nodular adenomatosis of iris pigment epithelium
TRANSCRIPT

Nodular Adenomatosis of Iris Pigment Epithelium
Mark o. M. Tso, M.D., Morton F. Goldberg, M.D., and Joel Sugar, M.D.
A 62-year-old man manifested multiple nodulargrowths in his left iris and unilateral glaucoma.Detailed clinical and pathologic studies showedthat these lesions were adenomas derived from thespurs of Fuchs, Michel, and Grunert in the irispigment epithelium. We suggest terming this newlydescribed entity nodular adenomatosis of the irispigment epithelium and propose a classification ofprimary neoplastic lesions of the iris.
PRIMARY NEOPLASTIC LESIONS of the iris differentiate in a variety of ways, depending on their derivation from the neural crest, neural ectoderm, or softtissue stroma.>' From the neural cresr'" develop thenormal iris stromal melanocytes, as well as freckles,nevi, and malignant melanomas. From the neuraltube,1-4·1O the medullary epithelium differentiatesinto the anterior and posterior layers of iris pigmentepithelium, the smooth muscle of the dilato andsphincter muscles, the spurs of Fuchs, Michel, andGrunert, and the clump cells of Koganei (type II) andneoplastic lesions of these structures. 3,11-20 Neoplasms of neural crest origin are common. Neoplasticlesions derived from the neural tube are infrequentlyseen, but they show a broad spectrum of differentiation.
We describe the clinical features of a patient inwhom multiple neoplastic proliferations arose fromthe spurs of Fuchs, Michel, and Grunert in the irispigment epithelium, and the light and electron microscopic features of the lesions. We do not believethat this entity has been described previously in theliterature and propose to term it nodular adenomatosis of the iris pigment epithelium.
Case Report
A 62-year-old white man complained of blurredvision in his left eye that was of recent onset. His
From the Department of Ophthalmology, University of Il1inoisat Chicago, Eye and Ear Infirmary, Chicago, Illinois. This studywas supported in part by core grant IP30EY01792 from theNational Eye Institute.
Reprint requests to Mark O. M. Tso, M.D., Department ofOphthalmology, University of Il1inois Eye and Ear Infirmary,1855 W. Taylor si.. Chicago, IL 60612.
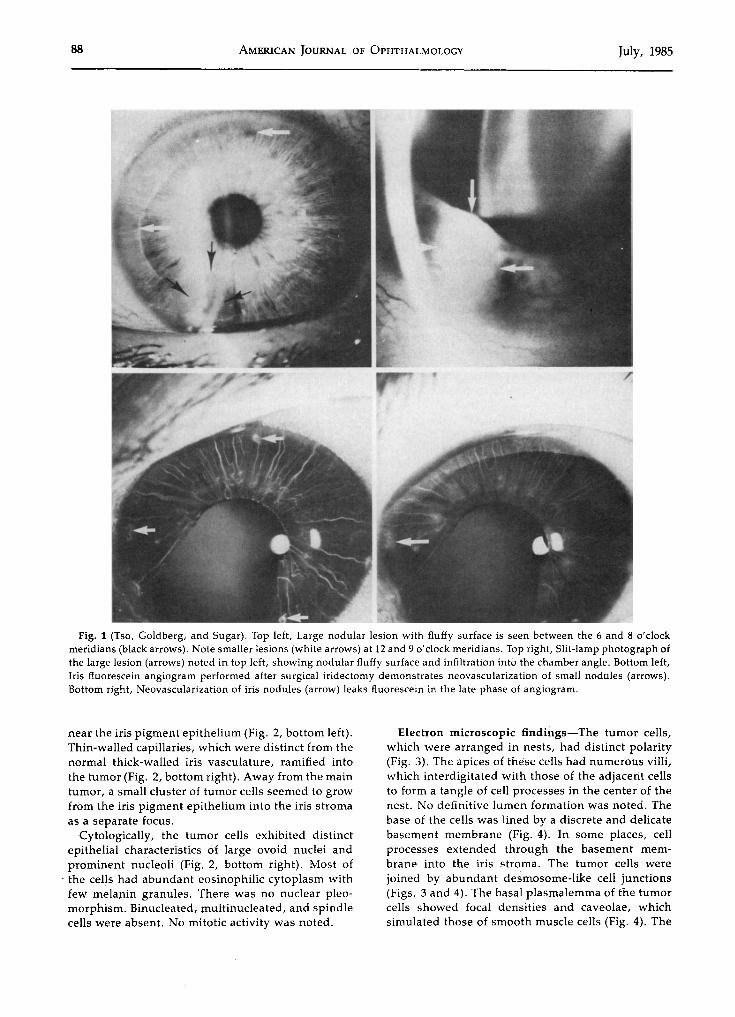
visual acuity was R.E.: 20/20 and L.E.: 20/30. Multiple small, honey-colored, nodular lesions (Fig. 1)were noted on the anterior surface of the iris at the12, 3, and 9 o'clock meridians. One large nodule,located between the 6 and 8 o'clock meridians, measured approximately 3 mm in diameter and infiltrated the anterior chamber angle. Multiple smaller pigmented lesions also were observed in the inferiorhalf of the chamber angle. A slit-lamp examinationshowed the lesions to be semitransparent with afluffy surface. The base of these tumors seemed tooriginate from the deep stroma of the iris. Fineneovascularization with capillary loops ramified intothe tumor nodules. In the right eye, only small, flat,pigmented iris freckles were observed, and the results of gonioscopic, fundus, and visual field examinations were normal.
