nonoperative treatment of tendinopathy...while sparing healthy tissue • cutting of tissue achieved...
TRANSCRIPT

Nonoperative Treatment of Tendinopathy
Health Care That Works
Andrews Research & Education Foundation October 14, 2016
Brett J. Kindle, M.D.

Disclosures
• Neither I, Brett Kindle, nor any family member(s), have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation.

Learning Objectives
• Review pathophysiology of tendinopathy • Discuss nonoperative treatment of tendinopathy • Understand indications & rationale of the treatments • Be aware of the current evidence supporting the
interventions • Discuss a potential treatment algorithm for tendinopathy
utilizing these interventions

Tendon Structure
• Myotendinous Junction
• Tendon
• Enthesis

Tendon Structure
Tropocollagen Triple Helix Structure

Tendon Mechanics�Stress: Strain curve
– I -- Toe Region, collagen fibers reduce their crimp angle – II -- Linear elongation of fibers – III -- “Microscopic failure” with triple helix slipping apart to failure of some fibers – IV -- “Macroscopic failure” with failure of additional fibers to complete failure
I
II
III
IV
Tendon Injury – Terms
• Tendinitis – Implying inflammatory pathology
• Tendinosis – Implying degenerative pathology w/o inflammatory
component
• Tendinopathy – Waist basket term meaning either of above terms
with or without pathology

Tendinopathy
• Multiple microtrauma à degeneration of tenocytes & ECM à failure to mature into normal tendon
• Angiofibroblastic hyperplasia
• Generates pain & increases risk of re-injury

Tendinopathy Cycle
Increaseddemandontendon
Inadequaterepair
Decreasedcollagen&
ECMproduc8onTenocyte
death
Furtherdecreaseincollagen&
ECM
Increasedvulnerabilitytoinjury
Adequaterepair

Tendinosis
• Macroscopic – Disorganized tissue – Soft, yellow/brown
appearance (normal is glistening white)
– Thickened tendon
hAp://www.thefootandankleclinic.com/achilles-tendon.htm
Achilles Tendinosis

Tendinosis
• Microscopic – Collagen degeneration – Fibrosis – Neovascularization – LACK of inflammation
Normal
Tendinosis
J.D. Rees et al, Rheumatology May 2006
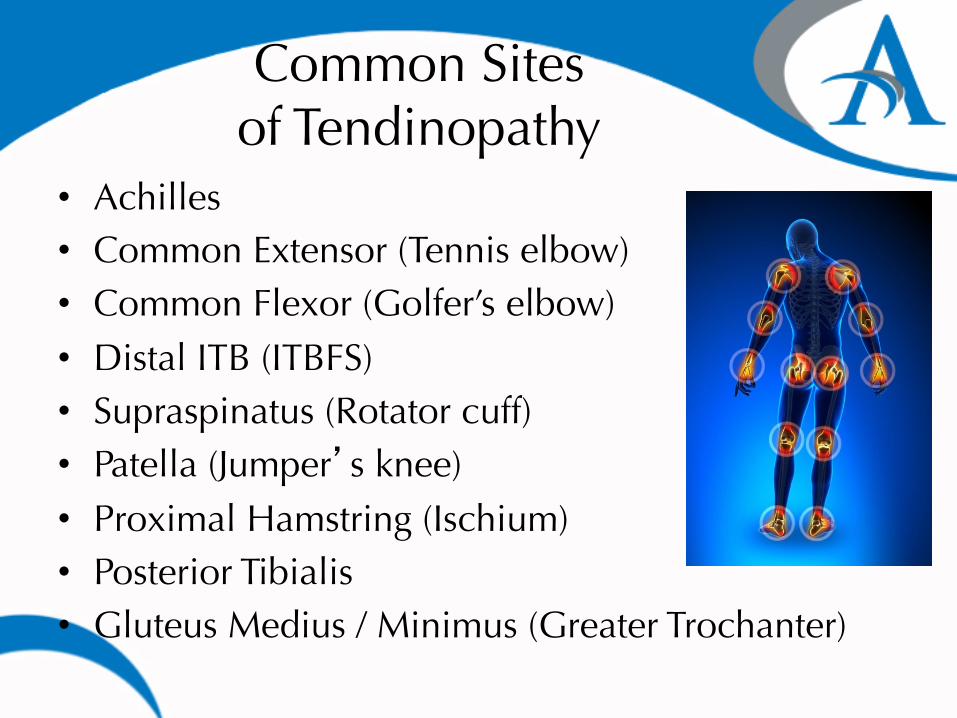
Common Sites �of Tendinopathy
• Achilles • Common Extensor (Tennis elbow) • Common Flexor (Golfer’s elbow) • Distal ITB (ITBFS) • Supraspinatus (Rotator cuff) • Patella (Jumper’s knee) • Proximal Hamstring (Ischium) • Posterior Tibialis • Gluteus Medius / Minimus (Greater Trochanter)

Traditional Treatments • Relative Rest
– How much is too much? – Better question… how much is too little ?
• Modalities – Ice
– Reduces blood flow & tendon metabolic rate which may slow healing
– Heat – Probably more beneficial than ice – Increases blood supply, removal of waste & brings in
fibroblasts / collagen to area • Orthotics/Bracing
o Is immobilization good for tendinosis ? • Physical Therapy
– Stretching – Strengthening – ART/CFM/Graston/ ASTYM

Eccentric Exercises
• Strength training, particularly eccentric-emphasis, has the best evidence supporting its use for tendinopathy of any treatment available.

