north american menopause society presidential plenary symposium: new findings from the kronos early...
TRANSCRIPT

North American Menopause Society
Presidential Plenary Symposium:
New Findings from the Kronos Early Estrogen Prevention Study (KEEPS) Randomized Trial
• Overview: KEEPS Rationale, Design, and Study Population
JoAnn E. Manson, MD, DrPHBrigham and Women’s HospitalHarvard Medical School
• KEEPS Biomarker and Vascular Imaging FindingsS. Mitchell Harman, MD, PhDKronos Longevity Research InstitutePhoenix VA Health Care System
• KEEPS Cognitive Function and Mood/Affective OutcomesSanjay Asthana, MD, FACP, FCRPUniversity of WisconsinNIA/NIH Wisconsin Alzheimer’s Dis. Research Ctr

• The core KEEPS was funded by the Phoenix-based Kronos Longevity Research Institute, which is supported by the not-for-profit Aurora Foundation, and was conducted at 9 U.S. academic medical centers.
• The KEEPS Cognitive Ancillary Study was supported by a grant from the National Institute on Aging, NIH.
Support

Principal Investigators
S. Mitchell Harman (KEEPS Director, KLRI) Frederick Naftolin (KEEPS Co-Director, NYU) Eliot A. Brinton/Paul Hopkins (U. of Utah) Marcelle I. Cedars (UCSF) Rogerio A. Lobo (Columbia) JoAnn E. Manson (Harvard) George R. Merriam (VA Puget Sound/U. of Washington) Virginia M. Miller (Mayo Clinic) Nanette Santoro (U. of Colorado)/Genevieve Neal-Perry (Einstein) Hugh S. Taylor (Yale)
Core Investigators and Ancillary Study Centers
Sanjay Asthana (Cognitive Study PI, U. of Wisconsin) Dennis M. Black (Biostatistical Center, UCSF) Matthew J. Budoff (CAC Reading Center, UCLA) Howard N. Hodis (CIMT Reading Center, USC)
Kronos Early Estrogen Prevention Study (KEEPS)

N = 727 women aged 42-59 (mean age, 52.7, within 3 yrs of FMP)
Trial Duration = 48 months
Multi-center double-blinded placebo-controlled RCT
Treatment Arms:
• Oral conjugated equine estrogens (o-CEE) given as Premarin®, 0.45 mg/d (lower dose than WHI)
• Transdermal Estradiol (t-E2) given by Climara® patch, 50 µg/d
• Placebo
(active arms received cyclical micronized progesterone [Prometrium®], 200 mg/d x 12 days/month; placebo arm received placebo Prometrium)
KEEPS Study Design

KEEPS: Specific Aims
To compare effects of oral vs transdermal estrogen vs placebo on:
1) Atherosclerosis progression as assessed by Carotid IMT
2) Development/progression of coronary artery calcium (CAC)
Other• CVD risk factors/biomarkers (BP, lipids, HOMA-IR)• Cognition and mood/depression (Ancillary Study)• Vasomotor symptoms, sexual function, QOL• Bone mineral density• Mammographic breast density/breast outcomes
(Ancillary Study)

• 42-59 years of age at randomization
• Final menses <3 years earlier
• Good general health
• Plasma FSH ≥ 35 mIU/ml and/or E2 levels <40 pg/ml
• Normal mammogram within one year before randomization
Inclusion Criteria

† p=0.0497
Mean SD
Age 52.7 2.6 Yrs since menopause 1.43 0.7BMI (kg/m2) 26.2 4.3Systolic BP (mm Hg) 119 15Diastolic BP (mm Hg) 75.0 9.2Total cholesterol (mg/dl) 208 34LDL cholesterol (mg/dl) 111 28
HDL cholesterol (mg/dl)† 72.0 15 (p
<0.05)
KEEPS Baseline Characteristics*
* Unless otherwise noted, there were no differences between treatment groups at baseline.

KEEPS Baseline Characteristics*
Race/Ethnicity
White 77%African-American 7%Hispanic 7%Asian 3%Other 6%
Education
No college degree 28%Bachelor’s degree 40%>4 years college 32%
Prior Hormone Use
Never 79%Current/Past 21%
Smoking
Never 76%Current/Past 24%
* Unless otherwise noted, there were no differences between treatment groups at baseline.

