noninvasive vascular diagnosis || noninvasive vascular testing for the trauma patient
TRANSCRIPT

417A.F. AbuRahma, D.F. Bandyk (eds.), Noninvasive Vascular Diagnosis,DOI 10.1007/978-1-4471-4005-4_34, © Springer-Verlag London 2013
Introduction
Over the past century, the surgical management of extremity vascular injuries has undergone dramatic changes. During the era of World War I and II, repair of vascular injuries was rarely performed and ligation of injured vessels was the stan-dard practice. Unfortunately, this practice resulted in an unacceptably high amputation rate in excess of 70% [ 1 ] . The poor results from arterial ligation prompted surgeons Hughes and Spencer to reconsider the proper management of trau-matic vascular injuries [ 2, 3 ] . As such, during the Korean War, vascular surgical techniques had advanced to allow
Abstract
For decades, the management of traumatic vascular injuries to the extremity has challenged surgeons. However, even during the dark times of con fl ict in the United States, where sur-geon faced an inordinate amount of mangled extremities, surgical technique was advanced and not only bene fi ted military personnel but eventually civilian victims. Parallel to the course of surgery with movement toward minimally invasive techniques, the diagnosis of vascular trauma has progressed from an invasive, often low-yielding surgical exploration to a selective, noninvasive paradigm. Outside of overt signs of vascular injury (e.g., pulsatile bleeding), reliance solely on physical examination lacked the sensitivity to support an adop-tion of a less invasive diagnostic approach. Ankle-brachial index (ABI) was paramount in guiding clinicians to proper selection of injured patients who bene fi ted from further diag-nostic investigations or observation. Color- fl ow duplex scanning also contributed to a non-invasive diagnostic testing for vascular injuries in the extremity. However, due to variability in results based on technician expertise, off-hour unavailability, and stagnant technological movement the role of color- fl ow duplex remained limited. Conversely, computed tomogra-phy is emerging as the diagnostic modality of choice for vascular trauma. Current multi-detector units allow accurate acquisition of long body segment in minutes. Due to the increasing application of computed tomography (CT) angiography, digital subtraction angiography has been relegated from the “gold standard” diagnostic modality to a treatment modality. This chapter discusses the progression of this overall change in the diagnostic management of patients with traumatic vascular injuries.
Keywords
Trauma • Lower extremity • Arterial injury • Diagnosis • Noninvasive • Vascular
Noninvasive Vascular Testing for the Trauma Patient
Vincent L. Rowe , John Moos , and Fred A. Weaver
34
V. L. Rowe , M.D., FACS (*) Division of Vascular Surgery, Department of Surgery , Keck School of Medicine at the University of Southern California , Los Angeles , CA , USA
Healthcare Consultation Center II , 1520 San Pablo Street, Suite 4300 , Los Angeles , CA 90033 , USA e-mail: [email protected]
J. Moos , M.D. • F. A. Weaver , M.D., FACS, MMM Division of Vascular Surgery, Department of Surgery , Keck Medical Center of USC , Los Angeles , CA , USA

418 V.L. Rowe et al.
implementation of formal repair for peripheral vascular arte-rial injuries. In the Vietnam War, further surgical re fi nements led to the repair of both arterial and venous injuries becom-ing the standard of care in the majority of clinical situations [ 4, 5 ] . Continuing re fi nements in arterial surgery over the ensuing three decades have reduced limb loss in most civil-ian series to less than 10–15% [ 6– 8 ] ; however, long-term disability, predominantly resulting from associated skeletal and nerve injuries, remains a persistent problem for 20–50% of patients [ 9 ] . To date, approximately 90% of all peripheral arterial injuries occur in an extremity. Civilian studies report the majority of arterial injuries to be in the upper extremity, while the past military experiences de fi nes lower extremity injuries to be more common [ 3 ] .
Mechanism of Injury
The initial and ultimate outcome of vascular injury depends, in large part, on the wounding agent or mechanism of injury. Determining the mechanism of injury, whether it be blunt, high velocity, or low velocity penetrating trauma, is of utmost importance if the surgeon is to utilize available diagnostic and treatment options appropriately. Peripheral vascular injuries in an urban environment most often result from pen-etrating trauma from knives or bullets. In a series of penetrat-ing injuries, arterial injuries were due to gunshot wounds in 64%, knife wounds in 24%, and shotgun blasts in 12% [ 10 ] .
