nopho nobos meeting and congress uppsala, sweden, may … · nopho nobos meeting and congress...
TRANSCRIPT

Thank you for visiting Uppsala and the NOPHO NOBOS congress 2012
NO
PH
O 30th
an
nu
al &
NO
BO
S 9th
meetin
g a
nd
con
gre
ss Up
psa
la, S
wed
en
, May 19 –
22, 2012
Programme and Abstract Book
NOPHO NOBOS Meeting and CongressUppsala, Sweden, May 19 – 22, 2012
30years

Programme and Abstract Book
NOPHO NOBOS Meeting and CongressUppsala, Sweden, May 19 – 22, 2012

2 NOPHO • NOBOS 2012
Organizing Committees
NOPHO
Britt-Marie Frost, chairJohan ArvidsonJosefine PalleSusan Pfeifer
NOBOS
Magnus Grabski, chairEva TurupAnn-Christin Björklund

NOPHO • NOBOS 2012 3
Contents
Organizing Committees 2
Welcome 7
Sponsors 8
General Information 11
Other practical information 13
Social program 16
Map of Uppsala 19
Exhibitors 20
University Hall 21
NOPHO progamme 23
Abstract overview 30
Free papers OrAl 45
Free Papers POSTEr PrESENTATIONS 65
NOBOS programme 95
Guest speakers 100
Free papers OrAl 103
Poster 119

4 NOPHO • NOBOS 2012 [email protected] [email protected]
www.medac.sewww.medac.fi
SE 1
79/0
4201
2
Head Head
NOPHO-NOBOSNOPHO-NOBOS
20122012
sponsorsponsor

Exjade är indicerat för behandling av kroniskt ökad järninlagring orsakad av frekventa blodtransfusioner (erytrocytkoncentrat ≥ 7 ml/kg/månad) till patienter med beta-talassemi major från 6 års ålder och äldre. Exjade är också indicerat för behandling av kroniskt ökad järninlagring när deferoxaminbehandling är kontraindicerad eller otillräcklig hos följande patientgrupper: patienter med övriga former av anemier, patienter i åldern 2–5 år, patienter med betatalassemi major med ökad järninlagring orsakad av blodtransfusioner (erytrocytkoncentrat ≥ 7 ml/kg/månad). Det rekommenderas att behandling sätts in efter transfusion av ungefär 20 enheter (omkring 100 ml/kg) erytrokoncentrat eller då det finns evidens från kliniska kontroller att kroniskt ökad järninlagring föreligger (t.ex. serumferritin > 1000 µg/l) Doseringen (uttryckt i mg/kg) skall beräknas och avrundas till närmaste hela tablettstorlek. Den rekommenderade initiala dygnsdosen av Exjade är 20 mg/kg kroppsvikt. Dosjusteringar kan göras i steg om 5 till 10 mg/kg och skall skräddarsys utifrån den enskilda patientens svar och behandlingsmål. Dispergerbar tablett 125, 250 och 500 mg. 84 tabletter i blister. Produktresumén uppdaterad 2011-12-19. R. F. ATC-kod: V03AC03. För fullständig information, förmån och priser v.g. se www.fass.se
Novartis Sverige AB | Box 1150 | 183 11 Täby | Tel 08-732 32 00 | www.novartis.se

6 NOPHO • NOBOS 2012

NOPHO • NOBOS 2012 7
Welcome to Uppsala, Sweden for a Rocking meeting 2012.
Dear NOPHO/NOBOS friends, colleagues, sponsors and guests!
On behalf of the organizing committee, we have the great honour and pleasure to welcome you all to a historical meeting in Uppsala. The 30th anniversary for NOPHO, and the 9th meeting for NOBOS. We do hope that this meeting not only will be as memorable as previous NOPHO meetings, but also to be an inspiration for the future.
Our work as doctors, nurses and scientists rocks, as well as our organizations, and we do hope that our scientific program and the social program will rock you all!
Many prominent speakers are invited to cover important topics, ranging from “novel therapy for brain tumours” to “ethical aspects on pediatric oncology decisions”, see Main themes below. We also hope for a lot of scientific contributions from our NOPHO and NOBOS members. This will as usual be an important part of the program.
A special section on Monday afternoon is about NOPHO/NOBOS history and future. Our Grand old men and ladies will join us in a program with a panel discussion where also the Swedish Childhood Cancer Foundation plays an important role. They celebrate their 30th anniversary as well during 2012. This will give us an opportunity to make the gala dinner extra glamorous at Uppsala castle.
The meeting would not be possible without funding and we are very grateful to all sponsors and especially to our Gold sponsors and to the Swedish Childhood Cancer Foundation.
We look forward to meet you all in Uppsala to enjoy science and rock´n roll together!
Welcome
Britt-Marie FrostNOPHO
Eva TurupNOBOS

8 NOPHO • NOBOS 2012
Sponsors
We will thank the following companies and foundations for their support. With-out them it would not have been possible to arrange these Annual meetings.
GOLD SPONSORS
NOPHO • NOBOS 2012 9
SILVER SPONSORS
Mary Béves Stiftelse för Barncancerforskning
10 NOPHO • NOBOS 2012
OTHERS EXHIBITORS AND SPONSORS
Vårdväskan.se
Bard Norden AB
Gilead Sciences Sweden AB
Hospira Nordic AB
MSD
MundiPharma AB
roche AB
NOPHO • NOBOS 2012 11
General Information
Conference venue The conference takes place in Uppsala University Main Building, University Park, the corner of Övre Slottsgatan/S:t Olofsgatan. The building was raised in the 1880s. Parliament had allocated funding, and King Oscar II laid the cornerstone in pouring rain on a spring day in 1879. On May 17, 1887 the building was inaugurated at a festive ceremony. The architect was Herman Teodor Holmgren
Conference secretariat opening hours Saturday May 19 12.00 – 16.00Sunday May 20 08.00 – 17.00Monday May 21 08.00 – 17.00 Tuesday May 22 08.00 – 14.00
Name badge Your name badge is your admission to the scientific sessions as well as to coffee and lunches. It should be worn at all times at the conference venue.
Internet access Wireless internet access is available at the venue. You get a personal login upon registration on site.
Coffee Coffee will be served in the entrance hall of the conference venue. Please see the program for time and place. You will need your name badge as a ticket.
Lunches lunches will be served at Norrlands Nation (Address: Västra Ågatan 14) May 20-21. On May 22 you get a lunch bag in the entrance hall of the conference venue. You will need your name badge as a ticket.
Social events Get together, Saturday 19, at 19.00Welcome reception will take place at Uppsala Congress & Consert UKK (Address: Vaksalagatan 1). A mingle buffet will be served. The reception is included in the registration fee (Please note that pre-registration is necessary). Please, bring your ticket with you.

12 NOPHO • NOBOS 2012
NOPHO Dinner, Sunday 20, at 19.00NOPHO Dinner will take place at Katalin (Address: Godsmagasinet Östra Station, roslagsgatan 1). The dinner is included in the registration fee for NOPHO delegates. (Please note that pre-registration is necessary). Please, bring your ticket with you.
NOBOS Dinner, Sunday 20, at 18.30 NOBOS Dinner will take place at Norrlands Nation (Address: Västra Ågatan 14).The dinner is included in the registration fee for NOBOS delegates. (Please note that pre-registration is necessary). Please, bring your ticket with you.
Fun & Run, Monday 21, at 06.30-07.30 in Stadsträdgården (near restaurant Flustret). Please, pick up your T-shirt already on Sunday, May 20, at the conference secretariat during afternoon coffee break. Gala Dinner, Monday 21, at 19.00-01.00 at Uppsala Castle (Please note that pre-registration is necessary). Please, bring your ticket with you.

NOPHO • NOBOS 2012 13
Other practical information
Money exchange, currency Swedish Krona (SEK) is the official currency in Sweden. An exchange office is available next to the tourist office (Forex). Address: Fyristorg 8. There are plenty of cash dispensers in Uppsala. Major international credit cards are accepted in most hotels, shops and restaurants.
Shopping in Uppsala Most stores in Uppsala are open between 10.00-19.00 on weekdays and 10.00-17.00 on Saturdays. Some stores are open on Sundays as well. Grocery stores usually have longer opening hours.
Tipping Service is included in the restaurant bills. Tips, however, are given to show appreciation of a good meal or a special service.
Transport to Stockholm Arlanda International Airport
Taxi You can pre-book a taxi at (+46) 123456 or at www.taxikurir.se. The price to get to Stockholm Arlanda International Airport is about SEK 460 (50 Euro).
Bus Bus 801 runs between Uppsala Central Station and Arlanda once an hour the whole day and night. The journey takes about 45 minutes and costs 100 SEK (10 Euro). You can buy your ticket by credit card through a ticket machine in terminal 2, 4 and 5 at Arlanda airport and at Uppsala Central station.
Train Trains leave Uppsala Central Station for Arlanda Airport 1-3 times/hour from 5.00 until 23.00. The journey takes 15-20 minutes and costs 95-140 SEK (10-14 Euro) if purchased in advance at Uppsala Central Station.
Emergency calls You should call 112 if anything happens which means that an ambulance, the police or the fire brigade needs to be called out. 112 is a special emergency number you can call wherever you may find yourself, from a fixed or a mobile telephone.

14 NOPHO • NOBOS 2012
International calls Dial 00 + country code + area code + phone number. For example to Spain 0034, to Norway 0047
Electricity In Sweden the electrical voltage used is 230V.
Pharmacy There are several pharmacies in Uppsala. look for “Apotek”.
Medical services Uppsala University Hospital, Akademiska sjukhuset, is located in central Uppsala. Telephone: +46 18 611 0000. The emergency room is called “Akuten” in Swedish.
Medical advice by phoneThe medical advice line provides 24-hour advice. A nurse will answer your call and give you advice and refer you to your local health centre or A&E unit. The nurses know which treatment services are available at all times of the day or night. Calling the medical advice line costs the same as a normal local call. Telephone: 1177 (+46 771 11 77 00)
Smoking Smoking is not allowed in the conference venues, or in any other public indoor establishments such as restaurants, bars, etc.
Organization Support Academic Conferences – SlU and Uppsala University in cooperationOffice contact details during office hours (8.00-16.00 local time) Tel: +46 (0)768 266 730/+46(0)1867 1003 E-mail: [email protected]

Swedish Orphan Biovitrum develops, manufactures and sells medications for a number of diseases, with a special emphasis on four specialist areas: hematology & hemophilia, inflammation/autoimmune diseases, inherited metabolic diseases and oncology.
We focus on medications for rare disease patients with a high unmet medical need. This category includes specialist and so called orphan drugs, which are mainly prescribed by clinical specialists and aimed at small well defined patient groups. These less common diseases are often neglected and inadequately treated which means that new medications can offer significant value for the patient and health care providers.
Sweden Denmark Finland NorwaySwedish Orphan Swedish Orphan Biovitrum A/S Oy Swedish Orphan Swedish Orphan Biovitrum ASBiovitrum AB (publ) Wilders Plads 5 Biovitrum AB Trollåsveien 6SE-112 76 Stockholm DK 1403 København K Keilaranta 19, 7th floor NO-1414 TrollåsenSweden Denmark Finland NorwayPhone: +46 8 697 20 00 Phone: +45 32 96 68 69 Phone: +358 201 558 840 Phone: +47 66 82 34 00
PG 90 20 90-0 www.barncancerfonden.se
TRE AV FYRA BARN ÖVERLEVER CANCER
16 NOPHO • NOBOS 2012
Social program
All social events require pre-registration and is included in the registration fees for delegates.
Saturday 19 May19.00 – 23.00 Get together / Welcome mingle reception at Uppsala Concert & Congress (UKK), light snacks with a taste of Sweden and drinks will be served.Address: Vaksala torg 1 – distances within Uppsala are short indeed, but if you want to go by taxi, say “konserthuset”. Vaksala torg 1 (see map)
In September 2007, Uppsala opened its new concert and congress hall, Uppsala Concert & Congress, which is located in the centre of the town. This magnificent building stands 8 floors high, and 37 meters tall (121 ft). It consists of 14,600 sq meters (157,153 sq ft) of function space.
The building offers a spectacular view, 360⁰ widescreen, of the city. The world famous Danish architect firm “Henning larsen Tegnestue” has created Uppsala Concert & Congress. The same firm also created the magnificent Opera house in Copenhagen and other famous buildings around the world.
The welcome party is casual indeed, and will present a young rock band, some street fashion photographers and a bar open until 23.00. You have the possibility to take the escalators to the viewing area, or maybe you prefer to watch the sunset by the outdoor tables.
NOPHO • NOBOS 2012 17
Sunday 20 May18.30 - 23.00 Dinner at Norrlands nation (NOBOS only) Address: Västra ågatan 14 (See map)
Norrlands nation is the largest student society in Uppsala. The nation owns a building complex of 5,500 sqm by the Fyris river in central Uppsala, with the older part from 1889, the facade being designed by Swedish architect Isak Gustaf Clason.
At 22.00 all NOBOS members are welcome to join the NOPHO dinner at Katalin for partying and dancing to the cover band ”DocV”, see below.
19.00 – 00.00 Dinner with rock’nroll at Katalin (NOPHO only)Address: roslagsgatan 1 (See map)
Katalin Varga started a music scene in Uppsala 25 years ago, and has by now an imperium where all artists, except those who fill up the Stockholm Globe arena, want to try out their new concert tour in a minor space but a major venue. If you arrive Friday May 18, you can listen to Eilen Jewell band (US). It is right by, east of, the central station.
At Katalin we will enjoy a three course dinner with refreshments. After the dinner there will be dancing to the band ”DocV”. They started to perform together in 1987 (!) and play soul and funk covers. The NOBOS gang will join NOPHO here after their dinner.
Dress: rocky and relaxed

18 NOPHO • NOBOS 2012
Monday 21 May06.30 – 07.30 Fun and run (NOPHO and NOBOS)Start: Café Fågelsången, Munkgatan 3
Enjoy a morning hour in the Uppsala’s crown jewel, the city park. The fun and run will take place along Uppsala ”Fyrisån”. Afterwards we will enjoy breakfast at Cafe Fågelsången. Breakfast is included in the registration fees for the runners.
19.00 – 01.00 Annual dinner and dance (NOPHO and NOBOS)
Uppsala Castle dates back to the 16th century and has been the site of numerous Historical events. The conference banquet will include a three-course gourmet dinner in the magnificent Hall of State, where Queen Christina of Sweden abdicated her throne in June of 1654. Today the castle houses the city of Uppsala’s and Uppsala University’s art collections. It is also the residence of the county governor.
Entertaining for the evening will be Uppsala Big Band ”Phontrattarne” with a mighty brass section, glitter and glam and also a ballet. Uppsala artist Anna-Karin Nytell-Oldeberg (AKO) will sing with/for us during the dinner. Don’t forget to bring dance friendly shoes.
Dress: you have the chance to dress up in your gala ballroom dress and suit, or choose a more comfortable party dress.

TYCHO HEDÉNS VÄG TYCHO HEDÉNS VÄG
Sernanders väg
Flogstavägen
Flogstavägen
Flogstavägen
Torshavnsgatan
Ihres
väg
Hess
elman
s väg
Nore
ens v
äg
Säve
s väg
Osloga
tan
hamns
g.
Köpe
n-
husgatan
Tavaste-
Nordengatan
Helsi
ngfor
sgata
n Ek
ebyv
ägen
Väno
rtsga
tan
Ekebydalsvägen
Flogsta
väge
n
Eriksbergsvägen
Gnejs
vägen
Granitvägen Granitvägen
Granitvägen
Grönstensvägen
Marmo rväge
n
Skogsbärsvägen
Urbergsvägen
Stenbergsvägen
Rödbergsvägen
Norrbergsvägen
Glimmervägen
Stigbergsvägen
Blodstensvägen Kvicks
tensväg
Täljstensv
Stadsskogsvägen
Bruksvä gen Bruksvägen Gråbergsvägen
Linds bergsvägen bergsgat Gustafs-
Birkagatan
Arosgatan
Hagundagatan
Karls
rogata
n
Drejargatan
Slöjdgat
an
Tege
lgatan
Be
rgag
atan
Kvar
nbog
atan
Läby
gatan
Norb
yväg
en
Reykjaviksgatan
Karlsrogatan
Berthåga byväg
Furud
alsvä
gen
Bert
ilsvä
gen
Heden
sberg
sväg
en
Albersvägen
Berthågav
Robertsvägen
Herbert
sväg
en
Berthåga Lindväg
Enge
lberts
väge
n
Fålhags- gatan
Björkgatan
Skomakargatan
Dimgatan
Tövädersgatan
Solskensgatan
Gränby
bilgata
Hökargränd
Österleden Slavstavägen
Storkällsvägen
Kvarnkullsvägen
Brillingevägen Brillingevägen
Smedje
-vägen
Alrunegatan
Alrunegatan
Kamom
illgatan
Fänkålsgatan
Tomatgatan
Betgatan
Timjansgatan Timjans- gatan
Lökgat
Krassegat
Morotsgat
Dillgat
Rädisegat
Ärtsgat
Vitkålsgatan Vitkålsgatan
Rättikgatan
Pepparrotsgatan
Gräslöksgatan
Sparrisgatan
Fålhagsle
den
Rödbetsgatan
Rödbetsgata
n
Kummingatan
Körvelgatan
Jordgubbsgatan
Vinbärsgatan
Krusbärsgatan
Kålrotsgatan
Sellerigatan
Rabarber
gata
n
Rotfrukts-
gatan
Paprika
g.
Senapsgat.
Melongat.
Melongat.
Pers
iljegat.
Purjogatan
Salladsg.
Årstagatan
Byggmästar- gatan
Murar-
ga
tan
Målarg.
Apelgatan
Apelgatan
Verkmästar- gatan
Snickargatan
Gröna gatan
Rita
rgat
an
Johannesbäcksgatan
Örbygatan
Vallbygatan
Jällagatan
Smedsbylegatan
Blomstigen
Majgatan
Mist
elgat
an
Klöver- gatan
Järne
ksgatan
Väppling- gatan
Mistelgatan
Näckrosgatan
Näckrosgatan
Vallmogatan
Bolandsgatan
Bolandsgatan
Nymansgatan
Danmarksgatan Danmarksgatan
Verkstadsgatan Verkstadsgatan
Stångjärnsgatan Spikgatan
Stålg
atan
Vaksa
la ky
rkvä
g
Fålhags- leden
Fålhagsleden
Axel Johanssons gata
Fyrisborgsgatan
Sylveniusgatan
Svederupsgatan
Stålgatan Lefflersgatan
Palmbladsgatan
Klar
bå
rsgatan
Hjor
trong
atan
Haeggströmsgatan
Fyrislundsgatan
Hansellisgatan
Edvard Berlingsgatan
Möllersvärdsgatan
Rapsgatan
Raps
gata
n
FYRYSLUNDSGATAN
Otto Myrbergs väg
Hildur Ottelins gata
Celsiusgatan
Torgnyg.
Elias Fries g
Pontus
Wikners gata
.
Viktoria- gatan Bredmans- gatan
Geije
rsgatan
Geijersg
atan
Tegnér
- g
atan
Hällbygatan
Prästgårdsgatan
Stabby
Allé
Norrlan
dsgata
n
lundsg. Stabby-
Ring
gatan
Eriksgat
an
Dalgata
n
Norrlan
dsga
tan
Vindhemsgatan
Jumkilsgatan
Floragatan
Seminariegatan
Präs
tgatan
Prinsgat
Humleg
atan
Stefansg
Klockar
g
Gimogatan
Vallongatan
Börjegatan
Börjegatan
Söderfo
rsgata
n Sk
ebog
atan
Tiundagatan
Kyrkogårdsgatan
Börjegatan
Väpna
rgatan
Tunabergsgatan
Fjärdhundragatan
Startga
tan
Vingga
tan Reagatan
Tunagatan
Tunagatan
Flygargatan
Fallskärmsg
Flottörgatan Spanargatan Kadettgatan Flottiljg
atan
Flottiljgatan
Divisionsgatan
Eskadergatan
Rotegatan
Pilotgatan
Hangargatan
Raketgatan
Radargatan
Bärbygatan
Stenkilsgatan
Hällkist- gatan Runstens- gatan
Tingshögs- gatan Lagmansgatan
Swedenborgsgatan
Ynglingagatan
Galgbacksgatan
Sandgropsgatan
Runebergsgatan
Fänr
ik S
tåls
gat
a
Sandels gata
Hurtig
s ga
ta
Mun
ters
gat
a Birger Sjöbergsg
Sehlstedtsg.
Elin Wägners g
Fredrika Bremers g
Karin
Boy
egat
an
Dager- ma nsga
tan
Ferli
nsga
tan
Lage
rlöfs
-
gata
n
Runebergsgatan
Almqvistgatan
Albert Engströmsgatan
Bellm
ansg
atan
Norbyvägen
Skogsmyrsvägen
Norra
Parkvägen Tallmovägen
Plöjarv.
Rättarv.
Konsum- vägen
Norra Parkvägen
Norby Källväg Plogvägen
Sälgvägen
Pilvägen
Emmy Rappes väg
Ulle
råke
rsvä
gen
Rosendalsvägen Vårdsätra
v.
Sibyllegatan
Tunåsenssjukhem
Domarringensskola
Lötenssportfält
Tunakyrkan
Tunabergsskolan
Fyrishov
Fyrishovcampingstugby
Fyrisfjädern
Fyrisskolan
Linnéträd-gården
Linné-museet
Inst förlärarutbildning
Linné-skolan
Nanna-skolan
Stadsbib-lioteket
Celsius-huset
Central-badet
Upplands-museet
Salu-hallen
KyrkansHus
Universitets-huset
Universitets-förvaltningen
CarolinaRediviva
Geijers-gården
UbboUppsalastudent-kår
Trefaldig-hetskyrkan
Botaniska trädgården
Linnéanum
Botaniska trädgården
Evolutions-biologisktcentrum
Evolutionsmuseet
Engelska parken.Humanistiskt centrum
The Svedberg-laboratoriet
Husläkarakuten
Observatoriet
Musicum
Katedralskolan
Biologiskamuseet
Vindhems-kyrkan
Sverker-skolan
Rackarberget
Studentvägen
Triangeln
Studenstaden
UppsalaSlott
Gunilla-klockanCarolinaparken
"Engelskaparken"
Lands-tingshuset
Katolskakyrkan
Stads-huset
Frälsnings-armén
Central-station
Folkets HusStadsteatern
Buss-station
Gods-magasinet
Vaksala-skolan
Öster-ängen
Årsta IP
Almtuna-kyrkan
Kvarn-gärdes-skolan
Gränbyskolan
Liljeforsskolan
Ishallen
UTK-hallen
Gränby centrum
S:t Perskyrka
Diös-hallen
Moskén
Heidenstamskolan
Bellmanskolan
Lötenkyrkan
Samariter-hemmetssjukhus ochkyrka
Bolandsskolan
Livets Ord
Lundellskaskolan
Johannesbäcks-skolan
Brantings-skolan
Årsta-kyrkan
Årsta-skolan
Ångelsta-skolan
Vaksalakyrka
Vaksalakyrkskola
Salabacke-kyrkan
Almtunaskolan
Balderskolan
Celsiusskolan
Läns-styrelsen
Livsmedels-verket
RikssalenFredsmuseet
Konstmuseet
Flustret
Svettis
Pump-huset
Hamnen
Slotts-källan
Stadsträdgården
Parksnäckan
Studenternas Idrottsplats
Akademiskasjukhuset
Akademiskasjukhuset
Läkemedelsverket
Magistern
Arkivcentrum
SverigesGeologiskaUndersökning
BrorHjorthsHus
BergaskolanFlogstaskolan
Eriksbergs-skolan
KungBjörnshög
Hågadals-skolan
Täljstens-skolan
Ekebyskolan
Gläntan
ZoologiBiologi
Paleontologi
Eklundshof
UppsalaHälsobrunn
Matematisktinformationsteknologisktcentrum (MIC)
Vasa-borgen
Gust
avia
num
Domkyrkan
Balder-skolan
S:tJoh
annis
kyrka
Mikaels-kyrkan
Ångström-laboratoriet
Lundellska skolan
Kungsängens gård
85
82
78,79
77
6
12 15
10
4035
30
60
91
95,96
88
70
Uppsala Science Park
Rudbeck-laboratoriet
Farmacevtiska studentkåren
Stallet
Geo-centrum Wallenberg
laboratoriet
Tropiska växthuset
BiomedicinsktCentrum (BMC)
Växtbiologiskainstitutionen
Ekonomikum
PelleSvanslös Hus
Polis-huset
Korskyrkan
UppsalaKonsert &Kongress
Stillhetenskapell
INFORMATION
TOURIST
Mot Ulva kvarn, Björklinge och Gävle
Mot Gamla Uppsala, Vals-gärde, Storvreta,Österbybruk
Mot Sunnersta,Ultuna,Sigtuna
Mot Valsätra,Gottsunda,Hammarskog
Mot Jälla, Gimo, Öst-hammar
Mot Svia,Norr-hällby
Mot Sävja,NåntunaKungshamn,Morga,Sigtuna
Mot Sten-hagen, Vänge, Vik,Enköping,Sala
Mot Linnés Hammarby, Fjällnora,Almunge
Mot Knivsta ochStockholm
Mot Jumkil,Östervåla, Gysinge
Torbjörnstorg
Kvarn-torget
Liljeforstorg
von Bahrska häcken von Bahrska häcken
Kapell-gärdsparken
Gränby sportfält
Vaksalatorg
S:t Erikstorg
OrpheiDrängarsplats
Fyristorg
StoraTorget
Forumtorget
GamlaTorget
Riddartorget
Odins-lund
Slotts-backen
Kyrkogård
Kyrkogård
Observatorie-parken
Skolparken
Fyrisån
Fyrisån
Fyrisån
Fyrisån
Svandammen
Polacksbacken
Kungsängen
Stadsskogen
Stadsskogen Golfbana
Svea-plan
Sten Sture-monumentet
Österplan
Österplan
M.L.Kingsplan
Tor
björnsgatan
Folkungagatan
Idrottsgatan
Idrottsgatan
Styrbjörnsgatan
Egilsgatan
Swedenborgsgatan Swedenborgsgatan Timm
ermansgatan
Vikingagatan
Vikingagatan
Auro ragatan
Hugleks- gatan
Hallstensgatan
Anundsgatan
Ingvarsgatan
Idunagatan
Sköldungagatan
Valhallagatan
Adilsgatan
Stjernshjelmsgatan
Västra Järnvägsgatan Repslagargatan
Gamla Uppsalagatan
Gamla Uppsalagatan
Fyrisvallsgatan
Ringgatan
Tegnérg
atan
Götgatan Götgatan V Strandg.
Geijersgatan
Sturegatan Sturegatan
Sysslomansgatan Sysslomansgatan Sysslomansgatan
Wallingatan
Börjegatan
To
rsgata
n
Fyrisgatan
Fredsgatan
Gluntens
gränd
Vasagatan
Oden
sgatan
Rektorsgatan Rundels- gränd
Övre Slottsgatan Övre Slottsgatan
Skolgatan
S
kolgatan
Skolgatan
Svartman
-gata
n
S:t Johannesgatan
S:t
Jo
hannes- g
atan
S:t Larsgatan
Villavägen Villavägen Villavägen
Gropgr
Åsgränd
Akad
emig
Va
ttugr
S:t Olofs
gatan
S
:t Olofs
-
gatan
S:t O
lofsgat
an
K
varnto
rgsg.
Eddagatan
Svartbäcksgatan Svartbäcksgatan
Linné-
gat
an
Östra Ågatan Östra Ågatan
Kloster-
g
atan
Biskopsgatan Trädgårdsgatan
S:t Eriksg
Valvg
S
:t Pers
gatan
S:t P
ersgat
an
Drottnin
ggatan
Slotts-
gr
änd
Munkgatan
Östra Ågatan Östra Ågatan
K
ungsängs- esplanaden
Flustergr.
Thunbergsvägen
Norbyvägen
Norbyvägen
Walle- riusvägen
Liljeborgsvägen
Kåbovägen Götavägen Artille
rigatan
Kåbovägen Kåbovägen Husargatan
Norra Rudbecksgatan
Borgv
Södra
Rudbeck
sg
atan
Svea
väge
n
Banérgatan
Banérgatan
Nedre Slottsgatan Sjukhusvägen Sjukhusvägen
Dag Hammarskjölds väg
LUTHAGSESPLANADEN
RÅBYVÄGEN
R
ÅBYV
ÄGEN
Kantorsgatan
Djäknegatan Djäknegatan
Portalgatan
Väk
targa
tan
Gärdets
bilgat
a
Thun
mansg
atan
Buréusgatan
Strindbergsgatan
Lenngrensgatan
Thorildsgatan Frödingsgatan
Karlfeldts gatan
Wennerbergsgatan
Thunmansgatan
K
varn-
ängs
gat
Ligga
r-
gatan
Kvarnskogatan
Trattg Skruvgat
Lurgatan
Långjä
rns
Hjulgatan
Kvarn- kammarg
Höganäs
gatan
Storgatan
N
orrtäljegatan
Salagatan Salagatan
Botvidsgatan
Väderkvarnsgatan Alriksg.
Vaksa
la- g
atan
Vaksala
gatan
Påvel
Snickar
esgr
Dragar- brunns- gatan Dragar- brunnsgatan
Kungsängsgatan
Smeds
gränd
Bangårdsgatan
Vretgrä
nd
Bäverns gränd
Kålsäng
s-
gränd
Hamnes
planad
en
Suttungs
gränd
Muningatan
Islandsgatan
Siktargatan Kungsängsgatan
Sågargatan Sågargatan
Mältargatan Mältargatan
Mastgatan
Stallängsgatan
Kungsgatan Kungsgatan Kungsgatan Kungsgatan
Strandbodgatan
Strandbod-
gatan
S
trand
bodk
ilen
Li
ljega
tan
Eskilsgatan
Hjalmar Brantingsgatan
Frodegatan
Ymergatan
Österängsgatan Österängsgatan
Petterslundsgatan
Björkgatan
Lindgatan
Torkelsgatan Torkelsgatan Torkelsgatan
Vildrosgatan Syréngatan
Marielundsgatan
Göransgatan
SVARTBÄCKSGATAN
VAKSALAGATA
N
VAKSALA
GATAN
Ulleråkersv.
Bred
- grä
nd Västra Ågatan
Bergsbrunnagatan
Knivstagatan
Alsikeg
atan
Oden- salag
Östuna
gatan
Levertingsgatan
Atterbomsgatan
Kyrkogårdsgatan
Kyrkogårdsgatan
Tiunda- gatan Krong.
Karls
rogata
n
S:tJohannesgatan
Löpar g
atan
Väktar
gatan
BÄRBYLEDEN
Blixtgatan
Molngatan
Stormgatan
Regngatan
Salabac
ksgata
n
Lästm
akargatan
Källparksgatan
Gränby
tvärg.
Marknadsgatan
Årstagatan
Hjalmar B
ranting
sgatan
Stockrosgatan
Törnlundsgatan
Ljungg.
Öxelgatan Björkgatan
Furu
gatan
Solrosgatan Rimbogata
n
Vallbygatan
Gunstagatan
Hammarbygatan Hammarby- gatan
Fålhagsleden
Säbygatan Märstagatan
Sofie
lunds
gatan
Villingeg.
Villin
gega
tan
Björkgatan
Vimpelgatan
Kungsgatan
KUNGÄNGSLEDEN
Lings väg
von Bahrs v.
Stagneliusgatan
Heiden
stam
sg.
Regementsvägen
Eklundsho fsvägen
Lä gerhyddsv.
Samari-
tergr.
Kungsängsvägen
Kungsängsvägen
Mot Linnés Hammarby, Husby-Långhundra
Bâtiment publicEspace vertHôtelEspace bâtiArtère principalRue Rue réservée aux autobusRue piétonnière
Public buildingPark areaHotelStreet blocksMain streetStreetStreet, only busesPedestrian precinct
Öffentliches GebäudePark, Hotel HäuserblocksHauptstraßeStraßeStraße, nur BusseFußgängerzone
Yleinen rakennusPuistoHotelliTiesulkuPääkatuTieTie vain busseile
Kävelykatu
Kalmar
V-Dala
Upplands
Göteborgs
Smålands
Värmlands
Stoc
kholm
s
Norrlands
G-H
Västgöta
Östgöta
Gotlands
S-Nerikes
Uppsala Tourism AB© Godkänd från sekretessynpunkt för spridning. Lantmäteriverket 1994-04-20. Reviderad oktober 2006
100 200 300 400 500 600m
Public building
Hotel
UPPSALA CITY
Uppsala Tourism AB Fyristorg 8, SE 753 10 Uppsala Phone: +46 (0)18-727 48 [email protected] www.uppsalatourism.se
Uppsala Tourism AB© Approved for free distribution.Lantmäteriverket 1994-04-20. Modified february 2007
100 200 300 400 500 600m
DisagårdenOdinsborg
Gamla Uppsala högar
GamlaUppsalamuseum
Gamla Uppsala kyrka
Gamla Uppsala
Disavägen
Till Ulva kvarn,Björklinge
Mot V
alsgä
rde,
Stor
vreta,
Öste
rbyb
ruk
Ärna- vägen
Islands-
bron
Västgöta-
spången
Nybron
Dombr
on
S:t Olof
s-
bron
Järn-
bron
Haglun
ds
bro
Edda-
spån
gen
Heimda
ls-
spån
gen
Fyrisvalls-
bron
Luthags-
bron
Important places 1. Train station 2. University Hall 3. Norrlands nation 4. Uppsala Konsert & Kongress 5. Katalin 6. Cafe Fågelsången 7. Entrance to Town park 8. Pump House
Hotells 9. Clarion Hotel Gillet 10. Scandic Hotel Uplandia 11. Hotel Uppsala 12. Hotel linné
1
23
4
5
67
8
910
11
12
20 NOPHO • NOBOS 2012
2
11 10
31 64 5
9 8 7
POSTERS
PO
ST
ER
S
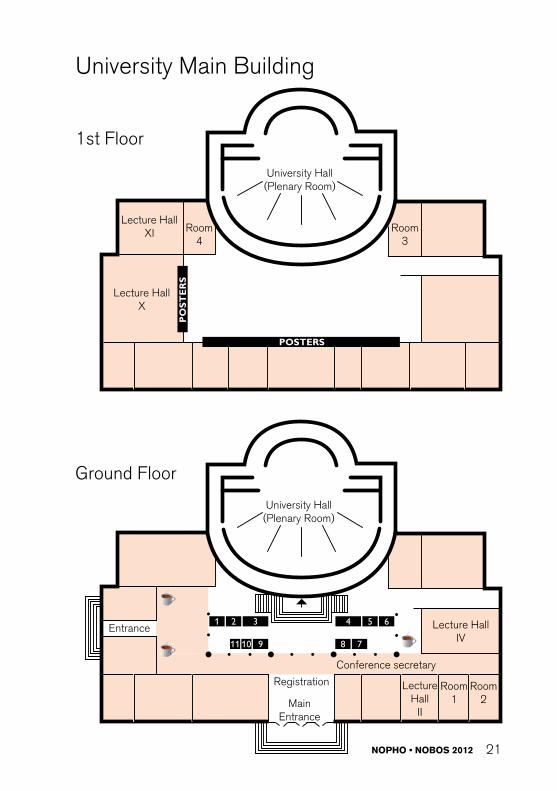
University Main Building
University Hall(Plenary Room)
University Hall(Plenary Room)
Lecture HallXI
Lecture HallX
Lecture HallIV
1st Floor
Ground Floor
MainEntrance
Entrance
Registration
Conference secretary
Room3
Lecture Hall
II
Room4
Room1
Room2
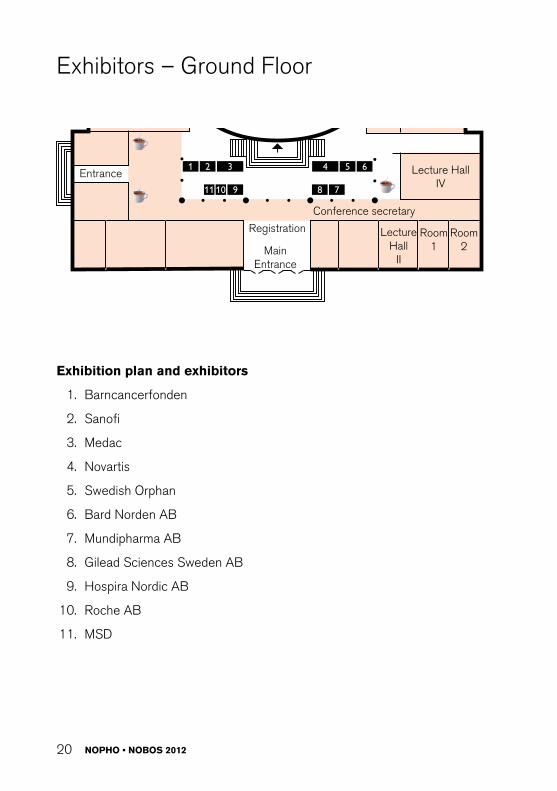
Exhibitors – Ground Floor
Exhibition plan and exhibitors
1. Barncancerfonden
2. Sanofi
3. Medac
4. Novartis
5. Swedish Orphan
6. Bard Norden AB
7. Mundipharma AB
8. Gilead Sciences Sweden AB
9. Hospira Nordic AB
10. roche AB
11. MSD
NOPHO • NOBOS 2012 21
University Main Building
2
11 10
31 64 5
9 8 7
POSTERS
PO
ST
ER
S
University Main Building
University Hall(Plenary Room)
University Hall(Plenary Room)
Lecture HallXI
Lecture HallX
Lecture HallIV
1st Floor
Ground Floor
MainEntrance
Entrance
Registration
Conference secretary
Room3
Lecture Hall
II
Room4
Room1
Room2
Celsite® Access Ports and Accessories for paediatric indications
Specially designed for mid to long term venous applications in babies and children

