northeast kansas public schools - edl · northeast kansas public schools ... hospital confinement...
TRANSCRIPT

NortheastKansasPublic Schools
Northeast Kansas Public Schools
Voluntary Employee Benefits Booklet

1
Welcome to Your Voluntary Benefits Program ........................................................................................2
Accident Insurance. .....................................................................................................................................3
Disability Insurance.....................................................................................................................................8
Term Life Insurance ...................................................................................................................................16
Critical Illness Insurance. ..........................................................................................................................19
Cancer Insurance.......................................................................................................................................23
Hospital Confinement Indemnity Insurance ..........................................................................................32
Service Information & Forms ...................................................................................................................36
David Clark
office: 913.451.1120, ext. 103913.451.2650 (f)[email protected]
Contents

2
Welcome to your Colonial Life benefits program
It’s time to enroll in your employee benefits.
This booklet has been provided to inform you of all the new Colonial Life coverage options availableto you. Please take the time to review the various plan designs and coverages and decide whichoption(s) best fit your needs.
Colonial Life values the opportunity to provide the Northeast Kansas Public School Employees these benefits.We look forward to meeting with you during this upcoming enrollment period and assisting you in takingadvantage of the Colonial Life plans of coverage that can help you best meet your family’s insurance needs.With some products, spouse and family coverage is also available. It can help you cover expenses such as:
� Accident insurance helps offset unexpected medical expenses, such as emergency room fees, deductibles and co-payments that can result from a fracture, dislocation or other covered accidental injury.
� Short-Term disability insurance replaces a portion of your income to help make ends meet if you become disabled from a covered accident or covered sickness.
� Life insurance enables you to tailor coverage for your individual needs and helps provide financial security for your family members. A helpful rule of thumb to determine the amount of life insurance you may need is to multiply your current salary by five to eight years.
� Critical illness insurance supplements your major medical coverage by providing a lump-sum benefit that you can use to pay the direct and indirect costs related to a covered critical illness, such as heart attack (myocardial infarction), end-stage renal failure, coronary artery bypass surgery, stroke or major organ transplant.
� Cancer insurance helps offset the out-of-pocket medical and indirect, non-medical expenses related to cancer that most plans don’t cover. This coverage also provides a benefit for specified cancer-screening tests.
� Hospital confinement indemnity insurance provides a lump-sum benefit for a covered hospital confinement or a covered outpatient surgery to help cover co-payments and deductibles that are not covered by most major medical plans.
Colonial Life benefit counselors will be available to assist you during open enrollment. We look forward to speaking with you soon.

3
Acc
iden
t 1.0
-Pre
mie
r
Accidents happen in places where you and your family spend the most time – at work, in the home and on the playground – and they’re unexpected. How you care for them shouldn’t be. In your lifetime, which of these accidental injuries have happened to you or someone you know?
● Sports-related accidental injury● Broken bone● Burn● Concussion● Laceration
● Back or knee injuries
security.
● Car accidents● Falls & spills● Dislocation● Accidental injuries that send you
to the Emergency Room, Urgent Care
What additional features are included?
● Worldwide coverage
● Portable
● Compliant with Healthcare Spending Account (HSA) guidelines
Will my accident claim payment be reduced if I have other insurance?You’re paid regardless of any other insurance you may have with other insurance companies, and the
otherwise).
What if I change employers?If you change jobs or leave your employer, you can take your coverage with you at no additional cost. Your coverage is guaranteed renewable as long as you pay your premiums when they are due or within the grace period.
Can my premium change?Colonial Life can change your premium only if we change it on all policies of this kind in the state where your policy was issued.
Visit coloniallife.com or call our Customer Service Department at 1.800.325.4368 for additional information.
Accident Insurance
4
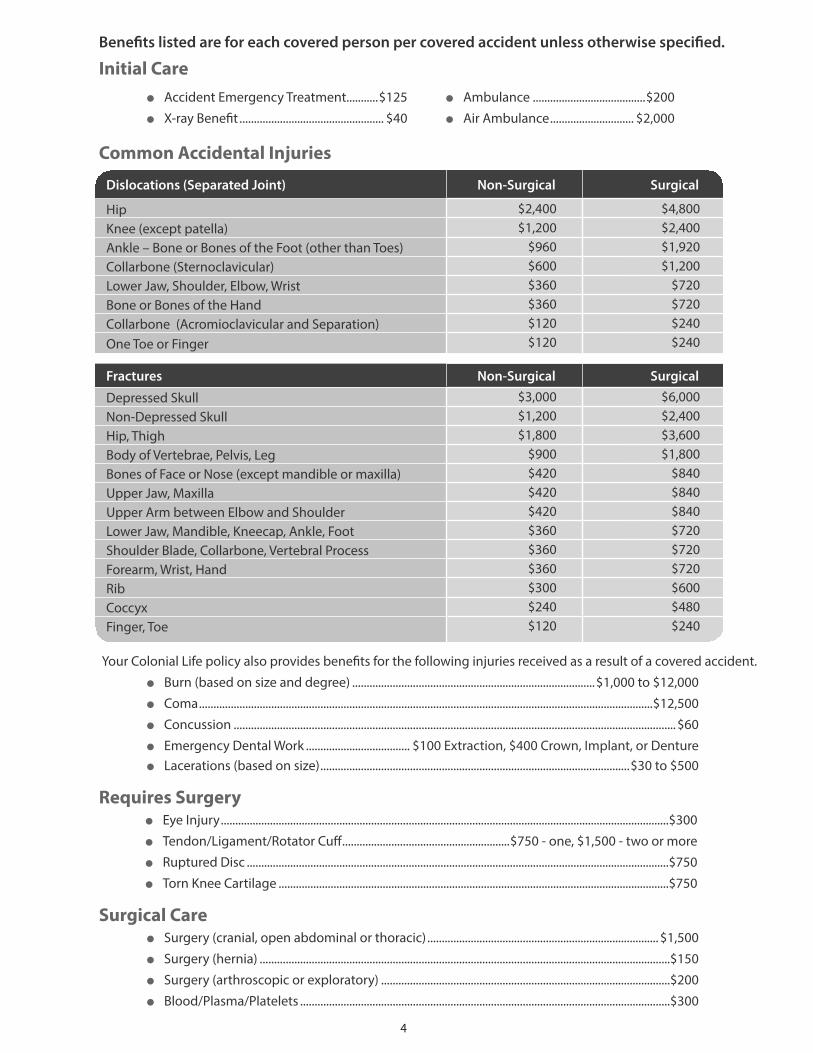
Your Colonial Life policy also provides benefits for the following injuries received as a result of a covered accident.
l Burn (based on size and degree) ....................................................................................$1,000 to $12,000
l Coma .............................................................................................................................................................$12,500
l Concussion .........................................................................................................................................................$60
l Emergency Dental Work .................................... $100 Extraction, $400 Crown, Implant, or Denturel Lacerations (based on size) ...........................................................................................................$30 to $500
Requires Surgeryl Eye Injury ...........................................................................................................................................................$300
l Tendon/Ligament/Rotator Cuff ..........................................................$750 - one, $1,500 - two or more
l Ruptured Disc ..................................................................................................................................................$750
l Torn Knee Cartilage .......................................................................................................................................$750
Surgical Carel Surgery (cranial, open abdominal or thoracic) ................................................................................ $1,500
l Surgery (hernia) ..............................................................................................................................................$150
l Surgery (arthroscopic or exploratory) ....................................................................................................$200
l Blood/Plasma/Platelets ................................................................................................................................$300
Benefits listed are for each covered person per covered accident unless otherwise specified.
Initial Carel Accident Emergency Treatment...........$125 l Ambulance .......................................$200
l X-ray Benefit .................................................. $40 l Air Ambulance ............................. $2,000
Common Accidental Injuries
Dislocations (Separated Joint) Non-Surgical Surgical
Hip $2,400 $4,800Knee (except patella) $1,200 $2,400Ankle – Bone or Bones of the Foot (other than Toes) $960 $1,920Collarbone (Sternoclavicular) $600 $1,200Lower Jaw, Shoulder, Elbow, Wrist $360 $720Bone or Bones of the Hand $360 $720Collarbone (Acromioclavicular and Separation) $120 $240One Toe or Finger $120 $240
Fractures Non-Surgical Surgical
Depressed Skull $3,000 $6,000 Non-Depressed Skull $1,200 $2,400 Hip, Thigh $1,800 $3,600 Body of Vertebrae, Pelvis, Leg $900 $1,800 Bones of Face or Nose (except mandible or maxilla) $420 $840 Upper Jaw, Maxilla $420 $840 Upper Arm between Elbow and Shoulder $420 $840 Lower Jaw, Mandible, Kneecap, Ankle, Foot $360 $720 Shoulder Blade, Collarbone, Vertebral Process $360 $720 Forearm, Wrist, Hand $360 $720 Rib $300 $600 Coccyx $240 $480 Finger, Toe $120 $240

5
Transportation/Lodging AssistanceIf injured, covered person must travel more than 50 miles from residence to receive special treatment and confinement in a hospital.
l Transportation .............................................................................$600 per round trip up to 3 round trips
l Lodging (family member or companion) ...............................................$150 per night up to 30 days for a hotel/motel lodging costs
Accident Hospital Carel Hospital Admission* ........................................................................................................ $1,500 per accident
l Hospital ICU Admission* ................................................................................................ $3,000 per accident* We will pay either the Hospital Admission or Hospital Intensive Care Unit (ICU) Admission, but not both.
l Hospital Confinement ......................................................... $275 per day up to 365 days per accident
l Hospital ICU Confinement ...................................................$550 per day up to 15 days per accident
Accident Follow-Up Carel Accident Follow-Up Doctor Visit .......................................................... $50 (up to 4 visits per accident)
l Medical Imaging Study ......................................................................................................$200 per accident (limit 1 per covered accident and 1 per calendar year)
l Occupational or Physical Therapy ..................................................... $35 per treatment up to 10 days
l Appliances .......................................................................................... $100 (such as wheelchair, crutches)
l Prosthetic Devices/Artificial Limb ....................................................$750 - one, $1,500 - more than 1
l Rehabilitation Unit .................................................$150 per day up to 15 days per covered accident, and 30 days per calendar year. Maximum of 30 days per calendar year
Accidental Dismembermentl Loss of Finger/Toe ............................................................................. $1,250 – one, $2,400 – two or more
l Loss or Loss of Use of Hand/Foot/Sight of Eye .................. $12,000 – one, $24,000 – two or more
Catastrophic AccidentFor severe injuries that result in the total and irrecoverable:
l Loss of one hand and one foot l Loss of the sight of both eyes
l Loss of both hands or both feet l Loss of the hearing of both ears
l Loss or loss of use of one arm and one leg or l Loss of the ability to speak
l Loss or loss of use of both arms or both legs
Named Insured ................ $25,000 Spouse ..............$25,000 Child(ren) .........$12,500
365-day elimination period. Amounts reduced for covered persons age 65 and over. Payable once per lifetime for each covered person.
Accidental DeathAccidental Death Common Carrier
l Named Insured $50,000 $200,000
l Spouse $50,000 $200,000
l Child(ren) $10,000 $40,000

673718-4-KS
EXCLUSIONS
We will not pay benefits for losses that are caused by or are the result of: hazardous avocations; felonies or illegal occupations; racing; semi-professional or professional sports; sickness; suicide or self-inflicted injuries; war or armed conflict; in addition to the exclusions listed above, we also will not pay the Catastrophic Accident benefit for injuries that are caused by or are the result of: intoxication.
For cost and complete details, see your Colonial Life benefits counselor. Applicable to policy form Accident 1.0-NS-KS. This is not an insurance contract and only the actual policy provisions will control.
Colonial Life 1200 Colonial Life BoulevardColumbia, South Carolina 29210coloniallife.com
©2013 Colonial Life & Accident Insurance Company.Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
Colonial Life and Making benefits count are registered service marks of Colonial Life & Accident Insurance Company.
5-13
Accident 1.0-Prem
ier
My Coverage Worksheet (For use with your Colonial Life benefits counselor)
Who will be covered? (check one)
Employee Only Spouse Only One Child Only Employee & Spouse
One-Parent Family, with Employee One-Parent Family, with Spouse Two-Parent Family
When are covered accident benefits available? (check one)
On and Off -Job Benefits Off -Job Only Benefits

