non-interventional study report - vfa.de · clinical development exelon® / rivastigmine...
TRANSCRIPT

Clinical Development
Exelon® / Rivastigmine
Non-interventional Study Report
CENA713DDE25
EXUBAD: A non-interventional study with Exelon® patch to
determine the impact of a training, based on „Demenz aktiv begegnen“ on the burden of the caregivers of patients with
Alzheimer’s Dementia
Author XXXXXXXXXXXXXXXXXXXXX (CRO: Institut Dr. Schauerte)
Document Status Final Version 1.2
Date of last version of the study report
04 September 2015
Property of Novartis Confidential
May not be used, divulged, published or otherwise disclosed without the consent of Novartis
NI Report Template Version 31 January 2013

Novartis Confidential 2 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table of contents
Table of contents ................................................................................................................. 2
List of abbreviations ............................................................................................................ 4
1 Synopsis ............................................................................................................................... 6
2 Marketing Authorization Holder ....................................................................................... 12
3 Study group ....................................................................................................................... 12
4 Milestones .......................................................................................................................... 13
5 Rationale and background ................................................................................................. 13
6 Research question and objectives ...................................................................................... 14
7 Amendments and updates to the protocol ......................................................................... 15
8 Research methods .............................................................................................................. 15
8.1 Study design........................................................................................................... 15
8.2 Setting .................................................................................................................... 16
8.3 Subjects .................................................................................................................. 16
8.3.1 Inclusion criteria .................................................................................... 17
8.3.2 Exclusion criteria .................................................................................. 18
8.4 Variables ................................................................................................................ 18
8.4.1 Start of observation/ initial visit ............................................................ 18
8.4.2 Evaluation of the training (only in the group of patients with
Exelon® patch plus training of caregiver) ............................................. 19
8.4.3 Follow-up checks during observation period ........................................ 19
8.4.4 End of the observation .......................................................................... 19
8.4.5 Observation plan ................................................................................... 20
8.5 Data sources and measurement .............................................................................. 21
8.6 Bias ........................................................................................................................ 22
8.7 Study size ............................................................................................................... 22
8.8 Monitoring ............................................................................................................. 22
8.9 Data transformation ............................................................................................... 22
8.10 Statistical methods ................................................................................................. 22
8.11 Quality control ....................................................................................................... 23
9 Results ............................................................................................................................... 23
9.1 Participants ............................................................................................................ 23
9.2 Descriptive data ..................................................................................................... 24
9.2.1 Demography .......................................................................................... 24
9.2.2 Living Conditions.................................................................................. 25

Novartis Confidential 3 Non-interventional study report Exelon
® patch/ CENA713DDE25
9.2.3 Diagnosis ............................................................................................... 27
9.2.4 Pretreatment of dementia ...................................................................... 27
9.2.5 Reason for switch and type of prescription of Exelon® patch .............. 29
9.2.6 Exelon®
patch daily dose ....................................................................... 30
9.2.7 Evaluation of the training “Demenz Aktiv Begegnen” ......................... 31
9.2.8 Follow-up visits ..................................................................................... 35
9.2.9 Mini-Mental State Examination ............................................................ 36
9.2.10 Discontinuation of the therapy with Exelon® patch .............................. 38
9.2.11 General circumstances of caregivers ..................................................... 39
9.2.12 Mini-Zarit assessment of caregiver burden ........................................... 43
9.2.13 GDS assessment of caregivers .............................................................. 45
9.3 Outcome data ......................................................................................................... 49
9.4 Main results ........................................................................................................... 49
9.5 Other analyses ........................................................................................................ 49
9.6 Adverse events and adverse reactions ................................................................... 50
9.6.1 Brief summary of adverse events .......................................................... 50
9.6.2 Display of adverse events ...................................................................... 51
9.6.3 Deaths, other serious events, and other significant adverse events ....... 59
10 Discussion .......................................................................................................................... 60
10.1 Key results ............................................................................................................. 60
10.2 Limitations ............................................................................................................. 62
10.3 Conclusion ............................................................................................................. 62
11 References ......................................................................................................................... 63

Novartis Confidential 4 Non-interventional study report Exelon
® patch/ CENA713DDE25
List of abbreviations
AD Alzheimer`s Dementia
ADR Adverse Drug Reaction
AE Adverse Event
AMG (deutsches) Arzneimittelgesetz – (German) Drug Law
BfArM Bundesinstitut für Arzneimittel und Medizinprodukte -
German Federal Institute for Drugs and Medical Devices
ChEI Cholinesterase Inhibitor
CRF Case Report/Record Form
CRO Contract Research Organization
e.g. exempli gratia (Latin); for example (English)
EMEA European Agency for the Evaluation of Medicinal Products
EU European Union
FSA Freiwillige Selbstkontrolle für die Arzneimittelindustrie – voluntary self-regulation
for the pharmaceutical industry
FU Follow-up
GDS Geriatric Depression Scale
i.e. id est (Latin); that is to say (English)
ICD International Statistical Classification of Diseases and Related Health Problems
IDS Institute Dr. Schauerte
INI Initial visit
MedDRA Medical Dictionary for Regulatory Activities
MMSE Mini Mental State Examination
N/A Not applicable
NIS Non-Interventional study
NMDA N-Methyl-D-Aspartate
nsADR Non-serious Adverse Drug Reaction
nsAEnr Non-serious Adverse Event non-related
PEI Paul-Ehrlich-Institut
PMS Post-marketing surveillance
PT Preferred Term
RMP Risk Management Plan
SADR Serious Adverse Drug Reaction
SAE Serious Adverse Event
SAEnr Serious Adverse Event non-related
SD Standard deviation

Novartis Confidential 5 Non-interventional study report Exelon
® patch/ CENA713DDE25
SmPC Summary of Product Characteristics
SOC System Organ Class
SOP Standard Operating Procedure
v Version
vs. Versus
VFA Verband Forschender Arzneimittelhersteller - Association of Researching
Pharmaceutical Manufacturers
WHO World Health Organization

Novartis Confidential 6 Non-interventional study report Exelon
® patch/ CENA713DDE25
1 Synopsis
Title EXUBAD: A non-interventional study (NIS) with Exelon® patch to determine
the impact of a training, based on „Demenz aktiv begegnen“ on the burden of the caregivers of patients with Alzheimer’s Dementia
Author(s): XXXXXXXXXXXXXXXXXX (CRO: Institut Dr. Schauerte)
Date: 04 SEP 2015
Keywords Exelon® patch, Alzheimer´s disease/ dementia, caregivers training, clinical
practice
Rationale and
background
Alzheimer's disease (AD) is a chronic neurodegenerative disorder and the most common cause of dementia (50-70 % of cases). It is a fatal and progressive disease that destroys brain cells in its course. This leads to problems in memory, thinking skills and behavior severe enough to interfere with a person’s work and social life. Alzheimer’s primarily affects older adults over 60 years of age; its prevalence and incidence increases with age.
Although there is currently no cure for AD, there are medications that help control the symptoms of the disease. The active ingredient rivastigmine is the first and only approved transdermal cholinesterase inhibitor (Exelon
®
patch).
A systematic review of the effectiveness of educational programs in dementia care shows that combined drug and non-drug therapies can improve the quality of life of patients and their families (Perry et al, 2011). "Demenz aktiv begegnen" is a training concept by Novartis for the training of caregivers of patients with AD. The goal of the training is to provide information about AD to relatives/ caregivers and patients so that they are able to better cope with the disease.
This study intended to observe whether and to what extent this training is beneficial to patients and their caregivers with respect to the long-term clinical course of the therapy as well as the burden and quality of life of family caregivers.
Research question
and objectives
The study objective was to compare two groups: Patients with AD treated with Exelon
® patch versus patients treated with Exelon
® patch whose
caregivers additionally participated in a training session based on "Demenz aktiv begegnen".
The following parameters were observed:
• The long-term clinical course of the therapy with Exelon® patch over 12
months (assessed by Mini Mental State Examination; MMSE)
• The burden on caregivers of AD patients (Mini-Zarit and Geriatric Depression Scale (GDS))
• The persistence with the Exelon® patch therapy over 12 months
(assessed by information from investigators and caregivers as well as calculated from the quantities of prescriptions)
Study design This post-marketing surveillance (PMS) was an open, prospective, two-arm,

Novartis Confidential 7 Non-interventional study report Exelon
® patch/ CENA713DDE25
non-interventional, multicenter observational study and was carried out within an approved indication in accordance with guidelines of the European Agency for the Evaluation of Medicinal Products (EMEA, “Volume 9A of the Rules Governing Medicinal Products in the European Union”), the recommendations of the Association of Researching Pharmaceutical Manufacturers (VFA), and applicable local law(s) and regulation(s) of the Federal Institute for Drugs and Medical Devices (BfArM).
Setting It was planned to observe 350 patients (5 patients per site) in 70 sites.
The study population consisted of male and female outpatients with Alzheimer's disease who were treated with Exelon
® patch based on the
decision of the treating physician independent of the participation in this study.
Subjects and study
size, including
dropouts
A total of 206 AD patients were enrolled at 41 sites in Germany in this non-interventional study which was conducted between 15 April 2013 and 21 November 2014. Six enrolled patients were excluded from the safety population, mainly due to missing informed consent. Among the 200 patients valid for safety analysis, 40 patients were excluded from efficacy analysis, mainly due to loss to follow-up (not any follow-up information documented).
The following inclusion and exclusion criteria were applied:
Inclusion criteria:
• Male and female patients with a secured or probable clinical diagnosis of mild to moderate degenerative Alzheimer dementia (AD)
• Medication with Exelon® patch according to the approval criteria and the
current Summary of Product Characteristics (SmPC)
• Patients who were newly treated with cholinesterase inhibitors or patients who showed insufficient response to another cholinesterase inhibitor or memantine in terms of clinical efficacy
• The caregiver and patient had to be able to answer the questions asked
Exclusion criteria:
• Applicable contraindications, as listed in the SmPC of Exelon® patch
• Patient suffered from a serious or instable physical illness preventing the full participation in the study
• Patients with skin diseases and a risk of developing skin irritations (e.g. atopic dermatitis)
• Patient or caregiver participated in a training program for Alzheimer's disease in the last 6 months or was part of a professional caregiver project
Written informed consent was obtained from all patients included and their caregivers.
Variables and data
sources
Data were recorded on standardized case report forms (CRF).
All variables were analyzed by descriptive statistical methods. The number of data available as well as missing data, mean, standard deviation (SD), minimum, quartiles, median and maximum were calculated for metric data. Frequency tables were generated for categorical data.

Novartis Confidential 8 Non-interventional study report Exelon
® patch/ CENA713DDE25
Statistical analyses were primarily of an explorative and descriptive nature.
The statistical evaluation was performed using the SAS® software package
release 9.2.
Results Results Summary — Study objectives
Results are based on the efficacy population (n=160). 119 (74.4 %) patients were in the cohort without trained caregivers vs. 41 patients (25.6 %) in the cohort with trained caregivers. More female (56.9 %) than male patients (41.3 %) were included in the study. The mean age of patients was 77.5 ± 6.7 years. The majority of all patients (60.0 %) were between 75 - 85 years. Most patients (71.3 %) lived primarily with their family members. The majority of patients were cared for by their spouses (55.6 %). In the opinion of the physicians more than half of the caregivers were fully able to take care of their AD patients (56.9 %). The estimated ability of the trained cohort (n=37/41; 90.2 %) was twice as high as the non-trained cohort (45.4 %).
The mean duration of AD since its first diagnosis was 10.8 ± 17.7 months. According to International Statistical Classification of Diseases and Related Health Problems (ICD)-10 classification of diagnoses the vast majority of all observed patients as well as the great majority of patients within the stratified cohorts (trained caregivers cohort 63.4 %; non-trained cohort 59.7 %) were affected by late-onset Alzheimer’s dementia.
More than two-thirds of patients (68.8 %) were treatment naïve prior to enrolment compared to 28.8% pretreated patients. A much larger proportion of patients (72.3 %) was treatment naïve in the cohort with untrained caregivers compared to 58.5 % in the trained cohort. More patients (36.6 %) in the group with trained caregivers had already received an anti-dementive pretreatment compared to 26.1 % in the untrained group. Of the 46 patients with previous treatment, the most frequently prescribed treatments were Donepezil (23.9 %), Axura
® (19.6 %) and Exelon
® capsules (10.9 %). The
most frequently used application form was oral (89.1 %).
As reasons for the switch to the Exelon® patch, “insufficient efficacy of
premedication”, “other/ unknown” and “side effects/ adverse events” reasons were documented in 45.7 %, 43.5 % and 15.2 % of pretreated patients, respectively. In the majority of patients (83.8 %), the Exelon
® patch was
newly prescribed. In the cohort with trained caregivers all patients but one (97.6 %) were newly adjusted to the Exelon
® patch compared to 79.0 % in
the non-trained cohort. At baseline, the vast majority of patients (83.8 %) was prescribed 4.6mg/24 hours Exelon
® patches. 97.6 % of patients with a
trained caregiver were adjusted to the initial dose of 4.6mg/24 hours compared to 79.0% in the non-trained cohort. At the first follow-up visit after 4 to 6 months, half of all observed patients were treated with the 9.5mg Exelon
® patch. This proportion remained nearly constant in the further
course of the observation. About one quarter of patients received the Exelon
® patch 13.3mg/24 hours at the second and third follow-up visit. As a
result of dose adjustments at the last individually documented visit, 16.3 % of patients received the 4.6mg/24 hours Exelon
® patch whereas 32.5 % were
prescribed the 9.5mg/24 hours Exelon® patch and 20.6 % the 13.3mg/24
hours Exelon® patch.
41 caregivers participated in the “Demenz aktiv begegnen” trainings after 4-10 weeks (Training 1) and 3-6 months (Training 2). The main focus of both trainings was evaluated to be the “treatment of dementia” (Training 1: 95.1 %

Novartis Confidential 9 Non-interventional study report Exelon
® patch/ CENA713DDE25
vs. Training 2: 80.5 %) and “dementia in general” (Training 1: 82.9 % and Training 2: 46.3 %). Another important focus of Training 2 (68.3 %) and to a lesser extent of Training 1 (51.2 %) was the subject “everyday life with dementia patients”. The average evaluation of the usefulness of the training was 8.5 ± 1.3 for Training 1 and 8.7 ± 1.2 for Training 2.
Physicians documented one initial visit (baseline visit), up to two follow-up visits per patient (1st FU: after 4-6 months; 2nd FU: after 8-10 months) and one final visit at the end of the observation after approximately one year or in case of premature study termination. The mean duration from the initial to the first follow-up visit was 4.6 ± 1.7 months for all observed patients. Mean duration from the first to the second follow-up visit was documented as 4.0 ± 1.7 months and from the second to the third follow-up visit as 3.4 ± 1.2 months.
At baseline and at each follow-up visit, physicians could document the severity of dementia using the MMSE, if it was performed in routine clinical practice. The average sum score of MMSE for the total study population was 20.5 ± 4.2 points at the start of the observation compared to 19.9 ± 4.5 points at the last individual follow-up visit. The mean MMSE score decreased slightly from start of observation to last individual visit by 0.7 ± 3.1 points.
Premature discontinuation of Exelon® patch therapy was recorded for 47
(29.4 %) of all observed patients. 13 of these patients were in the cohort with trained caregivers and 34 in the non-trained cohort. Mean duration until discontinuation of therapy in total was 7.5 ± 4.3 months. The average duration in the trained cohort was 8.7 ± 5.1 months and 6.8 ± 3.7 months in the non-trained cohort. Reasons for premature discontinuation were “adverse events” and “patient did not return” in 16 patients, respectively, and “insufficient efficacy” and “patient died” in 2 patients, respectively.
More female (57.5 %) than male caregivers (34.4 %) took part in the study. The majority of all caregivers (43.8 %) were over 70 years old. 35.0 % of all caregivers reported carrying full responsibility for administering the prescribed medication to their patient (29.3 % “with training” and 37.0 % “without training”). 72.5 % of caregivers had never before taken care of a close relative over a period of several weeks (80.5 % “with training” and 69.7 % “without training”).
At the initial visit 56.9 % of all caregivers considered the patient’s age to be the cause of AD (73.2 % “with training” and 51.3 % “without training”) while only 47.5 % thought so at the last documented visit (51.2 % “with training” and 46.2 % “without training”). At the initial visit, all caregivers believed to an average extent of 6.3 ± 1.9 points in the helpfulness of AD treatment with medication (6.3 ± 2.3 points “with training” and 6.3 ± 1.7 points “without training”). At the last documented visit, the caregivers believed in the helpfulness of medication to a lesser extent of 6.1 ± 2.1 points due to a decreased score among caregivers with training (5.5 ± 2.0 points “with training” and 6.3 ± 2.1 points “without training”).
The symptoms most common among the caregivers at the initial visit were insomnia and fatigue (32.5 %, respectively), followed by backache (26.3 %). At the last documented visit, the most common symptom was fatigue (24.4 %), followed by insomnia and backache (22.5 %, respectively). Nearly 60 % of caregivers at the initial visit and nearly 40 % at the last documented visit reported not taking any medication from the classes of drugs listed. At the initial visit, caregivers most often took antidepressants and sleeping pills

