nigel north clinical psychologist/neuropsychologist
TRANSCRIPT
Nigel NorthClinical Psychologist/Neuropsychologist
Almost 66% of beds are occupied by people over the age of 65
Increasing interest in improving acute hospital care for older people
Loss of autonomy, independence, mood disorder are issues for older people in acute medical wards
(DOH 2001, 2003, 2004)
A number of studies have identified psychosocial issues as influencing length of stay, engagement in rehabilitation and morbidity
These issues include depression, anxiety and cognitive problems
Other issues identified include, loss of control over environment, a reduction in meaningful and valued activity, loss of mobility and independence
(Siebens et al 2000, Eyres and Unsworth 2005, DOH 2008, Callum et al 2008)
A variety of physical health conditions associated with depression: Stroke, CHD, Diabetes, Cancer (NICE 2009)
Depression common in people with dementia (Baylor et al 2000) (62%)
Depression associated with a 50% increase in financial costs of medical care (Katon 2003)
Mood disorder may lead to deterioration in some conditions (Stroke, CHD, Diabetes) (NICE 2009). Cause vs consequence
Significant numbers of older people in hospital have depressive symptoms that may hinder their recovery (Cullum et al 2008)
Detection of Psychosocial Problems is poor (Jenkins et al 2010)
Adverse outcomes resulting from this may include:› Delayed Discharge (Holmes & House 2000)› Greater risk of readmission (Koenig 1999)› Higher mortality (Cullum et al 2008)› Functional status and cognitive decline predictive of LOS, Mortality, discharge destination (Campbell et al 2004)
Medication› Costs› Side effects
Psychological therapy› 1:1› Group› IAPT› Numbers of people to ‘treat’› Numbers of ‘Therapists’ required
Aim: › To increase social engagement› Provide cognitive and intellectual stimulation
› Improve well being and mood
Delivered by voluntary assistant psychologists
Rota for each week day (3 people for half a day)
One to one Group Designed to meet individuals needs and level of functioning
Medical Ward and Stroke Ward
Communication skills Psychological therapy skills (basic)
Education (dementia, neuroscience, values)
Problem solving skills Detection/Recognition of psychological disorder
‘Social Games’ (Bingo, Scrabble, Cards, Word and Number ‘Games’
Newspaper discussion groups Conversation groups Reminiscence (group/individual) Cognitive Retraining Approaches (Quiz, Crosswords, ‘Brain Training’)