Changes in Risk Factors, Blood Pressure
p=NS
p=NS

Changes in Risk Factors, LDL Cholesterol & Triglycerides

Changes in Risk Factors, HDL Cholesterol
Levels
* * *
**
Month

Changes in Risk Factors, Fasting Blood Sugar & Insulin Resistance
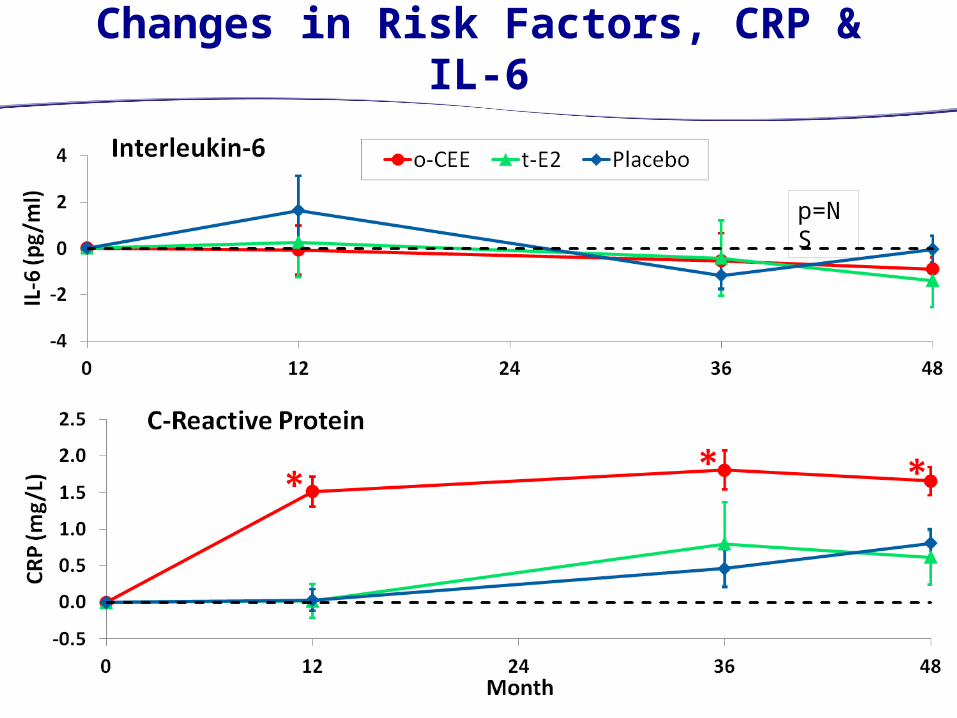
Changes in Risk Factors, CRP & IL-6
p=NS

Summary: Direction of Changes in Risk Factors*
* Relationship of some factors to CVD risk equivocal or subsidiary to related factors
Factor O-CEE T-E2Systolic BP Neutral NeutralDiastolic BP Neutral NeutralLDL Cholesterol Favorable NeutralTriglycerides Adverse NeutralHDL Cholesterol Favorable Neutral (?)Fasting Glucose Neutral FavorableHOMA-IR Neutral FavorableIL-6 Neutral NeutralCRP Adverse Neutral

Ultrasound Measurement of CIMT
Thickness of the common carotid artery intima-media layers measured by ultrasound (CIMT).
Hodis HN, et al.
Distal Far Wall CCA
Gray’s Anatomy, 1918, fig. 507
Arterial Lumen

Changes in Imaging Endpoints, CIMT
p=NS

Coronary Artery Calcium (CAC) by CAT Scan
Linear calcification in the left coronary artery in a KEEPS participant, Mayo Clinic

CAC Agatston Scores at Baseline
O- T- o-CEE t-E2 Placebo
p=NS

Percent of Subjects with Increases in CAC Score ≥ 5 Agatston Units
o-CEE t-E2 Placebo o-CEE t-E2 Placebo o-CEE t-E2 Placebo
p=NS
p=NS
p=NS

Serious Adverse Events Probably or Possibly Related to HT
Event o-CEE t-E2 Placebo p Value*
Cardiovascular Disease (MI) 0 1 0 0.43Stroke 0 0 0 N/AVenous Thrombotic Disease 0 1 1 0.72Breast Cancer 3 3 2 0.70Endometrial Cancer 2 1 0 0.45Endometrial Hyperplasia 2 1 1 0.99Deaths (all cause) 1 0 0 0.44
*Calculated by Chi Square (with Yates’ correction) for both estrogen groups pooled vs. placebo (2 x 2 table)

