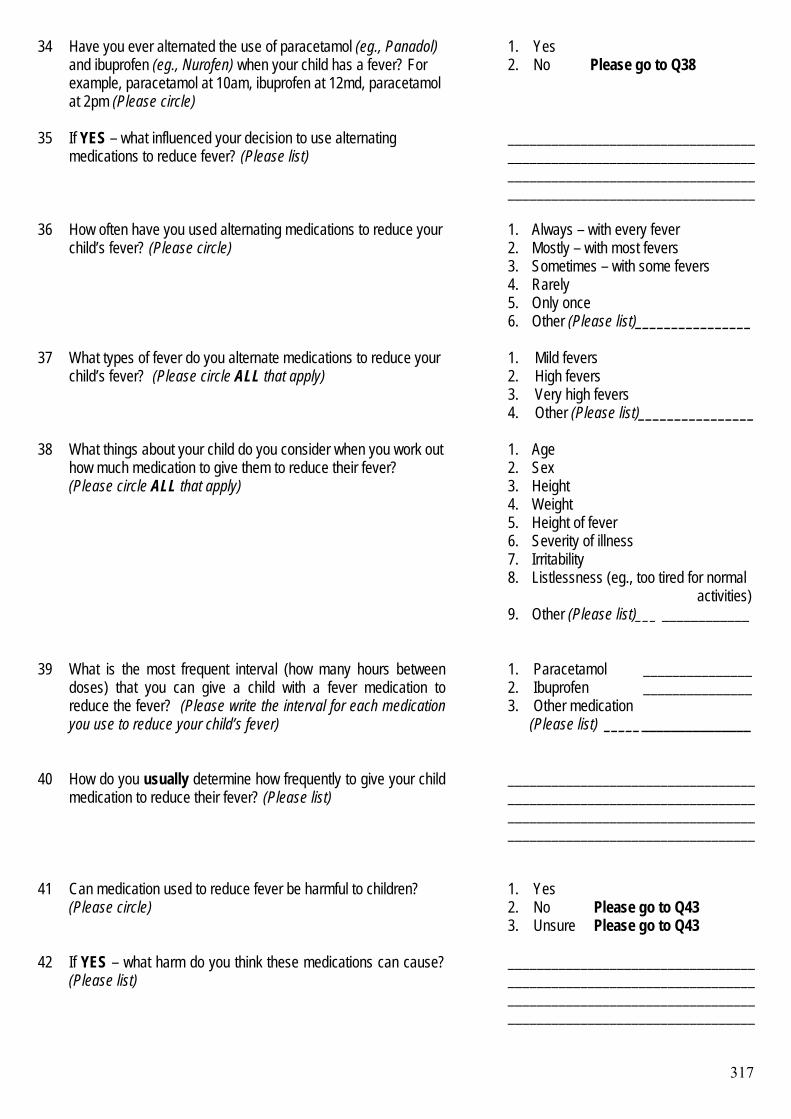
317
34 Have you ever alternated the use of paracetamol (eg., Panadol) and ibuprofen (eg., Nurofen) when your child has a fever? For example, paracetamol at 10am, ibuprofen at 12md, paracetamol at 2pm (Please circle)
1. Yes 2. No Please go to Q38
35 If YES – what influenced your decision to use alternating medications to reduce fever? (Please list)
____________________________________________________________________ ____________________________________________________________________
36 How often have you used alternating medications to reduce your child’s fever? (Please circle)
1. Always – with every fever 2. Mostly – with most fevers 3. Sometimes – with some fevers 4. Rarely 5. Only once 6. Other (Please list)________________
37 What types of fever do you alternate medications to reduce your child’s fever? (Please circle ALL that apply)
1. Mild fevers 2. High fevers 3. Very high fevers 4. Other (Please list)________________
38 What things about your child do you consider when you work out how much medication to give them to reduce their fever? (Please circle ALL that apply)
1. Age 2. Sex 3. Height 4. Weight 5. Height of fever 6. Severity of illness 7. Irritability 8. Listlessness (eg., too tired for normal activities) 9. Other (Please list)___ ____________
39 What is the most frequent interval (how many hours between doses) that you can give a child with a fever medication to reduce the fever? (Please write the interval for each medication you use to reduce your child’s fever)
1. Paracetamol _______________ 2. Ibuprofen _______________ 3. Other medication (Please list) ____________________
40 How do you usually determine how frequently to give your child medication to reduce their fever? (Please list)
________________________________________________________________________________________________________________________________________
41 Can medication used to reduce fever be harmful to children? (Please circle)
1. Yes 2. No Please go to Q43 3. Unsure Please go to Q43
42 If YES – what harm do you think these medications can cause? (Please list)
____________________________________________________________________ ____________________________________________________________________
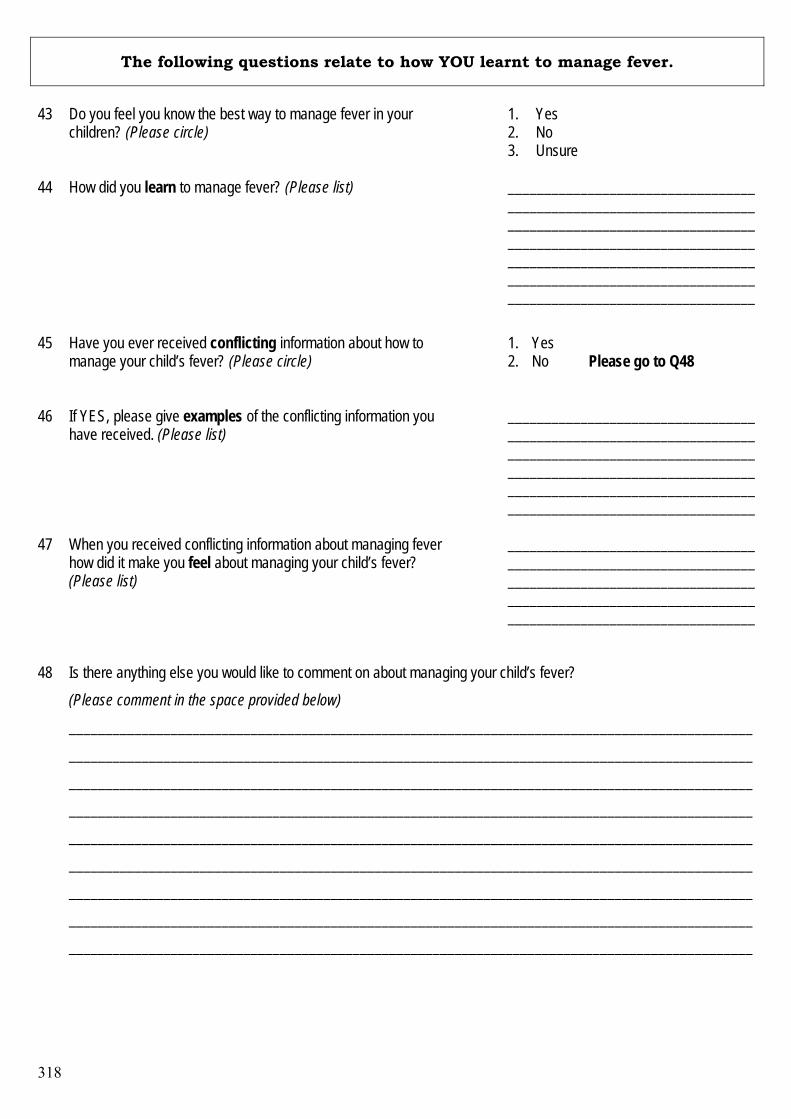
318
The following questions relate to how YOU learnt to manage fever.
43
Do you feel you know the best way to manage fever in your children? (Please circle)
1. Yes 2. No 3. Unsure
44 How did you learn to manage fever? (Please list)
____________________________________________________________________ __________________________________ __________________________________ ______________________________________________________________________________________________________
45 Have you ever received conflicting information about how to manage your child’s fever? (Please circle)
1. Yes 2. No Please go to Q48
46 If YES, please give examples of the conflicting information you
have received. (Please list)
____________________________________________________________________________________________________________________________________________________________________________________________________________
47 When you received conflicting information about managing fever how did it make you feel about managing your child’s fever? (Please list)
__________________________________ __________________________________ __________________________________ ____________________________________________________________________
48 Is there anything else you would like to comment on about managing your child’s fever? (Please comment in the space provided below)
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
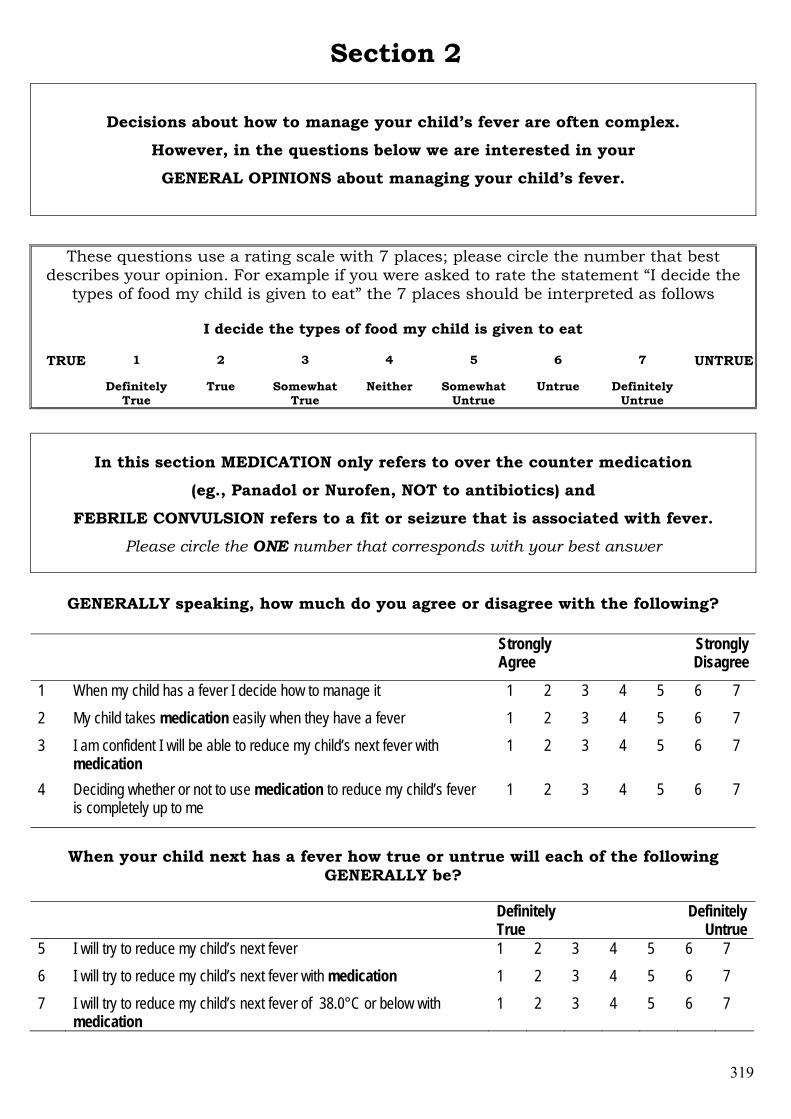
319
Section 2
Decisions about how to manage your child’s fever are often complex.
However, in the questions below we are interested in your
GENERAL OPINIONS about managing your child’s fever.
These questions use a rating scale with 7 places; please circle the number that best describes your opinion. For example if you were asked to rate the statement “I decide the
types of food my child is given to eat” the 7 places should be interpreted as follows
I decide the types of food my child is given to eat
1 2 3 4 5 6 7 TRUE
Definitely True
True Somewhat True
Neither Somewhat Untrue
Untrue Definitely Untrue
UNTRUE
In this section MEDICATION only refers to over the counter medication
(eg., Panadol or Nurofen, NOT to antibiotics) and
FEBRILE CONVULSION refers to a fit or seizure that is associated with fever. Please circle the ONE number that corresponds with your best answer
GENERALLY speaking, how much do you agree or disagree with the following?
Strongly Agree
Strongly Disagree
1 When my child has a fever I decide how to manage it 1 2 3 4 5 6 7 2 My child takes medication easily when they have a fever 1 2 3 4 5 6 7 3 I am confident I will be able to reduce my child’s next fever with
medication 1 2 3 4 5 6 7
4 Deciding whether or not to use medication to reduce my child’s fever is completely up to me
1 2 3 4 5 6 7
When your child next has a fever how true or untrue will each of the following
GENERALLY be?
Definitely True
Definitely Untrue
5 I will try to reduce my child’s next fever 1 2 3 4 5 6 7 6 I will try to reduce my child’s next fever with medication 1 2 3 4 5 6 7 7 I will try to reduce my child’s next fever of 38.0°C or below with
medication 1 2 3 4 5 6 7
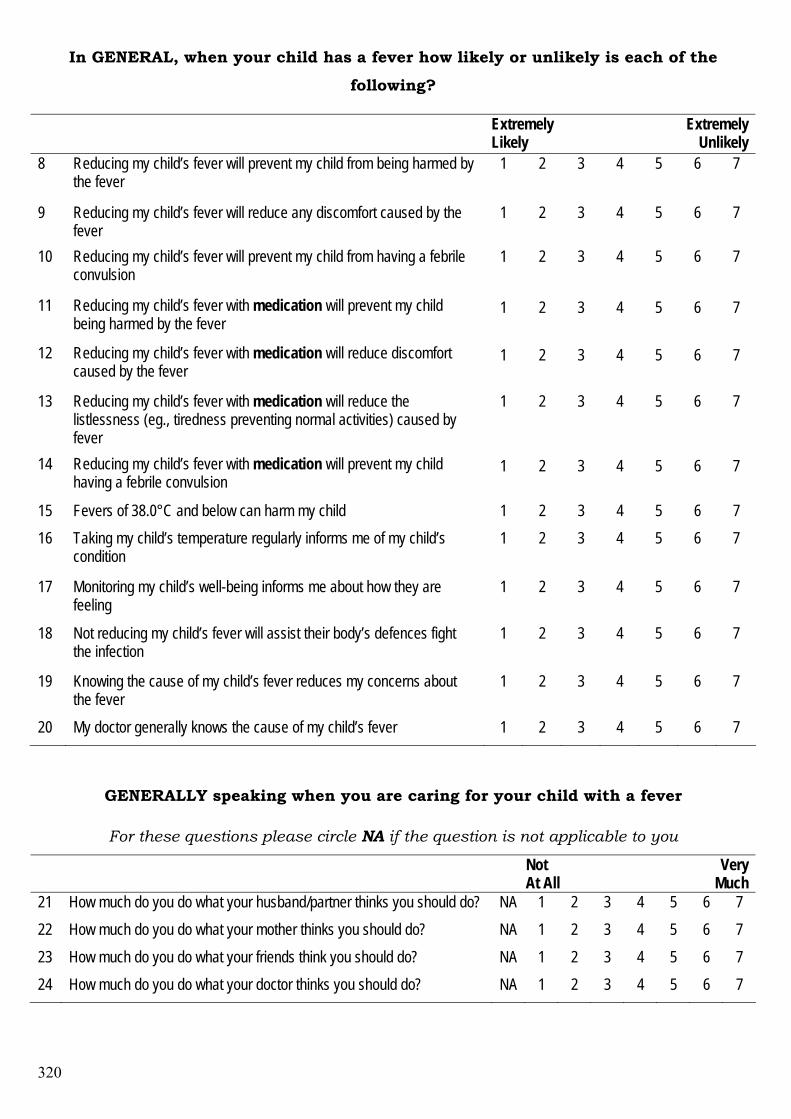
320
In GENERAL, when your child has a fever how likely or unlikely is each of the
following?
Extremely Likely
Extremely Unlikely
8 Reducing my child’s fever will prevent my child from being harmed by the fever
1 2 3 4 5 6 7
9 Reducing my child’s fever will reduce any discomfort caused by the fever
1 2 3 4 5 6 7
10 Reducing my child’s fever will prevent my child from having a febrile convulsion
1 2 3 4 5 6 7
11 Reducing my child’s fever with medication will prevent my child being harmed by the fever
1 2 3 4 5 6 7
12 Reducing my child’s fever with medication will reduce discomfort caused by the fever
1 2 3 4 5 6 7
13 Reducing my child’s fever with medication will reduce the listlessness (eg., tiredness preventing normal activities) caused by fever
1 2 3 4 5 6 7
14 Reducing my child’s fever with medication will prevent my child having a febrile convulsion
1 2 3 4 5 6 7
15 Fevers of 38.0°C and below can harm my child 1 2 3 4 5 6 7 16 Taking my child’s temperature regularly informs me of my child’s
condition 1 2 3 4 5 6 7
17 Monitoring my child’s well-being informs me about how they are feeling
1 2 3 4 5 6 7
18 Not reducing my child’s fever will assist their body’s defences fight the infection
1 2 3 4 5 6 7
19 Knowing the cause of my child’s fever reduces my concerns about the fever
1 2 3 4 5 6 7
20 My doctor generally knows the cause of my child’s fever 1 2 3 4 5 6 7
GENERALLY speaking when you are caring for your child with a fever
For these questions please circle NA if the question is not applicable to you
Not At All
Very Much
21 How much do you do what your husband/partner thinks you should do? NA 1 2 3 4 5 6 7 22 How much do you do what your mother thinks you should do? NA 1 2 3 4 5 6 7 23 How much do you do what your friends think you should do? NA 1 2 3 4 5 6 7 24 How much do you do what your doctor thinks you should do? NA 1 2 3 4 5 6 7
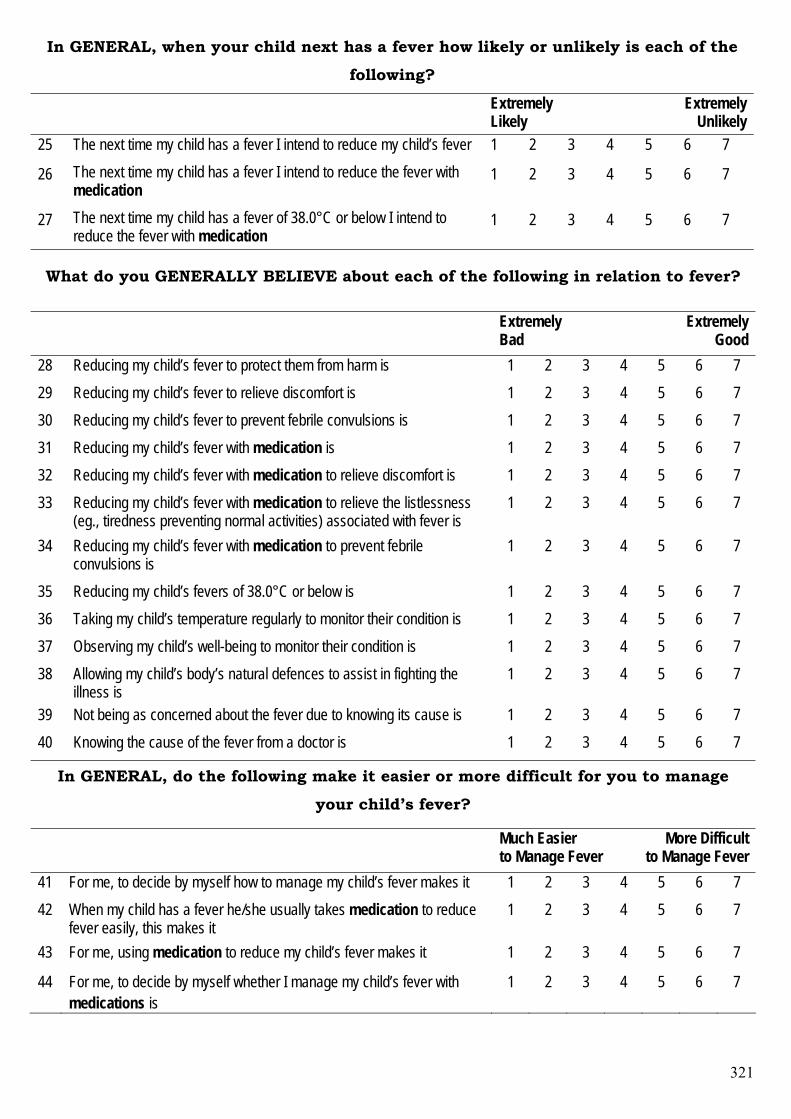
321
In GENERAL, when your child next has a fever how likely or unlikely is each of the
following?
Extremely Likely
Extremely Unlikely
25 The next time my child has a fever I intend to reduce my child’s fever 1 2 3 4 5 6 7
26 The next time my child has a fever I intend to reduce the fever with medication
1 2 3 4 5 6 7
27 The next time my child has a fever of 38.0°C or below I intend to reduce the fever with medication
1 2 3 4 5 6 7
What do you GENERALLY BELIEVE about each of the following in relation to fever?
Extremely Bad
Extremely Good
28 Reducing my child’s fever to protect them from harm is 1 2 3 4 5 6 7 29 Reducing my child’s fever to relieve discomfort is 1 2 3 4 5 6 7 30 Reducing my child’s fever to prevent febrile convulsions is 1 2 3 4 5 6 7 31 Reducing my child’s fever with medication is 1 2 3 4 5 6 7 32 Reducing my child’s fever with medication to relieve discomfort is 1 2 3 4 5 6 7 33 Reducing my child’s fever with medication to relieve the listlessness
(eg., tiredness preventing normal activities) associated with fever is 1 2 3 4 5 6 7
34 Reducing my child’s fever with medication to prevent febrile convulsions is
1 2 3 4 5 6 7
35 Reducing my child’s fevers of 38.0°C or below is 1 2 3 4 5 6 7 36 Taking my child’s temperature regularly to monitor their condition is 1 2 3 4 5 6 7 37 Observing my child’s well-being to monitor their condition is 1 2 3 4 5 6 7 38 Allowing my child’s body’s natural defences to assist in fighting the
illness is 1 2 3 4 5 6 7
39 Not being as concerned about the fever due to knowing its cause is 1 2 3 4 5 6 7 40 Knowing the cause of the fever from a doctor is 1 2 3 4 5 6 7
In GENERAL, do the following make it easier or more difficult for you to manage
your child’s fever?
Much Easier to Manage Fever
More Difficult to Manage Fever
41 For me, to decide by myself how to manage my child’s fever makes it 1 2 3 4 5 6 7 42 When my child has a fever he/she usually takes medication to reduce
fever easily, this makes it 1 2 3 4 5 6 7
43 For me, using medication to reduce my child’s fever makes it 1 2 3 4 5 6 7
44 For me, to decide by myself whether I manage my child’s fever with medications is
1 2 3 4 5 6 7
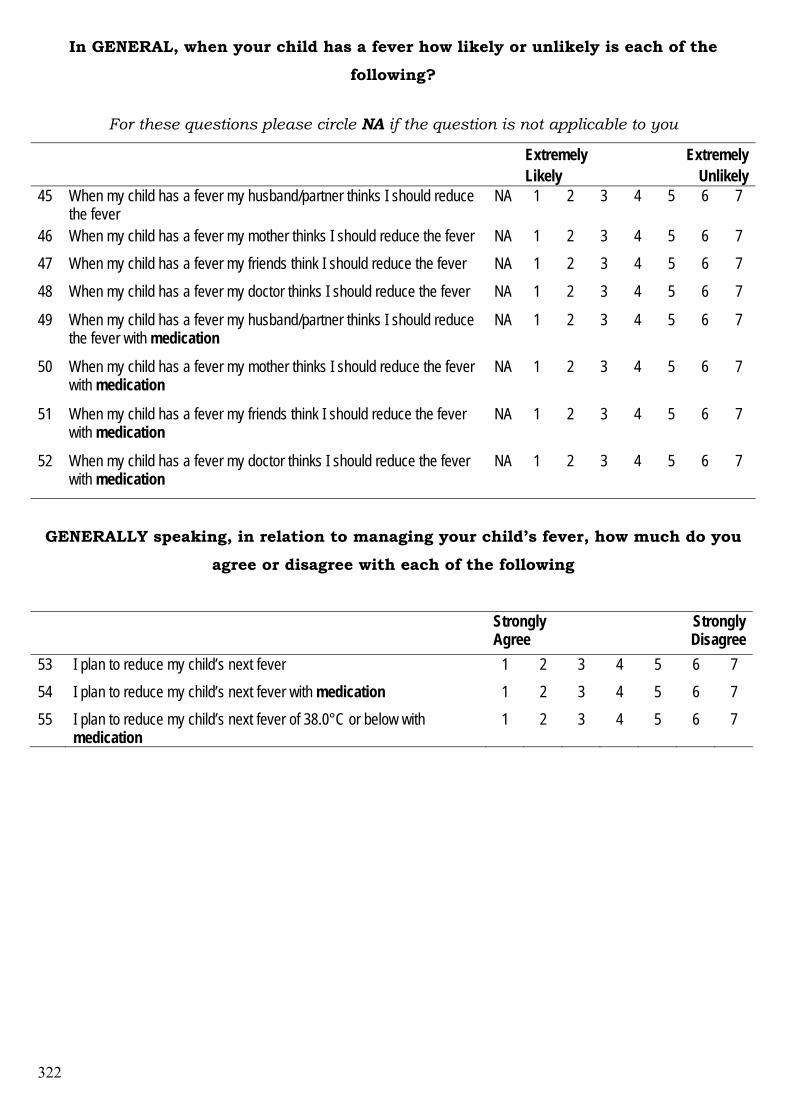
322
In GENERAL, when your child has a fever how likely or unlikely is each of the
following?
For these questions please circle NA if the question is not applicable to you
Extremely Likely
Extremely Unlikely
45 When my child has a fever my husband/partner thinks I should reduce the fever
NA 1 2 3 4 5 6 7
46 When my child has a fever my mother thinks I should reduce the fever NA 1 2 3 4 5 6 7 47 When my child has a fever my friends think I should reduce the fever NA 1 2 3 4 5 6 7
48 When my child has a fever my doctor thinks I should reduce the fever NA 1 2 3 4 5 6 7
49 When my child has a fever my husband/partner thinks I should reduce the fever with medication
NA 1 2 3 4 5 6 7
50 When my child has a fever my mother thinks I should reduce the fever with medication
NA 1 2 3 4 5 6 7
51 When my child has a fever my friends think I should reduce the fever with medication
NA 1 2 3 4 5 6 7
52 When my child has a fever my doctor thinks I should reduce the fever with medication
NA 1 2 3 4 5 6 7
GENERALLY speaking, in relation to managing your child’s fever, how much do you
agree or disagree with each of the following
Strongly Agree
Strongly Disagree
53 I plan to reduce my child’s next fever 1 2 3 4 5 6 7 54 I plan to reduce my child’s next fever with medication 1 2 3 4 5 6 7 55 I plan to reduce my child’s next fever of 38.0°C or below with
medication 1 2 3 4 5 6 7
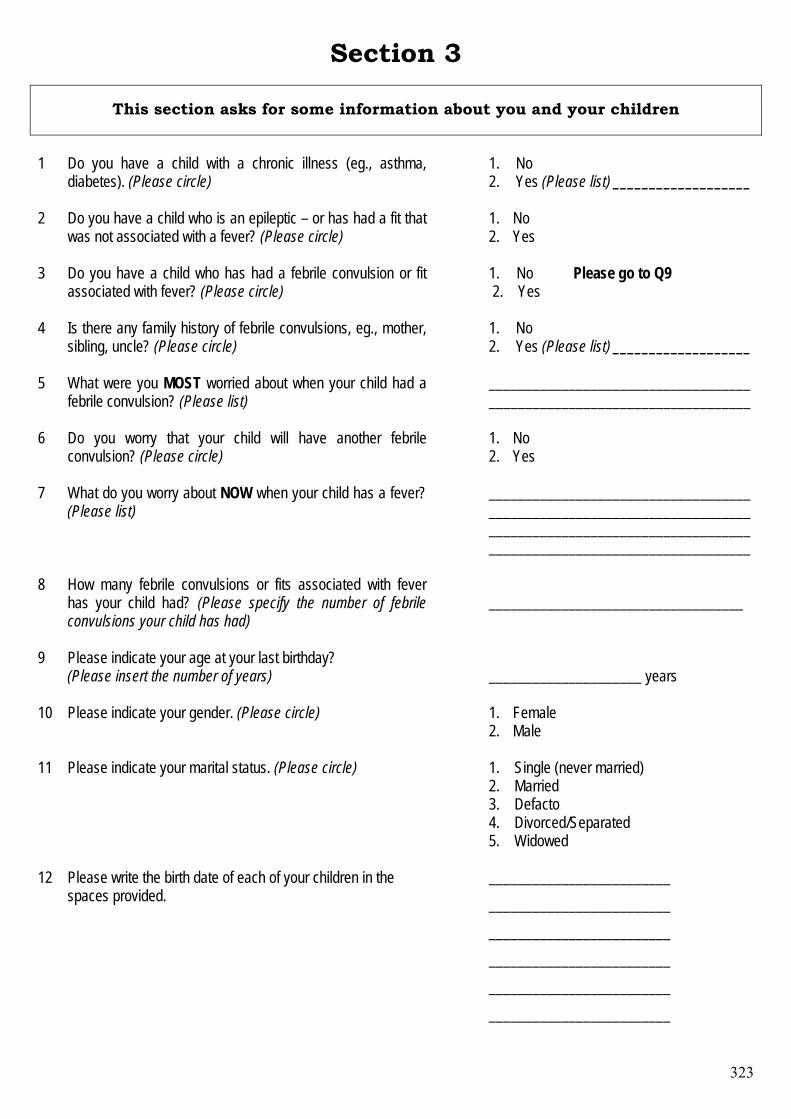
323
Section 3
This section asks for some information about you and your children 1
Do you have a child with a chronic illness (eg., asthma, diabetes). (Please circle)
1. No 2. Yes (Please list) ___________________
2 Do you have a child who is an epileptic – or has had a fit that was not associated with a fever? (Please circle)
1. No 2. Yes
3 Do you have a child who has had a febrile convulsion or fit associated with fever? (Please circle)
1. No Please go to Q9 2. Yes
4 Is there any family history of febrile convulsions, eg., mother, sibling, uncle? (Please circle)
1. No 2. Yes (Please list) ___________________
5 What were you MOST worried about when your child had a febrile convulsion? (Please list)
________________________________________________________________________
6 Do you worry that your child will have another febrile convulsion? (Please circle)
1. No 2. Yes
7 What do you worry about NOW when your child has a fever? (Please list)
________________________________________________________________________ ____________________________________ ____________________________________
8 How many febrile convulsions or fits associated with fever has your child had? (Please specify the number of febrile convulsions your child has had)
___________________________________
9 Please indicate your age at your last birthday? (Please insert the number of years)
_____________________ years
10 Please indicate your gender. (Please circle) 1. Female 2. Male
11 Please indicate your marital status. (Please circle)
1. Single (never married) 2. Married 3. Defacto 4. Divorced/Separated 5. Widowed
12 Please write the birth date of each of your children in the spaces provided.
_________________________ _________________________ _________________________ _________________________ _________________________ _________________________
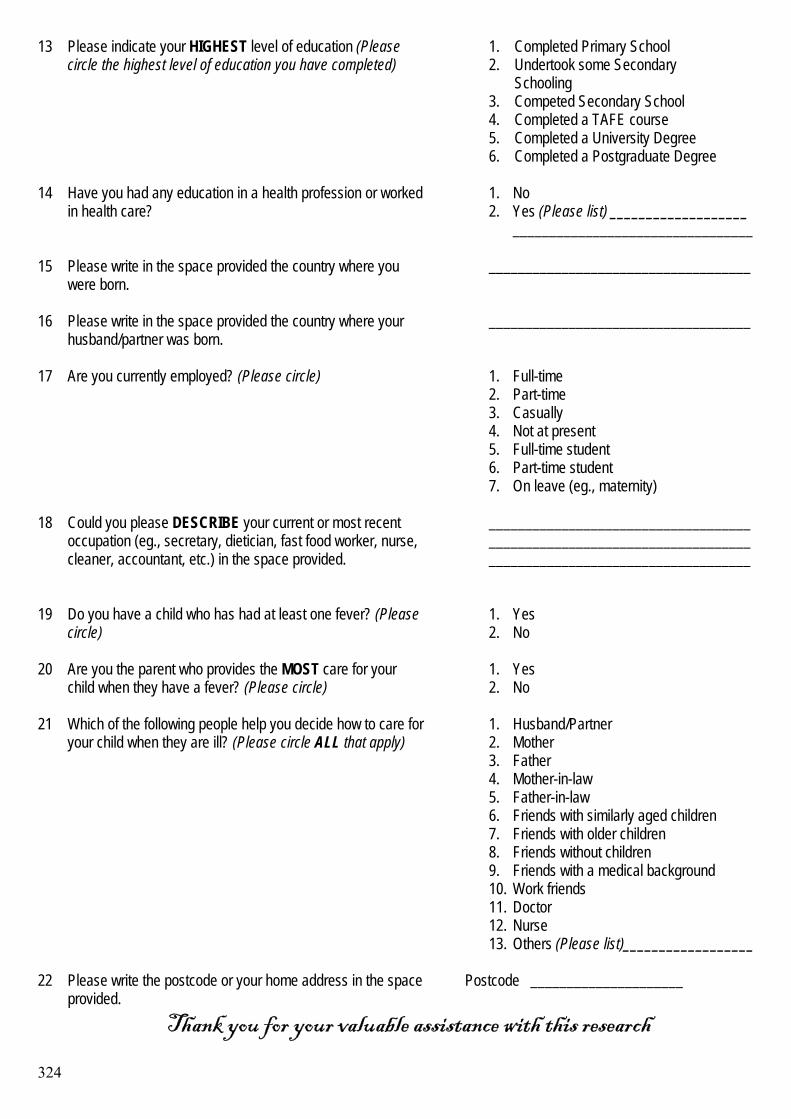
324
13 Please indicate your HIGHEST level of education (Please circle the highest level of education you have completed)
1. Completed Primary School 2. Undertook some Secondary Schooling 3. Competed Secondary School 4. Completed a TAFE course 5. Completed a University Degree 6. Completed a Postgraduate Degree
14 Have you had any education in a health profession or worked
in health care?
1. No 2. Yes (Please list) ___________________
_________________________________
15 Please write in the space provided the country where you were born.
____________________________________
16 Please write in the space provided the country where your husband/partner was born.
____________________________________
17 Are you currently employed? (Please circle)
1. Full-time 2. Part-time 3. Casually 4. Not at present 5. Full-time student 6. Part-time student 7. On leave (eg., maternity)
18 Could you please DESCRIBE your current or most recent occupation (eg., secretary, dietician, fast food worker, nurse, cleaner, accountant, etc.) in the space provided.
____________________________________ ____________________________________ ____________________________________
19 Do you have a child who has had at least one fever? (Please circle)
1. Yes 2. No
20 Are you the parent who provides the MOST care for your child when they have a fever? (Please circle)
1. Yes 2. No
21 Which of the following people help you decide how to care for your child when they are ill? (Please circle ALL that apply)
1. Husband/Partner 2. Mother 3. Father 4. Mother-in-law 5. Father-in-law 6. Friends with similarly aged children 7. Friends with older children 8. Friends without children 9. Friends with a medical background 10. Work friends 11. Doctor 12. Nurse 13. Others (Please list)__________________
22 Please write the postcode or your home address in the space provided.
Postcode _____________________
Thank you for your valuable assistance with this research
325
Appendix 3
Statements of Author Co-Contributions to
Manuscripts
326
Walsh, A. M., & Edwards, H. E. (2006). Management of childhood fever by
parents: literature review. Journal of Advanced Nursing, 54(2), 217-227.
In the case of this article in Chapter 3
Statement of Contribution of Co-Authors for Thesis by Published Paper The authors listed below have certified* that: 1. they meet the criteria for authorship in that they have participated in the conception, execution, or
interpretation, of at least that part of the publication in their field of expertise; 2. they take public responsibility for their part of the publication, except for the responsible author
who accepts overall responsibility for the publication; 3. there are no other authors of the publication according to these criteria; 4. potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or publisher
of journals or other publications, and (c) the head of the responsible academic unit, and 5. they agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
Contributor Statement of contribution*
Anne Walsh
5th August 2004
Study design, recruited participants, collected and analysed data, wrote the manuscript.
Prof. Helen Edwards
Study design and critical revision of the manuscript for important intellectual content, supervised the study.
Principal Supervisor Confirmation I have sighted email or other correspondence from all Co-authors confirming their certifying authorship and. _______________________ ____________________ ______________________ Name Signature Date
327
Walsh, A. M., Edwards, H. E., & Fraser, J. A. (2007 Online Early). Influences on parents' fever management: beliefs, experiences and information sources. Journal of Clinical Nursing, doi: 10.1111/j.1365-2702.2006.01890.x.
In the case of this article in Chapter 5:
Statement of Contribution of Co-Authors for Thesis by Published Paper
The authors listed below have certified* that: 6. they meet the criteria for authorship in that they have participated in the conception, execution, or
interpretation, of at least that part of the publication in their field of expertise; 7. they take public responsibility for their part of the publication, except for the responsible author
who accepts overall responsibility for the publication; 8. there are no other authors of the publication according to these criteria; 9. potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or publisher
of journals or other publications, and (c) the head of the responsible academic unit, and 10. they agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
Contributor Statement of contribution*
Anne Walsh
5th August 2004
Study design, recruited participants, collected and analysed data, wrote the manuscript.
Prof. Helen Edwards
Study design and critical revision of the manuscript for important intellectual content, supervised the study.
Dr. Jenny Fraser
Assisted in study design, study supervision and manuscript revision.
Principal Supervisor Confirmation I have sighted email or other correspondence from all Co-authors confirming their certifying authorship and. _______________________ ____________________ ______________________ Name Signature Date

