*nnvoj[bujpo pg 1fpqmf -jwjoh xjui )*7 boe … · evidence that conversion to a positive tuberculin...
TRANSCRIPT

ContentsI. Introduction ............................................................................................................................. 441
II. General principles for the immunization of PLHIV ........................................................... 442
III. Use of vaccines and immunoglobulins ................................................................................ 443 1. Liveattenuatedvaccines.................................................................................................. 443 1.1. BCGvaccine........................................................................................................... 443 1.2. Choleravaccine(CVD103-HgR)........................................................................... 444 1.3. Measles,mumpsandrubellavaccines................................................................... 444 1.4. Oralpoliovirusvaccine........................................................................................... 445 1.5. Rotavirusvaccine.................................................................................................... 445 1.6. Typhoid(Ty21a)vaccine......................................................................................... 445 1.7. Varicellavaccine..................................................................................................... 445 1.8. Yellowfevervaccine............................................................................................... 446 2. Killedorinactivatedvaccines.......................................................................................... 446 2.1. Choleravaccine(WC/rBs)...................................................................................... 446 2.2. Diphtheria,tetanusandpertussisvaccines............................................................. 447 2.3. Haemophilus influenzaetypebvaccine.................................................................. 447 2.4. HepatitisAvaccine.................................................................................................. 447 2.5. HepatitisBvaccine................................................................................................. 448 2.5.1. RecommendedscheduleforhepatitisBvaccinationinpatientsinfected withHIV...................................................................................................... 449 2.5.2. ResponsetohepatitisBvaccination............................................................ 449 2.5.3. RecommendedmonitoringofHIV-infectedpatients
afterHBVvaccination................................................................................. 449 2.6. Influenzavaccine..................................................................................................... 450 2.7. Meningococcalvaccine........................................................................................... 450 2.8. Pneumococcalvaccine............................................................................................ 450 2.8.1. Pneumococcalpolysaccharidevaccine........................................................ 450 2.8.2. Pneumococcalconjugatevaccine................................................................ 451 2.9. Inactivatedpoliovirusvaccine................................................................................ 451 2.10.Rabiesvaccine......................................................................................................... 452 2.11.Tick-borneencephalitisvaccine.............................................................................. 452 2.12.Typhoidvaccine(Vipolysaccharide)...................................................................... 453 2.13.Otherkilledantigens............................................................................................... 453 3. Useofimmunoglobulins.................................................................................................. 454 3.1. HepatitisBimmunoglobulin................................................................................... 454 3.2. Humannormalimmunoglobulin............................................................................. 454 3.2.1. HepatitisA.................................................................................................... 454 3.2.2. Measles........................................................................................................ 455 3.3. Humanrabiesimmunoglobulin............................................................................... 455 3.4. Tetanusimmunoglobulin......................................................................................... 455 3.5. Varicella-zosterimmunoglobulin............................................................................ 456
Annex 1. Summary of immunization recommendations for people immunocompromised due to HIV/AIDS .................................................................................. 457
Annex 2. WHO classification of HIV-associated immunodeficiency in infants and children ................................................................................................................ 458
Annex 3. Rabies vaccines ............................................................................................................ 459
Annex 4. Glossary ....................................................................................................................... 460
References .................................................................................................................................... 463

441
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
I. Introduction
ThisprotocolisbasedontheglobalWHOrecommendationsforvaccinatingpeoplewhoareHIV-infected.Atthesametime,itreflectstheepidemiologicalsituationandimmunizationprogrammeprioritiesoftheWHOEuropeanRegion.Thisprotocoldivertsfromglobalrecommendationsre-garding the use of bacille Calmette-Guérin (BCG) vaccine, oral poliovirus vaccine (OPV) andmeasles-containingvaccines (MCVs) includingmeasles,mumpsand rubella (MMR)vaccine. Italsoprovidesadditionalrecommendationsonthevaccinesandimmunoglobulinsusedoutsidetheroutinenationalimmunizationprogrammes.
ThisprotocolisdesignedprimarilyforHIV/AIDSclinicians.Itisrecommendedasabasisforde-velopingnationalrecommendationsthattakeintoaccountlocalepidemiologicalsituations.

442
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
II.GeneralprinciplesfortheimmunizationofPLHIV
AsHIVinfectionresultsinaprogressivedeteriorationoftheimmunesystem,therehasbeencon-cernthatsomevaccinescouldresultinsevereadverseeventsinHIV-infectedindividuals.
Sincenoimmunobiologicalproductiscompletelysafe,generalrecommendationsforvaccinatinginfants,childrenandadultsarebasedon:• thecharacteristicsofimmunobiologicalproducts• scientificknowledgeoftheprinciplesofactiveandpassiveimmunization• theepidemiologyofinfection• theriskandbenefitsofachievingoptimalprotectionagainstinfectiousdisease.
Untilfurtherresearchcanclearlydefinetherisksandbenefits,administrationofcertainvaccinestopeoplelivingwithHIV(PLHIV)shouldberestrictedoradministeredwithcautionafterathoroughriskassessmentbyexpertsinclinicalandpreventivemedicine.
Thetermsvaccinationandimmunizationareoftenusedinterchangeably.Vaccinationdenotesthephysicalactofadministeringanimmunobiologicalproduct(avaccineortoxoid)toapersonandrefers toactive immunization.“Immunization” isamore inclusive termdenoting theprocessofinducingorprovidingimmunityartificially,anditcanbeactiveorpassive.
GeneralprinciplesforvaccinationofPLHIVareasfollows.• Killedorinactivatedvaccinesdonotrepresentadangertoimmunocompromisedpeopleand
generallyshouldbeadministeredasrecommendedforotherpeople.• Live-virusor live-bacteriavaccinessuchasBCG,oralpoliovirus, typhoid(Ty21a),varicella
andyellowfevervaccinesmayposearisktoHIV-infectedpeople,whoshouldnotbegiventhemwithoutcarefulconsiderationoftherisksandbenefits,giventheirindividualstageofHIVdiseaseandlevelofimmunesuppression.
Forfurtherinformation,pleaserefertosectionIIIbelowforvaccine-specificconsiderationsandtoAnnex1forasummaryofrecommendations.

443
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
1BCGvaccine;diphtheria,tetanusandpertussis(DTP)vaccine;OPV;MMRvaccine;hepatitisBvaccine;andHiBvaccine.2ItshouldbenotedthatthesafetyinformationonadministrationofcertainvaccinestoPLHIVislimited,andthatcountriesareencouragedtoreportanyencounteredadverseeventsfollowingimmunization(AEFIs)totheirpharmacovigillanceorAEFIsurveillancesystems,keepinginmindthatsomeAEFIsmayoccurwithlargelatencyinPLHIV.3Forclinicalstaging,refertoProtocol1,Patient evaluation and antiretrovital treatment for adults and adolescents,Annex2,andProtocol11,Paediatric HIV/AIDS treatment and care,Annex1.
III.Useofvaccinesandimmunoglobulins
Generalaspectsofimmunogenicityofvaccinesshouldbetakenintoconsiderationwhenimmuniz-ingPLHIVagainstvaccine-preventablediseases.• Althoughthecapacity tomountbothcellularandhumoral immuneresponsestartsdeclining
afterbirthinHIV-infectedneonates,mostchildrenstillhaveanimmuneresponsecapacitydur-ingthefirsttwoyearsoflife.Studiesoftheimmunogenicityofimmunizationprogrammeswithrecommendedvaccines1haveshownsatisfactoryseroconversionratesintheearlystagesofHIVinfection.Eachvaccinehasitsownseroconversionrate,someofwhichcanbefoundinthissec-tion.However,theproportionofrespondersdecreaseswithprogressionfromHIVinfectiontoAIDS(1).
• SymptomaticHIV-infectedchildrenandadultshavesuboptimalimmunologicresponsestovac-cines (1–5).The response toboth liveandkilledantigensmaydecreaseas theHIVdiseaseprogresses(1).However,theresponsetohigherdosesofvaccineandthepersistenceofantibod-iesinHIV-infectedpatientshavenotbeensystematicallyevaluated.Althoughhigherdosesormorefrequentboostersmaybeconsideredforsuchpatients,firmrecommendationscannotbemadeatthispoint.
Specificconsiderationsfor thesafety2andefficacyof individualvaccinesand immunoglobulinsincludetheepidemiologyoftheparticulardiseaseandthepatient’slevelofimmunosuppression.
Thedegreetowhichapatientisimmunocompromisedshouldbedeterminedbyaphysician,usingtheWHOclinicalstagingsystem3and/orage-specificCD4countsandpercentages(seeAnnex2).
1. Live attenuated vaccines
1.1. BCG vaccineBCGvaccineprotectschildrenyoungerthan2againstdisseminatedandseveretuberculosis(TB),includingTBmeningitisandmiliaryTB.BCGhaslittleornoeffectinreducingthenumberofadultcasesofpulmonarytuberculosis.
ItisnotknownifHIVinfectionreducestheprotectionconferredbyBCGinchildren.ThereissomeevidencethatconversiontoapositivetuberculintestafterBCGis lessfrequent inHIV-infectedchildren(6),butthesignificanceofthisfindingisnotclear.Therehavebeencasereportsoflocalcomplications anddisseminatedBCG infection, evenyears after vaccinatingHIV-infected chil-dren.However,prospectivestudiescomparingBCGimmunizationinHIV-infectedanduninfectedinfantshaveshownnodifferenceinriskforcomplications(6).ThereneedstobeclosermonitoringforadverseeventsinareasofhighHIVprevalence,withspecificeffortstodistinguishBCGinfec-tionfromTB(7).

444
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
UntilfurtherresearchcanclearlydefinetherisksandbenefitsofBCGvaccination,itshouldbere-strictedtoasymptomaticchildren(duetoitspotentialtocausedisseminateddisease)whoareathighriskoftuberculosisinfection(8, 9),whichinturndependonthelocalprevalenceofTB.4Wheretheriskishigh,thepossiblebenefitsofBCGimmunizationoutweighthepossibledisadvantages.
1.1.1. Recommendations
• WhereTBincidenceislow,5BCGshouldnotbeadministeredtoHIV-infectedchildren,regard-lessoftheirclinicalstageorimmunodeficientstatus.Inallotherareas,BCGvaccinationshouldberestrictedtoHIV-positivechildrenwhoareasymptomatic.ChildrenwithsymptomsofHIVinfectionshouldnotreceiveBCGvaccine.
• BCGisnotrecommendedforadolescentsandadults,includingthosewithHIVinfection,be-causeithaslittleornoeffectinreducingthenumberofadultcasesofpulmonarytuberculosis(6).
• TBpreventivetherapyshouldbestronglyrecommendedforPLHIVthoughttobeinfectedwithMycobacterium tuberculosisandatriskofdevelopingTB(forfurtherinformation,pleaserefertoProtocol4,Management of tuberculosis and HIV coinfection).