Traditionally, high-velocity fi rearm injuries are thought to occur in the battle fi eld, but with increasing frequency, they are the causative agent in civilian vascular trauma. In addi-tion to the vascular injury, extensive associated musculoskel-etal injury is commonplace. Vascular injuries in this setting result from the dissipation of energy into the surrounding tis-sues, fragmentation of the projectile or of bone, or transmis-sion of the blast effect [ 11 ] . Experimental studies have demonstrated a positive correlation between muzzle velocity and the microscopic extent and “length” of damage to the vessel wall [ 12 ] . In many ways, these wounds mimic lower-velocity shotgun injuries in their devastating combination of penetrating and blunt tissue injury [ 13 ] .
Falls and motor vehicle accidents are the most common causes of blunt injury and are becoming more frequent, owing to the ever-increasing mobility of modern society [ 12, 14 ] . The morbidity of blunt vascular injuries can be magni fi ed by associated fractures, dislocations, and crush injuries to muscles and nerves.
Diagnostic Evaluation
Due to the fact that the majority of signi fi cant vascular inju-ries present with signs of either loss of extremity pulses, overt bleeding or shock, diagnosis is usually not a challenge.
However, in some situations, the initial vascular injury may remain undiagnosed until life threatening hemorrhage or end organ ischemia becomes evident.
History
Paramount to the initial assessment for a vascular injury is a proper history. First responders should be questioned for the following fi ndings at the scene of injury: presence or absence of shock, the amount and character of bleeding (bright-red pulsatile bleeding suggesting an arterial origin or dark blood suggesting a venous origin), or the use or application of a tourniquet. Upon arrival to the hospital, it is possible for the bleeding to have abated, falsely lowering the suspicion of a signi fi cant vascular injury. However, the clinician must remain aware of the remote possibility of a secondary hem-orrhagic event at anytime. Determination of the mechanism of injury is paramount in the history evaluation. Additional questioning is obtained concerning underlying comorbidi-ties, such as, long-standing diabetes mellitus, underlying peripheral arterial disease, or established peripheral neurop-athies that may confound the evaluation of vascular system.
Physical Examination
Similar for all trauma patients, the initial physical assess-ment must be performed after the patient is completely dis-robed. In any penetrating trauma, evaluation of the location of possible entry and exit wounds in relation to anatomic structures should be sought. After completion of the primary and secondary survey of the trauma patient, attention should be focused on the exclusion of a vascular injury. Comprehensive pulse examination still remains one of the most important assessment measures and should be per-formed on all patients with suspected vascular injury. Presence and strength of a pulse should be documented from the groin to the foot on both extremities. The clinician must be aware of the trauma patient who possesses underlying peripheral arterial disease (PAD). In this case, because of the bilateral distribution of chronic lower extremity PAD, the absence of pulses in the contralateral leg will serve as a vital comparison of the baseline circulatory status.
Clinical suspicion for a vascular injury should not be low-ered based on the presence of a normal pulse palpated distal to the area of injury. As many as 50% of patients can harbor an occult vascular injury with a reported “normal” pulse examination. In addition to a thorough pulse examination, capillary re fi ll and temperature should be documented. Because of the close proximity of major nerves to the extrem-ity vessels, a thorough neurologic examination is critical to assess the functional potential of the extremity. Interestingly, the incidence of nerve injury in the lower extremity is

41934 Noninvasive Vascular Testing for the Trauma Patient
reported to be one-third that of trauma to the upper extremity [ 15– 17 ] . In the infrageniculate region, the close proximity of major nerves has led to an incidence of associated nerve inju-ries between 8% and 58%. [ 15, 16, 18, 19 ] . Therefore, it is extremely important to document a thorough neurological examination. Nerve injuries have been reported to result in long-term severe neurological de fi cit in up to 20% of patients and is a key determinant in the decision for limb salvage or primary amputation, con fi rming the need for a thorough ini-tial evaluation [ 20, 21 ] .
Associated bony injuries are reported to occur in approxi-mately 35% of lower extremity penetrating and blunt trauma [ 15, 22 ] . In patients who present with obvious deformities, bony injuries are easily appreciated. However, even the most minor appearing injured extremity may harbor an occult bony disruption. Christian et al. identi fi ed unrecognized arte-rial injuries in 50% of patients presenting with severe tibial fractures [ 23 ] . Therefore, a series of plain radiographs to assure the absence of a fracture is obligatory in the evalua-tion of lower extremity trauma.