328
Walsh, A. M., Edwards, H., & Fraser, J. (Under Review). Underpinned by fear: a
community study of parents' fever management with young children. Journal of Advanced Nursing.
In the case of this article in Chapter 6:
Statement of Contribution of Co-Authors for Thesis by Published Paper
The authors listed below have certified* that: 11. they meet the criteria for authorship in that they have participated in the conception, execution, or
interpretation, of at least that part of the publication in their field of expertise; 12. they take public responsibility for their part of the publication, except for the responsible author
who accepts overall responsibility for the publication; 13. there are no other authors of the publication according to these criteria; 14. potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or publisher
of journals or other publications, and (c) the head of the responsible academic unit, and 15. they agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
Contributor Statement of contribution*
Anne Walsh
5th August 2004
Study design, recruited participants, collected and analysed data, wrote the manuscript.
Prof. Helen Edwards
Study design and critical revision of the manuscript for important intellectual content, supervised the study.
Dr. Jenny Fraser
Assisted in study design, study supervision and manuscript revision.
Principal Supervisor Confirmation I have sighted email or other correspondence from all Co-authors confirming their certifying authorship and. _______________________ ____________________ ______________________ Name Signature Date
329
Walsh, A., Edwards, H., & Fraser, J. (2007 Online Early). Over-the-counter
medication use for childhood fever: A cross-sectional study of Australian parents. Journal of Paediatrics and Child Health, doi:10.1111/j.1440-1754.2007.01161.x.
In the case of this article in Chapter 6:
Statement of Contribution of Co-Authors for Thesis by Published Paper The authors listed below have certified* that: 16. they meet the criteria for authorship in that they have participated in the conception, execution, or
interpretation, of at least that part of the publication in their field of expertise; 17. they take public responsibility for their part of the publication, except for the responsible author
who accepts overall responsibility for the publication; 18. there are no other authors of the publication according to these criteria; 19. potential conflicts of interest have been disclosed to (a) granting bodies, (b) the editor or publisher
of journals or other publications, and (c) the head of the responsible academic unit, and 20. they agree to the use of the publication in the student’s thesis and its publication on the
Australasian Digital Thesis database consistent with any limitations set by publisher requirements.
Contributor Statement of contribution*
Anne Walsh
5th August 2004
Study design, recruited participants, collected and analysed data, wrote the manuscript.
Prof. Helen Edwards
Study design and critical revision of the manuscript for important intellectual content, supervised the study.
Dr. Jenny Fraser
Assisted in study design, study supervision and manuscript revision.
Principal Supervisor Confirmation I have sighted email or other correspondence from all Co-authors confirming their certifying authorship and. _______________________ ____________________ ______________________ Name Signature Date
330
Appendix 4
Conference Abstracts
331
AUSTRALASIAN SOCIETY OF BEHAVIOURAL HEALTH AND MEDICINE (ASBHM)
4th Annual Scientific Conference Spencer on Byron, Takapuna
Auckland, New Zealand 9-11 February 2006
EDUCATION BASED ON THE THEORY OF PLANNED BEHAVIOR
PROMOTES EVIDENCE-BASED FEVER MANAGEMENT
Authors: 1Walsh, A., 1Edwards, H., 1Courtney, M., 2Wilson, J., 2Monaghan, S. & 2Young, J. 1 Queensland University of Technology, Australia 2 Royal Children's Hospital, Brisbane, Australia
Introduction: Reports of concerns about fever, inconsistent fever management practices and health professionals’ escalating inappropriate use of antipyretics continue despite evidence of benefits of mild to moderate fever. Current practices of alternating antipyretics to reduce fever and maintain ‘normal’ temperature highlights concerns. This controlled experiment explored the effectiveness of a peer education program (PEP) based on the Theory of Planned Behavior in changing paediatric nurses’ intentions to administer antipyretics to febrile children. Methods: The eight week program consisted of four one-hour sessions repeated regularly over two-weeks. The program promoted peer education and support and targeted peer groups. All nurses employed in paediatric medical wards of two metropolitan paediatric hospitals in Australia during the eight month research period were eligible to participate in the surveys. Hospitals were allocated to experimental and control conditions. The PEP was delivered to nurses at the experimental hospital only. Data were collected one month pre-PEP, one month post-PEP and four months post-PEP (latency data) by survey and chart audit. Charts of all eligible children admitted during data collection periods were audited. Results: The PEP significantly reduced nurses’ intentions to administer antipyretics to the next febrile child (p=0.01). Practice changes were demonstrated by chart audits. Mean temperatures when antipyretics were administered were higher one month post-PEP than pre-PEP (38.5°C vs 38.1°C), however, this was not maintained in latency data (38.2°C). Normative influences over intentions (p=0.01) and nurses’ perception of personal control reduced significantly (p=0.01) highlighting increased awareness of external influences over antipyretic administration. Following the program nurses were significantly less likely to believe their colleagues (p=0.00) or medical officers (p=0.03) expected them to administer antipyretics. Additionally they were less likely to comply with colleagues’ (p=0.01) or medical officers’ (p=0.05) expectations for antipyretic administration post PEP. Conclusions: The program successfully promoted evidence-based intentions and practices by reducing normative influences and incorrect perceptions of control over antipyretic administration.