The intraocular pressure, obtained by applanationtonometry, was R.E.: 13 mm Hg and L.E.: 22 mm Hg.Ophthalmoscopy disclosed a pale and totally cuppedleft optic disk. Goldmann visual fields showed adense inferior centrocecal scotoma on the left with asuperonasal step extending to fixation. The patientwas referred to an internist for systemic examinationfor a possible primary neoplasm with metastasis tothe eye. A chest roentgenogram, upper and lowergastrointestinal tract contrast studies, an intravenous pyelogram, bone and thyroid scans, and agallbladder series were normal.
A left-sector iridectomy was performed betweenthe 6 and 8 o'clock meridians to include the large anda smaller lesions. A fluorescein angiogram of the irisperformed after the surgical excision demonstratedlate leakage from the neovascularization of the remaining nodules. Six years after iridectomy, thelesions remained unchanged and the intraocularpressure of the left eye was controlled medically by aregimen of pilocarpine and timolol maleate.
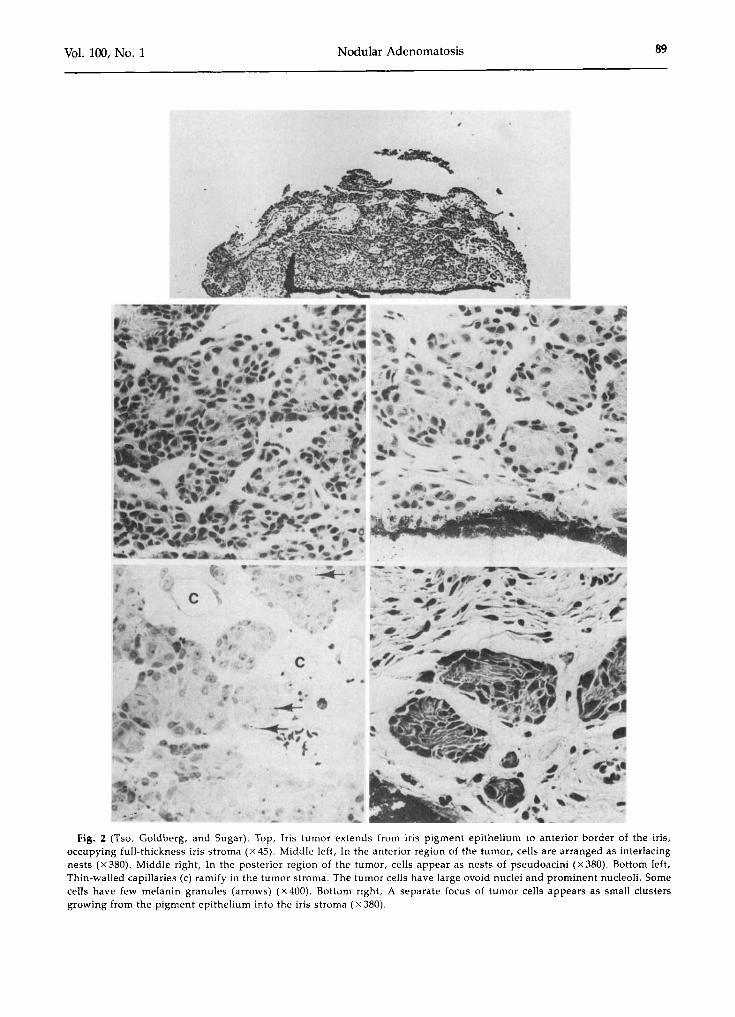
Light microscopic findings-A large tumor extended from the iris pigment epithelium through thefull-thickness iris stroma to the anterior border ofthe iris (Fig. 2, middle left). In the anterior region ofthe tumor, the cells were arranged as interlacingnests (Fig. 2, middle right), and the connective tissue stroma was eosinophilic and fibrillary. Deep inthe iris stroma, the tumor cells were arranged asdiscrete nests of pseudoacini (Fig. 2, bottom left). Afew isolated tumor cells were scattered in the stroma
©AMERICAN JOURNAL OF OPHTHALMOLOGY 100:87-95, JULY, 1985 87
88 AMERICAN JOURNAL OF OPHTHALMOLOGY July, 1985
Fig. 1 (Tso, Goldberg, and Sugar). Top left, Large nodular lesion with fluffy surface is seen between the 6 and 8 o'clockmeridians (black arrows). Note smaller lesions (white arrows) at 12 and 9 o'clock meridians. Top right, Slit-lamp photograph ofthe large lesion (arrows) noted in top left, showing nodular fluffy surface and infiltration into the chamber angle. Bottom left,Iris fluorescein angiogram performed after surgical iridectomy demonstrates neovascularization of small nodules (arrows).Bottom right, Neovascularization of iris nodules (arrow) leaks fluorescein in the late phase of angiogram.