Eccentric Exercises • Alfredson et al, AJSM, 1998 • Prospective • N=30 patients w/ achilles tendinosis 2-6 cm proximal to
insertion • Eccentric Intervention (N=15)
– Eccentric loading calf muscle w/ knee straight & bent (3 sets of 15 BID x12 weeks) using good leg to bring back to start position
• Surgical Intervention (N=15) • Outcome
– Both had great pain relief at 24 weeks – The exercise group had improved strength (eccentric &
concentric) to match that of the good leg – The surgery group had improvement, but still differed
significantly in strength from the good leg – Exercise group came to preinjury activity levels in 3 months,
surgery over 6 months

Manual or Instrument Assisted Stimulation
• Cross Frictional Massage • Active Release Therapy • Graston • ASTYM
– Basic idea is that stimulation of degenerated tendon will help to break up adhesions, scar tissue, increase circulation/ blood supply to area.
– This in turns initiate a healing cascade • Inflammation then proliferation of
fibroblasts…ultimately leads to new collagen formation
– Very few RCT’s on CFM, ART, & Graston

ASTYM Study
• Wilson et al, Journal of Sports Rehabilitation, 2000 – 20 pts with chronic patella tendinopathy
randomized to traditional PT (CFM, bicycle, stretching, exercising, ice 3x/wk for 4 wks) vs ASTYM (instead of CFM) 2x/wk for 4 wks
– After 6 wks, 10/10 ASTYM group had resolution of pain, 6/10 in traditional PT group
– After x- over 2/4 had resolution of pain with ASTYM tx.

Traditional Treatments
• NSAIDs – Process is NOT inflammatory at clinical presentation stage – May inhibit future healing of tendon
– not clinically proven – Benefit may purely be analgesia
• Corticosteroid Injections – Process is NOT inflammatory – May provide some pain relief – Can impede collagen synthesis & weaken tendon
– predisposes to rupture
• Surgery – Only w/ failure of conservative therapy – Involves release of adhesions, debridement
of degenerative tissue, & repair of partial tears – Success rates highly variable in studies,
probably 50%-80%

Corticosteroid Injections
• Used since the 1950’s • Side effects: skin depigmentation, fat
atrophy, tendon rupture • Krogh et al: Meta Analysis, AJSM, 2013 • No statistically significant difference in
benefit compared with placebo (10 trials, 310 pts) (lateral epicondylitis)
• Does show short-term pain reduction benefit
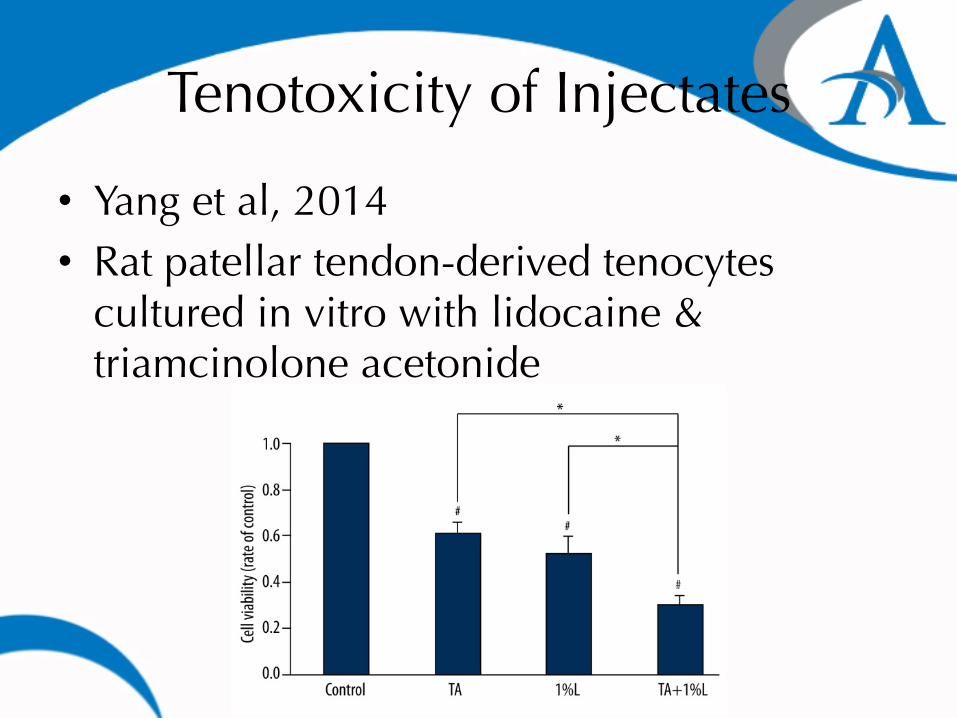
Tenotoxicity of Injectates
• Yang et al, 2014 • Rat patellar tendon-derived tenocytes
cultured in vitro with lidocaine & triamcinolone acetonide

Tenotoxicity of Injectates

Alternative Anesthetic
• Bacteriostatic Saline • Contains 0.9% benzyl alcohol • Stuns Na+ channels? • Tenotoxicity unknown

Modern Treatment Options
• Glyceryl trinitrate • Extracorporeal shockwave
therapy (ESWT) • Tendon scraping • Percutaneous needle
tenotomy • Percutaneous ultrasonic
tenotomy (Tenex)
• Platelet-rich plasma (PRP) • Autologous whole blood • Mesenchymal stem cells • Prolotherapy • Sclerotherapy • High-volume image-
guided injections

Glyceryl Trinitrate
• Mechanism: Modulation of local NO levels.
• Stimulation of collagen synthesis in fibroblasts.
• Also improves fracture healing in animal models.
• Achilles tendinopathy: – 1 RT: No benefit. – 3 RTs: Benefit. – Long-term follow-up:
Benefit persisted 3 yrs. – All studies non-insertional
disease.
• Patellar tendinopathy: – 1 RT: Did not improve
outcome over eccentric strengthening alone.

