nonalcoholic fatty liver disease -...
TRANSCRIPT

Second Annual Spring Hepatology Update 4/30/2016
1
Nonalcoholic Fatty Liver Disease
Kris V. Kowdley MD, FACP
Director, Liver Care Network
Director, Organ Care Research
Swedish Medical Center
Seattle, WA

Second Annual Spring Hepatology Update 4/30/2016
2
Abbreviations: NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis.
Graphic courtesy of Zobair M. Younossi, MD, MPH, FACG.
NA
FLD
Spectr
um
NASH Is Part of the Spectrum of NAFLD
NASH requires specific
pathologic criteria
• Exclusion of other liver
diseases
• Needed for prognosis

Second Annual Spring Hepatology Update 4/30/2016
3
Global Epidemiology of NAFLD
• Systematic literature search
– 700+ studies evaluated, 95 studies examined,
53 studies analyzed
• Global prevalence of NAFLD is 21.3%
– Highest prevalence in South America (35.3%) and
the Middle East (31.8%)
– Prevalence in North America 18.5%
• NASH was prevalent in 26.2% of the subjects
with NAFLD
Abbreviations: NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis.
Koenig AB, et al. Hepatology. 2015;62(1 suppl):1286A.

Second Annual Spring Hepatology Update 4/30/2016
4
Metabolic Abnormalities
Associated with NAFLD
Risk Factor1 Incidence (95% CI)
Hyperlipidemia 62.2% (45.3%–76.5%)
Obesity* 47.4% (34.2%–60.9%)
Metabolic syndrome 43.3% (29.4%–58.3%)
Hypertension 38.6% (32.1%–45.7%)
Hypertriglyceridemia 37.3% (25.4%–51.0%)
Diabetes 18% (13.6%–23.5%)
Abbreviation: NAFLD, nonalcoholic fatty liver disease.
1. Koenig AB, et al. Hepatology. 2015;62(1 suppl):1286A. 2. Younossi ZM, et al. Medicine (Baltimore). 2012;91:319-327.
*Although the vast majority of NAFLD patients are overweight or obese, patients with NAFLD may
also be lean.2

Second Annual Spring Hepatology Update 4/30/2016
5
NAFLD and NASH Natural History
NAFLD
NASH (26%)1NAFL (74%)1
StableFibrosis Progression2
(25%–35% of NASH patients)
Cirrhosis2
(9%–20% of NASH patients)
Liver Failure or HCC2
(40%–60% of cirrhotics over 5–7 y)
OLT or Death2
(22%–33% of cirrhotics)
Abbreviations:
HCC, hepatocellular carcinoma;
NAFLD, nonalcoholic fatty liver disease;
NASH, nonalcoholic steatohepatitis;
OLT, orthotopic liver transplantation.
1. Koenig AB, et al. Hepatology. 2015;62(1 suppl):1286A. 2. Ong JP, et al. Clin Liver Dis. 2007;11:1-16.

Second Annual Spring Hepatology Update 4/30/2016
6
• Patients with NAFLD (N = 432); 26.8% with NASH
• In multivariate analysis, elevated AST and ALT, presence
of diabetes mellitus, male gender, and white ethnicity were
associated with moderate-to-severe fibrosis
(P <.0001)
• Risk increases with increasing metabolic conditions
What Are the Clinical Predictors of
Advanced Fibrosis in NAFLD?
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; DM, diabetes mellitus; HTN, hypertension;
NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; VO, visceral obesity.
Hossain N, et al. Clin Gastroenterol Hepatol. 2009;7:1224-1229.
HTN DM HTN + DMHTN + DM
+ VOOR
(95% CI)
1.61 (1.21–2.01)
1.64 (1.13–2.17)
1.69 (1.11–2.28)
1.72(1.13–2.31)
P-value .0374 .0258 .0246 .0205