Novartis Confidential 10 Non-interventional study report Exelon
® patch/ CENA713DDE25
(10.6 % and 8.1 %, respectively), which were also most often taken at the last documented visit (10.0 % and 9.4 %, respectively). At the initial visit, 12.5 % of caregivers had been hospitalized in the last half year, 5.6 % had been on sick leave, and 2.5 % had been to rehabilitation. In the course of the study, a stay in the hospital, rehabilitation and/or sick leave was needed at least once by 3.1 %, 1.9 % and 3.8 % of caregivers, respectively.
The Mini-Zarit scale was used to assess the burden on the caregivers. The average sum score of Mini-Zarit for all caregivers was 4.6 ± 1.8 points at the start of the observation compared to 4.5 ± 1.7 points at the last individual follow-up visit. The score decreased somewhat in the course of therapy. The mean sum scores were consistently lower, i.e., worse, for caregivers without training (4.2 ± 1.7 points at initial visit and 4.3 ± 1.7 points at the last documented visit) than for the caregivers overall, while the trained caregivers (5.5 ± 1.5 points at initial visit and 5.0 ± 1.4 points at the last documented visit) consistently had better average scores than all caregivers.
Further the GDS was used to assess the burden on caregivers. The average sum score of GDS for all caregivers was 3.1 ± 2.9 points at the start of the observation compared to 3.0 ± 2.2 points at the last individual follow-up visit. The score remained largely constant in the course of therapy. The mean sum scores were consistently higher, i.e., worse, for caregivers without training (3.3 ± 3.0 points at initial visit and 3.2 ± 2.4 points at the last documented visit) than for the caregivers overall, while the average scores of the trained caregivers (2.8 ± 2.7 points at initial visit and 2.6 ± 1.7 points at the last documented visit) were consistently better than those of all caregivers and decreased in the course of the study.
Results Summary — Safety
Safety evaluation was based on the population of evaluable patients (n=200). Over a quarter of patients (n=52/200, 26.0%) were affected by at least one adverse event (AE) of any nature. The rate was lower in the group with untrained caregivers (n=26/129, 20.2%) than with trained caregivers (n=26/71, 36.6%). Adverse drug reactions, i.e., nsADR and SADR, occurred in 36/200 (18.0%) and 2/200 patients (1.0%), respectively. 18 patients (9.0%) had serious AEs without drug-relation (SAEnr), 2 patients (1.0%) had serious adverse drug reactions (SADR). 30 cases of medication error (15%) and 4 cases of lack of drug effect (2%) were documented. 5 patient deaths were recorded in the study, 1 of which was assessed to be drug-related. In patients with AEs, the number of AEs of any nature was most frequently 1 per patient (10.5%), followed by 2 AEs per patient (7.5%). Of the 129 AEs that occurred altogether, 24 were non-serious and not drug-related (nsAEnr), 63 were non-serious adverse drug reactions (nsADR), 39 were serious and not drug-related (SAEnr), and 3 were serious adverse drug reactions (SADR). Most AEs belonged to the system organ classes (SOCs) "skin and subcutaneous tissue disorders" (16.3%), "psychiatric disorders" (14.7%), "nervous system disorders" (13.2%), "gastrointestinal disorders" (10.1%), "general disorders and administration site conditions" (10.1%) and "cardiac disorders" (8.5%). The preferred terms (PTs) for the most frequently recorded AEs of any group were "nausea" (4.7%) and "depression" (3.9%).
Discussion This NIS in patients with mild to moderate AD showed a better Mini-Zarit and GDS in trained than in untrained caregivers both at baseline and the last individual FU. These validated questionnaires pointed to a stable or slightly reduced burden preferably in non-trained, mainly familiar caregivers. Thus, a

Novartis Confidential 11 Non-interventional study report Exelon
® patch/ CENA713DDE25
more detailed information on the disease and its perspective might increase the feeling of burden in trained caregivers. So far, there are only few data on long-term therapy in AD. This NIS also demonstrated a nearly stable severity of the disease within one year of therapy with the rivastigmine patch, which was well tolerated with a low frequency of ADRs. Additional training may therefore help the familial caregivers in daily life to reduce the burden of disease and to increase patient persistence for symptomatic therapy in patients with mild to moderate AD.
Marketing
Authorization
Holder
Novartis Pharma GmbH
Name(s) and
Affiliation(s) of
Principal
Investigator(s)
XXXXXXXXXX XXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXX XXXXXXXXXXX XXXXXXXXXXXXXXX XXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX

Novartis Confidential 12 Non-interventional study report Exelon
® patch/ CENA713DDE25
2 Marketing Authorization Holder
Novartis Pharma GmbH
Roonstraße 25
D-90429 Nürnberg
3 Study group
Principle investigator XXXXXXXXXX XXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXX XXXXXXXXXXX XXXXXXXXXXXXXXX XXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
Project Lead XXXXXXXXXXXXX
Novartis Pharma GmbH
Roonstraße 25, D-90429 Nürnberg Phone 0911 273 XXXXX Fax 0911 273 XXXXX Email: [email protected]
Senior Expert
Phase IV Manager
XXXXXXXXXXXXXX
Novartis Pharma GmbH
Roonstraße 25, D-90429 Nürnberg Phone 0911 273 XXXXX Fax 0911 273 XXXXX Email: [email protected]
Safety Manager XXXXXXXXXXXXXXX
Novartis Pharma GmbH
Roonstraße 25, D-90429 Nürnberg Phone 0911 273 XXXXX Fax 0911 273 XXXXX Email: [email protected]
Project coordinator
and statistics
XXXXXXXXXXXXXXX Institut Dr. Schauerte (IDS) Finkenstraße 7, D-80333 München Phone: 089/ 641-XXXXX Fax: 089/ 641- XXXXX E-mail: [email protected]

Novartis Confidential 13 Non-interventional study report Exelon
® patch/ CENA713DDE25
4 Milestones
Table 4.1 Study milestones
Milestone Planned date Actual date
Start of data collection 1 March 2013 08 April 2013
End of data collection 31 November 2014 21 November 2014
Final report of study results 31 December 2014 04 September 2015
5 Rationale and background
Alzheimer's disease (AD) is a chronic neurodegenerative disorder and the most common
cause of dementia (50-70% of cases). It is a fatal and progressive disease that destroys brain
cells in its course. This leads to problems in memory, thinking skills and behavior severe
enough to interfere with a person’s work and social life. Alzheimer’s primarily affects older
adults over 60 years of age; its prevalence and incidence increases with age (Alzheimer`s
Association, 2012).
Although there is currently no cure for AD, there are medications that help control the
symptoms of the disease. The active ingredient rivastigmine is the first and only approved
transdermal cholinesterase inhibitor (Exelon® patch).
Various acetylcholinesterase inhibitors (ChEI; active compounds rivastigmine, galantamine
and donepezil) and the N-methyl-D-aspartate (NMDA) antagonist memantine have been
approved to treat Alzheimer's symptoms (Cummings et al, 2002). The active ingredient
rivastigmine was approved in the EU in 2007 as the first and only transdermal cholinesterase
inhibitor (Exelon® patch). In many cases of chronic diseases it was shown that patients or
caregivers form opinions of their own about the cause of the disease, its nature (symptomatic
experience), the duration, the personal consequences or the resulting suffering and also about
the extent to which the disease can be controlled or cured. Patients also have opinions about
the type of treatment: This involves the perception of the necessity for treatment (such as the
absence of symptoms) and concerns about possible side effects. These views determine how
people deal with their disease in psychological and behavioral terms, such as compliance with
medication requirements (Horne & Weinman, 1999). As the disease progresses and treatment
options for the patients decline, the views of caregivers and physicians increasingly determine
the choice of treatment, adherence and persistence (Small & Dubois, 2007).
Persistence is defined as "the length of the time from the beginning to the discontinuation of a
treatment and is measured in units of time" (Hughes et al, 2007). A non-persistent behavior
occurs when the patient treatment is completely terminated - either because the patient
himself (or his supervisor) makes the decision to terminate or because the treating physician
decides to discontinue a particular treatment. Therefore, persistence is usually determined in
the form of an event history analysis; the patients either terminate the treatment before the end
of the observation or they continue to the end (e.g. right censored data). In one study,
persistence rates were 40% for twelve months; in several other studies, the observed
persistence was between 135-492 days (Small & Dubois, 2007).

Novartis Confidential 14 Non-interventional study report Exelon
® patch/ CENA713DDE25
So far, there are comparatively few studies that investigate which psychosocial therapies are
effective in improving the quality of life of caregivers of patients with dementia. A
systematic review of characteristics that can effect a response to such psychosocial therapies
has identified several parameters. Female caregivers are able to achieve the greatest effect by
training (Van Mierlo et al, 2012). A systematic review of the effectiveness of educational
programs in dementia care shows that combined drug and non-drug therapies can improve the
quality of life of patients and their families (Perry et al, 2011).
"Demenz aktiv begegnen" is a training concept by Novartis for the training of caregivers of
patients with AD. The goal of the training is to provide information about AD to relatives/
caregivers and patients so that they are able to better cope with the disease. The contents of
the training are information about AD itself, therapies, cognitive training, physical training as
well as legal and social aspects of the disease.
This study investigated whether and to what extent this training is beneficial to patients and
their caregivers with respect to the long-term clinical course of the therapy as well as the
burden and quality of life of family caregivers.
6 Research question and objectives
The study objective was to compare two patient groups: Patients with AD treated with
Exelon® patch versus patients treated with Exelon
® patch whose caregivers additionally
participated in a training based on "Demenz aktiv begegnen".
The following parameters were observed:
• The long-term clinical course of the therapy with Exelon® patch over 12 months (assessed
by Mini Mental State Examination; MMSE)
• The burden on caregivers of patients with AD (Mini-Zarit and GDS)
• The persistence with the Exelon® patch
therapy over 12 months (assessed by information
from investigators and caregivers as well as calculated from the quantities of
prescriptions)
The observation was meant to include newly adjusted patients in order to achieve an even
baseline at the time of the training of caregivers and, thus, to make the effects on the burden
of caregivers comparable.
Both groups of patients and their caregivers (with or without standard training) were included
in the NIS in accordance with routine clinical practice.

Novartis Confidential 15 Non-interventional study report Exelon
® patch/ CENA713DDE25
7 Amendments and updates to the protocol
Revision of Chapter "Adverse Events"
The changes in the European pharmacovigilance legislation concerning the
pharmacovigilance processes were adapted in the NIS and required a complete rewrite of
Chapter 7, "Adverse Events".
The following changes were made:
• Expansion of the term "adverse event"
• Modified reporting requirements and handling of adverse event notifications after
completion of the study
• Recurring manifestations, complications and similar events should be handled as a
follow-up
• Handling events of special interest (Risk Management Plan; RMP)
• Specification regarding handling of cases of "progression of the underlying disease"
Adjustment of the timeline
The timeline was updated.
8 Research methods
8.1 Study design
This post-marketing surveillance (PMS) was an open, prospective, two-arm, non-
interventional, multicenter observational study in accordance with section 4 paragraph 23
sentence 3 of German drug law (AMG, Arzneimittelgesetz) within an approved indication.
The treatment was performed according to clinical practice (including diagnosis and
monitoring) without a pre-defined observational test plan. The study was consistent with the
guidelines of EMEA (“Volume 9A of the Rules Governing Medicinal Products in the
European Union”), the “Freiwillige Selbstkontrolle für die Arzneimittelindustrie” (FSA)-
codex, the recommendations of the Federal Institute for Drugs and Medical Devices (BfArM)
and Paul-Ehrlich-Institut (PEI) for the planning, implementation and evaluation of
observational studies. In addition, the study was performed in accordance with the
Association of Researching Pharmaceutical Manufacturers (VFA) recommendations for
improving the quality and transparency of non-interventional studies.
The following visits were documented (if they took place):
Visit at the beginning of the observation: initial visit (INI)
Training 1 (Only for the group with training): after 4-10 weeks
Training 2 (Only for the group with training): after 3-6 months
1st follow-up visit (1. FU): after 4-6 months

Novartis Confidential 16 Non-interventional study report Exelon
® patch/ CENA713DDE25
2nd follow-up visit (2. FU): after 8-10 months
Visit at the end of the observation (3. FU): after approximately 1 year
Information was collected for the following patient groups during the observation:
Group with training: • patients with AD who were newly adjusted to Exelon® patch
• caregivers who participated in the training "Demenz aktiv
begegnen" in clinical practice
Group without training: • patients with AD who were newly adjusted to the Exelon® patch
• caregivers without training in clinical practice
All adverse events (AEs) had to be documented in designated report forms and sent to the
contract research organization (CRO) within 10 days after documentation. Serious adverse
events (SAEs) were recorded on a separate SAE form and had to be reported within 24 hours
to NOVARTIS Pharma GmbH, Drug Safety Department.
In case the study was prematurely discontinued, the reason had to be documented.
8.2 Setting
According to the observational plan, 350 patients with mild to moderate Alzheimer’s disease
were to be observed at 70 sites (5 patients per site). The participating investigators were
neurologists, psychiatrists, geriatricians, general practitioners and general practitioners
specialized in geriatrics. A total of 206 patients were actually enrolled at 41 sites. This non-
interventional study (NIS) was conducted between 15 April 2013 and 21 November 2014.
The study population consisted of male and female outpatients with Alzheimer's disease who
were treated with the Exelon® patch independently of participation in this study. Warnings
and contraindications were considered in accordance with the current Summary of Product
Characteristics (SmPC).
8.3 Subjects
A total of 206 patients were documented in this NIS. Six enrolled patients were excluded from
the safety population, mainly due to missing informed consent. Among the 200 patients valid
for safety analysis, 40 patients were excluded from efficacy analysis, mainly due to loss to
follow-up (not any follow-up information documented). The numbers of patients excluded
from either safety analysis or efficacy analysis are summarized in Figure 1 with detailed
reasons for exclusion.

Novartis Confidential 17 Non-interventional study report Exelon
® patch/ CENA713DDE25
Figure 1 Disposition of patients
8.3.1 Inclusion criteria
The inclusion and exclusion criteria for patients were:
Inclusion criteria:
• Male and female subjects with a secured or probable clinical diagnosis of mild to
moderate degenerative AD
• Medication with Exelon® patch according to the approval criteria and the current safety
information
• Patients who were newly treated with cholinesterase inhibitors or patients who showed
insufficient response to another cholinesterase inhibitor or memantine
• Ability of caregiver and patient to answer the questions asked
Total study population (n=206)
Exclusions from efficacy population N (%)
Total Safety Population 200 (100.0)
Lost to follow-up 38 (19.0)
Violation of inclusion/exclusion criteria 3 (1.5)
Retrospective recruitment 6 (3.0)
Missing documented prescription of Exelon® patch
at baseline
2 (1.0)
Total Efficacy Population 160 (80.0)
*Multiple responses possible
Exclusions from safety population N (%)
Total 206 (100.0)
No documented prescription of Exelon® patch 1 (0.5)
No written informed consent 5 (2.4)
Total Safety Population 200 (97.1)
Efficacy population (n=160)
Safety population (n=200)

Novartis Confidential 18 Non-interventional study report Exelon
® patch/ CENA713DDE25
8.3.2 Exclusion criteria
Exclusion criteria:
• Applicable contraindications, as listed in the Summary of Product Characteristics (SmPC)
of Exelon®
patch
• Serious or instable physical illness preventing the patient’s full participation in the study
• Skin diseases and a risk of patient for developing skin irritations (e.g. atopic dermatitis)
• Patient or caregiver participated in a training program for Alzheimer's disease in the last 6
months or was part of a professional caregiver project
Written informed consent was obtained from all patients included and their caregivers.
8.4 Variables
In this non-interventional study, only diagnostic procedures and therapeutic indications of
Exelon® patch conducted according to routine clinical practice were documented by the
physicians.
8.4.1 Start of observation/ initial visit
• Patient consent: A signed informed consent was required from the patient (and/ or his
[legal] representative) as well as from the caretaker (not in the legal, but the nursing sense)
prior to inclusion into the observation. The signed informed consent forms had to be
archived by the respective investigator.
• Demographic data (age, sex, height and weight)
• Diagnosis, medical history
• Any pre-treatment with another antidementive medication
• Prescription of Exelon® patch: dose strength and pack size
• MMSE score of the patient (only if recorded)
• Housing and living conditions of the patient (at home, in a nursing home)
• Relationship between caretaker and patient
• Suitability assessment of the caretaker by the treating physician
• Extent to which the patient is responsible for his own medication
• Time requirements for nursing/ care
• Caregiver:
- Age, gender
- Health status (physical, stress situation, depression)
- Opinion and attitude towards AD
- Expectations regarding the effectiveness of Exelon® patch

Novartis Confidential 19 Non-interventional study report Exelon
® patch/ CENA713DDE25
- Physical health (mood, treatment status and medical interventions)
- Psychotropic medication
8.4.2 Evaluation of the training (only in the group of patients with Exelon® patch plus training of caregiver)
• Date of training
• General conditions (duration, number of participants)
• Topics covered
• Evaluation form by the caregiver
8.4.3 Follow-up checks during observation period
• Date of observation
• Persistence
• Prescription of Exelon® patch: dose strength and pack size
• Patient MMSE score (if recorded)
• Documentation of adverse events
• Changes in time requirements for nursing
• Caregiver:
- Health status (physical, stress situation, depression)
- Opinion and attitude towards AD
- Expectations regarding the effectiveness of Exelon® patch
- Physical health (mood, status of treatment EXUBAD v 1.0 observation plan including
Amendment 1 11/06/2013 Page 13 medical interventions)
- Psychotropic medication
8.4.4 End of the observation
In accordance with clinical practice, the final observation was conducted approximately 12
months after initiation of treatment with the Exelon® patch.
The following observation parameters were collected:
• Date of observation
• Persistence
• Prescription of Exelon® patch: dose strength and pack size
• Patient MMSE score (if recorded)

Novartis Confidential 20 Non-interventional study report Exelon
® patch/ CENA713DDE25
• Documentation of adverse events
• Changes in time requirements for nursing
• Caregiver:
- Health status (physical, stress situation, depression)
- View and attitude towards AD
- Expectations regarding the effectiveness of Exelon® patch
- Physical health (mood, treatment status and medical interventions)
- Psychotropic medication
8.4.5 Observation plan
Table 8.1 Observation plan
Only if recorded Observation
start*
Training 1 Training 2 1st
Follow-up
2nd
Follow-up
End of ob-
servation**
(Group with training)
Visits Baseline 4-10 weeks 3-6
months
4-6
months
8-10
months 12 months
Inclusion /
exclusion criteria x
Informed consent x
Information about the
caregiver (age, health
status, relationship to
the patient)
x
Training (only for the
group with training) x x
Information about
training and evaluation x x
Information about the
persistence (physician
and caregiver)
x (x) x
MMSE (if done) x x (x) x
Information about
caregivers’ knowledge
of the disease and
expectations regarding
therapy
x x x
Information about
caregivers’ burden
(health status, Mini-
Zarit and GDS)
x x x
Adverse events x x x x x x
* Screening and baseline could take place simultaneously
** Or premature study discontinuation