Extracorporeal Shockwave Therapy
• Mechanism: Disrupt abnormal collagen.
• Stimulate tissue regeneration & cell recruitment
• Local analgesic effect.
• Patellar tendinopathy: – 1 RT: Benefit (but no
diff from surgery) – 2 case series: Benefit.
• Achilles tendinopathy: – 3 case series: Benefit
from 2 mos to 1 yr.
• Plantar fasciopathy: – 1 RT: Benefit.

ESWT (Orthotripsy) • May disrupt avascular, damaged tissues &
encourage revascularization & release of growth factors as well as recruitment of stem cells
• May create hyperstimulation analgesia – Gate Theory of Pain (Melzak & Wall) – Repeated stimulation of small fibers can block transmission of pain
• FDA approved for plantar fascia and lateral elbow pain
– Also used in patella tendon & achilles tendon • May be best used for chronic calcific tendinopathy
(achilles) – Much like breaking up kidney stones

ESWT (Orthotripsy)
• Peer K. et al, Clin J Sports Med, 2003 • N=27 w/ chronic patellar tendinopathy • ESWT (N=13)
– ESWT (3 sessions) after which activity was as tolerated by pain (uncertain if any therapy)
• Surgical (N=14) – Resection of degenerated tendon w/ tenotomy followed by
therapy • Outcome
– VISA & VAS scores were not significantly different at 22 & 26 months for ESWT & surgery respectively
– 8/13 in ESWT & 7/14 in surgical group achieved preinjury levels of sport
– ESWT did score higher overall

Percutaneous Needle Tenotomy • Utilization of a relatively
large-gauge (18-20) needle to repeatedly fenestrate the tendon, fragment calcifications, & abrade the osseous margin (as applicable).
• Mechanism: Convert chronic, non-healing injury into an acute injury with increased healing potential.

Percutaneous Needle Tenotomy: Case Series
• Housner 2009. • Among 14 tendons, 13
were lower limb: 5 patellar, 4 Achilles, 1 gluteus medius, 1 iliotibial tract, 1 proximal hamstring, 1 proximal rectus femoris.
• Improved VAS at 4 & 12 weeks post-procedure.
• Housner 2010. • 47 patellar tendons. • Average follow-up time: 45
months. • 81% excellent or good
satisfaction scores. • 72% excellent or good results
with return to activity. • 28/45: Unable to return to
desired activity level. • 6 subsequent surgeries. • 1 rupture 6 weeks post-
procedure.

Percutaneous Ultrasonic Tenotomy: Tenex
• Commercial release 2012
• Developed at Mayo Clinic
• Mechanism: Similar to PNT, but additional benefit of removal of degenerative tissue
• U/S frequency is specific to necrotic tissue

Tenex
TX1 Console
• User interface with circuitry for
precise & targeted tissue removal
• Targeted diseased tissue is removed
while sparing healthy tissue with
built-in safety features/sensors
TX1 Microtip
• Percutaneous (18 g) pen-like function
• Pre-assembled w/ foot pedal activation
• Single use – entirely disposable

• Console delivers optimized ultrasonic energy to end of TX1 Microtip that precisely cuts diseased tendon tissue while sparing healthy tissue
• Cutting of tissue achieved through
longitudinal movement of needle at speed of sound (ultrasonic) – cut tissue at tip only via “jack-hammer effect”
• Continuous saline irrigation cools TX1
Microtip to control unwanted heat & coupled to simultaneous removal of target tissue
Tenex: Proprietary Technology

Tenex
• Common extensor (tennis elbow) • Common flexor (golfer’s elbow) • Triceps • Patellar (jumper’s knee) • ITB • Achilles • Plantar fascia • Rotator cuff* • Proximal hamstring (ischium)* • Gluteus medius/minimus (greater trochanter)*

Tenex – Patient Selection
• Chronic pain (>3 months) – Recalcitrant to conservative care (rest, ice, PT, bracing)
• Point tenderness – Localized over site of abnormal tissue
• Ultrasound abnormalities – Hypoechogenity, thickening, neo-vascularization
• No contraindications (infxn, coagulopathy, anti-coagulants, active cancer)
• No other concurrent diagnoses

Ultrasound imaging used to identify diseased tissue & guide TX1 Microtip during procedure
Diseased tendon tissue
TX1 MicroTip placed into hypoechoic region
Removal of hypoechoic region
1. Visualize damaged tendon (dark region) via ultrasound
3. Foot-pedal activation of TX1 MicroTip precisely
cuts & debrides target damaged tissue
2. Guide TX1 Microtip to damaged tissue with ultrasound guidance
Tenex

Tenex • Ultrasound is key • Minimally invasive • Lower-complication rate compared
to open tenotomy • 20-35 minute procedure (1-5
minute cutting time) • Usually done in ASC / procedure
room* • Faster recovery times • 80+% success rate w/in 1-3 mos • Most post-procedure pain
managed with OTC meds

Tenex
• Koh et al • Prospective study - 20 patients, chronic lateral
epicondylitis, failed nonsurgical treatment • Single treatment with TX 1 • Postprocedure care - no PT, OTC pain control,
activity modification x2 weeks • Follow-up: 2 weeks, 1, 3, 6, 12, 24 & 36 months • Assessed adverse events, VAS pain score, quality
of life, diagnostic ultrasound

Tenex
Tenex
• Barnes, Beckley, & Smith • Prospective study - 19 patients, symptomatic >6 months • 7 medial & 12 lateral epicondylosis, failed conservative treatment • Single treatment with TX 1 & no additional intervention • Total procedure time <15 minutes with mean energy time 38 seconds • No complications • Clinical outcomes at baseline, 6 weeks, 3, 6 & 12 months: VAS, Mayo
elbow performance score (MEPS), DASH