332
AUSTRALIAN CONFEDERATION OF PAEDIATRIC AND CHILD HEALTH NURSES (ACPCHN)
9th International Biennial Paediatric and Child Health Nurses Conference,
17-19 May, 2006, Melbourne, Australia
PARENTS’ MANAGEMENT OF CHILDHOOD FEVER – THE NEED FOR EVIDENCE BASED EDUCATION
Authors: Anne Walsh, Helen Edwards, Jenny Fraser. School of Nursing, Queensland University of Technology Background Fevers are common events in the lives of young children. International studies continue to report parents’ concerns about childhood fevers. Parents find fevers frightening and base care on inaccurate information from other parents, friends, health professionals, parenting books and more recently the media and Internet rather than the latest scientific evidence. This research explores previously unknown fever management practices, concerns and information sources of Australian parents. Method Four hundred and one Queensland parents completed a self-report survey using an instrument developed from the literature and focused discussions with 15 parents. The survey identified parents’ definitions of fever, fever management practices, concerns and influences on their practices. Findings Parents define fever as 36.7°C to 41.2°C (mode 38.0°C). Most parents (91%) actively reduce fever with antipyretics for temperatures ranging from 37.0°C to 40.0°C (mode 38.0°C). Antipyretics administration is influenced by discomfort, distress or general unwellness (87%) and pain (32%). Parents are most concerned about febrile convulsions (45%), the cause of fever (26%), brain damage (23%) and serious illness (28%). They seek medical assistance for fevers considered ‘very high’ (38.0°C to 43.0°C, mode 40.0°C) (65%), symptoms of febrile illnesses such as cough, increased respirations and pain (44%), length of time child has been febrile (42%) and general unwellness (21%). Fever management is learnt from medical practitioners (61%), child health books (27%), mothers/mothers-in-law (23%) and nurses (16%) and through past experience (39%). Nearly half the parents (42%) had received conflicting information about fever management which made them feel confused (29%), concerned (18%), unsure about fever management (40%) or angry/frustrated (16%). Conclusions and Recommendations Parents’ fever management is not based on the latest scientific evidence. Paediatric and child health nurses are ideally placed to reduce parents’ concerns, increase their confidence and reduce the unnecessary use of health resources related to childhood fever. Key words: fever, parents’ concerns, parents’ management
333
INTERNATIONAL SOCIETY OF BEHAVIORAL MEDICINE
9th International Congress of Behavioral Medicine 29th November – 2nd December, 2006, Sofitel Central Plaza Hotel,
Bangkok, Thailand
PREDICTORS OF PARENTS’ INTENTIONS TO REDUCE CHILDHOOD FEVERS
Authors: Walsh, A.M.(*), Edwards, H.E., Fraser, J.A. Background Parents concerns about and immunological benefits of mild to moderate fevers have been reported for 25 years. Recent reports indicate practices of alternating antipyretics when fever has not reduced sufficiently. Purpose The purpose of this study was to explore the predictors of Australian parents’ intentions to reduce childhood fevers by non-pharmacological and pharmacological methods. Method A crossectional survey of 397 parents of children aged between 6-months and 5-years was undertaken. An instrument was developed from focused discussions with 15 parents, existing instruments and literature. Instrument face, content and construct validity were determined by an expert panel and readability by 10 parents. Predictors of intention to reduce fever, reduce fevers with antipyretics and reduce fevers of 38.0°C or below were determined through the Theory of Planned Behavior. Predictors explored were parents’ beliefs about benefits of reducing fever, normative influences on reducing fever and reducing fever with antipyretics and perceived control over fever management. Results Simultaneous regressions were conducted. Beliefs (42%) and norms relating to fever reduction (16%) were strongest predictors of intentions to reduce fever R2=.27. Norms about reducing fevers with antipyretics (47%) and beliefs (37%) positively influenced intentions to reduce fevers with antipyretics R2=.34 and norms about fever reduction had a negative influence (20%). Predictors of intentions to reduce fevers of 38.0°C or below were weaker R2=.14, however, beliefs (24%) and norms about reducing fevers with antipyretics (29%) predicted this practice. Conclusions Negative beliefs about fever and fever management and normative influences were the strongest predictors of parents’ fever management intentions. These findings highlight the need to target all parents’ beliefs about fever and its benefits and correct norms relating to reducing fever and the dangers of unnecessary and/or overuse of antipyretics in children with a febrile illness.
334
ASIA-PACIFIC ACADEMIC CONSORTIUM FOR PUBLIC HEALTH (APCPH)
38th APACPH Annual Conference – Partnership for Human Security and Health
Bangkok, Thailand December 3-6, 2006
Authors: Walsh, A. Edwards, H., Fraser, J.
INFLUENCE OF INACCURATE, CONFLICTING HEALTH INFORMATION ON
PARENTS’ MANAGEMENT OF CHILDHOOD FEVER Background Internationally, studies continue to report parents’ concerns about childhood fevers. Parents find fevers frightening and base care on inaccurate, often conflicting health information gathered from multiple sources. Purpose Identify impact of inaccurate and conflicting health information on fever management practices of parents of young children. Methods Four-hundred Queensland parents of children aged 6-months to 5-years completed a self-report survey developed from the literature and focused discussions with 15 parents. The survey identified parents’ definitions of fever, fever management practices, concerns and influences on their practices. Summary of results Inaccurate beliefs that fever is harmful (88%) causing brain damage and febrile convulsions influenced practices, eg., 24 hour monitoring, unnecessary initiation of fever reduction strategies and medication administration for temperatures considered fever 38.2ºC±0.7 (43%) and high fever 39.4ºC±0.8 (75%). Medical advice was sought for fever (15%) and high fever (64%). Despite believing fever reducing medications harmful (73%) parents routinely use them to reduce temperatures of 38.3ºC±0.6. Many (65%) used multiple medication combinations, eg., paracetamol, ibuprofen, homeopathic preparations; 52% had alternated medications and 35% administered medications at too frequent intervals, overdosing their child. Most parents (71%) believed they knew how to manage fever. Parents learnt about fever management from health professionals (80%), past experience (39%), literature (26%), peers (24%) and mothers (23%). Nearly half (42%) received conflicting information causing confusion and increased concerns (66%) and frustration (16%). Conclusions and Reflections Inaccurate, conflicting information influenced parents’ beliefs and practices. Low grade fevers precipitated unnecessary fever reduction strategies; health services utilisation and medication administration (some overdosing) although medications were believed harmful. Health professionals, responsible for health education, must ensure all parents of young children are provided with accurate, evidence-based, consistent fever management information, preferably before the firstborn has a fever.
335
GENERAL PRACTITIONER AND PRIMARY HEALTH CARE
2007 GP & PHC Research Conference
Sydney, Australia 23 to 25 May 2007
Authors: Walsh, A. Edwards, H., Fraser, J.
OVER-THE-COUNTER MEDICATION USE IN CHILDHOOD FEVER MANAGEMENT: HEALTH PROFESSIONALS WORKING WITH
PARENTS Background Internationally parents are overly concerned about and unnecessarily reduce childhood fever, often overdoing children with antipyretics. Objectives Identify Australian parents’ beliefs and practices in childhood fever management. Methods Crossectional survey of 401 Queensland parents recruited through advertising (48.4%), face-to-face (26.4%) and snowball (24.4%) methods. An instrument was developed, construct and content validity determined by an expert panel and item reliability by test-retest with nine parents. Areas targeted were beliefs about fever, medication use, influences on and barriers to medication use. Principal findings Parents, believing fever harmful, usually used antipyretics to reduce temperatures from 37.0°C to 40.0°C (38.3°C±0.6). Medical advice was sought for specific illness symptoms, length of illness, height of fever, inability to reduce fever or recurrent fever and children generally unwell. Antipyretic use was influenced by temperature, distress or general unwellness and pain or discomfort. Nearly all used paracetamol (94%) and most used ibuprofen (77%). Overdosing by too frequent administration was common with ibuprofen (31.8%), 4th hourly by 22%, and infrequent with paracetamol 3.8%. Alternating antipyretics was common (51.8%) and this practice was influenced by health professional recommendations and children remaining febrile post-antipyretic. Beliefs that antipyretics were harmful (73.2%) did not preclude administration. Medication refusals (44.0%) were overcome by using force, different administration methods including suppositories. Discussion Parents’ fears about negative outcomes from fever are highlighted by their use of over-the-counter medications to reduce low-grade fevers, despite believing these medications harmful. Errors in medication administration frequency indicate confusion from multiple medication use and alternating antipyretics. Implications Practice implications for health professionals will be to provide evidence-based information to parents targeting the benefits of fever, when and how to safely use medications and when to seek medical assistance. Parents need advice and reassurance on how to manage fever, a common, frightening event in childhood.
336
PAEDIATRICS & CHILD HEALTH ANNUAL MEETING INCORPORATED IN THE ROYAL AUSTRALIAN COLLEGE OF PHYSICIANS ANNUAL MEETING
6th - 10th May, 2007, Melbourne, Australia
EVIDENCE-BASED MANAGEMENT OF UNCOMPLICATED PAIN AND FEVER IN CHILDREN IN THE COMMUNITY SETTING Authors: Beggs S1, Carroll P2, Walsh A3, Nissen M4, Bennett S5, Yeo G-T6 1Royal Children’s Hospital, Parkville, VIC; 2University of NSW, Sydney, NSW; 3Queensland University of Technology, Kelvin Grove, QLD; 4Royal Children’s Hospital, Brisbane, QLD; 5Bennett, S. Pharmacy, Balmain, NSW; 6Berowra Family Medical Practice, Sydney, NSW. Introduction: Childhood fever is the most common reason for parents to seek medical attention.1 Despite successful educational interventions fever phobia persists.2 Healthcare professionals can play a pivotal role in educating parents on how best to manage such conditions. We provide practical, yet evidence-based, guidance on the management of children (aged 0-12 years) presenting in the community setting with pain and/or fever in association with common childhood ailments. Method Design: Electronic database searching (1966-August 2006) was conducted to identify articles relating to the management of pain and or fever in children aged 0-12 years. Additional articles were found through archives and the reference lists of identified articles. Recommendations: (1) Fever alone does not need to be treated. (2) Parents should watch for signs of development of potential serious problems (vomiting, irritability, lethargy, apathy) and seek further medical advice if a fever persists for more than 48 hours or if the child's condition deteriorates. (3) Paracetamol (15mg/kg) and ibuprofen (10mg/kg) are equally effective analgesics and antipyretics. (4) Both drugs are generally well tolerated, but the potential exists for more iatrogenic risks with ibuprofen use. (5) Alternating therapy is not recommended. Conclusions: While both paracetamol and ibuprofen may be appropriate for use in children, we need to encourage the quality use of all medicines. This means discouraging their use simply to lower temperature and primarily considering them for pain or fever with associated discomfort. Given that there is no obvious efficacy advantage to using ibuprofen, there appears no reason to change from continuing to use paracetamol as the first-line treatment of choice in paediatric patients. References: (1) Dixon G, et al. Clinical and consumer guidelines related to the management of childhood fever. A literature review. Journal of Research in Nursing 2006;11(3):263-278. (2) Walsh A, Edwards H. Management of childhood fever by parents: literature review. J Adv Nurs 2006;54(2):217-227.

337
Appendix 5
Media Interest Arising from the Research
Program

338
2006
Anne Walsh - "Fever" Media Coverage 6/4-13/4
Press
Feverish kids can get too much of a good thingSydney Morning Herald, 13/04/06, Health & Science, Page 3By: AAP Almost a third of parents overdose children with over-the-counter fevermedications, making youngsters susceptible to liver damage and stomachbleeding, a study has found. A Queensland University of Technologyreview of 24 years of global research found more than 30 per cent ofparents overdose their children on drugs such as paracetamol andibuprofen. Keywords: of Technology (1), University (2)
Clip ref: 21468021293 wordsType: News ItemPhoto: yes
Parents take cautious approach to medicineNorthern Daily Leader, 11/04/06, General News, Page 2By: None Almost a third of parents are overdosing children with over the counterfever medications a study has found, but a Tamworth pharmacist said mostparents were only too willing to seek his advice. A Queensland University ofTechnology (QUT) review of 24 years of international research found morethan 30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (3), University (1)
Clip ref: 21422912306 wordsType: News ItemPhoto: yes
Panicked parents unaware of medicine dangersDaily Telegraph, 10/04/06, General News, Page 13By: Clare Masters More than half of parents are inadvertently overdosing their children withoff-the-shelf medications such as paracetamol, potentially causing themlong-term health problems. A "pill-popping culture" is encouraging mumsand dads to over-medicate children and panicked parents are also mixingmedication, Australian research found. Keywords: of Technology (1), University (1)
Clip ref: 21404849364 wordsType: News ItemPhoto: yes
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.

Parents overdose youngAdelaide Advertiser, 07/04/06, General News, Page 7By: None Almost a third of parents overdose children with over the counter fevermedications, making youngsters susceptible to liver damage and stomachbleeding, a study has found. A review of 24 years of international researchby the Queensland University of Technology found more than 30 per centof parents overdosed their children on such drugs as paracetamol andibuprofen. Keywords: of Technology (1), QUT (1), University (1)
Clip ref: 21366614111 wordsType: News ItemPhoto: yes
Over counter overdosesBallarat Courier, 07/04/06, General News, Page 3By: None Almost a third of parents are overdosing children with over the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of international research found more than30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: of Technology (1), University (1)
Clip ref: 2137358673 wordsType: News ItemPhoto: yes
Parents overdosing children: studyBarrier Daily Truth, 07/04/06, General News, Page 8By: AAP Almost a third of parents are overdosing children with over the counterfever medication, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology (QUT) review of 24 years of international research found morethan 30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: of Technology (1), QUT (1), University (1)
Clip ref: 21430733254 wordsType: News ItemPhoto: yes
Overdosed childrenBorder Mail, 07/04/06, General News, Page 4By: None Almost a third of parents are overdosing children with over the counterfever medicine, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of International research found more than30 per cent of parents overdose their children on drugs such asparacetamol and Ibuprofen, with some suffering severe liver damage. Keywords: of Technology (1), University (1)
Clip ref: 2137396265 wordsType: News ItemPhoto: yes
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.
Parents overdosing children on medicationBurnie Advocate, 07/04/06, General News, Page 10By: None Almost a third of parents are overdosing children with over-the-counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of international research found more than30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (2), University (1)
Clip ref: 21372122238 wordsType: News ItemPhoto: yes
Parents OD kids on fever medicineCairns Post, 07/04/06, General News, Page 16By: None Almost a third of parents are overdosing children with over the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of international research found more than30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: of Technology (1), QUT (1), University (1)
Clip ref: 21372721109 wordsType: News ItemPhoto: yes
Parents are overdo sing children on painkillersCanberra Times, 07/04/06, General News, Page 3By: None Almost a third of parents are overdosing children with over-the-counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of international research found more than30 per cent of parents overdosed their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), University (3)
Clip ref: 21369909462 wordsType: News ItemPhoto: yes
Parents misusing fever medicationsDaily Advertiser, 07/04/06, General News, Page 8By: None Almost a third of parents are overdosing children with over the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology (QUT) review of 24 years of international research found morethan 30 per cent of parents overdose their children on drugs such - asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(2), QUT (3), University (2)
Clip ref: 21415115387 wordsType: News ItemPhoto: yes
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.
Parents overdosing children on fever medications: StudyDaily Mercury, 07/04/06, General News, Page 11By: Roberta Mancuso Almost a third of parents are overdosing children with over the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of international research found more than30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (2), University (1)
Clip ref: 21370205361 wordsType: News ItemPhoto: yes
Overdosing fever kidsGold Coast Bulletin, 07/04/06, General News, Page 12By: None Almost a third of parents are overdosing children with over-the-counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, says a study. A Queensland University of Technologyreview of 24 years of research found more than 30 per cent of parentsoverdose children on drugs such as paracetamol and ibuprofen. Keywords: of Technology (1), University (1)
Clip ref: 2137178776 wordsType: News ItemPhoto: yes
Parents can't get dose rightHerald Sun, 07/04/06, General News, Page 20By: Michelle Pountney Almost a third of parents overdose their children with medicines such asparacetamol and ibuprofen when they have a fever, increasing their child'srisk of liver damage and internal bleeding. An Australian review of 24 yearsof international research found mismanagement of fever was a universaltrend. Keywords: of Technology (1), University (1)
Clip ref: 21369054417 wordsType: News ItemPhoto: yes
Overdose fearsLaunceston Examiner, 07/04/06, General News, Page 4By: None Almost a third of parents are overdosing children with over-the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. The findings came from aQueensland University of Technology review of 24 years of internationalresearch.
Clip ref: 2137129844 wordsType: News ItemPhoto: yes
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.
Parents overdosing kidsNewcastle Herald, 07/04/06, General News, Page 19By: AAP Almost a third of parents are overdosing children with over-the-counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology (QUID review of 24 years of international research found morethan 30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (2), University (1)
Clip ref: 21370050265 wordsType: News ItemPhoto: yes
Parents overdosing children on fever medications: studyNews Mail, 07/04/06, General News, Page 10By: Roberta Mancuso Almost a third of parents are overdosing children with over the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology review of 24 years of international research found more than30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (2), University (1)
Clip ref: 21372775364 wordsType: News ItemPhoto: yes
Parents feed kids too many drugsQueensland Times, 07/04/06, General News, Page 6By: AAP Almost one third of parents overdose their children with over-the-counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology (QUT) review of 24 years of international research found morethan 30% of parents overdosed their children on drugs such asparacetamol and ibuprofen. Keywords: of Technology (1), QUT (2), University (1)
Clip ref: 21368790234 wordsType: News ItemPhoto: yes
Overdose fears for fever medicineSunshine Coast Daily, 07/04/06, General News, Page 7By: AAP Almost a third of parents are overdosing children with over-the-counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology (QUT) review of 24 years of international research found morethan 30% of parents overdose their children on drugs such as paracetamoland ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (3), University (1)
Clip ref: 21369934390 wordsType: News ItemPhoto: yes
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.