Extremity arterial injuries have varied clinical presenta-tions. A minority of patients present with obvious clinical evidence, or “hard signs,” of an arterial disruption such as pulsatile external bleeding, an enlarging hematoma, absent distal pulses, or an ischemic limb (Table 34.1 ). For patients with overt signs of arterial injury, immediate surgical explo-ration in the operating room, without further diagnostic test-ing, is preferred. In most instances, when arteriography is required, an intraoperative arteriogram is suf fi cient to iden-tify the location and extent of injury and to guide the surgical repair. These signs aid clinicians by stratifying patients into those with or without severe ischemia.
A complete vascular examination should include an ankle-brachial index (ABI). Pressure readings from the lower of the two pedal vessels are compared to the arm blood pres-sure. Doppler arterial pressure measurements and calculation of pressure indices was fi rst introduced in the 1970s for the assessment of chronic PAD limbs. However, it was not until the early 1990s when ABI became an effective diagnostic modality in the workup of a patient with a possible traumatic vascular injury. In a study of 100 consecutive injured limbs, Lynch and Johanason showed arterial injuries that required intervention were discovered in 14 cases, and an ABI less than 0.90 predicted the injury with 87% sensitivity and 97%
speci fi city [ 24 ] . Because two of the arteriograms were falsely positive, sensitivity and speci fi city of ABI less than 0.90 were even higher—95% and 97%—when clinical outcome was the standard. As such, ABI became a routine part of the vascular assessment of the injured extremity.
Imaging Studies
Ankle-Brachial Indices and Selective Angiography
The diagnostic approach to extremity trauma has changed dramatically over the last few decades. Initially, the in fl uences from combat experience lead to the aggressive approach of mandatory exploration for all penetrating trauma to an extremity. However, application of this policy to civilian injuries resulted in negative exploration rate as high as 84% in penetrating trauma patients [ 25 ] . These patients had under-gone expensive, nontherapeutic operations, which occasion-ally resulted in additional morbidity.
With the availability of arteriography in most trauma centers, this diagnostic modality supplanted wound explo-ration for penetrating extremity trauma. As was the case with wound exploration, mandatory or routine screening arteriography for proximity wounds, in the absence of other suspicious clinical fi ndings, resulted in a large proportion of normal arteriograms (90%), at signi fi cant cost [ 1 ] . In addition, arteriograms were found to be less than perfect, having a low, but real, incidence of false-negative and false-positive fi ndings. Because of its invasive nature and the potential nephrotoxicity of contrast media, arteriography also occasionally results in serious complications, thus increasing patient morbidity and further increasing the cost of care.
It became apparent that many unnecessary angiograms were performed in the trauma setting. Intense evaluation of the role of proximity in predicting a vascular injury leads to a signi fi cant change in the management of penetrating extremity trauma. Weaver et al. examined the yield of a vas-cular injury when proximity alone was the sole indicator for angiography in extremity trauma [ 26 ] . Over an 18-month period, 373 patients with penetrating trauma distal to the del-topectoral groove in the upper extremity and distal to the inguinal ligament in the lower extremity were evaluated. Arteriograms were obtained for patients with “hard or soft signs” of vascular trauma (Table 34.1 ) or in the absence of these fi ndings, when the path of the penetrating object was judged to be in close proximity to a major vascular structure. In the 216 patients with one or more abnormal physical fi ndings, an arterial injury was identi fi ed by arteriography in 65 (30%), whereas in the absence of physical fi ndings (157 patients) only minor injuries were identi fi ed in 17 (11%). Only a pulse de fi cit, neurologic de fi cit, or shotgun injury
Table 34.1 Traumatic vascular injury
Hard signs Soft signs
Observed pulsatile bleeding Signi fi cant hemorrhage by history
Arterial thrill by manual palpation Neurological abnormality Bruit auscultated over or near area of arterial injury
Diminished pulse compared to contralateral extremity
Absent distal pulse Proximity bony injury or penetrating wound Visible expanding hematoma

420 V.L. Rowe et al.
correlated ( p < 0.05) with arteriographic evidence of a major arterial injury.