Tenex
VAS Q-DASH
MEPS

Tenex
Tenex Surgery
Efficacy/painrelief 91% 77%
PosAreatmentvisits 2.5 4.25
Averageworkweeksmissed
1.1 8.2
Totalcost/savingsperpa8ent
Tenexwas$11,753lessthansurgery
• Moore et al • Prospective study - randomizing Tenex vs open surgery • 45 patients, chronic lateral epicondylosis, unresponsive to
conservative care: – 23 treated with TX 1 – 22 treated with open surgical repair
• Outcomes measured at 1 week, 1 & 6 months

Tenex
• Ellattrache (Kerlan Jobe) • Prospective study involving 16 patients–symptomatic for
at least 6 months (10 collegiate level athletes) • Failed conservative treatment • Single treatment with TX 1 & no additional intervention • No complications • Clinical outcomes: 15/16 (93%) had resolution of
symptoms at 3 months with full activity at 6 months • All 10 athletes return to their prior level of competition

Tenex
• Patel et al • Prospective study involving 12 patients–symptomatic for
at least 6 months, all failed conservative treatment, PT, orthotics, extracorporal shockwave, cortisone, 4 patients failed open or endoscopic fasciotomy
• Single treatment with TX 1 & no additional intervention • Twelve-month follow-up • No complications • Clinical outcomes: 11/12 (92%) pain-free at 3 months &
sustained at 12 months, significant improvement in quality of life by 6 months & sustained at 12 months

Tenex
• Ellis et al • Prospective study of 26 patients–symptomatic for
average of 18 months • Single treatment with TX 1 no additional
intervention • Mean cutting time of 4 minutes 24 seconds • Patient’s followed up in one week, one month, 12
months, in 16 months post • Clinical outcomes: 23/26 (80%) have pain relief in
one month & sustain at 16 months, 24/26 (92%) would have the procedure done again

Platelet-Rich Plasma (PRP)
• Type of injection therapy used for various chronic sports injuries to promote healing.

• First human application was described in mandibular reconstruction in oromaxillary surgery in 1998 (Robert Marx, Prof.
of Surgery & Chief of Oromaxillary Surgery Division at Univ. of Miami). • Since then, PRP has experienced a surge in clinical uses
& research • Endorsement from athletes
– Tiger Woods – Alex Rodriguez (NY Yankees) – Masahiro Tanaka (NY Yankees) – Kobe Bryant (LA Lakers) – Troy Polamalu (Pitts Steelers) – Hines Ward (Pitts Steelers, 2009)
History of PRP

Platelet-Rich Plasma (PRP) • So…. What is it?
– Autologous blood derived product – Plasma with concentrated platelets 2-6x above normal – Platelets contain granules which store GFs & cytokines – Alpha granules store platelet-derived growth factors which
act in chondrocytes & tenocytes to: – promote cartilage matrix synthesis – increase cell growth & migration – facilitate protein transcription
– PRP may inhibit growth of – Staphylococcus aureus & Escherichia coli – Not active against P. aeruginosa, K. pneumonia, or E. faecalis

Marx & Garg. Dental & Craniofascial applications of Platelet Rich Plasma. Quintessence Publishing Co., Inc. 2005
Normal Blood Platelet Rich Plasma

PRP • Alpha granule contents:
– Platelet-derived epidermal growth factor – Platelet-derived growth factor
• Chemoattractive for mesenchymal stem cells & monocytes
– Bone morphogenic protein – Transforming growth factor beta
• Mitogen for fibroblasts & enhances extracellular matrix production
– Insulin-like growth factor – Vascular endothelial growth factor
• Stimulates angiogenesis – Endothelial cell growth factor – Basic fibroblast growth factor

PRP u Delta granule contents:
u Adenosine
u Cytoprotective agent prevents tissue damage, stimulate macrophages for pro-inflammatory (IL-1, IL-18) or anti-inflammatory effects (IL-10)
u Serotonin
u Incr capillary dilatation, attracts fibroblasts & increases their proliferation, affects macrophage function by suppression of IFN-gamma induced 1a expression
u Histamine
u Vasodilator = incr inflam & immune cells greater access to marginate & enter the local area, activates macrophages
u Calcium
u Involved in keratinocyte proliferation & differentiation that is essential for wound-healing
u Also: Dopamine, cathespin D & E, elastases, hydrolases

Platelet-Rich Plasma (PRP) • How is it prepared?
– Various systems but basics are:

Platelet-Rich Plasma (PRP)
• How is it used? – Goal is to deliver GFs directly at site of
diseased tissue to stimulate the natural healing cascade & regeneration of tissue
– Tendons, Ligaments, Joints, Muscle injuries,
Intra-operative augmentation – Lateral Epicondylitis, Achilles tendinopathy,
Patellar tendinopathy – Plantar fasciitis – Osteoarthritis

Platelet-Rich Plasma (PRP) • How does it work?
– PRP is injected & becomes activated via collagen w/in connective tissue or cartilage to release GFs & cytokines
– Initiates & regulates all phases of healing cycle – Bioactive proteins stimulate local stem cells & enhance
extracellular matrix (ECM) gene expression – Recruits reparative cells from the local circulation or bone
marrow – Inhibits excess inflammation, apoptosis, & metalloproteinase
activity
• Pathways help restore damaged tissue & diminish pain – Modulate microvascular environment or alter efferent or
afferent neural receptors
• More is needed to understand the mechanism of action…


Platelet-Rich Plasma (PRP) • Allan Mishra et al, AJSM, 2006 • 140 pts with lateral epicondylosis • Intervention
– Treatment group – single PRP injection into CET followed by gradual increase in rehab program x4 weeks after which full activity allowed
– Control group – bupivacaine injection • Outcome
– 46%, 60% & 81% improvement in VAS pain scores at 1, 2 & 6 months respectively in tx group
– At final F/U (12-38 months) 93% pain free (<10/100 VAS) – No complications, no one got worse

Platelet-Rich Plasma (PRP)
• Plantar fasciopathy: 3 case series: Benefit at 10 mos-1 yr. • Achilles tendinopathy: 5 case series: Benefit at 6 mos-4 yrs. • Patellar tendinopathy: 3 case series: Benefit at 3 mos-1 yr. • Multiple tendon studies:
– Finnoff 2011: 31/41 lower limb tendons. Case series: Benefit at 14 mos. – Mautner 2013: 116/180 lower limb tendons. Case series: Benefit at 15 mos.