Second Annual Spring Hepatology Update 4/30/2016
7
What Is the Association Between
Metabolic Syndrome and NASH?
• Patients with NAFLD, no overt diabetes, and with liver biopsy (N = 304)
• NASH confirmed in 120/304 patients
• Metabolic syndrome* was independently associated with– Histologic NASH
(OR, 3.2; 1.2–8.9)
– Severe fibrosis (OR, 3.5; 1.1–11.2)
88
53
0
50
100
Pa
tie
nts
wit
h M
eta
bo
lic
S
yn
dro
me
(%
) P =.004
NASH Non-NASH
Abbreviations: NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; OR, odds ratio.
Metabolic syndrome was defined as having ≥3 of the following criteria: 1) fasting glucose 110 mg/dL; 2) central obesity;
3) arterial pressure 130/85 mm Hg or pharmacologically treated; 4) triglyceride levels 150 mg/dL or current use of fibrates;
and 5) high-density lipoprotein-cholesterol 40 mg/dL (men) and 50 mg/dL (women).
Marchesini G, et al. Hepatology. 2003;37:917-923.

Second Annual Spring Hepatology Update 4/30/2016
8
What Are the Clinical Predictors of
Liver-Related Mortality in NAFLD?Multivariate Survival Analysis
Factor aHR (95% CI)
Statistically
significant
predictors
NASH 9.16 (2.10–9.88)
Type 2 diabetes 2.19 (1.00–4.81)
Age 1.06 (1.02–1.10)
Other
Male gender 1.44 (0.62–3.34)
White race 1.85 (0.62–5.47)
Obesity 0.88 (0.38–2.04)
Hyperlipidemia 0.48 (0.19–1.23)
Abbreviations: aHR, adjusted health ratio; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis.
Stepanova M, et al. Dig Dis Sci. 2013;58:3017-3023.

Second Annual Spring Hepatology Update 4/30/2016
9
Univariate Survival Analyses
What Are the Histologic Predictors of
Liver-Related Mortality in NAFLD?
Abbreviations: HR, hazard ratio; LRM, liver-related mortality; MD, Mallory-Denk; NAFLD, nonalcoholic fatty liver disease.
Younossi ZM, et al. Hepatology. 2011;53:1874-1882.
HR (95% CI)
Portal
inflammation
(grade ≥2)
6.68 (2.20–20.3)P = .0008
Ballooning
(grade ≥2)
5.32 (1.89–14.9) P = .0015
MD bodies
(grade ≥2)
4.21 (1.66–10.7)P = .0024
Portal fibrosis
(grade >2)
14.1 (5.47–36.5)P <.0001
Pericellular
fibrosis (grade >2)
4.86 (1.73–13.7) P = .0027
On multivariate
analysis, only
significant fibrosis
(grade ≥3) was an
independent
predictor of LRM

Second Annual Spring Hepatology Update 4/30/2016
10
• Several case reports and case series of well-documented
cases of HCC in NAFLD patients1–3
• NAFLD is the 3rd most common cause of HCC1
– Cumulative incidence of HCC in NASH cirrhosis is 2.6% compared
with 4% in HCV2
– Absolute risk for NAFLD-HCC: 3%−6% over 8.2−21 years4
– NAFLD-HCC mortality: 0.25%–2.3% over 7.6–13.7 years4
• Characteristics5
– More common in males (73%), average age 67 years5
– Most often (76%) a single lesion, well to moderately differentiated5
– Larger tumors than metabolic syndrome and other overt causes of
chronic liver disease, including viral hepatitis: 12.8 cm vs 8.8 cm
vs 7.8 cm (P = .001)6
NAFLD and HCC
Abbreviations: HCC, hepatocellular carcinoma; HCV, hepatitis C virus; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis.
1. Mittal S, et al. Clin Gastroenterol Hepatol. 2015;13:594-601. 2. Ascha MS, et al. Hepatology. 2010;51:1972-1978. 3. Arase Y, et al. Hepatol Res.
2012;42:264-272. 4. White DL, et al. Clin Gastroenterol Hepatol. 2012;10:1342-1359. 5. Duan XY, et al. Hepatobiliary Pancreat Dis Int. 2012;11:18-
27. 6. Paradis V, et al. Hepatology. 2009;49:851-859.