Later, authors from the same institution sought to validate the utility of ABI in assessing patients with penetrating vas-cular trauma of the extremity. A follow-up study investigated the ability of Doppler indices to detect occult arterial injuries in a consecutive cohort of 514 patients with unilateral, iso-lated penetrating extremity injuries [ 27 ] . Arteriography was limited to patients with a pulse de fi cit, neurologic de fi cit, shotgun injury, or one or more “soft” signs or a Doppler ankle/brachial index (ABI) of less than 1.00. All patients with arteriographic evidence of a major arterial injury had either a pulse de fi cit or ABI below 1.00.
A selective use of angiography in evaluation of patients with penetrating extremity trauma was recently con fi rmed by Conrad [ 28 ] . Five hundred and thirty-eight patients were reviewed retrospectively. Similar to previous studies, angiog-raphy was limited to patients presenting with an abnormal pulse examination or Doppler indices less than 1.0. Patients with a normal physical examination and Doppler indices of 1.0 or greater were discharged home without further workup. Three hundred patients with asymptomatic proximity wounds and normal physical examination were discharged home. Fifty-one percent of these discharged patients were available for an average follow-up of 9.8 months. There were no missed injuries or late complications identi fi ed in the group.
For blunt extremity trauma, the indications for arteriogra-phy parallel what has been established for penetrating inju-ries. A prospective study analyzed the results of arteriography in 53 patients with unilateral blunt lower extremity trauma [ 29 ] . Thirty-one patients had physical fi ndings suggestive of an arterial injury, and an arterial injury was demonstrated in 15. A pulse de fi cit or decrease capillary re fi ll correlated signi fi cantly ( p < .05) with arteriographic evidence of injury. Of the 15 arterial injuries, 12 were found in patients who had one or both of these fi ndings and four of those injuries required repair. In the remaining 22 patients with neither a pulse de fi cit nor decreased capillary re fi ll, three minor inju-ries were found, none of which required repair.
Another series of blunt injuries focused speci fi cally on 115 patients with knee dislocations [ 30 ] . Popliteal artery injury was demonstrated arteriographically in 27 of 115 (23%) patients. An abnormal pedal pulse identi fi ed popliteal artery injuries with sensitivity of 85% and speci fi city of 93%. All injuries that required intervention were associated with a diminished pulse. Dennis reported an identical experience in 37 patients with knee dislocations [ 31 ] . In all patients who required popliteal repair, pedal pulses were absent. More recently, Abou-Sayed and Berger con fi rmed the sensitivity of physical examination in 52 patients with blunt popliteal artery injuries [ 32 ] . Twenty-three patients, with a normal pulse examination, did not undergo angiography and required no vascular interventions. Angiography was performed in 13
patients with normal pulse examinations (at the discretion of the attending surgeon); similarly, no clinically signi fi cant lesions were identi fi ed that required intervention. Again, the assertion that the clinical examination can de fi ne a subset of high-risk patients who need an arteriogram, and possibly surgical repair, was validated.
Based on these published reports, a consensus has devel-oped that for penetrating or blunt extremity trauma, arteriog-raphy is indicated only for patients with either an abnormal extremity pulse examination or Doppler index less than 1. Careful physical examination and pressure measurements appropriately select the vast majority of patients (>95%) who have signi fi cant arterial injury and require arteriography.
Plain Radiographs
Plain fi lms are part of a standard diagnostic evaluation for a trauma patient. In patients with blunt trauma, fractures or dislocations in key anatomical areas may alert the clinician to the possibility of a vascular injury (i.e., posterior knee dis-location). Radio-opaque markers placed at the point of entry and exit of penetrating trauma wounds may be helpful in determining the trajectory of the penetrating object. Attention to all foreign bodies should be given. In the special situation of a repeat trauma patient, the clinician must be aware of possible retained foreign bodies from prior trauma.
Color Flow Duplex Ultrasonography
Duplex ultrasonography is the melding of pulse-wave Doppler and high resolution B-mode ultrasound. Because of continued improvements in noninvasive vascular imaging, color fl ow duplex ultrasonography (CFD) has been suggested as a substitute for or complement to arteriography [ 33 ] . CFD has several obvious advantages: it is noninvasive, painless, portable, and can easily be brought to the patient’s bedside, emergency room, or operating room. Repeated and follow-up examinations are easily performed without morbidity and are relatively inexpensive. The duplex is also able to detect vascular injuries to non-conduit vessels such as the profunda femoris artery, where ABI measurements would be regis-tered as normal.