7
Accident Rates
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Accident 1.0 Rates
Base Plans
Off Job Accident Coverage
Insured Type Premier with Health ScreeningNamed Insured $22.37Employee & Spouse $29.88One Parent Family $32.19Two Parent Family $39.69
Accident 1.0 Optional Rider Rates 1 Unit of Off-Job Coverage = $100 of Off-Job Monthly Benefit; 1 Unit of On-Job Coverage = $50 of On-Job Monthly Benefit
Rates apply to employee or spouse. (Spouse only qualifies for Off-Job coverage)
On/Off-Job Accident Disability Rider*Monthly Premium per $50 On-Job and $100 Off-Job
Benefit Period 6 monthsElimination Period 0 7 14 30Issue Age 17 - 69 $2.20 $1.90 $1.35 $1.00
Benefit Period 12 monthsElimination Period 0 7 14 30Issue Age 17 - 69 $2.75 $2.40 $1.80 $1.50
Off-Job Only Accident Disability RiderMonthly Premium per $100 Off-Job
Benefit Period 6 monthsElimination Period 0 7 14 30Issue Age 17 - 69 $0.90 $0.80 $0.70 $0.55
Benefit Period 12 monthsElimination Period 0 7 14 30Issue Age 17 – 69 $1.20 $1.10 $1.00 $0.85

8
Educ
ator
Dis
abili
ty 1
.0-K
S
without a paycheck?Help protect your paycheck with Colonial Life’s short-term disability insurance.You use your paycheck mainly to pay for your home, your car, groceries, medical bills and utilities. What if you couldn’t go to work due to an accident or sickness?
Monthly Expenses: $_________________ $_________________ $_________________
$_________________ $_________________ $_________________
Total $_________________
Who’s being covered? You only You and your spouse You and your dependent children You, your spouse and your dependent children
How much coverage do I need? On-Job Accident/On-Job Sickness $______________ $______________ Select One On-Job Total Disability
Option A First 3 months $_____________/month $_____________/month
Next 9 months $_____________/month $_____________/month
Option B First 6 months $_____________/month $_____________/month
Next 6 months $_____________/month $_____________/month
Partial Disability
Up to 3 months $_____________/month $_____________/month
After an Accident: ___________ days After a Sickness: ___________ days
How much will it cost? Your cost will vary based on the level of coverage you select.
My Coverage Worksheet
Educator DisabilityIncome Insurance

9
Employee CoverageIn addition to disability coverage, this plan also provides employees with benefits for medical fees related to accidents, accidental death and dismemberment, as well as fractures and dislocations.
Even if you’re not disabled, the following benefits are payable for covered accidental injuries:
Medical Fees for Accidents OnlyDoctor’s Office or Urgent Care Facility Visit (Once per covered accident) ..................................................................$75X-Ray and Other Diagnostic Imaging (Once per covered accident) .............................................................................$75Emergency Room Visit (Once per covered accident) ...................................................................................................... $150
Accidental Death and Dismemberment Benefits Benefits payable for death or dismemberment.
l Accidental Death .............................................................................................................................................................. $25,000
l Loss of a Finger or Toe Single Dismemberment ................................................................................................................................................. $750 Double Dismemberment ............................................................................................................................................$1,500
l Loss of a Hand, Foot or Sight of an Eye Single Dismemberment ..............................................................................................................................................$7,500 Double Dismemberment ......................................................................................................................................... $15,000
l Accidental Death Common Carrier ........................................................................................................................... $50,000
Complete FracturesComplete Fractures requiring closed reductionHip, Thigh ....................................................................................................................................................................................$1,500Vertebrae ....................................................................................................................................................................................... 1,350 Pelvis ............................................................................................................................................................................................... 1,200Skull (depressed) ......................................................................................................................................................................... 1,125Leg .......................................................................................................................................................................................................900Foot, Ankle, Kneecap .....................................................................................................................................................................750Forearm, Hand, Wrist .....................................................................................................................................................................750Lower Jaw ..........................................................................................................................................................................................600Shoulder Blade, Collarbone ........................................................................................................................................................600Skull (simple) ....................................................................................................................................................................................525 Upper Arm, Upper Jaw .................................................................................................................................................................525Facial Bones ......................................................................................................................................................................................450Vertebral Processes ........................................................................................................................................................................300Coccyx, Rib, Finger, Toe ................................................................................................................................................................120

10
For a fracture or dislocation requiring an open reduction, your benefit would be 11/2 times the amount shown.
Additional Featuresl Waiver of Premium
l Worldwide Coverage
Complete Dislocations requiring closed reduction with anesthesiaHip ..................................................................................................................................................................................................$1,350Knee .....................................................................................................................................................................................................975Collarbone - sternoclavicular ......................................................................................................................................................750 Shoulder ............................................................................................................................................................................................750Collarbone - acromioclavicular separation ............................................................................................................................675Ankle, Foot ........................................................................................................................................................................................600 Hand ....................................................................................................................................................................................................525Lower Jaw ..........................................................................................................................................................................................450Wrist ....................................................................................................................................................................................................375Elbow ..................................................................................................................................................................................................300One Finger, Toe ................................................................................................................................................................................120
Complete Dislocations
Optional Spouse and Dependent Coverage
You may cover one or all of the eligible dependent members of your family for an additional premium.
Medical Fees for Accidents Only Doctor’s Office or Urgent Care Facility Visit (Once per covered accident) ..........................................................$75
X-Ray and Other Diagnostic Imaging (Once per covered accident) .....................................................................$75
Emergency Room Visit (Once per covered accident) .............................................................................................. $150
Accidental Death and Dismemberment Benefits l Accidental Death .................................................................................................................................... Spouse $10,000 Child(ren) $5,000
l Loss of a Finger or Toe
Single Dismemberment ...........................................................................................................................................$75
Double Dismemberment ..................................................................................................................................... $150
l Loss of a Hand, Foot or Sight of an Eye
Single Dismemberment ........................................................................................................................................ $750
Double Dismemberment ..................................................................................................................................$1,500
l Accidental Death Common Carrier .................................................................................................Spouse $20,000
Child(ren) $10,000