near the iris pigment epithelium (Fig. 2, bottom left).Thin-walled capillaries, which were distinct from thenormal thick-walled iris vasculature, ramified intothe tumor (Fig. 2, bottom right). Away from the maintumor, a small cluster of tumor cells seemed to growfrom the iris pigment epithelium into the iris stromaas a separate focus.
Cytologically, the tumor cells exhibited distinctepithelial characteristics of large ovoid nuclei andprominent nucleoli (Fig. 2, bottom right). Most of
. the cells had abundant eosinophilic cytoplasm withfew melanin granules. There was no nuclear pleomorphism. Binucleated, multinucleated, and spindlecells were absent. No mitotic activity was noted.
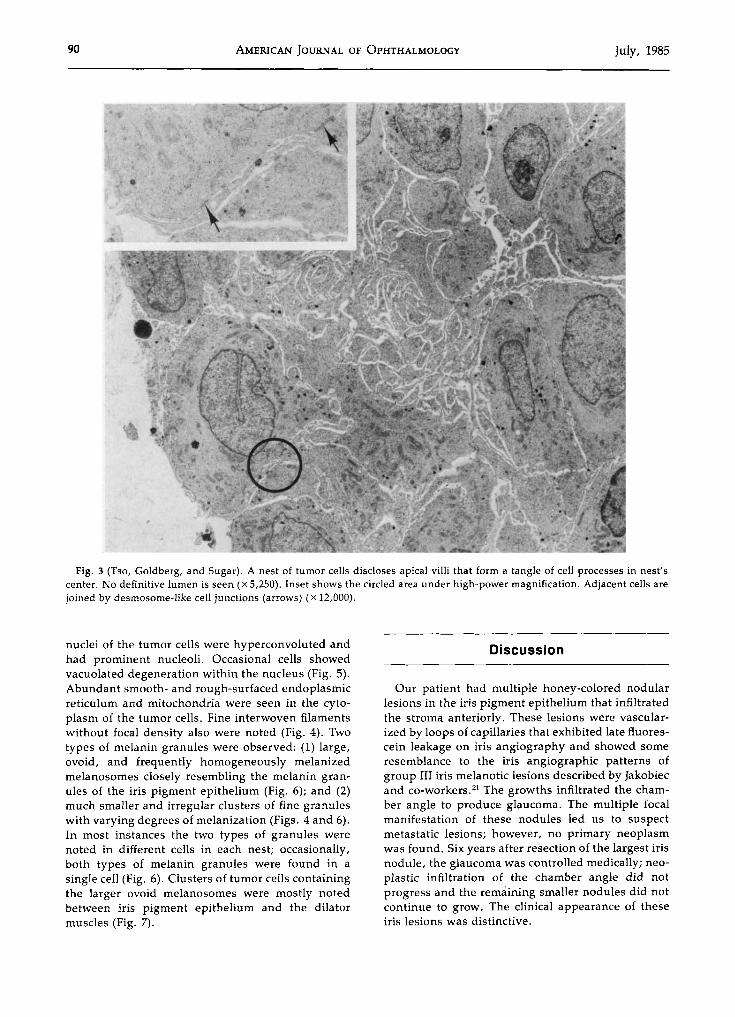
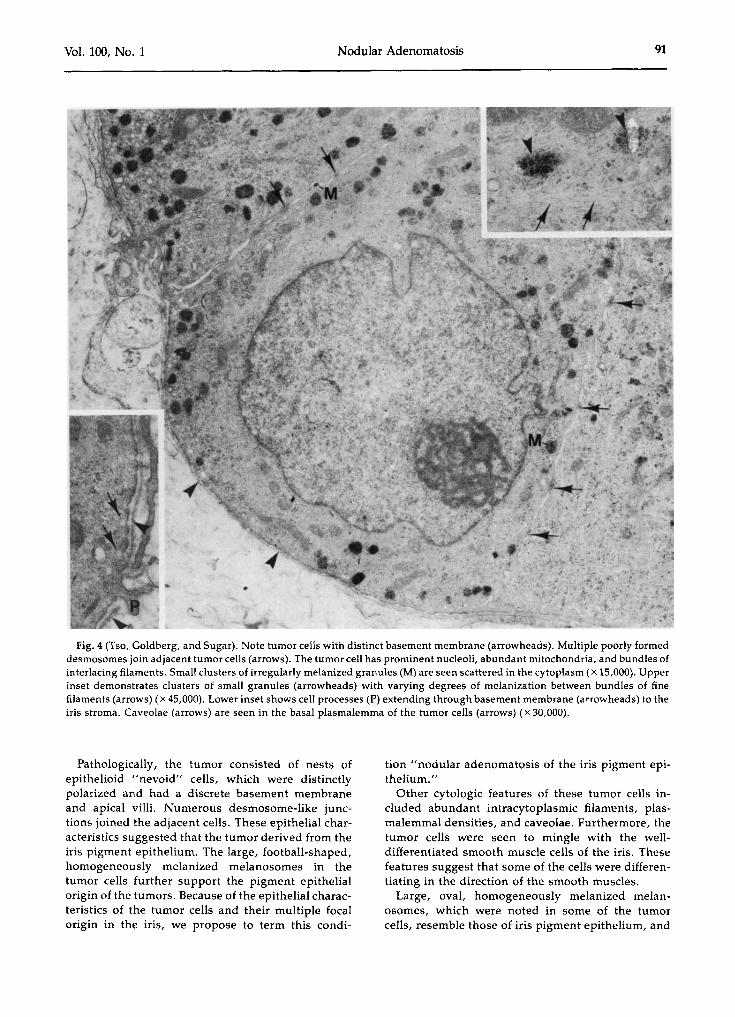
Electron microscopic findings-The tumor cells,which were arranged in nests, had distinct polarity(Fig. 3). The apices of these cells had numerous villi,which interdigitated with those of the adjacent cellsto form a tangle of cell processes in the center of thenest. No definitive lumen formation was noted. Thebase of the cells was lined by a discrete and delicatebasement membrane (Fig. 4). In some places, cellprocesses extended through the basement membrane into the iris stroma. The tumor cells werejoined by abundant desmosome-like cell junctions(Figs. 3 and 4). The basal plasmalemma of the tumorcells showed focal densities and caveolae, whichsimulated those of smooth muscle cells (Fig. 4). The
Vol. 100, No. 1 Nodular Adenomatosis 89
,
....·n,
*
,~ .i~. I'.~,h~~
.~ ~ ...:-::~~:~~.},.... ~_. ----Fig. 2 (Tso, Goldberg, and Sugar). Top, Iris tumor extends from iris pigment epithelium to anterior border of the iris,
occupying full-thickness iris stroma (X 45). Middle left, In the anterior region of the tumor, cells are arranged as interlacingnests (x380). Middle right, In the posterior region of the tumor, cells appear as nests of pseudoacini (x380). Bottom left,Thin-walled capillaries (c) ramify in the tumor stroma. The tumor cells have large ovoid nuclei and prominent nucleoli. Somecells have few melanin granules (arrows) (x 400). Bottom right, A separate focus of tumor cells appears as small clustersgrowing from the pigment epithelium into the iris stroma (x 380).
90 AMERICAN JOURNAL OF OPHTHALMOLOGY July, 1985
Fig. 3 (Tso, Goldberg, and Sugar). A nest of tumor cells discloses apical villi that form a tangle of cell processes in nest'scenter. No definitive lumen is seen (X 5,250). Inset shows the circled area under high-power magnification. Adjacent cells arejoined by desmosome-like cell junctions (arrows) (x 12,000).