Bynoe and colleagues reported sensitivity of 95%, speci fi city of 99%, and accuracy of 98% when CFD was used to evaluate blunt and penetrating injuries of the neck or extremities, and Fry and coworkers [ 34, 35 ] documented 100% sensitivity and 97.3% speci fi city in a similar series. In these two studies, however, a comparison arteriogram was available for only a minority of patients. Bergstein and asso-ciates reported on 67 patients who had 75 penetrating extrem-ity injuries, all of whom underwent both CFD and
42134 Noninvasive Vascular Testing for the Trauma Patient
arteriography [ 36 ] . Using arteriography as the gold standard, CFD had two false-negative results and one false-positive (sensitivity 50%, speci fi city 99%). Gagne and coworkers published a series of 37 patients with proximity injuries in 43 extremities [ 37 ] . Arteriography identi fi ed three injuries to the deep femoral, super fi cial femoral, and posterior tibial arteries that were not identi fi ed by CFD. However, CFD did detect a super fi cial femoral artery intimal fl ap that arteriog-raphy missed.
Despite some uncertainty about the ability of CFD to detect all arterial injuries, these reports suggest that nearly all major injuries that require therapeutic intervention can be identi fi ed, potentially at considerable costs savings as com-pared with arteriography [ 33 ] . Ordog has estimated a multi-million dollar cost savings if CFD and outpatient follow-up, rather than arteriography and inpatient observation, were used to exclude extremity arterial injuries [ 38 ] .
Contrary to the success of these reports, use of CFD in the workup of trauma patients presents some challenges. Technician dependence, limited availability during off hours, and limited visualization of chest and in some cases, the abdomen are possible pitfalls of CFD. Our institutional expe-rience with CFD in the evaluation of extremity trauma con fi rmed the operator dependence of CFD and, we felt for CFD to be used effectively, an institutional investment in experienced vascular technologists and interpreting physi-cians would be required [ 39 ] . This expense could be lessened over the long term if the current effort to train surgeons in the use of diagnostic ultrasound for intracavitary trauma were extended to include extremity vessels.
Computed Tomography Angiography
Years ago, computed tomography angiography (CTA) began challenging the need for digital angiography in the evalua-tion of trauma patients with suspected vascular injuries. However, now with advances in technology to newer 64-row multi-detector CT scanning, digital angiography is being supplanted by CTA in many trauma centers [ 40– 43 ] . Current scanners with multi-detector scanning and three-dimensional reformation capabilities provide rapid acquisition of isotro-pic data sets of long vascular territories within seconds. Therefore, CT scanning can now integrate extremity images in the routine thoraco-abdominal trauma imaging without a signi fi cant increase in scanning time. When compared to digital angiography for trauma patients, CTA has the distinct advantage of being equivalent in accuracy, more time ef fi cient, less invasive, and less expensive in the diagnosis of traumatic vascular injuries. Current CT scanning is also read-ily available and provides simultaneous imaging of surround-ing body structures and adjacent anatomical locations in a single examination. Through remote computer access, set
injection protocols and lack of arterial puncture complica-tions, staff radiologists can provide diagnostic reading offsite.