11
Educator Disability 1.0-KS
Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
71381-1
Will my disability income payment be reduced if I have other insurance?You’re paid regardless of any other insurance you may have with other insurance companies. Benefits are paid directly to you (unless you specify otherwise).
When am I considered totally disabled?Totally disabled means you are:l Unable to perform the material and substantial duties of your job; l Not working at any job; and l Under the regular and appropriate care of a doctor.
What if I want to return to work part-time after I am totally disabled?You may be able to return to work part-time and still receive benefits. We call this “Partial Disability.” This means you may be eligible for coverage if: l You are unable to perform the material and substantial
duties of your job for more than 20 hours per week, l You are able to work at your job or your place of
employment for 20 hours or less per week, l Your employer will allow you to return to your job or
place of employment for 20 hours or less per week; and l You are under the regular and appropriate care of a doctor.The total disability benefit must have been paid for at least one full month immediately prior to your being partially disabled.
When do disability benefits end?The total disability benefit will end on the policy anniversary date on or after the named insured’s 70th birthday.
What is a pre-existing condition?A pre-existing condition is when you have a sickness or physical condition for which you were treated, had medical testing, received medical advice, or had taken medication within 12 months testing, or before the effective date of your policy.
If you become disabled because of a pre-existing condition, Colonial Life will not pay for any disability period if it begins during the first 12 months the policy is in force.
Here are some
What if I change employers?If you change jobs or leave your employer, you can take your coverage with you at no additional cost. Your coverage is guaranteed renewable to age 70 as long as you continue to pay your premiums when they are due.
Can my premium change?You may choose the amount of coverage to meet your needs (subject to your income). You can elect more or less coverage which will change your premium. Colonial Life can change your premium only if we change it on all policies of this kind in the state where your policy was issued.
What is a covered accident or a covered sickness?A covered accident is an accident. A covered sickness means an illness, infection, disease or any other abnormal physical condition, not caused by an injury.
A covered accident or covered sickness:l Occurs after the effective date of the policy;l Occurs while the policy is in force; l Is of a type listed on the Policy Schedule; andl Is not excluded by name or specific description in
the policy.
EXCLUSIONSWe will not pay benefits for injuries received in accidents or sicknesses which are caused by or are the result of: flying; hazardous avocations; illegal activities; having a pre-existing condition as described and limited by the policy; racing; practicing for or participating in any semi-professional or professional sport; committing or trying to commit suicide or injuring yourself intentionally; being exposed to war or any act of war or serving in the armed forces of any country or authority.
For cost and complete details, see your Colonial Life benefits counselor. Applicable to policy form ED DIS 1.0-KS. Coverage may vary by state and may not be available in all states. This is not an insurance contract and only the actual policy provisions will control.
71752-3
frequently asked questions about Colonial Life’sdisability insurance:
Colonial Life 1200 Colonial Life BoulevardColumbia, South Carolina 29210coloniallife.com
5/11
©2011 Colonial Life & Accident Insurance Company.Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
Colonial Life and Making benefits count are registered service marks of Colonial Life & Accident Insurance Company.
12
Educator Disability Rates
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Educator Disability
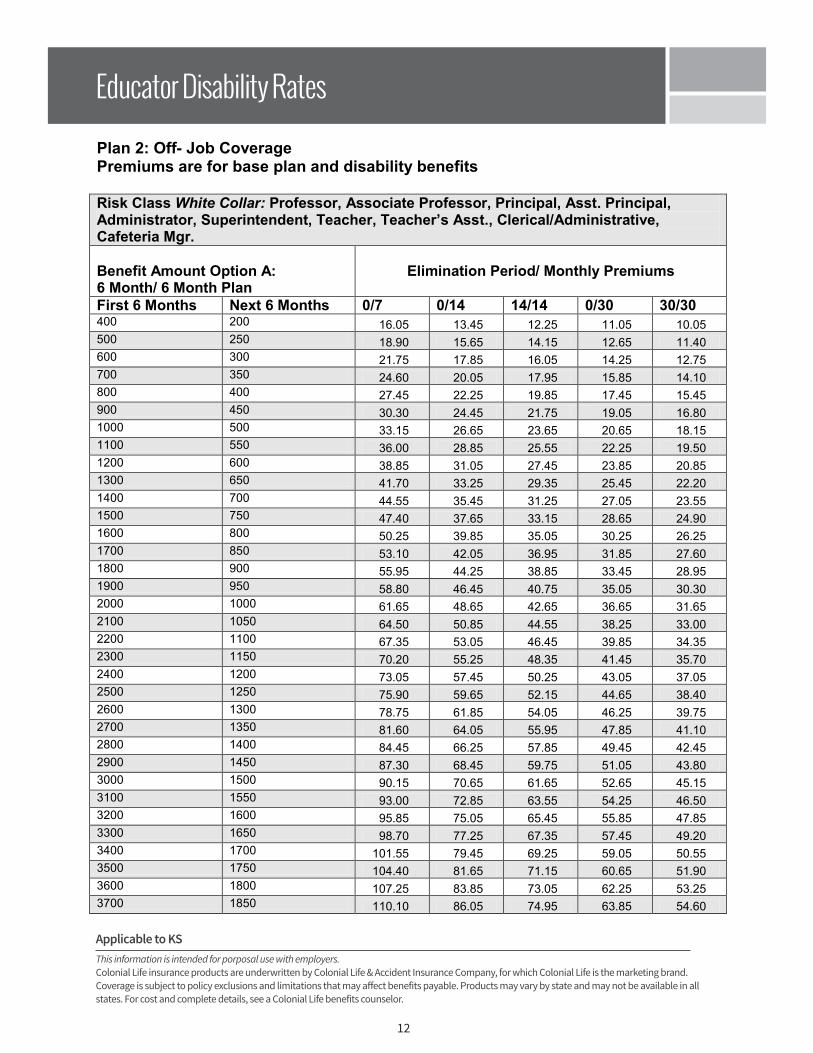
Plan 2: Off- Job Coverage Premiums are for base plan and disability benefits
Risk Class White Collar: Professor, Associate Professor, Principal, Asst. Principal, Administrator, Superintendent, Teacher, Teacher’s Asst., Clerical/Administrative, Cafeteria Mgr.
Benefit Amount Option A: 6 Month/ 6 Month Plan
Elimination Period/ Monthly Premiums
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/30400 200 16.05 13.45 12.25 11.05 10.05 500 250 18.90 15.65 14.15 12.65 11.40 600 300 21.75 17.85 16.05 14.25 12.75 700 350 24.60 20.05 17.95 15.85 14.10 800 400 27.45 22.25 19.85 17.45 15.45 900 450 30.30 24.45 21.75 19.05 16.80 1000 500 33.15 26.65 23.65 20.65 18.15 1100 550 36.00 28.85 25.55 22.25 19.50 1200 600 38.85 31.05 27.45 23.85 20.85 1300 650 41.70 33.25 29.35 25.45 22.20 1400 700 44.55 35.45 31.25 27.05 23.55 1500 750 47.40 37.65 33.15 28.65 24.90 1600 800 50.25 39.85 35.05 30.25 26.25 1700 850 53.10 42.05 36.95 31.85 27.60 1800 900 55.95 44.25 38.85 33.45 28.95 1900 950 58.80 46.45 40.75 35.05 30.30 2000 1000 61.65 48.65 42.65 36.65 31.65 2100 1050 64.50 50.85 44.55 38.25 33.00 2200 1100 67.35 53.05 46.45 39.85 34.35 2300 1150 70.20 55.25 48.35 41.45 35.70 2400 1200 73.05 57.45 50.25 43.05 37.05 2500 1250 75.90 59.65 52.15 44.65 38.40 2600 1300 78.75 61.85 54.05 46.25 39.75 2700 1350 81.60 64.05 55.95 47.85 41.10 2800 1400 84.45 66.25 57.85 49.45 42.45 2900 1450 87.30 68.45 59.75 51.05 43.80 3000 1500 90.15 70.65 61.65 52.65 45.15 3100 1550 93.00 72.85 63.55 54.25 46.50 3200 1600 95.85 75.05 65.45 55.85 47.85 3300 1650 98.70 77.25 67.35 57.45 49.20 3400 1700 101.55 79.45 69.25 59.05 50.55 3500 1750 104.40 81.65 71.15 60.65 51.90 3600 1800 107.25 83.85 73.05 62.25 53.25 3700 1850 110.10 86.05 74.95 63.85 54.60
13
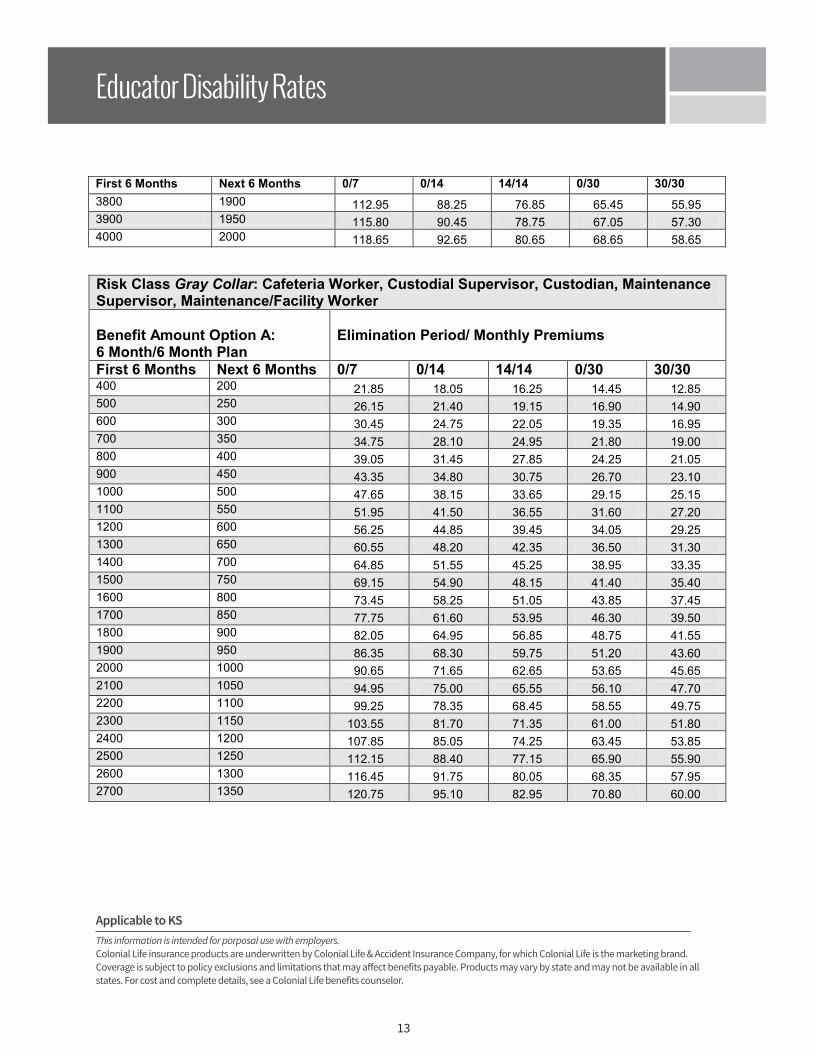
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/303800 1900 112.95 88.25 76.85 65.45 55.95 3900 1950 115.80 90.45 78.75 67.05 57.30 4000 2000 118.65 92.65 80.65 68.65 58.65 4100 2050 121.50 94.85 82.55 70.25 60.00 4200 2100 124.35 97.05 84.45 71.85 61.35 4300 2150 127.20 99.25 86.35 73.45 62.70 4400 2200 130.05 101.45 88.25 75.05 64.05 4500 2250 132.90 103.65 90.15 76.65 65.40 4600 2300 135.75 105.85 92.05 78.25 66.75 4700 2350 138.60 108.05 93.95 79.85 68.10 4800 2400 141.45 110.25 95.85 81.45 69.45 4900 2450 144.30 112.45 97.75 83.05 70.80 5000 2500 147.15 114.65 99.65 84.65 72.15
Risk Class Gray Collar: Cafeteria Worker, Custodial Supervisor, Custodian, Maintenance Supervisor, Maintenance/Facility Worker
Benefit Amount Option A: 6 Month/6 Month Plan
Elimination Period/ Monthly Premiums
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/30400 200 21.85 18.05 16.25 14.45 12.85 500 250 26.15 21.40 19.15 16.90 14.90 600 300 30.45 24.75 22.05 19.35 16.95 700 350 34.75 28.10 24.95 21.80 19.00 800 400 39.05 31.45 27.85 24.25 21.05 900 450 43.35 34.80 30.75 26.70 23.10 1000 500 47.65 38.15 33.65 29.15 25.15 1100 550 51.95 41.50 36.55 31.60 27.20 1200 600 56.25 44.85 39.45 34.05 29.25 1300 650 60.55 48.20 42.35 36.50 31.30 1400 700 64.85 51.55 45.25 38.95 33.35 1500 750 69.15 54.90 48.15 41.40 35.40 1600 800 73.45 58.25 51.05 43.85 37.45 1700 850 77.75 61.60 53.95 46.30 39.50 1800 900 82.05 64.95 56.85 48.75 41.55 1900 950 86.35 68.30 59.75 51.20 43.60 2000 1000 90.65 71.65 62.65 53.65 45.65 2100 1050 94.95 75.00 65.55 56.10 47.70 2200 1100 99.25 78.35 68.45 58.55 49.75 2300 1150 103.55 81.70 71.35 61.00 51.80 2400 1200 107.85 85.05 74.25 63.45 53.85 2500 1250 112.15 88.40 77.15 65.90 55.90 2600 1300 116.45 91.75 80.05 68.35 57.95 2700 1350 120.75 95.10 82.95 70.80 60.00
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Educator Disability Rates
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/303800 1900 112.95 88.25 76.85 65.45 55.95 3900 1950 115.80 90.45 78.75 67.05 57.30 4000 2000 118.65 92.65 80.65 68.65 58.65 4100 2050 121.50 94.85 82.55 70.25 60.00 4200 2100 124.35 97.05 84.45 71.85 61.35 4300 2150 127.20 99.25 86.35 73.45 62.70 4400 2200 130.05 101.45 88.25 75.05 64.05 4500 2250 132.90 103.65 90.15 76.65 65.40 4600 2300 135.75 105.85 92.05 78.25 66.75 4700 2350 138.60 108.05 93.95 79.85 68.10 4800 2400 141.45 110.25 95.85 81.45 69.45 4900 2450 144.30 112.45 97.75 83.05 70.80 5000 2500 147.15 114.65 99.65 84.65 72.15
Risk Class Gray Collar: Cafeteria Worker, Custodial Supervisor, Custodian, Maintenance Supervisor, Maintenance/Facility Worker
Benefit Amount Option A: 6 Month/6 Month Plan
Elimination Period/ Monthly Premiums
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/30400 200 21.85 18.05 16.25 14.45 12.85 500 250 26.15 21.40 19.15 16.90 14.90 600 300 30.45 24.75 22.05 19.35 16.95 700 350 34.75 28.10 24.95 21.80 19.00 800 400 39.05 31.45 27.85 24.25 21.05 900 450 43.35 34.80 30.75 26.70 23.10 1000 500 47.65 38.15 33.65 29.15 25.15 1100 550 51.95 41.50 36.55 31.60 27.20 1200 600 56.25 44.85 39.45 34.05 29.25 1300 650 60.55 48.20 42.35 36.50 31.30 1400 700 64.85 51.55 45.25 38.95 33.35 1500 750 69.15 54.90 48.15 41.40 35.40 1600 800 73.45 58.25 51.05 43.85 37.45 1700 850 77.75 61.60 53.95 46.30 39.50 1800 900 82.05 64.95 56.85 48.75 41.55 1900 950 86.35 68.30 59.75 51.20 43.60 2000 1000 90.65 71.65 62.65 53.65 45.65 2100 1050 94.95 75.00 65.55 56.10 47.70 2200 1100 99.25 78.35 68.45 58.55 49.75 2300 1150 103.55 81.70 71.35 61.00 51.80 2400 1200 107.85 85.05 74.25 63.45 53.85 2500 1250 112.15 88.40 77.15 65.90 55.90 2600 1300 116.45 91.75 80.05 68.35 57.95 2700 1350 120.75 95.10 82.95 70.80 60.00

14
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/302800 1400 125.05 98.45 85.85 73.25 62.05 2900 1450 129.35 101.80 88.75 75.70 64.10 3000 1500 133.65 105.15 91.65 78.15 66.15 3100 1550 137.95 108.50 94.55 80.60 68.20 3200 1600 142.25 111.85 97.45 83.05 70.25 3300 1650 146.55 115.20 100.35 85.50 72.30 3400 1700 150.85 118.55 103.25 87.95 74.35 3500 1750 155.15 121.90 106.15 90.40 76.40 3600 1800 159.45 125.25 109.05 92.85 78.45 3700 1850 163.75 128.60 111.95 95.30 80.50 3800 1900 168.05 131.95 114.85 97.75 82.55 3900 1950 172.35 135.30 117.75 100.20 84.60 4000 2000 176.65 138.65 120.65 102.65 86.65 4100 2050 180.95 142.00 123.55 105.10 88.70 4200 2100 185.25 145.35 126.45 107.55 90.75 4300 2150 189.55 148.70 129.35 110.00 92.80 4400 2200 193.85 152.05 132.25 112.45 94.85 4500 2250 198.15 155.40 135.15 114.90 96.90 4600 2300 202.45 158.75 138.05 117.35 98.95 4700 2350 206.75 162.10 140.95 119.80 101.00 4800 2400 211.05 165.45 143.85 122.25 103.05 4900 2450 215.35 168.80 146.75 124.70 105.10 5000 2500 219.65 172.15 149.65 127.15 107.15
Risk Class Blue Collar: Mechanic, Bus Driver
Benefit Amount Option A: 6 Month/6 Month Plan
Elimination Period/ Monthly Premium
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/30400 200 24.85 20.05 18.25 16.25 14.25 500 250 29.90 23.90 21.65 19.15 16.65 600 300 34.95 27.75 25.05 22.05 19.05 700 350 40.00 31.60 28.45 24.95 21.45 800 400 45.05 35.45 31.85 27.85 23.85 900 450 50.10 39.30 35.25 30.75 26.25 1000 500 55.15 43.15 38.65 33.65 28.65 1100 550 60.20 47.00 42.05 36.55 31.05 1200 600 65.25 50.85 45.45 39.45 33.45 1300 650 70.30 54.70 48.85 42.35 35.85 1400 700 75.35 58.55 52.25 45.25 38.25 1500 750 80.40 62.40 55.65 48.15 40.65 1600 800 85.45 66.25 59.05 51.05 43.05 1700 850 90.50 70.10 62.45 53.95 45.45 1800 900 95.55 73.95 65.85 56.85 47.85 1900 950 100.60 77.80 69.25 59.75 50.25
Educator Disability Rates
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/302800 1400 125.05 98.45 85.85 73.25 62.05 2900 1450 129.35 101.80 88.75 75.70 64.10 3000 1500 133.65 105.15 91.65 78.15 66.15 3100 1550 137.95 108.50 94.55 80.60 68.20 3200 1600 142.25 111.85 97.45 83.05 70.25 3300 1650 146.55 115.20 100.35 85.50 72.30 3400 1700 150.85 118.55 103.25 87.95 74.35 3500 1750 155.15 121.90 106.15 90.40 76.40 3600 1800 159.45 125.25 109.05 92.85 78.45 3700 1850 163.75 128.60 111.95 95.30 80.50 3800 1900 168.05 131.95 114.85 97.75 82.55 3900 1950 172.35 135.30 117.75 100.20 84.60 4000 2000 176.65 138.65 120.65 102.65 86.65 4100 2050 180.95 142.00 123.55 105.10 88.70 4200 2100 185.25 145.35 126.45 107.55 90.75 4300 2150 189.55 148.70 129.35 110.00 92.80 4400 2200 193.85 152.05 132.25 112.45 94.85 4500 2250 198.15 155.40 135.15 114.90 96.90 4600 2300 202.45 158.75 138.05 117.35 98.95 4700 2350 206.75 162.10 140.95 119.80 101.00 4800 2400 211.05 165.45 143.85 122.25 103.05 4900 2450 215.35 168.80 146.75 124.70 105.10 5000 2500 219.65 172.15 149.65 127.15 107.15
Risk Class Blue Collar: Mechanic, Bus Driver
Benefit Amount Option A: 6 Month/6 Month Plan
Elimination Period/ Monthly Premium
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/30400 200 24.85 20.05 18.25 16.25 14.25 500 250 29.90 23.90 21.65 19.15 16.65 600 300 34.95 27.75 25.05 22.05 19.05 700 350 40.00 31.60 28.45 24.95 21.45 800 400 45.05 35.45 31.85 27.85 23.85 900 450 50.10 39.30 35.25 30.75 26.25 1000 500 55.15 43.15 38.65 33.65 28.65 1100 550 60.20 47.00 42.05 36.55 31.05 1200 600 65.25 50.85 45.45 39.45 33.45 1300 650 70.30 54.70 48.85 42.35 35.85 1400 700 75.35 58.55 52.25 45.25 38.25 1500 750 80.40 62.40 55.65 48.15 40.65 1600 800 85.45 66.25 59.05 51.05 43.05 1700 850 90.50 70.10 62.45 53.95 45.45 1800 900 95.55 73.95 65.85 56.85 47.85 1900 950 100.60 77.80 69.25 59.75 50.25
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.