Platelet-Rich Plasma (PRP)
• Plantar fasciopathy: – Aksahin 2012: No benefit at 6 mos.
• Patellar tendinopathy: – Vetrano 2013: Benefit of PRP over ESWT up to 1 yr. – Dragoo 2014: Benefit of PRP+PNT+eccentrics over PNT
+eccentrics at 12 wks…similar outcomes at >26 wks.
• Achilles tendinopathy: – de Vos 2010/de Jonge 2011: No benefit at 1 yr. – Kearney 2013: No benefit at 6 mos.
• Many studies are biased

Autologous Whole Blood �Injections
• Mechanism: Similar to PRP. • Benefits/drawbacks of RBC/WBC injection
concomitantly? • RBCs: free radicals, proteolytic enzymes. • WBCs: growth factors, but free radicals,
MMP-8/9. • Patellar tendinopathy: 1 prospective cohort:
Benefit at 15 mos. • Achilles tendinopathy: 1 RT: Benefit at 12 wk. • 1 RT: No benefit at 12 wk.

Prolotherapy
• First described in the 1930’s • Several decades of large retrospective studies
on successful outcomes • Theory is that irritant solutions stimulate an
acute inflammatory reaction to initiate a healing cascade for injured soft tissues.
• This technique has been employed for chronic enthesopathies & ligamentous injuries/laxity.
• Procedure involves injection of chemical (sodium morrhuate) or osmotic (Dextrose) proliferants over a series of shots

Prolotherapy
• Mechanism: Dextrose-containing solution is hypertonic: Osmotic cell rupture.
• Phenol-glycerineglucose: Local cellular irritation. • Morrhuate sodium: Chemotactic attraction of inflammatory
mediators. • Proximal adductor tendinopathy: 1 case series (hypertonic
dextrose): Benefit at mean of 17 mos. • Achilles tendinopathy: 1 RT (hypertonic glucose): No benefit at
12 months.

Sclerotherapy
• Mechanism: Neo-vascularization may be involved in tendon pain.
• Neo-vessels, & presumably adjacent “neo-nerves,” are sclerosed.
– Polidocanol or sotradecol most often used. May also use lactate 2x normal levels, glutamate, & substance P
• Patellar tendinopathy: 2 case series: Benefit at 1-2 yrs.
• Achilles tendinopathy: 2 case series: Benefit at 6-8 mos. 1 RT: Benefit at 3 mos.

Sclerotherapy • RCT published in AJSM, 2012 by Hoksrud et al. • Prospective study 101 pt w jumper’s knee • Received 1-5 USG inj polidocanol 4-6 wk intervals • VISA-P collected before, 6, 12, 24 month after 1st injection • “Few patients cured, majority had reduced function &
substantial pain after 24 months follow up”

Nitric Oxide (NO) • NO is a short lived free radical
– Can induce apoptosis in inflammatory cells – Can cause angiogenesis & vasodilation
• Inhibition of NO has been shown to reduce collagen synthesis by wound fibroblast in vitro
• NO synthase inhibition in animal studies leads to a reduction in tendon cross sectional area & load to tendon failure
• Theory is that nitric oxide may enhance collagen synthesis & remodeling as well as vasodilate & clear inflammatory mediators or other pain mediating proteins.
• Be wary of side effects/ contraindications • Can be used as adjunct to other treatments

Nitric Oxide
• Dr. George Murrell has done significant research into this:
• Lateral epicondylosis – At 6 mo: 80% of nitrate group had no pain with
ADL’s as opposed to 60% with rehab alone • Achilles Tendinosis
– At 6 mo: 78% of nitrate group had no pain with ADL’s as opposed to 49% with rehab alone
• Supraspinatus tendinopathy – At 6 mo: 46% of nitrate group had no pain with
ADL’s as opposed to 24% with rehab alone

• Think of: PRP as ”Fertilizer” Stem Cells as ”Seeds”

Stem Cell�Use in Sports Medicine
• “We have had on big revelation in sports medicine over the last 50 years, and that was the arthroscope. I’ve been looking for the next wave, and stem cell therapy… will be it.”
Dr. James Andrews

Mesenchymal Stem Cells
• Mechanism: MSCs are multipotent stromal cells that can proliferate & differentiate into a variety of cell types, including tenocytes
• Increase rate of healing by release of growth factors, cytokines & trophic immune regulators
• Derived from bone marrow, adipose tissue, amniotic tissue, tendon, synovial tissue