Novartis Confidential 21 Non-interventional study report Exelon
® patch/ CENA713DDE25
8.5 Data sources and measurement
Data were recorded on standardized case report forms (CRF). All data management activities
and statistical analyses were performed by Institute Dr. Schauerte (IDS), Munich. All CRFs
were tracked and entered (single data entry) into the study database. Subsequently,
implausible and missing data were checked according to the query plan. Queries concerning
discrepant data were generated and sent to the study sites for resolution.
All CRFs were checked for hidden adverse events. Reporting of (S)AEs was performed
according to the project pharmacovigilance contract and relevant standard operating
procedures (SOPs) of Novartis Pharma GmbH. Adverse events were coded according to
Medical Dictionary for Regulatory Activities (MedDRA) 17.1. After closure of the study
database, all adverse events were reconciled and the data validation process was performed
according to the validation plan.
The term “adverse event” (AE) describes any unfavorable and unintended sign (including an
abnormal laboratory finding), symptom, or disease temporally associated with the use of a
medicinal product, whether or not related to this drug. Further details concerning the
definition of special AEs can be found in the observational plan, Chapter 7. Additionally, in
the observational plan it was pointed out to the physician that a worsening of MMSE (in the
sense of a progression of the underlying disease) had to be reported as AE under specific
circumstances.
Generally, a distinction is made between non-serious and serious adverse events, the latter
required to be reported to the Novartis Pharmacovigilance department within 24 hours of
awareness. A serious adverse event is any event which:
• results in death
• is life-threatening
• requires inpatient hospitalization or prolongation of existing hospitalization
• results in persistent or significant disability or incapacity
• leads to a congenital anomaly or birth defect
• is medically significant (i.e. an important medical event which significantly affects the
patient, but does not meet any of the above criteria)
Overall, adverse events are distinguished into four types based on the distinction serious/non-
serious and the causal relationship to Exelon®:
• nsAEnr: non-serious adverse events not related (investigator does not suspect a causal
relationship with Exelon®)
• nsADR: non-serious adverse drug reactions (causality assured, probable, possible or not
assessable)
• SAEnr: serious adverse events not related (investigator does not suspect a causal
relationship with Exelon®)
• SADR: serious adverse drug reaction (causality assured, probable, possible or not
assessable)

Novartis Confidential 22 Non-interventional study report Exelon
® patch/ CENA713DDE25
In order to ensure the safety of every patient treated with Exelon®, every pregnancy had to be
reported to the Novartis Pharmacovigilance department within 24 hours of awareness. The
pregnancy had to be documented on a separate pregnancy form (Post Marketing Surveillance
Pregnancy Form) in English and had to be reported by the treating physician directly to the
Pharmacovigilance of Novartis Pharma GmbH.
8.6 Bias
N/A
8.7 Study size
Data were to be collected from up to 350 patients at 70 study sites. 206 patients were actually
included at 41 sites. The participating investigators were neurologists, psychiatrists,
geriatricians, general practitioners and general practitioners specializing in geriatrics.
In accordance with the non-interventional character of this study, the group of patients treated
with Exelon® patch and with trained caregivers were recruited at study sites where training
was performed as a routine practice. Overall, 15 sites conducting training participated in this
study versus 26 sites not performing training.
8.8 Monitoring
Source Data Verification was performed at a total of 6 sites (3 per study arm) to check if all
information on the CRFs was consistent with and traceable to the source documents. Full
verification of the following was required: presence of informed consent, adherence to the
inclusion/ exclusion criteria, demographic data, documentation of SAEs, and the recording of
data required for the analyses of all primary and safety variables. For further details, please
refer to the Monitoring Plan.
8.9 Data transformation
N/A
8.10 Statistical methods
All variables were analyzed by descriptive statistical methods. The number of data available
as well as missing data, mean, standard deviation, minimum, quartiles, median and maximum
were calculated for metric data. Frequency tables were generated for categorical data.
Statistical analyses were primarily of an explorative and descriptive nature.
The statistical evaluation was performed using the SAS® software package release 9.2.

Novartis Confidential 23 Non-interventional study report Exelon
® patch/ CENA713DDE25
Methods used to examine subgroups and interactions
N/A
Missing data
The handling of missing values and discontinuations of therapy were described and justified
in the statistical analysis plan.
Sensitivity analyses
N/A
Any amendment to the plan of data analysis included in the study protocol, with a
rationale for the change
N/A
8.11 Quality control
Details of patient validity, data consistency checks and permissible data modifications are
described in the Data Management Plan.
9 Results
A total of 206 patients were enrolled at 41 sites in Germany in this non-interventional study
which was conducted between 15 April 2013 and 21 November 2014.
9.1 Participants
All parameters described in this section are based on the efficacy population (n=160). Of
these, 119 (74.4 %) patients were in the cohort without trained caregivers vs. 41 patients
(25.6 %) in the cohort with trained caregivers. The reason for this small number of caregivers
with training was that there haven`t been so many sites who performed this training during
their routine clinical practice. Due to this imbalance in numbers, the results of the two groups
have to be interpreted with caution.

Novartis Confidential 24 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.1 Population “with/ without training”
Training “Demenz Aktiv Begegnen” N (%)
Total 160 (100.0)
No 119 (74.4)
Yes 41 (25.6)
Source: Table 1/2; Table compendium
9.2 Descriptive data
9.2.1 Demography
Demographic data are summarized in Table 9-2 to Table 9-4.
Overall, more female (56.9 %) than male patients (41.3 %) were included in this non-
interventional study. In the patient group “with training” nearly two-thirds (65.9 %) were
female compared to 31.7 % male patients, whereas the proportion in the stratification group
“without training” was more balanced (female: 53.8 % vs. male: 44.5 %).
The mean age ± standard deviation (SD) of all patients was 77.5 ± 6.7 years. The average age
of patients in the trained caregivers group was 79 ± 5.6 years and without training 77 ± 6.9
years. The majority of all patients (60.0 %) were between 75 - 85 years.
Table 9.2 Sex, “with/ without training”
Sex
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 3 (1.9) 2 (1.7) 1 (2.4)
Male 66 (41.3) 53 (44.5) 13 (31.7)
Female 91 (56.9) 64 (53.8) 27 (65.9)
Source: Table 2.1/3; Table compendium
Table 9.3 Age (quantitative analysis), “with/ without training”
Age [years]
Training
Total No Yes
n = 160 n = 119 n = 41
Mean 77.5 77.0 79.0
SD 6.7 6.9 5.6
Median 77.0 77.0 79.0
Range 48.0 - 96.0 48.0 - 96.0 69.0 - 92.0
Source: Table 2.1/1; Table compendium

Novartis Confidential 25 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.4 Age in decades, “with/ without training”
Age [years]
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 1 (0.6) 1 (0.8) 0 (-)
< 65 3 (1.9) 3 (2.5) 0 (-)
≥ 65 - < 75 42 (26.3) 35 (29.4) 7 (17.1)
≥ 75 - < 85 96 (60.0) 69 (58.0) 27 (65.9)
≥ 85 18 (11.3) 11 (9.2) 7 (17.1)
Source: Table 2.1/2; Table compendium
9.2.2 Living Conditions
With respect to living conditions, the majority of patients (71.3 %) lived primarily with their
family members. This proportion was minimally higher in the trained caregivers’ cohort
(73.2 %) compared to the non-trained cohort (70.6 %). Less than one-fifth of the patients with
a trained caregiver (17.1 %) lived alone, as did slightly more patients in the non-trained cohort
(23.5 %).
Table 9.5 Living conditions, “with/ without training”
Living condition
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 0 (-) 0 (-) 0 (-)
Solitary 35 (21.9) 28 (23.5) 7 (17.1)
With family 114 (71.3) 84 (70.6) 30 (73.2)
Nursing home 9 (5.6) 6 (5.0) 3 (7.3)
Other 2 (1.3) 1 (0.8) 1 (2.4)
Unknown 0 (-) 0 (-) 0 (-)
Source: Table 2.1/5; Table compendium
Concerning patients’ relation to their caregivers, the majority of patients were cared for by
their spouses (55.6 %; n=89/160). More than half of the patients with untrained caregivers
were cared for by their spouses (58.8 %; n=70/119) and less than one-fifth by other untrained
relatives (18.5 %; n=22/119). However, in the group with training over two-fifths of the
spouses (46.3 %; n=19/41) and other relatives (41.5 %; n=17/41) were trained. For further
details, please refer to Table 9.6.

Novartis Confidential 26 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.6 Patient´s relation to his attendant, “with/ without training”
Patient’s relation to his attendant
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 0 (-) 0 (-) 0 (-)
No attendant 17 (10.6) 15 (12.6) 2 (4.9)
Spouse 89 (55.6) 70 (58.8) 19 (46.3)
Other relative 39 (24.4) 22 (18.5) 17 (41.5)
Paid caregiver 0 (-) 0 (-) 0 (-)
Nursing service 2 (1.3) 2 (1.7) 0 (-)
Other 2 (1.3) 2 (1.7) 0 (-)
Unknown 0 (-) 0 (-) 0 (-)
No regular caregiver / partner / spouse 1 (0.6) 1 (0.8) 0 (-)
No regular caregiver / other 2 (1.3) 2 (1.7) 0 (-)
Partner / spouse / other relative 3 (1.9) 2 (1.7) 1 (2.4)
Partner / spouse / nursing service 1 (0.6) 1 (0.8) 0 (-)
Partner / spouse / other 1 (0.6) 1 (0.8) 0 (-)
Other relative / nursing service 2 (1.3) 0 (-) 2 (4.9)
Partner / spouse / other relative / nursing
service 1 (0.6) 1 (0.8) 0 (-)
Source: Table 2.1/7; Table compendium
Physicians were asked to assess the impairment of the caregiver’s ability to take care of the
patient. In the opinion of the physicians more than half of the caregivers were fully able to
take care of their AD patients (n=91/160; 56.9 %). The estimated ability of the trained cohort
(n=37/41; 90.2 %) was twice as high as the non-trained cohort (n=54/119; 45.4 %). Results of
further stratified analyses can be found in Table 4/6 in the Table compendium.
Table 9.7 Impairment of the caregiver, “with/ without training”
Impairment of the caregiver
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 12 (7.5) 12 (10.1) 0 (-)
Not at all 91 (56.9) 54 (45.4) 37 (90.2)
Slightly 41 (25.6) 37 (31.1) 4 (9.8)
Strongly 9 (5.6) 9 (7.6) 0 (-)
Unknown 7 (4.4) 7 (5.9) 0 (-)
Source: Table 2.1/9; Table compendium

Novartis Confidential 27 Non-interventional study report Exelon
® patch/ CENA713DDE25
9.2.3 Diagnosis
Table 9.8 Alzheimer´s dementia known for [months], “with/ without training”
Alzheimer´s dementia known for [months]
Training
Total No Yes
n = 160 n = 119 n = 41
Mean 10.8 11.3 9.3
SD 17.7 18.4 15.7
Median 3.5 4.0 3.0
Range 0 - 106.0 0 - 106.0 0 - 62.0
Source: Table 2.2/1; Table compendium
The mean duration of AD since its first diagnosis was 10.8 ± 17.7 months. When comparing
both groups, the average duration of AD was slightly longer in the group without training
(11.3 ± 18.4 months) compared to the cohort with trained caregivers (9.3 ± 15.7 months).
According to ICD-10 (according to World Health Organization, WHO), diagnoses were
classified as follows: G.30.0 – Alzheimer’s dementia with early onset (<65 years), G.30.1 –
Alzheimer’s dementia with late onset (≥65 years), G30.9 – Alzheimer’s dementia,
unspecified, and “other” disease. The vast majority of all observed patients as well as the
great majority of patients within the stratified cohorts (trained caregivers cohort 63.4 %; non-
trained cohort 59.7 %) were affected by late-onset Alzheimer’s dementia. For further details,
please refer to the following table as well as Table 2.2/3 in the Table compendium.
Table 9.9 Diagnosis by ICD 10, “with/ without training”
Diagnosis by ICD 10
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 1 (0.6) 1 (0.8) 0 (-)
G30.0 Alzheimer´s dementia with early onset 2 (1.3) 2 (1.7) 0 (-)
G30.1 Alzheimer´s dementia with late onset 97 (60.6) 71 (59.7) 26 (63.4)
G30.9 Alzheimer´s dementia, unspecified 24 (15.0) 16 (13.4) 8 (19.5)
Other 36 (22.5) 29 (24.4) 7 (17.1)
Source: Table 2.2/2; Table compendium
9.2.4 Pretreatment of dementia
Of the 160 patients enrolled, more than two-thirds (68.8 %; n=110/160) were treatment naïve
prior to enrolment compared to 28.8 % (n=46/160) pretreated patients. According to the
physicians’ documentation, a much larger proportion of patients (72.3 %; n=86/119) was
treatment naive in the cohort with untrained caregivers compared to 58.5 % (n=24/41) patients
in the trained cohort. Conversely, more patients (36.6 %; n=15/41) in the group with trained
caregivers had already received an anti-dementive pretreatment compared to 26.1 %

Novartis Confidential 28 Non-interventional study report Exelon
® patch/ CENA713DDE25
(n=31/119) in the untrained group. Of those patients with previous treatment (n=46), the most
frequently prescribed treatments were Donepezil (n=11; 23.9 %), Axura® (n=9; 19.6 %) and
Exelon®
capsules (n=5; 10.9 %). The most frequently used application form was oral (89.1 %;
n=41/46). For further details, please refer to Table 9-10 to 9-12.
Table 9.10 Pretreatment yes/ no, “with/ without training”
Pretreatment
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Yes 46 (28.8) 31 (26.1) 15 (36.6)
No 110 (68.8) 86 (72.3) 24 (58.5)
Unknown 4 (2.5) 2 (1.7) 2 (4.9)
Source: Table 2.3/1; Table compendium
Table 9.11 Last pretreatment medication, “with/ without training”
Last pretreatment medication
Training
Total No Yes
N (%) N (%) N (%)
Total* 46 (100.0) 31 (100.0) 15 (100.0)
Missing 6 (13.0) 4 (12.9) 2 (13.3)
Exelon® capsule 5 (10.9) 5 (16.1) 0 (-)
Rivastigmine (generic drug) 2 (4.3) 1 (3.2) 1 (6.7)
Aricept® 4 (8.7) 3 (9.7) 1 (6.7)
Donepezil (generic drug) 11 (23.9) 4 (12.9) 7 (46.7)
Reminyl® 1 (2.2) 1 (3.2) 0 (-)
Galantamine (generic drug) 1 (2.2) 1 (3.2) 0 (-)
Axura® 9 (19.6) 8 (25.8) 1 (6.7)
Ebixa® 1 (2.2) 1 (3.2) 0 (-)
Memantine (generic drug) 1 (2.2) 0 (-) 1 (6.7)
Other 5 (10.9) 3 (9.7) 2 (13.3)
*Only pretreated patients; Multiple answers possible
Source: Table 2.3/2; Table compendium
Novartis Confidential 29 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.12 Application form of medication, “with/ without training”
Application form of medication
Training
Total No Yes
N (%) N (%) N (%)
Total* 46 (100.0) 31 (100.0) 15 (100.0)
Missing 2 (4.3) 1 (3.2) 1 (6.7)
Oral 41 (89.1) 28 (90.3) 13 (86.7)
Transdermal 3 (6.5) 2 (6.5) 1 (6.7)
Other 0 (-) 0 (-) 0 (-)
*Only pretreated patients
Source: Table 2.3/4; Table compendium
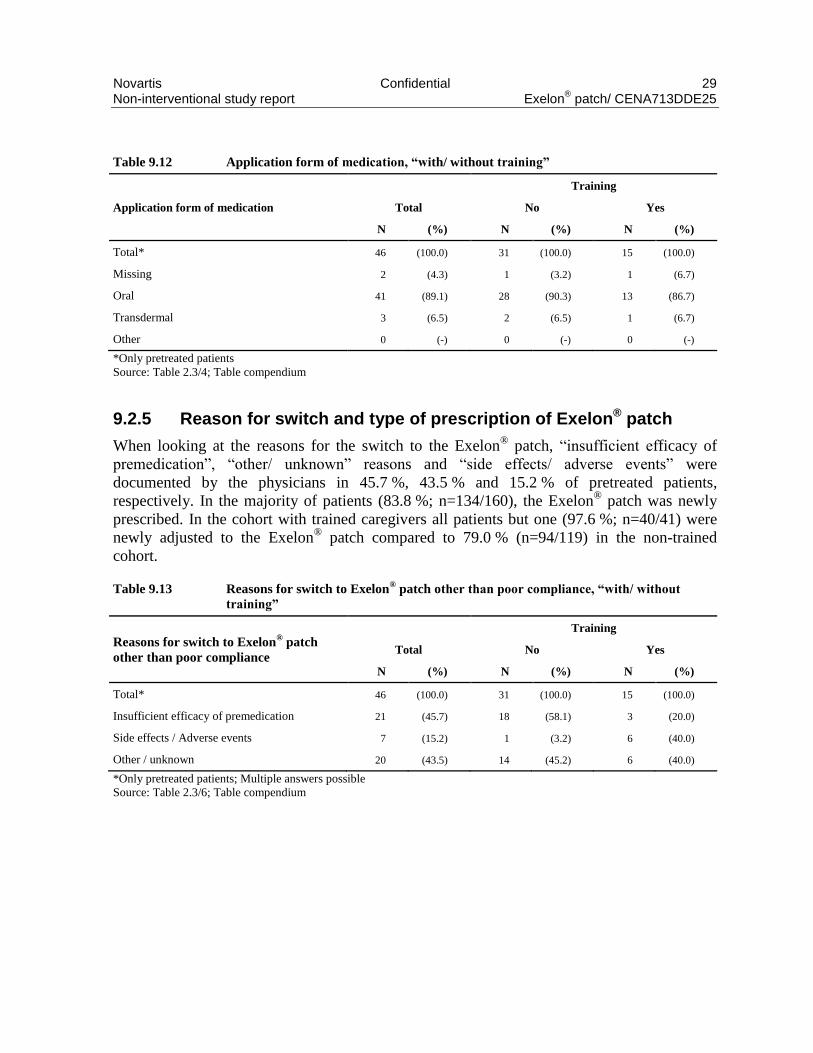
9.2.5 Reason for switch and type of prescription of Exelon® patch
When looking at the reasons for the switch to the Exelon® patch, “insufficient efficacy of
premedication”, “other/ unknown” reasons and “side effects/ adverse events” were
documented by the physicians in 45.7 %, 43.5 % and 15.2 % of pretreated patients,
respectively. In the majority of patients (83.8 %; n=134/160), the Exelon® patch was newly
prescribed. In the cohort with trained caregivers all patients but one (97.6 %; n=40/41) were
newly adjusted to the Exelon® patch compared to 79.0 % (n=94/119) in the non-trained
cohort.
Table 9.13 Reasons for switch to Exelon® patch other than poor compliance, “with/ without
training”
Reasons for switch to Exelon® patch
other than poor compliance
Training
Total No Yes
N (%) N (%) N (%)
Total* 46 (100.0) 31 (100.0) 15 (100.0)
Insufficient efficacy of premedication 21 (45.7) 18 (58.1) 3 (20.0)
Side effects / Adverse events 7 (15.2) 1 (3.2) 6 (40.0)
Other / unknown 20 (43.5) 14 (45.2) 6 (40.0)
*Only pretreated patients; Multiple answers possible
Source: Table 2.3/6; Table compendium