NOPHO • NOBOS 2012 23
Programme

24 NOPHO • NOBOS 2012
SATUrDAY12.00 – 16.00 Registration / Information open at Uppsala
university main building.
19.00 – 23.00 NOPHO & NOBOS Get together at Uppsala Konsert & kongress (UKK)
SUNDAY08.00 – 17.00 Registration / Information open
08.00 – 17.00 Poster viewing
09.00 – 09.50 Official grand opening with entertainment, Room: University Hall (Plenary Room)Choir: Tonprakt, Conductor: Anders ’Grosse’ Grotherus, Song: Thomaz Szendrö, Piano: leif Österlund
How to deal with difficult ethical problems in clinical praticeChair: Britt-Marie Frost
09.50 – 10.00 Introduction to EthicsAnders Castor, Lund, Sweden
10.00 – 10.40 Can clinical ethics committees be useful for clinicians?Reidun Førde, Olso, Norway
10.40 – 11.10 Coffee break
11.10 – 11.40 Moral deliberation in the wardNOPHO & NOBOS WG in Ethics
11.40 – 12.10 Where is the child? – Navigating the intersection between pain and hopes of cureMats G Hansson, Uppsala, Sweden
Supportive care
12.10 – 12.20 O1. When there is no chance of cure – where does palliation start and treatment end?Li Jalmsell, Uppsala, Sweden
12.20 – 12.30 O2. Is there a decrease in survival rates after reduction of therapy? A population based study of children with Hodgkin lymphoma.Charlotte Hopstadius, Uppsala, Sweden
12.30 – 14.00 Lunch at Norrlands nation

NOPHO • NOBOS 2012 25
Late complications and rehabilitationChair: Gustaf ljungman, Per Frisk
14.00 – 14.40 New Initiative to improve quality of life for childhood cancer survivors: E-mental health interventionsMartha Grootenhuis, Amsterdam, Netherlands
14.50 – 15.30 Hodgkin’s lymphoma: A paradigm for the study of late effects of cancer.Hamish Wallace, Edinburg, United Kingdom
15.30 – 16.00 Coffee break
16.00 – 16.40 Pediatric brain injury rehabilitation: Standard of Care and new Directions.Robert W. Butler, Portland, Oregon, USA
Selected free papersChair: Johan Arvidson
16.50 – 17.00 O3. Changes in patient survival of childhood solid tumors diagnosed 1985-2010 in the Nordic countries.Milada Cvancarova Småstuen, Norway
17.00 – 17.10 O4. Standard risk Medulloblastoma in Europe: studies completed and planned.Birgitta Lannering, Gothenburg, Sweden
17.10 – 17.20 O5. Vascular Endothelial Function in long-Term Survivors of Childhood Acute lymphoblastic leukemia: Effects of a Home-Based Exercise Program.Liisa Järvelä, Turku, Finland
17.20 – 17.30 O6. Presentation of the “Multinational EuropeanTrial for Children with the Opsoclonus Myoclonus Syndrome (OMS)”.Ingrid Øra, Lund, Sweden
17.30 – 17.40 O7. Procalcitonin for Detection of Infection – a Hope or a Hype? A cohort study of immunosuppressed children.Cecilie Rutkjær Jensen, Aarhus, Denmark
17.40 – 17.50 O8. Bone marrow remission status predicts leukemia contamination in ovarian biopsies collected for fertility preservation.Babak Asadi A, Oslo, Norway
17.50 – 18.00 Closing time – Summary

26 NOPHO • NOBOS 2012
MONDAY08.00 – 17.00 Registration / Information open
08.00 – 17.00 Poster viewing
08.20 – 08.30 Info from the organizers
08.30 – 10.30 NOPHO general assembly, Room: University Hall (Plenary Room)Thomas Leth-Frandsen, Copenhagen, Denmark
10.30 – 11.00 Coffee break
Late effectsChair: Gustaf ljungman & Per Frisk
11.00 – 11.10 O9. Estimated clinical benefit of protecting neurogenesis in the developing brain during radiation therapy for pediatric medulloblastoma.Malin Blomstrand, Gothenburg, Sweden
11.10 – 11.20 O10. Identification of somatic mutations in acute lymphoblastic leukemia by whole genome sequencing.Eva Berglund, Uppsala, Sweden
11.20 – 11.30 O11. Cardiovascular disease in adult lifte after childhood cancer in Scandinavia (AliCCS) - A large population-based patient cohortThorgerdur Gudmundsdottir, Copenhagen, Denmark
11.30 – 11.40 O12. Neurocognitive function in very long-term survivors of acute lymphoblastic leukemia treated with chemotherapy only.Adriani Kanellopoulos, Oslo, Norway
11.40 – 11.50 O13. Endocrine late effects in childhood cancer survivors. Under the research program “Adult life after Childhood Cancer in Scandinavia (AliCCS)”Sofie de Fine Licht, Copenhagen, Denmark
11.50 – 12.00 O14. reduced cerebral volumes in long term survivors of childhood lymphoblastic leukemia (All).Bernward Zeller, Oslo, Norway
12.00 – 12.10 O15. The Association of late Effects to Different Conditioning regimens and Previous leukaemia Treatment after Paediatric Allogeneic HSCT.Mari Wilhelmsson, Stockholm, Sweden
12.10 – 14.00 Lunch at Norrlands nation

NOPHO • NOBOS 2012 27
Translational research and novel treatments (Mary Béve Symposium) Chair: Josefine Palle & Kleopatra Georgantzi
13.30 – 14.10 Biology and treatment of infant AllRob Pieters, Rotterdam, Netherlands
14.10 – 14.40 Cellular drug resistance in childhood leukemia – an updateGudmar Lönnerholm, Uppsala, Sweden
14.40 – 14.50 Short break
14.50 – 15.30 Translational research and clinical trials in pediatric oncologyPeter Adamsson, Philadelphia, USA
15.30 – 16.00 Coffee break
16.00 – 16.10 O16. Pharmacogenetically based dosing of thiopurines in childhood acute lymphoblastic leukemia – influence on cure rates and risk of second cancer.Elisabeth Ørskov Sørensen, Copenhagen, Denmark
16.10 – 16.20 O17. Age-Dependence of Tumor Genetics in Unfavorable Neuroblastoma.Fredrik Hedborg, Uppsala, Sweden
16.20 – 16.30 O18. Familial hemophagocytic lymphohistiocytosis type 3 (FHl3) caused by deep intronic mutation and inversion in UNC13D.Marie Meeths, Stockholm, Sweden
16.30 – 16.40 Short break
16.40 – 17.40 The Swedish Childhood Cancer Foundation – Tribute to the pioneers. (NOPHO and NOBOS) room: University Hall (Plenary room)
NOPHO: Gunilla Berglund, Stanislaw Garwicz, Göran Gustafsson, Henrik Hertz, Gudmundur Jónmundsson, Anders Kreuger, Sverre Lie, Göran Lundell, Toivo Salmi, Minna Yssing, Lars Åhström
Richard Johansson, Founder of Swedish Childhood Cancer Foun-dation
From NOBOS Gitte Petersen and Margareta af SandebergFrom The Swedish Childhood Cancer Foundation Olle Björk
Song: Kristin NordströmInterviewer: Jenny Strömstedt

28 NOPHO • NOBOS 2012
TUESDAY08.00 – 14.00 Registration / Information open
08.00 – 12.00 Poster viewing
08.30 – 08.40 Info from the organizers
Infections in neutropenic patientsChair: Gustaf ljungman & Torben Ek
08.40 – 09.20 Infectious complications in children undergoing therapy for malignancyThomas Lehrnbecher, Frankfurt, Germany
09.20 – 09.30 Short break
Novel treatments for children with brain tumoursChair: Susan Pfeifer & Fredrik Hedborg
09.30 – 10.00 Strategies for curative treatment and quality of life as a basis for neurosurgical treatmentPelle Nilsson, Uppsala, SwedenPer Enblad, Uppsala, Sweden
10.00 – 10.10 O19 Swedish national biobank for pediatric neural tumorsSusan Pfeifer, Uppsala, Sweden
10.30 – 11.00 Coffee break
10.40 – 11.00 Proton radiotherapy, principles & advantagesKristina Nilsson, Uppsala, Sweden
11.00 – 11.40 Proton radiotherapy of brain tumors in childrenBreate Timmermann, Essen, Germany
11.40 – 12.00 The Scandion Clinic á Scandinavian centre for radiation therapy with proton beamsAnders Montelius, Uppsala, Sweden
12.00 – 12.10 Short break
NOPHO LectureChair: Thomas leth-Frandsen & Britt-Marie Frost
12.10 – 12.50 NOPHO lecture - Myriads of myeloid leukemiasAMl and alike.Henrik Hasle, Århus, Denmark

NOPHO • NOBOS 2012 29
12.50 – 13.10 Poster prize
13.10 – 13.20 Presentation of the next NOPHO 2013 conferense in KopenhagenThomas Leth-Frandsen, Copenhagen, Denmark
13.20 – 13.30 Closing timeBritt-Marie Frost, Uppsala, Sweden
13.30 Lunchbag

30 NOPHO • NOBOS 2012
Abstract Overview 2012
INVITED SPEAKERS
1. Introduction to EthicsAnders Castor, Lund, SwedenChair, NOPHO/NOBOS Working Grouop on Ethics
We encounter many ethical issues every day in our clinical praxis - many are trivial, some are more challenging, and a few are overwhelmingly difficult. Some are unique to a single patient; others are part of larger themes of difficult questions.
The NOPHO/NOBOS Working Group on Ethics is currently exploring a few such larger themes. One scenario most pediatric oncology teams recognize is the child who has failed treatment for cancer, and who faces an utterly dismal prognosis, but where there seems to be no end of possible last resort treatment options with curative (sometimes only theoretically so) potential. Should one always try to save life, as long as there is a mere theoretical chance of survival? If not, what are the relevant arguments against?
It hardly needs to be stated that scenarios like these from time to time causes divergent views between doctors and nurses. This is natural, and due to our differing professional roles. This can be good – if the differing views enrich our care. It can also be very bad, if it leads to conflict and ethical frustration. The conflicts can be defined and explored, and ways to handle them can be developed.
For the person at the center of dilemmas like these, the child; what do we tell them? How do we tell them? Who should tell them what (doctors, nurses, parents)? What do they need to be told?
One thing, however, is to come up with ideas concerning general themes, but quite another is to try to apply them to real cases. How can we go about doing that?
This introductory session aims at showing two different ways of practically tackling ethical dilemmas in the clinic: one is to involve an external ethical committee; another is to try a structured ethical discussion within the team. The methods have their strengths and weaknesses, and they are in no way mutually exclusive.

NOPHO • NOBOS 2012 31
2. Can clinical ethics committees be useful for clinicians?
Reidun Førde, Centre for medical ethics, University of Oslo, Norway
Medicine is increasingly complicated and value issues are integrated in every inch of the practice. At the same time, arenas to reflect and discuss are often lacking. Cultural heterogenity, increased patient autonomy and team work increase risk of conflicts around ethically challenging decisions. End of life decisions in child oncology may be particularly challenging, emotionally and ethically.
In Norway clinical ethics committees (CEC) have existed since 1996. To-day all health care trusts are obliged to have a CEC. These are multiprofessional committees often strengthened with legal and ethical competency, and many also have a lay member / patient representative.
In this lecture the work of these committees will be described, and examples will be given consisting of dilemmas related to child cancer. The most important role of CEC is to secure a good decision making process in which the value issues at state are illuminated and the interests and values of all relevant stakeholders are taken into consideration.

32 NOPHO • NOBOS 2012
3. Where is the child? – Navigating the intersection between pain and hopes of cure Mats Hansson, Centre for Research Ethics & Bioethics, Public Health and Caring Sciences, Uppsala University, Sweden
lisa is four years old. She was diagnosed with a Neuroblastoma 28 months ago. The tumour has resisted all kinds of treatment and there is no hope for cure at this stage. The tumour has started spreading with metastases in the bone and the liver. She is yet in no pain, and the staff experiences lisa as a happy, social and active young girl. They wish that lisa could be home for a while and visit her friends at the nursery school. lisa has a wonderful family supporting her and hoping for cure, even though they have been informed that the prognosis is very poor. At this stage the doctors are discussing a new experimental therapy aiming at tumor reduction by depositing beads, saturated with cytostatics, into tumor blood vessels. It will not affect the prognosis but may add a short period of life for lisa. What should be done and how? The parents are listening for any signs of cure and their hope for lisa is the last thing they will surrender. On the other hand, with metastases to the bone pain is expected to increase and if loosing a child is a tragedy for any parent, to see one’s beloved in severe pain is unbearable. And where is lisa in all this, what does she want? Keywords: Children, participation, communication, ethics

NOPHO • NOBOS 2012 33
4. New initiatives to improve quality of life for childhood cancer survivors: e-mental health interventions Martha Grootenhuis, Pediatrics University of Amsterdam, Pediatric Psychology, The Netherlands
E-Health is defined as the delivery of health services and information through the internet and related technologies. E-mental health (EMH) concerns the use of internet in mental health to prevent and treat mental health problems. For children the use of the computer and internet is part of their daily life. For these reasons we believe that EMH applications are also of great value for children especially because preventive interventions are necessary]. During this presentation two initiatives to improve quality of life of childhood cancer survivors using the internet are presented using patient reported outcomes (PrOs) in clinical practice and an online psycho-educational group. Health related Quality of life (HrQOl) questionnaires are increasingly used in clinical practice. These Patient reported Outcomes (PrOs) are provided to the paediatrician to facilitate communication with patients during a consultation. Currently, the use of PrOs in daily clinical practice is very time consuming and often has logistical problems. The use of a web-based programme can overcome these problems and contributes to an improved use of PrOs in clinical practice. We therefore developed an easily accessible website (www.hetklikt.nu) for outpatient treatment and a training programme for paediatricians to maximize the effectiveness and the practical use of PrOs. Based on positive experiences with the use of the KlIK PrOfile acquired during studies with children with cancer (Qlic-On study and children with JIA we conclude that the KlIK PrOfile contributes to systematically monitoring and discussing HrQOl issues during consultations. The development and implementation of the KlIK PrOfile will be presented during the symposium, as well as opportunities for systematic monitoring and screening of neuropsychological problems for CNS survivors. Considering the adverse effects of childhood cancer treatment, there is need for disease-specific psychosocial interventions for survivors of childhood cancer. A face-to-face psycho-educational group intervention (Op Koers) was developed, aimed at empowerment of survivors of childhood cancer by teaching disease-related coping skills. The program improved disease-related skills and psychosocial outcomes. An online psycho-educational group intervention could be an efficient way to reach more survivors. This online group chat-intervention has now been developed, in corporation with the Trimbos Institute, and is available on www.opkoersonline.nl. Experiences with the intervention and content will be presented. Keywords:

34 NOPHO • NOBOS 2012
5. Hodgkin lymphoma: A paradigm for the study of late effects of cancer Hamish B. Wallace, Royal Hospital for Sick Children, United Kingdom
The cure rates of first line treatment for classical Hodgkins lymphoma in children are very high with modern chemotherapy, often used in combination with involved field radiotherapy. The most effective regimens achieve cure rates in excess of 90% for early stage and 80% for advanced stage disease. Paediatric paradigms for primary treatment have evolved to reduce late effects whilst maintaining excellent cure rates, achieved by developing chemotherapeutic regimens that minimize late toxicity, and where rT is given at a low dose (20-25Gy). Chemotherapy is allocated using a risk adapted approach utilising prognostic factors associated with primary treatment failure and response to chemotherapy is under study in the current Euronet trial to guide either the final number of chemotherapy cycles or to limit or remove rT in patients who achieve complete remission with chemotherapy alone. The challenge is to continue to cure at least 90% of patients while minimising exposure to rT and gonadotoxic chemotherapy. radiotherapy causes both ovarian and uterine damage. There are no reports of uterine damage after chemotherapy. Uterine damage manifest by impaired growth and blood flow is a likely consequence of radiation to a field that includes the pelvis. Exposure of the pelvis to radiation is associated with an increased risk of miscarriage, mid-trimester pregnancy loss, preterm birth and low birth weight. As a result of increasing survival fertility preservation has become a major issue for the young patient about to start treatment for cancer. In this lecture I will discuss who is at risk and what can be done for these young patients. Female fertility preservation provides significantly different challenges to that for the male. Embryo freezing is now an accepted and well-established procedure in many centres, but is not available for children who do not have a partner. Cryopreservation of mature oocytes has become increasingly successful. However, for the young patient, cryopreservation of ovarian cortical tissue is extremely promising. Ovarian tissue cryopreservation has the potential advantages of preservation of a large number of oocytes within primordial follicles, it does not require hormonal stimulation when time is short, and is appropriate for the pre-pubertal girl. Disadvantages include the need for an invasive procedure, and the uncertain risk of ovarian contamination in haematological and other malignancies. Keywords: Hodgkin, radiotherapy, female fertility preservation

NOPHO • NOBOS 2012 35
6. Pediatric brain injury rehabilitation: standard of care and new directions Robert Butler, Oregon Health & Science University, Department of Pediatrics, USA
After a prolonged period of relative quiescence, outpatient brain injury rehabilitation has enjoyed a reawakening. Home based computer programs designed to improve and rejuvenate cognition are appearing on the market at a rate which parallels the development of outpatient programs during the 1980s. Now they are not just marketed to patients with a brain injury but also children with ADHD and seniors who want to stem the known natural declines in memory. These exercises are quite similar to many used two decades ago which were based on the concept of massed practice. The brain works in many ways like a big grey muscle and will think better if it is exercised. This approach was challenged back then, and it is challenged again. This talk will present models of pediatric and adult brain injury rehabilitation. A skills acquisition model will be advocated, and the importance of an extended real world team will be discussed. The introduction of problem solving skills training (PSST) to rehabilitation, within a context of metacognitive awareness, is presented as an approach that is designed to result in generalized improvement during real world challenges. Keywords: brain injury, rehabilitation, out patient programs

36 NOPHO • NOBOS 2012
7. Biology and treatment of infant ALL
Rob Pieters, Rotterdam, Netherlands
rob Pieters obtained his MSc in Human Movement Science and his MD in Medicine, both at the Free University of Amsterdam, in 1987. In 1991 he obtained his PhD at the same university for his research on drug resistance in leukemia. After finishing his training in pediatrics in 1995, he received a clinical fellowship in pediatric oncology from the Dutch Cancer Society. In 1996 he was appointed Associate Professor (UHD) in pediatric oncology/hematology at the Free University Hospital in Amsterdam.
In 1999, he accepted the position as Head of Pediatric Oncology/Hematology at the Erasmus MC-Sophia Children’s Hospital. In 2000 he was appointed as Professor in Pediatric Oncology at the Erasmus MC. In 1992, he received the Schweisguth Prize from the International Society of Pediatric Oncology for his research. He published over 400 book chapters and papers in peer-reviewed journals. He chairs the Dutch Childhood Oncology Group and is involved in many international collaborations and advisory committees on childhood cancer.
His research focuses on the role of molecular genetic abnormalities in leukemogenesis and outcome in childhood malignancies and the development of targeted therapies in childhood malignancies. Genetic and epigenetic abnormalities that are important for outcome in children with cancer are identified and their possible role in diagnostics and classification is determined. In addition, functional studies are done to develop new therapeutic strategies directed against these molecular abnormalities in childhood cancer cells. The final goal is to improve diagnostics and classification of childhood malignancies and to develop more effcetive and less toxic targeted therapies. This translational research has its main focus on pediatric leukemia, but also studies solid tumors.

