non-interactive 7 minute stations … · 7/4/2018 · • white pages: identification (pictures)...
TRANSCRIPT
1
NON-INTERACTIVE 7 MINUTE STATIONS Calculations: REVIEW MATH MODULES 1-5 for practice questions Roman Numerals: ss = 0.5 i = 1 v = 5 x = 10 l = 50 c = 100 d = 500 m = 1000
• If first value ≥ second value, the two are added ex// vi 5 > 1 5 + 1 = 6
• If first value < second value, it is subtracted ex// cm 100 < 1000 1000 – 100 = 900 Apothecary System:
• Estimates: ʒ = 5 mL ℥ = 6 drams/ounce = 30 mL ℥ = 25 g (sometimes 30 g)
• Exact conversions: ʒ = 3.55 mL ℥ = 8 drams/ounce = 28.44 mL
• Liquid medications where either the mitte or sig are in apothecary symbol: use estimates
• Oral liquid med where both mitte & sig are apothecary symbols: use estimates for sig, use exact conversion for mitte
• Semi-solid medications (creams & ointments), where mitte is given in ounces (by weight): use estimate (℥ = 25 g) Concentrations:
Concentration by percent • % w/w = grams of x in 100 g total mixture
• % w/v = grams of x in 100 mL total mixture
• % v/v = millilitres of x in 100 mL total mixture
• mg % = milligram of x in 100 mL (or 100 g) of total mixture
Concentration by parts • ppm = parts of x (g or mL) in 1,000,000 parts total mixture (g or mL)
• 1 x:y = parts of x (g or mL) in y parts total mixture (g or mL)
Concentration by moles • M (molarity) = moles of x in 1000 mL (1 L) of solution
• m (molality) = moles of x in 1000 g of solvent
• mol fraction = moles of x in the sum of the # of moles of each substance, as a fraction o ex// moles of x / mole of x + mole of y
• mol percent = mol fraction multiplied by 100% Conversions and miscellaneous: 1 kg = 2.2 lb 1 lb = 454 g 1 cm = 0.39 in 1 in = 2.54 cm
oC = 5/9 (xoF – 32o) oF = (9/5 xoC) + 32o
𝑚𝐸𝑞 = 𝑚𝑔∗𝑣𝑎𝑙𝑒𝑛𝑐𝑒
𝑎𝑡𝑜𝑚𝑖𝑐,𝑚𝑜𝑙𝑒𝑐𝑢𝑙𝑎𝑟 𝑜𝑟 𝑓𝑜𝑟𝑚𝑢𝑙𝑎 𝑤𝑒𝑖𝑔ℎ𝑡 valence = total # of +ve or -ve charges (not the charges added together)
Percent error = 𝑑𝑖𝑓𝑓𝑒𝑟𝑒𝑛𝑐𝑒 𝑏𝑒𝑡𝑤𝑒𝑒𝑛 𝑎𝑐𝑡𝑢𝑎𝑙 & 𝑒𝑥𝑝𝑒𝑐𝑡𝑒𝑑 𝑣𝑎𝑙𝑢𝑒𝑠
𝑒𝑥𝑝𝑒𝑐𝑡𝑒𝑑 𝑣𝑎𝑙𝑢𝑒𝑠 𝑥 100%
Nebules: Strength of nebule = mg/mL vs. amount of drug in mL (volume of each nebule affects amount of drug) Dose = mg Example: Budesonide dose is 0.25 mg BID and comes in Pulmicort 2 mL nebules 0.25 mg / 2 mL per nebule = 0.125 mg/mL Therefore, use pulmicort 0.125 mg/mL strength to get a dose of 0.25 mg

2
PharmaCare: NOTE: % covered in Zone Y if one spouse is born in 1939 or earlier is 75% instead of 70% LCA Calculations: 1. Actual Rx cost = AAC + professional fee (NOTE: if pt reached maximum, pharmacy can only charge max $10.00 fee)
Example: Rx for 7 fentanyl 50 µg patches (pt wants Duragesic brand) + $12.00 pharmacy fee
Duragesic is $150.28 for 5 patches = $30.06/patch AAC = $30.06/patch x 7 patches = $210.42 Actual Rx cost = $210.42 + $12.00 = $222.42
2. Amount PharmaCare will pay pharmacy (NOTE: PharmaCare will only pay max $10.00 fee)
a. Zone X = $0 b. Zone Y = 0.70 [(amount needed x LCA price) + $10.00]
Example: Rx for 7 Duragesic patches with LCA price = $7.4345/patch = 0.70 [(7 patches x $7.4345/patch) + $10.00] = $43.43
c. Zone Z = (amount needed x LCA price) + $10.00
3. Amount credited to patient’s maximum
a. Zone X = (amount needed x LCA price) + $10.00 b. Zone Y = 0.30 [(amount needed x LCA price) + $10.00]
Example: Rx for 7 Duragesic patches with LCA price = $7.4345/patch
= 0.30 [(7 patches x $7.4345/patch) + $10.00] = $18.61
c. Zone Z = $0 4. Amount patient pays pharmacy = Actual Rx cost – amount paid by PharmaCare NOTE: fully covered drugs that only have a MAX PRICE listed = LCA price NOTE: fully covered drugs that have MAX PRICE & LCA price, PharmaCare covers lower cost NOTE: P* can become fully covered with special authority

3
RDP Calculations: RDP program applies to medications in 5 drug categories: H2RA; NSAIDs; oral nitrates; ACEIs; CCBs with each class having “reference drugs” from which the RDP pricing is set 1. Actual Rx cost = AAC + professional fee (NOTE: if pt reached maximum, pharmacy can only charge max $10.00 fee)