Second Annual Spring Hepatology Update 4/30/2016
11
• Multicenter, observational, case-control study:
NAFLD-HCC (n = 145), HCV-HCC (n = 611)
• Compared with HCV-HCC, NAFLD-HCC
– Had more metabolic syndrome components
– Had larger tumor volume
– More often had an infiltrative pattern
– More often was found outside surveillance
• Cirrhosis present in 50% of NAFLD-HCC
patients
p=0.017
Clinical Patterns of HCC in
Patients with NAFLD
Abbreviations: HCC, hepatocellular carcinoma; HCV, hepatitis C virus; NAFLD, nonalcoholic fatty liver disease.
Piscaglia F, et al. Presented at: 50th EASL; April 20-26, 2015; Vienna, Austria. Abstract P0340.

Second Annual Spring Hepatology Update 4/30/2016
12
Trends in NASH-Related Liver
Transplantation Waitlist Registrations
• In 2013, NASH became
2nd indication for LT listing
• OR for waitlist mortality at
90 days
– NASH: 1, reference
– ALD: 0.77; P <.001
– HCV: 0.99; P = .92
• Compared with HCV,
NASH patients had the
lowest chance of getting
transplanted in 90 days
and 1 year
Abbreviations: ALD, alcoholic liver disease; HCV, hepatitis C virus; LT, liver transplantation;
NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; OR, odds ratio.
Wong RJ, et al. Gastroenterology. 2015;148:547-555.
170
45
14
-9-10
40
90
140
190
Ne
w W
ait
lis
t R
eg
istr
an
ts (
%)
Change in Liver Transplantation Waitlist
Registrants, 2004–2013
NASH ALD HCV ALD-HCV

Second Annual Spring Hepatology Update 4/30/2016
13
Key Diagnostic Challenges
• Lack of disease awareness and potential
severity among clinicians
• Lack of highly sensitive and specific
noninvasive diagnostic tools that are
readily available
• Lack of treatment approved by FDA

Second Annual Spring Hepatology Update 4/30/2016
14
Predictive Value of Liver
Aminotransferases in NAFLD
• Serum ALT can be normal in up to nearly 60%
of NAFLD patients with NASH1,2
• Serum ALT can be increased in up to 53% of
NAFLD patients with no NASH1,2
• Therefore, serum ALT level alone is not
predictive of NASH or fibrosis level1-3
– Normal ALT cannot rule out progression or NASH
– Increased ALT cannot predict NASH
Abbreviations: ALT, alanine aminotransferase; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis.
1. Fracanzani AL, et al. Hepatology. 2008;48:792-798. 2. Verma S, et al. Liver Int. 2013;33:1398-1405.
3. Torres DM, et al. Nat Rev Gastroenterol Hepatol. 2013;10:510-511.

Second Annual Spring Hepatology Update 4/30/2016
15
AASLD Practice Guidelines for NAFLD
• “Liver biopsy should be considered in patients with
NAFLD who are at increased risk to have
steatohepatitis and advanced fibrosis”
– “The presence of metabolic syndrome and the NAFLD
Fibrosis Score may be used for identifying patients who
are at risk for steatohepatitis and advanced fibrosis”
• “Liver biopsy should be considered in patients with
suspected NAFLD in whom competing etiologies for
hepatic steatosis and co-existing chronic liver
diseases cannot be excluded without a liver biopsy”
All of the above recommendations are: Strength – 1, Evidence – B.
Abbreviations: AASLD, American Association for the Study of Liver Diseases; NAFLD, nonalcoholic steatohepatitis.
Chalasani N, et al. Hepatology. 2012;55:2005-2023.