1.2. Cholera vaccine (CVD 103-HgR)
1.2.1. Recommendations
• Live,attenuatedoralcholeravaccine(usingCVD103-HgRstrain)iscontraindicatedinHIV-infectedpeopleduetoinsufficientsafetydata(11).
• ThekilledWC/rBscholeravaccineistherecommendedvaccineforHIV-infectedpeople(seesectionIII.2.1.belowforcholeravaccineWC/rBs).
1.3. Measles, mumps and rubella vaccines (MMR, MR, M and R vaccines6)HIV-infected asymptomatic children or children with signs of mild immunosuppression shouldroutinelyreceiveMMRandothermeasles-containingvaccines(MCVs), thesameasnon-infect-edchildren.Itisimportanttorememberthatimmunogenicityofmeaslesvaccineisdecreasedifthevaccineisadministeredinaperiodlessthansixmonthsafterhumannormalimmunoglobulin(HNIg)administration.
Although studies amongbothasymptomatic and symptomaticHIV-infectedpatients immunizedwithMMRvaccineandotherMCVshavenotdocumentedanyseriousorunusualadverseevents(1),theyarenotrecommendedforPLHIVwithevidenceofsevereimmunosuppression.Thelackofarecommendationisprimarilydueto:• areportofapneumoniacasefollowingmeaslesvaccineinanindividualwithsevereHIV-re-
latedimmunosuppression(12);• other evidence indicatingadiminishedantibody response tomeaslesvaccinationamong se-
verelyimmunocompromisedpeople(13);and• evidencelinkingmeaslesvaccineviralinfectiontosubsequentdeathinatleastsixseverelyim-
munocompromisedpeople(14).
1.3.1. Recommendations
• MMRandotherMCVsshouldnotbeadministeredtoPLHIV,eitherchildrenoradults,whoshowevidenceofsevere immunosuppression.Severe immunosuppressionisdefinedasCD4<200 cells/mm3 in adults and children ≥5 years, for severe immunosuppression in childrenyoungerthan5years,seeAnnex2(15–17).
4ItshouldbenotedthatevenamongcountrieswithagenerallylowprevalenceofTB,theremaybehighprevalenceingivensubpopulations,makingasubnationalpolicydesirable.5CountriesintheWHOEuropeanRegionwithacrudenotificationrateof<20per100000populationaredefinedaslow-incidence(10).6MMR:measles,mumpsandrubella;MR:measlesandrubella;M:measles;R:rubella.
445
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
• MMRandotherMCVsshouldbeconsideredforHIV-infectedpatientswhoareasymptomaticormildlyimmunosuppressed,aspertheroutinenationalschedule.
• For infantswithhighriskofexposure tomeaslesvirus,anadditionaldoseofsingle-antigenmeaslesvaccineadministeredat6–11monthsofageisrecommended,followedbyafirstdoseofroutineMMRoranothermeasles-containingvaccine(MCV)atage12monthsorolder(withaminimumintervalof1monthbetweendoses).
• HIV-infectedsymptomaticpatientswhoareexposedtomeaslesshouldreceiveHNIgregardlessoftheirpriorvaccinationstatus(seesectionIII.3.2.1belowforfurtherinformationonHNIg).
• Healthysusceptibleclosecontactsofimmunocompromisedpeople(includingPLHIV)shouldalsobevaccinated.
1.4. Oral poliovirus vaccine (OPV)AlthoughasymptomaticHIV-infectedchildrenmaybevaccinatedwithOPV(1, 18),datashowthatadministrationofOPVtochildrenwithcongenitalimmunodeficiencycanresultinsevere,progres-siveneurologicalinvolvement(paralyticdisease)(19–22).Therefore, inactivatedpoliovirusvac-cine(IPV)isrecommendedforbothsymptomaticandasymptomaticchildren(seesectionIII.2.9belowforIPV).
Inaddition,personsimmunizedwithOPVcanshedvaccinevirusintotheirenvironmentforuptoonemonth,consequently,HIV-positiveindividualsshouldhavelimitedcontactwithpersonsvac-cinatedwithOPV.IfOPVisinadvertentlyadministeredtoahouseholdmemberorotherclosecon-tact7ofanHIV-infectedindividual,regardlessofpriorimmunizationstatus,closecontactbetweenthemshouldbeavoidedforonemonthpost-vaccination.
1.4.1. Recommendation
• OPVshouldnotbeadministeredtoPLHIV,eitherchildrenoradults,regardlessoftheirimmu-nodeficiencystatus,ortomembersoftheirhouseholdorotherclosecontacts.
1.5. Rotavirus vaccine1.5.1. Recommendation
• RotavirusvaccineshouldnotbeadministeredtochildreninfectedwithHIVregardlessoftheirimmunodeficiency status, untilmore scientific evidence can clarify the safety and immuno-genicityprofileinHIV-infectedchildren.
1.6. Typhoid (Ty21a) vaccineWhileliveattenuatedtyphoidvaccine(usingtheTy21astrain)canbeadministeredtoHIV-infectedasymptomaticindividualswithoutriskaslongastheCD4cellcount>200cells/mm3,parenteralinactivatedvaccineistheoreticallyasaferalternative(23).
1.6.1. Recommendation
• Ty21avaccineshouldnotbeadministered toPLHIV,eitherchildrenoradults, regardlessoftheirimmunodeficiencystatus.
1.7. Varicella vaccineAlthougharecentsmallstudyindicatednoseriousadverseeventsfor10HIV-infectedchildren(24),peoplewithmoderateorseverecellularimmunodeficiencyresultingfromHIV,includingthosedi-agnosedwithAIDS,shouldnotreceivevaricellavaccine.However,childrenwithasymptomaticormildlysymptomaticHIVinfectionandaCD4cellcount≥25%shouldreceivethevaccineat12–15monthsofageorlater,withaseconddose4–8weeksafterthefirst.VaricellavaccineshouldnotbeadministeredtoHIV-infectedchildrenwithCD4cellcount<25%becauseofthepotentialdis-seminationofviralinfection(23).
7DefinedassomeonewhoriskstransmittinglivepoliomyelitisvaccinevirustoanHIV-infectedpersonthroughfaecalororalcontact.

446
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
HIV-infectedchildrenandadultswhoaresusceptibletovaricella-zostervirus(VZV)–includingthosewhohavenohistoryofchickenpox(primaryvaricella infection), thosewhohaveshingles(recurrentinfection)andthosewhoareseronegative–shouldavoidexposuretopeoplewithchick-enpoxorshingles.
Susceptiblehouseholdcontacts(especiallychildren)ofPLHIVshouldbevaccinatedwithvaricellavaccineiftheyhavenohistoryofchickenpoxandareseronegativeforHIV,sothattheywillnottransmitthevirustotheirHIV-infectedcontactsthatmaybesusceptibletoVZV(14).
1.7.1 Recommendations
• VaricellavaccineshouldnotbeadministeredtoHIV-infectedadults,regardlessoftheirimmu-nodeficiencystatus,ortoHIV-infectedchildrenwithmoderateorsevereimmunosuppression.
• VaricellavaccinationshouldberestrictedtochildrenwithasymptomaticormildlysymptomaticHIVinfection(CD4levels≥25%).
• SusceptiblehouseholdcontactsofPLHIVshouldbevaccinatedtopreventpossibletransmissionofVZV.
1.8. Yellow fever vaccineYellow fevervaccinevirusposes a theoretical riskof encephalitis toHIV-infectedpeople,whoshouldthusnotbegivenit.Yellowfever isendemicto33countries inequatorialAfricaand11countriesinSouthAmerica.Iftraveltosuchanareaisnecessary,patientsshouldbeadvisedontherisks,instructedinmethodsofavoidingmosquitoesandsuppliedwithvaccinationwaiverlettersbytheirphysicians.Sometravelclinicsmaydecidewhetherornottoadministerthevaccineonthebasisofaperson’sCD4cellcount.
PeoplewhoareknowntobeHIV-infectedandwhocannotavoidpotentialexposuretoyellowfevervirusshouldbeofferedthechoiceofvaccination.Vaccineesshouldbemonitoredforpossiblead-versereactions.SincevaccinationmaybelesseffectiveforHIV-positivepeoplethanforHIV-nega-tivepeople,measuringneutralizingantibodyresponsesbefore travelmaybeconsidered.Familymembersofimmunosuppressedpeoplemayalsobevaccinatedagainstyellowfeveriftherearenocontraindications(25).
1.8.1 Recommendation
• YellowfevervaccineshouldnotbeadministeredtopeopleinfectedwithHIV,eitherchildrenoradults,regardlessoftheirimmunodeficiencystatus,unlessbenefitsexceedrisks.
2. Killed or inactivated vaccinesKilledorinactivatedvaccinesdonotpresentadangertoimmunocompromisedpeopleandgeneral-lyshouldbeadministeredasrecommendedforotherpeople(17).Frequently,theimmuneresponseofimmunocompromisedpeopletokilledandinactivatedvaccineantigensisnotasgoodasthatofimmunocompetentpeople;higherdosesormorefrequentboostersmayberequired,althoughevenwiththesemodifications,theimmuneresponsemaybelessthanoptimal.
2.1. Cholera vaccine (WC/rBs)Avaccineconsistingofkilledwhole-cellVibrio choleraeO1combinationwitharecombinantB-subunitofcholeratoxin(WC/rBs)hasbeenshowntobesafeeveninpregnancyandduringbreast-feeding,andwelltoleratedbyHIV-positiveindividuals.
Givenorallyaccordingtoatwo-doseschedule,10–14daysapartinducesinitialprotectionin86%ofthevaccinees.Onaverage,thevaccineconfers50–60%protectionforatleast3years.TherehavebeennospecificreportsofWC/rBsvaccineefficacyinHIV-positiveindividualspub-lishedtodatebutarecentstudyconducted inMozambiquedemonstratedpromisingresults ina

447
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
populationinwhichapproximately25%wereHIV-positive.DurationofimmunityisunknowninHIV-infectedpeople.HIV-infectedadultswithCD4counts<100cells/mm3maybeexpected torespondpoorlytoimmunization,whereasthosewithCD4counts>100cells/mm3showimprovedresponsesafter twodoses (26).Theseobservations indicateapotentialbenefitofvaccination inthosewithearlyandmoderatelyadvancedclinicalHIVdisease(27).
2.1.1 Recommendations
• VaccinationshouldbeconsideredforselectedHIV-infectedpeopleiftheyareduetotraveltohighlyendemicareas,fallinoneoftheriskgroups(long-termtravellersandforthosewhodrinkuntreatedwater,eatpoorlycookedorrawseafood,orliveinunsanitaryconditionsindisease-endemicareas).