Children overdosed by parentsTownsville Bulletin, 07/04/06, General News, Page 4By: None Almost a third of parents are overdosing children with over the counterfever medications, making youngsters susceptible to liver damage andstomach bleeding, a study has found. A Queensland University ofTechnology (QUT) review of 24 years of international research found morethan 30 per cent of parents overdose their children on drugs such asparacetamol and ibuprofen. Keywords: Biomedical Innovation (1), Institute of Health (1), of Technology(1), QUT (3), University (1)
Clip ref: 21372699245 wordsType: News ItemPhoto: yes
Parents overdose sick childrenWest Australian, 07/04/06, General News, Page 5By: Cathy O'Leary An alarming one-third of Australian parents are accidentally overdosingtheir children by doubling up on common over-the-counter pain-killers suchas Panadol and Nurofen. As a result many children are being put at risk ofinternal bleeding and even liver damage. Keywords: of Technology (1), University (1)
Clip ref: 21368261348 wordsType: News ItemPhoto: yes
Fed: Parents overdosing children on fever medications: studyAAP Newswire, 06/04/06, National, Page 0By: AAP A study's found almost a third of parents are overdosing children with over-the-counter fever medications. And that's making them susceptible to liverdamage and stomach bleeding. Keywords: of Technology (1), University (1)
Clip ref: 21361014130 wordsType: AAP NewswirePhoto: no
Radio & TV
ABC North Coast NSW (Lismore)Afternoons - 12/04/06 02:51Terry SaraStation Phone 02 6627 2011 Anne Walsh from the Queensland University of Technology says there hasbeen an increase over the last 20 years internationally of parents whoprefer to use a medication to handle their children's fever. The mostcommon ones used are paracetamol and ibuprofin. Parents are better offlooking at their child and their wellbeing. Ms Walsh is currently looking atAustralian parents and how they handle fever. Interviewees: Anne Walsh, Queensland University of Technology NurseResearcher.Duration: 5.00Summary ID: 200021585263© Media Monitors
Demographics
Demographics are notavailable as the mediaoutlet has notcommissioned audienceresearch into thistimeslot.
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.
ABC 702 Sydney (Sydney)The World Today - 10/04/06 12:50Eleanor Hall A survey undertaken at the QLD Uni of Technology has shown that up tohalf of all Australian parents give their children the wrong dose ofmedication. Nursing researcher, Anne Walsh says 33% of parents try toreduce their childrens' fever by increased dosages and this shows a greaterreliance on medication. She explains that common medications bought insupermarkets could potentially cause much damage to children andparents should monitor them more carefully. Interviewees: Anne Walsh, Nursing Researcher, Qld Uni of TechnologyMentions: IbuprofenDuration: 3.34Summary ID: S00021551722© Media Monitors
Demographics
Male:Female:AB:GB:All People:
2700024300176002950051200
ABC 891 Adelaide (Adelaide)Drive - 07/04/06 04:18Deb TribeProducer Mr Michael Ockerby 08 8343 4410 Medical issues continued: Tribe says research by the Qld Uni ofTechnology has found 30% of parents overdose their children with over thecounter medications like Paracetamol and Ibuprofen. Grummet says anoverdose of Paracetamol can cause kidney problems. He says Ibuprofencauses kidney and gut problems. He says figures from the Royal Children'sHospital in Melbourne showed there were horrifying numbers of overdosedchildren. Interviewees: Phil Grummet, spokesman, Pharmacy Guild of AustraliaDuration: 2.45Summary ID: A00021533696© Media Monitors
Demographics
Male:Female:AB:GB:All People:
8000700050008000
15000
4BC (Brisbane)08:30 News - 07/04/06 08:32NewsreaderNews Director Mr Steve Speziale 07 3908 8200 QUT Nursing researcher Ann Walsh says half of all parents incorrectlydose their children with over the counter medication for fever. Interviewees: Ann Walsh, nursing researcher, QUTDuration: 0.34Summary ID: B00021524453© Media Monitors
Demographics
Male:Female:AB:GB:All People:
2060025800
48002700046300
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.

ABC 720 Perth (Perth)Mornings - 06/04/06 09:24Gillian O’ShaughnessyProducer Ms Alicia Hanson 08 9220 2729 Almost half of all parents incorrectly dose their children with over-the-counter medications to manager temperatures which may not actually dealwith the symptoms. Qld Uni of Technology nursing researcher Anne Walshsays international studies show many parents overdose or underdoseyoungsters. Walsh says Paracetamol and Ibuprofen are the most usedmedications. She explains some of the mistakes parents can make and thepossible ramifications. Interviewees: Anne Walsh, Nursing Researcher, Qld Uni of TechnologyDuration: 8.03Summary ID: P00021512020© Media Monitors
Demographics
Male:Female:AB:GB:All People:
1700016000
90001900034000
Subscribers should refer to the original article before making any financial decisions or forming anyopinions. This information is for the use of Media Monitors' subscribers only and may not beprovided to any third party for any purpose whatsoever without the express written permission ofMedia Monitors Australia Pty Ltd.
Ref: 21468021Copyright Agency Limited (CAL) licenced copy
Sydney Morning Herald13/04/2006Page: 3Section: Health & ScienceRegion: Sydney Circulation: 214299Type: Capital City DailySize: 103.02 sq.cms.Published: MTWTFS-
Ref: 21422912Copyright Agency Limited (CAL) licenced copy
Northern Daily Leader11/04/2006Page: 2Section: General NewsRegion: Tamworth NSW Circulation: 8344Type: RegionalSize: 261.72 sq.cms.Published: MTWTFS-
Ref: 21404849Copyright Agency Limited (CAL) licenced copy
Daily Telegraph10/04/2006Page: 13Section: General NewsRegion: Sydney Circulation: 397054Type: Capital City DailySize: 318.88 sq.cms.Published: MTWTFS-
Ref: 21366614Copyright Agency Limited (CAL) licenced copy
Adelaide Advertiser07/04/2006Page: 7Section: General NewsRegion: Adelaide Circulation: 196849Type: Capital City DailySize: 40.74 sq.cms.Published: MTWTFS-
Ref: 21373586Copyright Agency Limited (CAL) licenced copy
Ballarat Courier07/04/2006Page: 3Section: General NewsRegion: Ballarat VIC Circulation: 19390Type: RegionalSize: 27.39 sq.cms.Published: MTWTFS-
Ref: 21430733Copyright Agency Limited (CAL) licenced copy
Barrier Daily Truth07/04/2006Page: 8Section: General NewsRegion: Broken Hill NSW Circulation: 5812Type: RegionalSize: 95.44 sq.cms.Published: MTWTFS-

Ref: 21373962Copyright Agency Limited (CAL) licenced copy
Border Mail07/04/2006Page: 4Section: General NewsRegion: Albury-Wodonga VIC Circulation: 26361Type: RegionalSize: 21.83 sq.cms.Published: MTWTFS-
Ref: 21372122Copyright Agency Limited (CAL) licenced copy
Burnie Advocate07/04/2006Page: 10Section: General NewsRegion: Burnie TAS Circulation: 24764Type: RegionalSize: 107.40 sq.cms.Published: MTWTFS-
Ref: 21372721Copyright Agency Limited (CAL) licenced copy
Cairns Post07/04/2006Page: 16Section: General NewsRegion: Cairns QLD Circulation: 27955Type: RegionalSize: 43.52 sq.cms.Published: MTWTFS-
Ref: 21369909Copyright Agency Limited (CAL) licenced copy
Canberra Times07/04/2006Page: 3Section: General NewsRegion: Canberra Circulation: 36273Type: Capital City DailySize: 151.65 sq.cms.Published: MTWTFS-
Ref: 21415115Copyright Agency Limited (CAL) licenced copy
Daily Advertiser07/04/2006Page: 8Section: General NewsRegion: Wagga Wagga NSW Circulation: 12926Type: RegionalSize: 433.50 sq.cms.Published: MTWTFS-
Ref: 21370205Copyright Agency Limited (CAL) licenced copy
Daily Mercury07/04/2006Page: 11Section: General NewsRegion: Mackay QLD Circulation: 20553Type: RegionalSize: 192.41 sq.cms.Published: MTWTFS-

Ref: 21371787Copyright Agency Limited (CAL) licenced copy
Gold Coast Bulletin07/04/2006Page: 12Section: General NewsRegion: Gold Coast QLD Circulation: 42602Type: RegionalSize: 27.84 sq.cms.Published: MTWTFS-
Ref: 21369054Copyright Agency Limited (CAL) licenced copy
Herald Sun07/04/2006Page: 20Section: General NewsRegion: Melbourne Circulation: 53028Type: Capital City DailySize: 192.82 sq.cms.Published: MTWTFS-

Ref: 21371298Copyright Agency Limited (CAL) licenced copy
Launceston Examiner07/04/2006Page: 4Section: General NewsRegion: Launceston TAS Circulation: 35707Type: RegionalSize: 19.47 sq.cms.Published: MTWTFS-

Ref: 21370050Copyright Agency Limited (CAL) licenced copy
Newcastle Herald07/04/2006Page: 19Section: General NewsRegion: Newcastle NSW Circulation: 52598Type: RegionalSize: 166.56 sq.cms.Published: MTWTFS-

Ref: 21372775Copyright Agency Limited (CAL) licenced copy
News Mail07/04/2006Page: 10Section: General NewsRegion: Bundaberg QLD Circulation: 11878Type: RegionalSize: 193.19 sq.cms.Published: MTWTFS-
Ref: 21368790Copyright Agency Limited (CAL) licenced copy
Queensland Times07/04/2006Page: 6Section: General NewsRegion: Ipswich QLD Circulation: 12183Type: RegionalSize: 110.85 sq.cms.Published: MTWTFS-
Ref: 21369934Copyright Agency Limited (CAL) licenced copy
Sunshine Coast Daily07/04/2006Page: 7Section: General NewsRegion: Maroochydore QLD Circulation: 23552Type: RegionalSize: 212.70 sq.cms.Published: MTWTFS-
Ref: 21372699Copyright Agency Limited (CAL) licenced copy
Townsville Bulletin07/04/2006Page: 4Section: General NewsRegion: Townsville QLD Circulation: 27318Type: RegionalSize: 88.08 sq.cms.Published: MTWTFS-
Ref: 21368261Copyright Agency Limited (CAL) licenced copy
West Australian07/04/2006Page: 5Section: General NewsRegion: Perth Circulation: 202774Type: Capital City DailySize: 163.57 sq.cms.Published: MTWTFS-

Content Supplied by Australian Associated Press© AAP, All Rights Reserved. See disclaimer at http://aap.com.au/disclaimer.asp Ref: 21361014
AAP Newswire06/04/2006Section: NationalRegion: AustraliaPublished: MTWTFSS

370
2007
COPYRIGHT This report and its contents are for the use of Media Monitors' subscribers only and may not be provided to any third party for anypurpose whatsoever without the express written permission of Media Monitors Australia Pty Ltd.
DISCLAIMER The material contained in this report is for general information purposes only. Any figures in this report are an estimation andshould not be taken as definitive statistics. Subscribers should refer to the original article before making any financial decisions or forming anyopinions. Media Monitors makes no representations and, to the extent permitted by law, excludes all warranties in relation to the informationcontained in the report and is not liable to you or to any third party for any losses, costs or expenses, resulting from any use or misuse of thereport.
Anne Walsh PhD results media coverage
13/09/2007
Study finds parents dose fevered kids too heavilyQueensland Times, 13/09/07, General News, Page 11By: None
QUEENSLAND parents need proper education in managing fever in youngchildren as many give medication incorrectly and often unnecessarily, saysQueensland University of Technology (QUT) nursing researcher AnneWalsh. In a study of more than 400 Queensland parents, Ms Walsh hasfound 32 per cent of parents administer ibuprofen too often, with four percent for paracetamol.
Keywords: of Technology(1), QUEENSLAND(3), QUT(1), University(1)
Clip Ref: 00030079864
144 wordsType: News ItemPhoto: No
12/09/2007
Channel 9 (Brisbane)Brisbane Extra - 12/09/2007 5:37 PMLisa Wilkinson
According to new research, one in three parents are dosing their children tooheavily with medication when they are ill. Reporter Lisa Honeywillinvestigates safe dispensation of medications to children. Mother JodyMittelheuser says she regularly reaches for medication when her childrenhave a fever and says she follows directions closely. QUT Researcher AnneWalsh says parents are overusing medications. Walsh says she surveyed400m parents across Qld to see how they managed fever and says aboutone third were overmedicating their children. Paediatrician Dr Johanna Holtsays fever alone is not a reason to medicate children
Interviewees: Anne Walsh, QUT; Dr Johanna Holt, Paediatrician; JodyMittelheuser, MotherMentions: Nurofen; Panadol.Vision: Milo; PanadolDuration: 3.57Summary ID: B00027890491© Media Monitors
Demographics
Male:Female:AB:GB:All People:
377772490342331212506604868099
COPYRIGHT This report and its contents are for the use of Media Monitors' subscribers only and may not be provided to any third party for anypurpose whatsoever without the express written permission of Media Monitors Australia Pty Ltd.
DISCLAIMER The material contained in this report is for general information purposes only. Any figures in this report are an estimation andshould not be taken as definitive statistics. Subscribers should refer to the original article before making any financial decisions or forming anyopinions. Media Monitors makes no representations and, to the extent permitted by law, excludes all warranties in relation to the informationcontained in the report and is not liable to you or to any third party for any losses, costs or expenses, resulting from any use or misuse of thereport.
10/09/2007
ABC Far North (Cairns)Mornings - 10/09/2007 9:25 AMPat Morrish
Morrish talks about the topic of ill children being given incorrect dosages ofparacetamol for fever treatment. Morrish then speaks with Anne Walsh(*),Senior Research Fellow, Queensland University of Technology (QUT), abouther study into how Australians manage their children’s fever and her warningof misuse of over-the-counter medicine for children’s health can harm theirhealth. Walsh explains differences in fever medicine including differingdosage rates and response times including for paracetamol and ibuprofen.Walsh mentions that she is pleased that drug maker, Glaxo Smith Kleine ispaying attention to her research.
Interviewees: Anne Walsh(*), Senior Research Fellow, QueenslandUniversity of Technology (QUT).Duration: 5.00Summary ID: 400027853912© Media Monitors
Demographics
Male:Female:AB:GB:All People:
9001300
40019002200
07/09/2007
ABC New England North West (Tamworth)Inland Afternoons - 7/09/2007 3:13 PMAlison Buchanan
According to a study of 400 parents by the Queensland University ofTechnology, a percentage of parents are administering paracetamol andibuprofen incorrectly. Tim Logan from the Pharmacy Guild of Australia says itis not always smart to stop a fever. Giving too much paracetamol can causeliver damage, warns Logan, who explains says too much ibuprofen cancause digestive problems. Too many people believe that at larger dose willremedy people at a quicker pace, which is incorrect. People need to usemedicines wisely stresses Logan.
Interviewees: Tim Logan, Pharmacy Guild of AustraliaDuration: 7.30Summary ID: 200027835318This program or part thereof is syndicated to the following 3 station(s):-ABC Central West NSW (Orange), ABC Riverina (Wagga Wagga), ABCWestern Plains NSW (Dubbo)© Media Monitors
Demographics
Demographics are notavailable as the mediaoutlet has notcommissioned audienceresearch into this timeslot.
COPYRIGHT This report and its contents are for the use of Media Monitors' subscribers only and may not be provided to any third party for anypurpose whatsoever without the express written permission of Media Monitors Australia Pty Ltd.
DISCLAIMER The material contained in this report is for general information purposes only. Any figures in this report are an estimation andshould not be taken as definitive statistics. Subscribers should refer to the original article before making any financial decisions or forming anyopinions. Media Monitors makes no representations and, to the extent permitted by law, excludes all warranties in relation to the informationcontained in the report and is not liable to you or to any third party for any losses, costs or expenses, resulting from any use or misuse of thereport.
3AW (Melbourne)Afternoons - 7/09/2007 2:44 PMDenis Walter
Walter claims a newspaper article claims parents are giving children toomuch medicine or cannot manage fever. Anne Walsh, senior research fellow,Qld University of Technology explains her study on Qld parents and how theymanage mild fever in children and claims they are over medicating and overdosing children with ibuprofen by using it like it is paracetamol. Walsh warnsagainst over dosing with ibuprofen on dehydrated children as it causesgastro problems, headaches and asthma. Walsh explains how fever isbeneficial.
Interviewees: Anne Walsh, senior research fellow, Qld University ofTechnologyDuration: 4.59Summary ID: M00027834979© Media Monitors
Demographics
Male:Female:AB:GB:All People:
3300036000120004100069000
ABC 666 Canberra (Canberra)Morning - 7/09/2007 9:45 AMAlex Sloan
Interview with Anne Walsh, Senior Research Fellow Queensland Universityof Technology to discuss a study conducted on the over dosing of children oncommon medications such as Ibuprofen and Paracetamol. Walsh says itseems using two different medications at the same time parents arebecoming confused at which to give at and at what rate. Walsh discusseshow parents were selected for the study and advises of the the resultsdisclosed during the study with note that parents seem to be overworied by achilds fever. Walsh advises that health professionals may need to look at thelatest literature and suggests parents be educated in the benefits fevers havefor a child.
Interviewees: Anne Walsh, Senior Research Fellow Queensland Universityof TechnologyMentions: Dr Michael Fascher, Royal College of General PractitionersDuration: 9.24Summary ID: C00027831328© Media Monitors
Demographics
Male:Female:AB:GB:All People:
34005200160067008600
COPYRIGHT This report and its contents are for the use of Media Monitors' subscribers only and may not be provided to any third party for anypurpose whatsoever without the express written permission of Media Monitors Australia Pty Ltd.
DISCLAIMER The material contained in this report is for general information purposes only. Any figures in this report are an estimation andshould not be taken as definitive statistics. Subscribers should refer to the original article before making any financial decisions or forming anyopinions. Media Monitors makes no representations and, to the extent permitted by law, excludes all warranties in relation to the informationcontained in the report and is not liable to you or to any third party for any losses, costs or expenses, resulting from any use or misuse of thereport.
5AA (Adelaide)Pilkington & Conlon - 7/09/2007 8:08 AMChris Dittmar & Jane Doyle
Doyle says an interesting report from QUT has emerged that says parentsare not that good at treating their kids at home for high fevers. She says thereport says 33% of parents don't know how to manage fever in their childrenand often give excessive doses of over the counter medicines. Ford says attime there is some confusion about how to treat a child's fever. He says oftenparents think they should be able to stop a fever immediately which is notrealistic. He says a fever can be an indicator of white bloods cells trying toget rid of an infection. He says parents can give their kids a small does ofparacetamol to minimise the symptoms. Doyle says some doctors haverecommended parents alternate between different medications likeparacetamol and ibuprofen. Ford says doctors generally recommend parentsuse paracetamol because there are some complications with usingibuprofen. He says parents don't need to give their kids more than four dosesin a day. Dittmar asks if parents resort to medication to quickly. Ford saysthat might be a bit true. Dittmar says drinking a lot of water helps to reduce afever and sickness. He says fluid intake is so important.
Interviewees: Dr Peter Ford, SA President, AMADuration: 8.28Summary ID: A00027828283© Media Monitors
Demographics
Male:Female:AB:GB:All People:
2600034000100003800060000
ABC 702 Sydney (Sydney)05:30 News - 7/09/2007 5:31 AMNewsreader
New Queensland University of Technology research has found parents relytoo much on over the counter medications when their child has a fever.
Interviewees: Anne Walsh, Senior ResearcherDuration: 0.45Summary ID: S00027824735This program or part thereof is syndicated to the following 11 station(s):-ABC Central Coast (Gosford), ABC Central West NSW (Orange), ABC FarWest NSW (Broken Hill), ABC Illawarra (Wollongong), ABC Mid North CoastNSW (Port Macquarie), ABC New England North West (Tamworth), ABCNorth Coast NSW (Lismore), ABC Riverina (Wagga Wagga), ABC SouthEast NSW (Bega), ABC Upper Hunter (Muswellbrook), ABC Western PlainsNSW (Dubbo)© Media Monitors
Demographics
Male:Female:AB:GB:All People:
2100025000220002500046000
Parents dosing kids too heavilyHobart Mercury, 07/09/07, General News, Page 10By: AAP
A survey of parents has revealed that one third dose their children up ondrugs more heavily than necessary to treat fever. The Queensland studyshowed that the pain reliever ibuprofen was administered too frequently by32 per cent of more than 400 parents surveyed.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029980945
256 wordsType: News ItemPhoto: No
COPYRIGHT This report and its contents are for the use of Media Monitors' subscribers only and may not be provided to any third party for anypurpose whatsoever without the express written permission of Media Monitors Australia Pty Ltd.
DISCLAIMER The material contained in this report is for general information purposes only. Any figures in this report are an estimation andshould not be taken as definitive statistics. Subscribers should refer to the original article before making any financial decisions or forming anyopinions. Media Monitors makes no representations and, to the extent permitted by law, excludes all warranties in relation to the informationcontained in the report and is not liable to you or to any third party for any losses, costs or expenses, resulting from any use or misuse of thereport.
Parents quick to medicate childrenSunshine Coast Daily, 07/09/07, General News, Page 11By: TAMARA MCLEAN OF AAP
Ibuprofen is overused A SURVEY of parents has revealed that one thirddose their children up on drugs more heavily than necessary to treat fever.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029980111
352 wordsType: News ItemPhoto: No
Overzealous parents warned against overdosing a feverCourier Mail, 07/09/07, General News, Page 23By: Tamara McLean
ONE in three parents dose their children up on drugs more heavily thannecessary to treat a fever. A Queensland study released yesterday showedthat the pain reliever ibuprofen was administered too frequently by 32 percent of more than 400 parents surveyed.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029979528
229 wordsType: News ItemPhoto: No
Parents giving kids too much medicineAustralian, 07/09/07, General News, Page 3By: Clara Pirani
MedicaL reporter ONE-THIRD of parents don’t know how to manage fever intheir children and often give excessive doses of medicine. A survey of 400parents found 32 per cent gave their children incorrect amounts of ibuprofenand 4 per cent gave high levels of paracetamol.
Keywords: of Technology(1), Queensland(1), University(1)
Clip Ref: 00029979890
383 wordsType: News ItemPhoto: No
Parents overdose childrenWest Australian, 07/09/07, General News, Page 15By: None
One third of parents dose their children up on drugs more heavily thannecessary to treat fever, a survey shows. The Queensland study showed thatthe pain reliever ibuprofen was administered too frequently by 32 per cent ofmore than 400 parents surveyed.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029983083
117 wordsType:Photo: No
Children dosed up on painkillersMaitland Mercury, 07/09/07, General News, Page 7By: None
SYDNEY - A survey of parents has revealed that one third dose their childrenup on drugs more heavily than necessary to treat fever. The Queenslandstudy showed that the pain reliever ibuprofen was administered toofrequently by 32 per cent of more than 400 parents surveyed.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029983518
94 wordsType: News ItemPhoto: No
COPYRIGHT This report and its contents are for the use of Media Monitors' subscribers only and may not be provided to any third party for anypurpose whatsoever without the express written permission of Media Monitors Australia Pty Ltd.
DISCLAIMER The material contained in this report is for general information purposes only. Any figures in this report are an estimation andshould not be taken as definitive statistics. Subscribers should refer to the original article before making any financial decisions or forming anyopinions. Media Monitors makes no representations and, to the extent permitted by law, excludes all warranties in relation to the informationcontained in the report and is not liable to you or to any third party for any losses, costs or expenses, resulting from any use or misuse of thereport.
1 in 3 parents misuse painkillers Kids are all dosed upBorder Mail, 07/09/07, General News, Page 11By: None
A SURVEY of parents has revealed that one third dose their children up ondrugs more heavily than necessary to treat fever. The Queensland studyshowed that the pain reliever ibuprofen was administered too frequently by32 per cent of more than 400 parents surveyed.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029986358
330 wordsType: News ItemPhoto: No
Painkillers given to kids too often: studyBurnie Advocate, 07/09/07, General News, Page 16By: None
SYDNEY A survey of parents has revealed that one third dose their childrenup on drugs more heavily than necessary to treat fever. The Queenslandstudy showed that the pain reliever ibuprofen was administered toofrequently by 32 per cent of more than 400 parents surveyed. Most of thesewere giving the medication every four hours instead of the recommendedsix-to-eight hourly intervals.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029992382
94 wordsType: News ItemPhoto: No
06/09/2007
Fed: One in three parents giving painkillers too regularlyAAP Newswire, 06/09/07, National, Page 0By: AAP
By Tamara McLean, Medical Writer SYDNEY, Sept 6 AAP - A survey ofparents has revealed that one third dose their children up on drugs moreheavily than necessary to treat fever.
Keywords: of Technology(1), Queensland(2), University(1)
Clip Ref: 00029982370
391 wordsType: AAP NewswirePhoto: No
Study findsparents dosefevered kidstoo heavilyQUEENSLAND parents needproper education in managingfever in young children as manygive medication incorrectly andoften unnecessarily, saysQueensland University ofTechnology (QUT) nursingresearcher Anne Walsh.
In a study of more than 400Queensland parents, Ms Walshhas found 32 per cent of parentsadminister ibuprofen too often,with four per cent forparacetamol.
She said the most disturbingfinding was that 23 per cent ofparents gave their childrenibuprofen every four hoursinstead of the recommended sixto eight hourly intervals.
"All parents should learn howto manage fever before theirchild's first febrile episode," MsWalsh said.
She said incorrect use ofmedications could cause liverdamage and stomach upsets.
"In many cases it would bebetter if parents first managefever by giving their childrenmore fluids and rest, and keepingthem comfortable," Ms Walshsaid.
back
Ref: 30079864Copyright Agency Limited (CAL) licensed copy
Queensland Times13/09/2007Page: 11General NewsRegion: Ipswich QLD Circulation: 10947Type: RegionalSize: 70.26 sq.cmsMTWTFS-
ParentsdosingkidstooheavilyA SURVEY of parents hasrevealed that one thirddose their children up ondrugs more heavily thannecessary to treat fever.
The Queensland studyshowed that the pain re-liever ibuprofen was ad-ministered too frequentlyby 32 per cent of morethan 400 parents sur-veyed.
Most of these were giv-ing the medication everyfour hours instead of therecommended six-to-eighthourly intervals.
Lead researcher AnneWalsh, from the Queens-land University of Tech-nology. said the resultswere concerning, particu-larly as parents shouldnot be giving medicationto treat mild fever in thefirst place.
"The fact that they weregiving medication too fre-quently is a real worry,"Ms Walsh said.
"But what they don'tseem to understand is thata low-grade fever under 40degrees on its own doesnot need to be treated.
"The body has purpose-
ly set its temperaturehigher to try to stop bac-teria from multiplying:it's an immune response."
The standard painkillerparacetamol, branded asPanadol, and ibuprofen, anon-steroidal anti-inflammatory drug(NSAID) under brandslike Nurofen, are widelyused to treat pain andfever.
Too many parents werealternating between thetwo medications, makingtiming confusing.
"Given that such a highpercentage of parents aregiving ibuprofen too fre-quently, it may be thatthey are assuming it is thesame as paracetamolwhich can be given fourhourly," Ms Walsh said.
Many were administer-ing both at once, a poten-tially dangerous practicethat was not recom-mended.
Over administeringcould lead to liver damageand stomach upset, espe-cially if the child is dehy-drated by the fever.
AAP
back
Ref: 29980945Copyright Agency Limited (CAL) licensed copy
Hobart Mercury07/09/2007Page: 10General NewsRegion: Hobart Circulation: 47947Type: Capital City DailySize: 101.44 sq.cmsMTWTFS-
Parentsquick tomedicatechildrenIbuprofen is overusedBy TAMARA MCLEAN of AAPA SURVEY of parents has re-vealed that one third dosetheir children up on drugsmore heavily than necessaryto treat fever.
The Queensland studyshowed that the pain relieveribuprofen was administeredtoo frequently by 32% ofmore than 400 parents sur-veyed.
Most of these were givingthe medication every fourhours instead of the recom-mended six-to-eight hourlyintervals.
Lead researcher AnneWalsh, from the QueenslandUniversity of Technology,said the results were con-cerning, particularly as pa-rents should not be giving
medication to treat mild fev-er in the first place.
"The fact that they weregiving medication too fre-quently is a real worry," MsWalsh said.
"But what they don't seemto understand is that a low-grade fever under 40 degreeson its own does not need tobe treated.
"The body has purposelyset its temperature higher totry to stop bacteria frommultiplying; it's an immuneresponse."
The standard painkillerparacetamol, branded as Pa-nadol, and ibuprofen, a non-steroidal anti-inflammatorydrug (NSAID) under brandslike Nurofen, are widely usedto treat pain and fever.
Too many parents were al-ternating between the twomedications, making timingconfusing.
"Given that such a highpercentage of parents aregiving ibuprofen too fre-quently, it may be that theyare assuming it is the sameas paracetamol which can begiven four-hourly," MsWalsh said.
Many were administeringboth at once, a potentiallydangerous practice that wasnot recommended.
Over administering couldlead to liver damage and sto-mach upset, especially if thechild is dehydrated by thefever.
She said it was not pa-rents' fault they were mis-
managing fever, as they werejust following accepted prac-tice and trying to maintainsome control over their chil-dren's wellbeing.
However, there was an ur-gent need for evidence-basededucation for parents andthe health professionals whogive them information.
"In many cases it would bebetter if parents first managefever by giving their childrenmore fluids and rest, andkeeping them comfortable."
Unwell children should beclosely monitored and pa-rents should seek medicaladvice if they display severesymptoms, or show no im-provement within 48 hours.
-AAP
back
Ref: 29980111Copyright Agency Limited (CAL) licensed copy
Sunshine Coast Daily07/09/2007Page: 11General NewsRegion: Maroochydore QLD Circulation: 22743Type: RegionalSize: 210.93 sq.cmsMTWTFS-