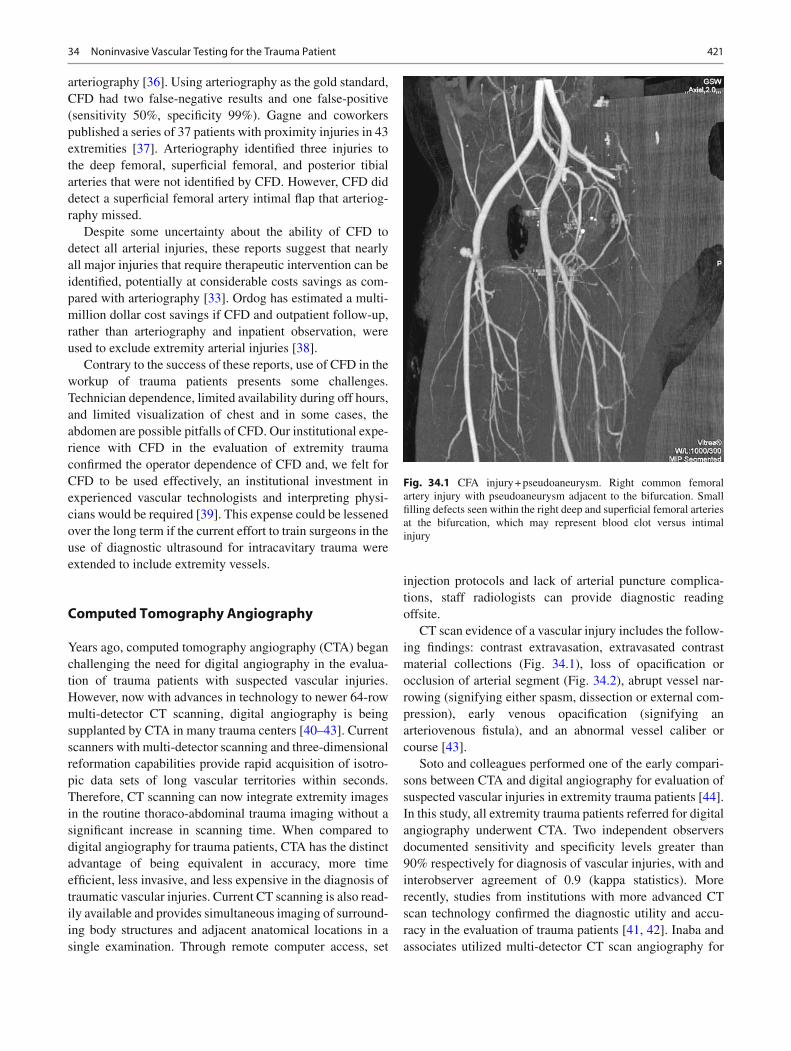
CT scan evidence of a vascular injury includes the follow-ing fi ndings: contrast extravasation, extravasated contrast material collections (Fig. 34.1 ), loss of opaci fi cation or occlusion of arterial segment (Fig. 34.2 ), abrupt vessel nar-rowing (signifying either spasm, dissection or external com-pression), early venous opaci fi cation (signifying an arteriovenous fi stula), and an abnormal vessel caliber or course [ 43 ] .
Soto and colleagues performed one of the early compari-sons between CTA and digital angiography for evaluation of suspected vascular injuries in extremity trauma patients [ 44 ] . In this study, all extremity trauma patients referred for digital angiography underwent CTA. Two independent observers documented sensitivity and speci fi city levels greater than 90% respectively for diagnosis of vascular injuries, with and interobserver agreement of 0.9 (kappa statistics). More recently, studies from institutions with more advanced CT scan technology con fi rmed the diagnostic utility and accu-racy in the evaluation of trauma patients [ 41, 42 ] . Inaba and associates utilized multi-detector CT scan angiography for
Fig. 34.1 CFA injury + pseudoaneurysm. Right common femoral artery injury with pseudoaneurysm adjacent to the bifurcation. Small fi lling defects seen within the right deep and super fi cial femoral arteries at the bifurcation, which may represent blood clot versus intimal injury

422 V.L. Rowe et al.
59 trauma patients with lower extremity injuries and docu-mented 100% sensitivity and speci fi city in the diagnosis of a clinically signi fi cant vascular injury [ 45 ] . The one missed injury in their patient cohort was secondary to artifact from a retained missile fragment. Most recently, Inaba and col-leagues followed up their earlier study and reported similar fi ndings [ 46 ] . Sensitivity and speci fi city both reached 100% in detecting clinically signi fi cant traumatic vascular injuries of the lower extremity. The shortcoming of computed tomog-raphy continued to appear in artifact formation from retained missile fragments. Other recognized disadvantages of CT angiography include artifact formation due to motion or calci fi ed plaques and high volume of iodinated contrast usage. If an endovascular treatment option is contemplated, deleterious effects of sequential intravenous contrast boluses must be considered in the patient management.
Magnetic Resonance Arteriography
Magnetic resonance arteriography (MRA) has increased in popularity for the diagnosis of vascular disorders; however, its application to trauma patients is not widely accepted. Compared with other modalities, MRA has the advantage of imaging multiple anatomical areas simultaneously and being noninvasive, preventing the need for contrast agents. Unfortunately, MRA is not easily accessible in the majority of hospitals, and the presence of metallic orthopedic instru-mentation limits widespread usage for trauma patients [ 47 ] .