Example: Rx for 120 Pepcid 20 mg tabs, i BID with professional fee = $12.00 and pt wants brand name Pepcid is $34.23/28 tabs = $1.223/tab Actual Rx cost = (120 tabs x $1.223/tab) + $12.00 = $158.76
2. Amount PharmaCare will pay pharmacy (NOTE: PharmaCare will only pay max $10.00 fee)
a. Zone X = $0 b. Zone Y = 0.70 [(days supplied x RDP price) + $10.00]
Example: Rx for 120 Pepcid 20 mg tabs BID with RDP price $22.062/30 days = 0.70 [(60 days x $22.062/30 days) + $10.00] = $37.88
c. Zone Z = (days supply x RDP price) + $10.00
3. Amount credited to patient’s maximum
a. Zone X = (days supply x RDP price) + $10.00 b. Zone Y = 0.30 [(days supply x RDP price) + $10.00]
Example: Rx for 120 Pepcid 20 mg tabs BID with RDP price $22.062/30 days = 0.30 [(60 days x $22.062/30 days) + $10.00] = $16.24
c. Zone Z = $0 4. Amount patient pays pharmacy = Actual Rx cost – amount paid by PharmaCare NOTE: reference drugs are LCA program drugs, and you can adapt a Rx of a non-reference drug to the reference drug NOTE: if RDP Special Authority is given (P* drugs in the RDP program), then it becomes an LCA drug Modernized RDP program: in effect (Dec. 1, 2016)
• Adding 3 new drug categories: ARBs, PPIs, and statins (HMG-coA reductase inhibitors)
• Changes to reference drugs of: H2RA, ACEI, and CCB categories
• No changes: NSAIDs and oral nitrates PharmaCare plans: more info in PharmaCare summary table on Connect
• Fair PharmaCare: residents of BC who have valid MSP coverage
• Plan B: permanent residents of licensed residential care facilities
• Plan C: assistance from Ministry of Housing and Social Development
• Plan D: registered with a Cystic Fibrosis clinic
• Plan F: severely handicapped BC children in the “at home” program
• Plan G: registered with a mental health service center
• Palliative Care Benefits Program: palliative care at home certified by a physician
• BC Centre for Excellence in HIV/AIDs: enrolled in the Centre by a physician
• Methadone Maintenance Program: for opioid dependence

4
Drug Information / Therapeutics Resources:
Category Resource Brief Intro
General Resources
CPS Drug monographs arranged in alphabetical info by brand name (or generic if no brands)
• Green pages: brand & generic names
• Pink pages: classifying drugs by therapeutic indication
• White pages: identification (pictures)
• Symbols: Prescription (Pr), Controlled Drug (C), Narcotic (N), Targeted Substance (Tc)
DIH Brief information on drugs (PK, ADR, storage), alphabetical by generic name
• Dosing information and forms are American
Martindale Information of drugs used throughout the world
• Volume A: drugs grouped by similar uses and actions
• Volume B: general index & preparations used in different countries
Rx Files Drug comparison resource; reference at back for symbols
Natural Medicines Provides evidence for safety & efficacy of NHPs, including potential interactions
Merck Manual Discussions of medical conditions (pathophysiology, etiology, diagnosis & treatment)
Merck Index Drug monographs providing info on chemical property (molecular weight, chemical structure, physical data)
• 2 indexes: chemical formula or by brand/generic name
Drug Interactions
Stockley’s Drug Interactions
Start with Index to find the medication, and look under it for the interacting product to find the page number Drug Interactions
Binder
Special Populations
Pregnancy and Lactation
Briggs’ Drugs in Pregnancy & Lactation
Go to guide with evidence summaries
Medications & Mother’s Milk Drug monographs with infant monitoring points
Pediatric
Pediatric & Neonatal Handbook Similar to DIH (also American)
BC Children’s Hospital Pediatric Dosage Guidelines
Appropriate dosing for neonates (pink pages) and infants (yellow pages)