Overzealous parents warnedagainst overdosing a feverTamara McLean
ONE in three parents dosetheir children up on drugsmore heavily than necess-ary to treat a fever.
A Queensland study re-leased yesterday showedthat the pain reliever ibu-profen was administeredtoo frequently by 32 percent of more than 400parents surveyed.
Most of these were giv-ing the medication everyfour hours instead of therecommended six-to-eighthourly intervals.
Lead researcher AnneWalsh, from the Queens-land University of Techno-
logy, said the results wereconcerning, particularly asparents should not be giv-ing medication to treatmild fever in the first place.
"What they (parents)don't seem to understandis that a low-grade feverunder 40 degrees on itsown does not need to betreated," Ms Walsh said.
"The body has pur-posely set its temperaturehigher to try to stop bac-teria from multiplying; it'san immune response."
The standard painkillerparacetamol, branded asPanadol, and ibuprofen, anon-steroidal anti-inflammatory drug under
brands such as Nurofen,were widely used to treatpain and fever.
She said many parentswere giving ibuprofen toofrequently and assuming itwas the same as para-cetamol which could begiven every four hours.
Over administeringcould lead to liver damageand stomach upset, es-pecially if the child wasdehydrated by the fever.
Unwell children shouldbe closely monitored andparents should seek medi-cal advice if they displaysevere symptoms, or showno improvement within48 hours.
back
Ref: 29979528Copyright Agency Limited (CAL) licensed copy
Courier Mail07/09/2007Page: 23General NewsRegion: Brisbane Circulation: 214451Type: Capital City DailySize: 89.10 sq.cmsMTWTFS-
Parents giving kids too much medicineClara PiraniMedical reporter
ONE-THIRD of parents don'tknow how to manage fever intheir children and often giveexcessive doses of medicine.
A survey of 400 parents found32 per cent gave their childrenincorrect amounts of ibuprofenand 4 per cent gave high levels ofparacetamol.
The finding that almost 25 percent gave their children ibupro-fen every four hours, instead ofthe recommended six- to eight-hourly intervals, was disturbing,said Queensland University ofTechnology senior research fel-low Anne Walsh, who conductedthe study.
"About 60 per cent of the
parents were university-educated, so I think if we did alarger version of this study, itwould be more widespread," MsWalsh said.
"If you give children too muchparacetamol, they can developliver damage. And if they take toomuch ibuprofen, it can causegastro and stomach upsets, andcan bring on asthma."
The survey found parents wereconfused about the advice theyreceived from doctors.
"A lot of parents involved inthe survey reported that theylearned about how to treat feverfrom their doctor, and many werereceiving conflicting advice andthey don't know what to do.
"Some doctors have recom-mended that parents alternate
medication, so they are givingmedications every few hours andare getting confused about thedosage and frequency."
More than 50 per cent ofparents were unnecessarily givingmedication to treat mild fevers,Ms Walsh said.
We urgently need evidence-based education for parents andthe health professionals who givethem information. There is dec-ades of research that proves amild fever is beneficial in fightinginfection, and there is little needto give medication for a fever lessthan 39 degrees."
Sydney GP and Royal Austral-ian College of General Practi-tioners spokesman MichaelFasher agreed that many parents
were overly-concerned aboutfever in children.
"In our culture, fever phobia isendemic. Fever phobia is a focuson fever in an unwell child that isunhelpful," Dr Fasher said.
"It's reasonable to use eitherparacetamol or Nurofen to im-prove the wellbeing of a childwho is miserable with a virileillness," he said. "But I agreethere is no evidence of the safetyof alternating drugs.
"The single most importantsign for parents to look for duringthe febrile period of these ill-nesses is if the child is becomingprogressively more drowsy andlethargic."
back
Ref: 29979890Copyright Agency Limited (CAL) licensed copy
Australian07/09/2007Page: 3General NewsRegion: National Circulation: 129000Type: NationalSize: 138.95 sq.cmsMTWTF

ParentsoverdosechildrenER1SE
One third of parentsdose their children upon drugs more heavilythan necessary totreat fever, a surveyshows.
The Queenslandstudy showed that thepain reliever ibuprofenwas administered toofrequently by 32 percent of more than 400parents surveyed.
Most of them gavethe medication everyfour hours instead of therecommendedsix-to-eight hourlyintervals.
Lead researcher AnneWalsh, fromQueensland Universityof Technology, said theresults were a concern,particularly as parentsshould not be givingmedication to treat mildfever in the firstplace.
"The fact that theywere giving medicationtoo frequently is a realworry," Ms Walsh said.
She said many parentsgot confused with thefour-hourly dosage rateof paracetamol.
back
Ref: 29983083Copyright Agency Limited (CAL) licensed copy
West Australian07/09/2007Page: 15General NewsRegion: Perth Circulation: 206025Type: Capital City DailySize: 50.34 sq.cmsMTWTFS-

Children dosedup on painkillers
SYDNEY - A survey ofparents has revealed thatone third dose their chil-dren up on drugs moreheavily than necessary totreat fever.
The Queensland studyshowed that the pain reliev-er ibuprofen was adminis-tered too frequently by 32per cent of more than 400parents surveyed.
Most of these weregiving the medicationevery four hours instead ofthe recommended six-to-eight hourly intervals.
Lead researcher AnneWalsh, from theQueensland University ofTechnology, said theresults were concerning,particularly as parentsshould not be giving med-ication to treat mild fever inthe first place.
back
Ref: 29983518Copyright Agency Limited (CAL) licensed copy
Maitland Mercury07/09/2007Page: 7General NewsRegion: Maitland NSW Circulation: 4418Type: RegionalSize: 33.95 sq.cmsMTWTF--
1 in 3 parents misuse painkillers
Kids are all dosed upA SURVEY of parents has revealedthat one third dose their children upon drugs more heavily than necessaryto treat fever.
The Queensland study showed thatthe pain reliever ibuprofen was admin-istered too frequently by 32 per cent ofmore than 400 parents surveyed.
Most of these were giving the medi-cation every four hours instead, of therecommended six-to-eight hourly in-tervals.
Lead researcher Anne Walsh, fromthe Queensland University of Technol-ogy, said the results were concerning,particularly as parents should not begiving medication to treat mild feverin the first place.
"The fact that they were giving med-ication too frequently is a real worry,"Ms Walsh said.
`But what they don't seem to under-
stand is that a low-grade fever under40 degrees on its own does not need tobe treated.
"The body has purposely set its tem-perature higher to try to stop bacteriafrom multiplying, it's an immune re-sponse."
The standard painkiller paraceta-mol, branded as Panadol, and ibupro-fen. a non-steroidal anti-inflammatorydrug (NSAID) under brands like Nuro-fen, are widely used to treat pain andfever.
Too many parents were alternatingbetween the two medications, makingtiming confusing.
"Given that such a high percentageof parents are giving ibuprofen toofrequently, it may be that they are as-suming it is the same as paracetamolwhich can be given four hourly," Ms
Many were administering both atonce, a potentially dangerous practicethat was not recommended.
Over administering could lead toliver damage and stomach upset, es-pecially if the child is dehydrated bythe fever.
She said it was not parents' faultthey were mismanaging fever, as theywere just following accepted practiceand trying to maintain some controlover their children's wellbeing.
However, there was an urgent needfor evidence-based education for par-ents and the health professionals whogive them information.
"In many cases it would be better ifparents first manage fever by givingtheir children more fluids and rest,and keeping them comfortable."
Walsh said.
back
Ref: 29986358Copyright Agency Limited (CAL) licensed copy
Border Mail07/09/2007Page: 11General NewsRegion: Albury-Wodonga VIC Circulation: 26617Type: RegionalSize: 172.73 sq.cmsMTWTFS-
Painkillers given tokids too often: study
SYDNEY - A survey of parents hasrevealed that one third dose their childrenup on drugs more heavily than necessary totreat fever. The Queensland study showedthat the pain reliever ibuprofen wasadministered too frequently by 32 per centof more than 400 parents surveyed.
Most of these were giving the medicationevery four hours instead of therecommended six-to-eight hourly intervals.
Lead researcher Anne Walsh, from theQueensland University of Technology, saidthe results were concerning, particularly asparents should not be giving medication totreat mild fever in the first place.
back
Ref: 29992382Copyright Agency Limited (CAL) licensed copy
Burnie Advocate07/09/2007Page: 16General NewsRegion: Burnie TAS Circulation: 24811Type: RegionalSize: 42.34 sq.cmsMTWTFS-

Content Supplied by Australian Associated Press© AAP, All Rights Reserved. See disclaimer at http://aap.com.au/disclaimer.asp
back
Ref: 29982370
AAP Newswire06/09/2007NationalRegion: AustraliaMTWTFSS
387
REFERENCES
Abdullah, M. A., Ashong, E. F., Al Habib, S. A., Karrar, Z. A., & Al Jishi, N. M.
(1987). Fever in children: diagnosis and management by nurses, medical students, doctors and parents. Annals of Tropical Paediatrics, 7(3), 194-199.
Ajzen, I. (1985). From intentions to actions: a theory of planned behavior. In J. Kuhl
& J. Beckmann (Eds.), Action control: from cognition to behavior (pp. 11-39). Berlin: Springer Verlag.
Ajzen, I. (1991). The Theory of Planned Behavior. Organizational Behavior and
Human Design Processes, 50, 179-211. Ajzen, I. (2005). Attitudes, personality and behavior (2nd ed.). New York: Open
University Press. Ajzen, I. (2006a). Constructing a TPB questionnaire: conceptual and
methodological considerations. Retrieved 8/3/07, 2007, from http://www.people.umass.edu/aizen/pdf/tpb.measurement.pdf
Ajzen, I. (2006b). Behavioral interventions based on the Theory of Planned
Behavior. Retrieved 21/2/07, 2007, from http://www-unix.oit.umass.edu/~aizen/pdf/tpb.intervention.pdf
Ajzen, I., & Fishbein, M. (1980). A theory of reasoned action. In Understanding
attitudes and predicting social behavior. Englewood Cliffs, New Jersey: Prentice-Hall.
Ajzen, I., & Madden, T. J. (1986). Prediction of goal-directed behavior: attitudes,
intentions and perceived behavioral control. Journal of Experimental Social Psychology, 22, 453-474.
Alander, S. W., Dowd, M. D., Bratton, S. L., & Kearns, G. L. (2001). Pediatric
acetaminophen poisoning - In reply. Archives of Pediatrics & Adolescent Medicine, 155(3), 418-419.
Albarracin, D., Johnson, B. T., Fishbein, M., & Muellerleile, P. A. (2001). Theories of Reasoned Action and Planned Behavior as Models of Condom Use: A Meta-Analysis,. Psychological Bulletin, 127(1), 142-161.
Al-Eissa, Y. A., Al-Sanie, A. M., Al-Alola, S. A., Al-Shaalan, M. A., Ghazal, S. S.,
Al-Harbi, A. H., et al. (2000a). Parental perceptions of fever in children. Annals of Saudi Medicine, 20(3-4), 202-205.
388
Al-Eissa, Y. A., Al-Zamil, F. A., Al-Sanie, A. M., Al-Salloum, A. A., Al-Tuwaijri, H. M., Al-Abdali, N. M., et al. (2000b). Home management of fever in children: rational or ritual? International Journal of Clinical Practice, 54(3), 138-142.
Allotey, P., Reidpath, D. D., & Elsisha, D. (2004). "Social medication" and the
control of children: a qualitative study of over-the-counter medication among Australian children. Pediatrics, 114(3), e378-e383.
Ames, J. T., Hayden, G. F., Campbell, R. E., & Lohr, J. A. (1982). Parents'
conception of their use of over-the-counter medicines. Clinical Pediatrics, 21(5), 298-301.
Anderson, A. R. (1988). Parental perception and management of school-age
children's fevers. Nurse Practitioner, 5(May), 8-18. Anderson, S., Cox, D. N., McKellar, S., Reynolds, J., Lean, M. E. J., & Mela, D. J.
(1998). Take five, a nutrition education intervention to increase fruit and vegetable intakes: impact on attitudes towards dietary change. British Journal of Nutrition, 80, 133-140.
Angalakuditi, M. V., Coley, K. C., & Krenzelok, E. P. (2006). Children's
acetaminophen exposures reported to a regional center. American Journal of Health-System Pharmacy, 63, 323-326.
Annegers, J. F., Hauser, W. A., Shirts, S. B., & Kurland, L. T. (1987). Factors
prognostic of unprovoked seizures after febrile convulsions. New England Journal of Medicine, 316, 493-498.
Arbuckle, J. L. (2005). AMOS 6 (Version 6.0.0). Bethlehem Pike Ste. PA: Spring
House. Armitage, C. J., & Conner, M. (2001). Efficacy of the Theory of Planned Behaviour:
a meta-analytic review. The British Journal of Social Psychology, 40, 471-499.
Atkins, E. (1982). Fever, its history, cause and function. Yale Journal of Biology and
Medicine, 55, 283-289. Australia Post. Australia Post Postcode Datafile pc-full_20051206, 2006. Available
from: http://www1.auspost.com.au/postcodes/ [accessed 8 January 2007]. Autret, E., Billard, C., Bertrand, P., Motte, J., Pouplard, F., & Jonville, A. P. (1990).
Double-blind, randomized trial of diazepam versus placebo for prevention of recurrence of febrile seizures. Journal of Pediatrics, 117(3), 490-494.
Bamberg, S., Ajzen, I., & Schmidt, P. (2003). Choice of travel mode in the theory of
planned bahavior: the roles of past behavior, habit and reasoned action. Basic and Applied Social Psychology, 25(3), 175-187.
389
Bandura, A. (1977). Social learning theory. Edgecliffe, NJ: Prentice-Hall. Banco, L., & Jayasherkaramurthy, S. (1990). The ability of mothers to read a
thermometer. Clinical Pediatrics, 29, 343-345. Baram, T. Z., & Shinnar, S. (2002). Febrile seizures. San Diego, CA: Academic
Press. Barrett, T. W., & Norton, V. C. (2000). Parental Knowledge of Different
Acetaminophen Concentrations for Infants and Children. Academic Emergency Medicine, 7(6), 718-721.
Baumann, R. J. (1999). Technical report: treatment of the child with simple febrile
seizures. Pediatrics, 103(6), e86. Baumann, R. J. (2001). Prevention and management of febrile seizures. Paediatric
Drugs, 3(8), 585-592. Beale, D. A., & Manstead, A. S. (1991). Predicting mothers' inteniotns to limit
frequency of infants sugar intake: testing hte Theory of Planned Behavior. Journal fo Applied Social Psychology, 21(5), 409-431.
Beggs, S., Carroll, P., Walsh, A., & Palmer, H. (under review). Managing uncomplicated pain and fever in children in the community setting. Medical Journal of Australia. Submitted 27th June 2007.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological
Bulletin, 107(2), 238-246. Berg, A. T. (1992). Febrile seizures and epilepsy: the contributions of epidemiology.
Paediatric and Perinatal Epidemiology, 6(2), 145-152. Berg, A. T. (1993). Are febrile seizures provoked by a rapid rise in temperature?
American Journal of Diseases of Children, 147(October), 1101-1103. Berg, A. T., & Shinnar, S. (1996a). Complex febrile seizures - treatment and
outcome. Epilepsia, 37(2), 126-133. Berg, A. T., & Shinnar, S. (1996b). Unprovoked seizures in children with febrile
seizures: short-term outcome. Neurology, 47(2), 562-568. Berg, A. T., Shinnar, S., Darefsky, A. S., Holford, T. R., Shapiro, E. D., Salmon, M.
E., et al. (1997). Predictors of recurrent febrile seizures: a prospective cohort study. Archives of Pediatrics & Adolescent Medicine, 151(4), 371 - 378.
Berg, A. T., Shinnar, S., Hauser, W. A., Alemany, M., Shapiro, E. D., Salmon, M. E.,
et al. (1992). A prospective study of recurrent febrile seizures. The New England Journal of Medicine, 327(16), 1122-1127.