• First identified in bone marrow by Caplan in 1991 and, subsequently, in adipose tissues by Zuk et al at UCLA in 2001, Mesenchymal Adult Stem Cells can differentiate into:
– Ligament – Tendon – Cartilage – Muscle – Bone – Adipose tissue
Mesenchymal Stem Cells
J O U R N A L of P R O L O T H E R A P Y | V O L U M E 3 , I S S U E 3 | A U G U S T 2 0 1 1 693
W O N D E R W H Y ? S T E M C E L L P R O L O T H E R A P Y I N R E G E N E R A T I V E M E D I C I N E
ligament tissue,134 intervertebral disc repair,135, 136 ischemic heart tissue,137, 138 graft-vs-host disease139 and osteogenesis imperfecta.140 (See Figure 2.) Of particular interest in musculoskeletal medicine is the observation in degenerative diseases, such as osteoarthritis, an individual’s adult stem cell frequency and potency may be depleted, with reduced proliferative capacity and ability to differentiate.141, 142 It has been suggested that addition of these missing stem cell elements might help these conditions. Studies have demonstrated such improvement with adult stem cell therapy by the successful regeneration of osteoarthritic damage and articular cartilage defects.143, 144 In 2003, Murphy et al. reported significant improvement in medial meniscus and cartilage regeneration with autologous stem cell therapy in an animal model. Not only was there evidence of marked regeneration of meniscal tissue, but the usual progressive destruction of articular cartilage, osteophytic remodeling and subchondral sclerosis commonly seen in osteoarthritic disease was reduced in MSC-treated joints compared with controls.145 In 2008, Centeno et al. reported significant knee cartilage growth and symptom improvement in a human case report using culture expanded autologous MSC’s from bone marrow.146
A U T O L O G O U S A D I P O S E F A T G R A F T S I N C O S M E T I C - P L A S T I C S U R G E R Y
Adipose tissues have long been a proven safe and efficacious structural tissue amenable to successful transplantation.147 For more than 50 years, cosmetic-plastic surgeons have attempted such transfers with variable success. It is clear that control of cellular fate and extracellular environment is critical in tissue regeneration and cell-based therapies.148
It was not until the advent of a patented, closed syringe system was introduced in 1990 (Tulip Medical™) that predictability of structural augmentation was fully appreciated.149 For many years cosmetic-plastic surgeons believed the key to a successful structural autologous
fat graft (AFG) was transplantation of intact cellular elements (mature adipocytes) into environments that had existing adipose tissues. However it was recognized that mature adipocytes did not undergo mitosis, therefore further understanding of how adipose tissue maintained its structural integrity and volumes became an important undertaking. The past decade in cosmetic-plastic surgery has been spent increasing understanding of the importance of adipose-derived stem-stromal elements to the replenishment and restoration of adipocytes in Vivo. As adult adipocytes enter senescence stages, adherent (cell-to-cell) adipose progenitor cells directly differentiate into adipocytes to replace the aging cells. These progenitor cells are capable of undergoing mitosis, however do so in an asymmetric manner, producing another, now adipose-lineage committed (unipotent or terminally commited), progenitor cell and a less differentiated progenitor cell, in order to maintain precursor numbers for future differentiation and restore stem-like progenitor availability. Further understanding of the importance of the autocrine and paracrine functions of such cells within their niche has demonstrated the complex microenvironmental factors involved in tissue maintenance and regeneration.
Figure 2. Flow chart elucidating possible commitment, lineage progression and maturation of adipose-derived mesenchymal stem cells.
Courtesy of Donna Alderman, D.O.

• Not entirely understood. • 1) Regeneration of cartilage has been
demonstrated in vitro & in animal models. (Agung et al. Knee Surg, 2006)
How Does MSCs Help Arthritis?

• 2) Paracrine mechanism (cell-to-cell talk) via cytokines & growth factors.
(Bunnell et al. Cell Res & Therapy 2010)
How Does MSCs Help Arthritis?

Many Ways to Prepare MSCs…

• In US, however, FDA does not allow culturing of the stem cells in clinics.
(FDA does not allow these cells to be “more than minimally manipulated” or be outside of the patient for over 24 hrs.) • Clinicians have used centrifuge to concentrate
MSCs from bone marrow (Bone Marrow Aspirate Concentrate) or adipose tissues (Adipose Derived Stromal Vascular Fraction)
Issue with “Expanded” MSCs
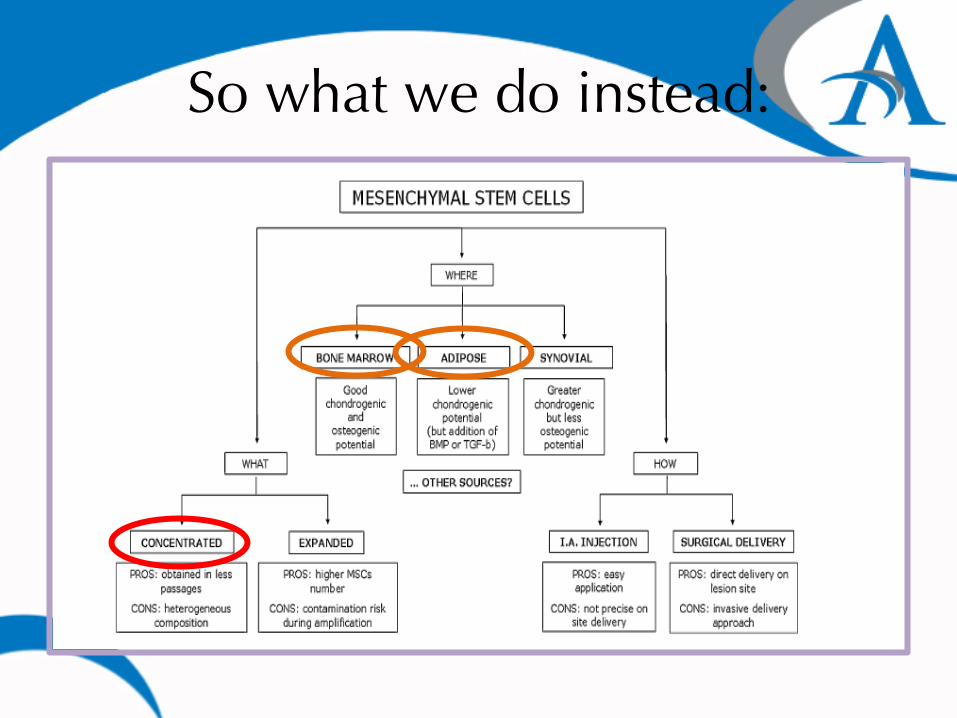
So what we do instead:

