nonsurgical management of inflammatory …...nonsurgical management of inflammatory periimplant...
TRANSCRIPT

Non
peri
impa
Avinash S. Bidra
Assistant Professor and Assistant Pro
The Journal of Prosthetic
surgical management of inflammatory
implant disease caused by food
ction: A clinical report
, BDS, MSUniversity of Connecticut Health Center, Farmington, Conn
The incidence, etiology, diagnosis, and management of infections and inflammatory disease around dental implants continueto be controversial. Although various researchers have described different etiologies and their ensuing treatments, none haveproven to be definitive. Terms such as periimplant mucositis and periimplantitis have gained popularity. Food impaction intothe periimplant sulcus and its role in inflammatory periimplant disease has not been previously reported in the literature. Thisarticle describes the nonsurgical management of a patient with a maxillary implant-supported overdenture, a recent historyof pain, and suppuration around one of the implants. A detailed analysis of the patient’s history and clinical findingsindicated a differential diagnosis of impaction of husks of masticated sunflower seeds into the periimplant sulcus. Thesituation was successfully resolved in 1 week by local irrigation with 0.12% chlorhexidine gluconate and the use of systemicantibiotics. (J Prosthet Dent 2014;111:96-100)
The incidence, etiology, diagnosis,and management of infections andinflammatory disease associated withdental implants are controversial.1-4
Inflammatory periimplant disease canbe broadly grouped into plaque-induced inflammatory diseases andnonplaque-induced inflammatory dis-eases (Table I). Historically, the terms‘periimplant mucositis’ and ‘peri-implantitis’ have been used to describeplaque-induced inflammatory diseasesaround dental implants.1 Little reliableevidence is available regarding themost effective interventions for treatingperiimplantitis.2,3 Periimplant mucosi-tis has been defined as “the presenceof inflammation in the mucosa at animplant, with no signs of loss of sup-porting bone.”4 However, the definitionof periimplantitis is controversial andhas been defined variously by differentsources. In the Glossary of PeriodontalTerms, it is defined as “inflammationaround a dental implant and/or itsabutment.”5 An alternative, more-specific definition is “plaque-inducedprogressive marginal bone loss ob-served on radiographs with clinicalsigns of infection of the periimplantsoft tissues.”2 A definition from arecent consensus group has describedperiimplantitis as “infection with
gram Dir
Dentis
suppuration associated with clinicallysignificant progressing crestal bone lossafter the adaptive phase.”6
Although these definitions appearsimilar, and state that periimplantitis isan infection with progressive bone loss,the key difference is one definition’semphasis on dental plaque and theother’s emphasis on the presence ofsuppuration. Although the implicationthat plaque and its associated patho-genic microorganisms cause dental-implant infection is controversial, arecent consensus group noted thatmany other etiologic factors may causeinfection, with progressive bone loss,and argued that periimplantitis is aninappropriate term to describe all thevarieties of progressive bone lossaround dental implants.6
Food impaction around natural orartificial teeth is a well-recognizedproblem in dentistry. The Glossary ofPeriodontal Terms defines food im-paction as “the forceful wedging offood into the interproximal space bymasticatory pressure (vertical impac-tion) or the forcing of food interprox-imally by tongue or cheek pressure(horizontal impaction).”5 For implantrestorations, this can also include thewedging of food into the periimplantsulcus. Common foods that are
ector, Post-Graduate Prosthodontics; Private p
try
empirically associated with food im-paction include popcorn, seeds, le-gumes, and nuts. The hull (husk)found in most seeds, including sun-flower seeds, is primarily composed ofcellulose,7 a polysaccharide that cannotbe broken down by human enzymes.8
The difference in the orientation ofsupracrestal connective tissue betweennatural teeth and dental implants iswell understood.9 The fibers around theimplants run parallel to the abutmentsurface and only adhere to the abut-ment surface as opposed to beingattached.9 As a result, the periimplantsulcus may be predisposed to foodand foreign body impactions.