NOPHO • NOBOS 2012 37
8. Cellular drug resistance in childhood leukemia – an update Gudmar Lönnerholm, Uppsala University, Childrens Hospital, Pediatrics, Sweden
Since 1995 Swedish centers have collected fresh leukemic cells for in vitro test of cellular drug sensitivity at diagnosis and relapse. Other Nordic centers joined when the NOPHO All 2000 treatment protocol was implemented. The in vitro test was added to this treatment protocol as a scientific study, not influencing treatment stratification. An update of the Nordic data will be presented, summarizing what has been learned since the project started. Several NOPHO publications have described the association between resistance to single agents and immunophenotypic or cytogenetic subgroups, supporting reports from other groups. NOPHO data show that resistance of leukemic cells can predict poor clinical outcome in intermediate and high risk All, but has less predictive power in the standard risk group of patients, characterized by late relapses. In a cohort of 85 patients, sensitivity to prednisolone and doxorubicin was found to correlate to MrD at end of induction therapy, and in a larger cohort of 230 children, sensitivity to vincristine and doxorubicin was found to add prognostic information to other known risk factors, including MrD. One important issue in the presentation will be to discuss the question of how to use the test in the future. Has it a role in clinical practice? Can it tell us important things about why patients don’t answer to therapy? Is it useful in the development and testing of new drugs? New and improved methods to test in vitro drug sensitivity will be briefly described, as well as how genetic and epigenetic methods are now used to try to understand the mechanisms of drug resistance. Keywords: childhood, leukemia, drugs, in vitro test, drug resistance

38 NOPHO • NOBOS 2012
9. Development of targeted new agents for children with cancer
Peter Adamson, Childrens Oncology Group, The Childrens Hospital of Philadelphia, USA
Advances made in the treatment of childhood malignancies over the past four decades have resulted in overall cure rates of approximately 80%. Despite these advances, several childhood cancers still have unacceptably low cure rates. Furthermore, even when treatment is successful, the acute and long-term morbidity of current therapy can be substantial. Development of targeted therapy for childhood cancer offers the prospect of more efficacious and less toxic therapeutics, but significant challenges exist in translating advances made in the laboratory or in adult cancers into the pediatric oncology realm. A significant number of monoclonal antibodies and small molecule inhibitors targeting signal transduction pathways have now completed pediatric phase 1 trials. Studies that integrate inhibitors with standard cytotoxic therapy are underway, but efficacy determinations will require an increasing number of randomized phase 2 trials to be performed. Increasing efforts to identify patient populations who may benefit from targeted therapy though biomarker research is needed.
Keywords: Signal Transduction Inhibitors Developmental Therapeutics
NOPHO • NOBOS 2012 39
10. Infectious complications in children undergoing therapy for malignancy Thomas Lehrnbecher, Johann Wolfgang Goethe-University, Pediatric Hematology and Oncology, Germany
Infectious complications are still a major cause of morbidity and mortality in pediatric patients undergoing therapy for malignancy, with therapy-induced neutropenia as the most important risk factor. In most centers, about two thirds of bacteremic isolates are Gram-positive pathogens, whereas Gram-negative organisms are isolated less frequently, but are associated with considerably higher mortality rates. Importantly, prolonged neutropenia increases the risk for invasive fungal disease. There is an ongoing debate whether and to what extent various preventive strategies may decrease the risk for infection. For example, immunomodulation with the hematopoietic growth factors G-CSF or GM-CSF ameliorates the time and/or the degree of neutropenia, but it is still unclear whether this translates into a clinical benefit. Similarly, preventive non-pharmacological strategies and prophylactic antimicrobial compounds are commonly used, but have been shown, if at all, to be effective in certain subgroups of patients only. In most neutropenic patients, fever is an important and early indication of infection, and according to current policies, the majority of febrile neutropenic children is being hospitalized and empirically treated with intravenous antibiotics. Although there is an increasing interest in strategies treating low-risk neutropenic children with fever with oral antibiotics only and/or in an outpatient setting, no available risk stratification for children has been validated in a prospective multicenter study. Similarly, the paradigm of empiric antifungal therapy in children with persistent or recurrent fever despite the use of broad-spectrum antibiotics is questioned by an increasing number of experts in the field, since the strategy of pre-emptive therapy may decrease the use of the costly antifungal drugs without increasing mortality. However, clinical trials in the pediatric population are lacking to date. Keywords: Infection – child – malignancy – prophylaxis – therapy

40 NOPHO • NOBOS 2012
11. Strategies for curative treatment and quality of life as a basis for neurosurgical treatment Pelle Nilsson, Per Enblad, Uppsala, Sweden
Neurosurgery is a cornerstone in the treatment of most tumors in the central nervous system. The quality of surgery has improved over the past decades mainly due to advances in technology related to imaging and monitoring. These advances have led to less morbidity following surgery. Parallel to this, there have also been advances in pathology with better characterisation of tumors in the central nervous system. To some extent, the advances in pathology and molecular biology have led to modifications in post surgery treatment of the patients and thereby reduced morbidity. New oncological treatments are to a great extent dependent on further developments in molecular pathology which will enable tailored treatments for specific subgroups of tumors.Until we have this knowledge, it is important to balance expectations from different specialities when discussing surgical goals. Quality of life for the patient, as well as survival, must be an essential part of all discussions concerning treatment of patients with central nervous tumors. The goals of surgery should be radical resection when we know that it can lead to cure, but it cannot be carried out at any cost to the patient. The surgeon must also be willing to modify surgery so that the goal is not cuarative treatment but is instead focused on reaching the highest level of quality of life for the patient. It is also important that all other specialists involved in this care remember this when discussing treatment strategies. With reductions in post operative morbidity this may not always be the case. In many of the conditions we are faced with, reality is that we have only rudimentary knowledge of the specific tumor and its characteristics. Treatment is ultimately some kind of surgery followed by standardized oncological treatment. Until we have greater knowledge about how a specific tumor behaves we must always remember the patients quality of life when deciding the goals of our different treatment strategies.

NOPHO • NOBOS 2012 41
12. Proton radiotherapy, principles & advantages Kristina Nilsson, Uppsala University hospital, Dept. of Oncology, Sweden
Proton therapy has been more and more used for treatment of children due to more optimal dose distribution, often resulting in substantial decreased dose to risk organs and expected less side effects. The access to proton treatments is however limited worldwide, but many new centers are under construction. Most of the proton centers are constructed for experimental purpose and has limitations for radiotherapy of both adults and children. New centers are hospital based and use the latest technique for modern proton beam therapy. The presentation will include technical aspects of the proton beam and the use of protons for pediatric radiotherapy. Keywords: radiotherapy, proton, dose distribution, passive scattering, scanned beam

42 NOPHO • NOBOS 2012
13. Proton radiotherapy of brain tumors in children Beate Timmermann, Westgerman Protontherapycenter Essen (WPE), Germany
Proton beam therapy (PT) is recognized to provide highly conformal dose in addition to enable conformal avoidance of critical structures. As compared to conventional photon treatments this conformality is achieved by a comparatively small number of treatment fields limiting the normal tissue receiving small and medium dose levels. Therefore, PT was understood as a tool potentially reducing the risk for secondary malignancy induction as well as for late effects. As children are particularly sensitive to radiation injury, children seem to be the cohort taking the most benefit from this technique. Today, local CNS treatment is the most common to be offered to the pediatric cohort in Europe and in US beside local sarcoma treatment. PT allows target coverage while minimal dose spread to normal brain tissue next to the target. Therefore sparing of the immature brain will be optimized. It is suggested from early reports, that secondary cancer incidence may be reduced by 50% when using PT. Another abstract was published regarding brain tumors in children evaluating neurobehavioral functioning showing stable doing after PT. At the Paul Scherrer Institute quality of life (Qol) analyses were performed again suggesting unchanged Qol after PT. However, Qol seems to be affected significantly already before starting PT by either tumor or pre-radiation treatments in the very young. In conclusion, PT should be explored especially in the pediatric cohort; however, all pediatric programs should be accompanied by prospective evaluations of late effects and Qol to gather more information on optimal use of PT. Keywords: proton therapy, children, brain tumors

NOPHO • NOBOS 2012 43
14. The Skandion Clinic - a Scandinavian centre for radiation therapy with proton beams Anders Montelius, The Skandion Clinic , Sweden
The Skandion Clinic is the first clinic for proton therapy in Scandinavia. Proton therapy makes it possible to treat cancer more effectively and with fewer side effects than with conventional radiotherapy. With proton therapy, the risk of damage to healthy tissues is minimised. The method can be applied for most common types of cancer and offers advantages when treating tumours close to radiosensitive tissues. Since less dose is deposited in non-target tissues, the risk of developing a new, radiation-induced cancer later in life is significantly reduced. This is of particular importance in paediatric patients and most of the children needing radiotherapy will be offered treatment with protons. The Skandion Clinic will be located in Uppsala in close proximity to the University Hospital and will be run jointly by the seven Swedish university hospitals. This is the first time that all of the Swedish counties with university hospitals have made a joint investment in a national centre for cancer treatment. The facility will be operated under the shared governance – distributed competence principle. This means that the preparations before treatment at Skandion including imaging, immobilisation, target definition and treatment planning as well as the follow up after treatment will be done at the collaborating university hospitals. The construction was initiated in June 2011 and the first patient is expected to be treated in 2015. The clinic is designed at present for treatment of 1000 patients per year, but with an option of future expansion. In the years left before clinical start, a number of issues need to be solved to make the best and optimal use of the distributed competence. The participating hospitals will need to educate and train their staff, develop clinical protocols and studies and in addition a number of logistic issues need to find the best solution. Keywords: Proton therapy, paedriatric patients, distributed competence


NOPHO • NOBOS 2012 45
Free PapersOrAl

46 NOPHO • NOBOS 2012
O1 SUPPORTIVE CARE
O1. When there is no chance of cure – where does palliation start and treatment end? Li Jalmsell, Uppsala Univeristy, Centre for Research Ethics & Bioethics, Sweden
Objective: In this study we aimed to gather information on the transition from curative to palliative care for Swedish children suffering from a malignancy. Method: Data was gathered from medical records of 95 children (59% of the eligible 159 children) dying from a malignancy between 2007 and 2009 with the focus to identify when transition from curative to palliative care took place, treatment-intensity the last two weeks of life, weather there was a written do-not-resuscitate decision and place of death. Differences in diagnosis were studied. results: 83 children (87% of children studied) were found to be in palliative care at time of death. The palliative phase ranged from the last day of life to a period of over 4 years. The median length of the palliative phase was approximately two months, being shorter for children suffering from hematological malignancies and longer for children suffering from brain-tumors. Children with hematological malignancies were also seen to have had a higher treatment intensity the last few weeks of life, e.g. been given chemotherapy, transfusions and antibiotics. No cardiopulmonary resuscitation was performed in any of the children being in palliative care, although there was only a written do-not-resuscitate decision for 45 (54%) of these children. Conclusions: We found the palliative phase of children with malignancies to be approximately two months. Children with hematological malignancies were generally treated more aggressively than others towards the end-of-life, being given antibiotics, transfusions and/or chemotherapy the last two weeks of life. In relation to this they also had a shorter palliative phase. A DNr-order was only present in 54% of children being in palliative care, although it was often understood that no cardiopulmonary resuscitation should be performed. Keywords: end-of-life, palliative phase, treatment, DNr Authors: Authors: li Jalmsell1 (presenting), Martin Forslund, Ulrika Kreicbergs2, Jan-Inge Henter2, Mats G. Hansson1 & Britt-Marie Frost3 1Centre for research Ethics & Bioethics. Uppsala University, Uppsala, Sweden, 2Department of Women and Child’s Health, Karolinska Institutet, Stockholm, Sweden, 3Department of Paediatrics, University Hospital of Uppsala, Uppsala, Sweden

NOPHO • NOBOS 2012 47
O2-3 EPIDEMIOLOGY
O2. Is there a decrease in survival rates after reduction of therapy? A population based study of children with Hodgkin lymphoma Charlotte Hopstadius, Department of Women´s and Children´s Health, Pediatric Hematology and Oncology, Sweden
Introduction/aim: Due to the treatment of Hodgkin lymphoma in children that has developed over the years, survival is excellent, but reported late effects of the disease and treatment have resulted in an intense work to find protocols that maintain the good survival rates but diminish the late effects. The aim was to investigate incidence, sex ratios, sub classifications, stages, treatment, relapse, survival and whether the decrease in treatment has resulted in a decline in overall survival (OS). Patients and methods: This work is based on information about 334 children, 0-17 years, among those 200 0-14 years, that were diagnosed with Hodgkin lymphoma (Hl) 1985-2009 and registered in the population based Swedish Childhood Cancer registry, with an average follow up time of 11.6 years (0-25.5 years). results: We found that the incidence is 0.5/100 000 children and sex ratio M/F= 1.65 (0-14 years), but the ratio changes with age. The frequencies of different subgroups are nodular sclerosis 68%, mixed cellularity 15%, nodular lymphocyte rich Hl 13%, lymphocyte depleted 1% and unknown Hl, 3%. 72% are diagnosed in early stages (I or II), only 10% in stage IV, and 34% are diagnosed with B-symptoms. 65% of the children have received radio therapy. 5 and 10 year OS are 0.97±0.01 and 0.96±0.01 respectively which is comparable to results from earlier protocols. Among those with relapse of disease 5 and 10 year OS are 0.84±0.07 and 0.79±0.08. Conclusion: There is no decrease in OS after reduction of treatment over the years. Keywords: Hodgkin lymphoma, survival, reduced treatment, epidemiology, children Authors: Charlotte Hopstadius, Annika Englund, Göran Gustafsson, Gustaf ljungman

48 NOPHO • NOBOS 2012
O3. Changes in patient survival of childhood solid tumors diagnosed 1985-2010 in the Nordic countries. Milada Cvancarova Småstuen, Cancer Registry of Norway, Registration, Norway
Background Classification of childhood solid tumours differs greatly from tumours diagnosed in adults. Thus establishment of childhood cancer registries is essential to monitor changes and progress in cancer care. Methods Status registrations were made partly from national population registries and partly from death registries only, as conditions differ between countries. Crude 5-year survival was modelled using the Kaplan-Meier method stratified by selected diagnostic groups, age groups and diagnostic period (diagnosed 1986-1995 and 1996-2010). The crude estimates were compared with log-rank tests. results In total, 12343 children <15 yrs of age were diagnosed with cancer during 1986-2010 in the Nordic regions (Denmark, Finland, Iceland, Norway, Sweden) and classified according to Birch & Marsden classification. Data were collected at the NOPHO solid tumour registry located at the Cancer registry of Norway. Children in the youngest age group 0-4.99 years at diagnosis had statistically significantly worse 5-year survival than the oldest ones. This might partly be due to a slightly worse prognosis for infants . The highest 5-year survival was reached by non-Hodgkin pts diagnosed 1996-2010: 88.3%, 95% CI [85.3 to 90.6] % which was significantly higher than 5-year survival for those diagnosed 1985-1995: 81.3%, 95% CI [77.0 to 84.8]%. There was a significant increase also for survivors of neuroblastoma: 71.1%, 95%CI[66.9 to 74.9]% vs 55.3%, 95%CI[50.4 to 60.6]%, and Ewing’s sarcoma: 78.6%, 95%CI[79.5 to 85.3]% and 61.4%, 95%CI [47.5 to 72.6]%, for those diagnosed 1985-95 and 1996-2010, respectively. There were no statistically significant changes in 5-year survival between the two diagnostic periods for pts diagnosed with Hodgkin lymphoma, retinoblastoma, Wilm’s tumor, hepatoblastoma, hepatocellular carcinoma, chondrosarcoma, soft-tissue sarcoma, non-germ cell. and other gonadal neoplasm and other unspecified carcinoma. Conclusions There has been some improvement in 5-year survival for those diagnosed after 1996 with the greatest improvement for survivors of non-Hodgkin lymphoma and neuroblastoma. Keywords: 5-year survival by diagnostic periods (1986-1995 and 1996-2010)
Authors: Milada Cvancarova, Jan Nygård, Hilde lie Koch, Olafur G. Jonsson, Henrik Schroder, Mikko Perkkio, Goran Gustafsson, Finn Wesenberg, on behalf of the Nordic Society of Paedric Haematology and Oncology

NOPHO • NOBOS 2012 49
O4-6 CANCER TREATMENT
O4. Standard risk Medulloblastoma in Europe: studies completed and planned Birgitta Lannering, , Pediatric Hematology-Oncology, Sweden
Background: The primary aim of the HIT-SIOP PNET 4 study was to compare in a randomized study hyperfractionated (HFrT) and conventional rT (STrT) with respect to survival and late effects. The second aim was to collect tumour material from a large uniformely treated group of patients to study biological markers for future risk grouping. Patients over 4 years with standard risk Medulloblastoma (M0) where randomised to craniospinal HFrT 1.0 Gy twice daily or STrT 1.8 Gy daily. Therafter chemotherapy with Cisplatin, CCNU and Vincristine was given in 8 courses. result: Between 2001 and 2006, 338 patients were included from over a hundred different centres in Europe. randomisation assigned 169 patients to each treatment arm. Central review of pathology and neuroradiology was performed. Median follow up for children in remission is 4.8 years. Sixtysix pts have relapsed. EFS at 3 and 5 years FU is 0.83± 0.02 and 0.79 ±0.02 with no significant difference between the two arms. Patients with a residual tumour > 1.5cm2 had a significantly increased risk for relapse as had children with prolonged delay between surgery and rT. Complete analysis of the whole set of biological markers planned was achieved in 50 %. Beta-catenin nuclear accumlulation and 17pq aberrations were the most predictive biological markers for prognosis. Conclusion: In this true multiinstitutional study EFS and OS was excellent. risk grouping for the upcoming studies PNET 5 and 6 will be based on biological markers analysed on fresh tumour material before inclusion as well as on clinical staging. Conventional rT remains the golden standard of treatment in this disease but some dose reductions will be adopted in the next studies. Keywords: brain tumour, radiotherapy, biological markers Authors: Birgitta lannering, Göran Gustafsson for the PNET group of SIOP-Europe.

50 NOPHO • NOBOS 2012
O5. Vascular Endothelial Function in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia: Effects of a Home-Based Exercise Program Liisa Järvelä, Turku university hospital, Department of Pediatrics, Finland
Sedentary lifestyle, obesity, insulin resistance, and other cardiometabolic risk factors are among the most often reported concerns in long-term survivors of childhood All. The role of endothelial dysfunction in the development of metabolic syndrome and cardiovascular disease in cancer survivors has also been discussed. It has been suggested that chemotherapy (e.g. anthracyclines and methotrexate) may cause direct endothelial damage, potentially increasing the significance of endothelial dysfunction in the development of metabolic and cardiovascular late effects in former cancer patients. We studied endothelial function and traditional cardiometabolic risk factors before and after a home-based exercise intervention in long-term survivors of childhood All. Twenty-one 16 to 30 year-old childhood All long-term survivors took part in a cross-sectional study, and 17 of them participated in a home-based exercise intervention. The median time since diagnosis was 15.9 years (range 11.3–21.4 y), and all the participants were in first continuous remission without BMT. Vascular endothelial function and metabolic risk factors were studied before and after the intervention. At baseline, brachial artery flow mediated dilation (FMD) was lower in the survivors than controls at the 40 second time point (p=0.01). In male survivors, the maximal FMD (p=0.01) and FMD area under the curve (p=0.01) were also poorer than in controls. FMD at 40 second time point (p<0.01), fasting plasma insulin (p<0.01), HOMA-Ir (p<0.01) and waist to hip ratio (p<0.01) improved during the exercise intervention. Poorer endothelial function was found in All survivors, compared to controls. The difference was more pronounced in male survivors. In addition to improvements in traditional cardiometabolic risk factors, endothelial function in All survivors improved with exercise. These findings emphasize the importance of physical activity in All survivors. We suggest that childhood All survivors should be encouraged to physical activity, and exercise programs should be aimed at this population. Keywords: acute lymphoblastic leukemia, cardiometabolic risk, endothelial function, late effect, physical activity Authors: liisa S. Järvelä, Harri Niinikoski, Päivi M. lähteenmäki (presenting author), Olli J. Heinonen, Mikko Arola, Jukka Kemppainen

NOPHO • NOBOS 2012 51
O6. Presentation of the “Multinational EuropeanTrial for Children with the Opsoclonus Myoclonus Syndrome (OMS)” Ingrid Øra, Skåne University Hospital, Lund University, Peditric Oncology and Hematology, Sweden
BACKGrOUND: OMS is a rare syndrome characterized by opsoclonus (rapid multi-directional eye movements), ataxia, myoclonus, and associated with irritability. Affected children are between 1 and 3 years of age. No exact data on incidence and co-occurrence with neuroblastoma exists, although 50-80% are reported with neuroblastoma. An immune-mediated mechanism of a cross-reactive autoantigen responsible for the symptoms of OMS is supported by the abnormalities in the cerebral spinal fluid IgG-index and response to immunosuppressive treatment, such as steroids or immunoglobulins. The neuroblastoma is mostly of low stage and treated by surgery only but the majority of the children experience long-term neurological deficits regarding cognitive, behavioural, and motor development. TrIAl AIMS: 1) To prospectively evaluate the response to the treatment schedule (see below); 2) To determine the percentage of neuroblastoma-associated OMS in a patient cohort investigated according to the uniform guidelines given in this trial; 3) To prospectively address the neurological and neuropsychological outcome with standardized evaluation of neurological deficits with a special focus on the long-term outcome; 4) To build up a European network involving peadiatric oncologists, neurologists, and psychologists involved in medical care of patients with OMS with the major aim of improving knowledge of the disease. STUDY DESIGN: All patients will undergo standard diagnostics for neuroblastoma and if detected, treated according to appropriate neuroblastoma trial. For OMS patients, treatment with dexamethasone pulses will immediately be initiated. A standardized scoring system of OMS symptoms will, after three months of treatment, determine whether intensification with cyclophosphamide pulses should be given. After additional three months, the scoring will determine whether a second escalation with rituximab is indicated. CONClUSION: An international collaboration is required to improve the knowledge, the treatment, and the outcome in OMS whose major challenges are the neurological sequelae. The trial is scheduled to open during autumn 2012. Keywords: Opsoclonus Myoclonus Syndrome, clinical trial, incidence, treatment, neurological sequele Authors: Ingrid Øra, national coordinator for Sweden and member of the Study Committee.