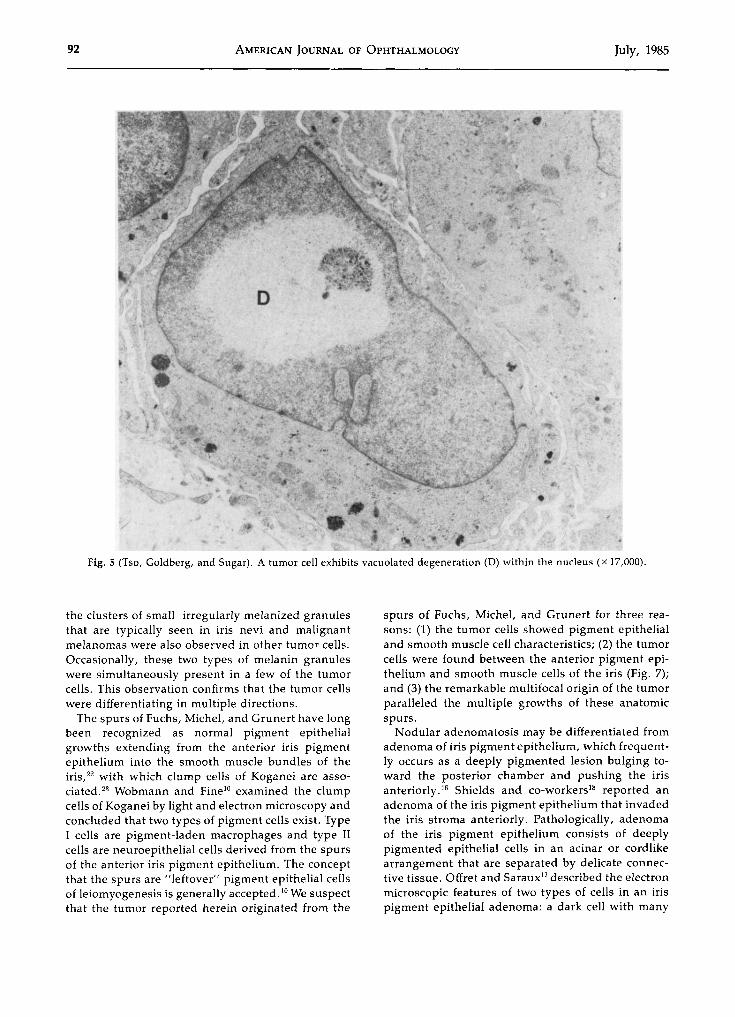
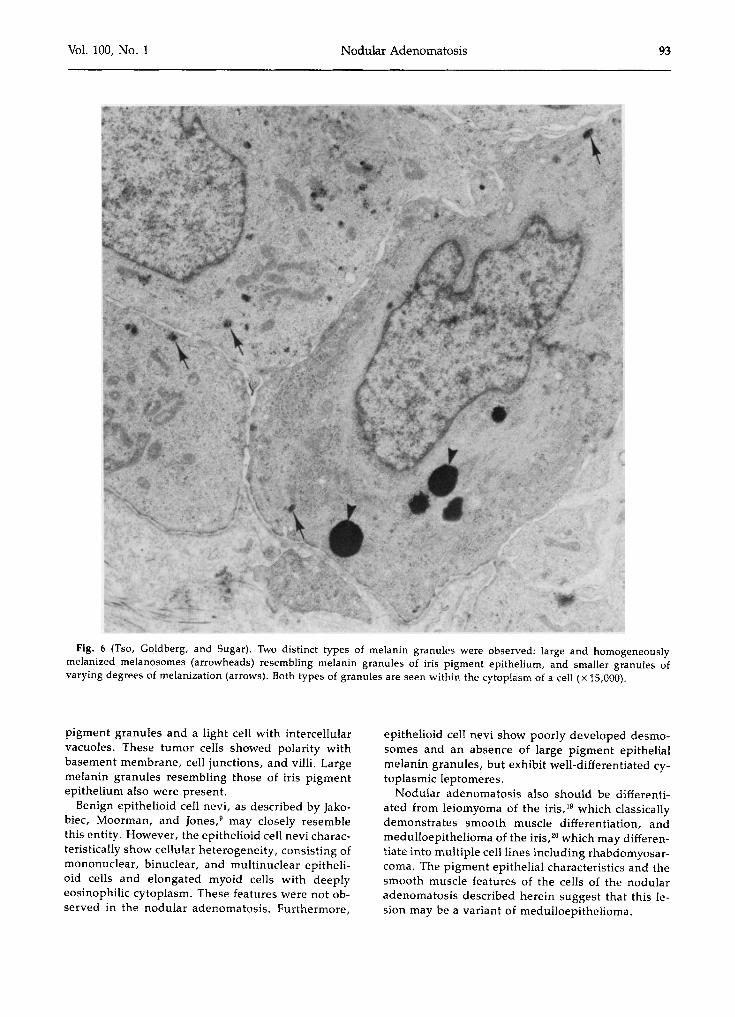
nuclei of the tumor cells were hyperconvoluted andhad prominent nucleoli. Occasional cells showedvacuolated degeneration within the nucleus (Fig. 5).Abundant smooth- and rough-surfaced endoplasmicreticulum and mitochondria were seen in the cytoplasm of the tumor cells. Fine interwoven filamentswithout focal density also were noted (Fig. 4). Twotypes of melanin granules were observed: (1) large,ovoid, and frequently homogeneously melanizedmelanosomes closely resembling the melanin granules of the iris pigment epithelium (Fig. 6); and (2)much smaller and irregular clusters of fine granuleswith varying degrees of melanization (Figs. 4 and 6).In most instances the two types of granules werenoted in different cells in each nest; occasionally,both types of melanin granules were found in asingle cell (Fig. 6). Clusters of tumor cells containingthe larger ovoid melanosomes were mostly notedbetween iris pigment epithelium and the dilatormuscles (Fig. 7).