Although evidence-based dentistryhas grown, clinical reports are stillconsidered important. As in medicine,they are able to detect novelty and formthe basis for detecting new concepts,etiologic clues, adverse effects, and newtreatments.10 In addition, clinical re-ports provide a foundation for progressin clinical science, independent of basicsubjects or epidemiologic insights.10
The purpose of this clinical report isto describe the nonsurgical manage-ment of a patient with a maxillaryimplant-supported overdenture and arecent history of dental implant infec-tion caused by food impaction.
ractice, Meriden, Conn.
Bidra

Table I. Comparison of 2 different types of inflammatory periimplant disease
ComparisonElement
Plaque-induced InflammatoryPeriimplant Disease
Nonplaque-induced InflammatoryPeriimplant Disease
Type ofpresentation
Chronic Acute or chronic
Incidence Controversial and not well documented Not well documented
Descriptionand etiology
(1) Periimplant mucositis (restricted to softtissues around implant)4; (2)
periimplantitis (includes soft tissues andsurrounding bone)2,5,6; primarily implicated
microorganisms for etiology includeanaerobic gram-negative bacteria15
Multifactorial etiology including following6: (1)patient factors such as systemic disease andmedication, oral disease and local infections,
noncompliance, smoking; (2) site-specific factors suchas hard- and soft-tissue quality and quantity;
presence of foreign body in periimplantsulcus (dental materials such as dental cement,displacement cord, impression materials, brokenbristles of toothbrush and/or oral hygiene aids,food impaction); (3) implant factors such as
osteogenicity, material, design, and susceptibilityto fracture; (4) clinician factors such asexperience, knowledge, skills, and ethics
Cause-effectrelationship
Difficult to prove causation andmore controversial6
Easier-to-isolate causing variable forsite-specific and implant-related factors
Primarytreatment
Antibacterial and antiplaque measures2 Antibacterial and elimination of causing variable
Treatmentmechanism
Involves host response and mandates biologiccascades for favorable regenerative outcomes
Does not mandate biologic cascades and may involvemechanical cascades to eradicate source of infection
Treatmentoutcome
Variable and may involve repetitive treatmentfor resolution of infection2,3
Definitive resolution of infection is possible ifetiology is isolated and eradicated
1 Patient’s initial presentation, showing suppurationaround abutment, with inflammation and erythema ofsurrounding tissue.
February 2014 97
CLINICAL REPORT
A 55-year-old white man presentedto the prosthodontist with pain, sup-puration, swelling, and a foul odor andtaste in his mouth. The patient did notreport any systemic discomfort or feverand malaise. He had a medical history
Bidra
of angina, arthritis, and hypertension.The patient’s dental history includedmaxillary complete edentulism treatedwith a 4-implant-supported over-denture with unsplinted abutments(Locator; Zest Anchors). All 4 implants(RN Standard Plus; Straumann) hadbeen placed 4 years earlier by his
previous dentist. The patient had beenseen for a periodic recall examination 8months earlier, and all the implants onthe maxilla and the opposing teeth inthe mandible were unremarkable.