Novartis Confidential 30 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.14 Type of prescription of Exelon
® patch, “with/ without training”
Type of prescription
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 3 (1.9) 3 (2.5) 0 (-)
First prescription 134 (83.8) 94 (79.0) 40 (97.6)
Follow-up prescription 23 (14.4) 22 (18.5) 1 (2.4)
Source: Table 2.3/7; Table compendium
9.2.6 Exelon® patch daily dose
Exelon® patch therapy was documented at the start of the observation and at each single
follow-up visit. The following dosage forms were predefined within the case report form:
Exelon®
patch 4.6mg/24 hours (5cm2 size containing 9mg rivastigmine), Exelon
® patch
9.5mg/24 hours (10cm2 size containing 18mg rivastigmine) and Exelon
® patch 13.3mg/24
hours (15cm2 size containing 27mg rivastigmine).
According to the Summary of Product Characteristics, the treatment is initiated with 4.6mg/24
hours Exelon® patch. After a minimum of four weeks of treatment and if well-tolerated, the
dose of the patch should be increased to the recommended daily effective dose of 9.5mg/24
hours as long as this dose is beneficial. After a minimum of six months of therapy with a dose
of 9.5mg/24 hours and a significant cognitive impairment or functional decline, the dose
could be increased to 13.3mg/24 hours.
Again, of note is that the total numbers in the stratification cohorts (trained caregivers; n=41
vs. non-trained; n=119) differ by one-third.
At baseline, the vast majority of patients (83.8 %; n=134/160) was prescribed 4.6mg/24 hours
Exelon® patches. Looking at the subgroup-specific results, patients with a trained caregiver
were adjusted to the initial dose of 4.6mg/24 hours in 97.6 % of cases (n=40/41) compared to
79.0 % (n=94/119) in the non-trained cohort. For further details, please refer to Table 9.15.
At the first follow-up visit after 4-5 months, half of all observed patients were treated with the
9.5mg Exelon® patch. This proportion remained nearly constant in the further course of the
observation. Regarding the Exelon® patch 13.3mg/24 hours, about one quarter of patients
received this strength at the second (2nd FU: n=28) and third follow-up visit (3rd FU: n=30).
As a result of dose adjustments at the last individually documented visit, 16.3 % of patients
received the 4.6mg/24 hours Exelon® patch (n=26/160) whereas 32.5 % (n=52/160) of
patients were prescribed the 9.5mg/24 hours Exelon® patch and 20.6 % (33/160) the
13.3mg/24 hours Exelon® patch. Comparing the two different subgroups at the last
documented visit, the proportions were distributed as follows in the cohorts without training
vs. with training: 12.6 % (n=15/119) vs. 26.8 % (n=11/41) of patients were treated with
4.6mg/24 hours Exelon®
patch. 37.0 % (n=44/119)/ 19.5 % (n=8/41) received the
recommended maintenance strength of 9.5mg/24 hours and 20.2 % (24/119)/ 22.0 % (n=9/41)

Novartis Confidential 31 Non-interventional study report Exelon
® patch/ CENA713DDE25
of patients were administered the maximum dose of 13.3mg/24 hours. Results of further
stratified analyses can be found in Table 2.3/8 to 2.3/9 and 4/3 in the Table compendium.
Table 9.15 Exelon® patch daily dose
Exelon® patch daily dose At initial visit 1st FU visit 2nd FU visit 3rd FU visit
Last
documented
visit*
N (%) N (%) N (%) N (%) N (%)
Total
Total 160 (100.0) 157 (100.0) 123 (100.0) 109 (100.0) 160 (100.0)
Missing 12 (7.5) 9 (5.7) 5 (4.1) 2 (1.8) 2 (1.3)
4.6mg Exelon® 134 (83.8) 57 (36.3) 30 (24.4) 29 (26.6) 26 (16.3)
9.5mg Exelon® 11 (6.9) 78 (49.7) 60 (48.8) 48 (44.0) 52 (32.5)
13.3mg Exelon® 3 (1.9) 13 (8.3) 28 (22.8) 30 (27.5) 33 (20.6)
Discontinuation 47 (29.4)
Without training
Total 119 (100.0) 118 (100.0) 97 (100.0) 81 (100.0) 119 (100.0)
Missing 12 (10.1) 9 (7.6) 5 (5.2) 2 (2.5) 2 (1.7)
4.6mg Exelon® 94 (79.0) 34 (28.8) 16 (16.5) 16 (19.8) 15 (12.6)
9.5mg Exelon® 11 (9.2) 68 (57.6) 52 (53.6) 40 (49.4) 44 (37.0)
13.3mg Exelon® 2 (1.7) 7 (5.9) 24 (24.7) 23 (28.4) 24 (20.2)
Discontinuation 34 (28.6)
With training
Total 41 (100.0) 39 (100.0) 26 (100.0) 28 (100.0) 41 (100.0)
4.6mg Exelon® 40 (97.6) 23 (59.0) 14 (53.8) 13 (46.4) 11 (26.8)
9.5mg Exelon® 0 (-) 10 (25.6) 8 (30.8) 8 (28.6) 8 (19.5)
13.3mg Exelon® 1 (2.4) 6 (15.4) 4 (15.4) 7 (25.0) 9 (22.0)
Discontinuation 13 (31.7)
*Last documented visit: 1st FU, 2nd FU or 3rd FU (end of observation)
Source: Table 4/2; Table compendium
9.2.7 Evaluation of the training “Demenz Aktiv Begegnen”
To determine the impact of training based on “Demenz aktiv begegnen” on the burden of
caregivers, 41 caregivers participated in the respective trainings after approximately 4-10
weeks (Training 1) and 3-6 months (Training 2). Physicians documented training dates as well
as questions concerning basic training information and an assessment of the respective
training. Questionnaires were completed immediately after each training.
Physicians were asked to complete the questionnaires after each training. The questionnaire
regarding basic training information contained the following questions:
• Did any adverse events occur since the last visit?
• How long did the current training take?

Novartis Confidential 32 Non-interventional study report Exelon
® patch/ CENA713DDE25
• How many participants attended in total? (number of patients/ number of caregivers)
• Which contents were covered during training?
More than half of the participating caregivers indicated that both trainings (Training 1,
56.1 %; Training 2, 70.7 %) took up to one hour. Only 39.0 % of the caregivers participating
in Training 1 and 22.0 % in Training 2 reported that the duration was between one to two
hours without a break.
Table 9.16 How long did the current event take? Only for population with training
How long did the current event take?
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
N (%) N (%)
Total 41 (100.0) 41 (100.0)
Missing 2 (4.9) 3 (7.3)
Up to one hour 23 (56.1) 29 (70.7)
Between one and two hours (without a break) 16 (39.0) 9 (22.0)
Source: Table 3/1; Table compendium
According to the physicians, almost half of the caregivers attended Training 1 alone (48.8 %)
whereas two-thirds attended Training 2 alone (65.9 %). The remaining caregivers participated
in groups of 2-12 participants in Training 1 (46.3 %, n=19) and Training 2 (26.8 %; n=11).
Over two-fifths of patients also attended Training 1 (41.5 %) alone versus approximately two-
thirds who attended Training 2 (68.3 %) alone. The remaining patients attended within a
group of 2-6 participants in Training 1 (29.3 %, n=12) and Training 2 (7.3 %, n=3). Further
details are presented in the following tables.

Novartis Confidential 33 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.17 How many patients participated in total?
How many patients participated in total?
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
N (%) N (%)
Total 41 (100.0) 41 (100.0)
Missing 2 (4.9) 3 (7.3)
0 10 (24.4) 7 (17.1)
1 17 (41.5) 28 (68.3)
2 1 (2.4) 2 (4.9)
3 8 (19.5) 1 (2.4)
4 1 (2.4) 0 (-)
5 1 (2.4) 0 (-)
6 1 (2.4) 0 (-)
Source: Table 3/2; Table compendium
Table 9.18 How many caregivers participated in total?
How many caregivers participated in total?
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
N (%) N (%)
Total 41 (100.0) 41 (100.0)
Missing 2 (4.9) 3 (7.3)
1 20 (48.8) 27 (65.9)
2 3 (7.3) 3 (7.3)
3 1 (2.4) 1 (2.4)
4 0 (-) 2 (4.9)
5 6 (14.6) 5 (12.2)
7 7 (17.1) 0 (-)
10 1 (2.4) 0 (-)
12 1 (2.4) 0 (-)
Source: Table 3/3; Table compendium
Furthermore, the patients’ caregivers were asked about the topics that were covered during the
trainings. In the following, the answers to these questions are summarized in Table 9-19 – 9-
21. The main focus of both trainings was the “treatment of dementia” (Training 1: 95.1 % vs.
Training 2: 80.5 %) and the topic “dementia in general” (Training 1: 82.9 % and Training 2:
46.3 %). Another important focus of Training 2 (68.3 %) and to a lesser extent of Training 1
(51.2 %) was the subject “everyday life with dementia patients”. While the focus of
“treatment of dementia” was placed on “drug therapy” (Training 1: 61.5 % and Training 2:
45.5 %), the target subject in “everyday life with dementia patients” was a discussion of
“behavior and handling” (Training 1: 61.9 % and Training 2: 82.1 %). For the complete
analysis of other training contents, please refer to Table 3/7 in the Table compendium.

Novartis Confidential 34 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.19 Which contents were covered during training?
Which contents were covered during training?
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
N* (%) N* (%)
Total 41 (100.0) 41 (100.0)
Missing 2 (4.9) 3 (7.3)
Dementia in general 34 (82.9) 19 (46.3)
Treatment of dementia 39 (95.1) 33 (80.5)
Everyday life with dementia patients 21 (51.2) 28 (68.3)
Rights and social affairs 14 (34.1) 8 (19.5)
Others 3 (7.3) 7 (17.1)
*Multiple answers possible
Source: Table 3/4; Table compendium
Table 9.20 Content – Treatment of dementia
Treatment of dementia
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
N* (%) N* (%)
Total 39 (100.0) 33 (100.0)
Missing 8 (20.5) 4 (12.1)
Non-drug therapy 9 (23.1) 5 (15.2)
Drug therapy 24 (61.5) 15 (45.5)
Handling the Exelon® patch 23 (59.0) 23 (69.7)
*Multiple answers possible
Source: Table 3/5; Table compendium
Table 9.21 Content – Everyday life with dementia patients
Everyday life with dementia patients
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
N* (%) N* (%)
Total 21 (100.0) 28 (100.0)
Missing 7 (33.3) 4 (14.3)
Behavior and handling 13 (61.9) 23 (82.1)
Safety in the household 9 (42.9) 11 (39.3)
*Multiple answers possible
Source: Table 3/6; Table compendium
The second part of the evaluation questionnaire concerned the usefulness and atmosphere of
training.
Both evaluations were documented on a visual analogue scale ranging from 0 = “not helpful”
to 10 = “extremely helpful” for the question “Were the contents of training helpful for you?”.
The average evaluation of this question was 8.5 ± 1.3 for Training 1 and 8.7 ± 1.2 for in
Training 2. The training atmosphere (ranging from 0 = unpleasant / tense to 10 = very

Novartis Confidential 35 Non-interventional study report Exelon
® patch/ CENA713DDE25
comfortable / relaxed) was similarly well-rated for both trainings (Training 1: 9.3 ± 0.8;
Training 2: 9.2 ± 0.8).
Table 9.22 Evaluation: Were the contents of training helpful for you?
Were the contents of the training helpful for you?
0=not helpful, 10=extremely helpful
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
n = 24 n = 19
Mean 8.5 8.7
SD 1.3 1.2
Median 8.5 9.0
Range 6.0 – 10.0 6.0 – 10.0
Source: Table 3/8; Table compendium
Table 9.23 Evaluation: How was the atmosphere in training?
How was the atmosphere in training for you?
0=unpleasant/tense, 10=very comfortable/relaxed
Training 1
(after 4-10 weeks)
Training 2
(after 3-6 months)
n = 24 n = 18
Mean 9.3 9.2
SD 0.8 0.8
Median 9.0 9.0
Range 8.0 – 10.0 8.0 – 10.0
Source: Table 3/9; Table compendium
In addition, the participants were asked to answer three general questions regarding the
contents in the trainings:
• What did you particularly like?
• What could be improved?
• What information would you still need?
For details concerning these questions, please refer to Table 3/10 – 3/12 in the Table
compendium.
9.2.8 Follow-up visits
Physicians documented one initial visit (baseline visit), up to two follow-up visits per patient
(1st FU: after 4-6 months; 2nd FU: after 8-10 months) and one final visit at the end of the
observation after approximately one year or in case of premature study termination. The mean
duration from the initial to the first follow-up visit was 4.6 ± 1.7 months for all observed
patients. Looking at the mean duration from the first to the second follow-up visit, this was
documented as 4.0 ± 1.7 months and from the second to the third follow-up visit as 3.4 ± 1.2
months. In the trained caregivers cohort, the longest mean observation duration (5.8 months ±
1.8 months) was between the initial and the first follow-up visit whereas the shortest
observation time was between the second and the third follow-up visit (3.2 months ± 1.0

Novartis Confidential 36 Non-interventional study report Exelon
® patch/ CENA713DDE25
months). The average intervals between visits in the non-trained cohort were similar to those
documented for the total study population. Further details can be found in Table 9.24.
Table 9.24 Time interval between visits
Time interval between visits [months] Initial visit – 1st FU 1st FU – 2nd FU 2nd FU – 3rd FU
Total n = 160 n = 125 n = 104
Mean 4.6 4.0 3.4
SD 1.7 1.7 1.2
Median 4.6 3.5 3.3
Range 0.9 – 11.2 0.2 – 10.3 0.4 – 9.2
Without training n = 119 n = 96 n = 81
Mean 4.2 4.1 3.4
SD 1.5 1.8 1.3
Median 4.4 3.7 3.4
Range 0.9 – 9.8 0.2 – 10.3 0.4 – 9.2
With training n = 41 n = 29 n = 23
Mean 5.8 3.4 3.2
SD 1.8 0.9 1.0
Median 5.6 3.2 3.2
Range 2.4 – 11.2 1.8 – 6.2 1.7 – 6.0
Source: Table 4/1; Table compendium
9.2.9 Mini-Mental State Examination
The severity of dementia was assessed by the Mini-Mental State Examination (MMSE) which
is a widely used screening instrument for Alzheimer’s disease. It covers various cognitive
functions including memory function, attention, language, visual-spatial skills, ability to
follow simple commands, language and orientation by assessing simple questions and
problems in a number of areas: the time and place of the test, repeating and recall of a list of
words, arithmetic such as the serial sevens, language use and comprehension, and basic motor
skills. The maximum MMSE score is 30 points. Any score greater than or equal to 27 points
(out of 30) is effectively normal (intact). Below this, scores can indicate severe (<10 points),
moderate (10-19 points) or mild (20-26 points) impairment.
At baseline and at each single follow-up visit, physicians were asked to document the result of
the MMSE for their patients, if it was performed in routine clinical practice. The average sum
score of MMSE for the total study population was 20.5 ± 4.2 points at the start of the
observation compared to 19.9 ± 4.5 points at the last individual follow-up visit. The mean
MMSE score decreased slightly in the course of therapy (see Table 9.25). In the stratification
cohort with trained caregivers, the lowest average MMSE score (16.9 ± 4.6 points) was
observed at the second follow-up visit whereas the mean MMSE score was always >20 points

Novartis Confidential 37 Non-interventional study report Exelon
® patch/ CENA713DDE25
in the cohort with untrained caregivers. For further details, please refer to Table 9.25 and
Table 4/4 in the Table compendium.
Table 9.25 Mini-Mental State Examination (MMSE) per visit, “with/ without training”
Mini-Mental State
Examination total
score
Initial visit 1st FU 2nd FU 3rd FU Last documented
visit*
Total n = 133 n = 108 n = 70 n = 72 n = 94
Mean 20.5 20.1 19.8 19.9 19.9
SD 4.2 4.7 4.7 4.6 4.5
Median 21.0 20.0 20.0 20.0 20.0
Range 10 – 28 4 – 30 8 – 30 5 – 30 5 – 30
Without training n = 98 n = 79 n = 56 n = 54 n = 71
Mean 20.7 20.3 20.5 20.2 20.2
SD 3.9 4.5 4.4 4.0 4.1
Median 21.0 20.0 20.0 20.0 20.0
Range 10 – 28 5 – 30 8 – 30 12 – 30 10 – 30
With training n = 35 n = 29 n = 14 n = 18 n = 23
Mean 19.9 19.7 16.9 18.8 18.9
SD 4.7 5.2 4.6 6.0 5.3
Median 20.0 20.0 17.0 20.5 20.0
Range 11 – 27 4 – 27 9 – 24 5 – 27 5 – 27
* Last documented visit: 1.FU, 2.FU or 3.FU (end of the study)
Source: Table 4/4; Table compendium
Table 9.26 shows the mean decrease of MMSE. Regarding all observed patients, the mean
MMSE score decreased slightly from start of observation to last individual visit by 0.7 ± 3.1
points. The MMSE score in the small cohort with trained caregivers decreased from baseline
to last follow-up visit by 1.0 ± 3.1 points in average compared to 0.6 ± 3.1 points in the group
without trained caregiver. For more details please refer to Table 9-26.