Geriatric
Geri-Rx Files For appropriateness of drugs used in older adults
Geriatric Dosage Handbook Similar to DIH (also American)
Anti-microbials
Bugs & Drugs Infectious diseases and Antimicrobial agents
• Yellow: antibiotic information (spectrum of activity, dosing)
• Blue: treatment recommendations
• Purple: dental
• Red: pregnancy/lactation
• Green: antimicrobial information
Sanford Guide to Antimicrobial Information
• Spectrum of activity chart
• Common indications chart
• Special populations (pediatrics, patients with decreased kidney function)
• Resistance patterns, dosing, abx availabilities = American
Institutional or Hospital
Handbook on Injectable Drugs
• Monographs organized by generic names (storage info, reconstitution info, routes)
• Compatibility information: in various solutions, with other drugs at Y site, with other drugs in IV solutions or syringes
Drug Prescribing in Renal Failure
• Drugs grouped into adult and pediatric tables based on drug class
• Comprehensive index at back
• Abbreviation definitions on pg. 16
5
Pharmacy Regulations: Drug Scheduling:
• Schedules and regulations: o Schedule 1 = Prescription o Schedule 1A = Controlled Prescription Program o Schedule 2 = Professional Services Area (no public access or opportunity for pt self-selection) o Schedule 3 = Professional Products Area (OTC must be visible and within 25 ft of the dispensary) o Schedule 4 = Emergency contraception (pharmacists can prescribe) o Unscheduled = non-pharmacy sale
• If asked about drug scheduling, go to the Drug Schedule Regulations in Tab 4 (Drug Distribution) of College Binder o Generic names: if given brand name, need to use CPS o Combination products: follow the most restrictive drug schedule
▪ Ex// ratio-Emtec-30 = APAP (unscheduled) + codeine 30 mg (schedule 1) = overall schedule 1 o Exempted product: codeine ≤ 8 mg or ≤ 20mg/30 mL + 2-3 medicinal (non-narcotic) ingredients = schedule 2 o New updates: check the pages following Drug Schedule Regulations for updates or changes to scheduling o Drug not on list: it is unscheduled, but be careful because some categories may be broad
▪ Ex// testosterone is not listed but falls under the category of sex hormones (schedule 1) Prescription Regulations:
• If asked about prescription requirements, refills, sales record and other files and records, go to the “Prescription Regulations” table in Tab 4 (Drug Distribution) of College Binder
Scope of practice and prescribing:
• Prescribing limitations: o MD, vets (species-specific), DDS: narcotics, controlled drugs, prescription drugs o Podiatrists: benzodiazepine and prescription drugs o Pharmacists: schedule 4 drugs o Optometrists: topical ophthalmics o Midwives, NDs, NPs: prescription drugs (see CPBC for scope)
• If asked about scope of prescribing for other HCPs, check for “Prescribing Schedules” or “Scope of Practice” documents in Tab 4 (Drug Distribution) of College Binder
Prescription Adaptations: “PPP-58 Orientation Guide” in Tab 3 (Legislation) of College Binder (Amendment to “Professional Practice Policies” NOTE: does not apply to narcotics, controlled drugs or targeted substances
• Change: changing dose, formulation, or regimen of a prescription to enhance patient outcomes ($10) o Can’t change dose or regimen for Rx for: cancer, CV disease, asthma, seizures or psychiatric conditions o Can complete missing information (even for above diseases) on a Rx if there is historical evidence
• Regimen: renewing a prescription for continuity of care ($10) o For stable, chronic conditions (same medication with no change for minimum of 6 months) o No psychiatric meds unless on a multi-disciplinary team o Renewals can’t exceed expiry of the prescription
• Substitution: making a therapeutic drug substitution within the same therapeutic class for a prescription ($17.10) o Limited to 8 therapeutic classes of medications: H2RAs, NSAIDs, nitrates, ACEI/ARBs, DHP CCBs, PPIs, statins