Discussion
Our patient had multiple honey-colored nodularlesions in the iris pigment epithelium that infiltratedthe stroma anteriorly. These lesions were vascularized by loops of capillaries that exhibited late fluorescein leakage on iris angiography and showed someresemblance to the iris angiographic patterns ofgroup III iris melanotic lesions described by Jakobiecand co-workers." The growths infiltrated the chamber angle to produce glaucoma. The multiple focalmanifestation of these nodules led us to suspectmetastatic lesions; however, no primary neoplasmwas found. Six years after resection of the largest irisnodule, the glaucoma was controlled medically; neoplastic infiltration of the chamber angle did notprogress and the remaining smaller nodules did notcontinue to grow. The clinical appearance of theseiris lesions was distinctive.
Vol. 100, No. 1 Nodular Adenomatosis 91
Fig. 4 (Tso, Goldberg, and Sugar). Note tumor cells with distinct basement membrane (arrowheads). Multiple poorly formeddesmosomes join adjacent tumor cells (arrows). The tumor cell has prominent nucleoli, abundant mitochondria, and bundles ofinterlacing filaments. Small clusters of irregularly melanized granules (M) are seen scattered in the cytoplasm (X 15,000). Upperinset demonstrates clusters of small granules (arrowheads) with varying degrees of melanization between bundles of finefilaments (arrows) (x 45,000). Lower inset shows cell processes (P) extending through basement membrane (arrowheads) to theiris stroma. Caveolae (arrows) are seen in the basal plasmalemma of the tumor cells (arrows) (x 30,000).
Pathologically, the tumor consisted of nests ofepithelioid "nevoid" cells, which were distinctlypolarized and had a discrete basement membraneand apical villi. Numerous desmosome-like junctions joined the adjacent cells. These epithelial characteristics suggested that the tumor derived from theiris pigment epithelium. The large, football-shaped,homogeneously melanized melanosomes in thetumor cells further support the pigment epithelialorigin of the tumors. Because of the epithelial characteristics of the tumor cells and their multiple focalorigin in the iris, we propose to term this condi-
tion "nodular adenomatosis of the iris pigment epithelium."
Other cytologic features of these tumor cells included abundant intracytoplasmic filaments, plasmalemmal densities, and caveolae. Furthermore, thetumor cells were seen to mingle with the welldifferentiated smooth muscle cells of the iris. Thesefeatures suggest that some of the cells were differentiating in the direction of the smooth muscles.
Large, oval, homogeneously melanized melanosomes, which were noted in some of the tumorcells, resemble those of iris pigment epithelium, and
92 AMERICAN JOURNAL OF OPHTHALMOLOGY July, 1985
Fig. 5 (Tso, Goldberg, and Sugar). A tumor cell exhibits vacuolated degeneration (D) within the nucleus (x 17,000).
the clusters of small. irregularly melanized granulesthat are typically seen in iris nevi and malignantmelanomas were also observed in other tumor cells.Occasionally, these two types of melanin granuleswere simultaneously present in a few of the tumorcells. This observation confirms that the tumor cellswere differentiating in multiple directions.