Second Annual Spring Hepatology Update 4/30/2016
16
Goals of Liver Biopsy
• Identify histologic features of NASH
– “Defined as the presence of hepatic
steatosis and inflammation with hepatocyte
injury (ballooning) with or without fibrosis”1
• Establish diagnosis
• Stage fibrosis
• Assess prognosis
• Rule out concomitant liver disease
– For example, hemochromatosis Abbreviation: NASH, nonalcoholic steatohepatitis.
1. Chalasani N, et al. Hepatology. 2012;55:2005-2023.

Second Annual Spring Hepatology Update 4/30/2016
17
Red Flags for Risk of Progression to
Advanced Fibrosis in Patients with NASH
• Older age (>45 years)1
• Obesity1,2
• Diabetes1
• AST/ALT ratio >11
• Metabolic syndrome, particularly features of
hypertension and insulin resistance3
• Hispanic > non-Hispanic white > black4
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; NASH, nonalcoholic steatohepatitis.
1. Angulo P, et al. Hepatology. 1999;30:1356-1362. 2. Ratziu V, et al. Gastroenterology. 2000;118:1117-1123.
3. Dixon JB, et al. Gastroenterology. 2001;121:91-100. 4. Williams CD, et al. Gastroenterology. 2011;140:124-131.

Second Annual Spring Hepatology Update 4/30/2016
18
Histologic Features Associated with
Disease Progression and Mortality
Hierarchy of
Mortality Risk
1. Fibrosis
2. Portal
inflammation
3. Diagnosis of
NASH
4. Ballooning
degeneratio
n
Abbreviations: CI, confidence interval; HR, hazard ratio; NASH, nonalcoholic steatohepatitis.
Loomba R, et al. Gastroenterology. 2015;149:278-281.
Stage 95% CI of HR
1 1.18, 2.81
2 1.20, 3.03
3 1.16, 3.12
4 3.35, 12.04
Risk of Mortality by
Fibrosis Stage
Stage 95% CI of HR
1 0.63, 8.91
2 2.26, 24.94
3 4.35, 43.65
4 11.94, 188.61
Risk of Liver-
Related Events by
Fibrosis Stage

Second Annual Spring Hepatology Update 4/30/2016
19
Noninvasive Tests for Liver Fibrosis
• Clinical or laboratory tests
– NAFLD Fibrosis Score
– FIB-4 index
– BARD
– AST/ALT ratio
• Imaging modalities
– Shear-wave elastography
• Supersonic imaging, Fibroscan, ARFI
• MRE
– MRI-based
• Liver MultiScan
Abbreviations: ALT, alanine aminotransferase; ARFI, acoustic radiation force impulse; AST, aspartate aminotransferase;
MRE, magnetic resonance elastography; MRI, magnetic resonance imaging; NAFLD, nonalcoholic fatty liver disease.

Second Annual Spring Hepatology Update 4/30/2016
20
NAFLD Fibrosis Score
• Derivation and validation of the scoring system
• 733 NAFLD patients: 480 derivation; 253 validation
• Multivariate analysis
– Age, hyperglycemia, BMI, platelet count, albumin,
AST/ALT ratio are independent predictors of
advanced fibrosis
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; NAFLD, nonalcoholic fatty liver
disease; NPV, negative predictive value; PPV, positive predictive value.
Angulo P, et al. Hepatology. 2007;45:846-854.
Cutoff Point GroupPredictive Value for
Advanced Fibrosis
Low cutoff point:
<–1.455
Derivation NPV 93%
Validation NPV 88%
High cutoff point:
>0.676
Derivation PPV 90%
Validation PPV 82%

Second Annual Spring Hepatology Update 4/30/2016
21
Formula1 Online calculator2
–1.675 + (0.037 x age [years])
+ (0.094 x BMI [kg/m2]) +
(1.13 x IFG/diabetes
[yes =1, no = 0]) +
(0.99 x AST/ALT ratio) –
(0.013 x platelet [109/L]) –
(0.66 x albumin [g/dL])
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index;
IFG, impaired fasting glucose; NAFLD, nonalcoholic fatty liver disease.
1. Angulo P, et al. Hepatology. 2007;45:846-854.
2. NAFLD Fibrosis Score Online Calculator. http://nafldscore.com/.
Calculating the
NAFLD Fibrosis Score
Measures:
– Age
– BMI (kg/mL)
– IGF/diabetes
– AST
– ALT
– Platelets
– Albumin
Available at: http://nafldscore.com