• Owingtoitslowefficacyandshortdurationofprotection,useofoldparenteralvaccine(basedoninactivatedphenol-killedwhole-cellV.choleraeO1)isnotrecommended,althoughthisvac-cineisstillproducedinsomecountries(28).
2.2. Diphtheria, tetanus and pertussis vaccines (DTP, DTaP, DT, TT and Td8)
2.2.1 Recommendations
• ForchildreninfectedwithHIV,irrespectiveoftheirimmunestatus,DTP(andDT)vaccineisindicatedonthesamescheduleanddosageasfornon-HIV-infectedchildren,includingtheuseoftheacellularpertussisform(DTaP)forboostersortheprimaryseries.
• TTandTdvaccinescanbeadministeredtoHIV-infectedadultsirrespectiveoftheirimmunestatus,usingthesamescheduleanddoseasfornon-HIV-infectedadults(25).
• SpecialattentionshouldbepaidtovaccinatingIDUswithTTorTdtopreventtetanuswheretherearenoneedleorsyringeexchangeprogrammes.
2.3. Haemophilus influenzae type b (HiB) vaccine Ingeneral,childrenolderthan2yearsdonotneedHiBvaccination,duetoage-dependentsuscepti-bilitytothedisease(11).Insomepeopletheorganismcausesaninvasiveinfection.Theexactmodeofinvadingthebloodstreamisunknown,butpreviousviralormycoplasmalinfectionoftheupperrespiratorytractmaybeacontributingfactor.Thebacteriaspreadviathebloodstreamtodistantsitesinthebody,themeningesinparticular.HIV-infectedchildrenandadultsareatincreasedriskforinvasiveHiBdiseaseduetoimmunosuppressionandshouldthereforebevaccinated.
Individualpatientriskforthediseaseandbenefitsfromvaccinationshouldbeconsideredbeforedecidingwhethertovaccinate.Insomesettings,theincidenceofHiBdiseasemaybehigheramongHIV-infectedadultsthannon-HIV-infectedadults(29, 30).
2.3.1 Recommendations
• PreviouslyunvaccinatedHIV-infectedindividualsolderthan2yearswhoareatriskforinvasiveHiBshouldbegivenatleastonedoseofvaccine.
• Immunocompromisedchildrenshouldbevaccinatedwiththesamedosageandscheduleasim-munocompetentchildren.
2.4. Hepatitis A vaccineTheriskofdevelopingsymptomaticillnessfollowinghepatitisAvirus(HAV)infectionisdirectlycorrelatedtoage.Inchildrenyoungerthan6,HAVinfectionisusuallyasymptomatic,whilesymp-tomaticdiseaseoccursmorecommonlyamongadults. InfectionwithHAVinduces lifelong im-munity. In areasof lowendemicity, hepatitisAusuallyoccurs as single cases amongpeople in
8DTP:diphtheriaandtetanustoxoidsandpertussisvaccine;DTaP:diphtheriaandtetanustoxoidsandacellularpertussisvac-cine;DT:diphtheriaandtetanustoxoids(forpaediatricuse);TT:tetanustoxoid;Td:tetanusanddiphtheriatoxoids(foradultuse).

448
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
high-riskgroupsorasoutbreaksinvolvingasmallnumberofpeople.Inareasofhighendemicity,mostpeopleareinfectedwithHAVwithoutsymptomsduringchildhood.Incountriesofloworin-termediateendemicity,adultdiseaseisseenmoreoften,andhepatitisAmayrepresentasubstantialmedicalandeconomicburden.
HepatitisAvaccineishighlyimmunogenic.Morethan95%ofadultswilldevelopprotectivean-tibodieswithinfourweeksofasingledose.Amongchildrenandadolescents,morethan97%willbeseropositivewithinamonthofthefirstdose.Inclinicaltrials,allrecipientshadprotectivelevelsofantibodiesaftertwodoses.Therefore,post-vaccinationtestingisnotindicated.TestingmethodssufficientlysensitivetodetectlowHAVantibodyconcentrationsaftervaccinationarenotapprovedforroutinediagnosticuse(14).
Dataconcerningthelong-termpersistenceofantibodyandofimmunememoryarelimitedbecausethecurrentlyavailablevaccineshavebeenunderevaluationforlessthan12years.Theneedforboosterdoseswillbedeterminedbyfuturesurveillancestudies(31).
2.4.1. Recommendations
HepatitisAvaccination(onedosewithabooster6–12monthslater)isstronglyrecommendedforpeopleatriskforHAVinfectionoritscomplications,irrespectiveoftheirHIVorimmunestatus.Riskgroupsinclude:• peoplewithchronicliverdisease;9
• menwhohavesexwithmen(MSM);• drugusers;10
• peoplewithclotting-factordisorders;• peoplewithoccupationalriskofinfection(e.g.somelaboratoryworkers);and• people≥1yearoldfromnon-endemiccountrieswhoare travellingtocountrieswithhighor
intermediateriskofHAVinfection.11
2.5. Hepatitis B vaccineWhile therearenodataregardingHIV-infectedchildrenand thedurationofprotectionaffordedbyHBVvaccine,availabledataforuninfectedchildrenshowthatvaccine-inducedantibodylevelsdeclinewithtime(14).Nevertheless,immunememoryremainsintactformorethan15yearsfol-lowingimmunizationinbothadultsandchildren.Adultsandchildrenwithnormalimmunestatusdonotrequireboosterdoses,norisroutineserologicaltestingindicated,exceptforchildrenofhepa-titisBsurfaceantigen(HBsAg)-positivemothers,whoshouldbetestedforHBsAgandhepatitisBsurfaceantibody(HBsAb)afterthethirddose.Ifthesurfaceantibodylevelis<10mIU/ml,theentirethree-vaccineseriesshouldberepeated.TestingforHBVcoreantibodiesinthesechildrenisdiscouragedbecausepassivelyacquiredmaternalantibodiesmaybedetectableupto24monthsofage.Theneedforboosterdosesafterlongerintervalswillcontinuetobeassessedasadditionalinformationbecomesavailable.12
9SusceptiblepeoplewithchronicliverdiseaseareatincreasedriskoffulminanthepatitisAshouldtheybecomeinfected.HIV-infectedpeoplewithevidenceofchronichepatitisCorhepatitisBdiseaseshouldbevaccinatedwithhepatitisAvaccine(14).10HAVispresentinthebloodattheonsetoftheillnessandhasonrareoccasionsbeentransmittedbytransfusion;thevirusismoreeasilyspreadinareasofpoorsanitationorpersonalhygiene,conditionscommonamongdrugusers(14, 23, 32).11Vaccinate2–4weeksbeforedeparture.AreasofhighorintermediateriskincludeallareasoftheworldexceptCanada,theUnitedStates,westernEuropeandScandinavia,Japan,NewZealandandAustralia(33).12Onlyforhaemodialysispatientsshouldtheneedforboosterdosesbeassessedbyannualtestingforantibodylevels;boosterdosesshouldbeprovidedwhenantibodylevelsgobelow10mIU/ml.
449
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
2.5.1. Recommendations
• HepatitisBvaccinationisrecommendedforadultsatincreasedriskforhepatitisBvirus(HBV)infection,irrespectiveoftheirHIVorimmunestatus,including:
o MSM; o heterosexualswithmultiplepartners, o sexuallytransmittedinfection(STI)patients; o sexworkers; o sexualpartnersandhouseholdcontactsofHBVcarriers; o IDUs; o prisoninmates,bothmaleandfemale; o peopleonhaemodialysis (although thehepatitisBvaccine is lesseffective in them, it is
recommendedforallsusceptiblehaemodialysispatients);and o healthcareworkers.13
• HepatitisBvaccinationisrecommendedforallinfantsatbirthandallchildrentoage18,irre-spectiveoftheirHIVorimmunestatus.Variousschedulesincludeorexcludeneonates,butallhavethesameeffectiveness.
2.5.1.1. Recommended schedule for hepatitis B vaccination in patients infected with HIV
HIV-infectedpatientslackingHBVinfectionmarkersorHBsAgnegativemarkersshouldbevac-cinated.• HepatitisBvaccinationshouldstartwiththeconventionaldose(20µgatMonths0,1,2and12
orMonths0,1and6)forpatientswithCD4count>500cells/mm3.• PaediatricdosageofhepatitisBvaccineis10µg.• InpatientswithCD4count200–500cells/mm3,anintensivescheduleisrecommended(20µg
atMonths0,1,2and12)(34).• Patientswhodonotrespondtothefirstcycleshouldreceiveboosterdosesoranewvaccination
cyclewith40µg.• PatientswithCD4counts<200cells/mm3whoarenotonantiretroviraltreatment(ART)should
firstreceiveART.Vaccinationshouldbedeferreduntilaclinicallysignificantimmunereconsti-tutionhasbeenachieved,preferentiallyaftertheCD4cellcounthasincreased>200cells/mm3.
2.5.1.2. Response to hepatitis B vaccination
• TheresponsetothevaccineisdependentontheCD4countatthetimeofvaccination,andmaybereducedinpatientswithaCD4count<500cells/mm3.
• AfterthehepatitisBvaccinationschedulehasbeencompleted,theresponserateis87%inHIV-positivepatientswithCD4count>500cells/mm3,andonly33%inpatientswithCD4count200–500cells/mm3(35).
• HepatitisCvirus(HCV)/HIVcoinfectionmaybeassociatedwithimpairedresponsestohepa-titisBvaccine,withfewerHBsAbtitresafterthethirdvaccinationthaninHIVmonoinfection.
2.5.1.3. Recommended monitoring of HIV-infected patients after HBV vaccination
• HBsAbtitreshouldbemonitoredfourweeksaftertheendoftheHBVvaccinationschedule,andboostervaccinationorrevaccination(1–3additionaldoses)shouldbeconsideredforpatientswhodonotdevelopprotectiveantibodies(HBsAb<10mIU/ml).However,theimmunogenicityofhigherdosesofvaccineisunknown,andfirmrecommendationsondosagecannotbemadeatthistime(15).
• Peoplewhofail toseroconvertaftervaccinationandremainatriskofHBVinfectionshouldbeannuallymonitoredforserologicalmarkersofHBV(HBsAgandHBcAb(hepatitisBcoreantibody)).
13Riskisoftenhighestduringtrainingperiods;therefore,itisrecommendedthatvaccinationbecompletedduringtraininginschoolsofmedicine,dentistry,nursing,laboratorytechnologyandotheralliedhealthprofessions(14).
450
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
• PeoplewhofailtodevelopdetectableHBsAbaftersixdosesshouldbetestedforHBsAg.• PeoplewhoarefoundtobeHBsAg-positiveshouldbecounselledaccordingly.• Vaccinenon-responderswhoareHBsAg-negative shouldbe considered susceptible toHBV
infectionandshouldbecounselledregardingprecautionstopreventitandtheneedtoobtainhepatitisBimmunoglobulin(HBIg)prophylaxisforanylikelyparenteralorsexualexposuretoHBsAg-positiveblood.