The spurs of Fuchs, Michel, and Grunert have longbeen recognized as normal pigment epithelialgrowths extending from the anterior iris pigmentepithelium into the smooth muscle bundles of theiris,22 with which clump cells of Koganei are assoelated." Wobmann and Fine10 examined the clumpcells of Koganei by light and electron microscopy andconcluded that two types of pigment cells exist. TypeI cells are pigment-laden macrophages and type IIcells are neuroepithelial cells derived from the spursof the anterior iris pigment epithelium. The conceptthat the spurs are "leftover" pigment epithelial cellsof leiomyogenesis is generally accepted. 10 We suspectthat the tumor reported herein originated from the
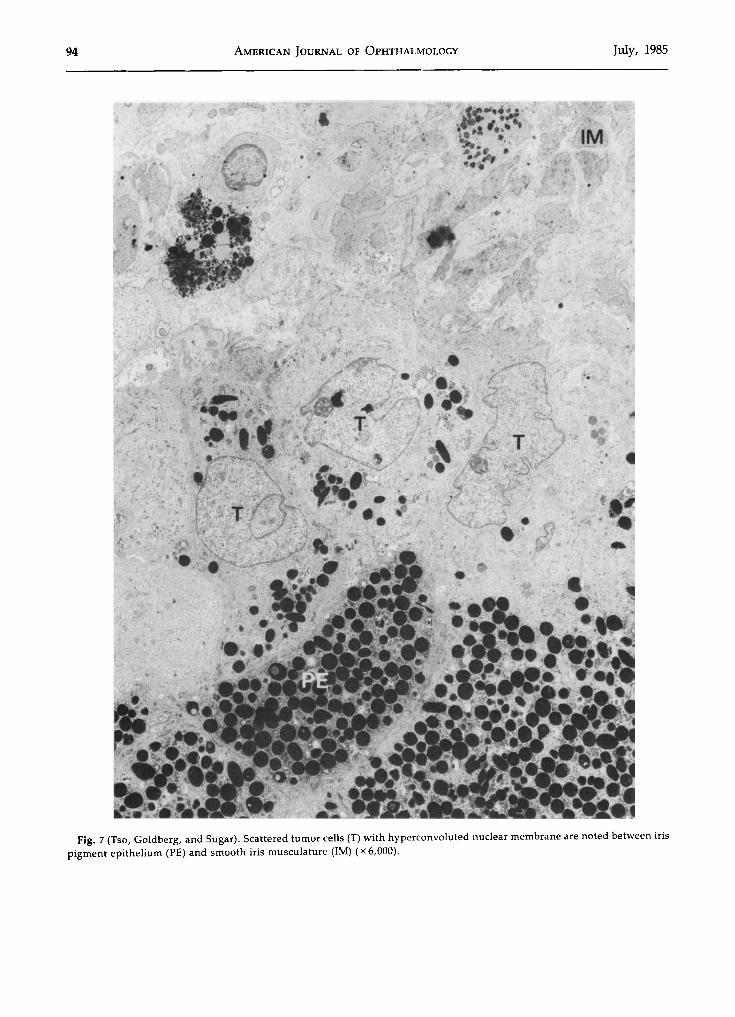
spurs of Fuchs, Michel, and Grunert for three reasons: (1) the tumor cells showed pigment epithelialand smooth muscle cell characteristics; (2) the tumorcells were found between the anterior pigment epithelium and smooth muscle cells of the iris (Fig. 7);and (3) the remarkable multifocal origin of the tumorparalleled the multiple growths of these anatomicspurs.
Nodular adenomatosis may be differentiated fromadenoma of iris pigment epithelium, which frequently occurs as a deeply pigmented lesion bulging toward the posterior chamber and pushing the irisanteriorly;" Shields and co-workers" reported anadenoma of the iris pigment epithelium that invadedthe iris stroma anteriorly. Pathologically, adenomaof the iris pigment epithelium consists of deeplypigmented epithelial cells in an acinar or cordiikearrangement that are separated by delicate connective tissue. Offret and Saraux" described the electronmicroscopic features of two types of cells in an irispigment epithelial adenoma: a dark cell with many
Vol. 100, No.1 Nodular Adenomatosis 93
Fig. 6 (Tso, Goldberg, and Sugar). Two distinct types of melanin granules were observed: large and homogeneouslymelanized melanosomes (arrowheads) resembling melanin granules of iris pigment epithelium, and smaller granules ofvarying degrees of melanization (arrows). Both types of granules are seen within the cytoplasm of a cell (x 15,000).
pigment granules and a light cell with intercellularvacuoles. These tumor cells showed polarity withbasement membrane, cell junctions, and villi. Largemelanin granules resembling those of iris pigmentepithelium also were present.
Benign epithelioid cell nevi, as described by [akobiec, Moorman, and jones," may closely resemblethis entity. However, the epithelioid cell nevi characteristically show cellular heterogeneity, consisting ofmononuclear, binuclear, and multinuclear epithelioid cells and elongated myoid cells with deeplyeosinophilic cytoplasm. These features were not observed in the nodular adenomatosis. Furthermore,
epithelioid cell nevi show poorly developed desmosomes and an absence of large pigment epithelialmelanin granules, but exhibit well-differentiated cytoplasmic leptomeres.
Nodular adenomatosis also should be differentiated from leiomyoma of the iris;" which classicallydemonstrates smooth muscle differentiation, andmedulloepithelioma of the iris," which may differentiate into multiple cell lines including rhabdomyosarcoma. The pigment epithelial characteristics and thesmooth muscle features of the cells of the nodularadenomatosis described herein suggest that this lesion may be a variant of medulloepithelioma.
94 AMERICAN JOURNAL OF OPHTHALMOLOGY July, 1985
Fig. 7 (Tso, Goldberg, and Sugar). Scattered tumor cells (T) with hyperconvoluted nuclear membrane are noted between irispigment epithelium (PE) and smooth iris musculature (1M) (x 6(000).