15
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/302000 1000 105.65 81.65 72.65 62.65 52.65 2100 1050 110.70 85.50 76.05 65.55 55.05 2200 1100 115.75 89.35 79.45 68.45 57.45 2300 1150 120.80 93.20 82.85 71.35 59.85 2400 1200 125.85 97.05 86.25 74.25 62.25 2500 1250 130.90 100.90 89.65 77.15 64.65 2600 1300 135.95 104.75 93.05 80.05 67.05 2700 1350 141.00 108.60 96.45 82.95 69.45 2800 1400 146.05 112.45 99.85 85.85 71.85 2900 1450 151.10 116.30 103.25 88.75 74.25 3000 1500 156.15 120.15 106.65 91.65 76.65 3100 1550 161.20 124.00 110.05 94.55 79.05 3200 1600 166.25 127.85 113.45 97.45 81.45 3300 1650 171.30 131.70 116.85 100.35 83.85 3400 1700 176.35 135.55 120.25 103.25 86.25 3500 1750 181.40 139.40 123.65 106.15 88.65 3600 1800 186.45 143.25 127.05 109.05 91.05 3700 1850 191.50 147.10 130.45 111.95 93.45 3800 1900 196.55 150.95 133.85 114.85 95.85 3900 1950 201.60 154.80 137.25 117.75 98.25 4000 2000 206.65 158.65 140.65 120.65 100.65 4100 2050 211.70 162.50 144.05 123.55 103.05 4200 2100 216.75 166.35 147.45 126.45 105.45 4300 2150 221.80 170.20 150.85 129.35 107.85 4400 2200 226.85 174.05 154.25 132.25 110.25 4500 2250 231.90 177.90 157.65 135.15 112.65 4600 2300 236.95 181.75 161.05 138.05 115.05 4700 2350 242.00 185.60 164.45 140.95 117.45 4800 2400 247.05 189.45 167.85 143.85 119.85 4900 2450 252.10 193.30 171.25 146.75 122.25 5000 2500 257.15 197.15 174.65 149.65 124.65
Spouse and Dependent PremiumsRider Monthly PremiumSpouse Accident & Sickness Benefit Coverage 5.50 Child(ren) Accident & Sickness Benefit Coverage 7.50
Educator Disability Rates
First 6 Months Next 6 Months 0/7 0/14 14/14 0/30 30/302000 1000 105.65 81.65 72.65 62.65 52.65 2100 1050 110.70 85.50 76.05 65.55 55.05 2200 1100 115.75 89.35 79.45 68.45 57.45 2300 1150 120.80 93.20 82.85 71.35 59.85 2400 1200 125.85 97.05 86.25 74.25 62.25 2500 1250 130.90 100.90 89.65 77.15 64.65 2600 1300 135.95 104.75 93.05 80.05 67.05 2700 1350 141.00 108.60 96.45 82.95 69.45 2800 1400 146.05 112.45 99.85 85.85 71.85 2900 1450 151.10 116.30 103.25 88.75 74.25 3000 1500 156.15 120.15 106.65 91.65 76.65 3100 1550 161.20 124.00 110.05 94.55 79.05 3200 1600 166.25 127.85 113.45 97.45 81.45 3300 1650 171.30 131.70 116.85 100.35 83.85 3400 1700 176.35 135.55 120.25 103.25 86.25 3500 1750 181.40 139.40 123.65 106.15 88.65 3600 1800 186.45 143.25 127.05 109.05 91.05 3700 1850 191.50 147.10 130.45 111.95 93.45 3800 1900 196.55 150.95 133.85 114.85 95.85 3900 1950 201.60 154.80 137.25 117.75 98.25 4000 2000 206.65 158.65 140.65 120.65 100.65 4100 2050 211.70 162.50 144.05 123.55 103.05 4200 2100 216.75 166.35 147.45 126.45 105.45 4300 2150 221.80 170.20 150.85 129.35 107.85 4400 2200 226.85 174.05 154.25 132.25 110.25 4500 2250 231.90 177.90 157.65 135.15 112.65 4600 2300 236.95 181.75 161.05 138.05 115.05 4700 2350 242.00 185.60 164.45 140.95 117.45 4800 2400 247.05 189.45 167.85 143.85 119.85 4900 2450 252.10 193.30 171.25 146.75 122.25 5000 2500 257.15 197.15 174.65 149.65 124.65
Spouse and Dependent PremiumsRider Monthly PremiumSpouse Accident & Sickness Benefit Coverage 5.50 Child(ren) Accident & Sickness Benefit Coverage 7.50
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
16
Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Term Life Insurance
Help protect the people who depend on youIf something happened to you, the last thing your family should have to worry about is financial burdens. Funeral expenses, medical bills and taxes could be just the beginning. How would they cover ongoing living expenses, such as a mortgage, utilities and health care?
Plan for the future with term life insurance from Colonial Life & Accident Insurance Company.
The advantages of term life insurance � Level death benefit. � Lower cost option compared with cash value insurance. � Coverage for specified periods of time, which can be during high-need years.
� Benefit for the beneficiary that is typically free from income tax.
Benefits and features � Guaranteed premiums do not increase during the term. � Coverage is guaranteed renewable to age 95 as long as premiums are paid when due.
� You can convert it to cash value insurance. � Portability allows you to take it with you if you change jobs or retire.
� An Accelerated Death Benefit is included.
Your cost will vary based on the level of coverage you select.
Talk with your Colonial Life benefits counselor for information
about what level of coverage would work best for you.
TERM LIFE 1000

17
Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Benefits worksheetFor use with your Colonial Life
benefits counselor
£ YOU $ __________________ FACE AMOUNT
Select the term period£ 10-year term£ 20-year term£ 30-year term
£ SPOUSE $ ______________ FACE AMOUNT
Select the term period£ 10-year term£ 20-year term£ 30-year term
Select any optional riders:
£ Spouse Term Life Rider $ _____________ face amount for ________-year term period
£ Children’s Term Life Rider $ _____________ face amount
£ Waiver of Premium Benefit Rider
£ Accidental Death Benefit Rider
HOW MUCH COVERAGE DO YOU NEED?
To learn more, talk with your Colonial Life
benefits counselor. EXCLUSIONS AND LIMITATIONSIf the insured commits suicide within two years (one year in CO and ND) from the coverage effective date, whether he is sane or insane (not applicable in AZ), we will not pay the death benefit. We will terminate this policy and return the premiums paid, without interest. In MO, should death occur as a result of suicide, our company is responsible only for the return of premiums paid when application is made with intent to commit suicide.
You will receive a policy summary or illustration (whichever is applicable to your state) when your policy is issued if this policy has exclusions, limitations or reductions of benefits. For costs and complete details, call or write your Colonial Life benefits counselor or the company. This brochure is applicable to policy forms TERM1000, R-TERM1000-ADB, R-TERM1000-CTR, R-TERM1000-STR, R-TERM1000-WAIVER (and applicable state variations, for example: TERM1000-TX, R-TERM1000-ADB-TX-1, R-TERM1000-CTR-TX, R-TERM1000-STR-TX and R-TERM1000-WAIVER-TX-1). See your Colonial Life benefits counselor for additional information specific for your state. This coverage contains limitations and exclusions that may affect benefits payable. Product may vary by state.
Cash value policy conversionYou can convert your policy to a Colonial Life cash value life insurance policy any time through age 75 (unless you have used the Accelerated Death Benefit or Waiver of Premium Benefit Rider) with no evidence of insurability. Premiums will be based on your age at the time you convert your policy.
Accelerated Death BenefitIf you are diagnosed with a terminal illness, you can request up to 75% of the policy’s death benefit, not to exceed $150,000. We deduct a fee only if you use the benefit, and your death benefit will then be reduced by the amount you receive. In addition, there may be tax consequences for receiving the accelerated benefit; ask your tax advisor for advice. Please refer to your policy for details.
Spouse coverage optionsTwo options are available for spouse coverage at an additional cost:
1. Spouse Term Life Policy: Offers guaranteed premiums and level death benefits equivalent to those available to you – whether or not you buy a policy for yourself.
2. Spouse Term Life Rider: Add a term rider for your spouse to your policy, up to a maximum death benefit of $50,000; 10-year and 20-year are available (20-year rider only available with a 20- or 30-year term policy).
Dependent coverageYou may add a Children’s Term Life Rider to cover all of your eligible dependent children with up to $10,000 in coverage each for one premium. The Children’s Term Life Rider may be added to either the primary or spouse policy, not both.
Waiver of Premium Benefit RiderThis rider waives all premiums (for the policy and any riders) if you become totally and permanently disabled before the age of 65. To be considered permanent, your total disability must continue with no interruptions for at least six consecutive months. Premiums waived by this rider do not have to be repaid. This rider is available for the spouse policy as well, subject to home office approval.
Accidental Death Benefit RiderThis rider provides an additional benefit to the beneficiary if the insured dies as a result of an accident before age 70. The benefit doubles if the injury resulting in death occurs while insured is a fare-paying passenger on a public conveyance, such as a commercial aircraft or taxicab. An additional seatbelt benefit is also payable.
©2014 Colonial Life & Accident Insurance Company, Columbia, SC | Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand. 7-14 | 64815-9
ColonialLife.com