2.6. Influenza vaccine14
Influenzamayresultinseriousillnessandcomplicationsforpeoplewhoareimmunocompromised.Vaccinationcanresultinprotectiveantibodylevelsinmanyimmunocompromisedrecipients(36).
2.6.1 Recommendations
• AlthoughthereiscurrentlylittleinformationregardingthefrequencyandseverityofinfluenzainPLHIV(37),vaccinationisrecommendedforallPLHIVbeforetheannualinfluenzaseason.
• TheantibodyresponsetovaccinemaybelowinpeoplewithadvancedHIVdisease;however,ithasnotbeenshownthataboosterdoseimprovestheirimmuneresponse(38).
2.7. Meningococcal vaccine
2.7.1 Recommendation
• Routineimmunizationwithmeningococcalvaccinecontainingappropriateserotypes15 isrec-ommendedforalltravellers,regardlessofHIVstatus,toareaswithepidemicmeningococcaldisease (32), and for those in high-risk groups, including peoplewith terminal complementcomponentdeficienciesandanatomicorfunctionalasplenia(39).
2.8. Pneumococcal vaccineTwotypesofpneumococcalvaccineareavailable:pneumococcalpolysaccharidevaccine(PPV)andpneumococcalconjugatevaccine (PCV).Pneumococcalvaccine is recommended foruse inpeoplewithchronicillnessesspecificallyassociatedwithincreasedriskofpneumococcaldiseaseoritscomplications,suchasconditionsassociatedwithimmunosuppression,includingHIVinfec-tion(40).
2.8.1. Pneumococcal polysaccharide vaccine (PPV)
Morethan80%ofnon-HIV-infectedhealthyadultswhoreceivePPVdevelopantibodiestoitssero-typeswithin2–3weeks.Elevatedantibodylevelspersistforatleastfiveyearsinhealthyadults,butfallmorequicklyinpeoplewithcertainunderlyingillnesses,includingHIVinfection.
2.8.1.1. Recommendations
• OnedoseofPPVshouldbeadministeredroutinely,irrespectiveofHIVandimmunestatus,to: o everyonewhoisolderthan65; o immunocompetentpeoplewhoareolderthan216andhavechronicillness(cardiovascular
disease, pulmonary disease, diabetes, alcoholism, cirrhosis or cerebrospinal fluid leaks);and
o immunocompromisedpeople(includingPLHIV)17whoareolderthan2andareatriskforpneumococcaldisease.
14SinceliveinfluenzavaccineiscontraindicatedinPLHIV,inactivatedinfluenzavaccineshouldbeused.15Themeningococcalvaccineshouldcoverserotypescausingmeningococcaldiseaseepidemicsintherelevantgeographicalarea.MeningococcalserogroupsA,BandCarefoundworldwide;serogroupYisfoundinsomepartsoftheUnitedStates;serogroupAisfoundinthe“Africanmeningitisbelt”fromSenegaltoEthiopia;serogroupW125isfoundinSaudiArabia.16Inchildren<2yearsold,antibodyresponsewithPPVtomostserotypesisgenerallypoor.17 Including (in addition toPLHIV)peoplewith splenicdysfunctionor absence (fromeitherdiseaseor surgical removal),Hodgkindisease,lymphoma,multiplemyeloma,chronicrenalfailure,nephriticsyndrome(atypeofkidneyfailure)orotherconditionsassociatedwithimmunosuppression(suchasorgantransplantation).
451
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
• PPVisrecommendedinHIV-infectedadultswithCD4countof>200cells/mm3andarestableonHAART.
• WhenCD4countis<200cells/mm3vaccinationmaybeconsideredforthosewithanincreasedriskforthedisease;however,itmaybelesseffectiveasimmuneresponseisdecreased.OnceHAARThasbeenadministeredandimmunefunctionrestoredsothatCD4countincreasesto>200cells/mm3,revaccinationshouldbeconsidered.
• Ifvaccinationstatusisunknown,patientswithHIVinfectionandotherswithimmunosuppres-sion(includingthosereceivinglong-termsystemiccorticosteroids)shouldbevaccinated(41).
• Routinerevaccinationofimmunocompetentpeopleyoungerthan65isnotrecommended.• People65andoldershouldbegivenaseconddoseiftheyreceivedthevaccinemorethanfive
yearspreviouslyandwereyoungerthan65atthetime.PLHIVandotherswhoareimmunocom-promisedandathighestriskshouldbegivenaseconddoseafterfiveyears.
• Revaccinationisalsorecommendedforchildrenvaccinatedatage2orolderwhoareathighestriskforseriousinfection,andforthosewithcertainunderlyingillnessesthatmakethemlikelytoexperiencearapiddeclineinpneumococcalantibodylevels.Theseconddoseshouldbead-ministered3–5yearsafterthefirst,thoughthereisnouppertimelimitforrevaccinationafter5years.
2.8.2. Pneumococcal conjugate vaccine (PCV)
PCVhasbeenshowntobeimmunogenicininfantsandchildren,includingthosewithHIVinfec-tion, regardlessof immunestatus.After fourdosesofPCV,virtuallyallhealthy infantsdevelopantibodiestoallserotypesinthevaccine.18
2.6.2.1 Recommendations
• Forinfants,dosesareroutinelygivenat2,4and6monthsofage,andaboosterdoseisrecom-mendedat12–15monthsofage.
• Unvaccinatedchildren7–11monthsold,includingthosewithHIV,shouldreceivetwodosesofPCV6–8weeksapart,followedbyaboosteratage12–15months.
• Unvaccinatedchildren12–23monthsoldshouldreceivetwodosesofPCV,6–8weeksapart.• Unvaccinatedhealthychildren24–59monthsoldshouldreceiveasingledoseofPCV.• Children24–59monthsoldwithHIVinfection,sicklecelldisease,asplenia,chronicillnessor
immunocompromisingconditionsshouldreceivetwodosesofPCV6–8weeksapart.Inordertoimprovetheboostereffect,onedoseofPPV6–8weeksafterthelastPCVdoseisrecom-mended.
• PCVisnotroutinelyrecommendedforchildrenolderthan5,regardlessofHIVstatus.• Revaccinationafteranage-appropriateprimaryserieswithPCVisnotcurrentlyrecommend-
ed.• Children2andolderwhoreceiveaprimaryseriesofPCVshouldalsohavePPV6–8weeks
afterthelastdoseofPCV.
2.9. Inactivated poliovirus vaccine (IPV)
2.9.1 Recommendations
• Inordertopreventtransmissionofvaccineand/orvaccine-derivedpoliovirusestoPLHIVIPVshouldbeadministeredtothefollowingpeoplewhenpolioimmunizationisindicated:
o infantsandchildreninfectedwithHIVregardlessoftheirimmunestatus; o householdmembersorotherclosecontacts;and o nursingpersonnelinclosecontactwithPLHIV.
18Presently,therearenotmuchdataforPLHIVresponsetoPCV,otherthanfromSouthAfricaandsmallerstudiesintheUnitedStates.
452
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
• ForunvaccinatedHIV-infectedadultsatincreasedriskofexposuretopoliovirus(suchastraveltoapolio-endemiccountry),aprimaryseriesofIPVisrecommended(25).
2.10. Rabies vaccineTwomaintypesofrabiesvaccineareinuse:nervetissue(Semple-type)vaccineandmoderncell-derivedvaccine.
ImmunocompromisedHIV-infectedpeoplemightnotdevelopsufficientimmunologicalresponse,as immunity depends upon theCD4+T-cell-dependent neutralizing antibody response to theGprotein.
2.10.1. Recommendations
• Rabiesvaccinesareusedforpost-exposureprotectionandpre-exposureimmunogenicity.Ra-biesvaccinesarenotcontraindicated forHIV-infectedpeopleandshouldbeadministered ifindicated(seeAnnex3).
• Ifpost-exposuretreatmentmustbegiventoimmunocompromisedHIV-positivepatients,intra-muscularvaccineandrabiesimmunoglobulinaremandatory,alongwithserologicalmonitoringoftheantibodyresponses(seesectionIII.3.3belowonrabiesimmunoglobulin).
• Peoplewhohavedemonstratedlessthan0.5IU/mlneutralizingantibodytitresafter4–5dosesofrabiesvaccineoverfourweeksshouldreceiveadditionaldosestoachievetherequiredlevel(23),asrabiesantibodytitres>0.5IU/mlarerequiredforprotection.
2.11. Tick-borne encephalitis vaccineTick-borneencephalitis, causedby tick-borneencephalitisvirus, infectionsoccur inmanypartsof Europe (Albania,Austria, Croatia, the Czech Republic, Denmark, Estonia, France (Alsace),Germany,Hungary,Latvia,Lithuania,Norway,Poland,theRussianFederation,Slovakia,southernandcentralSweden,Switzerland),correspondingtothedistributionofthetickreservoir.Thedis-easehasbeenknownbyseveralnames,includingRussianspring-summerencephalitis(RSSE),FarEasternencephalitisandcentralEuropeanencephalitis(CEE)(42).
Generallyrisktotheaveragetravellertoaffectedcountriesissmall.Infectionsarerelatedtoeitherleisureactivities suchashiking,walkingandhunting,orworking inagricultureand forestry inwarm,ruralorforestedpartsofendemicregions.Peopleatriskofinfectionincludeforesters,wood-cutters,farmers,militarypersonnel,laboratoryworkersandtouristswhocamp,huntandundertakefield-workinrural,forestedareas.
Pre-exposureprophylaxisisavailablewiththewholevirusinactivatedvaccines.Thestandardvac-cinationscheduleconsistsof2dosesgivenover4–12weeksapart,followedbyathirddose9–12monthslater.Inimmunocompetentadults,therateofseroconversionafter3dosesis85–100%.Forthoseatrisk,boostingisrecommendedevery3years.Therapidschedules19haveshownsimilaref-ficacyinhealthyindividualsandarepracticalfortravellers.WhethertherapidvaccinationscheduleiseffectiveinHIV-infectedpersonsisunknown.
OnlytwopublishedstudieshaveinvestigatedtheimmunogenicityofvaccinationinHIV-infectedpatients.ThesestudiessuggestthatthevaccineislessefficaciousinHIV-infectedindividualsthanthosenotinfectedwithHIV,particularlywithaCD4count<500cells/mm3.Althoughafour-dosevaccinationschedulegivenat0,1,2and9–12monthsmay improve responses inHIV-infectedpeople,evidenceinsupportofthisstrategyremainslimited(11).