Second Annual Spring Hepatology Update 4/30/2016
22
FIB-4 Index
• Originally developed to predict advanced
fibrosis in HIV/HCV coinfection1
• Subsequently studied in 541 patients with
NAFLD2
– AUROC 0.80
Abbreviations: AUROC, area under receiver operating characteristic curve; HCV, hepatitis C virus; HIV, human immunodeficiency
virus; NAFLD, nonalcoholic fatty liver disease; NPV, negative predictive value; PPV, positive predictive value.
1. Sterling RK, et al. Hepatology. 2006;43:1317-1325. 2. Shah AG, et al. Clin Gastroenterol Hepatol. 2009;7:1104-1112.
Cutoff PointPredictive Value for
Advanced FibrosisInterpretation
Low cutoff point:
<1.30
PPV 43%
NPV 90%
Absence of
advanced fibrosis: F0–1
High cutoff point:
>2.67
PPV 80%
NPV 83%
Presence of
advanced fibrosis: F3–4

Second Annual Spring Hepatology Update 4/30/2016
23
Formula1
Online calculator2
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase.
1. Sterling RK, et al. Hepatology. 2006;43:1317-1325.
2. Hepatitis C Online. http://www.hepatitisc.uw.edu/page/clinical-calculators/fib-4.
Calculator image used with permission from Hepatitis C Online.
Calculating the FIB-4
(Age [years] x AST [U/L])
(Platelet [x109] x √ALT [U/L])

Second Annual Spring Hepatology Update 4/30/2016
24
Transient Elastography
• Measures velocity of a low-frequency (50 Hz) elastic
shear wave propagating through the liver1
• Allows painless and simultaneous measurement of 2
quantitative parameters
– Liver stiffness expressed in kPa: correlates with fibrosis stage2
• Correlated to liver fibrosis stage2
– Controlled attenuation parameter expressed in dB/meter:
correlates with steatosis3
• Volume of liver tissue is 100 times bigger than biopsy4
• False positives: recent meal ingestion, acute hepatitis,
extrahepatic cholestasis, and congestion1
• Low applicability: obesity, ascites, operator inexperience1
1. Castera L, et al. Nat Rev Gastroenterol Hepatol. 2013;10:666-675. 2. Friedrich-Rust M, et al. Gastroenterology. 2008;134:960-974.
3. Sasso M, et al. J Viral Hepat. 2012;19:244-253. 4. Gómez-Domínguez E, et al. Aliment Pharmacol Ther. 2006;24:513-518.

Second Annual Spring Hepatology Update 4/30/2016
25
Magnetic Resonance ElastographySimple
Steatosis
Inflammation
But No Fibrosis Fibrosis
Graphics courtesy of Rohit Loomba, MD, MHSc.