Novartis Confidential 38 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.26 Change** of Mini-Mental State Examination total score, “with/ without training”
Change** of Mini-Mental State
Examination total score 1st FU 2nd FU 3rd FU
Last documented
visit*
Total n = 94 n = 68 n = 68 n = 87
Mean -0.2 -0.3 -0.8 -0.7
SD 2.5 2.7 3.2 3.1
Median 0.0 0.0 0.0 0.0
Range -8.0 – 6.0 -8.0 – 7.0 -10.0 – 7.0 -10.0 – 7.0
Without training n = 68 n = 54 n = 52 n = 66
Mean -0.1 0.1 -0.6 -0.6
SD 2.5 2.3 3.2 3.1
Median 0.0 0.0 0.0 0.0
Range -8.0 – 6.0 -5.0 – 7.0 -10.0 – 7.0 -10.0 - 7.0
With training n = 26 n = 14 n = 16 n = 21
Mean -0.2 -1.8 -1.6 -1.0
SD 2.5 3.4 3.3 3.1
Median 0.0 -1.0 -0.5 0.0
Range -8.0 – 3.0 -8.0 – 3.0 -9.0 – 3.0 -9.0 – 3.0
* Last documented visit: 1. FU, 2. FU or 3. FU (end of the study)
** MMST (visit) – MMST (baseline)
Source: Table 4/5; Table compendium
9.2.10 Discontinuation of the therapy with Exelon® patch
Premature discontinuation of Exelon® patch therapy was recorded for 29.4 % (n=47/160) of
all observed patients (31.7 % “with training” and 28.6 % “without training”; Table 5/1 in the
Compendium). Mean duration until discontinuation of therapy in total was 7.5 ± 4.3 months.
The average duration in the trained cohort was 8.7 ± 5.1 months and 6.8 ± 3.7 months in the
non-trained cohort. Reasons for premature discontinuation were “adverse events” and “patient
did not return” in 16 patients (10.0 %, respectively) and “insufficient efficacy” and “patient
died” in 2 patients (1.3 %, respectively). Other reasons were documented for 11 patients
(6.9 %). For further information as well as details of “other” reasons for premature
discontinuation, please refer to Table 5/1 to Table 5/4 in the Compendium.

Novartis Confidential 39 Non-interventional study report Exelon
® patch/ CENA713DDE25
9.2.11 General circumstances of caregivers
Demographic data are summarized in Table 9.27 and Table 9.28.
Overall, more female (57.5 %) than male caregivers (34.4 %) took part in this non-
interventional study. In the caregiver group “with training” nearly two-thirds (61.0 %) were
female compared to 39.0 % male caregivers, whereas the proportion in the stratification group
“without training” was 56.3 % female vs. 32.8 % male caregivers.
The majority of all caregivers (43.8 %) were over 70 years old. This was also the largest age
group of caregivers “with training” (39.0 %) and “without training” (45.4 %).
Table 9.27 Sex of caregiver, “with/ without training”
Sex
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 13 (8.1) 13 (10.9) 0 (-)
Male 55 (34.4) 39 (32.8) 16 (39.0)
Female 92 (57.5) 67 (56.3) 25 (61.0)
Source: Table 6.1/1; Table compendium
Table 9.28 Age of caregiver, “with/ without training”
Age [years]
Training
Total No Yes
N (%) N (%) N (%)
Total 160 (100.0) 119 (100.0) 41 (100.0)
Missing 14 (8.8) 14 (11.8) 0 (-)
< 35 3 (1.9) 3 (2.5) 0 (-)
≥ 35 - < 50 18 (11.3) 7 (5.9) 11 (26.8)
≥ 51 - < 60 28 (17.5) 22 (18.5) 6 (14.6)
≥ 61 - < 70 27 (16.9) 19 (16.0) 8 (19.5)
≥ 70 70 (43.8) 54 (45.4) 16 (39.0)
Source: Table 6.1/2; Table compendium
Over one-third (35.0 %) of all caregivers reported carrying full responsibility for
administering the prescribed medication to their patient (29.3 % “with training” and 37.0 %
“without training”; Table 6.1/3 in the Compendium). The vast majority (72.5 %) of caregivers
had never before taken care of a close relative over a period of several weeks (80.5 % “with
training” and 69.7 % “without training”; Table 6.1/4 in the Compendium).

Novartis Confidential 40 Non-interventional study report Exelon
® patch/ CENA713DDE25
The following table shows that at the initial visit over half (56.9 %) of all caregivers
considered the patient’s age to be the cause of AD (73.2 % “with training” and 51.3 %
“without training”) while only 47.5 % thought so at the last documented visit (51.2 % “with
training” and 46.2 % “without training”). A genetic disposition was initially thought to be the
cause by 22.5 % of caregivers (22.0 % “with training” and 22.7 % “without training”) and by
23.1 % of caregivers at the end of the study (14.6 % “with training” and 26.1 % “without
training”).
Table 9.29 What does caregiver think is the cause of patient’s AD?
Cause of AD At initial visit 1st FU visit 3rd FU visit
Last documented
visit*
N (%) N (%) N (%) N (%)
Total
Total 160 (100.0) 157 (100.0) 109 (100.0) 160 (100.0)
Missing 17 (10.6) 39 (24.8) 24 (22.0) 54 (33.8)
Age 91 (56.9) 80 (51.0) 63 (57.8) 76 (47.5)
Genetic disposition 36 (22.5) 42 (26.8) 30 (27.5) 37 (23.1)
Diet 4 (2.5) 3 (1.9) 5 (4.6) 5 (3.1)
Infection/ virus 2 (1.3) 1 (0.6) 1 (0.9) 1 (0.6)
Other 30 (18.8) 17 (10.8) 13 (11.9) 18 (11.3)
Without training
Total 119 (100.0) 118 (100.0) 81 (100.0) 119 (100.0)
Missing 16 (13.4) 31 (26.3) 18 (22.2) 41 (34.5)
Age 61 (51.3) 59 (50.0) 47 (58.0) 55 (46.2)
Genetic disposition 27 (22.7) 36 (30.5) 24 (29.6) 31 (26.1)
Diet 4 (3.4) 3 (2.5) 3 (3.7) 3 (2.5)
Infection/ virus 2 (1.7) 1 (0.8) 0 (-) 0 (-)
Other 22 (18.5) 10 (8.5) 6 (7.4) 10 (8.4)
With training
Total 41 (100.0) 39 (100.0) 28 (100.0) 41 (100.0)
Missing 1 (2.4) 8 (20.5) 6 (21.4) 13 (31.7)
Age 30 (73.2) 21 (53.8) 16 (57.1) 21 (51.2)
Genetic disposition 9 (22.0) 6 (15.4) 6 (21.4) 6 (14.6)
Diet 0 (-) 0 (-) 2 (7.1) 2 (4.9)
Infection/ virus 0 (-) 0 (-) 1 (3.6) 1 (2.4)
Other 8 (19.5) 7 (17.9) 7 (25.0) 8 (19.5)
*Last documented visit: 1st FU or 3rd FU (end of observation); Multiple responses possible
Source: Table 6.1/5; Table compendium
Caregivers opinion regarding the helpfulness of AD drug treatment was assessed on a visual
analogue scale ranging from 0 = “not helpful” to 10 = “extremely helpful”. At the initial visit,
all caregivers believed to an average extent of 6.3 ± 1.9 points in the helpfulness of AD
treatment with medication (6.3 ± 2.3 points “with training” and 6.3 ± 1.7 points “without

Novartis Confidential 41 Non-interventional study report Exelon
® patch/ CENA713DDE25
training”; Table 9.30). At the last documented visit the caregivers believed in the helpfulness
of medication to a lesser extent of 6.1 ± 2.1 points due to a decreased score among caregivers
with training (5.5 ± 2.0 points “with training” and 6.3 ± 2.1 points “without training”).
Table 9.30 To what extent in the opinion of the caregiver can treatment with medication help the AD
patient, “with/ without training”
Treatment with medication:
0= not helpful,
10= extremely helpful
Initial visit 1st FU 3rd FU Last documented
visit*
Total n = 137 n = 116 n = 80 n = 101
Mean 6.3 6.2 6.2 6.1
SD 1.9 2.1 2.0 2.1
Median 6.0 6.5 6.0 6.0
Range 1.0 – 10.0 0.0 – 10.0 0.0 – 10.0 0.0 – 10.0
Without training n = 96 n = 87 n = 59 n = 74
Mean 6.3 6.3 6.6 6.3
SD 1.7 2.0 1.9 2.1
Median 7.0 7.0 7.0 7.0
Range 2.0 – 10.0 0.0 – 10.0 2.0 – 10.0 0.0 – 10.0
With training n = 41 n = 29 n = 21 n = 27
Mean 6.3 5.8 5.1 5.5
SD 2.3 2.5 2.0 2.0
Median 6.0 6.0 5.0 6.0
Range 1.0 – 10.0 0.0 – 10.0 0.0 – 8.0 0.0 – 8.0
* Last documented visit: 1st FU or 3rd FU (end of the study)
Source: Table 6.1/6; Table compendium
As shown in the following table, the symptoms most common among the caregivers at the
initial visit were insomnia and fatigue (32.5%, respectively), followed by backache (26.3%),
brooding or repeated thoughts (25.0 %) and exhaustion (23.8 %). At the last documented visit,
the most common symptom was fatigue (24.4%), followed by insomnia and backache (22.5%,
respectively). Details of stratification by training status can be found in Table 6.1/7 in the
Compendium.

Novartis Confidential 42 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.31 Does the caregiver suffer from one of the following symptoms?
Symptom At initial visit 1st FU visit 2nd FU visit 3rd FU visit
Last
documented
visit*
N (%) N (%) N (%) N (%) N (%)
Total 160 (100.0) 157 (100.0) 123 (100.0) 109 (100.0) 160 (100.0)
Missing 44 (27.5) 65 (41.4) 54 (43.9) 45 (41.3) 73 (45.6)
Insomnia 52 (32.5) 37 (23.6) 24 (19.5) 25 (22.9) 36 (22.5)
Fatigue 52 (32.5) 40 (25.5) 34 (27.6) 29 (26.6) 39 (24.4)
Headache 22 (13.8) 18 (11.5) 21 (17.1) 20 (18.3) 25 (15.6)
Backache 42 (26.3) 32 (20.4) 30 (24.4) 26 (23.9) 36 (22.5)
Permanent sadness 16 (10.0) 8 (5.1) 4 (3.3) 3 (2.8) 6 (3.8)
Exhaustion 38 (23.8) 29 (18.5) 26 (21.1) 15 (13.8) 21 (13.1)
Loss of appetite and weight 4 (2.5) 6 (3.8) 3 (2.4) 2 (1.8) 3 (1.9)
Diminished ability to think
and concentrate 26 (16.3) 12 (7.6) 9 (7.3) 7 (6.4) 13 (8.1)
Loss of self-confidence 8 (5.0) 7 (4.5) 6 (4.9) 4 (3.7) 9 (5.6)
Brooding or repeated
thoughts 40 (25.0) 33 (21.0) 15 (12.2) 20 (18.3) 29 (18.1)
Difficulty to make decisions 16 (10.0) 6 (3.8) 5 (4.1) 4 (3.7) 9 (5.6)
*Last documented visit: 1st FU, 2nd FU or 3rd FU (end of observation); Multiple responses possible
Source: Table 6.1/7; Table compendium
Nearly 60 % of caregivers at the initial visit and nearly 40 % at the last documented visit
reported not taking any medication from the classes of drugs listed in Table 9.32. At the initial
visit caregivers most often took antidepressants and sleeping pills (10.6 % and 8.1 %,
respectively), which were also most often taken at the last documented visit (10.0 % and
9.4 %, respectively). Details of stratification by training status can be found in Table 6.1/8 in
the Compendium.
Table 9.32 Is the caregiver presently taking medication from one of the following classes of drugs?
Class At initial visit 1st FU visit 2nd FU visit 3rd FU visit
Last
documented
visit*
N (%) N (%) N (%) N (%) N (%)
Total 160 (100.0) 157 (100.0) 123 (100.0) 109 (100.0) 160 (100.0)
Missing 29 (18.1) 50 (31.8) 41 (33.3) 36 (33.0) 61 (38.1)
Antidepressants 17 (10.6) 11 (7.0) 12 (9.8) 12 (11.0) 16 (10.0)
Sedatives 6 (3.8) 7 (4.5) 6 (4.9) 6 (5.5) 6 (3.8)
Sleeping pills 13 (8.1) 12 (7.6) 9 (7.3) 11 (10.1) 15 (9.4)
Anxiolytics 1 (0.6) 0 (-) 0 (-) 0 (-) 0 (-)
Other neurological/
psychiatric medication 8 (5.0) 9 (5.7) 6 (4.9) 5 (4.6) 8 (5.0)
No, none 95 (59.4) 73 (46.5) 54 (43.9) 45 (41.3) 63 (39.4)
*Last documented visit: 1st FU, 2nd FU or 3rd FU (end of observation); Multiple responses possible
Source: Table 6.1/8; Table compendium

Novartis Confidential 43 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.33 summarizes the medical interventions on behalf of the caregiver in the last half
year before the start of the study and in the course of the study, stratified by training status. At
the initial visit, 12.5 % of caregivers had been hospitalized in the last half year, 5.6 % had
been on sick leave, and 2.5 % had been to rehabilitation. In the course of the study, a stay in
the hospital, rehabilitation and/or sick leave was needed at least once by 3.1 %, 1.9 % and
3.8 % of caregivers, respectively. Details of stratification by training status can be found in
Table 6.1/9 in the Compendium.
Table 9.33 Medical interventions on behalf of the caregiver
Training
Total No Yes
N (%) N (%) N (%)
In the last half year before study start
Total 160 (100.0) 119 (100.0) 41 (100.0)
Hospitalization 20 (12.5) 15 (12.6) 5 (12.2)
Rehabilitation treatment 4 (2.5) 3 (2.5) 1 (2.4)
Sick leave 9 (5.6) 6 (5.0) 3 (7.3)
In the course of the study
Total 160 (100.0) 119 (100.0) 41 (100.0)
Hospitalization 5 (3.1) 2 (1.7) 3 (7.3)
Rehabilitation treatment 3 (1.9) 2 (1.7) 1 (2.4)
Sick leave 6 (3.8) 5 (4.2) 1 (2.4)
Multiple responses possible
Source: Table 6.1/10; Table compendium
9.2.12 Mini-Zarit assessment of caregiver burden
The Mini-Zarit scale is used to assess the burden on caregivers of AD patients. The possible
answers to the following seven items are assigned points (“never” 1 point, “occasionally” 0.5
points, “more often” 0 points / total score range 0 to 7) and constitute the sum score. The
questionnaire was filled out by the caregiver at the initial visit and the first and third follow-up
visit (or end of observation). The following analyses are based on the total of available
questionnaires.
1. Difficulties in the family
In total, the most frequent answers of the caregivers were “never” (n=85/144, 59.0 %) at the
initial visit and “never” (n=67/112, 59.8 %) at the last documented visit. The percentage
among caregivers without training was slightly lower (53.4 % at initial visit and 57.0 % at the
last documented visit), while the trained caregivers more often reported never having
difficulties in the family (73.2 % at initial visit and 66.7 % at the last documented visit). In
both groups of caregivers the answers remained consistent in the course of the study.