19ForFSMEImmun:2doses14daysapartasprimarycourseandfollowedbyathirddose9-12monthslater;forEncepur:3dosesondays0,7and21asprimarycourseandfollowedbyafourthdose12-18monthslater.
453
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
2.11.1. Recommendations
• ImmunizationshouldbeconsideredforHIV-infectedpeoplewhointendtowalk,camporworkinheavilyforestedregionsofaffectedcountriesduringlatespringorsummerwhentheticksaremostactive,particularlyifstayinginareaswithheavyundergrowth.
• Thevaccineisalsorecommendedforexpatriateswhoseprincipalareaofresidenceisinanareawheretick-borneencephalitisisendemic.
• EitherthestandardortherapidvaccinationschedulemaybeconsideredforHIV-infectedpeoplewithaCD4count>400cells/mm3.
• InHIV-infectedindividualswithaCD4count<400cells/mm3,serologicaltestingmaybecon-sideredonemonthaftertheseconddose.
• Incaseofaninadequateantibodyresponse,twofurthervaccinedosesshouldbegiven,oneim-mediatelyandoneat9–12monthsafterthefirstdose.
• Intheabsenceofserologicaltesting,a4-dosevaccinationschedule(0,1,2and9–12months)shouldbeadoptedtoimproveresponserates(11).
• TheboosterrecommendationisthesameforHIV-infectedindividualsasforimmunocompetentpeople.
• Due to the possibility of reduced responses to vaccination in immunocompormisedHIV-in-fected individuals, the importance of protective clothing and insect repellent use should beemphasized.
2.12. Typhoid vaccine (Vi polysaccharide)HIV-infectedpeopleare at increased riskof infectionwithSalmonella species. In addition, im-munodeficiencypredisposes patients to bacteraemia, antibiotic resistance, relapsingdisease andpersistentinfection(11).
AparenteralkilledvaccinecomposedofpurifiedVipolysaccharide(from S. typhi)hasbeenshowntobemoderately(50–80%)effective(43),withonedoseadministeredsubcutaneouslyorintramus-cularly.Thevaccineconfersprotection7daysafterinjectionforatleast2years.Forpersonsatrisk,boostingisrecommendedevery3years.
2.12.1. Recommendations
• Owingtolowefficacyandhighratesofassociatedadverseevents,useofold,heatinactivatedwholecelltyphoidvaccineisnotrecommended,althoughthisvaccineisstillproducedinsomecountriesmainlyforeconomicreasons(43).
• Althoughnotrequiredforinternationaltravel,vaccinationwiththeVipolysaccharidevaccineisrecommendedforallHIV-infectedpeoplewhoareduetotraveltoareasinwhichthereisarecognizedriskofexposureandwhowillbeintimatewithadocumentedcarrier.
• Onedoseofthevaccineshouldbegivenatleast2weeksbeforetheexpectedexposure.• Abooster is recommendedevery3years in thosewhoremainat risk, this intervalmightbe
consideredtobereducedto2years,iftheCD4countis<200cells/mm3,astyphoidvaccinesarenot100%protectiveandresponsesmaybefurtherreducedinPLHIV.
• Travellersshouldbeadvisedtofollowstrictfoodanddrinkprecautions.
2.13. Other killed antigensOthervaccinescontainingkilledantigens,includingJapaneseencephalitis,plagueandanthrax,donotposearisktoPLHIV,regardlessoftheirimmunologicalstatus.
2.13.1. Recommendation
• ThesevaccinesshouldbeusedinthesamemannerasfornonHIV-infectedpeople.
454
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
3. Use of immunoglobulins
3.1. Hepatitis B immunoglobulin (HBIg)TemporaryimmunitymaybeobtainedusingHBIgforpost-exposureprophylaxis.HBIgisusedforpassiveimmunizationof:• newborninfantsofHBsAg-positivemothers;• peoplehavingpercutaneous,mucousmembraneorsexualexposuretoHBsAg-positivebloodor
bodyfluids;and• livertransplantpatients.
3.1.1. Recommendations
• Immunocompromisedpeople,includingPLHIV,shouldreceiveHBIgforthesameindicationsandinthesamedosesasimmunocompetentpeople.
• Asarule,HBIgshouldbeusedasanadjuncttohepatitisBvaccine.AllcandidatesforHBIgarebydefinitioninahigh-riskcategoryandshouldthereforebeconsideredforaconcurrenthepatitisBvaccineseries.
• ThepeopleforwhomHBIgisindicatedinclude: o prematureinfantswhoareborntoHBsAg-positivewomenandwomenwithunknownHB-
sAgstatus,andwhoshouldreceiveimmunoprophylaxiswithhepatitisBvaccineandmayreceiveHBIg20atorshortlyafterbirth;
o infantsborntoHBsAg-positivemothers,preferablywithin12hoursofbirthbutatadiffer-entsitefromthehepatitisBvaccination;
o HBsAg-negativepeoplewhodonotrespondtoHBVvaccine,andwhoshouldbecounselledonpreventingHBVinfectionandtheneedforHBIgprophylaxisagainstanypossibleparen-teralexposuretoHBsAg-positiveblood;
o susceptiblesexualcontactsofpeoplewithacuteHBVinfection,within14daysofthelastsexualcontact;21
o unvaccinated infantswhosemothersorprimarycaregivershaveacuteHBVinfection, inwhichcasethefirstdoseofthehepatitisBvaccineseriesshouldalsobegiven;22and
o peoplewhoarehouseholdcontactsofpeoplewithacuteHBVinfectionandwhohavebeenexposedtothebloodoftheinfectedperson(forexample,bysharingatoothbrushorrazor),inwhichcasetheyshouldalsobegiventhefirstdoseofthehepatitisBvaccineseries.23
3.2. Human normal immunoglobulin (HNIg)
3.2.1. Hepatitis A
3.2.1.1. Recommendations
• ForthepreventionofhepatitisA,24HNIgshouldbeadministeredinthesamewaytobothimmu-nocompromisedandimmunocompetentpeopleandforthesameindications(25).ConcurrentadministrationofHNIgandhepatitisAvaccinedoesnotappeartosignificantlyinfluencetheformationofprotectiveantibodies(23).
• HNIgisindicatedtopreventhepatitisAinthefollowinggroupsofpeople: o peopletravellingtohigh-riskareaslessthanfourweeksafteraninitialdoseofhepatitisA
vaccineshouldreceiveHNIgatadifferentsitefromthehepatitisAvaccination;
20Theprotectionagainstperinatallyacquiredinfectionachievedbyimmediate(within24hours)hepatitisBvaccinationisnotsignificantlyimprovedbytheadditionofHBIg(44).21Ifthelastsexualcontactwasmorethan14daysprior,hepatitisBvaccinationshouldbeinitiated,althoughtheamountofprotectionaffordedbypost-exposureprophylaxisgiventhislateisnotknown.HBIgisnotrecommendedinthissituation.22HBIgisnotneededforinfantswhohavereceivedorarescheduledtoreceiveaseconddoseofvaccine.23RoutinehepatitisBvaccinationshouldalsobeconsideredfornonsexualhouseholdcontactswithoutbloodexposure,espe-ciallychildrenandadolescents.24TopreventHAVinfection,administrationofHNIgisrecommendedbeforeorwithintwoweeksofHAVexposure.LateradministrationofHNIgoftenonlyattenuatestheclinicalexpressionofHAVinfection.
455
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
o childrenyoungerthan1travellingtohigh-riskareasshouldreceive0.02–0.06ml/kg,de-pendingonlengthofstay,sincehepatitisAvaccineisnotapprovedforchildrenyoungerthan1;
o peopleexposedtoHAVwhohavenotpreviouslyreceivedhepatitisAvaccine,whoshouldbegivenHNIgassoonaspossiblewithintwoweeksofexposure;
o peopleinclosecontactwithapersonwhohashepatitisA; o staffandchildrenatchildcarecentreswhereahepatitisAcasehasbeendiagnosed;and o peopleincertaincommon-sourceexposuresituations(forexample,patronsofafoodestab-
lishmentwithanHAV-infectedfoodhandlerwheretheriskoftransmissionisdeterminedtobehigh).
• PeoplewhoreceivedadoseofhepatitisAvaccineatleastonemonthbeforeanexposuredonotneedHNIg.
3.2.2. Measles
3.2.2.1. Recommendations
• For immunocompromisedpeople(including thosewithHIVinfection),HNIg is indicated topreventmeaslesfollowingexposure.
• Ifimmediateprotectionagainstmeaslesisrequiredforimmunocompromisedpatientswithcon-traindicationsformeaslesvaccination,includinginfantsyoungerthan1,passiveimmunizationwithHNIg0.5ml/kgofbodyweight(maximumdose15ml)shouldbeadministeredintramus-cularlyassoonaspossibleafterexposure.
• ExposedsymptomaticHIV-infectedpatientsshouldreceiveHNIgregardlessoftheirpreviousvaccinationstatus,asmeaslesvaccinemaynotbeeffectiveinsuchpatientsandthediseasemaybesevere.
• ForimmunocompromisedpeoplereceivingHNIgformeaslesprophylaxis,measlesvaccinationshouldbedelayedforsixmonthsfollowingHNIgadministration.
3.3. Human rabies immunoglobulin (HRIg)
3.3.1. Recommendations
• Immunocompromisedpatients,includingthosewithHIVinfection,shouldreceiveHRIgforthesameindicationsandinthesamedosesasimmunocompetentpatientsdo.
• HRIgis indicatedforCategoryIIIcontact(singleormultiple transdermalbitesorscratches,contaminationofmucousmembranewithsalivafromlicks),alongwith thefirstdoseof therabiesvaccineseries.
• HRIgtreatmentisnotnecessaryforpeoplevaccinatedagainstrabieswhohavedemonstratedneutralizingantibodytitresofatleast0.5IU/ml(twointramusculardosesofacell-derivedvac-cineseparatedbythreedaysaresufficientforsuchcases).
• If post-exposure treatment must be given to an immunocompromised HIV-infected person,HRIgismandatory,alongwiththefirstdoseofanintramuscularrabiesvaccineseries.
• Inaddition,theantibodyresponsesshouldbemonitoredserologically.Forfurtherdetails,seeAnnex3.

456
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
3.4. Tetanus immunoglobulin (TIg)
3.4.1. Recommendations
• TIgisrecommendedforpeoplewithtetanusandtopreventtetanusininadequatelyimmunizedpeoplewithwoundsorotherconditionsassociatedwithtetanus,regardlessoftheirHIVandim-munestatus.TIgneutralizescirculatingunboundtetanustoxin.Itdoesnotaffecttoxinthathasreachedthenervoussystem.