Second Annual Spring Hepatology Update 4/30/2016
26
MRE—Accuracy in Predicting and
Identifying Fibrosis
Prospective study of ability of MRE to predict fibrosis in NAFLD
patients1
• AUROC 0.924
Individual participant data pooled analysis of ability of MRE to detect
fibrosis in NAFLD patients2
• AUROC for stage ≤1, 0.86; stage ≥2, 0.87; stage ≥3, 0.90; stage 4, 0.91
Cross-sectional analysis of a prospective cohort to compare
performance of MRE vs clinical prediction rules (CPR) for predicting
advanced fibrosis3
• AUROC for MRE, 0.957
• AUROC for CPRs, 0.796–0.861
Abbreviations: AUROC, area under receiver operating characteristic curve; MRE, magnetic resonance elastography;
NAFLD, nonalcoholic fatty liver disease.
1. Loomba R, et al. Hepatology. 2014;60:1920-1928. 2. Singh S, et al. Eur Radiol. 2015 Aug 28. [Epub ahead of print].
3. Cui J, et al. Aliment Pharmacol Ther. 2015;41:1271-1280.
Second Annual Spring Hepatology Update 4/30/2016
27
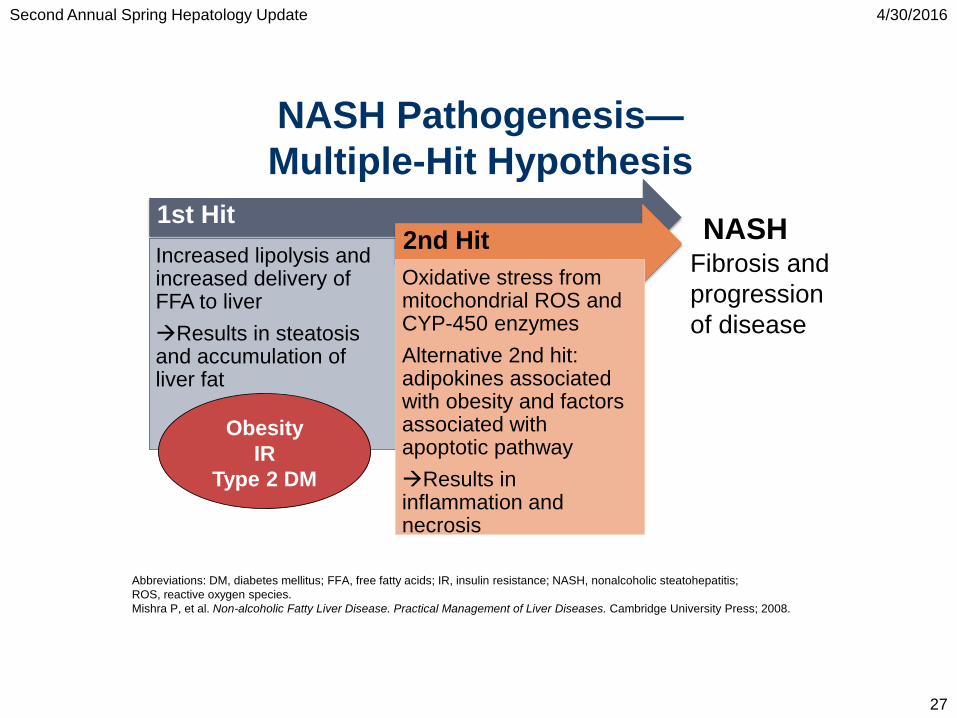
NASH Pathogenesis—
Multiple-Hit Hypothesis
1st Hit
Increased lipolysis and increased delivery of FFA to liver
Results in steatosisand accumulation of liver fat
2nd Hit
Oxidative stress from mitochondrial ROS and CYP-450 enzymes
Alternative 2nd hit: adipokines associated with obesity and factors associated with apoptotic pathway
Results in inflammation and necrosis
Abbreviations: DM, diabetes mellitus; FFA, free fatty acids; IR, insulin resistance; NASH, nonalcoholic steatohepatitis;
ROS, reactive oxygen species.
Mishra P, et al. Non-alcoholic Fatty Liver Disease. Practical Management of Liver Diseases. Cambridge University Press; 2008.
NASHFibrosis and
progression
of disease
Obesity
IR
Type 2 DM

Second Annual Spring Hepatology Update 4/30/2016
28
Key Concepts in the
Pathogenesis of NASH
Browning JD, et al. J Clin Invest. 2004;114:147-152.
From Dr. Loomba:
Delete if cannot get
permission to use.