52 NOPHO • NOBOS 2012
7-8 SUPPORTIVE CARE
O7. Procalcitonin for Detection of Infection – a Hope or a Hype? A cohort study of immunosuppressed children Cecilie Rutkjær Jensen, Department of Pediatrics, Aarhus University Hospital Skejby, Denmark
Children with malignancies often develop febrile illness after chemotherapy. Diagnosis of bacterial infection and prompt initiation of the correct antibiotic therapy are essential. A prospective cohort study was conducted (November 2009 to October 2010) to assess the value of plasma levels of procalcitonin (PCT) and C-reactive protein (CrP) in order to predict clinical outcome in febrile children with cancer. Plasma levels for PCT and CrP were obtained at t0 (admission) and t1 (24 hours ± 12 hours later) in all patients hospitalized with fever. Blood cultures and blood samples were collected at admission and daily until defeverescense. Febrile episodes were classified as fever of unknown origin (FUO), local infection or bacteremia. Of the 252 febrile episodes 18% were classified as bacteremias and 35% as FUO. In a multivariate regression analysis PCT≥ 0.5 ng/ml was a significant risk factor for bacteremia contrary to CrP ≥ 50 mg/l. Using ≥ 0.5 ng/ml as cut off level for bacteremia, PCT demonstrated a high NPV: 93% at t0, 94% at t1 and a relatively high sensitivity (68% at t0; 78% at t1) and specificity (72 % at t0; 62% at t1). This was superior to CrP which at the cut off level of ≥ 50 mg/l had a NPV of 86% at t0 and 89% at t1, a sensitivity of 36% at t0 and 71% at t1 and a specificity of 63% at t0 and 40% at t1. In conclusion we found that PCT may be a better prognostic predictor of bacteremia than CrP. Keywords: infection, procalcitonin, CrP, cancer, children Authors: Cecilie rutkjær Jensen1 Mette Møller Handrup1 Henrik Hasle1 Henrik Schrøder1 1Department of Pediatrics, Aarhus University Hospital Skejby

NOPHO • NOBOS 2012 53
O8. Bone marrow remission status predicts leukemia contamination in ovarian biopsies collected for fertility preservation Babak Asadi A., Oslo University Hospital- Rikshospitalet, Norwegian Resource Center for Womens Health, Norway
Cryopreservation of ovarian cortex before gonadotoxic chemotherapy and autotransplantation of the thawed tissue back to the cured patient is a potential fertility preservation method for childhood cancer patients. The most life-threatening concern is the possibility of reseeding leukemic cells with ovarian autotransplantation. In order to evaluate how the bone marrow remission status (overt leukemia n=5, molecular relapse n=2, molecular remission n=6) affects the minimal residual leukemia in ovarian samples individual leukemia specific Ig/TCr gene rearrangements or fusion gene products were measured by rQ-PCr. Ovarian samples of the 6 girls with molecular bone marrow remission for 10-30 weeks prior ovarian biopsy, showed no evidence of residual leukemia in ovarian tissue at detection level of 0.01%-0.0003%. One of the two patients with increasing levels of minimal residual leukemia in bone marrow showed evidence of disease-specific genetic marker (fusion transcript) at level of 0.001% in ovarian biopsy specimen while that of the other patient remained negative. All the ovarian samples collected at overt leukemia showed evidence of leukemia contamination at level of 0.2-57%. Conclusion: Present study demonstrates that bone marrow minimal residual leukemia status predicts leukemic cell contamination in the ovary. leukemia contamination is highly likely if ovarian tissue is collected at the time of diagnosis. Postponing the ovarian biopsy until bone marrow molecular remission has been achieved may result in less leukemic contamination in cryopreserved ovarian tissue. Whether the leukemia therapy affects the primordial follicles and their maturation capacity remains to be solved in future. Keywords: Fertility preservation, ovary, minimal residual leukemia, remission status Authors: Kirsi Jahnukainen, Helena Tinkanen, Anne Wikström, leo Dunkel, Ulla M. Saarinen-Pihkala, Sirpa Mäkinen, Babak Asadi A, Irma Oskam, Kim Vettenranta, Veli Kairisto, Tiina laine, Vesa Juvonen Presenting author: Babak Asadi A

54 NOPHO • NOBOS 2012
O9-15 LATE EFFECTS
O9. Estimated clinical benefit of protecting neurogenesis in the developing brain during radiation therapy for pediatric medulloblastoma Malin Blomstrand, Department of Oncology and Centre for Brain Repair and Rehabilitation, University of Gothenburg, Sweden
Purpose: To assess the feasibility and estimate the benefit of sparing the neurogenic niches when irradiating the brain of pediatric medulloblastoma (MB) patients based upon clinical outcome data. Pediatric MB survivors suffer a high risk of neurocognitive side-effects, often attributed to the whole-brain irradiation that is part of standard management. Neurogenesis is very sensitive to radiation and limiting the radiation dose to the hippocampus and the subventricular zone (SVZ) may preserve neurocognitive function. Materials and methods: radiotherapy plans were created using four techniques, standard opposing fields, intensity-modulated radiotherapy (IMrT), intensity-modulated arc therapy (IMAT) and intensity-modulated proton therapy (IMPT). To evaluate the potential clinical benefit of dose reduction in hippocampus and SVZ, we used recently published dose-response data from a large clinical series with long-term follow-up on neurocognitive function of pediatric patients treated with radiation. results: Mean dose (range) to the hippocampus and SVZ (average for both sites) could be limited to 88.3% (83.6-91.0%), 77.1% (71.5-81.3%) and 42.3% (26.6-51.2%) with IMAT, IMrT and IMPT respectively, while maintaining at least 95% of the prescribed dose in 95% of the whole-brain target volume. Estimated risks (95% confidence interval) for developing memory impairment after a prescribed dose of 23.4 Gy were 47% (21-69%), 44% (21-65%), 41% (22-60%) and 33% (23-44%) with opposing fields, IMAT, IMrT and IMPT, respectively. Conclusions: Neurogenic niche sparing during cranial irradiation of pediatric MB patients is feasible and is estimated to lower the risks of long-term neurocognitive sequelae. Best sparing is achieved with intensity modulated proton therapy, thus making this an attractive option to be tested in a prospective clinical trial. Key words: CNS, medulloblastoma, radiotherapy, neurocognitive sparing, risk modelling Keywords: CNS, medulloblastoma, radiotherapy, neurocognitive, risk-modelling Authors: Malin Blomstrand+, N. Patrik Brodin+, Per Munck af rosenschöld, Ivan r. Vogelius, Gaspar Sánchez Merino, Anne Kiil-Berthlesen, Klas Blomgren, Birgitta lannering, Søren M. Bentzen, Thomas Björk-Eriksson*

NOPHO • NOBOS 2012 55
O10. Identification of somatic mutations in acute lymphoblastic leukemia by whole genome sequencing Eva Berglund, Uppsala University, Medical Sciences, Sweden
Next generation sequencing technology enables detailed analysis of whole cancer genomes. With this technology, it is possible to sequence four human genomes in less than two weeks. Sequencing of protein-coding regions (exomes) and whole genomes have already been applied to different cancers, including leukemias. These studies have identified novel genes with recurrent somatic mutations, and thereby shed light on the genes and pathways involved in the development of cancer. Although functionally important mutations can occur in different parts of the genome, most studies of cancer genomes have focused on protein-coding regions. Whole genome sequencing makes it possible to detect point mutations in other genomic regions than exons, small and large copy number alterations and large structural rearrangements. We have sequenced the whole genomes of matched diagnostic and constitutional samples from four carefully selected patients with pediatric acute lymphoblastic leukemia (All) of different cytogenetic subtypes. We have identified several potentially deleterious somatic mutations in exons. In addition, we observed somatic mutations in conserved non-exonic regions that potentially have regulatory functions, copy number alterations and structural variants. To assess whether the mutations have an effect on gene expression, we also sequenced the transcriptomes for the cancer samples. We are currently studying whether the identified genes and regions are recurrently mutated in All, using additional samples collected by the NOPHO groups. Keywords: acute lymphoblastic leukemia, whole genome sequencing, somatic mutation Authors: Eva Berglund, Carl Mårten lindqvist, Behrooz Torabi, Jessica Nordlund, Niklas Henriksson, Erik Forestier, Gudmar lönnerholm, Ann-Christine Syvänen

56 NOPHO • NOBOS 2012
O11. CARDIOVASCULAR DISEASE IN ADULT LIFE AFTER CHILDHOOD CANCER IN SCANDINAVIA (ALiCCS) - A large population-based patient cohort www.aliccs.org Thorgerdur Gudmundsdottir, Danish Cancer Society Research Center, Survivorship Unit, Denmark
Introduction Major improvements of treatment resulting in a growing population of childhood cancer survivors have increased the awareness of adverse long-term sequelae of the life-saving treatments. In a large population-based study, we assessed the risk for cardiovascular disease in childhood cancer survivors, thus avoiding some of the shortcomings of previous studies. Patients and methods Hospitalizations for cardiovascular disease were evaluated in a cohort of 25,652 childhood cancer survivors and 128,243 population comparisons from Denmark, Iceland and Sweden. The nationwide cancer registries, central population registries and hospital registries were used to identify cancer patients, comparisons and hospitalizations. Survivors were diagnosed with cancer below age 20 and recruited from beginning of cancer registration in the 1940s through 2008. Cohort members were followed-up individually for cardiovascular diseases through register linkages. Hospitalization rate ratios (Hrrs) for selected cardiac outcomes in survivors were calculated using a Cox proportional hazards model with population comparisons as referent. results Preliminary results show that survivors were significantly more likely to be diagnosed with ischemic heart disease (Hrr 1.63, 95% CI 1.44-1.84, based on 308 survivor cases), heart failure (Hrr 3.71, 3.36-4.09; 596 cases), cardiomyopathy (Hrr 1.67, 1.50-1.87; 389 cases), valvular abnormality (Hrr 4.25, 3.56-5.08; 190 cases) and cerebrovascular incidents (Hrr 2.36, 2.04-2.73; 240 cases) than comparisons. In general the highest risk was observed among survivors diagnosed in the age group 0-10 years, the most recent treatment period and in those with leukaemia and lymphoma. The probability of being hospitalized for cardiovascular diseases continued to be higher among survivors than comparisons in the total follow-up period even >30 years since diagnosis. Conclusions Survivors of childhood cancer are at substantial risk for cardiovascular disease compared to the general population. Awareness of this excess risk is important for clinicians and the growing survivor population, and essential for optimizing patient follow-up and counselling. Keywords: Childhood cancer, late complications, cardiovascular diseases, hospitalizations, clinical epidemiology Authors: Thorgerdur Gudmundsdottir, MD, Jeanette Falck Winther, MD, Klaus Kaae Andersen, MSc, PhD, Henrik Hasle, Professor, MD, PhD, Jørgen H Olsen, MD, DMSc, on behalf of AliCCS.

NOPHO • NOBOS 2012 57
O12. Neurocognitive function in very long-term survivors of acute lymphoblastic leukemia treated with chemotherapy only Adriani Kanellopoulos, Oslo University Hospital, Rikshospitalet, Department of pediatrics, Norway
Objective: There is a concern regarding cognitive late effects after treatment for acute lymphoblastic leukemia (All). After prophylactic cranial irradiation with its detrimental effects on intellectual function and learning ability has been largely abandoned, potential neurotoxic effects of CNS-directed intrathecal and systemic chemotherapy are receiving increasing attention. The aim of the current study was to assess neuropsychological function in a cohort of very long-term All survivors (lTSs) treated with chemotherapy only. Patients and Methods: This survey is part of a Norwegian cross-sectional follow-up study on lTSs of childhood All diagnosed 1970-2002 at age <16 years. One-hundred and twelve lTSs treated with chemotherapy only and 130 healthy controls matched for age, gender and IQ were administered a neuropsychological test battery focusing on speed of information processing, verbal learning and memory, executive functions and working memory. Treatment details were obtained from the medical records. results: Median age at diagnosis was 5.2 years (range 0.3-15.9), median follow-up time 22.0 years (range 7.4-40.0). Twenty-four (23%) of the lTSs had been treated before 1980. Compared to controls, lTSs scored significantly lower on all neurocognitive domains, especially speed of information processing, executive function and working memory (p<0.001, effect sizes 0.78-1.35). However, we did not find any association between neuropsychological performance and cumulative doses of cytotoxic drugs (high-dose or intrathecal methotrexate, steroids, vincristine), age at diagnosis, gender or follow-up time. Conclusions: In our study, lTSs of childhood All treated exclusively with chemotherapy showed significantly poorer neuropsychological performance in all tested domains compared to age-, gender- and IQ-matched controls, but we did not identify any demographic or treatment-related associations. The clinical impact of our observations remains to be clarified. Keywords: Childhood cancer survivor, acute lymphoblastic leukemia, late effects, CNS-directed chemotherapy, neurocognitive function Authors: Adriani Kanellopoulos (presenting author), Stein Andersson, Bernward Zeller, Anders Fjell, Kristine Walhovd, Sophie D. Fosså and Ellen ruud

58 NOPHO • NOBOS 2012
O13. ENDOCRINE LATE EFFECTS IN CHILDHOOD CANCER SURVIVORS. Under the research program “Adult Life after Childhood Cancer in Scandinavia (ALiCCS)” (www.aliccs.org) Sofie de Fine Licht, Danish Cancer Society Research Center, Survivorship Unit, Denmark
Introduction With the remarkable improved survival of childhood cancer, late effects of the cancer and its treatment become more apparent. Using the unique population-based registries in the Nordic countries with long-term and virtually complete follow-up, we investigated if childhood cancer survivors were at increased risk of endocrine late effects compared to the general population, thus avoiding some of the shortcomings of previous studies. Methods We identified 25,652 children from Denmark, Iceland and Sweden diagnosed with cancer before the age of 20, from the beginning of cancer registration in the 1940s through 2008, who were alive at the start of the hospital registries (Denmark 1977, Iceland 1999 and Sweden 1964). A population comparison cohort of 128,243 individuals, matched by gender, country and age, were randomly selected from the central population registries. Study subjects were followed-up for endocrine disorders in the national hospital registries, which include all hospitalizations. Cox proportional hazard models were used to estimate hospitalization rate ratios (Hrr) of endocrine late effects in childhood cancer survivors compared to the population cohort members. results Preliminary results show that survivors of childhood cancer are at increased risk of a broad range of endocrine disorders compared to the population comparison cohort. Crude estimates show an increased risk of hypothyroidism (Hrr=7.89, 95% CI:7.04-8.84), hyperthyroidism (Hrr 1.52, 1.24-1.86), diabetes mellitus (Hrr 1.95, 1.75-2.17), hypoparathyroidism (Hrr 11.95, 6.63-21.54), hyperparathyroidism (Hrr 5.48, 3.94-7.61), pituitary hypofunction (Hrr 69.36, 57.34-83.91), pituitary insufficiency (Hrr 11.59, 9.09-14.78), adrenocortical diseases (Hrr 19.23, 14.61-25.32), ovarian dysfunction (Hrr 3.58, 2.99-4.29) and testicular dysfunction (Hrr 28.24, 20.13-39.63). rate ratios adjusted for age at diagnosis and year of treatment will be presented. Conclusion Preliminary results show that childhood cancer survivors are at highly increased risk of endocrine late effects, which is important knowledge for optimizing treatment protocols, with fewer late effects and continuing high survival rates. Keywords: Childhood cancer, late effects, endocrine disorders, hospitalizations, clinical epidemiology. Authors: Sofie de Fine licht, MSc, Jeanette Falck Winther, MD, Klaus Kaae Andersen, MSc, PhD, Henrik Hasle, Professor, MD, Jørgen H Olsen, DMSc on behalf of AliCCS

NOPHO • NOBOS 2012 59
O14. Reduced cerebral volumes in long term survivors of childhood lymphoblastic leukemia (ALL) Bernward Zeller, Oslo University Hospital, Pediatric Medicine, section for oncology/hematology, Norway
Background: During the last two decades, CNS-irradiation has largely been abandoned in the treatment of All, mainly due to CNS-related long term effects. At the same time, it has become evident that even chemotherapy alone is associated with an increased risk of neurocognitive impairment. New neuroimaging techniques may enhance our understanding of CNS late effects. The aim of our study was to investigate cerebral volumes of long term survivors compared to healthy controls. Methods: 130 (65 female, 65 male) survivors from childhood All diagnosed between 1970 and 2002 at an age of < 16 years were investigated with cerebral MrI and neuropsychological testing 23 (7-40) years after diagnosis. Mean age was 29 (18-46) years. Only 18/130 had received cranial radiation treatment with a dose of 20 (12-25) Gy. Morphometric analyses including whole-brain segmentation were performed with a well-validated semi-automated procedure (FreeSurfer). 130 healthy adults, matched on age, gender and IQ, without history of previous cancer served as controls. results: Compared to healthy controls, All survivors showed significantly reduced total brain volume and reduced volumes of a number of anatomical regions, including cerebral cortex, white matter, thalamus, caudate, hippocampus and amygdala. The most pronounced effect was found for caudate, which on average was 5.2 % smaller in All survivors. In All survivors, no association could be found between grade of volume reduction and disease or treatment characteristics. In particular, neither radiation therapy, total dose of methotrexate (MTX), nor number of intrathecal MTX injections were associated with neuroanatomical volumes. Conclusions: Structural MrI of long term survivors from childhood All demonstrated reduced volumes of total brain and several specific brain structures compared to healthy controls. Both etiological mechanisms and significance of these findings require clarification in future studies. Keywords: Volumetry, brain, acute lymphoblastic leukemia, MrI, childhood Authors: Bernward Zeller, Christian K Tamnes, Inge Amlien, Stein Andersson, Paulina Due-Tønnessen, Anders Fjell, Adriani Kanellopoulos, Kristine Walhovd, Ellen ruud.

60 NOPHO • NOBOS 2012
O15. The Association of Late Effects to Different Conditioning Regimens and Previous Leukaemia Treatment after Paediatric Allogeneic HSCT Mari Wilhelmsson, Karolinska University Hospital, Department of Pediatrics, Sweden
Nearly all children treated with HSCT will experience at least one late effect. The aim of the study was to compare remission status prior to HSCT (Cr1 vs. Cr2 or higher among leukaemia patients) and the different conditioning regimens (single dose total body irradiation (sTBI), fractioned TBI (fTBI), chemotherapy with busulfan (B), chemotherapy without B) in the entire material including leukaemias and other diagnoses and their association to the chronic sequelae. Medical records of children (1-18 years) who underwent allogeneic HSCT in Huddinge and Helsinki from 1980 to 2000 surviving at least 7 years after transplantation (n=174) were retrospectively reviewed. When comparing Cr1 versus Cr¡Ý2, no differences were found in the need of hormonal substitution (thyroxin: 51% vs. 49%, growth hormone: 43% vs. 51%, estrogen: 43% vs. 52%, testosterone: 41% vs 59%, respectively). The type of conditioning regimen had a significant impact on the need of substitution with thyroxin (sTBI 67% vs. fTBI 31%), growth hormone (sTBI 65% vs. fTBI 32%) and estrogen (B 67% vs. chemo without B 10%) while no significant differences in hormone substitution were detected between B and TBI. Significantly higher numbers of non-hormonal chronic conditions graded according to CTCAE v3.0 were detected when comparing sTBI vs. fTBI and B vs. chemo without B but not B vs. TBI (0 CTCAE conditions: sTBI 4%, fTBI 21%, B 5%, chemo w/o B 30%; >3 CTCAE conditions: 63%, 36%, 43%, 5% respectively). No association between remission status at HSCT and number of CTCAE conditions was detected. Conclusions: It is mainly the type of conditioning regimen at HSCT and not the previous leukaemia treatment that determines the chronic sequelae of the survivors. Both hormonal and other chronic sequelae were more common after sTBI vs. fTBI. The morbidity associated with busulfan did not significantly differ from the TBI associated morbidity. Keywords: Allogeneic HSCT, TBI, busulfan, Cr, chronic sequelae. Authors: Mari Wilhelmsson, Anu Vatanen, Birgit Borgström, Britt Gustafsson, Mervi Taskinen, Ulla M. Saarinen-Pihkala, Jacek Winiarski, Kirsi Jahnukainen. The presenting author:Mari Wilhelmsson

NOPHO • NOBOS 2012 61
O16-18 TRANSLATIONAL RESEARCH O16. Pharmacogenetically based dosing of thiopurines in childhood acute lymphoblastic leukemia – influence on cure rates and risk of second cancer Elisabeth Ørskov Sørensen, Rigshospitalet, Department of Pediatrics, Denmark
The response to 6-mercaptopurine (6MP) in childhood acute lymphoblastic leukemia (All) is influenced by the activity of the enzyme thiopurine methyltransferase (TPMT). In the NOPHO All-92 protocol patients with low TPMT activity (TPMTlA) had a reduced risk of relapse compared to TPMT wild-type (TPMTWT) patients (7% vs. 18%; P=0.03), but also an increased risk of developing a second malignant neoplasm (SMN) (6% vs. 2%, P=0.06). All patients received a 6MP starting dose of 75 mg/m2/day when entering maintenance therapy. The average tolerable 6MP dose during maintenance therapy was only 50 mg/m2/day for TPMTlA patients and the dose of 6MP was positively related to the risk of SMN. Thus, in order to reduce the risk of SMN the 6MP starting dose was reduced to 50 mg/m2/day for TPMT heterozygous patients in the NOPHO All2000 protocol. Of 1020 children treated by the NOPHO All2000 protocol, 723 had their TPMT genotype determined (660 TPMTWT, 62 TPMT heterozygous (8.6%), 1 TPMT deficient (0.1%)). The median 6MP starting dose was 50.0 mg/m2/day (50% range, 46.3-60.2) for heterozygous patients. The risk of SMN did not differ between TPMTWT and TPMTlA patients (1.1%±0.5% vs. 2.5%±2.5%; P=0.41). The only TPMTlA patient who developed an SMN received a 6MP starting dose of 75.8 mg/m2/day. The risk of SMN was significantly increased for standard risk patients compared to higher risk patients (2.4%±0.9% vs. 0.2%±0.2%; P=0.007). There was no difference in the risk of relapse between TPMTWT and TPMTlA patients (17.9%±1.9% vs. 19.5%±5.8%; P=0.65). This study indicates that reduced intensity of 6MP dosage may reduce the risk of SMN for TPMTlA patients but leads to an increased risk of relapse. Strategies are needed to identify TPMTlA patients at risk of SMN and reduce their starting 6MP dosage, while treating the remaining TPMTlA patients with starting 6MP doses of 75 mg/m2/day. Keywords: Acute lymphoblastic leukemia, 6-mercaptopurine, thiopurine methyltransferase, relapse, second malignant neoplasia Authors: Elisabeth Ørskov Sørensen, Mette levinsen, Jacob Nersting, Arja Harila-Saari, Olafur G. Jonsson, Anne-Grete Bechensteen, Jonas Abrahamsson, Stefan Söderhäll, Kjeld Schmiegelow

62 NOPHO • NOBOS 2012
O17. Age-Dependence of Tumor Genetics in Unfavorable Neuroblastoma Fredrik Hedborg, Uppsala University, Department of Womens and Childrens Health, Sweden
Purpose Aggressive neuroblastoma remains a therapeutic challenge. Here, we have addressed the genetic heterogeneity of this important clinical entity. Patients and Methods Whole-genomic BAC and SNP array platforms were used to generate DNA copy number profiles from 34 high-risk or lethal outcome neuroblastomas consecutively collected in Sweden. The age-dependence of MYCN amplification (MNA) status of such tumors was studied via the Swedish Childhood Cancer registry. results The analyses revealed MNA or segmental 11q loss in 28/34 tumors, aberrations that were mutually exclusive, except for two tumors. At diagnosis, children with MNAnot11q- tumors were significantly younger than those with 11q-notMNA tumors; mean: 27.4 vs. 69.5 months (p=0.008; n=14/12) and MNAnot11q- tumors displayed fewer additional segmental chromosomal aberrations than 11q-notMNA tumors; mean: 5.5 vs. 12.0; p<0.001. Among 11q-notMNA tumors the number of segmental aberrations correlated positively with age at diagnosis (Pearson Correlation 0.606; p=0.037). Among tumors without MNA and segmental 11q loss (n=6) one tumor displayed amplicons on 11q and 12q and three others bore evidence of progression from lower risk tumors. The early presentation of MNA neuroblastomas was confirmed from independent registry data, showing an average age at diagnosis of 29.2 months for cases not included in the present study (n=43). Conclusion MNA and 11q loss define two major genetic variants of unfavorable neuroblastoma with apparent differences in pace of tumor evolution and genomic integrity. less common variants of aggressive neuroblastoma may result from genetic progression of low-risk neuroblastoma or from 12q amplification. Such nosological diversity may have therapeutic implications. Keywords: high-risk neuroblastoma, MYCN amplification, 11q deletion, DNA copy number, tumor evolution Authors: Cihan Cetinkaya, Tommy Martinsson, Catarina Träger, Per Kogner, Jan P. Dumanski, Teresita Díaz de Ståhl and Fredrik Hedborg

NOPHO • NOBOS 2012 63
O18. Familial hemophagocytic lymphohistiocytosis type 3 (FHL3) caused by deep intronic mutation and inversion in UNC13D Marie Meeths, Karolinska Institutet, Dept of Womens and Childrens Health, Sweden
Familial hemophagocytic lymphohistiocytosis (FHl) is an autosomal recessive, often-fatal hyperinflammatory disorder. Mutations in PrF1, UNC13D, STX11, and STXBP2 are causative of FHl2, 3, 4, and 5, respectively. In a majority of suspected FHl patients from Northern Europe, sequencing of exons and splice sites of such genes required for lymphocyte cytotoxicity revealed no or only monoallelic UNC13D mutations. Here, in 21 patients, we describe 2 pathogenic, noncoding aberrations of UNC13D. The first is a point mutation localized in an evolutionarily conserved region of intron 1. This mutation selectively impairs UNC13D transcription in lymphocytes, abolishing Munc13-4 expression. The second is a 253-kb inversion straddling UNC13D, affecting the 3 prime-end of the transcript and likewise abolishing Munc13-4 expression. Carriership of the intron 1 mutation was found in patients across Europe, whereas carriership of the inversion was limited to Northern Europe. Notably, the latter aberration represents the first description of an autosomal recessive human disease caused by an inversion. These findings implicate an intronic sequence in cell-type specific expression of Munc13-4 and signify variations outside exons and splice sites as a common cause of FHl3. Based on these data, we propose a strategy for targeted sequencing of evolutionary conserved noncoding regions for the diagnosis of primary immunodeficiencies. Keywords: UNC13D, familial hemophagocytic lymphohistiocytosis, immunodeficiency, inversion, Alu element. Authors: Meeths M, Chiang SC, Wood SM, Entesarian M, Schlums H, Bang B, Nordenskjöld E, Björklund C, Jakovljevic G, Jazbec J, Hasle H, Holmqvist BM, rajic l, Pfeifer S, rosthøj S, Sabel M, Salmi TT, Stokland T, Winiarski J, ljunggren HG, Fadeel B, Nordenskjöld M, Henter JI, Bryceson YT.