18
Term Life Rates
Applicable to KS . This information is only intended for proposal use with employers. Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand. Colonial Life & Accident Insurance Company 1200 Colonial Life Boulevard, Columbia, South Carolina 29210
Term Life 1000 Sample Monthly Premiums
10 Year Term Policy $10,000
Face Amount $25,000
Face Amount $50,000
Face Amount $75,000
Face Amount $100,000
Face Amount Issue Age
Non-tobacco
Tobacco Non-tobacco
Tobacco Non-tobacco
Tobacco Non-tobacco
Tobacco Non-tobacco
Tobacco
25 $5.13 $5.74 $6.83 $8.35 $9.67 $12.71 $12.50 $17.06 $15.33 $21.42
35 5.13 6.17 6.83 9.42 9.67 14.83 12.50 20.25 15.33 25.67
45 6.48 9.88 10.21 18.69 16.42 33.38 22.63 48.06 28.83 62.75
55 9.83 20.12 18.58 44.29 33.17 84.58 47.75 124.88 62.33 165.17
65 19.58 35.67 42.96 83.17 81.92 162.33 120.88 241.50 159.83 320.67
75 55.20 74.87 132.00 181.17 260.00 358.33 388.00 535.50 516.00 712.67
20 Year Term Policy $10,000
Face Amount $25,000
Face Amount $50,000
Face Amount $75,000
Face Amount $100,000
Face Amount Issue Age Non-
tobacco Tobacco Non-
tobacco Tobacco Non
tobacco Tobacco Non-
tobacco Tobacco Non
tobacco Tobacco
25 $5.22 $5.90 $7.04 $8.75 $10.08 $13.50 $13.13 $18.25 $16.17 $23.00
35 5.53 7.07 7.81 11.67 11.63 19.33 15.44 27.00 19.25 34.67
45 7.66 12.33 13.15 24.81 22.29 45.63 31.44 66.44 40.58 87.25
55 13.24 23.83 27.10 53.56 50.21 103.13 73.31 152.69 96.42 202.25
65 28.94 45.24 66.35 107.10 128.71 210.21 191.06 313.31 253.42 416.42
30 Year Term Policy $10,000
Face Amount $25,000
Face Amount $50,000
Face Amount $75,000
Face Amount $100,000
Face Amount Issue Age Non-
tobacco Tobacco Non-
tobacco Tobacco Non-
tobacco Tobacco Non-
tobacco Tobacco Non
tobacco Tobacco
25 $5.55 $7.07 $7.88 $11.67 $11.75 $19.33 $15.63 $27.00 $19.50 $34.67
35 6.29 8.92 9.73 16.29 15.46 28.58 21.19 40.88 26.92 53.17
45 9.85 14.70 18.63 30.75 33.25 57.50 47.88 84.25 62.50 111.00
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
19
Insurance
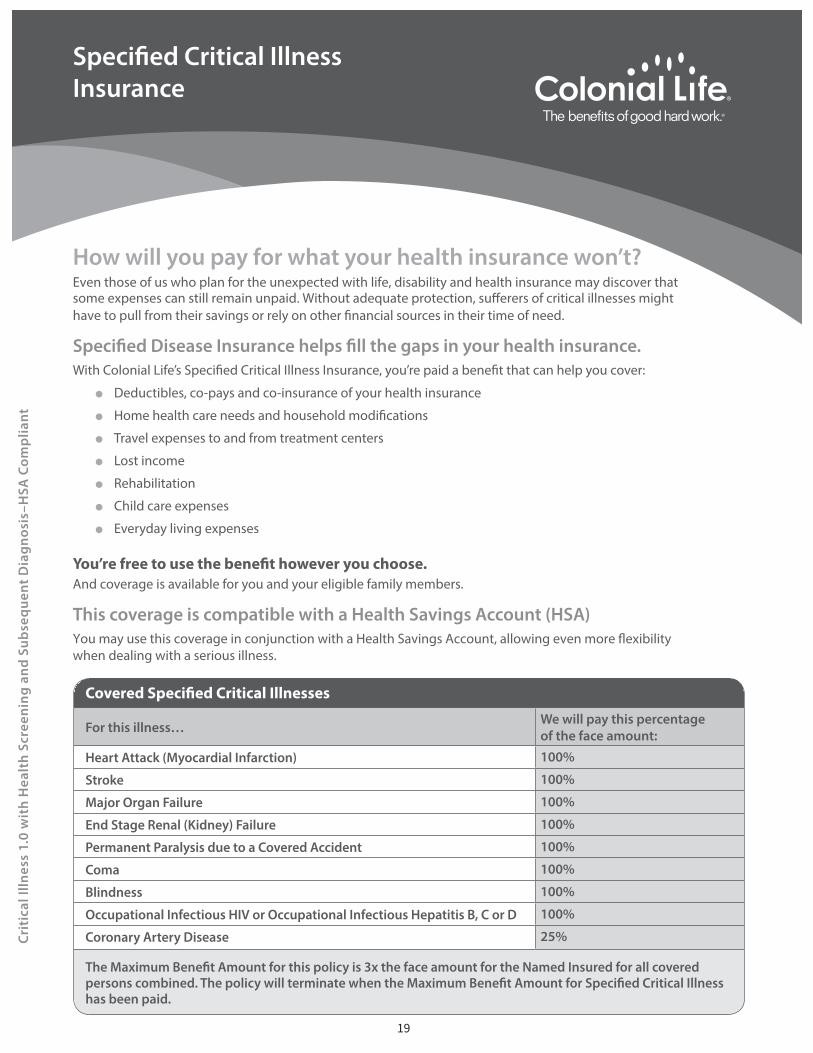
How will you pay for what your health insurance won’t?Even those of us who plan for the unexpected with life, disability and health insurance may discover that some expenses can still remain unpaid. Without adequate protection, su�erers of critical illnesses might have to pull from their savings or rely on other �nancial sources in their time of need.
● Deductibles, co-pays and co-insurance of your health insurance
●
● Travel expenses to and from treatment centers
● Lost income
● Rehabilitation
● Child care expenses
● Everyday living expenses
And coverage is available for you and your eligible family members.
This coverage is compatible with a Health Savings Account (HSA)You may use this coverage in conjunction with a Health Savings Account, allowing even more �exibility when dealing with a serious illness.
For this illness… We will pay this percentageof the face amount:
Heart Attack (Myocardial Infarction) 100%
Stroke 100%
Major Organ Failure 100%
End Stage Renal (Kidney) Failure 100%
Permanent Paralysis due to a Covered Accident 100%
Coma 100%
Blindness 100%
Occupational Infectious HIV or Occupational Infectious Hepatitis B, C or D 100%
Coronary Artery Disease 25%
has been paid.
Crit
ical
Illn
ess
1.0
wit
h H
ealt
h Sc
reen
ing
and
Sub
sequ
ent
Dia
gnos
is–H
SA C
omp
liant

20
Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
71761-1
Colonial Life 1200 Colonial Life BoulevardColumbia, South Carolina 29210coloniallife.com
6/11
©2011 Colonial Life & Accident Insurance Company.Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
Colonial Life and Making benefits count are registered service marks of Colonial Life & Accident Insurance Company.
You can use this coverage more than onceSubsequent Diagnosis… of a different Specified Critical Illness If you receive a benefit for a Specified Critical Illness, and later you are diagnosed with a different
Specified Critical Illness, we will pay the percentage of the original face amount.
Subsequent Diagnosis… of the same Specified Critical Illness
If you receive a benefit for a Specified Critical Illness, and later you are diagnosed with the same Specified Critical Illness (except those listed below), we will pay 25% of the original face amount. (Critical illnesses that do not qualify are: Coronary Artery Disease and Occupational Infectious HIV or Occupational Infectious Hepatitis B, C or D.)
Dates of Diagnoses of Specified Critical Illnesses must be separated by at least 180 days.
Health Screening BenefitNew technology can help improve your chances of surviving a serious illness through early detection and treatment. We will pay this benefit if any covered person incurs a charge for and has any of the following screening tests performed while your policy is in force.
l Stress test on a bicycle or treadmilll Serum cholesterol test to determine levels of HDL and LDLl Carotid dopplerl Electrocardiogram (ECG/EKG)l Echocardiogram (ECHO)l Chest x-rayl Colonoscopyl Mammographyl Pap smearl PSA (blood test for prostate cancer)
24 tests included – No Lifetime Limit
This policy has exclusions and limitations. Premium will vary based on plan chosen. This is not an insurance contract and only the actual policy provisions will control. For cost and complete details of the coverage, see your Colonial Life benefits counselor. Applicable to policy form CI-1.0 or CI-1.0-PL9 (including state abbreviations where used, such as CI-1.0-TX).
71763-2
Crit
ical
Illn
ess
1.0
wit
h H
ealt
h Sc
reen
ing
and
Sub
sequ
ent
Dia
gnos
is–H
SA C
omp
liant

21
Critical Illness Rates
Critical Illness 1.0 HSA Compliant PlanCritical Illness with Subsequent Diagnosis + Health Screening Monthly Premiums
Non-Tobacco
NamedInsured
Named Insured& Spouse
Named Insured& Dependent Children
Named Insured, Spouse & Dependent Children
17-24 $0.25 $0.38 $0.25 $0.3825-29 $0.34 $0.52 $0.34 $0.5230-34 $0.45 $0.68 $0.45 $0.6835-39 $0.75 $1.15 $0.75 $1.1540-44 $0.92 $1.42 $0.92 $1.4245-49 $1.28 $1.97 $1.28 $1.9750-54 $1.77 $2.72 $1.77 $2.7255-59 $2.25 $3.46 $2.25 $3.4660-64 $2.93 $4.50 $2.93 $4.5065-70 $3.34 $5.13 $3.34 $5.13Rates illustrated per unit. 1 unit=$1,000
Tobacco
NamedInsured
Named Insured& Spouse
Named Insured &Dependent Children
Named Insured, Spouse & Dependent Children
17-24 $0.35 $0.55 $0.35 $0.5525-29 $0.51 $0.78 $0.51 $0.7830-34 $0.73 $1.12 $0.73 $1.1235-39 $1.15 $1.77 $1.15 $1.7740-44 $1.55 $2.38 $1.55 $2.3845-49 $2.08 $3.20 $2.08 $3.2050-54 $2.76 $4.24 $2.76 $4.2455-59 $3.61 $5.54 $3.61 $5.5460-64 $4.49 $6.90 $4.49 $6.9065-70 $5.15 $7.91 $5.15 $7.91Rates illustrated per unit. 1 unit=$1,000
Health Screening Benefit
NamedInsured
Named Insured& Spouse
Named Insured &Dependent Children
Named Insured, Spouse & Dependent Children
$2.15 $3.30 $2.15 $3.30To calculate the monthly premium: Multiply the unit premium amount by the number of units of critical illness coverage purchased; then add the flat amount per policy for the health screening benefit.

22
Critical Illness Rates
Critical Illness 1.0 HSA Compliant PlanCritical Illness with Subsequent Diagnosis + Health Screening + Cancer Monthly
Premiums Non-Tobacco
NamedInsured
Named Insured& Spouse
Named Insured &Dependent Children
Named Insured, Spouse & Dependent Children
17-24 $0.43 $0.65 $0.60 $0.8325-29 $0.65 $0.99 $0.82 $1.1730-34 $0.89 $1.37 $1.06 $1.5435-39 $1.26 $1.94 $1.44 $2.1140-44 $1.56 $2.40 $1.74 $2.5845-49 $2.13 $3.27 $2.30 $3.4550-54 $3.08 $4.72 $3.25 $4.9055-59 $3.87 $5.94 $4.04 $6.1260-64 $5.23 $8.04 $5.41 $8.2265-70 $5.83 $8.95 $6.00 $9.13Rates illustrated per unit. 1 unit=$1,000
Tobacco
NamedInsured
Named Insured& Spouse
Named Insured &Dependent Children
Named Insured, Spouse & Dependent Children
17-24 $0.61 $0.93 $0.78 $1.1125-29 $0.97 $1.49 $1.15 $1.6730-34 $1.44 $2.22 $1.62 $2.3935-39 $2.03 $3.12 $2.21 $3.3040-44 $2.60 $4.00 $2.78 $4.1845-49 $3.43 $5.27 $3.60 $5.4450-54 $4.80 $7.37 $4.97 $7.5555-59 $6.20 $9.52 $6.37 $9.7060-64 $8.04 $12.35 $8.21 $12.5365-70 $9.01 $13.84 $9.18 $14.01Rates illustrated per unit. 1 unit=$1,000
Health Screening Benefit
NamedInsured
Named Insured& Spouse
Named Insured &Dependent Children
Named Insured, Spouse & Dependent Children
$2.15 $3.30 $2.15 $3.30To calculate the monthly premium: Multiply the unit premium amount by the number of units of critical illness coverage purchased; then add the flat amount per policy for the health screening benefit.