On clinical examination, the leftmaxillary implant at the left lateralincisor region showed obvious suppu-ration around the abutment, and thesurrounding tissue appeared inflamedand erythematous (Fig. 1). The implantand abutment were immobile, and asharp sound was heard on tapping theabutment. No tenderness to percussionof the abutment was noted, but the softtissues around the implant were tenderon palpation. The remaining 3 implantsappeared healthy (Fig. 2). A new peri-apical radiograph of the implant wasmade and did not reveal the presenceof any foreign body (Fig. 3). The ra-diographic bone levels noted on thisradiograph were not significantlydifferent from those on the panoramicradiograph made 8 months earlier(Fig. 4). The radiographs revealed some
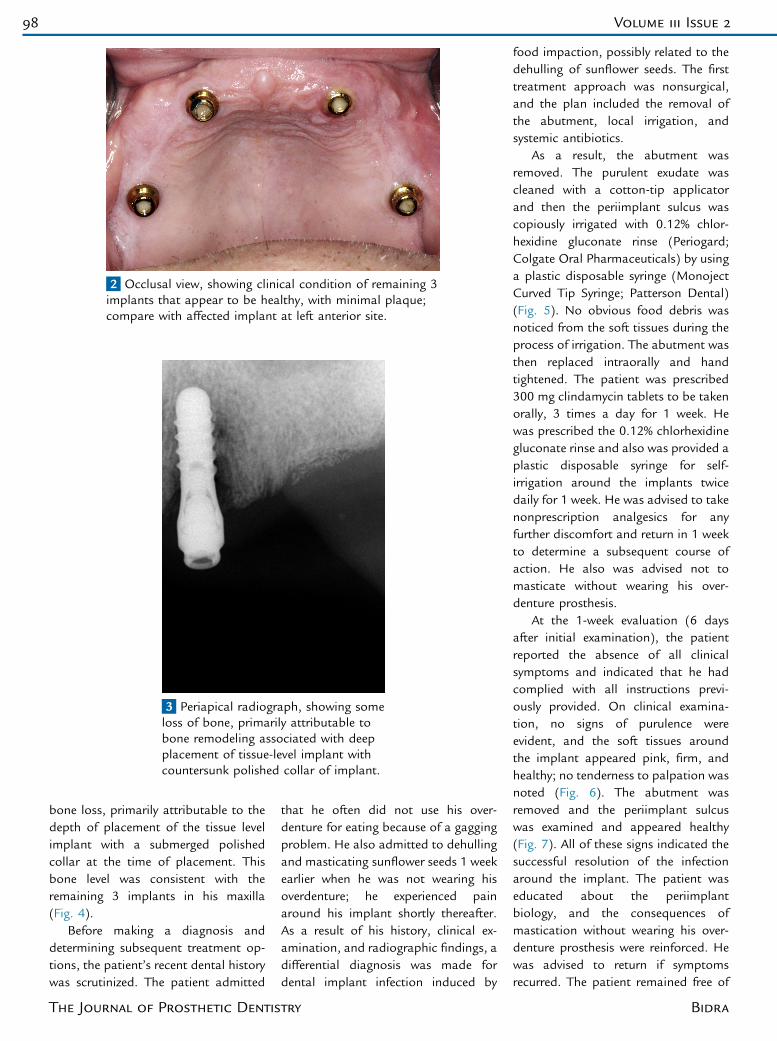
2 Occlusal view, showing clinical condition of remaining 3implants that appear to be healthy, with minimal plaque;compare with affected implant at left anterior site.
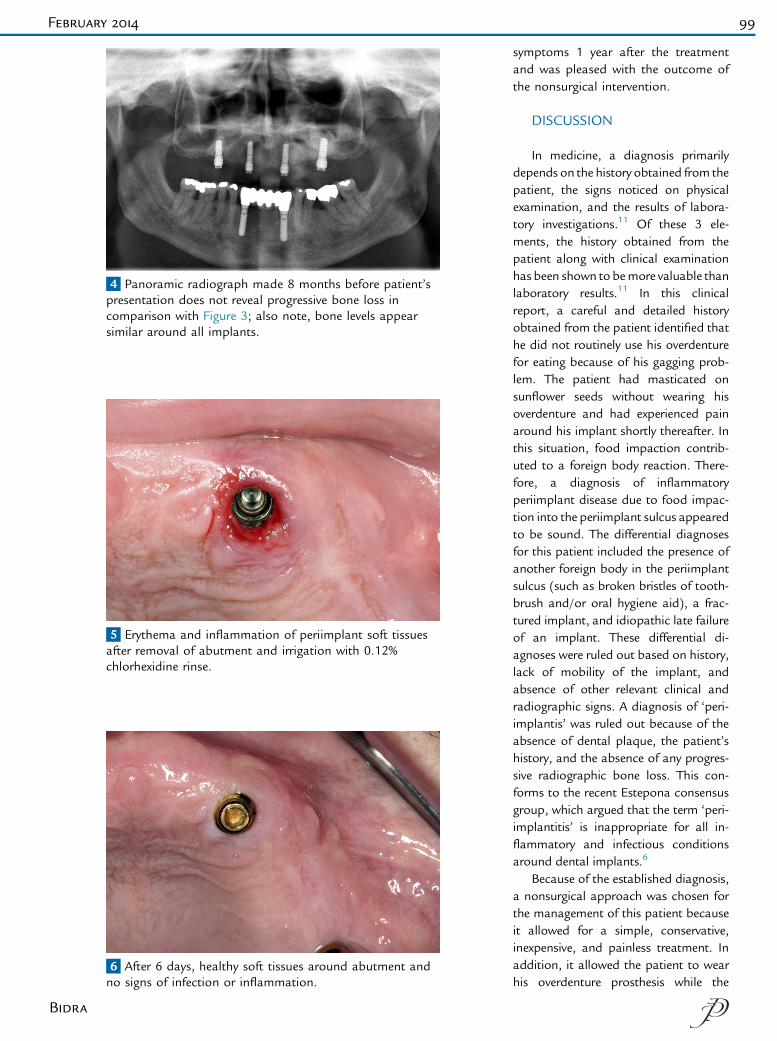
3 Periapical radiograph, showing someloss of bone, primarily attributable tobone remodeling associated with deepplacement of tissue-level implant withcountersunk polished collar of implant.
98 Volume 111 Issue 2
bone loss, primarily attributable to thedepth of placement of the tissue levelimplant with a submerged polishedcollar at the time of placement. Thisbone level was consistent with theremaining 3 implants in his maxilla(Fig. 4).
Before making a diagnosis anddetermining subsequent treatment op-tions, the patient’s recent dental historywas scrutinized. The patient admitted
The Journal of Prosthetic Dentis
that he often did not use his over-denture for eating because of a gaggingproblem. He also admitted to dehullingand masticating sunflower seeds 1 weekearlier when he was not wearing hisoverdenture; he experienced painaround his implant shortly thereafter.As a result of his history, clinical ex-amination, and radiographic findings, adifferential diagnosis was made fordental implant infection induced by
try