Voluntary participation but all approached unless ward indicated otherwise
Assessment of Mood (Brief Assessment Schedule Depression Cards , BASDEC)
Satisfaction Questionnaires, 5 point scale (Activities, Ward Environment, Care)
Length of Stay (LOS) June 2010 – April 2011 LOS assessed two months before and two months after intervention
1. No of participants 110 (82 males, 28 females)
2. Average Age: 80.4 years (SD = 9.7)3. Significant reduction in depression
between pre and post assessment (67 vs 13)
4. Significant increase in satisfaction with activities available on the ward
5. Significant increase in patient satisfaction with ward environment
6. Significant increase in satisfaction with care provided on the ward
42 ‘Mild’ Cognitive Impairment 18 Moderate Cognitive Impairment ?Dementia?
“The activities were so very useful and helpful”
“The chats and cards were really good”
“I enjoyed the hand massage and chatting, it makes the day go quicker”
“This has been really good, I wish I could see them after I leave here”
“I enjoyed the activities, particularly a good chat”
“I am usually so lonely with no-one to talk to, everyone is so busy doing their work, I really appreciate having these people coming in”
“I have made new friends here through the conversation groups”
“It made me feel more alive, more alert, more me”
“It’s great, it really adds something to the day, you feel more useful, more involved”
Collected by the hospital in hours
Data for two months prior to the start of the project and for a follow up period of two months after it
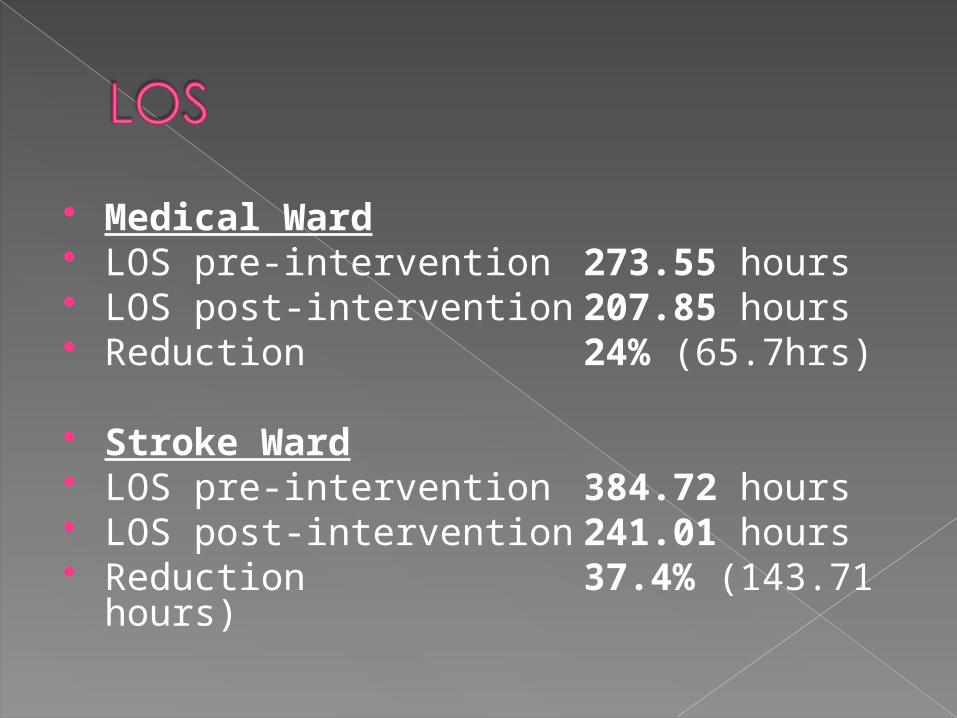
Medical Ward LOS pre-intervention 273.55 hours LOS post-intervention 207.85 hours Reduction 24% (65.7hrs)
Stroke Ward LOS pre-intervention 384.72 hours LOS post-intervention 241.01 hours Reduction 37.4% (143.71 hours)
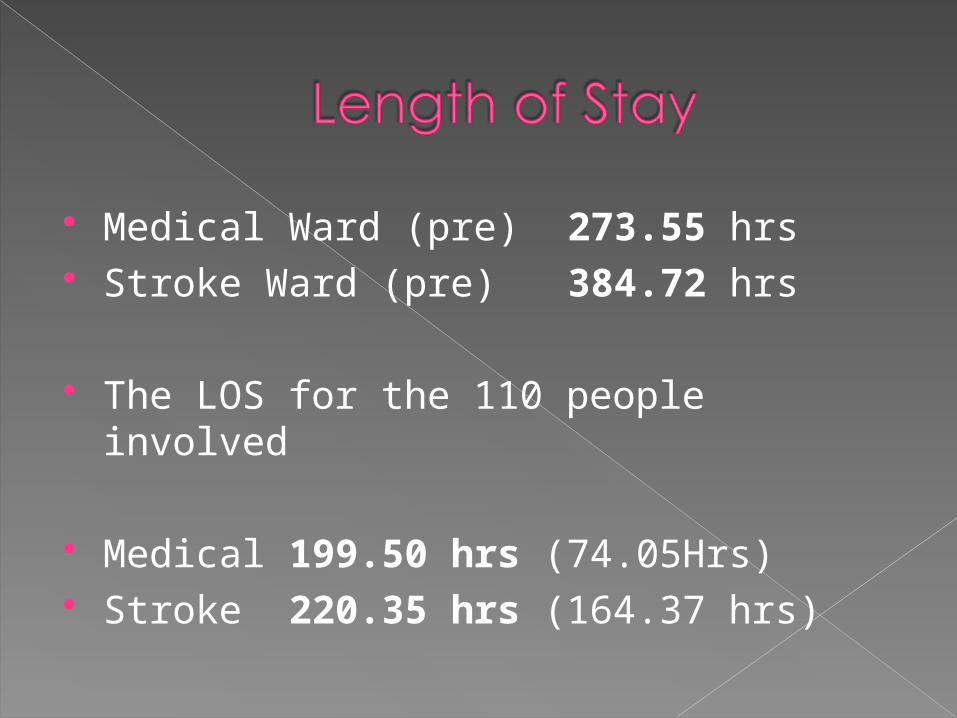
Medical Ward (pre) 273.55 hrs Stroke Ward (pre) 384.72 hrs
The LOS for the 110 people involved
Medical 199.50 hrs (74.05Hrs) Stroke 220.35 hrs (164.37 hrs)
The project improves mood The project improves satisfaction ?? Length of Stay Costs are negligible. The project was run by volunteers of which we have hundreds. Three hours of training was given to the volunteers at the beginning of the project and five hours of supervision given during the project (Total of 8 hours of an assistant psychologist’s time = £96
To be continued………