23
Cancer Insurance
CANCER ASSIST
How would cancer impact your way of life?Hopefully, you and your family will never face cancer. If you do, a financial safety net can help you and your loved ones focus on what matters most — recovery.
If you were diagnosed with cancer, you could have expenses that medical insurance doesn’t cover. In addition to your regular, ongoing bills, you could have indirect treatment and recovery costs, such as child care and home health care services.
Help when you need it mostCancer coverage from Colonial Life & Accident Insurance Company can help protect the lifestyle you’ve worked so hard to build. It provides benefits you can use to help cover:
■ Loss of income
■ Out-of-network treatment
■ Lodging and meals
■ Deductibles and co-pays

24
Paul and Kim were preparing for their second child when they learned Paul had cancer. They quickly realized their medical insurance wouldn’t cover everything. Thankfully, Kim’s job enabled her to have a Colonial Life Cancer Insurance policy on Paul to help them with expenses.
Paul’s wellness benefit helped pay for the screening that discovered his cancer.
When the couple traveled several hundred miles from their home to a top cancer hospital, they used the policy’s lodging and transportation benefits to help with expenses.
The policy’s benefits helped with deductibles and co-pays related to Paul’s surgery and hospital stay.
SURGERY SECOND OPINION DOCTOR’S SCREENING
Wellness Benefit Travel Expenses Out-of-pocket Costs
One Family’s Journey
With Colonial Life’s Cancer Insurance:■ Coverage options are available for you and
your eligible dependents.
■ Benefits are paid directly to you, unless you specify otherwise.
■ You’re paid regardless of any other insurance you may have with other companies.
■ You can take coverage with you, even if you change jobs or retire.
Cancer Facts & Figures, American Cancer Society, 2013
For illustrative purposes only.
ONLY of ALLCANCERS are hereditary.

25
Paul has been cancer-free for more than four years. His Colonial Life cancer policy provides a benefit for periodic scans to help ensure the cancer stays in check.
Paul used his plan’s benefits to help pay for experimental treatments not covered by his medical insurance.
TREATMENT RECOVERY
Experimental Care Follow-up Evaluations
Colonial Life’s Cancer Insurance offers more than 30 benefits that can help you with costs that may not be covered by your medical insurance.
Treatment Benefits (Inpatient or Outpatient)
■ Radiation/Chemotherapy
■ Anti-nausea Medication
■ Medical Imaging Studies
■ Supportive or Protective Care Drugs and Colony Stimulating Factors
■ Second Medical Opinion
■ Blood/Plasma/Platelets/ Immunoglobulins
■ Bone Marrow or Peripheral Stem Cell Donation
■ Bone Marrow or Peripheral Stem Cell Transplant
■ Egg(s) Extraction or Harvesting/ Sperm Collection and Storage
■ Experimental Treatment
■ Hair/External Breast/Voice Box Prosthesis
■ Home Health Care Services
■ Hospice (Initial or Daily Care)
Surgery Benefits■ Surgical Procedures
■ Anesthesia
■ Reconstructive Surgery
■ Outpatient Surgical Center
■ Prosthetic Device/Artificial Limb
Travel Benefits■ Transportation
■ Companion Transportation
■ Lodging
Inpatient Benefits■ Hospital Confinement
■ Private Full-Time Nursing Services
■ Skilled Nursing Care Facility
■ Ambulance
■ Air Ambulance
Additional Benefits■ Family Care
■ Cancer Vaccine
■ Bone Marrow Donor Screening
■ Skin Cancer Initial Diagnosis
■ Waiver of PremiumCancer Facts & Figures, American Cancer Society, 2013
LIFETIME RISK OF DEVELOPING CANCER
MEN1 in 2
WOMEN1 in 3
Colonial Life’s Cancer Insurance provides benefits to help with cancer expenses — from diagnosis to recovery.

26
ColonialLife.com
WAITING PERIODThe policy and its riders may have a waiting period. Waiting period means the first 30 days following the policy’s coverage effective date during which no benefits are payable. If your cancer has a date of diagnosis before the end of the waiting period, coverage for that cancer will apply only to losses commencing after the policy has been in force for two years, unless it is excluded by name or specific description in the policy.
EXCLUSIONSWe will not pay benefits for cancer or skin cancer:
■ If the diagnosis or treatment of cancer is received outside of the territorial limits of the United States and its possessions; or
■ For other conditions or diseases, except losses due directly from cancer.
The policy and its riders may have additional exclusions and limitations. For cost and complete details of the coverage, see your Colonial Life benefits counselor. Coverage may vary by state and may not be available in all states. Applicable to policy form CanAssist and rider forms R-CanAssistIndx, R-CanAssistProg and R-CanAssistSpDis (including state abbreviations where applicable – for example: CanAssist-TX).
101481
Optional RidersFor an additional cost, you may have the option of purchasing additional riders for even more financial protection against cancer. Talk with your benefits counselor to find out which of these riders are available for you to purchase.
■ Initial Diagnosis of Cancer Rider — Pays a one-time, lump-sum benefit for the initial diagnosis of cancer. You may choose a benefit amount in $1,000 increments between $1,000 and $10,000. If your dependent child is diagnosed with cancer, we will pay two and a half times ($2,500 - $25,000) the chosen benefit amount.
■ Initial Diagnosis of Cancer Progressive Payment Rider — Provides a lump-sum payment of $50 for each month the rider has been in force after the waiting period and before cancer is first diagnosed.
■ Specified Disease Hospital Confinement Rider — Pays $300 per day if you or a covered family member is confined to a hospital for treatment for one of the 34 specified diseases covered under the rider.
If cancer impacts your life, you should be able to focus on getting better — not on how you’ll pay your bills. Talk with your Colonial Life benefits counselor about how cancer insurance can help provide financial security for you and your family.
©2014 Colonial Life & Accident Insurance CompanyColonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
1-14

27
Air Ambulance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $2,000 per tripTransportation to or from a hospital or medical facility [max. of two trips per confinement]
Ambulance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $250 per tripTransportation to or from a hospital or medical facility [max. of two trips per confinement]
AnesthesiaAdministered during a surgical procedure for cancer treatment
■ General Anesthesia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25% of Surgical Procedures Benefit■ Local Anesthesia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $30 per procedure
Anti-nausea Medication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $40 per day administered orDoctor-prescribed medication for radiation or chemotherapy [$160 monthly max.] per prescription filled
Blood/Plasma/Platelets/Immunoglobulins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $150 per dayA transfusion required during cancer treatment [$10,000 calendar year max.]
Bone Marrow Donor Screening . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50Testing in connection with being a potential donor [once per lifetime]
Bone Marrow or Peripheral Stem Cell Donation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $500Receiving another person’s bone marrow or stem cells for a transplant [once per lifetime]
Bone Marrow or Peripheral Stem Cell Transplant . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $4,000 per transplantTransplant you receive in connection with cancer treatment [max. of two bone marrow transplant benefits per lifetime]
Cancer Vaccine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50An FDA-approved vaccine for the prevention of cancer [once per lifetime]
Companion Transportation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $0.50 per mileCompanion travels by plane, train or bus to accompany a covered cancer patient more than 50 miles one way for treatment [up to $1,000 per round trip]
Egg(s) Extraction or Harvesting/Sperm Collection and StorageExtracted/harvested or collected before chemotherapy or radiation [once per lifetime]
■ Egg(s) Extraction or Harvesting/Sperm Collection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $700■ Egg(s) or Sperm Storage (Cryopreservation) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200
Experimental Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $250 per dayHospital, medical or surgical care for cancer [$12,500 lifetime max.]
Family Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $40 per dayInpatient or outpatient treatment for a covered dependent child [$2,000 calendar year max.]
Hair/External Breast/Voice Box Prosthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200 per calendar yearProsthesis needed as a direct result of cancer
Home Health Care Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $75 per dayExamples include physical therapy, occupational therapy, speech therapy and audiology; prosthesis and orthopedic appliances; rental or purchase of durable medical equipment [up to 30 days per calendar year or twice the number of days hospital confined, whichever is greater]
Hospice (Initial or Daily Care) An initial, one-time benefit and a daily benefit for treatment [$15,000 lifetime max. for both]
■ Initial hospice care [once per lifetime] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $1,000■ Daily hospice care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50 per day
BENEFIT DESCRIPTION BENEFIT AMOUNT
Cancer InsuranceLevel 2 Benefits
Our cancer insurance helps provide financial protection through a variety of benefits. These benefits are not only for you but also for your covered family members.
For more information, talk with your
benefits counselor.
CANCER ASSIST LEVEL 2 – KS

28
The policy has limitations and exclusions that may affect benefits payable. Most benefits require that a charge be incurred. Policy may not be available in all states and may vary by state. For cost and complete details, see your benefits counselor.
This chart highlights the benefits of policy form CanAssist-KS. This chart is not complete without form #101481 (including state abbreviations where used – for example: 101481-NC).
Hospital ConfinementHospital stay (including intensive care) required for cancer treatment
■ 30 days or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $150 per day■ 31 days or more . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $300 per day
Injected Chemotherapy Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $350Administration by medical personnel once per calendar week
Lodging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50 per dayHotel/motel expenses when being treated for cancer more than 50 miles from home [70-day calendar year max.]
Medical Imaging Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $125 per studySpecific studies for cancer treatment [$250 calendar year max.]
Outpatient Surgical Center . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200 per daySurgery at an outpatient center for cancer treatment [$600 calendar year max.]
Private Full-time Nursing Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $75 per dayServices while hospital confined other than those regularly furnished by the hospital
Prosthetic Device/Artificial Limb . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $1,500 per device or limbA surgical implant needed because of cancer surgery [payable one per site, $3,000 lifetime max.]
Radiation/ChemotherapyWeekly Benefit [max. once per week]
■ Radiation delivered by medical personnel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $500Monthly Chemotherapy Benefit [max. once per month]
■ Injected by medical personnel [1-24 months] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200■ Injected by medical personnel [25+ months] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $100■ Self-Injected . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200■ Pump . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200■ Topical . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200■ Oral Hormonal [1-24 months] . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200■ Oral Hormonal [25+ months]. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $100■ Oral Non-Hormonal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200
Reconstructive Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $40 per surgical unitA surgery to reconstruct anatomic defects that result from cancer treatment[up to $2,500 per procedure, including 25% for general anesthesia]
Second Medical Opinion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $200A second physician’s opinion on cancer surgery or treatment [once per lifetime]
Skilled Nursing Care Facility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $100 per dayConfinement to a covered facility after hospital release [up to the number of days paid for hospital confinement]
Skin Cancer Initial Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $300A skin cancer diagnosis while the policy is in force [once per lifetime]
Supportive or Protective Care Drugs and Colony Stimulating Factors . . . . . . . . . . . . . . . . . . . . . . $100 per dayDoctor-prescribed drugs to enhance or modify radiation/chemotherapy treatments [$800 calendar year max.]
Surgical Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50 per surgical unitInpatient or outpatient surgery for cancer treatment [$3,000 max. per procedure]
Transportation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $0.50 per mileTravel expenses when being treated for cancer more than 50 miles from home [up to $1,000 per round trip]
Waiver of Premium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Is availableNo premiums due if the named insured is disabled longer than 90 consecutive days
BENEFIT DESCRIPTION BENEFIT AMOUNT
©2014 Colonial Life & Accident Insurance CompanyColonial Life products are underwritten by
Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
3-14
ColonialLife.com
101483-KS

29
For more information, talk with your
benefits counselor.
To encourage early detection,our cancer insurance offers benefits for wellness and health screening tests.
Part One: Cancer Wellness/ Health Screening Provided when one of the tests listed below is performed after the waiting period and while the policy is in force. Payable once per calendar year, per covered person.
Waiting period means the first 30 days following the policy’s coverage effective date during which no benefits are payable.
The policy has exclusions and limitations. For cost and complete details of the coverage, see your Colonial Life benefits counselor. Coverage may vary by state and may not be available in all states. Applicable to policy form CanAssist (and state abbreviations where applicable – for example: CanAssist-TX).
Cancer Wellness Tests■ Bone marrow testing■ Breast ultrasound■ CA 15-3 [blood test for breast cancer]■ CA 125 [blood test for ovarian cancer]■ CEA [blood test for colon cancer]■ Chest X-ray■ Colonoscopy■ Flexible sigmoidoscopy■ Hemoccult stool analysis■ Mammography■ Pap smear■ PSA [blood test for prostate cancer]■ Serum protein electrophoresis
[blood test for myeloma]■ Skin biopsy■ Thermography■ ThinPrep pap test■ Virtual colonoscopy
Part Two: Cancer Wellness — Additional Invasive Diagnostic Test or Surgical ProcedureProvided when a doctor performs a diagnostic test or surgical procedure after the waiting period as the result of an abnormal result from one of the covered cancer wellness tests in Part One. We will pay the benefit regardless of the test results. Payable once per calendar year, per covered person.
Health Screening Tests■ Blood test for triglycerides■ Carotid Doppler■ Echocardiogram [ECHO]■ Electrocardiogram [EKG, ECG]■ Fasting blood glucose test■ Serum cholesterol test for HDL
and LDL levels■ Stress test on a bicycle or treadmill
101486
Cancer InsuranceWellness Benefits
©2014 Colonial Life & Accident Insurance CompanyColonial Life products are underwritten by
Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
1-14