References
1. Patel K, Rowe VL. Vascular trauma to the extremities, chapter 155. In: Rutherford R, editor. Vascular surgery, vol. 2. 7th ed. Philadelphia: W.B. Saunders Publishers; 2010. p. 2361–73.
2. Hughes CH. Arterial repair during the Korean war. Ann Surg. 1958;147:555.
3. Rich NM. Surgeon’s response to battle fi eld vascular trauma. Am J Surg. 1993;166:91.
4. Rich NA, Baugh JH, Hughes CW. Acute arterial injuries in Vietnam: 1,000 cases. J Trauma. 1970;10:359.
5. Martin LC, McKenney MG, Sosa JL, et al. Management of lower extremity arterial trauma. J Trauma. 1994;37(4):591–9.
6. Melton SM, Croce MA, Patton JH, et al. Popliteal artery trauma. Ann Surg. 1997;225:518.
7. Wagner WH, Caulkins E, Weaver FA, et al. Blunt popliteal artery trauma: 100 consecutive cases. J Vasc Surg. 1988;7:736.
8. Wagner WH, Yellin AE, Weaver FA, et al. Acute treatment of popliteal artery trauma: the importance of soft tissue injury. Ann Vasc Surg. 1994;8:557.
9. Weaver FA, Papanicolaou G, Yellin AE. Dif fi cult peripheral vascu-lar injuries. Surg Clin North Am. 1996;76:843.
10. Pasch AR, Bishara RA, Lim LT, et al. Optimal limb salvage in pen-etrating civilian vascular trauma. J Vasc Surg. 1986;3:189.
11. Fackler ML. Wound ballistics: a review of common misconcep-tions. JAMA. 1988;259:2730.
12. Amato JJ, Billy LJ, Gruber RP, et al. Vascular injuries: an experi-mental study of high and low velocity missile wounds. Arch Surg. 1970;101:167.
13. Mayer JP, Lim LT, Schuler JJ, et al. Peripheral vascular trauma from close-range shotgun injuries. Arch Surg. 1985;120:1126.
14. White RA, Scher LA, Samson RH, et al. Peripheral vascular inju-ries associated with falls from heights. J Trauma. 1987;27:411.
15. Ballard JL, Bunt TJ, Malone JM. Management of small artery vas-cular trauma. Am J Surg. 1992;164:316–9.
16. Rich NM, Spencer FC. Concomitant fractures and nerve trauma. In: Rich NM, Spencer FL, editors. Vascular trauma. Philadelphia: WB Saunders Co; 1978. p. 125–56, 380–1.
17. Rowe VL, Salim A, Lipham J, Asensio J. Shank arterial injuries. Vascular trauma: complex and challenging injuries, part II. Surg Clin N Am. 2002;82(1):91–104.
18. Bole PV, Purdy RT, Munda RT, Moallem S, DeVanesan J, Clauss RH. Civilian arterial injuries. Ann Surg. 1976;183:13–23.
19. Smith RF, Elliott JP, Hageman JH, Szilagyi DE, Xavier AO. Acute penetrating arterial injuries of the neck and limbs. Arch Surg. 1974;109:198–205.
20. Sitzmann JV, Ernst CB. Management of arm arterial injuries. Surgery. 1984;96:895–901.
21. Weaver FA, Rosenthal RE, Waterhouse G, et al. Combined skeletal and vascular injuries of the lower extremities. Am Surg. 1984;50(4):189–97.
Fig. 34.2 Right popliteal artery injury. Pseudoaneurysm of the proxi-mal right popliteal artery in the adductor canal with a short segment of occlusion just distal to the pseudoaneurysm. There is distal reconstitu-tion of the popliteal artery

42334 Noninvasive Vascular Testing for the Trauma Patient
22. Grossman MD, Reilly P, McMahan D, et al. Gunshot wounds below the popliteal fossa: a contemporary review. Am Surg. 1999;65(4):360–5.
23. Christian EP, Bosse MJ, Robb G. Reconstruction of large diaphy-seal defects without free fi bular transfer, in grade III-B tibial frac-tures. J Bone Joint Surg Am. 1989;71A:994–1004.
24. Lynch K, Johansen K. Can Doppler pressure measurement replace “exclusion” arteriography in the diagnosis of occult extremity arte-rial trauma? Ann Surg. 1991;214:737.