Second Annual Spring Hepatology Update 4/30/2016
29
Lifestyle change
• Foundation of any treatment plan
• Difficult to achieve and sustain
• Not enough for morbidly obese patients

Second Annual Spring Hepatology Update 4/30/2016
30
RCT Intensive Lifestyle Change and Weight
Loss
48 weeks
Responders:
NAS reduction
of > 3
Promrat Hepatol 2010;51:121

Second Annual Spring Hepatology Update 4/30/2016
31
Class Drug Status
Farnesoid X receptor agonist Obeticholic acid III; Breakthrough*
Fatty acid/bile acid modifier Aramchol IIb; Fast Track*
Dual inhibitor of CCR2 and CCR5 Cenicriviroc IIb; Fast Track*
Dual peroxisome proliferator-
activated receptor alpha/delta
agonist
Elafibranor
(GFT505)
IIb; Fast Track*
Anti-lysyl oxidase-like 2
monoclonal antibody
Simtuzumab IIb
Apoptosis signal-regulating kinase
1 inhibitor
GS-4997 II
Galectin-3-inhibitor GR-MD-02 II; Fast Track*
Niemann–Pick C1-like 1 protein
selective blocker
Ezetimibe II
*FDA.
Therapies in Phase II/III Testing for NASH

Second Annual Spring Hepatology Update 4/30/2016
32
Abbreviations: FXR, farnesoid X receptor; NASH, nonalcoholic steatohepatitis; RXR, retinoid X receptor.
Kuipers F, et al. Nat Rev Endocrinol. 2014;10:488-498. Ratziu V. Nat Rev Gastroenterol Hepatol. 2013;10;676-685.
Zhang Y, Edwards PA. FEBS Lett. 2008;582:10-18. Graphic courtesy of Anne S. Henkel, MD.
Farnesoid X Receptor and Its Role in
NASH
Cholesterol
CYP7a1
DecreaseFibrosis
Hepatic
Stellate Cell
RXR
FXR
Glucose Intolerance
Hepatic Triglycerides
Bile Acids
?
Hepatocyte

Second Annual Spring Hepatology Update 4/30/2016
33
Elafibranor (GFT505)—
Mechanism of Action• Dual PPAR alpha/delta agonist1
• Improves lipid and glucose metabolism in prediabetic patients2
• Improves hepatic and peripheral insulin sensitivity in obese
patients3
• Improves steatohepatitis and fibrosis in mouse NASH models1
• Antifibrotic and anti-inflammatory effect1
PPAR-α PPAR-δ
Expression1 Hepatocytes Ubiquitous
Action1 Lipid and lipoprotein
metabolism
Anti-inflammatory
Mitochondrial function,
fatty acid oxidation, and
insulin sensitivity
Anti-inflammatory
Abbreviations: NASH, nonalcoholic steatohepatitis; PPAR, peroxisome proliferator-activated receptor.
1. Cariou B, et al. Expert Opin Investig Drugs. 2014;23:1441-1448. 2. Cariou B, et al. Diabetes Care.
2011;34:2008-2014. 3. Cariou B, et al. Diabetes Care. 2013;36:2923-2930.

Second Annual Spring Hepatology Update 4/30/2016
34
Phase IIb, 72-week, randomized, double-blind, placebo-
controlled study to assess efficacy and safety of OCA in
patients with NASH; planned interim analysis before end
of treatment
Arms
Patients283 patients ≥18 years of age
Histologic evidence of NASH based on a liver biopsy
obtained ≤90 days prior to randomization; NAS ≥4
Endpoints
Primary
Histologic improvement in NAS from baseline, with no
worsening in fibrosis; decrease in NAS of ≥2 points
Secondary
Resolution of NASH; change in NAS, hepatocellular
ballooning, steatosis, lobular/portal inflammation; change in
liver enzymes, insulin resistance, weight-related measures,
and QOL
Abbreviations: NAS, NAFLD Activity Score; NASH, nonalcoholic steatohepatitis; OCA, obeticholic acid; QOL, quality of life.
Neuschwander-Tetri BA, et al. Lancet. 2015;385:956-965.
Design
1) OCA 25 mg/day
2) Placebo
OCA—Phase IIb FLINT Trial