30
Cancer InsuranceSpecified Disease Hospital Confinement Rider
CANCER ASSIST SPECIFIED DISEASE RIDER | 7-14 | 101547
Rider BenefitsWe will pay this benefit if after the waiting period* you incur charges for and are confined to a hospital for treatment of one of the specified diseases listed above.
Rider Features � Guaranteed renewable as long as your cancer insurance policy is in force. � Covers the same family members as your cancer insurance policy. � Pays benefits regardless of any other insurance you have with other insurance companies.
� Pays benefits directly to you, unless you specify otherwise.
* Waiting Period means the first 30 days following each insured person’s coverage effective date during which time no benefits are payable.
This rider has exclusions and limitations. For cost and complete details of the coverage, see your Colonial Life benefits counselor. Coverage may vary by state and may not be available in all states. Applicable to rider form R-CanAssistSpDis (including state abbreviations where used, for example: R-CanAssistSpDis-TX).
For more information, talk with your Colonial Life
benefits counselor.
©2014 Colonial Life & Accident Insurance Company, Columbia, SC | Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
� Adrenal Hypofunction (Addison’s Disease)
� Botulism � Bubonic Plague � Cerebral Palsy � Cholera � Cystic Fibrosis � Diphtheria � Encephalitis (including
Encephalitis contracted from West Nile Virus)
� Huntington’s Chorea � Legionnaires’ Disease � Lou Gehrig’s Disease
(Amyotrophic Lateral Sclerosis)
� Lyme Disease � Malaria � Meningitis (bacterial)
� Multiple Sclerosis � Muscular Dystrophy � Myasthenia Gravis
� Necrotizing Fasciitis � Osteomyelitis � Poliomyelitis � Rabies � Reye’s Syndrome � Scleroderma � Scarlet Fever � Sickle Cell Anemia � Systemic Lupus � Tetanus
Specified Diseases � Toxic Epidermal Necrolysis � Toxic Shock Syndrome � Tuberculosis (Mycobacterial)
� Tularemia � Typhoid Fever � Variant Creutzfeldt-Jakob
Disease (Mad Cow Disease)
� Yellow Fever
In addition to cancer, there are many other diseases that could lead to a costly hospital stay. Fortunately, there’s a way to help protect your family’s financial future.
At an additional cost, Colonial Life & Accident Insurance Company offers an optional specified disease rider for your cancer insurance. This rider adds valuable coverage for a variety of specified diseases.

31
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Cancer Rates
Individual Cancer Rates
LEVEL 2 – Monthly Premiums - Composite Rates
Employee Employee/Spouse
One-ParentFamily
Two-ParentFamily
Level 2 WITHOUT Cancer Wellness/Health Screening
Premium $15.00 $23.50 $15.30 $23.80
Level 2 with $25 Cancer Wellness/Health Screening
Premium $16.45 $25.75 $16.75 $26.05
Level 2 with $50 Cancer Wellness/Health Screening
Premium $17.90 $28.00 $18.20 $28.30
Level 2 with $75 Cancer Wellness/Health Screening
Premium $19.75 $30.90 $20.05 $31.20
Level 2 with $100 Cancer Wellness/Health Screening
Premium $21.65 $33.85 $21.95 $34.15
OPTIONAL RIDERS
Employee Employee/Spouse
One-ParentFamily
Two-ParentFamily
Specified Disease Hospital Confinement Rider
Premium $1.25 $1.75 $1.25 $1.75
Initial Diagnosis of Cancer Rider (per $1,000)
Premium $1.50 $2.50 $1.60 $2.60
Initial Diagnosis of Cancer Progressive Payment Rider
Premium $7.80 $17.05 $7.80 $17.05
Individual Cancer Rates
LEVEL 2 – Monthly Premiums - Composite Rates
Employee Employee/Spouse
One-ParentFamily
Two-ParentFamily
Level 2 WITHOUT Cancer Wellness/Health Screening
Premium $15.00 $23.50 $15.30 $23.80
Level 2 with $25 Cancer Wellness/Health Screening
Premium $16.45 $25.75 $16.75 $26.05
Level 2 with $50 Cancer Wellness/Health Screening
Premium $17.90 $28.00 $18.20 $28.30
Level 2 with $75 Cancer Wellness/Health Screening
Premium $19.75 $30.90 $20.05 $31.20
Level 2 with $100 Cancer Wellness/Health Screening
Premium $21.65 $33.85 $21.95 $34.15
OPTIONAL RIDERS
Employee Employee/Spouse
One-ParentFamily
Two-ParentFamily
Specified Disease Hospital Confinement Rider
Premium $1.25 $1.75 $1.25 $1.75
Initial Diagnosis of Cancer Rider (per $1,000)
Premium $1.50 $2.50 $1.60 $2.60
Initial Diagnosis of Cancer Progressive Payment Rider
Premium $7.80 $17.05 $7.80 $17.05
Individual Cancer Rates
LEVEL 2 – Monthly Premiums - Composite Rates
Employee Employee/Spouse
One-ParentFamily
Two-ParentFamily
Level 2 WITHOUT Cancer Wellness/Health Screening
Premium $15.00 $23.50 $15.30 $23.80
Level 2 with $25 Cancer Wellness/Health Screening
Premium $16.45 $25.75 $16.75 $26.05
Level 2 with $50 Cancer Wellness/Health Screening
Premium $17.90 $28.00 $18.20 $28.30
Level 2 with $75 Cancer Wellness/Health Screening
Premium $19.75 $30.90 $20.05 $31.20
Level 2 with $100 Cancer Wellness/Health Screening
Premium $21.65 $33.85 $21.95 $34.15
OPTIONAL RIDERS
Employee Employee/Spouse
One-ParentFamily
Two-ParentFamily
Specified Disease Hospital Confinement Rider
Premium $1.25 $1.75 $1.25 $1.75
Initial Diagnosis of Cancer Rider (per $1,000)
Premium $1.50 $2.50 $1.60 $2.60
Initial Diagnosis of Cancer Progressive Payment Rider
Premium $7.80 $17.05 $7.80 $17.05

32
My Coverage Worksheet
Who’s being covered? You only You and your spouse You and your dependent children You, your spouse and your dependent children
● Waiver of Premium
T
● $____________per c● Rehabilitation Unit $100 per day
Simply call our Policyholder Service Center at 1.800.325.4368 or visit coloniallife.com for additional information.
Indemnity Insurance
Med
ical
Bri
dge S
M 3
000
Pla
n 1-
KS
How will you cover all of your medical expenses?Larger deductibles. Higher co-payments. You may be left with more out-of-pocket costs.
out-of-pocket expenses related to a covered accident or covered sickness.

33
When is the Hospital Confinement benefit paid? The Hospital Confinement benefit is paid when any covered person is confined in a hospital or in an observation unit for at least 20 continuous hours.
When is the Rehabilitation Unit benefit paid? The Rehabilitation Unit benefit is paid when any covered person is transferred to a rehabilitation unit immediately after a period of hospital confinement. There is a maximum of 15 days per covered confinement with no more than 30 days per calendar year.
What is the Waiver of Premium benefit? The Waiver of Premium benefit waives premium when the named insured is confined to a hospital for more than 30 continuous days.
Here are some frequently asked questions about Colonial Life’s
hospital confinement indemnity insurance:
What if I change employers?Benefits are portable. If you change jobs or retire, you can take your coverage with you at no increase in premium.
How are my benefits paid?Benefits are paid directly to you, unless you specify otherwise. Benefits are paid regardless of any other coverage you may have with other insurance companies.
100111-1
EXCLUSIONS
We will not pay benefits for injuries received in accidents or sicknesses which are caused by: dental procedures; elective procedures and cosmetic surgery; illegal activities; pregnancy of a dependent child; suicide or injuries which any covered person intentionally does to himself; war; pre-existing conditions as defined in the policy. We will not pay benefits for hospital confinement of a newborn child following his birth unless he is injured or sick. Pre-existing Condition means having a sickness or physical condition for which any covered person was treated, had medical testing, received medical advice or had taken medication within 12 months before the effective date of this policy.
For cost and complete details, see your Colonial Life benefits counselor. Applicable to policy number MB3000-KS. This is not an insurance contract and only the actual policy provisions will control.
6/11
Med
ical
Bri
dge S
M 3
000
Pla
n 1-
KS
Colonial Life 1200 Colonial Life BoulevardColumbia, South Carolina 29210coloniallife.com
©2011 Colonial Life & Accident Insurance Company.Colonial Life products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
Colonial Life and Making benefits count are registered service marks of Colonial Life & Accident Insurance Company.

34
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Hospital Confinement Indemnity Rates
Medical BridgeSM 3000 Benefits - Plan 1
Base Plan: Hospital Confinement and Rehabilitation Unit
Hospital Confinement XRehabilitation Unit XWaiver of Premium X
This plan is a Health Savings Account (HSA)-compliant plan. This plan may also be offered to employees who do not have an HSA.
Hospital Confinement Benefit Level 1: $500 Level 2: $1,000 Level 3: $1,500
Rehabilitation Unit Benefit*: $100 per day up to 15 days per confinement as an inpatient in a rehabilitation unit. 30-day maximum per covered person per calendar year. Must occur immediately after the hospital confinement.
Waiver of Premium Benefit: after 30 continuous days of the employee’s hospital confinement. Waives premium for the entire policy.
*The pre-existing condition limitation is applicable to these benefits.

35
Medical BridgeSM 3000Plan 1 Benefit Amount Options & Monthly Premiums
Hospital Confinement
AA $500 AB $1,000 AC **$1,500*Requires prior underwriting approval for all accounts, based on Major Medical deductible information.** Requires prior underwriting approval for Health Care, Governmental, and Educator groups based on Major Medical deductible information.
Medical BridgeSM 3000Base Plan: Hospital Confinement and Rehabilitation Unit
Employee
AA AB AC17-49 $5.90 $11.30 $16.70 50-59 $8.20 $15.70 $23.20 60-64 $10.65 $20.40 $30.15 65-74 $13.35 $25.60 $37.85
Employee & SpouseAA AB AC
17-49 $12.65 $24.30 $35.95 50-59 $17.50 $33.60 $49.70 60-64 $23.20 $44.60 $66.00 65-74 $29.05 $55.80 $82.55
Employee & Dependent ChildrenAA AB AC
17-49 $10.10 $19.40 $28.70 50-59 $12.20 $23.40 $34.60 60-64 $15.00 $28.80 $42.60 65-74 $18.75 $36.00 $53.25
Employee, Spouse & Dependent ChildrenAA AB AC
17-49 $15.40 $29.50 $43.60 50-59 $19.85 $38.10 $56.35 60-64 $25.25 $48.40 $71.55 65-74 $31.70 $60.70 $89.70
Applicable to KSThis information is intended for porposal use with employers.Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.Coverage is subject to policy exclusions and limitations that may affect benefits payable. Products may vary by state and may not be available in all states. For cost and complete details, see a Colonial Life benefits counselor.
Hospital Confinement Indemnity Rates

36
How to file a wellness claim � The quickest way to receive the applicable benefits for
your health screening services is to file a wellness claim via our secure My Colonial Life for Policyholders section of ColonialLife.com. By filing through the website, you can receive your benefit in a matter of days.
� For wellness screenings within 12 months of the date you are filing the claim, go to ColonialLife.com, log in to the My Colonial Life policyholder section, and click on File a Wellness Claim Online. Or you may use the automated customer service center at 1-800-325-4368.
� For wellness screenings over 12 months from the date you are filing the claim, you’ll be directed to print out a paper claim form and complete it manually. Fill it out, and submit the claim as the form instructs. Be sure to review and sign all pages where indicated.
How to file disability claims � Where indicated on the form, be sure to:
– Have the doctor verify the dates of disability and furnish dates of treatment.
– Have the employer confirm the dates missed from work.
� Read and sign the claims authorization page. We cannot obtain additional information from your doctor without proper consent.
� Submit your claim:
– Fax the completed form to 1-800-880-9325. Include your name and Social Security number on each page of your fax as indicated. If you fax the claim, you do not need to mail the original document to us; keep it for your records.
OR
– Mail the completed forms to Colonial Life (see the Contact us section of this document).
Service guide for policyholders
The quickest, easiest way to manage your business with us is through the My Colonial Life policyholder section of ColonialLife.com. Join now for convenient access to your policy and claims information.
If you’re not already signed up:
� Visit ColonialLife.com, and click Login on the home page.
� Click Request access to our policyholder or plan administrator website, and you’ll be directed to a sign-up page.
n File a wellness claim.
n Check on the status of your claim.
n Check your policy information.
n Download claim and service forms.
n Update your contact information.
As a My Colonial Life member, you can:

37
How to file other claims � On the Claims page of the My Colonial Life site, click on File All
Other Types of Claims, and choose the form you need for your specific claim.
� Complete the form that applies to your specific claim. Be sure the information includes a diagnosis from your doctor, along with copies of any appropriate medical bills, if required. Make sure you sign and date the certification and the authorization portion of the claim form.
Optional servicesThe first page of Colonial Life’s claim forms explains optional services that you can request by initialing the blanks provided.
The options include authorizing Colonial Life to:
� Release information to your benefits representative, plan administrator or family member.
� Communicate claims information via electronic messaging to your home phone number.
Processing your claim � When we receive information regarding your claim, you will be
notified by telephone or email.
� If you select the electronic messaging option, you will receive a call when the claim is processed.
� We will notify you by letter if we need any additional information from your doctor or any other source(s). We welcome your assistance in encouraging your doctor to provide the needed information as quickly as possible.
� If your claim is for a sickness or health condition, we may need to contact your doctor or request copies of medical records to confirm information, which may lengthen the claim processing time.
� Our goal is to provide prompt and accurate claims service. Remember, you can always check the status of your claim via the My Colonial Life site.
Ongoing claimsTotal disability benefits provided by your coverage are based on disability information submitted on your claim form.
Because Colonial Life cannot pay benefits for time you have not yet missed from work, you may be asked to provide verification of your ongoing disability and the dates you are unable to work. Your doctor and employer must confirm all disability dates. Please include medical treatment dates on your claim form. ©2014 Colonial Life & Accident Insurance Company
Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
5-14 | 43233-36
Contact usOnline
Log in to the My Colonial Life website to contact us by email.
Telephone 1-800-325-4368
Contact Center representatives are available Monday through Friday, 8 a.m. – 8 p.m. EST.
Automated service information is available every day throughout the year.
Please have your Social Security or policy number ready when you call.
Hearing-impaired customers Customers with a Telecommunications
Device for the Deaf (TDD) should call 803-798-4040.
Mailing addressColonial Life Contact Center
P.O. Box 100195, Columbia, SC 29202-3195
ColonialLife.com
Important remindersn Be sure to view the claims videos on the
Claims page of the My Colonial Life site, for quick tips on how to complete your claim form quickly, easily and correctly.
n Be sure to complete all sections of the claim form. Incomplete information may cause a delay in the resolution of your claim.
n When you mail the claim form or other information, please keep a copy of your information for your records.
n If you want us to send any applicable claim benefits by overnight delivery and deduct the fee from your claim payment, initial the overnight line in the “Optional Service” section of the claim form.

38
Request foR seRvice: What type of service are you requesting? Please check only the boxes that apply.
1 General InformatIonInsured’s name as currently listed on the policy: Social Security Number (SSN): Date of Birth(mm/dd/yyyy):
List all policy numbers related to this request (required to process):
Employer Name:
2 name ChanGe Please attach a copy of legal evidence.
Previous Name: Current Name: Reason: Correction Marriage/Divorce Other
3 address ChanGeAddress: Apt. #: City: State: ZIP:
Telephone: ( ) Mobile: ( ) Email:
4 request for ChanGe of BenefICIary form
Please visit us at our website, coloniallife.com, or contact us at 1.800.325.4368 to request a copy of the Change of Beneficiary form.
5 PremIum Payment method ChanGe Please select one of three easy payment methods.
1. Please deduct monthly premiums from my banking account.
RANGE: A). 1st-5th B). 6th-10th C). 11th-15th D). 16th-20th E). 21st-26th. Your draft will occur on one of the dates within the range you have selected.
Please attach a voided check, and circle one range of days you would like your checking account to be drafted. Signature of checking account owner:
_________________________________________
oR
2. Please bill me directly.
Choose one of the following: Quarterly (Submit a payment
3 times your monthly premium.) Semi-annually (Submit a payment
6 times your monthly premium.) Annually (Submit a payment
12 times your monthly premium.)
oR
3. Change to Payroll Deductions.
Employer Name:
_______________________________
Billing Control Number or Account Number:
_______________________________Please contact your Plan Administrator to start payroll deduction.
6 CanCellatIon, surrender or PolICy ChanGe You must also complete sections 9 and 12 on the reverse side.
Cancel/surrender the policy/policies (This option will cancel or cash surrender your policy/policies.)
Cancel the following riders on the policy/policies: (This option will cancel policy riders only.)
Spouse Rider Dependent Rider (This will cancel coverage for ALL dependents.) Other (name rider) ______________________________________________
Change Two-Parent to Individual Change Two-Parent to One-Parent Change One-Parent to Individual
Please provide name, birthdate, and social security number for spouse/dependent(s) continuation:
Name: Date of Birth: SSN:
Name: Date of Birth: SSN:
7 PolICy loan You must complete sections 9 and 12 on the reverse side. Select either Section 7 or 8 per policy number, not both.
Please select one option per policy
number.
I am requesting a policy loan for the following amount: $______________________ I am requesting a policy loan for the maximum amount available.
If the amount requested is more than the available cash value, we will process this request for the maximum amount available.
Check this box also if you are requesting information regarding repayment of your loan on your universal life policy.
By signing on the reverse side, I hereby assign the policy to the insurer as collateral.Policy loans are available on select life policies only. Minimum loan amounts may apply as stated in your policy contract. You will receive annual loan and interest notices until the loan is fully repaid. For information regarding repayment of your loan, please contact us at 1.800.325.4368.
2-13 05897-31
Colonial life & accident Insurance Company
Continued on Reverse Side ➡
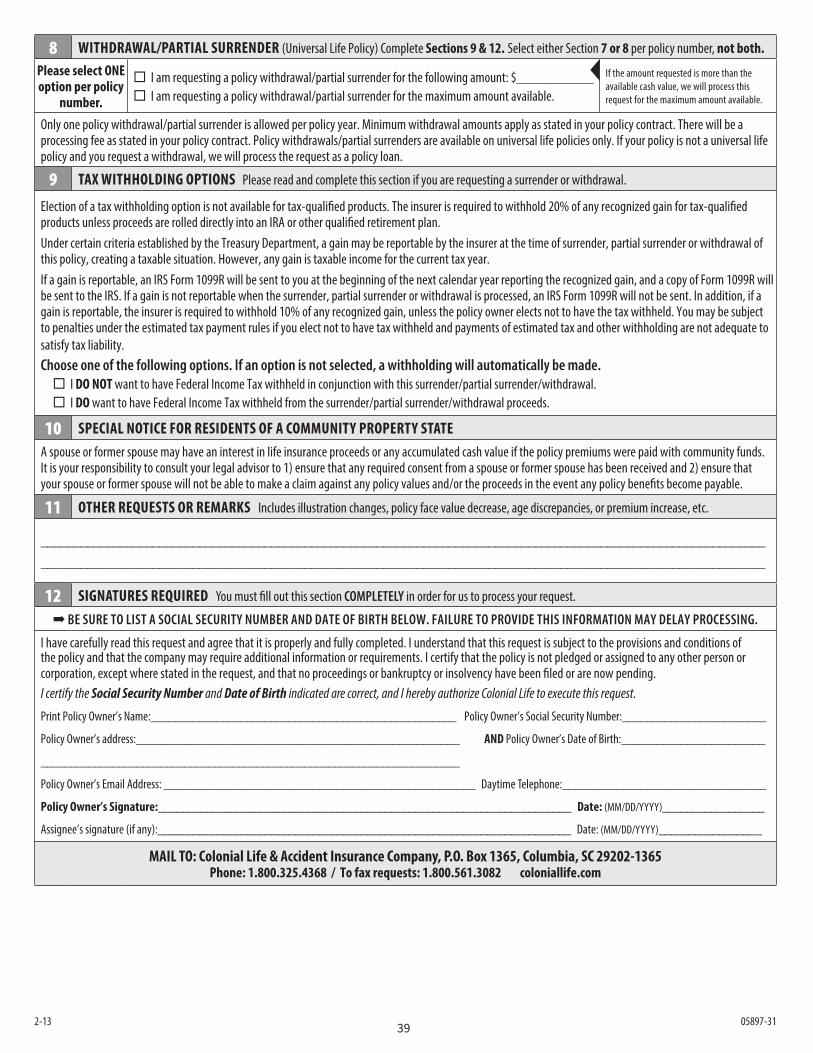
39
8 WIthdraWal/PartIal surrender (Universal Life Policy) Complete sections 9 & 12. Select either Section 7 or 8 per policy number, not both.
Please select one option per policy
number.
I am requesting a policy withdrawal/partial surrender for the following amount: $___________ I am requesting a policy withdrawal/partial surrender for the maximum amount available.
If the amount requested is more than the available cash value, we will process this request for the maximum amount available.
Only one policy withdrawal/partial surrender is allowed per policy year. Minimum withdrawal amounts apply as stated in your policy contract. There will be a processing fee as stated in your policy contract. Policy withdrawals/partial surrenders are available on universal life policies only. If your policy is not a universal life policy and you request a withdrawal, we will process the request as a policy loan.
9 tax WIthholdInG oPtIons Please read and complete this section if you are requesting a surrender or withdrawal.
Election of a tax withholding option is not available for tax-qualified products. The insurer is required to withhold 20% of any recognized gain for tax-qualified products unless proceeds are rolled directly into an IRA or other qualified retirement plan.Under certain criteria established by the Treasury Department, a gain may be reportable by the insurer at the time of surrender, partial surrender or withdrawal of this policy, creating a taxable situation. However, any gain is taxable income for the current tax year.If a gain is reportable, an IRS Form 1099R will be sent to you at the beginning of the next calendar year reporting the recognized gain, and a copy of Form 1099R will be sent to the IRS. If a gain is not reportable when the surrender, partial surrender or withdrawal is processed, an IRS Form 1099R will not be sent. In addition, if a gain is reportable, the insurer is required to withhold 10% of any recognized gain, unless the policy owner elects not to have the tax withheld. You may be subject to penalties under the estimated tax payment rules if you elect not to have tax withheld and payments of estimated tax and other withholding are not adequate to satisfy tax liability.Choose one of the following options. If an option is not selected, a withholding will automatically be made. I do not want to have Federal Income Tax withheld in conjunction with this surrender/partial surrender/withdrawal. I do want to have Federal Income Tax withheld from the surrender/partial surrender/withdrawal proceeds.
10 sPeCIal notICe for resIdents of a CommunIty ProPerty stateA spouse or former spouse may have an interest in life insurance proceeds or any accumulated cash value if the policy premiums were paid with community funds. It is your responsibility to consult your legal advisor to 1) ensure that any required consent from a spouse or former spouse has been received and 2) ensure that your spouse or former spouse will not be able to make a claim against any policy values and/or the proceeds in the event any policy benefits become payable.
11 other requests or remarks Includes illustration changes, policy face value decrease, age discrepancies, or premium increase, etc.
____________________________________________________________________________________________________________________________________________________________________________________________________________________________
12 sIGnatures requIred You must fill out this section COMPLETELY in order for us to process your request.
➡ BE SURE TO LIST A SOCIAL SECURITY NUMBER AND DATE OF BIRTH BELOW. FAILURE TO PROVIDE THIS INFORMATION MAY DELAY PROCESSING.
I have carefully read this request and agree that it is properly and fully completed. I understand that this request is subject to the provisions and conditions of the policy and that the company may require additional information or requirements. I certify that the policy is not pledged or assigned to any other person or corporation, except where stated in the request, and that no proceedings or bankruptcy or insolvency have been filed or are now pending.I certify the Social Security Number and Date of Birth indicated are correct, and I hereby authorize Colonial Life to execute this request.
Print Policy Owner’s Name:___________________________________________________ Policy Owner’s Social Security Number:________________________
Policy Owner’s address:______________________________________________________ and Policy Owner’s Date of Birth:________________________
______________________________________________________________________
Policy Owner’s Email Address: ____________________________________________________ Daytime Telephone:__________________________________
Policy owner’s signature:_____________________________________________________________________ date: (MM/DD/YYYY)_________________
Assignee’s signature (if any):_____________________________________________________________________ Date: (MM/DD/YYYY)_________________
maIl to: Colonial life & accident Insurance Company, P.o. Box 1365, Columbia, sC 29202-1365Phone: 1.800.325.4368 / to fax requests: 1.800.561.3082 coloniallife.com
2-13 05897-31

40
Notes

41
Notes

42
Notes

ColonialLife.com©2014 Colonial Life & Accident Insurance Company, Columbia, SC | Colonial Life insurance products are underwritten by Colonial Life & Accident Insurance Company, for which Colonial Life is the marketing brand.
10-14 | NS-14124