Drug Interchangeability: examples: brand generics; capsules suspensions (NOT creams and ointments) Emergency Refills (PPP-31): “Professional Practice Policies” in Tab 3 (Legislation) of College Binder
• To ensure continuity of care (try to renew under PPP-58 before deferring to PPP-31)
• Emergency refills can be provided without access to prescription (evidence such as an empty rx vial, a label, or a copy of the rx receipt is sufficient)
• Pharmacist providing the emergency refill is named as the prescriber on the prescription label & patient’s medication profile (not required to notify original prescriber)

6
Medication Reviews: under “PharmaCare Policy Manual: Medication Review Services, Section 8.9” MR-S: $60 MR-PC: $70 MR-F: $15 Eligibility criteria:
• BC resident, have a BC PHN, not covered under PharmaCare Plan B
• At least 5 different qualifying meds (Schedule 1 Rx medication or insulin) entered onto PharmaNet within the last 6 months and before the med review is provided
• Clinical need for service: o Prescriber requested medication review o Patient has multiple diseases, one or more chronic diseases o Patient’s medication regimen includes one or more NHP o Patient has a DTP o Patient recently discharged from hospital o Patient has multiple prescribers o Patient is receiving med(s) that require lab monitoring
• Not exceed max allowable (max 1 MR-S or MR-P per 6 months and max 4 MR-F per 12 months)
• Sign acknowledgement on Best Possible Medication History Form Resolution of DTPs:
Necessary • Unnecessary drug therapy
• Needs additional therapy
Effective • Ineffective drug
• Dosage too low (dose, dosing interval, drug interactions)
Safety • Adverse drug reaction
• Dosage too high (dose, dosing interval, drug interactions)
Adherence • Identify reason (cost, route, timing, etc) Changing Rx: reason, v/o, dr’s name, date, your initials Other tidbits :
• CrCl (mL/min) = [ 140−𝑎𝑔𝑒
𝑆𝐶𝑟 x 90 ] (x 0.85 if female)
• Recommendations and OTC selections Dose Max
Acetaminophen < 12 years old 10 – 15 mg/kg/dose po q4-6h prn 65 mg/kg/24 h
≥ 12 years old 325 – 650 mg po q4-6h prn 4000 mg/24 h
Ibuprofen < 2 years old 5 mg/kg/dose po q6-8 h prn 40 mg/kg/day
2 – 12 years old 5-10 mg/kg/dose po q6-8 h prn 40 mg/kg/day
> 12 years old 200 mg po q4h prn OR 400 mg po q6-8 h prn 1200 mg/24 h
Osteoporosis Calcium 1200 mg Vitamin D 800 IU
Tech Check: PQRSD3E
• Label (check for spelling errors/typos as well): o Patient o Doctor o Drug o DIN o Auxiliary labels
o Quantity (mitte) – includes calculations o Sig o Refills o Dosage form
• Product: drug, DIN, expiry, dosage forms REVIEW METHADONE AND SUBOXONE TECH CHECKS
• Expiry of formulations: o Non-aqueous: earliest expiry date of any API or 6 months, whichever is earlier o Water-containing oral: 14 days at room temperature o Water-containing topical/dermal; mucosal liquid; semi-solid: 30 days

7
Opioid Management
Clinical scenario Tolerance Dependence Addiction
Short-term Low risk MANGEABLE
Low risk PROBLEMATIC
Low risk PROBLEMATIC
Long-term High risk PROBLEMATIC (need dosage increase)
High risk PROBLEMATIC
High risk PROBLEMATIC
Palliative High risk EXPECTED
High risk MANAGEABLE
Addiction PROBLEMATIC
• Do not adjust daily dose when switching dosage forms of same drug o EXCEPT: reduce codeine phosphate by 25% when switching to codeine contin (240 mg PO4 180 mg contin)
• Reduce dose of new opioid by 25-50% when switching, depending on: clinical scenario, frailty of patient, supervision level of patient’s environment, relative potency of new opioid, original dose, available dosage forms
• Mix of long-acting and short-acting in regimen design o Chronic pain: 75 – 80% of total daily dose as long-acting, with remainder as short-acting o Cancer/palliative pain: breakthrough doses to be in addition to long-acting product