Significant o-CEE by Risk interaction for the Verbal Learning and Memory Factor
Women at “low” CVD risk receiving the o-CEE drug therapy were significantly more likely than the Placebo group to improve on Verbal learning and memory ability across time.
Results: Cognition and Cardiovascular Risk Profile

Results: Tests of Mood and Affect
Profile of Mood States (POMS)• Total Score• Depression-Dejection• Tension-Anxiety
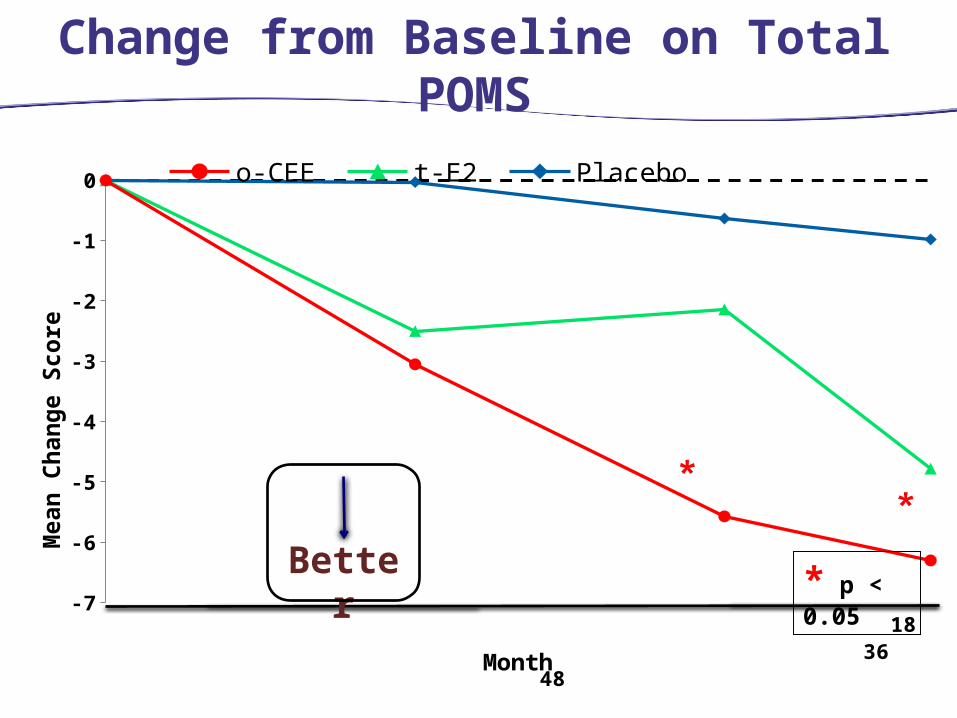
Change from Baseline on Total POMS
-7
-6
-5
-4
-3
-2
-1
0 o-CEE t-E2 Placebo
Month
Mea
n Ch
ange
Sco
re
18 36 48
* p < 0.05Better

Change from Baseline on POMS Depression-Dejection
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
1.5
*
o-CEE t-E2 Placebo
Month
Mea
n Ch
ange
Sco
re
18 36 48
* p < 0.05Better

Change from Baseline on POMS Tension-Anxiety
18 36 48
Better * p < 0.05

• Both o-CEE and t-E2 had favorable effects on vasomotor sx, sexual function, QOL, bone density (presented elsewhere).
• Both had neutral effects on BP (adverse effect in WHI).
• Both had generally favorable or neutral effects on CVD biomarkers (but differences related to first-pass liver metabolism).
• Both had neutral effects on CIMT and CAC (but ns trend for latter).
• Both had neutral effects on cognition (adverse effect in WHI, age >65).
• Differences: o-CEE improved mood, t-E2 improved HOMA-IR and some advantages for sexual function.
• KEEPS highlights the need for individualized decision making about HT, given different treatment priorities and risk factor status of women.
• Additional research on HT in newly menopausal women, including different formulations/doses/routes of delivery, is needed.
Overall Summary and Conclusions