• DosageisthesameforPLHIVasforothers.• Forthetreatmentoftetanus,asingleintramusculardoseof3000–5000unitsisgenerallyrecom-
mendedforchildrenandadults.• IndicationsforTIgare: o woundsthatareneithercleannorminorinpeoplewhohavehadnomorethantwoprior
dosesofTd toxoid (vaccine)orwhohaveanuncertainhistoryofTIg immunization,Tdtoxoidsshouldalsobeadministered;25
o anyinjuryotherthanacleanminorwound,incombinationwithacontraindicationforteta-nustoxoid;or
o symptomsconsistentwithtetanusdisease.• Intravenousimmunoglobulin(IgIV)containstetanusantitoxinandmaybeusedifTIgisnot
available.
3.5. Varicella-zoster immunoglobulin (VZIg)ThemostimportantuseofVZIgisforpassiveimmunizationofneonatesandsusceptibleseverelyimmunocompromisedpeople,includingPLHIV,aftersignificantexposuretochickenpoxorzoster.ImmunocompromisedpatientswhoareexposedtovaricellaandreceiveVZIgmayhavelowerratesofcomplicationsandinfections.TherisksofVZIgappeartobenegligible,thoughthecostcanbesubstantial.
3.5.1. Recommendations
• Forprophylaxisofchickenpox,susceptibleHIV-infectedchildren(thosewhohavenohistoryofchickenpoxorshinglesorwhohavenodetectableVZVantibodies)shouldbeadministeredVZIgassoonaspossiblewithin96hoursafterclosecontactwithchickenpoxorshingles.
• VZIgisalsorecommendedforVZV-susceptibleHIV-infectedpregnantwomenwithin96hoursafterexposuretoVZV.Iforalaciclovirisused,VZVserologyshouldbeperformedsothatthedrugcanbediscontinuedifthepatientisseropositiveforVZV(25).
25Earlydosesoftoxoiddonotinduceimmunity,butonlyprimetheimmunesystem.TheTIgprovidestemporaryimmunitybydirectlyprovidingantitoxin,ensuringthataprotectivelevelofantitoxinisachievedevenifanimmuneresponsehasnotyetoccurred.
457
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
Annex1.Summaryofimmunizationrecommenda-tionsforpeopleimmunocompromisedduetoHIV/AIDS
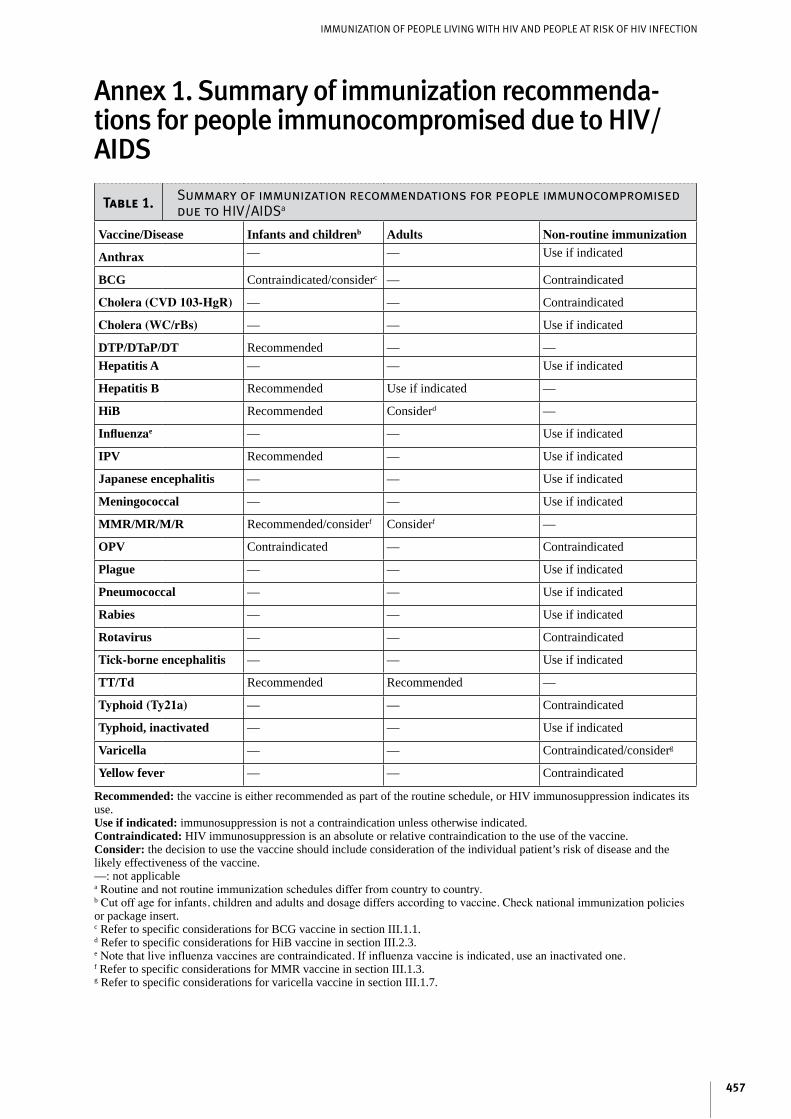
Table 1. Summary of immunization recommendations for people immunocompromised due to HIV/AIDSa
Vaccine/Disease Infants and childrenb Adults Non-routine immunization
Anthrax — — Useifindicated
BCG Contraindicated/considerc — Contraindicated
Cholera (CVD 103-HgR) — — Contraindicated
Cholera (WC/rBs) — — Useifindicated
DTP/DTaP/DT Recommended — —Hepatitis A — — Useifindicated
Hepatitis B Recommended Useifindicated —
HiB Recommended Considerd —
Influenzae — — Useifindicated
IPV Recommended — Useifindicated
Japanese encephalitis — — Useifindicated
Meningococcal — — Useifindicated
MMR/MR/M/R Recommended/considerf Considerf —
OPV Contraindicated — Contraindicated
Plague — — Useifindicated
Pneumococcal — — Useifindicated
Rabies — — Useifindicated
Rotavirus — — Contraindicated
Tick-borne encephalitis — — Useifindicated
TT/Td Recommended Recommended —
Typhoid (Ty21a) — — Contraindicated
Typhoid, inactivated — — Useifindicated
Varicella — — Contraindicated/considerg
Yellow fever — — Contraindicated
Recommended:thevaccineiseitherrecommendedaspartoftheroutineschedule,orHIVimmunosuppressionindicatesitsuse.Use if indicated:immunosuppressionisnotacontraindicationunlessotherwiseindicated.Contraindicated:HIVimmunosuppressionisanabsoluteorrelativecontraindicationtotheuseofthevaccine.Consider:thedecisiontousethevaccineshouldincludeconsiderationoftheindividualpatient’sriskofdiseaseandthelikelyeffectivenessofthevaccine.—:notapplicableaRoutineandnotroutineimmunizationschedulesdifferfromcountrytocountry.bCutoffageforinfants,childrenandadultsanddosagediffersaccordingtovaccine.Checknationalimmunizationpoliciesorpackageinsert.cRefertospecificconsiderationsforBCGvaccineinsectionIII.1.1.dRefertospecificconsiderationsforHiBvaccineinsectionIII.2.3.eNotethatliveinfluenzavaccinesarecontraindicated.Ifinfluenzavaccineisindicated,useaninactivatedone.fRefertospecificconsiderationsforMMRvaccineinsectionIII.1.3.gRefertospecificconsiderationsforvaricellavaccineinsectionIII.1.7.
458
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
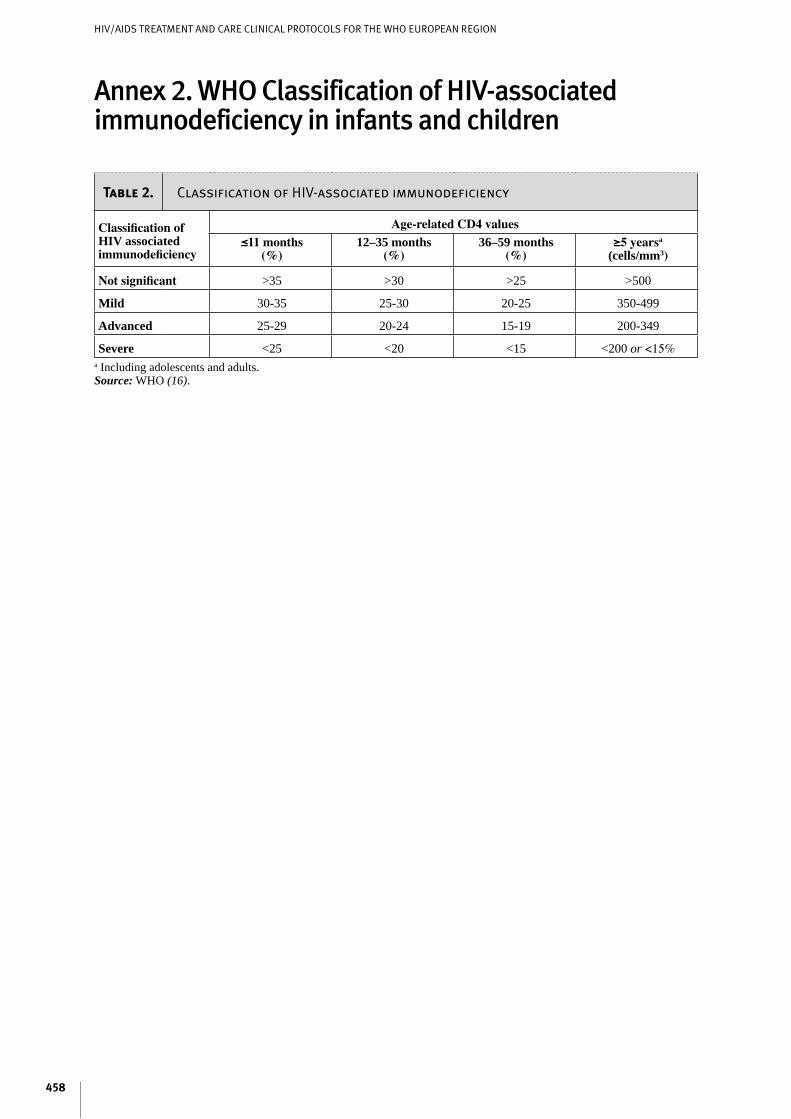
Annex2.WHOClassificationofHIV-associatedimmunodeficiencyininfantsandchildren
Table 2. Classification of HIV-associated immunodeficiency
Classification of HIV associated immunodeficiency
Age-related CD4 values≤11 months
(%)12–35 months
(%)36–59 months
(%)≥5 yearsa
(cells/mm3)
Not significant >35 >30 >25 >500
Mild 30-35 25-30 20-25 350-499
Advanced 25-29 20-24 15-19 200-349
Severe <25 <20 <15 <200or<15%aIncludingadolescentsandadults.Source:WHO(16).