Second Annual Spring Hepatology Update 4/30/2016
35
FLINT Primary Endpoint—Improved
Liver Histology at Week 72
Histologic response =
• ≥2-point
improvement in NAS
– NAS = steatosis
grade (0–3) +
inflammation grade
(0–3) + ballooning
grade
(0–2)
• No worsening of
fibrosisAbbreviations: NAS, NAFLD activity score; OCA, obeticholic acid.
Neuschwander-Tetri BA, et al. Lancet. 2015;385:956-965.
P =.0002
21
45
0
10
20
30
40
50
60
Placebo OCA 25 mg
Pa
tie
nts
(%
)
(n = 109) (n = 110)
Histologic Response Rate

Second Annual Spring Hepatology Update 4/30/2016
36
3538
31
19
53
61
46
35
0
10
20
30
40
50
60
70
80
Lobularinflammation
Steatosis Hepatocellularballooning
Fibrosis
Pa
tie
nts
wit
h Im
pro
ve
me
nt
(%)
P <.01
FLINT—Improved Secondary
Histologic Outcomes at Week 72
P = .001
Abbreviation: OCA, obeticholic acid.
Neuschwander-Tetri BA, et al. Lancet. 2015;385:956-965.
P <.05
P <.01
Placebo (n = 109)
OCA 25 mg (n = 110)

Second Annual Spring Hepatology Update 4/30/2016
37
Elafibranor (GFT505)—Phase IIb
GOLDEN TrialPhase IIb, 1-year, international, multicenter, randomized,
double-blind, placebo-controlled trial to assess the safety
and efficacy of elafibranor in noncirrhotic patients with NASH
Arms1,21) Elafibranor 80 mg
2) Elafibranor 120 mg
3) Placebo
Patients1,2
274 patients ≥18 years of age
Histologic evidence of NASH based on a liver biopsy;
treatment with vitamin E, polyunsaturated fatty acids, or
ursodeoxycholic acid discontinued 3 months prior to biopsy
Endpoints1
Primary
Resolution of NASH with no worsening of fibrosis
Secondary
Change in NAS, fibrosis, liver enzymes, lipid parameters,
metabolic markers, safety markers
Abbreviations: NAS, NAFLD Activity Score; NASH, nonalcoholic steatohepatitis.
1. ClinicalTrials.gov. NCT01694849. https://clinicaltrials.gov/ct2/show/NCT01694849.
2. Ratziu V, et al. Hepatology. 2015;62(suppl 1):262A.
Design1

Second Annual Spring Hepatology Update 4/30/2016
38
GOLDEN—Preliminary Findings
• Primary endpoint was not met in
initial assessment
– Elafibranor was not better than
placebo in resolving NASH
– After controlling for baseline
heterogeneity of severity and center
effect, the primary endpoint was met
• Main caveats
– High placebo response due to
inclusion of milder disease
– Subset analysis: NAS >5 shows
significant improvement in elafibranor
120-mg group vs placebo
Abbreviations: ELF, elafibranor; NAS, NAFLD Activity Score; NASH, nonalcoholic steatohepatitis; PBO, placebo.
Ratziu V, et al. Hepatology. 2015;62(suppl 1):262A.
27.5
14.8
19.5
00
10
20
30
40
Re
sp
on
se
Ra
te (
%)
ELF 120 mg
PBO
NAS 4–5 NAS >5

Second Annual Spring Hepatology Update 4/30/2016
39
Conclusions
• Nonalcoholic fatty liver disease (NAFLD) has
tremendous clinical, economic, and patient-reported
outcome burden to patients and to society
– This burden is growing globally
• Nonalcoholic steatohepatitis (NASH) is the progressive
form of NAFLD
• Histologic fibrosis (stage 2 or more) predicts
liver-related mortality
• Pathogenesis of NASH is complex, requiring multiple hits
• Biomarkers should be based on pathogenetic pathways
• Treatment targets to be carefully chosen