noonan syndrome
DESCRIPTION
NOONAN SYNDROMETRANSCRIPT

WELCOME TO CASE WELCOME TO CASE PRESENTATIONPRESENTATION
PRESENTER:DR. Md Akhtaruzzaman MD STUDENT
MODERATOR:DR. Asraf uddin chowdhuryAssistant professor of cardiologyNICVD
Particulars of the patientParticulars of the patient
Name- Mr. Raihanul Islam
Age- 21 years
Address: Vill; Lognosa, PO. Borura, Dist; Comilla.
Date of admission: 23/04/09
Chief complaintChief complaint
Exertional palpitation and shortness of breath – 2 months
History of present illnessHistory of present illnessPatient developed palpitation for last 2
months which is precipitated by physical exertion and relieved by rest.
He also complain of shortness of breath for two months. Initially it occurred on moderate exertion but now it occurs on
minimal exertion but not at rest. There is
no diurnal variation. He gave no history of orthopnea and PND. It is not associated with cough.
There is no H/O chest pain,flushing, vertigo, heat intolerance, alteration of consciousness, syncope and polyuria,
No H/O thrombo-embolic manifestation.

History of present illness-Cont’dHistory of present illness-Cont’d Since his childhood, he developed
palpitation and shortness of breath during playing and running but no H/O squatting or color change.
He admitted in this hospital 2 months back and referred to surgery department.
Past History: No history suggestive of cyanotic spell or
rheumatic fever.
Treatment history :
He is taking Tab. Propranolol .
• Family history: Lives with parents and 2 brothers.
No H/O congenital heart disease in his family.

Social history: Student of Hons. 1st year
He belongs to middle class family.
Immunization history: He completed schedule of immunization.
General ExaminationGeneral ExaminationPatient cooperative, decubitus on choice.
Webbing of neck, low set ear, bilateral ptosis – present
No lymphadenopathy
Anamia, cyanosis, jaundice and clubbing- Absent
Thyroid gland – Normal
Pulse – 74 bpm, regular
BP – 110/70 mm of Hg
Respiratory rate – 18/min
Temp – normal



Systemic ExaminationSystemic Examination
Cardiovascular system:
• Pulse – 74 bpm, normal in volume & character, no radio radial & radio femoral delay. Condition of the vessel wall – normal, All peripheral pulses are symmetrically present.
• BP – 110/70 mm of Hg
• JVP – Prominent ‘a’ wave present.
Precordium
Shape of the chest – Pectus excavatum
Apex beat at left 5th intercostal space, medial to mid clavicular line & normal in character.
Lt. parasternal heave & epigastric pulsation – Present.
No palpable P2
Systolic thrill present at the Pulmonary area.
Cardiovascular system: Cont’d
S1 – normal, Aortic component of S2 normal and pulmonary component of S2 is soft.
There is ejection systolic murmur, grade 4/6 in pulmonary area radiating to left clavicle which increased during inspiration.
There is ejection click at pulmonary area, more marked during expiration
There is a pansystoloic murmur of grade 3/6 in left lower parasternal area which increased during inspiration.


Salient featureSalient featureMr Raihanul Islam 21 years of age, non-
diabetic, normotenssive admitted with complaints of exertional palpitation and dyspnoea since childhood which is increased for the last two months . He gave no history of cyanotic spell or and history suggestive of rheumatic fever past.
On examination, there is bilateral congenital ptosis ,webbing of neck and low set ear .
Pulse is regular and prominent ‘a’ wave in JVP.

There is a pectus excavatum deformity of chest wall. Apex beat is palpable at left 5th intercostal space, medial to midclavicular line and normal in character. Left parasternal heave and epigastric pulsation present. P2 not palpable.
There is systolic thrill in pulmonary area.
S1 normal in apical area, P2 is soft.
There is harsh ejection systolic murmur of grade 4/6, heard over pulmonary area which is louder during inspiration radiating to the left clavicle.

There is ejection click at pulmonary area, more marked during expiration
There is a pansystoloic murmur of grade 3/6 in left lower parasternal area which increased during inspiration.
Provisional diagnosisProvisional diagnosis Pulmonary stenosis with Noonan syndrome
Differential diagnosis:VSD with Noonan syndrome
ASD with Noonan syndrome.
Aortic stenosisNoonan syndrome.