Novartis Confidential 44 Non-interventional study report Exelon
® patch/ CENA713DDE25
2. Difficulties with friends, leisure time or job
The total number of caregivers most often responded with “never” (n=81/144, 56.3 %) at the
initial visit and “never” (n=67/112, 59.8 %) at the last documented visit. The percentage
among caregivers without training was somewhat lower (50.5 % at initial visit and 58.2 % at
the last documented visit), while the trained caregivers more often reported never having such
difficulties (70.7 % at initial visit and 63.6 % at the last documented visit).
3. Impact on health (physical and/or mental)
Most of all caregivers responded with “never” (n=60/144, 41.7 %) at the initial visit and
“occasionally” (n=50/112, 44.6 %) at the last documented visit. Caregivers without training
most frequently reported an occasional impact on their health (48.5 % at initial visit and
41.8% at the last documented visit), while the trained caregivers initially most often
responded with “never” (73.2 %) and most often with “occasionally” (51.5 %) at the last
documented visit.
4. Do you have the impression that you don’t recognize the patient anymore?
Caregivers most frequently responded with “never” (n=93/144, 64.6 %) at the initial visit and
“never” (n=65/112, 58.0 %) at the last documented visit. In particular, the percentage among
caregivers without training was somewhat lower (60.2 % at initial visit and 55.7 % at the last
documented visit), while the trained caregivers more often reported never having such an
impression (75.6 % at initial visit and 63.6 % at the last documented visit).
5. Are you worried about the patient’s future?
The answers most often provided by caregivers were “occasionally” (n=67/144, 46.5 %) at the
initial visit and “occasionally” (n=55/112, 49.1 %) at the last documented visit. The
percentage among caregivers without training was slightly higher (46.6 % at initial visit and
50.6 % at the last documented visit), while the trained caregivers slightly less often reported
such occasional worries (46.3 % at initial visit and 45.5 % at the last documented visit).
6. Would you like (more) support in caring for the patient?
The most frequent answers by caregivers overall were “occasionally” (n=68/144, 47.2 %) at
the initial visit and “occasionally” (n=54/112, 48.2 %) at the last documented visit. Caregivers
without training responded more often with “occasionally” (53.4 % at initial visit and 55.7 %
at the last documented visit), while the trained caregivers most often reported never wanting
more support (56.1 % at initial visit and 54.5 % at the last documented visit).
7. Do you feel burdened when caring for the patient?
Caregivers in total most often responded with “never” (n=59/144, 41.0 %) at the initial visit
and “occasionally” (n=54/112, 48.2 %) at the last documented visit. Caregivers without
training answered most often with “occasionally” (38.8 % at initial visit and 45.6 % at the last
documented visit), while the trained caregivers most frequently never felt burdened at the
initial visit (56.1 %) and most often felt occasionally burdened at the last documented visit
(54.5 %).
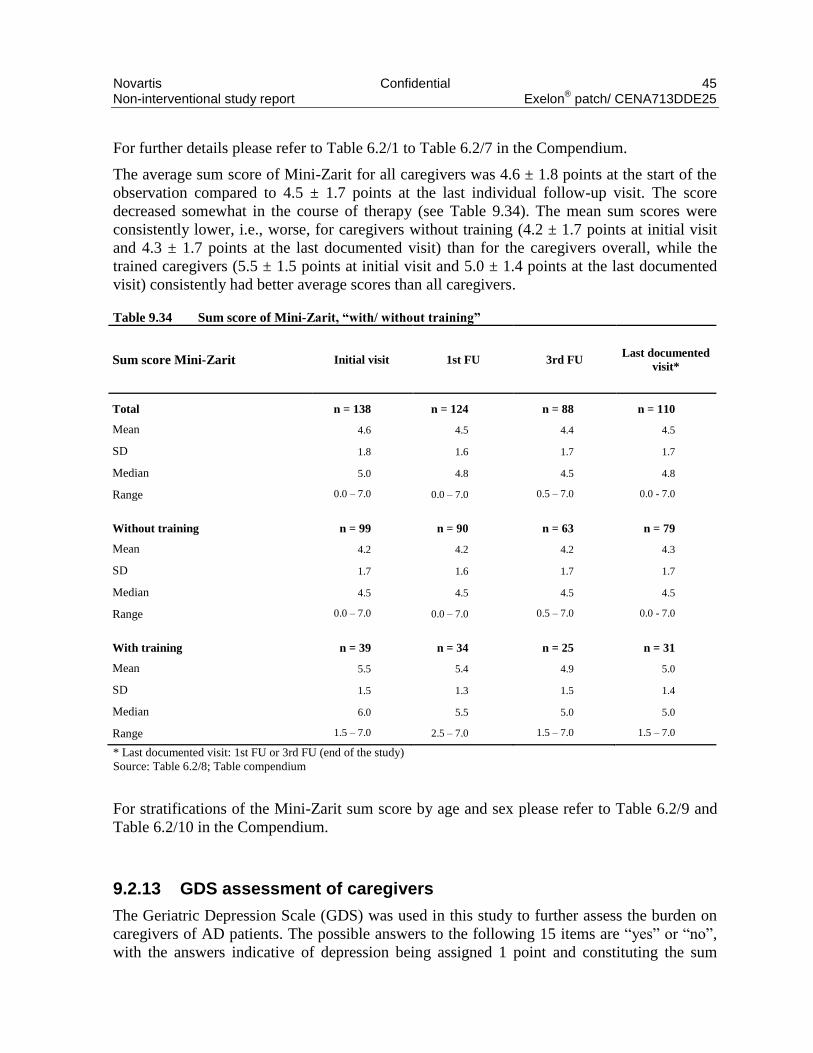
Novartis Confidential 45 Non-interventional study report Exelon
® patch/ CENA713DDE25
For further details please refer to Table 6.2/1 to Table 6.2/7 in the Compendium.
The average sum score of Mini-Zarit for all caregivers was 4.6 ± 1.8 points at the start of the
observation compared to 4.5 ± 1.7 points at the last individual follow-up visit. The score
decreased somewhat in the course of therapy (see Table 9.34). The mean sum scores were
consistently lower, i.e., worse, for caregivers without training (4.2 ± 1.7 points at initial visit
and 4.3 ± 1.7 points at the last documented visit) than for the caregivers overall, while the
trained caregivers (5.5 ± 1.5 points at initial visit and 5.0 ± 1.4 points at the last documented
visit) consistently had better average scores than all caregivers.
Table 9.34 Sum score of Mini-Zarit, “with/ without training”
Sum score Mini-Zarit Initial visit 1st FU 3rd FU Last documented
visit*
Total n = 138 n = 124 n = 88 n = 110
Mean 4.6 4.5 4.4 4.5
SD 1.8 1.6 1.7 1.7
Median 5.0 4.8 4.5 4.8
Range 0.0 – 7.0 0.0 – 7.0 0.5 – 7.0 0.0 - 7.0
Without training n = 99 n = 90 n = 63 n = 79
Mean 4.2 4.2 4.2 4.3
SD 1.7 1.6 1.7 1.7
Median 4.5 4.5 4.5 4.5
Range 0.0 – 7.0 0.0 – 7.0 0.5 – 7.0 0.0 - 7.0
With training n = 39 n = 34 n = 25 n = 31
Mean 5.5 5.4 4.9 5.0
SD 1.5 1.3 1.5 1.4
Median 6.0 5.5 5.0 5.0
Range 1.5 – 7.0 2.5 – 7.0 1.5 – 7.0 1.5 – 7.0
* Last documented visit: 1st FU or 3rd FU (end of the study)
Source: Table 6.2/8; Table compendium
For stratifications of the Mini-Zarit sum score by age and sex please refer to Table 6.2/9 and
Table 6.2/10 in the Compendium.
9.2.13 GDS assessment of caregivers
The Geriatric Depression Scale (GDS) was used in this study to further assess the burden on
caregivers of AD patients. The possible answers to the following 15 items are “yes” or “no”,
with the answers indicative of depression being assigned 1 point and constituting the sum

Novartis Confidential 46 Non-interventional study report Exelon
® patch/ CENA713DDE25
score. A score > 5 points is suggestive of depression. The GDS questionnaire was filled out by
the caregiver at the initial visit and the first and third follow-up visit (or end of observation).
The following analyses are based on the total of available questionnaires.
1. Are you basically satisfied with your life?
In total, the vast majority of caregivers answered in the affirmative at the initial visit
(n=132/142, 93.0 %) and at the last documented visit (n=103/110, 93.6 %). The percentage of
“yes” among caregivers without training was comparable (94.1 % at initial visit and 91.0 % at
the last documented visit), while all the trained caregivers were satisfied at the end of the
study (90.2 % at initial visit and 100.0 % at the last documented visit).
2. Have you dropped many of your activities and interests?
The total number of caregivers more often responded with “no” at the initial visit (n=91/142,
64.1 %) and at the last documented visit (n=68/110, 61.8 %). The percentage of “no” among
caregivers without training was somewhat lower (61.4 % at initial visit and 61.5 % at the last
documented visit), while the trained caregivers more often reported not having dropped many
activities or interests (70.7 % at initial visit and 62.5 % at the last documented visit).
3. Do you feel that your life is empty?
The majority of all caregivers responded with “no” at the initial visit (n=125/142, 88.0 %) and
at the last documented visit (n=99/110, 90.0 %). The percentage of “no” was somewhat higher
among caregivers without training (91.1 % at initial visit and 91.0 % at the last documented
visit) and lower among the trained caregivers (80.5 % at initial visit and 87.5 % at the last
documented visit).
4. Do you often get bored?
Caregivers more frequently responded with “no” at the initial visit (n=133/142, 93.7 %) and at
the last documented visit (n=105/110, 95.5 %). This was comparable to the percentage of
“no” among caregivers without training (95.0 % at initial visit and 94.9 % at the last
documented visit) and among the trained caregivers (90.2 % at initial visit and 96.9 % at the
last documented visit).
5. Are you in good spirits most of the time?
The answer more often provided by caregivers was “yes” at the initial visit (n=108/142,
76.1 %) and at the last documented visit (n=77/110, 70.0 %). The percentage of “yes” was
somewhat lower among caregivers without training (75.2 % at initial visit and 66.7 % at the
last documented visit) and higher among the trained caregivers (78.0 % at initial visit and
78.1 % at the last documented visit).
6. Are you afraid that something bad is going to happen to you?
The more frequent answer by caregivers overall was “no” at the initial visit (n=116/142,
81.7 %) and at the last documented visit (n=88/110, 80.0 %). This was comparable to the
percentage of “no” among caregivers without training (82.2 % at initial visit and 78.2 % at the

Novartis Confidential 47 Non-interventional study report Exelon
® patch/ CENA713DDE25
last documented visit) and among the trained caregivers (80.5 % at initial visit and 84.4 % at
the last documented visit).
7. Do you feel happy most of the time?
Caregivers in total more often responded with “yes” at the initial visit (n=122/142, 85.9 %)
and at the last documented visit (n=95/110, 86.4 %). The percentage of “yes” was slightly
lower among caregivers without training (85.1 % at initial visit and 85.9 % at the last
documented visit) and slightly higher among the trained caregivers (87.8 % at initial visit and
87.5 % at the last documented visit).
8. Do you often feel helpless?
In total, the more frequent answer of the caregivers was “no” at the initial visit (n=118/142,
83.1 %) and at the last documented visit (n=99/110, 90.0 %). The percentage of “no” was
somewhat lower among caregivers without training (80.2 % at initial visit and 88.5 % at the
last documented visit) and higher among the trained caregivers (90.2 % at initial visit and
93.8 % at the last documented visit).
9. Do you prefer to stay at home, rather than going out and doing new things?
The total number of caregivers more often responded with “yes” at the initial visit (n=86/142,
60.6 %) and at the last documented visit (n=62/110, 56.4 %). The percentage of “yes” was
comparable among caregivers without training (61.4 % at initial visit and 56.4 % at the last
documented visit) and slightly lower among the trained caregivers (58.5 % at initial visit and
56.3 % at the last documented visit).
10. Do you feel you have more problems with memory than others?
The majority of all caregivers responded with “no” at the initial visit (n=126/142, 88.7 %) and
at the last documented visit (n=96/110, 87.3 %). The percentage of “no” was higher among
caregivers without training (93.1 % at initial visit and 88.5 % at the last documented visit) and
lower among the trained caregivers (78.0 % at initial visit and 84.4 % at the last documented
visit).
11. Do you think it is wonderful to be alive now?
Caregivers more frequently responded with “yes” at the initial visit (n=113/142, 79.6 %) and
at the last documented visit (n=83/110, 75.5 %). The percentage of “yes” was somewhat
lower among caregivers without training (77.2% at initial visit and 73.1 % at the last
documented visit) and higher among the trained caregivers (85.4 % at initial visit and 81.3 %
at the last documented visit).
12. Do you feel pretty worthless the way you are now?
The answer more often provided by caregivers was “no” at the initial visit (n=131/142,
92.3 %) and at the last documented visit (n=106/110, 96.4 %). The percentage of “no” among
caregivers without training was comparable (93.1 % at initial visit and 94.9 % at the last

Novartis Confidential 48 Non-interventional study report Exelon
® patch/ CENA713DDE25
documented visit), while all the trained caregivers negated feeling worthless at the end of the
study (90.2 % at initial visit and 100.0 % at the last documented visit).
13. Do you feel full of energy?
The more frequent answer by caregivers overall was “no” at the initial visit (n=90/142,
63.4 %) and at the last documented visit (n=67/110, 60.9 %). The percentage of “no” was
somewhat higher among caregivers without training (66.3 % at initial visit and 61.5 % at the
last documented visit) and lower among the trained caregivers (56.1 % at initial visit and
59.4 % at the last documented visit), meaning that more of the latter felt full of energy.
14. Do you feel that your situation is hopeless?
Caregivers in total more often responded with “no” at the initial visit (n=129/142, 90.8 %) and
at the last documented visit (n=102/110, 92.7 %). The percentage of “no” was somewhat
lower among caregivers without training (89.1 % at initial visit and 89.7 % at the last
documented visit) and higher among the trained caregivers, all of whom felt their situation
was not hopeless at the end of the study (95.1 % at initial visit and 100.0 % at the last
documented visit).
15. Do you think that most people are better off than you are?
In total, the more frequent answer of the caregivers was “no” at the initial visit (n=104/142,
73.2 %) and at the last documented visit (n=85/110, 77.3 %). The percentage of “no” was
somewhat lower among caregivers without training (70.3 % at initial visit and 74.4 % at the
last documented visit) and higher among the trained caregivers (80.5 % at initial visit and
84.4 % at the last documented visit).
For further details please refer to Table 6.3/1 to Table 6.3/15 in the Compendium.
The average sum score of GDS for all caregivers was 3.1 ± 2.9 points at the start of the
observation compared to 3.0 ± 2.2 points at the last individual follow-up visit. The score
remained largely constant in the course of therapy (see Table 9.35). The mean sum scores
were consistently higher, i.e., worse, for caregivers without training (3.3 ± 3.0 points at initial
visit and 3.2 ± 2.4 points at the last documented visit) than for the caregivers overall, while
the average scores of the trained caregivers (2.8 ± 2.7 points at initial visit and 2.6 ± 1.7 points
at the last documented visit) were consistently better than those of all caregivers and
decreased in the course of the study.
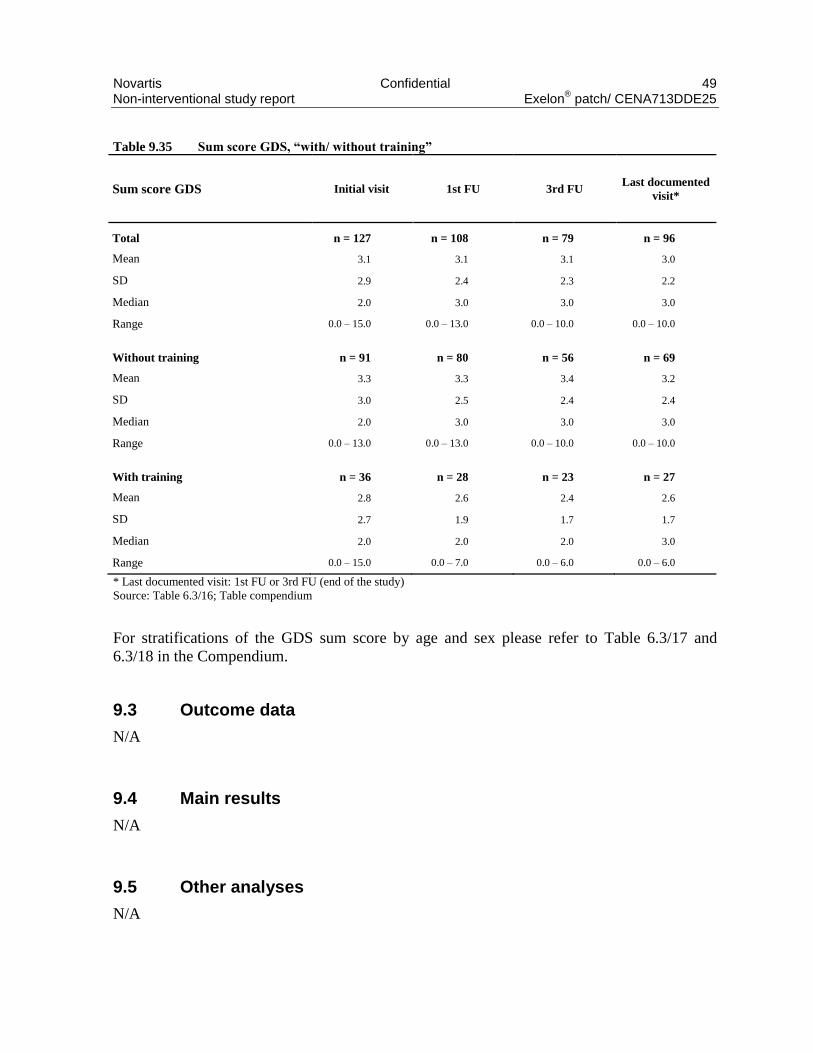
Novartis Confidential 49 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.35 Sum score GDS, “with/ without training”
Sum score GDS Initial visit 1st FU 3rd FU Last documented
visit*
Total n = 127 n = 108 n = 79 n = 96
Mean 3.1 3.1 3.1 3.0
SD 2.9 2.4 2.3 2.2
Median 2.0 3.0 3.0 3.0
Range 0.0 – 15.0 0.0 – 13.0 0.0 – 10.0 0.0 – 10.0
Without training n = 91 n = 80 n = 56 n = 69
Mean 3.3 3.3 3.4 3.2
SD 3.0 2.5 2.4 2.4
Median 2.0 3.0 3.0 3.0
Range 0.0 – 13.0 0.0 – 13.0 0.0 – 10.0 0.0 – 10.0
With training n = 36 n = 28 n = 23 n = 27
Mean 2.8 2.6 2.4 2.6
SD 2.7 1.9 1.7 1.7
Median 2.0 2.0 2.0 3.0
Range 0.0 – 15.0 0.0 – 7.0 0.0 – 6.0 0.0 – 6.0
* Last documented visit: 1st FU or 3rd FU (end of the study)
Source: Table 6.3/16; Table compendium
For stratifications of the GDS sum score by age and sex please refer to Table 6.3/17 and
6.3/18 in the Compendium.
9.3 Outcome data
N/A
9.4 Main results
N/A
9.5 Other analyses
N/A

Novartis Confidential 50 Non-interventional study report Exelon
® patch/ CENA713DDE25
9.6 Adverse events and adverse reactions
Safety evaluation is based on the population of evaluable patients (n=200).
9.6.1 Brief summary of adverse events
As shown in Table 9/36, over a quarter of patients (n=52/200, 26.0%) were affected by at
least one adverse event (AE) of any nature. The rate was lower in the group with untrained
caregivers (n=26/129, 20.2%) than with trained caregivers (n=26/71, 36.6%). Adverse drug
reactions, i.e., nsADR and SADR, occurred in 36/200 (18.0%) and 2/200 patients (1.0%),
respectively. 18 patients (9.0%) had serious AEs without drug-relation (SAEnr), 2 patients
(1.0%) had serious adverse drug reactions (SADR). 30 cases of medication error (15%) and 4
cases of lack of drug effect (2%) were documented. 5 patient deaths were recorded in the
study, 1 of which was assessed to be drug-related (see Narratives in the Appendix). In patients
with AEs, the number of AEs of any nature was most frequently 1 per patient (10.5%),
followed by 2 AEs per patient (7.5%; Table 7/2 in the Compendium).
Of the 129 AEs that occurred altogether, 24 were non-serious and not drug-related (nsAEnr),
63 were non-serious adverse drug reactions (nsADR), 39 were serious and not drug-related
(SAEnr), and 3 were serious adverse drug reactions (SADR; Table 7/9 in the Compendium).
Most AEs belonged to the SOCs "skin and subcutaneous tissue disorders" (16.3%),
"psychiatric disorders" (14.7%), "nervous system disorders" (13.2%), "gastrointestinal
disorders" (10.1%), "general disorders and administration site conditions" (10.1%) and
"cardiac disorders" (8.5%; Table 7/8 in the Compendium). The preferred terms (PTs) for the
most frequently recorded AEs of any group were "nausea" (4.7%) and "depression" (3.9%).
Detailed classifications of all AEs are given in the following section.
Table 9.36 Number of adverse events by patient
Training
Total No Yes
n* % n* % n* %
Total patients 200 100.0 129 100.0 71 100.0
Any adverse events 52 26.0 26 20.2 26 36.6
Non-serious adverse events (nsAEnr) 13 6.5 4 3.1 9 12.7
Non-serious adverse drug reactions (nsADR) 36 18.0 19 14.7 17 23.9
Serious adverse events (SAEnr) 18 9.0 4 3.1 14 19.7
Serious adverse drug reactions (SADR) 2 1.0 1 0.8 1 1.4
Cases of death 5 2.5 4 3.1 1 1.4
Medication error 30 15.0 18 14.0 12 16.9
Lack of drug effect 4 2.0 2 1.6 2 2.8
*Multiple responses possible
Source: Table 7/1; Table compendium