64 NOPHO • NOBOS 2012
O19. Swedish national biobank for pediatric neural tumors Susan Pfeifer, Uppsala, Sweden
A national Swedish biobank for neural tumors has been initiated by the Swedish Childrens Cancer Foundation (BCF) and its neural network NBCNS (CNS tumors and neuroblastoma in children), together with VCTB (The Swedish Childhood CNS Tumor Working Group) and VSTB (The Swedish Childhood Solid Tumor Working Group), and the six universities in Sweden which have responsibility for treatment of children with brain tumors and neuroblastoma. The national biobank is situated at the Karolinska University Hospital. The goal of the biobank is to facilitate research and increase knowledge of pediatric CNS tumors and neuroblastoma, and to develop diagnostics and new therapies for children with neural tumors. The sample collection in the national biobank will include surplus tumor tissue from children biopsied/operated on clinical indications for brain tumors and neuroblastoma, cell lines or stem cells isolated from biopsies, blod, plasma, and CSF from patients, and for genetic analyses blood from parents. Tumor biopsies from patient autopsies may be included. Traumatized tissue resected from pediatric patients undergoing surgery for brain traumas or CNS bleeding, as well as epilepsy surgery may come in question as reference tissue. A link to the VCTB and VSTB clinical patient registries will be established for every patient sample. Biobanking and registration of patient data requires patient /parent consent. The biobank project has been approved by the regional ethical comittee. Specific research projects will require additional ethical approval. The plan is to collect about 200 biopsies before distributing material for research. A central pathology review of all biobanked tumor biopsies is planned. Basic analyses of biobanked samples such as whole genomic arrays, rNA expression arrays, and protein analyses are planned for tumor subtyping. A home page for the national biobank is under construction. Keywords: Swedish national biobank pediatric neural tumors Authors: Susan Pfeifer, Department of Pediatric Oncology, Uppsala University Hospital, and Monica Nister, Department of Oncology-Pathology, Karolisnka Institutet, Sweden For the biobank group, NBCNS

NOPHO • NOBOS 2012 65
Free PapersPOSTEr PrESENTATIONS

66 NOPHO • NOBOS 2012
P1-6 SUPPORTIVE CARE P1. Central Venous Catheters and Catheter Locks in Children with Cancer: a Prospective Randomized Trial of Taurolidine versus Heparin Mette Møller Handrup, Department of Pediatrics, Denmark
Purpose: Central venous catheters (CVCs) are a major risk factor of bloodstream in children with cancer. Taurolidine, a derivate from the aminosulphonic acid taurinamide, has shown efficacy in preventing catheter-related bloodstream infections (CrBSI) in adult patients. The purpose of this study was to determine if taurolidine used as a catheter lock can reduce the number of CrBSI in tunneled CVC in pediatric patients with cancer. Patients and Methods: During a study period of 34 months, 129 newly placed tunneled CVCs in 112 patients were randomly assigned to standard lock with heparin solution or experimental lock with a taurolidine solution (ClinicalTrials.gov Identifier NCT00735813). results: Sixty-five CVCs were included in the standard group and sixty-four CVCs in the experimental group. The two groups were comparable regarding patients’ characteristics except that there were more boys in the experimental group. A total number of 68 bloodstream infections of which 27 were CrBSIs were observed among 37,837 CVC-days. A lower rate of CrBSI (0.3 per 1,000 CVC-days) was observed in the experimental arm compared with the standard arm (1.2 per 1,000 CVC-days, incidence rate ratio (Irr) =0.21; 95% confidence interval (CI) 0.06 to 0.58; p=0.001). A lower rate of total bloodstream infections (1.3 per 1,000 CVC-days) was also observed in the experimental arm compared with the standard arm (2.4 per 1,000 CVC-days, Irr=0.55; 95% CI 0.32 to 0.91; p=0.02). Median interval from catheter insertion until first CrBSI was significantly lower in the standard group (140 days, range 12-542) compared with the experimental group (246 days, range 12-811; p=0.04). Premature removal of the CVC due to infection and overall CVC survival were similar in the two study groups. No adverse affects were observed in the group locked with taurolidine. Conclusion: locking of long-term tunneled CVC with taurolidine is efficacious and safe in reducing catheter-related bloodstream infections in children with cancer. Keywords: Central venous catheter, Catheter-related bloodstream infections, Taurolidine, Biofilm Authors: Mette Møller Handrup, Jens Kjølseth Møller and Henrik Schrøder

NOPHO • NOBOS 2012 67
P2. Impact of hydrochloric acid instillation on the premature removal rate for central venous catheters in children with Acute Lymphoblastic Leukemia Mette Madsen, Aalborg Hospital, Childrens department, Denmark
Background: Bacteremias associated with indwelling central venous catheters (CVC) cause significant morbidity in children with cancer. Hydrochloric acid (HCl) instillations have been reported to salvage CVCs with antibiotic-refractory infection. We implemented this treatment in 2002. The impact on the survival of catheters has been evaluated in a retrospective cohort study of children with acute lymphoblastic leukemia (All). Methods: Children with newly diagnosed All having their first CVC inserted before (n = 16, the comparison cohort 1999-2001) and after introducing the procedure (n = 24, the intervention cohort 2002-2005) were studied. All bacteremic episodes were reviewed, recording bacteriological findings and treatment, and the time to premature or planned removal of the CVC was determined. results: In the comparison cohort 31% of bacteremic episodes (9/29) led to removal of the CVC, compared to 5.5% (2/36) in the intervention cohort (P=0.01). Thus, the rate of catheter loss due to infection fell from 56% (9 of 16) to 8.3% (2 of 24) after introducing HCl treatment (P=0.003). Overall, the premature catheter removal rate fell from 75% (12/16) to 46% (11/24) (P=0.10). The improved chance of the CVC remaining in place till elective removal was clearly evident in a cusum plot. In a subgroup analysis of 21 monobacterial infections with coagulase negative staphylococci, a significant decrease in systemic and lock antibiotic therapy was found. No adverse events were noted. A cusum plot showing results in a subsequent series of children diagnosed with All 2006-2010 will be presented. Conclusions: HCl instillations significantly reduced the need to remove and replace CVCs. The procedure is practical, appears to be safe, and may reduce consumption of antibiotics. Keywords: Catheter-associated bacteremia, hydrochloric acid, indwelling central venous catheter, acute lymphoblastic leukaemia, children Authors: Mette Madsen, MD and Steen rosthoej, MD Presenting author: Mette Madsen

68 NOPHO • NOBOS 2012
P3. Assessment of transfusion-related iron overload in children treated for cancer and non-malignant disorders Jelena Rascon, Centre for pediatric oncology and hematology, Lithuania
Objectives: to assess the frequency of transfusion-related iron overload in children treated for malignancies and non-malignant disorders. Patients and methods: Two groups of patients were prospectively evaluated. The first one consisted from 41 consecutive patients newly diagnosed pediatric cancer or benign blood disorders from 1st of February 2011 till 10th of February 2012 (leukemias n = 19, solid tumors n = 18, non-malignant disorders n = 4). Serum iron, ferritin and UIBC were measured at diagnosis and later-on following 10, 15, 20 etc. transfusions. The second group consisted from 46 cancer survivors (median follow up 31 months [range 6-120], leukemias n = 27, solid tumors n = 16, non-malignant disorders n = 3). repetitive assessment of ferritin in this cohort was performed at the same period from 1st of February 2011 till 10th of February 2012. results: during the study period 14 from 41 (34.1%) newly diagnosed patients received 10 and more erythrocyte concentrates (EC) (acute leukemias n =10, solid tumors n = 3, SAA n =1). Five from 14 have completed intensive chemotherapy including HSCT (n = 2) while the remaining 9 patients are still under the treatment. Higher transfusion load assessed as EC ml/kg BW correlated with higher ferritin and lower UIBC level (Pearson’s correlation coefficient was 0.591, p < 0.001 and -0.496, p = 0.003, respectively) but did not with serum iron (p = 0.231). In the second group the median time from the last EC transfusion to the study enrollment was 9.5 months (range 0-84). Median number of transfused EC and amount of EC ml/kg BW were 14 (range 1 – 144) and 110.1 (range 4.1 – 899.9) ml/kg respectively. Higher amount of EC ml/kg BW correlated strongly with higher ferritin level (Pearson’s correlation coefficient was 0.686, p < 0.001). Serial measurement of ferritin showed slow decrease of iron store over the time. Conclusion: 34.1% of children treated for malignancies and non-malignant blood disorders receive multiple transfusions. Iron overload measured as ferritin and UIBC correlates strongly with previous transfusion load. Keywords: iron overload, late effects Authors: Jelena rascon1, lina ragelienë1,2, Sigita Stankevièienë1, Tadas Þvirblis3 1 Children‘s Hospital, Affiliate of Vilnius University Hospital Santariskiu Klinikos, Centre for Pediatric Oncology and Hematology 2 Vilnius University, Faculty of Medicine 3 Department of Hematology, Hematology, Oncology and Transfusion Medicine Center, Vilnius University Hospital Santariskiu Clinics, Vilnius, lithuania

NOPHO • NOBOS 2012 69
P4. Severe lactic acidosis in a patient with acute lymphoblastic leukemia – a case report Aina Ulvmoen, Oslo universitetssykehus HF, Pediatrics, Norway
lactic acidosis (lA) in malignancies is a rare condition that has been reported in cases of leukemia and lymphomas. All associated with lA is linked to poor prognosis. Abnormal tumor metabolism and decreased clearance due to hepatic or renal dysfunction may explain the development of lA. Chemotherapy has been noted to correct the lA. A 10-year-old boy was admitted to the children´s hospital because of anemia. Upon admittance he had a two week history of fatigue, dizziness, nausea, headaches and a 4 kilogram weight loss. The clinical examination revealed a relatively healthy looking boy with pale skin, multiple hematomas on the legs and a palpably enlarged spleen. The laboratory data showed pH 7.34, pCO2 3.5, bicarbonate 13.8, base excess -10.7, and lactate 15.0. Serum sodium was 135, potassium 4.1, chloride 95, and the anion gap 26 mEq/l. The blood cell count showed hemoglobin 4.5 g/dl, WBC 6.0 x 109/l and platelets 105 x 109/l. lD was elevated at 1191 and uric acid at 791. The blood smear showed neutrophilic left shift and the presence of 28 % lymphoblasts. The bone marrow confirmed acute lymphoblastic leukemia of B cell precursor phenotype. The patient was initially treated with forced diuresis and rasburicase. Bicarbonate was administered because of sustained lA. Induction therapy was started on day 3 according to NOPHO All 2008 non-high risk protocol with prednisolone, vincristine and doxorubicin. On day 15 and 29 the patient was in remission. The lA improved gradually, but the lactate value has generally stayed near the upper limit of normal. During maintenance therapy , a CNS leukemic relapse was identified, and he was shifted to the All-rEZ BFM 2002 protocol. Thus, lA and high anion gap is a serious condition that should be considered in patients with haematological malignancies and raise awareness of cancer recurrence. Keywords: lactic acidosis, All, prognosis, leukemic recurrence. Authors: Aina Ulvmoen (presenting author), Monica Cheng Munthe-Kaas, and Marit Hellebostad

70 NOPHO • NOBOS 2012
P5. Hemoglobin and ferritin measurements and prevalence of anemia among adolescents in Tromsø, Norway Trond Flægstad, University and University Hospital, Tromsø, Pediatrics, Norway
Background: Iron deficiency, anemia, or a combination of both conditions may have negative health consequences for children and adolescents. There are few updated population based studies of adolescents from the Nordic countries including measurements of hemoglobin and the prevalence anemia. Methods: Measurements of hemoglobin and ferritin of 869 adolescents (range 15-17 years and 46.7 % girls) from a cross sectional populations based study in Tromsø (2010 and 2011) are reported. The reference population was defined as participants without acute or chronic inflammation. results: 19.2 % (n= 78 / 406) of all girls had ferritin < 12 µgram/l. The prevalence of anemia was 22.9 % (n = 92 / 401) among girls according to the WHO definition of anemia (hemoglobin < 12 g/dl) and 46.7 % of these girls had ferritin < 12 µgram/l. 7.5 % (n = 30 / 401) had hemoglobin levels < 11.4 g/dl, which is the 2.5 hemoglobin percentile for girls in the reference population. 64.3 % of the same girls had ferritin < 12 µgram/l. 1.9 % (n = 9 /463) of all boys had ferritin < 12 µgram/l. The prevalence of anemia was 3.7 % (n = 17 / 455) among boys according to the WHO definition of anemia (hemoglobin < 13 g/dl) and 23.5 % of anemic boys had ferritin < 12 µgram/l. Hemoglobin levels at 12.9 g/dl was the 2.5 percentile cut-off for boys in the reference population and 2.9 % (n = 13 / 455) had hemoglobin levels below this cut-off in the whole sample. 30.4 % of the same boys had ferritin < 12 µgram/l. Conclusion: Anemia and low level of ferritin are highly prevalent among pubertal girls in Tromsø. The prevalence of anemia was three times higher with the WHO definition, compared to anemia defined as hemoglobin levels below the 2.5 percentile for reference persons in the same population. The results may indicate that the WHO definition of anemia is inappropriate for 15-17 year old Norwegian girls, possibly overestimating the prevalence of anemia. Keywords: anemia, adolescents, ferritin Authors: Niklas Stabell Anne Texmo Prytz Ida Heiberg Trond Flægstad

NOPHO • NOBOS 2012 71
P6. A descriptive study of the incidence, experience and treatment of oral mucositis in children and adolescents during stem cell transplantation Tove Kamsvåg-Magnusson, Akademiska sjukhuset/Uppsala Universitet, Inst för Kvinnor och Barns hälsa, Sweden
Background: Oral mucositis (OM) is a common adverse effect of chemo- and radiotherapy, which is highly debilitating and painful for the patient and threatens the effectiveness of therapy. There is limited knowledge about the impact of mucositis in children who undergo hematopoietic stem cell transplantation (HSCT) today and there are no guidelines for the treatment of OM in children. The aim of this study is to investigate the incidence, experience and treatment of oral mucositis in children and adolescents who have undergone HSCT. Methods: Questionnaires addressing symptoms, consequences, and treatment of mucositis were sent to families of children (0-18 years old) who had undergone HSCT in Sweden 2008-2011. A total of 127 parent-questionnaires and 69 child-questionnaires (children ≥7 years) were sent out. results: The response rate was 56 % for parents and 51% for children. The following results are from the parents’ report but corresponded well to those of the children. The mean age of the child was 9.1 years. OM was next to nausea ranked as the most distressing condition during treatment. 85 % of the children had pain in the mouth, 94 % dysgeusia and 51 % ulcers. Most pain was associated with eating, brushing teeth and oral examination. 44 % had problems eating solid food and 32% had problems ingesting liquids. 1/3 of the children had received prophylactic treatment against OM. 69 % reported daily assessments of oral status. 40 % of the parents reported unsatisfactory effect of the pain treatment for mucositis that the child had received during HSCT. Conclusions: OM affects many children undergoing HSCT causing much pain and discomfort. Treatment of OM and its symptoms in children and adolescents is presently insufficient, more evidence of such treatment is needed, and subsequently there is a need to establish a more evidence-based care. Keywords: oral mucositis, children, adolescents, hematopoietic stem cell transplantation Authors: Tove Kamsvåg-Magnusson, Jenny Thorsell, Johan Arvidson, Karin Mellgren, Jacek Toporski, Jacek Winiarski, Anncarin Svanberg, Gustaf ljungman

72 NOPHO • NOBOS 2012
P7-14 LATE EFFECTS
P7. Long-term impact of TBI on self-reported quality of life for long-term survivors of lymphoblastic malignancy in childhood Johan Arvidson, Uppsala University Childrens Hospital, pediatric oncology, Sverige
In the present study we have the possibility to compare self-reported long-term consequences for adult survivors of first line and second line therapy for lymphoblastic malignancies. The standardized HrQol measure SF-36 has previously been used in childhood survivors, but none has hitherto used the SEIQol-DW, considering the individual perspective on factors influencing Qol. In this study we use both. The objective was to study the impact of disease and treatment on IQol and HrQol in long-term survivors of lymphoblastic malignancy treated with and without TBI in the absence of graft versus host disease. The SCT group, (n=18) were all treated with TBI as part of the conditioning regimen. The non-SCT group (n=52), were at least 18 years of age at the time of the study, and were all in Cr1 except one patient. Median follow-up time after end of therapy for the two groups was 18 and 14 years respectively. results include frequencies and ratings of important areas in life, and an overall individual Qol-score (SEIQol Index). Individual positive and negative consequenses are reported. Scale ratings of SF-36 are presented groupwise. significant differences between the two groups can be detected. Most surprisingly, the only significant predictor for both low SEIQol Index and Physical Component Summary (PCS from SF36) was unemplyed/sick leave (worse) versus student/working (better). Other factors included in the multiple linear regression analysis were TBI, age, time from end of therapy, education, cranial irradiation therapy and sex. This is the first study to compare IQol in (very) long-term survivors of lymphoblastic malignancies treated with and without TBI, in the absence of cGvHD. The findings show that the SCT and the non SCT group report similar important life areas although the influence of TBI seems to render more negative consequences in life. Keywords: individual QOl health-related QÒl total body irradiation childhood lymphoblastic malignancies long-term follow-up Authors: Johan Arvidson, PhD lena Wettergren, PhD, Per Frisk, PhD Kay K Sundberg, PhD,

NOPHO • NOBOS 2012 73
P8. Rapid acute ovarian failure during cancer treatment in young girls regardless of type and dose of treatment. Helena Mörse, Skåne University Hospital, Lund University, Paediatric Oncology/Haematology, Sweden
Aim: We are conducting a prospective observational study of prepubertal and pubertal girls during and after cancer treatment to determine ovarian response to cancer treatment in relation to clinical factors, Patients and methods: In the present interim analysis, thirtyfour of 51 consecutive female cancer patients aged 0-18 years were included. Eleven of the patients had reached menarche (mean age 14,5 years) and 23 had not (mean age 6,5 years). Serum/plasma levels of anti-Müllerian hormone (AMH), inhibin B, FSH, lH, oestradiol (E2) were measured at diagnosis and every three months during and after treatment. COrrECTED VErSION: results: All patients had detectable AMH levels at diagnosis. All showed a rapid decline in AMH after 3 months of treatment, regardless of AMH at diagnosis, age, menarche or treatment given. Those given radiotherapy below the diaphragm and/or stem cell transplantation (n=10) had no ovarian recovery during or after treatment. However, recovery was observed in those given standard treatment for acute lymphatic leukaemia (n=7) already during low-dose chemotherapy. Three months after treatment stop, 50 % of all patients had recovered ovarian function measured as AMH and inhibin B, despite relatively high doses of alkylating agents. Conclusions: We here present, to our knowledge, the first prospective study of ovarian function during and after cancer treatment in young female patients. rapid acute ovarian failure is seen in all girls after initiation of cancer treatment as measured by AMH and inhibin B. Depending on the regimen, half of the cases show prompt ovarian recovery during or after discontinuation of treatment. Our study suggests that those without such recovery are at high risk of premature ovarian insufficiency. Keywords: ovarian reserve, cancer treatment, anti-Müllerian hormone, prepuberty, puberty Authors: Helena Mörse (1), Maria Elfving (2), Anna lindgren (3), Pål Wölner-Hanssen (4), Claus Yding Andersen (5), Ingrid Øra (1) 1) Dept. of Paediatric Oncology and Haematology, Clinical Sciences; 2) Dept. of Paediatric Endocrinology, Clinical Sciences; 3) Centre for Mathematical Sciences; 4) Dept. of reproductive Medicine, Clinical Sciences, all lund University, lund, Sweden. 5) laboratory of reproductive Biology, rigshospitalet, University of Copenhagen, Copenhagen, Denmark

74 NOPHO • NOBOS 2012
P9. Factors associated with poor quality of life in survivors of childhood acute lymphoblastic leukemia and lymphoma Adriani Kanellopoulos, Oslo University Hospital, Rikshospitalet, Department of Pediatrics, Norway
Objective: Previous studies of health-related quality of life (Qol) in childhood cancer survivors have not focused on factors associated with poor Qol in order to identify paths to improvement. Therefore the aims of this study were: 1) To assess Qol in long-term survivors (lTSs) of childhood acute lymphoblastic leukemia (All) and lymphomas compared to age-matched controls from the general population (NOrMs). 2) To investigate factors associated with poor Qol in lTSs. Patients and Methods: 285 lTSs (149 All, 91 Hodgkin lymphoma and 45 Non-Hodgkin lymphoma) diagnosed between 1970 and 2002 at age <19 years participated in this Norwegian population-based cross-sectional follow-up study. The lTSs completed a mailed questionnaire including the Short Form 36 (SF-36) as Qol-measure and items concerning socio-demographic and somatic and mental health issues. NOrMs consisted of five controls for each lTS (N=1,425). Poor Qol was defined as SF-36 physical and/or mental component summary score <40. Treatment details were obtained from the clinical records. results: Median age at survey was 29.6 years (range 18.3-54.4), median follow-up time 21.1 years (range 6.9-39.4). 110 lTSs (39%) had received radiotherapy. Compared to NOrMs, lTSs scored significantly lower on 7 of 8 SF-36 subscales (p<0.001). Among NOrMs 18% had poor Qol versus 32% among lTSs (p<0.001). In bivariate regression analyses, fatigue, neuroticism, anxiety, depression, older age at survey, female sex, not holding job, chronic health conditions, chronic pain, regular use of medication or psychotropics, obesity and insomnia were all significantly associated with poor Qol. In multivariate analysis, levels of fatigue, anxiety, depression, as well as obesity and insomnia were significantly associated with poor Qol. Conclusions: lTSs had significantly poorer Qol than age-matched NOrMs. Fatigue, anxiety, depression, obesity and insomnia were significantly associated with poor Qol in lTSs. Since these factors are amenable to interventions, they should be investigated at follow-up examinations. Keywords: Health-related quality of life, childhood cancer survivors, acute lymphoblastic leukemia, lymphoma Authors: Adriani Kanellopoulos (presenting author), Hanne M. Hamre, Sophie D. Fosså, Alv A. Dahl and Ellen ruud

NOPHO • NOBOS 2012 75
P10. Cardiorespiratory fitness in young adults after stem cell transplantation in childhood Per Frisk, Department of Women’s and Children’s Health, Uppsala University, Sweden
Data are scarce on cardiorespiratory fitness (CrF) in young adults after stem cell transplantation (SCT) in childhood. Decreased CrF is associated with a higher risk of cardiovascular disease (CVD) and all-cause mortality. limitations in CrF after SCT might theoretically be caused by therapy-related impairment at any level in the oxygen transport chain, including the lungs, heart, and muscles. After SCT, patients may also develop an imbalanced body composition with more fat and less fat-free mass (FFM). CrF is conventionally expressed as oxygen uptake at peak effort (VO2peak) divided by body weight (in kilograms). Dividing VO2peak by FFM might be a more appropriate approach, better reflecting the metabolically active tissue during exercise. We assessed CrF in 17 patients at a median of 17.7 years after SCT and compared them with 17 sex- and age-matched healthy controls. Body composition was assessed with dual energy X-ray absorptiometry. We found no difference in VO2 at rest or in heart rate reserve between the patients and the controls. VO2 at anaerobic threshold (AT, 1296 vs 1954 ml/min, p<0.001), O2 pulse (10.7 vs 16.7 ml/beat, p<0.001), and max workload (147 vs 248 W, p<0.001) were significantly lower among the patients. VO2peak was significantly lower in the patients after controlling both for body weight (31.2 vs 41.4 ml/kg/min, p=0.008) and for FFM (47.4 vs 56.3 ml/kg/min, p=0.022). We conclude, that testing during physical activity is needed to detect damages to CrF after SCT and that the findings with lower values for VO2 at AT and at maximal workload are multifactorial. Keywords: Cardiorespiratory fitness, stem cell transplantation Authors: Anders Öberg, Margareta Genberg-Andrén, Per Frisk, Hans Hedenström

76 NOPHO • NOBOS 2012
P11. Pulmonary function following allogeneic stem cell transplant in pediatric cancer patients in Finland: A retrospective cohort study of 51 patients Laura Madanat-Harjunoja, HUCS, Jorvi Hospital, Finland
Haematopoietic stem cell transplant (HSCT) has over the past 30 years become the curative treatment for children diagnosed with a wide range of malignant and benign conditions. In this setting, intensive preconditioning treatments, including alkylating agents and total body irradiation place these patients at high risk of developing various late morbidities. respiratory complications are expected to occur in every other patient receiving a stem cell transplant and account for 40% of all deaths. The aim of the study was to evaluate the timeframe and occurrence of pulmonary dysfunction following stem cell transplant for childhood haematological malignancies as well as potential risk factors for pulmonary dysfunction. A reptrospective evaluation of medical records of 51 patients aged over 6years treated with HSCT in a single centre were evaluated. Patients had taken part in spirometry measurements prior to HSCT (baseline) as well as 6-12 (spiro1), 18-24mos (spiro2) and 3-5yrs (spiro3) post HSCT. Main outcome measures were changes observed in FVC and FEV1 over time. The Wilcoxon signed rank test was used to analyse changes in pulmonary function tests over time. Mann-Whitney statistics were used to analyse potential explanatory factors. Significant reductions of 15.6% (p<0.05) in FVC could be seen when comparing baseline spirometry and spirometry conducted at first post HSCT follow-up visit. FVC reduction was progressive as a significant reduction of 11.4% (p<0.05) was also seen between baseline and the spirometry performed on the last follow-up. Some improvement was seen between the spiro1 and spiro 2 as the FVC changed 6.6% (p<0.05). Similar decline profiles over time were observed for FEV1. Acute- and chronic graft-versus-host-disease were separately significantly associated with FVC decline. Patients who have undergone HSCT are at elevated risk of restrictive lung disease and should be followed-up with spirometry. Acute- and chronic graft-versus-host-disease are significant risk factors for these pulmonary complications. Keywords: pulmonary function, late-effects, stem cell transplant Authors: laura Madanat-Harjuoja, Saara Valjento, Kim Vettenranta, Merja Kajosaari, Mervi TaskinenPresenting author: laura Madanat-Harjuoja

NOPHO • NOBOS 2012 77
P12. Evaluation of late cardiac effects of anthracyclines with cardiac MRI in late survivors of childhood cancer Kaisa Ylänen, Tampere University and University Hospital, Pediatric Department, Finland
Introduction: late anthracycline cardiotoxicity can manifest years after therapy as either symptomatic heart failure or as asymptomatic left ventricular dysfunction. Cardiac MrI is considered as the golden standard in the assessment of cardiac function due to its ability to visualize the heart in any plane without a need for an optimal acoustic window and with an excellent reproducibility of measurements. Anthracycline cardiotoxicity may result in focal myocardial fibrosis detectable as late enhancement in cardiac MrI. The aim of our study was to investigate these abnormalities with cardiac MrI. Material: 62 late survivors of childhood cancer with a median age of 15.2 (7.8-20.6) yrs were studied with the cardiac MrI. Their median cumulative anthracycline dose was 185 (80-386) mg/m2. Their median age at the time of initial diagnosis was 3.8 (0.03-13.8) yrs and the median follow-up time was 7.8 (4.9-18) yrs. Methods: The cardiac MrIs were performed using a 1.5 Tesla device. Ventricular dimensions and function were assessed with an electrocardiography-gated steady-state free-precession cine MrI sequence. left ventricle volumes and ejection fraction (lVEF) were measured from the short axis planes. Intravenous gadolinium based contrast was given (0.1 mmol/kg) and contrast enhanced images acquired after 5-15 minutes. results: The mean lVEF was 50.3% (SD 5.7), the mean left ventricular end systolic volume (lVESV) was 44.3 (8.7)ml/m2 and the mean end diastolic volume was 89.3 (14.8)ml/m2. Half of the patients had lVEF < 50%, and 18% had lVEF < 45%. None of our patients had late gadolinium enhancement. Conclusion: With a minimum of five years after the cessation of therapy for childhood cancer including anthracyclines 50% of survivors had abnormal lVEF. Especially the lVESV was larger than that referenced for normal pediatric population. late gadolinium enhancement was not detected. These results emphasize the need for a meticulous follow-up of the late cardiac effects of childhood cancer therapy. Keywords: anthracycline, cardiotoxicity, cardiac MrI, late gadolinium enhancement Authors: Kaisa Ylänen, Päivi Savikurki-Heikkilä, Anneli Eerola, Tuija Poutanen, Kim Vettenranta

78 NOPHO • NOBOS 2012
P13. Primary amenorrhea after allogeneic HSCT associates to previous leukaemia therapy and use of TBI or busulfan based conditioning therapy Anu Vatanen, Childrens Hospital, Helsinki University Central hospital, Division of Hematology-Oncology and Stem Cell Transplantation, Finland
Primary amenorrhea with a need of hormonal replacement therapy is a common adverse effect among girls after hematopoietic stem cell transplantation, particularly when total body irradiation(TBI) is included in the conditioning regimen. Aim of the study was to evaluate the impact of previous leukaemia therapy (Cr1 vs. Cr¡Ý2, CNS irradiation yes/no among leukaemia patients) and different conditioning regimens (single TBI (sTBI), fractioned TBI (fTBI), chemotherapy with busulfan (B), chemo without B including both leukaemic and non-malignant cases) on the incidence of spontaneous menarche. Medical records of girls who underwent allogeneic HSCT at the age of 1-18 years at Huddinge and Helsinki University Hospitals between years 1980 through 2000 who were alive at least 7 years after HSCT (n=88) were retrospectively reviewed. Significantly more girls who were in Cr1 vs. Cr¡Ý2 at HSCT had a spontaneous menarche (57% vs. 14%). None of the 7 girls who received CNS irradiation prior HSCT had a spontaneous menarche compared to 15 out of 29 not exposed to CNS irradiation (P<0.05). No significant differences in the incidence of spontaneous menarche were detected when comparing conditioning with sTBI (31%) vs. fTBI (50%), B (56%) vs. TBI (46%) or B vs. chemo without B (100%). Significantly fewer girls (10%) of the ones who received conditioning without TBI or busulfan needed estrogen replacement therapy when compared to those with busulfan- (67%) and TBI-based conditioning (80%). Conclusions: Previous leukaemia therapy and use of CNS irradiation prior to HSCT associates to ovarian dysfunction after HSCT. Busulfan and TBI are as likely to cause primary amenorrhea with a need of hormonal replacement therapy Keywords: Ovarian dysfunction, Cr, CNS irradiation, allogeneic HSCT, busulfan Authors: Anu Vatanen, Mari Wilhelmsson, Birgit Borgström, Britt Gustafsson, Mervi Taskinen, Ulla M. Saarinen-Pihkala, Jacek Winiarski, Kirsi Jahnukainen. The presenting author: Anu Vatanen.