food impaction, possibly related to thedehulling of sunflower seeds. The firsttreatment approach was nonsurgical,and the plan included the removal ofthe abutment, local irrigation, andsystemic antibiotics.
As a result, the abutment wasremoved. The purulent exudate wascleaned with a cotton-tip applicatorand then the periimplant sulcus wascopiously irrigated with 0.12% chlor-hexidine gluconate rinse (Periogard;Colgate Oral Pharmaceuticals) by usinga plastic disposable syringe (MonojectCurved Tip Syringe; Patterson Dental)(Fig. 5). No obvious food debris wasnoticed from the soft tissues during theprocess of irrigation. The abutment wasthen replaced intraorally and handtightened. The patient was prescribed300 mg clindamycin tablets to be takenorally, 3 times a day for 1 week. Hewas prescribed the 0.12% chlorhexidinegluconate rinse and also was provided aplastic disposable syringe for self-irrigation around the implants twicedaily for 1 week. He was advised to takenonprescription analgesics for anyfurther discomfort and return in 1 weekto determine a subsequent course ofaction. He also was advised not tomasticate without wearing his over-denture prosthesis.
At the 1-week evaluation (6 daysafter initial examination), the patientreported the absence of all clinicalsymptoms and indicated that he hadcomplied with all instructions previ-ously provided. On clinical examina-tion, no signs of purulence wereevident, and the soft tissues aroundthe implant appeared pink, firm, andhealthy; no tenderness to palpation wasnoted (Fig. 6). The abutment wasremoved and the periimplant sulcuswas examined and appeared healthy(Fig. 7). All of these signs indicated thesuccessful resolution of the infectionaround the implant. The patient waseducated about the periimplantbiology, and the consequences ofmastication without wearing his over-denture prosthesis were reinforced. Hewas advised to return if symptomsrecurred. The patient remained free of
Bidra
4 Panoramic radiograph made 8 months before patient’spresentation does not reveal progressive bone loss incomparison with Figure 3; also note, bone levels appearsimilar around all implants.