459
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
Annex3.RabiesvaccinesPre-exposurerabiesvaccinationmaybeperformedwithanyofthemoderncell-derivedvaccinesandisrec-ommendedforanyoneatriskforexposuretorabiesvirus.Traditionally,thisrecommendationincludes:• laboratorystaff• veterinarians• animalhandlers• wildlifeofficerswithfrequentexposuretopotentiallyinfectedanimals• visitorstohighlyrabies-enzooticareas26whomaybeexposedtorabieshosts.27
Thepre-exposurescheduleofmoderncell-derivedrabiesvaccinesrequiresintramusculardosesof1mlor0.5ml,dependingonthevaccine,givenonDays0,7and28.28Theindicationforpost-exposurevaccina-tionwiththesevaccines(withorwithoutrabiesimmunoglobulin)dependsonthetypeofcontactwiththerabidanimal.29Dependingonvaccinetype,thepost-exposurescheduleprescribesintramusculardosesof1mlor0.5mlgivenas4–5dosesoverfourweeks.Forrabies-exposedpatientswhohavepreviouslyunder-gonecompletepre-exposurevaccinationorpost-exposuretreatmentwithcell-derivedrabiesvaccines,twointramusculardosesofacell-derivedvaccineseparatedbythreedaysaresufficient.Rabiesimmunoglobulintreatmentisnotnecessaryinsuchcases.Thesamerulesapplytopeoplevaccinatedagainstrabieswhohavedemonstratedneutralizingantibodytitresofatleast0.5IU/ml.
Thehumandiploidcellrabiesvaccineisregardedasthegoldstandardforcell-derivedrabiesvaccines.30TheWHOrequirementisapotencyofatleast2.5IUperintramusculardoseforallcell-derivedvaccines.Despitetheuseofpotent,moderncell-derivedvaccines,aboutonefailureinonemillionpost-exposuretreatmentsdoesoccur.Carefulanalysesshowthatsuchfailuresarealmostalwaysassociatedwithseverelesionsonorneartheheadand/orinappropriateadministrationofthetreatment.
Acompletepost-exposuretreatmentusingnervetissuevaccinesinvolvesaprolongedandpainfulimmuniza-tioncourseofupto23injections.Furthermore,protectivepotencynervetissuevaccinesareinferiortomod-erncell-derivedvaccines.Obviously,thesevaccinesarenotrecommendedforpre-exposureimmunization.
26Morethan2.5billionpeopleliveinregionswhererabiesisendemic,inAfrica,AsiaandSouthAmerica.Itisestimatedthateachyearatleast50000peoplediefromrabies,andthatmorethan10millionreceivepost-exposurevaccination.Childrenaged5–15yearsareatparticularrisk(23).27Accordingtoage-stratifiedstudiesofincidence,thoseatgreatestriskareprobablychildrenlivinginrabies-enzooticregionsofthedevelopingworld(23).28Majorvaccinemanufacturersrecommendoneboosterdoseafteroneyear,andtoensureprotectioninpeopleatcontinuedrisk,boostervaccinationseveryfiveyears,orideally,atintervalsdictatedbyregulartestingforrabiesantibodies(titres>0.5IU/mlrequiredforprotection).29ThetypesofcontactareCategoryI:touchingorfeedinganimals,orlicksontheskin;CategoryII:nibblingofuncoveredskin,minorscratchesorabrasionswithoutbleeding,orlicksonbrokenskin;andCategoryIII:singleormultipletransdermalbitesorscratches,orcontaminationofamucousmembranewithsalivafromlicks.ForCategoryI,notreatmentisrequired;forCategoryII,immediatevaccinationisrecommended;andforCategoryIII,immediatevaccinationandadministrationofrabiesimmunoglobulinarerecommended,inadditiontoimmediatewashingandflushingofallbitewoundsandscratches.30Othercell-derivedrabiesvaccinesareverocellandpurifiedchickembryocellvaccines.Noclinicallyimportantdifferenceswereobservedwhenthesevaccineswereevaluatedtogetherwithhumandiploidcellvaccinesinstudiesonbothpost-exposureprotectionandpre-exposureimmunogenicity(23).
460
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
Annex4.GlossaryActive immunity isusuallypermanentprotectionproducedbyaperson’sownimmunesystem.Onewaytoacquireactiveimmunityistohavethenaturaldisease.Ingeneral,oncepatientsrecoverfrominfectiousdiseases,theywillbeimmunetothosediseasesfortherestoftheirlives.
Antibodiesareproteinsthatareproducedbytheimmunesysteminresponsetospecificantigens,therebyhelpingthebodyfightinfectionandforeignsubstances.
Antigensaresubstances,foreigntothebody,thatstimulatetheproductionofantibodiesbytheimmunesys-tem.Antigenscaneitherbelive(suchasvirusesandbacteria)orinactivated.
Anantitoxinisasolutionofantibodies(forexample,diphtheriaantitoxinandbotulinumantitoxin)derivedfromtheserumofanimalsimmunizedwithspecificantigens.Antitoxinsareusedforconferringpassiveim-munityandfortreatmentandareusuallypermanent.
Anasymptomatic HIV-infected personisonewithaconfirmedHIVdiagnosisbutwithnoclinicalsignsorsymptomsoftheinfection,correspondingtoWHOClinicalStage1.(Forstaging,seeProtocol1,Patient evaluation and antiretrovital treatment for adults and adolescents,Annex2, andProtocol11,Paediatric HIV/AIDS treatment and care,Annex1).
Acontraindication isaconditioninarecipient thatgreatly increases thelikelihoodofaseriousadversereaction that could seriouslyharm the recipient. Ingeneral,vaccines shouldnotbeadministeredwhenacontraindicatedconditionispresent.
Animmune responseisthedefencethattheimmunesystemdevelopsagainstantigens.Itusuallyinvolvestheproductionofproteinmolecules,antibodies(orimmunoglobulins),andofspecificcells(alsoknownascell-mediated immunity)whosepurposeistofacilitatetheeliminationofforeignsubstances.
Theimmune systemisacomplexsystemofinteractingcellswhoseprimarypurposeistoidentifyforeignsubstancesreferredtoasantigens,andtodefenditagainstinfection,diseaseandotherforeignsubstances.Thebody’simmunesystemnaturallyproducesantibodiesinthisdefenceprocess.
Immunityistheabilityofthehumanbodytotoleratethepresenceofmaterialindigenoustothebodyandtoeliminateforeignmaterial.Thisdiscriminatoryabilityprovidesprotectionfrominfectiousdisease,sincetheimmunesystemidentifiesmostmicrobesasforeign.Immunitytoamicrobeisusuallyindicatedbythepresenceofanantibodytothatorganism.Immunityisgenerallyveryspecifictoasingleorganismorgroupofcloselyrelatedorganisms.Therearetwobasicmechanismsforacquiringimmunity,activeandpassive.
Immunoglobulin (Ig)isasterilesolutioncontainingantibodiesfromhumanblood,alsoknownashumannormal immunoglobulin (HNIg), immune serum globulin (ISG) or gamma globulin (IgG). Ig is used topreventthespreadofsomediseasesamongpeoplewhoareinclosecontactwitheachother.Intendedforintramuscularadministration,itisprimarilyindicatedforroutinemaintenanceofimmunityamongcertainimmunodeficientpeopleandforpassiveimmunizationagainstmeaslesandhepatitisA.IgdoesnottransmithepatitisBvirus,HIVorotherinfectiousdiseases.
Immunizationisaninclusivetermdenotingtheprocessofinducingorprovidingimmunityartificiallybyadministeringanimmunobiologicalproduct.Immunizationcanbeactiveorpassive.Active immunizationistheproductionofantibodyorotherimmuneresponsesthroughtheadministrationofavaccineortoxoid.Passive immunizationistheprovisionoftemporaryimmunitybytheadministrationofpreformedantibod-ies,suchasimmunoglobulinsandantitoxins.

461
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
Immunologic memoryispersistentprotectionformanyyearsafteraninfection.Followingexposureoftheimmunesystemtoanantigen,certaincells(memoryB-cells)continuetocirculateintheblood(andalsointhebonemarrow)formanyyears.Uponexposuretotheantigen,thesememorycellsbegintoreplicateandproduceveryrapidlytore-establishprotection.
Immunosuppression is thesuppressedimmunestatusofanindividualcausedbydiseases(suchasHIV/AIDS,congenitalimmunodeficiency,leukaemia,lymphomaorgeneralizedmalignancy)ordrugs(suchasalkylatingagents,antimetabolitesorradiationtherapy).ThelevelofimmunosuppressioncanbemeasuredbyCD4countorbyCD4percentageoftotallymphocytes.
Inactivated vaccinescanbecomposedofwholevirusesorbacteria,orfractionsofeither.Fractionalvac-cinesareeitherprotein-basedorpolysaccharide-based.Protein-basedvaccinesincludetoxoids(inactivatedbacterial toxins)andsubunitorsubvirionproducts.Mostpolysaccharide-basedvaccinesarecomposedofpurecell-wallpolysaccharidefrombacteria.Conjugatepolysaccharidevaccinesarethoseinwhichthepoly-saccharideischemicallylinkedtoaprotein.Thislinkagemakesthepolysaccharideamorepotentvaccine.Vaccineantigensmayalsobeproducedbygeneticengineeringtechnology.Theseproductsaresometimesreferredtoasrecombinantvaccines.
Intravenous immunoglobulin (IgIV)isaproductderivedfrombloodplasmafromadonorpoolsimilartotheIgpool,butpreparedsoitissuitableforintravenoususe.IgIVdoesnottransmitinfectiousdiseases.Itisprimarilyusedforreplacementtreatmentinprimaryantibody-deficiencydisordersandforthetreatmentofKawasakidisease, immunethrombocytopenicpurpura,hypogammaglobulinaemiainchronic lymphocyticleukaemia,andsomecasesofHIVinfection.
Live attenuated vaccinesareproducedbymodifyingadisease-producing(“wild”)virusorbacteria inalaboratory.Theresultingvaccineorganismretainstheabilitytoreplicateandproduceimmunity,butitusu-allydoesnotcauseillness.
Passive immunity isprotectionbyproductsproducedbyananimaloranotherhumanand transferred totherecipient,usuallybyinjection.Passiveimmunityoftenprovideseffectiveprotection,butthisprotectionwanesovertime,usuallyafewweeksormonths.
Specific immunoglobulinsarespecialpreparationsobtainedfrombloodplasmafromdonorpoolsprese-lectedforhighantibodycontentagainstaspecificantigen(forexample,hepatitisBimmunoglobulin,vari-cella-zosterimmunoglobulin,rabiesimmunoglobulinortetanusimmunoglobulin).LikeIgandIgIV,thesepreparationsdonottransmitinfectiousdiseases.