NOPHO • NOBOS 2012 79
P14. Final testicular size is less affected by busulfan-containing conditioning regimen when compared to TBI after allogeneic HSCT in childhood Kirsi Jahnukainen, Childrens Hospital, Helsinki University Central Hospital, Division of Hematology-Oncology and Stem Cell Transplantation, Finland
Spermatogenetic cell failure with decreased testicular growth during puberty is observed among most of the male patients after HSCT, irrespectively of conditioning. However, the probability to recover may be associated to the type of conditioning. The aim of the study was to compare the effects of previous leukaemia therapy (Cr1 vs. Cr¡Ý2, CNS irradiation yes/no among leukaemia patients) and different conditioning regimens (single dose total body irradiation (sTBI), fractioned TBI(fTBI), chemotherapy with busulfan (B), chemotherapy without B including both leukaemic and non-malignant cases) on final testicular size. Medical records of boys who underwent allogeneic HSCT at the age of 1-18 years at Huddinge and Helsinki University Hospitals from 1980 through 2000 and survived at least 7 years after transplantation (n=90) were retrospectively reviewed and final testicular size recorded (n=63). There were significant differences in final testicular sizes after conditioning with TBI vs. B (8,3¡À4,7 ml vs. 17,6¡À4,7 ml) and fTBI vs. sTBI (9,5¡À5,2 ml vs. 6,2¡À2,4 ml). No significant differences were detected between B vs. chemotherapy without B (17,6¡À4,7 ml vs. 14,3 ¡À 5,3 ml). Final testicular size was smaller (p<0.05) among those who got CNS irradiation prior to HSCT (5,6 ¡À 1,8 ml) vs. those non-irradiated (9,0 ¡À 5,5 ml) and those who underwent HSCT in pre-puberty (9,0 ¡À 5,4 ml) vs. after onset of puberty (12,8 ¡À 5,8 ml). Cr1 vs. Cr ¡Ý2 status at HSCT did not affect the final testicular size. Conclusions: Final testicular size is less affected by busulfan- than by TBI-based conditioning and may suggest higher functional level of spermatogenesis after chemotherapy-based conditioning. Keywords: HSCT, TBI, busulfan, final testicular size Authors: Mari Wilhelmsson, Anu Vatanen, Birgit Borgström, Britt Gustafsson, Mervi Taskinen, Ulla M. Saarinen-Pihkala, Jacek Winiarski, Kirsi Jahnukainen

80 NOPHO • NOBOS 2012
P15-18 CANCER TREATMENT
P15. Weekly vinblastine is a therapeutic option in recurrent/refractory pediatric low-grade gliomas Christoffer Ehrstedt, Dep of Women´s and Children´s Health, Uppsala University Children´s Hospital, Sweden
Background: In a majority of cases efficient treatment of low-grade gliomas in the pediatric population is achieved by surgery, sometimes accompanied by chemotherapy according to the lGG SIOP 2003 protocol. However, some cases of lGG is refractory, treatment options in these cases often consists of lGG SIOP 2003 relapse protocol or radiotherapy. Vinblastine can be used as a secondline chemotherapy. Methods: Four patients with refractory low grade gliomas was given vinblastine intravenously. These patients had previously failed chemotherapy and/or radiation for unresectable low-grade glioma. Tumor location has differed, 1 brainstem, 1 optic pathway, 1 thalamus, 1 cerebellar. Three of the patients was given vinblastine at a dose of 6mg/m2 weekly, the fourth patient received a 50% dose reduction because of intolerable side-effects. The treatment was given for at least 12 months in three of the cases. results: There have been significant reduction of tumor size in the 3 patients who have received vinblastine for at least 12 months. response to treatment have been followed at three months interval with MrI. None of the patients have been forced to discontinue the treatment because of intolerable side-effects. The fourth patient has been treated for three months and follow-up with MrI indicates a slight reduction of tumor size. Conclusion: Vinblastine should be considered as a secondline chemotherapy in refractory low grade gliomas. Extended administration (>12 months) seems to be tolerated well. If untolerable sideeffects dose reduction should be tried. Keywords: low- grade glioma, relapse, vinblastine Authors: Christoffer Ehrstedt MD ¹, Ann-Christin Björklund ¹, Bo Strömberg MD PhD ¹, Fredrik Hedborg MD PhD ¹, Susan Pfeifer MD PhD ¹, Evaldas laurencikas MD PhD ² ¹ Deparment of Women’s and Children’s Health, Uppsala University Children´s Hospital and ² Department of radiology, Uppsala University Hospital, Sweden

NOPHO • NOBOS 2012 81
P16. Asparaginase associated allergy in children and adolescents treated according to the NOPHO ALL-2008 protocol Louise Tram Henriksen, Departement of paediatrics, Denmark
Background: Asparaginase associated allergy is a serious adverse event (SAE) in All treatment. In the NOPHO All-2008 protocol, SAE registrations are performed quarterly. In Feb 2012, the number of asparaginase allergy registrations summarized to 74 cases which is approximately 10% of all SAEs. Asparaginase associated allergy results in discontinuation of treatment and may thus lead to a poorer survival. Study design: The study is a review of the allergy-concerning-data present in the NOPHO All-2008 database. Aim: To perform a detailed characterization of asparaginase associated allergy in the All-2008 protocol and to link this information to the development of asparaginase antibodies. Patients: 74 patients, aged 1-17,9 years and registered with allergy in the NOPHO-All-2008 database. Methods: A questionnaire has been sent to all the participating centers. Antibody profile is measured in the allergic patients using an ElISA method. Preliminary results: 31 of 74 questionnaires are completed so far. Allergic reactions seem to appear early in treatment (after 1-5 injections) with the majority after the 2nd PEG-asparaginase injection. The severity of allergic reactions seen range from grade 1-4, mostly grade 2-3 (CTCAE v3.0). Three anaphylactic reactions (grade 4) were seen though. The time from asparaginase injection to development of the allergic reaction ranged from <2 hours up to 24 hours after PEG-asparaginase injection. Most allergic reactions (21/31) happened less than 2 hours after the asparaginase injection. More results from the questionnaire and antibody analysis will be presented. Keywords: NOPHO All-2008, Asparaginase-associated-allergy, questionnaire, antibody development Authors: louise Tram Henriksen, Birgitte Klug Albertsen, Ellen ruud, Arja Harila-Saari, Jonas Abrahamsson, Goda Vaitkeviciene, Ólafur G. Jónsson, Kaie Pruunsild

82 NOPHO • NOBOS 2012
P17. TPMT geno- and phenotyping during treatment of childhood leukaemia – what to trust? Malin Lindqvist Appell, Linköping University, IMH/Drug research, Sweden
In the Nordic Countries, children diagnosed with acute lymphoblastic leukaemia follows a common treatment protocol, where stratification into risk groups based on prognostic factors determines the exact treatment schedule. The antimetabolite 6-mercaptopurine is an important part of the treatment and is metabolised through three competing pathways: methylation to inactive metabolite methyl mercaptopurine via thiopurine methyltransferase (TPMT); oxidation via xanthine oxidase to 6-thiouric acid; and formation of thioinosine moNOPHOsphate catalysed by hypoxanthine phosphoribosyl transferase. The aim of this study was to investigate TPMT activity during treatment, as well as factors influencing the TPMT activity and the metabolism of 6-mercaptopurine. The mean TPMT activity at diagnosis was 9.6 ±2.3 for TPMT wildtypes (n=47) and 4.8 ±0.3 for TPMT heterozygous individuals (n=4). Of individuals with the TPMT genotype TPMT*1/*1, 40% had an initial activity at diagnosis below the cut off for normal activity (9 U/ml prBC). All heterozygous individuals (TPMT*1/*3A or *1/*3C), had an initial activity below 9 U/ml prBC. TPMT was measured at 6 time points from diagnosis until up to 24 months after end of maintenance therapy. The TPMT activity in wild type individuals increased significantly and reached its highest value during maintenance therapy (14.6 vs 9.6 U/ml prBC at diagnosis, p = 0.001). Four individuals heterozygous for TPMT showed an increase in TPMT activity in the same pattern as the TPMT wildtypes. Drugs with the potential to influence the TPMT activity level will be discussed. Metabolite levels before and after high dose MTX infusions were measured in red blood cells. The thioguanine nucleotide (TGN) levels decreased 60h after MTX infusion, a phenomenon that could be due to up-regulation of drug transporters in the cell membrane of the red blood cell. Keywords: Keywords: 6-mercaptopurine, thiopurine methyltransferase, acute lymphoblastic leukemia, thioguanine metabolites, genotyping Authors: Malin lindqvist Appell and Stefan Söderhäll

NOPHO • NOBOS 2012 83
P18. Body mass index and toxic death among high risk patients in NOPHO ALL 2008 Bendik Lund, St. Olavs Hospital, Dept. of Pediatrics, Norway
The NOPHO All2008 protocol has emphasized the delicate balance between efficacy and toxicity in childhood cancer therapy. In that protocol patients with a historical pEFS below 50% (T-All a/o WBC >100K w/ M3 BM day 15 or MrD >0.1% d29, hypodiploidy, Mll rearrangements, or MrD >0.1% d79) were allocated to very intensive repetitive block Hr-therapy. Although highly efficacious with so far no resistant disease patients and a cumulative relapse rate among Hr patients of only 11% for BCP and 15% for T-All, the cumulative risk of toxic death has been >20%, so far requiring three amendments to the block therapy. The Hr toxic death rate has been highest for the adolescents, especially boys, indicating that the “metabolic syndrome”-like condition known to occur in many teenagers could have played a role. During treatment some patients will develop signs of the metabolic syndrome with obesity, hypertension, dyslipidemia, and insulin resistance. Collins and co-workers (JPHO 2010) found that the 15% fraction of children frankly overweight (BMI>85th percentile) at start of All treatment increased to 40% at the end of treatment. Butturini (JCO 2007) demonstrated a significant lower EFS-rate (72 vs 77%) and increased relapse rate (26% vs 20%) among the 8% obese among 4260 CCG-patients (BMI>95th percentile for age and sex) and the effect of obesity was most prominent in patients >10 years of age. Of the 651 children (1.0-17.9 years) in the All2008 database as of January 2012, 17 of the 111 Hr patients died in first remission. 7 of these 17 DCr1 were > 10 years. 5 out of these 7 had BMI at start of treatment >20.00. The age and sex adjusted BMI standard deviation scores of the total cohort are being analyzed and will be presented in detail at the annual meeting. Keywords: Childhood All Body mass index Toxic death Event free survival Authors: Bendik lund (presenting author), Klaus Müller, Mats Heyman, Ann Åsberg, Kim Vettenranta, Jonas Abrahamson, Olafur Gisli Jonsson, Kaie Pruunsild, Goda Vaitkeviciene, Kjeld Schmiegelow

84 NOPHO • NOBOS 2012
P19-26 TRANSLATIONAL RESEARCH P19. Optimization of three-dimensional cell culture systems to differentiate rat male germ cells in vitro. Jan-Bernd Stukenborg, Karolinska Institutet, Women s and Children s Health, Sweden
Objectives: Survival rates of children with cancer have been increased by improved treatment strategies. However, late side effects affecting future fertility do still exist. So far, no treatment can be offered to rescue fertility in those patients, in particular due to the lack of relevant experimental models. In rodents, differentiation of pre-meiotic into post-meiotic germ cells using a 3D-soft-agar-culture-system (SACS) has recently been described. Here, we compared the influence of different cell culture media and gonadotropins on rodent testicular cells in vitro. Methods: Single cell suspensions of isolated testicular cells from 7 days post partum (dpp) rat testes were cultured in six different culture media using SACS with or without FSH and hCG treatment. Cultures were maintained up to 55 days at 34°C and 5% CO2. We analysed germ cell differentiation morphologically, immunohistochemically and by rT-PCr. Since leydig cells provide an important hormonal milieu required for spermatogenesis, we also monitor testosterone level in those culture media. results: In vitro proliferation and apoptosis of rat testicular cells forming cell colonies was confirmed by immunocytochemical detection of proliferating cell nuclear antigen (PCNA) and TUNEl staining. Cells cultured without gonadotropin supplementation in SACS showed fewer colonies with highly condensed structures than cultured with gonadotropins. Additionally, cultures with gonadotropins showed a more stable expression for somatic cell genes. Highest testosterone production could be demonstrated with DMEM medium with glutamine. Conclusions: Our experiments demonstrate effects of gonadotropins and distinct culture media on hormonal function of leydig cells and spermatogenesis in vitro. This technique now has to be translated into human spermatogenesis and has to be functionally proven in further studies. It might open scenarios to adapt these techniques for human male germ cells from testicular biopsies as a potential strategy for fertility preservation of pre-pubertal boys suffering from gonadotoxic side effects of oncological treatments. Keywords: testis, late effects, in vitro spermatogenesis, fertility, germ cells Authors: Ahmed reda, Mi Hou, luise landreh, Kristín rós Kjartansdóttir, Konstatin Svechnikov, Olle Söder, Jan-Bernd Stukenborg Department of Women s and Children s Health, Pediatric Endocrinology Unit; Q2:08; Karolinska Institutet and University Hospital, SE-17176 Stockholm, Sweden

NOPHO • NOBOS 2012 85
P20. In Vitro Differentiation of Putative Testicular Cells from Human Embryonic Stem Cells in Suspension Culture Jan-Bernd Stukenborg, Karolinska Institutet, Women’s and Children’s Health, Sweden
Objective: Survival rates among childhood cancer patients have progressively increased over the past four decades particularly due to the development of more effective cancer treatments. 3 out of 4 children will get cured from their disease. However, this success has come to a cost and an increasing number of cured patients will face late effects of sub- or infertility as a result of the disease itself or the cancer treatments, including chemo- and radiotherapy. So far, these children do not have any or only a highly reduced chance to parent own biological children later in life. Establishing a robust in vitro culture model for differentiation of hESCs towards germ cells would be of great importance for studying molecular and cellular mechanisms of spermatogenesis as well as male infertility. Material and Methods: In this study, we culture three undifferentiated hESC lines (HS207, HS360, HS401) as spheres in suspension without supporting feeder layer. Cells were cultured at 37°C and 5% CO2 for 21days in spheres before stimulation with BMP7. We analysed germ cell differentiation morphologically, immunohistochemically as well as by Q-PCr. results: In addition to cell morphologies similar to those of early germ and immature Sertoli cells, the spheres showed also organization of putative germ and Sertoli cells reminding of those found in pre-pubertal human testis. When analyzing the stimulated and un-stimulated spheres with Q-PCr as well as immunohistochemical staining, we observed expression of specific markers for male germ and somatic cells at rNA and protein level after two weeks of differentiation. Conclusion: In this study we show for the first time that a sphere culture methodology can be applied for differentiation of hESCs towards putative male gonadal cells showing similar morphologies as well as gene and protein expression profiles similar to those for germ, Sertoli and leydig cells. Keywords: late effects, fertility, gonadal dysfunction, stem cells, male germ cells Authors: Kristín rós Kjartansdóttir1,2,3, Ahmed reda3, Kelly Day1, Olle Söder3, Outi Hovatta1, Jan-Bernd Stukenborg3. 1Department of Clinical Science, Intervention and Technology, Division of Obstetrics and Gynecology, Karolinska Institutet, Huddinge, Sweden, 2laboratory of reproductive Biology, Scientific Unit, Horsens Hospital, Denmark, 3Department of Women’s and Children’s Health, Pediatric Endocrinology Unit; Q2:08; Karolinska Institutet and University Hospital, SE-17176 Stockholm, Sweden

86 NOPHO • NOBOS 2012
P21. Genome-wide DNA methylation analysis for prediction of relapse in pediatric acute lymphoblastic leukemia Jessica Nordlund, Uppsala University, Department of Medical Sciences, Sweden
DNA methylation plays an important role as a modulator of gene expression and in the control of cell differentiation. It may be one of the mechanisms that drive malignant transformation of progenitor B- and T-cells into acute lymphoblastic leukemia (All) cells. Thus CpG sites with aberrant DNA methylation patterns could contribute to the variation between All patients with respect to their clinical outcome and response to chemotherapeutic treatments. recent advances in genotyping technology have made it possible to analyze DNA methylation on a genome-wide scale. We utilized DNA methylation arrays (Illumina) containing >450,000 probes that allow examination of known and potentially functional CpG sites in different genomic regions throughout the genome. We used the 450k arrays to investigate if the DNA methylation patterns in All cells collected at the time of diagnosis can be used to improve prediction of clinical outcome of All patients. Using the 450K arrays, we analyzed ~1,000 DNA samples, including 92 All-remission sample pairs, 30 samples taken at All relapse, and 711 additional diagnostic All samples of different All subtypes collected within NOPHO. Using multivariate analysis we detected CpG sites and regions that were predictive of clinical outcome in All. We also identified CpG sites that can be used as biomarkers for refined stratification of patients into subgroups for alternative, improved treatment. To elucidate the functional roles of DNA methylation in the transformation of blood progenitor cells into leukemic cells, we compared the methylation profiles of the All cells to those of mononuclear cells isolated from the bone marrow of All patients at remission and CD19+ B-cells, CD3+ T-cells, and CD34+ hematopoietic stem cells from healthy blood donors. This analysis identified ~25,000 differentially methylated CpG sites in ~5,200 gene regions containing leukemia-specific changes in their methylation patterns. Keywords: Acute lymphoblastic leukemia, Epigenetics, DNA methylation, Multivariate survival analysis Authors: Jessica Nordlund1*, Christofer Bäcklin2*, Anders lundmark1, Eva Freyhult2, Trond Flaegstad3†, Eik Forestier4†, Britt-Marie Frost5†, Mats Heyman6†, Jukka Kanerva 7†, Kjeld Schmiegelow8†, Stefan Söderhäll6†, Gudmar lönnerholm5†, Mats G. Gustafsson2 & Ann-Christine Syvänen1

NOPHO • NOBOS 2012 87
P22. Low-dose aspirin targets tumor-associated inflammation and delays neuroblastoma tumor growth in vivo Lena-Maria Carlson, Karolinska Institutet, Sweden
Purpose: Tumor-associated inflammation is a driving force in several adult cancers, and intake of low-dose aspirin has proven to reduce cancer incidence. little is known about tumor-associated inflammation in pediatric neoplasms and no in vivo data exists on the effectiveness of low-dose aspirin on established tumors. Our study evaluates inflammatory patterns paralleling neuroblastoma (NB) tumor growth in vivo and low-dose aspirin as a therapeutic option for high-risk NB. Experimental design: Spontaneously arising tumors in the transgenic TH-MYCN NB mouse model were monitored for tumor-associated inflammation at various stages of disease using flow cytometry, immunohistochemistry and qrT-PCr. Homozygous pups received daily low-dose aspirin using oral gavage (10mg/kg, n=8) or no treatment (n=15), from the age of 4.5 weeks to 6 weeks of age. results: Ex vivo analysis of tumors revealed a transition from an adaptive immune response predominated by CD8+ T-cells in neoplastic lesions from 5 week old homozygous mice, towards enrichment in immature cells of the innate immune system, including myeloid-derived suppressor cells, dendritic cells (DCs), and tumor-associated macrophages (TAMs) during tumor progression. An M1 to M2 transition of TAMs was demonstrated, paralleled by a deterioration of DC status. Ten days of anti-inflammatory treatment with low-dose aspirin significantly reduced tumor burden (p<0.01 ) and the presence of tumor-associated cells of the innate immune system (p<0.01 ). Conclusions: Tumor-associated inflammation progresses during NB growth and anti-inflammatory treatment with low-dose aspirin reduces tumor burden in the TH-MYCN transgenic mouse model of NB, suggesting a new treatment option for high-risk NB patients. Keywords: Inflammation, neuroblastoma, aspirin, TH-MYCN, COX Authors: lena-Maria Carlson, Agnes rasmuson, lova Segerström, Baldur Sveinbjörnsson and Per Kogner

88 NOPHO • NOBOS 2012
P23. Tumor hypoxia drives differentiation in neuroblastoma Fredrik Hedborg, Uppsala University, Womens and Childrens Health, Sweden
Background and Purpose: Previous research has demonstrated that morphologically differentiated cells in stroma-poor neuroblastoma are hypoxic and show neuroendocrine (chromaffin) features, including highly induced transcript levels from the gene coding for Insulin-like Growth Factor 2 (IGF2). To further characterise the total change in mrNA expression pattern in neuroblastoma by hypoxia, expression array studies were undertaken. Methods: 5 neuroblastoma cell lines and 2 control cell lines of other primitive neuronal origin (MBl and stPNET) were exposed to 42 hours of anoxia. 20K array analyses of hypoxia-induced changes in gene expression were conducted. real-time rT-PCr confirmation was performed for hypoxia-induced genes that were specific for neuroblastoma cells. Data were also confirmed via in situ hybridisation and/or immunohistichemical analyses of tumor tissues from clinical neuroblastoma and xenograft tumors from the studied cell lines. The fetal expression of genes of interest were examined histologically in sympathetic nervous system structures of first trimester. results: IGF2 was the top induced gene and several other highly induced genes were identified - all of which were characterized by being specifically expressed in fetal paraganglia (equivalent to the adult adrenal medulla). The validity of these results was confirmed by demonstrating that the newly identified genes were co-expressed with IGF2 in clinical tumor tissue irrespective of clinical subtype. Conclusions: The findings provide solid evidence for a chromaffin differentiation effect by hypoxia in neuroblastoma, thus providing deeper insights into its biology and possible conceptual tools for targeting the problem of tumor hypoxia. The findings are contradictory to previous research in this area and therefore call for re-evaluation of existing data. Keywords: neuroblastoma, tumor hypoxia, differentiation, chromaffin, novel concept Authors: Fredrik Hedborg

NOPHO • NOBOS 2012 89
P24. A prospective evaluation of degranulation assays in the rapid diagnosis of familial hemophagocytic syndromes Yenan Bryceson, Karolinska Institutet, Department of Medicine, Stockholm
Familial hemophagocytic lymphohistocytosis (FHl) is a life-threatening disorder of immune regulation caused by defects in lymphocyte cytotoxicity. rapid differentiation of primary, genetic forms from secondary forms of hemophagocytic lymphohistiocytosis (HlH) is crucial for treatment decisions. We prospectively evaluated the performance of degranulation assays based on surface upregulation of CD107a on NK cells and CTl in a cohort of 494 patients referred for evaluation for suspected HlH. Seventy-five of 77 patients (97%) with FHl3-5 and 11/13 patients (85%) with Griscelli syndrome type 2 or Chediak-Higashi syndrome had abnormal resting NK cell degranulation. In contrast, NK cell degranulation was normal in 14/16 patients (88%) with X-linked lymphoproliferative disease and in 8/14 patients (57%) with FHl2, who were identified by diminished intracellular SAP, XIAP, and perforin expression, respectively. Among 66 patients with a clinical diagnosis of secondary HlH, 13/59 (22%) had abnormal resting NK degranulation, while 0/43 had abnormal degranulation using Il-2 activated NK cells. Active disease or immunosuppressive therapy did not impair the assay performance. Overall, resting NK cell degranulation below 5% provided a sensitivity for a genetic degranulation disorder of 96% and a specificity of 88%. Thus, degranulation assays allowed a rapid and reliable classification of patients, benefitting treatment decisions. Possibilities for further improvements of diagnostic assays for FHl will be discussed. Keywords: Hemophagocytic lymphohistocytosis lymphoproliferation Primary immunodeficiency Cytotoxic lymphocytes Authors: Yenan T. Bryceson, Daniela Pende, Andrea Maul-Pavicic, Kimberly C. Gilmour, Heike Ufheil, Thomas Vraetz, Samuel C. Chiang, Stefania Marcenaro, raffaella Meazza, Ilka Bondzio, Denise Walshe, Gritta Janka, Kai lehmberg, Karin Beutel, Udo zur Stadt, Nadine Binder, Maurizio Arico, lorenzo Moretta, Jan-Inge Henter, Stephan Ehl