▪ Size of breakthrough dose is typically 10-15% of daily dose at each dose ▪ Regular use of > 3 BT doses per day indicates regimen should be adjusted (although occasional use of
more is fine if reasoning clear) Opioid Rotation
• Same as any other opioid conversion – reduce dose by 25 – 50% Opioid Taper
• Doses can be reduced by 5-20% (or more) depending on scenario: o Community environment: 10% per week (or even month) or slower o Highly supervised environment: 10-30% per week or more o Institutionalized detox facility: highly variable (50% or more)
• Taper usually needs to be slowed as taper progresses – slow rate by 50% once patient reaches 30% of original dose Opioid Monitoring: Pasero Opioid-induced sedation scale
• S = sleep, easy to arouse
• 1 = awake and alert
• 2 = slightly drowsy, easily aroused
• 3 = frequently drowsy, arousable, drifts off to sleep during conversation
• 4 = somnolent, minimal or no response to stimuli Opioid Constipation
• If no BM for > 3 days (after expected BM): soften AND stimulate
• Prevention on opioids: stimulate +/- soften
• Regular, but hard: PEG/lactulose + increased fluid intake
• Irregular, but soft and without pain: no treatment required Transdermal Fentanyl Dosing: not for opioid naïve (only use for pts already receiving ≥ 60 mg/day morphine equivalents) 1. Duragesic Monograph Approach
a. Estimate daily ORAL morphine equivalence. DO NOT account for incomplete cross-tolerance. b. Select Duragesic dose based on provided table. (Morphine ranges are very broad = likely too low for 50% of pts) c. Titrate dosage up every 3-6 days until analgesic efficacy is reached.
2. Nomogram (ex// Fraser Health)
• Don’t use 12 patch by itself (it’s for titrating only)
• Nomograms are unidirectional!
• Provides information on recommended dose and schedule for the switch, also breakthrough pain doses
8
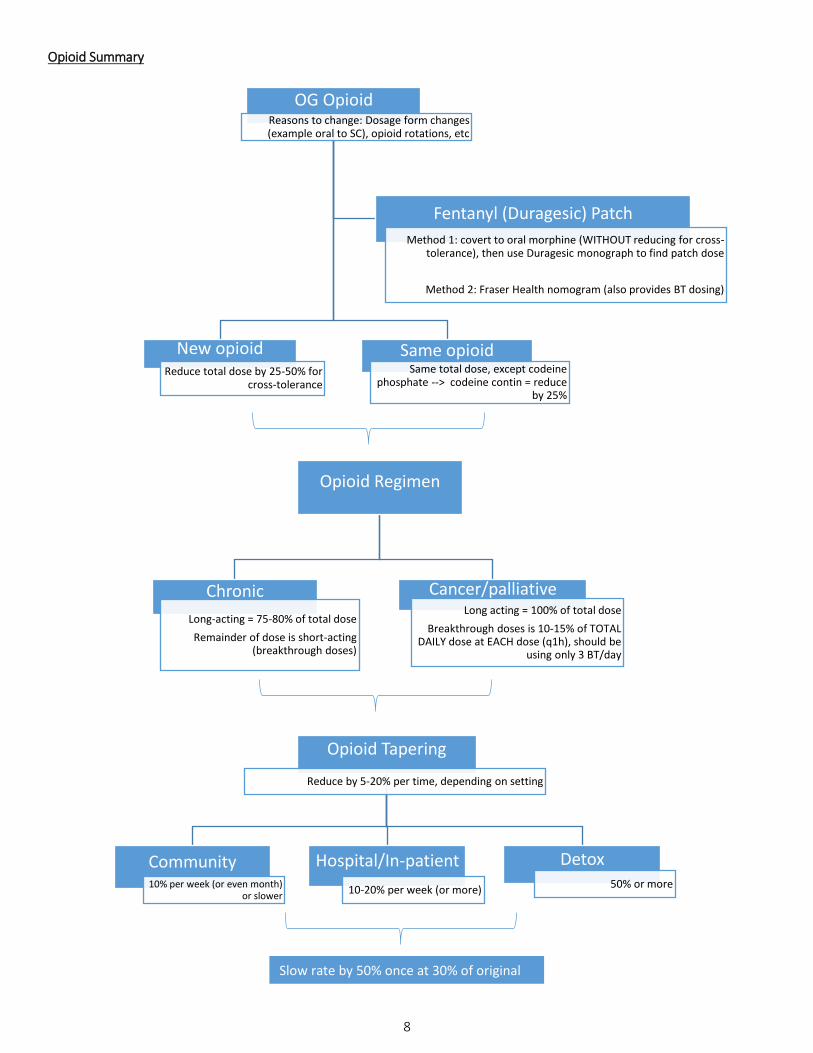
Opioid Summary
OG OpioidReasons to change: Dosage form changes (example oral to SC), opioid rotations, etc
Same opioidSame total dose, except codeine
phosphate --> codeine contin = reduce by 25%
New opioid Reduce total dose by 25-50% for
cross-tolerance
Fentanyl (Duragesic) Patch
Method 1: covert to oral morphine (WITHOUT reducing for cross-tolerance), then use Duragesic monograph to find patch dose
Method 2: Fraser Health nomogram (also provides BT dosing)
Opioid Regimen
Chronic
Long-acting = 75-80% of total dose
Remainder of dose is short-acting (breakthrough doses)
Cancer/palliative Long acting = 100% of total dose
Breakthrough doses is 10-15% of TOTAL DAILY dose at EACH dose (q1h), should be
using only 3 BT/day
Opioid Tapering
Reduce by 5-20% per time, depending on setting
Detox50% or more
Hospital/In-patient
10-20% per week (or more)
Community10% per week (or even month)
or slower
Slow rate by 50% once at 30% of original dose
9
Benzodiazepine Tapers
• General rates are 5-20% every 2 weeks in a community setting (or slower!!!)
• Longer acting BZDs easier to taper, switch from original BZD to: diazepam (young & healthy) or lorazepam (hepatic impairment or geriatric)
o Direct switching from BZD to BZD is poorly tolerated – can transition or cross-over from one BZD to the other Tools (click for link):
• MSE (summary): Mental Status Exam o 5 components: appearance and behavior; speech & language; mood; thoughts & perception; cognition
• PHQ-9 : Patient Health Questionnaire (self-reported) o Diagnostic tool for depression:
▪ Q1+Q2 = one or both should be rated as 2-3 ; Q1 – Q9 = ≥ 5 boxes within shaded section
• Scoring: minimal = 1-4; mild = 5-9; moderate = 10-14; moderately severe = 15-19; severe = 20-27 ▪ Q10 = “somewhat, very or extremely difficult”
• GAD-7 : Generalized Anxiety Disorder Questionnaire (self-reported) o Screening tool for anxiety (NOT diagnostic)