390
Berg, A. T., Shinnar, S., Shapiro, E. D., Salomon, M. E., Crain, E. F., & Hauser, W. A. (1995). Risk factors for a first febrile seizure: a matched case-control study. Epilepsia, 36(4), 334-341.
Bernath, V. F., Anderson, J. N., & Silagy, C. A. (2002). Tepid sponging and
paracetamol for reduction of body temperature in febrile children. Medical Journal of Australia, 176, 130.
Bethune, P., Gordon, K., Dooley, J., Camfield, C., & Camfield, P. (1993). Which
child will have a febrile seizure? American Journal of Diseases of Children, 147, 35-39.
Betz, C. L., & Grunfeld, A. F. (2006). Fever phobia in the emergency department: a
survey of children's caregivers. European Journal of Emergency Medicine, 13(3), 129-133.
Betz, C. L., Hunsberger, M. M., & Wright, S. (Eds.). (1994). Family centred nursing
care of children (2 nd ed.). Philadelphia: W.B. Saunders. Bhrolchain, C. N. (2004). Parents' beliefs and expectations when presenting with a
febrile child at an out-of-hours general practice clinic. Child: Care, Health and Development, 30(1), 92-93.
Bilenko, N., Tessler, H., Okbe, R., Press, J., & Gorodischer, R. (2006). Determinants
of antipyretic misuse in children up to 5 years of age: A cross-sectional study. Clinical Therapeutics, 28(5), 783-793.
Birchley, N., & Conroy, S. (2002). Parental management of over-the-counter
medicines. Paediatric Nursing, 14(9), 24-28. Bland, M. J., & Altman, D. G. (1986). Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet, i, 307-310. Blatteis, C. M. (2003). Fever: pathological or physiological, injurious or beneficial?
Journal of Thermal Biology, 28(1), 1-13. Blatteis, C. M. (2004). The cytokine-prostaglandin cascade in fever production: fact
or fancy? Journal of Thermal Biology, 29(7-8), 359-368. Blatteis, C. M. (2006). Endotoxic fever: New concepts of its regulation suggest new
approaches to its management. Pharmacology & Therapeutics, 111, 194-223. Blatteis, C. M., Feleder, C., Perlik, V., & Li, S. (2004). Possible sequence of
pyrogenic afferent processing in the POA. Journal of Thermal Biology, 29(7-8), 391-400.
Blatteis, C. M., & Sehic, E. (1997). Prostaglandin E2: a putative fever mediator. In P.
A. Mackowiak (Ed.), Fever: Basic Mechanisms and Management (2nd ed., pp. 117–148). New York: Raven-Lippincott.