90 NOPHO • NOBOS 2012
P25. Targeting the Hedgehog signal transduction pathway at the level of GLI inhibits neuroblastoma cell growth in vitro and in vivo Malin Wickström, Karolinska Institutet, Sweden
Background: Hedgehog (HH) signaling is an important regulator of embryogenesis that has also been associated with the development of several types of cancer. HH signaling is characterized by Smoothened (SMO)-dependent activation of the GlI transcription factors, which regulate the expression of several genes critical for proper cell growth during development. Neuroblastoma has recently been shown to express high levels of HH signaling molecules. Methods: Cytotoxic activity of HH inhibitors was studied in cell viability assays. The molecular mechanisms were characterized using cell- and molecular biology techniques. A xenograft study in mice was performed to validate the therapeutic effects and toxicity in vivo. results: Using specific compounds blocking SMO (cyclopamine and SANT1) or GlI1/GlI2 (GANT61) activity revealed that inhibition of HH signaling at the level of GlI was the most efficient target in reducing neuroblastoma growth. The GANT61 sensitivity positively correlated to the expression levels of GlI1 and negatively to MYCN expression in the neuroblastoma cell lines tested. Additionally, GANT61 downregulated GlI1, C-MYC, MYCN and Cyclin D1 expression, and induced apoptosis of neuroblastoma cells, in-line with the reduction of cell numbers elicited by GlI1 knockdown. Furthermore, GANT61 enhanced the effects of chemotherapeutic drugs used in the treatment of neuroblastoma in an additive or synergistic manner and significantly reduced the growth of established neuroblastoma xenografts in nude mice. Conclusions: Taken together this study suggests that inhibition of HH-signaling is a highly relevant therapeutic target for high-risk neuroblastoma lacking MYCN amplification and should be considered for clinical trials testing. Keywords: Neuroblastoma, Hedgehog signaling, Small molecule inhibitor, New therapeutic targets Authors: Malin Wickström, Cecilia Dyberg, Takashi Shimokawa, Jelena Milosevic, Ninib Baryawno, Ole M Fuskevåg, rolf larsson, Per Kogner, Peter G Zaphiropoulos, John I Johnsen

NOPHO • NOBOS 2012 91
P26. Minimal residual disease markers in childhood acute myeloid leukemia Lotte Abildgaard, Aarhus University Hospital, Department of Pediatrics, Denmark
Introduction AMl is a heterogeneous disease with a high relapse risk despite intensive therapy. response to treatment and cytogenetic abnormalities are the main prognostic factors. Unfortunately, many children lack markers amenable to real-time quantitative PCr (rQ-PCr) and thereby complicating minimal residual disease (MrD) monitoring. Steinbach et all found several genes (WT1, SPAG6, ST18, MSlNK, PrAME, GAGED2) to be overexpressed in childhood AMl. Knowledge of normal expression in children and of any influence of infection or hematological regeneration is sparse. Patients and Methods Bone-marrow (BM) and peripheral blood (PB) samples were collected from 53 children undergoing heart surgery. Samples were analyzed with rQ-PCr in order to describe the normal expression of the six genes. Diagnostic and follow-up BM and PB samples from 13 children with All t(12;21) were analyzed in order to elucidate if hematological recovery affects expression levels. results WT1, SPA6, ST18 and GAGED2 had the lowest median number of copies pr. 1000 ABl copies in PB/BM of 0.08/3.2, 1.0/2.0, 1.7/4.2, and 0.09/0.1, respectively. We found the normal expression in children to be four times higher than in healthy adults analyzed in the same laboratory. In children, no consistent association between expression-levels and age for any of the genes were found. Children with All who at diagnosis had gene-expression levels within normal range were analyzed at day 15 and 28 after treatment start. A raise in expression levels to above normal range were found in 44% of SPAG6, 20% of ST18, and 33% of MSlN samples implying influence by regenerating bone-marrow. Conclusion and Perspectives The data emphasize the importance of age-matched reference values when using overexpressed genes. So far the most promising genes for MrD-monitoring are WT1 and GAGED2 but the influence of infection on the expression-levels are yet to be determined. Keywords: AMl, MrD, rQ-PCr, overexpressed genes, reference values Authors: lotte Abildgaard, Hans Beier Ommen, Charlotte Guldborg Nyvold and Henrik Hasle, lotte Abildgaard is presenting author

92 NOPHO • NOBOS 2012
P27-28 EPIDEMIOLOGY
P27. Hyperleukocytosis in childhood acute lymphoblastic leukemia: impact on early morbidity and mortality in Nordic and Lithuanian patients in 1992-2011 Goda Vaitkeviciene, Vilnius University Children Hospital, Center of Oncology and Hematology , Lithuania
Hyperleukocytosis increases early morbidity and mortality in childhood acute lymphoblastic leukemia (All) both due to massive organ infiltration and leukostasis at presentation and due to severe metabolic disturbances that may develop soon after initiation of therapy. We explored early morbidity and mortality as well as treatment strategies among the 0-15 year old children with All in Nordic countries (N=208) and lithuania (N=32) with white blood cell count (WBC) ≥200.0x109/l, treated in the Nordic countries or lithuania between January 1992 and September 2011. So far data from 63% of patients have been collected. Of those for whom immunophenotype was available 60% had T-cell and 50% had B-cell precursor All. 60% of the latter were infants. 14% of patients had clinical signs of CNS or peripheral nerve affection. Three of them had intracerebral hemorrhages and two had leukemic infiltrates detected by CT or MrI. 13% of patients developed pulmonary symptoms due to lung function impairment or mediastinal masses. Cytoreduction procedures such as exchange transfusions or leukapheresis were performed to 7% and 3% of the patients, respectively. 4% of patients underwent dialysis. Seven percent of patients died within the first month due to intracerebral hemorrhages (N=5), septic shock (N=3), bleeding (N=1) or leukemia progression (N=1). Keywords: acute lymphoblastic leukemia, children, hyperleukocytosis, tumor lysis syndrome Authors: Goda Vaitkeviciene, Mats Heyman, Olafur G. Jonsson, Birgitte lausen, Arja Harila-Saari, Margaretha Stenmarker, Mervi Taskinen, Ann Åsberg, lina rageliene, Kjeld Schmiegelow

NOPHO • NOBOS 2012 93
P28. Pediatric Patients with Bone Sarcomas in Finland during 1991-2005. A nationwide, population based study Joni Serlo, University of Helsinki, Faculty of Helsinki, Finland
Aim Our objective was to study the incidence and 5-year overall survival (OS) rates of pediatric patients with bone sarcomas in Finland. Methods The data was collected from the Finnish National Cancer register. The incidences were calculated based on the official population data for each year (1). The Finnish Population register Centre was contacted to get up-to-date information of survival. Survival rates were determined using the Kaplan-Meier analysis. results Altogether 95 patients less than 18 of age at the time of diagnosis were identified. Excluded were three patients because their tumors turned out to be benign and five patients because of missing data. There were 62 patients with osteosarcoma, 21 with Ewings sarcoma and four with chondrosarcoma. Thus the annual incidence for bone sarcomas in this population was 4.8 per million: 3.4 for osteosarcoma, 1.1 for Ewings sarcoma and 0.2 for chondrosarcoma. The 5-year OS was 76% for patients with osteosarcoma, 76% for Ewings sarcoma and 100% for chondrosarcoma. This difference was not statistically significant. Conclusions Five-year OS of Finnish patients less than 18 years of age with bone sarcomas is 77%. There was no difference in survival between patients with osteosarcoma, Ewings sarcoma or chondrosarcoma. The low incidence and number of malignant pediatric bone tumors should initiate a discussion on a more centralized treatment of these patients with one or maximum two Childrens Hospitals in Finland. Significance To our knowledge, this is the first nationwide, population based study establishing the 5-year OS in pediatric bone sarcoma patients in Finland Keywords: bone sarcoma, pediatric, incidence, survival Authors: Serlo, Joni M.D.1,2; Helenius, Ilkka M.D., Ph.D.2; Vettenranta, Kim M.D., Ph.D.3; Sampo, Mika M.D., Ph.D.4; riikonen Pekka M.D., Ph.D.5; Tarkkanen, Maija M.D., Ph.D.4

94 NOPHO • NOBOS 2012

NOPHO • NOBOS 2012 95
Programme

96 NOPHO • NOBOS 2012
SATUrDAY12.00 – 16.00 Registration / Information open at Uppsala
university main building.
19.00 – 23.00 NOPHO & NOBOS Get together at Uppsala Konsert & kongress (UKK)
SUNDAY08.00 – 17.00 Registration / Information open
08.00 – 17.00 Poster viewing
09.00 – 09.50 Official grand opening with entertainment, Room: University Hall (Plenary Room)Choir: Tonprakt, Conductor: Anders ’Grosse’ Grotherus, Song: Thomaz Szendrö, Piano: Leif Österlund
How to deal with difficult ethical problems in clinical pratice
09.50 – 10.00 Introduction to EthicsAnders Castor, Lund, Sweden
10.00 – 10.40 Can clinical ethics committees be useful for clinicians?Reidun Førde, Olso, Norway
10.40 – 11.10 Coffee break
11.10 – 11.40 Moral deliberation in the wardNOPHO & NOBOS WG in Ethics
11.40 – 12.10 Where is the child? – Navigating the intersection between pain and hopes of cureMats G Hansson, Uppsala, Sweden
12.10 – 12.20 When there is no chance of cure – where does palliation start and treatment end?Li Jalmsell, Uppsala, Sweden
12.20 – 12.30 Is there a decrease in survival rates after reduction of therapy? A population based study of children with Hodgkin lymphoma.Charlotte Hopstadius, Uppsala, Sweden
12.30 – 14.00 Lunch at Norrlands nation

NOPHO • NOBOS 2012 97
NOBOS: Lecture hall X
Chairs: Sigrún Þóroddsdóttir and Ann-Christin Björklund
14.00 – 14.40 Welcome speech and news from the NOBOS Board
14.40 – 15.00 The first Hospice for Children and Youth in SwedenAnn Edner, Nacka, Sweden
15.00 – 15.20 Difficult ethical situations in pediatric cancer care - A grounded theory (GT) study of ethical team discussionsCecilia Bartholdson, Stockholm, Sweden
15.30 – 16.00 Coffee break
16.00 – 16.20 Guided Self-help as Intervention for Traumatic Stress in Parents of Children with cancer:Martin Cernvall, Uppsala, Sweden
16.20 – 16.40 Multidisciplinary team for children with CraniopharyngiomasAnette Sjölund, Gothenburg, Sweden
MONDAY08.00 – 17.00 Registration / Information open
08.00 – 17.00 Poster viewing
Chairs: Anne Thorvildsen and Margaretha Jenholt Nolbris
08.30 – 08.40 Info from the organizers, room: lecture hall X
08.40 – 09.30 Cancer during adolescence – coping and psychosocial function in alongitudinal perspective.Gunn Engvall, Uppsala, Sweden
09.30 – 09.50 Transitioning to everyday life: Adolecent leukemia patients lived expirience. Implications for nursing care in an out patient clinicDorte Brinkmann Kristensen, Aalborg, Denmark
09.50 – 10.10 What about teenagers and young adultsMaria Olsson, Gothenburg, Sweden

98 NOPHO • NOBOS 2012
10.10 – 10.30 Young adult cancer survivor’s experiences of psychosocial rehabilitationJens Nygren, Halmstad, Sweden
10.30 – 11.00 Coffee break
10.45 – 13.30 NOBOS board meeting, room 2
11.00 – 12.00 round table discussion: • late effect, Mod: Charlotte Castor , lecture hall XI• Nutrition, Mod: Carina Fondin, room 3• Pain, Mod: Gunn Engvall, lecture hall IV• Palliation, Mod: Ann Edner, lecture hall X• Isolation, Mod: Margareta af Sandeberg, lecture hall II
12.00 – 13.30 Lunch at Norrlands nation
Chairs: Helle Borg Christensen and Jóhanna lilja Hjörleifsdóttir
13.30 – 14.20 Hospital-based home care for children with cancer.Helena Hansson, Copenhagen, Denmark
14.20 – 14.40 Children’s health, when diagnosed with cancer: their own and their parent’s experiences.Laura Darcy, Borås, Sweden
14.40 – 14.50 Short break
14.50 – 15.10 The impact of communication prior to and after the loss of a brother or sister to cancer - A nationwide long-term follow-upAlexandra Eilegård, Stockholm, Sweden
15.10 – 15.30 Bedside handover: Parents and children’s perception of change-of-shift report at the bedsideLiselott Pettersson, Uppsala, Sweden Katarina Wallin, Uppsala, Sweden
15.30 – 16.00 Coffee break
16.00 – 16.20 Swedish nurses’ descriptions of being an expert nurse in paediatric oncology careKarin Enskär, Jönköping, Sweden
16.20 – 16.40 Short break

NOPHO • NOBOS 2012 99
16.40 – 17.40 The Swedish Childhood Cancer Foundation – Tribute to the pioneers. (NOPHO and NOBOS) room: University Hall (Plenary room)
NOPHO: Gunilla Berglund, Stanislaw Garwicz, Göran Gustafsson, Henrik Hertz, Gudmundur Jónmundsson, Anders Kreuger, Sverre Lie, Göran Lundell, Toivo Salmi, Minna Yssing, Lars Åhström
Richard Johansson, Founder of Swedish Childhood Cancer Foundation
From NOBOS Gitte Petersen and Margareta af SandebergFrom The Swedish Childhood Cancer Foundation Olle Björk
Song: Kristin Nordström Interviewer: Jenny Strömstedt
TUESDAY08.00 – 14.00 Registration / Information open
08.00 – 12.00 Poster viewing
Chairs: Angelica Höök and Mette Normann Hansen
08.30 – 08.40 Info from the organizers, lecture hall X
08.40 – 09.30 Childhood cancer, school and infectionsMargareta af Sandeberg, Stockholm, Sweden
09.30 – 09.50 A mothers perspektiv on proton therapyAnna Silfver, Fagersta, Sweden
09.50 – 10.10 Internet based coaching for children after braun tumor treatment Anette Sjölund, Gothenburg, Sweden
10.10 – 10.40 Coffee break
10.40 – 11.00 Education day for relatives of children with cancerCharlotte Castor, Lund, Sweden
11.00 – 11.20 Participatory innovation process for development of a digital peer support service for children with cancerEva-Lena Einberg, Halmstad, Sweden
11.20 – 11.40 Presentation for the 10th NOBOS congress 2014 in Bergen.Sunniva Helland, Norway
11.40 – 12.00 Evaluationform
12.00 – 12.20 Closing time Gitte Petersen, Denmark
12.20 lunchbag

100 NOPHO • NOBOS 2012
GUEST SPEAKErS NOBOS
Cancer during adolescence – coping and psychosocial function in a longitudinal perspective
Gunn Engvall, phD, Pediatric Nurse, Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden
Background: A cancer disease and subsequent treatment cause physical, emotional, and social concerns for adolescents, requiring strategies to handle these concerns. The distress may cause anxiety and depression and influence the individual’s health-related quality of life.Aim: The aim was to investigate coping shortly after diagnosis and psychosocial function longitudinally among individuals struck by cancer during adolescence.Method: Sixty-one Swedish adolescents, 13-19 years of age, were included. Open and closed-ended questions were collected at seven occasions from shortly after diagnosis to 4 years after diagnosis. Nurses and physicians were matched to adolescents and answered questions regarding the adolescents’ coping shortly after diagnosis.Results: Adolescents recently diagnosed with cancer used a range of strategies to cope with distress shortly after diagnosis. Nurses and physicians have difficulties assessing how adolescents recently diagnosed with cancer cope with disease- and treatment-related distress. Three psychosocial states were identified: poor, average, and good psychosocial function. Shortly after diagnosis more individuals than expected by chance were found in the states of poor or average psychosocial function. This changed over time. Four years after diagnosis 77% were found in the state of good psychosocial function whereas 15% were found in the state of poor psychosocial function. The great majority of respondents reported negative and positive consequences three and four years after. Concomitant negative and positive cancer-related consequences appear stable over time and dialectical forces of negative and positive as well as distress and growth coexist after cancer during adolescence.Conclusion: It is difficult for nurses and physicians to identify how adolescents cope with disease and treatment related distress; the majority of individuals experience a state of good psychosocial function in the extended phase of survival; and distress and personal growth often go hand in hand after cancer during adolescence.

NOPHO • NOBOS 2012 101
HOSPITAL-BASED HOME CARE FOR CHILDREN WITH CANCER
Helena Hansson, Research nurse, Copenhagen University Hospital Rigshospitalet,Christoffer Johansen, professor, dr.med., the Danish Cancer Society, Copenhagen,Inger Hallström, professor, RN, Faculty of Medicine, Division of Nursing, Lund University,Hanne Kjærgaard, PhD., RM, Copenhagen University Hospital,Kjeld Schmiegelow, professor, dr.med. Copenhagen University Hospital Rigshospitalet
Background: The increasing impact on the child and the family due to the child’s cancer and treatment with frequent hospital visits calls for alternative ways to provide care. Hospital-based home care (HBHC) is an alternative provision of care in which the patient’s treatment is provided at home instead of at the hospital, although the evidence base is limited.Aim: The aim of the study was to evaluate a HBHC programme in relation to parents’ satisfaction with the care, safety, the psychosocial impact on the child and their family, and costs.Method: A HBHC programme was conducted where children with cancer received a part of their treatment at home if they were being treated with intravenous chemotherapy and lived within 50 kilometres of the university hospital. The programme was evaluated by: 1) an interview study describing family members’ experiences, 2) a descriptive study assessing the feasibility, and 3) a controlled questionnaire study in which a subsample of the programme population was compared to a standard hospital care group assessing the psychosocial impact on the child and their family.Results: Fifty-one children with different cancer diagnosis were included in the HBHC programme. All parents included in the HBHC were satisfied and preferred home care. There were no serious adverse events and costs did not increase. We found significant higher quality of life scores in the home care group indicating better physical health and less worry for these children. No significant difference was found in the psychosocial impact on the family.Conclusion: This study shows that HBHC visits can safely replace hospital visits with a high patient satisfaction and preference for HBHC care to equal costs. The children’s quality of life may be enhanced in specific aspects and HBHC appears to support the families’ perceived needs to maintain family functions while lightening the distress.

102 NOPHO • NOBOS 2012
Childhood cancer, school and infections
Margareta af Sandeberg, PhD, RN, Pediatric hematology and oncolgy, Astrid Lindgrens Childrens Hospital, Karolinska University Hospital, Stockholm, Sweden.
Background: The school situation is often affected during childhood cancer treatment. Due to uncertainty about whether it increases the risk of infection school attendance is not always recommended.
Objectives: The aim was to investigate the school situation and health-related quality of life (HrQOl) of school-aged children (7-16 years) during initial cancer treatment and 4 to 6 years after diagnosis.
Method: A cohort of school-aged children (n=126) diagnosed with cancer and starting chemotherapy and/or radiation therapy was followed. Data on school attendance and HrQOl was collected during three different weeks, one month (T1), 2.5 months (T2) and 5 months (T3) after start of treatment. Furthermore, demographic and clinical data and school attendance among children who were free from infection before the start of two observation periods (19 days) were analysed regarding the association to the start of antimicrobial treatment. A median of 5 years after diagnosis 63 of the former patients participated in a follow-up study with telephone interviews open-ended and structured questions about school situation and self-rated independence. The survivors’ responses from structured questions were compared with those from age-matched comparison group drawn from the general population (n=257).
Results: School attendance significantly increased during the first 5 months of cancer treatment, while self-reported HrQOl remained decreased. HrQOl was positively related to school attendance. Hospital visits and fatigue were the most common reasons for school absence. School attendance did not appear to increase the risk of infections. Despite that 62% of the survivors, a median of 5 years after diagnosis considered their school situation to be more or less the same as their peers’ situation, a significant proportion reported difficulties in school because of physical and cognitive limitations. The survivors scored significantly higher on the independence dimension than the controls. The results support the encouragement of school attendance during cancer treatment.

NOPHO • NOBOS 2012 103
Free PapersOrAl

104 NOPHO • NOBOS 2012
NOBOS FREE PAPER 1
The first Hospice for Children and Youth in Sweden
Ann Edner, M.D., Ph D., Lilla Erstagården, Ersta sjukhus, Nacka, Sweden
Background: In Autumn 2010 the first hospice for children and youth, lilla Erstagården, opened in Sweden. It was a lot of prework done to do this able. looking outside Sweden the world´s first hospice for children and youth opened in Oxfordshire, UK, in November 1982 and shortly thereafter the United States got the same. Children´s hospice care focuses on life and living. Providing hospice services for children and youth with life- threatening conditions and their families presents an uniquely difficult and rewarding task. One of the challenges faced is that many pediatric referrals come to hospice very late. Parents need the support of hospice care services, but are not willing to give up on aggressive therapies for their child/youth. Results: The first Swedish Hospice for Children and Youth is placed at Erstagården south of Stockholm and have the capacity to take care of 5(-7) children with their families. It´s open for incurable, progressive sickness, but also for irreversible non-progressive sickness where the parents need to be relieved pressure. Preferably patients from the Stockholm area are referred to the Children´s Hospice, but it´s also possible to send patients living outside Stockholm. The palliative care include medical personnel (nurses, doctor), physiotherapist, occupational therapist, psychologist, care for the soul/spirit. We also think that complementary treatment is very important, for example we have introduced the first therapy dog in pediatric care. She is a labradoodle and is named ”livia”. Conclusion: The first hospice for children and youth has now been running for more than a year. Patients and/or their families have been satisfied during the care. The therapy dog has been successfully introduced.

NOPHO • NOBOS 2012 105
NOBOS FREE PAPER 2
DIFFICULT ETHICAL SITUATIONS IN PEDIATRIC CANCER CARE – A GROUNDED THEORY (GT) STUDY OF ETHICAL TEAM DISCUSSIONS
Cecilia Bartholdson, RN, PhD student, Department of women and childs health, Karolinska institute, Stockholm, Sweden, Kim Lutzén, RN, Professor, Cecilia Petersen, MD, PhD, Pernilla Pergert, RN, PhD
Purpose: Pediatric cancer care often entails difficult ethical problems deriving from value conflicts concerning what is morally right to do in the clinical situation. The purpose of this study is to explore healthcare staffs’ experiences of difficult ethical situations in pediatric cancer care. The aim is to (1) evaluate and gain knowledge about ethical team discussions and to (2) evaluate and gain knowledge about main concerns of caregivers during ethical team discussions. Method: Ethical discussions (n:6-8) will be performed at the pediatric oncology unit at Astrid lindgren Children´s hospital in Sweden, three have been done. The ethical discussions will involve multidisciplinary teams in pediatric cancer care. The team discussions are similar to focus group interviews with a moderator and an observer. After the team discussions, individual interviews will be performed (two have been done) and patient records will be collected. Data are presently being analyzed using grounded theory. Results: According to preliminary results caregivers were not aware of their co-workers perceptions regarding the ethical problems before the ethical team discussion. During the team discussion, led by a facilitator, it became clear and more obvious what the ethical problems and arguments held by team members were. Team members felt consistent and showed feelings of trust and understanding. The ethical team discussion give care team members increased confidence in each other and a common direction. It also raised ethical principles and values. Conclusion: Ethical team discussions are important for caregivers in order to create an understanding environment and opportunities for inter-professional ethical dialogues. When all professionals have a chance to express their opinions, arguments and experiences the full picture of the patient’s situation becomes clearer and the decision can be made on a wider basis. Furthermore, hypotheses and variables derived can be used in future research.

106 NOPHO • NOBOS 2012
NOBOS FREE PAPER 3
Guided Self-help as Intervention for Traumatic Stress in Parents of Children with Cancer: Conceptualization, Intervention Strategies, and two Case Studies
Martin Cernvall, MSc, PhD-student, Department of Public Health and Caring Sciences, Uppsala University, Uppsala, Sweden, Per Carlbring, PhD, Umeå University, Gustaf Ljungman, MD PhD, Uppsala University, Louise von Essen, PhD, Uppsala University
Background: Being a parent of a child diagnosed with cancer poses an enormous stressor. Indeed, several parents have difficulties adjusting to such a situation and react with symptoms of traumatic stress, depression and reduced quality of life. However, there is little conceptual work on behavioral mechanisms that contribute to suboptimal adaption in these parents. Objectives/Aim: We present a conceptualization in which experiential avoidance and rumination are suggested to contribute to increased levels of traumatic stress and sub-optimal adaption. Based on this conceptualization, a recently developed intervention for parents of children with cancer, in the form of guided self-help, is presented as well as two case studies serving as an initial evaluation of this approach. Methods: The guided self-help intervention is based on cognitive and behavioral principles and targets arousal, avoidance and rumination specifically. Participants in the case studies were two mothers of children diagnosed with cancer, one on and one off treatment. Both participants provided pre-, post- and follow-up assessments of symptoms of traumatic stress, depression and quality of life. Results/Conclusion: Using Jacobson and Truax (1991) criteria, both participants evidenced clinical significant and reliable improvements in symptoms of traumatic stress, depression and quality of life during the intervention and the results were largely maintained at follow up. This indicates that controlled research is warranted and an ongoing randomized controlled trial investigating the efficacy of this approach is outlined.

NOPHO • NOBOS 2012 107
NOBOS FREE PAPER 4
Multidisciplinary team for children with Craniopharyngiomas
Anette Sjölund, Nurse consultant in pediatric neuro oncology, Pediatric oncology center, Queen Silvia Childrens Hospital, Gothenburg, Sweden, Marianne Jarfelt, MD PhD, Pediatric oncology center, Queen Silvia Childrens Hospital, Gothenburg, Sweden
Craniopharyngiomas are rare benign brain tumors. The survival rate is very high around 90%. However because of the location in the hypothalamic and pituitary region most patients with craniopharyngiomas suffer from multiple deficits in hypothalamic-pituitary function and need hormone replacement therapy. Additionally, many of these patients suffer from other hypothalamic symptoms such as extreme hypothalamic obesity and changes in personality. There is also a risk for more rare complication like daytime sleepiness. Visual loss because of tumor pressure of the optic chiasma may also occur. long-term sequelae substantially reduce the quality of life for these patients and their families. Effective follow up for patients with a craniopharyngioma requires communication and coordination with many different professionals. Therefore we found it very important to centralize the follow up and establish a multidisciplinary team. The team gives information and support to the family in order to control the tumor, optimize the hormonal replacement, prevent difficult eating problems, make neuropsychological investigations and give psychological support. Guidelines have been developed and presented to the regional pediatric clinics. The multidisciplinary team will be evaluated by questionnaires to the parents about the information and support. Another part of the evaluation will be to survey patient cases in order to focus on the benefits of a multidisciplinary team.