Asymptomatic HIV-infected person isapersonpresentingwithsignsandsymptomsofHIVinfection.Mild,advancedandsevereHIVdiseasecorrespondstoWHOClinicalStages2,3and4,respectively(seeAnnex2andtheannexesmentionedunder“asymptomaticHIV-infectedperson”above).
Atoxoidisamodifiedbacterialtoxinthathasbeenmadenon-toxicbutretainstheabilitytostimulatetheformationofantitoxin.
Vaccinationisthephysicalactofadministeringanyimmunobiologicalagent(vaccine,toxoidorimmuno-globulin)toapersontoproduceactiveimmunity.
Vaccineisasuspensionoflive(usuallyattenuated)orinactivatedmicroorganisms(e.g.bacteria,virusesorrickettsiae)or fractions thereof,administered to induce immunityandprevent infectiousdiseasesor theirconsequences.Somevaccinescontainhighlydefinedantigens(suchasthepolysaccharideofHaemophilus influenzatypeborthesurfaceantigenofhepatitisB);otherscontainantigensthatarecomplexorincom-pletelydefined(forexample,killedBordetella pertussisorliveattenuatedviruses).Vaccinesinteractwiththe

462
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
immunesystemandoftenproduceanimmuneresponsesimilartothatproducedbythenaturalinfection,butdonotsubjecttherecipienttothediseaseanditspotentialcomplications.Vaccinesproduceimmunologicalmemorysimilartothatacquiredbyhavingthenaturaldisease.

463
ImmunIzatIon of PeoPle lIvIng wIth hIv and PeoPle at RIsk of hIv InfectIon
References1. Onorato IM,Markowitz LE, OxtobyMJ. Childhood immunization, vaccine-preventable diseases
andinfectionwithhumanimmunodeficiencyvirus.The Pediatric Infectious Disease Journal,1988,6:588–595.
2. OpravilMetal.Poorantibodyresponseaftertetanusandpneumococcalvaccinationinimmunocom-promised,HIV-infectedpatients.Clinical and Experimental Immunology,1991,84(2):185–189.
3. BorkowskyWetal.Antibodyresponsestobacterialtoxoidsinchildreninfectedwithhumanimmu-nodeficiencyvirus.The Journal of Pediatrics,1987,110:563–566.
4. HuangKLetal.AntibodyresponsesafterinfluenzaandpneumococcalimmunizationinHIV-infectedhomosexualmen.JAMA,1987,257:2047–2050.
5. KleinRSetal.ResponsestopneumococcalvaccineamongasymptomaticheterosexualpartnersofpersonswithAIDSandintravenousdrugusersinfectedwithhumanimmunodeficiencyvirus.Journal of Infectious Diseases,1989,160:826–831.
6. TB/HIV: a clinical manual,2nded.Geneva,WorldHealthOrganization,2004.7. GlobalAdvisoryCommitteeonVaccineSafety.SafetyofBCGvaccinationinimmunocompromised
individuals. Weekly Epidemiological Record, 2003, 32(8):283 (http://www.who.int/wer/2003/en/wer7832.pdf,accessed25June2006).
8. UnitedStatesCentersforDiseaseControl.DisseminatedMycobacterium bovisinfectionfromBCGvaccinationofapatientwithacquiredimmunodeficiencysyndrome.MMWR,1985,34:227–228.
9. NinaneJetal.DisseminatedBCGinHIVinfection.Archives of Disease in Childhood,1988,63:1268–1269.
10. BroekmansJFetal.Europeanframeworkforturberculosiscontrolandeliminationincountrieswithlowincidence.TheEuropean Respiratory Journal,2002,19(4):765–775.
11. British HIV Association immunization guidelines for HIV-infected adults.London,BritishHIVAs-sociation,FirsteditionApril2006.(http://www.bhiva.org,accessed16November2006).
12. CentersforDiseaseControl.Measlespneumonitisfollowingmeasles-mumps-rubellavaccinationofapatientwithHIVinfection,1993.MMWR,1996,45(28):603–606.
13. PalumboPetal.Population-basedstudyofmeaslesandmeaslesimmunizationinhumanimmunode-ficiencyvirus-infectedchildren.The Pediatric Infectious Disease Journal,1992,11(12):1008–1014.
14. AtkinsonW,HamborskyJ,WolfeS,eds.Epidemiology and prevention of vaccine-preventable dis-eases,8thed.Washington,DC,PublicHealthFoundation,2005.
15. CentersforDiseaseControl.1993revisedclassificationsystemforHIVinfectionandexpandedsur-veillancecasedefinition forAIDSamongadolescents andadults.MMWR: Recommendations and Reports,1992,41(RR-17):1–19.
16. Antiretroviral therapy of HIV infection in infants and children in resource-limited settings: towards universal access: recommendations for a public health approach: 2006.Geneva,WorldHealthOr-ganization, 2006 (http://www.who.int/hiv/pub/guidelines/WHOpaediatric.pdf, accessed 21 August2006).
17. AtkinsonWLet al.General recommendationson immunization: recommendationsof theAdviso-ryCommitteeonImmunizationPractices(ACIP)andtheAmericanAcademyofFamilyPhysicians(AAFP).MMWR: Recommendations and Reports,2002,51(RR-2):1–35.
18. EPIvaccinesinHIV-infectedindividuals:thesafetyofEPI-recommendedvaccinesinHIV-infectedindividuals.Geneva,WorldHealthOrganization,2001(http://www.who.int/vaccines-diseases/diseas-es/HIV.shtml,accessed6December2004).
19. SixbeyJW.Routineimmunizationandtheimmunosuppressedchild.Advances in Pediatric Infectious Diseases,1987,2:79–114.
20. WrightPFetal.Vaccine-associatedpoliomyelitis inachildwithsex-linkedagammaglobulinemia.The Journal of Pediatrics,1977,91:408–412.
21. Wyatt HV. Poliomyelitis in hypogammaglobulinemics. Journal of Infectious Diseases, 1973,128(6):802–806.
22. DavisLEetal.Chronicprogressivepoliomyelitissecondarytovaccinationofanimmunodeficientchild.The New England Journal of Medicine,1977,297(5):241–245.
23. Core information for the development of immunization policy: 2002 update: Expanded Programme on Immunization of the Department of Vaccines and Biologicals.Geneva,WorldHealthOrganiza-
464
hIv/aIds tReatment and caRe clInIcal PRotocols foR the who euRoPean RegIon
tion,2003(http://www.who.int/vaccines-documents/DocsPDF02/www557.pdf,accessedon29June2006).
24. ArmenianSHetal.Safetyandimmunogenicityoflivevaricellavirusvaccineinchildrenwithhumanimmunodeficiencyvirustype1.The Pediatric Infectious Disease Journal,2006,25(4):368–370.
25. CentersforDiseaseControl.RecommendationsoftheAdvisoryCommitteeonImmunizationPrac-tices (ACIP): use of vaccines and immunoglobulins in personswith altered immunocompetence.MMWR: Recommended Reports,1993,42(RR-4):1–18.
26. LewisDJetal.ImmuneresponsefollowingoraladministrationofcholeratoxinBsubunittoHIV-1-infectedUKandKenyansubjects.AIDS1994;8:779-785.
27. Sanchez JL et al. Protective efficacy of oralwhole-cell/recombinant-B-subunit cholera vaccine inPeruvianmilitaryrecruits.Lancet1994;344:1273-1276.
28. WHO.WHOpositionpaper.Weekly Epidemiological Record.20April2001.No.16,2001,76,117-124.(http://www.who.int/topics/cholera/vacccines/en/index.html,accessed21September2006).
29. FarlyMMetal.InvasiveHaemophilus influenzaediseaseinadults:aprospective,population-basedsurveillance.Annals of Internal Medicine,1992,116:806–812.
30. SteinhartRetal.InvasiveHaemophilus influezaeinfectionsinmenwithHIVinfection.JAMA,1992,268(23):3350–3352.
31. VanDammePetal.HepatitisAboostervaccination:isthereaneed?The Lancet,2003,362(9389):1065–1071.
32. FrequentlyaskedquestionsabouthepatitisA.Atlanta,CentersforDiseaseControlandPrevention,2006(http://www.cdc.gov/ncidod/diseases/hepatitis/a/faqa.htm,accessedon22June2006).
33. Vaccine-preventable diseases, vaccines and vaccination. In:Nuttall I, ed. International travel and health: situation as on 1 January 2005.Geneva,WorldHealthOrganization,2005:103–104(http://whqlibdoc.who.int/publications/2005/9241580364_chap6.pdfaccessedon29June2006).
34. TedaldiEetal.HepatitisAandBvaccinationpracticesforambulatorypatientsinfectedwithHIV.Clinical Infectious Diseases,2004;38:1478–1484.
35. WelchK,MorseA.ImprovingscreeningandvaccinationforhepatitisBinpatientscoinfectedwithHIVandhepatitisC.American Journal of Gastroenterology,2002,97:2928–2929.
36. HodgesGRetal.ResponsetoinfluenzaAvaccineamonghigh-riskpatients.Southern Medical Jour-nal,1979,72(1):29–32.
37. SafrinS,RushJD,MillJ.Influenzainpatientswithhumanimmunodeficiencyvirusinfection.Chest,1990,98:33–37.
38. GrossPAetal.Influenzaimmunizationinimmunosuppressedchildren.Journal of Pediatrics,1978,92(1):30–35.
39. AdvisoryCommitteeonImmunizationPractices(ACIP).Vaccine side-effects, adverse reactions, con-traindications and precautions.Atlanta,CentersforDiseaseControl,1996.
40. LandesmanSH,SchiffmanG.Assessmentoftheantibodyresponsetopneumococcalvaccineinhigh-riskpopulations.Reviews of Infectious Diseases,1981,3(Suppl.):S184–S197.
41. CentersforDiseaseControl.Preventionofpneumococcaldisease:recommendationsoftheAdvisoryCommitteeonImmunizationPractices(ACIP).MMWR:Recommended Reports,1997,46(RR-08):1–24(http://www.cdc.gov/mmwr/PDF/rr/rr4608.pdfaccessed14November2006).
42. Requirementsfortick-borneencephalitisvaccine(inactivated)2.In:WHOExpertCommitteeonBio-logicalStandardization.WHO Expert Committee on Biological Standardization: forty-eighth report.Geneva,WorldHealthOrganization,1999:4463(WHOTechnicalReportSeries889;http://www.who.int/biologicals/publications/trs/areas/vaccines/tick_encephalitis/WHO_TRS_889_A2.pdf, accessed16November2006).
43. WHO.WHOpositionpaper.Weekly Epidemiological Record.2000,32(75):257–264(http://www.who.int/wer,accessed21September2006).
44. WHOpositionontheuseofhepatitisBvaccines.Weekly Epidemiological Record,2004,28(79):255–263(http://www.who.int/wer/2004/en/wer7928.pdfaccessed25June2006).