391
Blatteis, C. M., Sehic, E., & Li, S. (1998). Afferent pathways of pyrogen signaling. Annals of the New York Academy of Sciences, 856(1), 95-107.
Blatteis, C. M. (2003). Fever: pathological or physiological, injurious or beneficial?
Journal of Thermal Biology, 28(1), 1-13. Blue, C. L. (1995). The predictive capacity of the theory of reasoned action and the
theory of planned behavior in exercise research: an integrated literature review. Research in Nursing & Health, 18, 105-121.
Blue, C. L., Wilbur, J., & Marston-Scott, M. (2001). Exercise among blue-collar
workers: application of the theory of planned behavior. Research in Nursing & Health, 24(6), 481-493.
Blumenthal, I. (1998). What parents think of fever. Family Practice, 15(6), 513-518. Blumenthal, I. (2000). Fever and the practice nurse: management and treatment.
Community Practitioner, 73(3), 519-521. Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley. Boulant, J. (2000). Role of the preoptic-anterior hypothalamus in thermoregulation
and fever. Clinical Infectious Diseases, 31, S157-161 Bradshaw, J. (1972). The concept of social need. New Society (March), 640-643. Breakwell, G. M. (2006). Interviewing methods. In G. M. Breakwell, S. Hammond,
C. Fife-Schaw & J. A. Smith (Eds.), Research Methods in Psychology (3rd ed., pp. 232-253). London: Sage Publications Ltd.
Broome, M. E., Dokken, D. L., Broome, C. D., Woodring, B., & Stegelman, M. F.
(2003). A study of parent/grandparent education for managing a febrile illness using the CALM approach. Journal of Pediatric Health Care, 17(4), 176-183.
Browne, G. J., Currow, K., & Rainbow, J. (2001). Practical approach to the febrile
child in the emergency department. Emergency Medicine, 13, 426-435. Bruce, J. L., & Grove, S. K. (1992). Fever: pathology and treatment. Critical Care
Nurse, 12(1), 40-49. Bruhn, F. W., Lelyveld, S., & Ludwig, S. (1991). High fever in a young child.
Patient Care, 25(13), 114-117. Burnard, P. (1991). A method of analysing interview transcripts in qualitative
research. Nurse Education Today, 11, 461-466. Bursey, M., & Craig, C. (2000). Attitudes, subjective norm, perceived behavioral to
adult smoking cessation after coronary artery bypass graft surgery. Public Health Nursing, 17(6), 460-467.
392
Byrne, B. M. (2001). Structural Equation Modeling with AMOS: basic concepts, applications, and programming. Mahwah, NJ: Lawrence Erlbaum Associates, Publishers.
Camfield, P. R., & Camfield, C. S. (1997). Management and treatment of febrile
seizures. Current Problems in Pediatrics, 27, 6-13. Carson, S. M. (2003). Alternating acetaminophen and ibuprofen in the febrile child:
Examination of the evidence regarding efficacy and safety. Pediatric Nursing, 29(5), 379.
Casey, G. (2000). Fever management in children. Pediatric Nursing, 12(3), 38-42. Casey, R., McMahon, F., McCormick, M. C., Pasquariello, P. S., Zavod, W., &
King, F. H. (1984). Fever therapy: an educational intervention for parents. Pediatrics, 73(5), 600-605.
Cha, E. S., Doswell, W. M., Kim, K. H., Charron-Prochownik, D., & Patrick, T. E.
(2006). Evaluating the Theory of Planned Behavior to explain intention to engage in premarital sex amongst Korean college students: A questionnaire survey. International Journal of Nursing Studies, doi:10.1016/j.ijnurstu.2006.04.015
Chamberlain, J. M., Terndrup, T. E., & Alexander, D. T. (1995). Determination of normal ear temperature with an infrared emission detection thermometer. Annals of Emergency Medicine, 25, 15.
Chandra, J., & Bhatnagar, S. K. (2002). Antipyretics in children. Indian Journal of Pediatrics, 69(1), 69-74.
Chang, Y. C., Guo, N. W., Huang, C. C., Wang, S. T., & Tsai, J. J. (2000).
Neurocognitive attention and behavior outcome of school-age children with a history of febrile convulsions: a population study. Epilepsia, 41(4), 412-420.
Chang, Y. C., Guo, N. W., Wang, S. T., Huang, C. C., & Tsai, J. J. (2001). Working
memory of school-aged children with a history of febrile convulsions: a population study. Neurology, 57(1), 37-42.
Chou, C. P., & Bentler, P. M. (1995). Estimates and tests in structural equation
modeling. In R. Hoyle (Ed.), Structural Equation Modeling (pp. 37-55). Thousand Oaks, CA: Sage.
Chien, C., Marriott, J., Ashby, K., & Ozanne-Smith, J. (2003). Unintentional ingestion of over the counter medications in children less than 5 years old Journal of Paediatrics and Child Health, 39(4), 264-269.
Chung, B., Wat, L. C. Y., & Wong, V. (2006). Febrile Seizures in Southern Chinese
Children: Incidence and Recurrence. Pediatric Neurology, 34(2), 121-126. Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159.
393
Commission on Classification and Terminology of the International League Against Epilepsy. (1989). Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia, 30, 389-399.
Connell, F. (1997). The causes and treatment of fever: a literature review. Nursing
Standard, 12(11), 40-43. Conner, M., & Sparks, P. (2005). Theory of Planned Behavior and health behaviour.
In M. Conner & P. Norman (Eds.), Predicting health behaviour: research and practice with social cognition models (2nd ed., pp. 170-222). New York: Open University Press.
Cranswick, N., & Coghlan, D. (2000). Paracetamol efficacy and safety in children:
the first 40 years. American Journal of Therapeutics, 7(2), 135-141. Crocetti, M., Moghbeli, N., & Serwint, J. (2001). Fever phobia revisited: have
parental misconceptions about fever changed in 20 years? Pediatrics, 107(8), 1241-1246.
Crocetti, M., & Serwint, J. R. (2005). Fever: separating fact from fiction.
Contemporary Pediatircs, 22(1), 34-42. Cunha, B. A., Bigamon-Beltran, M., & Gobbo, P. N. (1984). Implications of fever in
a critical care setting. Heart and Lung, 13(5), 460-465. Curran, P. J., West, S. G., & Finch, J. F. (1997). The robustness of test statistics to
nonnormality and specification error in confirmatory factor analysis. Psychological Methods, 1, 16-29.
Curtis, N., & Starr, M. (2000). Infectious diseases. In J. Smart & T. Nolan (Eds.), Paediatric handbook (6th ed., pp. 365-405). Calton South, Victoria: Blackwell Science.
D'Auria, J. P. (1997). Fever. In J. A. Fox (Ed.), Primary health care of children (pp.
770-776). New York: Mosby. Del Vecchio, M. T., & Sundel, E. R. (2001). Alternating antipyretics: Is this an
alternative? Pediatrics, 108(5), 1236. Deng, C. T., Zulkifli, H. I., & Azizi, B. H. (1996). Parental reactions to febrile
seizures in Malaysian children. Medical Journal of Malaysia, 51(4), 462-468. Dershewitz, R. A. (1993). Fever. In R. A. Dershewitz (Ed.), Ambulatory Pediatric
Care (2nd ed., pp. 668-670). Philadelphia: J.B. Lippincott Company. Diaz, E. M. (2002). Theory of planned behavior and pedestrians' intentions to violate
traffic regulations. Transportation Research Part F, 5, 169-175.
394
Dlugosz, C. K., Chater, R. W., & Engle, J. P. (2006). Appropriate Use of Nonprescription Analgesics in Pediatric Patients. Journal of Pediatric Health Care, 20(5), 316-325.
Dodgson, J., Henly, S., Duckett, L., & Tarrant, M. (2003). Theory of planned
behavior-based models for breastfeeding duration among Hong Kong mothers. Nursing Research, 52(3), 148-158.
Doran, T. F., De Angelis, C., Baumgardner, R. A., & Mellits, E. D. (1989).
Acetaminophen: more harm than good for chickenpox. Journal of Pediatrics, 114, 1045-1048.
Downs, D. S., & Hausenblas, H. A. (2005). Elicitation studies and the theory of
planned behavior: a systematic review of exercise beliefs. Psychology of Sport and Exercise, 6(1), 1-31.
Drwal-Klein, L. A., & Phelps, S. J. (1992). Antipyretic therapy in the febrile child.
Clinical Pharmacy, 11(12), 1005-1021. Duff, G. W. (1986). Is fever beneficial: a clinical perspective. Yale Journal of
Biology and Medicine, 59, 125-130. Edwards, H. E., Courtney, M. D., Wilson, J. E., Monaghan, S. J., & Walsh, A. M.
(2001b). Fever management practices: what pediatric nurses say. Nursing and Health Sciences, 3(3), 119-130.
Edwards, H. E., Courtney, M. D., Wilson, J. E., Monaghan, S. J., & Walsh, A. M.
(2003). Fever management audit: Australian nurses antipyretic usage. Pediatric Nursing, 29(1), 31-37.
Edwards, H., Nash, R., Najman, J., Yates, P., Fentiman, B., Dewar, A., et al. (2001a).
Determinations of nurses' intention to administer opioids for pain relief. Nursing and Health Sciences, 3(3), 149-159.
Edwards, H., Nash, R., Yates, P., Walsh, A., Fentiman, B., McDowell, J., et al.
(2001). Improving pain management by nurses: a pilot peer intervention program. Nursing and Health Sciences, 3, 35-45.
Edwards, H., Walsh, A., Courtney, M., Monaghan, S., Wilson, J., & Young, J.
(2007). Improving paediatric nurses' knowledge and attitudes in childhood fever management. Journal of Advanced Nursing, 57(3), 257-269.
Edwards, H., Walsh, A., Courtney, M., Monaghan, S., Wilson, J., & Young, J. (in
press 10th June 2006). Promoting evidence-based childhood fever management through a peer education program based on the Theory of Planned Behavior. Journal of Clinical Nursing.
El-Radhi, A. S., & Carrol, J. (1994). Fever and hyperthermia. In Fever in pediatric
practice (pp. 15-49). Oxford: Blackwell Science.
395
Erlewyn-Lajeunesse, M. D. S., Coppens, K., Hunt, L. P., Chinnick, P. J., Davies, P., Higginson, I. M., et al. (2006). Randomised controlled trial of combined paracetamol and ibuprofen. Archives of Disease in Childhood, 91, 414-416.
eMIMS. (2007). eMIMS2007. Retrieved 5th May, 2007, from www.mims.com.au Ewles, l., & Simnett, I. (2003). Promoting health: a practical approach (5th ed.).
London: Bailliere Tindall. Ferraro, K. (2004). The influence of parental perceptions on the use of booster seats:
an application of the theory of planned behavior. Unpublished Thesis Developmental Psychology, Fordham University, New York, USA.
Fife-Shaw, C. (2006). Introduction to structural equation modelling. In G.
MBreakwell, S. Hammond, C. Fife-Shaw & J. A. Smith (Eds.), Research Methods in Psychology (pp. 444-464). London: Sage Publications Ltd.
Fischer, H., Moore, K., & Roaman, R. R. (1985). Can mothers of infants read a
thermometer? Clinical Pediatrics, 24, 120. Fishbein, M. (1963). An investigation of the relationships between beliefs about an
object and the attitude toward that object. Human Relations, 16, 233-240. Fishbein, M. (2000). The role of theory in HIV prevention. Aids Care, 12(3), 273-
278. Fishbein, M., & Ajzen, I. (1972). Attitudes and opinions. Annual Review of
Psychology, 23, 487-544. Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: an
introduction to theory and research. Reading, MA: Addison-Wesley. Fishbein, M., Hennessy, M., Kamb, M., Bolan, G. A., Hoxworth, T., Iatesta, M., et
al. (2001). Using intervention theory to model factors influencing behavior change. Evaluation and the Health Professions, 24(4), 363-384.
Fisher, J. D., & Fisher, W. A. (2002). The information-motivation-behavioral skills
model. In R. J. DiClemente, R. A. Crosby & M. C. Kegler (Eds.), Emerging theories in health promotion practice and research: strategies for improving public health (pp. 40-70). San Franscisco CA: Jossey-Bass.
Flury, T., Aebi, C., & Donati, F. (2001). Febrile seizures and parental anxiety: does
information help? Swiss Medical Weekly, 131(37-38), 556-560. Francis, J. J., Eccles, M. P., Johnston, M., Walker, A., Grimshaw, J., Foy, R., et al.
(2004). Constructing questionnaires based on the Theory of Planned Behaviour: a manual for health service researchers. Newcastle upon Tyne, UK: Quality of Life and Management of Living Resources. http://www.rebeqi.org/?pageID=40&ItemID=86
396
Freeman, J. M. (1992). The best medicine for febrile seizures. The New England Journal of Medicine, 327(16), 1161 - 1163.
Friedman, A., & Barton, L. (1990). Efficacy of sponging vs acetaminophen for
reduction of fever. Pediatric Emergency Care, 6(1), 6-7. Fruthaler, J. (1985). Fever in children: phobia vs facts. Hospital Practitioner, 20, 49-
53. Galvez, C. A. (2001). How Peruvian mothers appraise pneumonia and the predictors
of their intention to seek medical care when their children have signs of pneumonia. Dissertation Abstracts International: Section B: The Sciences & Engineering, 62(4), 1825.
Gehri, M., Guignard, E., Djahnine, S. R., Cotting, J. Q., Yersin, C., Paolo, E. R., et
al. (2005). When fever, paracetamol? Theory and practice in a paediatric outpatient clinic. Pharmacy World & Science, 27(3), 254.
Gildea, J. H. (1992). When fever becomes an enemy. Pediatric Nursing, 18(2), 165-
167.
Godin, G., & Kok, G. (1996). The theory of planned behavior: a review of its applications to health-related behaviors. The Science of Health Promotion, 11(2), 87-98.
Goldberger, E. (1986). A primer of water, electrolyte, and acid-base syndromes (7th
ed.). Philadelphia: Lea & Febiger. Goldman, R. D. (2006). Alternating ibuprofen and acetaminophen may be more
effective in the treatment of fever in children. The Journal of Pediatrics, 149(1), 140-141.
Goldman, R. D., Ko, K., Linett, L. J., & Scolnik, D. (2004). Antipyretic efficacy and
safety of ibuprofen and acetaminophen in children. Annals of Pharmacotherapy, 38(1), 146-150.
Goldman, R. D., & Scolnik, D. (2004). Underdosing of acetaminophen by parents
and emergency utilization. Pediatric Emergency Care, 20(2), 89-93. Gollwitzer, P. M. (1999). Implementation intentions: strong effects of simple plans.
American Psychologist, 54(7), 493-503. Graham, M. H., Burrell, C. J., & Douglas, R. M. (1990). Adverse effects of aspirin,
acetaminophen, and ibuprofen on immune function, viral shedding, and clinical status in rhinovirus-infected volunteers. Journal of Infectious Diseases, 162, 1277.
Green, J. L., & Thorogood, N. (2004). Qualitative methods in health research.
London: Sage.
397
Green, S. B., & Salkind, N. J. (2005). Using SPSS for Windows ad Mackintosh: analysing and understanding data (4th ed.). Upper Saddle River, New Jersey: Pearson Education.
Greenbaum, T. L. (2000). Moderating focus groups: a practical guide for group
facilitation. Thousand Oaks CA: Sage Publications. Gribetz, B., & Cronley, S. A. (1987). Underdosing of Acetaminophen by parents.
Pediatrics, 80(5), 630-633. Grossman, D., Keen, M. F., Singer, M., & Asher, M. (1995). Current nursing
practices in fever management. MEDSURG Nursing, 4(3), 193-198. Gummeson, L., Jonsson, I., & Conner, M. (1997). Predicting intentions and
behaviour of Swedish 10-16-year-olds at breakfast. Food Quality and Preference, 8(4), 297-306.
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. (2006a).
Multivariate data analysis (6th ed.). Upper Saddle River, NJ: Pearson Education Inc.
Hankins, M., French, D., & Horne, R. (2000). Statistical guidelines for studies of the
theory of reasoned action and the theory of planned behaviour. Psychology & Health, 15(2), 151-161.
Hara, K., Tanabe, T., Aomatsu, T., Inoue, N., Tamaki, H., Okamoto, N., et al.
(2007). Febrile seizures associated with influenza A. Brain and Development, 29, 30-38.
Hardeman, W., Johnston, M., Johnston, D., Bonetti, D., Wareham, N., & Kinmonth,
A. (2002). Application of the Theory of Planned Behaviour in behaviour change interventions: a systematic review. Psychology & Health, 17(2), 123-158.
Herrgard, E. A., Karvonen, M., Luoma, L., Saavalainen, P., Maatta, S., Laukkanen,
E., et al. (2006). Increased number of febrile seizures in children born very preterm: Relation of neonatal, febrile and epileptic seizures and neurological dysfunction to seizure outcome at 16 years of age. Seizure, 15(8), 590-597.
Herzog, L. W., & Coyne, L. J. (1993). What is Fever - normal temperature in infants
less than 3 months old. Clinical Pediatrics, 32(3), 142-146. Heubi, J. E., Barbacci, M. B., & Zimmerman, H. J. (1998). Therapeutic
misadventures with acetaminophen: hepatotoxicity after multiple doses in children. Journal of Paediatrics, 132, 22.
Hirtz, D. G., Nelson, K. B., & Ellenberg, J. H. (1983). Seizures following childhood
immunizations. Journal of Pediatrics, 102, 14-18.
398
Holtzclaw, B. J. (1992). The febrile response in critical care: state of the science. Heart & Lung, 21(5), 482 - 501.
Hoyt, W. T., Warbasse, R. E., & Chu, E. Y. (2006). Construct Validation in
Counseling Psychology Research The Counseling Psychologist, 34(6), 769-805.
Hu, L.-T., & Bentler, P. M. (1999). Cut off criteria for fit indexes in covariance
structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1-55.
Huang, C. C., Wang, S. T., Chang, Y. C., Huang, M. C., Chi, Y. C., & Tsai, J. J.
(1999). Risk factors for a first febrile convulsion in children: a population study in southern Taiwan. Epilepsia, 40(6), 719-725.
Huang, M. (2001). Effects of educational intervention for parents of children with
febrile convulsions. University of Washington. Doctoral Dissertation. Huang, M. C., Liu, C. C., & Huang, C. C. (1998). Effects of an Educational Program
on Parents with Febrile Convulsive Children. Pediatric Neurology, 18(2), 150-155.
Huang, M. C., Liu, C. C., Huang, C. C., & Thomas, K. (2002). Parents responses to
first and recurrent febrile convulsions. Acta Neurologica Scandinavica, 105, 293-299.
Hunter, J. (1973). Study of antipyretic therapy in current use. Archives of Disease in
Childhood, 48, 313-315. Hutt, M. J., Trueman, M., & Hutt, S. J. (1999). Parental perceptions of pre-
adolescent children who have experienced a febrile convulsion: effects of social class and gender. British Journal of Clinical Psychology, 38(Pt 1), 59-72.
Hyam, E., Brawer, M., Herman, J., & Zviele, S. (1989). What's in a teaspoon?
Underdosing with acetaminophen in family practice. Family Practice, 6, 221-223.
Impicciatore, P., Nannini, S., Pandolfini, C., & Bonati, M. (1998). Mothers'
knowledge of, attitudes toward, and management of fever in preschool children in Italy. Preventive Medicine, 27(2), 268-273.
Ipp, M., & Jaffe, D. (1993). Physicians' attitudes toward the diagnosis and
management of fever in children 3 months to 2 years of age. Clinical Pediatrics, 32(2), 66-70.
Isaacs, S. N., Axelrod, P. I., & Lorber, B. (1990). Antipyretic orders in a university
hospital. American Journal of Medicine, 82, 580-586.
399
Janke, J. R. (1994). Development of the breast-feeding attrition prediction tool. Nursing Research, 43(2), 100-104.
Johnson, E. W., Dubovsky, J., Rich, S. S., O'Donovan, C. A., Orr, H. T., Anderson,
V. E., et al. (1998). Evidence for a novel gene for familial febrile convulsions, FEB2, linked to chromosome 19p in an extended family from the Midwest. Human Molecular Genetics., 7(1), 63-67.
Kai, J. (1996a). Parents' difficulties and information needs in coping with acute
illnesses in preschool children: a qualitative study. British Journal of Medicine, 313, 987-990.
Kai, J. (1996b). What worries parents when their preschool children are acutely ill,
and why: a qualitative study. British Medical Journal, 313, 983-986. Kallestrup, P., & Bro, F. (2003). Parents' beliefs and expectations when presenting
with a febrile child at an out-of-hours general practice clinic. British Journal of General Practice, 53(486), 43-44.
Kapasi, A. A., Lorin, M. I., Nirken, M. H., & Yudovich, M. (1980). Parents'
knowledge and sources of knowledge about antipyretic drugs. Journal of Pediatrics, 97, 1035-1037.
Karwowska, A., Nijssen-Jordan, C., Johnson, D., & Davies, H. (2002). Parental and
health care provider understanding of childhood fever: a Canadian perspective. Canadian Journal of Emergency Medicine, 4(6), 394-400.
Kearns, G. L., Leeder, J. S., & Wasserman, G. S. (1998). Acetaminophen overdose
with therapeutic intent. The Journal of Pediatrics, 132(1), 5-8. Kelly, L., Morin, K., & Young, D. (1996). Improving caretakers' knowledge of fever
management in preschool children: is it possible? Journal of Pediatric Health Care, 10(4), 167-173.
Kilmon, C. (1987). Parents' knowledge and practices related to fever management.
Journal of Pediatric Health Care, 1(4), 173-179. Kinmonth, A., Fulton, Y., & Campbell, M. J. (1992). Management of feverish
children at home. British Medical Journal, 305(7), 1134-1136. Kira, R., Torisu, H., Takemoto, M., Nomura, A., Sakai, Y., Sanefuji, M., et al.
(2005). Genetic susceptibility to simple febrile seizures: Interleukin-1[beta] promoter polymorphisms are associated with sporadic cases. Neuroscience Letters, 384(3), 239-244.
Kjeldsen, M., Kyvik, K., Friis, M., & Christensen, K. (2002). Genetic and
environmental factors in febrile seizures: a Danish population-based twin study. Epilepsy Research, 51(1-2), 167.
400
Kline, R. B. (2005). Principles and practices of structural equation modeling (2nd ed.). New York: The Guilford Press.
Kluger, M. J. (1979). Phylogeny of fever. Federation Proceedings, 38(1), 30-34. Kluger, M. (1986). Is fever beneficial. The Yale Journal of Biology and Medicine,
59(2), 89-95. Kluger, M., J., Kozak, W., Conn, C. A., Leon, L. R., & Soszynski, D. (1996). The
adaptive value fo fever. Infectious Disease Clinics of North America, 10(1), 1-20.
Kluger, M. J., Ringler, D. H., & Anver, M. R. (1975). Fever and survival. Science,
188, 166-168. Kluger, S. L., & Johnson, W. G. (1998). Genetics of the febrile seizure susceptibility
trait. Brain and Development, 20, 265-274. Knoebel, E. E., Narang, A. S., & Ey, J. L. (2002). Fever: to treat or not to treat.
Clinical Pediatrics, 41(1), 9-16. Kramer, M. S., Naimark, L. E., & Leduc, D. G. (1985). Parental fever phobia and its
correlates. Pediatrics, 75(6), 1110-1113. Kramer, M. S., Naimark, L. E., Roberts-Brauer, R., McDougall, A., & Leduc, D. G.
(1991). Risks and benefits of paracetamol antipyresis in young children with fever of presumed viral origin [see comments]. Lancet, 337(8741), 591-594.
Kridli, S. A., & Newton, S. E. (2005). Jordanian married Muslim women's intentions
to use oral contraceptives. International Nursing Review, 52, 109-114. Kok, G. (1993). Why are so many health promotion programs ineffective? Health
Promotion Journal of Australia, 3(2), 12-17. Kolfen, W., Pehle, K., & Konig, S. (1998). Is the long-term outcome of children
following febrile convulsions favorable? Developmental Medicine & Child Neurology, 40(10), 667-671.
Kozer, E., Barr, J., Bulkowestein, M., Avgil, M., Greenberg, R., Matias, A., et al.
(2002). A prospective study of multiple supratheraoeutic acetaminophen doses in febrile children. Veterinary and Human Toxicology, 44(2), 106-109.
Kudsen, F. U., Paerregaard, A., Andersen, R., & J., A. (1996). Long term outcome
for febrile convulsions. Archives of Diseases in Childhood, 74, 13-18. Laditan, A. A. (1994). Seizure Recurrence after a 1st Febrile Convulsion. Annals of
Tropical Paediatrics, 14(4), 303-308.
401
Lagerlov, P., Helseth, S., & Holager, T. (2003). Childhood illnesses and the use of paracetamol (acetaminophen): a qualitative study of parents' management of common childhood illnesses. Family Practice, 20(6), 717-723.
Lagerlov, P., Loeb, M., Slettevoll, J., Lingjaerde, O. C., & Fetveit, A. (2006).
Severity of illness and the use of paracetamol in febrile preschool children; a case simulation study of parents' assessments. Family Practice, 23, 618-623.
Lawton, L. (1999). Approaches to needs assessment. In E. R. Perkins, I. Simnett &
L. Wright (Eds.), Evidence-based health promotion (pp. 325-332). West Sussex: John Wiley & Sons.
Li, S. F., Lacher, B., & Crain, E. F. (2000). Acetaminophen and ibuprofen dosing by
parents. Pediatric Emergency Care, 16(6), 394-397. Lien, N., Lytle, L., & Komro, K. (2002). Applying theory of planned behavior to
fruit and vegetable consumption of young adolescents. American Journal of Health Promotion, 16(4), 189-197.
Linder, N., Sirota, L., Snapir, A., Eisen, I., Davidovitch, N., Kaplan, G., et al. (1999).
Parental knowledge of the treatment of fever in children. Israel Medical Association Journal: IMAJ, 1(3), 158-160.
Ling, S. G. (2000). Parental response and understanding towards febrile convulsion.
Medical Journal of Malaysia, 55(4), 419-423. Lorin, M. I. (1990). Pathogenesis of fever and its treatment. In F. Oski, DeAngellis,
C.D., Feigin, R.D., McMillan, J.A., Warshaw, J.B. (Ed.), Principles and practices of pediatrics (pp. 111-1113). Philadelphia PA: Lippincott.
Lorin, M. I. (1994). Pathogenesis of fever and its treatment. In F. Oski, DeAngellis,
C.D., Feigin, R.D., McMillan, J.A., Warshaw, J.B. (Ed.), Principles and practice of pediatrics (2nd ed., pp. 1111-1113). Philadelphia PA: J.B. Lippincott.
Lorin, M. I. (1999). Pathogenesis of fever and its treatment. In J. B. McMillan, C.
DeAngelis, R. D. Feigin & J. B. Warshaw (Eds.), Oski's Pediatrics: principles and practices (3rd ed., pp. 848-850). Philadelphia: Lippincott, Williams & Wilkins.
Lwanga, S. K., & Lemeshow, S. (1991). Sample size determination in health studies.
Geneva: World Health Organization. MacCallum, R. C., & Austin, J. T. (2000). Applications of Structural Equation
Modeling in Psychological Research. Annual Review of Psychology, 51(1), 201-226.
MacDonald, B. K., Johnson, A. L., Sander, J. W., & Shorvon, S. D. (1999). Febrile
convulsions in 220 children--neurological sequelae at 12 years follow-up. European Neurology, 41(4), 179-186.
402
Mackowiak, P. A. (1994). Fever: blessing or curse? a unifying hypothesis. Annals of Internal Medicine, 120(12), 1037-1040.
Mackowiak, P. A. (2000a). Diagnostic implications and clinical consequences of
antipyretic therapy. Clinical Infectious Diseases, 31, S230-S233. Mackowiak, P. A. (2000b). Temperature regulation and the pathogenesis of fever. In
G. L. Mandell, J. E. Bennett & R. Dolin (Eds.), Principles and practices of infectious diseases (pp. 604-622). Philadelphia: Curchill Livingstone.
Mackowiak, P. A., & Boulant, J. A. (1996). Fever's glass ceiling. Clinical Infectious
Diseases, 22(3), 525-536. Mackowiak, P., Wasserman, S. S., & Levine, M. M. (1992). A critical appraisal of
98.6 deg F, the upper limit of the normal body temperature, and other legacies of Carl Reinhold August Wunderlich. Journal of the American Medical Association, 268, 1578-1580.
Mahadevan, S. B. K., McKiernan, P. J., Davies, P., & Kelly, D. A. (2006).
Paracetamol induced hepatotoxicity. Archives of Disease in Childhood, 91(7), 598-603.
Mahar, A. F., Allen, S. J., Milligan, P., Suthumnirund, S., Chotpitayasunondh, T.,
Sabchareon, A., et al. (1994). Tepid sponging to reduce temperature in febrile children in a tropical climate. Clinical Pediatrics, 33(4), 227-231.
Manfredini, R., Vergine, G., Boari, B., Faggioli, R., & Borgna-Pignatti, C. (2004).
Circadian and seasonal variations of first febrile seizure. The Journal of Pediatrics, 145(6), 838-839.
Manstead, A. S. R., Proffitt, C., & Smart, J. (1983). Predicting and understanding
mothers' infant feeding inteniotns and behavior: testing the Theroy of Reasoned Action. Journal of Personality and Social Psychology, 44, 657-671.
Marsh, H. W., & Hau, K. T. (1999). Confirmatory factor analysis for small sample sizes. In R. Hoyle (Ed.), Statistical strategies for small sample research (pp. 252-284). Thousand Oaks CA: Sage.
Marcil, I., Bergeron, J., & Audet, T. (2001). Motivational factors underlying the
intention to drink and drive in young male drivers. Journal of Safety Research, 32, 363-376.
Mason, S., Thorp, S., & Burke, D. (2003). Prehospital use of paracetamol among
children attending the accident and emergency department. Emergency Medicine Journal, 20(1), 88-89.

403
Matziou, V., Brokalaki, H., Kyritsi, H., Perdikaris, P., Gymnopoulou, E., & Merkouris, A. (in press, corrected proof). What Greek mothers know about evaluation and treatment of fever in children: An interview study. International Journal of Nursing Studies. http://www.sciencedirect.com/science/article/B6T7T-4NT253J-1/2/ac7ad1d4894c71bcce879df3d5e6e8f9
May, A., & Bauchner, H. (1992). Fever phobia: the pediatrician's contribution.
Pediatrics, 90(6), 851-854. Mayoral, C. E., Marino, R. V., Rosenfeld, W., & Greensher, J. (2000). Alternating
antipyretics: is this an alternative. Pediatrics, 105(5), 1009-1012. McCamish, M., Timmins, P., Terry, D., & Gallois, C. (1993). A theory-based
intervention: the theory of reasoned action in action. In D. Terry, C. Gallois & M. McCamish (Eds.), The theory of reasoned action: its application to ADIS-preventative health (pp. 185-205). Oxford: Pergamon Press.
McCaul, K. D., Sandgren, A. K., O'Neil, H. K., & Hinsz, V. B. (1993). The value of
the theory of planned behavior, perceived control and self-efficacy expectations for predicting health-protective behaviors. Basic and Applied Social Psychology, 14, 231-252.
McCarthy, P. L. (Ed.). (1999). Fevers and the evaluation of the child with who has
fever (5th ed.). Philadelphia: W.B. Saunders Company. McCarron, K. (1986). Fever-the cardinal vital sign. Critical Care Quarterly, 9, 15-
18. McCaul, K. D., Sandgren, A. K., O'Neil, H. K., & Hinsz, V. B. (1993). The value of
the theory of planned behavior, perceived control and self-efficacy expectations for predicting health-protective behaviors. Basic and Applied Social Psychology, 14, 231-252.
McCullough, H. N. (1998). Acetaminophen and ibuprofen in the management of
fever and mild to moderate pain in children. Paediatrics and Child Health, 3(4), 246-251.
McErlean, M. A., Bartfield, J. M., Kennedy, D. A., Gilman, E. A., Stram, R. L., &
Raccio-Robak, N. (2001). Home antipyretic use in children brought to the emergency department. Pediatric Emergency Care, 17(4), 249-251.
Miles, F. K., Kamath, R., Dorney, S. F., Gaskin, K. J., & O'Loughlin, E. V. (1999).
Accidental paracetamol overdosing and fulminant hepatic failure in children. Medical Journal of Australia., 171(9), 472-475.
Miller, R. (1996). The effect on parents of febrile convulsions. Paediatric Nursing,
8(9), 28-31.
404
Millward, L. J. (2006). Focus groups. In G. M. Breakwell, S. Hammond, C. Fife-Schaw & J. A. Smith (Eds.), Research methods in psychology (3rd ed., pp. 274-298). London: Sage Publications Ltd.
Minicheillo, V., Sullivan, G., Greenwood, K., & Axford, R. (Eds.). (2004).
Handbook of research methods for nursing and health science (2nd ed.). Frenchs Forest, NSW: Pearson Education Australia.
Morgan, D. L. (2004). Focus groups. In S. N. Hesse-Biber & P. Leavy (Eds.),
Approaches to qualitative research: a reader on theory and practice (pp. 263-285). Qxford: Oxford University Press.
Morrison-Beedy, D., Cote-Arsenault, D., & Fischeck Feinstein, N. (2001).
Maximising results with focus groups: moderator and analysis issues. Applied Nursing Research, 14(1), 48-53.
Mukherjee, A., & Mukherjee, A. (2002). Febrile convulsion--an overview. Journal of
the Indian Medical Association, 100(5), 317-319, 326. Murphy, K. A. (1992). Acetaminophen and ibuprofen: fever control and overdose.
Pediatric Nursing, 18(4), 428-431. Murphy, K. A., & Liebman, M. (1995). Fever care: does nursing instruction make a
difference? Journal of Emergency Nursing, 21(5), 461-463. Nabulis, M. N., Tamin, H., Mahfoud, Z., Itani, M., Sabra, R., Chamseddine, F., et al.
(2006). Alternating ibuprofen and acetaminophen in the treatment of febrile children: a pilot study. BMC Medicine. doi:10.1186/1741-7015-4-4
Nakayama, J., & Arinami, T. (2006). Molecular genetics of febrile seizures. Epilepsy
Research, 70S, S190-S198. National Collaborating Centre for Women's and Children's Health [NCCWCH]
(2007). Feverish illness in children. London, UK: Royal College of Obstetricians and Gynaecologists (RCOG Press).
Nelson, D. S., & Ellenberg, J. H. (1983). Febrile seizures. In F. E. Dreifuss (Ed.),
Pediatric Epileptology. Classification and management of seizures in the child (pp. 173-198). Boston, MA.: John Wright-PSG.
Nelson, K. B., & Ellenberg, J. H. (1978). Prognosis in children with febrile seizures.
Pediatrics, 61, 720-727. Nelson, K. B., & Ellenberg, J. H. (Eds.). (1981). Febrile seizures. New York: Raven
Press. Ng, D. K. K., Lam, J. C. Y., & Chow, K. W. (2002). Childhood fever revisited. Hong
Kong Medical Journal, 8(1), 39-43.
405
Nolan, M. T., & Mock, V. (2000). Measuring patient outcomes. Thousand Oaks: Sage Publications.
Offringa, M., Bossuyt, P. M. M., Lubsen, J., Ellenberg, J. H., Nelson, K. B.,
Knudsen, F. U., et al. (1994). Risk factors for seizure recurrence in children with febrile seizures: a pooled analysis of individual patient data from five studies. Journal of Pediatrics, 124(4), 574-584.
Okumura, A., Uemura, N., Suzuki, M., Itomi, K., & Watanabe, K. (2004).
Unconsciousness and delirious behavior in children with febrile seizures. Pediatric Neurology, 30(5), 316-319.
Olsson, U. H., Foss, T., & Breivik, E. (2004). Two equivalent discrepancy functions
for maximum likelihood estimation: do their test statistics follow a noncentral CM-square distribution under model misspecifications? Sociological Methods and Research, 32, 453-510.
Olsson, U. H., Foss, T., Troye, S. V., & Howell, R. D. (2000). Estimation in
structural equation modelling under conditions of misspecification of nonnormatily. Structural Equation Modelling, 7, 557-595.
O'Neill-Murphy, K., Liebman, M., & Barnsteiner, J. H. (2001). Fever education:
does it reduce parent fever anxiety? Pediatric Emergency Care, 17(1), 47-51. Onoe, S., & Nishigaki, T. (2006). EEG spectral analysis in children with febrile
delirium. Brain and Development, 26, 513-518. Ouellette, E. M. (Ed.). (1993). Febrile seizures (2nd ed.). Philadelphia: J.B.
Lippincott Company. Patch, C., Tapsell, L., & Williams, P. (2005). Attitudes and intentions toward
purchasing novel foods enriched with omega-3 fatty acids. Journal of Nutrition Education & Behavior, 37(5), 235-241.
Parmar, R. C., Shau, D. R., & Bavdekar, S. B. (2001). Knowledge, attitude and
practices of parents of children with febrile convulsion. Journal of Postgraduate Medicine, 47(1), 19-23.
Pearce, C., & Curtis, N. (2005). Fever in children. Australian Family Practice, 34(9),
769-771. Polit, D. F., & Beck, C. T. (2006). Essentials of nursing research: methods,
appraisal, and utilization. Philadelphia: Lippincott. Polit, D. F., & Hungler, B. P. (1999). NursIng research: principles and methods.
New York: Lippincott. Poirier, M. P., Davis, P. H., Gonzalez-del Rey, J. A., & Monroe, K. W. (2000).
Pediatric emergency department nurses' perspectives on fever in children. Pediatric Emergency Care, 16(1), 9-12.