108 NOPHO • NOBOS 2012
NOBOS FREE PAPER 5
TRANSITIONING TO EVERYDAY LIFE: ADOLECENT LEUKEMIA PATIENTS LIVED EXPIRIENCE. IMPLICATIONS FOR NURSING CARE IN AN OUT PATIENT CLINIC
Dorte Brinkmann Kristensen, Pediatric oncology ward 303B, Aalborg Hospital, Denmark, Nurse Mette Mølgaard Nielsen,Pediatric oncology ward 303B, Aalborg Hospital, Denmark
Purpose: This project aims to generate knowledge about what kind of care the young leukaemia patient needs after a long and in many ways restricted period of treatment. In the survey six seventeen to twenty-one year old leukaemia patients are asked about their experience with returning to everyday life and how they cope with being a survivor after a long treatment for a serious disease. The purpose of the survey is to examine what kind of care the young leukaemia patient might need subsequent to treatment for leukaemia. Method: Six out of eight possible informants participated in the survey. The survey was performed in 14 days. The interviews were preformed based on an interview guide advocating a questioning technique derived from a constructivist way of thinking. The questions are asked as reflexive questions. The young patients are encouraged to ask the questions, and to answer back again, based on what is important for him or her. Outcome: Five out of six young leukaemia patients have managed to get back to their normal lives. Even though the young patients have a good youth life, they still have unresolved thoughts and issues that they would rather not talk about. None of the young patients believes that the treatment would affect the future. Conclusion: - The young leukaemia patients need a network to support them when returning to a normal life. - The young leukaemia patients need support in coping with the concerns and the emotional strain the treatment can create in the subsequent period, in a way that is adapted to the young patient’s personal development. - The young leukaemia patients wish to be met in the oncology outpatient ward with the special needs teenagers have.

NOPHO • NOBOS 2012 109
NOBOS FREE PAPER 6
What about teenagers and young adults
Maria Olsson, Reg Nurse, Pediatric Oncology unit, Queen Silvias Childrens Hospital, Gothenburg, Sweden.
Background: Today the focus on young people with cancer increase around the world, especially the western parts of the world, where the issue has been that this age group needs to be seen as a subgroup among cancer patients. In these countries the questions are raised on, what is the knowledge in aetiology of this age group, where to treat them and what kind of healthcare professionals are needed in the care for young persons. Aim: The aim is to describe the areas of care for teenagers and young adults with cancer.
Method: literature, study visits and experience.
Result: The result will present a summary of definitions and descriptions of the young cancer patient in Sweden. Further on it will give a summary of different kinds of care systems around the world for teenagers and young adults. Finally the presentation will give a description on health care issues that are important for teenagers and young adults.
110 NOPHO • NOBOS 2012
NOBOS FREE PAPER 7
Young adult cancer survivor’s experiences of psychosocial rehabilitation
Jens M Nygren, PhD, School of Social and Health Sciences, Halmstad University, Halmstad, Sweden, Jennie Stigmar RN
Background: Increased knowledge on the long-term health outcomes of childhood cancer survivors has focused attention towards psychosocial oncology during the rehabilitation process. For school-age children school attendance after cancer treatment correlates with the experience of health-related quality of life and innovative interventions for psychosocial oncology will therefore benefit from integrating school nurses in communication of the resource. Aim/Objective: The objective of this study was to establish innovation incentives based on young adult cancer survivor’s experiences of psychosocial rehabilitation following their treatment. Methods: Eligibility for the study cohort included diagnosis and treatment for paediatric acute lymphoblastic leukemia in Sweden prior to age 15 years between 1985-1997 and survival for at least 10 years (n=416). A brief questionnaire including both closed and open questions was sent out by mail to all eligible subjects still living in Sweden and with a valid address in the population register (n=374). responses (n=213, 57%) were analysed by descriptive statistics and qualitative content analysis. Results/Conclusions: Only a few of the survivors in the cohort had maintained contact with their paediatric oncology clinic (n=30, 14%). However, continuation of regular clinical check-ups related to cancer treatment (n=61, 28%) were more common. Of those who had no contact with health services, 61% were satisfied and 39% dissatisfied with the contact being terminated. A majority of survivors reported that they did not have experience of psychosocial rehabilitation focused on knowledge formation (58%), strategies for action (66%), or support (58%) to continue life the best way possible. This study highlights the potential for innovative resources for psychosocial rehabilitation during adolescence and the importance of supporting children’s and young adult’s initiatives to re-establishing contact with health care related to psychosocial rehabilitation. The school nurse can play a significant role in communication of such resources due to their proximity to children’s daily life post treatment.

NOPHO • NOBOS 2012 111
NOBOS FREE PAPER 8
Children’s health, when diagnosed with cancer: their own and their parent’s experiences.
Laura Darcy, PhD student & Lecturer, Insitution for Caring Science, University College Borås, Borås, Sweden
Background: Care and treatment within paediatric oncology has been very successful, with the majority of children surviving their illness. However, this requires intensive periods of treatment, often with debilitating side effects and long and frequent hospital stays. To allow qualified and evidence based care to children requires increased knowledge of how cancer affects the small child’s life. Aim: To explore the child’s health and everyday life shortly after receiving a cancer diagnosis. Method: Data has been collected from thirteen newly diagnosed children and their parents connected to the oncology unit, The Queen Silvia’s Children’s Hospital, Gothenburg, though semi-structured interviews. A preliminary analysis has been made using qualitative content analysis. Preliminary Results: Four major themes were identified: The Invisible Child, A Sense of Powerlessness, Social Isolation and Integrity under Attack. All parents express that the research situation was the first where the child was in focus rather than the cancer. All speak of two different children, the child before and after diagnosis and treatment. The child feels powerless over her rapidly changed everyday world. From having gained self control many now need necessary assistance with their basic and every day needs e.g. using diapers, needing a pram for mobilisation, and assistance with eating or sleeping. From having attending preschool and having friends, most are now isolated, the child now having or no opportunities to mix with other children. The need for physical nearness with their parents and siblings is central. The child’s integrity is under constant attack from caregivers. Play therapy is mentioned by all children and parents as vital in keeping that which is healthy, in focus. Many children often look at old photos and films of themselves but are reluctant to be photographed or filmed at present.

112 NOPHO • NOBOS 2012
NOBOS FREE PAPER 9
The impact of communication prior to and following the loss of a brother or sister to cancer - A nationwide long-term follow-up.
Alexandra Eilegård, RN, PhD, Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden, Gunnar Steineck, MD, PhD, Tommy Nyberg, MSc, Ulrika Kreicbergs, RN, PhD
Background: living with a cancer ill child puts a strain on all family members, even though the manifestation of fear and worry associated with the illness and the prognosis may differ. Not only is the illness in itself distressing; but also the treatment side effects may be threatening. Both the physical and psychological symptoms and side effects in the ill child (e.g. anxiety and pain) may be difficult and unsettling for the parents and the siblings’ to witness. Siblings tend to become invisible during the illness period and possible even more so after bereavement.
Objective: To assess long-term psychological distress in siblings who lost a brother or sister to cancer two to nine yeas earlier, as compared with a control group of non-bereaved siblings from the general population.
Design: During 2009, we conducted a nationwide follow-up study in Sweden, using an anonymous study specific questionnaire. Siblings who had lost a brother or sister to cancer between the years 2000 and 2007 were invited to participate, and also a control group of non-bereaved siblings from the general population. The Hospital Anxiety and Depression scale (HADS) was used to measure psychological distress; and to test for differences in the ordinal outcome responses between the groups, we used Wilcoxon-Mann-Whitney rank-sum test.
Results: Among the bereaved siblings 174/240 (73%) participated and among the non-bereaved 219/293 (75%). Self-assessed low self-esteem (p=0.002), difficulties falling asleep (p=0.005) and low level of personal maturity (p=0.007) at follow-up was more prevalent among bereaved siblings. However, anxiety (p=0.298) and depression (p=0.946), according to HADS, were similar.
Conclusion: Bereaved siblings are at increased risk of low self-esteem, low level of personal maturity and difficulties falling asleep as compared with non-bereaved peers. Yet, the bereaved were not more likely to report anxiety or depression.

NOPHO • NOBOS 2012 113
NOBOS FREE PAPER 10
BEDSIDE HANDOVER Parents and children´s perception of change-of- shift report at the bedside
Liselott, Pettersson, Paediatric Onology Nurse, Paediaric hematology & oncolgy, Uppsala University Children´s Hosptal, Sweden, Katarina Wallin, Paediatric Onology Nurse, Paediaric hematology & oncolgy, Uppsala University Children´s Hosptal, Sweden
With today’s requirements of laws, decrees, regulations and with patients as well as relatives expectations regarding, both information about and participation in treatment and care decisions, force the health care system to improve and secure this with new reporting systems.Parents at the paediatric hematology & oncology ward in Uppsala, Sweden has submitted comments, both written and spoken about that they do not receive adequate and continuous information about ongoing planned care and treatment during hospitalization in the hospital.The aim of this project was to investigate the parents and children’s view on the information and participation concerning the child’s care and treatment at the paediatric oncology ward. The aim was also to test a new reporting system and introduce this at the unit.The results were assessed by a pre- and post questionnaire answered by children and parents in connection to implementation of a new reporting system - Bedside Handover was implemented. In the patient room with child and parents present, the outgoing nurse reported to the incoming ward staff through a checklist.The results showed that all parties had knowledge of planned care, treatment, which improved the flow of information, including the participation of parents and child concerning the child’s care and treatment. This reporting system puts the patient in focus, and understandable communication is used. Misunderstandings, frustration and irritation can be avoided and encouragement in participation is lifted.Bedside handover was introduced as a daily routine in december 2010 at the paediatric hematology & oncology ward in Uppsala. Evaluation with questionnaire 10 months after the introduction confirms that children and parents receive satisfactory information regarding planned care and treatment and feel they are involved in the daily care. Keywords: bedside report, parent, children, information, participation
[email protected]@akademiska.se

114 NOPHO • NOBOS 2012
NOBOS FREE PAPER 11
Swedish nurses’ descriptions of being an expert nurse in paediatric oncology care
Karin Enskär, Professor, Department of Nursing, School of Health Sciences, Jönköping University, Sweden and School of Life Sciense, Skövde University, Sweden
Paediatric oncology is a highly specialized area, and has therefore a need for nurses with specialist knowledge. The transition from being a novice nurse to an expert in a certain field is complicated. The aim of this study was to describe paediatric oncology nurses perceptions of their role of an expert nurse in paediatric oncology care. 66 nurses working in paediatric oncology care participated through writing their narrative. The narratives were analyzed with content analysis. Three categories were found; 1, An expert has confidence in his or her knowledge; 2, An expert provides high quality care; and 3, An expert is given possibilities for professional growth. The conclusion is that when the nurse s given possibilities for continuous education and reflection, and have a feeling of satisfaction at being able to fulfil the child/family’s needs, it can enhances the nurse’s to become experts and maintain expert competence.

NOPHO • NOBOS 2012 115
NOBOS FREE PAPER 12
Proton therapy in Switzerland
Anna Silfver, Fagersta, Sweden
Anna Silfver, mother of five children including 6 year old boy who has a brain tumor. Was told in August 2008 that Melwin was affected by a brain tumor Ependymoma grade II. Surgery was done immediately, which removed a considerable amount of the tumor, but all would not go away. The tumor which at this time remains in the cerebellum is growing all around (on both sides of) the brainstem. More surgery is not an option because it´s joined with the sensitive parts of the central nervous system and large arteries, which means too large life-threatening risks. In September -08 began a chemotherapy program to hopefully be able to slow tumor growth. Melwin struggled through this tough and intensive chemotherapy until the end of April -09. The tumor did not, unfortunately, care much about the chemotherapy, it has not grown, but not decreased slightly, the tumor is completely unchanged. This meant that the doctors at Uppsala University Hospital, where Melwin always been treated, felt that we must move on to stage two, proton radiation. Proton radiation was seen as the only chance for Melwin, the only way to get the tumor to reduce or, at best, die completely. Conventional radiation was not to think about, when the damage would be much too large to healthy tissue in Melwins brain, which is still under development. However, it was several times the numbers that Melwin would undergo conventional radiation at the radiation Institute in Uppsala. It was determined that Melwin would go abroad to get their proton radiation in which case this is not done in Sweden during anesthesia. To anesthetize Melwin at each radiation time was a must, since he is far too small to be able to sit still and fixed in the head during radiation. The tours were a lot before we got away. Would we be able to go the whole family. Or only one adult with Melwin? We would stay in Switzerland for 8 weeks, because Melwin would do the radiation 33 times. The County Council were contacted. Who would pay for all this? How was the family affected of all this?

116 NOPHO • NOBOS 2012
NOBOS FREE PAPER 13
Internet based coaching for children after brain tumor treatment
Anette Sjölund, Nurse consultant in pediatric neuro oncology, Pediatric oncology center, Queen Silvia Childrens Hospital, Gothenburg, Sweden
As part of my work as a nurse consultant in pediatric neuro-oncology I often meet children treated for brain tumor suffering from cognitive sequelae with effects on learning capacity and the school situation. During the last two years a study at my institution aims to find out if physical activity may significantly improve cognitive function in these children. So far fourteen children aged 7-16 years have played physical active computer games during 10 weeks for 30 minutes /day. My part has been to provide coaching to the child once a week in order to support the child and the family during the intervention. The coaching has been computer based, using a web camera and sound. Coaching sustained the child’s experience of playing computer games which helped to motivate and encourage the child to continue the study. For the coach communicative and technical skills are important. Internet based coaching may strengthen the child’s independence. This computer based coaching technique can be an instrument for communication and support for children treated for brain tumor and suffering from cognitive sequelae

NOPHO • NOBOS 2012 117
NOBOS FREE PAPER 14
Education day for relatives of children with cancer
Charlotte Castor, Pediatric Nurse, Lund, Sweden
When a child is ill in cancer the whole family becomes involved emotionally and literally, often over a long period of time. It is well known that the families are in great need of support and understanding from people close to them and not only from hospital staff. In order to facilitate this, interventions are made from the hospital towards the school of the sick child and its siblings. Also special attention is given to brothers and sisters by an assistant nurse working dedicated towards siblings.
The aims of this education day, taken place in a hospital in the south of Sweden, were to provide close relatives and friends with knowledge which would make it possible for them to give better support to the sick child and its family.
In 2011 an intervention took place which offered the opportunity for all parents of a child newly diagnosed with cancer to invite relatives to attend an a one-day education session in the hospital. 55 relatives, mostly grandparents, aunts and uncles, participated. During 6 hours, representatives from different professions provided education in childhood cancer, nursing-concerns during treatment, psychosocial needs and symptoms, and information on available support groups. During the day, financial support from Barncancerföreningen Södra made it possible for us to serve lunch, coffee and fruit.
At the end of the day evaluation forms were collected from the participants. 2 months later evaluations and comments from the families were also collected. The evaluation forms are presently being analysed, and will be presented at NOBOS along with, experiences and details of the program.

118 NOPHO • NOBOS 2012
NOBOS FREE PAPER 15
Participatory innovation process for development of a digital peer support service for children with cancer
Eva-Lena Einberg, RN, MNSc, School of Social and Health Sciences, Halmstad University, Halmstad, Sweden, Petra Svedberg, PhD, Pontus Wärnestål, PhD, Michel Thomsen, PhD, Jennie Stigmar, RN, Karin Enskär, PhD, Maria Åkesson, PhD, Jens Nygren, PhD
Background: Surviving cancer during childhood imposes a number of physical and psychosocial difficulties later in life. Peer support has been recognised as an important contributor to health and well-being but empirical evidence that could guide development of peer support programs for school aged children is scarce. The process presented here is focused on generic exploration of children’s needs and expectations related to peer support innovations to promote health and wellbeing of children with cancer.
Aim: To establish a participatory innovation process that grasps the underlying behaviours and goals of children that will affect the design of a digital peer support service.
Method: Focus group interview is a child-friendly technique that promotes participation and access to children’s perspectives, insights and experiences related to their health. Healthy children 8-12 years of age were recruited from a local elementary school. Focus groups (n=5 groups) were carried out in two sessions for each group (n=4 children per group) with an interval of 1-2 weeks. Adjustments were made between each focus group to adapt the meeting structure to a level commensurate with the children’s experience, age and abilities and to focus discussions on innovation incentives related to a digital peer support service.
Results: The adaptation process involved adjustments of the focus group structure to match children in the selected age group and to the aims of the innovation process. A mixture of informative and creative techniques (such as open questions, brainstorming, drawing, photography and storytelling) assisted the children in talking and expressing themselves. The children were pleased to participate and wanted to meet again in this kind of study group. The adapted focus group sessions are now being used in the research and innovation process with children (8-12yrs) with experience of cancer treatment.

NOPHO • NOBOS 2012 119
POSTEr

120 NOPHO • NOBOS 2012
NOBOS POSTER 1
Psychological health in siblings who lost a brother or sister to cancer two to nine years earlier
Alexandra Eilegård, rN, PhD, Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden, Gunnar Steineck, MD, PhD, Tommy Nyberg, MSc, Ulrika Kreicbergs, rN, PhD
Background: When a child is diagnosed with cancer the whole family will face a traumatic and life changing period. Siblings of cancer ill children tend to be invisible and forgotten during the illness-period and possible even more so when bereaved.
Objectives/aim: To study siblings’ psychological health two to nine years after the loss of a brother or sister to cancer, in relation to communication with health-care professionals, family and others prior to and after the loss.
Method: A Swedish nationwide follow-up study of individuals, who had lost a sibling to cancer two to nine years earlier, was conducted using a study-specific questionnaire. And The Hospital Anxiety and Depression scale (HADS). Data are presented as percentages (%) and relative risks (rr).
Results: 174 (73%) sibling’s participated in the study. Those participants who avoided the health-care professionals (other than physicians), for fear of being in their way during their brother or sister’s last month of life, reported an increased risk of anxiety as compared with those who did not avoid them (HADS 11), rr=2.2 (1.1-4.6). Those siblings who talked less about their feelings regarding their brother or sister’s illness (with other than family had an increased risk of anxiety rr=2.8 (1.3-6.2). As did siblings who avoided talking with/asking parents their own feelings regarding their deceased child, rr=2.4 (1.1-5.4).
Conclusion: When bereaved siblings avoid talking with health-care professionals, for fear of being in their way, (especially during the last month in the cancer ill brother or sisters’ life) their risk of long-term anxiety is increased. Additionally, not talking to others (including their parents) also increases the siblings’ risk of long-term anxiety.

NOPHO • NOBOS 2012 121
NOBOS POSTER 2
Bereaved siblings’ perception of participating in research - a nationwide study
Alexandra Eilegård, rN, PhD, Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden, Gunnar Steineck, MD, PhD, Tommy Nyberg, MSc, Ulrika Kreicbergs, rN, PhD
Background: The sparse research on siblings bereaved due to cancer, as compared to non-bereaved, may be explained by ethical, methodological and practical concerns. A major concern is fear of inflicting harm by asking about their deceased brother or sister.
Objectives/aim: The objective of the present study is to examine bereaved siblings perception of research participation.
Method: A Swedish nationwide study on avoidable and modifiable healthcare related factors in paediatric oncology among bereaved siblings who lost a brother or sister to cancer between the years 2000 and 2007. Data are presented as proportions; differences between groups were statistically tested at the five percent significant level using Fisher’s exact test.
Results: Out of 240 eligible siblings, 174 responded (73 %). None of the siblings (0/168) thought their participation would affect them negatively long-term. However, 12 percent (21/168) stated it was a negative experience to fill out the questionnaire; 84 % (142/169) found it to be a positive experience. Women were more likely to report their participation positive in a long-term perspective compared to men (p=0.018).
Conclusions: None of the bereaved siblings in this Swedish nationwide study anticipated any long-term negative effect from their research participation. A majority reported it as positive to revisit their needs and experiences throughout their brother or sisters’ illness and death two to nine years following the loss. We believe that the stepwise approach used in this study contributed to the high acceptance.

122 NOPHO • NOBOS 2012
NOBOS POSTER 3
Debriefing; A Method to Cope When a Child Dies
Anna Hjort, rN, Paediatric Hematology and Oncology A4, Aarhus University Hospital, Aarhus N, Denmark
Background: While the health care staff are competent in caring for palliative children and their families little focus has been put on the needs for support and reflection among the health care staff themselves. Debriefing is a meeting in which each participant can express their thoughts and feelings in relation to an event. Debriefing is a collective support method in which a defragmented story can be collected into a coherent story. In 2007 debriefing was integrated as a method in the department.
Aims: To support each individual health care staff member to develop professional and personal skills after the death of a patient in the department or when the child dies at home.
Methods: A debriefing coordinator summons internal and external collaborators to debriefing maximum 14 days after the death of a child. Debriefing is scheduled to one hour. Patient confidentiality is mandatory. If general or specific issues appear participants are responsible themselves to take this further if needed. An important aspect of debriefing is to make room for the participants to express their thoughts individually. listening only is also a form of participation. No explanations are requested on rights or wrongs. The main objective is to ensure that each individual leaves debriefing with a feeling of relief. No loose ends should be left behind. In 2008, a questionnaire was sent out both to the group of nurses and the multidisciplinary team to evaluate the concept of debriefing in the department.
Results: The questionnaires supported the healthcare staffs´ satisfaction with the concept of debriefing. Ethical and professional reflections within the multidisciplinary team are found to be fruitful to all concerned when terminating and progressing. As a result of debriefing the palliative care and procedures around patient and family in a difficult situation have improved significantly.

NOPHO • NOBOS 2012 123
NOBOS POSTER 4
Diase Specific Teams - a Way to Improve Quality of Care.
Helle Borg Christensen, rN, Department of paediatric haematology and oncology, Aarhus University Hospital, Arhus, Denmark, Lis Blond Poylsen, CN, Department of paediatric haematology and oncology, Aarhus University Hospital, Arhus, Denmark,
Background: While the health care staff are competent in caring for palliative children and their families little focus has been put on the needs for support and reflection among the health care staff themselves. Debriefing is a meeting in which each participant can express their thoughts and feelings in relation to an event. Debriefing is a collective support method in which a defragmented story can be collected into a coherent story. In 2007 debriefing was integrated as a method in the department.
Aims: To support each individual health care staff member to develop professional and personal skills after the death of a patient in the department or when the child dies at home.
Methods: A debriefing coordinator summons internal and external collaborators to debriefing maximum 14 days after the death of a child. Debriefing is scheduled to one hour. Patient confidentiality is mandatory. If general or specific issues appear participants are responsible themselves to take this further if needed. An important aspect of debriefing is to make room for the participants to express their thoughts individually. listening only is also a form of participation. No explanations are requested on rights or wrongs. The main objective is to ensure that each individual leaves debriefing with a feeling of relief. No loose ends should be left behind. In 2008, a questionnaire was sent out both to the group of nurses and the multidisciplinary team to evaluate the concept of debriefing in the department.
Results: The questionnaires supported the healthcare staffs´ satisfaction with the concept of debriefing. Ethical and professional reflections within the multidisciplinary team are found to be fruitful to all concerned when terminating and progressing. As a result of debriefing the palliative care and procedures around patient and family in a difficult situation have improved significantly.
[email protected]@rm.dk

124 NOPHO • NOBOS 2012
NOBOS POSTER 5
TOWARDS A DAY HOSPITAL
Marita Nieminen, rN, paediatric haematology and oncology, Tampere University Hospital, Tampere, Finland, Mikko Arola, Deputy Chief Physician, Sirpa Bamberg, Ward Manager, Minna Hautala, rN, Ville Laine, rN, Saila Mäkinen, rN, Marjatta Mattsson, Medical Secretary, Marjo Virkki, Quality Instructor
Background: The paediatric haematology and oncology unit at Tampere University Hospital has 12 beds and 8-9 daily appointments at the outpatient clinic. The unit will move to new facilities in 2014. The operation of the unit will change so that only haematological and oncological patients will be treated at the ward. At the moment the ward also treats other patients in the speciality of internal medicine. The new layout is designed for 12 beds at the ward and 4 beds at the day hospital, and the operation of the outpatient clinic will continue almost unchanged.
Objectives: The operation will be divided into three units: the ward, the day hospital and the outpatient clinic. The aim of this project was to look at the job descriptions of the different occupational groups as well as primary nursing, to map out the demand for additional training, and to plan these to match with the new operation. Another aim was to plan the operation to be more cost-effective and flexible by e.g. restructuring the heavy telephone traffic.
Methods: A questionnaire on the operation of the day hospital and the demand for additional training was conducted among the staff at the paediatric haematology and oncology unit. Job descriptions of the nurses, the primary nurses, the secretaries and the instrument technician were updated. The heavy telephone traffic was directed at a single nurse, and families were also advised to call the secretary when e.g. scheduling appointments.
Results: Job description of the nurse will be clearer because in the future the unit will only treat haematological and oncological patients. In the future, the contribution of nurses and secretaries can also be used in a more flexible way. The primary nurse takes care of the families of patients with multiple problems and/or patients in terminal stage in a more flexible way within the unit. With more spacious and appropriate facilities, patient and occupational safety will improve. With appropriate facilities, clear job descriptions and further training, work satisfaction and motivaton are likely to improve. With new and functioning facilities, the multidisciplinary team will be able to provide the family with a good quality of treatment and care.

NOPHO • NOBOS 2012 125
NOBOS POSTER 6
Acknowledging the school-aged siblings of children with cancer at Tampere University Hospital ward L06
Minna Rautanen, rN, Paediatric Haematology and Oncology Ward (l06), Tampere University Hospital, Tampere, Finland, Leena Ahola-Jalonen, rN, Tiina Vaaja, rN
The scope of this study is to clarify and address the attention and support families have experienced during their stay at Tampere University Hospital ward l06. We are also aiming to understand the family requirements and expectations for supporting siblings in more detail. The basic assumption in this study is to not allow siblings to visit the ward during the stay. There is limited space in the ward, however a new layout is in the planning phase. According to systematic reviews, siblings of cancer patients seem to suffer from psychosomatic disorders.
Data acquisitions were made with a questionnaire, which was delivered to six (6) families. The questions were related to acknowledging the siblings 3-12 months after the cancer was diagnosed. The answers were sorted according to themes and similarities were observed.
Two main themes were discovered:ing, empowerment and exhausting experiences. In the improvement area three main themes rise into consideration, physical environment, exact and concrete information about care and the examinations and issues regarding psychological load (pressure).
As a result we would like to highlight the following: More free space (rooms etc) is needed. We suggest frequent meetings with the primary nurse at the beginning of treatment. SSupport from a psychologist should be available in a location close to home in order to carry on with this activity if sudden problems occur. A DVD by Sylva, published in 2012, will introduce the care and treatment of a child with cancer. In addition, it is highly recommended to publish information pages or a video onon the ‘s ward internet pages.

Comfortable and very convenient rollaway for spouses and other relatives
Trusted by hospitals worldwide!
Order online www.bed-bath.com or call +46 42 26 66 66
NOPHO • NOBOS 2012 127
ENJOY COPENHAGEN
At the waterfront
NOPHO Annual Meeting 2013
CopenhagenMay 31st-June 4th

128 NOPHO • NOBOS 2012

Thank you for visiting Uppsala and the NOPHO NOBOS congress 2012
NO
PH
O 30th
an
nu
al &
NO
BO
S 9th
meetin
g a
nd
con
gre
ss Up
psa
la, S
wed
en
, May 19 –
22, 2012
Programme and Abstract Book
NOPHO NOBOS Meeting and CongressUppsala, Sweden, May 19 – 22, 2012
30years