Novartis Confidential 51 Non-interventional study report Exelon
® patch/ CENA713DDE25
9.6.2 Display of adverse events
The most frequent AEs by MedDRA PT are summarized in the following table.
The most common SOC was "skin and subcutaneous tissue disorders", affecting 7.5%
(n=15/200) of patients (Table 7/3 in the Compendium). The most frequent PTs in this SOC
were "erythema", "skin irritation" and "skin reaction" in 4/200 (2.0%) patients, respectively,
followed by "pruritus" and "rash" (1.5%, respectively). AEs belonging to the SOC
"psychiatric disorders" were reported for a total of 12/200 (6.0%) patients. The PT
"depression" occurred in 5/200 (2.5%) patients, followed by "aggression" in 3 patients and
"agitation" in 2 patients. Patients were further affected in about equal parts by the SOCs
"general disorders and administration site conditions" (5.5%), "gastrointestinal disorders"
(5.0%) and "nervous system disorders" (5.0%), the most common PT of administration site
conditions being "application site erythema" in 4 patients (2.0%) and the most common PT of
gastrointestinal disorders being "nausea" in 6 patients (3.0%).
Table 9.37 Patient-based classification of adverse events by MedDRA PT (only PTs ≥1.0%)
Adverse events
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Total patients 200 100.0
All patients with AEs 52 26.0
All patients without AEs 148 74.0
Cardiac disorders Myocardial infarction 2 1.0
Ear and labyrinth disorders Vertigo 3 1.5
Gastrointestinal disorders Abdominal pain upper 2 1.0
Diarrhoea 3 1.5
Nausea 6 3.0
General disorders and administration site
conditions
Application site erythema 4 2.0
Application site pruritus 2 1.0
Death 2 1.0
Infections and infestations Pneumonia 2 1.0
Injury, poisoning and procedural
complications
Fall
2 1.0
Investigations Mini mental status examination abnormal 2 1.0

Novartis Confidential 52 Non-interventional study report Exelon
® patch/ CENA713DDE25
Adverse events
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Metabolism and nutrition disorders Vitamin B12 deficiency 2 1.0
Nervous system disorders Headache 2 1.0
Paraesthesia 2 1.0
Polyneuropathy 2 1.0
Psychiatric disorders Aggression 3 1.5
Agitation 2 1.0
Depression 5 2.5
Skin and subcutaneous tissue disorders Erythema 4 2.0
Pruritus 3 1.5
Rash 3 1.5
Skin irritation 4 2.0
Skin reaction 4 2.0
*Multiple responses possible
Source: Table 7/3; Table compendium
Stratification of AEs by caregiver training is shown in Table 7/3 in the Compendium.
Table 9/38 summarizes the most frequent nsAEnr by MedDRA PT.
The most common SOC was "psychiatric disorders", affecting 3.5% (n=7/200) of patients
(Table 7/4 in the Compendium). The most frequent PTs in this SOC were "depression" in
4/200 (2.0%) patients and "aggression" (n=2/200, 1.0%). nsAEnr belonging to the SOC
"nervous system disorders" were reported for a total of 4/200 (2.0%) patients, with the PT
"paraesthesia" occurring in 2/200 (1.0%) patients. 2 patients (1.0%) were affected by the PT
"vitamin B12 deficiency" in the SOC "metabolism and nutrition disorders".
Table 9.38 Patient-based classification of non-serious adverse events by MedDRA PT (only PTs
≥1.0%)
Non-serious adverse events not related
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Total patients 200 100.0
All patients with nsAEnr 13 6.5
All patients without nsAEnr 187 93.5

Novartis Confidential 53 Non-interventional study report Exelon
® patch/ CENA713DDE25
Non-serious adverse events not related
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Metabolism and nutrition disorders Vitamin B12 deficiency 2 1.0
Nervous system disorders Paraesthesia 2 1.0
Psychiatric disorders Aggression 2 1.0
Depression 4 2.0
*Multiple responses possible
Source: Table 7/4; Table compendium
Stratification of nsAEnr by caregiver training is shown in Table 7/4 in the Compendium. A
listing of the nsAEnr can be found in Table 7/10 in the Compendium.
The following table shows the most frequent nsADR by MedDRA PT.
The by far most common SOC was "skin and subcutaneous tissue disorders", affecting 7.5%
(n=15/200) of patients (Table 7/5 in the Compendium). The most frequent PTs in this SOC
were "erythema", "skin irritation" and "skin reaction" in 4/200 (2.0%) patients, respectively,
followed by "pruritus" and "rash" (1.5%, respectively). nsADR belonging to the SOC
"gastrointestinal disorders" were reported for a total of 7/200 (3.5%) patients. The PT
"nausea" occurred in 5/200 (2.5%) patients, followed by "diarrhoea" in 3 patients. Patients
were further affected by the SOC "general disorders and administration site conditions"
(n=6/200, 3.0%), the most common PTs being "application site erythema" in 4 patients (2.0%)
and "application site pruritus" in 2 patients (1.0%). 3 patients (1.5%) were affected by the PT
"vertigo" in the SOC "ear and labyrinth disorders".

Novartis Confidential 54 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.39 Patient-based classification of non-serious adverse drug reactions by MedDRA PT (only
PTs ≥1.0%)
Non-serious adverse drug reactions
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Total patients 200 100.0
All patients with nsADR 36 18.0
All patients without nsADR 164 82.0
Ear and labyrinth disorders Vertigo 3 1.5
Gastrointestinal disorders Diarrhoea 3 1.5
Nausea 5 2.5
General disorders and administration site
conditions
Application site erythema 4 2.0
Application site pruritus 2 1.0
Investigations Mini mental status examination abnormal 2 1.0
Nervous system disorders Headache 2 1.0
Psychiatric disorders Agitation 2 1.0
Skin and subcutaneous tissue disorders Erythema 4 2.0
Pruritus 3 1.5
Rash 3 1.5
Skin irritation 4 2.0
Skin reaction 4 2.0
*Multiple responses possible
Source: Table 7/5; Table compendium
Stratification of nsADR by caregiver training is shown in Table 7/5 in the Compendium. A
listing of the nsADR can be found in Table 7/11 in the Compendium.
Table 9/40 summarizes the most frequent SAEnr by MedDRA PT.
The most common SOC was "cardiac disorders" in 3.0% (n=6/200) of patients (Table 7/6 in
the Compendium), with the PT "myocardial infarction" affecting 1.0% (n=2/200) of patients.
SAEnr belonging to the SOC "nervous system disorders" were reported for a total of 5/200
(2.5%) patients, with the PT "polyneuropathy" occurring in 2/200 (1.0%) patients. Patients

Novartis Confidential 55 Non-interventional study report Exelon
® patch/ CENA713DDE25
were further affected by the SOC "general disorders and administration site conditions"
(n=4/200, 2.0%), the most common PT being "death" in 2 patients (1.0%).
Table 9.39 Patient-based classification of serious adverse events by MedDRA PT
Serious adverse events not related
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Total patients 200 100.0
All patients with SAEnr 18 9.0
All patients without SAEnr 182 91.0
Blood and lymphatic system disorders Anaemia 1 0.5
Cardiac disorders Atrial fibrillation 1 0.5
Cardiac failure 1 0.5
Cardiomyopathy 1 0.5
Left ventricular failure 1 0.5
Myocardial infarction 2 1.0
Tricuspid valve incompetence 1 0.5
Gastrointestinal disorders Abdominal pain upper 1 0.5
Nausea 1 0.5
Pancreatic steatosis 1 0.5
General disorders and administration site
conditions
Cardiac death 1 0.5
Death 2 1.0
Gait disturbance 1 0.5
Pyrexia 1 0.5
Infections and infestations Pneumonia 2 1.0
Sepsis 1 0.5
Injury, poisoning and procedural
complications
Anaemia postoperative 1 0.5
Fall 2 1.0
Femur fracture 1 0.5
Post procedural haematoma 1 0.5
Investigations Troponin increased 1 0.5
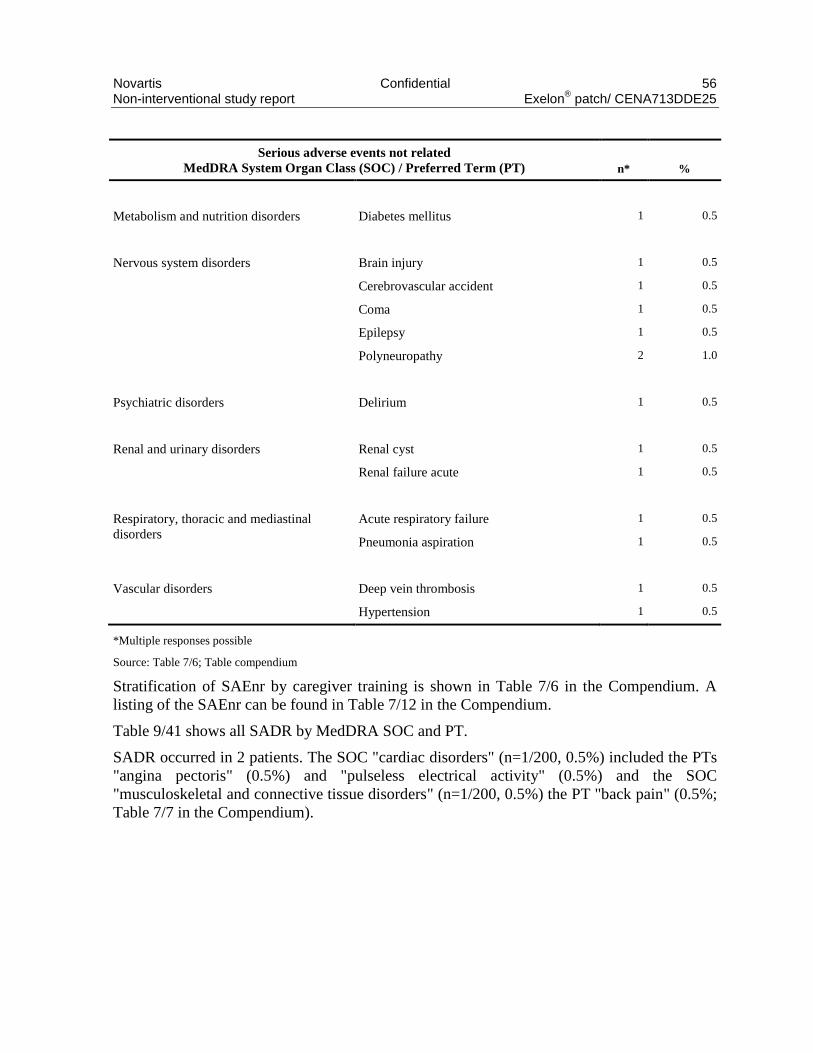
Novartis Confidential 56 Non-interventional study report Exelon
® patch/ CENA713DDE25
Serious adverse events not related
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Metabolism and nutrition disorders Diabetes mellitus 1 0.5
Nervous system disorders Brain injury 1 0.5
Cerebrovascular accident 1 0.5
Coma 1 0.5
Epilepsy 1 0.5
Polyneuropathy 2 1.0
Psychiatric disorders Delirium 1 0.5
Renal and urinary disorders Renal cyst 1 0.5
Renal failure acute 1 0.5
Respiratory, thoracic and mediastinal
disorders
Acute respiratory failure 1 0.5
Pneumonia aspiration 1 0.5
Vascular disorders Deep vein thrombosis 1 0.5
Hypertension 1 0.5
*Multiple responses possible
Source: Table 7/6; Table compendium
Stratification of SAEnr by caregiver training is shown in Table 7/6 in the Compendium. A
listing of the SAEnr can be found in Table 7/12 in the Compendium.
Table 9/41 shows all SADR by MedDRA SOC and PT.
SADR occurred in 2 patients. The SOC "cardiac disorders" (n=1/200, 0.5%) included the PTs
"angina pectoris" (0.5%) and "pulseless electrical activity" (0.5%) and the SOC
"musculoskeletal and connective tissue disorders" (n=1/200, 0.5%) the PT "back pain" (0.5%;
Table 7/7 in the Compendium).

Novartis Confidential 57 Non-interventional study report Exelon
® patch/ CENA713DDE25
Table 9.40 Patient-based classification of serious adverse drug reactions by MedDRA SOC and PT
Serious adverse drug reactions
MedDRA System Organ Class (SOC) / Preferred Term (PT) n* %
Total patients 200 100.0
All patients with SADR 2 1.0
All patients without SADR 198 99.0
Cardiac disorders Angina pectoris 1 0.5
Pulseless electrical activity 1 0.5
Musculoskeletal and connective tissue
disorders
Back pain 1 0.5
*Multiple responses possible
Source: Table 7/7; Table compendium
Stratification of SADR by caregiver training is shown in Table 7/7 in the Compendium. A
listing of the SADR can be found in Table 7/13 in the Compendium.
The event-based classification of AEs by MedDRA PT is summarized in Table 9/42. Most
AEs belonged to the SOCs "skin and subcutaneous tissue disorders" (n=21/129, 16.3%),
"psychiatric disorders" (14.7%), "nervous system disorders" (13.2%), "gastrointestinal
disorders" (10.1%), "general disorders and administration site conditions" (10.1%) and
"cardiac disorders" (8.5%; Table 7/8 in the Compendium). The most frequent PTs were
"nausea" (n=6/129, 4.7%) in the SOC "gastrointestinal disorders" and "depression" (3.9%) in
the SOC "psychiatric disorders". Stratification by the types of AEs revealed all skin and
subcutaneous tissue disorders to be nsADR.
Table 9.41 Event-based classification of adverse events by MedDRA PT (only PTs ≥1.0%)
MedDRA SOC / PT
All adverse
events
nsAEnr
nsADR
SAEnr
SADR
n % n % n % n % n %
Total AEs 129 100.0 24 100.0 63 100.0 39 100.0 3 100.0
Cardiac disorders Myocardial infarction 2 1.6 0 - 0 - 2 5.1 0 -
Ear and labyrinth
disorders
Vertigo 4 3.1 0 - 4 6.3 0 - 0 -
Gastrointestinal
disorders
Abdominal pain upper 2 1.6 0 - 1 1.6 1 2.6 0 -
Diarrhoea 3 2.3 0 - 3 4.8 0 - 0 -

Novartis Confidential 58 Non-interventional study report Exelon
® patch/ CENA713DDE25
MedDRA SOC / PT
All adverse
events
nsAEnr
nsADR
SAEnr
SADR
n % n % n % n % n %
Nausea 6 4.7 0 - 5 7.9 1 2.6 0 -
General disorders and
administration site
conditions
Application site
erythema
4 3.1 0 - 4 6.3 0 - 0 -
Application site pruritus 2 1.6 0 - 2 3.2 0 - 0 -
Death 2 1.6 0 - 0 - 2 5.1 0 -
Infections and
infestations
Pneumonia 2 1.6 0 - 0 - 2 5.1 0 -
Injury, poisoning and
procedural complications
Fall 2 1.6 0 - 0 - 2 5.1 0 -
Investigations Mini mental status
examination abnormal
2 1.6
0
-
2
3.2
0
-
0
-
Metabolism and nutrition
disorders
Vitamin B12 deficiency 2 1.6
2
8.3
0
-
0
-
0
-
Nervous system
disorders
Headache 3 2.3 0 - 3 4.8 0 - 0 -
Paraesthesia 2 1.6 2 8.3 0 - 0 - 0 -
Polyneuropathy 2 1.6 0 - 0 - 2 5.1 0 -
Psychiatric disorders Aggression 3 2.3 2 8.3 1 1.6 0 - 0 -
Agitation 2 1.6 0 - 2 3.2 0 - 0 -
Depression 5 3.9 4 16.7 1 1.6 0 - 0 -
Skin and subcutaneous
tissue disorders
Erythema 4 3.1 0 - 4 6.3 0 - 0 -
Pruritus 3 2.3 0 - 3 4.8 0 - 0 -
Rash 3 2.3 0 - 3 4.8 0 - 0 -
Skin irritation 4 3.1 0 - 4 6.3 0 - 0 -
Skin reaction 4 3.1 0 - 4 6.3 0 - 0 -
Source: Table 7/8; Table compendium
Stratification of the AEs by caregiver training is shown in Table 7/8 in the Compendium.