▪ Question 1-7 scoring: minimal = 0-4; mild = 5-9; moderate = 10-14; severe = 15-21 ▪ Question 8 assess impairment “somewhat, very, or extremely difficult”
• BPRS : Brief Psychiatric Rating Scale o Tests positive, negative, and affective sx; useful for monitoring (most useful in mod-severe psychoses) o Some items are self-reported, some observed (# 3, 4, 6, 7, 13, 14, 16, 18)
• AIMS: Abnormal Involuntary Movement Scale (clinician reported) o Conduct entire exam prior to scoring patient; rate highest amplitude or frequency observed o Positive score for tardive dyskinesia= score of 2 in ≥ 2 movements or score of 3-4 in a single movement
▪ Don’t total scores (score of 1 in 4 movements ≠ positive score of 4)
• CIWA : Clinical Institute Withdrawal Assessment (clinician reported) o Incorporate vital signs into assessment o CIWA-Ar score: mild = 0-9; moderate = 10-19; severe = ≥ 20
• Diabetic Foot o Use the highest (L vs. R) for total score and follow-up accordingly
▪ 0-6 = annual; 7-12 = every 6 m; 13-19 = every 3 m; 20-25 = every 1-3 m
• Brief Pain Inventory o Pain score: average the scores from questions 3-6 o Functional Score: average the scores from question 9 (A-G)

10
INTERACTIVE STATIONS Patient Counselling
• Introduction: name, patient identifier, offer to counsel, explain purpose, state time factor
• Background information: SCHOLAR-MAC, preg/breastfeeding, what did dr tell you
• Medication: name (brand & generic), type/purpose, sig, supply (mitte), refills
• Side effects: important SES, how to manage them, what to do if they don’t go away
• Interactions: identify and explain interactions, recommend rx/doc consult for new Rx/OTC/NHPs
• Storage: RT (or fridge), KOOROC, cleaning
• Self-monitoring/follow-up: what & when to expect, what to do if no effects, OTC/non-drug measures, phone pt
• Conclusion: summarize and check pt’s understanding
Dosage Forms Counselling: MAIN POINTS (always check product insert or box for special instructions)
Rectal Suppository: info from IA #1 (PY1 term 2)
• If suppository is soft, hold under cool water to harden it
• Cut suppository in half lengthwise with a clean, single-edge razor blade
• Can use finger cot or disposable glove
• Lie on side with lower leg straightened out & upper leg bent forward towards stomach; lift upper buttock to expose
rectal area
• Insert suppository (pointed end first) with your finger (can use finger cot/disposable glove) until it passes muscular
sphincter of rectum (1/2 to 1 in infants, 1 in for adults) and then hold buttocks together for a few seconds
• Remain lying down for about 15 mins to avoid the suppository from coming out
Vaginal Suppository/Cream: info form IA #1 (PY1 term 2)
• Ask woman if she is comfortable using a tampon and/or if she has used a tampon (technique is the same)
• Suggest ways of inserting: seated on a toilet; standing with one leg on toilet seat or on side of bath tub; lying down
similar to rectal
• Insert applicator deep into vagina, as far as comfortable without force, then depress plunger slowly & remove
applicator from vagina
• Recommend to use at bedtime to reduce vaginal leakage; also can use napkin or pad to protect clothing
• Can use these products while menstruating and pregnant (in pregnancy use lower concentrations to be safe)
Eye Drops: info from e-CTC
• Shake well if medication is a suspension
• Tilt head back or lie down, keeping both eyes open, gently pull lower eyelid of the affected eye down to form a pouch
• Hold the bottle almost horizontally and bring it up to your eye from the side, holding the tip about 2.5 cm (1 in) away
from the eyelid
• Look upwards by moving your eyes only and put one drop into the pouch of the lower eyelid
• Look down for several seconds, slowly release the lower lid and then gently close the eyes for 30 secs – 5 mins