406
Porter, R. S., & Wenger, F. G. (2000). Diagnosis and treatment of pediatric fever by caretakers. Journal of Emergency Medicine, 19(1), 1-4.
Principi, N., Esposito, S., Gasparini, R., Marchisio, P., & Crovari, P. (2004). Burden
of influenza in healthy children and their households. Archives of Disease in Childhood, 89(11), 1002-1007.
Prochaska, J. O., Johnson, S., & Lee, P. (1998). The transtheoretical model of
behavior change. In E. B. Schron, J. K. Ockene & W. L. McBee (Eds.), The handbook of health behavior change (2nd ed., pp. 59-84). New York: Springer Publishing Company.
Purssell, E. (2000). The use of antipyretic medications in the prevention of febrile
convulsions in children. Journal of Clinical Nursing, 9(4), 473-480. Quine, L., Rutter, D. R., & Arnold, L. (2001). Persuading school-age cyclists to use
safety helmets: effectiveness of an intervention based on the Theory of Planned Behavior. British Journal of Health Psychology, 6, 327-345.
Rantala, H., Tarkka, R., & Uhari, M. (2000). Preventive treatment for recurrent
febrile seizures. Annals of Medicine, 32(3), 177-180. Reeves-Swift, R. (1990). Rational management of a child's acute fever. MCN,
American Journal of Maternal Child Nursing, 15(2), 82-85. Renfroe, D. H., O'Sullivan, P. S., & McGee, G. W. (1990). The relationship of
attitude, subjective norm, and behavioral intent to the documentation behavior of nurses. Scholarly Inquiry for Nursing Practice, 4(1), 47-60.
Rivis, A., & Sheeran, P. (2003). Descriptive Norms as an Additional Predictor in the
Theory of Planned Behaviour: A Meta-Analysis. Current Psychology: Developmental, Learning, Personality, Social, 22(3), 218-233.
Robbins, H., Hundley, V., & Osman, L. M. (2003). Minor illness education for
parents of young children. Journal of Advanced Nursing, 44(3), 238-247. Robinson, J. S., Schwartz, M., Magwene, K. S., Kreugel, S. A., & Tamburello, D.
(1989). The impact of fever education on clinic utilization. American Journal of Diseases in Children, 143, 698-704.
Rhodes, R. E., & Courneya, K. S. (2005). Threshold assessment of attitude,
subjective norm, and perceived behavioral control for predicting exercise intention and behavior. Psychology of Sport and Exercise, 6(3), 349-361.
Rhodes, R. E., Courneya, K. S., & Jones, L. W. (2005). The theory of planned
behavior and lower-order personality traits: interaction effects in the exercise domain. Personality and Individual Differences, 38(2), 251-265.
Robertson, J. (2002). Management of the child with fever. Collegian, 9(2), 40-42.
407
Rosenstock, I. M. (1974). Historical origins of the Health Belief Model. Health Education Monographs, 2, 328-335.
Roth, J., Rummel, C., Harre, E.-M., Voss, T., Mutze, J., Gerstberger, R., et al.
(2004). Is interleukin-6 the necessary pyrogenic cytokine? Journal of Thermal Biology, 29(7-8), 383-389.
Russell, F. M., Shann, F., Curtis, N., & Mulholand, K. (2003). Evidence on the use
of paracetamol in febrile children. Bulletin of the World Health Organisation, 81(5), 367-372.
Rutter, N., & Metcalfe, D. H. (1978). Febrile convulsions - what do parents do?
British Medical Journal, 2, 1345-1346. Sadovsky, R. (2001). Managing fever without source in infants and children.
American Family Physician, 63(11), 2273. Sadovsky, R. (2002). Managing seizures associated with fever in children. American
Family Physician, 65(10), 2155. Sagraves, R. (1999). Pediatric pharmacology. Febrile seizures -- treatment and
prevention or not? Journal of Pediatric Health Care, 13(2), 79-85. Samples, J. F. (1985). Circadian rhythm: basis for screening fever. Nursing
Research, 34, 377-379. Saphyakhajon, P., & Greene, G. (2006). Alternating acetaminophen and ibuprofen in
children may cause parental confusion and is dangerous. Archives of Pediatric Adolescent Medicine, 160(July), 757.
Sarrell, M., Cohen, H. A., & Kahan, E. (2002). Physicians', nurses', and parents'
attitudes to and knowledge about fever in early childhood. Patient Education and Counselling, 46, 61-65.
Sarrell, M., & Kahan, E. (2003). Impact of a single-session education program on
parental knowledge of and approach to childhood fever. Patient Education and Counseling, 51, 59-63.
Sarrell, E. M., Wielunsky, E., & Cohen, H. A. (2006). Antipyretic treatment in young
children with fever: acetaminophen, ibuprofen, or both alternating in a randomized, double-blind study. Archives of Pediatrics & Adolescent Medicine, 160(2), 197.
Scheifele, D. W. (Ed.). (1994). Infectious disease: fever (2nd ed.). New York: Little,
Brown Company. Schmitt, B. D. (1980). Fever phobia: misconceptions of parents about fevers.
American Journal of Diseases in Children, 134(2), 176-181. Schmitt, B. D. (1984). Fever in childhood. Pediatrics, 74 (Suppl), 929-936.
408
Schmitt, B. D. (1994). Fever in childhood. Pediatrics, 94(5), 929-936. Schmitt, B. D. (2006). Concerns over alternating acetaminophen and ibuprofen for
fever. Archives of Pediatrics and Adolescent Medicine, 160(7), 160-757. Schnaiderman, D., Lahat, E., Sheefer, T., & Aladjem, M. (1993). Antipyretic
effectiveness of acetaminophen in febrile seizures: ongoing prophylaxis versus sporadic usage. European Journal of Pediatrics, 152(9), 747-749.
Sharber, J. (1997). The efficacy of tepid sponge bathing to reduce fever in young
children. American Journal of Emergency Medicine, 15(2), 188-192. Shinnar, S., & O'Dell, C. (2004). Febrile seizures. Pediatric Annals, 33(6), 394-401. Singhi, S., Padmini, P., & Sood, V. (1991). Urban parents' understanding of fever in
children: its danger and treatment practices. Indian Pediatrics, 28(5), 501-505.
Soon, W. S., Cheong, S. K., & Hong, C. Y. (2003). Fever phobia in a primary
healthcare setting: a Singapore perspective. Annals Academy of Medical Journal, Singapore, 32(2 Supp), S26-27.
SPSS. (1996-2003). Data Entry Builder Release 4.0.0 (Version 4.0). Chicago, IL,
US: SPSS Inc. SPSS. (2004). SPSS for Windows, Version 13.0 (Version 11.0). Chicago, IL, US:
SPSS Inc. Stanley, E. D., Jackson, G. G., Panusarn, C., Rubenis, M., & Dirda, V. (1975).
Increased virus shedding with aspirin treatment of rhinovirus infection. Journal of the American Association of Medicine, 231(12), 1248-1251.
Starko, K. M., Ray, C. G., & Dominguez, L. B. (1980). Reyer's Syndrome and
salicyclate use. Pediatrics, 66, 859-864. Steele, R. W., & Garrison, N. (2005). Fever with bacteremia in children. Consultant
(February), 186-192. Stivers, T., Mangione-Smith, R., Elliott, M., McDonald, L., & Heritage, J. (2003).
Why do physicians think parents expect antibiotics? What parnets report vs what physicians believe. The Journal of Family Practice, 52(2), 140-148.
Stone, C. A. (1990). Infections in children. In M. E. Connal & B. A. Johnson (Eds.),
Pediatric emergencies: a handbook for nurses (pp. 111-119). Rockville, Maryland: Aspen Publishers.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.).
Boston, MA: Pearson Education Inc.
409
Taveras, E. M., Durousseau, S., & Flores, G. (2004). Parents' beliefs and practices regarding childhood fever - A study of a multiethnic and socioeconomically diverse sample of parents. Pediatric Emergency Care, 20(9), 579-587.
Terry, D. J., & O'Leary, J. E. (1995). The Theory of Planned Behavior: the effects of
perceived behavioral control and self-efficacy. British Journal of Social Psychology, 34, 199-220.
Thoman, J. E., Duffner, P. K., & Shucard, J. L. (2004). Do serum sodium levels
predict febrile seizure recurrence within 24 hours? Pediatric Neurology, 31(5), 342-344.
Thomas, D. O. (1995). Fever in children: friend or foe? RN, 58(4), 42-48. Thomas, V., Riegel, B., Andrea, J., Murray, P., Gerhart, A., & Gocka, I. (1994).
National survey of pediatric fever management practices among emergency department nurses. Journal of Emergency Nurses, 20(6), 505.
Titchen, T., Cranswick, N., & Beggs, S. (2005). Adverse drug reactions to
nonsteroidal anti-inflammatory drugs, COX-2 inhibitors and paracetamol in a paediatric hospital. British Journal of Clinical Pharmacology, 59(6), 718-723.
Trewin, D. (2005). Australian standard geographical classification (ASGC).
Canberra: Australian Bureau of Statistics. Uhari, M., Rantala, H., Vainionpaa, L., & Kurttila, R. (1995). Effect of
acetaminophen and of low intermittent doses of diazepam on prevention of recurrences of febrile seizures. The Journal of Pediatrics, 126(6), 991-995.
Usherwood, T. P. (1991). Development and randomised controlled trial of a booklet
of advice for parents. British Journal of General Practice, 41, 58-62. Van den Bruel, A., Bruynickx, R., Vermeire, E., Aerssens, P., Aertgeets, B., &
Buntinx, F. (2005). Signs and symptoms in children with a serious infection: a qualitative study. Retrieved 31-8-06, 2006, from www.biomedcantral.com/1471-2296/6/36
van Esch, A., Steyerberg, E. W., Moll, H. A., Offringa, M., Hoes, A. W., Habbema,
J. D., et al. (2000). A study of the efficacy of antipyretic drugs in the prevention of febrile seizure recurrence. Ambulatory Child Health, 6(1), 19-26.
Van Esch, A., Van Steensel-Moll, H. A., Steyerberg, E. W., Offringa, M., Habbema,
J. D., & Derksen-Lubsen, G. (1995). Antipyretic efficacy of ibuprofen and acetaminophen in children with febrile seizures. Archives of Pediatrics & Adolescent Medicine, 149(6), 632-637.
410
van Stuijvenberg, M., de Vos, S., Tjiang, G. C., Steyerberg, E. W., Derksen-Lubsen, G., & Moll, H. A. (1999). Parents' fear regarding fever and febrile seizures. Acta Paediatrica, 88(6), 618-622.
van Stuijvenberg, M., Derksen-Lubsen, G., Steyerberg, E. W., Habbema, J. D., &
Moll, H. A. (1998). Randomized, controlled trial of ibuprofen syrup administered during febrile illnesses to prevent febrile seizure recurrences. Pediatrics, 102(5), E51.
van Stuijvenberg, M., Steyerberg, E. W., Derksen-Lubsen, G., & Moll, H. A. (1998).
Temperature, age, and recurrence of febrile seizure. Archives of Pediatrics & Adolescent Medicine, 152(12), 1170-1181.
Van Ryn, M., & Vinokur, A. D. (1992). How did it work? an examination of the
mechanisms through which an intervnetion for the unemployed promoted job-search behaviors. Amercian Journal of Community Psyhcology, 20, 577-597.
van Zeijl, J. H., Mullart, R. A., Borm, G. F., & Galama, J. M. D. (2004). Recurrence
of febrile seizures in the respiratory season is associated with influenza A. The Journal of Pediatrics, 145(6), 800-805.
VandenBosch, T. M., Lahaie, M., Rickelmann, M. A., & Gutridge, V. (1993).
Redesigning fever management through research utilization. Michigan Nurse, December, 9-11.
Vane, J. R., & Botting, R. M. (1998). Anti-inflammatory drugs and their mechanism
of action. Inflammation Research, 47(14), 78-87. Verbeke, W., & Vackier, I. (2005). Individual determinants of fish consumption:
application of the theory of planned behaviour. Appetite, 44(1), 67-82. Verity, C. M., & Golding, J. (1991). Risk of epilepsy after febrile convulsions: A
national cohort study. British Medical Journal, 303, 1373. Vestergaard, M., Basso, O., Henriksen, T. B., Ostergaard, J., & Olsen, J. (2002).
Febrile convulsions and sudden infant death syndrome. Archives of Diseases in Childhood, 86(2), 125-126.
Wallace, R. H., Berkovic, S. F., Howell, R. A., Sutherland, G. R., & Mulley, J. C.
(1996). Suggestion of a major gene familial febrile convulsion mapping to 8q13-21. Journal of Medical Genetics, 33, 308-312.
Walsh, A. M., & Edwards, H. E. (2006). Management of childhood fever by parents:
literature review. Journal of Advanced Nursing, 54(2), 217-227. Walsh, A. M., Edwards, H. E., Courtney, M. D., Wilson, J. E., & Monaghan, S. J.
(2005). Fever management: paediatric nurses' knowledge, attitudes and influencing factors. Journal of Advanced Nursing, 49(5), 453-464.
411
Walsh, A. M., Edwards, H. E., Courtney, M. D., Wilson, J. E., & Monaghan, S. J. (2006). Paediatric fever management: Continuing education for clinical nurses. Nurse Education Today, 26, 71-77.
Walsh, A. M., Edwards, H. E., & Fraser, J. A. (2007a). Influences on parents' fever
management: beliefs, experiences and information sources. Journal of Clinical Nursing. doi:10.1111/j.1440-1754.2007.01161.x
Walsh, A., Edwards, H., & Fraser, J. (2007b). Over-the-counter medication use for
childhood fever: A cross-sectional study of Australian parents. Journal of Paediatrics and Child Health, doi:10.1111/j.1440-1754.2007.01161.x.
Walson, P. D., Galletta, G., Chomilo, F., Braden, N. J., Sawyer, L., & Scheinbaum,
M. L. (1992). Comparison of multidose ibuprofen and acetaminophen therapy in febrile children. American Journal of Disease in Medicine, 146(5), 626-632.
Wambach, K. A. (1997). Breastfeeding intention and outcome: A test of the theory of
planned behavior. Research in Nursing & Health, 20(1), 51-59. Wambach, K. A., & Koehn, M. (2004). Experiences of infant-feeding decision-
making among urban economically disadvantaged pregnant adolescents. Journal of Advanced Nursing, 48(4), 361-370.
Wang, Y.-S., Lin, H.-H., & Luarn, P. (2006). Predicting consumer intention to use
mobile service. Information Systems Journal, 16(2), 157-179. Waruiru, C., & Appleton, R. (2004). Febrile seizures: an update. Archives of Disease
in Childhood, 89(8), 751-756. Wassmer, E., & Hanlon, M. (1999). Effects of information on parental knowledge of
febrile convulsions. Seizure, 8(7), 421-423. Waterhouse, J., Drust, B., Weinert, D., Edwards, B., Gregson, W., Atkinson, G., et
al. (2005). The circadian rhythm of core temperature: origin and some implications for exercise performance. Chronobiology International, 22(2), 207-225.
Waterston, T. (2002). Managing fever and febrile convulsions in children. The
Practitioner, 246(1634), 356-359. Watson, W. A., Litovitz, T. L., Klein-Schwartz, W., Rodgers, G. C., Youniss, J.,
Reid, N., et al. (2004). 2003 Annual Report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. American Journal of Emergency Medicine, 22(5), 335-404.
Watts, R., Robertson, J., & Thomas, G. (2003). Nursing management of fever in
children: a systematic review. International Journal of Nursing Practice, 9(1), S1-8.
412
Watts, R., Robertson, J., Thomas, G., & Panel, R. (2001). The nursing management of fever in children: a systematic review. Adelaide, Australia: The Joanna Briggs Institute for Evidence Based Nursing and Midwifery.
Webster, J., & Osborne, S. (2005). Using the right type of evidence to answer
clinical questions. In M. Courtney (Ed.), Evidence for Nursing Pracitce (pp. 37-62). Sydney, Australia: Elsevier australia.
Weston, R., & Gore, P. A. (2006). A brief guide to structural equation modelling.
The Counselling Psychologist, 34, 719. Weinstein, M. P., Iannini, P. B., Stratton, C. W., & Eickhoff, T. C. (1978).
Spontaneous bacterial peritonitis. a review of 28 cases with emphasis on improved survival and factors influencing prognosis. The American Journal of Medicine, 64(4), 592-598.
Weiss, J., & Herskowitz, L. (1983). House officer management of the febrile child. A
survey. Clinical Pediatrics., 22(11), 766-769. Wellington, L., White, K. M., & Liossis, P. (2006). Beliefs underlying intentions to
participate in group parenting education. AeJAMH (Australian e-Journal for the Advancement of Mental Health), 5(3), 1-9.
Weston, R., & Gore, P. A. (2006). A brief guide to structural equation modelling.
The Counselling Psychologist, 34, 719. White, K. M., Terry, D. J., & Hogg, M. A. (1994). Safer sex behavior: the role of
attitudes, norms, and control factors. Journal of Applied Social Psychology, 24, 2164-2192.
Whitehead, D., & Russell, G. (2004). How effective are health education programs -
resistence, reactance, rationality adn risk? Recommendations for effective practice. International Journal of Nursing Studies, 41, 163-172.
Wilkinson, S. (2003). Focus groups. In J. A. Smith (Ed.), Qualitative psychology: a
practical guide to research methods (pp. 184-204). London: Sage Publishing Inc.
World Medical Association, W. (2004, 9/10/2004). World Medical Association
Declaration of Helsinki: ethical principles for medical research involving human subjects. Retrieved 21/8/06, 2006, from http://www.wma.net/e/policy/b3.htm
Wood Baker, C., Little, T. D., & Brownell, K. D. (2003). Predicting Adolescent
Eating and Activity Behaviors: The Role of Social Norms and Personal Agency. Health Psychology, 22(2), 189-198.
Wright, A. D., & Liebelt, E. L. (2007). Alternating antipyretics for fever reduction in
children: an unfounded practice passed down to parents from pediatricians. Clinical Pediatrics, 46, 146-150.

413
Yung, & Bentler, P. M. (1996). Bootstrapping techniques in analysis of mean and
covaraince structured. In Marcoulides, G.A. & Schumacker, R.E. (Eds) Advanced Structural Equation Modeling: Isues and Techniques. Mahwah, NJ: Lawrence Erlbaum Associates.
Zeisberger, E. (1999). From humoral fever to neuroimmunological control of fever.
Journal of Thermal Biology, 24(5-6), 287-326.