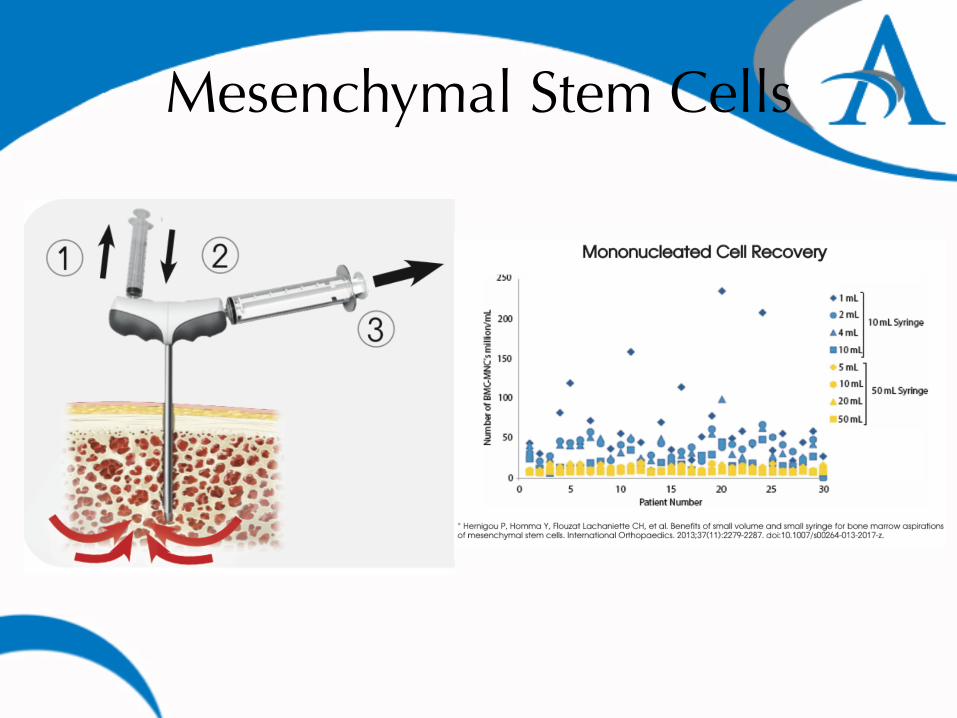
Obtaining BMAC:
BoneMarrowAspira8on&Centrifuga8on.

Mesenchymal Stem Cells
• FDA closely regulates based on principles of:
– Minimal manipulation – Homologous use (adipose?) – Noncombination products – Lack of systemic effect or autologous

Mesenchymal Stem Cells:�Obtaining “BMAC”
Mesenchymal Stem Cells
Mesenchymal Stem Cells
• Several animal studies show improvement of biomechanical properties, tissue architecture & functionality
• Lateral epicondylitis: 1 RT with skin-derived tenocyte-like cells (vs autologous plasma injections), 11/12 w/ benefit at 6 mos.
• Patellar tendinopathy: – Prospective, randomized, double blind controlled trial, skin
derived tendon-like cell injections had statistically significant & faster improvement in pain & reduced functional disability at 6 months compared to PRP group (N=46)
– Case series, bone marrow derived stem cells injected & followed up over the course of 5 years. 7/8 said they would have the procedure again & were completely satisfied. Statistically significant improvement for KOOS scores.

Mesenchymal Stem Cells
• Future questions – Which harvest site is best – How many injections – Duration between injections – Does needle size damage the cells – Does temperature affect the cells – Inhibition or synergy with other
products – Growth factor injection

High-Volume Image-Guided Injections
• Mechanically disrupt neovessels/neonerves through injection of a high volume of fluid, typically between a tendon & associated fat pad (Achilles tendon & Kager’s fat pad; patellar tendon & Hoffa’s fat pad).

High-Volume Image-Guided Injections
• Maffulli 2013: Achilles tendinopathy. • 94 patients. Injected with 10 mL of 0.5%
bupivacaine, 25 mg of aprotinin, & up to 40 mL of normal saline. Follow-up to 12 months. Significant improvement in VISA-A.
• Morton 2014: Patellar tendinopathy. • 20 patients. Injected with 10 mL of 0.5%
bupivacaine, 25 mg hydrocortisone, & 30 mL of normal saline at the interface of patellar tendon & Hoffa’s fat pad. Eccentric loading rehabilitation protocol. Follow-up at 12 weeks. Significant improvement in VISA-P.

Tendon Scraping
• Mechanically disrupt neo-vessels/neo-nerves, typically at the interface between a tendon & associated fat pad (Achilles tendon & Kager’s fat pad; patellar tendon & Hoffa’s fat pad).

Tendon Scraping
• Alfredson 2011: Achilles tendinopathy. • 88 tendons: Case series of open surgical
scraping. • 37 tendons: Randomized to open surgical
scraping vs. percutaneous needle scraping. • Mean follow-up: 18 months. • VAS significantly improved. • In randomized arm, no significant different
between open surgical scraping & percutaneous needle scraping.

Treatment Decisions
• Chronicity of injury. • Degree of disability. • Failure of eccentric
strengthening? • Failure of common sense? • Patient’s fitness level. • Patient’s competition
level. • Patient’s expectations.
• Patient’s desired activities. • Patient’s commitment &
compliance level. • Co-morbid &
environmental factors. • Benefits vs risks of
particular treatment. • Age. • Cost.

Inside vs. Outside Interventions
• “Inside” tendon interventions may take longer to recover from.
• May also have better long-term outcomes.
• May have greater risk of tendon rupture (questionable).
• Treating the disease process? • Delayed gratification?
• “Outside” tendon interventions may have a quicker recovery & return-to-play schedule.
• May have better short-term outcomes.
• May be lower risk. • Temporizing measure? • Treating pain more than
the disease process?