5 Erythema and inflammation of periimplant soft tissuesafter removal of abutment and irrigation with 0.12%chlorhexidine rinse.
6 After 6 days, healthy soft tissues around abutment andno signs of infection or inflammation.
February 2014 99
Bidra
symptoms 1 year after the treatmentand was pleased with the outcome ofthe nonsurgical intervention.
DISCUSSION
In medicine, a diagnosis primarilydepends on the history obtained from thepatient, the signs noticed on physicalexamination, and the results of labora-tory investigations.11 Of these 3 ele-ments, the history obtained from thepatient along with clinical examinationhas been shown to bemore valuable thanlaboratory results.11 In this clinicalreport, a careful and detailed historyobtained from the patient identified thathe did not routinely use his overdenturefor eating because of his gagging prob-lem. The patient had masticated onsunflower seeds without wearing hisoverdenture and had experienced painaround his implant shortly thereafter. Inthis situation, food impaction contrib-uted to a foreign body reaction. There-fore, a diagnosis of inflammatoryperiimplant disease due to food impac-tion into the periimplant sulcus appearedto be sound. The differential diagnosesfor this patient included the presence ofanother foreign body in the periimplantsulcus (such as broken bristles of tooth-brush and/or oral hygiene aid), a frac-tured implant, and idiopathic late failureof an implant. These differential di-agnoses were ruled out based on history,lack of mobility of the implant, andabsence of other relevant clinical andradiographic signs. A diagnosis of ‘peri-implantis’ was ruled out because of theabsence of dental plaque, the patient’shistory, and the absence of any progres-sive radiographic bone loss. This con-forms to the recent Estepona consensusgroup, which argued that the term ‘peri-implantitis’ is inappropriate for all in-flammatory and infectious conditionsaround dental implants.6
Because of the established diagnosis,a nonsurgical approach was chosen forthe management of this patient becauseit allowed for a simple, conservative,inexpensive, and painless treatment. Inaddition, it allowed the patient to wearhis overdenture prosthesis while the

7 After 6 days, absence of erythema and inflammation ofperiimplant soft tissues after removal of abutment.
100 Volume 111 Issue 2
infection was being resolved. Clindamy-cin was the antibiotic of choice in thispatient because of its broad spectrum ofactivity against aerobic and anaerobicpathogens and significant tissue pene-tration, including bone, its high oral ab-sorption, and its stimulatory effects onthe host immune system.12 Similarly, a0.12% chlorhexidine gluconate rinse waschosen because of its antimicrobial effi-cacy, substantivity, and good history ofmanagement of periimplant infections.13
Currently, insufficient evidence is avail-able in the scientific literature for the useof systemic antibiotics for the manage-ment of periimplant infections.14 There-fore, the use of systemic clindamycin inthis patient was dictated primarily byempiricism and the assessment of therisk:benefit ratio by the author. Therationale for using a systemic antibioticalong with a topical antimicrobial agentwas to ensure broad-spectrum antimi-crobial coverage to prevent the progres-sion of infection. A lack of response tothis first-line treatment at the 1-weekevaluation would have necessitated sur-gical anti-infective management with anopen-flap debridement and possibleguided bone regeneration procedures. Toprevent a similar condition in the future,the patient was reminded of the impor-tance of wearing his prosthesis duringmastication and of maintaining goodoral hygiene.