INVESTIGATION:INVESTIGATION:
Hb% - 13.6 gm/dl
ESR- 26 mm in 1st hour
T.C- 6,800/Cmm
D.C- N-64%
L-32%
E-2%
M-2%
RBS- 4.4 mmol/L
S.Creatinine-1 mg/dl
S. Na+- 135 mmol/L, S. K+- 3.4 mmol/L

ECG:
Left axis deviation
Poor progression R wave in chest lead
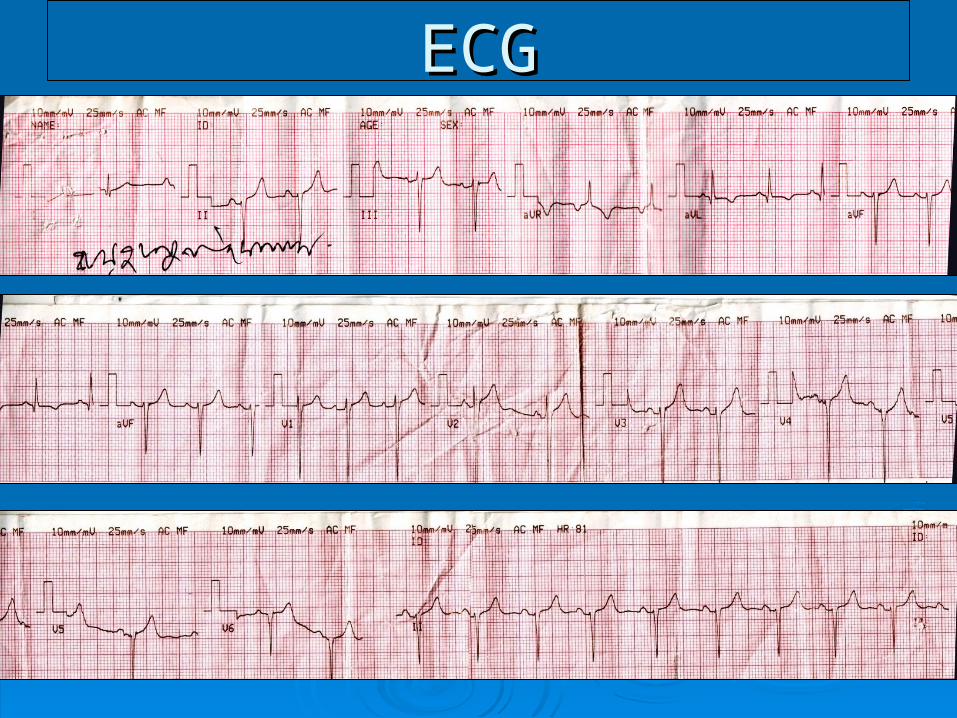
ECGECG

X – RAY CHEST P/A VIEW :
Oligaemic lung field
Post stenotic dilatation of pulmonary artery
Mild cardiomegaly with RV type apex

CHEST X-RAY P/A CHEST X-RAY P/A VIEWVIEW
ECHOCARDIOGRAM:
Severe pulmonary stenosis mainly valvular (PPG 70mm of Hg)
Asymmetrical septal hypertropy with mild SAM
TR grade II, mild PR.

CARDIAC CATH.CARDIAC CATH.Cardiac cath; pressure oxymetry(per)
SVC-
high -59
low -62
IVC-
high -78
low -76
RA-high -65
mid 13/8/10 -66
low - -68
RV body- 120/15/ 40 -66
EDP 20
No left to right shunt
CATH FINDINGS: Pressure study shows:
High right ventricular systolic pressure and right ventricular end diastolic pressure,
High RA mean pressure
OXYMETRY shows:
No significant oxygen stepup
Trajectory shows no abnormal communication.
Graphy; Left brachiocephalic venography shows left persistant superior venacava.
RV graphy shows both valvular and infundibular stenosis.
Post stenotic dilation of main pulmonary artery.

CONFIRMED DIAGNOSIS :
Pulmonary stenosis
Persistent left superior venacava
Noonan syndrome