Novartis Confidential 59 Non-interventional study report Exelon
® patch/ CENA713DDE25
As shown in Table 9/43, the outcome of most AEs was "complete recovery" (n=57/129,
44.2%), followed by "condition unchanged" (20.9%) and "death" (10.9%). Stratification by
the types of AEs revealed the vast majority of AEs with the outcome "complete recovery" to
be nsADR.
Table 9.42 Outcome of adverse events
Outcome
All adverse
events nsAEnr nsADR SAEnr SADR
n % n % n % n % n %
Total 129 100.0 24 100.0 63 100.0 39 100.0 3 100.0
Not reported 18 14.0 9 37.5 3 4.8 4 10.3 2 66.7
Complete recovery 57 44.2 5 20.8 43 68.3 9 23.1 0 -
Condition improving 10 7.8 0 - 5 7.9 5 12.8 0 -
Condition deteriorated 2 1.6 0 - 2 3.2 0 - 0 -
Condition unchanged 27 20.9 10 41.7 10 15.9 7 17.9 0 -
Recovered with sequelae 1 0.8 0 - 0 - 1 2.6 0 -
Death 14 10.9 0 - 0 - 13 33.3 1 33.3
Source: Table 7/9; Table compendium
Stratification of the outcome by caregiver training is shown in Table 7/9 in the Compendium.
9.6.3 Deaths, other serious events, and other significant adverse events
9.6.3.1 Listing of deaths, serious adverse events and other significant adverse events
Listings of fatal SAEnr and fatal SADR can be found in Table 7/14 and Table 7/15 in the
Compendium, respectively.
All events concerning drug ineffectiveness and medication errors are listed in Table 7/16.
Medication errors that happened in this study were raising the dose directly from 4.6 mg to
13.3 mg, staying below the minimum 6-month use of 9.5 mg patches before raising the dose
to 13.3 mg, decrease of dosage, inappropriate use of patch, and multiple patch use.
AEs of excluded patients are listed in Table 7/17.
9.6.3.2 Narratives of deaths
Case narratives of fatal serious adverse events can be found in the Appendix.

Novartis Confidential 60 Non-interventional study report Exelon
® patch/ CENA713DDE25
10 Discussion
10.1 Key results
For the last decade, a great amount of research on pharmacological treatment of AD has been
made, including research on existing symptomatic therapy of AD like cholinesterase-
inhibitors, e.g. rivastigmine (Rainer, 2013; Seibert et al, 2012).
This post-marketing NIS was performed to compare an up to 12-month treatment with the
rivastigmine (Exelon®) patch in newly diagnosed AD patients with or without training of
caregivers according to "Demenz aktiv begegnen". The course of the disease, the persistence
to therapy and the quality of life of family caregivers under daily-life conditions were
investigated. To assess these parameters, the MMSE was used as a well-established scale to
screen for cognitive function in the course of AD (Arevalo‐Rodriguez et al, 2015), the Mini-
Zarit as validated measure of burden on caregivers with 7/22 instead of 12/22 items (original
version: Zarit et al, 1980; mini-Zarit: Revel Da Rocha et al, 2002) and the GDS to determine
potential depressive symptoms in caregivers with 15/22 items (original version: Gauggel &
Birkner, 1999; 15 items: Sheikh & Yesavage, 1986).
A total of 160 out of 206 patients enrolled at 41 sites in Germany between April 2013 and
November 2014 were valid for analysis. Both sex (56.9% female and 41.3% male) and age
distribution (with an average age of 77.5 years) did not match recent prevalence data for AD
(Bickel, 2014; S3-Leitlinie, 2009). In addition, differing from a general AD population, >90%
of patients were living at home with/without their family and had a short median history of
AD (3.5 months). Thus, older patients (>85 years) and patients with a long AD history were
underrepresented. These differences were in accordance with the objectives and inclusion
criteria for this study. It was expected to include patients starting with a therapy and
caregivers getting their first training in an earlier stage of the disease. This is also attributed to
the use of Exelon® patch, which is licensed for patients with mild-to-moderate AD (Exelon
®
SmPC), i.e. patients with severe AD were not to be included. Thus, Exelon® patch was the
first specific treatment of AD in 2/3 of the evaluable patients.
Caregivers of 41 AD patients (mean age of patients 79.0 years) attended the training in
contrast to caregivers of 119 patients (mean age of patients 77.0 years) who didn`t have the
opportunity to attend such training. As training was only performed in sites routinely offering
trainings, this imbalance gives a good impression about the current care situation. The
impairment of the caregiver’s ability to take care of the patient in the two study arms varied.
About 90% of caregivers with training were not impaired, but about 50% of those without
training were impaired to different extents. This might result from a different patient selection
of sites that performed training.
Overall, assessment of the disease severity by the MMSE sum score (mean ±SD) was nearly
stable with 20.5 ±4.2 points (N=133) at baseline and 19.9 ±4.5 points (N=94) after 12 month
of rivastigmine patch therapy or the last individual FU visit, independent from training.
Similar persistence of MMSE results was obtained from other studies after treatment with the
rivastigmine patch over 24 weeks (e.g., Adler et al, 2014; see for review: Dhillon, 2011) or
even a reduced MMSE decline using rivastigmine tablets versus no treatment for up to 5 years
(Small et al, 2005). In short-term patch studies, MMSE even showed an improvement up to 4

Novartis Confidential 61 Non-interventional study report Exelon
® patch/ CENA713DDE25
months (Seibert et al, 2012). In this study, 29.4% of all patients had prematurely discontinued
dosing at the last individual FU visit, including 10% who withdrew due to AEs and 1.3%
documented to be non-responders according to physician’s judgment. The average treatment
duration for those patients who discontinued the study prematurely was shorter with 8.7 ±5.1
months (trained cohort) and 6.8 ±3.7 months (untrained cohort). This difference between the
trained and untrained group suggests a benefit of training the caregivers on the persistence of
the antidementive therapy which is in accordance with a previous study (Riepe et al, 2015).
Rivastigmine patch doses were increased from 4.6 mg at baseline (84%) to 9.5/13.3 mg in
more than half of patients. This increase is lesser then observed in other studies (Adler et al,
2014; Articus et al, 2011).
Two Training sessions “Demenz Aktiv Begegnen” has been attended by 41/160 (25.6%) of
caregivers who perceived both trainings as helpful to uttermost helpful in an outmost friendly
atmosphere. Surprisingly, caregivers with training felt that their burden concerning the
Alzheimer`s dementia of their relatives was not eased but rather increased, whereas caregivers
without training rated this burden more often as eased. This is in contrast to the lesser
impairment of caregivers in the training-group but could result from a more detailed
information on the disease and its perspective that might increase the feeling of a burden in
general (Beinart et al, 2012; Hauber et al, 2014).
Validated caregiver questionnaires were available at baseline for 90.0% (Mini-Zarit) and
88.8% (GDS) of all patients, with a rate of 100% from the 41 trained caregivers. This rate was
reduced to 70.0%/68.8% (Mini-Zarit/GDS) for all caregivers and to 80.5%/78.0% for trained
caregivers at the last individual FU, respectively. The 7-item Mini-Zarit was consistently
higher (better) for all items with an average sum score from baseline versus the last individual
FU for trained caregivers (5.5 ±1.5 vs. 5.0 ±1.4 points) than for caregivers without training
(4.2 ±1.7 vs. 4.3 ±1.7 points). Again, these results reflected a slightly increasing burden
during this study for caregivers with, but not for those without training for possible reasons
stated above. Overall, there was no change in the Mini-Zarit (4.6 ±1.8 vs. 4.5 ±1.7 points). In
a previous study where rivastigmine has been co-administered with memantine over 28
weeks, there has been a statistically significant improvement (Dantoine et al, 2006). However,
regarding the most important issues (Bachner et al, 2007; Ballesteros et al, 2012; Braun et al,
2010; Cheng et al, 2014) 2 (trouble outside family), 5 (fear about future of patient) and 7
(burden while caring), there was rather a stable or improved outcome for these items in this
study.
Interestingly, the GDS mean sum scores were also consistently lower (i.e., better) for trained
caregivers (2.8 ±2.7 vs. 2.6 ±1.7 points) than for caregivers without training (3.3 ±3.0 vs. 3.2
±2.4 points). The trained caregivers scored better than the untrained caregivers on nearly all
15 items of the abbreviated GDS questionnaire with negligible improvements during the NIS
in both groups. This difference might be due to the lesser impairment of the caregivers in the
group with training but might also result from the higher interaction and information they
received during the training sessions.
Nevertheless, in view of the relatively long observation period in the present study with the
rivastigmine patch alone, it remains remarkable, that overall results of the MMSE remained

Novartis Confidential 62 Non-interventional study report Exelon
® patch/ CENA713DDE25
nearly constant and caregivers stated no more than a small increase in disease burden, mainly
for their relatives, if at all.
Safety evaluation comprised the documentation and analysis of treatment-emergent
AEs/SAEs. Overall, 52/200 of the patients (26.0%) in this NIS experienced at least 1 AE or
SAE. A total of 5 patients died. The cause of death was documented as “natural death”
(twice), “electromechanical decoupling after anterior myocardial infarction”, “cardiac failure,
sepsis and poly-uric acute renal failure”, and “reflective cardiac death, hypoxic cerebral
death”, respectively. In 36 (18.0%) patients with AEs and 2 (1.0%) patients with SAEs, these
were classified as ADR/SADR. Considering the low patient number, this study showed
similar tolerability of rivastigmine patch compared to other non-interventional (Articus et al,
2011) or clinical studies (Winblad et al, 2007).
10.2 Limitations
In contrast to clinical trials, a NIS is not designed to prove the efficacy and tolerability of a
drug, but can provide valuable information on drug use in real-life settings. Besides the
relative small number of patients, in particular patients with trained caregivers, the restriction
of reported outcome measures to the widely used and validated MMSE and GSD – for
feasibility reasons in a NIS – does not reflect all relevant capabilities of daily life in patients
with a complex disease. The imbalance between the small number of 41 patients with trained
and 119 patients with untrained caregivers might have impaired the validity of results of this
statistical comparison.
10.3 Conclusion
This NIS in patients with mild to moderate AD showed a better Mini-Zarit and GDS in trained
than in untrained caregivers both at baseline and the last individual FU. These validated
questionnaires pointed to a stable or slightly reduced burden preferably in non-trained, mainly
familiar caregivers. Thus, a more detailed information on the disease and its perspective might
increase the feeling of burden in trained caregivers. So far, there are only few data on long-
term therapy in AD. This NIS also demonstrated a nearly stable severity of the disease within
one year of therapy with the rivastigmine patch, which was well tolerated with a low
frequency of ADRs. Additional training may therefore help the familial caregivers in daily life
to reduce the burden of disease and to increase patient persistence for symptomatic therapy in
patients with mild to moderate AD.

Novartis Confidential 63 Non-interventional study report Exelon
® patch/ CENA713DDE25
11 References
[1] ADLER, G., MUELLER, B., ARTICUS, K. (2014) The transdermal formulation of rivastigmine
improves caregiver burden and treatment adherence of patients with Alzheimer's disease under
daily practice conditions. Int J Clin Prac; 68(4): 465-70.
[2] ALZHEIMER`S ASSOCIATION USA. (2012) Alzheimer’s Disease Facts and Figures.
Alzheimer´s Association; 2012. Available from:
http://www.alz.org/downloads/facts_figures_2012.pdf
[3] AREVALO‐RODRIGUEZ, I., SMAILAGIC, N., ROQUÉ, I., FIGULS, M., ET AL. (2015)
Mini‐Mental State Examination (MMSE) for the detection of Alzheimer's disease and other
dementias in people with mild cognitive impairment (MCI). The Cochrane Library 2015.
[4] ARTICUS, K., BAIER, M., TRACIK, F., ET AL. (2011) A 24-week, multicentre, open
evaluation of the clinical effectiveness of the rivastigmine patch in patients with probable
Alzheimer’s disease. Int J Clin Pract; 65(7): 790-6.
[5] BACHNER, Y.G., O’ROURKE, N. (2007) Reliability generalization of responses by care
providers to the Zarit Burden Interview. Aging Mental Health; 11(6): 678-685.
[6] BALLESTEROS, J., SANTOS, B., GONZÁLEZ-FRAILE, E., ET AL. (2012) Unidimensional
12-item Zarit Caregiver Burden Interview for the assessment of dementia caregivers’ burden
obtained by item response theory. Value in Health; 15(8): 1141-1147.
[7] BEINART, N., WEINMAN, J., WADE, D., BRADY, R. (2012) Caregiver Burden and
Psychoeducational Interventions in Alzheimer’s Disease: A Review. Dement Geriatr Cogn
Disord Extra; 2: 638-648.
[8] BICKEL, H. (2014) Die Epidemiologie der Demenz [The epidemiology of dementia]. In:
Infoblatt Demenz. Deutsche Alzheimer Gesellschaft. https://www.deutsche-
alzheimer.de/fileadmin/alz/pdf/factsheets/infoblatt1_haeufigkeit_demenzerkrankungen_dalzg.pd
f, accessed 14 July 2015.
[9] BRAUN, M., SCHOLZ, U., HORNUNG, R., MARTIN, M. (2010) Die subjektive Belastung
pflegender Ehepartner von Demenzkranken. Z Gerontol Geriatr; 43(2): 111-119.
[10] CHENG, S.T., KWOK, T., LAM, L.C. (2014) Dimensionality of burden in Alzheimer
caregivers: confirmatory factor analysis and correlates of the Zarit Burden interview.
International Psychogeriatrics; 26(09): 1455-1463.
[11] CUMMINGS, J.L., FRANK, J.C., CHERRY, D., KOHATSU, N.D., KEMP, B., HEWETT, L.,
MITTMAN, B. (2002) Guidelines for managing Alzheimer's disease: Part II. Treatment. Am
Fam Physician; 65(12): 2525-34.
[12] DANTOINE, T., AURIACOMBE, S., SARAZIN, M., BECKER, H., PERE, J.J., BOURDEIX,
I. (2006) Rivastigmine monotherapy and combination therapy with memantine in patients with
moderately severe Alzheimer's disease who failed to benefit from previous cholinesterase
inhibitor treatment. Int J Clin Pract; 60(1): 110-8.

Novartis Confidential 64 Non-interventional study report Exelon
® patch/ CENA713DDE25
[13] DEUTSCHE GESELLSCHAFT FÜR PSYCHIATRIE, PSYCHOTHERAPIE UND
NERVENHEILKUNDE UND DEUTSCHE GESELLSCHAFT FÜR NEUROLOGIE. (2009)
S3 - Leitlinie "Demenzen" [Guideline Dementia]. In: Diagnose und Behandlungsleitlinie
Demenz. http://link.springer.com/chapter/10.1007/978-3-642-13092-2_2, accessed 20 May
2015.
[14] DHILLON, S. (2011) Rivastigmine transdermal patch: a review of its use in the management of
dementia of the Alzheimer’s type. Drugs; 71: 1209-31.
[15] GAUGGEL, S., BIRKNER, B. (1999) Validity and reliability of a German version of the
Geriatric Depression Scale (GDS). Zeitschrift Klin Psychologie; 28: 18-27.
[16] HAUBER, A.B., MOHAMED, A.F., JOHNSON, F.R., COOK, M., ARRIGHI, H.M., ZHANG,
J., GRUNDMAN, M. (2014) Understanding the relative importance of preserving functional
abilities in Alzheimer’s disease in the United States and Germany. Qual Life Res; 23(6): 1813-
1821.
[17] HORNE, R., WEINMAN, J. (1999) Patients' beliefs about prescribed medicines and their role in
adherence to treatment in chronic physical illness. J Psychosom Res; 47(6): 555-67.
[18] HUGHES, D., COWELL, W., KONCZ, T., CRAMER, J., INTERNATIONAL SOCIETY FOR
PHARMACOECONOMICS & OUTCOMES RESEARCH ECONOMICS OF MEDICATION
COMPLIANCE WORKING GROUP. (2007) Methods for integrating medication compliance
and persistence in pharmacoeconomic evaluations. Value Health; 10(6): 498-509.
[19] PERRY, M., DRAASKOVIC, I., LUCASSEN, P., VERNOOIJ-DASSEN, M., VAN
ACHTERBERG, T., RIKKERT, M.O. (2011) Effects of educational interventions on primary
dementia care: A systematic review. Int J Geriatr Psychiatry; 26: 1-11.
[20] RAINER, M. (2013) Cholinesterasehemmer zur Therapie der Alzheimerschen Krankheit: Gibt
es klinisch relvante Unterschiede? J Neurol Neurochir Psychiatr; 1999: 21-21.
[21] REVEL DA ROCHA, V., HARITCHABALET, I., KERVINIO, C., ET AL. (2002)
Construction d’une échelle simplifiée pour la détection en médecine générale du fardeau de
l’aidant d’une personne âgée dépendante. L’Année Gérontologique; 16: 131-7.
[22] RIEPE, M., WEINMAN, J., OSAE-LARBI, J., ET AL. (2015) Factors Associated with Greater
Adherence to and Satisfaction with Transdermal Rivastigmine in Patients with Alzheimer’s
Disease and Their Caregivers. Dement Geriatr Cogn Disord; 40: 107-119.
[23] SEIBERT, J., TRACIK, F., ARTICUS, K., Spittler S. (2012) Effectiveness and tolerability of
transdermal rivastigmine in the treatment of Alzheimer’s disease in daily practice.
Neuropsychiatr Dis Treat; 8: 141-7.
[24] SHEIKH, J.I., YESAVAGE, J.A. (1986) Geriatric Depression Scale (GDS) recent evidence and
development of a shorter version. Clinical Gerontologist; 1: 165-173.
[25] SMALL, G., DUBOIS, B. (2007) A review of compliance to treatment in Alzheimer's disease:
potential benefits of a transdermal patch. Curr Med Res Opin; 23(11): 2705-13.

Novartis Confidential 65 Non-interventional study report Exelon
® patch/ CENA713DDE25
[26] SMALL, G.W., KAUFER, D., MENDIONDO, M.S., ET AL. (2005) Cognitive performance in
Alzheimer’s disease patients receiving rivastigmine for up to 5 years. Int J Clin Pract; 59: 473-7.
[27] VAN MIERLO, L.D., MEILAND, F.J.M., VAN DER ROEST, H.G., DROES, R.-M. (2012)
Personalised caregiver support: Effectiveness of psychosocial interventions in subgroups of
caregivers of people with dementia. Int J Geriatr Psychiatry; 27: 1-14.
[28] WINBLAD, B., CUMMINGS, J., ANDREASEN, N., ET AL. (2007) A six-month double-blind,
randomized, placebo-controlled study of a transdermal patch in Alzheimer's disease -
rivastigmine patch versus capsule. Int J Geriatr Psychiatry; 22(5): 456-467.
[29] ZARIT, SH., REEVER, K.E., BACH-PETERSON, J. (1980) Relatives of the impaired elderly:
Correlates of feelings of burden. Gerontologist; 20: 649-55.