The Journal of Prosthetic Dentis
SUMMARY
This clinical report described thesuccessful management of a patientwith a maxillary overdenture with in-flammatory periimplant disease causedby food impaction into the periimplantsulcus. The diagnosis was based oncareful analysis of the patient’s historyand clinical signs. The infection wasresolved in 1 week by local irrigationwith 0.12% chlorhexidine gluconaterinses and the use of systemic clinda-mycin. A nonsurgical intervention inthis patient allowed for the simple,conservative, inexpensive, and painlessmanagement of the inflammatoryperiimplant disease. A patient’s foodintake history and the possibility offood impaction into the periimplantsulcus should be considered for differ-ential diagnosis of inflammatory peri-implant disease.
REFERENCES
1. Lindhe J, Meyle J. Periimplant diseases:Consensus Report of the Sixth EuropeanWorkshop on Periodontology. J Clin Perio-dontol 2008;35(suppl 8):282-5.
2. Esposito M, Grusovin MG, Worthington HV.Interventions for replacing missing teeth:treatment of periimplantitis. CochraneDatabase Syst Rev 2012;1:CD004970.
3. Bidra AS. No reliable evidence suggestingwhat is the most effective interventions fortreating periimplantitis. Evid Based Dent2012;13:50-1.
try
4. Zitzmann NU, Berglundh T. Definition andprevalence of periimplant diseases. J ClinPeriodontol 2008;35(suppl 8):286-91.
5. Glossary of periodontal terms 2001. 4th ed.Chicago: American Academy of Periodon-tology; 2001. p. 20, 38. Available at: http://www.joponline.org/page/glossary. AccessedOctober 28, 2013.
6. Albrektsson T, Buser D, Chen ST, Cochran D,DeBruyn H, Jemt T, et al. Statements fromthe Estepona consensus meeting onperiimplantitis, February 2-4, 2012. ClinImplant Dent Relat Res 2012;14:781-2.
7. Demir G, Nemlioglu S, Yazgic U, Dogan EE,Bayat C. Determination of some importantemissions of sunflower oil production in-dustrial wastes incineration. J Sci Ind Res2005;64:225-8.
8. DeBruyne LK, Pinna K, Whitney E. Nutritionand diet therapy. 8th ed. Stamford: CengageLearning; 2008. p. 40-1.
9. Listgarten MA, Lang NP, Schroeder HE,Schroeder A. Periodontal tissues and theircounterparts around endosseous implants.Clin Oral Implants Res 1991;2:1-19.
10. Vandenbroucke JP. In defense of case reportsand case series. Ann Intern Med 2001;134:330-4.
11. Hampton JR, Harrison MJ, Mitchell JR,Prichard JS, Seymour C. Relative contribu-tions of history-taking, physical examination,and laboratory investigation to diagnosis andmanagement of medical outpatients. Br MedJ 1975;2:486-9.
12. Brook I, Lewis MA, Sándor GK, Jeffcoat M,Samaranayake LP, Vera Rojas J, et al. Clin-damycin in dentistry: more than just effectiveprophylaxis for endocarditis? Oral Surg OralMed Oral Pathol Oral Radiol Endod2005;100:550-8.
13. Lambert PM, Morris HF, Ochi S. The influ-ence of 0.12% chlorhexidine digluconate rin-ses on the incidence of infectiouscomplications and implant success. J OralMaxillofac Surg 1997;55(suppl 5):25-30.
14. van Winkelhoff AJ. Antibiotics in the treat-ment of periimplantitis. Eur J Oral Implantol2012;5(suppl):S43-50.
15. Ata-Ali J, Candel-Marti ME, Flichy-Fernández AJ, Peñarrocha-Oltra D, Balaguer-Martinez JF, Peñarrocha Diago M, et al.Periimplantitis: associated microbiota andtreatment. Med Oral Patol Oral Cir Bucal2011;16:e937-43.
Corresponding author:Dr Avinash S. BidraUniversity of Connecticut Health Center263 Farmington Avenue, L6078Farmington, CT 06030E-mail: [email protected]
Copyright ª 2014 by the Editorial Council forThe Journal of Prosthetic Dentistry.
Bidra