• Can press gently on side of bridges of nose with thumb and index finger to help keep med from going down tear duct
• Wait 3-5 mins between drops of the same medication, 5-10 mins before applying a drop of another medication

11
Nasal spray: info from CTMA pg. 193
• Shake well if medication is suspension
• With your head upright but not tilted backward, press your finger against one side of your nose to close the nostril
• Spray the medication into the open nostril, with the tip directed away from the middle of the nose and back towards
the nostril cavity, and breathe in slowly through the nose
• Remove nasal spray from nostril and breathe out through the mouth
• Repeat on other side (nostril) and then blow nose in 3-5 mins
Eardrops: info from CTMA pg. 165
• Warm eardrops to body temperature by holding the bottle in your hands for a few minutes
• Shake well if medication is suspension
• Tilt your head or lie on your side so the ear you are treating is facing up, then straighten the ear canal
o Adults and children > 3 yo: gently pull the top of the ear up and back
o For children < 3 yo: gently pull the top of the ear down and back
• Hold the dropper above the ear and place the prescribed number of drops into the ear, and stay in the same position
for 3-5 minutes after using the drops
• Wait 5-10 mins before putting drops in the second ear (as you would have to tilt your head the other way)
Transdermal Patch:
• Wash hands before and after applying (but do not use soap)
• Leave patch in packet/foiled pouch, until you are ready to apply it; DO NOT CUT PATCH
• Apply to dry, non-hairy, clean, non-irritated (no cuts, scrapes, pimples, etc) skin areas
• Remove old patch (press adhesive sides together to stick and dispose safety) and replace with new patch (if
appropriate) on a different site (rotate sites to prevent irritation and impaired absorption; can re-use sites in a week)
Inhalers: info from The Lung Association documents posted on Connect
• Breathe out before placing mouthpiece in mouth
• Hold breath for 5-10 seconds before breathing out again
• Wait 1 minute between doses
• Rinse mouth (and face if using face mask) if using a steroid
MDI • Prime inhaler before first use or if it’s been dormant
• Shake inhaler (except QVAR or Alvesco)
• Breathe in slowly and deeply as you depress the canister
CARE: remove med canister from plastic casing & wash casing with warm, soapy water (once a week)
MDI with
spacer or
face mask
• Same preparation as above (prime and shake)
• With spacer/face mask on, breathe out, depress canister into spacer, and breathe in slowly & deeply
CARE: wash plastic casing of MDI (remove med canister) & spacer/face mask with warm, soapy water
Diskus • Keep device horizontal, push thumb grip open and slide lever until “click” is heard
• Breathe in quickly, deeply, and steadily
CARE: wipe mouthpiece with dry cloth/tissue. Store in dry place (away from heat/sun) and keep thumb
grip closed until ready to use
Turbuhaler • Twist cap counter-clockwise to remove; then turn colored base as far as possible in one direction,
and then turn back in the opposite direction until “click” is heard
• Breathe in quickly and deeply (FORECEFUL INHALATION)
CARE: clean mouthpiece using dry cloth/tissue

12
Twisthaler • Twist cap counter-clockwise to remove – DOSE IS ALREADY LOADED and ready to use
• Breathe in fast and deep
• Twist clockwise to close cap until a “click” is heard (this LOADS THE NEXT DOSE)
CARE: clean mouthpiece using dry cloth/tissue
Respimat ASSEMBLY: with cap closed, press safety catch to remove clear base of inhaler. Push narrow end of med
cartridge into inhaler as far as it will go. Place inhaler upright on flat surface and push finger down on
cartridge (to go all the way in). Put clear base back into place. Once assembled, do not take apart.