25. Guede JW, Hobson RW, Padberg FT, et al. The role of contrast arte-riography in suspected arterial injuries of the extremities. Am Surg. 1985;51:89.
26. Weaver FA, Yellin AE, Bauer M, et al. Is arterial proximity a valid indication for arteriography in penetrating extremity trauma? A prospective analysis. Arch Surg. 1990;125:1256.
27. Schwartz MR, Weaver FA, Yellin AE, et al. Re fi ning the indications for arteriography in penetrating extremity trauma: a prospective analysis. J Vasc Surg. 1993;17:166.
28. Conrad MF, Patton Jr JH, Parikshak M, et al. Evaluation of vascular injury in penetrating extremity trauma: angiographers stay home. Am Surg. 2002;68:269.
29. Applebaum R, Yellin AE, Weaver FA, et al. The role of routine arteriography in blunt lower extremity trauma. Am J Surg. 1990;160:221.
30. Fayiga YJ, Valentine RJ, Myers SI, et al. Blunt pediatric vascular trauma: analysis of forty-one consecutive patients undergoing oper-ative intervention. J Vasc Surg. 1994;20:419.
31. Dennis JW, Frykberg ER, Veldenz HC, et al. Validation of nonop-erative management of occult vascular injuries and accuracy of physical examination alone in penetrating extremity trauma: 5- to 10-year follow up. J Trauma. 1998;44:24.
32. Abou-Sayed H, Berger DL. Blunt lower-extremity trauma and popliteal artery injuries. Revisiting the case for selective arteriogra-phy. Arch Surg. 2002;137:585.
33. Meissner M, Paun M, Johansen K. Duplex scanning for arterial trauma. Am J Surg. 1991;161:552.
34. Fry WR, Smith RS, Sayers DV, et al. The success of duplex ultra-sonographic scanning in diagnosis of extremity vascular proximity trauma. Arch Surg. 1993;128:1368.
35. Bynoe RP, Miles WS, Bell RM, et al. Noninvasive diagnosis of vascular trauma by duplex ultrasonography. J Vasc Surg. 1991;14:346.
36. Bergstein JM, Blair JF, Edwards J, Towne JB, Wittmann DH, Aprahamian C, Quebbeman EJ. Pitfalls in the use of color- fl ow duplex ultrasound for screening of suspected arterial injuries in penetrated extremities. J Trauma. 1992;33:395–402.
37. Gagne PJ, Cone JB, McFarland D, et al. Proximity penetrating extremity trauma: the role of duplex ultrasound in the detection of occult venous injuries. J Trauma. 1995;39:1157.
38. Ordog GJ, Balasubramanium S, Wasserber J, et al. Extremity gun-shot wounds: I. Identi fi cation and treatment of patients at high risk of vascular injury. J Trauma. 1994;36:358.
39. Schwartz M, Weaver F, Yellin A, Ralls P. The utility of color fl ow Doppler examination in penetrating extremity arterial trauma. Am Surg. 1993;59:375.
40. Fleiter TR, Mervis S. The role of 3D-CTA in the assessment of peripheral vascular lesions in trauma patients. Eur J Radiol. 2007;64:92.
41. Busquéts AR, Acosta JA, Colón E, et al. Helical computed tomo-graphic angiography for the diagnosis of traumatic arterial injuries of the extremities. J Trauma. 2004;56:625.
42. Peng PD, Spain DA, Tataria M, et al. CT angiography effectively evaluates extremity vascular trauma. Am Surg. 2008;74:103.
43. Gakhal MS, Sartip KA. CT Angiography signs of lower extremity vascular trauma. Am J Roentgenol. 2009;193:W49.
44. Soto JA, Múnera F, Cardoso N, et al. Diagnostic performance of helical CT angiography in trauma to large arteries of the extremi-ties. J Comput Assist Tomogr. 1999;23(2):188.
45. Inaba K, Potzman J, Munera F, et al. Multi-slice CT angiography for arterial evaluation in the injured lower extremity. J Trauma. 2006;60:502.
46. Inaba K, Branco BC, Reddy S, et al. Prospective evaluation of mul-tidetector computed tomography for extremity vascular trauma. J Trauma. 2011;70:808.
47. Rubel IF, Potter H, Barie P, et al. Magnetic resonance venography to evaluate deep venous thrombosis in patients with pelvic and acetabular trauma. J Trauma. 2001;51:622.