Vol. 100, No.1 Nodular Adenomatosis 95
We would like to propose a new classification ofprimary neoplastic lesions of the iris. (1) Melanoticlesions arising from the neural crest include irisfreckles, nevi, melanocytomas, epithelioid cell nevi,and malignant melanomas. These lesions are observed in the iris stroma with various degrees ofpigmentation. (2) Tumors derived from the posterioriris epithelium, such as the benign adenomas of theiris pigment epithelium reported by Morris and Henkind." mostly extend into the posterior chamber asdeeply pigmented nodular growths. (3) Tumors develop from the anterior iris pigment epithelium,including leiomyoma, nodular adenomatosis, andmedulloepithelioma and grow into the iris stroma.They are variably pigmented and show a wide spectrum of differentiation. (4) Hamartomas and otherproliferative dysgenetic lesions from the iris pigmentepithelium are exemplified by the cases reported byKlein! and Iakobiec and colleagues.! While hamartomas are not strictly neoplastic lesions, they are included in this classification because clinically theymay resemble other neoplasms of the iris. (5) Primary soft tissue tumors include angiomata and neurofibromata." This classification has the distinct advantage of grouping lesions embryologically as wellas anatomically in different layers of the iris and maybe helpful in the differential diagnosis of primaryiridic neoplasms.
References
1. Klien, B. A.: The ciliary margin of the dilator muscle ofthe pupil. Arch. Ophthalmol. 15:985, 1976.
2. [akobiec, F. A., Howard, G., and DeVoe, A. G.: Sectorhamartoma of the iris. Arch. Ophthalmol, 93:614, 1975.
3. Ashton, N.: Primary tumors of the iris. Br. J. Ophthalmol. 48:650, 1964.
4. Fine, B. S., and Yanoff, M.: Ocular Histology. TheUveal Tract. Hagerstown, Harper and Row, 1979, pp. 197214.
5. [akobiec, F. A., and Silbert, G.: Are most iris melanomas really nevi? A clinicopathologic study of 189 lesions.Arch. Ophthalmol. 99:2117, 1981.
6. Lee, W. R.: The fine structure of three malignant mela-
nomas of the iris. Albrecht von Graefes Arch. Klin. Exp.Ophthalmol. 188:91, 1973.
7. Iwamoto, T., Jones, 1., and Howard, G.: Ultrastructural comparison of spindle A, spindle B and epithelioid-typecells in uveal malignant melanoma. Invest. Ophthalmol.11:873, 1972.
8. Iwamoto, T., Reese, A. B., and Mund, M. 1..: Tapiocamelanoma of the iris. Part 2. Electron microscopy of themelanoma cells compared with normal iris melanocytes.Am. J. Ophthalmol. 74:851, 1972.
9. [akobiec, F. A., Moorman, 1.. T., and Jones, 1. S.: Benign epithelioid cell nevi of the iris. Arch. Ophthalmol.97:917, 1979.
10. Wobmann, P. R., and Fine, B. S.: The clump cells ofKoganei. A light and electron microscopic study. Am. J.Ophthalmol. 73:90, 1972.
11. Asbury, M. K.: Epithelial tumors of the iris. Am. J.Ophthalmol. 27:1094, 1944.
12. Laval, J.: Benign pigment-epithelium tumors of theiris. Arch. Ophthalmol. 48:66, 1952.
13. Duke, J. R., and Dunn, S. N.: Primary tumors of theiris. Arch. Ophthalmol. 59:204, 1958.
14. Reese, A. B.: Tumors of the Eye, 2nd ed. Hagerstown,Harper and Row, 1963, p. 70.
15. Vrabec, F., and Soukup, F.: Malignant epithelioma ofthe pigmented epithelium of the human iris. Am. J. Ophthalmol. 56:403, 1963.
16. Mortis, D. A., and Henkind, P.: Neoplasms of the irispigment epithelium. Am. J. Ophthalmol, 66:31, 1968.
17. Offret, H., and Saraux, H.: Adenoma of the irispigment epithelium. Arch. Ophthalmol. 98:875, 1980.
18. Shields, J. A., Augsburger, J. J., Sanborn, G. E., andKlein, R. M.: Adenoma of the iris-pigment epithelium.Ophthalmology 90:735, 1983.
19. de Buen, S., Olivanes, M. 1.., and Charlin, c.: Leiomyoma of the iris. Br. J. Ophthalmol. 55:353, 1971.
20. Zimmerman, 1.. E., and Broughton, W. 1..: A clinicopathologic and follow-up study of fifty-six intraocularmedulloepitheliomas in ocular and adnexal tumours. In[akobiec, F. A. (ed.): Ocular and Adnexal Tumors. Birmingham, Aesculapius Publishing Co., 1978, pp. 181-196.
21. [akobiec, F. A., Depot, M. J., Henkind, P., and Spencer, W. H.: Fluorescein angiographic patterns of iris melanocytic tumours. Arch. Ophthalmol. 100:1288, 1982.
22. Last, R. J.: Eugene Wolff's Anatomy of the Eye andOrbit, 6th ed. Philadelphia, W. B. Saunders, 1968, P: 88.
23. Duke-Elder, S., and Wybar, K. c.: The Anatomy ofthe Visual System. In Duke-Elder, S. (ed.): System of Ophthalmology, vol. 2. St. Louis, C. V. Mosby, 1961, p. 184.