• Prime 3 times before use (i.e. twist 3 times)
• TOP (turn, open, press):
o Turn: with cap closed, turn base a half-turn in direction of black arrow until it clicks.
o Open: cap until it snaps fully back
o Press: dose release button while taking a slow, deep breath and continue to breathe in
• Make sure not to cover air vents with fingers
CARE: wipe mouthpiece inside and out with a damp cloth (once a week)
Breezhaler • Pull cap off and tilt mouthpiece to open inhaler; place capsule in chamber & close until it “clicks”
• Press both buttons once and release to pierce capsule
• Breathe in rapidly and slowly. Repeat inhalation to ensure entire capsule is inhaled
CARE: wipe mouthpiece with dry cloth/tissue
Handihaler • Open lid and mouthpiece, place capsule in centre chamber, and close mouthpiece until it “clicks”
• Press green button once and release to pierce capsule
• Breathe in slowly and deeply. Repeat inhalation to ensure entire capsule is inhaled
CARE: open lid, lift up mouthpiece and piercing button to open base; rinse with warm water; air dry
Ellipta • Breathe in long, steady, and deep breath
CARE: when ready to use, peel back lid to open foil tray. Write “TRAY OPENED” and “DISCARD” (6 weeks
from date tray is opened) dates on inhaler. Mouthpiece can be cleaned with dry cloth/tissue
Genuair • Press green button once (should be facing patient) and release (check color control window is green)
• Breathe in strongly and deeply, and continue breathing even after you hear a “click”
• Check color control window is red, if not repeat inhalation
CARE: wipe mouthpiece with dry tissue/cloth
Nebulizer • Ensure nebulizer is plugged in, and attach tubing to air outlet
• Unscrew top of medication cup, fill it with dose, and screw on the top
• Turn on compressor and ensure medication is misting
• Place mask on face our mouthpiece in mouth and breathe in and out slowly through mouth
CARE: wash mask and nebulizer medication chamber in warm, soapy water; air-dry before use
13
Diabetes pens:
• Pick correct pen with type of insulin (insulin is not interchangeable between brands)
o Humulin line = Luxura; Novolin line = Novolin Pen; Sanofi insulin = ClikSTAR Pen
o Just match brand name on insulin vials to the pen
• Pick an injection site (fastest absorption abdomen > back of arms > outer thighs > upper buttocks)
o Rotate injection sites daily within that area to prevent fatty lumps from forming
o Avoid injection within 2-inch area around belly button, and don’t inject into scar tissue
• For each new cartridge, dial up a couple of units to ensure that insulin is “primed” or “loaded”
• Try shortest and thinnest gauge needle (4 mm, 32G first); pinching of skin prior to injection not necessary
o Needles are interchangeable EXCEPT NovoTwist needles
o Only use once, and dispose in sharps container
• Soap and water sufficient to clean skin (alcohol not needed)
• If insulin is a suspension, it needs to be “shaken” (by rolling insulin in hands or moving in an up/down motion)
• Inject at a 90o angle and hold for 10 seconds
• Remove insulin cartridge (from pen) if it has been > 28 days from first use, expired, discolored, or empty
Other resources for counselling stations:
• Doctor Requests / Recommendations
• Physical assessment checklists (check Appendix VI)