Proposed Treatment Approach • Tier 1: • Activity modifications. • Training program evaluation
& modification. • Technique evaluation &
modification. • Equipment/gear evaluation &
modification. • Eccentric strengthening
program.
• Tier 2: • Combination HVIGI +
tendon scraping (where applicable).
• Tenotomy (where applicable, available, cost-effective).
• Nitrates • ESWT

Proposed Treatment Approach
• Tier 3: • Combination of
tenotomy & PRP injection. $
• Tier Four: • MSCs (possible
combination with tenotomy). $$$$$
• ALL of these interventions beyond Tier One need more high-quality studies.
Summary
• There are numerous promising treatment options for tendinopathy; however, more high-quality evidence supporting their use is needed.
• Characteristics of the patient & the considered treatments should help guide therapy; there is insufficient evidence for a universally agreed-upon treatment approach at this time.

Take Home Points • Tendon degeneration & neovascularization are
prominent features of tendinosis • NSAIDs & steroid injections are NOT indicated, but are
still widely used in treatment of tendinosis • Several novel, nonsurgical interventions for recalcitrant
tendinopathy are emerging • Tenex is a minimally invasive debridement procedure
that has significant data supporting its use for treating tendinosis
• Regenerative medicine (PRP & SCs) for MSK application is still in its infancy with limited available evidence, but appears promising & safe, offering an exciting alternative to recalcitrant MSK conditions

References • Abate M. Pathogenesis of tendinopathies: inflammation or degeneration? Arthritis Res
Ther. 2009;11:235. • Alfredson H, et al. Heavy-load eccentric calf muscle training for the treatment of
chronic Achilles tendinosis. Am J Sports Med. 1998;26:360-6. • Alfredson H. Ultrasound & Doppler-guided mini-surgery to treat midportion Achilles
tendinosis: results of a large material & a randomised study comparing two scraping techniques. Br J Sports Med. 2011;45:407-10.
• Alfredson H, et al. Sclerosing injections to areas of neo-vascularisation reduce pain in chronic Achilles tendinopathy: a double-blind randomised controlled trial. Knee Surg Sports Traumatol Arthrosc. 2005;13:338-44.
• Chan O, et al. High volume image guided injections in chronic Achilles tendinopathy. Disabil Rehabil. 2008;30:1697-708.
• Finnoff JT, et al. Treatment of chronic tendinopathy with ultrasound-guided needle tenotomy & platelet rich plasma injection. PM R. 2011;3:900-11.
• Fridman R, et al. Extracorporeal shockwave therapy for the treatment of Achilles tendinopathies: a prospective study. J Am Podiatr Med Assoc. 2008;98:466-8.

References • Housner JA, et al. Should ultrasound-guided needle fenestration be considered as a
treatment option for recalcitrant patellar tendinopathy? A retrospective study of 47 cases. Clin J Sport Med. 2010;20:488-90.
• Kawase T, et al. Platelet-rich plasma derived fibrin clot formation stimulates collagen synthesis in periodontal ligament & osteoblastic cells in vitro. J Periodontol. 2003;64:858.
• Kon E, et al. Platelet-rich plasma: new clinical application: a pilot study for treatment of jumper’s knee. Injury. 2009;40:598-603.
• Krogh TP, Bartels EM, Ellingsen T, Stengaard-Pedersen K, Buchbinder R, Fredberg U, Bliddal H, Christensen R. Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review & network meta-analysis of randomized controlled trials. Am J Sports Med. 2013 Jun;41(6):1435-46.
• Mautner K, et al. Outcomes after ultrasound-guided platelet-rich plasma injections for chronic tendinopathy: a multicenter, retrospective review. PM R. 2013;5:169-75.
• Murawski CD, et al. A single platelet-rich plasma injection for chronic midsubstance Achilles tendinopathy: a retrospective preliminary analysis. Foot Ankle Spec. 2014;7:372-6.
• Peers K. et al: Cross Sectional Outcome Analysis of Athletes With Chronic Patellar Tendinopathy Treated Surgically & by Extracorporeal Shock Wave Therapy. Clin J Sports Med. 2003. 13:79-83.

References • Pettrone F. et al: Extracorporeal Shock Wave Therapy Without Local Anesthesia for
Chronic Lateral Epicondylitis. J Bone & Joint Surgery. 2005. 87A(6):1297-1304. • Rees J.D. et al: Current Concepts in the Management of Tendon Disorders.
Rheumatlogy. 2006. 45:508-521. • Sharma P. et al: Tendon Injury & Tendinopathy: Healing & Repair. J Bone & Joint
Surgery. 2005. 87A(1)187-202. • Sharma P. et al: Biology of Tendon Injury: Healing, Modeling & Remodeling. J
Musculoskeletal Neuronal Interaction. 2006. 6(2):181-90. • Stevens A. & Lowe J. Human Histology – Second Edition. Mosby. p. 50-52. • Tasto J. et al: Microtenotomy Using a Radiofrequency Probe to Treat Lateral
Epicondylitis. J Arthroscopic & Related Surgery. 2005. 21(7):851-60. • Topol G. et al: Efficacy of Dextrose Prolotherapy in the Elite Male Kicking Sport
Athletes With Chronic Groin Pain. Arch Phys Med Rehabil. 2005. 86:697-702. • Williams R. et al: The Effect of Ciprfloxacin on Tendon, Paratenon & Capsular
Fibroblast Metabolism. AJSM. 2000. 28(3):364-9 • Yang SL, Zhang YB, Jiang ZT, Li ZZ, Jiang DP. Lidocaine potentiates the deleterious
effects of triamcinolone acetonide on tenocytes. Med Sci Monit. 2014 Nov 29;20:2478-83.
